State Awards From Most of the Rural Health Fund Could Vary Only Modestly Despite Large Differences in Rural Needs
Issue Brief
The July 2025 budget reconciliation law, known as the One Big Beautiful Bill, established the Rural Health Transformation Program (referred to here as the “rural health fund”), which will distribute $50 billion to states with approved applications. The rural health fund was created to help offset the impact on rural areas of the law—which includes an estimated $911 billion in federal Medicaid spending reductions over ten years, including an estimated $137 billion in rural areas based on KFF estimates. The fund was also motivated by ongoing concerns about the financial vulnerability of many rural hospitals. CMS has indicated that the funds are intended to be used for investments in “system transformation” rather than for “perpetual operating expenses.” Funds can be used to support rural areas in a variety of ways, including by promoting prevention and chronic disease management interventions, supporting collaboration among rural health facilities, and recruiting clinical workers to rural areas. However, payments to providers for care cannot exceed 15% of total funds, though providers could benefit in other ways, such as through investments in existing buildings and infrastructure (restricted to 20% of total funds).
The law states that half of the fund ($25 billion) will be distributed equally to states with approved applications (i.e., without regard to need) while granting the Centers for Medicare & Medicaid (CMS) broad discretion over how to distribute the remaining funds. In September 2025, CMS released a Notice of Funding Opportunity (NOFO) explaining that the remainder ($25 billion) would be distributed across approved states based on measures of state need ($12.5 billion), as well as the quality of proposed initiatives, state policy, and other factors. The state application deadline was on November 5, 2025. CMS is required to make award decisions by the end of the year and plans to distribute the first $10 billion in January 2026.
This brief provides estimates of how $37.5 of the $50 billion fund could be distributed across states if all states are approved for funding. This $37.5 billion includes the portions of the fund that can be calculated or estimated based on available data, i.e., the $25 billion that will be distributed equally across states and the $12.5 billion that will be distributed based on CMS’s evaluation of measures of state need (such as the size of a given state’s rural population). Estimates of the latter are based on data from the Sheps Center, which are based on criteria specified by CMS in the NOFO using information available to the public. DC and Puerto Rico and the other U.S. territories are ineligible for funding and so were excluded from the analysis. Estimated awards in text are rounded to the nearest $10 million or to the nearest $10 per rural resident, as applicable. See Methods for more details.
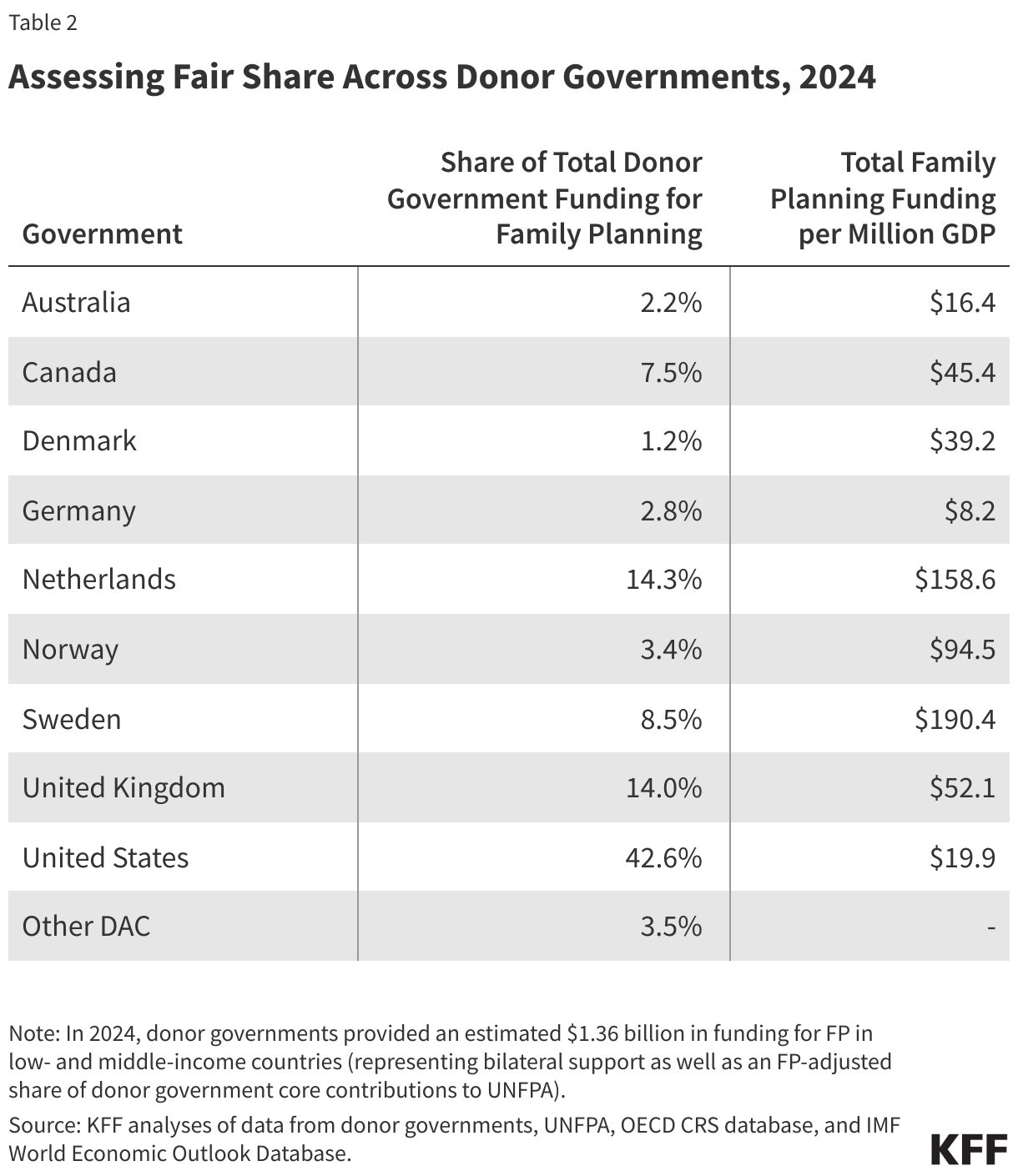
Awards from the $37.5 billion (of the $50 billion) could range from an estimated $550 million (in Rhode Island) to just over $1 billion (in Texas) over five years if all states were approved for funding. These differences are relatively modest compared to the wide variation across states in rural health needs.
Actual awards based on the first $37.5 billion would differ if CMS does not award funding to every state or if the agency decides to reduce awards for a given state over time. Actual awards to states may also differ if CMS uses different data to allocate funds or applies different criteria when distributing funds than what was indicated in the NOFO. For example, when evaluating the share of hospitals receiving Medicaid disproportionate share hospital (DSH) payments, CMS is expected to use more current data than are available to the public.
States could receive more than the estimates in this analysis, because totals will include their portion of the $12.5 billion that will be distributed based on CMS’s discretionary scoring of state policy, state initiatives, and other factors, and these scores are not yet known. State initiatives will be scored based on their quality by a merit review panel. This analysis will be updated after CMS announces the first year of funding.
Estimated Awards
Estimated Awards From $37.5 Billion of the $50 Billion Rural Health Fund Could Range From $550 Million to Just Over $1 Billion Over Five Years if All States Were Approved for Funding
If the $37.5 billion is distributed to all states, states will receive $750 million over five years, on average, with estimates ranging from $550 million in Rhode Island to just over $1 billion in Texas (Figure 1). Estimated awards for most states (32) are within 10% of the $750 million average (i.e., between $675 million and $825 million), despite wide variation in rural health needs.
Some states with relatively small rural populations could receive a disproportionate share of the $37.5 billion based on other factors. For example, Alaska has a small total population and the fifth smallest rural population in the country, but it could receive the fifth largest award from the $37.5 billion ($940 million). Most of the extra dollars that Alaska is estimated to receive from the $12.5 billion based on state need reflect the fact that a portion would go exclusively to the five states with the largest land area. Alaska is the largest state in the country and could receive $260 million from that pool.
Figure 1
As noted above, the $37.5 billion evaluated in this brief includes the $25 billion that will be distributed equally across states and the $12.5 billion that will be distributed based on measures of state need (Figure 2). Each state with an approved application would receive $500 million over five years from the $25 billion distributed equally across states if all states receive funding. If not all states are approved for funding, states with approved applications will receive more.
States will receive $250 million over five years, on average, from the $12.5 billion to be allocated based on state needs (again, assuming all states are approved for funding). Estimated awards from that $12.5 billion pool range from $50 million in Rhode Island to $530 million in Texas.
The remaining $12.5 billion of the $50 billion fund—which is based on state initiatives, state policy, and other factors—will result in additional funds for some or all states with approved applications, but cannot be estimated yet because of uncertainty about how CMS will score these factors (which, for example, will depend in part on whether states commit to certain policy changes in their applications and follow through over time).
Figure 2
Distribution Based on State Need
A Quarter of the $50 Billion Fund, $12.5 Billion, Will be Distributed Based Exclusively on Specific Measures of State Need
Of the $50 billion fund, a quarter ($12.5 billion) will be distributed based exclusively on specific measures of state need as defined by CMS (see below). In addition, $8 billion will be distributed based on the quality of state initiatives as determined by CMS (see below); that evaluation may take state needs into account to some degree, but the extent to which it will do so is unclear. State initiatives will be evaluated based on strategy, projected impact, sustainability beyond the funding period, and other factors, according to CMS.
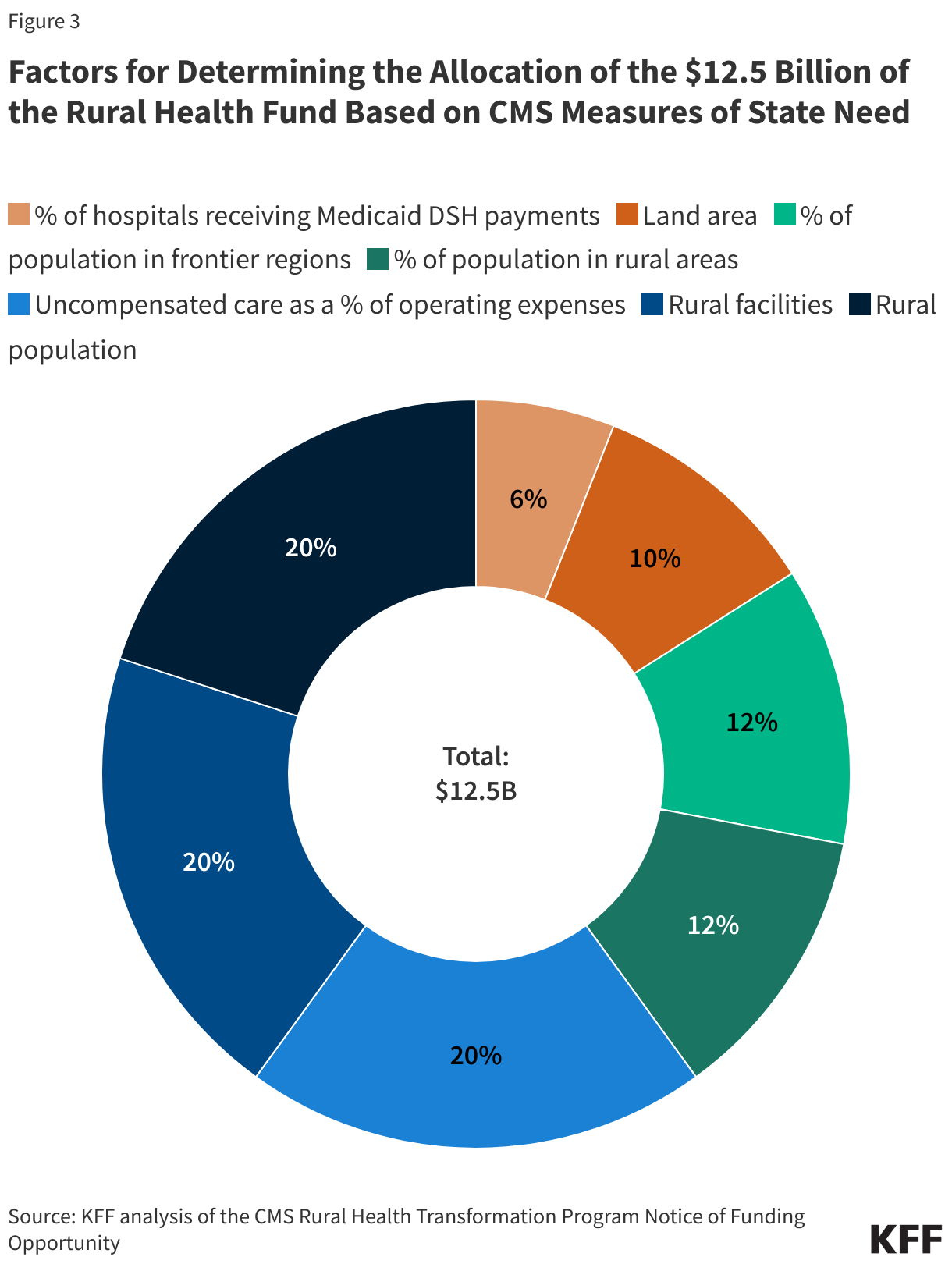
Based on criteria published by CMS, the $12.5 billion based exclusively on measures of state need will be distributed as follows:
- 40% of the $12.5 billion is based on the rural population and number of rural health care facilities in a state (20% each). CMS has published how it plans to define “rural” for purposes of distributing these dollars, though there are many potential ways of doing so. For example, CMS uses a broad definition of “rural hospitals” that includes all hospitals in areas classified as rural by the Health Resources & Services Administration (HRSA) (which itself is broader than some definitions) as well as any other hospital that receives certain Medicare rural payment designations or that is classified by Medicare as urban but reclassified as rural for certain payment purposes.
- 20% of the $12.5 billion is based on uncompensated care as a percent of operating expenses among all hospitals (i.e., not just those in rural areas). Uncompensated care tends to be higher in states that have not expanded Medicaid under the Affordable Care Act, such as Texas and Georgia. Further, CMS is using data from 2021; uncompensated care may have dropped over time among states that have recently expanded Medicaid (like Oklahoma and Missouri in 2021 and North Carolina and South Dakota in 2023).
- 24% of the $12.5 billion is based on the share of the population in rural areas and the share in frontier regions (12% each). These factors do not account for the total size of the population in each state or the size of rural health care systems (which is also the case for three other factors, like land area). As a result, states with a relatively large share of the population living in rural and frontier areas but relatively small rural populations and few rural hospitals may still receive a greater than average share of these dollars (e.g., as is the case for Alaska, North Dakota, and Wyoming) while the reverse may be true for states with large rural populations and many rural hospitals (e.g., as is the case for California, Florida, and Texas). Nonetheless, as noted above, 20% of the $12.5 billion is based directly on rural population and 20% on rural facilities.
- 10% of the $12.5 billion will be based on land area and will only go to the five largest states. These five states could each receive large allocations from this pool (ranging from an estimated $240 to $260 million if all were approved for funding), while states just outside of the top five and all other states will not receive funds based on land mass.
- 6% of the $12.5 billion is based on the share of all hospitals (not just those in rural areas) receiving Medicaid disproportionate share hospital (DSH) payments. Medicaid DSH status is based in part on the extent to which hospitals care for Medicaid and other low-income patients but also on specific criteria that vary across states.
Largest and Smallest Awards
Texas, California, New Mexico, Montana, and Alaska Are Expected to Receive the Largest Amounts From the $37.5 billion, Reflecting Differences Based on CMS Criteria of State Need
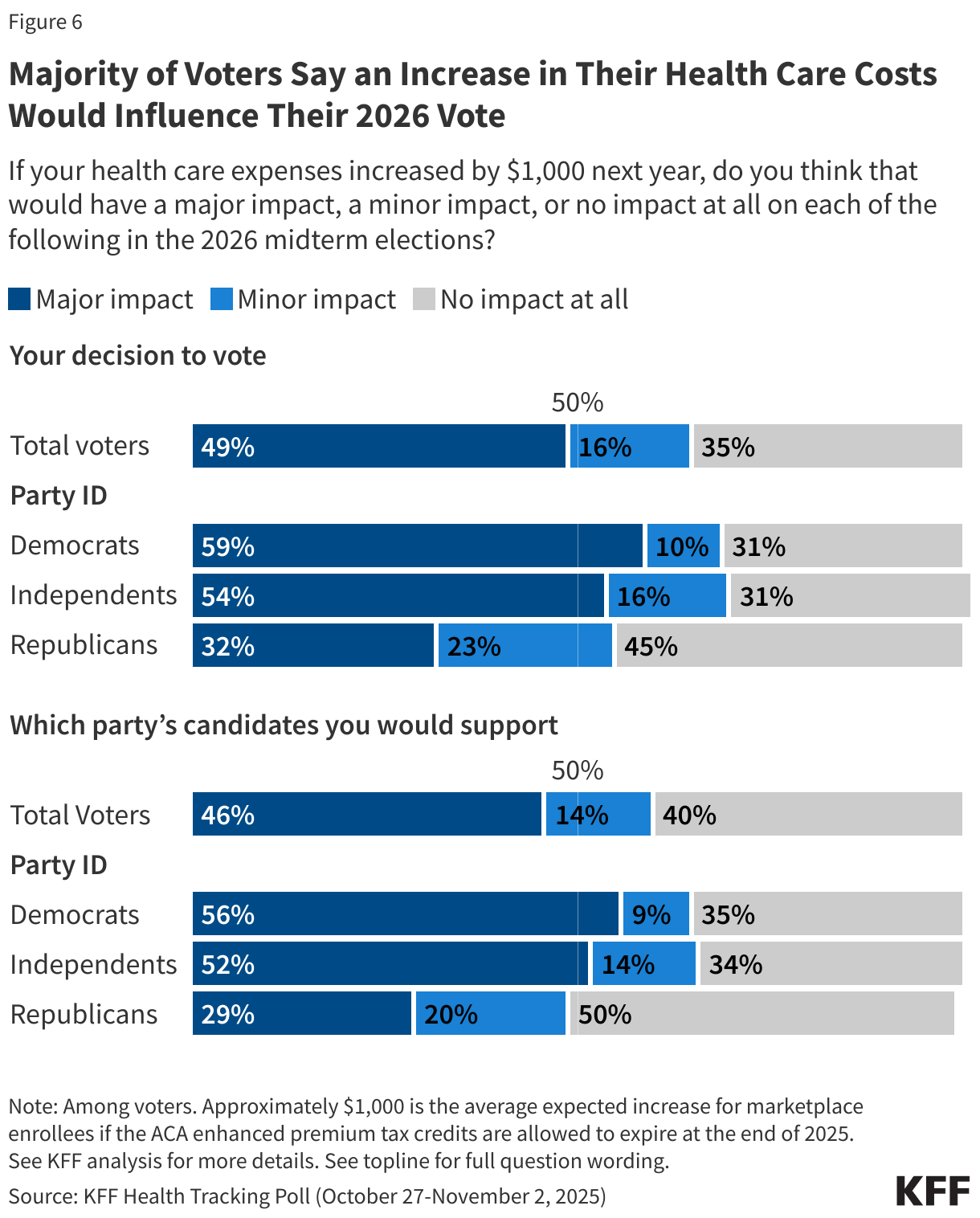
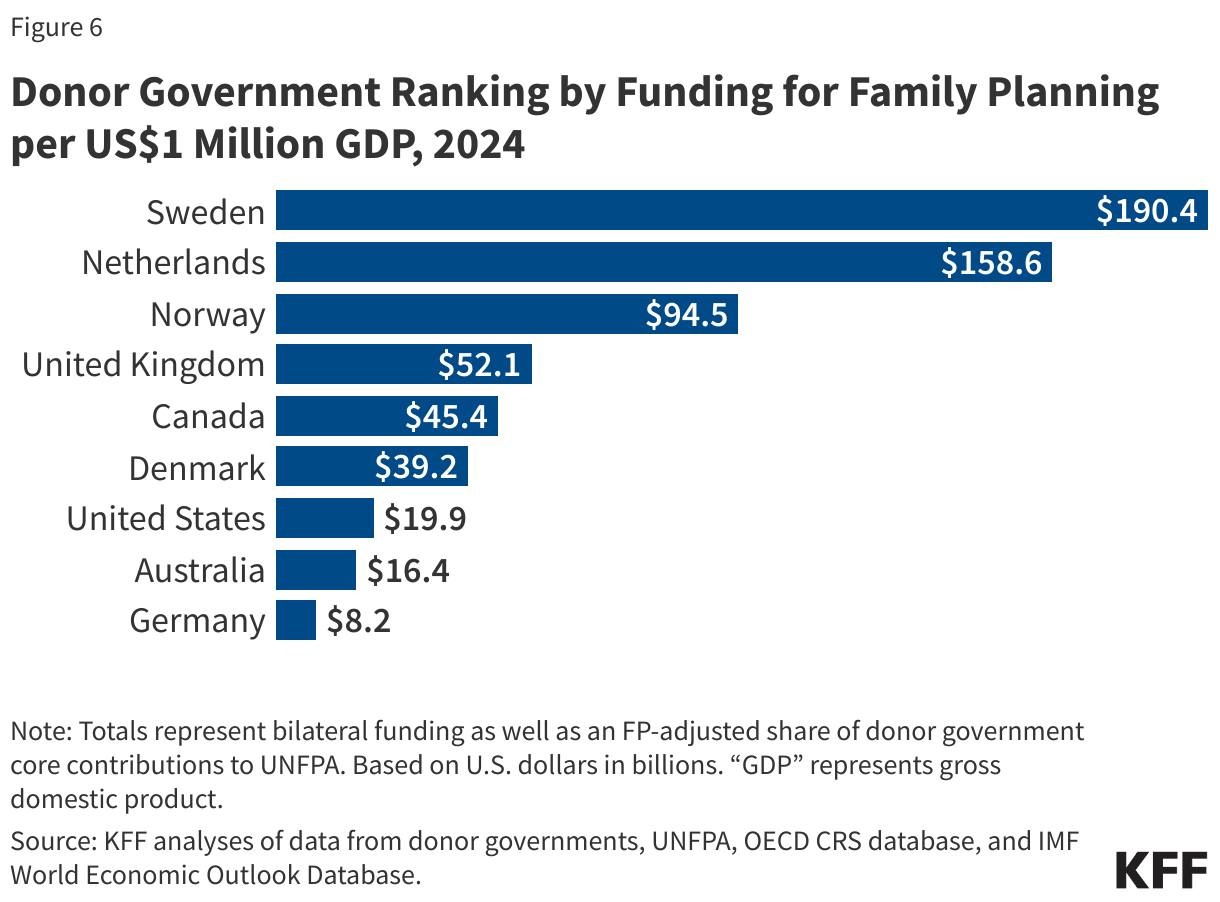
Estimated awards for these five states range from $940 to $1,030 million over five years from the $37.5 billion (Figure 1). As noted, $25 billion of the $37.5 billion will be distributed equally across states, meaning that any differences across states relate to the $12.5 billion distributed based on measures of state need ($12.5 billion). Most of the extra dollars that these five states are estimated to receive relative to others are attributable to the states’ relatively large land area, one of several factors used to allocate funds based on state need (Figure 3). Estimated awards based on this factor range from $240 million in New Mexico to $260 million in Alaska. Only the five largest states would receive funding from this pool based on their land area.
Figure 4
Missouri, Mississippi, North Carolina, Georgia, and Oklahoma could receive the next largest awards from the $37.5 billion, with estimates ranging from $820 to $840 million over five years. These states are estimated to receive more funds than average because they have relatively large rural populations and numbers of rural facilities and had relatively high levels of hospital uncompensated care in the year evaluated, among other factors. Despite these differences, their estimated awards are only roughly 10 percent more than the average award across all states ($750 million over five years) from the $37.5 billion.
Rhode Island, Massachusetts, Delaware, Connecticut, and New Jersey could have the lowest awards from the $37.5 billion, with estimates ranging from $550 to $610 million over five years. These are all relatively small states in or near the Northeast that rank relatively low on most factors, including rural population and the number of rural facilities.
Payments Per Rural Resident Could Vary Widely
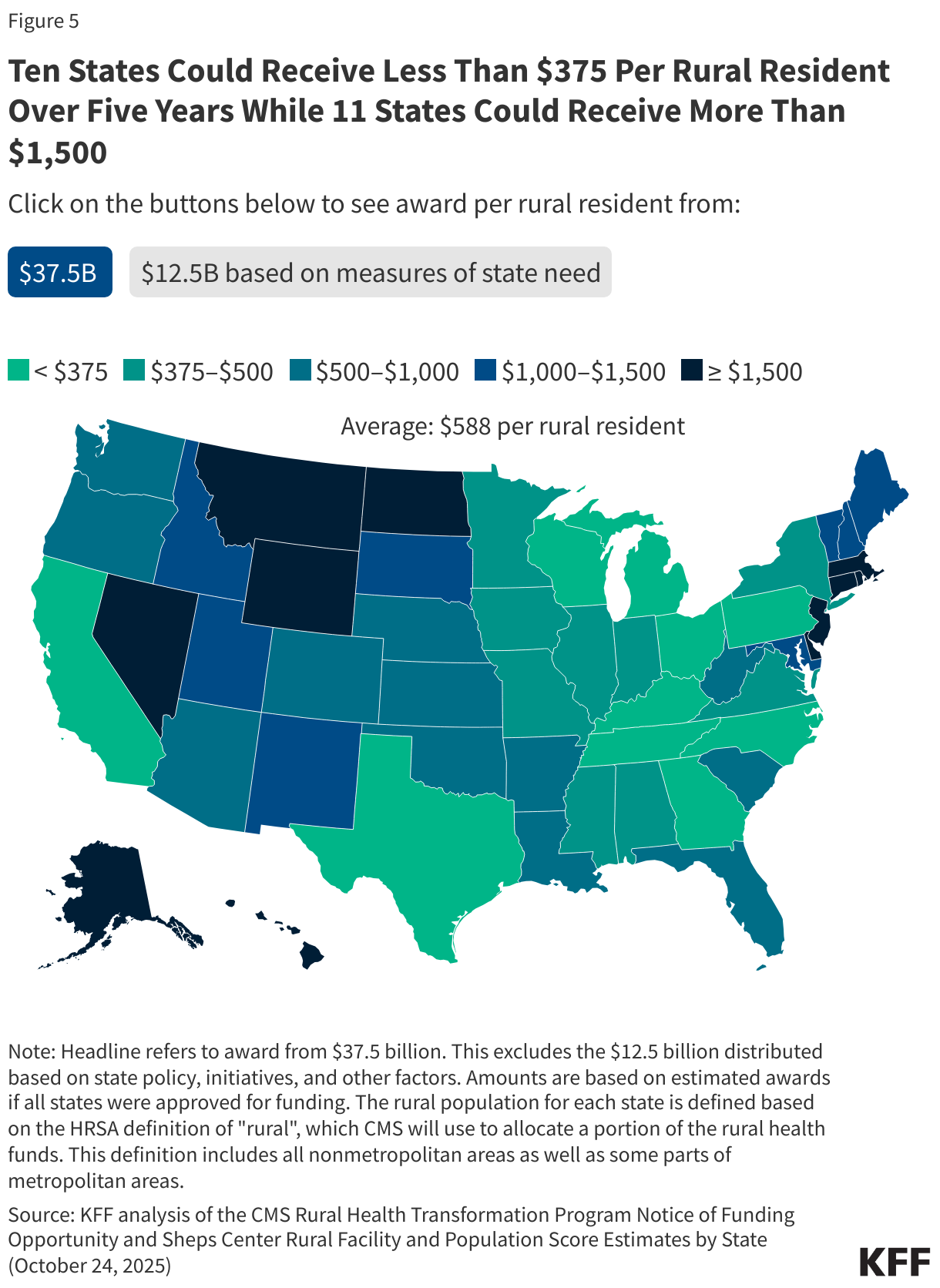
Ten States Could Receive Less Than $375 Per Rural Resident Over Five Years While 11 States Could Receive More Than $1,500, Before Disbursements Based on State Policy, Initiatives, and Other Factors
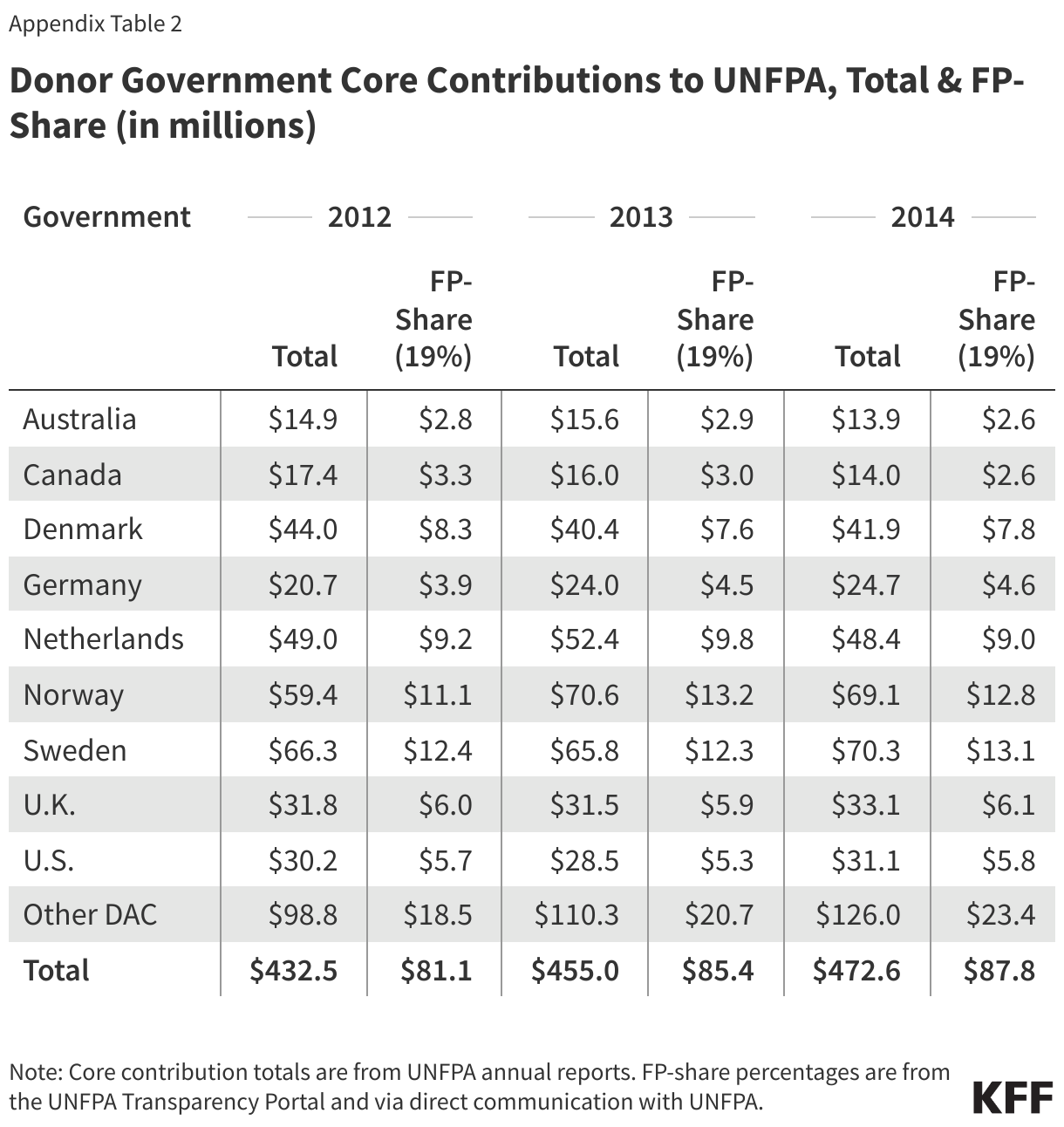
Estimated awards from the $37.5 billion are partially, but not closely, tied to rural population, resulting in large differences in the amount each state could receive per rural resident. Assuming all states receive funds, the average award per rural resident across all states would be $590, but this amount per rural resident would vary widely across states. Texas could receive the least amount per rural resident ($240) while Rhode Island could receive the largest amount ($22,150, an outlier) (Figure 3). This in part reflects the fact that estimated state awards vary much less than differences in rural populations, principally due to the equal distribution of the first $25 billion across all states with approved applications but also reflecting the structure of the $12.5 billion distributed based on measures of need (only 20% of which is directly based on rural population).
Additional Factors Affecting Awards
Most of the Remaining $12.5B Will be Distributed Based on State Policy and CMS’s Evaluation of States' Proposed Initiatives
Of the remaining $12.5 billion, $8 billion (64%) is expected to be distributed across states based on the quality of their proposed initiatives, $3.75 billion (30%) based on state policies, and $0.75 billion (6%) based on other factors. It is not yet clear how, and how much, this portion of the award will differ across states, or the extent to which these funds will align with different measures of rural health needs.
According to CMS, the first bucket ($8 billion) will be distributed based on a qualitative review of a state’s proposed initiatives and, in later years, the state’s progress in implementing their plan. Proposed initiatives will be scored by a merit review panel selected by CMS. Panel members have not been announced to the public.
The second bucket ($3.75 billion) will be distributed based on whether a state has adopted, made progress towards adopting, or committed to adopting certain policies. Some of these policies aim to promote competition among health care providers, such as by expanding scope of practice for nurse practitioners and other non-physicians. Among other factors, three measure states’ progress in implementing certain Make America Health Again (MAHA) policies.
The remaining funds ($750 million) will be distributed based on other factors, such as the share of dual eligibles in integrated care plans and the quality of Medicaid and Children's Health Insurance Program (CHIP) data reporting to CMS.
Looking Ahead
CMS will decide which states to fund by the end of the year, and how to allocate the first year of funding across states. The agency will allocate $10 billion per year to states with approved applications over a five-year period (fiscal years 2026 through 2030), and it plans to distribute the first round of $10 billion in January 2026. CMS will use the same funding formula for each year, but the distribution of funds across states will likely change over time. This is in part because a quarter of the funds—i.e., the $12.5 of $50 billion excluded from analyses in this brief—is based on factors that are likely to change over time, including states’ progress in implementing policy changes and their proposed initiatives. The distribution could also change over time depending on whether CMS chooses to withhold, reduce, or recover funds from a given state for noncompliance or other reasons.
It is not clear what share of the $50 billion fund will go to rural hospitals and other rural health care providers or the extent to which any direct and indirect benefits of the fund will offset their losses under the reconciliation law. While some policymakers promoted the rural health fund as a way to support rural hospitals, the funds can also be used for much broader purposes. CMS has indicated that the funds are intended to be used for investments in “system transformation” rather than “perpetual operating expenses.” CMS has stipulated that payments to hospitals and other providers for patient care cannot exceed 15% of total funds, though providers could benefit in other ways, such as through investments in existing buildings and infrastructure (which are restricted to 20% of total funds). Evaluating the implications for rural hospitals will depend on how CMS allocates funds to states and how much of these funds states distribute to rural hospitals, other providers, and for other state initiatives.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
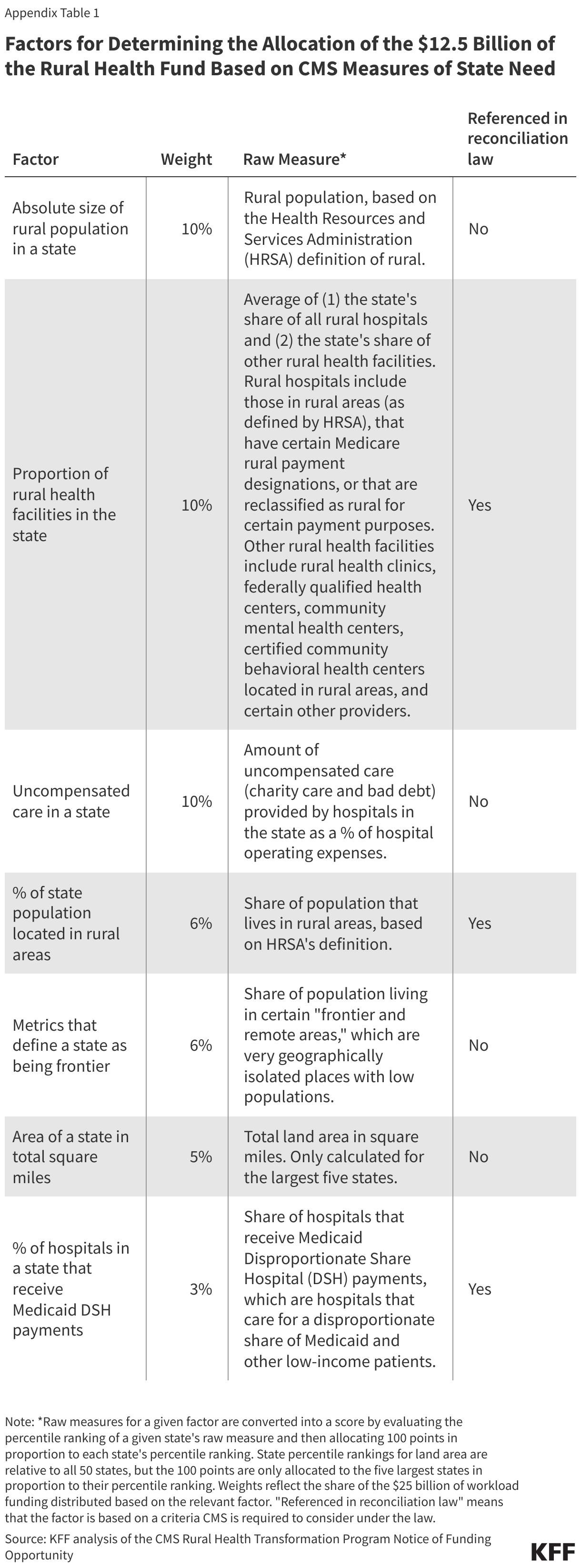
Of the $50 billion rural health fund, half ($25 billion) will be distributed equally among states with approved applications and half ($25 billion) will be distributed among approved states based on a set of 23 factors, weighted to varying degrees, as detailed by CMS in the Notice of Funding Opportunity (NOFO). CMS refers to the first half as “baseline funding” and the second half as “workload funding.” Weighted scores based on the workload funding factors will total to 100 points across all states. A state’s share of the $25 billion will depend on their total weighted score divided by 100, and its share of funds distributed based on a given factor will equal their weighted score for that factor divided by 100. The reconciliation law determined the overall allocation of baseline and workload funding, but gave CMS discretion to define more specifically how the workload funding would be distributed.
Of the $37.5 billion evaluated in this brief, $25 billion reflects the baseline funding that will be distributed equally across states with approved applications, as described in the law. If all states are approved for funding, each state would, by definition, receive $500 million over five years from this pool of funding. If not all states are approved for funding, the $25 billion of baseline funding will be distributed equally among states with approved applications only, meaning that each would receive more than $500 million.
The other $12.5 billion of the $37.5 billion evaluated will be based on CMS measures of state need. This corresponds to the half ($12.5 billion) of the workload funding that will be distributed based on seven factors that CMS refers to as “rural facility and population factors” (three of which are based on measures listed in the reconciliation law). Appendix Table 1 includes details about these factors based on the NOFO. We obtained estimated scores by state for each of these factors and their weighted total by state from the UNC Sheps Center Rural Facility and Population Score Estimates by State, as updated on October 24, 2025. The Sheps Center generated these estimates based on their interpretation of the NOFO and available data.
We converted estimated scores for a given factor into a dollar amount by: (1) calculating the share of workload funding distributed based on that factor (i.e., multiplying $25 billion by the weight for that factor) and (2) multiplying the result by the state share of the distribution based on that factor (i.e., the score divided by 100). Each state’s total distribution from the $12.5 billion based on state need is the sum of the factor allocations calculated in (2).
We calculated the total award from the $37.5 billion as $500 million per state plus the estimated award from the $12.5 billion. To calculate the award per rural resident, we divided by the state rural population as defined by CMS for the first factor, which was available from the Sheps Center estimates.
This analysis does not include the second half of the workload funding ($12.5 billion) that will be distributed based on state initiatives, state policy, and other factors, but cannot be estimated yet because of uncertainty about how CMS will score these factors. We do describe what share of the $12.5 will be distributed based on state initiatives, state policy, and other factors based on the weights assigned to each of the factors included in these three buckets. Some of these factors (health and lifestyle, individuals dually eligible for Medicare and Medicaid, remote care services, and data infrastructure)—representing 30% of the $12.5 billion—will be scored by evaluating how states rank based on a weighted average of measures from two buckets. For example, health and lifestyle factors will be evaluated based on the state rank of a weighted average of their score on certain state initiatives (75%) and the adoption of a certain policy (25%). The contribution of each bucket in those cases cannot be fully disentangled because of the structure of the calculation, which involves a ranking of a weighted average. In those cases, we apportioned the funding from these factors to each bucket based on the weights used to generate the weighted average (e.g., 75% or 25%).
Appendix