The U.S. & The Global Fund to Fight AIDS, Tuberculosis and Malaria
This fact sheet does not reflect recent changes that have been implemented by the Trump administration, including a foreign aid review and restructuring. For more information, see KFF’s Overview of President Trump’s Executive Actions on Global Health.
Key Facts
- The Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), founded in 2002, is an independent, multilateral financing entity designed to raise significant resources and accelerate efforts to end the HIV, tuberculosis (TB), and malaria epidemics.
- The U.S. government (U.S.), which provided the Global Fund with its founding contribution, is its largest single donor; between FY 2001 and FY 2024 regular Congressional appropriations to the Global Fund totaled approximately $26 billion. In FY 2021, an additional $3.5 billion was provided by Congress as emergency funding to respond to the COVID-19 pandemic.
- The U.S. also plays a key role in the organization’s governance and oversight, having its own Board seat and sitting on two of the Board’s committees.
- As of October 2024, the Global Fund had approved more than $78 billion in funding to almost 130 countries for its core HIV, TB, and malaria programs; the Global Fund estimates these investments have helped to save 65 million lives. In addition to its core programmatic activities, the Global Fund played a major role in COVID-19 response efforts, awarding over $5 billion to respond to COVID-19 as of July 2024, and continues to support countries as they shift from emergency pandemic response to longer-term health systems strengthening and pandemic preparedness efforts.
- The Global Fund’s eighth replenishment cycle, where it will mobilize resources from donors for its next funding cycle, will take place in 2025.
What is the Global Fund?
Overview
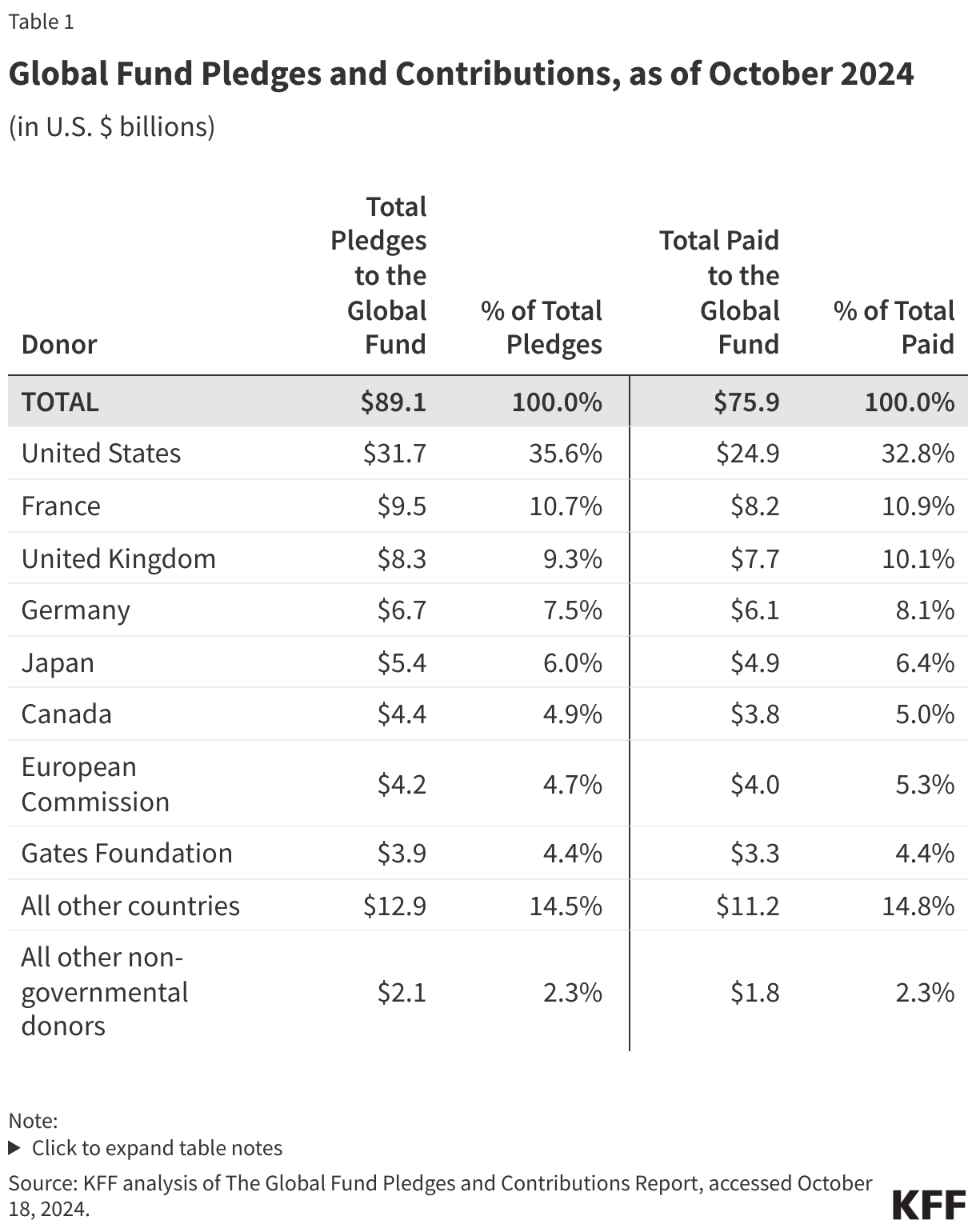
The Global Fund is an independent, multilateral financing entity designed to raise significant new resources to combat HIV, tuberculosis (TB), and malaria in low- and middle- income countries. First proposed in 2001, the Global Fund began operations in January 2002 and receives funding from both public and private donors to finance programs developed and implemented by recipient countries. The Global Fund uses a “country-defined” and “results-based financing” model that focuses on country ownership and is supported by investments from both donors and implementing countries (by contrast, bilateral support is provided from donors directly to recipient country governments, non-governmental organizations, and other entities and often reflects donor-defined priorities). To date, approximately $89 billion1 has been pledged by all donors (governments, the private sector, and private foundations) to the Global Fund, including $15.7 billion at the latest replenishment conference for the 2023-2025 funding cycle. Using these resources, the Global Fund has approved more than $78 billion in grants to almost 130 countries2 for its core HIV, TB, and malaria programs, and awarded over $5 billion in funding to respond to the COVID-19 pandemic’s impact on efforts related to these three epidemics.3 The Global Fund’s eighth replenishment cycle, where it will mobilize resources from donors for its next funding cycle, will take place in 2025.
The U.S. has played an integral role in the Global Fund since its inception. Under the George W. Bush administration, the U.S. provided the Global Fund with its founding contribution and was involved in the initial negotiations on the multilateral organization’s design. Under the Obama administration, the U.S. pledged $12.3 billion to the Global Fund over three replenishment periods.4 The Trump administration had proposed funding cuts to the Global Fund and a reduced pledge amount, although Congress rejected these proposals.5 The Biden administration signaled increased support for the Global Fund, particularly given its direct role in responding to the COVID-19 pandemic (see the Global Fund & COVID-19 section below), and pledged $6 billion over a three-year period6 at the latest replenishment conference in September 2022. The U.S. also provided an additional $3.5 billion in FY 2021 emergency funding to the Global Fund to address the impact of COVID-19 on HIV, TB, and malaria programs.
In addition to being the Global Fund’s single largest donor (see Table 1), the U.S. has a permanent seat on the Board of the Global Fund, giving it a key role in governance and oversight.7 The Global Fund has been called the “multilateral component” of the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), the U.S. government’s global effort to combat HIV (see the KFF fact sheet on PEPFAR), serving as a significant part of the U.S. government’s global health response, expanding its reach to more countries, and leveraging additional donor resources.
Still, long-ongoing discussions include the appropriate balance of U.S. funding between the Global Fund and U.S. bilateral programs, how to ensure the Global Fund’s sustainability and ability to provide the needed level of support (particularly given continued high demand for its support from countries, even amid a shortfall in available resources), and more broadly, the role of multilateralism in U.S. global health policy.8 Further, the appropriate shape of its role in strengthening health and community systems and, more broadly, pandemic preparedness and response, (its latest strategy includes a new pandemic preparedness and response objective) is also the subject of discussion.9
Funding Model & Organizational Structure10
The Global Fund was established as an independent foundation under Swiss law and operates as a multilateral financing entity. Funding is pooled from multiple sources, including from donor governments, the private sector, and private foundations. Countries submit proposals to the Global Fund, and if approved, funding is provided using a performance-based system where a grant is regularly monitored and evaluated to determine if it should be extended or discontinued based on the effectiveness of the program. Eligibility for funding is based on a country’s income classification and disease burden.11 Also, in order to incentivize recipient countries to increase their domestic investments and increase country ownership (ultimately preparing countries for graduation from Global Fund support), the Global Fund includes a policy that at least 15% of funding is conditional upon increases in co-financing (see KFF brief on co-financing for more).12
The Global Fund’s organizational structure includes a broad set of stakeholders, and the U.S. government is involved in many of its core structures:
- Board. The Board guides policy and strategic decisions and approves all funding. There are 20 voting members (10 implementers and 10 donors) and 8 non-voting members as follows:
- Implementers:
- Developing countries: seven members, one from each of the six WHO regions and an additional member from Africa.
- Civil Society: three members, one from a developing country non-governmental organization (NGO), one from a developed country NGO, and one representative from an NGO who is a person living with HIV/AIDS or from a community living with TB or malaria.
- Donors:
- Government: eight members, including the U.S., which has a permanent Board seat. The U.S. also sits on the Audit & Finance and Ethics & Governance Committees.
- Private Sector: one member.
- Private Foundation: one member.
- Non-voting: eight members, including the Global Fund Executive Director, the Board Chair and Vice-Chair, one representative from Global Fund partner organizations, one representative each from WHO, UNAIDS, and the World Bank, and one representative from certain public donors that are not part of a voting donor constituency.
- Implementers:
- Secretariat. Based in Geneva, the Secretariat manages day-to-day operations. Because the Global Fund finances but does not implement programs, it does not maintain any in-country staff.
- Office of the Inspector General. An independent body of the Global Fund that reports directly to the Board through its Audit and Finance Committee, the Office of the Inspector General provides the Board with audits and investigations of the Fund’s activities, in an effort to promote good practices, reduce funding risks, and report on potential abuse.
- Technical Review Panel (TRP). An independent body of global health and development experts (which has included U.S. government experts) appointed by the Board to evaluate the merits of all proposals and make funding recommendations to the Board.
- Independent Evaluation & Learning. An independent body consisting of an Evaluation & Learning Office and Independent Evaluation Panel (IEP) that provides advisory services and oversight on the Fund’s evaluation efforts, including progress toward achieving the goals laid out in its strategy.13
- Country Coordinating Mechanisms (CCMs). The country-level entity comprised of public and private sector representatives, such as governments, businesses, and NGOs, that submits proposals to the Global Fund and oversees funded grants within a country. U.S. representatives sit on CCMs in almost all PEPFAR focus countries and often help with proposal development. The U.S. has also entered into a memorandum of understanding (MOU) in several countries to bring together PEPFAR with Ministries of Health and the Global Fund to clarify collaboration and partnership activities, particularly in the area of antiretroviral drug procurement.
- Principal Recipients (PR). The legal entity chosen by the CCM to receive Global Fund disbursements, implement programs or contract with sub-recipients, and provide regular reports and progress updates to the Secretariat.
- Local Funding Agents (LFA). Since it does not have an in-country presence, the Global Fund contracts with a local entity (usually an accounting firm) to monitor program implementation, ensure financial accountability, and provide funding recommendations to the Secretariat.
Results
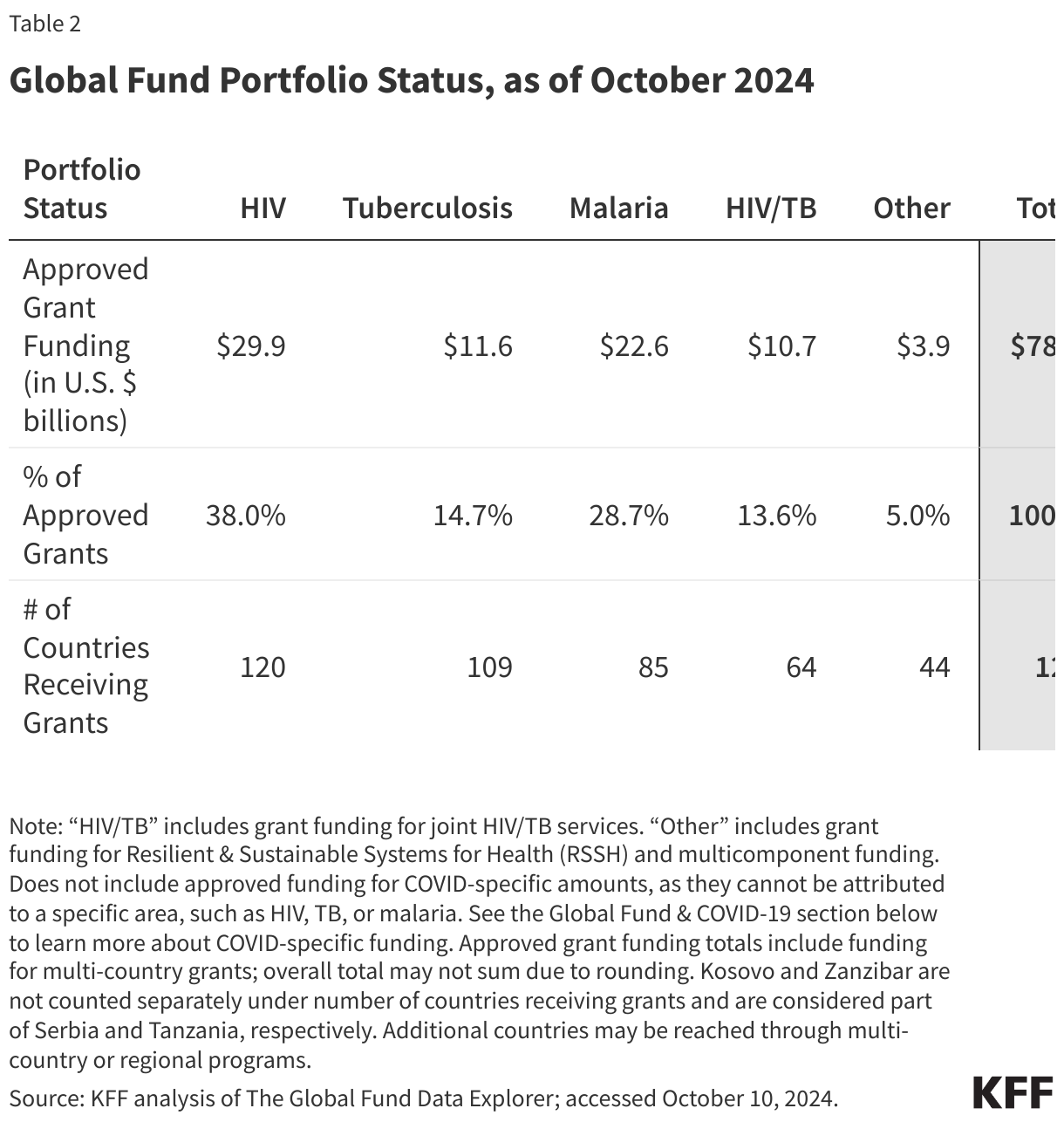
The Global Fund, which was the second largest donor to global health programs in 2022 (the U.S. was the largest),14 estimates that, since 2002, its grants have helped save the lives of 65 million people who would have otherwise died due to complications from AIDS, TB, or malaria and reduced the combined death rate from these three diseases by 61%. As of October 2024, the Global Fund had approved more than $78 billion in funding for its core HIV, TB, and malaria activities and, as of July 2024, awarded over $5 billion in funding to respond to COVID-19 (see the Global Fund & COVID-19 section below).15 Funding supports a wide range of prevention, treatment, and care activities and health systems development and strengthening. Most approved funding has supported HIV programs, followed by malaria and TB (see Table 2). This funding has reached almost 130 countries,16 including not only countries that also have received U.S. bilateral support for HIV, TB, and/or malaria but also many others that have not.17 The African region has received the largest share of approved funding (68%), followed by South-East Asia (11%).18
U.S. Engagement with the Global Fund
In addition to U.S. engagement in governance and oversight of the Global Fund, U.S. financial support has been significant and is a key component of U.S. involvement (see figure).19 The U.S. first contributed to the Global Fund in FY 2001, and then upon the creation of PEPFAR in 2003, Congress incorporated all U.S. support for the Global Fund under the PEPFAR umbrella. At that time, Congress authorized up to $1 billion for the Global Fund for FY 2004 and “such sums as may be necessary” for FY 2005-FY 2008. In the 2008 reauthorization of PEPFAR, Congress authorized up to $2 billion in FY 2009 and “such sums as may be necessary” for FY 2010-FY 2013.” In 2013, 2018, and 2024, Congress again reauthorized PEPFAR, and while those reauthorizations included provisions related to U.S. support for the Global Fund (see below), they did not include specific funding authorization amounts. Since the 2024 reauthorization was a short-term extension (through March 2025), discussions about the next reauthorization of PEPFAR, including expiring provisions related to the Global Fund, are ongoing. See the KFF policy watch on PEPFAR reauthorization key issues as well as the KFF brief on PEPFAR legislation over time.
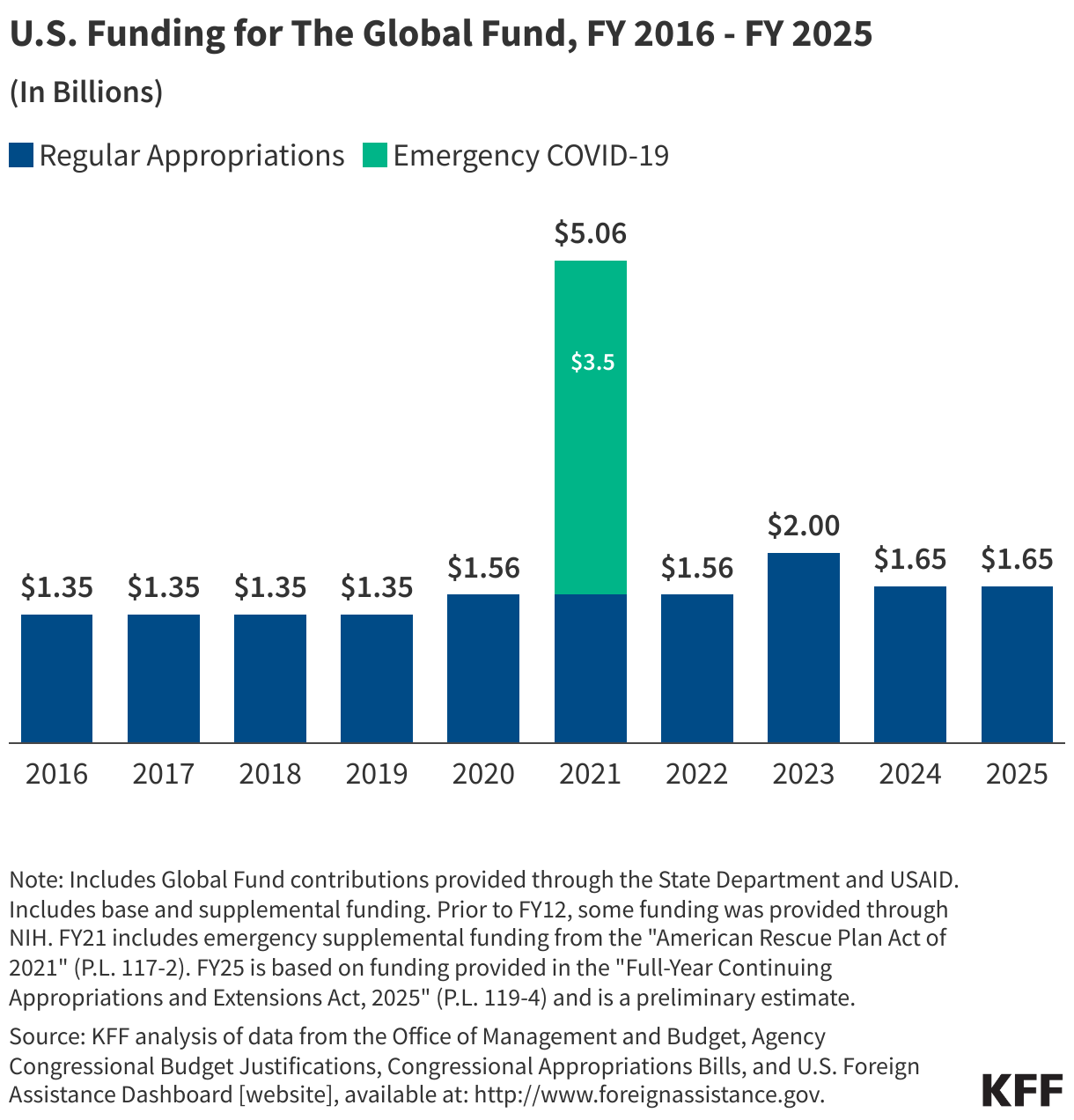
Congress specifies support for the Global Fund each year as part of PEPFAR appropriations, and funding is typically provided through the Department of State, although funding has also been provided through USAID and NIH in past years. Between FY 2001 and FY 2024, regular Congressional appropriations to the Global Fund totaled approximately $26 billion.20 In FY 2021, an additional $3.5 billion was provided as emergency funding to respond to the COVID-19 pandemic.21 Congress has historically matched or provided more to the Global Fund each year than the President has requested. (See the KFF budget tracker and the KFF fact sheet on the U.S. Global Health Budget: Global Fund for details on historical appropriations for the Global Fund.)
While Congress has provided strong funding support for the Global Fund, it has also regularly passed provisions that placed restrictions on U.S. contributions:22
- Requiring that total U.S. contributions do not exceed 33% of total contributions from all donors, a provision that was part of the original PEPFAR authorization and maintained in the reauthorizations. Designed to leverage U.S. contributions to increase support from other donors and to limit the U.S. from becoming the predominant donor to the Global Fund, it was invoked only once, in FY 2004 when appropriated funds were held back until the following fiscal year when the 33% cap would not be exceeded.
- Setting aside 5% of U.S. contributions to cover the cost of technical assistance to Global Fund grantees, a provision first included in foreign operations appropriations bill language in 2005 and in subsequent years.
- Authorizing the Secretary of State to withhold a percentage of the U.S. contribution until the Global Fund could demonstrate improved oversight and accountability in grant disbursement.
- Requiring, as part of the FY 2012 through FY 2024 appropriations bills, that the administration consult with Congress prior to making multi-year funding pledges.
The Global Fund & Emergency Responses
COVID-19
Since the beginning of the COVID-19 pandemic, the Global Fund acted to support countries in their efforts to address COVID-19’s impact on HIV, TB, and malaria programs. The Global Fund established a “COVID-19 Response Mechanism” (C19RM) in April 2020, and also allowed for grant flexibilities that gave countries the ability to use a certain percentage of their current grants for COVID-19 response activities. As of July 2024, the Global Fund had awarded over $5 billion in funding to more than 100 countries to support countries’ responses to COVID-19.23 Support from the Global Fund to countries was used to:
- support national COVID-19 response efforts, including purchasing tests, treatments, and medical supplies;
- mitigate COVID-19’s impact on Global Fund-supported programs; and
- improve health and community-led response systems.
As countries shifted from emergency pandemic response to longer-term efforts, the Global Fund allowed countries to reprogram their C19RM funds for health systems strengthening and pandemic preparedness activities. Today, the Global Fund reports that its partner countries have made a full recovery from the impacts of the COVID-19 pandemic and that service delivery metrics have surpassed pre-COVID-19 levels.
Mpox
Since Mpox was first declared a public health emergency of international concern in 2022, the Global Fund has worked to strengthen partner countries’ response to Mpox outbreaks by allowing grant flexibilities and repurposing of funds from HIV grants and C19RM funding. Specifically, countries may request support from Global Fund grants for activities such as disease surveillance, laboratory system strengthening, strengthening the workforce, as well as community engagement.
- Includes pledges through 2025. Includes COVID-specific emergency contributions. ↩︎
- Does not include countries that may have received funding through multi-country or regional programs. Additional countries may be reached through multi-country or regional programs. ↩︎
- Core activities represent HIV, TB, HIV/TB, malaria, multi-purpose, and Resilient & Sustainable Systems for Health (RSSH) funding only; the more than $78 million in approved funding does not include a breakdown of COVID-specific amounts as they cannot be attributed to a specific area, such as HIV, TB, or malaria. KFF analysis of The Global Fund Data Service: https://data-service.theglobalfund.org/downloads; accessed October 2024. The Global Fund, Dataset: Funding Approved for COVID-19 Response; July 2024. ↩︎
- The U.S. pledged $4 billion in both the FY11-FY13 and FY14-16 replenishment cycles and $4.3 billion in the FY17-FY19 replenishment cycle. U.S. State Department, Obama Administration’s Pledge to Global Fund to Fight HIV/AIDS, Malaria and Tuberculosis, October 5, 2010. The Global Fund, Fourth Voluntary Global Fund Replenishment Pledges, December 2013. White House, Office of the Press Secretary. Statement by National Security Advisor Susan E. Rice on the United States’ Global Fund Pledge; August 31, 2016. ↩︎
- Fulfillment of a pledge is dependent on annual Congressional appropriations. The Trump administration proposed reducing U.S. contributions to the Global Fund in each of its annual budget requests to Congress. In addition, the Trump administration proposed a pledge of $3.3 billion, matching $1 for every $3 contributed by other donors for the next replenishment period, a decline of more than $1.0 billion compared to the U.S. pledge during the prior replenishment period under the Obama administration (up to $4.3 billion, matching $1 for every $2 provided by other donors). See U.S. Department of State, FY2021 Congressional Budget Justification – Department of State, Foreign Operations, and Related Programs, February 2020. ↩︎
- The pledge period for the Global Fund’s seventh replenishment is 2023-2025. ↩︎
- Global Fund: http://www.theglobalfund.org/; as of September 2024. KFF analysis. White House, President Announces Proposal for Global Fund to Fight HIV/AIDS, Malaria and Tuberculosis; May 11, 2001. ↩︎
- Global Fund, The Global Fund Strategy 2023-2028, November 2021. The Global Fund, Thematic Report: Pandemic Preparedness and Response, May 2022. ↩︎
- Global Fund, Results Report 2024, September 2024. ↩︎
- Center for Global Development, Overview of the Global Fund to Fight AIDS, Tuberculosis and Malaria. ↩︎
- All low- and lower-middle-income countries are eligible for Global Fund grants regardless of disease burden; disease burden criteria only apply to upper-middle-income countries to determine their eligibility. ↩︎
- The Global Fund funding model includes a co-financing requirement for countries to show progressive government spending on health and progressive up-take of recurrent costs associated with key programs, as well as a co-financing incentive that at least 15% of a country’s allocation is withheld until the country has committed to additional investments over and above previous levels of spending. Global Fund, Website: Funding Model: Throughout the Cycle: Co-financing, available at: https://www.theglobalfund.org/en/funding-model/throughout-the-cycle/co-financing/. ↩︎
- The Independent Evaluation & Learning function replaces the Technical Evaluation Reference Group (TERG). Global Fund, Website: Independent Evaluation & Learning, available at: https://www.theglobalfund.org/en/iel/; accessed September 2024. ↩︎
- KFF analysis of OECD DAC CRS database, June 2024. ↩︎
- KFF analysis of the Global Fund Data Explorer: https://data.theglobalfund.org/home; accessed September 2024. The Global Fund, Dataset: Funding Approved for the COVID-19 Response; July 2024. ↩︎
- Does not include countries that may have received funding through multi-country or regional programs. Additional countries may be reached through multi-country or regional programs. ↩︎
- KFF analysis of the Global Fund Data Explorer: https://data.theglobalfund.org/home; accessed October 2024. ↩︎
- KFF analysis of the Global Fund Data Explorer: https://data.theglobalfund.org/home; accessed October 2024. Regions based on WHO regional classifications. ↩︎
- KFF analysis of data from the Office of Management and Budget, Agency Congressional Budget Justifications, Congressional Appropriations Bills, and U.S. Foreign Assistance Dashboard [website], available at: www.foreignassistance.gov. ↩︎
- This amount ($26 billion) represents the total amount of funding specified by Congress through FY 2024. However, the $32 billion pledged by the U.S. (seen in Table 1) includes the latest replenishment which runs through 2025, so the amounts will not match. ↩︎
- KFF analysis. The American Rescue Plan Act of 2021 included $3.75 billion “to support programs for the prevention, treatment, and control of HIV/AIDS in order to prevent, prepare for, and respond to coronavirus, including to mitigate the impact on such programs from coronavirus and support recovery from the impacts of the coronavirus,” of which not less than $3.5 billion was for the Global Fund. U.S. Congress, Public Law No: 117-2; March 11, 2021. KFF, Global Funding Across U.S. COVID-19 Supplemental Funding Bills, March 2021. ↩︎
- KFF analysis. U.S. Congress, Public Law No: 110-293; July 30, 2008. U.S. Senate Committee on Foreign Relations (Minority Staff Report), Fraud and Abuse of Global Fund Investments at Risk without Greater Transparency; April 5, 2011. U.S. Congress, Public Law No: 112-74; December 23, 2011. KFF, PEPFAR Reauthorization: Side-by-Side of Legislation Over Time, August 18, 2022. ↩︎
- Global Fund, Dataset: Funding Approved for COVID-19 Response; July 2024. ↩︎




 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma