KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
At the start of the pandemic, Congress enacted the Families First Coronavirus Response Act (FFCRA), which included a temporary requirement that Medicaid programs keep people continuously enrolled and, in exchange, states received enhanced federal funding. Under the continuous enrollment provision, Medicaid enrollment has grown substantially compared to before the pandemic and the national uninsured rate has declined. Provisions in the Consolidated Appropriations Act (CAA), signed into law in December 2022, end the continuous enrollment provision on March 31, 2023, and phase down the enhanced federal Medicaid matching funds through December 2023. When the continuous enrollment provision ends, however, millions of people could lose Medicaid, potentially reversing recent gains in health insurance coverage.
A key question is whether people losing Medicaid will be able to transition to and retain other forms of coverage, including Affordable Care Act (ACA) marketplace plans with premium assistance or employer-sponsored health benefits.
This brief uses pre-pandemic data from the 2016-2019 Medical Expenditure Panel Survey (MEPS) to examine the extent to which people enroll in and retain other coverage during the 12 months following disenrollment from Medicaid/CHIP. See the “Methods” section at the end of this brief for more details. Key findings include:
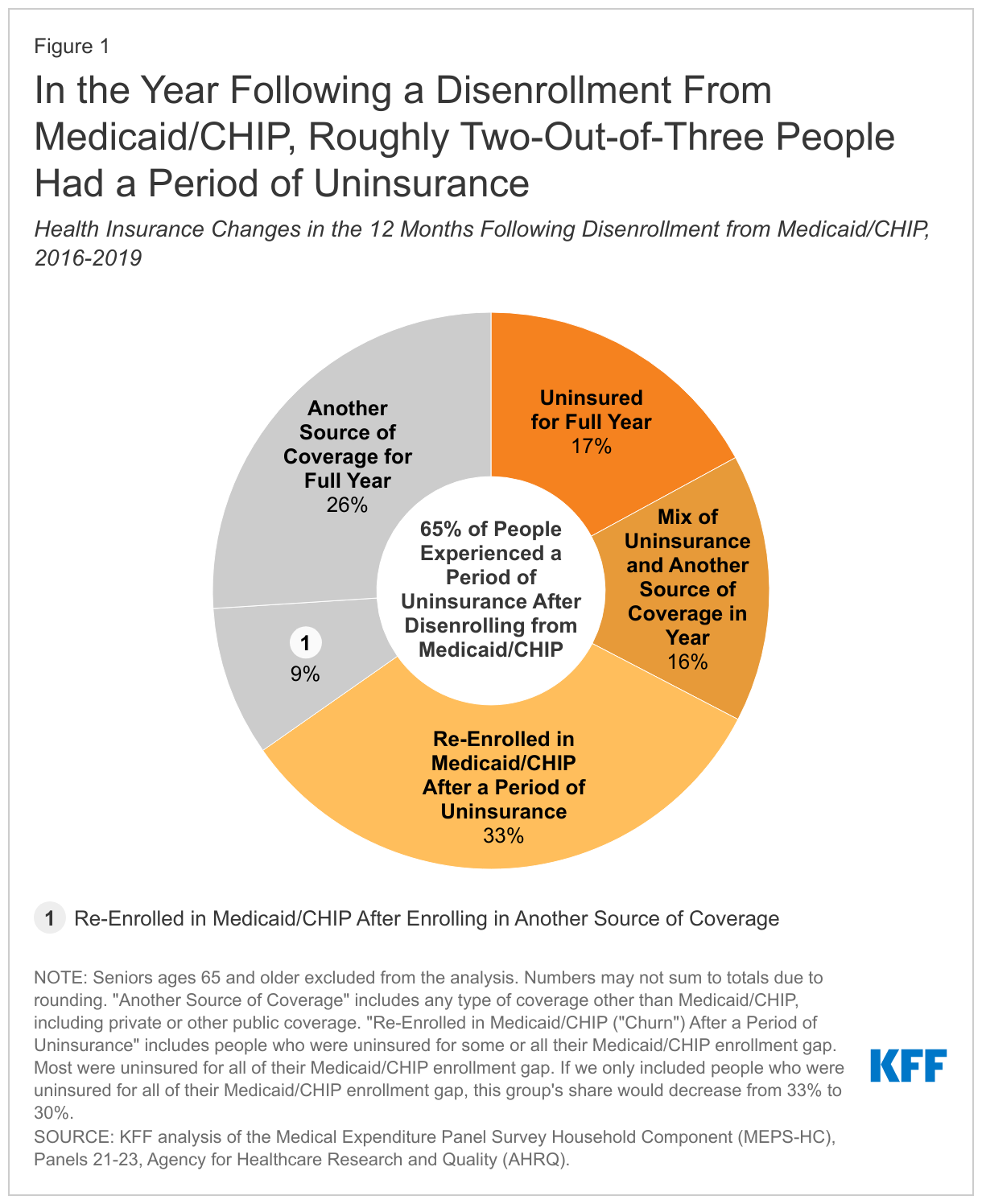
In the year following a disenrollment from Medicaid/CHIP, roughly two-thirds (65%) of people had a period of uninsurance.
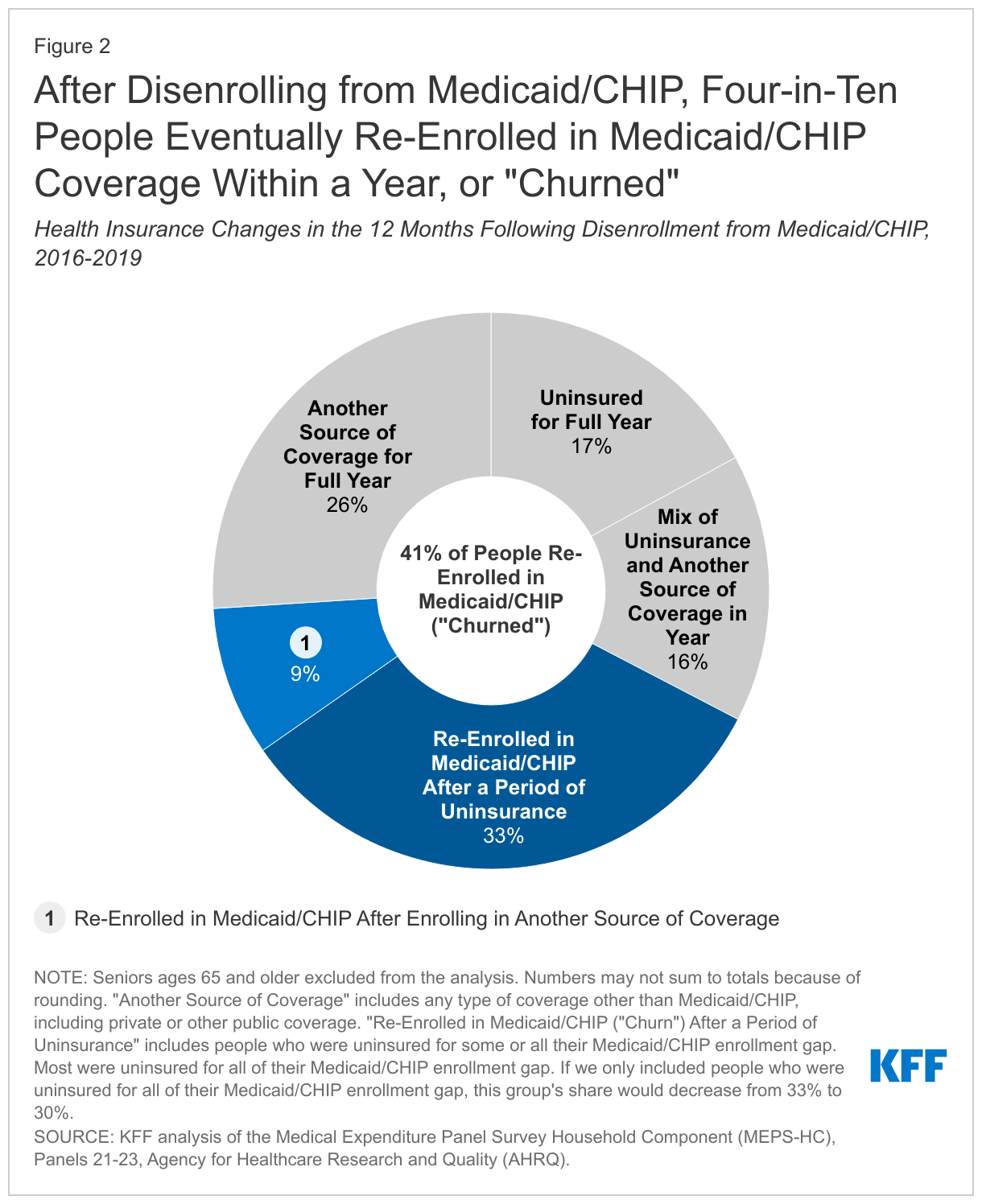
Roughly four in ten (41%) people who disenrolled from Medicaid/CHIP eventually re-enrolled in Medicaid/CHIP within a year (or “churn”).
Key Findings
In the year that followed a disenrollment from Medicaid/CHIP, roughly two-thirds (65%) of people had a period of uninsurance while just 35% were continuously enrolled in coverage (Figure 1). The 65% of Medicaid/CHIP enrollees who experienced uninsurance after disenrolling consists of people who were: uninsured for the full year (17%), uninsured for some of the year and had another source of coverage during the year (16%), and uninsured after disenrolling but eventually re-enrolled in Medicaid/CHIP (or “churned”) before the end of the year (33%). The 35% of Medicaid/CHIP enrollees who maintained coverage for the full year after disenrollment from Medicaid/CHIP consist of people who: were enrolled in another source of coverage for the full year (26%) and had another source of coverage for some of the year but also re-enrolled in Medicaid/CHIP before the year ended (9%). Notably, most1 of the people who were covered for the full year after disenrollment had a period of overlapping coverage before losing Medicaid/CHIP during which time they had both Medicaid/CHIP and private health insurance.
Roughly four in ten (41%) people who disenrolled from Medicaid/CHIP would eventually go on to re-enroll in Medicaid/CHIP within a year (Figure 2). That group consists of people who re-enrolled in Medicaid/CHIP after a period of uninsurance (33%) and who re-enrolled after having other coverage (9%). Among all enrollees who churned, 79% were uninsured before they re-enrolled in Medicaid/CHIP. Churn occurs for several reasons. Enrollees may experience short-term changes in income that make them temporarily ineligible. Churn may also happen when people who are still eligible for Medicaid/CHIP lose coverage for administrative reasons, such as difficulties completing annual renewals. Ultimately, churning on and off Medicaid/CHIP can limit access to care and lead to delays in getting needed care. Even for people who have other coverage before re-enrolling in Medicaid/CHIP, churning can cause disruptions in coverage when it requires people to change their health care providers or to navigate through different benefit packages.
Implications
These findings highlight that many people do not transition to and retain other coverage after they disenroll from Medicaid/CHIP. Overall, 65% of the people had a gap in coverage during the year following disenrollment from Medicaid/CHIP and only 26% of people enrolled in and retained another source of coverage for the full year after losing Medicaid/CHIP coverage. Of people who disenroll from Medicaid/CHIP, 41% re-enrolled within the year. That number includes 33% who re-enrolled in Medicaid/CHIP after a period of uninsurance, suggesting that many people were still eligible when they lost Medicaid/CHIP coverage. Even among people who initially enrolled in other coverage, 34% did not retain it for the full year; these individuals eventually lost their other coverage (and become uninsured) or they re-enrolled in Medicaid/CHIP. Generally, people in our analysis who had overlapping coverage (i.e., Medicaid/CHIP and private coverage) prior to losing Medicaid/CHIP were less likely to become uninsured or churn compared to those who did not have overlapping coverage.
KFF estimates that between 5 and 14 million people will lose Medicaid coverage when states “unwind” the continuous enrollment provision this year. Beginning April 1, 2023, states can resume disenrollments for the first time since March 2020. Some of the people who will be disenrolled during the unwinding will be ineligible and will become uninsured if they do not transition to other coverage. Others will lose coverage for administrative reasons despite still being eligible. While the millions of people who lose coverage during the unwinding will face similar challenges as those included in this analysis, there are also important differences today. For one, Congress extended enhanced subsidies for the ACA marketplace, which were first included in the American Rescue Plan Act (ARPA) during the pandemic, making those plans more affordable through 2025. Additionally, because of the continuous enrollment provision, an increasing number of Medicaid enrollees today report also being enrolled in private insurance compared to before the pandemic, which should reduce coverage disruptions for these individuals when they disenroll from Medicaid. However, this only represents a subset of people who will be disenrolled during the unwinding process. Most individuals who will lose Medicaid during the unwinding because they are no longer eligible will still need to transition to (and retain) other health insurance to avoid a gap in coverage.
State Medicaid agencies and other stakeholders can take several steps to reduce coverage disruptions and churn during the unwinding period. Broadly, these actions could include improving state eligibility systems, streamlining renewal procedures, communicating with enrollees about the need to complete a renewal, and facilitating transitions to the ACA marketplace or separate CHIP coverage for people found ineligible for Medicaid. The federal government has issued guidance aimed at reducing coverage disruptions for Medicaid/CHIP enrollees and has imposed new reporting requirements to monitor states’ unwinding processes. Although our analysis provides a pre-pandemic baseline for peoples’ health insurance changes after losing Medicaid/CHIP coverage, state policies for the unwinding will have a major impact on whether people will be more successful in transitioning to other coverage after losing Medicaid compared to pre-pandemic trends.
Methods
Data Source
This analysis uses data from the Medical Expenditure Panel Survey (MEPS) for panels 21, 22, and 23, which were collected between 2016 and 2019. MEPS panels generally cover a two-year period (24 months), although panel 23 was extended for an additional year due to the coronavirus pandemic. Our analysis only used the first 2 years (24 months) of panel 23. Our estimates account for the MEPS survey design and use longitudinal weights. We used monthly insurance variables to identify Medicaid enrollees and health insurance outcomes during the study period.
Study Population and Exclusions
We limited our analysis to individuals who were disenrolled from Medicaid/CHIP within the first 13 months of the survey panel to allow for a full 12-month follow-up period. We further limited the analysis to people with at least four consecutive months of Medicaid/CHIP before they disenrolled to exclude anyone who was enrolled under presumptive eligibility or for emergency services but then determined to be ineligible. We excluded people ages 65 and older and those under 65 with Medicare because Medicare is the primary payer for acute care when people have both Medicare and Medicaid. Finally, we excluded a small number of individuals who were out of the survey’s scope during the study period (for example, if someone dies, moves out of the country, or becomes institutionalized). After these exclusions, our final sample included 1,160 respondents.
Health Insurance Status
For each month during the panel, we created an indicator that classified individuals as either enrolled in Medicaid; having other, non-Medicaid coverage; or as uninsured. For people with Medicaid, we also created another indicator that identified whether individuals had a secondary source of coverage while enrolled in Medicaid. Notably, in 2018, MEPS modified how they asked the health coverage questions for individuals living in the same household as the primary respondent. Up to 2018 health coverage questions were asked at the household level (e.g., “Has anyone in the family been covered by…?”), but the questionnaire was updated to ask these questions as the person level (e.g., “Was Person 1 covered by…?”). However, we expect that the change had minimal impact on how respondents reported health insurance coverage for household members.
Thirty-five percent of people disenrolled from Medicaid/CHIP had health coverage for the full year after disenrollment. Of these people, 71% had both Medicaid/CHIP and private health insurance before losing Medicaid/CHIP. Typically, these individuals only had 1 to 4 months of overlapping coverage before disenrolling from Medicaid/CHIP. Generally, people with multiple sources of coverage before disenrolling were more likely have coverage for the full year and were less likely to churn compared to people who did not have overlapping coverage. ↩︎
As 2023 kicks off, a number of issues are at play that could affect coverage and financing under Medicaid, the primary program providing comprehensive health and long-term care coverage to low-income Americans. The Consolidated Appropriations Act, passed in December 2022, ends the Medicaid continuous enrollment provision on March 31, 2023 with a phase-down in enhanced federal matching funds. The unwinding of this provision, as well as the trajectory of the pandemic and the economy, will have implications for Medicaid enrollees, providers, managed care plans, and the states that operate these programs. A divided Congress will make it difficult to pass federal legislation, and while the Administration is expected to continue to use existing authority to improve coverage, access, and health equity, limited action at the federal level will push even more policy focus to the states. The first glimpse of state policy priorities will be revealed in Governors’ state of the state addresses and proposed budgets. Within this context, this issue brief examines key issues to watch in Medicaid in 2023.
Medicaid Coverage and Financing
The Medicaid continuous enrollment provision in place during the pandemic has increased enrollment and reduced the uninsured rate, but will end in March 2023. Provisions in the Families First Coronavirus Response Act (FFCRA) required states to ensure continuous enrollment in Medicaid in exchange for enhanced federal matching funds during the Public Health Emergency (PHE). Largely due to these policies, enrollment in Medicaid and the Children’s Health Insurance Program (CHIP) grew to 91 million in September 2022, an increase of 27.9% from February 2020 (prior to the pandemic). KFF estimates that through federal fiscal year 2022, states received more than double the amount in federal fiscal relief relative to the costs of enrollment due to the continuous enrollment provision, with some variation across states. The Consolidated Appropriations Act ends the continuous enrollment provision on March 31, 2023, and phases down the enhanced federal Medicaid matching funds through December 2023. States can resume disenrollments beginning April 1 but must meet certain eligibility and reporting requirements to continue to be eligible for enhanced funding. An estimated 5 to 15 million people could lose Medicaid coverage during unwinding and how states manage the process could affect how many people are able to maintain coverage.
Debate about Medicaid expansion will shift back to the states. Democrats in Congress last year discussed a federal option to fill in the Medicaid coverage gap but ultimately did not pass it, and such an approach is now highly unlikely with divided control in Washington. The American Rescue Plan Act (ARPA) included a two-year fiscal incentive to encourage remaining “non-expansion” states to newly adopt the Affordable Care Act (ACA) Medicaid expansion. Over 2 million individuals living in the 11 states that have not adopted the ACA Medicaid expansion fall into the “coverage gap.” These individuals do not qualify for Medicaid (as their income exceeds Medicaid eligibility limits in their respective states) but have incomes below poverty, making them ineligible for premium subsidies in the ACA Marketplace. A KFF analysis shows that all non-expansion states would see a net fiscal benefit from the ARPA incentive for two years if they adopt the expansion. The ARPA federal incentive reignited discussion around Medicaid expansion in a few non-expansion states during the last state legislative session. Notably, every state that has adopted expansion since 2019 has done so not through legislative or executive processes, but as a result of a successful ballot initiative. Most recently, South Dakota became the 40th state to expand Medicaid after voters approved a ballot question in November 2022. Although expansion ballot initiatives have been successful in all seven states where they have gone to voters (Idaho, Maine, Missouri, Nebraska, Oklahoma, and Utah), most of the remaining non-expansion states do not have ballot initiative processes. North Carolina may be the state most likely to expand Medicaid next given how far efforts advanced last year, with active efforts in Kansas and Wyoming as well.
Some states and the Administration are expected to continue to implement incremental policies to expand coverage. ARPA included an option, made permanent in the Consolidated Appropriations Act, to allow states to extend postpartum coverage from 60 days to 12 months. Under current law, after the 60 days of postpartum coverage, many people who qualify for pregnancy-related Medicaid lose that coverage because Medicaid eligibility levels for parents are much lower than for pregnant people in most states, and especially in non-expansion states. As of January 2023, more than two-thirds of the states have taken steps to extend postpartum coverage. The Consolidated Appropriations Act also included a requirement for all states to implement 12 months of continuous coverage for children. In addition, Oregon received waiver approval to provide continuous eligibility for children from birth to age 6 and 2 years of continuous eligibility for all enrollees ages 6 and up, including adults; other states are seeking similar waivers for multi-year continuous eligibility. KFF analysis shows that for children, continuous eligibility policies help to provide coverage stability. Finally, the Administration released a proposed regulation designed to make it easier for individuals to obtain and retain coverage.
New state and federal attention to Medicaid financing could emerge in 2023. Medicaid financing is shared by the federal government and the states. Consequently, economic factors that affect state revenues including inflation, supply chain issues, and declining labor force participation rates, along with phase-down of the enhanced FMAP tied to the end of the continuous enrollment provision will have fiscal implications for states. In our annual state survey, states noted that inflation and workforce shortages were driving higher labor costs and pressure from providers for rate increases. Many states use reimbursement methodologies for some provider types, such as nursing facilities, that may automatically adjust for inflation. In addition, at the federal level the House of Representatives is likely to focus on measures to reduce the federal deficit and, while unlikely to pass in the Senate, proposals to limit federal spending for Medicaid could be debated again in Congress.
What to Watch:
What will happen to Medicaid enrollment during the unwinding of the continuous enrollment provision? How will changes vary across states? How many people losing Medicaid coverage will transition to other sources of insurance like the Affordable Care Act marketplaces, and what will happen to the number of uninsured?
Will any additional states implement Medicaid expansion or other coverage expansions like 12-month postpartum coverage?
How will administrative actions, including oversight of the unwinding of the continuous enrollment provision, waiver approvals, and new regulations contribute to changes in coverage?
How will broader economic factors, like inflation, affect state financing of Medicaid and will Congress debate broader proposals to cap federal Medicaid spending?
Access and Health Equity
Capitated managed care remains the predominant delivery system for Medicaid in most states. More than three-quarters of states that contract with MCOs (35 of 41) reported that 75% or more of their Medicaid beneficiaries were enrolled in MCOs as of July 1, 2022. Several states have recently implemented Medicaid managed care programs. Beginning July 1, 2021, North Carolina implemented its first MCO program, enrolling more than 1.8 million Medicaid beneficiaries in MCOs as of December 2022. Missouri implemented the ACA Medicaid expansion in October 2021, enrolling all expansion adults in Medicaid MCOs, and Oklahoma expects to implement capitated, comprehensive Medicaid managed care in October 2023. State managed care contracts vary widely in the populations required to enroll, the services covered, and the quality and performance incentives and penalties employed. Five multi-state, for-profit “parent” firms – Centene, UnitedHealth Group, Anthem, Aetna/CVS, and Molina – each have Medicaid MCOs in 12 or more states and account for half of all Medicaid MCO enrollment. MCOs are expected to play a large role in helping enrollees maintain coverage during the unwinding of the continuous enrollment provision. The Administration is expected to release revised regulations about Medicaid managed care and assuring access in Medicaid in the Spring of 2023.
In response to the pandemic, all states took action to expand coverage and access to telehealth in Medicaid, particularly for behavioral health services. In particular, nearly all states added or expanded audio-only telehealth coverage. These policy changes contributed to high telehealth utilization by Medicaid enrollees during the pandemic, overall and especially for behavioral health services. The rapid expansion of Medicaid telehealth policies and utilization has prompted state and federal questions about the quality of services delivered via telehealth. Most states have implemented or are planning initiatives to assess telehealth quality, though many states report ongoing considerations and uncertainty over how to effectively evaluate quality. States also report actions to address other telehealth challenges, including access to technology and broadband, program integrity, outreach and education, and equity. Most states have or plan to adopt permanent Medicaid telehealth expansions that will remain in place after the pandemic, including expansions of allowable modalities, services, and providers. At the same time, some states are considering guardrails on such policies, particularly for audio-only telehealth.
Beyond telehealth, many states are taking steps to expand access to behavioral health services as the pandemic has heightened demand for these services. Nine in ten Americans believe the nation is in the midst of a mental health crisis. Behavioral health conditions (i.e., mental health and substance use disorders) are more prevalent in Medicaid enrollees compared to people with other coverage, with data from 2020 showing that approximately 39% of Medicaid enrollees were living with a mental health or substance use disorder. States have been expanding behavioral health benefits and access to care, including by adopting strategies to bolster the behavioral health workforce. These state efforts track with continued activity at the federal level: the Consolidated Appropriations Act and the 2022 Bipartisan Safer Communities Act included an array of provisions to expand access and funding for behavioral health, such as provisions to require guidance on expanding Medicaid-covered mental health services in schools, expand Certified Community Behavioral Health Clinics (CCBHC), fund new psychiatry residency positions, and eliminate administrative requirements to prescribe buprenorphine.
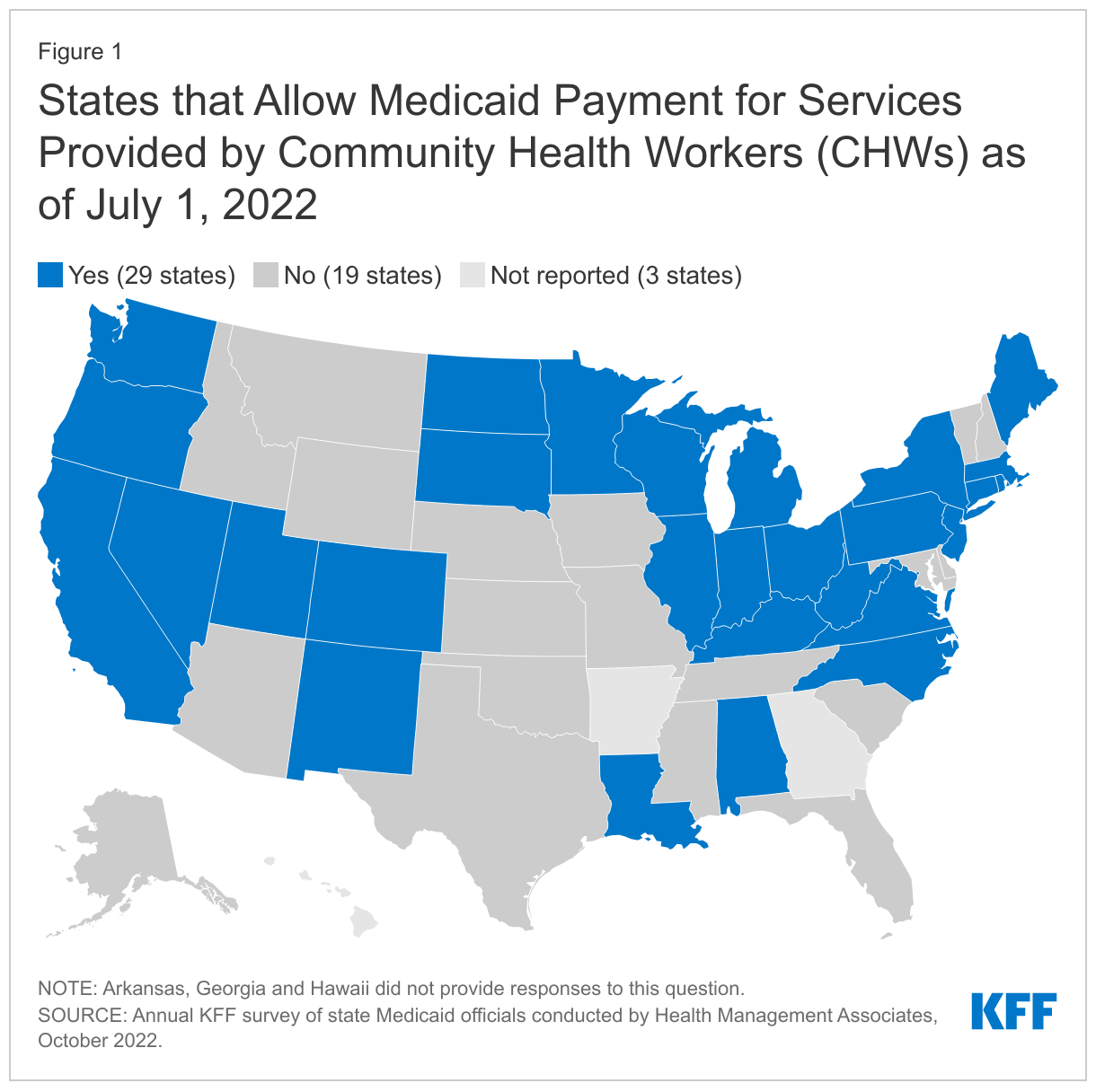
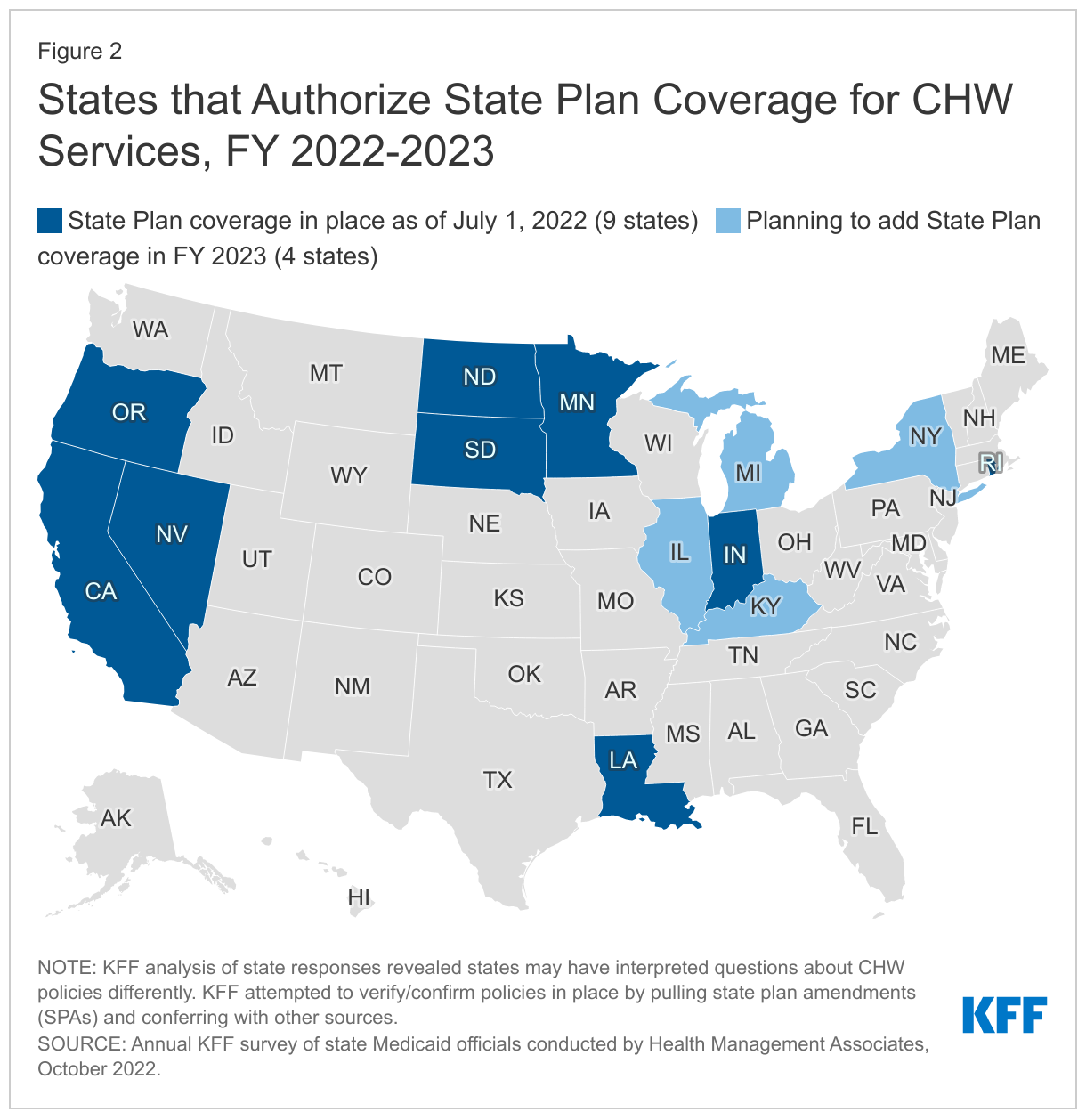
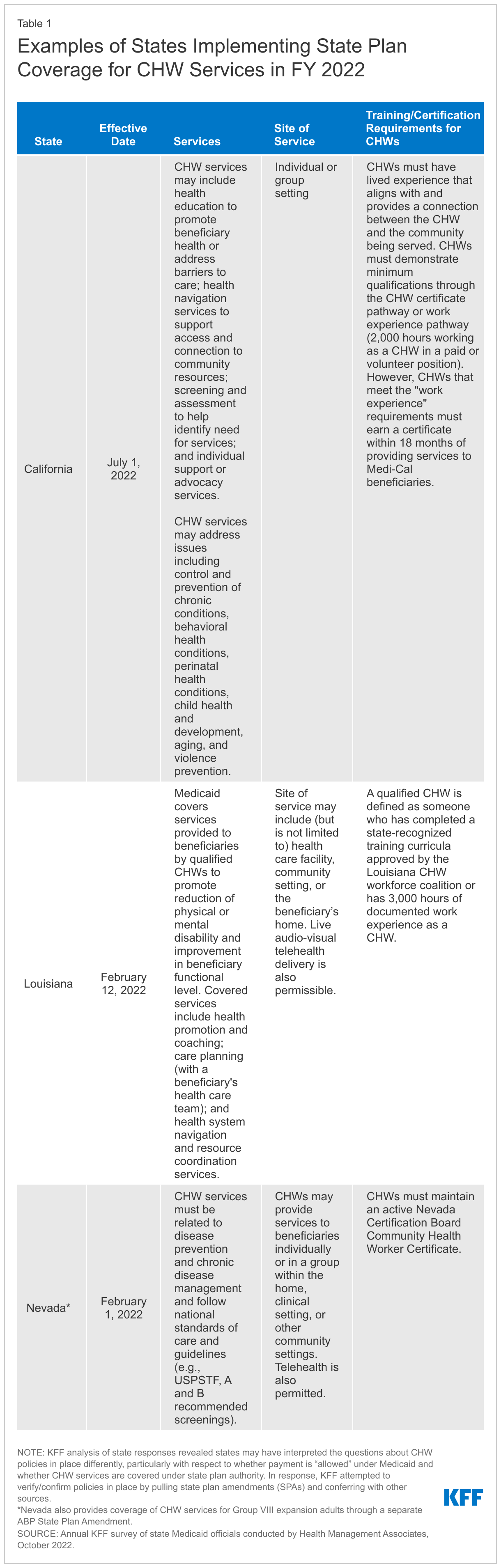
States and the Administration have identified advancing health equity as an important priority for the Medicaid program. The pandemic exacerbated longstanding racial and ethnic disparities in health and health care. Medicaid policies that could help address health equity include closing the “coverage gap” for adults in non-expansion states; increasing coverage among those eligible but not enrolled; and expanding benefits such as pregnancy and postpartum services, housing and housing-related supports, and community health worker services. High-quality, comprehensive data are essential for identifying and addressing health disparities and measuring progress over time and the majority of states are implementing strategies to improve race, ethnicity, and language (REL) data completeness. States are also using MCO financial quality incentives (e.g., performance bonuses, withholds) tied to health equity-related performance goals and other MCO contract requirements to advance health equity. Other reported state Medicaid initiatives to reduce racial health disparities include outreach to underserved populations, increasing cultural competency, and establishing departments and dedicated staff positions focused on promoting equity. In addition, states have received or are seeking Section 1115 waivers that aim to advance equity.
States and the Administration are implementing strategies to leverage Medicaid to address social determinants of health (SDOH) through managed care and Section 1115 waivers. The Biden Administration has encouraged states to propose waivers that expand coverage, reduce health disparities, and/or advance “whole-person care,” including by addressing health-related social needs (HRSN). Recent waivers approved in four states (AR, AZ, MA, and OR) include HRSN services to address food insecurity and/or housing instability for targeted populations. Additionally, following the approval of a California proposal to use “in lieu of” services (ILOS) to offer a menu of health-related services through managed care authority, the Centers for Medicare and Medicaid Services (CMS) recently released additional guidance on the use of in lieu of services and settings in Medicaid managed care to reduce health disparities and address unmet HRSN (such as housing instability and nutrition insecurity).
What to watch?
How effective will state and administration efforts to leverage Medicaid be in addressing SDOH and reducing health disparities? How will states use authorities including Section 1115 and managed care to pursue these goals?
What kinds of permanent telehealth expansions and/or guardrails will state Medicaid agencies adopt, and how will these policy changes be informed by data analyses, federal guidance, and cost concerns?
Will the Administration release new guidance in 2023 to address access to care and what provisions will be included in the anticipated access and revised managed care regulations?
Will Congress pass additional legislation and / or will states take additional actions to improve access to and funding for behavioral health services?
Enrollment and Access Among People Eligible for Medicaid through Age or Disability
The new proposed rule on eligibility and enrollment could increase enrollment among all Medicaid eligibility groups, but especially among seniors and people with disabilities. A proposed rule designed to make it easier for people to obtain and maintain coverage in Medicaid and CHIP includes provisions to simplify the enrollment and renewal processes for seniors and people with disabilities by applying many of the ACA’s simplified eligibility processes for children and other adult eligibility groups to these groups. There would also be simplified enrollment procedures for people who receive supplemental security income and people who are enrolled in Medicare but eligible for Medicaid coverage of Medicare premiums. KFF analysis finds that over one-third of Medicare-Medicaid enrollees lose Medicaid coverage within one year of their initial enrollment, which is one of the reasons for the proposed changes. CMS expects that the rule would increase Medicaid enrollment by nearly 3 million full-year equivalents, with seniors and people with disabilities accounting for over half of that total.
Staff and residents at long-term care facilities have been disproportionately affected by the pandemic. Over one-fifth of all deaths from COVID-19 were among residents and staff in long-term care facilities as of June 12, 2022. Although initial vaccination rates were high and the death rate among nursing facility residents and staff dropped, take-up of boosters and of the new bivalent booster has been much lower. Going into the 2022-2023 winter period, fewer than half of residents and one quarter of staff were up-to-date with their vaccinations, which may result in higher death rates moving forward. Compounding the challenges with COVID-19 illness is the ongoing workforce shortage for long-term care facilities. Whereas employment in most health care sectors has rebounded from the sharp drop in March 2020, employment in long-term care facilities remains well-below pre-pandemic levels.
The pandemic also highlighted workforce shortages and unmet need among people who use long-term services and supports (LTSS) delivered in home and community settings (HCBS). In a KFF survey of HCBS programs, nearly all states reported that workforce shortages were the number one impact of the COVID-19 pandemic on HCBS services and 44 states reported that at least one HCBS provider permanently closed. Virtually all states increased payment rates in response, but some of those increases are temporary rather than permanent. Many changes to HCBS programs relied on temporary funding through the ARPA or temporary authorities available during the PHE. Policymakers of both parties have called for additional and longer-term changes to HCBS including eliminating waiting lists for services, increasing opportunities for family members to be paid caregivers, enabling more people to live in their homes as they age, and permanently increasing wages for all HCBS providers.
There is bipartisan interest in improving the coordination for Medicare-Medicaid enrollees (also known as “dual eligibles”). People who are enrolled in both Medicare and Medicaid tend to have significant health and functional needs and higher health care spending than people with only Medicare or Medicaid. Policymakers have expressed interest in improving the coordination between Medicare and Medicaid with the goals of improved health outcomes and, possibly, reduced health care spending. Most recently, a bipartisan group of senators released a request for information, soliciting input from patients, providers, payors, and other stakeholders.
What to Watch:
How will the final eligibility and enrollment rule increase enrollment for seniors and people with disabilities?
Will nursing facility residents and staff be at increased risk of death as the virus evolves and immunity wanes among people who are vaccinated but not up to date? What efforts will emerge to improve rates of booster take-up?
How will the end of ARPA funding and PHE authorities affect access to HCBS?
Will bipartisan interest in improving the coordination between Medicare and Medicaid result in new legislation addressing Medicare-Medicare enrollees and their access to care?
Early in the COVID-19 pandemic, many outpatient visits and elective hospitalizations were delayed, avoided, or cancelled, leading to a sharp decline in health care utilization. However, there have been expectations that there will be pent-up demand for this missed care.
Using a variety of data sources, this chart collection examines the latest available data on how health services utilization has changed over the course of the pandemic. We find that, as of mid-to-late 2022, utilization of healthcare is generally rebounding, but some of that use is likely for COVID-related treatment, testing, or vaccination, making it difficult to assess how non-COVID care compares to the amount of care people received pre-pandemic. It is likely that utilization of some services, particularly for non-COVID care, remains below expectations based on pre-pandemic trends.
The chart collection is available on the Peterson-KFF Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
Assessing the Role of Treaties, Conventions, Institutions, and Other International Agreements in the Global COVID-19 Response: Implications for the Future
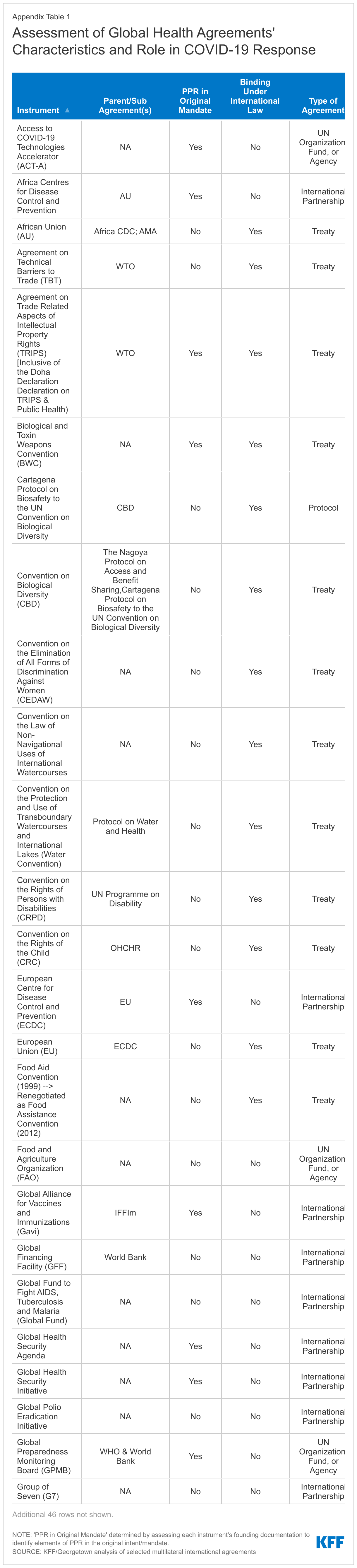
The COVID-19 pandemic has tested global health governance and international law in unprecedented ways, revealing weaknesses and gaps in the existing global health security architecture and fueling debate over how to strengthen global governance of disease. In December of 2021, the World Health Assembly (WHA) agreed to launch a process to develop a new international agreement on pandemic prevention, preparedness and response, with at least an initial outcome expected in 2024. To date, there has been no detailed examination of existing global health treaties, commitments, partnerships, organizations, and other global health agreements (hereafter referred to as “agreements”) to identify gaps and potential areas of collaboration moving forward. To help inform these discussions, we reviewed existing agreements to assess their potential role in pandemic preparedness and response efforts, and whether they were used to respond to COVID-19. Key findings are as follows:
71 agreements were identified as having a role in global health. These agreements, some of which are more than 100 years old and others that were established only recently, address a wide range of areas including diseases (HIV, malaria, tuberculosis, etc.), vulnerable populations (children, women, refugees, etc.), the environment, and trade/intellectual property, among others.
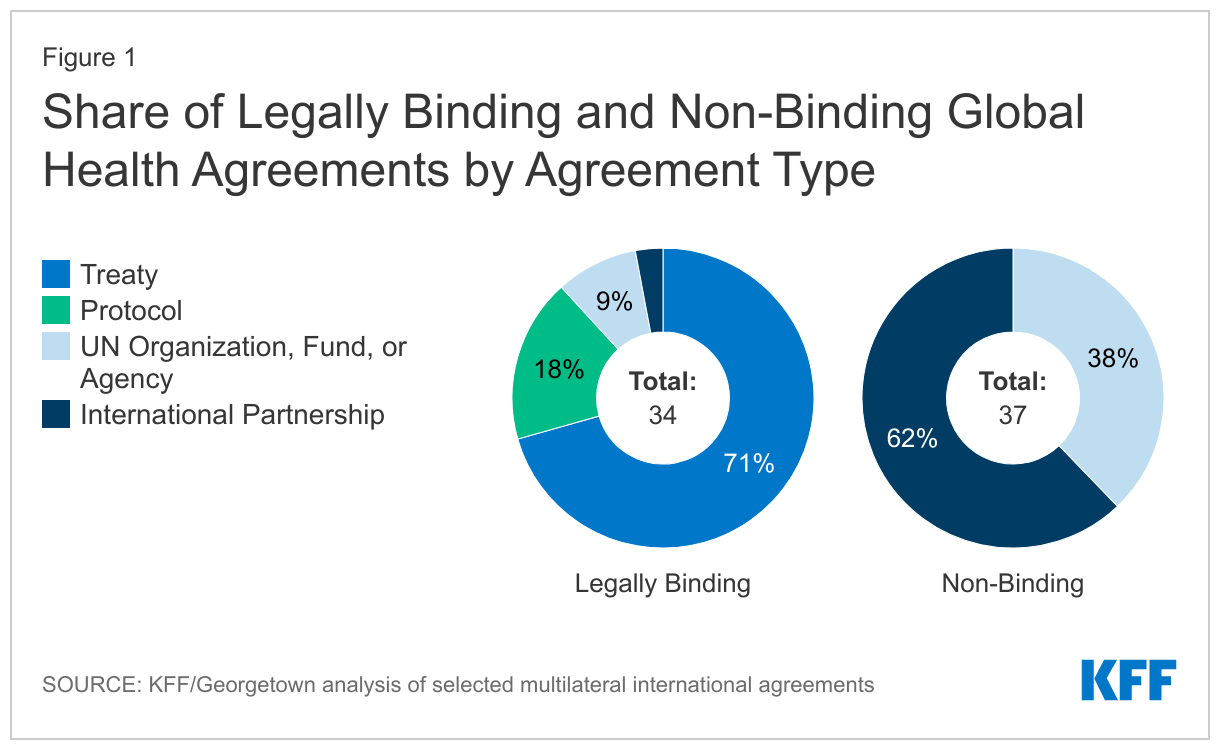
Nearly half (34) of these agreements are binding under international law. Legally binding agreements are those intended to create enforceable legal obligations in the international arena on their parties.1 The 34 binding agreements include treaties, protocols (which are associated with existing treaties), and the terms of memberships in some United Nations (UN) entities such as the World Health Organization (WHO). The remaining 37 agreements, while not legally binding, may confer obligations and commitments upon participating countries.
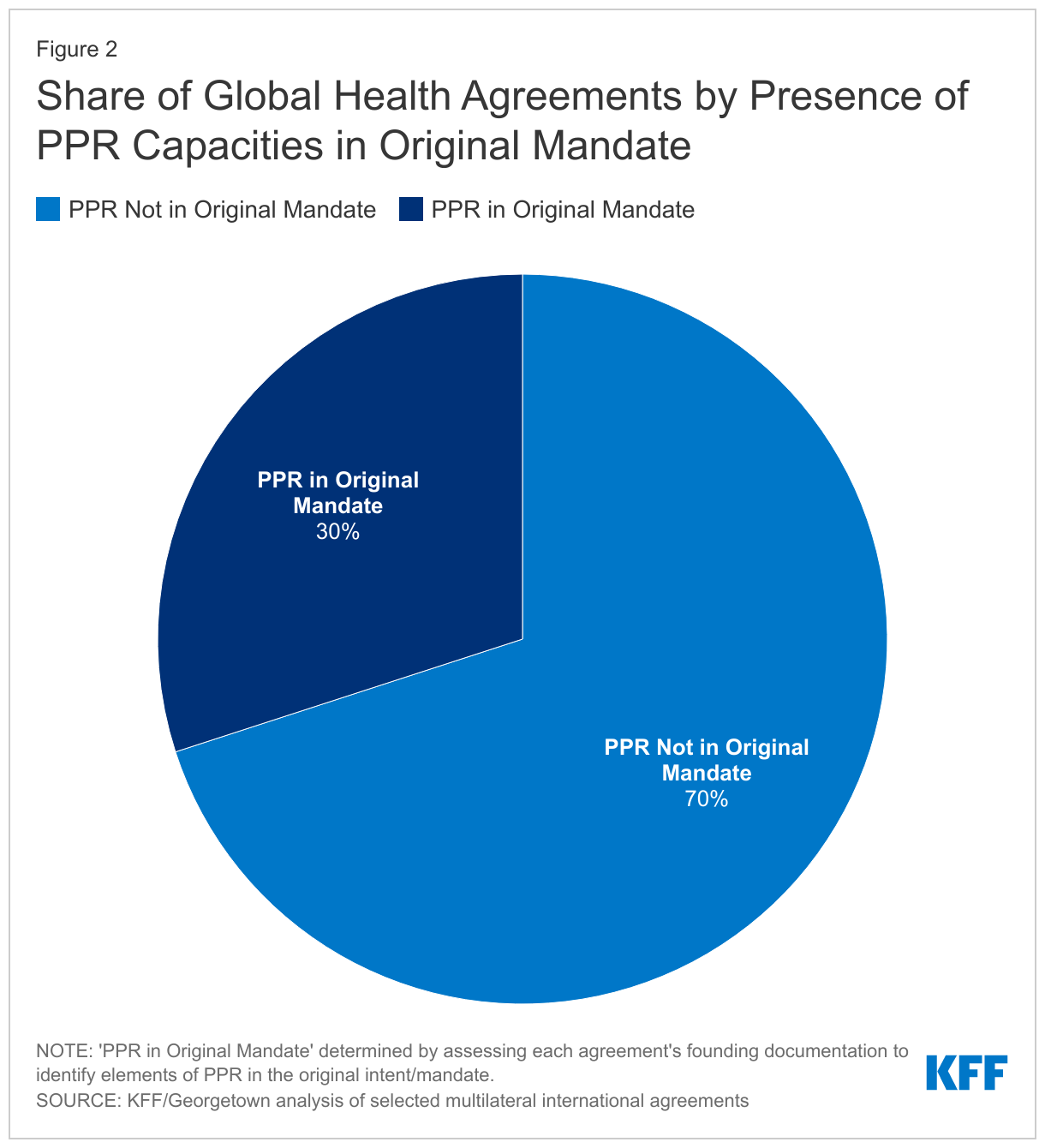
Less than one-third (21 or 30%) of the agreements have pandemic preparedness and response (PPR) as part of their original mandate. Of these 21 agreements, 9 are legally binding under international law.
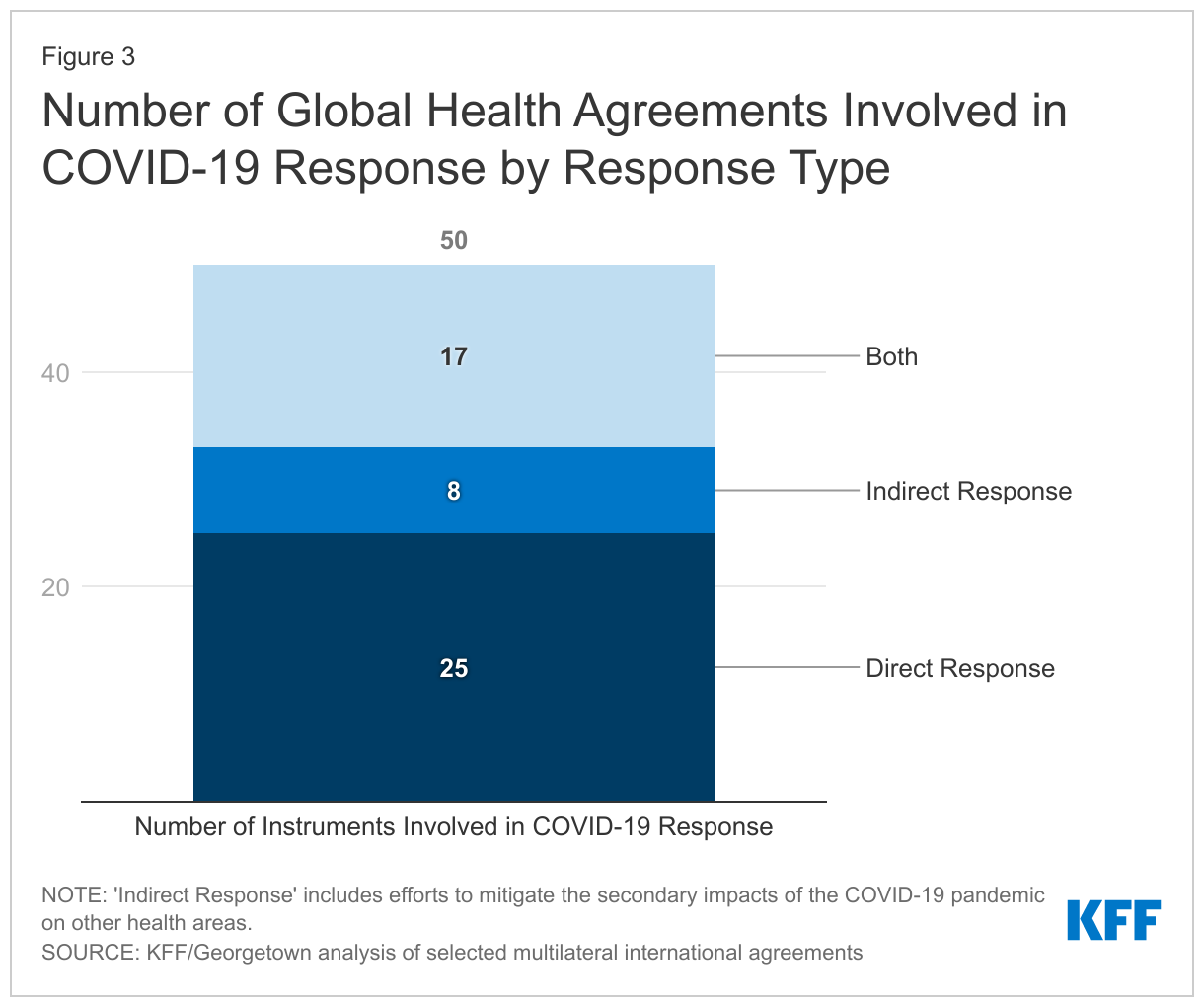
Still, most (50 or 70%) of these agreements participated in the COVID-19 response. They were either involved directly (25), via activities specifically aimed at addressing the pandemic, indirectly (8), through activities that addressed the impacts of the pandemic on other health areas, or some combination of both (17). Thirty-six did not have PPR in their original mandate but either adapted existing efforts or started new activities to address the pandemic.
The 71 agreements identified in this review could play a key role in the next phase of pandemic preparedness and response, including many that did not have PPR in their original mandate. As the global community considers a new international instrument to help prepare for and respond to future pandemics, our analysis finds that many of the existing agreements were mobilized to address COVID-19 and others have PPR as part of their original mandate. The extent to which these existing agreements could be part of future preparedness efforts remains to be seen but further research could help to highlight whether additional strengthening or further adaptation is needed, as well as highlight gaps that may persist.
Introduction
The COVID-19 pandemic tested global health governance and international law in unprecedented ways, revealing weaknesses and gaps in the existing global health security architecture and fueling debate over how to strengthen global governance of disease. Starting in late 2020, nations and expert groups began discussing the potential need for a new international agreement addressing pandemic preparedness and response (PPR). In December 2021, the World Health Assembly (WHA) agreed to launch a process to develop such an agreement. As part of this process, the WHA has established an Intergovernmental Negotiating Body (INB) “to draft and negotiate a WHO convention, agreement or other international agreement on pandemic prevention, preparedness and response” with an outcome for consideration expected in 2024. At its meeting held in July 2022, INB members agreed that at least some elements of the new international pandemic agreement should be legally-binding, although this decision is not yet final. The INB recently released a draft of the agreement which lays out a proposed governance structure for the new agreement as well as the PPR activities parties may be expected to undertake, such as improving supply chains and logistics networks, supporting information sharing and technology transfer, increasing research and development capabilities, and strengthening health systems and workforce. However, final text is not expected until 2024.
To help inform the current conversation, we reviewed existing international global health agreements (e.g. International Health Regulations), organizational charters (e.g., World Health Organization; Global Fund to Fight AIDS, Tuberculosis and Malaria; etc.), and institutions that have issued declarations addressing global health issues (e.g., World Bank, G7, G20, etc.) to assess their role in pandemic preparedness and response efforts, including whether they have played a role in the COVID-19 response, to help identify existing gaps and potential areas of collaboration with other organizations in the PPR space. This analysis builds on work researchers at KFF and Georgetown University conducted more than a decade ago exploring U.S. involvement in international health treaties and other global health organizations. For this analysis, we confirmed whether the agreements included in our original analysis were still active and identified additional agreements that should be included (e.g., those that have taken on a greater role in health or were created since the original paper was published). We assessed the extent to which each agreement has been involved in the COVID-19 response (either directly or indirectly) and/or possessed pandemic preparedness and response capacities. We considered agreements to be “directly” involved in the COVID-19 response if they addressed the impacts of COVID itself (e.g., provided medical countermeasures or other COVID-specific support). Agreements considered to be “indirectly” involved were those that sought to address the impacts of COVID on other health areas (e.g., provided support to maintain or reduce the effect of COVID on the response to another communicable disease). We defined agreements broadly to include both those that were legally-binding as well as non-binding agreements, partnerships, and the charters establishing United Nations entities and formally established global institutions (see Methodology for more detail).
Findings
Overall, we identified 71 global health agreements, including 46 that were included in our original analysis.2 An additional 13 were already established but had not been originally included (they had taken on a greater role in health) and 12 were more recently created. The earliest agreement was established in 1902 (the Pan American Health Organization, originally the Pan-American Sanitary Bureau) and the most recent in 2021 (The Treaty of the African Medicines Agency). They span a range of focus areas, including diseases (HIV, malaria, tuberculosis, etc.), vulnerable populations (children, women, refugees, etc.), the environment, and trade/intellectual property, among others, and have varying levels of enforcement power and strength. Though a minority of the agreements reviewed had PPR in their original mandate, most were utilized in the COVID-19 response in some way, with many organizations taking on new roles to do so. Our specific findings are as follows:
Legal Status
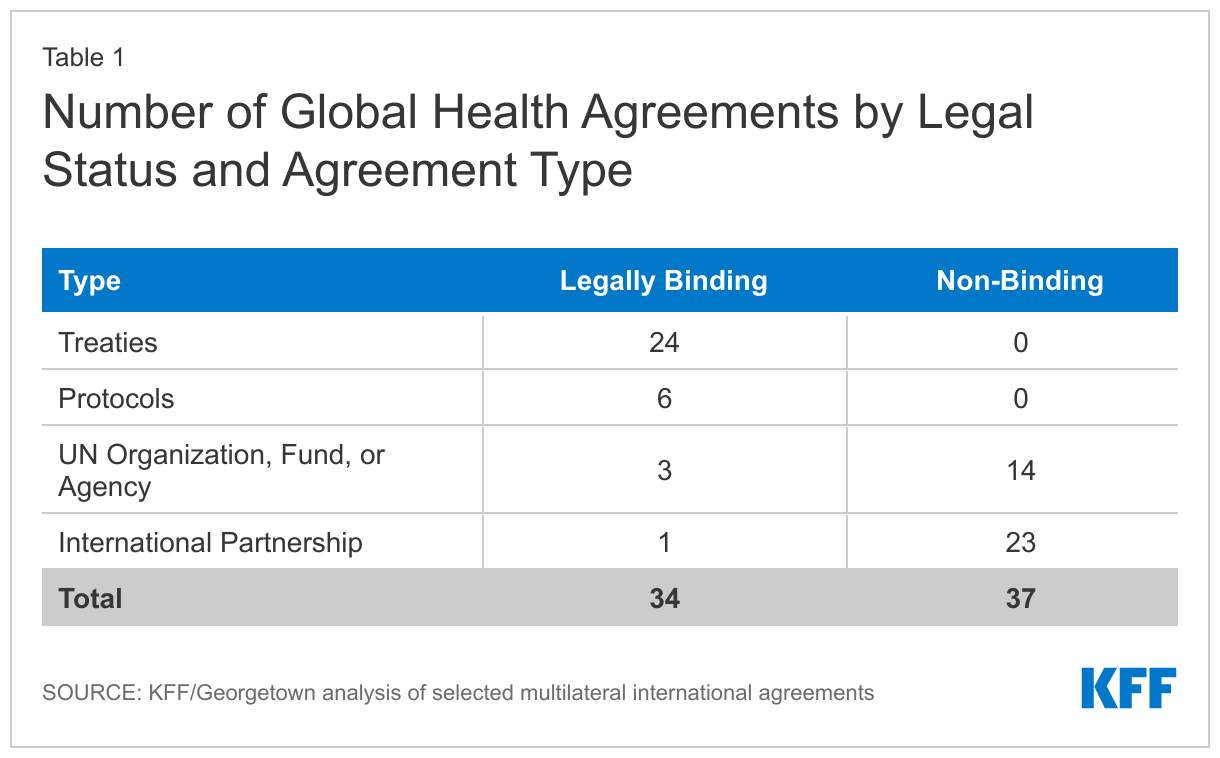
Nearly half (34) of the 71 agreements reviewed are legally-binding under international law (see Figure 1). These include 24 treaties, 6 protocols (which are associated with existing treaties), 3 United Nations organizations, funds, or specialized agencies (WHO, WTO, and WIPO), and one other international agreement (OECD) (see Table 1). Treaties include trade-related agreements under the World Trade Organization (WTO), which are binding under international law for WTO member countries, membership in international health organizations such as the World Health Organization (WHO) and the Pan American Health Organization (PAHO), and other legally binding agreements such as the International Health Regulations (2005)3 . Protocols include many of the agreements focused on environmental issues such as the Kyoto and Nagoya protocols.
The remaining 37 agreements are not legally-binding under international law, but include agreements that confer obligations on members, including participation in organizations with global health mandates. Most of these (23) are “international partnerships”, which include initiatives such as the Sustainable Development Goals (SDGs) and Universal Health Coverage (UHC) 2030, as well as formal institutional arrangements of regional member states, such as the Africa Centres for Disease Control and Prevention (CDC), and broader alliances such as the Group of Seven (G7), Group of Twenty (G20), and North American Leaders’ Summit (NALS). “United Nations organizations, funds, or agencies” made up the remainder (14) and include entities such as the United Nations Environmental Programme (UNEP), United Nations Children’s Fund (UNICEF), and United Nations Population Fund (UNFPA).
PPR in Original Mandate
Of the 71 agreements examined, 21 (30%) included PPR, in some capacity, as part of their original mandate (see Figure 2). For example, the International Health Regulations (IHR) (2005) require countries to possess certain capacities around PPR, including detecting, assessing, reporting, and responding to public health emergencies. The Africa CDC’s agreement obligates the body to work with member countries to build disease surveillance systems capable of identifying health threats and to provide response support during health emergencies. Similarly, the European Centre for Disease Control and Prevention’s founding documents outline a surveillance and response strategy for emerging health threats. The Agreement on Trade Related Aspects of Intellectual Property Rights (TRIPS) and the accompanying Doha Declaration on the TRIPS Agreement and Public Health recognize the gravity of public health emergencies and speak to the potential for intellectual property rights flexibilities in the context of these public health emergencies.
Nine of these 21 are legally-binding. These are: The Agreement on the Application of Sanitary and Phytosanitary Measures (SPS Agreement), Biological and Toxin Weapons Convention (BWC); The IHR (2005); The Nagoya Protocol on Access and Benefit-Sharing; The Pan-American Sanitary Code; The Protocol on Water and Health; The TRIPS Agreement; the Treaty of the African Medicines Agency, and the World Health Organization.
COVID-19 Responses
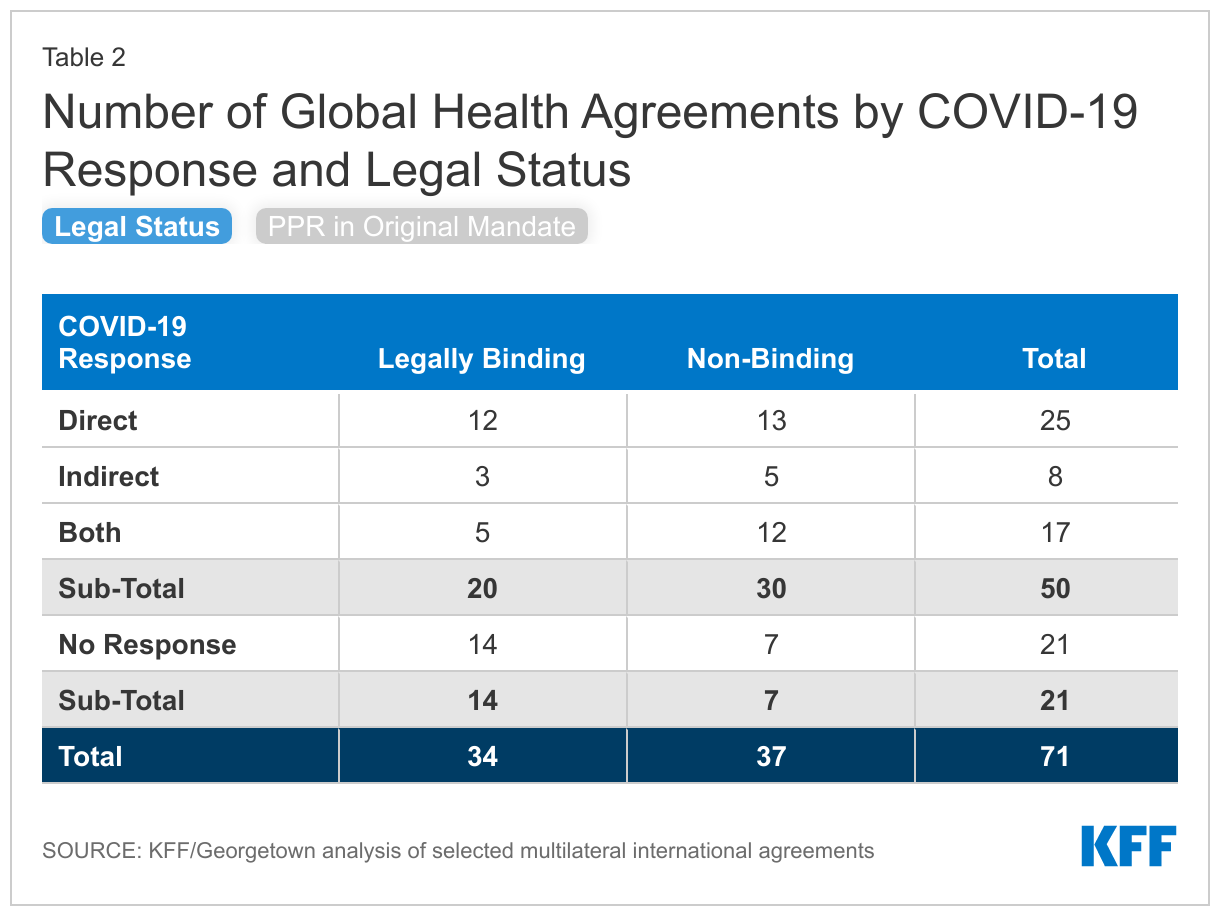
Most (50 or 70%) of the agreements reviewed were utilized to respond to the COVID-19 pandemic either directly (25), via activities specifically aimed at addressing the pandemic, indirectly (8), through activities that addressed the impacts of the pandemic on other health areas, or some combination of both (17) (see Figure 3). Twenty-one of these agreements are legally-binding (see Table 2).
The 25 agreements that exclusively supported the direct impacts of COVID-19 undertook a range of activities, such as provisioning medical countermeasures, training health care workers, shoring up laboratories and other health systems, and developing new governance mechanisms to coordinate the response. For example, the Access to COVID-19 Tools Accelerator (ACT-A) supported a range of activities focused on addressing the COVID-19 pandemic, including supporting the procurement of diagnostic tools, therapeutics, vaccines, and personal protective equipment, the World Organisation for Animal Health created several expert groups to develop guidelines related to animal health and COVID-19, and the Global Polio Eradication Initiative shifted its efforts to assist in the COVID-19 response by training laboratory workers to detect the virus.
Eight addressed only the indirect impacts of COVID-19 on other areas that aligned with their mandates. For example, the Stop TB Partnership issued guidance to help high TB burden countries integrate their TB and COVID-19 testing systems, and the Joint United Nations Programme on HIV/AIDS (UNAIDS) provided guidance on maintaining progress on HIV prevention in the context of the COVID-19 pandemic.
Seventeen engaged in both direct and indirect COVID-19 responses. For example, the Global Fund to Fight AIDS, Tuberculosis and Malaria procured COVID-19 diagnostics, treatments, and oxygen for the countries in which it works and set up the COVID-19 Response Mechanism (C19RM) to fund countries’ efforts to mitigate the impacts of COVID-19 on HIV, TB, and malaria; the United Nations World Food Programme supported both the delivery of COVID-19 supplies, such as personal protective equipment (PPE), as well as food assistance to address food insecurity resulting from the pandemic; and the Pan American Health Organization (PAHO) assisted countries in the procurement and delivery of vaccines, as well as provided guidance on maintaining essential health services in the context of COVID-19.
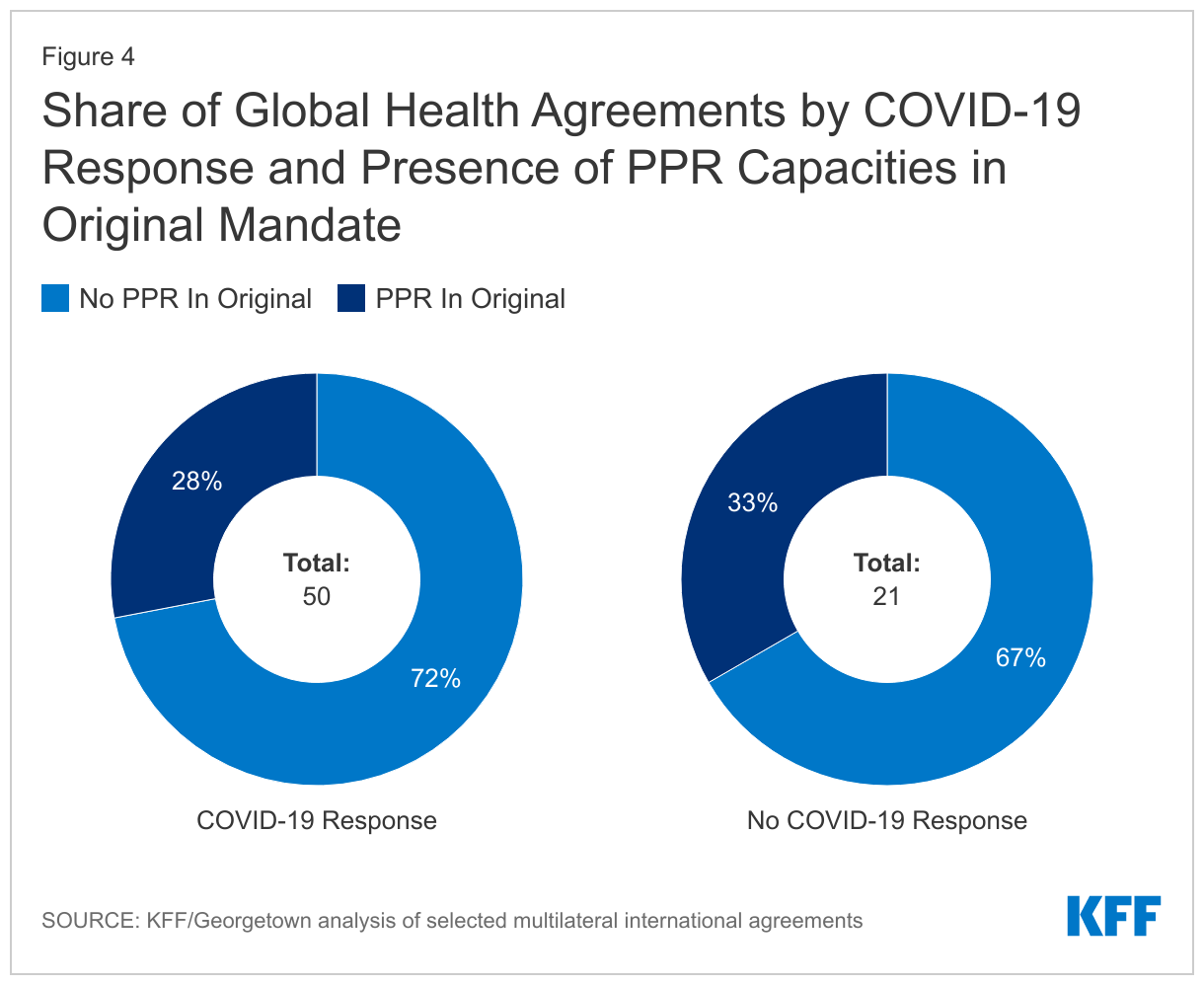
Most of the agreements involved in responding to COVID-19 (36 of 50) did not have PPR in their original mandate but adapted to address the pandemic (see Figure 4). These include the Global Fund, which established the COVID-19 Response Mechanism (C19RM) to provide grants to low- and middle-income countries for the purchase of test, treatments, and personal protective equipment (PPEs), and the World Bank, which established the COVID-19 Fast Track Facility and provided support for vaccine rollout.
A subset of agreements that were not involved in the COVID-19 pandemic response (7) contain PPR capacities in their original mandate. In some cases, this may be because COVID-19 fell outside their organizational scope (for example, water-borne diseases) or because these agreements were created very recently (for example, the Treaty of the African Medicines Agency).
Discussion
The COVID-19 pandemic has highlighted major gaps in global pandemic preparedness and response capabilities. This analysis outlines the international agreements already involved in pandemic preparedness and response to inform the development of a new pandemic agreement designed to address these gaps. Overall, we find that most of the agreements reviewed (50 of 71) have been involved in addressing the COVID-19 pandemic, either directly or indirectly. Most of these do not have PPR in their original mandate but, rather adapted to address the pandemic. In addition, half of the 71 agreements (34) are legally-binding, including 20 that responded to COVID. This suggests that there are already capacities to address PPR within existing agreements that could potentially be coordinated with a new framework. Importantly, though, this analysis does not attempt to assess the effectiveness of an agreement’s response to COVID-19 or its PPR capabilities more broadly, and future research could seek to do so. In addition, while most of the agreements responding to COVID-19 did so by adapting their work, we did not assess what was required to make such adaptations (e.g., whether new authorizations or mandates were needed). As global leaders continue to pursue the development of a new pandemic instrument, this review may help to identify agreements with existing PPR capabilities, including whether they need strengthening or further adaptation, as well as highlight gaps that may persist.
Methodology
We sought to identify multilateral international treaties, commitments, partnerships, organizations, and other agreements (“agreements”) that were health-specific or had a significant health component.4
We started with the list of agreements compiled and criteria used for our previous analysis, “U.S. Participation in International Health Treaties, Commitments, Partnerships, and Other Agreements”. Since the original report was completed over a decade ago, we revisited and reviewed the initial list to confirm whether each agreement was still active. We also revisited the sources (listed below) to determine if additional agreements warranted inclusion in this analysis (for example, if they had taken on a greater role in health or were created after the initial analysis). Each agreement was reviewed by multiple members of the team to ensure the accuracy of categorizations.
We analyzed both legally binding and nonbinding agreements and categorized each by type of agreement, and whether components of PPR were present in the agreement’s founding documents.5 Legally binding agreements were compiled based on a review of the Department of State’s required annual report to Congress on all Treaties in Force, the United Nations Treaty Collection, the Library of Congress reference collection on Treaties, the Congressional Research Service, and other reference documents. Nonbinding agreements were compiled based on a desktop review and include multilateral organizations, partnerships, consortia, and other arrangements. As such, the nonbinding list of agreements is comprehensive to the best of our knowledge but may not be exhaustive.
We then assessed each agreement to determine if it was involved in responding to COVID-19 either directly (through actions or the provision of services aimed at addressing the COVID-19 pandemic) or indirectly, to address the secondary effects of the pandemic (e.g., actions or the provision of services aimed at addressing other health-related activities, such as food aid, that have been directly affected by the pandemic). If an agreement was deemed to be “directly” involved in the COVID-19 response, it was automatically included under the PPR categorization. Agreements addressing the “secondary effects” of the COVID-19 response might not necessarily mean they would be involved in PPR activities. As such, there were several that were not involved in the COVID-19 response that were included under the PPR categorization. If an agreement was not deemed to be involved in the COVID-19 response or PPR, it was listed as “Other”. Several agreements resulted from or are directly related to previously established agreements (e.g., the Nagoya Protocol was established following the Convention on Biological Diversity) or are under the auspices of another entity (e.g., WHO manages the implementation of the International Health Regulations). In these instances, the parent agreement is classified as having the same role in the COVID-19 response as the sub-agreements.
Table 3: Agreement Role(s) in Global COVID-19 Response: Definitions
Category
Definition
COVID-19 Response
Direct
Supports efforts aimed directly at responding to and mitigating the impacts of the COVID-19 pandemic.
Secondary Effects
Supports mitigating the potential effects on other health activities resulting from the COVID-19 pandemic.
Pandemic Preparedness & Response (PPR)
Manages, directs, or supports efforts to prepare and respond to potential disease outbreaks. If an agreement is categorized as contributing to the COVID-19 response (either direct or secondary effects), it is deemed to also support PPR, but not vice versa.
Other
Aims to prevent or reduce the likelihood of virus emerging that could result in a pandemic or aids in the strengthening of country health systems.
Appendix
Anna Rouw, Adam Wexler and Jen Kates are with KFF.Kate Toole, Anjali Britto, and Rebecca Katz are with Georgetown University.
This total is inclusive of entities that have transformed or been renamed since the last publication (e.g. the International Health Partnership is now Universal Health Coverage 2030). ↩︎
The International Health Regulations (2005) were created under the auspices of another agreement included in this analysis, the WHO Constitution. ↩︎
The United Nations defines multilateral treaties as international agreements concluded between three or more parties, each possessing treatymaking capacity. Parties that have treaty-making capacity include sovereign States as well as international organizations with treaty-making capacity (e.g., the European Union). See: The United Nations Treaty Handbook. Bilateral agreements (country-to-country) were not included in this analysis. ↩︎
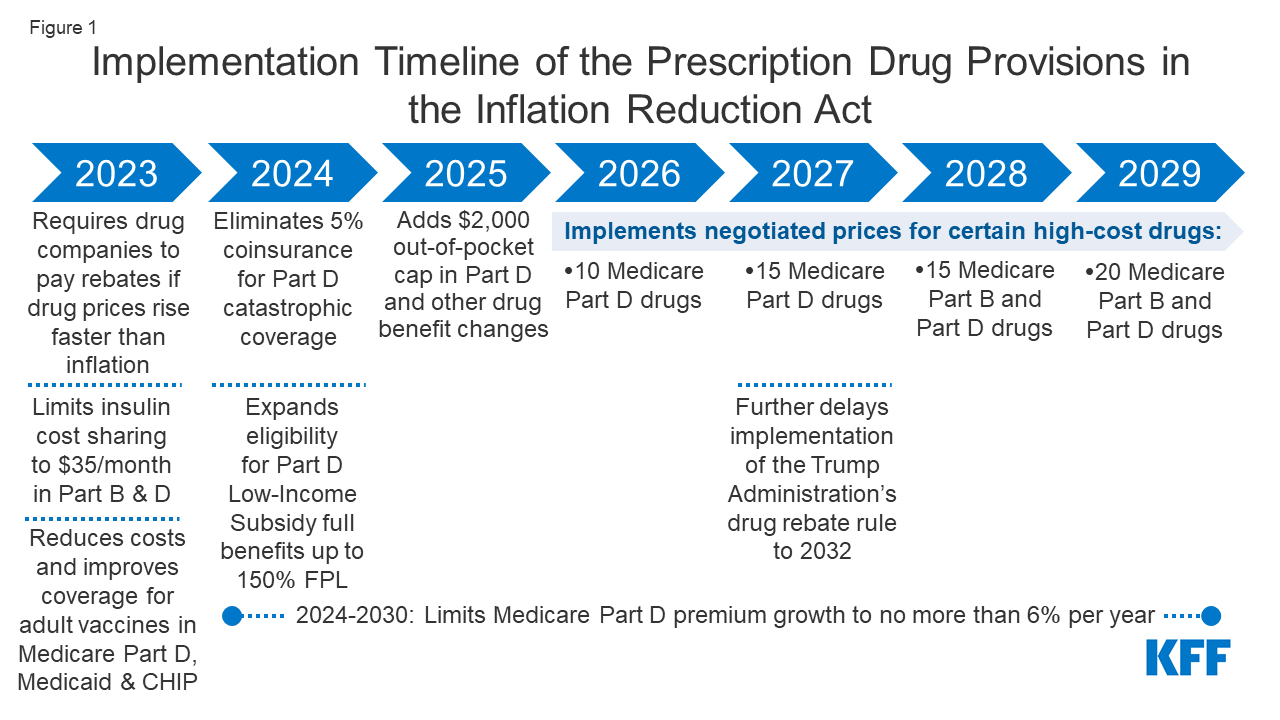
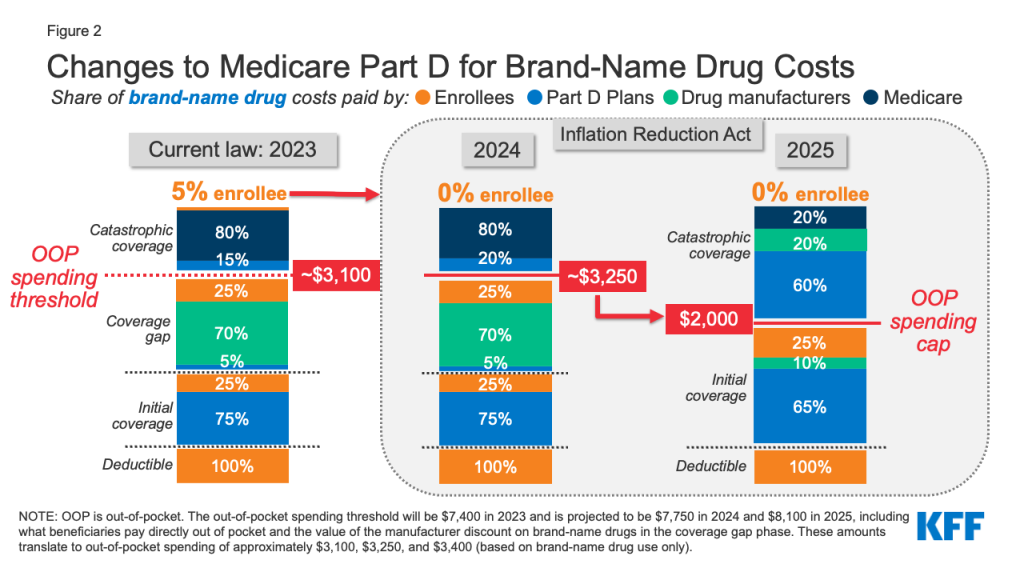
On August 16, 2022, President Biden signed into law the Inflation Reduction Act of 2022, which includes a broad package of health, tax, and climate change provisions. The law includes several provisions to lower prescription drug costs for people with Medicare and reduce drug spending by the federal government. These provisions will take effect beginning in 2023 (Figure 1). This brief examines the potential impact of these provisions for Medicare beneficiaries nationally and by state.
The Inflation Reduction Act includes two policies that are designed to have a direct impact on drug prices:
Requiresthe federal government to negotiate prices for some high-cost drugs covered under Medicare. Medicare Part D and Part B drug spending is highly concentrated among a relatively small share of covered drugs, mainly those without generic or biosimilar competitors. Under the Inflation Reduction Act, brand-name and biologic drugs without generic or biosimilar equivalents covered under Medicare Part D (retail prescription drugs) or Part B (administered by physicians) that are among the highest-spending Medicare-covered drugs and are nine or more years (small-molecule drugs) or 13 or more years (biologicals) from FDA approval are eligible for negotiation. The number of negotiated drugs is limited to 10 Part D drugs in 2026, another 15 Part D drugs in 2027, another 15 Part B and Part D drugs in 2028, and another 20 Part B and Part D drugs in 2029 and later years.
The number of Medicare beneficiaries who will see lower out-of-pocket drug costs in any given year under this provision, and the magnitude of savings, will depend on which drugs are subject to negotiation, the number of Medicare beneficiaries who use those drugs, and the price reductions achieved through the negotiation process relative to prices that would have been applied in the absence of the new law.
Requiresdrug manufacturers to pay rebates to Medicare if they increase prices faster than inflationfor drugs used by Medicare beneficiaries. From 2019 to 2020, half of all drugs covered by Medicare had price increases above the rate of inflation over that period (which was 1%, prior to the recent surge in the annual inflation rate), and among those drugs with price increases above the rate of inflation, one-third had price increases of 7.5% or more, the annual inflation rate in early 2022. The inflation rebate provision will be implemented in 2023, using 2021 as the base year for determining price changes relative to inflation. (The legislation originally included drug use by people with private insurance in the calculation of the rebate, but that language was dropped based on a ruling by the Senate parliamentarian that it did not comply with budget reconciliation rules.)
The number of Medicare beneficiaries who will see lower out-of-pocket drug costs in any given year and the amount of out-of-pocket savings under this provision will depend on how many beneficiaries use drugs whose prices increase more slowly than would otherwise occur and the magnitude of price reductions relative to baseline prices. For Part B drugs with price increases greater than inflation, beneficiary coinsurance will be based on 20% of the drug’s lower inflation-adjusted price. This provision could have spillover effects on people with private insurance if it results in slower price growth for drugs covered by private insurance.
The Inflation Reduction Act includes several provisions that will reduce out-of-pocket spending for Medicare beneficiaries:
Caps Medicare beneficiaries’ out-of-pocket spending under the Medicare Part D benefit, first by eliminating coinsurance above the catastrophic threshold in 2024 and then by adding a $2,000 cap on spending in 2025. The law also limits annual increases in Part D premiums for 2024 to 2030 and makes other changes to the Part D benefit design. Under current law, the catastrophic threshold is based on the amount beneficiaries themselves pay out-of-pocket plus the value of the manufacturer discount on the price of brand-name drugs in the coverage gap phase. In 2022, the catastrophic threshold is set at $7,050, and beneficiaries pay about $3,000 out of pocket for brand-name drugs before reaching the catastrophic coverage phase, where they pay 5% coinsurance on their drugs until the end of the year. Based on current estimates, beneficiary out-of-pocket spending at the catastrophic coverage threshold is estimated to increase from $3,000 in 2022 to roughly $3,100 in 2023 and $3,250 in 2024.
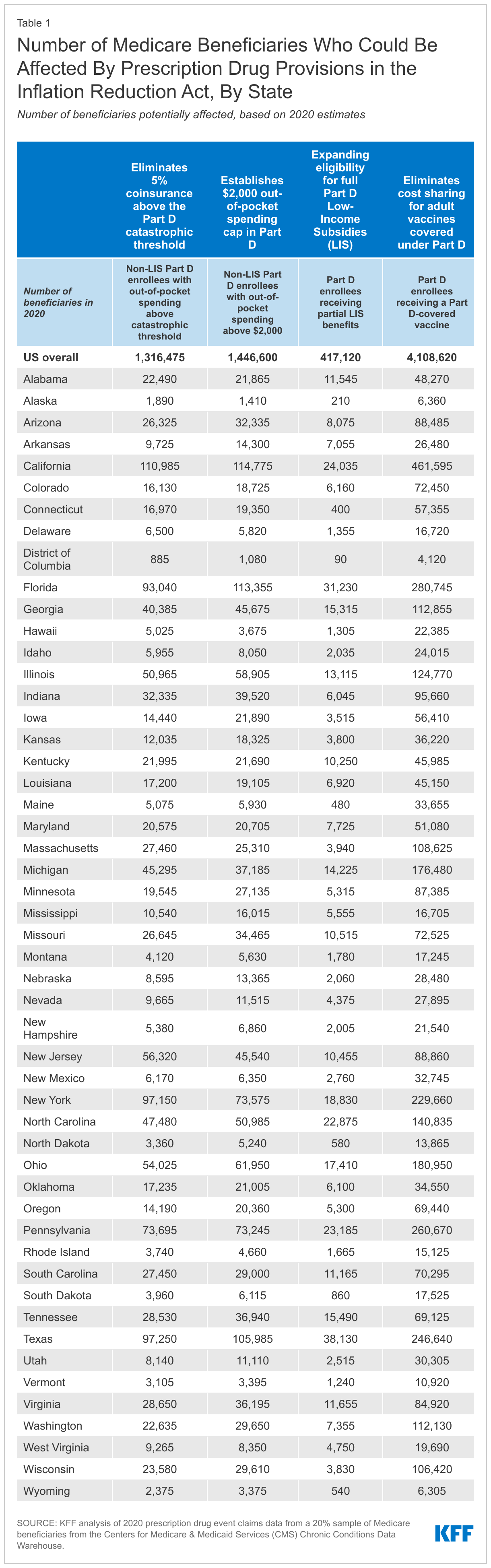
In 2020, 1.4 million Medicare Part D enrollees without low-income subsidies had annual out-of-pocket drug spending of $2,000 or more, including 1.3 million enrollees who had spending above the catastrophic coverage threshold (which equaled roughly $2,700 in out-of-pocket costs that year for brand-name drugs alone). (See Table 1 for state-level estimates.) Among these 1.4 million enrollees, most (1.0 million or 69%) spent between $2,000 and $3,000 out of pocket, while roughly 0.3 million (19%) had spending of $3,000 up to $5,000, and 0.2 million (11%) spent $5,000 or more out of pocket.
These estimates of how many beneficiaries will be helped by capping out-of-pocket drug spending under Medicare Part D starting in 2024 are conservative because they do not account for expected increases in annual out-of-pocket drug spending between 2020 and 2024/2025, the increase in the number of beneficiaries on Medicare, or higher utilization and spending associated with the increased affordability of prescription drugs due to this benefit improvement.
Capping out-of-pocket drug spending under Medicare Part D will be especially helpful for beneficiaries who take high-priced drugs for conditions such as cancer or multiple sclerosis. For example, in 2020, among Part D enrollees without low-income subsidies, average annual out-of-pocket spending for the cancer drug Revlimid was $6,200 (used by 33,000 beneficiaries); $5,700 for the cancer drug Imbruvica (used by 21,000 beneficiaries); and $4,100 for the MS drug Avonex (used by 2,000 beneficiaries).
Limits cost sharing for insulin to $35 per month for people with Medicare, beginning in 2023, including covered insulin products in Medicare Part D plans, beginning January 1, 2023, and for insulin furnished through durable medical equipment under Medicare Part B, beginning July 1, 2023. (A provision to limit monthly insulin copays for people with private insurance did not receive the 60 votes needed to remain in the bill after being ruled out of compliance with reconciliation rules by the parliamentarian and was removed from the legislation prior to passage.)
3.3 million Medicare Part D enrollees used an insulin product in 2020 (the most recent data available), including 1.7 million enrollees without low-income subsidies who spent $54 on average per insulin prescription that year. The number of Medicare beneficiaries who will pay less out of pocket for insulin beginning in 2023 will depend in part on whether they are currently enrolled in a Part D plan that is participating in an Innovation Center model in which participating plans cover selected insulin products at a monthly copayment of $35.
Eliminates cost sharing for adult vaccines covered under Medicare Part D, as of 2023, and improves access to adult vaccines under Medicaid and CHIP.
4.1 million Medicare beneficiaries received a vaccine covered under Part D in 2020, including 3.6 million who received the vaccine to prevent shingles. (See Table 1 for state-level estimates.)
The Medicaid and CHIP provision improves vaccine coverage for Medicaid-enrolled adults because vaccine coverage is optional and varies by state. According to a recent survey, half of states (25) did not cover all vaccines recommended by the Advisory Committee on Immunization Practices (ACIP) in 2018–2019, and 15 of 44 states responding to the survey imposed cost sharing requirements on adult vaccines.
Expands eligibility for full Part D Low-Income Subsidies (LIS) in 2024 to low-income beneficiaries with incomes up to 150% of poverty and modest assets and repeals the partial LIS benefit currently in place for individuals with incomes between 135% and 150% of poverty. Beneficiaries receiving partial LIS benefits typically pay some portion of the Part D premium and standard deductible, 15% coinsurance, and modest copayments for drugs above the catastrophic threshold, while those receiving full LIS benefits pay no Part D premium or deductible and only modest copayments for prescription drugs until they reach the catastrophic threshold, when they face no cost sharing.
0.4 million Medicare beneficiaries received partial LIS benefits in 2020. Annual out-of-pocket costs for these beneficiaries could fall by close to $300, on average, under the new law, based on the difference between average out-of-pocket drug costs for LIS enrollees receiving full benefits versus partial benefits in 2020. (See Table 1 for state-level estimates.)
This provision will benefit low-income Black and Hispanic Medicare beneficiaries in particular, who are more likely than white beneficiaries to have incomes between 135% and 150% of poverty.
The Inflation Reduction Act also includes a provision to further delay implementation of the Trump Administration’s drug rebate rule until 2032, rather than take effect in 2027. The rebate rule would eliminate the anti-kickback safe harbor protections for prescription drug rebates negotiated between drug manufacturers and pharmacy benefit managers (PBMs) or health plan sponsors in Medicare Part D. This rule was estimated to increase Medicare spending and premiums paid by beneficiaries.
Discussion
High and rising drug prices are a top health care affordability concern among the general public, with large majorities of Democrats and Republicans favoring policy actions to lower drug costs. Provisions in the Inflation Reduction Act are expected to lower out-of-pocket spending by people with Medicare and lower drug spending by the federal government. Prior to consideration by the Senate, CBO estimated the prescription drug provisions would reduce the federal deficit by $288 billion over 10 years (2022-2031). CBO has not yet released a final estimate of budget effects that reflect changes made to the legislation before final passage, such as the $35 per month limit on cost sharing for insulin for people with Medicare and the removal of the provision that applied the inflation rebate to prescription drug use by people with private insurance.
The prohibition against the federal government negotiating drug prices was a contentious provision of the Medicare Modernization Act of 2003, the law that established the Medicare Part D program, and lifting this prohibition has been a longstanding goal for many Democratic policymakers. The pharmaceutical industry has argued that allowing the government to negotiate drug prices would stifle innovation. CBO has estimated that 15 out of 1,300 drugs, or 1%, would not come to market over the next 30 years as a result of the drug provisions in the reconciliation legislation.
The requirement for drug companies to pay rebates for price increases faster than inflation will help to limit annual increases in drug prices for people with Medicare and possibly also those with private insurance. While it is possible that drug manufacturers may respond to the inflation rebates by increasing launch prices, overall, this provision is expected to limit out-of-pocket drug spending growth and put downward pressure on premiums by discouraging drug companies from increasing prices faster than inflation.
Capping Medicare beneficiaries’ out-of-pocket spending under the Medicare Part D benefit – first by eliminating coinsurance above the catastrophic threshold in 2024 and then by adding a $2,000 cap on spending in 2025 – will be the first major change to the Medicare Part D benefit since 2010, when lawmakers included a provision in the Affordable Care Act to close the so-called Part D “donut hole.” A cap on out-of-pocket drug spending for Medicare Part D enrollees will provide substantial financial protection to people on Medicare with high out-of-pocket drug costs. This includes Medicare beneficiaries who take just one very high-priced specialty drug for medical conditions such as cancer, hepatitis C, or multiple sclerosis and beneficiaries who take a handful of relatively costly brand or specialty drugs to manage their medical conditions.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.Juliette Cubanski, Tricia Neuman, and Meredith Freed are with KFF. Anthony Damico is an independent consultant.
The Inflation Reduction Act of 2022, signed into law by President Biden on August 16, 2022, includes several provisions to lower prescription drug costs for people with Medicare and reduce drug spending by the federal government. This legislation has taken shape amidst strong bipartisan, public support for the government to address high and rising drug prices. CBO estimates that the drug pricing provisions in the law will reduce the federal deficit by $237 billion over 10 years (2022-2031).
The prescription drug provisions included in the Inflation Reduction Act will:
This brief summarizes these provisions and discusses the expected effects on people, program spending, and drug prices and innovation.
Require the Federal Government to Negotiate Prices for Some Drugs Covered Under Medicare
Under the Medicare Part D program, which covers retail prescription drugs, Medicare contracts with private plan sponsors to provide a prescription drug benefit. The law that established the Part D benefit included a provision known as the “noninterference” clause, which stipulates that the HHS Secretary “may not interfere with the negotiations between drug manufacturers and pharmacies and PDP [prescription drug plan] sponsors, and may not require a particular formulary or institute a price structure for the reimbursement of covered part D drugs.” In addition, the Secretary of HHS does not currently negotiate prices for drugs covered under Medicare Part B (administered by physicians). Instead, Medicare reimburses providers based on a formula set at 106% of the Average Sales Price (ASP), which is the average price to all non-federal purchasers in the U.S, inclusive of rebates (other than rebates paid under the Medicaid program).
The Part D non-interference clause has been a longstanding target for some policymakers because it has limited the ability of the federal government to leverage lower prices, particularly for high-priced drugs without competitors. Medicare Part D and Part B drug spending is highly concentrated among a relatively small share of covered drugs, mainly those without generic or biosimilar competitors. A recent KFF Tracking Poll finds large majorities support allowing the federal government to negotiate drug prices and this support holds steady even after the public is provided with the arguments that were made for and against this proposal.
Provision Description
The Inflation Reduction Act amends the non-interference clause by adding an exception that requires the Secretary of HHS to negotiate prices with drug companies for a small number of single-source brand-name drugs or biologics without generic or biosimilar competitors that are covered under Medicare Part D (starting in 2026) and Part B (starting in 2028). Under the new Drug Price Negotiation Program, the number of drugs selected for price negotiation is 10 Part D drugs for 2026, another 15 Part D drugs for 2027, another 15 Part D and Part B drugs for 2028, and another 20 Part D and Part B drugs for 2029 and later years. These drugs will be selected from the 50 drugs with the highest total Medicare Part D spending and the 50 drugs with the highest total Medicare Part B spending. The number of drugs with negotiated prices available will accumulate over time.
Certain categories of drugs are excluded from the negotiation process, including:
Drugs that have a generic or biosimilar available
Drugs that are less than 9 years (for small-molecule drugs) or 13 years (for biological products) from their FDA-approval or licensure date
“Small biotech drugs” (until 2029), defined as those which account for 1% or less of Part D or Part B spending and account for 80% or more of spending under each part on that manufacturer’s drugs
Drugs with Medicare spending of less than $200 million in 2021 (increased by the CPI-U for subsequent years)
Drugs with an orphan designation as their only FDA-approved indication
All plasma-derived products
The legislation also delays selection of biologic drugs for negotiation by up to two years if a biosimilar product is likely to enter the market in that time.
The law establishes an upper limit for the negotiated price (the “maximum fair price”) for a given drug. The limit is the lower of the drug’s enrollment-weighted negotiated price (net of all price concessions) for a Part D drug, the average sales price for a Part B drug, or a percentage of a drug’s average non-federal average manufacturer price: 75% for small-molecule drugs and vaccines more than 9 years but less than 12 years beyond approval; 65% for drugs between 12 and 16 years beyond approval or licensure; and 40% for drugs more than 16 years beyond approval or licensure.
When negotiating the “maximum fair price” for a drug, the HHS Secretary is required to consider the following criteria:
The manufacturer’s research and development costs, including the extent to which the manufacturer has recouped these costs
The current unit costs of production and distribution
Federal financial support for novel therapeutic discovery and development related to the drug
Data on pending and approved patent applications, exclusivities, and certain other applications and approvals
Market data and revenue and sales volume data in the US
Evidence about alternative treatments, including:
The extent to which the drug represents a therapeutic advance as compared to existing therapeutic alternatives and the costs of these alternatives
Prescribing information for the drug and its therapeutic alternatives
Comparative effectiveness of the drug and its therapeutic alternatives, taking into accounts their effects on specific populations, such as individuals with disabilities, the elderly, the terminally ill, children, and other patient populations
The extent to which the drug and its therapeutic alternatives address unmet needs for a condition that is not adequately addressed by available therapy.
The law explicitly directs that the HHS Secretary “shall not use evidence from comparative clinical effectiveness research in a manner that treats extending the life of an elderly, disabled, or terminally ill individual as of lower value than extending the life of an individual who is younger, non-disabled, or not terminally ill.”
Part D drugs with negotiated “maximum fair prices” are required to be covered by all Part D plans. Medicare’s payment to providers for Part B drugs with negotiated prices will be 106% of the maximum fair price (rather than the current payment of 106% of the average sales price). (A separate section of the law increases Medicare payments to providers for the administration of biosimilar biologic products to 108% of the average sales price from October 1, 2022 through December 31, 2027.)
An excise tax will be levied on drug companies that do not comply with the negotiation process. The excise tax starts at 65% of a product’s sales in the U.S. and increases by 10% every quarter to a maximum of 95%. As an alternative to paying the tax, manufacturers can choose to withdraw all of their drugs from coverage under Medicare and Medicaid. In addition, manufacturers that refuse to offer an agreed-upon negotiated price for a selected drug to “a maximum fair price eligible individual” (i.e., Medicare beneficiaries enrolled in Part B and/or Part D) or to a provider of services to maximum fair price eligible individuals (such as a physician or hospital) will pay a civil monetary penalty equal to 10 times the difference between the price charged and the maximum fair price.
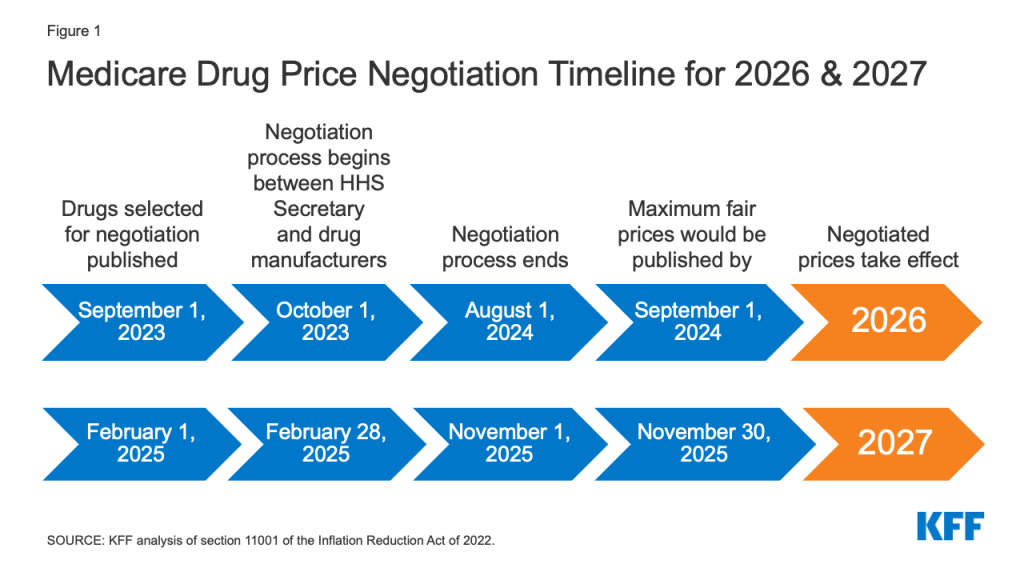
The timeline for the negotiation process spans roughly two years, although the timeline is modified for 2026, the first year that negotiated prices will be available under this new program (Figure 1). For the 10 Part D drugs with negotiated prices taking effect on January 1, 2026, the list of 10 Part D drugs selected for negotiation will be published on September 1, 2023, based on spending data for the 12-month period from June 1, 2022 to May 31, 2023. The period of negotiation between the Secretary and manufacturers of these drugs will occur between October 1, 2023 and August 1, 2024, and the negotiated “maximum fair prices” will be published no later than September 1, 2024. For 2027, which is an example of timing for a typical year in terms of the timeline for establishing negotiated prices, the list of 15 Part D drugs selected for negotiation will be published on February 1, 2025. The period of negotiation between the Secretary and manufacturers of the selected drugs will occur between February 28, 2025 and November 1, 2025 and the negotiated “maximum fair prices” will be published no later than November 30, 2025. For Part B drugs, the initial period of drug price negotiation between the Secretary and manufacturers of selected drugs will take place between February 28, 2026 and November 1, 2026, with negotiated prices first available in 2028.
Figure 1: Medicare Drug Price Negotiation Timeline for 2026 & 2027
The legislation appropriates funding of $3 billion in fiscal year 2022 for implementing the drug price negotiation provisions over the 2023-2031 period.
Effective Date
Negotiated prices for the first set of selected drugs covered under Part D will be available in 2026. For drugs covered under Part B, the first year negotiated prices will be available is 2028.
People Affected
The provision to allow the Secretary to negotiate drug prices will put downward pressure on both Part D premiums and out-of-pocket drug costs, although the number of Medicare beneficiaries who will see lower out-of-pocket drug costs in any given year under the drug price negotiation program and the magnitude of savings will depend on how many and which drugs are subject to the negotiation process and the price reductions achieved through the negotiations process relative to what prices would otherwise be.
Budgetary Impact
CBO estimates $98.5 billion in Medicare savings over 10 years (2022-2031) from the drug negotiation provisions in the Inflation Reduction Act.
Effects on the Development of New Drugs
CBO estimates that the drug pricing provisions in the Inflation Reduction Act, including but not limited to the new Medicare drug price negotiation program, will have a very modest impact on the number of new drugs coming to market in the U.S. over the next 30 years: 13 fewer out of 1,300, or a reduction of 1% (about 1 fewer drug over the 2023-2032 period, about 5 fewer drugs in the subsequent decade, and about 7 fewer drugs in the decade after that).
Require Drug Manufacturers to Pay Rebates for Price Increases Above Inflation for Drugs Used by People with Medicare
To date, Medicare has had no authority to limit annual price increases for drugs covered under Part B or Part D. In contrast, Medicaid has a rebate system that requires drug manufacturers to provide refunds if prices grow faster than inflation. Year-to-year drug price increases exceeding inflation are not uncommon and affect people with both Medicare and private insurance. Our analysis shows that half of all drugs covered by Medicare had list price increases that exceeded the rate of inflation between 2019 and 2020. A separate analysis by the HHS Office of Inspector General showed average sales price (ASP) increases exceeding inflation for 50 of 64 studied Part B drugs in 2015.
Provision Description
The Inflation Reduction Act requires drug manufacturers to pay a rebate to the federal government if prices for single-source drugs and biologicals covered under Medicare Part B and nearly all covered drugs under Part D increase faster than the rate of inflation (CPI-U). Price changes will be measured based on the average sales price for Part B drugs and the average manufacturer price for Part D drugs. If price increases are higher than inflation, manufacturers will be required to pay the difference in the form of a rebate to Medicare. The rebate amount is equal to the total number of units sold in Medicare multiplied by the amount, if any, by which a drug’s price in a given year exceeds the inflation-adjusted price. For Part B drugs with price increases greater than inflation, beneficiary coinsurance will be based on 20% of the drug’s lower inflation-adjusted price. The base year for measuring cumulative price changes relative to inflation is 2021.
Rebate dollars would be deposited in the Medicare Supplementary Medical Insurance (SMI) trust fund. Manufacturers that do not pay the required rebate amount will face a penalty equal to at least 125% of the original rebate amount.
The legislation appropriates 10-year (2022-2031) funding of $160 million to the Centers for Medicare & Medicaid Services (CMS) for implementing the inflation rebate provisions ($80 million for Part B and $80 million for Part D).
Effective Date
The Part D inflation rebate provision takes effect in 2022, the starting point for measuring drug price increases, with rebate payments required beginning in 2023. The Part B inflation rebate provision takes effect in 2023.
People Affected
These provisions are expected to limit out-of-pocket drug spending growth for people with Medicare and put downward pressure on premiums by discouraging drug companies from increasing prices faster than inflation. The number of Medicare beneficiaries who will see lower out-of-pocket drug costs in any given year resulting from these provisions will depend on how many and which drugs have lower price increases and the magnitude of price reductions relative to what prices would otherwise be.
Budgetary Impact
CBO estimates a net federal deficit reduction of $63.2 billion over 10 years (2022-2031) from the drug inflation rebate provisions in the Inflation Reduction Act. This includes net savings of $56.3 billion ($71.8 billion in savings to Medicare and $0.3 billion in savings for other federal programs, such as DoD, FEHB, and subsides for ACA Marketplace coverage, offset by $15.7 billion in additional Medicaid spending) and higher federal revenues of $6.9 billion.
Effects on Launch Pricing
Drug manufacturers may respond to the inflation rebates by increasing launch prices for drugs that come to market in the future. CBO projects that higher launch prices would primarily affect Medicaid spending. This is because, although the basic Medicaid drug rebate would be larger (since it is calculated as a percentage of the average manufacturer price), the higher Medicaid drug rebates would not offset higher launch prices. According to CBO, Medicare Part D plan sponsors and private insurers would be less affected than Medicaid by higher launch prices because they would still be able to negotiate rebates with drug companies and potentially refuse to cover drugs with very high launch prices. However, they may have less leverage in some instances, such as when there are no therapeutic alternatives available or when drugs are covered under a Part D “protected class”. In addition, if launch prices rise for Part B drugs, the HHS Secretary would have no authority to negotiate lower prices unless and until the new drug meets the criteria for selection for drug price negotiation under the negotiation process described above.
Cap Out-of-Pocket Spending for Medicare Part D Enrollees and Other Part D Benefit Design Changes
Medicare Part D currently provides catastrophic coverage for high out-of-pocket drug costs, but there is no limit on the total amount that beneficiaries pay out of pocket each year. Under the current benefit design, Part D enrollees qualify for catastrophic coverage when the amount that they pay out of pocket plus the value of the manufacturer discount on the price of brand-name drugs in the coverage gap phase exceeds a certain threshold amount. Enrollees with drug costs high enough to exceed the catastrophic threshold are required to pay 5% of their total drug costs above the threshold until the end of the year unless they qualify for Part D Low-Income Subsidies (LIS). In 2022, the catastrophic threshold is set at $7,050, and beneficiaries pay about $3,000 out of pocket for brand-name drugs before reaching the catastrophic coverage phase.
Medicare pays 80% of total costs above the catastrophic threshold (known as “reinsurance”) and plans pay 15%. Medicare’s reinsurance payments to Part D plans now account for close to half of total Part D spending (47%), up from 14% in 2006 (increasing from $6 billion in 2006 to $52 billion in 2021).
Under the current structure of Part D, there are multiple phases, including a deductible, an initial coverage phase, a coverage gap phase, and the catastrophic phase. During the coverage gap benefit phase, enrollees pay 25% of drug costs for both brand-name and generic drugs; plan sponsors pay 5% for brands and 75% for generics; and drug manufacturers provide a 70% price discount on brands (there is no discount on generics). Under the current benefit design, beneficiaries can face different cost-sharing amounts for the same medication depending on which phase of the benefit they are in, and can face significant out-of-pocket costs for high-priced drugs because of coinsurance requirements and no hard out-of-pocket cap.
Provision Description
The Inflation Reduction Act amends the design of the Part D benefit. For 2024, the law eliminates the 5% beneficiary coinsurance requirement above the catastrophic coverage threshold, effectively capping out-of-pocket costs at approximately $3,250 that year. Beginning in 2025, the legislation adds a hard cap on out-of-pocket spending of $2,000, indexed in future years to the rate of increase in per capita Part D costs (Figure 2).
Figure 2: Changes to Medicare Part D for Brand-Name Drug Costs
The law also modifies liability for Medicare Part D plans and drug manufacturers, starting in 2025, and reduces Medicare’s liability for spending above the out-of-pocket cap. Medicare’s share of total costs above the spending cap (“reinsurance”) will decrease from 80% to 20% for brand-name drugs and to 40% for generic drugs. Medicare Part D plans’ share of costs will increase from 15% to 60% for both brands and generics above the cap, and drug manufacturers will be required to provide a 20% price discount on brand-name drugs. The legislation also requires manufacturers to provide a 10% discount on brand-name drugs between the deductible and the annual out-of-pocket spending cap, replacing the 70% price discount in the coverage gap phase under the current benefit design.
The law also provides for an adjustment to the calculation of the base beneficiary premium for 2024 through 2029, limiting premium increases to no more than 6% from the prior year. For 2030, the bill includes a provision to lower the beneficiary share of the cost of standard drug coverage (currently set at 25.5%) to ensure that the premium does not increase by more than 6% from 2029. The legislation also allows Part D enrollees the option of spreading out their out-of-pocket costs over the year rather than face high out-of-pocket costs in any given month.
Effective Date
The Part D benefit redesign provisions take effect beginning in 2024, with the elimination of the 5% coinsurance for catastrophic coverage and the first year of the Part D premium adjustment. Other changes take effect in 2025, including the $2,000 cap on out-of-pocket drug spending, spreading out of costs, and changes to liability for total costs above the spending cap.
People Affected
Medicare beneficiaries in Part D plans with relatively high out-of-pocket drug costs are likely to see substantial out-of-pocket cost savings from these changes. This includes Medicare beneficiaries with spending above the catastrophic threshold due to just one very high-priced specialty drug for medical conditions such as cancer, hepatitis C, or multiple sclerosis and beneficiaries who take a handful of relatively costly brand or specialty medications to manage their medical conditions.
Based on our analysis, 1.4 million Part D enrollees incurred annual out-of-pocket costs for their medications above $2,000 in 2020, averaging $3,355 per person. This estimate includes 1.3 million enrollees who had spending above the catastrophic coverage threshold (which equaled roughly $2,700 in out-of-pocket costs that year for brand-name drugs alone). These estimates are a conservative measure of how many beneficiaries will be helped by capping out-of-pocket drug spending under Medicare Part D starting in 2024 because they do not account for expected increases in annual out-of-pocket drug spending between 2020 and 2024/2025, the increase in the number of beneficiaries on Medicare, or higher utilization and spending associated with the increased affordability of prescription drugs due to this benefit improvement.
Based on their average out-of-pocket spending, these 1.4 million Part D enrollees would have saved $1,355, or 40% of their annual out-of-pocket costs, on average, if a $2,000 cap had been in place in 2020. Part D enrollees with higher-than-average out-of-pocket costs will save substantial amounts with a $2,000 out-of-pocket spending cap. For example, the top 10% of beneficiaries (145,000 enrollees) with average out-of-pocket costs for their medications above $2,000 in 2020 – who spent at least $5,567 – would have saved $3,567 (64%) in out-of-pocket costs with a $2,000 cap.
Capping out-of-pocket drug spending under Medicare Part D will be especially helpful for beneficiaries who take high-priced drugs for conditions such as cancer or multiple sclerosis. For example, in 2020, among Part D enrollees without low-income subsidies, average annual out-of-pocket spending for the cancer drug Revlimid was $6,200 (used by 33,000 beneficiaries); $5,700 for the cancer drug Imbruvica (used by 21,000 beneficiaries); and $4,100 for the MS drug Avonex (used by 2,000 beneficiaries).
With the new hard cap on out-of-pocket spending, it is possible that enrollees could face higher Part D premiums resulting from higher plan liability for drug costs above the spending cap, though these premium increases could be mitigated by the provisions to stabilize premiums between 2024 and 2030. Plans will likely face financial incentives to exercise greater control of costs below the new spending cap, such as through more utilization management or increased generic drug utilization, which could help to limit potential premium increases.
Budgetary Impact
CBO estimates these provisions will increase federal spending by $30 billion over 10 years (2022-2031), which consists of $29.9 billion in higher spending associated with Part D benefit redesign and $0.1 billion in higher spending associated with the provision to spread out out-of-pocket costs.
Limit Cost Sharing for Insulin for People with Medicare
For Medicare beneficiaries with diabetes who use insulin, coverage is provided under Medicare Part D, the outpatient prescription drug benefit, and may also be covered under Part B when used with an external insulin pump. Because Part D plans vary in terms of the insulin products they cover and costs per prescription, what enrollees pay for insulin products also varies. Beneficiary coinsurance under Medicare Part B is 20% of the Medicare-approved amount.
Currently, Medicare beneficiaries can choose to enroll in a Part D plan participating in an Innovation Center model in which enhanced drug plans cover insulin products at a monthly copayment of $35 in the deductible, initial coverage, and coverage gap phases of the Part D benefit. Participating plans do not have to cover all insulin products at the $35 monthly copayment amount, just one of each dosage form (vial, pen) and insulin type (rapid-acting, short-acting, intermediate-acting, and long-acting). In 2022, a total of 2,159 Part D plans are participating in this model, or roughly one third of all Part D plans. Nearly half (45%) of non-LIS enrollees are in PDPs participating in the insulin model in 2022, based on August 2021 enrollment. The model was launched in response to rising prices for insulin, which have attracted increasing scrutiny from policymakers, leading to congressionalinvestigations and overall concerns about affordability and access for people with diabetes who need insulin to control blood glucose levels.
Provision Description
The Inflation Reduction Act limits monthly cost sharing for insulin products to no more than $35 for Medicare beneficiaries, including insulin covered under both Part D and Part B, and no deductible will apply. All Medicare Part D plans, both stand-alone drug plans and Medicare Advantage drug plans, will be required to charge no more than $35 for whichever insulin products they cover, although plans will not be required to cover all insulin products. For 2026 and beyond, the law limits monthly Part D copayments for insulin to the lesser of $35, 25% of the maximum fair price (in cases where the insulin product has been selected for negotiation), or 25% of the negotiated price in Part D plans.
Effective Date
The monthly cap on insulin cost sharing in Medicare takes effect January 1, 2023 for insulin covered under Part D and July 1, 2023 for insulin covered under Part B.
People Affected
A $35 cap on monthly cost sharing for insulin products is expected to lower out-of-pocket costs for insulin users in Medicare Part D without low-income subsidies. In 2020, 3.3 million Medicare Part D enrollees used insulin. Among Medicare Part D insulin users who do not receive low-income subsidies, average out-of-pocket costs per prescription across all insulin products was $54 in 2020 – over 50% more than the $35 monthly copay cap for insulin that will begin in 2023.
According to our analysis of 2019 Part D formularies, a large number of Part D plans placed insulin products on Tier 3, the preferred drug tier, which typically had a $47 copayment per prescription during the initial coverage phase. However, once enrollees reached the coverage gap phase, they faced a 25% coinsurance rate, which equates to $100 or more per prescription in out-of-pocket costs for many insulin therapies, unless they qualified for low-income subsidies. Paying a flat $35 copayment rather than 25% coinsurance or a higher copayment amount could reduce out-of-pocket costs for many insulin products.
Budgetary Impact
CBO estimates additional federal spending of $5.1 billion ($4.8 billion for Medicare Part D and $0.3 billion for Medicare Part B) over 10 years (2022-2031) associated with the insulin cost-sharing limits in the Inflation Reduction Act.
Eliminate Cost Sharing for Adult Vaccines Covered Under Part D and Improve Access to Adult Vaccines in Medicaid and CHIP
Medicare covers vaccines under both Part B and Part D. This separation of coverage for vaccines under Medicare is because there were statutory requirements for coverage of a small number of vaccines under Part B before the 2006 start of the Part D benefit. Vaccines for COVID-19, influenza, pneumococcal disease, and hepatitis B (for patients at high or intermediate risk), and vaccines needed to treat an injury or exposure to disease are covered under Part B. All other commercially available vaccines needed to prevent illness are covered under Medicare Part D.
For the influenza, pneumococcal pneumonia, hepatitis B, and COVID-19 vaccines covered under Medicare Part B, patients currently face no cost sharing for either the vaccine itself or its administration. For other Part B vaccines, such as those needed to treat an injury or exposure to a disease such as rabies or tetanus, Medicare covers 80% of the cost, and beneficiaries are responsible for the remaining 20%. Unlike most vaccines covered under Part B, vaccines covered under Part D can be subject to cost sharing, because Part D plans have flexibility to determine how much enrollees will be required to pay for any given on-formulary drug, including vaccines. (Part D enrollees who receive low-income subsidies (LIS) generally pay relatively low amounts for vaccines and other covered drugs.) Under Part D, cost sharing can take the form of flat dollar copayments or coinsurance (i.e., a percentage of list price).
With regard to Medicaid and CHIP, coverage of adult vaccines is optional and varies by state. According to a recent survey, half of states (25) did not cover all vaccines recommended by the Advisory Committee on Immunization Practices (ACIP) in 2018–2019, and 15 of 44 states responding to the survey imposed cost sharing requirements on adult vaccines.
Provision Description
The Inflation Reduction Act requires that adult vaccines covered under Medicare Part D that are recommended by the Advisory Committee on Immunization Practices (ACIP), such as for shingles, be covered at no cost. This makes coverage of vaccines under Medicare Part D consistent with coverage of vaccines under Medicare Part B, such as the flu and COVID-19 vaccines. The law also requires state Medicaid and CHIP programs to cover all approved adult vaccines recommended by ACIP and vaccine administration, without cost sharing.
Effective Date
These provisions take effect in 2023.
People Affected
Eliminating cost-sharing for adult vaccines covered under Medicare Part D could help with vaccine uptake among older adults and will lower out-of-pocket costs for those who need Part D-covered vaccines. Our analysis shows that in 2020, 4.1 million Medicare beneficiaries received a Part D-covered vaccine, including 3.6 million who received the vaccine to prevent shingles, and aggregate out-of-pocket spending on Part D vaccines was $0.3 billion. In 2018, Part D enrollees without low-income subsidies paid an average of $57 out of pocket for each dose of the shingles shot, which is generally free to most other people with private coverage.
Requiring state Medicaid and CHIP programs to cover all adult vaccines recommended by ACIP without cost sharing is expected to increase access to some adult vaccines under Medicaid. Using a recent survey’sstate level data and 2019 adult Medicaid enrollment data, a separate KFF analysis estimates about 4 million adults could gain coverage of at least one or more vaccines.
Budgetary Impact
CBO estimates that these provisions will increase federal spending by $7 billion over 10 years (2022-2031), including $4.4 billion for Medicare and $2.5 billion for Medicaid and CHIP.
Expand Eligibility for Part D Low-Income Subsidies
Provision Description
The Part D Low-Income Subsidy (LIS) Program helps beneficiaries with their Part D premiums, deductibles, and cost sharing, providing varying levels of assistance to beneficiaries at different income and asset levels up to 150% of poverty. Based on data from CMS, in 2020, 13.1 million Medicare beneficiaries received either full or partial LIS benefits, representing 28% of all Part D enrollees that year.
Medicare beneficiaries who are also enrolled in Medicaid, who generally have incomes up to 135% of poverty, automatically receive full LIS benefits. Individuals who do not automatically qualify for LIS can enroll if they meet certain income and asset requirements set by the federal government and can receive full or partial LIS benefits depending on their income and assets. Beneficiaries qualify for full LIS benefits if they have income up to 135% of poverty and resources up to $9,900 individual, $15,600 couple in 2022 (including a $1,500 per person allowance for funeral/burial expenses). Beneficiaries qualify for partial LIS benefits if they have income between 135-150% of poverty and resources up to $15,510 individual, $30,950 couple in 2022.
Beneficiaries who receive full LIS benefits pay no Part D premium or deductible and only modest copayments for prescription drugs until they reach the catastrophic threshold, at which point they face no additional cost sharing. Some beneficiaries who receive partial LIS benefits pay no monthly premium while others pay a partial monthly Part D premium (with subsidies of 75%, 50%, or 25% of the monthly premium, depending on their income); all partial LIS recipients also pay an $89 annual deductible (in 2022), 15% coinsurance up to the out-of-pocket threshold, and modest copayments for drugs above the catastrophic threshold.
The Inflation Reduction Act makes individuals with incomes up to 150% of poverty and resources at or below the limits for partial LIS benefits eligible for full benefits under the Part D Low-Income Subsidy Program. The law eliminates the partial LIS benefit currently in place for individuals with incomes between 135% and 150% of poverty.
Effective Date
Expansion of eligibility for full Part D LIS benefits takes effect in 2024.
People Affected
Providing full Medicare Part D LIS benefits to Part D enrollees with incomes up to 150% of poverty could help an estimated 0.4 million beneficiaries, based on the number of beneficiaries receiving partial LIS benefits in 2020. Annual out-of-pocket drug costs for these beneficiaries could fall by close to $300, on average, based on the difference between average out-of-pocket drug costs for LIS enrollees receiving full benefits versus partial benefits in 2020 – plus additional savings associated with more generous premium subsidies.
These averages understate the potential cost savings for the smaller share of low-income enrollees with extraordinarily high drug costs, such as partial LIS beneficiaries who take high-cost specialty drugs. This is because for high-cost drugs, with total prices in the thousands of dollars, 15% coinsurance can translate into substantial out-of-pocket costs. For example, partial LIS enrollees taking Humira or Enbrel for rheumatoid arthritis would pay around $1,900 for a year’s worth of these medications in 2022, while full LIS enrollees would pay less than $20 annually. Thus, savings for partial LIS enrollees would be roughly $1,900 on cost sharing for one of these medications alone. Annual savings would be similar for other high-cost specialty drugs, with the majority of savings occurring below the catastrophic threshold where partial LIS enrollees currently pay 15% coinsurance but full LIS enrollees pay low flat copays for brand-name drugs of either $3.95 or $9.85, depending on their income and asset levels.
Budgetary Impact
CBO estimates that this provision will increase federal spending by $2.2 billion over 10 years (2022-2031).
Further Delay Implementation of the Trump Administration’s Drug Rebate Rule
Provision Description
The Inflation Reduction Act further delays implementation of the November 2020 final rule issued by the Trump Administration that would have eliminated rebates negotiated between drug manufacturers and pharmacy benefit managers (PBMs) or health plan sponsors in Medicare Part D by removing the safe harbor protection currently extended to these rebate arrangements under the federal anti-kickback statute. This rule was slated to take effect on January 1, 2022, but the Biden Administration delayed implementation to 2023, the Infrastructure Investment and Jobs Act signed into law on November 15, 2021 delayed implementation to 2026, and the Bipartisan Safer Communities Act signed into law on June 25, 2022 included a further delay to 2027.
Effective Date
This provision takes effect in 2027, delaying implementation of the rebate rule until 2032.
People affected
Since the rebate rule never took effect, delaying it is not expected to have a material impact on Medicare beneficiaries. Had the rule taken effect, it was expected to increase premiums for Medicare Part D enrollees, according to both CBO and the HHS Office of the Actuary (OACT). OACT estimated that a small group of beneficiaries who use drugs with significant manufacturer rebates could have seen a substantial decline in their overall out-of-pocket spending under the rule, assuming manufacturers passed on price discounts at the point of sale, but other beneficiaries would have faced out-of-pocket cost increases.
Budgetary Impact
Because the rebate rule was finalized (although not implemented), its cost has been incorporated in CBO’s baseline for federal spending. Therefore, delaying implementation of the rebate rule is expected to generate savings. CBO estimates savings of $122.2 billion from delaying implementation of the Trump Administration’s rebate rule between 2027 (when the Inflation Reduction Act delay takes effect) and 2032. In addition, CBO estimated savings of $50.8 billion between 2023 and 2026 for the three-year delay of this rule included in the Infrastructure Investment and Jobs Act and savings of $20.9 billion in 2026 and 2027 for the one-year delay included in the Bipartisan Safer Communities Act. This is because both CBO and Medicare’s actuaries estimated substantially higher Medicare spending over 10 years as a result of banning drug rebates under the Trump Administration’s rule – up to $170 billion higher, according to CBO, and up to $196 billion higher, according to the HHS Office of the Actuary (OACT).
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities
Many states use community health worker (CHW) services to address the health needs of targeted populations, including enrollees with chronic conditions or complex behavioral or physical health needs. Services provided by CHWs may include culturally appropriate health promotion and education, assistance in accessing medical and non-medical services, translation services, care coordination, and social support. Research evidence indicates CHW interventions can be effective in reducing health disparities in communities of color and promoting health equity.1,2,3 These interventions have also been shown to be effective in improving health for individuals with a wide range of chronic conditions.4 Though few studies have focused on CHW programs serving Medicaid beneficiaries, some evidence exists that these interventions can reduce health care costs and improve outcomes.5 CHW services may also potentially play a role in helping individuals access health care in areas with provider shortages.6 In September 2022, the Biden Administration announced that it was awarding $225 million in American Rescue Plan funding to train over 13,000 CHWs, the largest ever one-time federal investment in the CHW workforce. The Consolidated Appropriations Act of 2023 also authorized $50 million annually to build CHW workforce capacity from state fiscal year (FY) 2023 through FY 2027.7 These investments represent growing interest among federal and state policymakers in the potential role of CHWs in strengthening population health.
KFF’s 22nd annual Medicaid budget survey (conducted in 2022) asked states about CHW coverage policies in place as of July 1, 2022 (the beginning FY 2023 for most states)8 and planned for FY 2023. Key findings from the survey (supplemented by other available research) include:
Medicaid payment for CHW services: As of July 1, 2022, over half of responding states (29 of 48) reported allowing Medicaid payment for services provided by CHWs.9
CHW coverage changes planned for FY 2023: A number of states reported plans to implement Medicaid coverage/payment of CHW services under state plan authority or through other coverage pathways, including under Section 1115 authority. Notably, a few states reported planning to target CHW interventions to pregnant and postpartum populations.
Certification and training. Though the survey did not include questions about CHW certification and training programs, several states reported plans to introduce new certification and/or standardized training programs for CHWs in FY 2023.
Efforts to expand CHW workforce. States also reported working with stakeholders to identify best practices for expanding the number of CHWs and for supporting broader acceptance of CHWs by Medicaid providers, health plans, and enrollees.
Background
Community Health Workers (CHWs) are frontline workers who have close relationships with the communities they serve, allowing them to better liaise and connect community members to health care systems.10 They often share life experiences, language, socioeconomic status, and race/ethnicity with members of the communities in which they work, allowing them to foster greater trust between community members and the health care system.11 As of May 2021, there were an estimated 61,010 CHWs working in the United States.12
CHW examples include care coordinators, community health educators, outreach and enrollment agents, patient navigators, and peer educators. Services provided by CHWs may include culturally appropriate health promotion and education, assistance in accessing medical and non-medical services, translation services, care coordination, patient advocacy, home visits, and social support.13 CHWs have also played an important role in trying to mitigate the spread of COVID-19.14 Training and certification requirements for CHWs vary widely, depending on the specific role/responsibilities and employer (e.g., community-based organizations, federally qualified health centers (FQHCs), health departments, or hospitals). No national curriculum or core training exists; however, in recent years, some states have developed standardized core competency trainings and certification requirements for CHWs.15 The move to greater standardization of the CHW role may carry some trade-offs, as some studies have found that more explicitly defining the role of CHWs and introducing certification can create new barriers to entry into the profession, undermining the grassroots nature of the workforce.16,17
Historically, most CHW programs have been run and funded through community health centers and other community-based organizations.18 States may authorize Medicaid payment for certain CHW services under state plan or Section 1115 demonstration authority. States may allow or require managed care organizations (MCOs) to provide CHW services or include CHWs in care teams. Many states use CHW services to address the health needs of targeted populations including enrollees with chronic conditions or complex behavioral or physical health needs, enrollees receiving targeted case management services, or frequent users of health care services.19
Findings
MEDICAID CHW SERVICE coverage approaches
States can take a variety of approaches to authorize payment for or encourage use of CHW services within Medicaid programs. State approaches to covering CHW services may be influenced by state specific factors including existing delivery systems and payment models and state policy and program goals. Primary coverage approaches and general considerations are outlined below:
State plan coverage. States can authorize Medicaid payment for CHW services under different state plan benefits including under the preventive services benefit20 or outpatient services benefit. Requirements for authorizing coverage vary by specific state plan benefit.21 Generally, Medicaid payment is authorized for a specific set of services, provided under the supervision of a physician or licensed provider. States may also define CHW certification and training requirements.22 Federal Medicaid rules require services authorized under state plan to be available to all full benefit Medicaid beneficiaries (with certain exceptions).
ACA Health Home option. The Medicaid health homes state plan option (created under Section 2703 of the Affordable Care Act (ACA))23 allows states to establish health homes to coordinate care for individuals with chronic conditions. States may encourage or require use of CHWs as part of a Health Homes care team. States receive a 90% federal match rate for qualified Health Home service expenditures for the first eight quarters under each Health Home state plan amendment (SPA);24 states can (and have) created more than one Health Home program to target different populations. As of September 2022, 19 states (including DC) had a total of 33 approved Medicaid health home models.
Managed care arrangements. Some states provide CHW services through Medicaid managed care arrangements, including by adding requirements related to CHWs in MCO contracts. CHW services may be reflected in the medical component of the MCO capitation rate (e.g., if these services are specifically authorized under the state plan and the MCO is required to provide them, or if services fall under care coordination provisions25 ). MCOs may also choose to provide CHW services as “value-added” services even when they are not covered under the state plan (or factored into the capitation rate).26 As of July 2022, 41 states (including DC) contract with comprehensive, risk-based managed care plans to provide care to at least some of their Medicaid beneficiaries.
Section 1115 demonstration waivers. Under Section 1115 waiver authority certain Medicaid requirements can be waived and states can be permitted to use federal Medicaid funds in ways that federal rules do not otherwise allow. For example, states may cover CHW services under Section 1115 demonstration authority by allowing CHWs to provide services to Medicaid certain enrollees (e.g., as part of a pilot program), through authorizing incentive payments for CHW-related activities, or by providing funding for CHW infrastructure. Alternative delivery system models requiring team-based care may also allow for more flexibility in paying for CHW services. CHW provisions may be part of broader (and often complex) state Section 1115 waivers which usually involve a lengthy approval (and negotiation) process with the Centers for Medicare and Medicaid Services (CMS). Section 1115 waivers are generally approved for five years and are subject to transparency, public notice, evaluation, and other federal requirements.
As of July 1, 2022, over half of responding states (29 of 48) reported allowing Medicaid payment for services provided by CHWs (Figure 1).27,28 Coverage approaches vary and may include payment authorized under state plan, CHWs included as part of a Health Home program care team, CHWs included as members of interdisciplinary teams or networks under a Section 1115 demonstration waiver, or CHW services provided by MCOs.29
CHW COVERAGE UNDER STATE PLAN AUTHORITY
Nine states (California, Indiana, Louisiana, Minnesota, North Dakota, Nevada,30Oregon, Rhode Island, and South Dakota) reported payment is authorized under the Medicaid state plan for a specific set of services provided by CHWs as of July 1, 2022.31, 32 ,33 ,34 This includes four states (California, Louisiana, Nevada, and Rhode Island) that implemented coverage in 2022 (FY 2022 or the beginning of FY 2023). Four additional states (Illinois, Kentucky, Michigan, and New York) reported plans to implement coverage of CHW services under state plan authority in FY 2023.
The table below summarizes features of a few recently implemented CHW state plan amendments.
At least four additional states reported plans to implement Medicaid coverage/payment of CHW services under state plan authority (as a covered benefit) in FY 2023, including:
In Illinois, CHWs are currently funded through Medicaid MCO administrative dollars and through the Healthcare Transformation Collaborative. Medicaid MCOs may employ CHWs or pay for CHW services with administrative dollars. Healthcare Transformation Collaboratives are provider-led collaboratives focused on innovative and equity-focused solutions to reimagine healthcare in Illinois; many have incorporated CHWs in their proposals. The state is working to add certified CHWs as a Medicaid provider type and covered Medicaid service through a state plan amendment; this will allow CHWs to bill Medicaid directly and be reimbursed for services. A CHW certification is under development.
Kentucky currently has a CHW program funded with state dollars. It is a collaboration between the Department for Public Health and the University of Kentucky. State legislation was passed in the 2022 Kentucky legislative session mandating that the Department for Medicaid Services reimburse for CHWs and work with other stakeholders to create a public/private partnership that expands CHWs throughout the state. The Department is currently working with stakeholders to identify best practices and reimbursement models to expand the CHW footprint in 2023.
Michigan Medicaid has developed and enhanced contract requirements for MCOs relative to the provision of CHW services, while direct reimbursement mechanisms have not (to date) been defined or implemented through program policy. MCOs have been required to ensure they meet the contractually defined ratio of CHWs to members which has evolved from a volume ratio of 1:20,000 to 1:5,000 over time. In FY 2023, Michigan will be exploring opportunities to leverage learnings from the CHW services through MCOs and identifying appropriate policy, coverage, and reimbursement methodology to support broader acceptance and use of CHWs across all managed care programs and fee-for service. The state reported plans to add CHW services as a covered benefit in FY 2023.
New York will seek a state plan amendment to add coverage of CHWs for pregnant and postpartum individuals in 2023.
CHW COVERAGE INITIATIVES under DEMONSTRATION AND Other authorities
Several states reported other CHW coverage initiatives planned for FY 2023 including under Section 1115 demonstration authority or planned as part of a CMS Center for Medicare and Medicaid Innovation (CMMI) model. Examples include:
As part of the MassHealth Section 1115 demonstration, Massachusetts has provided delivery system reform incentive payment (DSRIP) funding to accountable care organizations (ACOs) to hire CHWs and has funded CHW core competency trainings (which align with CHW core competencies developed by the Massachusetts Department of Public Health and enable CHWs to meet one of the qualifications for CHW certification). The state has also developed and funded advanced CHW trainings in mental health, substance use disorder, and telehealth and trainings for CHW supervisors. As of July 2022, 600 health care workers had participated in the CHW core competency and CHW supervisor trainings. As part of their next Section 1115 waiver, the state has authority to sub-capitate primary care within ACO models, which will allow financing of team-based care for primary care services in a non-FFS model. These sub-capitation funds can be used to hire CHWs in support of the team-based care model. The state will also be funding additional core competency and advanced trainings in mental health, substance use disorder, and telehealth trainings for CHWs during the next waiver period.
Maine plans to add CHWs to its maternal opioid model of care early FY 2023. This model is a Center for Medicare and Medicaid Innovation (CMMI) initiative that supports the delivery of integrated physical and behavioral health care and wrap-around services for pregnant and postpartum women with opioid use disorder and their infants. Maine’s model provides a team-based approach to care for the eligible population, currently including a perinatal provider, substance use counselor, patient navigator, nurse care manager, recovery coach, and perinatal provider.
The New Jersey Division of Medical Assistance and Health Services (DMAHS), in partnership with the state Department of Health (DOH), have identified CHWs as a promising resource to enhance care coordination, address disparities, and improve outcomes for Medicaid beneficiaries. To support and advance this work, the state has requested expenditure authority as part of its Section 1115 renewal application to support a set of CHW pilots, to be administered by interested MCOs in collaboration with DMAHS and the NJ DOH's Colette Lamothe-Galette Community Health Worker Institute.35 (The goal of the Institute is to create a standardized community health worker training and certification program, resulting in a robust CHW workforce.) DMAHS also participates in a CHW sustainability workgroup led by DOH members from the Institute.
North Carolina will incorporate CHWs as “care management extenders” within their “Tailored Plan” care management model. The state will launch its “Tailored Plans” on April 1, 2023, offering integrated services to enrollees with significant behavioral health needs and intellectual/developmental disabilities (I/DD). Care management extenders can support care managers in delivering care management and meeting member contact requirements.36 CHWs that have completed the NC CHW standardized core competency training meet extender qualification requirements. North Carolina Medicaid is also preparing to leverage existing contract authority with its “Standard Plans” to expand the number of CHWs used throughout its Medicaid managed care system by establishing a CHW staffing requirement ratio. The state is also considering how health plan-level requirements filter down to providers with local care management responsibilities and how to encourage community-based organization partnership and deployment of CHWs.
Looking Ahead
In this year’s 22nd annual budget survey, states reported focusing on both longstanding issues and new priorities, including new and expanded initiatives to improve equity and reduce health disparities, improve behavioral health access and supports, and address workforce challenges. Many states also reported new and expanded benefits related to enrollees’ social needs. Research indicates community health workers can play a role in reducing racial and ethnic health disparities and addressing health-related social needs among Medicaid beneficiaries. CHWs may also potentially play a role in helping individuals access health care in areas with provider shortages.37 As states look to expand the use of CHWs in the future, evidence from recently implemented and existing CHW programs and from the infusion of ARPA and other federal funds to increase CHW workforce capacity may provide important experience and lessons to inform these efforts.
Chidinma A. Ibe, Debra Hickman and Lisa A. Cooper, “To Advance Health Equity During COVID-19 and Beyond, Elevate and Support Community Health Workers,” JAMA Health Forum 2, no.7 (July 2021), https://doi.org/10.1001/jamahealthforum.2021.2724. ↩︎
Sonia Ahmed, et al. “Community health workers and health equity in low- and middle-income countries: systematic review and recommendations for policy and practice,” International Journal for Equity in Health 21, no. 49 (April 2022), https://doi.org/10.1186/s12939-021-01615-y. ↩︎
Miya L. Barnett, et al. “Mobilizing Community Health Workers to Address Mental Health Disparities for Underserved Populations: A Systematic Review” Administration and Policy in Mental Health and Mental Health Services Research 45, (July 2017), https://doi.org/10.1007/s10488-017-0815-0. ↩︎
Richard Crespo et al. “An Emerging Model for Community Health Worker–Based Chronic Care Management for Patients With High Health Care Costs in Rural Appalachia.” Preventing Chronic Disease 17 (February 2020), http://dx.doi.org/10.5888/pcd17.190316. ↩︎
Erica T. Marshall, et al, “Home Visits for Children With Asthma Reduce Medicaid Costs.” Preventing Chronic Disease 17 (February 2020), http://dx.doi.org/10.5888/pcd17.190288. ↩︎
State fiscal years begin on July 1 except for these states: New York on April 1; Texas on September 1; Alabama, District of Columbia, and Michigan on October 1. ↩︎
States were asked, “As of July 1, 2022, does your state allow for Medicaid payment for services provided by a CHW – i.e., an individual who serves as a liaison between the community and health care and social services including, for example, promotoras, care coordinators, community health educators, outreach and enrollment agents, patient navigators, etc. (but excluding doulas and peer educators)?” ↩︎
Megan Coffinbargar, April J. Damian and John M. Westfall, “Risks and Benefits to Community Health Worker Certification.” Health Affairs Forefront (July 2022), doi: 10.1377/forefront.20220705.856203.
↩︎
A 2014 update to the Center for Medicare and Medicaid Services’ (CMS) regulatory definition of preventive services allows these services to be provided by non-licensed providers, including CHWs. ↩︎
For example, to add coverage under the preventive services benefit, states need to submit a state plan amendment (SPA) that describes the specific CHW services to be delivered, qualifications for practitioners who will deliver the services, limitations on services, and payment methodology. For CHW services covered under the outpatient hospital services benefit, states are not required to identify these services in the state plan. https://www.macpac.gov/wp-content/uploads/2022/04/Medicaid-coverage-of-community-health-worker-services-1.pdf↩︎
For substance use disorder (SUD) Health Homes approved on or after October 1, 2018, the SUPPORT Act extends the enhanced federal match rate from eight to ten quarters. ↩︎
States were asked, “As of July 1, 2022, does your state allow for Medicaid payment for services provided by a CHW – i.e., an individual who serves as a liaison between the community and health care and social services including, for example, promotoras, care coordinators, community health educators, outreach and enrollment agents, patient navigators, etc. (but excluding doulas and peer educators)?” ↩︎
KFF analysis of state responses revealed states may have interpreted questions about CHW policies differently. KFF attempted to verify/confirm policies in place by pulling state plan amendments (SPAs) and conferring with other sources. ↩︎
KFF count of states that “allow Medicaid payment” for CHW services may differ from and include more states than reported by other sources, as KFF broadly defined related Medicaid CHW coverage approaches to include coverage under Medicaid state plan authority (see EN 31 below), CHWs as part of a Health Home program care team (allowed or required by state), CHWs included as members of interdisciplinary team or network under Section 1115 waiver (allowed or required by state), and CHW services provided by MCOs (allowed or required by state). KFF count may include states that allow MCOs to provide CHW services using administrative funds or as “value-added” services. ↩︎
Nevada also provides coverage of CHW services for Group VIII expansion adults through a separate ABP State Plan Amendment. ↩︎
States were asked “As of July 1, 2022, is payment authorized under the State Plan for a specific set of services provided by CHWs under the supervision of, or recommended by, a physician or other licensed provider?” ↩︎
Alaska provides state plan coverage for Community Health Aides/Practitioners (CHA/Ps) but the state confirmed CHA/Ps are service providers, not public health workers and do not fit the definition of CHW established by the APHA. However, Alaska may be counted as a state that allows payment for CHW services in other sources. ↩︎
KFF analysis of state responses revealed states may have interpreted questions about CHW policies differently. KFF attempted to verify/confirm policies in place by pulling state plan amendments (SPAs) and conferring with other sources. ↩︎
Several states reported that they authorize payment under the state plan for a specific set of services provided by CHWs but are not reflected in our count / here. These states were excluded because we were unable to identify/locate the corresponding state plan amendment. These states may have been referencing coverage under the ACA Health Homes state plan option. States that were excluded from the state plan authority count were not reported by other sources as reimbursing for CHW services under state plan authority. ↩︎
KFF’s Kaiser Health News (KHN) is launching a weekly one-minute health information segment for CBS News Radio stations that will help millions of listeners stay informed and make better health decisions.
CBS News Radio began offering the KHN Health Minute to its more than 700 affiliate stations weekly on Jan. 12. The brief segments will include a broad range of health stories and consumer information reported by KHN’s nationwide team of health reporters. Listeners can expect stories ranging from navigating medical bills and debt, to changes in health care delivery and policy and public health. A signature focus of the minutes will be on what all the changes and policy debates that people hear about actually mean for them.
In the first KHN Health Minute, hear how noise pollution affects health and why an optimistic outlook may help people live longer.
The collaboration is the latest product of an ongoing partnership between CBS News and KHN.
“Expanding on KHN’s partnership with CBS, I’m thrilled to offer the network’s radio listeners across the country the KHN Health Minute,” said KHN Editor-in-Chief Elisabeth Rosenthal. “It offers a fun, fast and informative way to keep up with the latest and most important health care news.”
“Every day health news is in the headlines as we battle new and emerging threats. Our listeners will benefit greatly with this topical information that is both accessible and actionable,” said Craig Swagler, vice president and general manager of CBS News Radio. “The powerful audience reach of the radio medium connects on-the-go listeners with health information they need and can use instantaneously.”
Listeners can check for the KHN Health Minute on their local CBS News Radio station.
The broader partnership also features regular appearances by Dr. Céline Gounder, KHN’s senior fellow and editor-at-large for public health, on all of CBS News’ platforms, as well as stories, segments, and specials drawing upon reporting from across KHN’s newsroom and bureaus. It includes the popular “Bill of the Month” series, in which Rosenthal appears regularly on “CBS Mornings” to discuss surprising medical bills and what they tell us about the U.S. health care system. “Bill of the Month” is a collaborative investigative project of KHN and NPR.
KHN, a program of KFF, is an award-winning news service with a national newsroom in Washington, D.C., and a rapidly growing network of regional bureaus in California, the Midwest, the Mountain States, and the South, as well as a new Rural Health Desk. KHN works with many editorial partners, and media outlets can republish KHN stories at no charge. News organizations interested in working with KHN should contact the news service at KHNPartnerships@kff.org.
About KFF and KHNKHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis, Polling and Survey Research and Social Impact Media, KHN is one of the four major operating programs at KFF. KFF is an endowed nonprofit organization providing information on health issues to the nation.
About CBS News Radio:
CBS News Radio provides news, talk, information, entertainment, and special events coverage to more than 700 radio stations in the United States, with affiliates in 24 of the top 25 markets. CBS News Radio is also heard hourly on the SiriusXM Platform on P.O.T.U.S. (Channel 124). CBS News Radio is home to the “CBS World News Roundup,” the nation’s longest-running news program, debuting in 1938. In addition to providing breaking news and information, the division provides simulcasts of the CBS EVENING NEWS, FACE THE NATION, and 60 MINUTES to affiliates. CBS News Radio programming is available digitally through the CBS News Radio app, Apple Music, Amazon’s Alexa service, and on the web.
As the nation marks the 50th anniversary of the Supreme Court of the United States landmark Roe v. Wade decision, which the Supreme Court overturned, 14 states have active litigation challenging state abortion bans and restrictions. A new KFF brief explains how individuals and organizations suing to block the bans are framing their legal challenges based on different state constitutional protections and state laws now that the battleground over abortion rights rests with states.
The legal challenges presented in state courts generally fall into three categories:
Broad Constitutional Challenges: In Ohio, Oklahoma, Georgia, and Utah, among others, the abortion ban challenges include claims that state constitutional protections, such as liberty, due process, and privacy rights include a right to abortion.
Health Care Amendment Challenges: Some state constitutions were amended to include a right to make health care and health insurance decisions in efforts to block the ACA’s individual coverage mandate. In Wyoming and Ohio, abortion advocates argue that this amendment includes the right to decide whether to have an abortion.
Religious Freedom Challenges: In Florida, Indiana, Kentucky, Utah, and Wyoming, people from various religious backgrounds argue abortion bans infringe on their religious rights.
In time, these challenges will reach each state’s highest court, ultimately deciding the constitutionality of state-level abortion bans determining whether abortion will be available in the state.
The Supreme Court of the United States decision in Dobbs returned the decision to restrict or protect abortion to states. In many states, abortion providers and advocates are challenging state abortion bans contending that the bans violate the state constitution or another state law.
These challenges generally fall into three categories:
Broad Constitutional Challenges: In Ohio, Oklahoma, Georgia, and Utah, among others, the abortion ban challenges include claims that state constitutional protections, such as liberty, due process, and privacy rights encompass a right to abortion.
Health Care Amendment Challenges: Some state constitutions were amended to include a right to make health care and health insurance decisions in an effort to block the ACA’s individual coverage mandate. In Wyoming and Ohio, abortion advocates argue that this amendment includes the right to make a decision about whether or not to have an abortion.
Religious Freedom Challenges: In Florida, Indiana,Kentucky,Missouri, Utah, and Wyoming people from various religious backgrounds argue abortion bans either unduly infringe on their religious exercise or violate state constitutional protections against the establishment of religion.
A number of state courts have responded favorably to many of these arguments and have temporarily blocked several bans while litigation on their constitutionality is ongoing. In time, these challenges will reach each state’s highest court, which will be the ultimate arbiter of the constitutionality of state-level abortion bans.
Introduction
Since the Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization, overturning Roe v. Wade and Planned Parenthood v. Casey, the legal landscape at the state level has been activated as never before. With the aim of restricting access to abortion, many states moved swiftly to lift court orders previously blocking bans, revive dormant pre-Roe bans, certify “trigger” bans, and enact new laws. Lacking federal protections, abortion providers have been on the front lines challenging these bans in state courts, questioning their constitutionality, not under the United States Constitution, but under each state’s constitution. Since the Dobbs decision, 23 states have tried to implement a complete ban or a pre-viability ban. In 6 states, these laws are currently blocked by courts. For an overview of the current legal status of abortion across the country, please see our abortion dashboard.
Although State Constitutions are similar to one another in many respects, each state has its unique judicial history and binding precedent, with State Supreme Court rulings diverging on liberty, privacy, and due process protections. Additionally, some states have amended their constitutions to include different abortion protections, while others have moved to assert that their constitution confers no right to abortion. Given these differences, abortion bans and restrictions that may be unconstitutional in some states, may be constitutionally permissible in others. As a result, the types of challenges on state constitutional grounds have varied in states banning – or attempting to ban – abortion access, including those where the question of a constitutional right to abortion had never reached their highest courts, the ultimate arbiters of the constitutionality of state laws.
Despite the variety in the types of legal challenges to abortion bans, a few patterns in the approaches have emerged in the abortion litigation landscape. In this issue brief, we present an overview of some of the types of challenges presented in state courts since the Dobbs ruling in June 2022 and highlight some of the novel strategies that are being used to defend access to abortion in states that have enacted abortion bans.
Background
Before the Supreme Court of the United States (SCOTUS) Dobbs decision, the supreme courts of ten states had recognized a constitutional right to abortion in their states’ constitutions, but often under differing guarantees and protections. For example, in Montana in 1999, the state’s highest court found that the state constitution contained stringent protections of the right to privacy, exceeding those provided by the federal constitution, and, as such, ruled that procreative autonomy (the right to decide whether or when to have children) is protected under the right to privacy. Florida and Minnesota are two other states where the highest courts have ruled that their states’ constitutions include a more expansive right to privacy than SCOTUS had found in the federal constitution. In Massachusetts, the state’s highest court recognized that the right to abortion is found within the state constitutional due process rights.
Currently, nine state supreme court decisions finding state constitutional protections for abortion are binding precedent and have not been overturned by a subsequent decision or constitutional amendment. (Table 1). Just as SCOTUS overturned Roe, state supreme courts may overturn their previous decisions upholding the right to abortion in their state constitutions. In 2018, the Iowa Supreme Court found that the state constitutional rights of due process and equal protection encompassed the right to abortion. However, in June 2022, the Iowa court reversed itself, finding that the state constitution confers no fundamental right to abortion.
While a state’s highest court has final say about the constitutionality of laws under its constitution, the legislature and electorate may amend the constitution at a future date, rendering previous court decisions moot or severely impacting the landscape of litigation in that state. For example, in 2000 the Tennessee Supreme Court issued a decision finding the state’s constitutional protections for privacy encompassed a right to abortion. However, in 2014, voters approved a ballot measure amending the state’s constitution and explicitly expressing that the constitution did not confer a right to abortion, superseding the 2000 court’s ruling. In addition to Tennessee, Arkansas, Louisiana, and West Virginia (Table 2) have passed ballot measures to amend their state constitutions to curtail the right to abortion. Although these amendments may not explicitly prohibit abortion in the state, they can prevent the state supreme courts from ruling that other, broader constitutional protections encompass a right to abortion. This allows state legislatures to enact abortion bans and restrictions with the confidence that the state’s highest court will not find them unconstitutional and unenforceable.
After the Dobbs decision, some states used ballot measures to attempt to amend their constitutions. The ballot measures seeking to curtail the right to abortion in Kansas and Kentucky failed, while California, Michigan, and Vermont (Table 3) successfully passed constitutional amendments recognizing a right to abortion. Enshrining these rights in the state constitution amounts to a much stronger, more stable protection than simply enacting laws recognizing such a right, which can be repealed with a change in party control of a state legislature. In contrast, a constitutional amendment that explicitly protects a right to abortion, or reproductive autonomy more broadly is much harder to change or repeal.
Challenges in State Courts Following the Dobbs Decision
Who is challenging the abortion bans in state courts?
Most legal challenges to state abortion bans are being brought by abortion care providers and clinics, presenting claims on behalf of themselves, their staff, and their patients. This is common in lawsuits regarding the right to access abortion care. Many prominent cases, such as Planned Parenthood v. Casey and Dobbs v. Jackson Women’s Health Organization, have been brought by providers and clinics.
Although there is a long history of providers and clinics challenging abortion restrictions, officials in some states dispute the legal “standing” providers have to bring these suits. For courts to be able to hear a case at all there must be a party with a real, concrete injury whose protection depends on an intervention by the Court. Usually, a person can only challenge the constitutionality of a law if it infringes on their own rights, not broadly the rights of others. However, legal challenges to abortion bans and restrictions brought by providers and clinics generally argue there is a constitutional right to receive abortion care and restrictive laws violate this right. In this way, providers argue that the rights of their patients – not necessarily their own – are being infringed by the bans.
This practice of suing to vindicate the rights of a closely related party (in this case providers and their patients) is called “third-party standing.” It allows a person or organization to assert the rights of another individual when it is difficult for them to assert their own rights, and the parties’ interests are closely aligned. Given the time limited duration of a pregnancy, it is difficult for pregnant people to personally challenge abortion restrictions while often facing numerous obstacles including financial limitations, and concerns for privacy and personal safety. For almost 47 years, federal and state courts have permitted doctors and clinics to sue on their behalf. The Supreme Court of the United States established third-party standing for abortion doctors on behalf of their patients in a 1976 decision, Singleton v. Wulff. That case was brought by two doctors challenging the exclusion of abortion in Missouri’s Medicaid program. Justice Blackmun wrote for the court, “aside from the woman herself, the physician is uniquely qualified, by virtue of his confidential, professional relationship with her, to litigate the constitutionality of the state’s interference with, or discrimination against, the abortion decision.” Singleton recognized that women can be fearful to assert their abortion rights out of concern for their privacy.
However, since the Supreme Court’s decision in Dobbs, some state courts have become more receptive of arguments against providers’ third party standing. Most notably, in Florida, a state Court of Appeals called into question providers’ ability to sue on behalf of patients in its decision refusing to block an abortion ban. If the ability of providers and clinics to bring challenges to courts is curtailed, it may be more difficult for these challenges to proceed successfully if only those who are seeking abortion are permitted to sue.
In addition to clinics and providers, other individuals and groups have challenged abortions bans. Some recent notable cases include a challenge under the Indiana Religious Freedom Restoration Act, where five unnamed women and a Jewish pro-choice organization are contesting the constitutionality of the state ban constitutionality on freedom of religious exercise grounds. This challenge is detailed below. Another notable case is the lawsuit disputing the constitutionality of the Wyoming’s total abortion ban, where a pregnant woman and a woman of reproductive age, along with two physicians, a clinic, and an advocacy organization are suing the state. This challenge rests on constitutional privacy rights and the right to make health care decisions. And, finally, in Wisconsin, the state’s Attorney General and Medical Examining Board filed a lawsuit seeking judgment that the state’s pre-Roe ban is unenforceable, arguing that the ban is incompatible and at odds with the many other abortion statutes the state enacted since the decision in Roe.
Types of Challenges
General Constitutional Challenges
In many states, lawsuits challenging the constitutionality of bans argue that the laws violate due process, liberty, equal protection, or privacy rights, or a combination of these rights. Although the states’ constitutional protections are similar, state Supreme Courts have diverged in their interpretation of these rights, with some recognizing that certain state constitutional rights are more expansive than their federal counterparts. There is active litigation in Ohio, Oklahoma, Georgia, Indiana, Kentucky, Utah and Wyoming, which include constitutional violations as the part of the basis of their challenges to the states’ abortion bans.
In issuing a preliminary injunction blocking the enforcement of Ohio’s abortion ban, the state trial court judge found that the Ohio Constitution includes the right to abortion in the right to “liberty” and in the “Due Course of Law” provision which states: “All courts shall be open, and every person, for an injury done him in his land, goods, person or reputation, shall have a remedy by due course of law, and shall have justice administered without denial or delay. Suits may be brought against the state, in such courts and in such manner, as may be provided by law.” The court also relied on the Health Care Amendment to the constitution which is discussed below.
In Wyoming, the presiding judge also found that the abortion ban’s exceptions regarding cases of rape or incest and medical emergencies could be found to be unconstitutionally vague. Judges in both Ohio and Wyoming also found the abortion bans would violate each state’s equal protection provisions, despite the states’ arguments that these laws apply to everyone equally.
In January 2023, the South Carolina Supreme Court struck down the state’s 6 -week ban as violating the state’s constitutional privacy provision. Unlike the U.S. federal constitution, South Carolina’s constitution has an explicit right to privacy. While each state court is independent and is not obliged to follow other state court decisions, the South Carolina Supreme Court reviewed the decisions of other state Supreme Courts to inform their own ruling that the right to privacy includes the right to abortion. Ten other states also have an explicit right to privacy in their state constitutions.1
Health Care Amendment Challenges
In Wyoming and Ohio, the legal challenges to abortion bans revolve around some of these same constitutional protections most other challenges rely on, but also around each respective state constitution’s amendment regarding health care and health insurance. These two states, along with Alabama, Arizona, and Oklahoma2 , amended their constitutions in the wake of the passing of the Affordable Care Act (ACA), to create a right to make health care and insurance decisions and block the insurance coverage mandate in the federal ACA. By creating a right to make decisions about health care and health insurance, the state legislatures hoped they could secure the individual right to refuse to purchase health insurance and to ensure the right to purchase private health insurance, thereby circumventing the law’s individual mandate to obtain insurance. In Wyoming, the constitutional amendment was approved in a ballot measure in the November 2012 elections. This amendment safeguards the right to health care access, broadly giving every adult the right to make his or her own health care decisions. In Ohio, the Health Care Freedom Amendment was approved in a November 2011 ballot measure. This amendment protects the right to purchase health care, stating that “[n]o federal, state, or local law or rule shall prohibit the purchase or sale of health care or insurance.”
Despite the narrow intent of the amendments to block ACA implementation, their broad language has allowed providers and advocates in Ohio and Wyoming to successfully argue that these measures create a general constitutional right to make health care decisions. And abortion, they argue, is health care under any ordinary definition of health care. Thus, providers argue, these amendments protect the right to make health care decisions and then logically protecting the decision about whether to have an abortion, making Ohio’s 6-week LMP ban and Wyoming’s total ban unconstitutional.
In response, state defendants that oppose abortion rights in both cases argue these health care amendments do not remove a state’s ability to regulate health care, or outlaw abortion. The state Courts in both states, however, were receptive to the argument that the right to make health care decisions encompasses the right to make decisions about whether to have an abortion and blocked the bans from being enforced. Judges in both courts asserted that, regardless of the intent with which the amendment was passed, the plain meaning of the language used in it likely conferred a right to abortion. In short, the state trial court judges agreed with the argument that abortion qualifies as health care and the general constitutional protection to make health care decisions created by the amendments would make the bans unconstitutional. Both cases are expected to reach each state’s highest court, where the constitutionality of the bans will ultimately be decided.
Religious Freedom Challenges based on State Constitutions and The Religious Freedom Restoration Act
Individuals, religious faith leaders and organizations have brought legal challenges in several states including Florida, Indiana, Kentucky, Missouri, Utah and Wyoming claiming their state’s abortions restrictions violate their religious freedom. Some of these litigants base their claims solely on the state’s constitution’s right to freely exercise one’s religion, while others are challenging their state abortion restrictions on their state’s Religious Freedom Restoration Act. Indiana’s case is the only religious challenge to an abortion ban to date where a court has responded to the state RFRA arguments at hand and evaluated their validity.
The plaintiffs in Indiana have based their challenge only on the state’s RFRA law. The Indiana RFRA law, adopted in 2015, “prohibits government action that substantially burdens a person’s religious exercise, unless the burden is in furtherance of a compelling governmental interest and is the least restrictive means of furthering that interest.” Several states have similar laws that are modeled after a 1993 federal law by the same name, which applies only to federal laws, not to state or local laws. Federal and state RFRA laws have been used to challenge laws requiring contraceptive coverage and anti-discrimination laws. Most notably, the federal Religious Freedom Restoration Act was the basis for the lawsuit brought by Hobby Lobby to challenge the contraceptive coverage requirement based on the for-profit corporation’s religious objections to certain contraceptive methods.
In the Indiana case, a group of women and a religious pro-choice organization argue the state’s abortion ban substantially burdens their religious exercise. Specifically, the plaintiffs argue that their respective religions (Judaism, Islam, and Unitarian Universalism) direct them to obtain abortion care under circumstances that the ban does not allow. This includes situations where the pregnancy jeopardizes the mental health of the pregnant person or their physical health, without necessarily causing serious risk of substantial and irreversible physical impairment of a major bodily function, as the ban’s health exception would require. Plaintiffs thus argue that their sincere beliefs would be substantially burdened if the ban went into effect. They further argue that the state’s right to protect potential life is not a strong enough interest to overcome their religious exercise rights – which are protected by Indiana’s RFRA – and bar them from receiving abortion care in situations where their sincerely held religious beliefs would call for them to seek it.
On December 2, 2022, the Marion County Superior Court granted a preliminary injunction, blocking the ban from being enforced against the plaintiffs, while the underlying question is resolved. Another Indiana state trial court had already issued an order blocking this ban from being enforced due to a previous challenge to the law, which argued the liberty guarantees of the Indiana Constitution provide a right to privacy that includes the right to determine whether not to have an abortion. The state has appealed both court decisions blocking enforcement of the ban and is requesting the Indiana Supreme Court eliminate the preliminary injunction in the RFRA challenge.
Conclusion
The fate of the constitutionality of abortion bans and the legal availability of abortion services in states where there are ongoing legal battles will most likely rest on each state’s highest court. Since SCOTUS issued its decision in Dobbs, the South Carolina Supreme Court has ruled that their state constitution protects the right to abortion. Conversely, a week before Dobbs’ decision, the Iowa Supreme Court overturned their previous decision, and found that their state constitution does not include any protections for abortion. It will take some time for the other cases underway to reach their respective State Supreme Courts and to have decisions on the states’ constitutional protections of abortion that will ultimately affect abortion access across the nation.
Appendix Table 1
The states of Alaska (Const. art. 1, § 22), Arizona (Const. art. 2, § 8), California (Const. art. 1, § 1), Florida (Const. art. 1, § 23), Hawai’i (Const. art. 1, § 6), Illinois (Const. art. 1, § 6), Louisiana (Const. art. 1, § 5), Montana (Const. art. 2, § 10), New Hampshire (Const. art. 2-b), South Carolina (Const. art. 1, § 10), and Washington (Const. art. 1, sec. 7) all contain explicit protections of the right to privacy. ↩︎