Legal Challenges to State Abortion Bans Since the Dobbs Decision
Key Takeaways
The Supreme Court of the United States decision in Dobbs returned the decision to restrict or protect abortion to states. In many states, abortion providers and advocates are challenging state abortion bans contending that the bans violate the state constitution or another state law.
These challenges generally fall into three categories:
- Broad Constitutional Challenges: In Ohio, Oklahoma, Georgia, and Utah, among others, the abortion ban challenges include claims that state constitutional protections, such as liberty, due process, and privacy rights encompass a right to abortion.
- Health Care Amendment Challenges: Some state constitutions were amended to include a right to make health care and health insurance decisions in an effort to block the ACA’s individual coverage mandate. In Wyoming and Ohio, abortion advocates argue that this amendment includes the right to make a decision about whether or not to have an abortion.
- Religious Freedom Challenges: In Florida, Indiana, Kentucky, Missouri, Utah, and Wyoming people from various religious backgrounds argue abortion bans either unduly infringe on their religious exercise or violate state constitutional protections against the establishment of religion.
A number of state courts have responded favorably to many of these arguments and have temporarily blocked several bans while litigation on their constitutionality is ongoing. In time, these challenges will reach each state’s highest court, which will be the ultimate arbiter of the constitutionality of state-level abortion bans.
Introduction
Since the Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization, overturning Roe v. Wade and Planned Parenthood v. Casey, the legal landscape at the state level has been activated as never before. With the aim of restricting access to abortion, many states moved swiftly to lift court orders previously blocking bans, revive dormant pre-Roe bans, certify “trigger” bans, and enact new laws. Lacking federal protections, abortion providers have been on the front lines challenging these bans in state courts, questioning their constitutionality, not under the United States Constitution, but under each state’s constitution. Since the Dobbs decision, 23 states have tried to implement a complete ban or a pre-viability ban. In 6 states, these laws are currently blocked by courts. For an overview of the current legal status of abortion across the country, please see our abortion dashboard.
Although State Constitutions are similar to one another in many respects, each state has its unique judicial history and binding precedent, with State Supreme Court rulings diverging on liberty, privacy, and due process protections. Additionally, some states have amended their constitutions to include different abortion protections, while others have moved to assert that their constitution confers no right to abortion. Given these differences, abortion bans and restrictions that may be unconstitutional in some states, may be constitutionally permissible in others. As a result, the types of challenges on state constitutional grounds have varied in states banning – or attempting to ban – abortion access, including those where the question of a constitutional right to abortion had never reached their highest courts, the ultimate arbiters of the constitutionality of state laws.
Despite the variety in the types of legal challenges to abortion bans, a few patterns in the approaches have emerged in the abortion litigation landscape. In this issue brief, we present an overview of some of the types of challenges presented in state courts since the Dobbs ruling in June 2022 and highlight some of the novel strategies that are being used to defend access to abortion in states that have enacted abortion bans.
Background
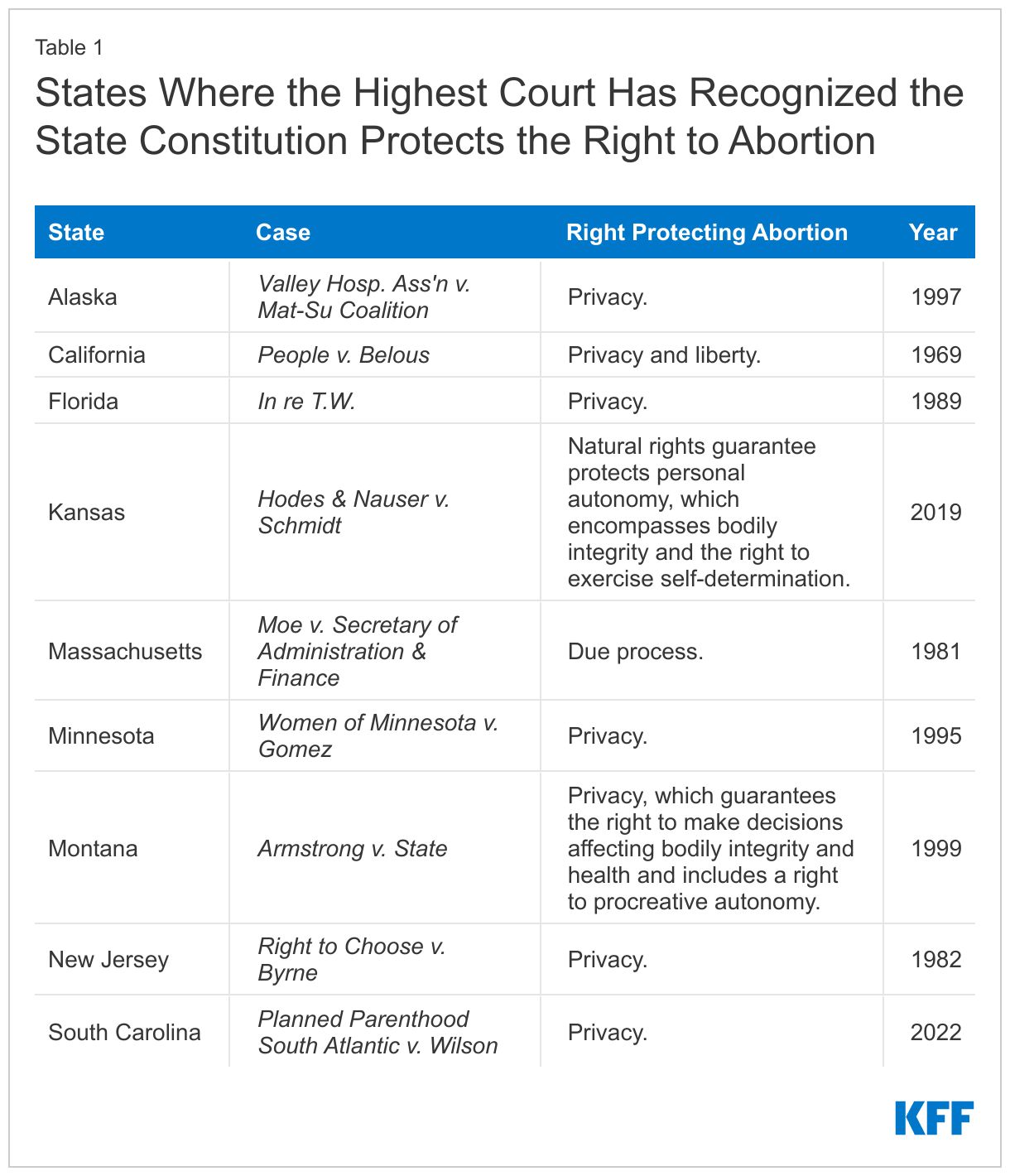
Before the Supreme Court of the United States (SCOTUS) Dobbs decision, the supreme courts of ten states had recognized a constitutional right to abortion in their states’ constitutions, but often under differing guarantees and protections. For example, in Montana in 1999, the state’s highest court found that the state constitution contained stringent protections of the right to privacy, exceeding those provided by the federal constitution, and, as such, ruled that procreative autonomy (the right to decide whether or when to have children) is protected under the right to privacy. Florida and Minnesota are two other states where the highest courts have ruled that their states’ constitutions include a more expansive right to privacy than SCOTUS had found in the federal constitution. In Massachusetts, the state’s highest court recognized that the right to abortion is found within the state constitutional due process rights.
Currently, nine state supreme court decisions finding state constitutional protections for abortion are binding precedent and have not been overturned by a subsequent decision or constitutional amendment. (Table 1). Just as SCOTUS overturned Roe, state supreme courts may overturn their previous decisions upholding the right to abortion in their state constitutions. In 2018, the Iowa Supreme Court found that the state constitutional rights of due process and equal protection encompassed the right to abortion. However, in June 2022, the Iowa court reversed itself, finding that the state constitution confers no fundamental right to abortion.
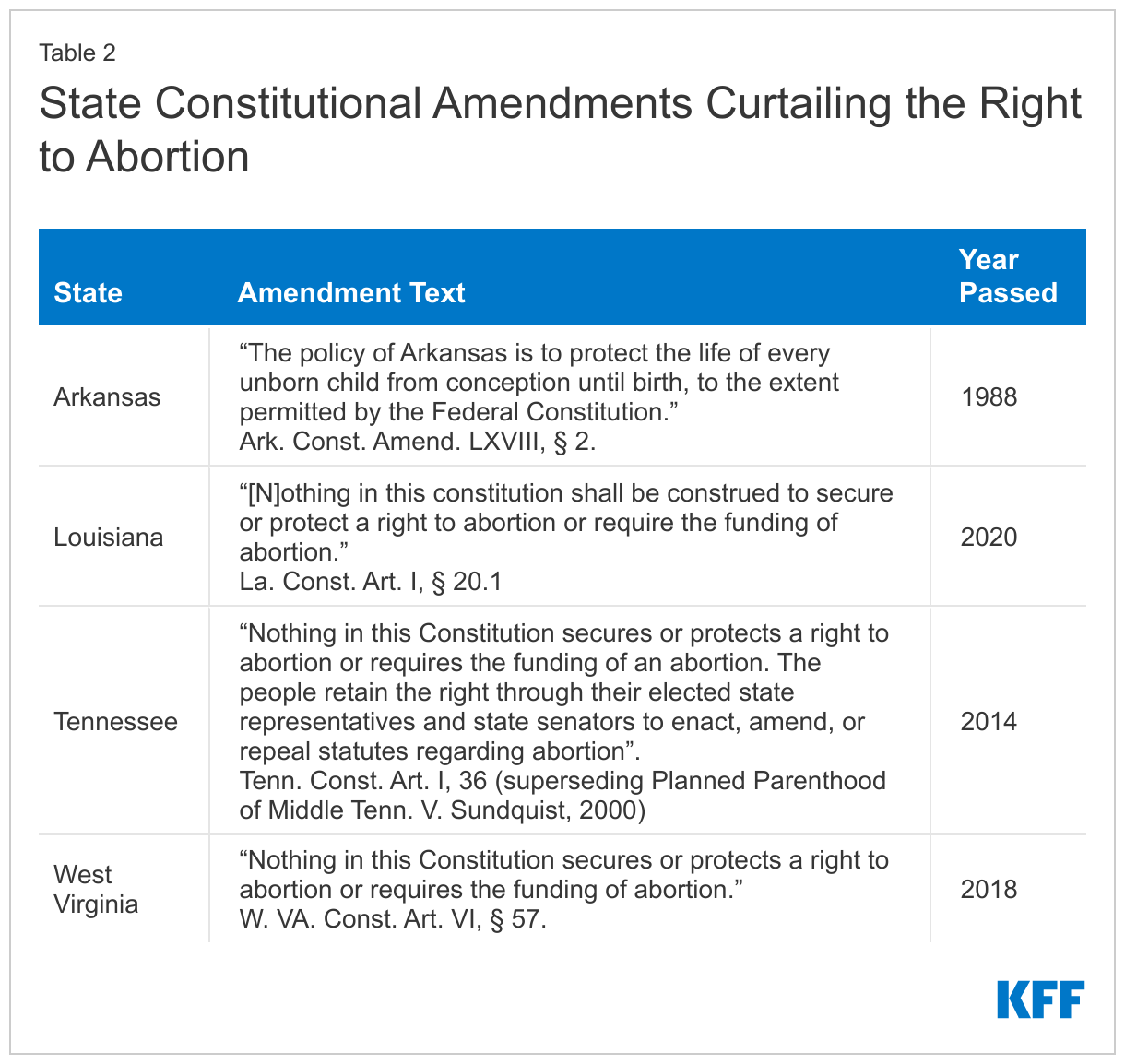
While a state’s highest court has final say about the constitutionality of laws under its constitution, the legislature and electorate may amend the constitution at a future date, rendering previous court decisions moot or severely impacting the landscape of litigation in that state. For example, in 2000 the Tennessee Supreme Court issued a decision finding the state’s constitutional protections for privacy encompassed a right to abortion. However, in 2014, voters approved a ballot measure amending the state’s constitution and explicitly expressing that the constitution did not confer a right to abortion, superseding the 2000 court’s ruling. In addition to Tennessee, Arkansas, Louisiana, and West Virginia (Table 2) have passed ballot measures to amend their state constitutions to curtail the right to abortion. Although these amendments may not explicitly prohibit abortion in the state, they can prevent the state supreme courts from ruling that other, broader constitutional protections encompass a right to abortion. This allows state legislatures to enact abortion bans and restrictions with the confidence that the state’s highest court will not find them unconstitutional and unenforceable.
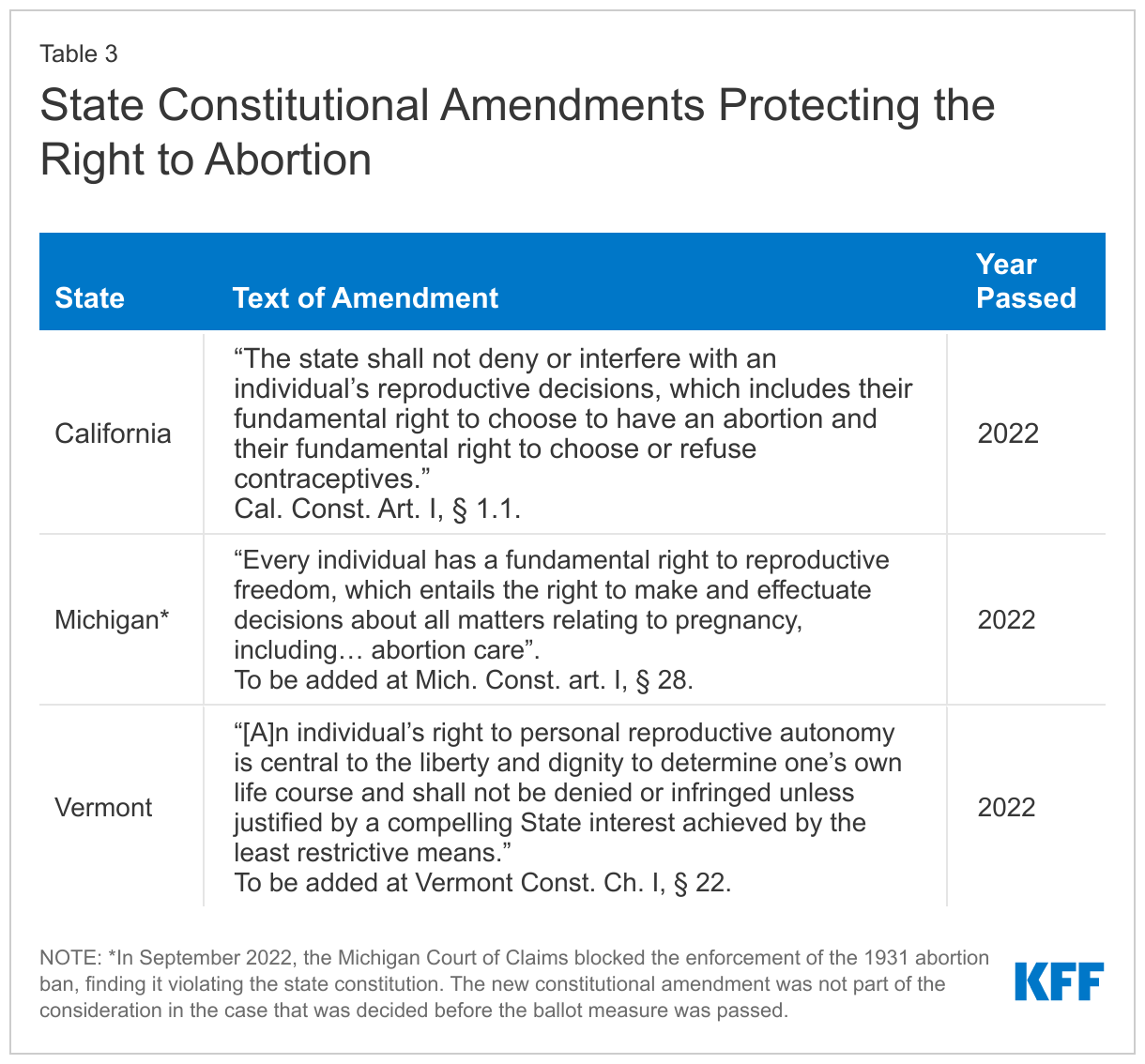
After the Dobbs decision, some states used ballot measures to attempt to amend their constitutions. The ballot measures seeking to curtail the right to abortion in Kansas and Kentucky failed, while California, Michigan, and Vermont (Table 3) successfully passed constitutional amendments recognizing a right to abortion. Enshrining these rights in the state constitution amounts to a much stronger, more stable protection than simply enacting laws recognizing such a right, which can be repealed with a change in party control of a state legislature. In contrast, a constitutional amendment that explicitly protects a right to abortion, or reproductive autonomy more broadly is much harder to change or repeal.
Challenges in State Courts Following the Dobbs Decision
Who is challenging the abortion bans in state courts?
Most legal challenges to state abortion bans are being brought by abortion care providers and clinics, presenting claims on behalf of themselves, their staff, and their patients. This is common in lawsuits regarding the right to access abortion care. Many prominent cases, such as Planned Parenthood v. Casey and Dobbs v. Jackson Women’s Health Organization, have been brought by providers and clinics.
Although there is a long history of providers and clinics challenging abortion restrictions, officials in some states dispute the legal “standing” providers have to bring these suits. For courts to be able to hear a case at all there must be a party with a real, concrete injury whose protection depends on an intervention by the Court. Usually, a person can only challenge the constitutionality of a law if it infringes on their own rights, not broadly the rights of others. However, legal challenges to abortion bans and restrictions brought by providers and clinics generally argue there is a constitutional right to receive abortion care and restrictive laws violate this right. In this way, providers argue that the rights of their patients – not necessarily their own – are being infringed by the bans.
This practice of suing to vindicate the rights of a closely related party (in this case providers and their patients) is called “third-party standing.” It allows a person or organization to assert the rights of another individual when it is difficult for them to assert their own rights, and the parties’ interests are closely aligned. Given the time limited duration of a pregnancy, it is difficult for pregnant people to personally challenge abortion restrictions while often facing numerous obstacles including financial limitations, and concerns for privacy and personal safety. For almost 47 years, federal and state courts have permitted doctors and clinics to sue on their behalf. The Supreme Court of the United States established third-party standing for abortion doctors on behalf of their patients in a 1976 decision, Singleton v. Wulff. That case was brought by two doctors challenging the exclusion of abortion in Missouri’s Medicaid program. Justice Blackmun wrote for the court, “aside from the woman herself, the physician is uniquely qualified, by virtue of his confidential, professional relationship with her, to litigate the constitutionality of the state’s interference with, or discrimination against, the abortion decision.” Singleton recognized that women can be fearful to assert their abortion rights out of concern for their privacy.
However, since the Supreme Court’s decision in Dobbs, some state courts have become more receptive of arguments against providers’ third party standing. Most notably, in Florida, a state Court of Appeals called into question providers’ ability to sue on behalf of patients in its decision refusing to block an abortion ban. If the ability of providers and clinics to bring challenges to courts is curtailed, it may be more difficult for these challenges to proceed successfully if only those who are seeking abortion are permitted to sue.
In addition to clinics and providers, other individuals and groups have challenged abortions bans. Some recent notable cases include a challenge under the Indiana Religious Freedom Restoration Act, where five unnamed women and a Jewish pro-choice organization are contesting the constitutionality of the state ban constitutionality on freedom of religious exercise grounds. This challenge is detailed below. Another notable case is the lawsuit disputing the constitutionality of the Wyoming’s total abortion ban, where a pregnant woman and a woman of reproductive age, along with two physicians, a clinic, and an advocacy organization are suing the state. This challenge rests on constitutional privacy rights and the right to make health care decisions. And, finally, in Wisconsin, the state’s Attorney General and Medical Examining Board filed a lawsuit seeking judgment that the state’s pre-Roe ban is unenforceable, arguing that the ban is incompatible and at odds with the many other abortion statutes the state enacted since the decision in Roe.
Types of Challenges
General Constitutional Challenges
In many states, lawsuits challenging the constitutionality of bans argue that the laws violate due process, liberty, equal protection, or privacy rights, or a combination of these rights. Although the states’ constitutional protections are similar, state Supreme Courts have diverged in their interpretation of these rights, with some recognizing that certain state constitutional rights are more expansive than their federal counterparts. There is active litigation in Ohio, Oklahoma, Georgia, Indiana, Kentucky, Utah and Wyoming, which include constitutional violations as the part of the basis of their challenges to the states’ abortion bans.
In issuing a preliminary injunction blocking the enforcement of Ohio’s abortion ban, the state trial court judge found that the Ohio Constitution includes the right to abortion in the right to “liberty” and in the “Due Course of Law” provision which states: “All courts shall be open, and every person, for an injury done him in his land, goods, person or reputation, shall have a remedy by due course of law, and shall have justice administered without denial or delay. Suits may be brought against the state, in such courts and in such manner, as may be provided by law.” The court also relied on the Health Care Amendment to the constitution which is discussed below.
In Wyoming, the presiding judge also found that the abortion ban’s exceptions regarding cases of rape or incest and medical emergencies could be found to be unconstitutionally vague. Judges in both Ohio and Wyoming also found the abortion bans would violate each state’s equal protection provisions, despite the states’ arguments that these laws apply to everyone equally.
In January 2023, the South Carolina Supreme Court struck down the state’s 6 -week ban as violating the state’s constitutional privacy provision. Unlike the U.S. federal constitution, South Carolina’s constitution has an explicit right to privacy. While each state court is independent and is not obliged to follow other state court decisions, the South Carolina Supreme Court reviewed the decisions of other state Supreme Courts to inform their own ruling that the right to privacy includes the right to abortion. Ten other states also have an explicit right to privacy in their state constitutions.1
Health Care Amendment Challenges
In Wyoming and Ohio, the legal challenges to abortion bans revolve around some of these same constitutional protections most other challenges rely on, but also around each respective state constitution’s amendment regarding health care and health insurance. These two states, along with Alabama, Arizona, and Oklahoma2 , amended their constitutions in the wake of the passing of the Affordable Care Act (ACA), to create a right to make health care and insurance decisions and block the insurance coverage mandate in the federal ACA. By creating a right to make decisions about health care and health insurance, the state legislatures hoped they could secure the individual right to refuse to purchase health insurance and to ensure the right to purchase private health insurance, thereby circumventing the law’s individual mandate to obtain insurance. In Wyoming, the constitutional amendment was approved in a ballot measure in the November 2012 elections. This amendment safeguards the right to health care access, broadly giving every adult the right to make his or her own health care decisions. In Ohio, the Health Care Freedom Amendment was approved in a November 2011 ballot measure. This amendment protects the right to purchase health care, stating that “[n]o federal, state, or local law or rule shall prohibit the purchase or sale of health care or insurance.”
Despite the narrow intent of the amendments to block ACA implementation, their broad language has allowed providers and advocates in Ohio and Wyoming to successfully argue that these measures create a general constitutional right to make health care decisions. And abortion, they argue, is health care under any ordinary definition of health care. Thus, providers argue, these amendments protect the right to make health care decisions and then logically protecting the decision about whether to have an abortion, making Ohio’s 6-week LMP ban and Wyoming’s total ban unconstitutional.
In response, state defendants that oppose abortion rights in both cases argue these health care amendments do not remove a state’s ability to regulate health care, or outlaw abortion. The state Courts in both states, however, were receptive to the argument that the right to make health care decisions encompasses the right to make decisions about whether to have an abortion and blocked the bans from being enforced. Judges in both courts asserted that, regardless of the intent with which the amendment was passed, the plain meaning of the language used in it likely conferred a right to abortion. In short, the state trial court judges agreed with the argument that abortion qualifies as health care and the general constitutional protection to make health care decisions created by the amendments would make the bans unconstitutional. Both cases are expected to reach each state’s highest court, where the constitutionality of the bans will ultimately be decided.
Religious Freedom Challenges based on State Constitutions and The Religious Freedom Restoration Act
Individuals, religious faith leaders and organizations have brought legal challenges in several states including Florida, Indiana, Kentucky, Missouri, Utah and Wyoming claiming their state’s abortions restrictions violate their religious freedom. Some of these litigants base their claims solely on the state’s constitution’s right to freely exercise one’s religion, while others are challenging their state abortion restrictions on their state’s Religious Freedom Restoration Act. Indiana’s case is the only religious challenge to an abortion ban to date where a court has responded to the state RFRA arguments at hand and evaluated their validity.
The plaintiffs in Indiana have based their challenge only on the state’s RFRA law. The Indiana RFRA law, adopted in 2015, “prohibits government action that substantially burdens a person’s religious exercise, unless the burden is in furtherance of a compelling governmental interest and is the least restrictive means of furthering that interest.” Several states have similar laws that are modeled after a 1993 federal law by the same name, which applies only to federal laws, not to state or local laws. Federal and state RFRA laws have been used to challenge laws requiring contraceptive coverage and anti-discrimination laws. Most notably, the federal Religious Freedom Restoration Act was the basis for the lawsuit brought by Hobby Lobby to challenge the contraceptive coverage requirement based on the for-profit corporation’s religious objections to certain contraceptive methods.
In the Indiana case, a group of women and a religious pro-choice organization argue the state’s abortion ban substantially burdens their religious exercise. Specifically, the plaintiffs argue that their respective religions (Judaism, Islam, and Unitarian Universalism) direct them to obtain abortion care under circumstances that the ban does not allow. This includes situations where the pregnancy jeopardizes the mental health of the pregnant person or their physical health, without necessarily causing serious risk of substantial and irreversible physical impairment of a major bodily function, as the ban’s health exception would require. Plaintiffs thus argue that their sincere beliefs would be substantially burdened if the ban went into effect. They further argue that the state’s right to protect potential life is not a strong enough interest to overcome their religious exercise rights – which are protected by Indiana’s RFRA – and bar them from receiving abortion care in situations where their sincerely held religious beliefs would call for them to seek it.
On December 2, 2022, the Marion County Superior Court granted a preliminary injunction, blocking the ban from being enforced against the plaintiffs, while the underlying question is resolved. Another Indiana state trial court had already issued an order blocking this ban from being enforced due to a previous challenge to the law, which argued the liberty guarantees of the Indiana Constitution provide a right to privacy that includes the right to determine whether not to have an abortion. The state has appealed both court decisions blocking enforcement of the ban and is requesting the Indiana Supreme Court eliminate the preliminary injunction in the RFRA challenge.
Conclusion
The fate of the constitutionality of abortion bans and the legal availability of abortion services in states where there are ongoing legal battles will most likely rest on each state’s highest court. Since SCOTUS issued its decision in Dobbs, the South Carolina Supreme Court has ruled that their state constitution protects the right to abortion. Conversely, a week before Dobbs’ decision, the Iowa Supreme Court overturned their previous decision, and found that their state constitution does not include any protections for abortion. It will take some time for the other cases underway to reach their respective State Supreme Courts and to have decisions on the states’ constitutional protections of abortion that will ultimately affect abortion access across the nation.
Appendix Table 1

- The states of Alaska (Const. art. 1, § 22), Arizona (Const. art. 2, § 8), California (Const. art. 1, § 1), Florida (Const. art. 1, § 23), Hawai’i (Const. art. 1, § 6), Illinois (Const. art. 1, § 6), Louisiana (Const. art. 1, § 5), Montana (Const. art. 2, § 10), New Hampshire (Const. art. 2-b), South Carolina (Const. art. 1, § 10), and Washington (Const. art. 1, sec. 7) all contain explicit protections of the right to privacy. ↩︎
- Oklahoma Constitution Article II, § 37. ↩︎