Delivering HIV Care and Prevention in the COVID Era: A National Survey of Ryan White Providers
Key Findings
The COVID-19 pandemic has posed significant challenges for health systems and access to care in the United States, including for people with HIV and the systems that serve them. To better understand pandemic’s impact on HIV, we surveyed the nation’s directly funded Ryan White providers. Ryan White, the federal HIV safety net program, serves over half of those in the country diagnosed with the disease, providing outpatient HIV care and support services. Our key findings are as follows:
- Respondents described an immediate pivot to new ways of providing HIV care and prevention during the early months of the pandemic.
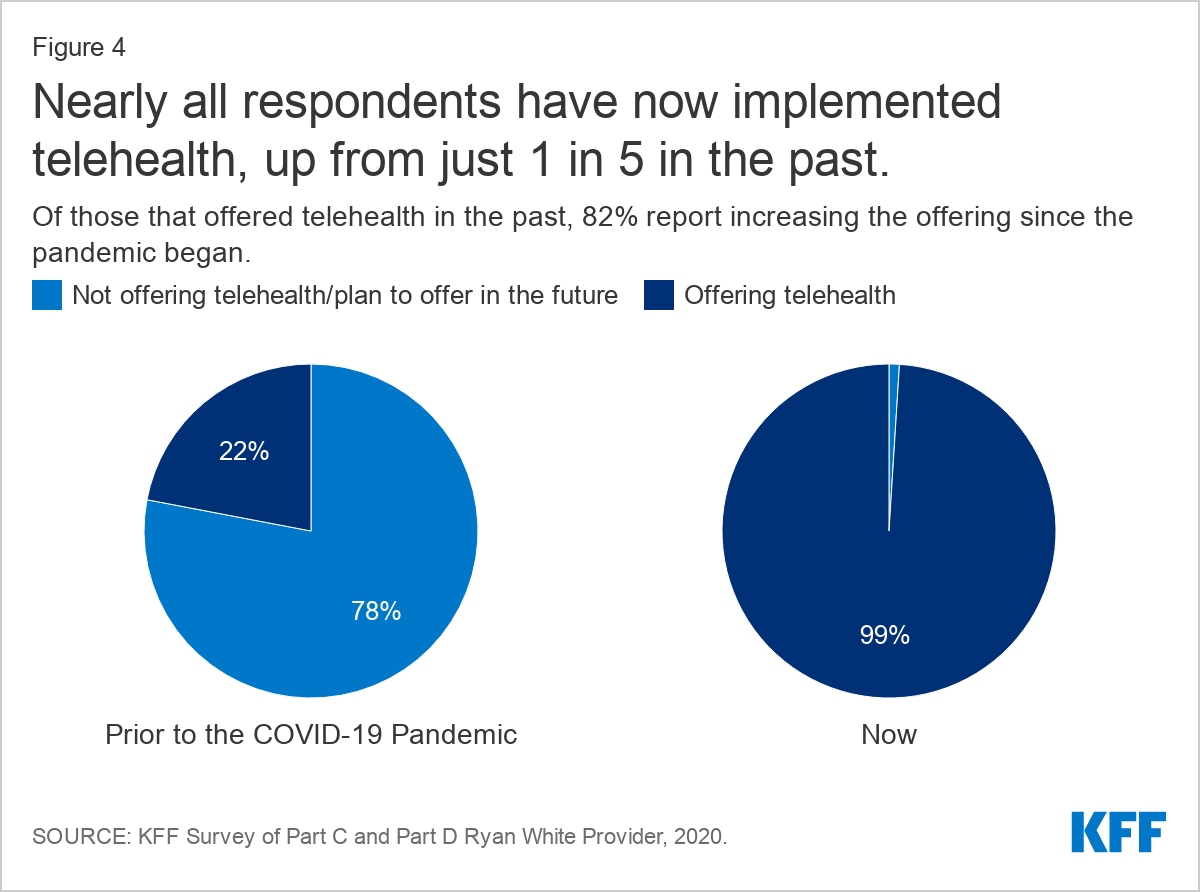
- Nearly all are now offering telehealth services (99%), up from 22% in the past, and are conducting about half of patient visits virtually, on average. However, the “digital divide” means telehealth services are not an option for all patients.
- Most (89%) are offering multi-month prescriptions for antiretrovirals (ARVs), and half reported that this practice has increased due to COVID-19.
- Seven in ten (70%) are conducting onsite COVID-19 testing.
- Nearly one-third (30%) reported an increase in new clients and nearly 40% of respondents saw a change in payer mix, primarily an increase in clients who were uninsured, followed by private coverage losses, and then increases in clients with Medicaid.
- Respondents report that clients face significant stress and uncertainty amidst the pandemic, noting declines in mental health, job loss, and decreased access to support services, among other challenges.
- Respondents also experienced significant challenges related to staffing. More than one-quarter (27%) reported staff layoffs or furloughs and the same share reduced staff hours. Moreover, staff morale was a challenge reported by three-quarters (74%) of respondents.
- Operating challenges were common, including for the 28% who shut down all or most of their HIV prevention services in response to the pandemic. Other challenges included difficulty connecting with service partners and increased costs.
- Following COVID-era public health guidelines remains a challenge for some who experience inadequate clinical space for social distancing (32%), insufficient access to COVID-19 testing (22%)and insufficient PPE (10%).
- However, despite these historic challenges, respondents largely report adjusting to a “new normal” and significant resiliency in adapting to new ways of providing care.
Issue Brief
Introduction
The COVID-19 pandemic has posed significant challenges for health systems and access to care in the United States, including for people with HIV and the systems that serve them. While it does not appear that people with well controlled HIV are at greater risk for more severe complications associated with COVID-19, 4 in 10 people with HIV in the U.S. do not have sustained viral suppression and CDC suggests that those with a low CD4 count or not on antiretroviral treatment could be at higher risk. In addition, many of the individuals invested in the nation’s HIV response – especially those with an expertise in infectious disease – have shifted at least some of their attention away from HIV to focus on the pandemic.
To better understand how COVID-19 has affected the HIV service delivery environment and people with HIV, we surveyed the nation’s Ryan White-funded providers. The Ryan White HIV/AIDS Program is the largest federal program designed specifically for people with HIV in the U.S., serving over half of those in the country diagnosed with the disease. It provides outpatient care and support services to individuals and families affected by HIV, functioning as the “payer of last resort” by filling the gaps for those who have no other source of coverage or face coverage limits or cost barriers. Funding is provided to states, cities, and providers throughout the country. In addition, recognizing the new stresses the pandemic might mean for Ryan White and people with HIV, Congress appropriated $90 million in emergency supplemental funding for the program through the CARES Act.
Methods
Between August 18, 2020 and September 4, 2020 we surveyed directly funded Ryan White HIV/AIDS Program medical provider grantees (i.e. those funded through Part C or Part D). We identified all Part C and Part D grantees funded in FY2020 using publicly available grantee data. In total we identified 390 unduplicated grantees. The named contact for each grantee organization was sent a confidential survey using Survey Monkey containing closed and open-ended questions. We received 161 responses and 8 bounce backs, representing a 42% response rate. Raw survey data was downloaded and analyzed using Excel. Open-ended qualitative responses were analyzed using an inductive framing approach.
While all respondents received Ryan White funding to provide HIV care and treatment, many also received funding from other sources, including to conduct HIV prevention activities. Survey questions and responses are not limited to activities carried out using Ryan White funding.
Respondent Characteristics
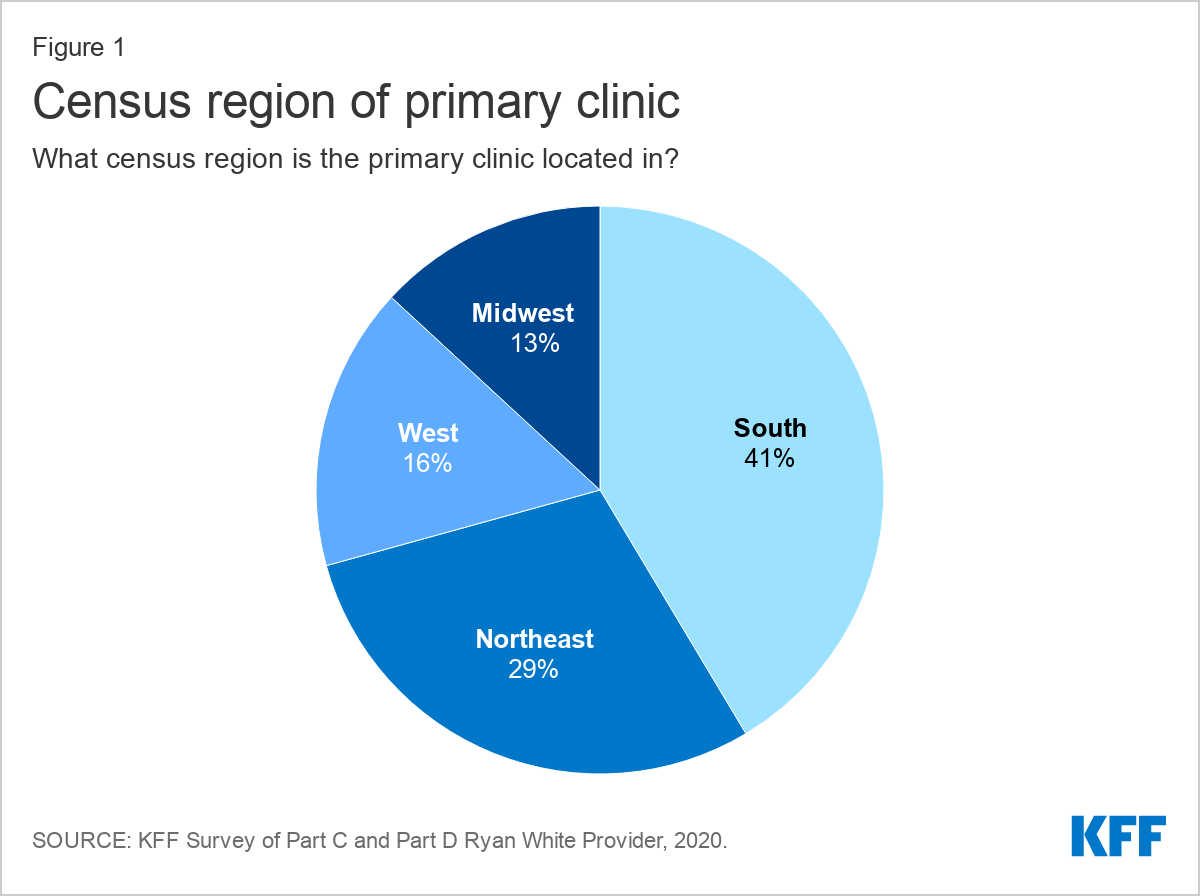
Respondent organizations were located in 38 states, Washington, D.C., and Puerto Rico. A plurality of respondents (41%) were based in the Southern U.S, followed by the Northeast (29%), the West (16%), and the Midwest (13%).
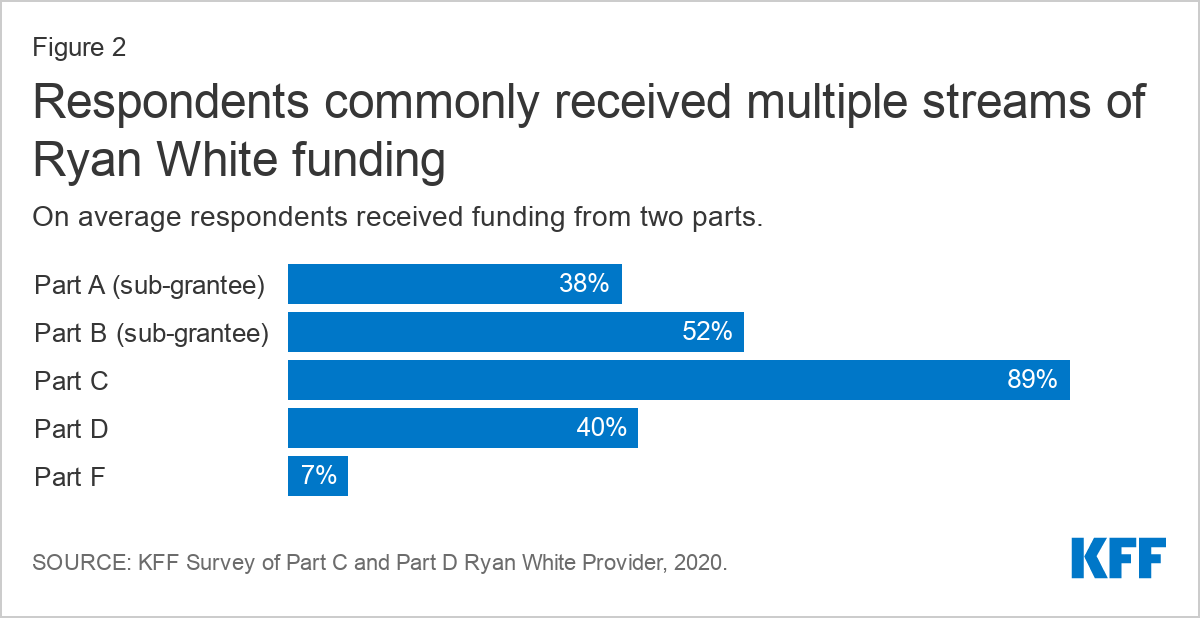
Respondents reported receiving funding from a range of Ryan White Program parts, with many reporting funding from multiple streams (two on average). The most common funding stream was from Part C (89%, funding for community-based organizations providing outpatient HIV health and support services), followed by Part B as a sub grantee (52%, funding directed to states). Forty percent (40%) were Part D grantees (funding for community based ambulatory programs focusing on family-centered care and support services for women, infants, children, and youth with HIV). Smaller shares received funding from Part A as a sub-grantee (38%, funding directed to hard hit urban areas) and Part F (7%, funding for dental care).
Findings
Changes to Services
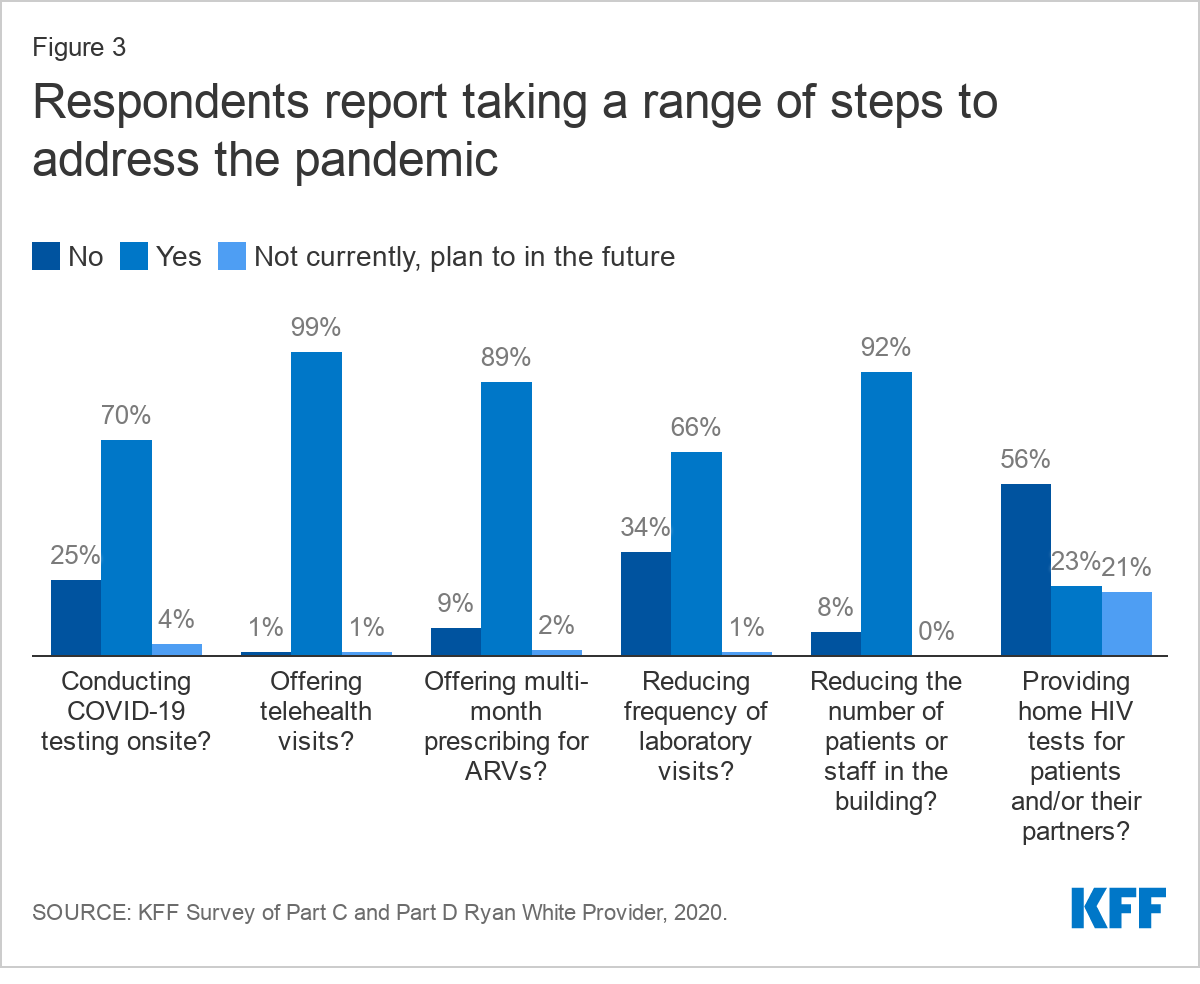
Providers reported significant program changes made in response to the COVID-19 pandemic and described an immediate pivot to new ways of providing HIV care and prevention. Nearly all reported offering telehealth services (99%) and reducing the number of staff or patients in the building at one time (92%). Most reported offering multi-month prescriptions for antiretrovirals (ARVs) (89%), conducting onsite COVID-19 testing (70%), and reducing frequency of laboratory visits (66%). Over half (56%) reported providing clients with home HIV tests, with an additional 21% planning to offer home HIV tests in the future. Respondents described tinkering with new offerings and service closures to find the right balance for their clinic and patient population.
“We have less onsite primary care visits but increased telehealth visits. Decreased support groups onsite, but increased teletherapy with individual clients. We have adjusted with workarounds to keep our clients engaged, frequent wellness checks, and supplied with resources, including COVID supplies.” --Part A, B, C, and D grantee, Midwest
Virtually all providers reported now using telehealth, compared to 22% who did so before COVID-19. Leveraging telehealth was one of the most common COVID-era changes made by providers, with virtually all (99%) saying they offer this service. Of those that did offer telehealth in the past, most (82%) reported expanding telehealth due to COVID-19. Respondents described that this was easier for those who had pre-existing telehealth infrastructure before the pandemic, while some who lacked this prior experience struggled with implementation.
“The transition to Telehealth and use of other virtual platforms that worked effectively and were HIPAA complaint, was a challenge. There were significant delays in even getting the needed equipment due to backorders…” --Part A, B, and C grantee, West
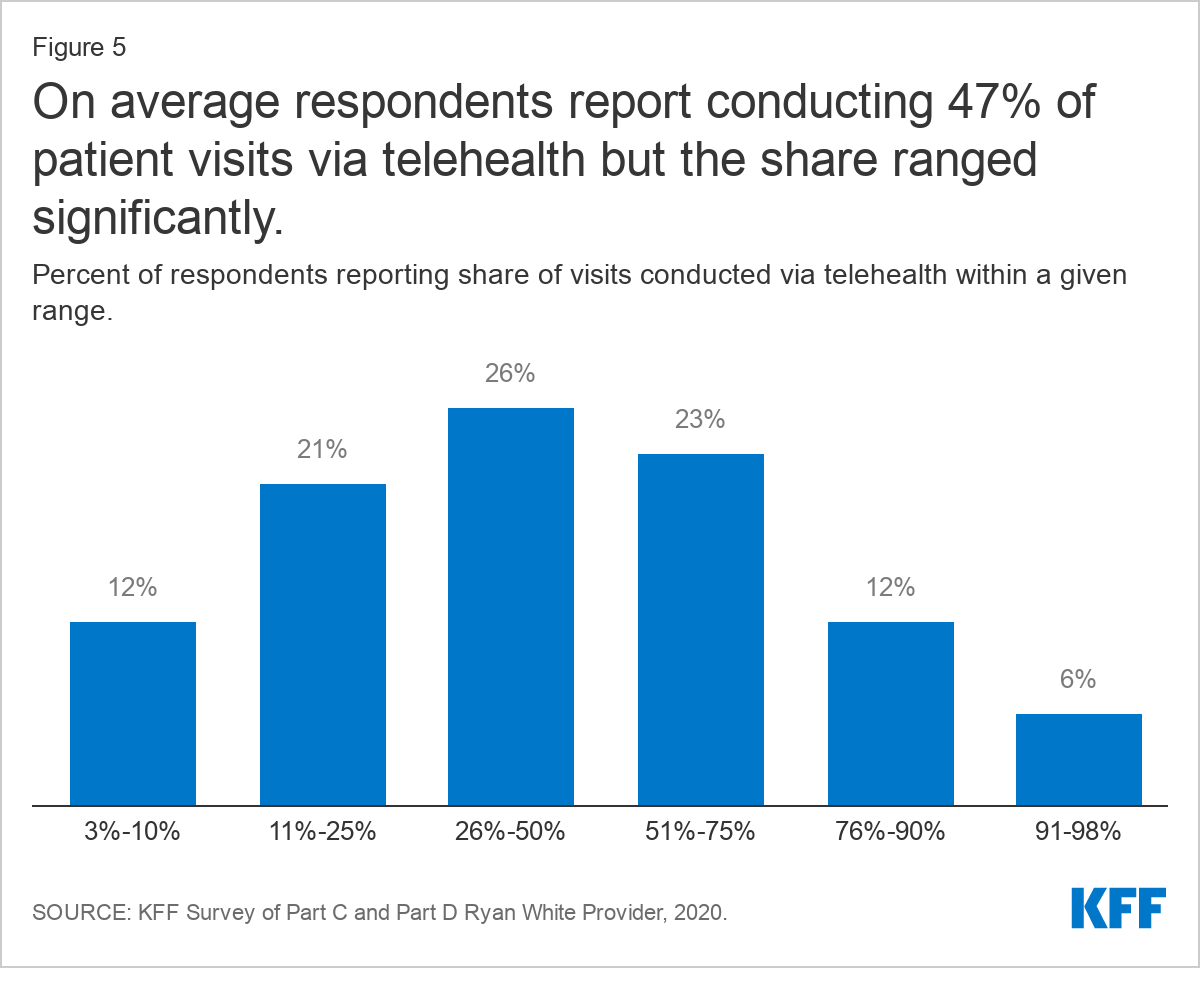
On average, providers now report conducting about half (47%) of patient visits through telehealth (including via video and phone) but that share varied significantly. Forty-one percent (41%) of respondents report using telehealth more than 50% of the time and 6% report using it more than 90% of the time. Six percent (6%) of respondents reported using telehealth more lightly, for less than 10% of visits. In addition to infrastructure challenges, some who reported less frequent use of telehealth were limited by institutional policy. As one provider said, “our larger health care system has been unable (because of security issues) to let us do video visits, only telephone. I believe video would greatly improve these interactions.”
Respondents generally expressed that integrating telehealth services more widely into their practices was an important step forward, not just in providing care during the pandemic, but that they would retain the practice in the long term. Many explained that they were able to connect with historically hard to reach populations and others said they were able to stretch scarce provider time further. Some stated that retention in care had improved and “no shows” declined as a result. They described learning how to make telehealth work best for their patients and saw it as a critical tool for maintaining care during the pandemic.
"I think that telemedicine has been an invaluable tool that has enabled us to stay in contact with patients during this uncertain time and while it is efficient and convenient, we still need to work doubly hard to connect and relate to our patients. We need to project through our screens the compassion and concern we have for them, to continually reassure them, and ensure that they continue to receive quality care regardless of how it is delivered. Patients have been responsive to telehealth as evidenced by show rates over the past 4+ months which is a good indicator that retention in care and viral suppression can be maintained and/or improved." --Part B, C, and D grantee, South
However, many also discussed the “digital divide, noting telehealth only worked well for certain patient populations, with respondents largely agreeing on who was best and worst served (see Table 1).
“Telehealth is working for our practice. We do face barriers with connection problems, and older patients that are not technically knowledgeable…We also have patients that are not on unlimited plans. Telehealth has helped our bottom line. We are able to reach some patients, younger group, that otherwise are not easy to reach.” --Part C grantee, South
| Table 1: Respondents Generally Agreed on Which Groups Most Benefited from/Struggled with Telehealth | |
| Most Benefited | Most Struggled |
| Younger populations/tech savvy individuals | Older populations/less tech savvy individuals |
| Those in rural areas with limited transportation (with tech access) | Those without internet/computer/smartphone access, those with limited phone data, including those in rural areas without broadband & cell infrastructure |
| Those with childcare responsibilities | Unstably housed individuals |
| Medically uncomplicated and stable individuals | Medically complex and vulnerable individuals |
| Some historically harder to reach patients | Those who lack privacy to make calls |
| Those penalized for taking time off at work | Those in need of translation services |
| Established patients | New patients |
Some reported taking steps to address technology gaps, including offering technical support, and by providing clients with phones, phone cards, data plans, internet access, and mobile hotspots. In addition, some described offering telehealth or technology training for staff and patients, sometimes focusing on a specific population, such as seniors. In many cases, respondents used supplemental Ryan White Funding provided through the CARES Act (see Box 1) to cover these costs.
Box 1: Respondent’s Reported Use of CARES Act Funding
Areas bolded denote the most common responses, mentioned by multiple respondents. (Alphabetical Order)
COVID-19 best practices consulting, infection control review, COVID-19 educational materials for patients
COVID-19 testing
Emergency financial assistance
Housing/rental assistance, isolation lodging, utilities for clients, clinic rent
Infrastructure changes (e.g. to support telehealth, to provide for social distancing)
Marketing/outreach of HIV care and COVID-19 testing
Medical supplies for clinic and for clients (e.g. BP cuff, thermometer, pulse ox machines)
Medical transportation, new vehicle for patient and meal transport
Nutrition assistance: stocking clinic food pantry, groceries, grocery cards, meal delivery
PPE, sanitation supplies/services, Plexiglas, partitions, and air purifiers
Premium assistance and medications (OTC medications, ARVs)
Staff salaries for existing staff/prevent layoffs and salaries to support new staff: E.g. Home health care providers (medical assistant), case management/medical case management, full and part-time physicians and nurses (including to assist with overflow from infectious diseases physicians occupied by COVID-19 response), telehealth coordinators, medical triage staff for COVID-19 screening, mental/behavioral health and social service support staff, peer advocate, community healthcare workers, COVID-19 nurse staffed to work with HIV positive clients.
Supplies and care packages for clients (in some cases mailed to clients): E.g. masks, sanitizer, coloring books/pens, gas cards, clothing, gift cards for basic supplies (e.g. food, cleaning supplies, personal hygiene products etc.)
Telehealth infrastructure: E.g. tablets, computers, phones, phone cards, phone service/mobile hot spots for clients, licenses (e.g. for Doxy.me and Zoom), webcams, microphones, and computers.
Note: The Coronavirus Aid, Relief, and Economic Security, or CARES, Act was the third major legislative initiative to address the COVID-19 Pandemic. Additional information available here.
Providers noted that while telehealth is well suited for certain types of visits, it is inadequate for others. Generally, providers explained it worked well for routine visits or follow-up care, and prescription drug refills. Some thought it was also working well for behavioral health/social work, though others thought social service visits worked better in person. One stated “Telehealth has been especially important for maintaining mental health services.”
"Telehealth is working well for medical follow up, case management and eligibility appointments for individuals who are stable and virally suppressed..." --Part A, B, and C grantee, West
As time has gone on and it has become clear that there will not be an immediate end to the pandemic, some respondents expressed concern about patients being without in-person visits or laboratory services in the long term. They believed conducting all services via telehealth as a stopgap measure was reasonable at first, but several respondents described now wanting to bring patients back onsite for at least some in person care, for both clinical and reimbursement reasons. Some also worried that reliance on telehealth in the long term could increase patient isolation. Others worried providers “would miss things” by not seeing patients in-person for extend periods of time.
"…While initially medical care visits were easily provided through telehealth, there is more concern amongst providers, as the time drags on. They are concerned about actually having the opportunity to examine patients and also to monitor labs..." --Part B, C, and D grantee, South
"Telehealth is very helpful. No-show rates decreased. Only challenge is to bring in those pts with co-morbidities who have not been seen face-to-face for over 6 months now. Providers want them to come in at least once, then continue telehealth. Pts with comorbidities need to be closely monitored." --Part A and C grantee, Northeast
Just a few respondents had a more pessimistic view of telehealth overall and were unable to get past seeing it as inferior way to practice medicine. They believed that telehealth didn’t allow them to gather critical health information or, in one case, that the technology actually got in the way of the visit.
"Telehealth is good reassurance for patients, but it has not been very helpful in terms of HIV primary care -- we cannot get vital signs and monitor BP, we don't have labs, and we cannot as easily connect pts to in-clinic resources. It feels "better than nothing" but doesn't feel like the highest quality of care…" --Part C grantee, Northeast
While some described being able to leverage telehealth to conduct more visits and generate additional revenue, most described reimbursement challenges. A primary issue hinged on the fact that payers would reimburse for video but not telephonic visits, while many patients preferred or only had technology to support phone calls. One provider noted that they could bill for their time but not collect facility fees with telehealth visits.
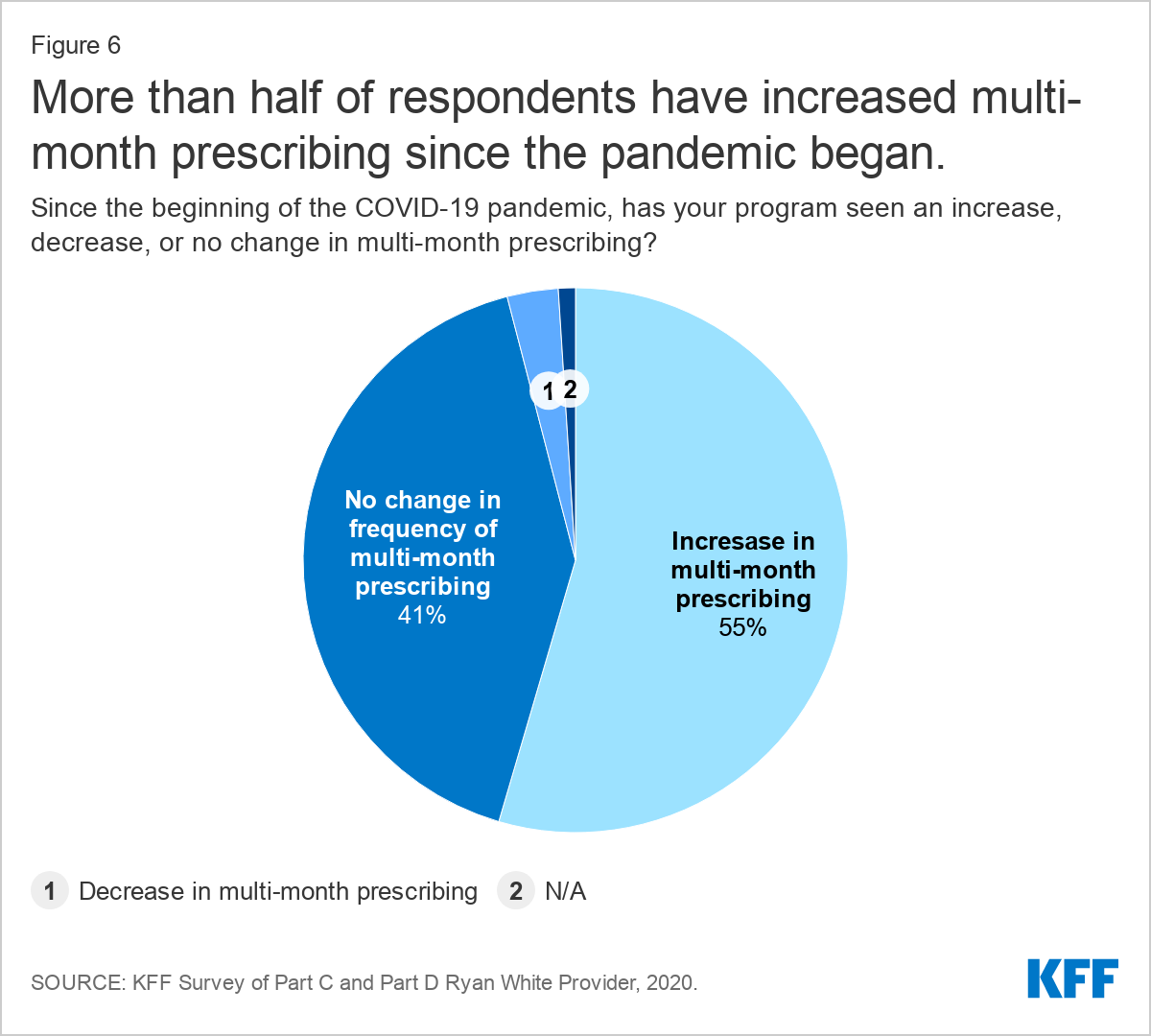
Multi-month dispensing of HIV medications was offered by nine in ten (89%) respondents, with many saying they have increased this practice. More than half (54%) say that the practice has increased since the pandemic began, though a large share (41%) report no change.
In addition to multi-month prescribing, respondents also reported offering new options to facilitate access to medications. Some are now offering home delivery of medications, often by clinic staff such as case workers, and others are more heavily using mail order prescription delivery services.
Changes to Patient Population
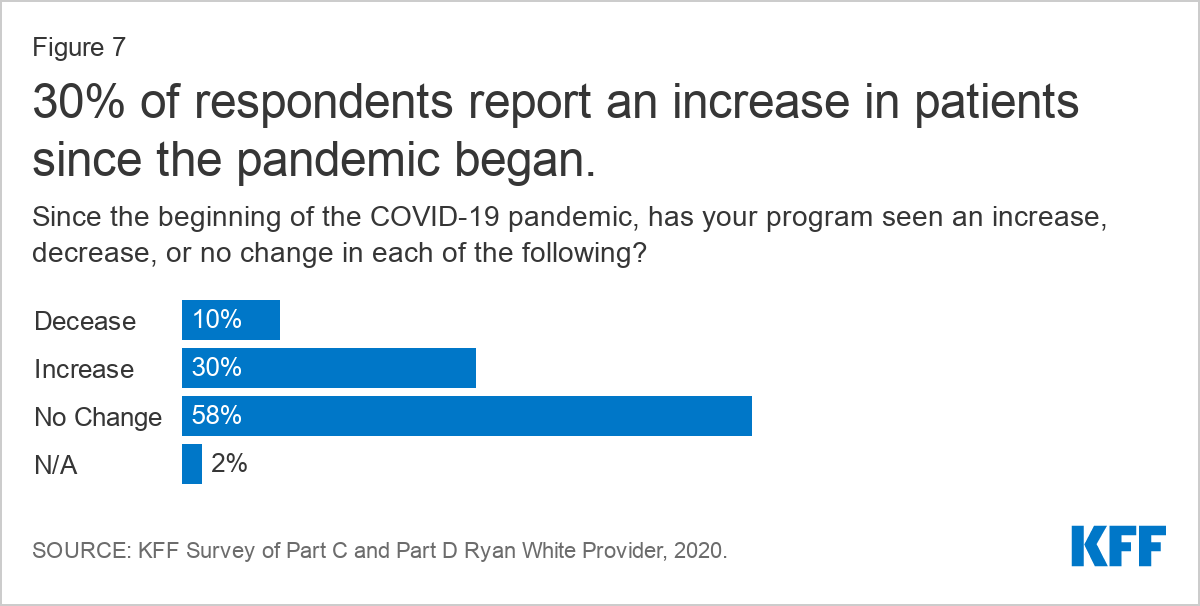
Nearly one-third of respondents (30%) reported an increase in new patients since the pandemic began. Some respondents believed they were seeing more clients because engagement and retention in care was easier for certain individuals through new telehealth offerings, though it may also be due to increasing need and coverage losses.
Two respondents noted that some HIV positive clients who had previously fallen out of care, reengaged with the health system in the wake of the pandemic, fearful of what becoming infected with COVID-19 might mean for them.
"We've seen an increase in patients who had been out of care returning to care over COVID fears…" --Part A and D grantee, South
"…Because we were a COVID testing site early on we did see an increase in patients that had fallen out of their HIV care coming to the COVID testing and asking also about getting back into HIV care, because they were concerned about being vulnerable to COVID." --Part A and C grantee, South
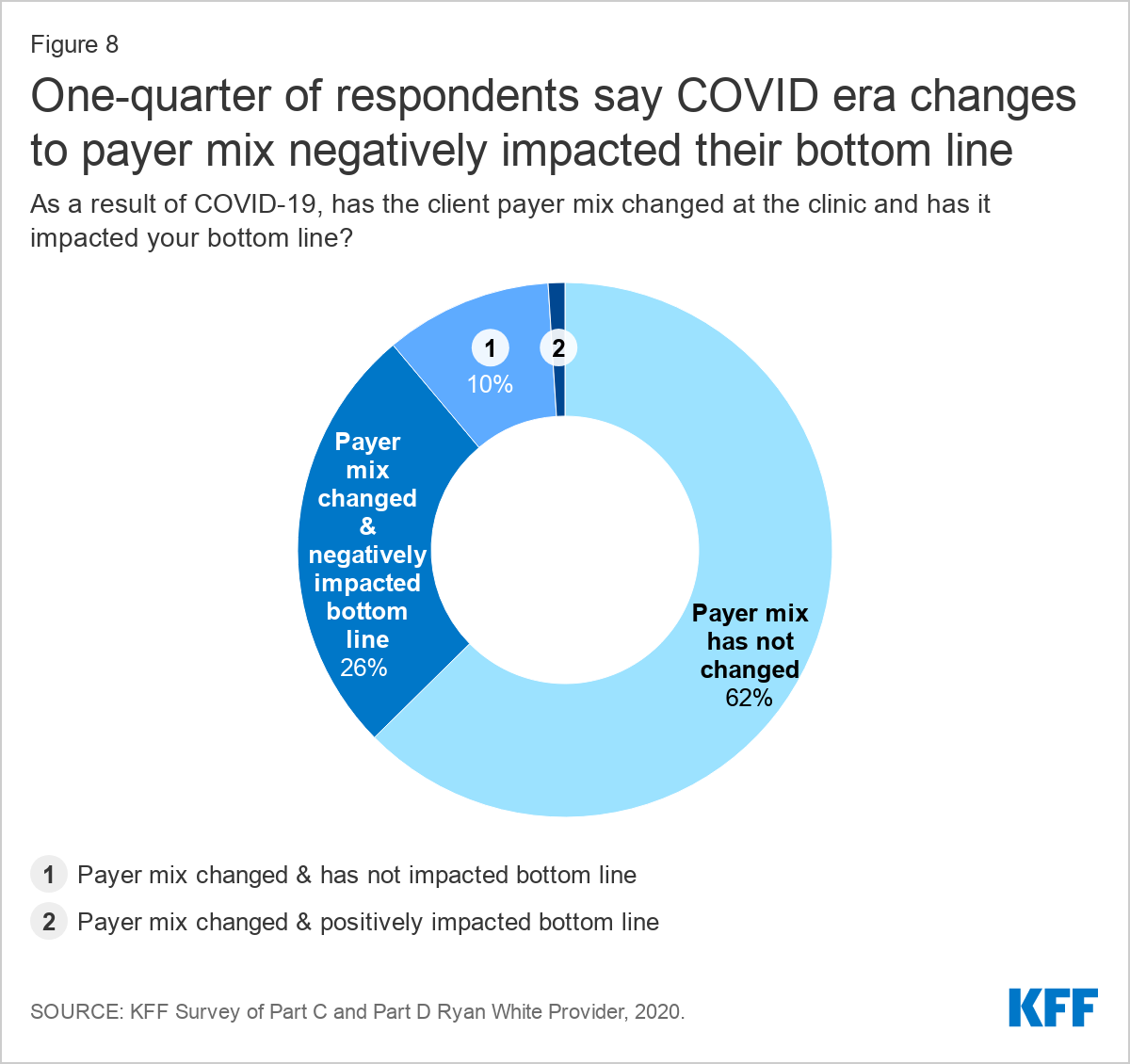
Nearly 40% of respondents reported changes to their payer mix. Respondents were asked whether their clinic saw a change in overall payer mix as a result of the pandemic, that is, have clients gained or lost insurance coverage. Payer mix can impact clinic bottom line and certain care experiences. While most (62%) reported that they have not seen a change in payer mix, nearly 40% have seen a shift, with more than one quarter (26%) saying the change has negatively impacted their bottom line. One in ten said that payer mix has changed, but it has not impacted bottom line. Only 1% of respondents reported a payer mix change with a positive bottom line impact.
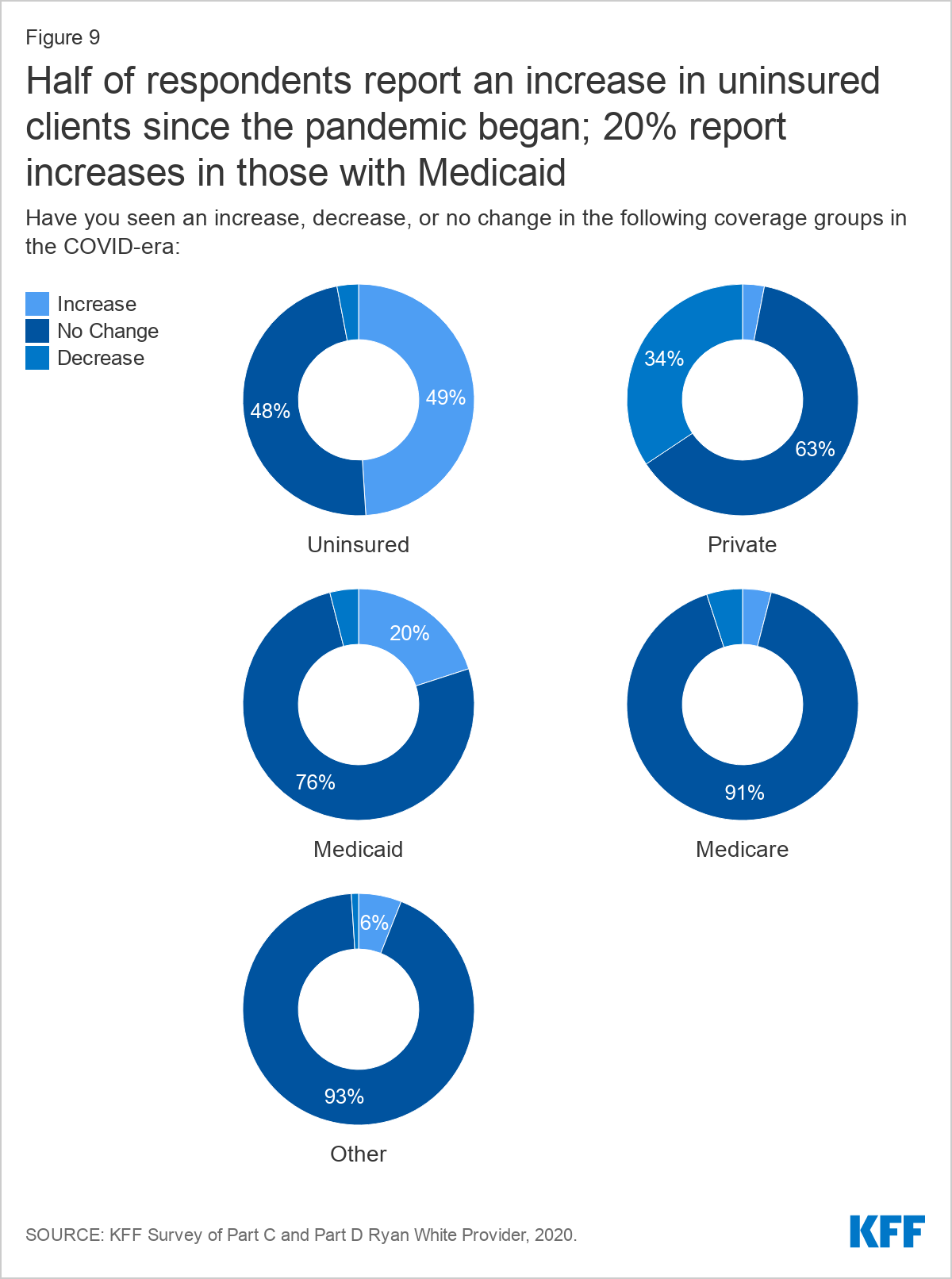
When asked about specific changes experienced under the pandemic, respondents reported even higher rates of coverage changes. About half of respondents (49%) reported an increase in uninsured patients, one-third (34%) reported decreases in clients with private coverage, and 20% reported increases in clients with Medicaid coverage. Fluctuations in Medicare and other coverage were smaller.
There were differences in client coverage changes reported by respondents in Medicaid expansion states compared to those in non-expansion states (or in states that had not yet implemented expansion). While large shares of respondents reported increases in uninsured clients across the board, this was somewhat less common among respondents in Medicaid expansion states compared to those in states that had not expanded their programs (45% v 55%). This could be attributed to increases in Medicaid coverage and less of decline in private coverage among clients in expansion state. Twenty-eight percent (28%) of respondents in expansion states reported increases in clients with Medicaid coverage, while just 9% of those in non-expansion states reported Medicaid increases. Twenty-nine percent (29%) of those in expansion states and 43% of those in non-expansion states reported declines in clients with private coverage.
| Table 2: Share of Respondents Reporting Coverage Changes in The COVID Era, by Medicaid Expansion Status | ||||||||||
| Uninsured | Private | Medicaid | Medicare | Other | ||||||
| Exp. | Non-Exp. | Exp. | Non-Exp. | Exp. | Non-Exp. | Exp. | Non-Exp. | Exp. | Non-Exp. | |
| Increase | 45% | 55% | 2% | 5% | 28% | 9% | 4% | 3% | 7% | 5% |
| Decrease | 3% | 3% | 29% | 43% | 2% | 7% | 3% | 7% | 0% | 3% |
| No Change | 52% | 41% | 69% | 52% | 70% | 84% | 92% | 90% | 93% | 92% |
Impact on Clients
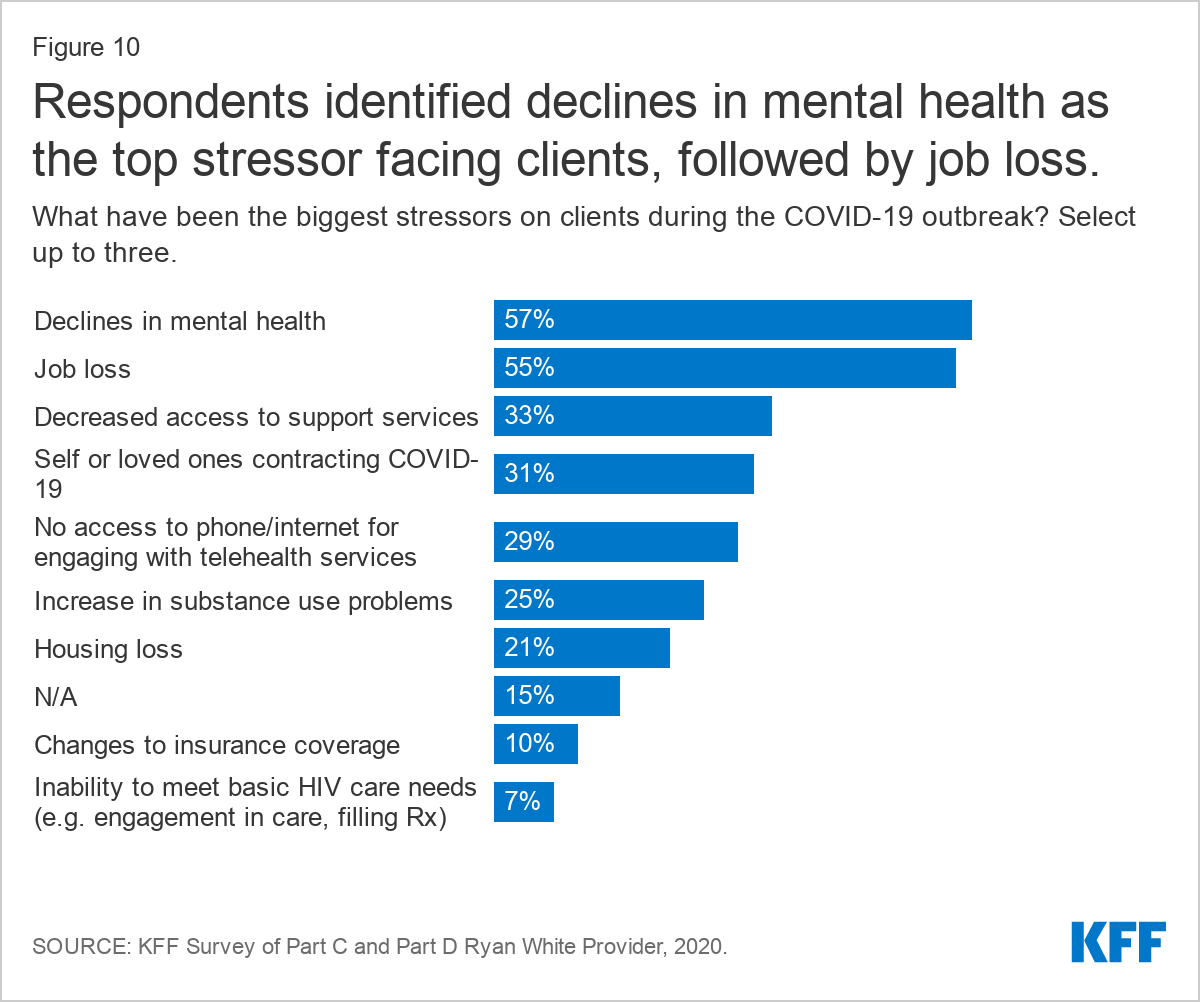
Respondents reported that clients faced significant stress and uncertainty amidst the pandemic and noted that these experiences translated to increased social service needs. Respondents were asked to select the three most significant stressors impacting their clients from a list. The top stressor, identified by 57% of respondents, was declines in client mental health, followed by job loss (55%) and decreased access to support services (33%). Also ranked highly were lack of access to technology to support telehealth encounters (29%) and increases in substance use problems (25%). Housing loss was a top stressor identified by one in five respondents (21%). Smaller shares pointed to insurance loss (10%) and inability to meet HIV care needs (7%). Those who selected “other” (15%) most commonly expanded their answer to identify fear, isolation, and stress related to the pandemic as the biggest challenges facing their clients, including for those working in high risk settings. Other stressors for patients included food insecurity and inability to safely use transportation. Some were also concerned about patients who were afraid to return to care due to possible COVID exposure, including those who are immunocompromised.
"For many of our HIV+ patients, engaging with staff and medical providers is the only actual in person engagement that they have. In the era of COVID, many clients have expressed increased feeling of isolation, anxiety and/or depression."--Part A, B and C grantee, West
"A number of our patients work (as nutrition aides and CNAs) in local nursing homes heavily impacted by the pandemic. Others work at grocery stores, restaurants and in other "essential worker" roles. The stress of reporting to work in an environment with increased potential for COVID exposure has been a big stressor." --Part B and C grantee, Northeast
"Immunocompromised patients are afraid to come in and be exposed to COVID-19. We have offered COVID testing as part of their appointment and they seem to feel safer knowing people are testing as they come to their appointments."--Part C grantee, West
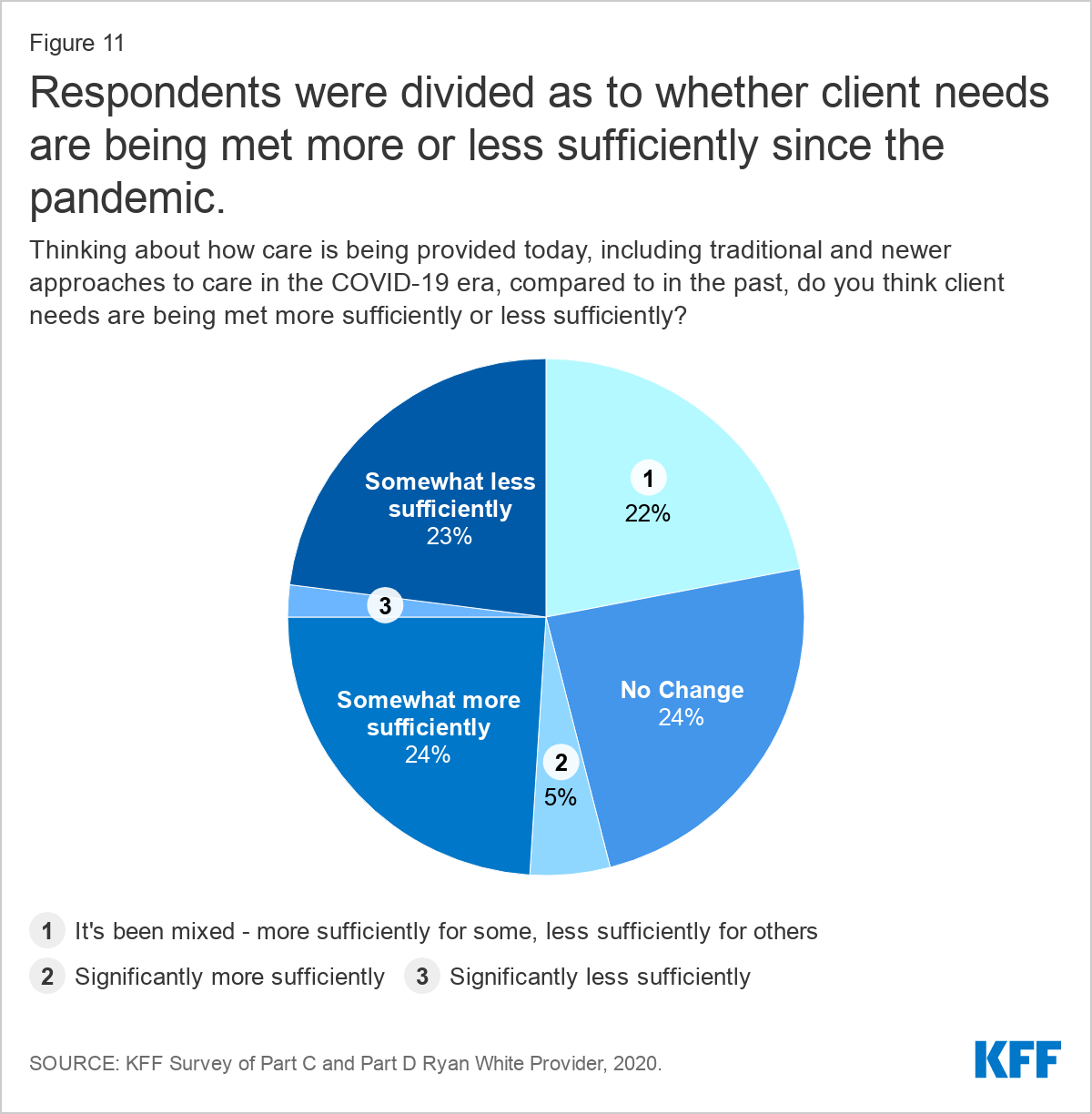
Respondents described that some patients and staff adjusted smoothly to the changes brought on by the COVID-19 pandemic while others had a more challenging time. When asked to consider how well clients’ needs were being met compared to pre-COVID times, nearly equal shares, said that needs were being met somewhat more sufficiently (24%), somewhat less sufficiently (23%), that there had been no change (24%), or that the experience had been mixed ( 22%). In a separate question, respondents elaborated, that those patients better engaged in care in the COVID-era compared to the past were largely individuals who adapted well to telehealth services. Those who most struggled were patients with increased social service needs or those who did not adapt easily to telehealth.
"We transitioned to virtual care for all services during late March/early April, then returned to full on-site services in May…In terms of HIV care, our capacity is similar but patients have higher needs due to the financial and behavioral stresses of the COVID pandemic. In addition, layoffs affecting clinical staff have impacted the clinical workflow." --Part A and C grantee, Northeast
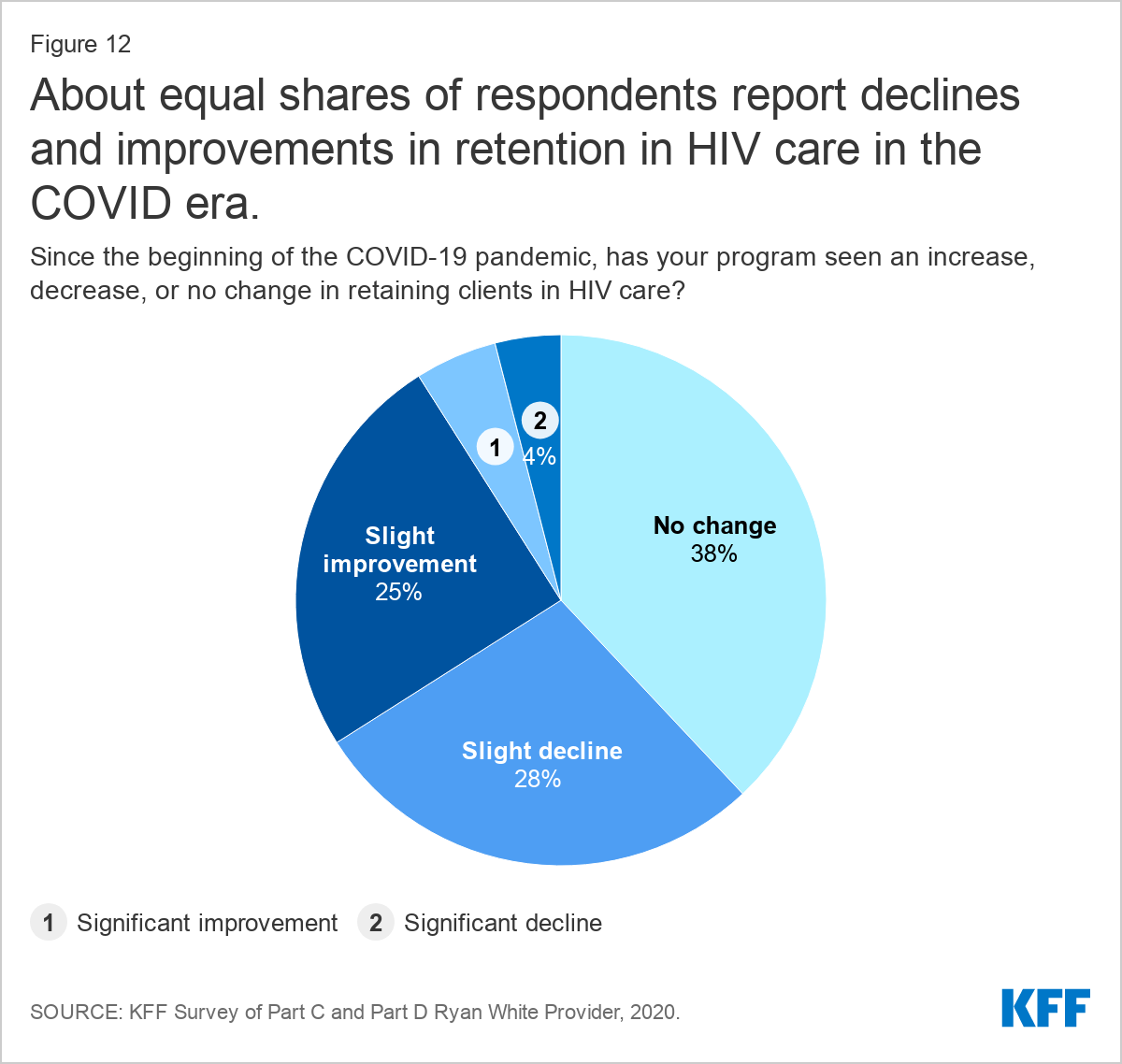
Respondents were similarly split as to how retention in HIV care during the pandemic compared to experiences in the past. A plurality reported no change in retention in care (38%) and similar shares reported a slight improvement (25%) or slight decline (28%). Improvements in retention were sometimes attributed to leveraging telehealth while some attributed drops in retention to more limited access to social support groups and in person services.
Operating Challenges
Despite the steps respondents report taking to maintain care and prevention opportunities during the pandemic, operating challenges were common. For instance, four in ten respondents (41%) reported that they were facing increased operating costs.
Additionally, more than one-quarter (28%) report shutting down all or most of their HIV prevention services at some point in response to the pandemic. Smaller shares shuttered HIV care services at some point during the pandemic (5%). More than one in ten (13%) shut down all or most support services at some point.
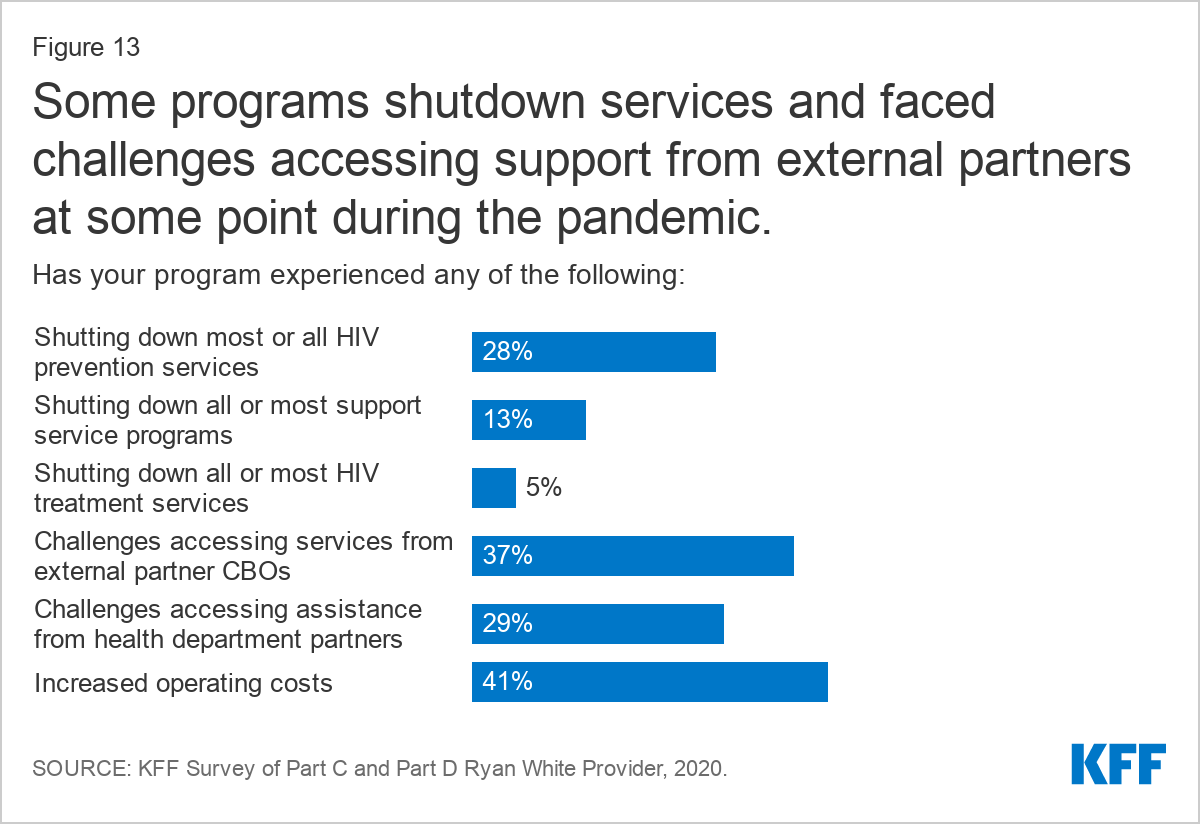
Large shares of respondents also reported difficulty connecting with service partners. Challenges accessing services from community-based organizations were reported by 37% of respondents and 29% reported challenges accessing assistance from health department partners.
While some providers reduced HIV services or ran into barriers with access to partner organizations, others offered creative approaches to continuing these activities, such as opening a testing hotline and outfitting a van for parking lot HIV testing. (See Box 2: Best Practices Identified by Respondents.)
Box 2: Respondent Identified Best Practices in the COVID-era
Telehealth
- Providing training
- Getting staff buy-in
- Getting technology to patients
- Offer drive through appointments to help clients set up their phones for telehealth
Clinical
- Scheduling labs in advance to reduce waiting
- Provision of home HIV (and STI) testing
- Staff delivery of prescription medication (e.g. case managers, patient navigators)
- Imbedding nurse practitioner in call center
- On call weekend coverage for mental health services and medical case management
- Purchased medical van (with CARES Act funding) to bring care to patients
- Increase flexibility of where patients can get labs drawn
- Operating a testing hotline
- Outfitting van for parking lot HIV testing
- Social services
- Extensive case management to maintain contact
- Use of taxi vouchers/Uber/Lyft for appointments
- Use of “psycho-educational” Zoom groups to address social isolation
- Case managers picked up food bank packages and provide contactless delivery to clients
Administrative
- Administrative staff working from home
Other
- Coordination between patient care navigators and local health department linkage to care program to help reconnect unstably housed populations
"We have continued to provide HIV testing at our site but have not been able to go to partner agencies to provide testing. With less testing encounters, our opportunity to educate on PrEP reduced. We quickly implemented telehealth services for medical care and behavioral health." --Part A, B, and C grantee, South
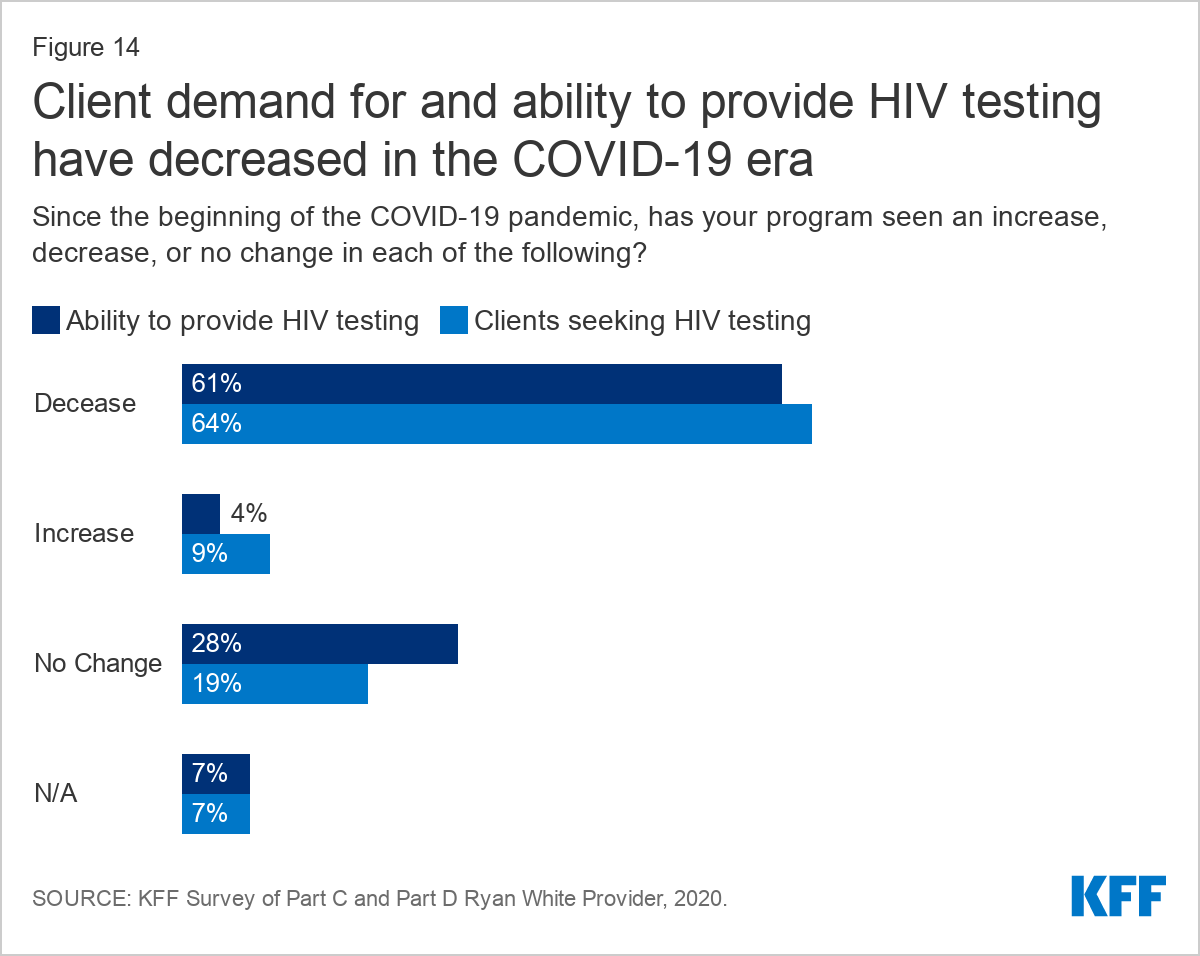
Most respondents (61%) reported a decreased ability to provide HIV testing during the pandemic and a similar share (64%) reported decreased demand. Smaller shares reported increased capacity (4%) and increased demand (9%). Some worried this drop off in HIV testing would lead to a “surge” of potentially late diagnoses later on. Others expressed concern that decreased HIV testing would impact grant deliverables and future funding.
"We saw a decrease in new [HIV] diagnoses and transfers into care…[W]e are concerned about potentially higher #'s of undiagnosed cases or new patients who haven't yet engaged with us due to COVID19 and worry about a 'surge' of diagnoses later in the year with potentially delayed diagnosis." --Part A, B, and C grantee, South
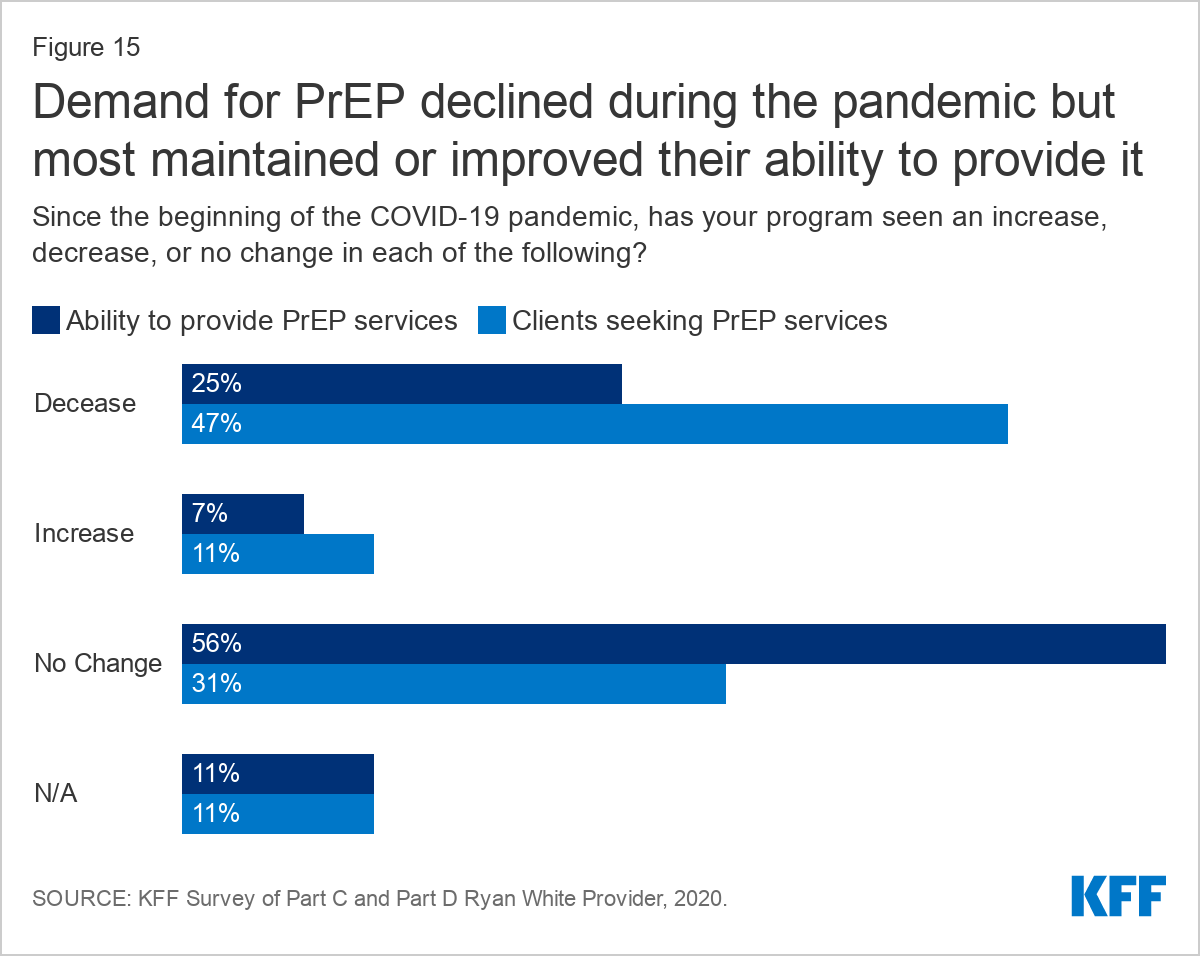
Some respondents (25%) reported a decline in their ability to offer PrEP, as well as declines in clients seeking these services (47%). Most (56%) had seen no change in their ability to offer PrEP and a smaller share saw an increased capacity (7%). One in ten (11%) reported an increase in demand for PrEP services.
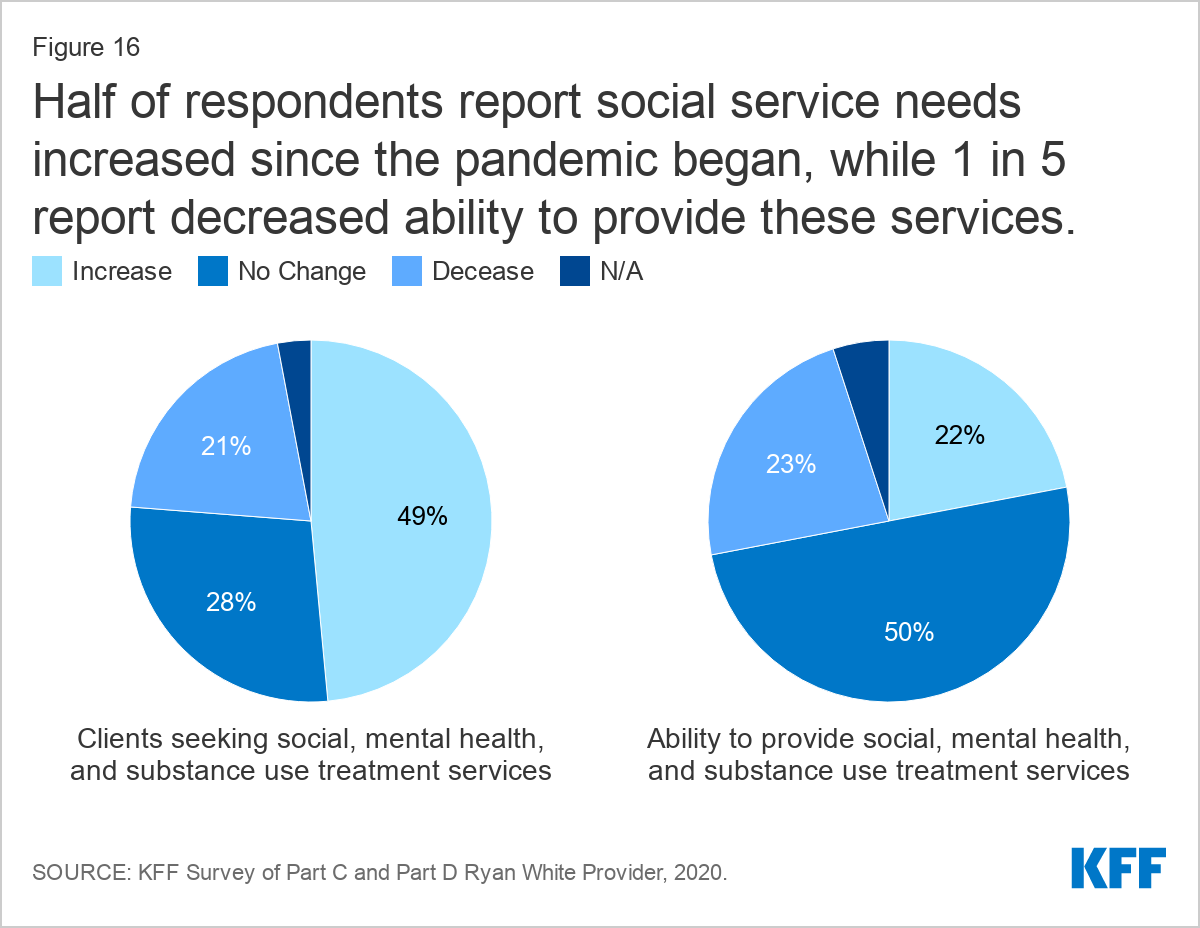
Meeting social service needs was a challenge for some at a time when many saw increased need among clients. Half of respondents (49%) reported increased social, mental health, and substance use service needs during the pandemic. While half retained or increased their ability to provide these support services, nearly one-quarter (23%) reported this capacity had declined.
Staffing challenges were common among respondents. Possibly related to service closures, over one-quarter (27%) of respondents reported staff layoffs or furloughs and the same share reported reducing staff hours. Respondents also described that infection control efforts lead to increased workload, in some cases making meeting grant demands challenging. Likewise, closure of certain activities, such as HIV testing, also presented barriers for meeting grant deliverables for some.
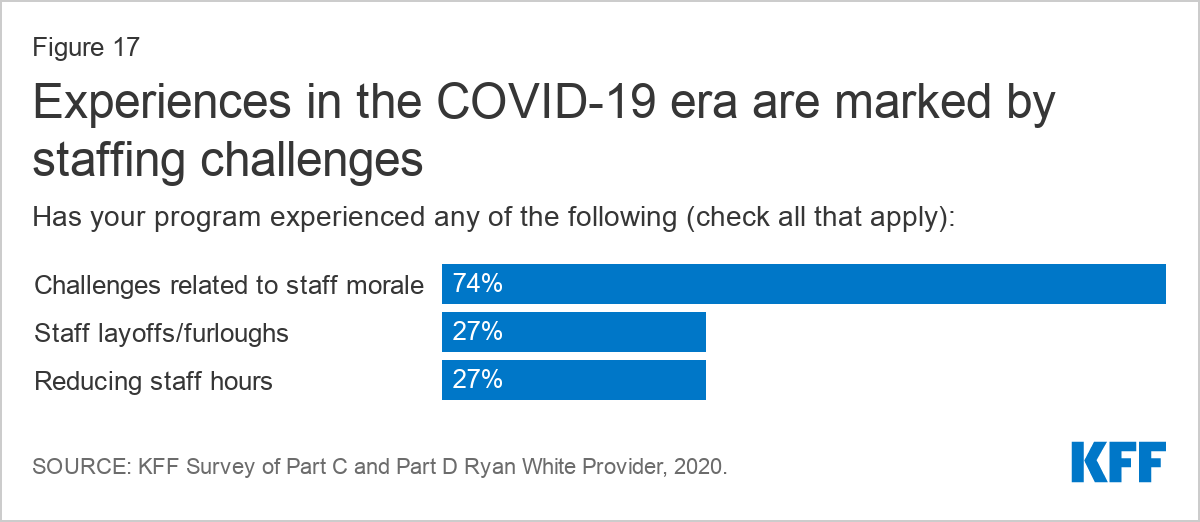
Moreover, staff morale was a challenge reported by three-quarters (74%) of respondents. Respondents described substantial trauma, fear, and strain related to working in healthcare during the COVID-19 pandemic, with one respondent reporting that at least half of their staff had contracted the infection and had significant trauma. Some reported staff had resigned due to fear of COVID-19. In addition to the stress of providing health services during the pandemic, staff also struggled personally as they balanced home and family responsibilities. Many staff faced strain related to increased workload due to staffing limitations, infection control work, and as their peers were diverted to aid with COVID response. Additionally, divisions between staff who were able to work from home and staff required to be on site were reported by some.
"Our organization was hit hard by covid and the refrigerated trailers holding dead bodies were parked outside our clinic. Many staff still struggle with the trauma of working through the pandemic and knowing seeing so many people die. At least half the staff contracted covid and about 1/4 had someone die from covid." --Part C and D grantee, Northeast
"Reduced volume of billable visits with same levels of staffing and increased workload on infection control, PPE, etc. has been a significant financial and morale strain." --Part C grantee, Midwest
"Staff is very stressed out and feeling isolated despite attempts to stay connected with regular zoom calls. Difficult to sustain enthusiasm for projects or services." --Part C and D grantee, West
"COVID has taken a very significant emotional toll on our HIV staff. Many love their jobs because of the support they are able to offer our clients. Having face to face session severely limited has made them feel that their jobs are much less rewarding, which just adds to the rest of the personal and professional stress they are dealing with. Even though we are healthcare providers, well trained in universal precautions, when a staff member of client was actually diagnosed with COVID, there was a great deal of anxiety and even some panic regarding staff risk of infection." --Part A, B, and C grantee, West
"Staff morale is down. People have personal challenges with kids, parents, etc. Many staff have contracted COVID or been exposed to it." --Part A and C grantee, South
"Reduced volume of billable visits with same levels of staffing and increased workload on infection control, PPE, etc. has been a significant financial and morale strain." --Part C grantee, Midwest
While most respondents report sufficient resources in key areas to maintain COVID-era public health practices and safe work and clinical environments, critical gaps remained for many.
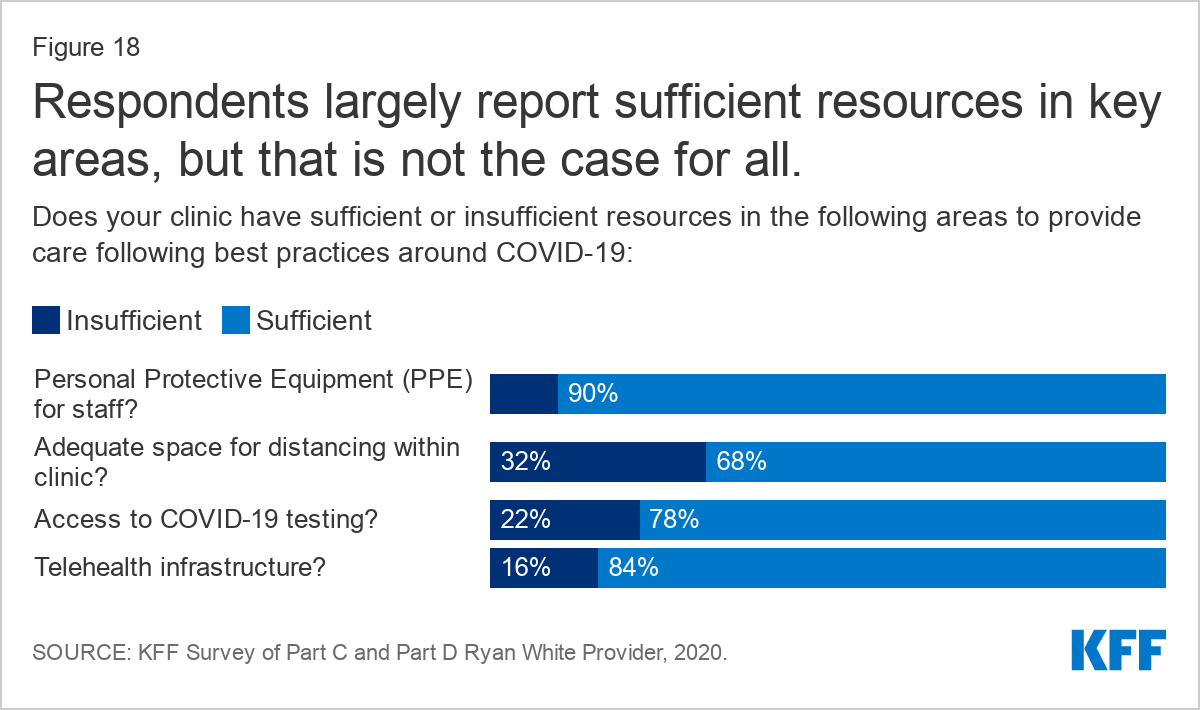
The most common gap, identified by one-third (32%) of respondents, was inadequate space for social distancing within the clinic. Respondents elaborated that lack of space was particularly concerning for staff sand patient safety. Potentially related to office crowding, 16% reported insufficient telehealth infrastructure.
"Lack of physical space to coordinate new services (COVID) and social distancing. Staff are sitting on top of each other and the waiting room is jammed with both healthy and sick people. Staff morale!!" --Part B and C grantee, Midwest
One in five (22%) reported insufficient access to COVID-19 testingIn some cases this appears to have meant lack of access to testing altogether but other respondents expressed that while they had access to COVID-19 testing, long result delays meant that testing access was inadequate.
One in ten (10%) respondents reported insufficient PPE for staff six months into the pandemic, including difficulty accessing items like N-95 masks and sanitizer. Others noted that while they have sufficient PPE now, they were very low resourced early on and worry the supplies could be hard come by again. As one respondent said the “future is hard to predict.” In some cases, respondents associated insufficient resources to operate safely with low staff morale.
"PPE supplies remain a moving target. We currently have enough, that may change. But the available supply for purchase is slowing catching up with demand…" --Part A and C grantee, South
"All of the items listed above are sufficient today. However, as we continue with COVID-19 in the months to come, these items like PPE, telehealth equipment, etc. might be insufficient." --Part A, B and C grantee, West
Many respondents who were able to adapt to follow public health guidelines, reported using CARES Act funding to do so. For example, respondents purchased telehealth equipment for themselves and clients, purchased masks and sanitation supplies, and modified their clinical spaces (see Box 1 for a detail on how respondents used CARES Act funding).
Discussion
The majority of Ryan White grantee respondents reported a quick pivot to new ways of providing HIV care and prevention in the COVID-era. They rapidly made significant changes to their operations, in some cases shutting services down all together but more commonly, introducing new offerings such as telehealth and multi-month prescribing. Some faced challenges when these changes were first implemented, including being unsure of how much of operations to shut down, struggling through technology learning curves, and dealing with staffing difficulties but many described eventually finding their footing and reopening to some degree within a “new normal.” Many respondents saw the supplemental Ryan White CARES Act funding as critical to their ability to adjust to new service and staffing needs and some worried about its continued availability as the pandemic wears on. However, some continued to struggle, including at least one respondent who has yet to reopen for any in person visits.
"Our ability to provide services was impacted significantly in March during the initial phases of transition to telehealth. Since then, our outreach, retention in care, and viral suppression rates have recovered to pre-pandemic levels due to extensive outreach efforts on the part of our staff and the successful implementation of telehealth." --Part C and D grantee, Northeast
"Initially, we struggled to make sure services continued to be available. Now we the changes and innovations we have made will make a lasting positive impact on our Program and services." --Part B and C grantee, Northeast
Most found that the new ways of providing care, worked very well for certain patients, including in retaining some previously hard to reach patients in care, and many foresee continuing such practices in the long-term. However, respondents also worried that some patients were being left behind and were concerned that as the pandemic wears on, medicine practiced exclusively virtually will cause problems. Respondents were especially eager to get patients back in for laboratory testing.
Additionally, many faced a shifting payer mix, struggled with engaging with community partners, and some continued to lack basic COVID era necessities, such as PPE. Patient and staff well-being was a top concern for most respondents. Both groups were dealing with significant stress and trauma. Respondents were very mixed in how well they believed they were able to meet client needs and retain them in care during the pandemic. However, despite the clear strain the pandemic has taking on clinical staff, most report resiliency and are figuring out how to best operate during an extraordinary time.
"While it has been challenging at times, it has definitely highlighted the resiliency of our clients and our staff!" --Part A, B and C grantee, South
This work was supported in part by the Elton John AIDS Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.