VOLUME 22
Public Trust in Vaccine Information, Misrepresented Vaccine Studies, and HIV and PrEP Stigma
Summary
This volume examines findings about trusted sources of vaccine information from the latest KFF Tracking Poll on Health Information and Trust. It also explores how the misrepresentation of scientific studies, legal developments, and evolving public health guidance are contributing to the spread of false health narratives around vaccines, HIV and PrEP. Lastly, it summarizes new research on the use of generative AI to counteract vaccine misinformation, highlighting both its potential and limitations.
Featured: Latest KFF Tracking Poll on Health Information and Trust Finds Trust in Doctors for Vaccine Information Remains High, With Partisans Divided on Trust in Other Sources
The latest KFF Tracking Poll on Health Information and Trust finds that individual doctors remain the most trusted sources of reliable vaccine information among the public, while trust in other sources is lower and often characterized by large partisan gaps.
Large majorities of adults and parents say they have at least a “fair amount” of trust in their own doctor (83%) or their child’s pediatrician (81%) to provide reliable information about vaccines. Fewer, but still majorities, trust vaccine information from government health agencies including their local public health department, the CDC, and the FDA, while about half trust pharmaceutical companies and half of parents trust their children’s school or daycare.
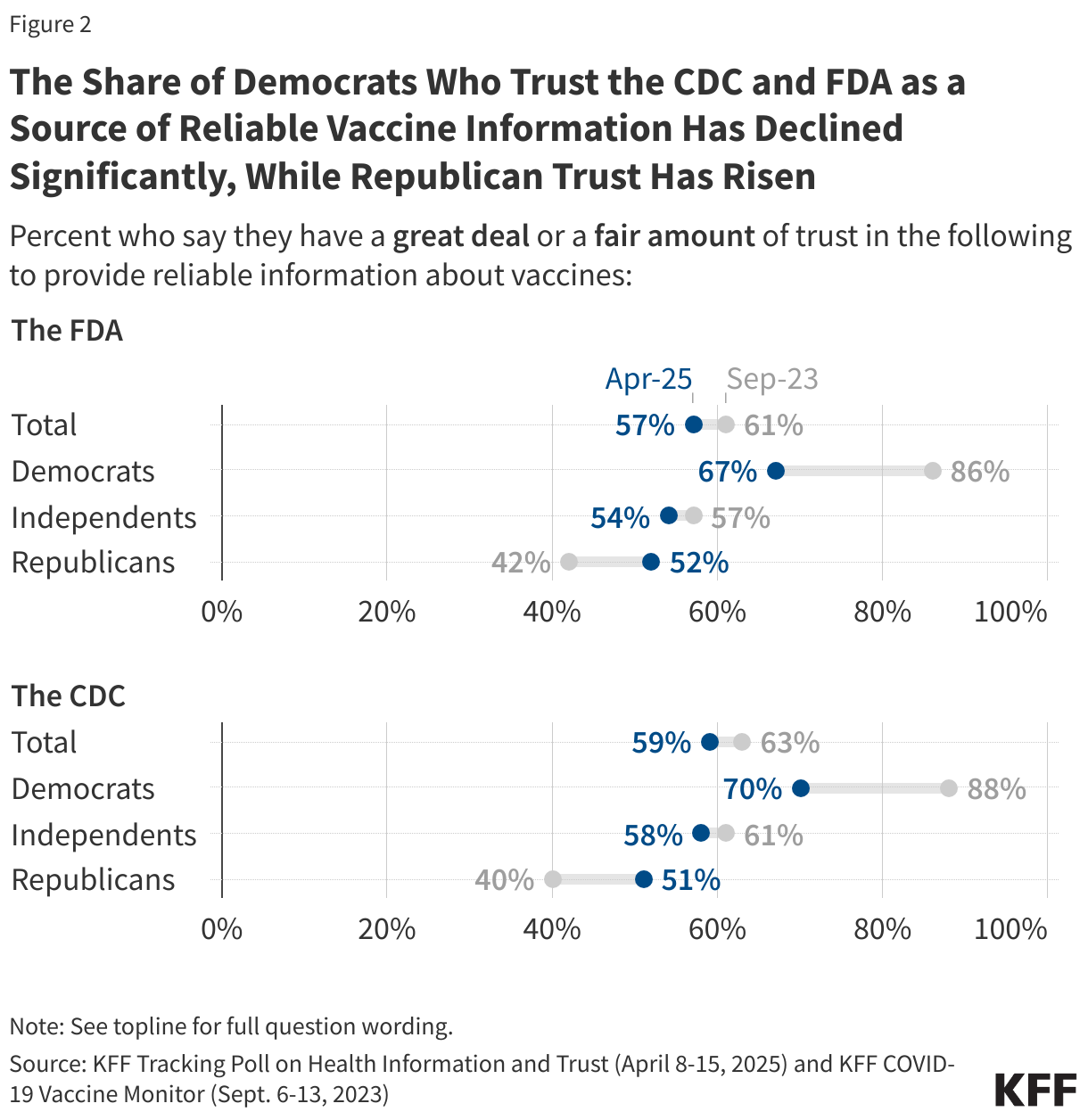
While majorities across partisans express trust in their doctor or child’s pediatrician to provide vaccine information, Democrats are more likely than Republicans to trust their doctor (93% v. 78%) or, among parents, their child’s pediatrician (91% v. 73%) as a source of reliable vaccine information. Additionally, larger shares of Democrats compared to Republicans express trust in vaccine information from government health agencies, though this gap has narrowed since the start of President Trump’s second term as trust has declined among Democrats and risen among Republicans. For example, 70% of Democrats and 51% of Republicans now say they trust the CDC for reliable vaccine information, a gap of 19 percentage points. In 2023 under the Biden administration, that gap stood at 48 percentage points (88% of Democrats vs. 40% of Republicans).
Republicans, in turn, are much more likely than independents and Democrats to trust President Trump and HHS Secretary Robert F. Kennedy, Jr. on vaccines. Three quarters of Republicans say they trust President Trump (74%) and Secretary Kennedy (73%) to provide reliable information about vaccines, making Republicans as likely to trust President Trump and Secretary Kennedy as they are to trust their own doctor on the subject.

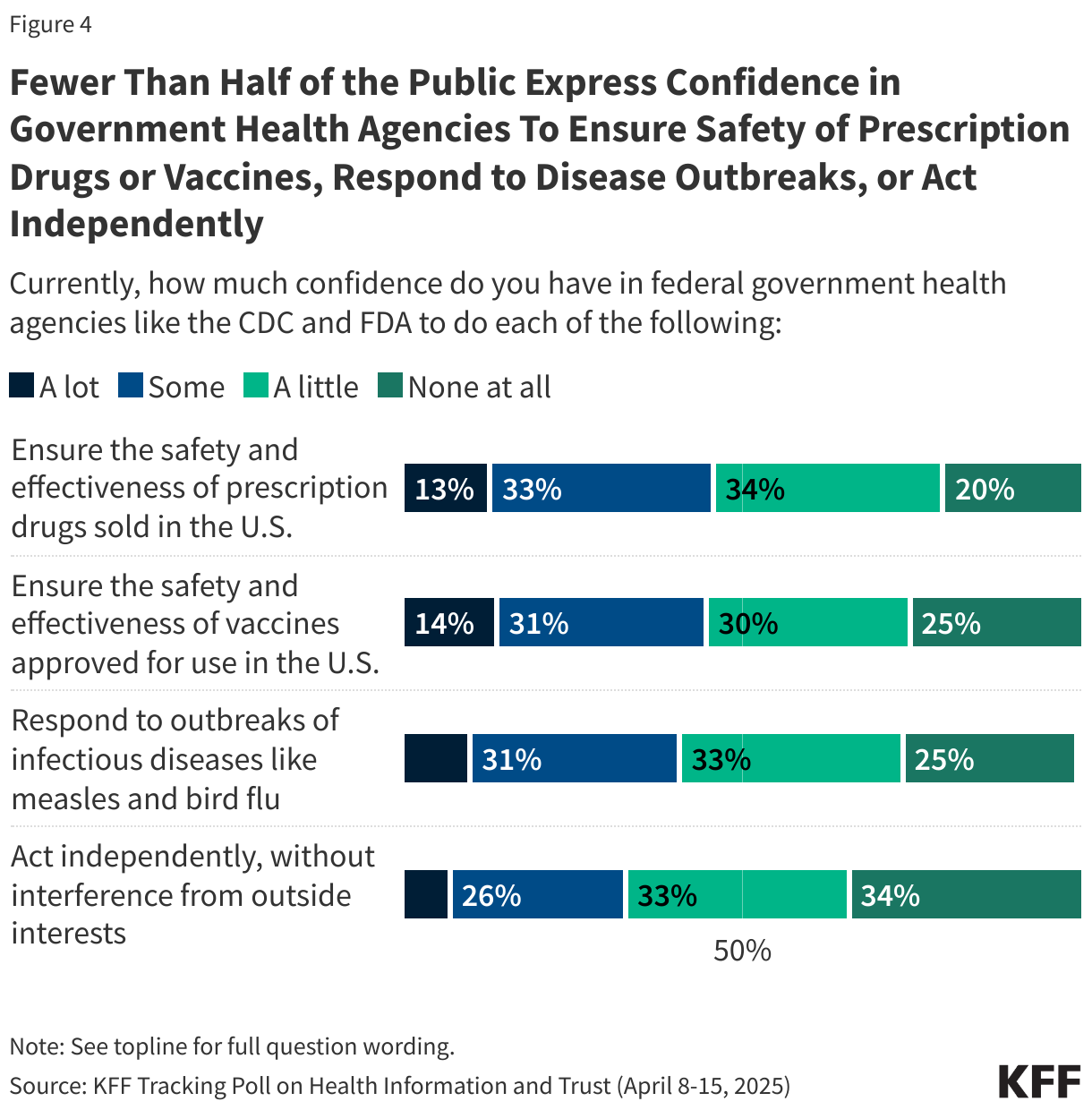
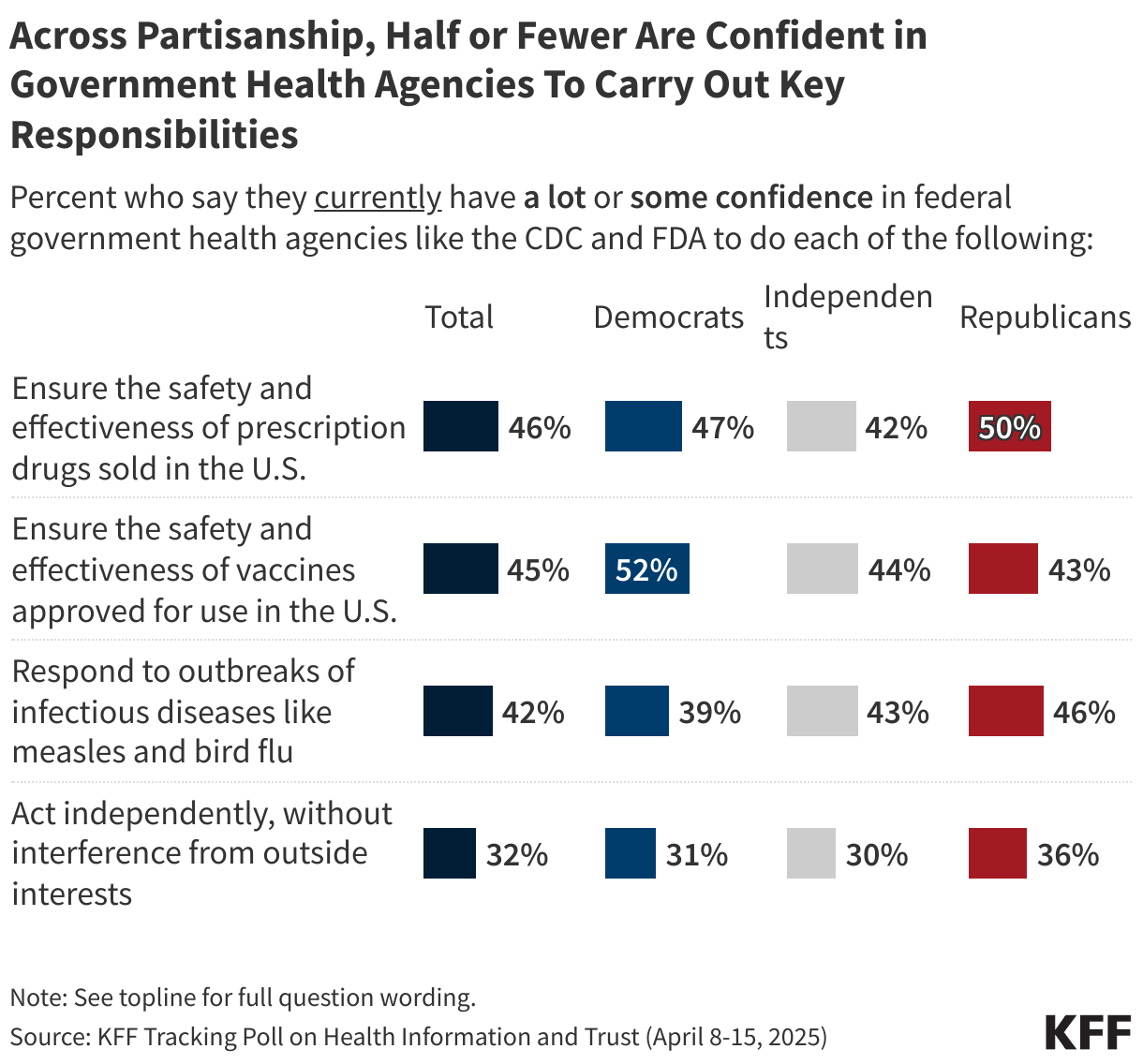
The poll also finds that fewer than half the public express “a lot” or “some” confidence in government health agencies to carry out key responsibilities, including ensuring the safety and effectiveness of prescription drugs (46%) or vaccines (45%), responding to outbreaks of infectious diseases (42%), or acting independently without interference from outside interests (32%). Across partisans, half or fewer express at least “some” confidence in these agencies to carry out each of these responsibilities.
Recent Developments
Flu Vaccine Study Misrepresented Online Amid Severe Season

Influenza deaths in the United States during the 2024-2025 flu season are higher than in previous years. Although the flu vaccine can prevent severe illness, hospitalization, and death, rates of vaccination have declined since 2020. The effectiveness of seasonal flu vaccines can vary year-to-year based on how similar the vaccine is to the circulating virus, but vaccines can offer protection against severe outcomes even when they are not well-matched to circulating strains. Data from the CDC supports the effectiveness of this season’s vaccine to protect against serious outcomes, and past data show that protecting against these outcomes is a primary benefit of the flu vaccine. As influenza deaths rise, the CDC continues to recommend that everyone 6 months of age and older receive a flu vaccine every season, with rare exceptions.
But some social media posts are sharing findings from a preprint study from researchers at the Cleveland Clinic to suggest that the flu vaccine is unsafe or ineffective without sharing context about the outcomes evaluated. The study, which has not yet been peer-reviewed, looked at more than 53,000 healthcare workers during the 2024-2025 flu season and found a higher rate of infection among those who were vaccinated. However, the authors explain that flu vaccine effectiveness depends on how closely the vaccine strains match the circulating virus in a given year. The study also did not evaluate the severity of illness, such as hospitalization or death, which are the primary outcomes vaccines are intended to prevent. Protection against infection with the flu can vary, but vaccines are consistently shown to reduce the risk of serious illness. After the study was posted online, a Cleveland Clinic spokesperson clarified to PolitiFact that the study did not represent the general public and does not suggest that flu vaccination increases the risk of flu.
After the study appeared on medRxiv, social media posts began circulating with misleading claims that the flu vaccine is ineffective or harmful. For example, one account that has previously shared false claims about vaccines online wrote, “Just like the COVID jabs and pretty much any other ‘vaccine’ it appears that the flu shot is an abject failure. In a preprint study from the Cleveland Clinic, employees that got the flu shot had a 27% HIGHER chance of contracting the flu.” Another post called for the removal of the flu vaccine from the market, “pending large prospective studies of their safety and effectiveness.” These posts do not acknowledge that the study did not evaluate severe outcomes. Their claims about the vaccine’s effectiveness, therefore, are misleading and unsupported by the study’s findings.
Despite these claims, most Americans remain confident in the flu vaccine’s safety. KFF’s latest April Tracking Poll on Health Information and Trust shows that most of the public (74%) is at least “somewhat confident” in the safety of the flu vaccines. While majorities across partisans express confidence in the safety of the flu vaccines, Democrats are more likely than Republicans to say they are “very” or “somewhat confident” vaccines for the flu are safe (88% v. 68%).
Misleading Claims About HIV and PrEP Resurface Amid Preventive Care Challenge

Stigmatizing claims about HIV and PrEP, a medication that can be taken to prevent HIV, continue to circulate online, reinforcing barriers to prevention. Such rhetoric has resurfaced in response to the Supreme Court case Kennedy v. Braidwood Management last month. The case challenges the Affordable Care Act’s preventive services mandate, which requires PrEP (as a highly rated preventive service) be covered without cost-sharing for most people with private insurance.
In their filings, the plaintiffs argue that requiring insurers to cover PrEP violates their religious beliefs “by making them complicit in facilitating homosexual behavior, drug use, and sexual activity outside of marriage between one man and one woman,” and that it promotes “homosexual behavior, prostitution, sexual promiscuity, and intravenous drug use.” A 2021 scoping review published in AIDS and Behavior found that PrEP-related stigma is common, often focusing on judgments about having sex without a condom or having multiple sex partners. Such beliefs may contribute to low uptake: in 2023, only 31.3% of people aged 16 and older with indications for PrEP were prescribed the drug.
However, the body of research around PrEP use and sexual risk behaviors is mixed as limitations make it difficult to draw generalizable conclusions. A 2018 systematic review found no conclusive evidence that PrEP use leads to increased sexual risk behaviors. On the contrary, the review found that offering PrEP services provides an opportunity for at-risk populations to access sexual health care, testing, treatment, and counseling that they would not otherwise receive. Multiple studies have shown that when taken as prescribed, PrEP reduces the risk of acquiring HIV through sex by about 99% and through injecting drug use by at least 74%.
Polling Insight: A 2023 KFF poll found that about eight in ten adults (82%) say it would be more difficult to reduce the number of new HIV infections in the U.S. if PrEP were no longer required to be covered by insurance. The share who say PrEP no longer being covered will make it more difficult to reduce new HIV infections includes majorities across partisanship, and a majority of lesbian, gay, bisexual, and transgender adults.

In addition, most adults (76%) – including majorities across party and race and ethnicity — view HIV/AIDS as a serious issue in the U.S., and almost two-thirds of adults (63%) are not sure if people in the U.S. who need medication to prevent getting HIV are able to get it.
Fast Track Designation for Bird Flu Vaccine Contributes to Claims that Threat of Bird Flu is Manufactured

Online conversations about bird flu spiked on April 10 after a vaccine manufacturer announced that the FDA had granted Fast Track designation to its mRNA vaccine candidate. The designation is meant to speed up the development and review process for promising vaccines targeting major public health threats. In this case, it will help accelerate clinical trials for the vaccine, which began Phase 1 in November 2024 with federal funding.
The day before the announcement, a self-described news account with over 369,000 followers on X posted that Pfizer and Moderna were in talks with the government to develop bird flu vaccines. Although HHS had previously awarded $590 million to Moderna to support development, Pfizer has not received the same designation or funding. Still, among the more than 10,000 comments on the post, many of the most-engaged-with responses amplified the idea that preparing for a potential outbreak suggests the threat is exaggerated or manufactured. Others have misrepresented the meaning of “fast track,” falsely suggesting that the vaccine is being rushed without proper safety testing, when, in reality, the designation allows for more frequent communication with the FDA and eligibility for priority and rolling review—it does not mean safety protocols are bypassed.
AI & Emerging Technology
AI-Generated Messages Show Mixed Results in Correcting Vaccine Misinformation

A study from a researcher at the University of Michigan explored how generative AI can help public health communicators craft messages tailored to specific audiences. The experiment tested AI-generated corrections for vaccine misinformation, customized to match personality traits like extraversion or beliefs in pseudoscience. Participants rated their agreement with vaccine misbeliefs before and after receiving a correction, which was either AI-generated or drawn from real-world examples.
Messages tailored to extraversion performed as well as high-quality generic messages, especially among those who scored high in extraversion. But, messages aimed at people with strong pseudoscientific beliefs were ineffective and, in some cases, backfired, reinforcing skepticism. The study’s author concluded that while well-targeted AI-generated messages show promise, some messages may be counterproductive, underscoring the need for human oversight. The study adds to research examining the use of AI in public health communication. A 2023 systematic review in Journal of Medical Internet Research found that conversational AI tools can be effective in vaccine communication, especially when messages are personalized.
The findings highlight both the potential and limitations of using AI in public health messaging. KFF polling has shown that trust in AI-generated content remains low: most of the public (56%) – including half of adults who use AI — are not confident that they can tell the difference between what is true and false when it comes to information from AI chatbots.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.

The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Sign up to receive KFF Monitor
email updates
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The Public Good Projects (PGP) provides media monitoring data KFF uses in producing the Monitor.