Stand-Alone Drug Plans Cover a Larger Share of Medicare Part D Enrollees Living in the Most Rural Areas Than Medicare Advantage Plans
The growing role of Medicare Advantage has been a defining feature of Medicare in recent years, with Medicare Advantage plans now covering more than half of all eligible Medicare beneficiaries. While most Medicare Advantage enrollees (and most people with Medicare overall) live in urban areas, as of 2024, most Medicare beneficiaries who live in the nation’s most rural counties are enrolled in traditional Medicare, not Medicare Advantage. This means that reliance on Medicare’s stand-alone prescription drug plans (PDPs) for coverage of the Medicare Part D prescription drug benefit is likely to be greater among Medicare beneficiaries living in the most rural parts of the country.
Concerns about the stability of the Medicare Part D stand-alone drug plan market have arisen recently as changes to the Part D benefit have taken effect that have increased plan costs, including a new $2,000 out-of-pocket spending cap. These costs have a greater impact on premiums for stand-alone drug plans because Medicare Advantage plans can use rebate dollars to reduce or eliminate Part D premiums, which is not an option for PDPs. To address these concerns, the Biden Administration implemented a demonstration program in 2024 to help stabilize the PDP market and prevent large year-over-year premium increases through the availability of enhanced premium subsides, designed to last for up to three years. While the demonstration helped limit premium increases in 2025, the number of PDPs dropped considerably and substantial variation in monthly PDP premiums persisted.
The Trump administration has not provided a clear signal as to whether it will continue the premium stabilization demonstration for 2026 and if so what the specific parameters will be. However, President Trump issued an executive order that, among other provisions, seeks recommendations from the Department of Health and Human Services and the Office of Management and Budget on ways to stabilize and reduce Part D premiums, without specifically mentioning stand-alone drug plans. Scaling back the PDP premium stabilization demonstration to a large degree could result in continued increases in PDP premiums and further reductions in PDP availability, which would have implications for access to and affordability of Part D drug coverage among Medicare beneficiaries enrolled in PDPs, including those living in the nation’s most rural areas.
To understand the role of Medicare Part D stand-alone PDPs in serving rural Medicare beneficiaries, this data note analyzes 2025 Part D enrollment in PDPs and Medicare Advantage drug plans by geographic area nationally and at the state level. The analysis defines geographic areas using Urban Influence Codes published by the U.S. Department of Agriculture. (See Methods for details.)
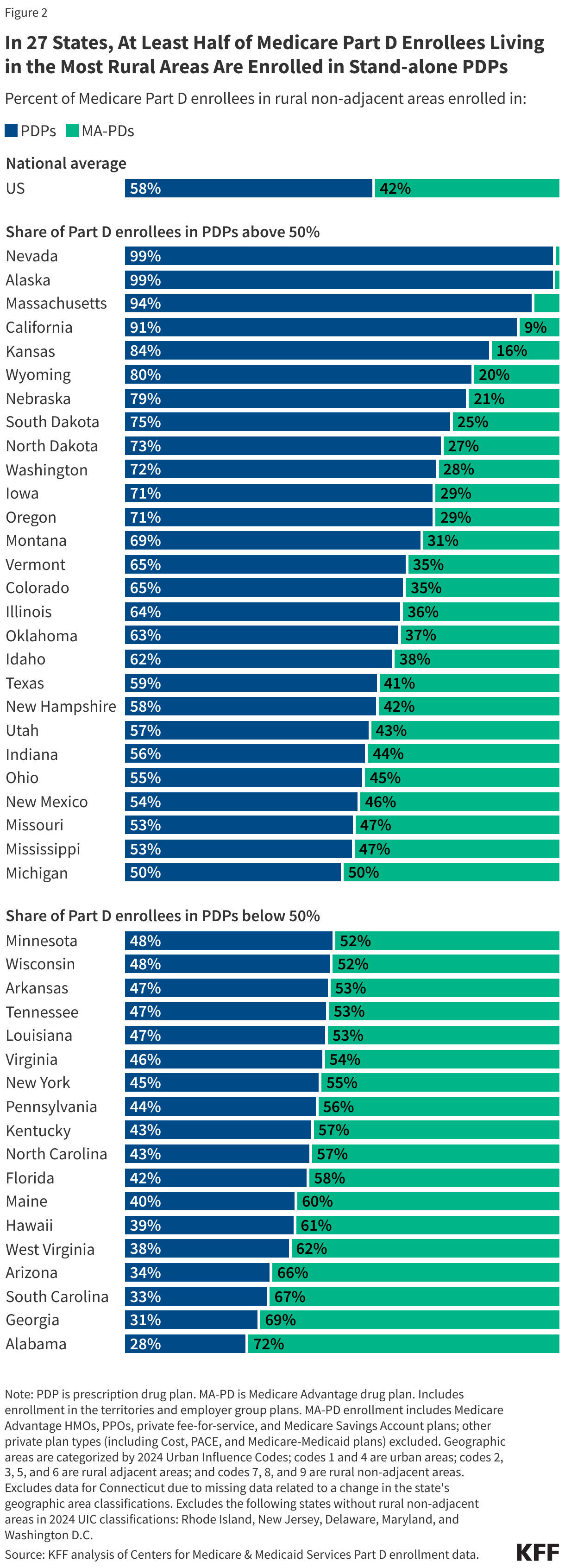
Nearly 6 in 10 Medicare Part D enrollees living in the nation’s most rural areas are enrolled in stand-alone PDPs in 2025. Among Medicare Part D enrollees who live in the most rural areas in 2025, nearly 6 in 10 (58%) are enrolled in stand-alone PDPs, while the remainder (42%) are enrolled in Medicare Advantage drug plans (MA-PDs) (Figure 1). This compares to 46% of Part D enrollees living in rural areas adjacent to urban areas enrolled in PDPs and 41% of Part D enrollees living in urban areas in PDPs.

In 27 states, at least half of Medicare Part D enrollees living in the most rural areas are enrolled in stand-alone PDPs. This includes 8 states with 75% or more of Part D enrollees in the most rural areas in PDPs (Nevada, Alaska, Massachusetts, California, Kansas, Wyoming, Nebraska, and South Dakota) (Figure 2). More limited participation of local providers in Medicare Advantage plan provider networks is likely to factor into lower overall Medicare Advantage (and MA-PD) enrollment and higher PDP enrollment in some rural areas.
In most states, a larger share of Medicare Part D enrollees living in the most rural areas are enrolled in PDPs than those who live in less rural or urban areas. In 35 states, a larger share of Medicare Part D enrollees living in the most rural areas of the state are enrolled in PDPs compared to those who live in less rural areas and in urban areas (Figure 3). For example, in Kansas, 84% of Part D enrollees in the most rural areas are enrolled in PDPs compared to 53% of those in urban areas; in California, 91% of Part D enrollees in the most rural areas are enrolled in PDPs compared to 39% of Part D enrollees in urban areas; in Idaho, 62% of Part D enrollees in the most rural areas are in PDPs compared to 36% of those in urban areas.
Additionally, in 15 states (Alaska, Massachusetts, Kansas, Wyoming, Nebraska, South Dakota, North Dakota, Iowa, Montana, Vermont, Illinois, New Hampshire, New Jersey, Delaware, and Maryland) and the District of Columbia, PDPs cover half or more of Part D enrollees living in all geographic areas in the state.

This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Juliette Cubanski and Tricia Neuman are with KFF. Anthony Damico is an independent consultant.
Methods
This analysis uses March 2025 Medicare Part D enrollment data from the Centers for Medicare & Medicaid Services to analyze the share of Medicare Part D enrollees who are enrolled in stand-alone prescription drug plans and Medicare Advantage drug plans in counties that are part of urban or rural areas, using the 2024 Urban Influence Codes published by the U.S. Department of Agriculture. To examine the role of urban influence, which affects access to infrastructure, including for the delivery of health care services, rural counties are further classified as adjacent to or not adjacent to an urban (metropolitan) area.
This analysis categorizes the 9 Urban Influence Codes as follows:
Urban
1: Large metro (in a metro area with at least 1 million residents)
4: Small metro (in a metro area with fewer than 1 million residents)
Rural non-adjacent
2: Micropolitan, adjacent to a large metro area
3: Noncore, adjacent to a large metro area
5: Micropolitan, adjacent to a small metro area
6: Noncore, adjacent to a small metro area
Rural non-adjacent
7: Micropolitan, not adjacent to a metro area
8: Noncore, not adjacent to a metro area and contains a town of at least 5,000 residents
9: Noncore, not adjacent to a metro area and does not contain a town of at least 5,000 residents
In this analysis, large and small metropolitan areas (Urban Influence Codes 1 and 4) are referred to as “urban” areas; rural counties not adjacent to an urban (metropolitan) area (Urban Influence Codes 7, 8, and 9) are referred to as the “most rural” areas, and rural counties adjacent to an urban (metropolitan) area (Urban Influence Codes 2, 3, 5, and 6) are referred to as “less rural” areas.
The denominator for this analysis is Medicare Part D enrollees, which can include those with either Part A or Part B or both parts. A separate KFF analysis examines the share of eligible Medicare beneficiaries with coverage under traditional Medicare and Medicare Advantage, which includes those with both Part A and Part B and is therefore a different denominator than that which is used in this analysis. In addition, not all Medicare beneficiaries are enrolled in a Part D plan.