VOLUME 14
Misleading Narratives and Social Media Shape Contraception Perceptions
This is Irving Washington and Hagere Yilma. We direct KFF’s Health Information and Trust Initiative and on behalf of all our colleagues at KFF, we’re pleased to bring you this edition of our bi-weekly Monitor.
KFF Authors:
 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma Summary
This volume examines misleading claims about birth control, focusing on the distortion of emergency contraceptives, such as Plan B, as abortifacients. It also explores how social media and patient-provider communication shape perceptions of hormone-based contraceptives’ safety and effectiveness, particularly in response to online messaging that inaccurately promotes fertility awareness methods as safer alternatives.
Recent Developments
Narratives Claiming Contraceptives Terminate Pregnancies Complicate Access

Emergency contraception (EC) and intrauterine devices (IUDs) are safe, effective methods for preventing pregnancy, but some anti-abortion groups misrepresent these methods, particularly EC, as abortifacients. These claims are rooted in the misconception that these methods can terminate an existing pregnancy, prevent the implantation of a fertilized egg, or affect a developing embryo. Despite the FDA clarifying in 2022 on the Plan B label that it does not block implantation, misinformation persists. This narrative has fueled opposition to policies that expand access to contraceptives, with some lawmakers claiming to support birth control but also embracing policies rooted in these false claims. KFF policy experts explain that these misconceptions underpin legal and legislative challenges. For example, in the Supreme Court case Burwell v. Hobby Lobby Stores, Inc. (2014), the plaintiffs successfully argued that covering IUDs and EC under the ACA violated their religious beliefs, claiming that they “believed” that these methods are abortifacients. In 2024, similar misinformation threatened the adoption of state legislation in Missouri and Louisiana aimed at improving contraception access, as some lawmakers expressed concerns these methods may induce abortions. The Missouri legislation ultimately passed after delays attributed to concerns from anti-abortion groups, but the proposed Louisiana law failed to advance after its introduction.
KFF Data Insights:
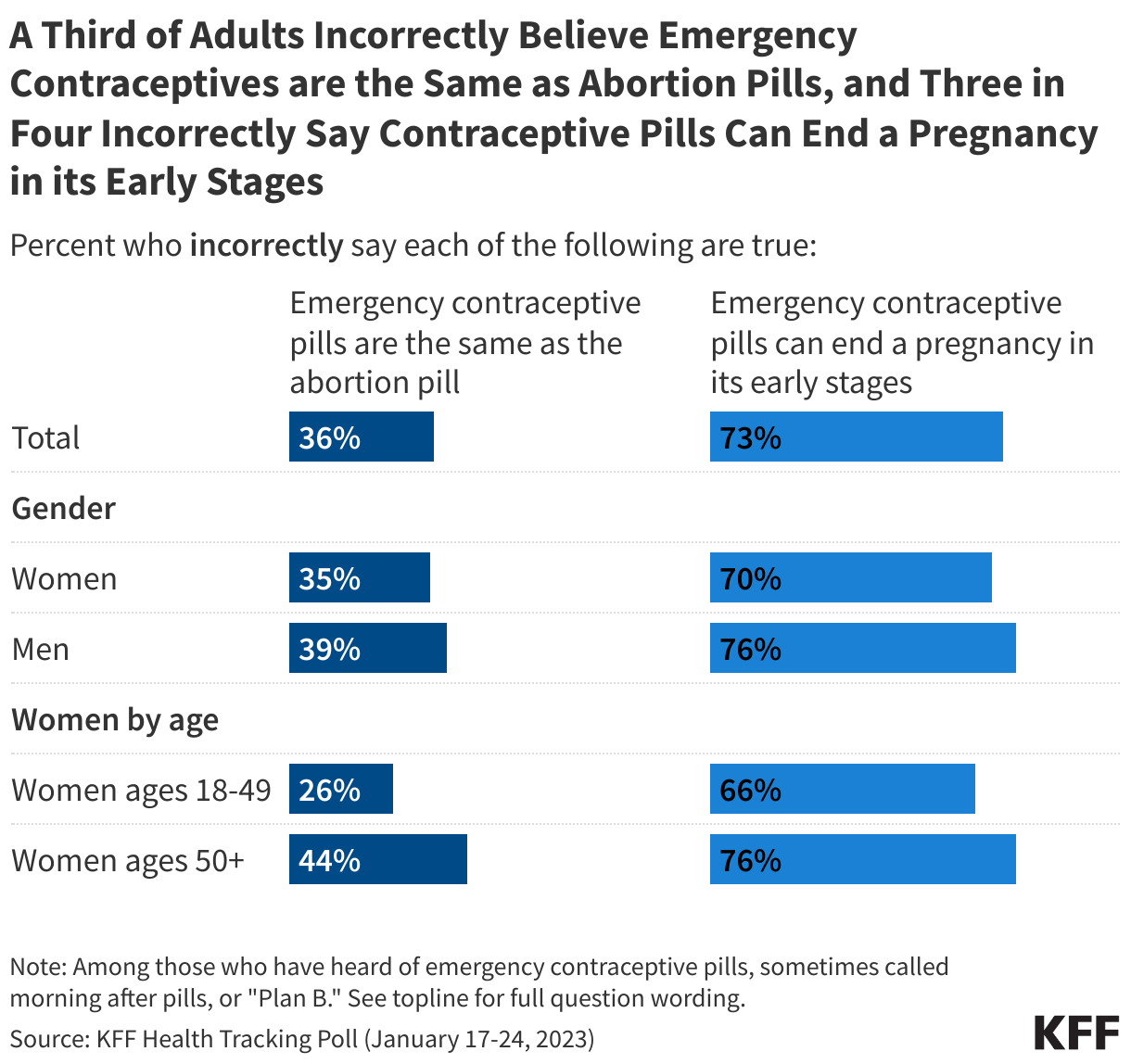
KFF polling has found that while the vast majority of U.S. adults (93%) have heard of emergency contraceptive (EC) pills, sometimes called the morning after pill or “Plan B,” knowledge gaps remain when it comes to accessing the medication and how it works.
One-third of adults who have heard of EC pills (including similar shares of women and men) incorrectly say that “emergency contraceptive pills are the same as the abortion pill,” and about three in four (including similar shares of women and men) incorrectly say that “emergency contraceptive pills can end a pregnancy in its early stages.” Women ages 18 to 49 are less likely than older women to say these false statements are true, though a majority (66%) still incorrectly believe that emergency contraceptive pills can end a pregnancy in its early stages.
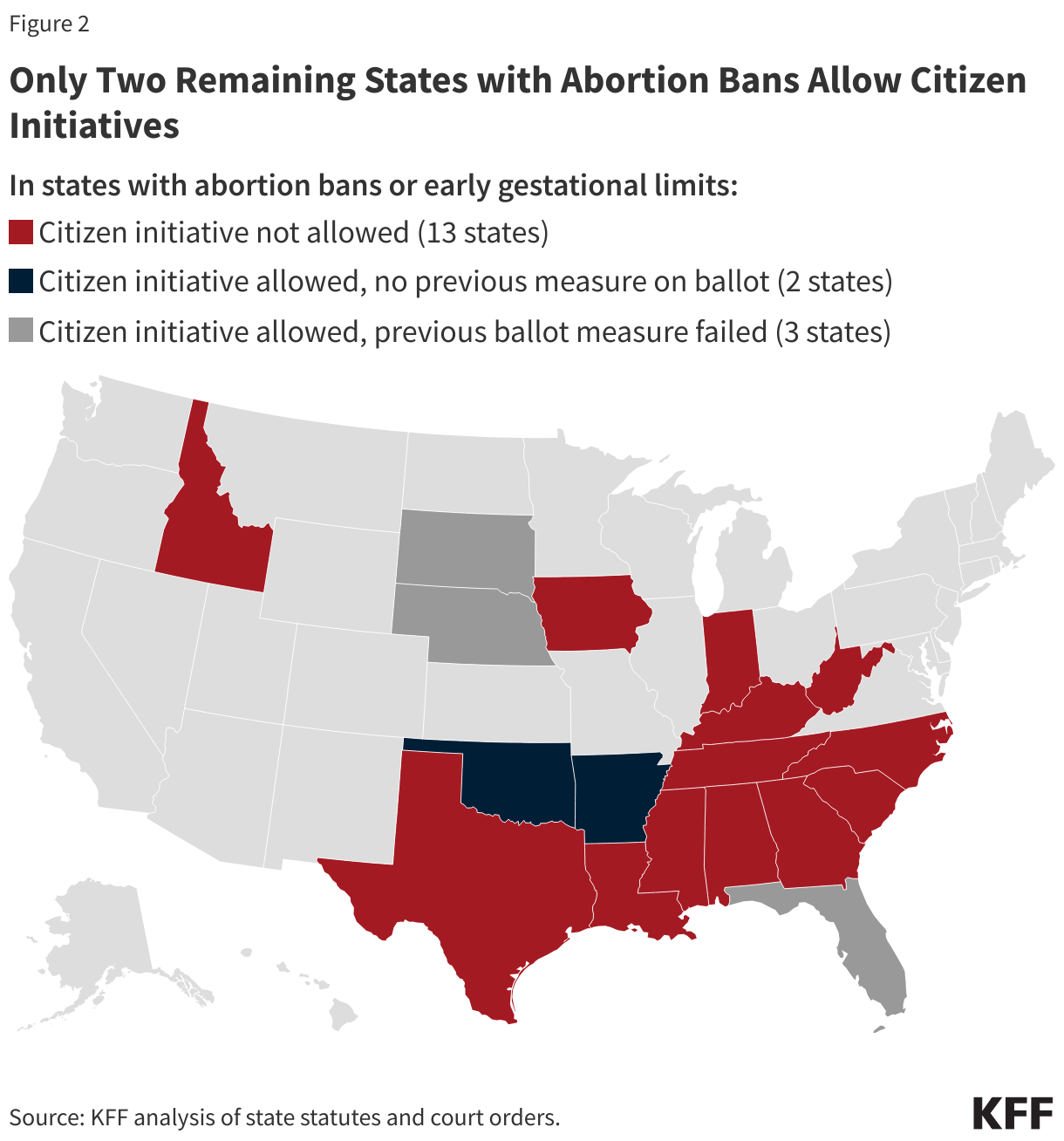
Abortion bans have created uncertainty among providers and patients about the legality of EC in some states. According to a KFF issue brief, many bans define pregnancy as beginning at fertilization and effectively grant personhood to fertilized eggs. Combined with misconceptions that some contraceptives are abortifacients, this language can lead to abortion bans being interpreted as restricting access to contraceptives. KFF polling from 2023 finds that about half of women in states where abortion is banned either believe EC is illegal or are unsure of its legality. This uncertainty extends to providers, who may delay or deny services like IUDs and EC out of fear their actions could be misinterpreted as inducing abortion.
Social Media Wellness Trends Share False Information About Hormonal Contraception

Misleading claims about contraceptive safety and effectiveness on social media could be driven by a number of factors including lack of high-quality contraceptive counseling, lack of knowledge of potential side effects, as well as wellness influencers who speak out against hormones. Social media platforms like TikTok, YouTube, and X amplify this misinformation with content creators frequently sharing unsubstantiated claims about the harms of hormonal contraceptives. These posts, often part of a broader trend against synthetic hormones, link hormonal contraceptive use to infertility, mental health challenges, and other health concerns. Personal anecdotes about side effects, coupled with critiques of pharmaceutical companies and the healthcare system, fuel these narratives. By sharing personal experiences and presenting themselves as relatable and independent, influencers are able to establish trust in a way that traditional health experts may not.
KFF Data Insights:
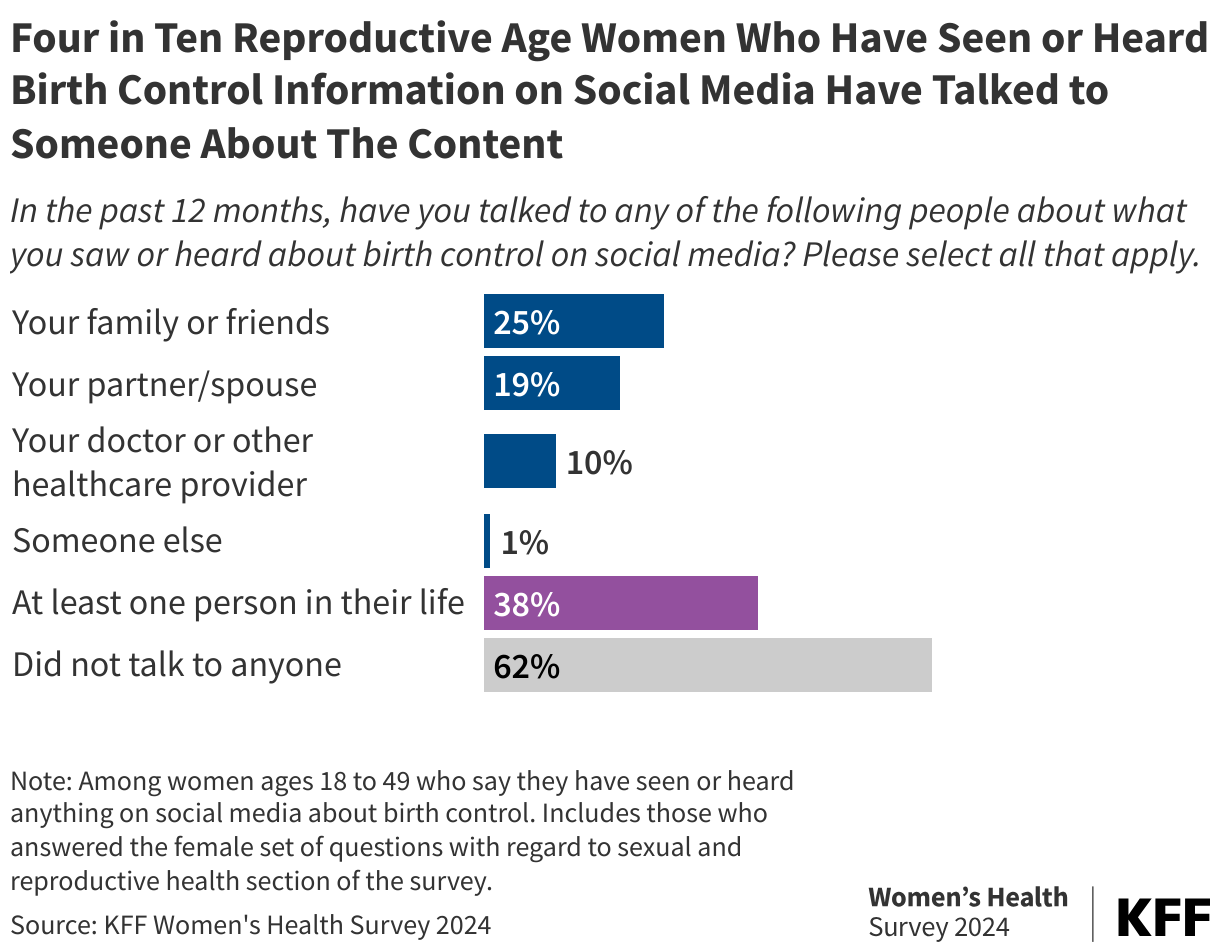
A November 2024 analysis of the KFF Women’s Health Survey examined women's experiences with contraception and the impact of contraceptive information on social media. The analysis found that approximately four in ten (39%) women of reproductive age report having encountered content related to birth control on social media in the past year. However, few women reported making or considering changes to their birth control method based on social media content.
Among those who have seen or heard birth control-related content on social media, 38% reported discussing the content with somebody in their lives. This includes about a quarter (25%) who had conversations with family or friends, 19% with their spouse or partner, and 10% who discussed the content with a doctor or healthcare provider.
Some content creators who advocate for avoiding synthetic hormones promote “natural” family planning methods—such as fertility awareness, cycle tracking, or the rhythm method—as healthier alternatives. These methods involve monitoring the menstrual cycle and avoiding intercourse or using non-hormonal birth control on fertile days. However, these approaches are generally less effective than hormonal contraceptives due to their reliance on precise knowledge and consistent application. Despite the proven effectiveness of hormonal contraceptives in preventing pregnancy, there are anecdotal reports of some women discontinuing their use, in part due to non-evidence-based fears fueled by such misinformation. While hormonal contraception may not be suitable for everyone, many individuals using “natural” family planning methods face challenges from a lack of proper guidance and difficulties with consistent use.
Contraceptive Counseling and Education Could Play a Role in Mitigating Misinformation

Health professionals have an opportunity to address questions or concerns about side effects outside of social media. The 2022 KFF Women’s Health Survey found that healthcare providers are both the primary (57%) and preferred source (74%) of information for many reproductive-age women using contraception. The main area of desired information is side effects with about half (52%) of reproductive-age women using contraception reporting wanting more information about additional side effects of their chosen contraceptive method.
An example where social media spurred a change in clinical practice relates to IUD insertions. After a number of people spoke about and recorded their painful experiences with IUD insertions on social media, the CDC issued new guidance for clinicians to ensure pain management is offered and covered by insurance during IUD insertions.
In recent decades, clinicians have prioritized getting their patients on the most effective contraceptive methods without centering patient needs and preferences, while downplaying their experiences and side effects. This has led to distrust and opened the door for social media content to fill a void on contraception information, but at a cost. There have been recent efforts to prioritize and center counseling and contraceptive options based on patient choices rather than focused on effectiveness alone. In addition to counseling in a clinical setting, reliable and trusted organizations are increasingly using social media to discuss and educate people about contraceptive methods, side effects, and effectiveness as a countervailing force to address misinformation.
Research Insights
Impact of Physician Misconceptions About Contraception on Family Planning Care

Research published in the American Journal of Obstetrics & Gynecology surveyed physicians at the University of Wisconsin to examine their beliefs about contraception, particularly regarding misconceptions that methods like IUDs and ECs cause abortion. While most physicians surveyed correctly identified that pills, implants, and injections do not cause abortion, 17% believed IUDs and 39% thought EC were abortifacients. Male physicians and those with higher religiosity were more likely to hold these misconceptions. Obstetricians, gynecologists, and physicians who had some abortion education during training were less likely to believe IUDs and EC cause abortion compared to other specialties or those without training.
Source: Swan, L. E., Cutler, A. S., Lands, M., Schmuhl, N. B., & Higgins, J. A. (2023). Physician beliefs about contraceptive methods as abortifacients. AJOG, 78(1), 33-34.
Framework for Understanding How People Respond to Misinformation

An article in Human Communication Research introduces the Misinformation Resilience and Response Model (MRRM), which explains how individuals respond to misinformation. When faced with conflicting information, people experience cognitive dissonance and are motivated to resolve it. If they recognize misinformation, they may use strategies like counterarguing or avoidance, which can change their attitudes, emotions, or behaviors, such as sharing misinformation or altering health or political views. This model highlights the need for targeted intervention strategies to address misinformation effectively, but future research could help refine these strategies and improve their practical applications.
Source: Amazeen, M. A. (2024). The misinformation recognition and response model: an emerging theoretical framework for investigating antecedents to and consequences of misinformation recognition. Human Communication Research, 50(2), 218-229.
AI & Emerging Technology
Effectiveness of AI Chatbots in Addressing Health Misinformation

AI-powered chatbots show potential in addressing health misinformation by encouraging user engagement and reflection, but a 2023 systematic review on contraceptive knowledge found mixed results on their effectiveness. Some studies reviewed indicated increased contraception uptake in certain groups, while others saw no change in knowledge or intentions. This suggests that while chatbots offer convenience, their lack of emotional sensitivity and limited competency can hinder their effectiveness. A more recent study in the Harvard Misinformation Review also explored AI interventions aimed at addressing misinformation, but this time around belief in conspiracy theories. The study found that using an AI chatbot to prompt individuals to reflect on the reasons for their beliefs led to a reduction in the strength of that belief. However, this effect was less pronounced among individuals with strongly held beliefs, highlighting the challenge of changing deeply entrenched views. These findings point to the need for further research to determine the features that make AI chatbots effective in countering health misinformation.
This edition was created in close collaboration with KFF’s Women’s Health Policy team.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.

The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Sign up to receive KFF Monitor
email updates
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The Public Good Projects (PGP) provides media monitoring data KFF uses in producing the Monitor.