How Would Drug Price Negotiation Affect Medicare Part D Premiums?
Proposals to allow the federal government to negotiate prescription drug prices, such as H.R. 3, the Elijah E. Cummings Lower Drug Costs Now Act, aim to lower out-of-pocket drug costs for Medicare beneficiaries and private plan enrollees and achieve savings for Medicare. The debate over a budget reconciliation package in the coming weeks, and possibly months, is likely to focus heavily on the savings to Medicare, which can be used to expand Medicare benefits and fund other health care priorities. However, by lowering Medicare spending for Part D, which covers retail prescription drugs, drug price negotiation proposals would also be expected to lower premiums that beneficiaries pay for Part D coverage.
According to an analysis by Medicare’s actuaries of the version of H.R. 3 that passed the House of Representatives in the 116th Congress, the drug price negotiation provisions in the legislation would reduce spending by Medicare Part D enrollees by $117 billion between 2020 and 2029, including a reduction of $102.6 billion in cost sharing for people who use drugs covered under Part D that are subject to negotiation, and another $14.3 billion reduction in Part D premiums (in addition to Medicare savings). This data note estimates average premium savings attributable to the negotiations provision of H.R. 3 on a per capita basis for Part D enrollees who pay premiums (including those receiving partial low-income subsides) in dollar amounts and as a share of the base beneficiary premium, based on aggregate premium reductions and baseline premiums projected by Medicare’s actuaries through 2029.
How does drug price negotiation affect Part D premiums?
Under Part D, beneficiary premiums are calculated to cover 25.5 percent of costs for standard coverage, which includes benefit payments before the catastrophic coverage threshold as well as catastrophic costs (i.e., reinsurance). Allowing the federal government to negotiate drug prices is expected to result in lower drug prices for those drugs subject to negotiation, which would lower Medicare spending for the standard drug benefit and lower Part D premiums, with significant reductions in reinsurance spending (i.e., costs above the catastrophic threshold). These reductions are expected to be somewhat offset by cost increases attributable to a reduction in rebates paid by drug manufacturers to Part D plans (which plans use to lower their total costs) and higher prices for new drugs.
What is the expected magnitude of savings on Part D premiums per enrollee?
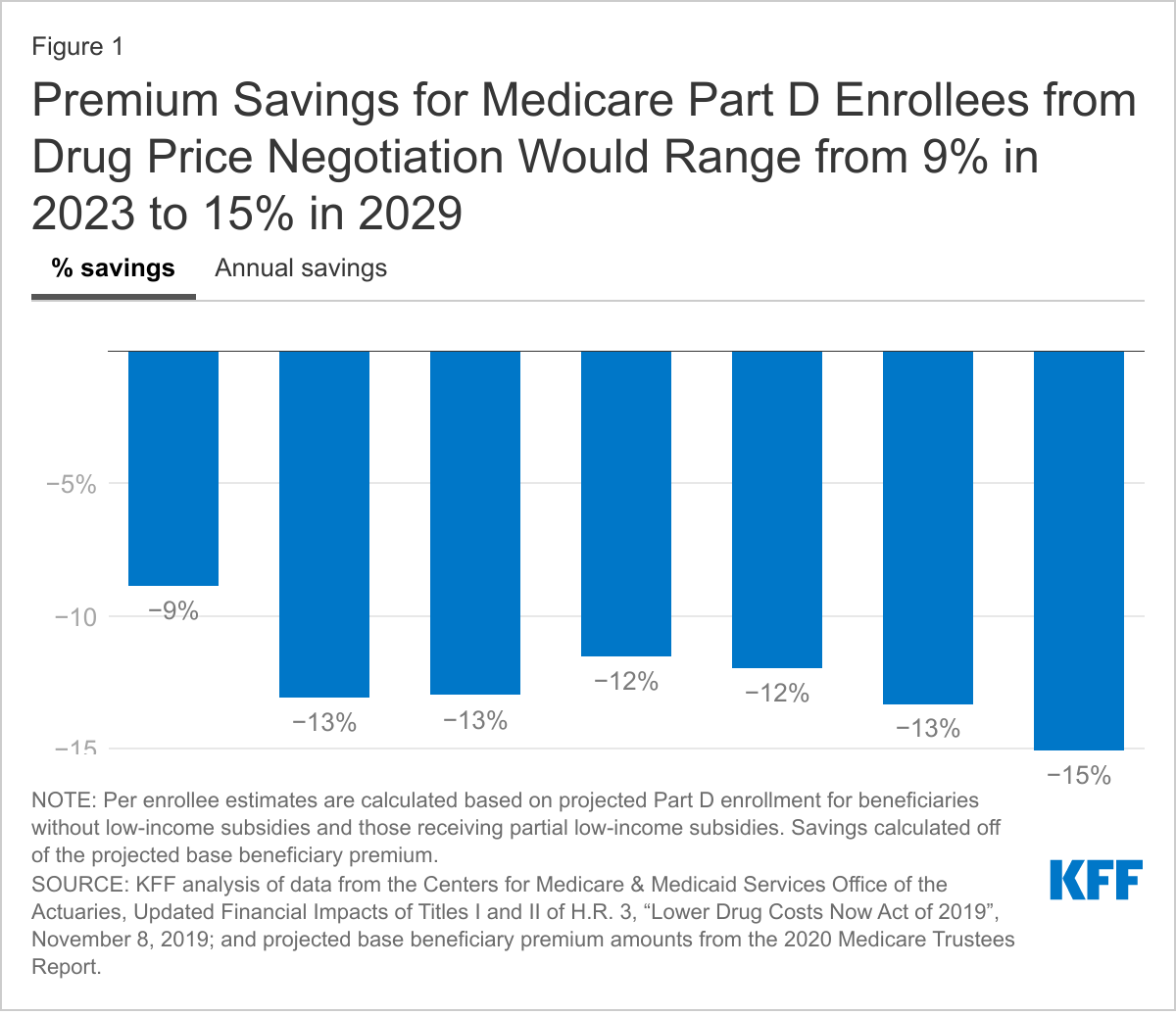
Under drug price negotiation, premium savings for Medicare beneficiaries are projected to increase from an estimated 9% of the Part D base beneficiary premium in 2023 to 15% in 2029. Medicare’s actuaries have estimated that the Part D base beneficiary premium, which covers the cost of basic Part D coverage, will increase from around $440 per year in 2023 to around $560 in 2029. The $14 billion in aggregate Part D premium savings from drug price negotiation over a decade translates into estimated per capita savings for Part D enrollees who pay premiums of $39 annually in 2023, increasing to $85 annually in 2029 (Figure 1). This translates to savings of 9% of the base beneficiary premium in 2023 and 15% in 2029.
These estimates may understate premium savings for Medicare beneficiaries that could be achieved under the current version of H.R. 3, which requires the Secretary to negotiate prices for a larger number of drugs in year 2 than the prior version of H.R. 3 that the actuaries analyzed. In addition, savings could be higher or lower than our estimates depending on the actual base beneficiary premium each year as well as premiums for plans that beneficiaries enroll in, which vary widely each year from the base premium amount. These estimates also do not reflect the interactive effects of other provisions in H.R. 3, such as the Part B and Part D inflation caps or Part D benefit redesign, which would also affect beneficiary premiums and cost sharing.
{kind=link}
This work was supported in part by Arnold Ventures. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.