It has been reported that the Centers for Disease Control and Prevention (CDC) will not renew its main, five-year, HIV prevention grant for community-based organizations (CBOs) (grant number PS21-2102). CBOs have long been part of the front-line of the HIV response. As noted in the original CBO grant announcement, “because of their accessibility, history, and credibility in the community, CBOs are recognized and remain important partners in providing comprehensive high-impact HIV prevention services.” Grantees have used these funds to conduct a range of integrated prevention activities, including HIV and other STI testing, linkage-to-care efforts, PrEP navigation, and partner services, among many other efforts.
Separately, CDC has made supplemental funding available to state and local health departments to carry out HIV prevention activities under a separate preexisting grant mechanism (PS24-0047), which health departments can apply for.1 Those health departments receiving supplemental grants under PS24-0047 are encouraged but not required to engage community-based partners, with higher suggested allocations going to those in “Ending the HIV Epidemic (EHE)” jurisdictions.2 These supplements would not replace direct-to-CBO funding (PS21-2102) but could provide some organizations with future resources. Ultimately, different health departments will make different decisions, but the new approach could affect the budgets and sustainability of some community-based organizations, particularly those that are already less well-resourced. More broadly, this would be a marked change in how CDC carries out its HIV prevention work, ending direct funding to CBOs, which it had been doing since the late 1980s.
Advocates and members of Congress have expressed concern about this development, reportedly coming at the direction of the Office of Management and Budget (OMB). It also comes at a time when there are questions about the federal commitment to HIV prevention, with the Trump administration seeking to eliminate CDC HIV prevention funding altogether (although Congress has rejected these requests). The administration has also taken actions aimed at limiting or terminating federal funding or programing, particularly for projects that address LGBTQ+ issues and racial/ethnic health disparities. Per available award information, many of the funded CBOs specifically sought to address HIV in these communities with their grants, especially working to ensure efforts reach Black, Latino, and transgender people, groups disproportionately impacted by HIV.
To better understand the extent of this change, this analysis uses data from USAspending.gov, the federal government’s official source of federal award and spending information, to provide a snapshot of where, to whom, and at what level the CBO (PS21-2102) grants were distributed. Overall, it finds that CBOs stand to lose significant amounts of funding for HIV prevention going forward, with potentially more than $230 million at stake. The largest number of these organizations are located in the South, the region with the greatest number of HIV diagnoses in the U.S.
Findings
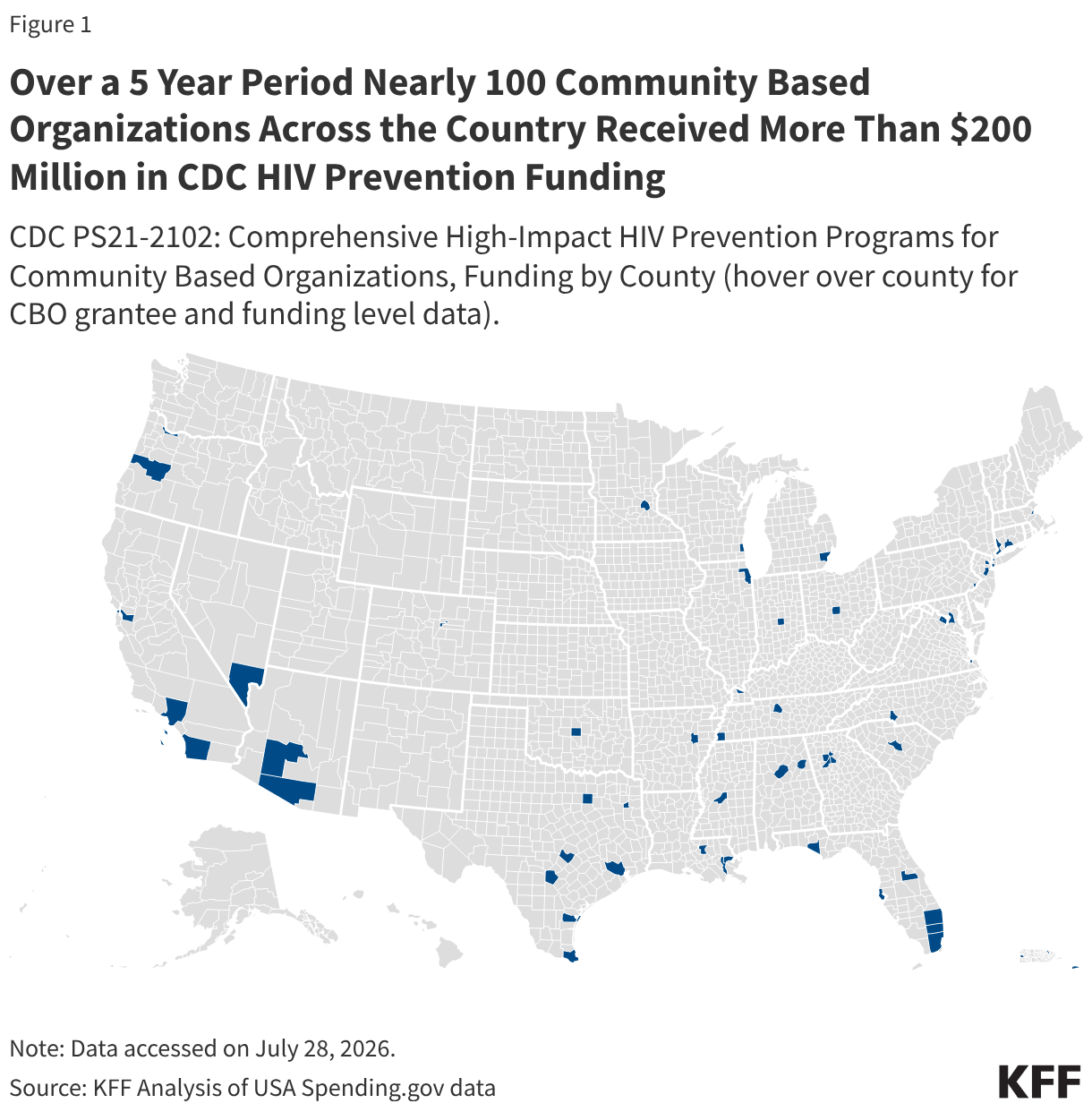
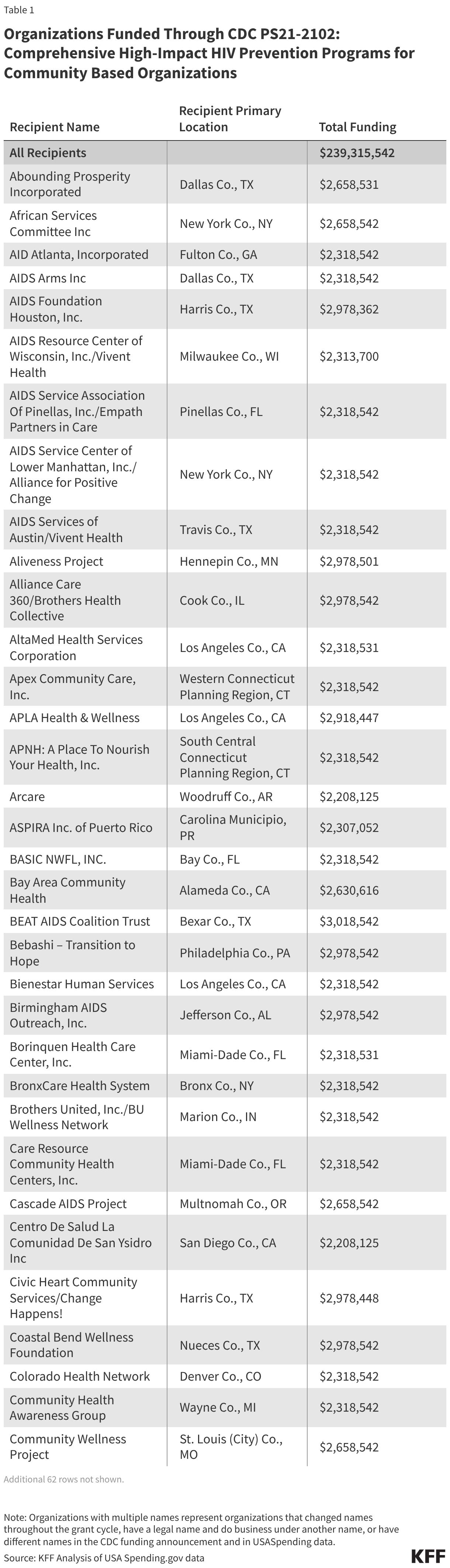
- Including both base and supplemental/continuation amounts, funding for CBOs through PS21-2102 totaled $239.3 million over the grant period, initially five years (2021-2025), with some additional funding distributed in 2026. (See Figure 1, Table 1).
- Over the entire period, grants ranged from $2.2 million (received by two organizations: Arcare in Woodruff County, AR and Centro De Salud La Comunidad De San Ysidro Inc. in San Diego County, CA) to $3.0 million (received by BEAT AIDS Coalition Trust in Bexar County, TX). The most common funding amount was $2.3 million, received by 46 grantees.
- On an annual basis, each organization received approximately $442,000. Supplemental or continuation3 funding ranged, depending on the year, between approximately $100,000-$300,000 per grantee.
- Of the $239.3 million for PS21-2102, $212.8 million was provided through base funding (89%), while the remainder ($26.5 million, 11%) was provided through supplemental funding in various years.
- Funding was awarded to 96 community organizations across 62 counties/jurisdictions in 31 states, Washington D.C., Puerto Rico, and the U.S. Virgin Islands. The states with the greatest concentration of CBOs receiving funding were California, Florida, and Texas (each with 11 CBOs). CBO funding averaged $7 million per state, ranging from $2.2 million (Arkansas) to $29.2 million (Texas). By county, the average amount allocated to CBOs was $3.9 million, ranging from $2.2 million in Woodruff County, AR, for a single grantee, to $14.5 million in Los Angeles County, CA for six grantees.
- Half of all funding was channeled to the South. Forty-nine percent (49%) of all funds, or $118 million, was awarded to organizations in the South, a region that accounts for over half of HIV diagnoses. Organizations in the West (18%), Northeast (16%), and Midwest (14%) saw more even award distribution. Organizations in the Caribbean received 3% of award funding.
- For some CBOs, direct CDC funding represented a significant share of their revenue, and they may be more vulnerable to funding reductions. For example:
- Community Wellness Project in St. Louis (City), MO, received a base award of $441,625 per year. According to their 990s, in 2024 this represented 20% of the organization’s revenue and in 2021, 45%.4
- NAESM Inc. in Fulton County, GA also received an award of $441,625 per year. Based on their 2024 990, one year of grant funding would have been equal to 10% of their overall revenue and, 31% of revenue in 2021.5
- APNH: A Place to Nourish Your Health, Inc. in South Central Connecticut Planning Region, CT also received $441,625 per year. Based on their 990, one year of grant funding would have been equal to 18% of their overall revenue in 2024.6
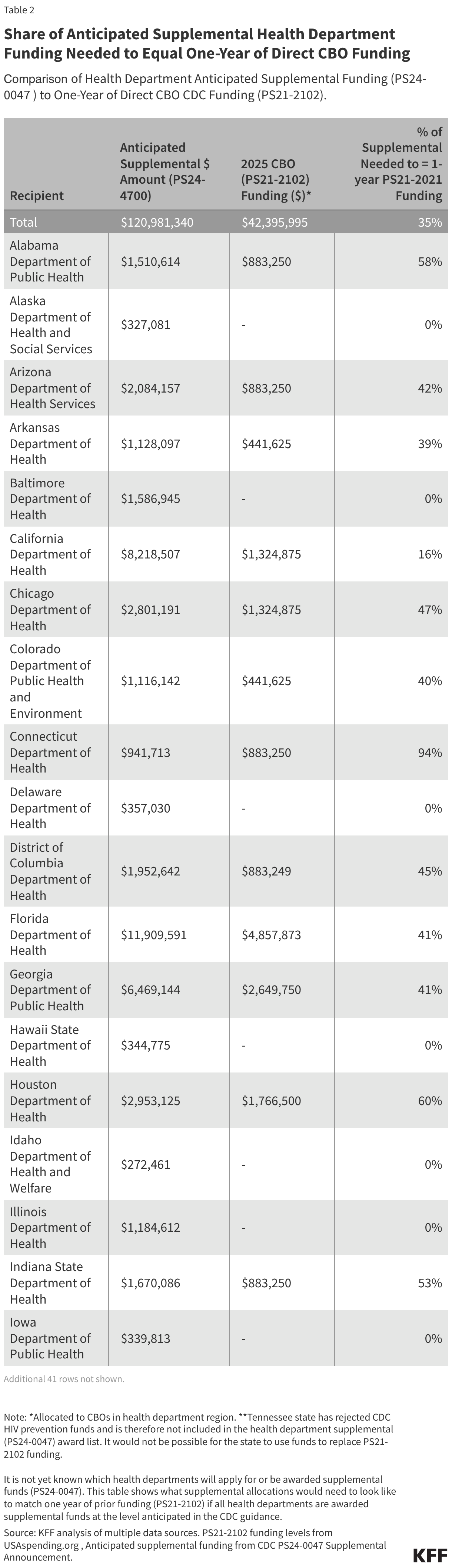
- The new supplemental funding provided to health departments (PS24-0047) appears unlikely to be able to replace the resources PS21-2102 provided directly to community organizations. Even if all health departments in jurisdictions with former CBO grantees (36 jurisdictions in total) applied for and were awarded additional PS24-0047 funding at the level described and chose to allocate resources to CBOs at the minimum levels recommended by CDC, local organizations would see a decline in funding compared to what they received under PS21-2102.
- Estimated one-year PS24-0047 supplemental funding to CBOs would be 27% to 71% lower than the final year of the PS21-2102 base amount when provided at the minimum recommended levels.7
- 29 of the 36 health departments (81%) home to former CBO grantees would need to make greater than the highest minimum recommended allocations of PS24-0047 supplemental funding to match prior direct-to-CBO (PS21-2102) funding.
- To match the level of funding CBOs had been receiving, overall health departments would need to allocate 35% of their awards to CBOs, a share above the minimum recommended by CDC (10% or 25% minimum depending on jurisdiction, see note and methods).2 Some would not be able to match PS21-2102 funding with their award. (See Table 2.)
- This ranges by jurisdiction, from 13% of the award in two jurisdictions (North Carolina and Ohio) to over 100% of funding in three jurisdictions (Minnesota, Oregon, and the U.S. Virgin Islands)
- Additionally, Tennessee has rejected CDC HIV prevention funds and therefore is not eligible for supplemental awards and will not have these resources to allocate to CBOs. Similarly, if other health departments do not apply for or are not awarded the PS24-0047 supplemental funds, there will be nothing to allocate to CBOs from this account.
It is not yet known which health departments applied for or will be awarded the supplemental funds, nor what share of funds health departments will ultimately decide to allocate to community groups. However, this analysis finds that even if they choose to fund CBOs at the minimum recommended levels, the level of funding going to CBOs would be reduced in many regions, including some that would see significant drops. Facing fewer resources, organizations may be less equipped to provide or support HIV prevention programs, which could in turn affect the HIV prevention response, increasing the vulnerability of some communities to additional HIV cases.
Methods
PS21-2102 funding totals: PS21-2102 funding levels were obtained from USAspending.gov on July 28, 2026. Funding was examined for the full five-year grant period (2021-2025) and includes base year funding and supplemental or “revision” amounts. Funding was also captured for continuation funding provided in 2026. State and county designations are those assigned in USAspending.gov.
Estimated PS24-0047 CBO supplemental funding and comparison to historic direct-to-CBO PS21-2102: Estimated PS24-0047 supplemental funding levels was obtained from the CDC’s “Updated Supplement Guidance” for Notice of Funding Opportunity Number (NOFO): CDC-RFA-PS-24-0047. In this announcement, 60 health departments are identified as eligible to apply for the new supplemental funding. Among the 96 organizations previously funded by PS21-2102, all but two organizations (located in Tennessee, and discussed in text) were located in these jurisdictions. These organizations are based in 36 of the 60 eligible health department regions.
Assessing how estimated one-year PS24-0047 supplemental funding allocated to CBOs would compare to the final year of the PS21-2102 base funding at minimum recommended levels: CDC encourages grantees “to provide a minimum of 10% of the supplemental funding to support partnerships with community-based organizations (CBOs)…[and for] EHE jurisdictions…to provide a minimum of 25% of funding” to CBOs. CDC has historically expressed specifically what share of health department PS24-0047 funds are for EHE and which are not, but that information is not yet available. Since it is not yet known what share of funds is likely to be treated as EHE, we applied blanket 10% and 25% allocation scenarios to the estimated supplemental award levels to develop a range of minimum anticipated funding. Because the PS24-0047 supplemental amount is for one year, only the final year (FY 2025) base amount of the PS21-2102 awards is used in that part of the analysis.