Introduction
The Supreme Court’s Dobbs ruling has heightened interest in affirming the right to contraception. While the Court’s majority opinion stated that the Dobbs decision does not “cast doubt on precedents that do not concern abortion,” Justice Thomas argued in his concurring opinion that in future cases, the Court should reconsider precedent that relied on the same principles as Roe – including Griswold v. Connecticut, the Court’s 1965 landmark decision that recognized the right of married people to obtain contraceptives – and overturn those decisions. The prospect of the Court overturning Griswold moved some in Congress to introduce federal legislation that would protect the right to contraception, though that legislation is unlikely to advance in the current divided Congress. Similarly, some state legislators have recently introduced measures to protect the right to obtain contraceptives.
However, even with the current constitutional protections of Griswold in place, uncertainty has emerged around people’s ability to access certain contraceptive methods, such as IUDs and emergency contraceptive pills (often confused with medication abortion), which are erroneously believed by many to be abortifacients. If, as the Supreme Court’s majority indicated, the basis for their reasoning hinges on whether “potential life” is involved in a law, the conflation of contraception with abortifacients could be the reasoning in a future case or in the application of certain laws. Since the Dobbs decision in 2022, a growing number of states have passed laws or constitutional amendments to secure the right to contraception for their residents. Recently, former president Donald Trump said that he believes the right to contraception should be up to the states, a statement he followed up with a social media posting saying that he would not limit contraception. With several state ballot initiatives on the path to be facing the voters November 2024 and the former president’s statement on contraception, this issue is likely to emerge as an election issue this fall. Senate Majority Leader Schumer also recently stated his intention to take a vote to the Senate floor on a bill that would protect contraceptive access nationally. This issue brief explains how misinformation about contraceptives and how pregnancy is defined in state abortion bans may impact contraceptive access, and outlines the legal protections some states have established to affirm the right to obtain contraceptives.
Background
Supreme Court Decisions Recognizing the Right to Contraception
Currently, the right to contraception is protected by two landmark Supreme Court decisions, Griswold v. Connecticut (1965) and Eisenstadt v. Baird (1972). In Griswold, the Court recognized that the constitutional right to privacy encompasses the right of married people to obtain contraceptives. Prior to the Griswold decision, many states outlawed contraceptives, prohibiting clinicians from prescribing, or even discussing, contraceptive methods with their patients. After the Griswold decision, some states continued to have these prohibitions for single people, only allowing married women to obtain contraceptives. These laws spurred the litigation that resulted in the High Court’s decision in Eisenstadt, where the Court extended the constitutional protections of Griswold to unmarried people.
Misconceptions about Emergency Contraceptives (EC) and IUDs
Although intrauterine devices (IUDs) and emergency contraceptives (EC) – such as Plan B, Ella, and the emergency application of IUDs – work by preventing pregnancy, many people mistakenly believe they are abortifacients and can end a pregnancy. Polls indicate that as many as 73% of people incorrectly think emergency contraceptive pills can end a pregnancy in its early stages. Additionally, some people wrongly believe that IUDs work primarily by preventing implantation of a fertilized egg on the uterine lining. However, research has shown that these contraceptive methods work by inhibiting ovulation or by making it harder for sperm to reach an egg. Despite some common misconceptions, emergency contraceptive methods and regular use of the IUD do not terminate a pregnancy, stop the implantation of a fertilized egg, or affect a developing embryo.
Exclusion of Emergency Contraceptives in State Programs
Although Medicaid programs are required to cover family planning services, some states have attempted to exclude certain contraceptive methods from their state Medicaid programs. In 2020, Texas received permission from the Trump Administration to exclude emergency contraceptives from its Medicaid-funded family planning program, after requesting to exclude coverage in 2017. This waiver will remain in effect until December 2024. Similarly, in 2021 the Missouri senate voted on a bill that would have barred coverage of emergency contraceptives from the state’s Medicaid program. This measure failed, and it is unclear whether Missouri had the authority to enforce this restriction without receiving authorization from the federal government. And in 2023, Iowa stopped paying for Plan B for survivors of sexual assault through its Crime Victim Compensation Program. Although these measures affect coverage of emergency contraceptives – not their legality – they still constitute attempts to restrict access to certain contraceptive methods. Additionally, in 2021, the Idaho legislature enacted a law that bars “abortion-related activities” in school-based clinics, which prohibits health clinics at public schools, including higher education institutions, from dispensing emergency contraceptives, except in cases of rape.
Some Abortion Bans May be Interpreted to Limit Contraceptive Access
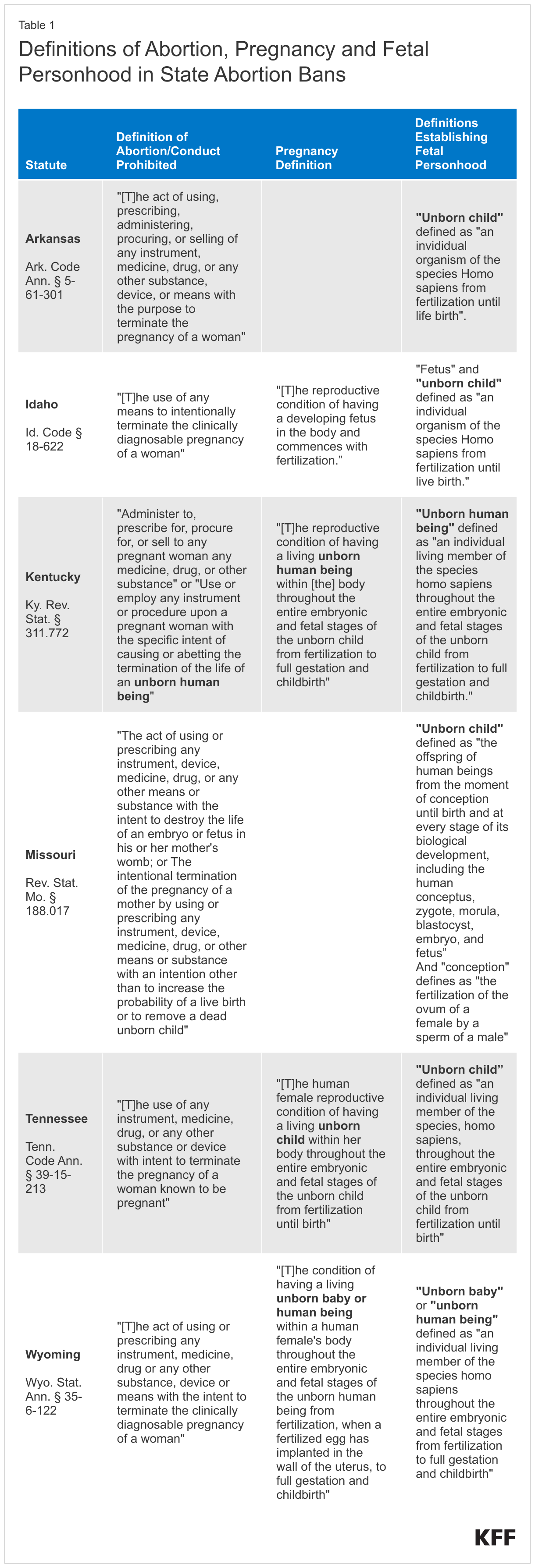
The definitions that abortion bans in some states employ, coupled with the misunderstanding that certain contraceptives are abortifacients, may be used to limit access to contraceptives. While leading medical organizations define pregnancy to begin at the implantation of a fertilized egg, a number of abortion bans define pregnancy to begin at fertilization and “fetus” and “unborn children” as living humans from fertilization until birth. The total abortion ban in Tennessee, for instance, defines pregnancy as the “reproductive condition of having a living unborn child within [the pregnant person’s] body throughout the entire embryonic and fetal stages of the unborn child from fertilization until birth.” If abortion bans establish that a pregnancy exists from the moment of fertilization, preventing the implantation of a fertilized egg could be construed as terminating a pregnancy. This kind of definition could potentially be used to ban or restrict contraceptive methods that people incorrectly believe to end a pregnancy.
For example, Missouri defines abortion to outlaw “[the] termination of the pregnancy of a mother by using or prescribing any instrument, device, medicine, drug, or other means or substance with an intention other than to increase the probability of a live birth or to remove a dead unborn child”. The ban additionally defines “unborn child” as “the offspring of human beings from the moment of conception” — which they define as fertilization — “until birth.” The ban does not provide a definition for pregnancy, but instead establishes personhood for fertilized eggs, which could be interpreted as banning anything that prevents the implantation of a fertilized egg on the uterine lining, a possibility the state’s governor did not firmly deny in the immediate aftermath of the Dobbs decision. As a result, when the state’s abortion ban went into effect, a major hospital system in Missouri immediately stopped providing Plan B – an emergency contraceptive – out of fear of charges that could have resulted from a prosecutor’s misunderstanding of how Plan B works. The hospital system resumed providing the emergency contraceptive after the Attorney General’s office and the governor clarified that the ban did not affect Plan B. However, this situation demonstrates how the definitions included in abortion bans, which imply pregnancy starts at fertilization, coupled with misunderstandings of how contraceptives work, could limit access to the full range of contraceptive methods.
Currently, most other abortion bans that define pregnancy to begin at fertilization also limit the definition of abortion to providing procedures or medication to people “known to be pregnant” or with “clinically diagnosable pregnancies”. This definition of abortion would preclude these bans from being used to limit contraceptives. This is because contraceptives – emergency or otherwise – do not end an existing pregnancy and emergency contraceptives are only effective up to 5 days after intercourse, while the earliest a pregnancy can be clinically confirmed is approximately 10 to 11 days after fertilization. Even with a misunderstanding of how contraceptives work, these bans do not affect conduct prior to the time when a pregnancy can be confirmed. Additionally, the abortion bans in a few states explicitly clarify that they do not prevent the prescription, sale, or transfer of birth control devices and oral contraceptives.
Notably this issue came up in the 2023 race for Kentucky Governor. In a questionnaire from a state anti-abortion organization, one Republican contender indicated his support for fetal personhood, and prohibiting public funds for abortion with a definition that included contraceptive methods such as the “morning after pill,” Norplant, Depo Provera and the so-called “standard birth control pill.” While the definition was provided by the anti-abortion organization, not the candidate, it illustrates the lack of understanding of contraceptive mechanisms of action and fails to distinguish between a drug or device that prevents pregnancy and those that are used to terminate a pregnancy.
Other Fetal Personhood Laws May Also Interfere with Access to Contraceptives
Laws and policies that define personhood to start at fertilization may similarly be used to limit access to contraceptives. For instance, the 2024 Alabama Supreme Court ruling holding that the state’s wrongful death law for minors applies from the moment of fertilization – including in vitro fertilization (IVF) – set precedent that could be used to limit access to certain contraceptives. Such an application of the law could result in the criminalization of actions perceived to threaten fertilized eggs, including the use of contraceptive methods people wrongly believe prevent the implantation of a fertilized egg, such as oral emergency contraceptives and the IUD.
State Protections for the Right to Contraception
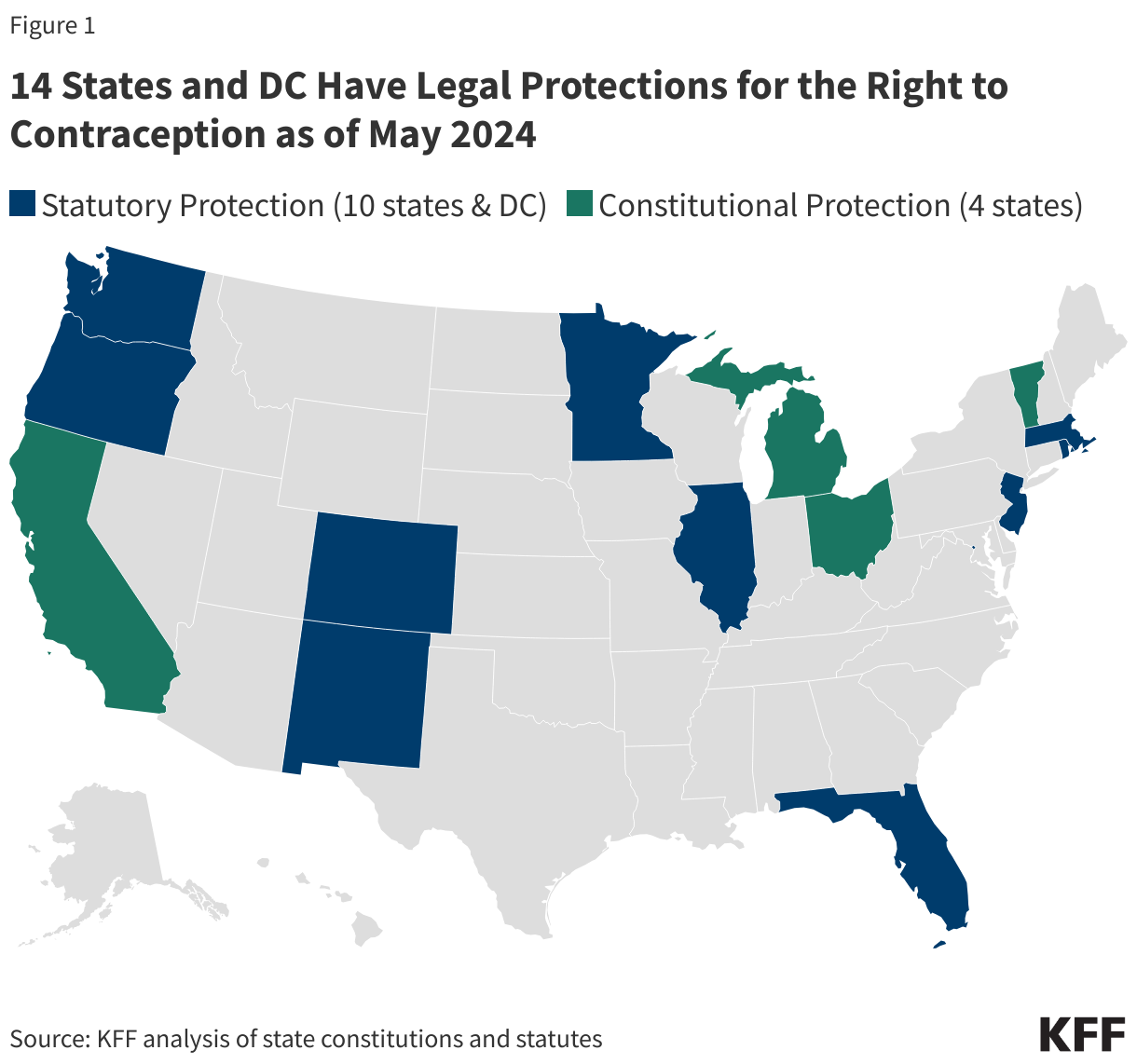
Fourteen states – California, Colorado, Florida, Illinois, Massachusetts, Michigan, Minnesota, New Jersey, New Mexico, Ohio, Oregon, Rhode Island, Vermont, and Washington – and D.C. currently have legal or constitutional protections for the right to contraception. In six states and D.C., these protections were enacted since the Supreme Court’s decision in Dobbs in June 2022 as a legislative and citizen response to the fall of Roe. In California, Michigan, and Vermont, voters passed constitutional amendments through ballot measures in the November 2022 election recognizing a broad right to reproductive autonomy, which includes the right to use or refuse contraceptives. In these states, the right to reproductive autonomy also includes the right to abortion and sterilization. In addition to the three states that had constitutional amendments in the November 2022 ballot, the legislatures in D.C., Minnesota, and New Mexico have enacted laws protecting contraception since June 2022. And in 2023, Ohio voters approved Proposition 1, amending their state constitution to protect reproductive decisions, including those regarding contraception and abortion.
Although a number of the protections for contraception were enacted post-Dobbs, more than half of the states that have such protections instituted them before June 2022. Most of these laws – including those in Colorado, Illinois, Massachusetts, New Jersey, Rhode Island, and Vermont – were passed in the years leading up to the fall of Roe. Of the states that currently protect the right to contraception, all but three enacted these protections after 2019. The states of Oregon, Washington, and Florida had enacted their laws protecting contraceptives in 2007, 1991, and 1972, respectively.
Most laws protecting the right to contraception also protect a broader set of reproductive health care decisions, such as miscarriage management, maternity care, and assisted reproduction. Some states, such as Florida and Oregon, however, have more specific laws protecting the right to contraception. Oregon has separate protections for emergency contraception, voluntary sterilization, and termination of pregnancy. In fact, Florida is the only state with a statutory right to contraception that also has passed abortion bans, with a 6-week LMP ban in effect.
Much like any other legal protection, enshrining these rights in the state constitution creates stronger and more stable protection than simply enacting laws, which can be repealed with a change in party control of the state legislature or Governor. In contrast, a constitutional amendment that explicitly protects the right to contraception, or reproductive autonomy more broadly, is harder to change or repeal.
Proposed State Bills and Constitutional Amendments
Legislators in several states have introduced bills and proposed constitutional amendment ballot measures to protect the right to contraception since the Dobbs decision. Legislators in Hawai’i, Maryland, Nevada, and Washington, among other states, have proposed constitutional amendments to create protections for contraception. Most of these measures are in committee or awaiting a vote with the legislature, but the Maryland and Nevada measures have passed. Maryland’s proposed constitutional amendment will be on the November 2024 ballot. In Nevada, constitutional measures must pass twice in the legislature before they are placed on a ballot and the earliest it may be listed on the ballot is November 2026. Further, lawmakers in several states, including Arizona, Iowa, and Virginia, have introduced bills protecting the right to contraception during the 2023 and 2024 legislative session. None of these bills passed during the 2023 legislative session. The Virginia bill introduced during the 2024 session has passed both chambers, but it was vetoed by the governor.
Federal Response
At the federal level, the Right to Contraception Act – a bill that would have protected the right to obtain and use contraceptives – and the Access to Safe Contraception Act – which would prevent states from banning the prescription, provision, or use of FDA-approved contraceptives – were introduced in the House and the Senate in the weeks after the Supreme Court issued the Dobbs decision. Shortly after the bill was introduced, the then Democrat-led House passed the Right to Contraception Act, but it did not receive a vote in the Senate due to a lack of the necessary votes needed to end a filibuster. The Right to Contraception Act was reintroduced in the current Congressional session in June 2023, but it does not have sufficient support to pass in the House or end the filibuster in the Senate at this time. Senate Majority Leader Charles Schumer has announced his intention to fast-track a Senate floor vote that would codify the right to contraception that was granted in the Griswold case assuring that this will be raised by Democrats as an election issue.
In the months following the Dobbs decision, President Biden issued two executive orders aiming to protect access to reproductive health care services, including contraceptives. While the executive orders do not specifically address the “right” to contraception, they call on federal agencies and regulators to assure that access to contraceptive services and supplies is broad and unimpeded by barriers related to costs, coverage, availability, and other factors. For example, in July 2022, under the directive of one of these executive orders, the U.S. Department of Health and Human Services issued guidance reminding retail pharmacies of their obligations under federal civil rights law. Specifically, the guidance pointed out that “if [a] pharmacy otherwise provides contraceptives (e.g., external and internal condoms) but refuses to fill a certain type of contraceptive because it may prevent pregnancy, the pharmacy may be discriminating on the basis of sex.”
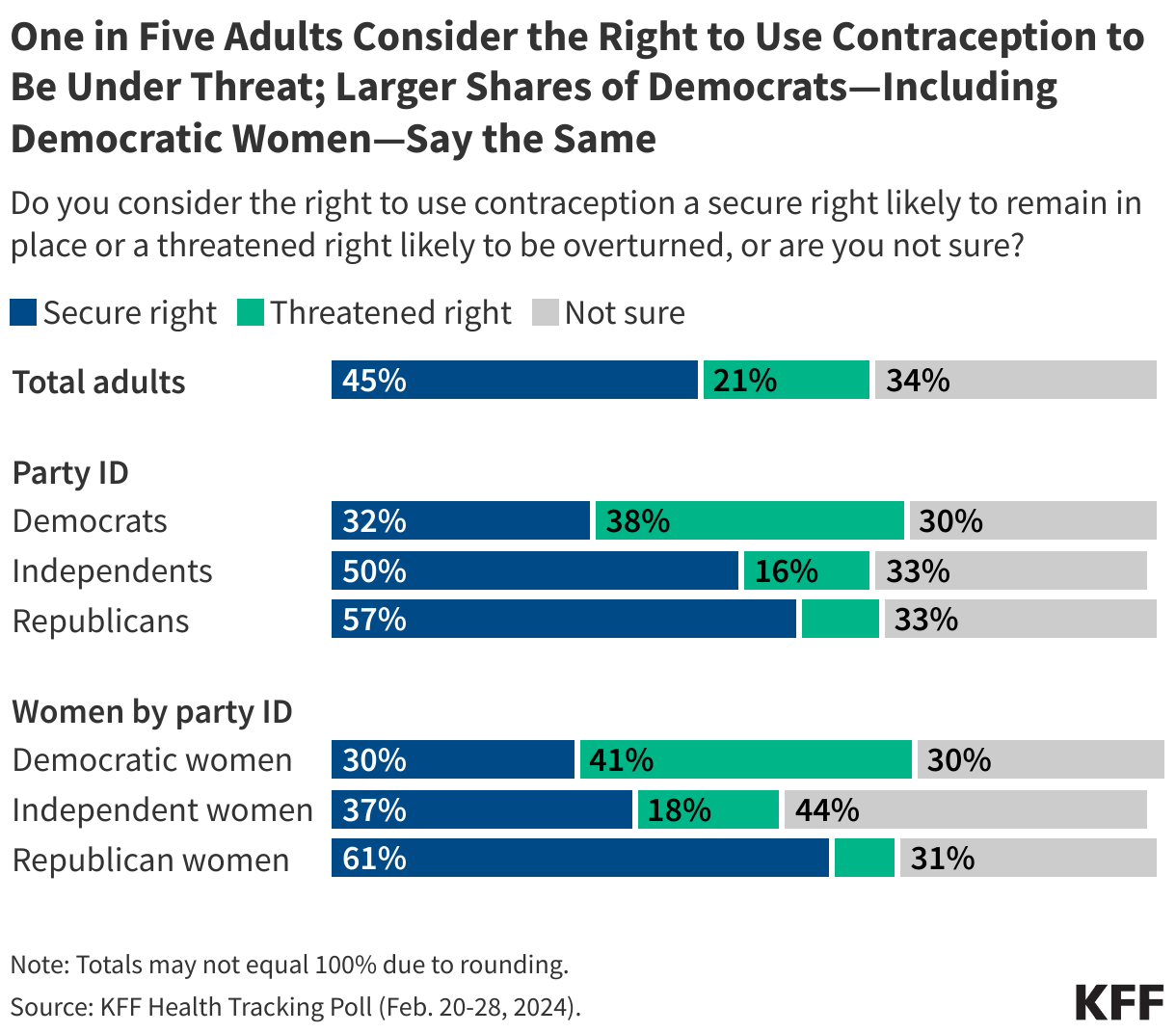
Recent KFF polling suggests that 21% of adults consider the right to contraception to be a threatened right, rising to over one-third of Democrats. One in four Democratic women feel that the right to contraception is under threat, but concern is lower among Republican women (8%). Notably, many are not sure whether it is a secure right, but that may change as the issue gets additional attention in the upcoming election.
This brief updates and expands upon a brief with the same title published in March 2023.

 Larry Levitt
Larry Levitt 
 Julie Rovner
Julie Rovner