The Role of Adult Children of Immigrants in the U.S. Health Care Workforce
Introduction
Immigrants and their children form a growing share of the U.S. population and make important contributions to the country’s culture, economy, and workforce. One of the major reasons why immigrants come to the U.S. is for improved educational and employment opportunities for their children. Many children of immigrants realize their parents’ dreams by attaining high levels of education and jobs that allow for an improved quality of life. Adult children of immigrants also play an important role in supporting the U.S. workforce and economy, particularly in certain sectors, including health care. This brief examines key characteristics of nonelderly adult children of immigrants and their role in the workforce, including the health care workforce, based on KFF analysis of 2023 Current Population Survey data (see Methods for details). All differences described in the text are statistically significant at p<0.05. Key takeaways include the following:
- Nonelderly adult children of immigrants are more likely than those with U.S.-born parents to be under age 35 and to be Hispanic or Asian. Six in ten (62%) nonelderly adult children of immigrants are under age 35 and three-quarters are Hispanic (55%) or Asian (22%). In comparison, about four in ten (37%) of nonelderly adults with at least one U.S.-born parent are under 35 years and one in ten is Hispanic (9%) or Asian (1%). About three in ten (28%) nonelderly adults who are immigrants themselves are under 35 years and three-quarters are Hispanic (49%) or Asian (25%).
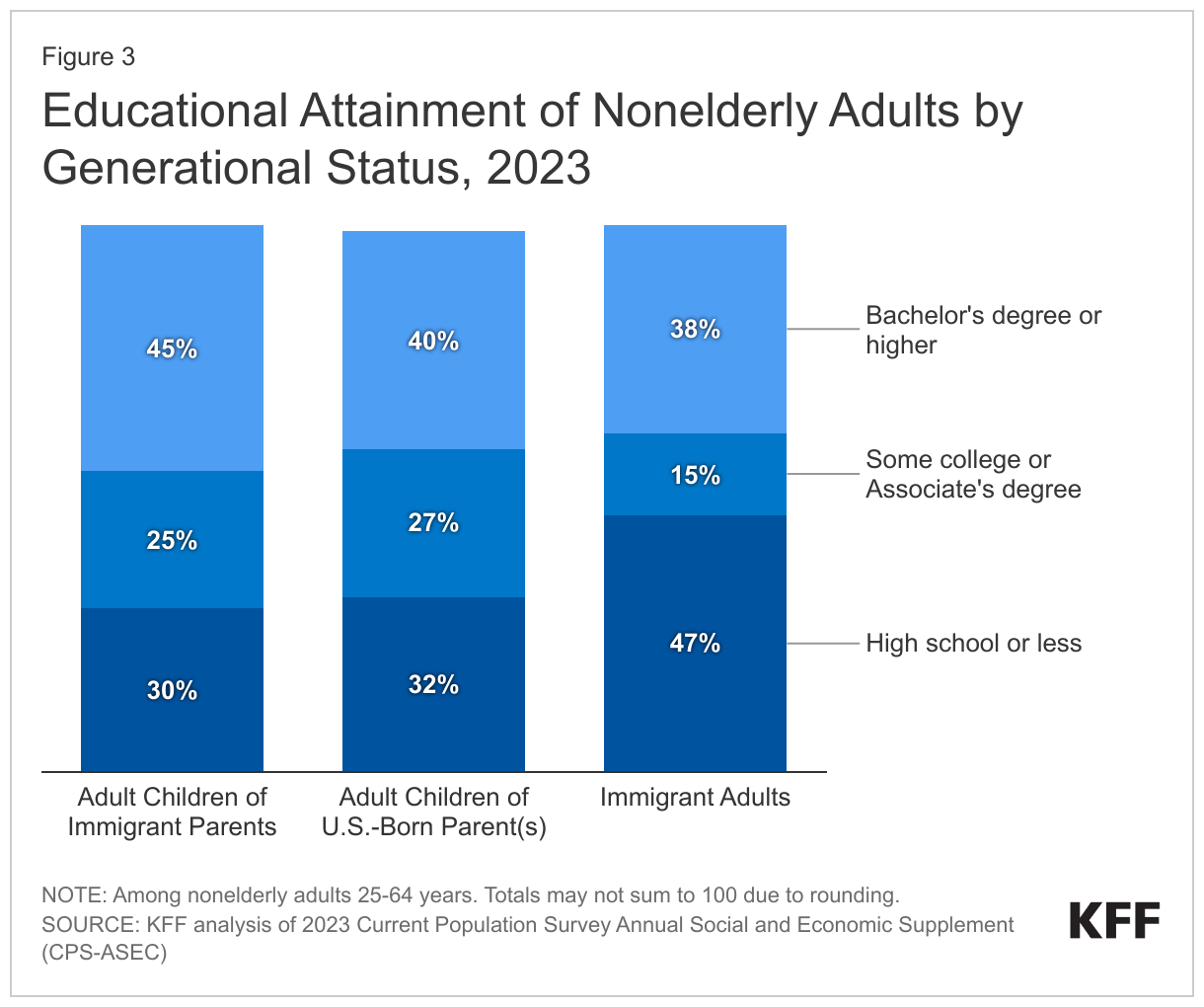
- Nonelderly adult children of immigrants have somewhat higher educational attainment compared to their peers with U.S.-born parents and immigrant adults. Among those ages 25 to 64 (who are less likely to be students), over four in ten (45%) adult children of immigrants have a bachelor’s degree or higher compared with 40% of those with at least one U.S.-born parent and 38% of immigrant adults.
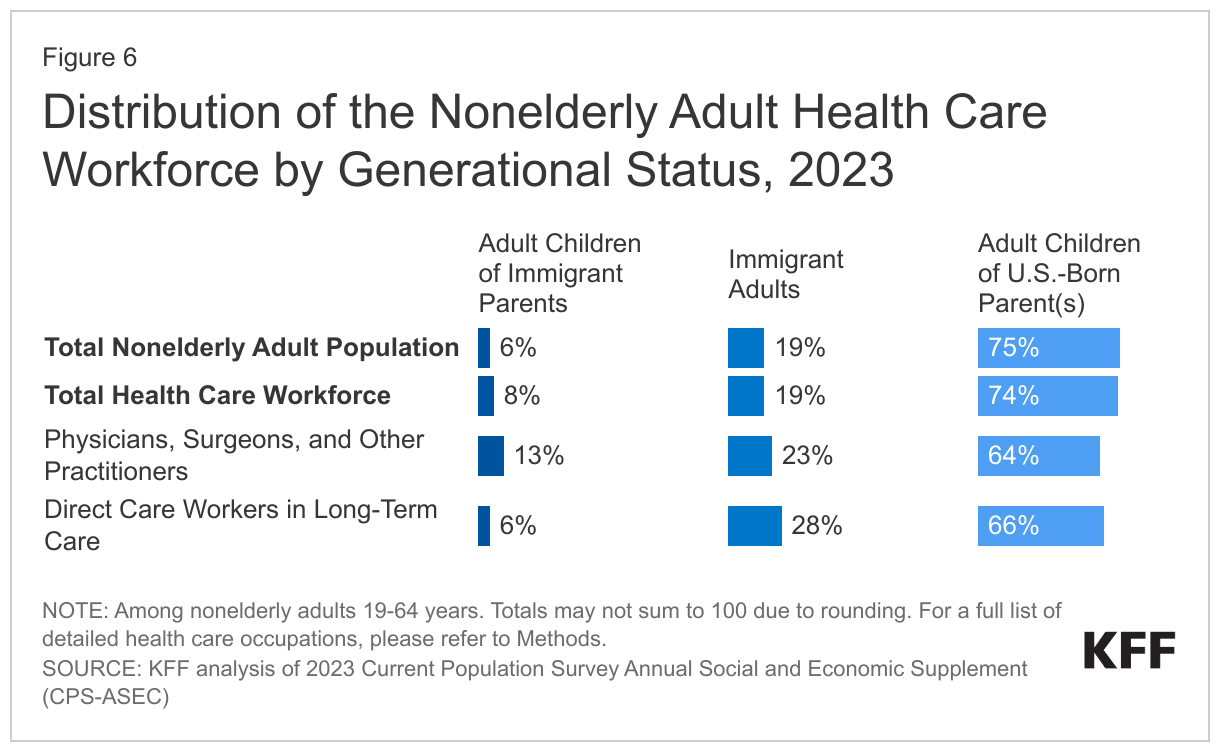
- About three-quarters (76%) of nonelderly adult children of immigrants and nonelderly adult immigrants (75%) are working and they make outsized contributions to the health care workforce. In particular, adult children of immigrants make up twice the share of physicians, surgeons, and other health care practitioners compared with their share of the population (13% vs. 6%). Immigrant adults also make up a larger share of physicians, surgeons, and other health care practitioners than they do of the population (23% vs. 19%) and play a particularly large role as direct care workers in long-term care settings, accounting for almost three in ten (28%) of these workers. In contrast, nonelderly adults with at least one U.S.-born parent make up a smaller share of physicians, surgeons, and other health care practitioners as well direct care workers in long-term care relative to their share of the population.
- Four in ten (39%) nonelderly adult children of immigrants live in households with an annual income of $90,000 or more and most (67%) have private health coverage. Similarly, about one in three (36%) of nonelderly adults with at least one U.S.-born parent and a quarter (25%) of nonelderly adult immigrants have annual household incomes of $90,000 or more. However, adult children of immigrants are less likely than adult children of U.S.-born parents to have private health coverage (67% vs. 76%) and more likely to be uninsured (13% vs. 8%), although they are more likely than immigrant adults to have coverage. Their higher uninsured rates relative to their peers with at least one U.S.-born parent may reflect that they are more likely to be employed in construction, food services, or transportation occupations, which may be less likely to offer employer-sponsored coverage.
These data suggest that proposals to limit workforce participation of immigrants or to end birthright citizenship for the children of some immigrants may adversely impact the U.S. workforce and economy. A reduction in the population of first- and second-generation immigrants may increase workforce shortages. The current health care workforce shortage in particular, which is projected to continue across professions, including allied health, long-term support services, behavioral health, and specialty physicians, may be exacerbated by such limitations given the disproportionate roles of both adult children of immigrants as well as immigrant adults in various health care occupations and industries. Worsening shortages could have negative effects on the nation’s health and well-being as well as the economy.
Background
In addition to the 45.5 million immigrants residing in the U.S. as of 2023, there are over 25.6 million U.S.-born individuals residing in the country who have immigrant parents (both parents born outside the U.S.), half of whom are nonelderly adults ages 19 to 64.1 Immigrants and their adult children make up a growing share of the population and play an important role in the nation’s communities, workforce, and economy. Other research has shown that adult children of immigrants have higher levels of educational attainment and work in higher-earning professions than their parents. Analysis further shows that children of immigrants contribute more in taxes on average than their parents or the rest of the U.S.-born population, and their fiscal contributions exceed their costs associated with health care, education, and other social services. Moreover, as older generations exit the workforce, immigrants and their U.S.-born children have been the primary drivers of workforce growth, accounting for 83% of the growth in the U.S. labor force between 2010 and 2018.
At the same time, immigration remains a hot-button political issue in the U.S. and there is pervasive anti-immigrant rhetoric. A few states, like Florida, recently passed laws that seek to limit immigrants’ ability to participate in the workforce, and, at the national level, presidential candidates have made recent proposals to end or limit birthright citizenship, a right guaranteed under the 14th amendment of the U.S. Constitution for children born in the U.S. regardless of their parents’ immigration status. Such proposals, which are intended to deter immigration, would not only impact immigrants’ and their children’s access to health care but could have broader ramifications for the nation’s workforce and economy, potentially exacerbating existing worker shortages, including in health care.
This brief analyzes data from the 2023 Current Population Survey Annual Social and Economic Supplement (CPS-ASEC) to present demographic, employment, and socioeconomic characteristics of nonelderly adults 19 to 64 years born in the U.S. to immigrant parents (“adult children of immigrant parents”) (defined as having both parents born outside the U.S) and how they compare to “adult children of U.S.-born parents” (defined as having at least one parent born in the U.S.) and immigrant adults (see Methods for more details).
Demographic Characteristics
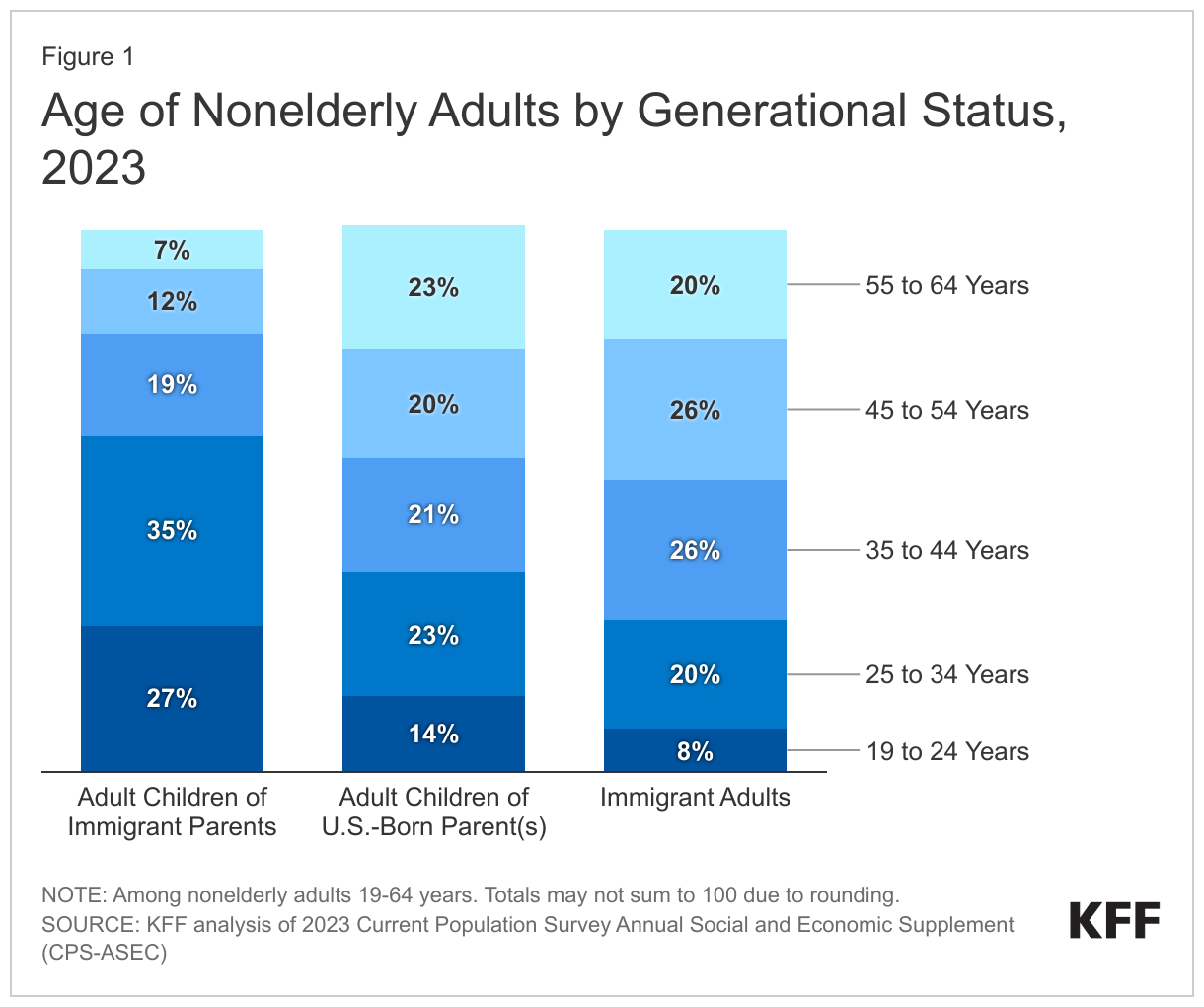
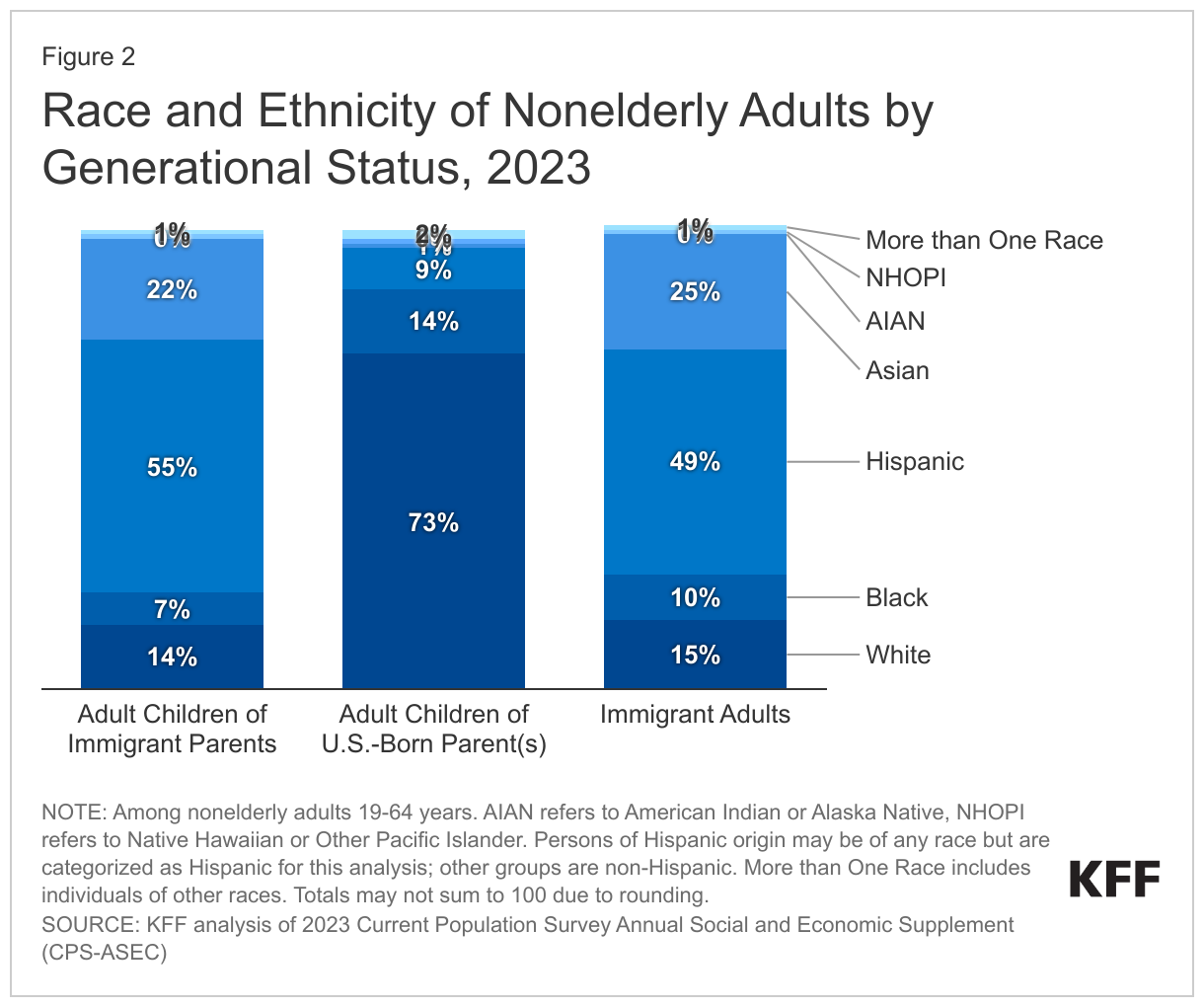
Adult children of immigrants are more likely to be younger (under 35 years) and more likely to be Hispanic or Asian than adult children of U.S.-born parents. Six in ten (62%) adult children of immigrants are between 19 and 34 years compared to 37% with at least one U.S.-born parent and 28% of immigrant adults (Figure 1). In addition, almost three-quarters of adult children of immigrants (77%) and immigrant adults (74%) are Hispanic or Asian compared to one in ten (10%) with at least one U.S.-born parent (Figure 2).
Adult children of immigrants have somewhat higher educational attainment levels compared to their peers with U.S.-born parents and immigrant adults. Among those between the ages of 25 and 64 years (who are more likely to have completed school), over four in ten (45%) of adult children of immigrants have a bachelor’s degree or higher compared with 40% of those with at least one U.S.-born parent and 38% of immigrant adults (Figure 3).
Employment Characteristics
Three in four (76%), or nearly 8.7 million adult children of immigrants are employed, accounting for 6% of the nonelderly adult workforce, which is similar to their share of the nonelderly adult population (6%). Immigrants make up about one in five of the nonelderly adult workforce and population, while the remaining three-quarters of the nonelderly workforce and population are comprised of adults with at least one U.S.-born parent.
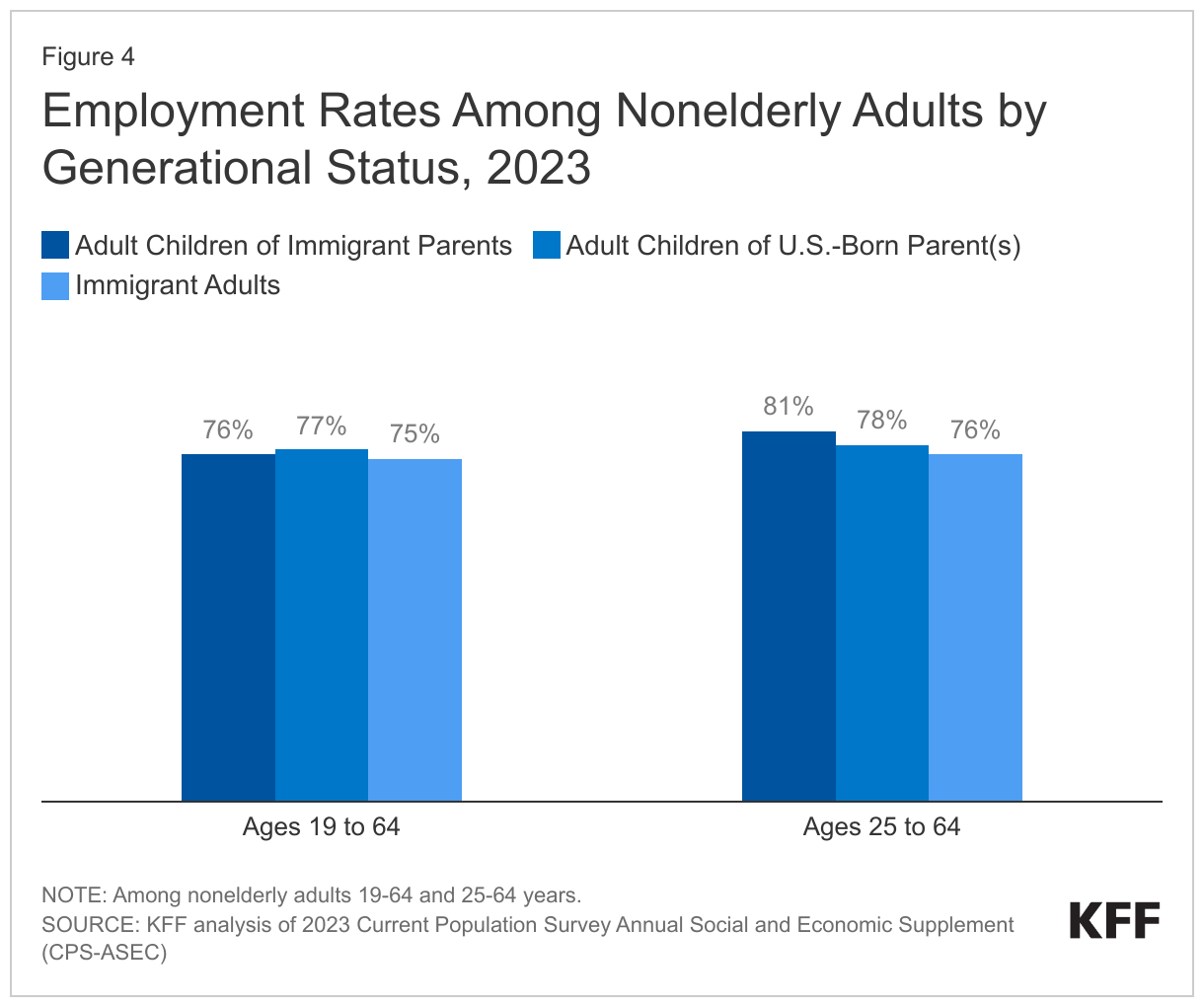
Employment rates for adult children of immigrants are similar to their counterparts with at least one U.S.-born parent and immigrant adults with roughly three in four employed, although among those ages 25 to 64, they are higher for adult children of immigrants. Among nonelderly adults between ages 25 to 64 (who are less likely to be students), about eight in ten (81%) adult children of immigrants are employed compared with 78% of their peers with at least one U.S.-born parent and 76% of immigrant adults in this age group.
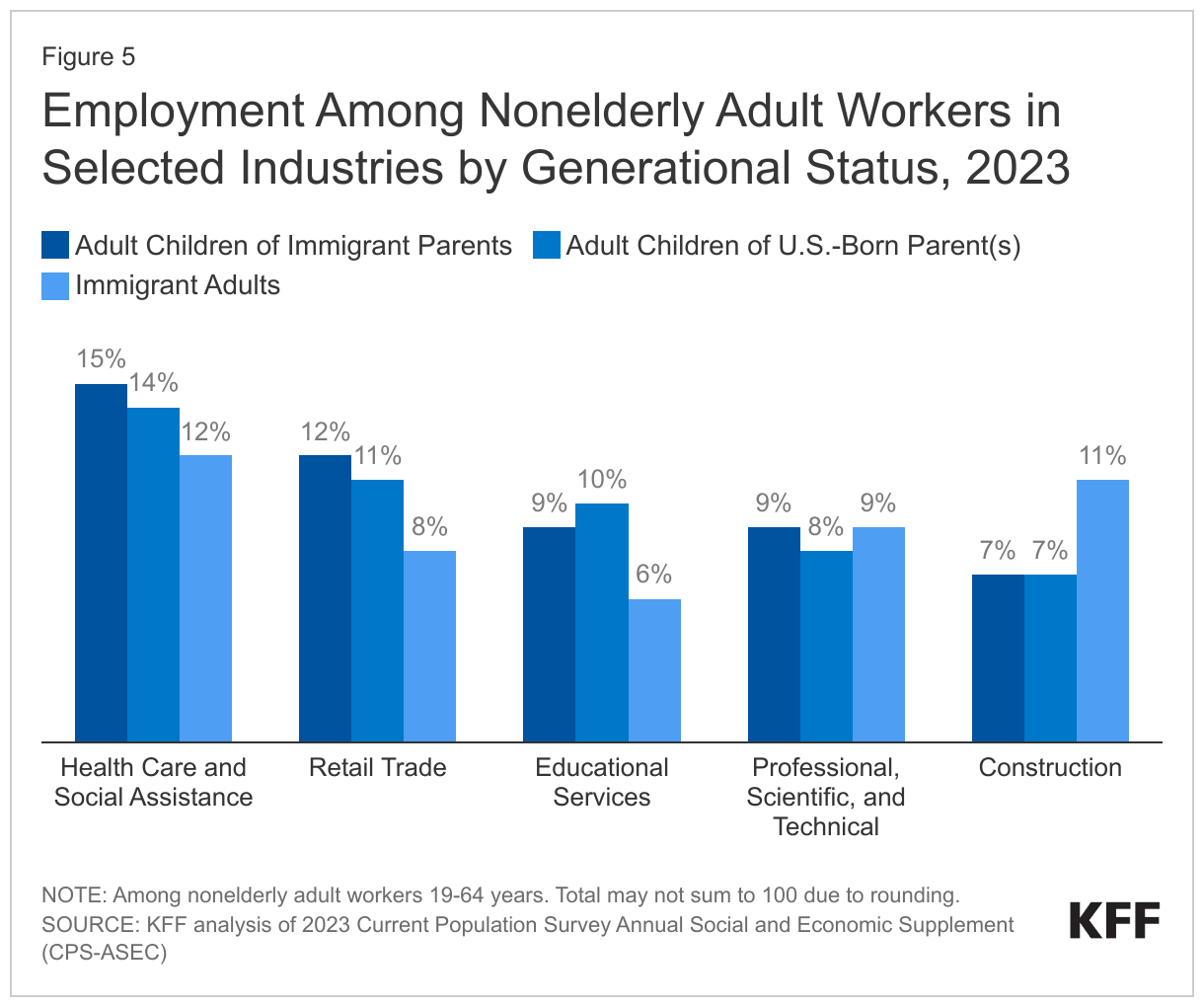
The top five industries in which adult children of immigrants are employed include health care and social assistance; retail trade; educational services; professional, scientific, and technical; and construction industries (Figure 5). Industry patterns for adult children of immigrants and their counterparts with U.S.-born parents are largely similar, with significant shares working in health care and social assistance (15% and 14%), retail trade (12% and 11%), professional, scientific, and technical industries (9% and 8%), educational services (9% and 10%), and in construction (7% for both). While significant shares of immigrant adults also are employed in health care and social assistance (12%) and professional, scientific, and technical industries (9%), their rates are lower, and over one in ten work in construction (11%). Significant shares of immigrant adults also are employed in food service (8%) and transportation (7%) industries.
Role in the Health Care Workforce
Adult children of immigrants and immigrant adults account for larger shares of physicians, surgeons, and other practitioners relative to their share of the nonelderly population. Specifically, adult children of immigrants make-up 13% of physicians, surgeons, and other practitioners, over twice their share of the nonelderly population (6%), and immigrant adults account for about a quarter (23%) of people in these occupations compared with 19% of the nonelderly population (Figure 6). (See Methods for details on health care occupation groupings.) Immigrant adults also play a particularly large role in the long-term care (LTC) workforce, making up almost three in ten (28%) of direct care workers in LTC settings, including registered nurses, licensed practical nurses, certified nursing assistants, home health aides, and personal care aides working in nursing homes, residential care facilities, or home health services. Reflecting this role, research has found that increased immigration is associated with improved staffing levels at U.S. nursing homes and consequently leads to improved outcomes for patients. On the other hand, adult children of at least one U.S.-born parent make up a smaller share of physicians, surgeons, and other practitioners as well as direct care workers in LTC than they do of the population (64% and 66% vs. 75%).
Income and Health Coverage
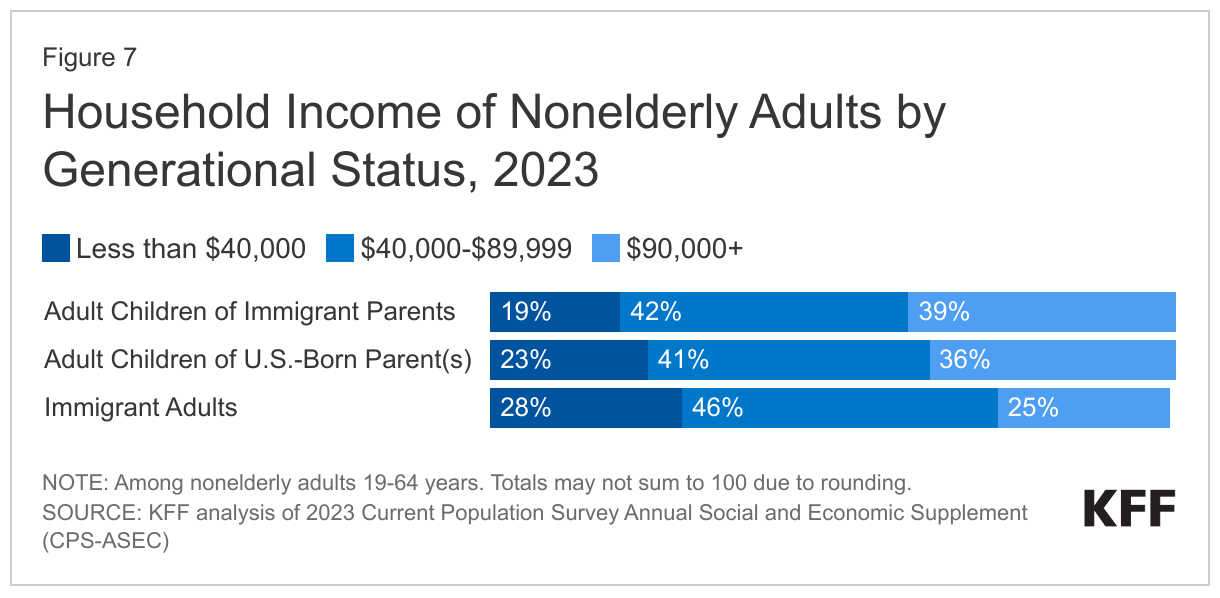
Adult children of immigrants attain greater upward mobility than their parents and have somewhat higher household incomes than immigrant adults as well as adult children of U.S.-born parents. Reflecting their higher rates of educational attainment and employment patterns, four in ten (39%) nonelderly adult children of immigrants live in households with an annual income of $90,000 or more compared with about one in three (36%) nonelderly adult children of U.S.-born parents and a quarter (25%) of nonelderly adult immigrants (Figure 7).
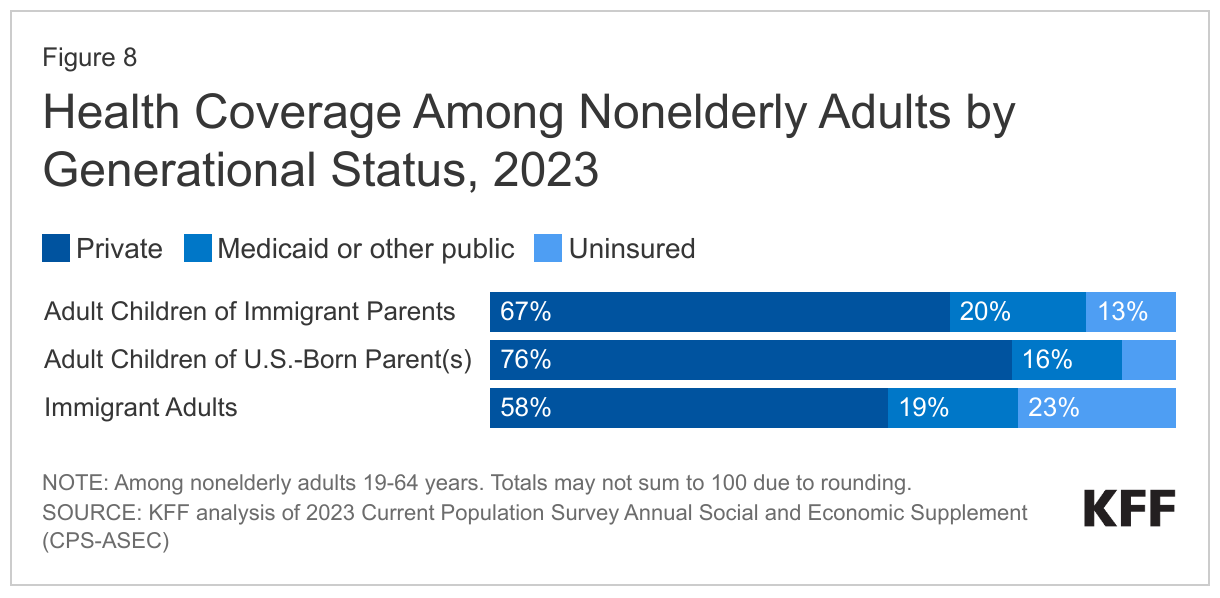
Most adult children of immigrants and immigrant adults have private health coverage, but they are more likely than adult children of U.S.-born parents to be uninsured (Figure 8). Despite high rates of employment and higher incomes, adult children of immigrants are less likely than adult children of U.S.-born parents to have private health coverage (67% vs. 76%) and are more likely to have Medicaid or other public coverage (20% vs. 16%) or to be uninsured (13% vs. 8%). However, they are more likely than immigrant adults to have private coverage (67% vs. 58%) and less likely to be uninsured (13% vs. 23%). While many adult children of immigrants work in health care and other professional occupations, they are more likely than those with at least one U.S. born parent to be in construction, food services, or transportation occupations, which may be less likely to offer employer-sponsored coverage. The higher uninsured rates among immigrant adults also reflect eligibility restrictions for federally funded coverage options, including Medicaid. Given their higher uninsured rates, immigrants and adult children of immigrants likely face increased barriers to accessing care and are at increased financial risk for health care costs.
Methods
The data in this brief are based on KFF analysis of the 2023 Current Population Survey Annual Social and Economic Supplement (CPS-ASEC) and are limited to nonelderly adults 19 to 64 years. Adult children of immigrant parents are defined as nonelderly adults born in the U.S. or its territories who have both parents born outside the U.S. or its territories; adult children of U.S.-born parent(s) are defined as nonelderly adults born in the U.S. or its territories who have at least one parent also born in the U.S. or its territories; and immigrant adults are defined as individuals born outside the U.S. or its territories.
The total health care workforce is defined as occupation codes 3000 through 3655. Physicians, surgeons, and other practitioners are defined as occupation codes 3000-3120 (chiropractors, dentists, dietitians, nutritionists, optometrists, pharmacists, physicians, surgeons, physician assistants, and podiatrists). Direct care workers in long-term care are defined as occupation codes 3255 (registered nurses), 3500 (licensed practical and licensed vocational nurses), 3603 (nursing assistants), 3601 (home health aides), or 3602 (personal care aides) working in industry codes 8170 (home health care services), 8270 (nursing care facilities), or 8290 (residential care facilities).
- KFF analysis of 2023 Current Population Survey Annual Social and Economic Supplement (CPS-ASEC). ↩︎