At the start of each administration, U.S. presidents often use their executive authority to reorganize the federal government in ways that reflect their priorities, and in his second term in office, President Trump is no exception. The Trump administration’s actions include sweeping reorganizations and large-scale staff reductions at virtually every department in the federal government, including a “dramatic restructuring” within the U.S. Department of Health and Human Services (HHS) and changes at other agencies that have responsibilities for various aspects of the Medicare program.
Medicare, the program that provides health coverage to more than 68 million adults ages 65 and older and younger people with disabilities, is administered primarily by the Centers for Medicare & Medicaid Services (CMS), an agency within HHS, but a number of other federal agencies within and outside of HHS, such as the Social Security Administration, the U.S. Department of Justice, and the U.S. Department of Treasury also play key roles in supporting the operations of the Medicare program.
While both President Trump and Speaker Johnson have vowed to not cut Medicare benefits, it is not clear how the reorganizations, staff reductions, resignations and retirements, along with budget cuts within these federal agencies will impact the administration of the program, or have spillover effects on coverage and benefits for people with Medicare.
This brief highlights some of the key federal agencies and offices that play a role in making Medicare work and, to the extent possible, describes the recent staffing and organizational changes that could affect the operations of Medicare in the future, based on publicly available information. Data related to staff reductions are likely to be conservative to the extent that they do not take into account employees who resigned as part of the “Fork in the Road” deferred resignation program or other voluntary departures or resignations, including early retirements, leaving unfilled positions within their respective offices. The information may also not reflect some number of employees who were let go and then asked to return to work, and do not account for potential increases in staff if federal courts intervene.
Centers for Medicare & Medicaid Services (CMS)
CMS, a federal agency within HHS, administers the Medicare program. CMS functions as an insurance payer and regulator, implementing and enforcing laws that affect Medicare beneficiaries, health plans, and providers, including approximately 380,000 Medicare-certified providers (such as hospitals and skilled nursing facilities), 1.5 million physicians and non-physician practitioners, and dozens of private insurers offering Medicare Advantage and Part D drug plans.
Within the scope of its statutory authority, CMS sets provider payment rates, makes coverage decisions, and coordinates benefits for beneficiaries. Its Center for Medicare serves as the central office for these policies and operations. Through its Center for Clinical Standards & Quality, CMS develops and enforces quality and safety standards that providers must meet in order to participate in the Medicare and Medicaid programs. The agency also contracts with State Survey Agencies to enforce nursing home standards and, through its Center for Program Integrity, works on efforts to combat fraud and abuse—often in collaboration with other entities, such as the HHS Office of Inspector General and the Department of Justice.
Through its Innovation Center, CMS implements various health care and service delivery models designed to improve the quality and affordability of patient care and reduce health care costs. Additionally, through its Medicare-Medicaid Coordination Office, CMS works with states and other entities to coordinate and streamline the delivery of Medicare and Medicaid benefits for people with both types of coverage (known as dual-eligible individuals). Further, the CMS Office of Minority Health has undertaken efforts to advance health equity in Medicare and other programs, such as the rural health initiative.
CMS is also responsible for consumer information and protections, including managing the 1-800-MEDICARE helpline, distributing the Medicare & You handbook, and supporting the Medicare Beneficiary Ombudsman, which assists beneficiaries with complaints, grievances, appeals, and other Medicare-related inquiries.
Many of these CMS activities are subject to notice-and-comment rulemaking, a process that involves review by the White House’s Office of Management and Budget (OMB).
Recent staffing and organizational changes within CMS
According to a March 27, 2025 HHS document, CMS has reduced its workforce by 300 federal employees since the start of the Trump administration—about 4% of its staff. At the time, the agency did not clarify whether this figure includes employees who voluntarily accepted buyouts or elected early retirement. The Trump administration’s FY 2026 budget justification for CMS, released May 30, 2025, estimates 192 fewer full-time equivalent employees (FTEs) compared to FY 2025. The document acknowledges that these FTE levels are subject to change per the planned HHS reorganization.
While HHS has not publicly disclosed how these staffing reductions were distributed across CMS offices, media reports indicate that affected staff include those from the Medicare-Medicaid Coordination Office (about a third of its staff), Office of Minority Health (closure of the entire office), Office of Equal Opportunity and Civil Rights (entire office), and the Office of Program Operations and Local Engagement. Additionally, HHS eliminated half of its 10 regional offices—including those in Boston, Chicago, New York City, San Francisco, and Seattle—which serve 22 states and include CMS division offices. These regional offices enable HHS to maintain closer contact with state, local, and tribal governments in implementing HHS programs and policies, and develop and maintain partnerships with local organizations, including beneficiary coalitions and professional associations. According to an op-ed by HHS Secretary Robert Kennedy, their functions will be transferred to HHS’ remaining regional offices and staff in Washington D.C.
Further, the Trump administration proposes in its FY 2026 HHS budget to shift the 340B Drug Pricing Program from the Health Resources and Services Administration (HRSA) to CMS. The 340B Program requires drug manufacturers participating in Medicaid to provide discounts on outpatient prescription drugs to certain safety net providers that treat low income and uninsured patients.
Social Security Administration
The Social Security Administration (SSA) plays a central role in determining Medicare eligibility and enrolling individuals into the program. In 2021, SSA enrolled 3.8 million new Medicare beneficiaries, including one in seven (14%) who qualified for Medicare on the basis of receiving Social Security Disability Insurance benefits. SSA also handles automatic deductions of monthly Medicare Part B (and in some cases, Part D) premiums from Social Security benefit payments, and receives data from the Internal Revenue Service to determine income-related monthly adjustment amounts for higher-income beneficiaries.
SSA also provides support to low-income Medicare beneficiaries by processing applications for the Medicare Part D Low-Income Subsidy (also called “Extra Help”), which helps to cover Part D premiums and cost sharing for nearly 14 million Medicare beneficiaries with limited incomes and resources. The agency then sends Extra Help eligibility data to state Medicaid programs to initiate enrollment into the Medicare Savings Program, which helps to cover Medicare premiums and, in many cases, cost sharing, for more than 10 million low-income Medicare beneficiaries. Finally, SSA is responsible for processing name changes, and, along with CMS, can mail Medicare replacement cards. Disruptions to these administrative processes can affect beneficiary access to care, for example, by resulting in claims denials.
Recent staffing and organizational changes at SSA
The Social Security Administration announced plans to reduce its workforce by 7,000 federal employees (roughly 12% of its workforce) and to eliminate 6 of its 10 regional offices. According to the agency, the 7,000 employees will include a limited number of employees offered buyouts and voluntary retirement. In addition, the agency issued (and later rescinded) a proposal that would have reduced access to its national 1-800 number by requiring individuals, including those applying for Medicare, to verify their identities in person. This proposal prompted significant phone wait times and additional strain on the agency’s website, resulting in slowdowns and crashes, according to media reports. Although the proposal was withdrawn, it highlighted the potential negative implications of changes to the agency’s operations on older adults and people with disabilities, including Medicare beneficiaries.
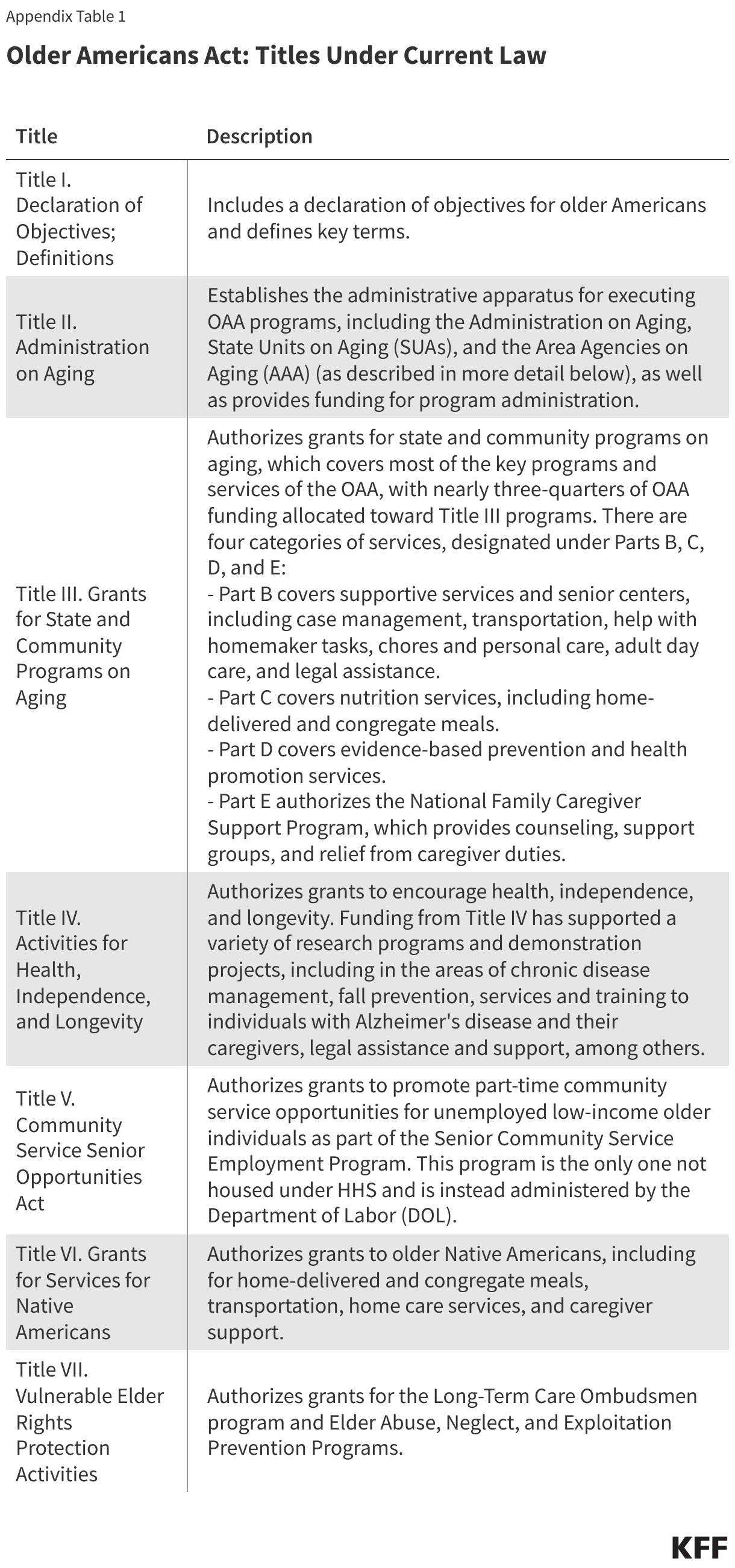
The Administration for Community Living (ACL): Through its Administration on Aging, ACL has administered programs under the Older Americans Act, a federal law that funds community social services for older adults, such as home-delivered and congregate meals, family caregiver support, the Long-Term Care Ombudsman program, and the National Center on Elder Abuse. Additionally, the ACL has administered:
- The State Health Insurance Assistance Program (SHIP), which provides one-on-one counseling, outreach, and education to Medicare beneficiaries. More than 4 million Medicare beneficiaries, their families, and caregivers received one-on-one counseling from SHIPs in 2022.
- The Senior Medicare Patrol program (SMP), which helps Medicare beneficiaries detect and report health care fraud, errors, and abuse. In 2023, 2 million people were reached through educational and outreach events under the SMP, with Medicare recovering more than $100 million in fraudulent claims (separate from recoveries under other fraud and abuse activities).
HHS announced that ACL will be dissolved, and the programs it administers will be absorbed into a newly-established Administration for Children, Families, and Communities. During the recent HHS staffing changes, four in 10 (40%) staff at ACL were either laid off or offered early retirement and buyouts to leave the agency, according to media reports.
The Assistant Secretary for Planning and Evaluation (ASPE): ASPE advises the HHS Secretary on various health policy matters, including analyzing issues to support the Secretary’s role as Trustee of the Medicare Trust Funds; supporting the Physician-Focused Payment Model Technical Advisory Committee; and providing analyses on several Medicare policy areas, including prescription drugs (e.g., the Medicare Drug Price Negotiation Program), federal spending on Medicare Advantage plans, and the impact of the CMS Innovation Center models and the Medicare Shared Savings Programs on Medicare spending and quality. Additionally, ASPE issues the annual U.S Federal Poverty Guidelines, which are used to determine eligibility for various federal programs including Medicaid, the Medicare Savings Program, and the Medicare Part D Low-Income Subsidy program.
HHS plans to merge ASPE with the Agency for Healthcare Research and Quality (AHRQ), the Office of Research Integrity, and the National Center for Health Statistics (formerly in the CDC) to create a new Office of Strategy. About 70% of ASPE’s 140 staff members have either been laid off or offered buyouts and early retirement during the recent staffing changes, according to reports in the media, but the President’s FY 2026 budget justification for HHS estimates 91 FTEs for planning and evaluation within the new Office of Strategy. AHRQ, which oversees the largest survey on U.S health care expenditures, including Medicare, and manages CAHPS, a set of survey tools used by Medicare Advantage and other plans to measure patient experience, reportedly laid off about half of its staff, according to media reports.
HHS Office of Inspector General: The HHS OIG is an independent body that oversees HHS’s programs with a focus on preventing and reducing waste, fraud, and abuse, including in Medicare. Its activities include auditing health care providers and grantees (e.g., reviewing diagnoses submitted by Medicare Advantage plans for use in CMS’ risk adjustment program), collaborating with the Department of Justice to operate the Health Care Fraud and Abuse Control Program (HCFAC), and enforcing penalties against entities that have been convicted of violations. In FY 2023, efforts by the HCFAC program returned nearly $1 billion to the Medicare Trust Funds.
At the HHS OIG, the Trump administration fired the former HHS Inspector General as well as other Inspectors General in January. It is unclear how many of HHS OIG’s 1,600 staff were laid off or accepted buyouts or early retirements during the recent HHS layoffs.
Newly-created Assistant Secretary for Enforcement: As part of the restructuring within HHS, a new Assistant Secretary for Enforcement has been created to oversee four existing offices: 1) Office of Medicare Hearings and Appeals, which handles disputes and appeals raised by Medicare beneficiaries and providers related to coverage and payments, 2) the Departmental Appeals Board, which provides a final administrative review of disputed Medicare claims, 3) the HHS Office for Civil Rights, which enforces various federal civil rights laws (e.g., the Age Discrimination Act) and HIPAA rules, and 4) the Office for Human Research Protections, which protects the rights of individuals who volunteer for biomedical and behavioral research. The Office of Medicare Hearings and Appeals currently adjudicates approximately 46,000 appeals annually, while the Departmental Appeals Board oversaw nearly 13,000 cases at the end of 2024.
Other HHS offices: In addition to the agencies and offices listed above, there are other offices that support Medicare operations, such as the HHS Office of the General Counsel, which provides legal counsel and supports enforcement and compliance functions in Medicare and other federal programs.
Other Federal Agencies Beyond HHS
The Department of Justice (DOJ): The DOJ supports Medicare in various ways, including representing and defending HHS in litigations, such as lawsuits challenging the Medicare drug price negotiation program and a case against Medicare Advantage plans alleging unlawful kickbacks and discrimination. Through its Health Care Fraud Unit, the DOJ enforces anti-fraud and abuse laws. In FY 2023, efforts by the Health Care Fraud and Abuse Control Program—a joint effort between DOJ and HHS OIG—resulted in nearly $1 billion transferred to the Medicare Trust Funds.
Additionally, the DOJ’s Antitrust Division, in coordination with the Federal Trade Commission, enforces federal antitrust laws that address anticompetitive practices among health care providers and within the Medicare Advantage program.
An internal memorandum proposes a major overhaul at the DOJ but does not mention changes or staffing reductions in the Department’s Health Care Fraud Unit or Antitrust Division.
The U.S Treasury Department: The U.S Treasury manages two trust fund accounts with $1 trillion in revenue that finance Medicare: the Hospital Insurance Trust Fund and the Supplementary Medical Insurance Trust Fund. In addition, the Internal Revenue Services (IRS), an agency within the Treasury Department, provides income data to the Social Security Administration to help determine income-related monthly adjustments for Medicare Part B and Part D premiums. The Treasury also helps to administer the Medicare Secondary Payer program, which outlines the circumstances in which private or other health insurance plans serve as the primary payer and Medicare acts as the secondary payer for beneficiaries with other forms of health insurance.
The Treasury Department is expected to eliminate approximately 20% of its workforce, according to a report submitted to the U.S. Office of Personnel Management (OPM) and obtained by the media. It is unclear whether, or how, these cuts would affect the oversight and investment of the Medicare Trust Funds.