VOLUME 25
Shifts in Funding Priorities and Vaccine Guidance Contribute to Safety Myths. Plus, Reactions to Ruling in U.S. v. Skrmetti
Summary
This volume examines how the U.S. government’s cancellation of $766 million in contracts with Moderna to develop pandemic flu vaccines, along with unfounded claims by new vaccine advisors, has contributed to the spread of persistent myths about the safety of mRNA technology. It also explores how shifting COVID-19 vaccine guidance and false claims are re-igniting misleading narratives about miscarriage. Lastly, it analyzes how reactions to a Supreme Court ruling upholding a state ban on gender-affirming care for minors further misconceptions and inflammatory language.
Recent Developments
Cancellation of mRNA Flu Vaccine Contract Leads to Renewed Safety Debate
The federal government’s termination of $766 million in contracts with Moderna for the development of vaccines against pandemic influenza viruses, including the H5N1 bird flu, has led to renewed conversation about the virus and debate about the safety of mRNA vaccines. Moderna said that its vaccine candidate against H5 avian flu had progressed through early clinical trials involving 300 healthy adults, with 97.8% of participants achieving protective levels of antibody titers three weeks after the second dose. A spokesperson for the Department of Health and Human Services (HHS) attributed the contract cancellation to “safety concerns,” falsely claiming that “mRNA technology remains under-tested,” even though mRNA vaccines for COVID-19 were tested in Phase 3 clinical trials involving more than 70,000 adults. Millions of doses have been administered worldwide, and monitoring data supports their strong safety profile. Despite this, administration officials have previously made broad, unfounded claims about the safety of mRNA vaccines, and several states are considering banning the technology.
KFF analysis of social media showed that mentions of mRNA vaccines increased on May 29, the day after the contract cancellation, appearing more than twice as often as the daily average over the previous two weeks. Online reaction was divided, with some users expressing concern over public health risks while others celebrated the cancellation as a stand against pharmaceutical companies. The most-engaged-with post, from a commentator with more than 1.4 million followers on X, said, “No more blank checks for big Pharma to run experiments on the American people!” Several posts amplified misleading narratives about the safety of mRNA vaccines, with one account with over 900,000 followers and medical credentials in their biography writing, “Americans are done funding failed mRNA experiments that enrich pharma giants and endanger public health.” The most viral posts combined distrust of pharma with vaccine skepticism, which is a familiar pairing in high-engagement misinformation.
Polling Insights: KFF’s April Tracking Poll on Health Information and Trust found that mRNA technology is obscure to much of the public, including partisans. Overall, about one-third (32%) of U.S. adults say vaccines that use mRNA technology are “generally safe” – twice the share of those who say they are “generally unsafe” (16%). However, half (52%) of adults say they do not know enough about mRNA technology to say whether it is safe or not. While Republicans and independents are much more likely than Democrats to say mRNA vaccines are “generally unsafe,” most Republicans (61%) and roughly half of independents and Democrats report not knowing enough about this technology to say.

Unfounded Claims About Spike Protein May Cause Confusion About mRNA Vaccine Safety
Misconceptions about mRNA vaccines continue, as people express uncertainty about how these vaccines impact their health long term. One common concern is that the spike protein produced by the COVID-19 mRNA vaccine is toxic and can cause damage to a person’s organs. mRNA vaccines for COVID-19 trigger an immune response by instructing cells to create the spike protein found on the surface of the SARS-CoV-2 virus, but the spike proteins created by the vaccine are not toxic and are quickly degraded by the body. Studies have not found evidence that the spike proteins created by vaccines damage organs. Still, the claim has been spread by health officials, including new members of the federal Advisory Committee on Immunization Practices (ACIP). One new appointee to the group, which advises the Centers for Disease Control and Prevention (CDC) on immunization schedules and recommendations for the public, has previously falsely claimed that the spike protein can cause “permanent damage” in children’s organs and that mRNA vaccines can cause cancer or a form of AIDS. Other new members have made similar unfounded statements about mRNA safety, with one writing, “The evidence is mounting and indisputable that mRNA vaccines cause serious harm including death, especially among young people.”
The claims reflect broader public misconceptions. In the 30 days leading up to June 20, approximately 66% of social media posts identified by KFF that mentioned the spike protein in COVID-19 vaccines referenced safety, while 21% discussed potential toxicity. Beyond public perception, the misconceptions held by ACIP appointees can impact the CDC’s immunization recommendations and, therefore, which vaccines are covered at no cost by insurance providers.
Polling Insights: KFF’s April Tracking Poll on Health Information and Trust found that about nearly half (45%) of the public report having heard the false claim that mRNA vaccines can alter your DNA, and while few think this myth is “definitely true,” most express uncertainty. Overall, just 3% of adults say it is “definitely true” that mRNA vaccines can change your DNA with much larger shares (24%) saying this is “definitely false.” However, most adults fall in a malleable middle category, saying this claim is either “probably true” (26%) or “probably false” (45%).
The share who believe or lean toward believing this myth differs across partisans, with Republicans and independents each about twice as likely as Democrats to say it is “definitely true” or “probably true” that mRNA vaccines can change your DNA (37% of Republicans and 33% of independents v. 13% of Democrats).

Miscarriage Myths Reemerge as HHS Changes COVID Vaccine Recommendations

Misleading reports of fetal loss following COVID-19 vaccination are contributing to concern over the safety of the vaccine for pregnant people. A 2024 meta-analysis published in BMJ found no increased risk of adverse pregnancy or perinatal outcomes following vaccination during pregnancy. In fact, vaccination reduced the risk of hospitalization with COVID-19 during pregnancy by 94%. However, false claims made by a Florida OB-GYN during a May 21 Senate subcommittee hearing have further fueled these concerns. The doctor repeated the debunked narrative that a 2021 study in The New England Journal of Medicine showed an 82% miscarriage rate following COVID-19 vaccination, but his interpretation only included people who were vaccinated in their first or second trimesters and reported completing their pregnancies by the time of follow-up interviews three months later. The actual study found a miscarriage rate of 12.6%, in line with the prevalence of miscarriage in all known pregnancies.
The testimony caused large spikes in social media posts linking COVID-19 vaccines to miscarriage. One account with more than 1.7 million followers posted video of the testimony and repeated the doctor’s false claim that the COVID-19 vaccine functions like abortion medications. Although mentions of miscarriage or fetal loss make up a small portion of overall COVID-19 vaccine conversations, of those that do mention it, the most-engaged-with content amplifies the false claim that the vaccine causes miscarriage in up to 80% of pregnancies. Following the testimony, HHS announced that the CDC would no longer recommend COVID-19 vaccines for healthy children or pregnant people, again citing misleading studies to support the policy shift. Reactions to the HHS announcement were mixed, with some on social media calling for more by banning COVID-19 for all people. Others expressed fear about how this may impact vaccine availability for those who chose to be vaccinated, as the CDC no longer recommends COVID-19 vaccination during pregnancy but still lists pregnancy as a high-risk underlying condition.
Misconceptions and Inflammatory Language Follow Supreme Court Ruling on Gender-Affirming Care

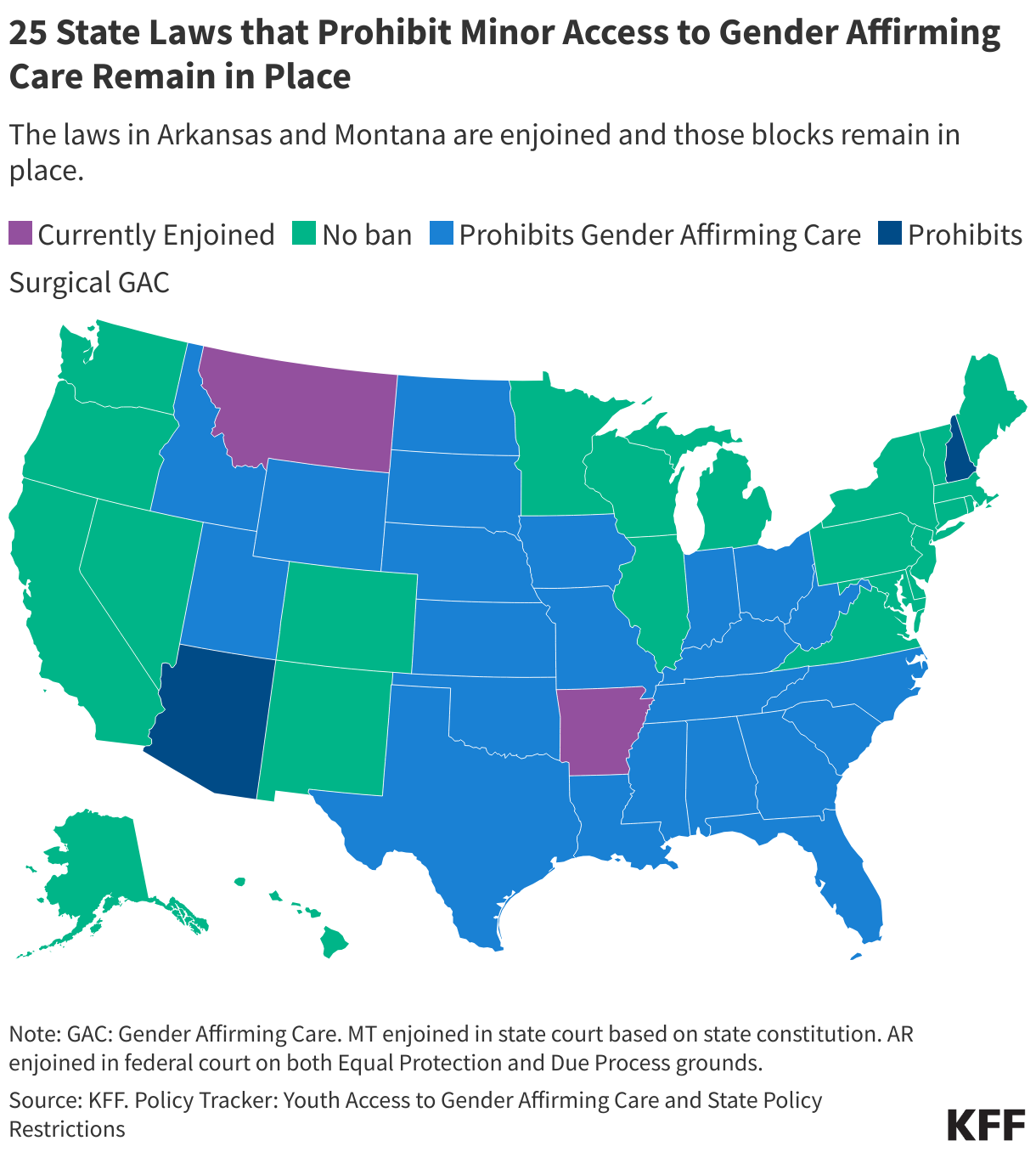
The June 18 Supreme Court’s decision to uphold a Tennessee law banning gender-affirming care for minors led to one of the largest spikes in news reports and social media conversations about gender-affirming care in 2025 thus far. Many of the posts repeated misconceptions about gender-affirming care that underlie most similar bans, including the inaccurate belief that it is experimental or lacks sufficient evidence. In reality, many of the medical treatments involved, like puberty blockers and hormone therapies, have been used safely for decades in cisgender children and adults to treat conditions including delayed and precocious puberty. U.S. medical associations, including the American Medical Association, American Academy of Pediatrics, and the American Psychological Association, support youth access to gender-affirming care, pointing to evidence that such care improves mental health outcomes for transgender youth. Research has found gender-affirming medical interventions to be associated with lower odds of depression and suicidality.
Posts also frequently used emotionally charged language to evoke fear, inaccurately referring to gender-affirming care as “mutilation,” “castration,” or “maiming,” and comparing it to female genital mutilation. Female genital mutilation includes non-medical procedures recognized as human rights violations. In the last 30 days, as of June 20, approximately 12% of social media posts about gender-affirming care identified by KFF included such terms, up from 7% in the previous 30 days. One podcaster with 3.7 million followers celebrated the ruling on X, calling it “a fatal blow to the child mutilation industry,” while Attorney General Pam Bondi said the decision “allows states to protect vulnerable children from genital mutilation.” Mentions of these terms previously spiked on June 2, after the Federal Bureau of Investigation (FBI) asked the public to report providers who they said “mutilate” children by offering gender-affirming surgery to minors.
The use of such language can suggest violence or harm and has been used in unsubstantiated claims that schools or healthcare providers are providing transition-related care without parental knowledge or consent. In reality, the most common forms of transition, especially for minors, are non-medical, such as altering clothing, hairstyle, or pronouns to better fit their gender identity. When medical interventions are pursued, they are consensual, medically supervised, and evidence-based treatments. Surgical interventions are relatively uncommon among adults and very rare among minors. One study of more than 22 million youth found that fewer than .01% of transgender and gender diverse adolescents ages 13 to 17 underwent gender-affirming surgery, and none under 12 received such care.
AI & Emerging Technology
AI Usefulness in Diagnostics May be Limited by Human Interactions

While previous research has shown artificial intelligence chatbots to be capable of passing the United States Medical Licensing Exam, a new study from researchers at the University of Oxford highlights that human interactions with these tools may limit their accuracy and usefulness. Researchers tested whether large language models (LLMs) could help members of the public correctly identify health conditions and determine a course of action in 10 common medical scenarios. They found that when performing alone, the LLMs correctly identified conditions in 94.9% of cases. But, real people using the same models identified relevant conditions in only 34.5% of cases, underperforming a control group that did not use the AI chatbots.
The researchers examined the transcripts of participant interactions with the chatbots, observing cases where the participants provided incomplete information and where the LLMs misinterpreted prompts. They noted that the AI models often provide users with 2-3 different possible options, allowing users to have the final decision, and that at least one of the suggested conditions was relevant in at least 65.7% of conversations with participants. Since users performed poorly at making the correct choice, the study authors suggested that the usefulness of LLMs could be improved by including explanations, structured outputs, or clear recommendations. Despite AI’s strong performance on medical benchmarks and in controlled scenarios, misunderstandings between human users and chatbots could amplify confusion or lead to misdiagnoses. The researchers recommend involving human users in safety testing prior to the deployment of these tools in clinical settings.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.

The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Sign up to receive KFF Monitor
email updates
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The Public Good Projects (PGP) provides media monitoring data KFF uses in producing the Monitor.