KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Women have been affected by HIV since the beginning of the epidemic and face unique challenges in accessing optimal prevention, care, and treatment resources.1
In 2022, women accounted for about 1 in 5 (19%) new HIV diagnoses in the U.S.2
Women of color, particularly Black women, have been disproportionately impacted and represent the majority of women living with HIV, as well as the majority of new diagnoses among women.
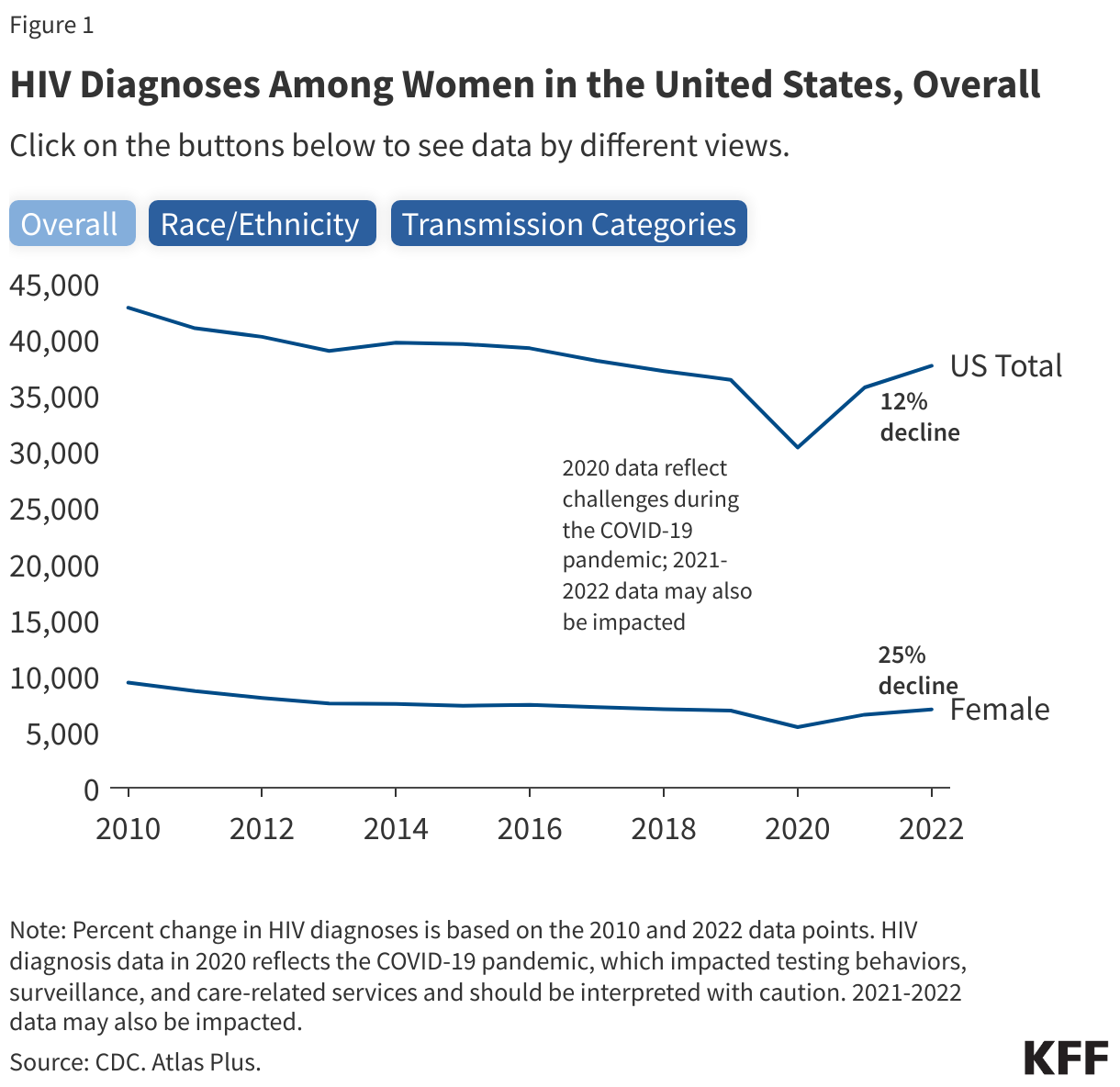
Recent data indicates that HIV diagnoses among women fell 25% between 2010 and 2022, compared to a 12% decline across the population overall. Decreases in HIV diagnoses have occurred for nearly every racial/ethnic group besides White women (Figure 1). However, rates of HIV diagnoses among women of color are much higher.
Overview
Today, there are more than 1.2 million people estimated to be living with HIV in the U.S., including 268,800 (22%) who are women.
Women accounted for 19% of the 6,980 new HIV diagnoses in 2022 and are diagnosed with HIV at slightly older ages than men are.
Between 2010-2022, while HIV diagnoses decreased by 12% among the population overall, the decline was twice as large among women (25%). Decreases in HIV diagnoses have occurred for nearly every racial/ethnic group besides White women (Figure 1). However, rates of HIV diagnoses among women of color are much higher.
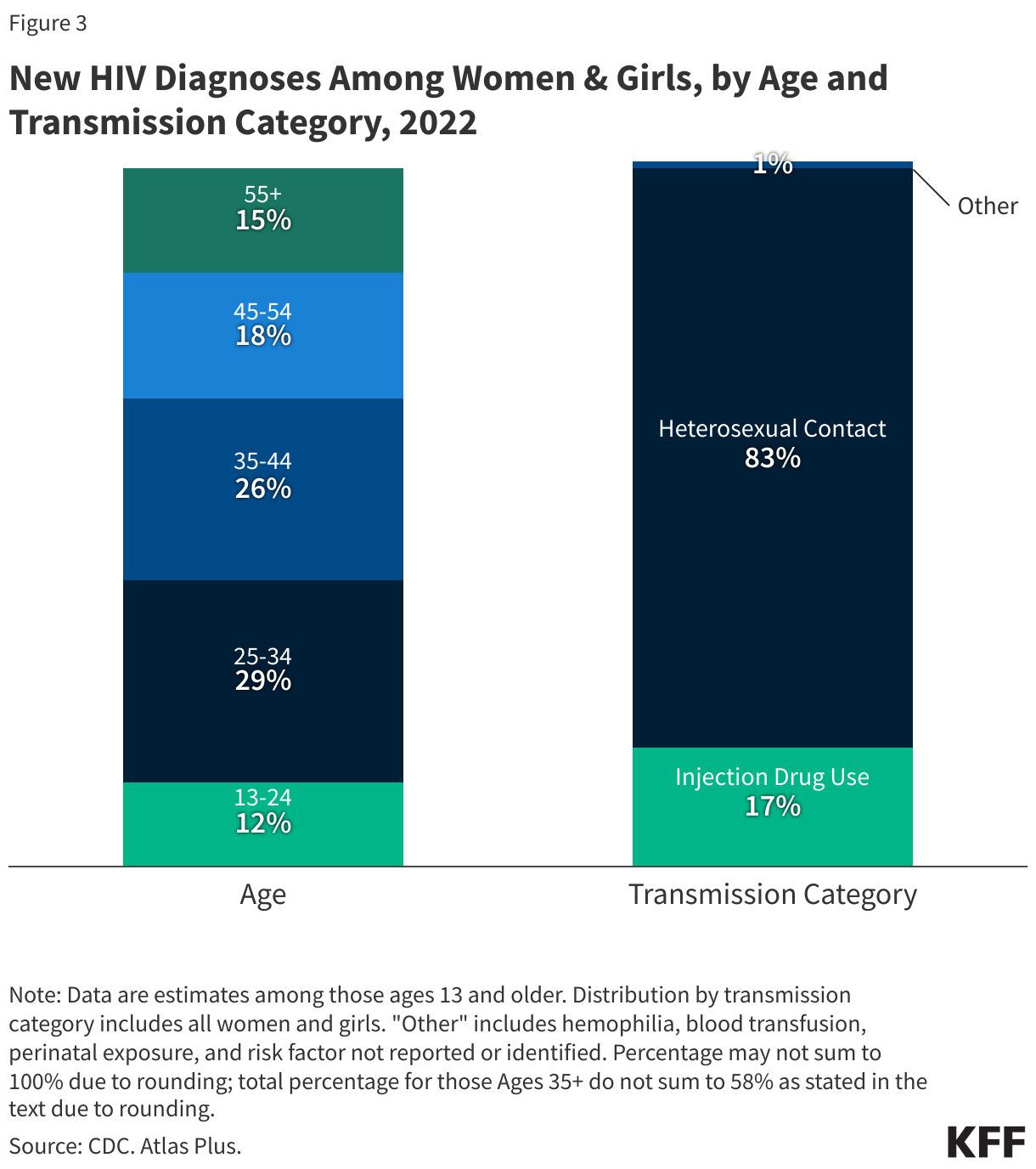
Of new HIV diagnoses among women in 2022, 83% were attributable to heterosexual sex, 17% were attributable to injection drug use, and 1% were attributed to other causes.
Women with and at risk for HIV face several challenges to getting the services and information they need, including socio-economic and structural barriers such as poverty, cultural inequities, and intimate partner violence (IPV).
Race/Ethnicity
Women of color, particularly Black women, are disproportionately affected by HIV, accounting for the majority of new HIV diagnoses, the majority of women living with HIV, and highest rates of HIV-related deaths among women with HIV in the U.S.
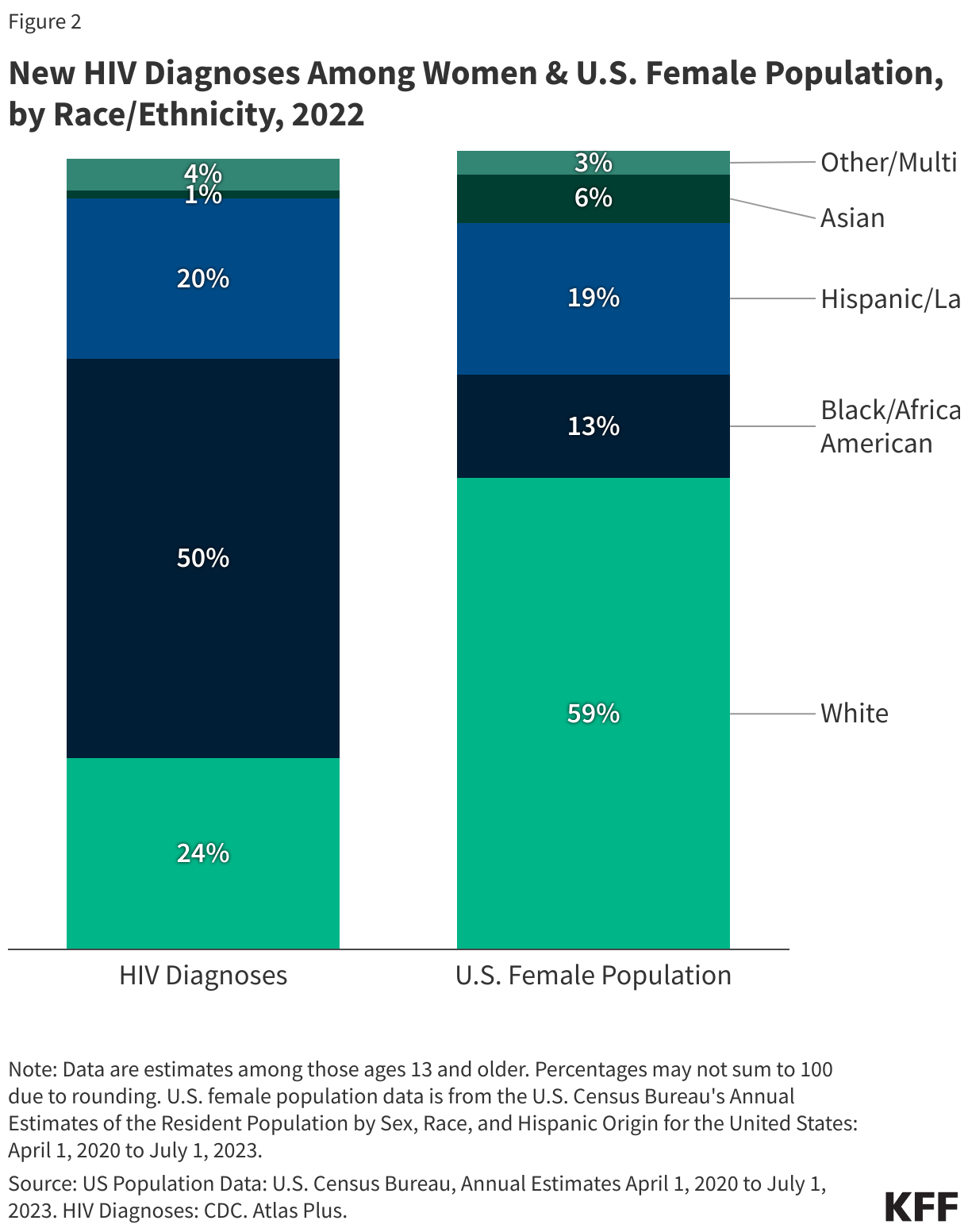
In 2022, Black women accounted for half (50%) of HIV diagnoses among women, while only accounting for 13% of the U.S. female population. White women accounted for 24% and Hispanic/Latina women accounted for 20% of HIV diagnoses among women (Figure 2).
HIV diagnoses decreased 58% among Multiracial women, 39% among Black women, 9% among Hispanic/Latina women, and 3% among Asian women between 2010 and 2022. In this same timeframe, HIV diagnoses increased 21% among White women.
Rates of new HIV diagnoses are much higher for Black, Multiracial, and Hispanic/Latina women than for White women. In 2022, the rate of new HIV diagnoses for Black women was 10 times higher than the rate for White women (19.2 per 100,000 compared to 1.9); the rate for Multiracial women (8.2) was 4 times higher; the rates for Hispanic/Latina women (5.5) and American Indian/Alaska Native women (5.5) were nearly 3 times higher; the rate for Native Hawaiian/Other Pacific Islander women (4.6) was more than 2 times higher. The rate of new HIV diagnoses among Asian women (1.1) was less than that of White women (1.9).
In 2021, HIV was the 9th leading cause of death for Black women ages 25-34, behind diabetes. Black women accounted for the greatest share of deaths (of any cause) among women with diagnosed HIV in 2022 (57%), followed by White women (20%), and Hispanic/Latina women (15%).
Age
Women ages 25-34 accounted for the largest share (29%) of HIV diagnoses among women in 2022, followed by those ages 35-44 (26%). (Figure 2).
Women are diagnosed with HIV at slightly older ages than men are. Women 35 years old and older accounted for 58% of new diagnoses among women in 2022. Comparatively, men in this age group accounted for 41% of diagnoses among men.
Transmission
In 2022, HIV diagnoses among women were mostly attributed to heterosexual sex (83%), followed by injection drug use (17%), and 1% were attributed to other causes. Heterosexual transmission accounts for a greater share of HIV diagnoses among Black and Hispanic/Latina women (90% and 87%, respectively) compared to White women (64%). Among White women, injection drug use accounts for a greater share of diagnoses (36%), relative to Black and Hispanic/Latina women (9%, 12%). (See Figure 3.)
Mother-to-child transmission of HIV in the U.S. has decreased dramatically since its peak in 1991 due to antiretroviral therapy (ART), which significantly reduces the risk of transmission from a woman to her baby (to 1% or less). Still, some perinatal infections occur each year, the majority of which are among Black women, and there continues to be missed opportunities for preventing mother-to-child transmissions, such as testing late in pregnancy. Of the 42 infants born with HIV in 2022, two-thirds (67%) were Black.
Geography
Although HIV diagnoses among women have been reported throughout the country, the impact of the epidemic is not uniformly distributed.
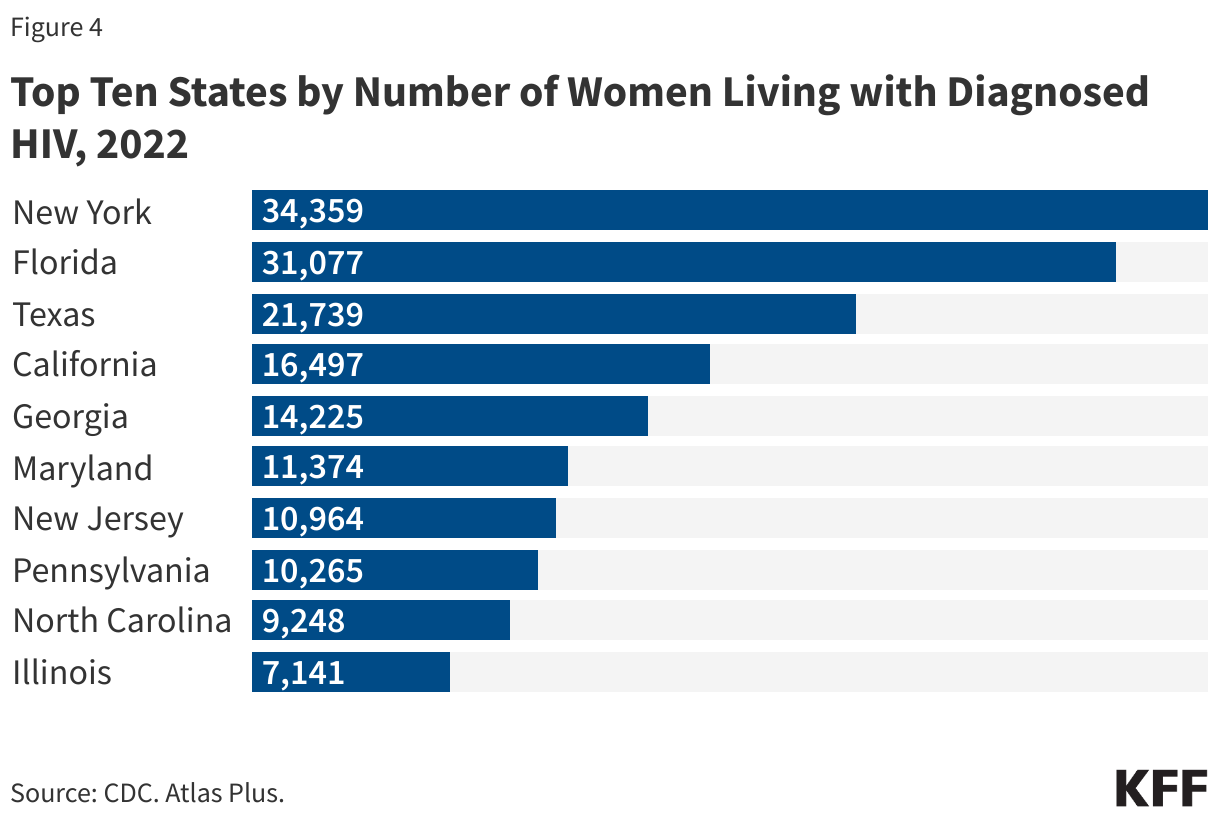
Ten states account for two-thirds of women living with diagnosed HIV (67% in 2022); with 5 states accounting for nearly half (47%) (Figure 4). While the District of Columbia ranked 18th among states in terms of the number of women living with diagnosed HIV (3,629 in 2022), the rate per 100,000 women living with an HIV diagnosis was the highest, nearly 7 times the national rate for women (1,189 per 100,000 compared to 174 per 100,000 nationally), similar to the share in other high populous urban areas.
Thirty-five counties account for almost half (46%) of all women living with an HIV diagnosis in the U.S., with Bronx County, New York having the greatest number (9,454) and highest rate (1,552 per 100,000) of women living with an HIV diagnosis.
Transgender Women
Transgender women are disproportionately affected by HIV and face stigma, discrimination, and exclusion in accessing testing, treatment, and health care, relative to other women.
Since the beginning of the HIV epidemic, national surveillance of and research on the impacts of HIV on transgender women, as well as transgender and gender-diverse people more broadly, has been limited.
Although transgender women account for a small share of people estimated to be living with HIV (1%) among transgender women, 14% are estimated to be living with HIV.
In 2022, transgender women accounted for 87% of 994 new HIV diagnoses among transgender and gender-diverse people. Among transgender women, looking across race/ethnicity, Black transgender women had the highest share of HIV diagnoses (41%), followed by Hispanic/Latina transgender women (39%), whereas White transgender women accounted for 13% of diagnoses. HIV diagnoses among transgender women were mostly attributed to sexual contact (89%).
HIV interacts with women’s reproductive health on many levels, impacting menstruation, reducing fertility, and predisposing pregnant people to greater risk of complications. In addition, antiretroviral therapy may impact contraceptive efficacy. During pregnancy, people with HIV can take additional measures to prevent mother-to-child-transmission of HIV such as adherence to antiretroviral regimens and labor and delivery procedures.
Mothers living with HIV can reduce the risk of transmission to their babies via breastfeeding to less than 1% through antiretroviral therapy.
Women with other sexually transmitted infections (STIs) are at increased risk for contracting HIV. Women with HIV are at increased risk for developing or contracting a range of conditions, including human papillomavirus (HPV), which can lead to cervical cancer, and severe pelvic inflammatory disease.
Sexual and reproductive health clinics provide an important entry point for reaching women at risk for and living with HIV. Nearly two-thirds (63%) of women receiving care at sexual and reproductive health clinics report it as their usual source of medical care.
Research efforts are exploring a number of new HIV prevention technologies which could be particularly beneficial for women, such as cervical barriers and microbicides. The long-acting injectable lenacapavir has also been shown to be highly effective in preventing HIV among women but is not yet approved in the U.S. Once approved, this will be an important addition to the prevention toolkit for women, particularly given its relatively low burden of twice annual injections.
Intimate Partner Violence (IPV) and HIV
Women living with HIV are disproportionately affected by intimate partner violence (IPV), including physical, sexual, and emotional abuse compared to the general population. Intimate partner violence (IPV), sometimes referred to as domestic violence, has been shown to be associated with increased risk for HIV among women, as well as poorer treatment outcomes for those who are already positive.
In the U.S., 35% of women living with HIV experienced physical (i.e. non-sexual) IPV in their lifetime, compared to 24% of men living with HIV.
In many cases, the factors that put women at risk for HIV are similar to those that make them vulnerable to experiencing trauma or IPV: women in violent relationships are at a greater risk for contracting STIs, including HIV, than women in non-violent relationships, and women who experience IPV are more likely to report risk factors for HIV. These experiences are interrelated and can become a cycle of violence, HIV risk, and HIV acquisition.
Women may also be at increased risk of experiencing violence upon disclosure of their HIV status to partners.
HIV Prevention
The CDC recommends routine HIV screening for all adults, including women, ages 13-64, in health care settings, as well as repeat screening at least annually for those at high risk. The CDC also separately recommends that all pregnant women be screened for HIV, and that those at high-risk for HIV have repeat HIV screening in the third trimester. Testing of newborns is also recommended if the mother’s HIV status is unknown.
Additionally, the United States Preventive Services Task Force (USPSTF) recommends HIV testing (including specifically for pregnant women), IPV screening, many STI screenings, and pre-exposure prophylaxis (PrEP) which means that most insurers are required to cover these services without cost-sharing.
Despite these recommendations, only 37% of women in the U.S. ages 18-64 report having been tested for HIV at some point. Black women are much more likely to report having been tested in the past year compared to White women (21% compared to 6%).
PrEP is a safe and highly effectivepreventive medication that reduces the risk of acquiring HIV through sex by 99%. Women have been underrepresented in PrEP uptake and use and not all forms of PrEP are approved for people assigned female at birth. Recent developments in PrEP research have shown lenacapavir to be highly effective in preventing HIV among cisgender and transgender women.
Access to Care & Treatment
As is the case for all people, there are several sources of care and treatment for women living with and at risk for HIV in the U.S., including government programs such as Medicaid, Medicare, and the Ryan White Program for those who are eligible.
Looking across the care continuum, women see progress but continue to face challenges related to diagnosis, linkage to care, and viral suppression. At the end of 2022, among all women living with HIV, 90% were diagnosed, 48% were retained in care, and 57% were virally suppressed, similar to the shares among men.
Among women with HIV, 21% were diagnosed late – that is, were diagnosed with AIDS within 3 months of testing positive for HIV, the same share as among men. This suggests that one in five women are not adequately being served by HIV testing services and are not getting into care within ideal timeframes.
Unless otherwise noted, the term “women” in this factsheet refers to sex assigned at birth. ↩︎
Unless otherwise noted, HIV data come from KFF analysis of the Centers for Disease Control and Prevention (CDC) data in the CDC’s National Center for HIV, Viral Hepatitis, STD, and Tuberculosis Prevention tool: Atlas Plus. https://www.cdc.gov/nchhstp/about/atlasplus.html↩︎