KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
On May 14, 2026, the U.S. Supreme Court blocked a lower court order in Louisiana v. FDA that would have restricted the nationwide distribution of mifepristone. The Court’s action leaves current FDA rules in place, allowing the drug to be prescribed via telehealth and dispensed by mail or at retail pharmacies while the litigation continues, pending a final decision by the Supreme Court.
Medication abortion—most commonly a two-drug regimen of mifepristone and misoprostol—has become a central legal battleground in the years since Dobbs v. Jackson Women’s Health Organization. Over 25 years ago, the U.S. Food and Drug Administration (FDA) approved mifepristone, along with a requirement that the drug be dispensed in person by a physician. In 2023, after reviewing research that continued to demonstrate its safety even when dispensed through telehealth, the FDA eliminated the requirement that the drug be dispensed in person, enabling the drug to be mailed or dispensed by retail pharmacies. This change has allowed clinicians to dispense the drug via mail and enabled tens of thousands of patients to access medication abortion in states where the provision of abortion is outlawed.
Multiple lawsuits filed after 2022 have focused specifically on the FDA’s role in regulating mifepristone: whether the agency can set conditions of use through its Risk Evaluation and Mitigation Strategy (REMS), whether courts can override the agency’s scientific and administrative judgments, and how state abortion bans interact with federal drug regulation. In 2024, the Supreme Court ruled in Alliance for Hippocratic Medicine v. FDA, that a group of doctors, associations and organizations that oppose abortion lacked legal standing to challenge the FDA’s approval of mifepristone, but did not reach the merits of their claims.
Three state-led lawsuits are now claiming that FDA policy enabling remote prescribing and mailing of mifepristone harms states by undermining their abortion restrictions and generating downstream costs. Several provider- and organization-led cases argue the opposite: that FDA restrictions – which allow mifepristone to be mailed, but only through certified prescribers and pharmacies — remain unlawfully burdensome given the drug’s safety record. This brief reviews the case now before the Supreme Court, Louisiana v. FDA, provides an overview of the other pending litigation involving mifepristone, and the mounting tension between states seeking to protect abortion and states banning the provision of abortion.
Overview of the Case
In October 2025, Louisiana filed a lawsuit against the FDA claiming the agency violated the Administrative Procedure Act (APA) when it approved the 2023 REMS for mifepristone. Louisiana also claims that the 2023 REMS violates an 1873 anti-obscenity law, the Comstock Act, which prohibits the mailing of any medication used for abortion. The 2023 REMS no longer required that the drug be dispensed in person to patients and enabled the medication to be mailed or dispensed at retail pharmacies like most prescription drugs. The state of Louisiana alleges that this revised dispensing requirement has harmed the state and interferes with their ability to regulate abortion in their own state (Louisiana bans the provision of abortions). The Trump Administration defended the FDA and said that an internal review was already underway to examine the 2023 approval decision and the medication’s safety record in light of the updated dispensing policies. In April 2026, the U.S. District Court for the Western District of Louisiana paused the litigation for six months to give the FDA time to continue its review of the drug’s safety. Louisiana appealed this decision to the 5th Circuit Court of Appeals.
On May 1, 2026, a three-judge panel of the U.S. Court of Appeals for the Fifth Circuit granted Louisiana’s request to roll back the FDA rules that enabled remote prescribing, mailing and retail pharmacy dispensing while the appeal proceeds. This decision, which required mifepristone to be dispensed only in person, took effect immediately with implications for abortion access nationwide, not just in states where abortion is banned. That evening Danco Laboratories, one of the drug manufacturers and an intervenor-defendant, filed an emergency motion asking the Fifth Circuit to pause its decision for one week to allow them time to appeal to the U.S. Supreme Court. The following day, after the Fifth Circuit did not respond to Danco’s motion, Danco and GenBioPro (another mifepristone manufacturer) filed emergency appeals to the Supreme Court. Justice Alito granted a one-week administrative stay of the Fifth Circuit’s decision.
On appeal the Supreme Court will first consider whether the Plaintiffs have legal standing to bring this case; without legal standing, the case does not proceed. Both the district court and the Fifth Circuit Court of Appeals found Louisiana has legal standing because it has shown injury caused by the FDA’s 2023 REMS that can be alleviated by a court decision. However, in a similar case, Alliance for Hippocratic Medicine v. FDA, the Supreme Court ruled that a group of doctors and health providers did not have standing for multiple reasons including that they could not show a concrete injury resulting from the updated FDA mifepristone dispensing requirements.
In this lawsuit Louisiana asserts that the policy of allowing mifepristone to be mailed has harmed the state’s ability to enforce its abortion ban and has caused the state to spend state Medicaid funds on patients who took mifepristone received by mail and then needed emergency care for complications. Specifically, “Louisiana identifies $92,000 it paid in Medicaid costs from two women who needed emergency care in 2025 from complications caused by out-of-state mifepristone.”
The FDA, and the drug manufacturers (GenBioPro and Danco), claim that Louisiana has failed to show legal standing. The FDA regulates drugs and has no oversight over states or providers. They assert that the FDA’s 2023 REMS does not implicate the State’s sovereign “power to create and enforce a legal code.” The Defendants further argue that Louisiana’s alleged Medicaid-based economic harm is too “attenuated” to establish standing, suggesting Louisiana cannot show that the FDA’s policy of allowing mifepristone to be mailed led to their alleged economic harm. Patients could obtain mifepristone out of state, bring it back to Louisiana, and suffer the same complications, they argue.
The Defendants (the FDA, Danco and GenBioPro) assert that if Louisiana is granted standing in this case, a state could challenge any federal policy alleged to have caused a visit to a doctor or a hospital for which the state pays the bills. The Defendants cite to the examples the Supreme Court provided in the decision denying the Alliance for Hippocratic Medicine standing: “EPA roll[ing] back emissions standards for power plants,” “[a] federal agency increas[ing] a speed limit from 65 to 80 miles per hour,” and the federal government “repeal[ing] certain restrictions on guns.”
The FDA’s Tightrope Walk—Defending Agency Authority While Not Defending the 2023 REMS
The FDA’s posture in this case and the related litigation has been complicated by the transition from the Biden administration, which embraced reproductive rights, to the Trump administration, which supports abortion restrictions. The agency is defending the lawsuits. But, after pressure from anti-abortion organizations and state attorneys general, in September 2025, the FDA announced it was conducting a comprehensive review of mifepristone, including the 2023 REMS. When announcing the review, the FDA wrote, “HHS’s decision to do so is informed by the lack of adequate consideration underlying the prior REMS approvals, and by recent studies raising concerns about the safety of mifepristone as currently administered.” The Fifth Circuit relied on that statement in its ruling, finding that the FDA conceded in the September 2025 letter that it did not comply with the Administrative Procedures Act when removing the in-person dispensing requirement.
The Trump administrations FDA position contrasts with the administrative record underlying the FDA’s 2023 REMS decision, which shows the FDA’s removal of the in-person dispensing requirements was grounded in more than two decades of experience with mifepristone. The 2023 analysis included: its 2021 review of published literature; safety information submitted during the COVID-19 pandemic; more than five years of adverse data; a separate one-year assessment report for the REMS; and information provided by advocacy groups, individuals and manufacturers. The FDA found that all this information supported the safety of the REMS modification in 2023. The FDA further found there were “no new safety concerns” related to the removal of the in-person dispensing requirement. It therefore concluded that, “[r]emoving the in-person dispensing requirement will render the REMS less burdensome to healthcare providers and patients and provided all other requirements of the REMS are met, including the additional requirement for pharmacy certification, the REMS will continue to ensure that the benefits of mifepristone for medical abortion outweigh the risks.”
Enforcement of a Court Decision Directed at the FDA
A court order to rescind the 2023 REMs would again require in person dispensing, resulting in regulatory pressure on Mifepristone manufacturers (Danco, GenBioPro and Evita Solutions) to ensure that providers certified to dispense mifepristone comply with a court order, and only dispense the medication in person. Furthermore, it is unprecedented for a federal court to compel the FDA to modify the REMS for an approved medication and could potentially undermine the agency’s authority to determine and regulate drug safety.
Even if the Court suspends the FDA’s policy of dispensing mifepristone by mail, that will not end the use of telehealth in the provision of medication abortions. Some clinics and providers will respond by switching to a misoprostol-only regimen. While this single drug regimen is less effective (approximately 80-100% depending on the regimen and pregnancy duration) than using the highly effective mifepristone and misoprostol regimen (between 91.9 to 99.7% depending upon the gestational duration and route or interval of misoprostol administration) it is still a demonstrated protocol that is used in many countries. While misoprostol alone is effective, it can also cause abortion patients to experience more side effects, including greater pain, bleeding, and gastrointestinal effects than the regimen with mifepristone and misoprostol combined.
Conflict Between States
Interstate Conflict and the Rise of Shield Laws
Many states that are protective of abortion rights have implemented so-called “shield laws.” These laws are designed to protect telehealth providers prescribing and mailing mifepristone in their state from criminalization across state lines. As GenBioPro and Danco highlight in their appeals to the Supreme Court: “Louisiana’s filings below made clear—the alleged frustration of Louisiana’s laws occurs because other “states have enacted ‘shield laws’ to protect medical practitioners in their states from extradition for prescribing” mifepristone. This difference in state policies is yet again a natural result of this Court “return[ing]” abortion policy to the states,” in the Dobbs ruling.
Under shield laws, in June 2025approximately 55% of telehealth medication abortions were provided to people living in states with abortion bans or telemedicine bans according to the #WeCount project of the Society of Family Planning. That month, 45% of telehealth medication abortions were mailed to patients in states without restrictions reflecting the uneven availability of abortion even in states where abortion is not restricted. Texas and Louisiana have attempted to prosecute or fine telehealth providers in California and New York but have been blocked by shield laws.
New State Laws Regulating Mifepristone
Beyond regulating abortion generally, states have implemented new laws specifically targeting medication abortion. These laws often prohibit the prescription, dispensing, or mailing of abortion-inducing drugs within state borders, and in some instances impose criminal penalties on providers. Such measures operate in direct tension with the FDA’s policy set forth in the REMS for mifepristone. For example, Mississippi recently passed a new law (effective July 1, 2026) that makes it unlawful to manufacture, distribute, dispense or prescribe abortion medication. Anyone who violates the law may face civil liability and up to 10 years in prison. Louisiana has enacted a law that classifies mifepristone and misoprostol as controlled substances, which limits the appropriate storage and dispensing; however, this law is currently being challenged in state court. Texas also passed a new law that allows private citizens to sue individuals or entities that provide, mail, or transport abortion medication to or from Texas.
Proposed Federal Bills and Investigations
Dissatisfied with the pace of the FDA review, Senator Josh Hawley, an anti-abortion leader, has introduced a bill that would rescind the FDA’s approval of mifepristone. He has also launched an investigation into mifepristone manufacturers Danco Laboratories and GenBioPro seeking information about adverse events associated with the drug, claiming that the drug is risky based on the results of the same study cited by HHS officials. In April 2026, Indiana Senator Jim Banks sent a letter to the Federal Trade Commission Chairman urging the Commission to investigate abortion drug manufacturers for allegedly engaging in deceptive trade practices and promoting misleading safety claims.
Other Cases Involving the FDA and Medication Abortion
In recent years, courts have issued conflicting rulings on the FDA’s 2023 decision to eliminate the in-person dispensing requirement. (Table 1) In July 2025, a federal court in Washington upheld the REMS revisions, while in October 2025, a federal court in Hawaii (Purcell v. Kennedy)ruled that the FDA violated the Administrative Procedure Act, “by failing to provide a reasoned explanation for its restrictive treatment of the drug ”when it maintained restrictions on access to mifepristone in 2023. The court has ordered the FDA to review evidence it allegedly overlooked including, “the wealth of peer-reviewed evidence proving mifepristone’s safety, including when delivered by telemedicine as well as how FDA’s restrictions burden patient access.”
Additional lawsuits underway brought by states, Missouri, Idaho, Kansas, Florida, and Texas, also challenge either the FDA’s original approval or subsequent modifications to the REMS. Florida and Texas have agreed to pause their litigation while the FDA continues its internal review.
Whole Woman’s Health Alliance, an independent abortion provider in Virginia with other independent abortion providers in Montana and Kansas, filed a lawsuit (Whole Woman’s Health Alliance v. FDA) against the FDA in May 2023, asserting that the FDA violated the Administrative Procedure Act when imposing REMS on mifepristone. The lawsuit seeks to remove all the REMS for mifepristone. This case is ongoing, and the Plaintiffs have opposed a stay to allow the FDA to continue its internal review.
Separate litigation is also testing whether the FDA’s regulation of mifepristone preempts state restrictions. In GenBioPro v. Raynes (West Virginia), GenBioPro challenged the state’s near-total abortion ban; in July 2025, the Fourth Circuit affirmed dismissal of the case, holding that the FDA’s mifepristone policies do not preempt West Virginia’s ban. In a second case, brough in North Carolina, Bryant v. Stein(formerly Bryant v. Moore), a physician argues that the FDA’s dispensing framework for mifepristone preempts additional state-law restrictions—on the theory that the FDA considered more stringent limits on mifepristone and chose not to adopt them, so states may not impose those same restrictions. There is a Louisiana state court challenge brought by Birthmark Doula Collective to Louisiana’s law which classifies mifepristone and misoprostol as controlled substances, subjecting these medications to controlled-substance storage, prescribing and dispensing rules. This case tests whether a state can use controlled-substance classification to restrict access to medication.
Looking Ahead
The return of mifepristone to the Supreme Court underscores how many questions remain post-Dobbs about how state authority to regulate abortion intersects with federal authority to regulate drugs. In Louisiana v. FDA, the immediate question before the Court is whether Louisiana has legal standing to challenge FDA’s 2023 REMS. Justice Alito issued an administrative stay of the Fifth Circuit’s decision until May 11, 2026. How the Supreme Court handles the emergency appeal once that stay expires will determine whether the rollback of the 2023 REMS remains in effect while the case proceeds and will signal how the Supreme Court views deference to the FDA on matters of drug approval and safety.
While the Supreme Court considers this case, related lawsuits are pulling in opposite directions—other state-led challenges also seeking to restore the in-person dispensing requirement for mifepristone, provider-led cases arguing the current REMS are unlawfully burdensome, and preemption cases testing whether states can restrict an FDA-approved drug. At the same time, state shield laws offer protections to providers who prescribe and mail medication abortion to patients in states with abortion bans, intensifying interstate conflict and raising new questions about enforcement and jurisdiction.
Rapid technological developments in artificial intelligence (AI) have resulted in growing public attention to the potential benefits and challenges of these developments as they relate to health care. The Trump administration recently released A National Policy Framework for Artificial Intelligence (“AI Framework”), a set of legislative recommendations that could jump-start congressional activity on the application of AI across a variety of policy areas, not just health care. A core part of the AI Framework emphasizes establishing federal AI policy that preempts many state AI laws to reduce barriers for deploying AI applications. Preemption could nullify state consumer protections governing the use of AI in health coverage, such as prior authorization, and claims review and appeals. This Issue Brief discusses the types of consumer protections for use of AI in prior authorization and claims review, describes the Trump administration’s AI Framework, and highlights areas to watch as Congress considers AI legislation.
Use of AI in Prior Authorization and Claims Review
The use of AI technology has been embraced by all participants in the claims review cycle: patients, providers, and insurers. The box below describes current uses of AI technology for each party involved in prior authorization and claims review. Prior authorization and claims review are related but distinct steps in the coverage review and reimbursement process (claims review cycle) where AI might be used. Prior authorization is a managed care tool that evaluates whether an item or service is covered by a health plan prior to a patient’s receipt of the care. Claims review is often associated with a determination by an insurer after care is provided about whether and how much to pay for the item or service. Both involve similar decision-making and consumer appeal rights.
The claims review cycle includes health plan decisions made before a patient receives care (prior authorization review), after the care is received (often called retrospective or post-claim review), and while a patient is receiving the care (called concurrent review). Where the medical necessity of a service is involved, the term “utilization review” is often used to describe this process (definitions differ across state and federal requirements).
Parties Involved in the Prior Authorization and Claims Reviews Process and Their Use of AI
Insurers
Health insurers and other third-party administrators (TPAs), such as pharmacy benefit managers (PBMs), use some form of automation to process the millions of health care claims they review each year. Automation broadly includes the use of algorithms. One definition describes algorithms as a “procedure or set of rules that is applied to a dataset to achieve a certain function or purpose.” Such algorithms, or decision trees, have been used to generate approvals for treatment and have existed in the health care administration for some time.
AI has gained attention in recent years for its use to improve the speed and efficiency of existing automated processes, learn from historical claims outcomes (i.e., claims information an insurer has from its enrollees), and predict coverage determinations based on past patterns. Technology companies are vying for insurers and TPAs to adopt their AI-related products with the promise of faster, more accurate claims review. According to a recent National Association of Insurance Commissioners (NAIC) survey of 93 insurance companies in 16 states, 84% of responding insurers across health care insurance product lines use AI or machine learning for a broad range of tasks such as utilization management practices, disease management programs, and prior authorization processes.
Health Care Providers
Providers—hospitals and clinicians—use AI to enhance their ability to prepare and submit health insurance claims for reimbursement from insurers and TPAs. AI tools are being added to health system “revenue cycle management” (RCM)—the processes used to manage health system financial operations and improve functions such as coding, insurance eligibility checks, and billing. For example, generative AI allows clinicians to create patient encounter summaries (using ambient scribes) that are automatically included in the patient’s electronic health record and moved across interoperative systems and generate content to accelerate the prior authorization and claims review process. The use of AI to create electronic records of patient visits can also allow providers to maximize payments for services by assigning billing codes that command higher rates.
Patients
These same AI systems can assist patients (and their doctors) in appealing a prior authorization or claim denial by, for example, using a patient’s medical information, health plan documents, and clinical guidelines to generate appeal letters and other documentation needed in the appeal process. Various entities are promoting these tools directly to patients; some services charge a fee, and others do not. In addition, recent efforts to enhance data interoperability have encouraged the industry to develop apps that patients can use to consent to the sharing of their health information for multiple purposes, including to help with prior authorization review.
Connection to Interoperability. Developments in technologies to enhance interoperable systems (electronic data sharing among plans, providers, and patients) may make data more readily available for the application of AI technology in prior authorization and claim decision-making. Federal regulations will soon require some health plans to implement application programming interfaces (APIs) to collect and share data among patients, plans, and providers in an effort to streamline and expedite prior authorization review. While this may be helpful to patients and providers, increased data sharing could also result in data being captured inappropriately and used for purposes that might not be allowed under current interoperability agreements, for example, for commercial sale and/or to train new AI tools.
Risks to consumers include the potential for inaccurate or biased outcomes and privacy breaches. AI systems can help insurers and TPAs triage and make coverage decisions, often without any human involvement in the process. Yet the nature of much of this decision-making requires an individualized, sometimes clinical, review of a patient’s unique circumstances. The use of an AI-based algorithm to aid in these decisions may limit full review of a claim when no human judgment is applied. Many insurers made a voluntary pledge in 2025 to have medical professionals review prior authorization denials that involve clinical issues. Still, the use of AI by an insurer or TPA in claims review, even for purely administrative, nonclinical tasks, might lead to incorrect predictions and decisions if the AI model’s data input is incorrect or missing key information. In the past few years, patients have brought class action lawsuits challenging the use of specific algorithms in claims denials, arguing that their denials were improper due to a failure to perform an individual assessment and a lack of transparency about the algorithms and underlying data used to train the AI tool. These cases are still moving through the courts.
Data used in AI tools, either obtained through a patient’s electronic medical record or uploaded by the patient, could create privacy and security risks that may not be protected under the Health Insurance Portability and Accountability Act of 1996 (HIPAA). HIPAA applies only to health plans, health care providers, and health care clearinghouses, not to the technology companies and other third-party entities that access health information. Patient information obtained through an interoperable electronic health records (EHR) system has been the topic of recent litigation, with an EHR technology company claiming that another company obtained patient data under false pretenses and sold it.
Furthermore, the reliability of an AI tool can be compromised when trained on biased data. For example, one study found that algorithms using health care costs as a proxy for health care needs greatly underestimated the needs of Black patients compared to White patients. Health care costs are often lower for Black patients because they have less access to care, not because they have less clinical need. In this case, treatment decisions based on such algorithms may exacerbate health disparities.
The Trump Administration’s AI Framework
Promoting AI development. While the Trump administration’s AI Framework contains few details and no recommendations specific to health care or insurance claims review, it broadly recommends expanding the use of AI and imposing only limited federal restrictions through existing agency structures and “industry-led standards.” For example, the AI Framework recommends legislation that would prevent the U.S. from “coercing technology providers, including AI providers, to ban, compel or alter content based on partisan or ideological agendas.” It also recommends that Congress authorize resources to make federal datasets accessible to “industry and academia” for training AI systems.
Preempting some state law protections while keeping others. A prominent part of the AI framework is its proposal that Congress develop national standards that preempt “cumbersome” state AI laws. This would create federal legislation that aims to stop or prevent these state laws from being implemented. The Administration suggests that these state laws result in a patchwork of different requirements that could restrict U.S. competitiveness. The AI framework also says that states should not be allowed to penalize AI developers for a third party’s “unlawful conduct” involving their models.
At the same time, the Administration recommends that any legislation “respect the principles of federalism” and not preempt traditional state policy power that allows states to enforce general state laws against AI developers and users, including laws to “protect children, prevent fraud, and protect consumers.”
This framework is consistent with earlier Trump administration actions, including a December 2025 Executive Order restricting state AI regulation and establishing a Department of Justice litigation task force to challenge state AI laws that conflict with federal policy. A July 2025 AI Action Plan (stemming from another Executive Order) included a recommendation that federal agencies not allow AI-related federal funding to states with “burdensome AI regulations.” The AI Action Plan was released shortly after congressional Republicans’ unsuccessful attempt to include a 10-year ban on state regulation of AI in the 2025 budget reconciliation law.
Significantly changing the previous administration’s policies. The Trump administration’s actions mark a significant shift in priorities and approach to AI policy from those of the Biden administration, which sought to establish federal safeguards for the use of AI in health care. The Trump administration rescinded a Biden-era Executive Order that set out an agenda for the development and use of AI “to protect American consumers from fraud, discrimination, and threats to privacy” and “promote safe and responsible” use in health care.
Federal and State Efforts to Regulate AI Use in Prior Authorization and Claim Review
Federal Regulation and Oversight of AI
Few federal standards apply specifically to the use of AI in the prior authorization and claims review process, but all coverage decision-making for both public and private coverage includes general standards intended to ensure reviews are fair, substantive, and timely. These standards are fragmented across federal agencies with separate oversight responsibilities for different health coverage markets.
For private employer-sponsored plans, the federal government, through the U.S. Department of Labor (DOL), oversees claims and appeals process requirements in the Employee Retirement Income Security Act (ERISA). ERISA generally exempts self-insured plans established by private employers from most state insurance laws, including claims review protections, and would likely preempt state AI laws that relate to the claims review process. Most workers with employer-sponsored insurance are in a self-funded plan, meaning that many consumers are not guaranteed state protections related to the use of AI in claims review, where they exist.
These ERISA claims and appeals rules were the basis for reforms applied across all private health coverage in the Affordable Care Act. These reforms established a federal floor of protections for the internal claims and appeals process for those with Marketplace and off-Marketplace private insurance and added an option for all consumers with private coverage to appeal denied claims through an “external review” by an entity independent of the plan.
ERISA requires all employer plan sponsors to ensure the “full and fair” review of all health claims. What “full and fair” means in the context of the use of AI tools in the claims process is yet to be interpreted through guidance or updated regulation. ERISA also contains “fiduciary” rules requiring employers and other fiduciaries to act in the best interest of plan enrollees and monitor vendors’ activities. While these standards might provide some protection to employees related to an employer plan’s use of AI, in practice, fiduciary standards have rarely been applied to employer health plans, and to date, enrollees have not been successful in advancing litigation to challenge employers for breaching their fiduciary duties related to the health plans they sponsor.
Still, one recent DOL case against a large TPA alleged a fiduciary violation and a failure to follow ERISA claims rules when the TPA automatically denied claims in bulk without making an individual medical necessity evaluation for each under the terms of the plan. While these allegations did not necessarily involve AI, the TPA allegedly used an automated process without human review to issue denials. This case was settled with the establishment of a fund to compensate enrollees for improperly denied claims.
Federal guidance specific to AI use in prior authorization and claims review in Medicare and Medicaid has been limited. Both programs have their own claims and appeal consumer protections under federal requirements (and some state standards also apply to Medicaid).
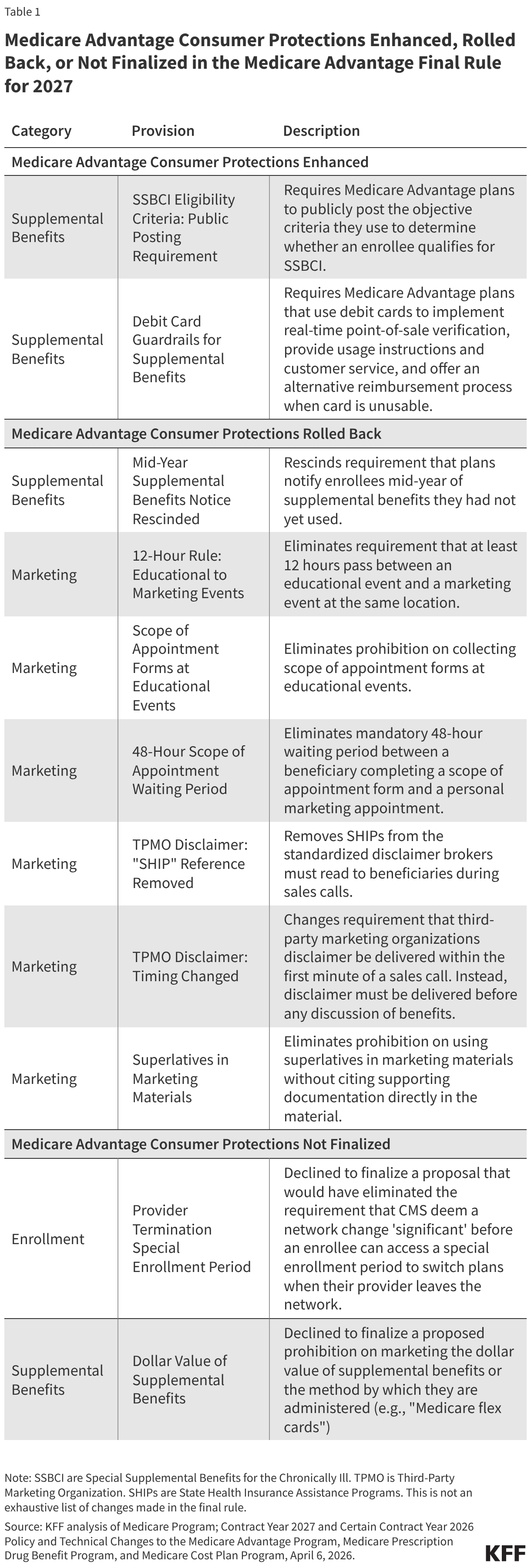
Medicare.2023 Medicare Advantage regulations and additional 2024 guidance clarify that Medicare Advantage organizations cannot make medical necessity decisions using an algorithm or software that does not consider individual circumstances. Denials based on medical necessity must be reviewed by a health care professional. Regulations proposed in 2024 that addressed bias and discrimination in the use of AI by Medicare Advantage plans were not finalized by the Trump administration. Additionally, the federal government is testing the use of AI to make certain prior authorization decisions for specific services in traditional Medicare through its Wasteful and Inappropriate Services Reduction (WISeR) Model, contracting with AI technology companies to administer this pilot program in six states.
Medicaid. Current Medicaid regulations do not directly address the use of automation in prior authorization. Medicaid managed care regulations require that any managed care organization (MCO) decision to deny services be made by “an individual” with appropriate expertise, but do not explicitly address AI use. Through state managed care contracts (which are reviewed and approved by CMS), states can set requirements for plan performance and reporting, such as requiring plans to disclose the use of AI in prior authorization processes. The Medicaid and CHIP Payment and Access Commission (MACPAC) has recently issued draft recommendations on the use of automation in Medicaid prior authorization.
State AI Consumer Protections in Prior Authorization and Claims Review
In recent years, some states have advanced laws and regulations aimed at protecting consumers from possible harm stemming from algorithmic decision-making systems, such as privacy breaches, inaccuracies, and bias. AI-related legislation continues to be debated in almost every state legislature, with some efforts garnering bipartisan support. Some states have issued regulations and other guidance under existing laws instead of or in addition to new state laws.
State laws specify new and existing AI consumer protections. Some state laws contain wide-ranging protections meant to cut across different sectors of the economy and apply to a broad range of entities, such as developers and those who deploy or use the technology for business purposes. Other state laws are specific to industry sectors (e.g., health care), topics (e.g., employment, civil rights, education), or uses, such as utilization review in health insurance.
Broad state laws include those that prohibit unfair or deceptive acts and practices. All 50 states have broad consumer protection laws that prohibit unfair or deceptive acts or practices. These laws are enforced by state attorneys general, and sometimes also allow a consumer to sue directly for a violation of the law (a “private right of action”) instead of relying on the state alone to enforce it. Colorado and Utah are examples of states that have amended their consumer protection laws to provide for general AI consumer protections.
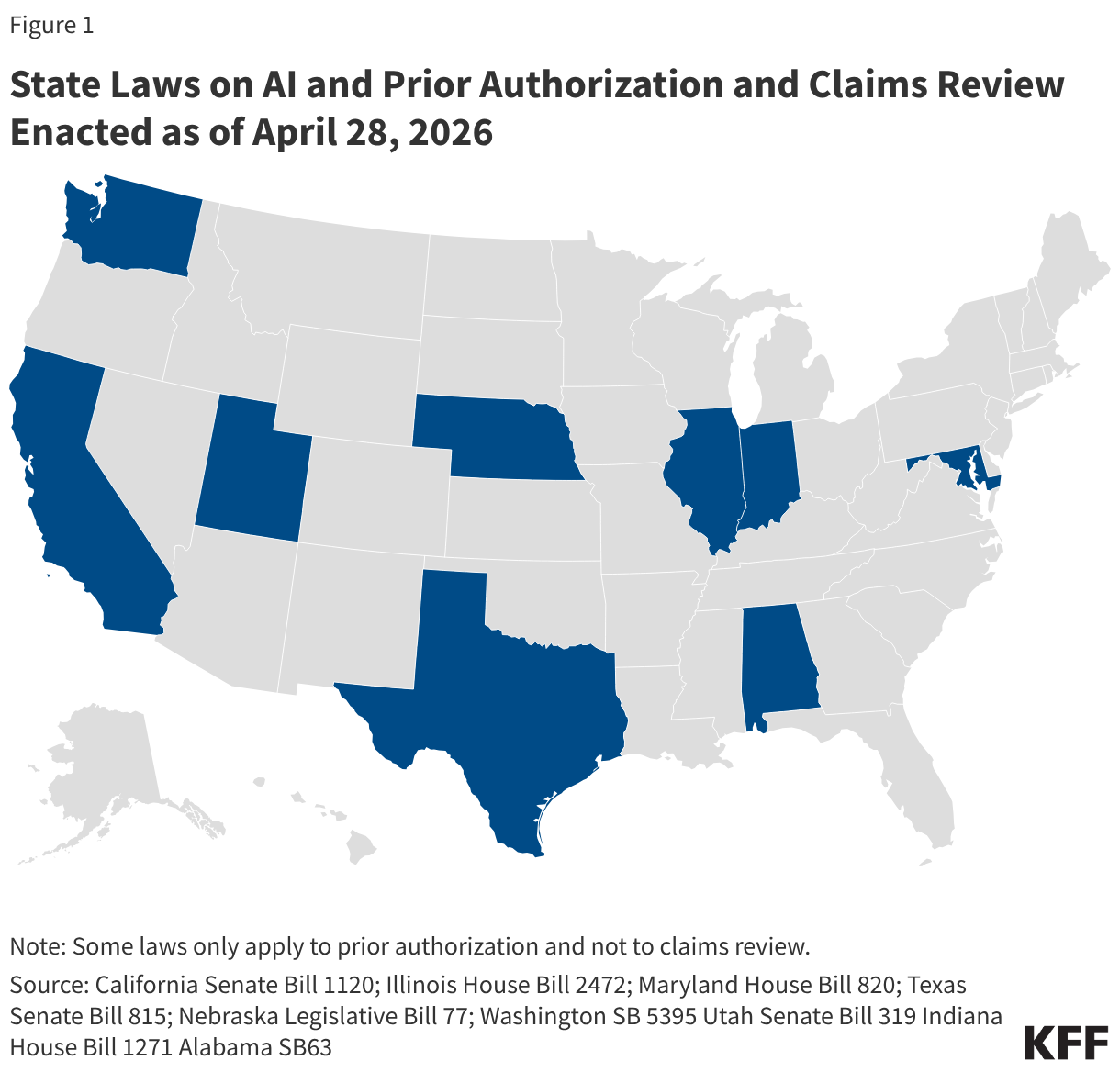
Depending on the specific state law, these broader consumer protection laws might be used to address consumer harm resulting from the use of AI in prior authorization and claims review. Additionally, a growing number of states have updated longstanding state health insurance standards for managed care related to utilization review to clarify how these rules apply to AI (Figure 1). Almost all of the laws are focused on the decision-making process of utilization review, sometimes defined under state rules as individualized decisions about whether a given service is medically necessary based on the patient’s individual clinical circumstances. These laws do not necessarily include administrative claim review decisions that do not involve a medical necessity determination, such as whether a claim is for care that is excluded under the plan.
Each state law related to the use of AI in prior authorization and/or claim review has its own unique requirements, but major themes include:
Human review of claim denials required. Some state laws include a provision that only a licensed health care provider may issue adverse determinations (a denial) and that AI cannot be used as the sole decisionmaker. For example, Illinois law requires that only a “clinical peer” make an adverse determination based on medical necessity and does not allow the sole use of an “algorithmic automated process” to make these decisions.
AI tools must take individual clinical circumstances into account. A couple of these states require that any AI tool used for utilization review bases its determination on an enrollee’s unique clinical history. Alabama, for instance, mandates that insurers who use artificial intelligence to make prior authorization determinations ensure that they base these decisions on an enrollee’s clinical history and clinical circumstances.
Disclosure of AI use. A few of these states, such as Utah for example, require entities that use AI to conduct utilization review to disclose its use to the public, the state department of insurance, health care providers in their network, and each enrollee.
Review of AI tool outcomes. Some state laws also require entities that perform utilization review to periodically review performance and outcomes of AI tools they use in order to check accuracy and reliability. California law requires that an AI tool be periodically assessed and revised to ensure maximum accuracy and reliability.
Limits on the use of patient data to protect privacy. Several of these state laws include language that prohibits those conducting utilization review from using patient data beyond its intended purpose and contrary to HIPAA or state law confidentiality protections. Maryland law is one example.
AI tools must be open to inspection, including the underlying algorithms. Some of these laws mandate that AI tools for utilization review be open to audit by regulators. In Texas, the commissioner is allowed to audit and inspect a utilization review agent’s use of an automated decision system for utilization review at any time.
AI protections against bias and discrimination. A few state laws, such as Washington's, require that AI tools be applied “fairly and equitably” and cannot result in discrimination, either directly or indirectly, against an enrollee.
New state guidance aims to exercise state authority to regulate AI use. Some states have issued guidance to make clear how existing state legal protections apply to AI. For example, in 2024, the Massachusetts Attorney General released a public Advisory explaining how the state’s existing consumer protection, civil rights, and data privacy laws apply to developers, suppliers, and users of AI, and how they could impact consumers in Massachusetts.
Insurance regulators in some other states have taken a similar approach, issuing new guidance to clarify how existing state law applies to AI and provide more specific information to insurers about their obligations concerning the use of AI. As of early April 2026, at least 25 states have issued guidance based on a model bulletin adopted in 2023 by the National Association of Insurance Commissioners (NAIC). The model bulletin applies to all types of state-regulated insurance (not just health insurance) and addresses the use of AI across all aspects of the insurance life cycle, including claims administration and payment, fraud detection, product development, and rating and pricing. It establishes the expectation that consumer-facing decisions made or supported by AI systems comply with existing insurance laws and regulations, including protections against unfair trade practices and illegal discrimination. It also instructs insurers to adopt policies and procedures with specifics about how AI is used and to implement controls to mitigate the risk of adverse outcomes. It specifies that insurance oversight includes the ability of regulators to inquire about the development, deployment, use, and outcomes of any AI system or predictive model used by insurers or their third-party vendors, as well as request information about system validation, testing, and ongoing audits of AI systems.
Issues To Watch
Striking a balance between the advancement of technological innovation that might save time and money and preventing harm to consumers is not a new challenge. It has been at the heart of consumer protection law for decades. AI presents just the latest policy challenge that policymakers, regardless of party affiliation, are faced with. For health insurance claims review specifically, calls for additional transparency and oversight of the process are longstanding and predate the use of AI. Future congressional action on AI will likely be shaped by the following issues:
The role of state-level consumer protections. Whether the federal government can preempt the application of state consumer protection laws in this area is an open question. The Trump administration’s AI framework appears to acknowledge that certain state protections should continue to apply. A key issue in the development of any federal legislation will be deciding what state actions are consistent with states’ traditional role in overseeing health care and insurance and should be preserved, and which ones are best placed at the federal level for uniformity and consistency. Setting a clear framework for when state and federal protections can and cannot coexist will likely be part of the policy debate.
Some federal preemption provisions can create uncertainty and confusion for consumers. Ongoing legal battles, for example, about whether state pharmacy benefit laws apply to self-insured employer plans under ERISA preemption, are in the process of being clarified through court decisions. This leaves consumers in limbo about what protections they have. Given the rapid changes and risks associated with AI technologies, whether federal preemption is a workable approach for state AI laws is another open question.
Benefits and limitations of a national framework. A single federal standard that preempts most state protections could be easier to build consensus around and simpler for the public to understand, but the current deregulatory agenda for the federal government could mean lax oversight of fast-developing technology. A recent proposed interoperability regulation, for instance, would eliminate some federal certification standards for health IT developers, including those related to transparency of AI data sources and audit reporting.
On the other hand, federal agencies that have not played a role in AI and claims review in the past could increase oversight activities. For example, the Federal Trade Commission has some responsibilities for enforcing unfair and deceptive trade practices standards. Also, some have suggested that the Food and Drug Administration (FDA) should regulate the algorithms that health plans use to determine coverage in the same way the agency oversees AI used in medical devices through a premarket review and evaluation of these tools.
Evaluation of the impact of AI tools in prior authorization and claims review. Providers may use AI to enhance their billing and collection capabilities, and plans work in the opposite direction by using AI in claims review and audit to rein in spending, raising the question of how these tools impact costs to the health system overall. The challenge is to evaluate these tools in real time to determine whether the benefits of AI use in this area (and efforts to encourage its development under federal legislation) outweigh the risks. Access to information about the precise mechanisms of these tools is limited, and efforts to obtain information, for instance, about the AI tools involved in the CMS WISeR model, have resulted in litigation.
Assessment of risks to patients. The enthusiasm about AI technology that might assist consumers in navigating the complexity of insurance bills, claims, and appeals is sometimes tempered by concerns about the risks of incorrect information and claim denials, bias, and privacy and security. Privacy is a particular concern, given the limits of the federal HIPAA standards in reaching the technology companies involved in developing or implementing AI solutions. A KFF poll found that 77% of the public is concerned about the privacy of personal health information provided to AI tools.
In addition to the risk involved when a consumer enters their health information into an AI tool, improper access to this information to test or train AI is also a risk. The Trump administration’s AI framework urges Congress to provide resources to make “federal datasets” available to industry and academia. Concerns about the federal government accessing individually identifiable data from federal agencies to train AI models or for other purposes are growing, raising questions about what additional safeguards might be important in protecting consumers.
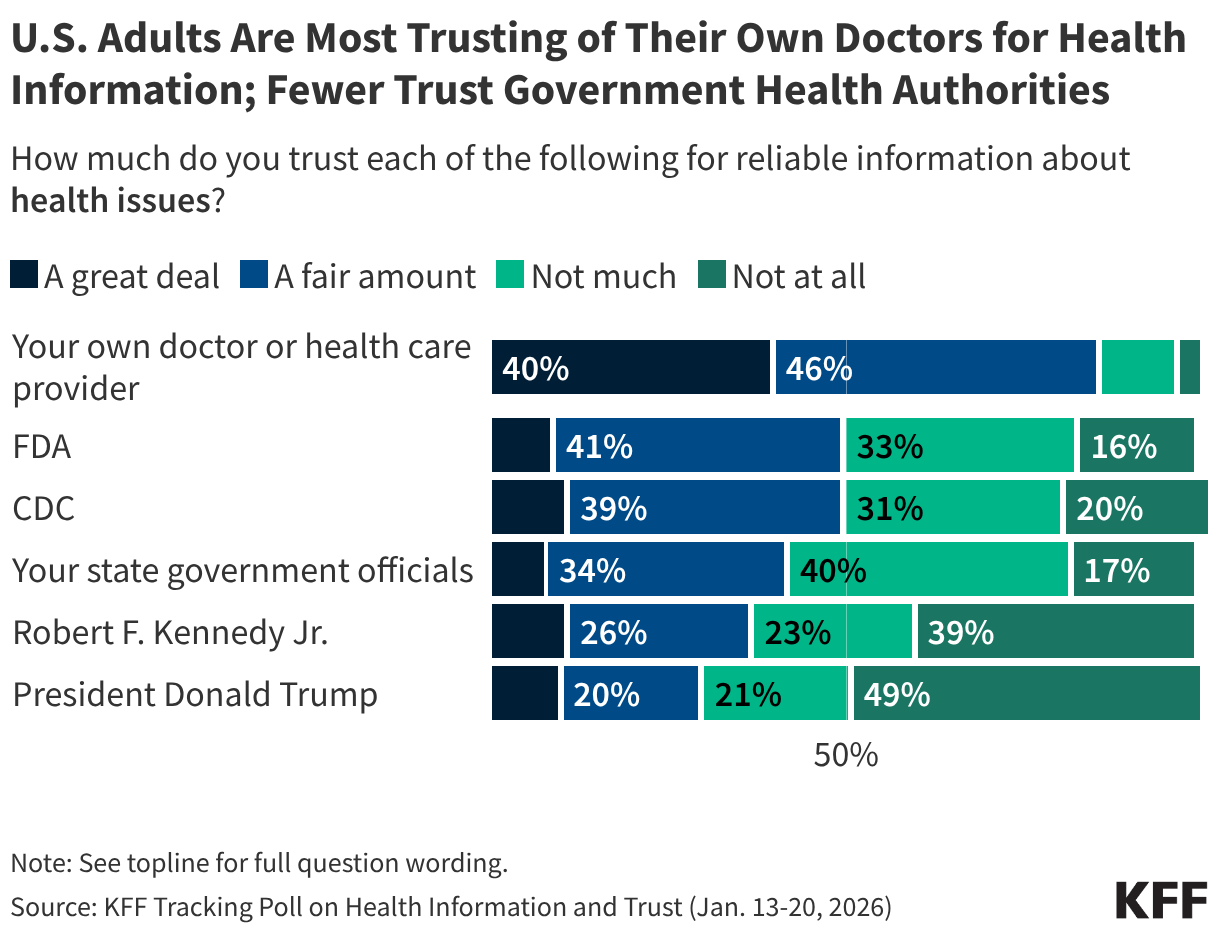
Doctors and other health care providers are the public’s most trusted source of health information, while trust in government health agencies and officials is much more divided. A large majority of adults express at least “a fair amount” of trust in their doctor for reliable information about health issues, while half say they trust the CDC or FDA and fewer than half express trust in their state government officials, HHS Secretary Robert F. Kennedy, Jr., or President Trump.
Partisanship shapes who the public trusts for health information, especially when it comes to Secretary Kennedy and President Trump. Two-thirds of Republicans, rising to three-quarters among MAGA-supporting Republicans, say they trust Secretary Kennedy and President Trump for reliable health information compared to one-third or fewer independents and Democrats who say the same. On the other hand, Democrats are somewhat more likely than Republicans to trust their state officials for health information, while similar shares of Democrats and Republicans say they trust the CDC or FDA. Individual health care providers are the most-trusted source for health information across partisanship.
Across demographic groups – including age, gender, race and ethnicity, and education – health care providers remain the most trusted source of health information. For other health information sources, trust does not differ consistently across most of these groups, but White adults and those without a college degree are more likely than their peers to express trust in Secretary Kennedy and President Trump for health information.
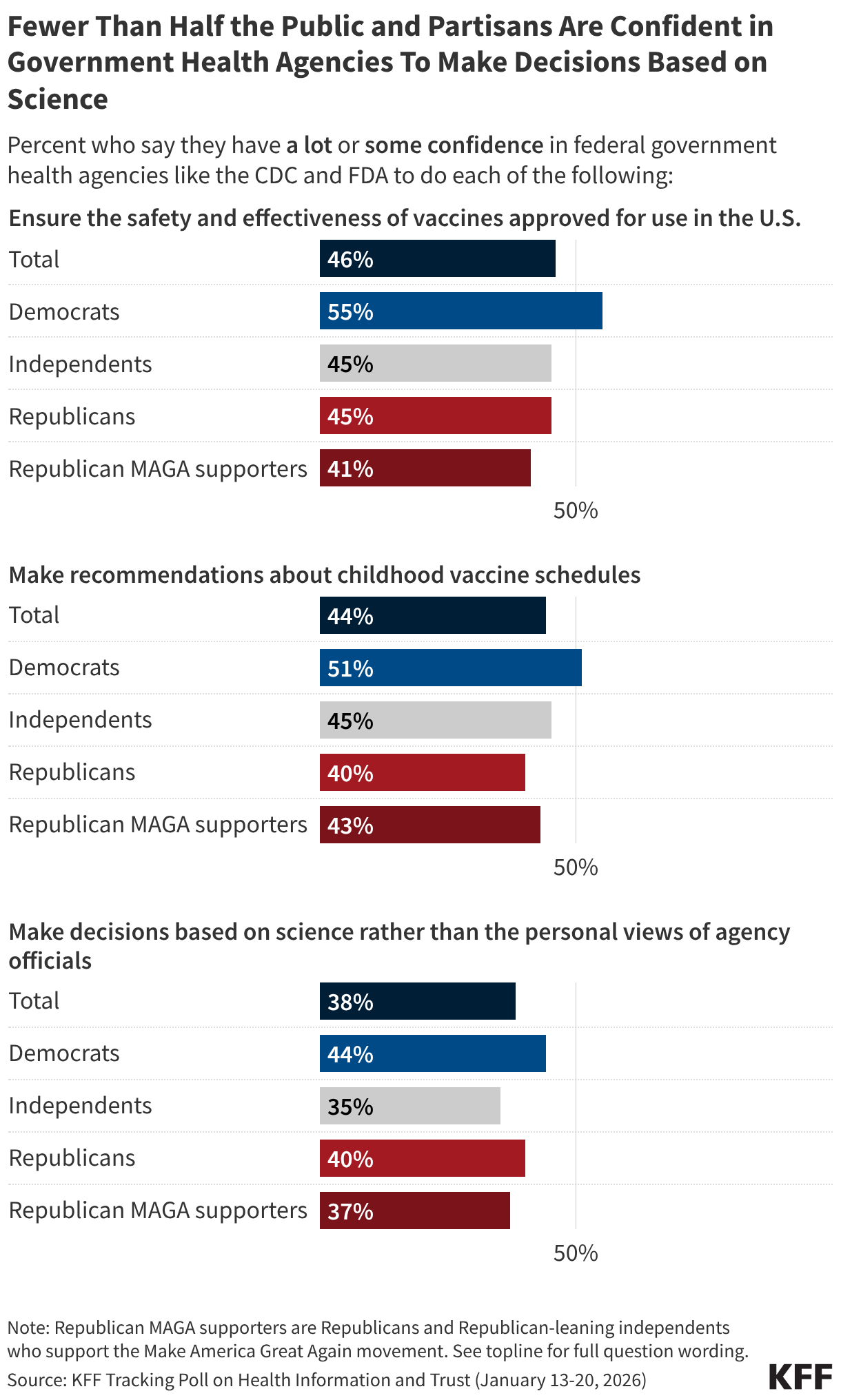
Most of the public lacks confidence in agencies like the CDC or FDA to carry out many of their core responsibilities. While Democrats are somewhat more likely than Republicans to have at least “some confidence” in government health agencies to ensure vaccine safety and effectiveness and make recommendations about the childhood vaccine schedule, fewer than half across partisans have confidence in these agencies to make decisions based on science. For more information, see KFF’s January 2026 Tracking Poll on Health Information and Trust.
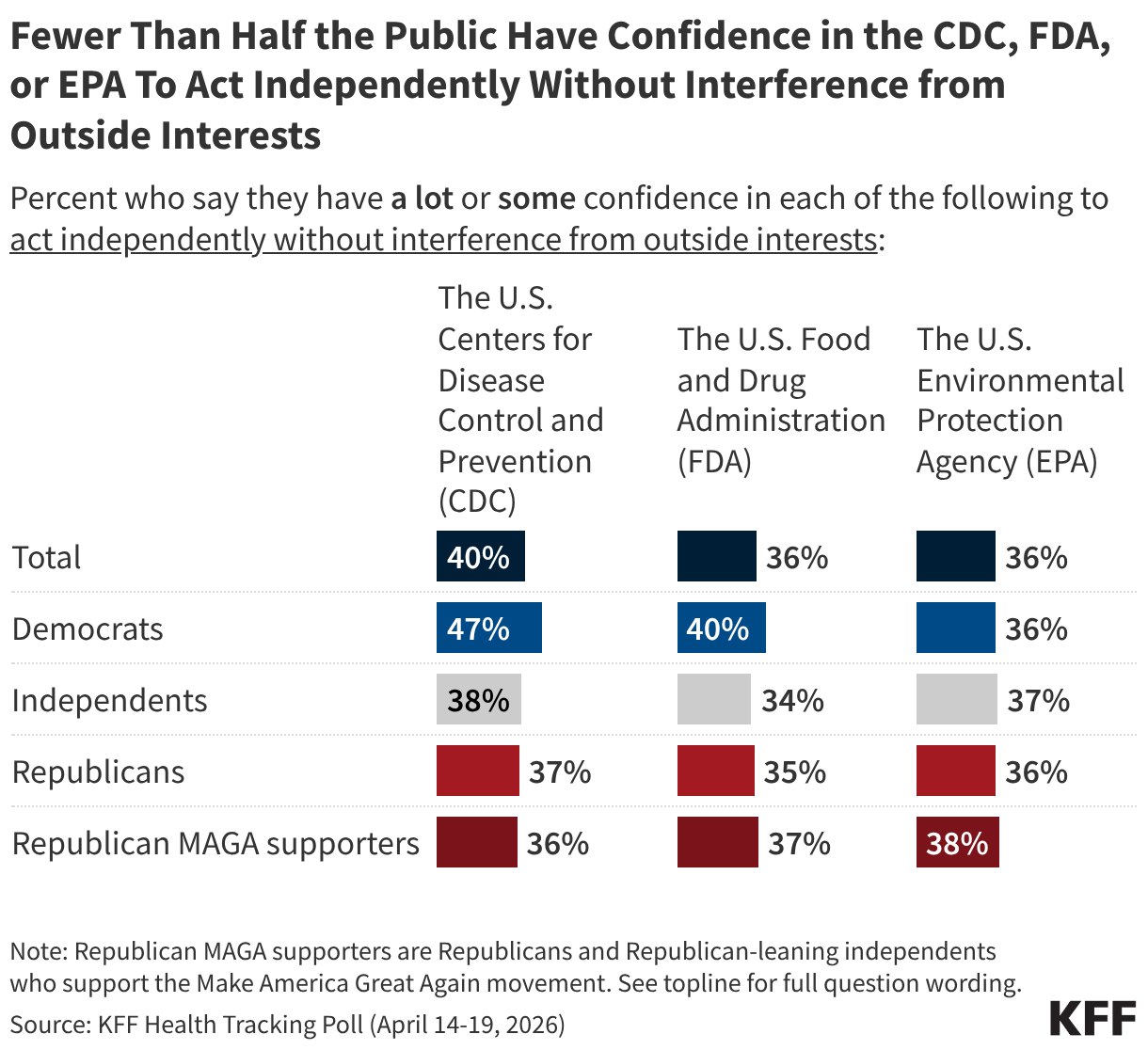
Less than half of the public and partisans express at least “some confidence” in the CDC, FDA, or EPA to act independently without outside interference. Democrats are somewhat more likely to say they have confidence in the CDC to act independently, with almost half expressing confidence. On the other hand, four in ten or fewer adults and partisans express confidence in the independence of the FDA or the EPA. For more information, see KFF’s April 2026 Health Tracking Poll.
Trends in Trust of Government Health Agencies and Officials
At the onset of the COVID-19 pandemic, there were high levels of bipartisan trust in information about the new virus from the U.S. Centers for Disease Control and Prevention (CDC). Trust in the agency for information about COVID-19 vaccines, and vaccines more generally, subsequently declined amid widening partisan divisions and large drops in Republican trust. Democratic trust in the agency has since declined significantly following President Trump’s reelection and the confirmation of Robert F. Kennedy Jr. as HHS Secretary. Amid these partisan shifts, half of the public now express trust in the CDC for reliable vaccine information. Keep scrolling to see trends among the public and partisans.
KFF polling has found trust in vaccine information from other health agencies and officials has also declined amid partisan divisions since 2020, including for the U.S. Food and Drug Administration (FDA), state government officials, and local public health departments.
Who Parents Trust for Childhood Vaccine Information
Among parents of children under age 18, pediatricians are the most trusted source of reliable vaccine information. Smaller shares, but still majorities, also trust their local public health department, the CDC, and the FDA. Over half of parents trust their friends and family for vaccine information, while far fewer express trust in Robert F. Kennedy Jr., pharmaceutical companies, or health and wellness influencers. As with the public overall, partisanship plays a role in who parents trust for vaccine information. For more information, see the KFF/Washington Post Survey of Parents.
Among parents, Secretary Kennedy garners trust on vaccines from a majority of Republican supporters of the Make America Great Again, or MAGA, movement (18% of all parents) and supporters of the Make America Healthy Again, or MAHA, movement (38% of all parents). While slim majorities of these MAGA and MAHA parents trust Kennedy for vaccine information, larger shares express trust in their child’s pediatrician.
News, Social Media, and AI
Use and Trust of News Sources for Health Information
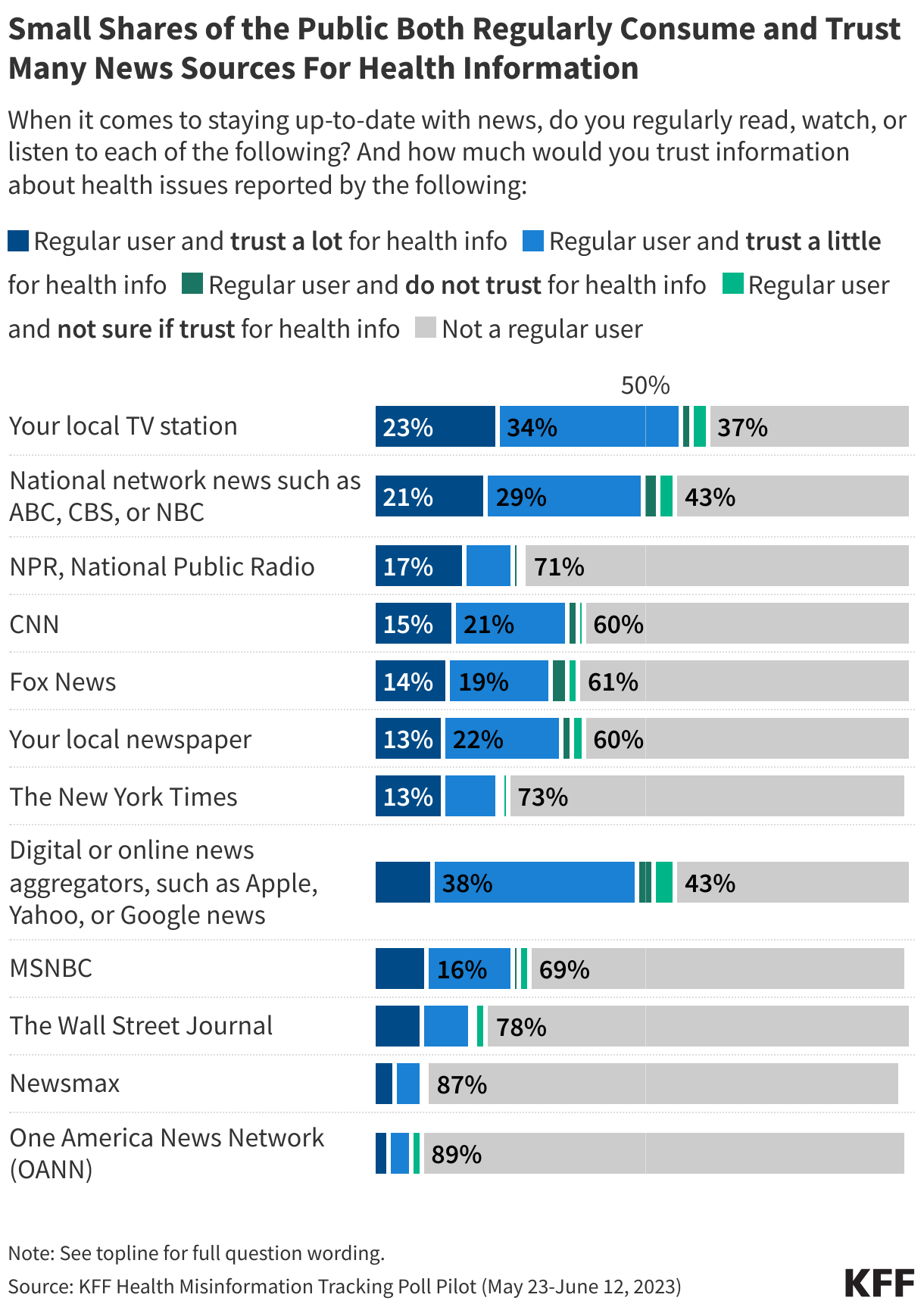
KFF’s Health Misinformation Tracking Poll Pilot measured the public’s consumption of a variety of television, print, radio, and digital news media sources as well as their trust in these sources for information about health issues. Overall, few adults both regularly consume most news sources and trust them a lot for information on health issues, with local and network television news topping the list. Nearly a quarter (23%) of adults say they regularly watch their local TV station and would trust it “a lot” for health information, while a similar share (21%) say the same about national network news. Other news sources, including NPR, CNN, Fox News, local newspapers, The New York Times, digital news aggregators, and MSNBC have trusting audiences that make up between one in ten and one in six of the overall public.
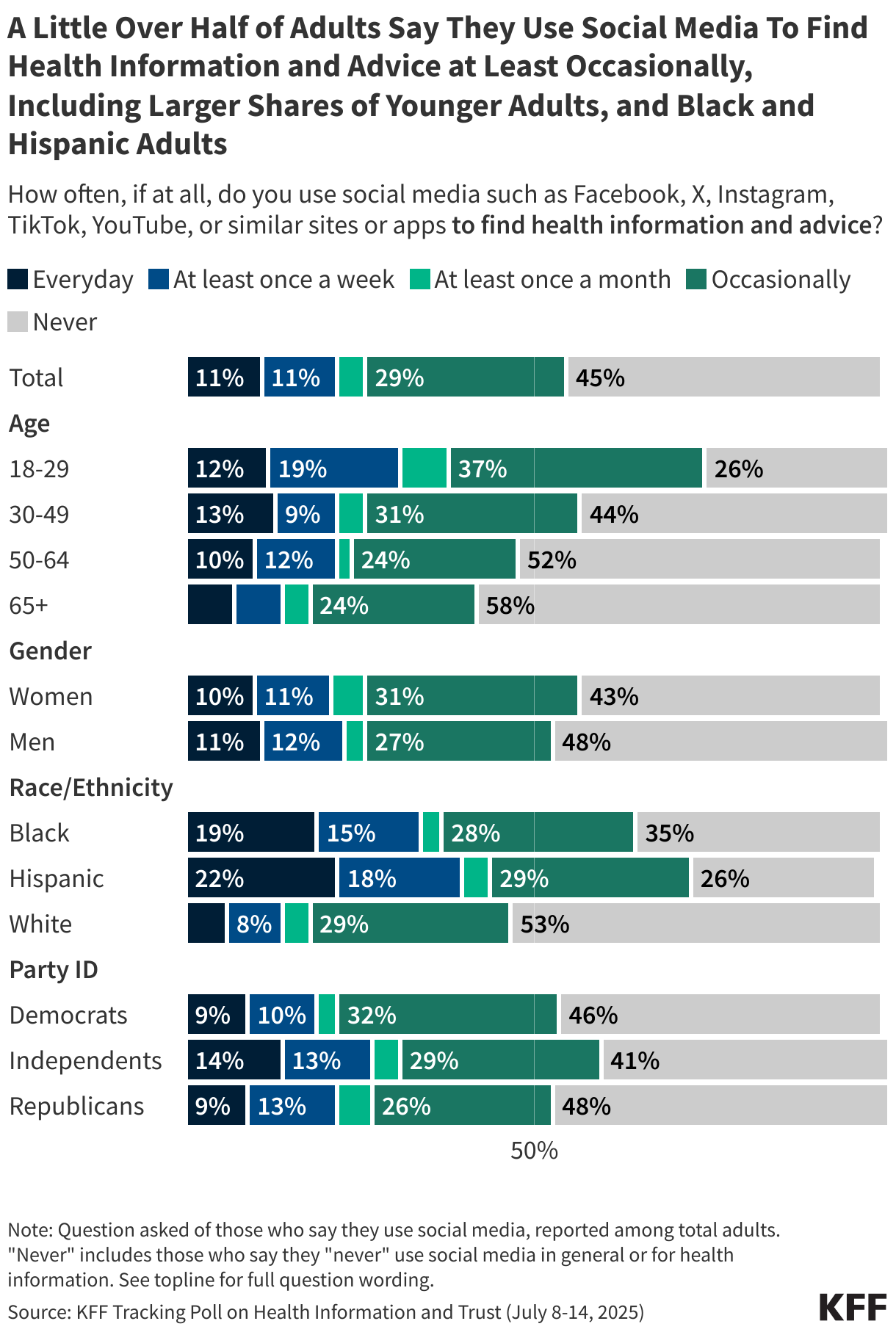
Just over half of adults say they use social media to find health information and advice “at least occasionally,” including larger shares of younger adults, and Black and Hispanic adults. For more information on social media use and trust see KFF’s July 2025 Tracking Poll on Health Information and Trust.
While just over half of the public report actively using social media to find health information and advice, larger shares report being exposed to such information, with majorities saying they have recently seen content related to weight loss, diet, or nutrition and mental health.
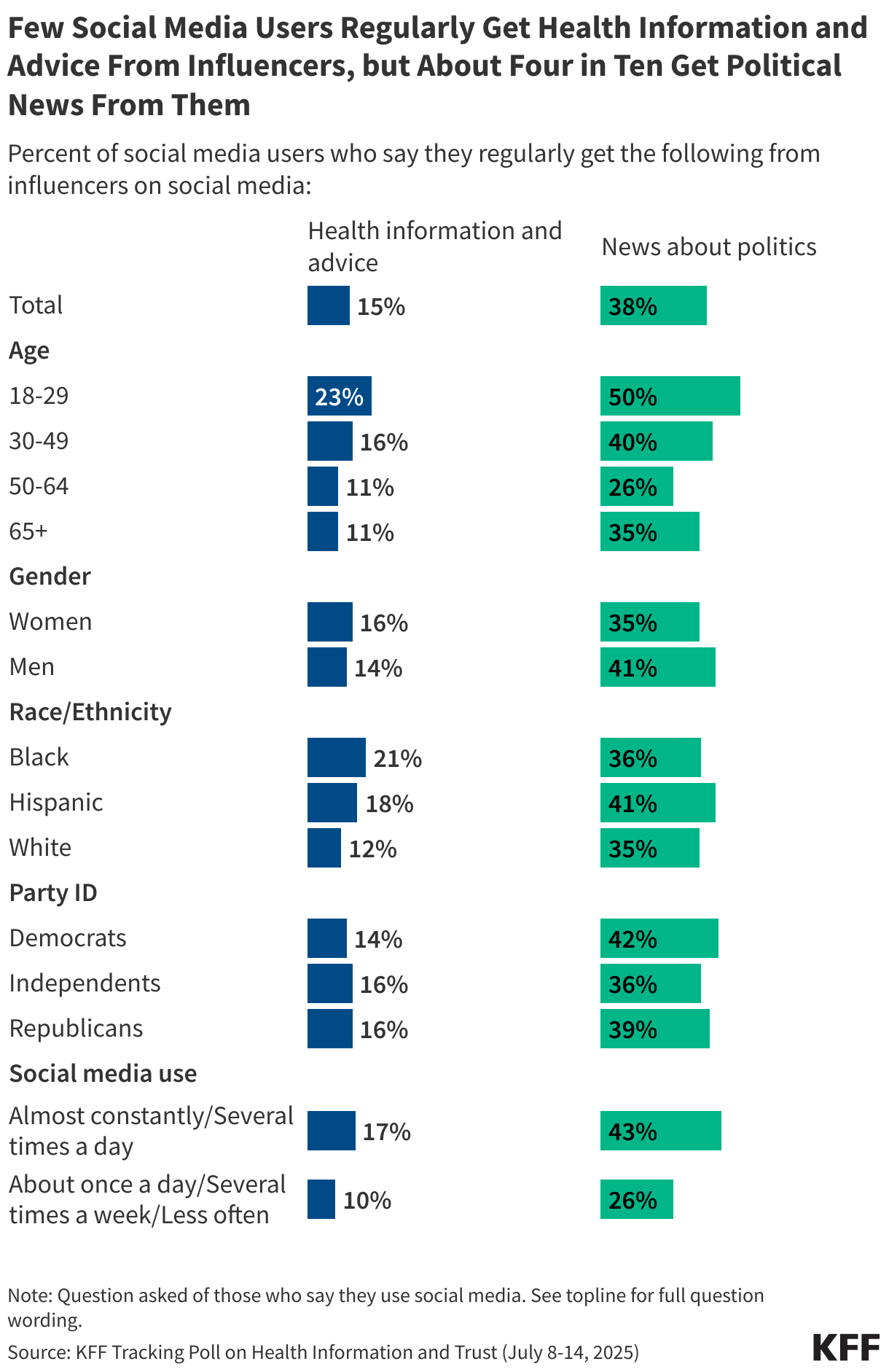
While four in ten social media users say they regularly get information about news and politics from social media influencers, far fewer (15%) say they turn to influencers for health information and advice. Younger adults, Black adults, and more frequent social media users are more likely than their peers to say they rely on influencers for health information. For more information on the relative impact of influencers on the public and health policy debates, see KFF CEO Drew Altman’s column.
Across different social media platforms, fewer than half of users say they find at least “some” of the health information they see on these platforms to be trustworthy. Younger users tend to be more trusting than older users of health content on certain platforms including TikTok, YouTube, Instagram, and Reddit.
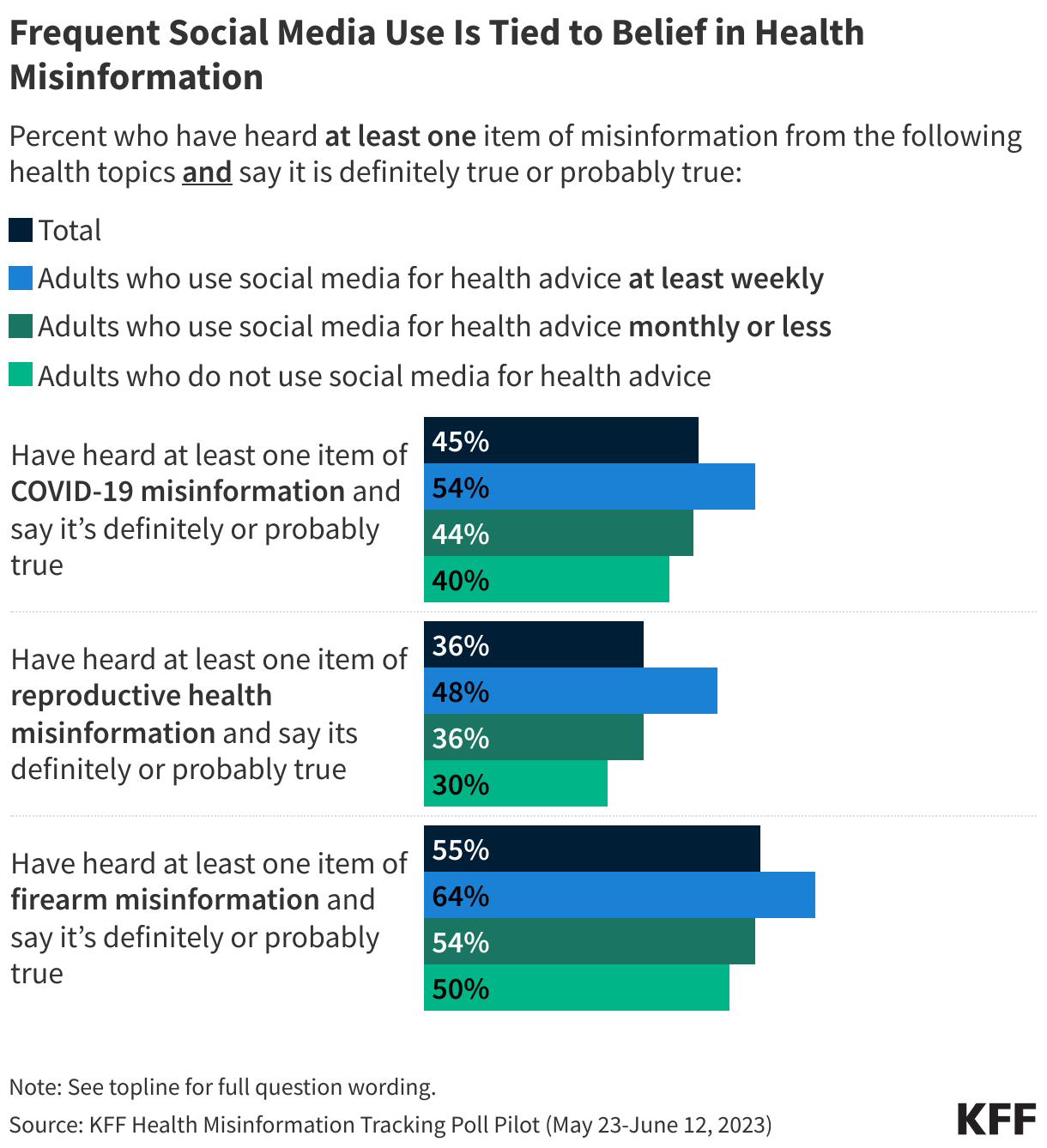
While few say they trust social media when it comes to health, KFF’s 2023 Health Misinformation Tracking Poll Pilot found that that those who turn to social media more frequently for health information may be more susceptible to health misinformation. Adults who reported using social media at least weekly were more likely than less frequent users to believe at least one false claim related to either COVID-19, reproductive health, or firearms.
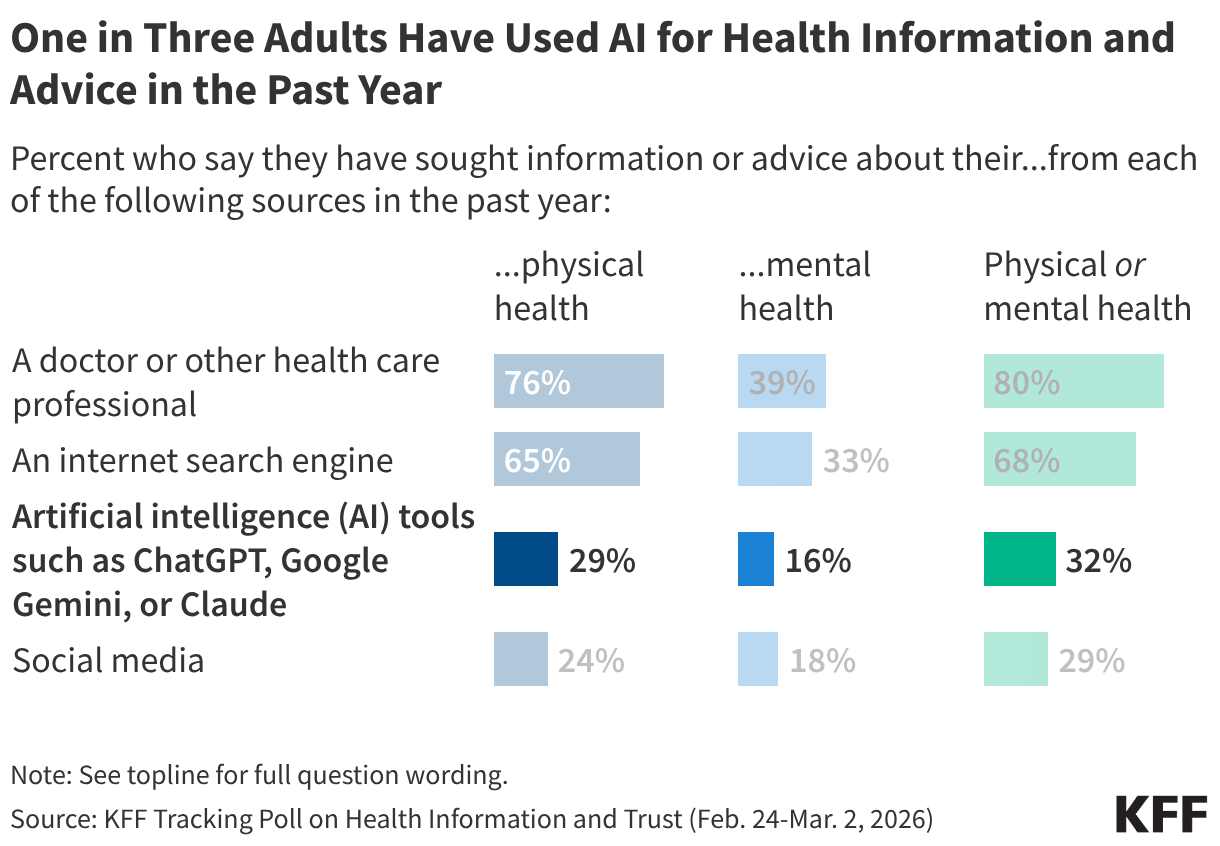
About a third (32%) of the public reports turning to AI chatbots for health information and advice in the past year – rivaling social media as a health information source, but less common than reliance on health care providers or internet search engines (where they may be encountering AI generated results, even if they are not looking for them). The share of adults using AI for health information includes three in ten who say they’ve used these chatbots in the past year for information or advice about their physical health, and one in six who’ve used them for mental health information or advice. For more information, see KFF’s March 2026 Tracking Poll on Health Information and Trust.
Larger shares of younger adults report turning to AI for either physical health or mental health information in the past year. When it comes to mental health advice, uninsured adults and Black and Hispanic adults are more likely than insured adults and White adults to have turned to AI.
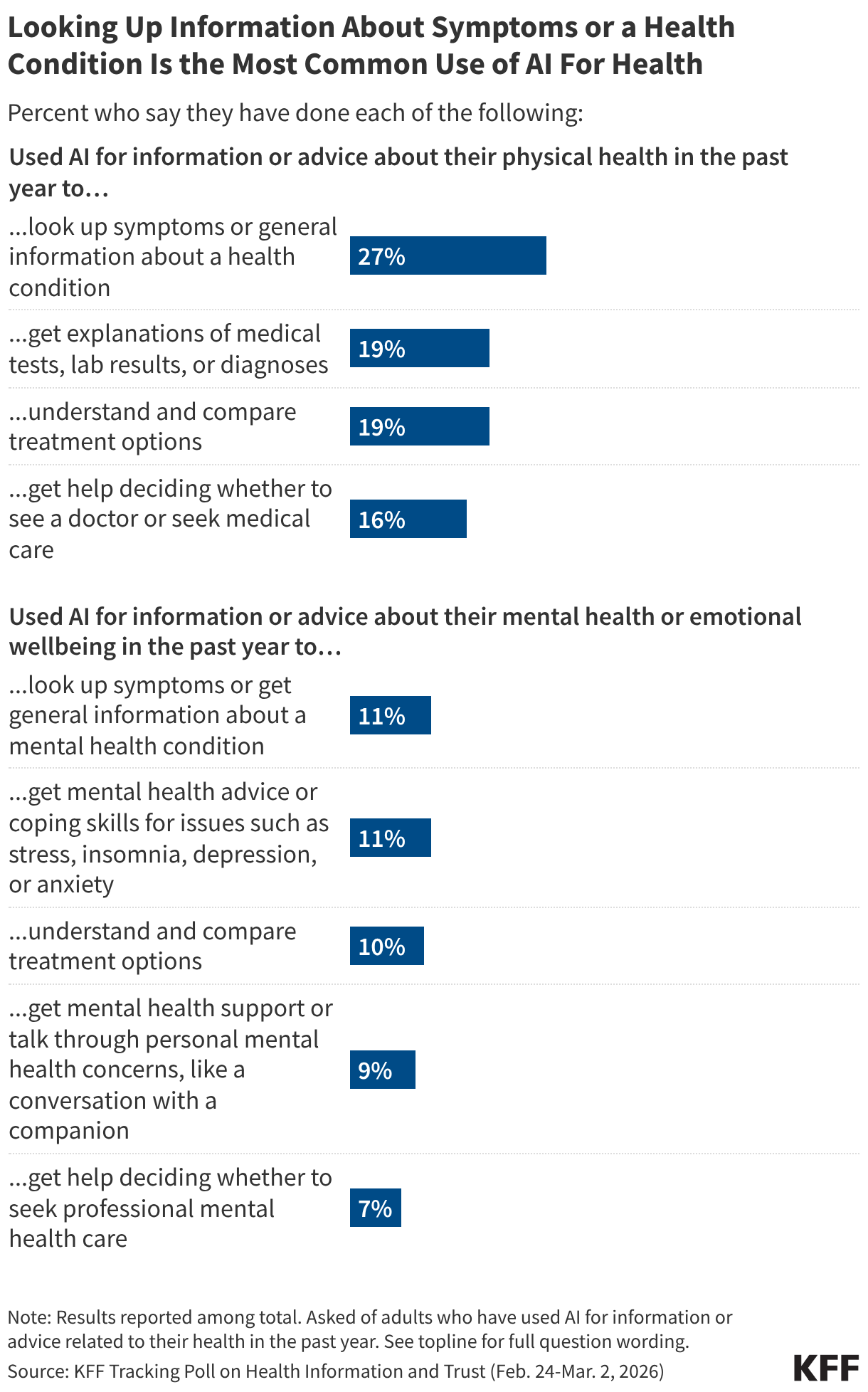
People report using AI for either physical health or mental health information in a variety of ways, most commonly to look up symptoms or general information about health conditions. Fewer say they used AI to help make decisions about whether to seek medical care for either physical or mental health concerns.
The most common reason people cite for turning to AI for health advice is wanting quick or immediate support. Many also cite wanting to look up information before seeing a provider or feeling more comfortable looking up health questions privately. One in five cite health care access or affordability issues as major reasons for turning to AI for health questions, including larger shares of younger adults and those with lower household incomes
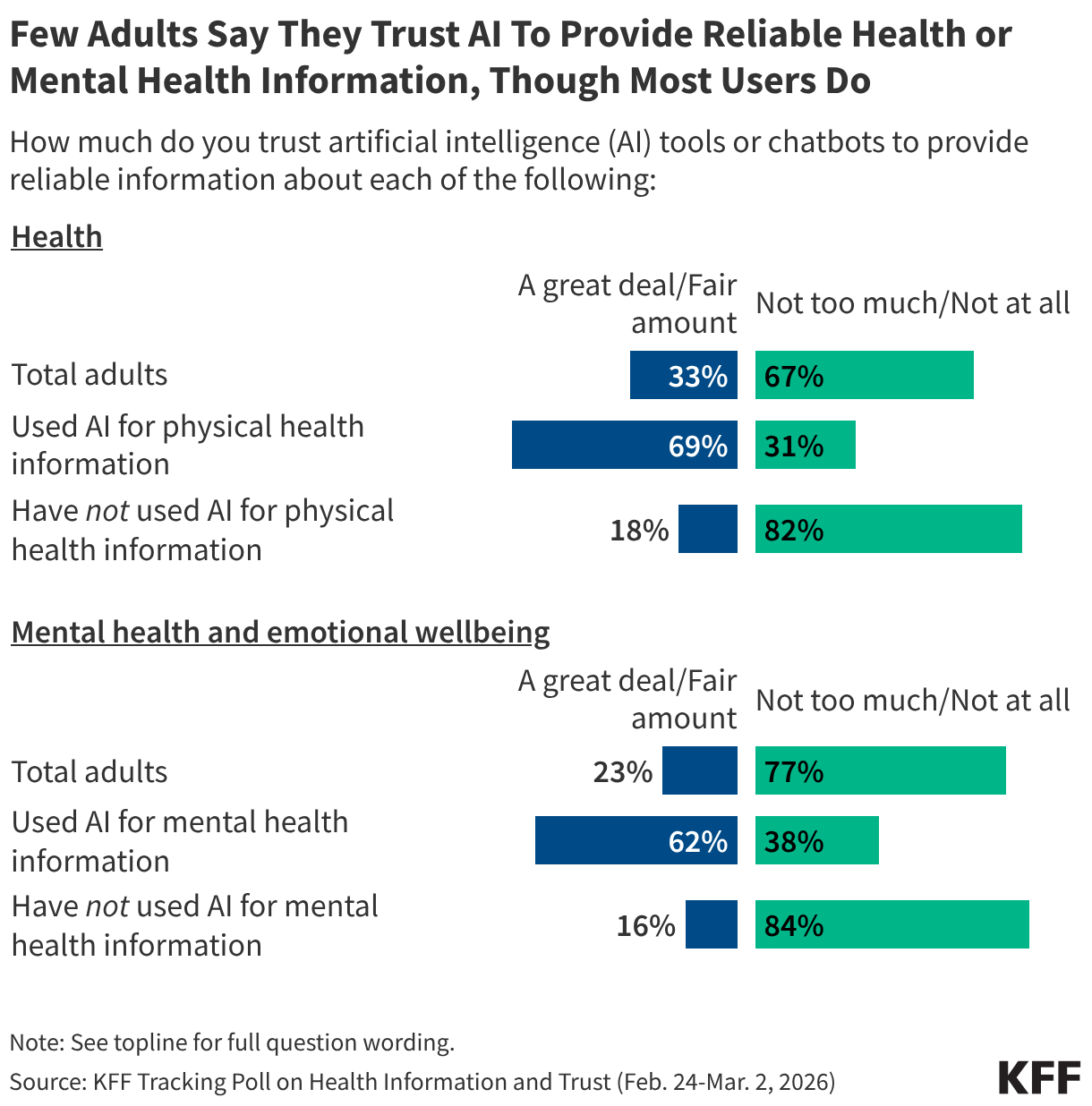
Among the public overall, few adults say they trust AI tools to provide reliable information about health, but most adults who have used AI for health information and advice say they trust these chatbots to provide reliable health information.
False or Unproven Health Claims
Awareness and Belief in False or Unproven Health Claims
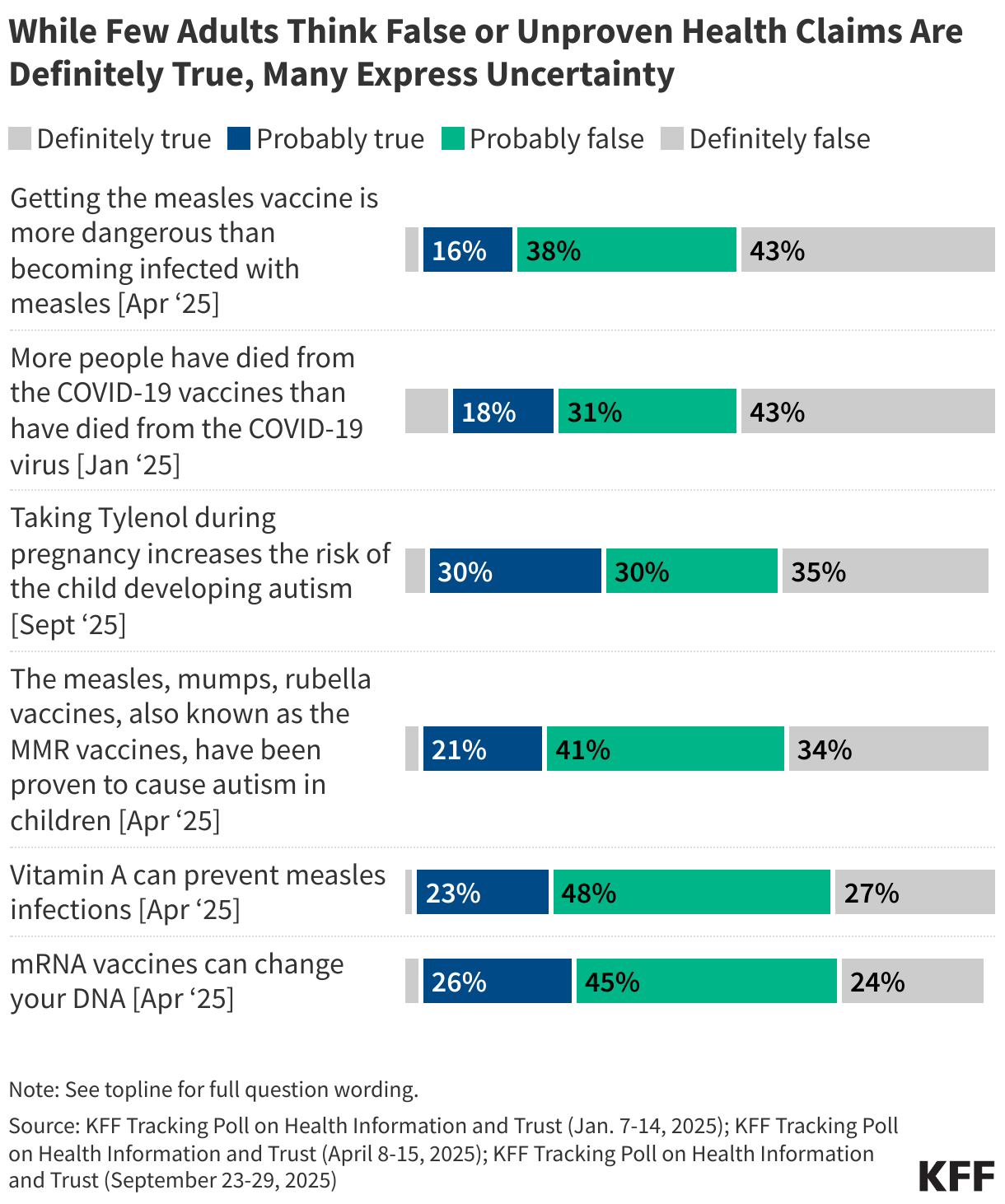
Exposure to health misinformation is often widespread, but relatively small shares of the public express certainty that many false or unproven claims are true. In fact, most of the public fall in a “malleable middle,” saying these claims are either “probably true” or “probably false.” The public’s uncertainty around false or unproven health claims related to COVID-19 , vaccines , measles and the purported causal link between Tylenol and autism presents an opportunity for interventions to clear up confusion and deliver accurate information.
KFF polls have measured exposure to a wide array of false, misleading, and unproven health claims since 2023. Exposure varies widely depending on the topic and prominence of news coverage of the claim. The most widely heard of those tested in KFF polls is that taking Tylenol during pregnancy increases the risk of a child developing autism, a claim cited by President Trump in a widely covered September 2025 press conference.
Across an array of false or unproven health claims measured in KFF surveys, few adults are certain these claims are “definitely true” while much larger shares consistently say they are “definitely false.” For most claims, at least half express uncertainty, falling into the malleable middle and saying the claims are either “probably true” or “probably false.” The six most recent claims measured in KFF surveys in 2025 are shown below.
KFF polling has measured exposure to and belief in false or unproven claims across a wide array of topics. For information on belief in additional claims about COVID-19, reproductive health, and gun violence, see KFF’s Health Misinformation Tracking Poll Pilot. For information on additional false claims related to COVID-19, see KFF’s May 2022, and October 2021 COVID-19 Vaccine Monitors.
KFF polling has found partisanship and education play a substantial role in belief of false or unproven health claims about vaccines, COVID-19 and measles. Republicans and adults without a college degree are consistently more likely than Democrats and college educated adults, respectively, to believe or lean towards believing false claims related to COVID-19, measles, and vaccines.
Beyond partisanship and education, younger adults and Hispanic adults are more likely than their peers to believe or lean toward believing some of these false or unproven health claims but not others. These differences show that susceptibility to health misinformation among some groups can vary depending on the topic, which may reflect different information channels relied upon by these groups (see social media and news sources sections for more info).
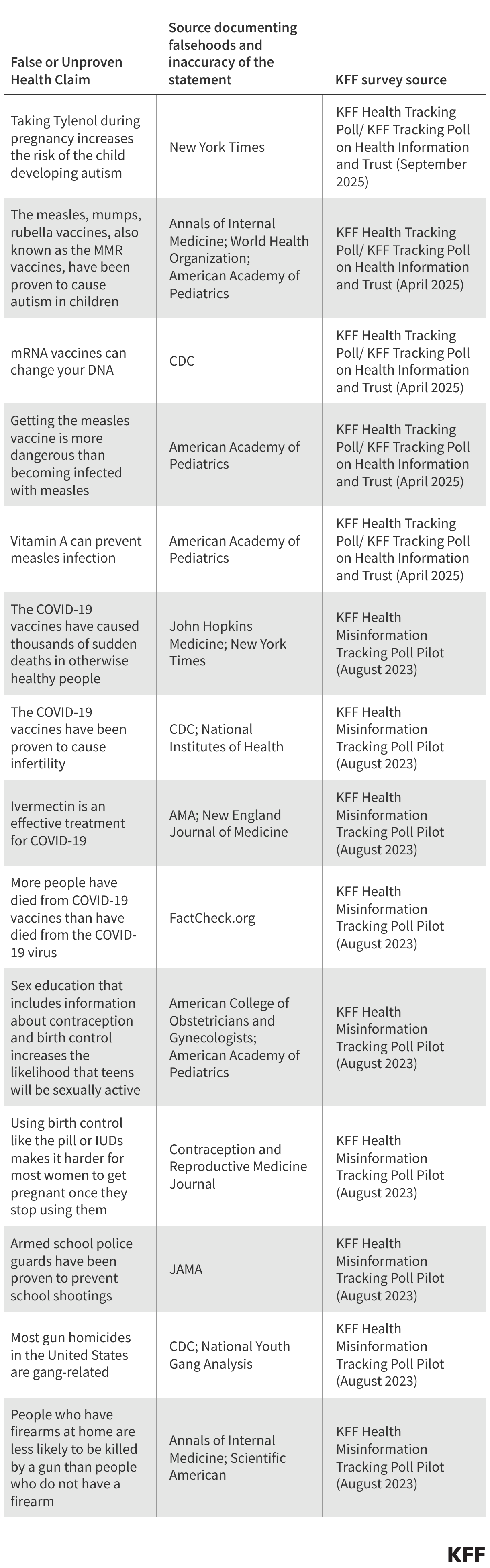
KFF polling has sought to examine the public’s exposure to and belief in a wide array of false or unproven health claims. Many of the false or unproven claims measured in KFF surveys have been amplified by or directly made by government officials, while others have been more nebulously shared and spread in public media over the years. Below is a list of sources to document these claims’ inaccuracy.
Most U.S. adults, including majorities across partisans, express confidence in the safety of many routine vaccines for children, including MMR, polio, and hepatitis B. Similarly, large majorities of adults ages 50 and over are confident that vaccines for pneumonia and shingles are safe. Views on the safety of COVID-19 and flu vaccines for both adults and children are more divided, with large shares of Democrats expressing confidence compared with smaller shares of Republicans. For more information, see KFF’s January 2026 and April 2025 Tracking Polls on Health Information and Trust.
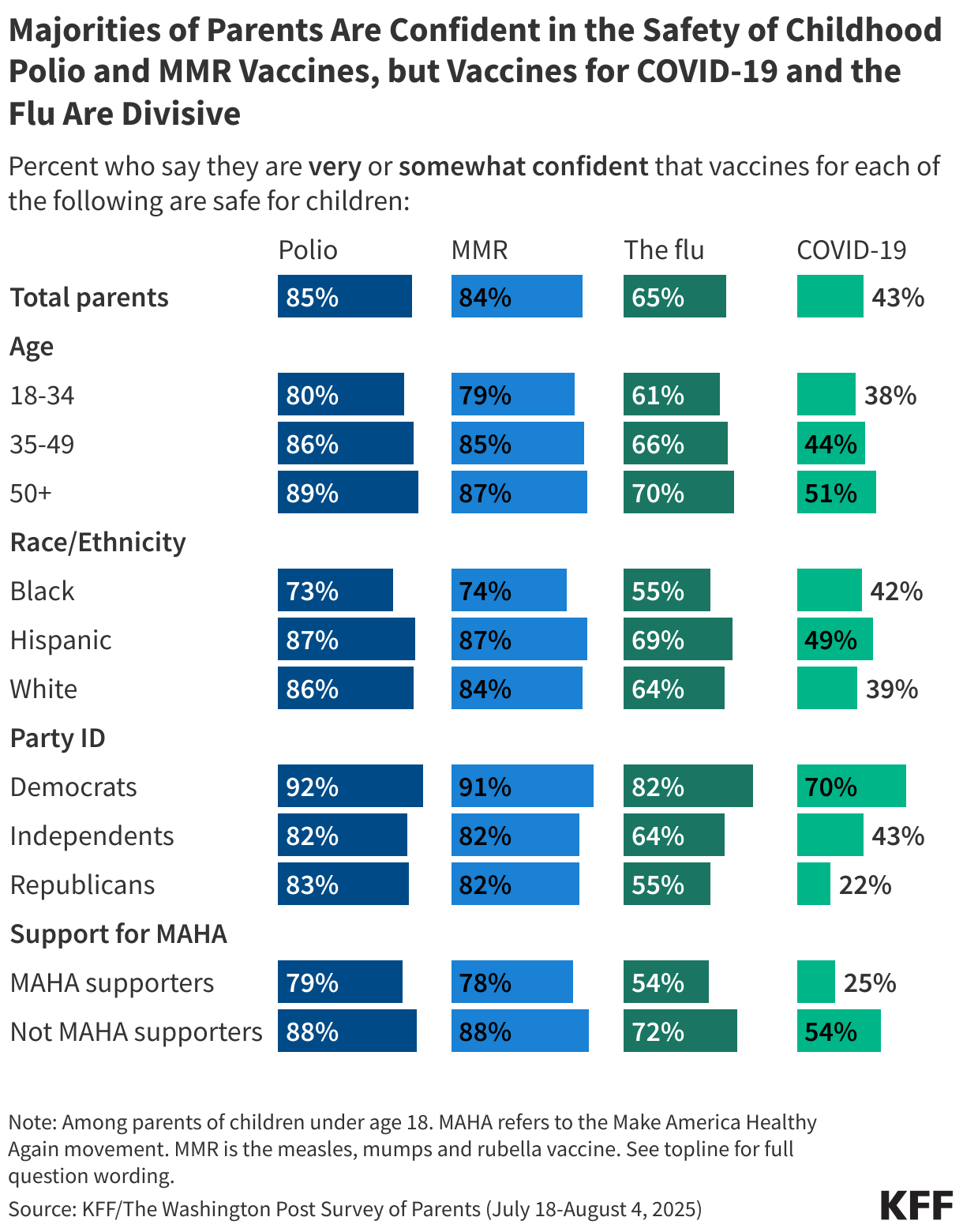
In summer 2025, large majorities of parents expressed confidence in the safety of childhood vaccines for polio and measles, mumps, and rubella (MMR), but parents’ views on the safety of flu and COVID-19 vaccines were more polarized. About two-thirds of parents say the flu vaccines are safe for children, while fewer than half say the same about COVID-19 vaccines, with divisions along partisan lines. Beyond partisanship, parents who support the Make America Healthy Again (MAHA) movement (38% of parents), Black parents and parents under age 35 are less likely than their peers to be confident that many routine vaccines are safe for children. For more information, see the KFF/Washington Post Survey of Parents.
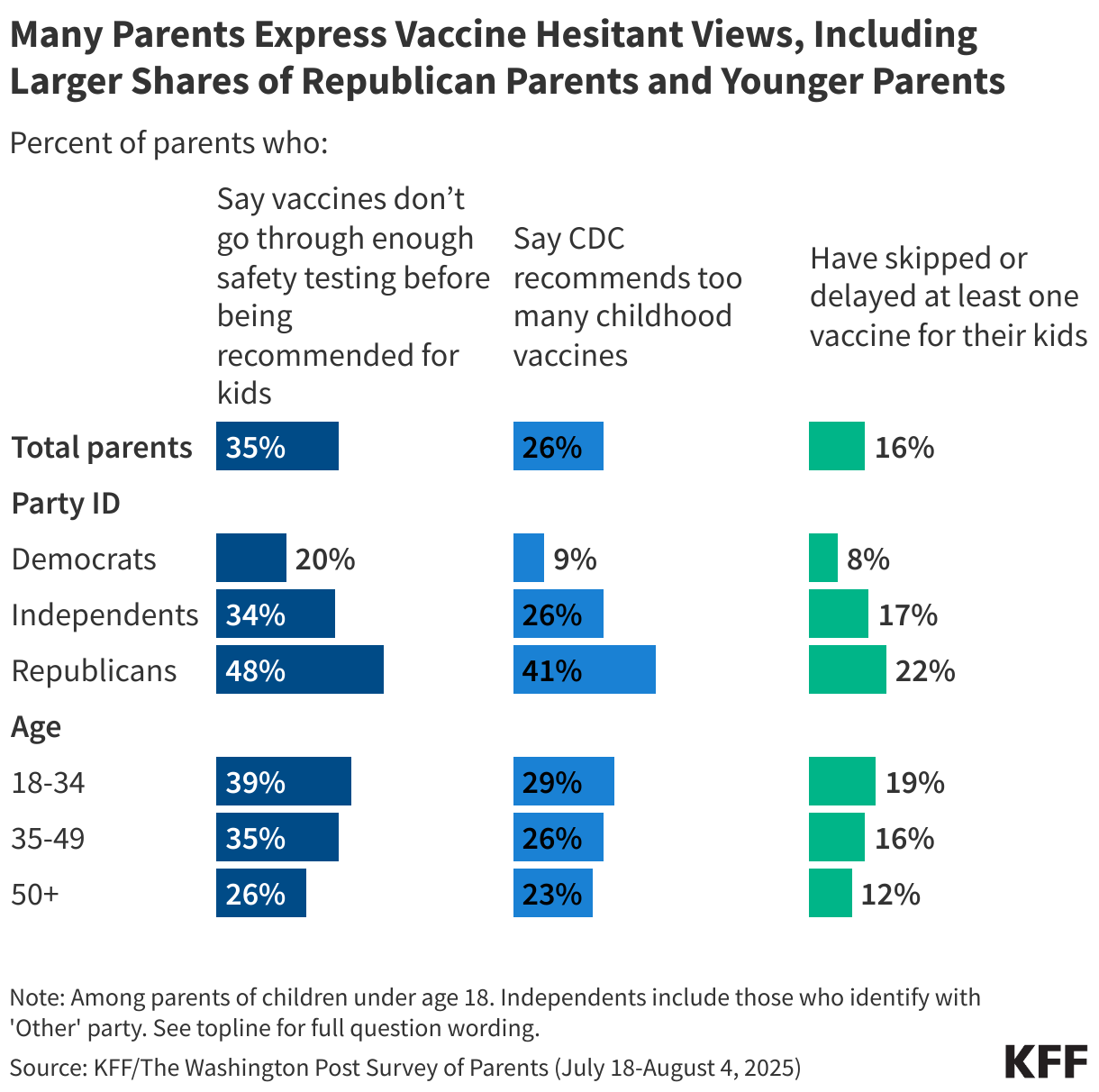
Most parents report keeping their children up to date on childhood vaccines, but about one in six say they have ever skipped or delayed at least one childhood vaccine for any of their children (excluding seasonal vaccines like flu and COVID-19). Despite strong uptake, many parents express skepticism towards vaccine safety testing and the number of vaccines recommended by the CDC (this survey was fielded prior to recent changes to the childhood vaccine schedule announced by HHS in January 2026). Younger parents and those who identify as Republicans are more likely than their counterparts to endorse vaccine-skeptical attitudes and to report skipping vaccines for their own children. For more information, see the KFF/Washington Post Survey of Parents.
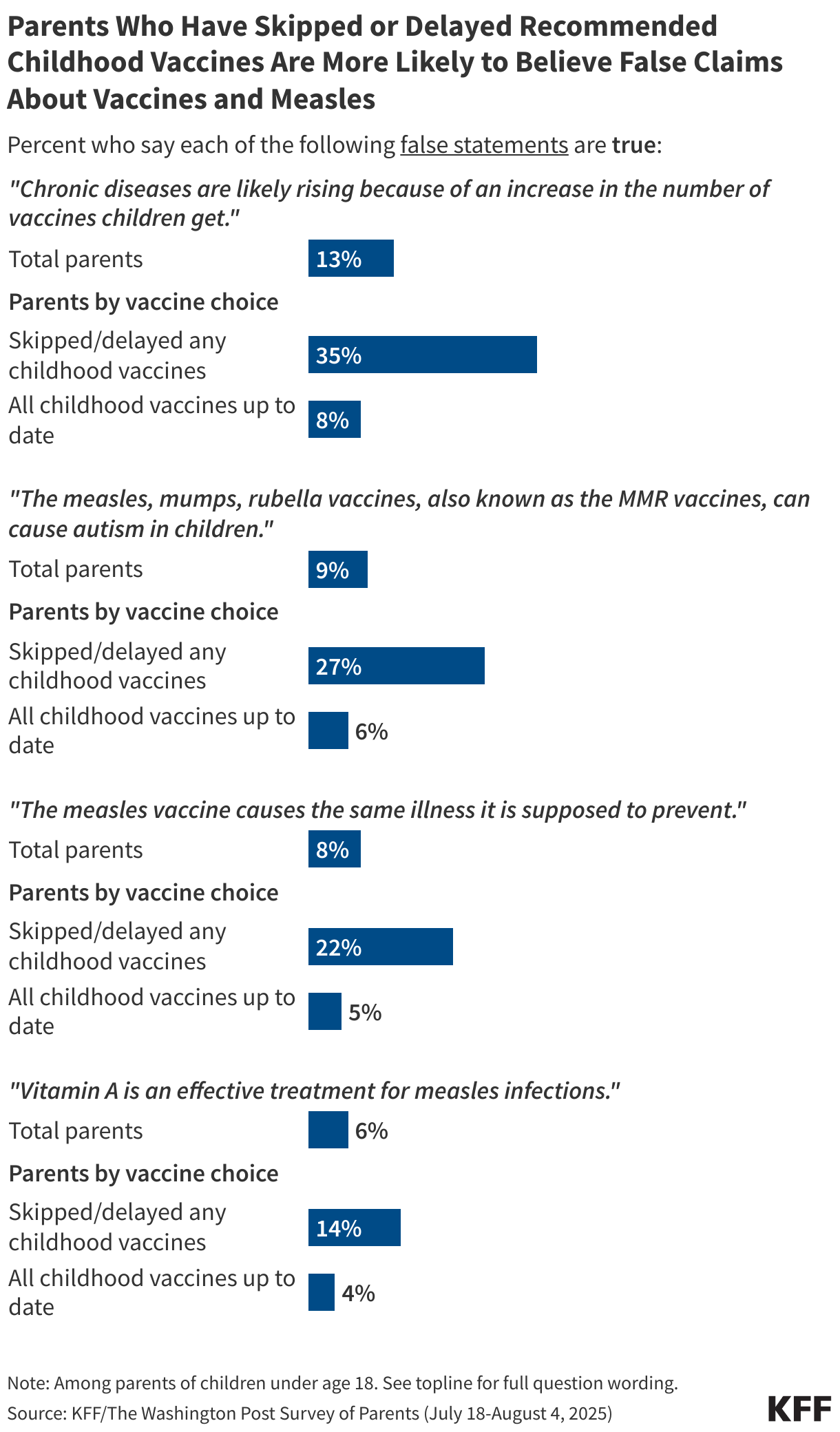
The KFF/Washington Post Survey of Parents tested belief in several false, misleading, or unproven claims amplified by HHS Secretary Robert F. Kennedy Jr related to vaccines, measles, and autism. While few parents think these claims are true, parents who have skipped or delayed at least one recommended vaccine for their children are at least three times as likely as those who have kept their children up to date to say these false or unproven claims about vaccines or measles are true.
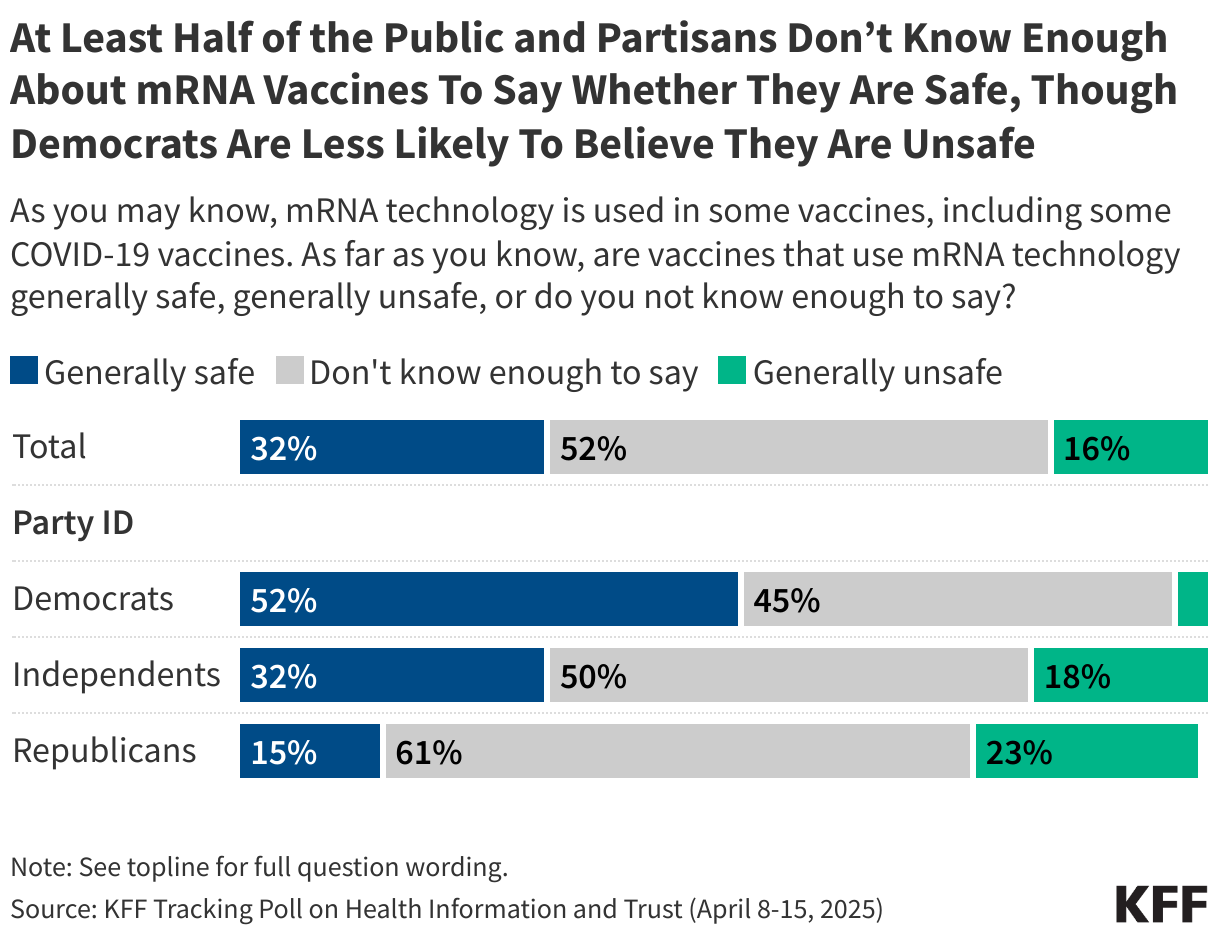
COVID-19 vaccines and some other vaccines currently under development rely on a vaccine technology known as messenger-RNA (mRNA), which has long been the subject of misinformation. While few adults view mRNA technology as unsafe, the technology remains obscure to much of the public, with about half saying they don’t know enough to say. For more information, see KFF’s April 2025 Tracking Poll on Health Information and Trust.
News Release
MAHA Health Concerns Resonate Broadly but Lag Behind Health Care Costs Even for MAHA Voters
MAHA Voters Are More Supportive Than Other Voters of the Trump Administration's Food and Vaccine Policy Though Less Than 1 in 3 "Strongly Approve"
Chemical food additive and pesticide concerns associated with the Make America Health Again (MAHA) movement are shared broadly across the public. But when it comes to voters, health care costs are a higher priority and bigger motivator, even among MAHA supporters, a new KFF Health Tracking Poll finds.
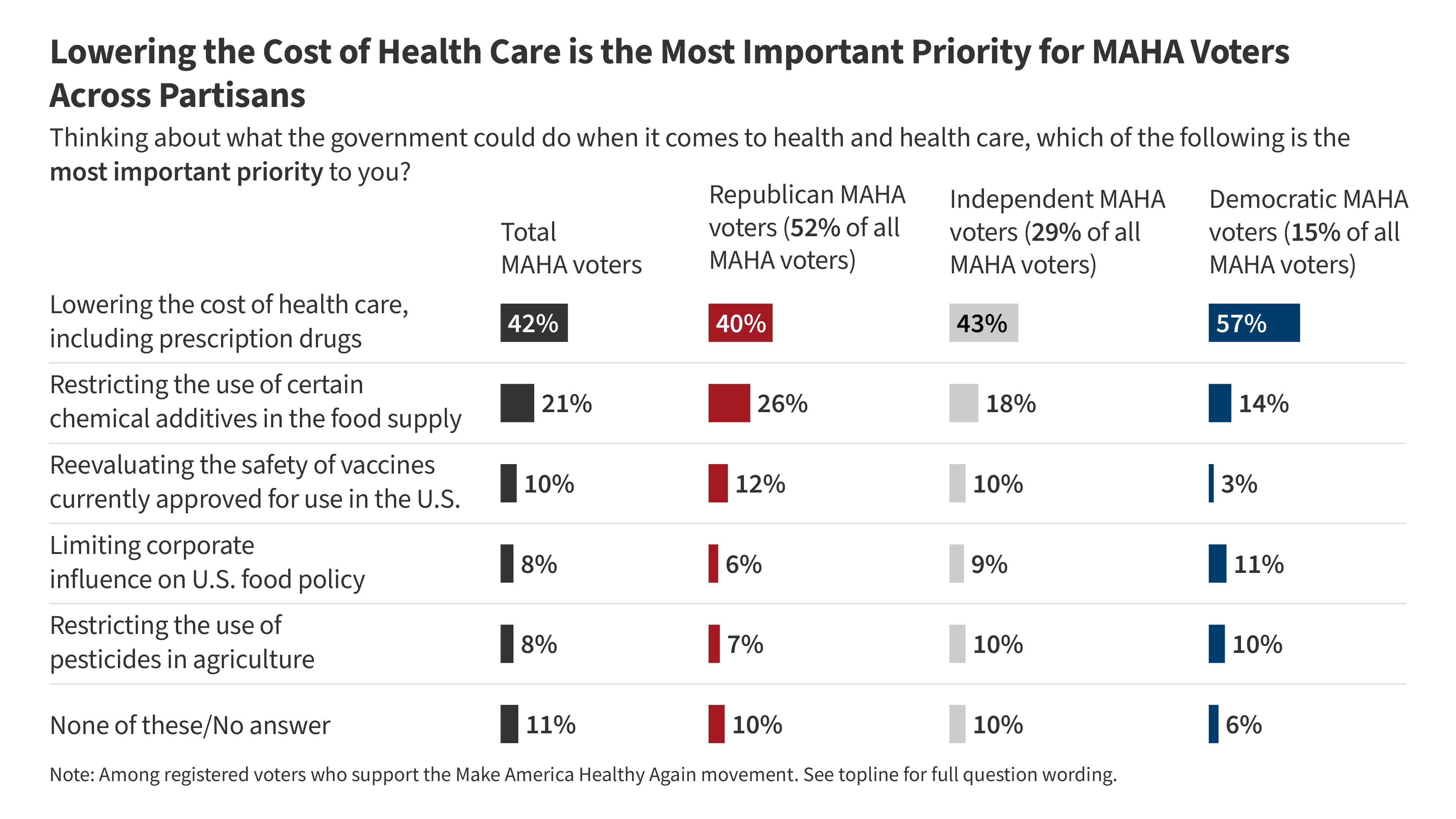
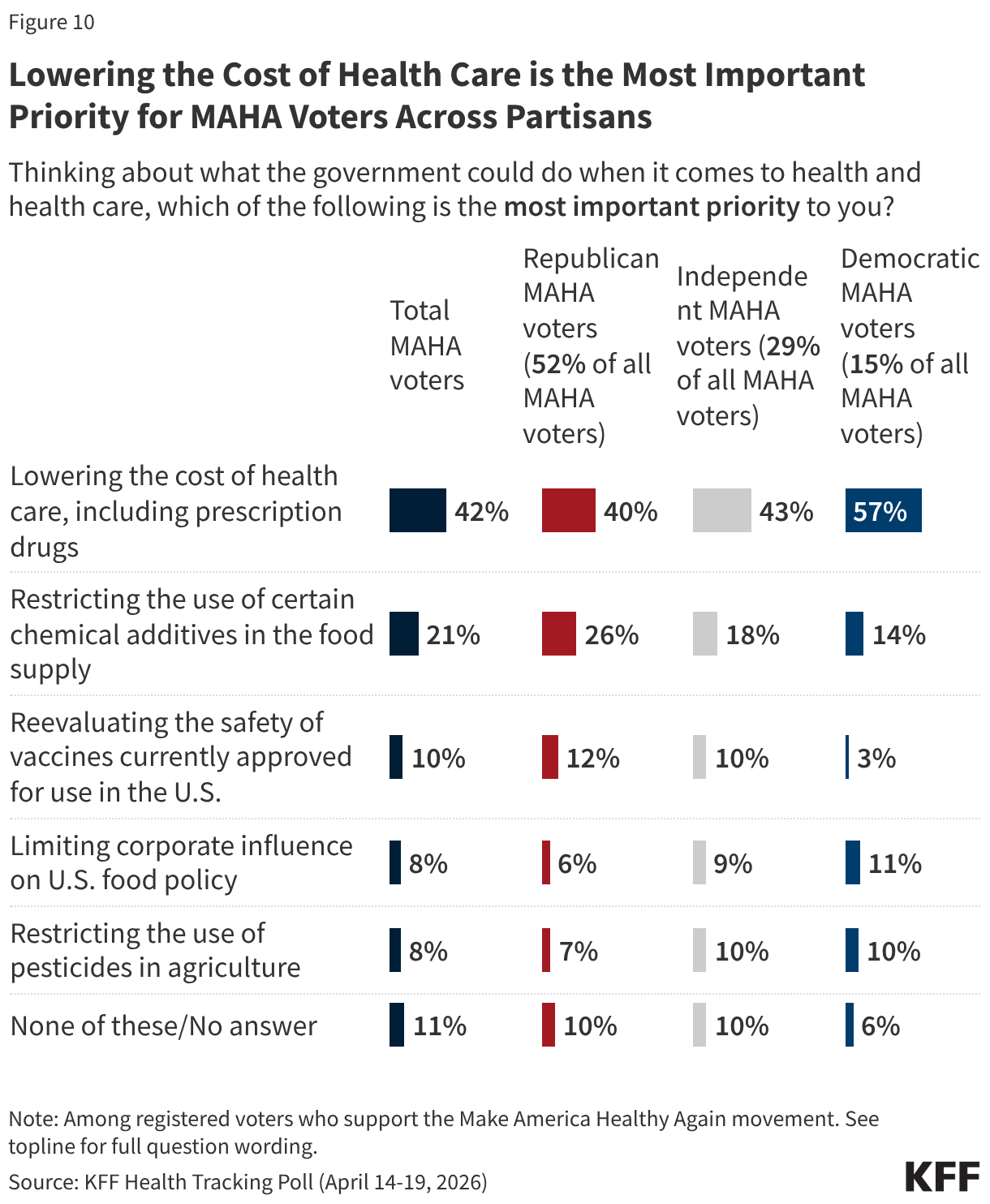
When asked to identify their most important health priority for government to address, far more MAHA-supporting voters identify lowering the cost of health care (42%) than other issues more closely associated with the movement, such as restricting the use of chemical additives in the food supply (21%), reevaluating the safety of vaccines (10%), limiting corporate influence on food policy (8%), or restricting the use of pesticides in agriculture (8%).
At least half of MAHA voters also say that the cost of health care will have a “major impact” on their decision to vote (51%) and which party’s candidate they will support (56%) in the upcoming midterms. That’s more than say the same about vaccine policy (36% say it will impact their decision to vote, 40% say it will impact which candidate they will support) or food safety (43% say it will impact their decision to vote, 45% say it will impact which candidate they will support), two issues closely aligned with MAHA, a movement promoted by the Trump administration and by Health and Human Services (HHS) Secretary Robert F. Kennedy Jr.
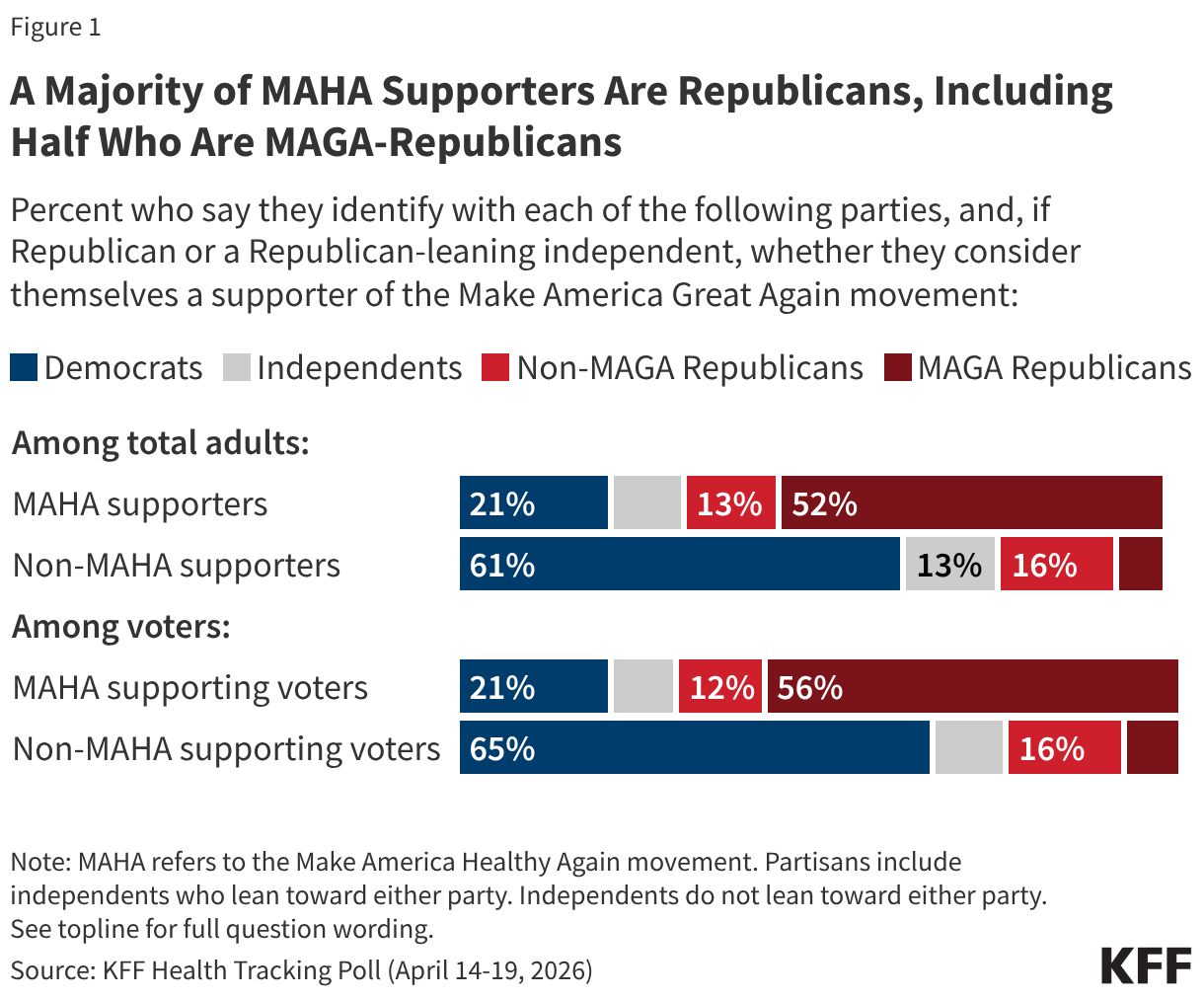
Overall, about four in ten (41%) adults—and a similar share of voters (43%)—say they are supporters of the MAHA movement, with support closely tied to partisanship and support of President Trump’s Make America Great Again (MAGA) movement.
Among voters who support MAHA, about half (52%) identify as Republicans, 29% identify as independents, and about one in seven (15%) identify as Democrats. A majority (56%) of MAHA voters identify as Republican or Republican-leaning and support the MAGA movement. The pattern of prioritizing health costs ahead of other MAHA issues is consistent across these partisan subgroups.
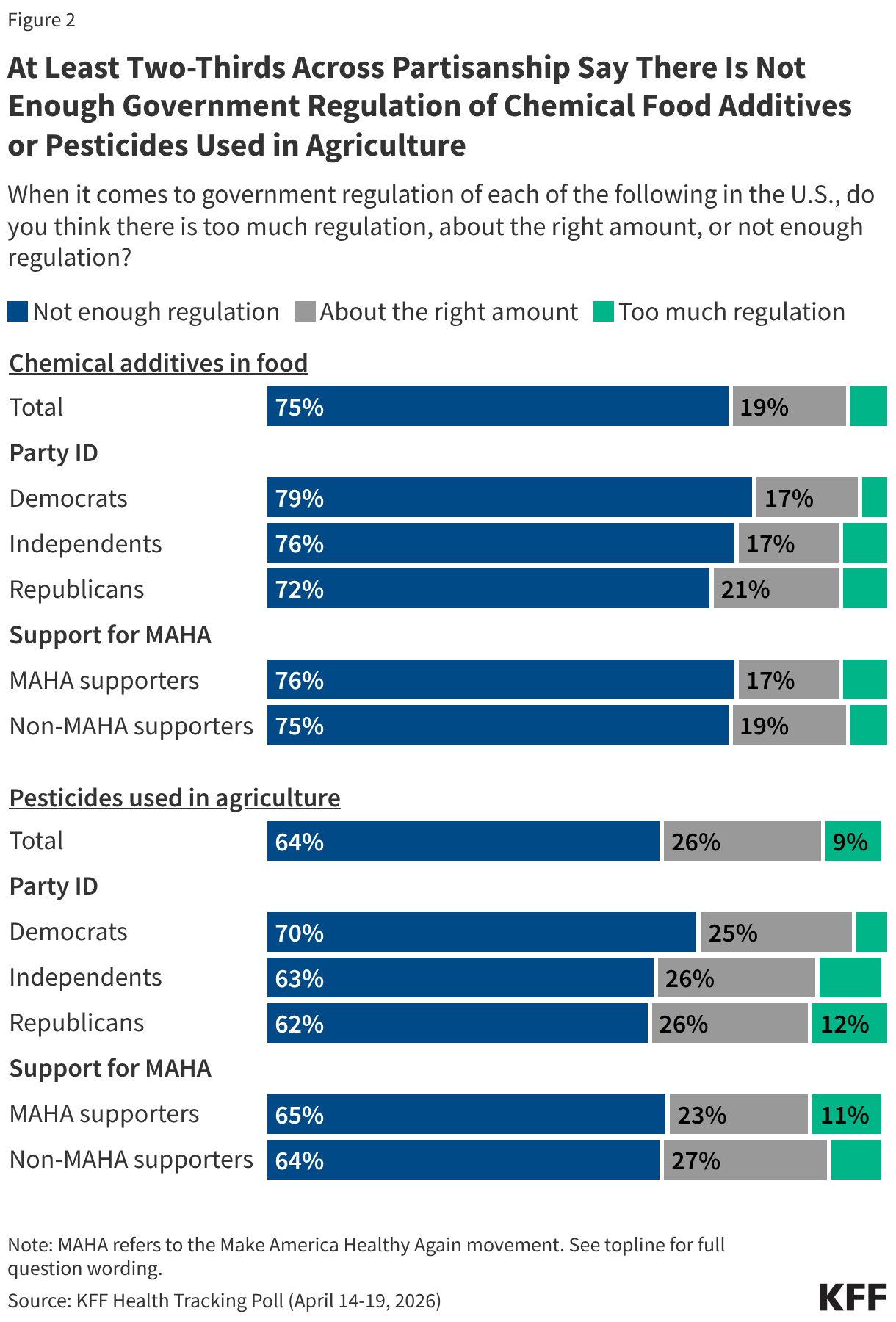
Other MAHA Health Concerns Are Shared by the Broader Public Majorities of the public say there is not enough regulation of chemical additives in food (75%) or of pesticides used in agriculture (64%)—including majorities across partisans, among MAHA supporters, and those who do not support the movement.
Most of the public—across partisans and MAHA supporters—also share a distrust of federal health agencies and food and drug industries:
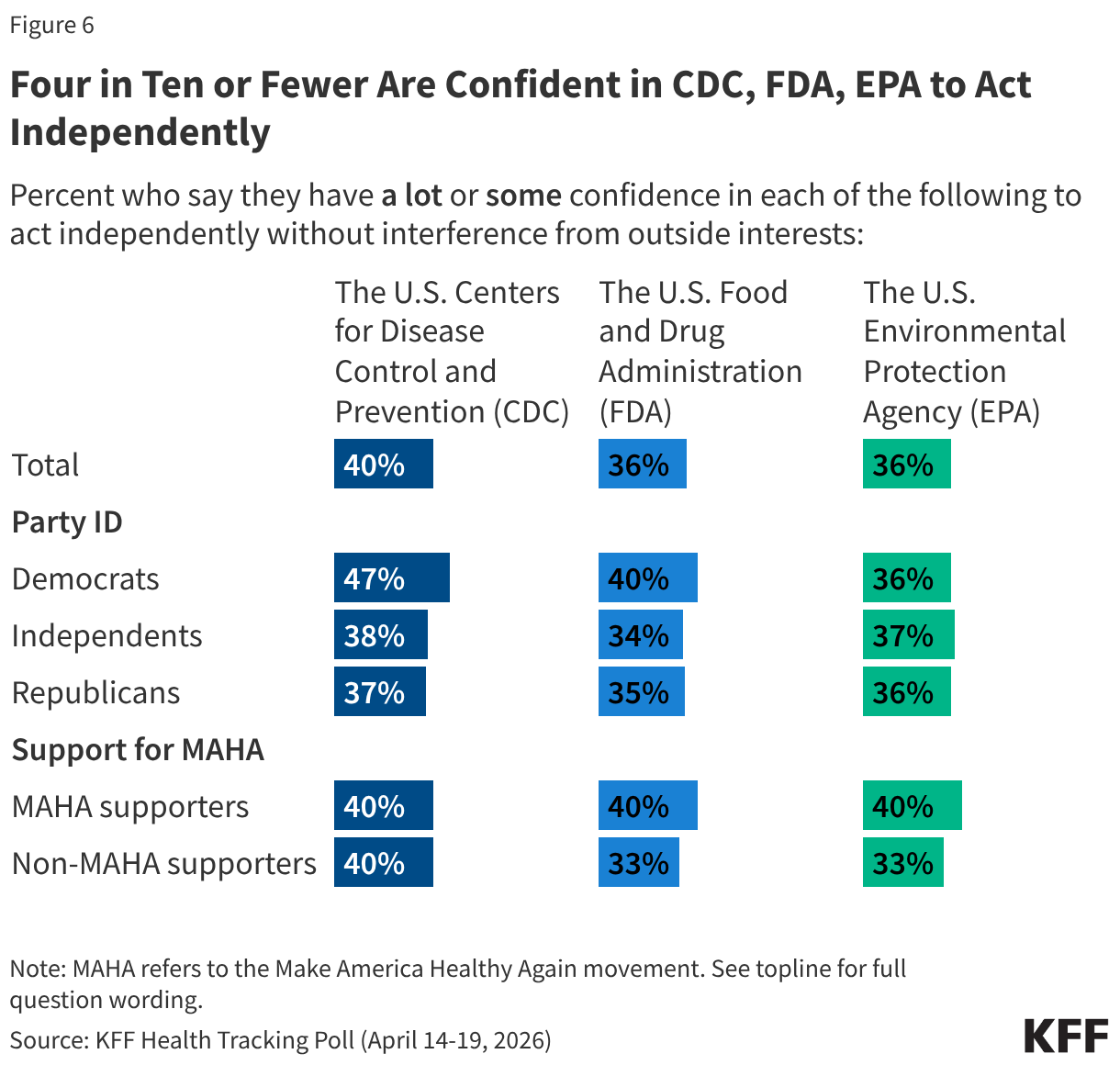
Four in ten or fewer adults say they have at least some confidence in the U.S. Centers for Disease Control and Prevention (CDC: 40%), the U.S. Food and Drug Administration (FDA: 36%), or the U.S. Environmental Protection Agency (EPA: 36%) to act independently without interference from outside interests. Democrats are more likely than Republican or independent adults to trust the CDC, but partisan differences largely disappear for the FDA and EPA.
Less than half of U.S. adults trust agricultural companies (40%), food and beverage companies (25%), or pharmaceutical companies (21%) to act in the public’s best interest. Low levels of trust in these industries are also present across partisans.
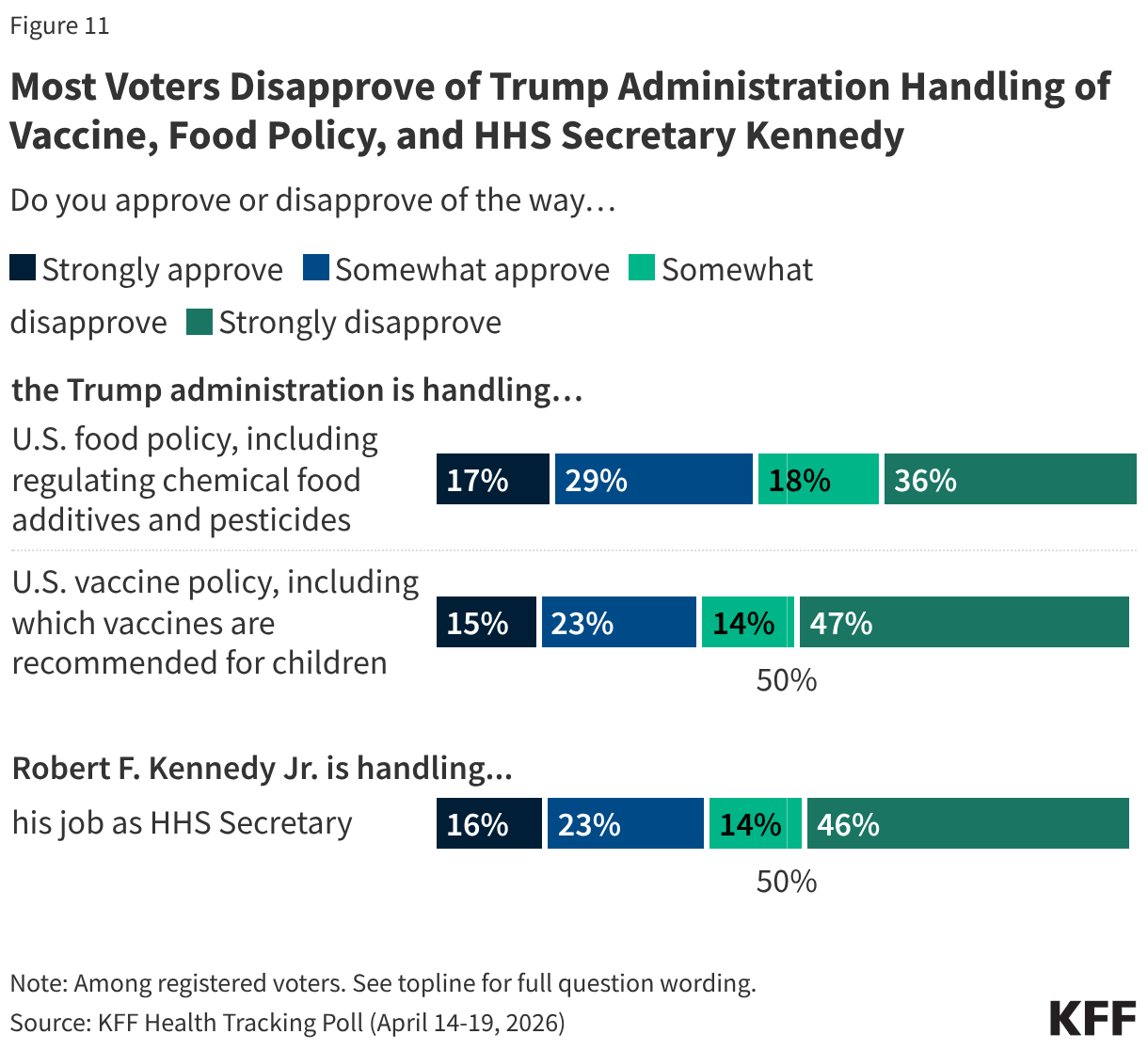
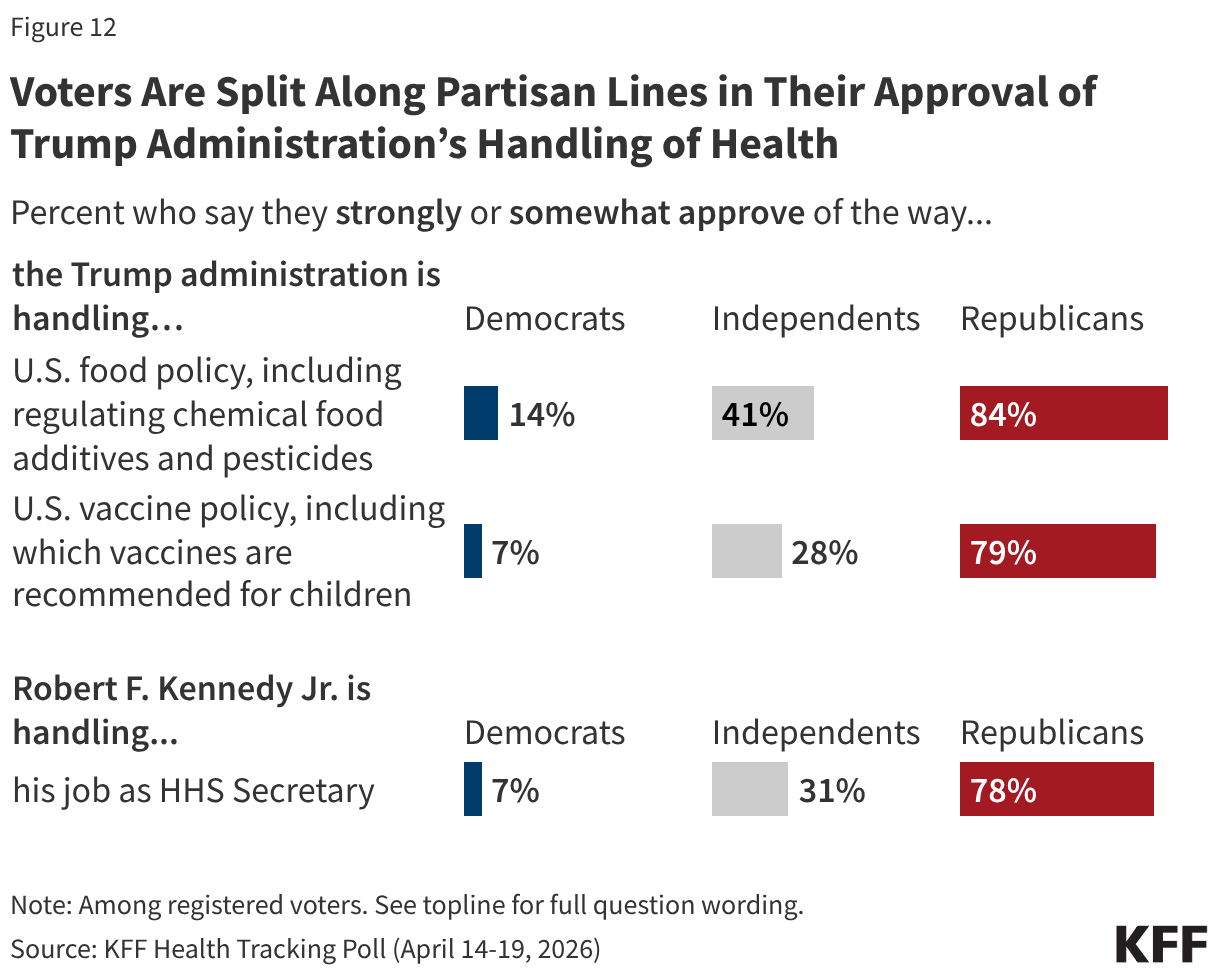
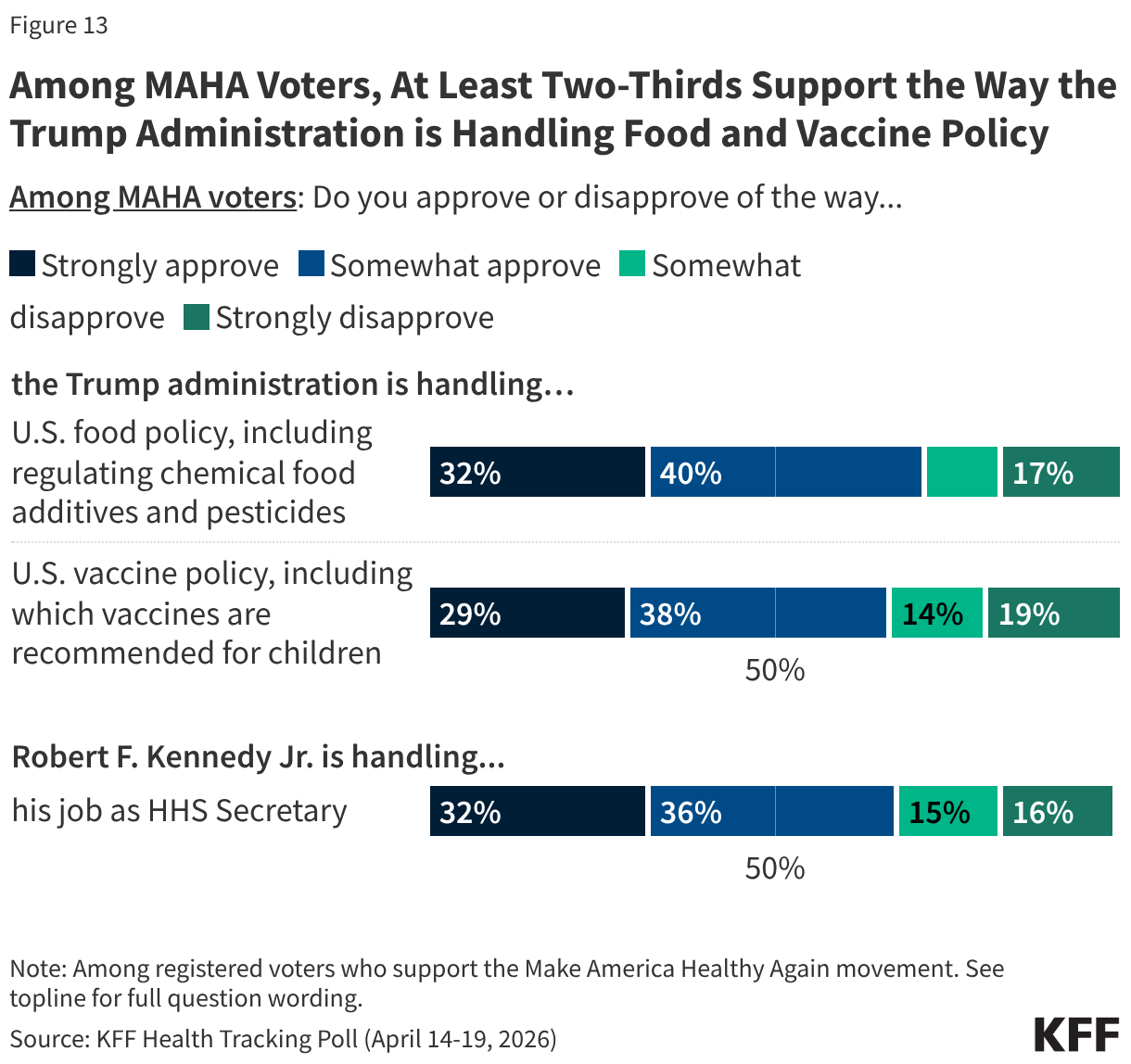
About 1 in 3 MAHA Voters Strongly Approve of HHS Secretary Kennedy’s Job Performance MAHA voters approve more than other voters of how the Trump administration is handling food policy, including chemical additives and pesticides (72% vs. 27%), and vaccine policy (67% vs. 17%), as well as how HHS Secretary Robert F. Kennedy Jr. is handling his job (69% vs. 17%). However, less than one-third of MAHA voters “strongly approve” of the Trump administration on food policy (32%) and vaccine policy (29%) and of the HHS Secretary’s handling of his job (32%)—while similar shares of MAHA voters disapprove in all three areas. This is a fairly tepid rating for a group that aligns with Kennedy’s signature movement.
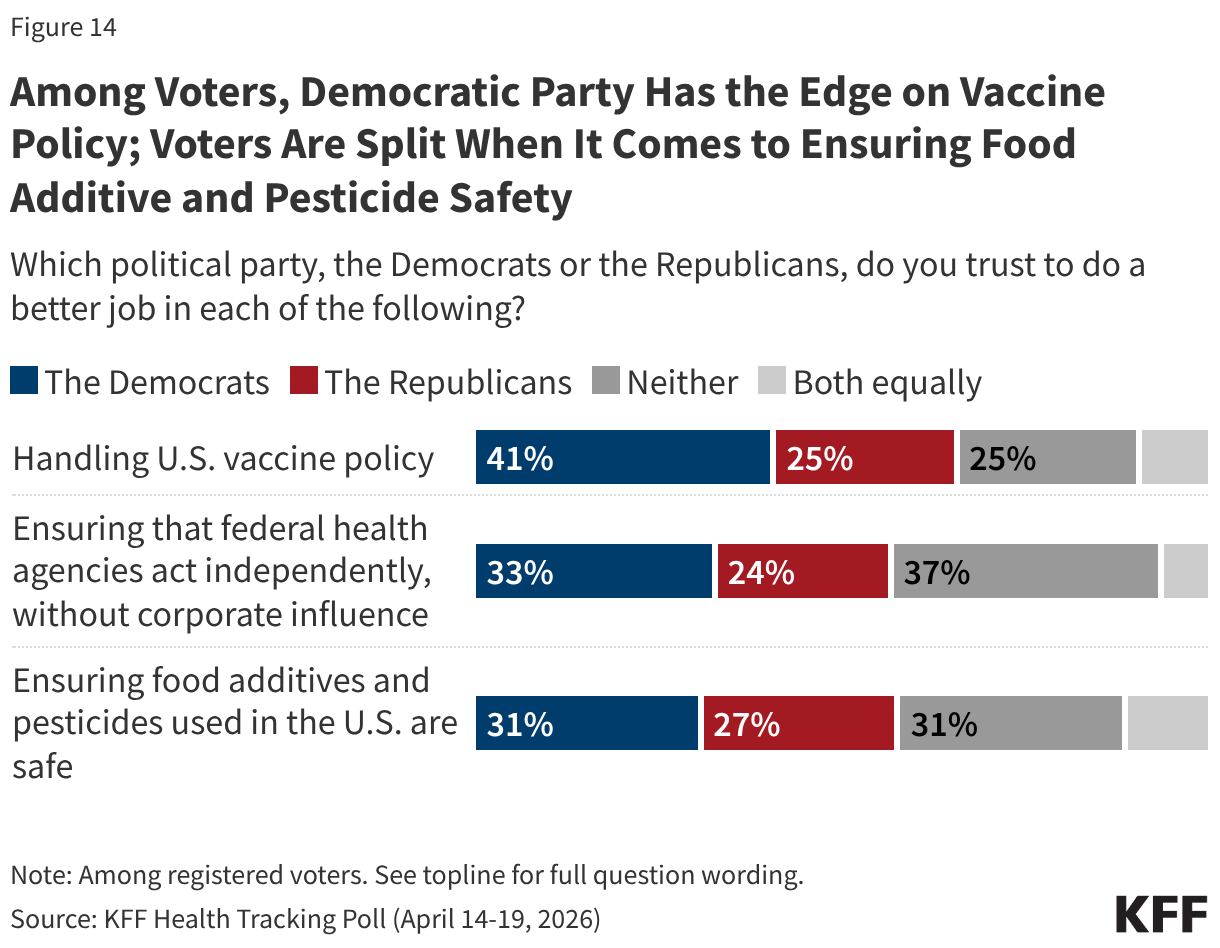
Overall, voters are evenly divided on whether they trust Democrats (31%) or Republicans (27%) to handle the safety of food additives and pesticides, and a similar share (31%) gives neither party the advantage on this issue. Meanwhile, the Democratic Party holds the advantage over the Republican Party in who voters trust to handle vaccine policy (41% vs. 25%) and ensure that federal health agencies act independently without corporate influence (33% vs. 24%).
Designed and analyzed by public opinion researchers at KFF, this survey was conducted April 14-19, 2026, online and by telephone among a nationally representative sample of 1,343 U.S. adults in English and in Spanish. The margin of sampling error is plus or minus three percentage points for the full sample. For results based on other subgroups, the margin of sampling error may be higher.
About four in ten (41%) U.S. adults say they support the Make America Healthy Again (MAHA) movement – a group largely made up of Republicans and supporters of the Make America Great Again (MAGA) movement. Yet, many of the concerns elevated by the MAHA movement about food safety and corporate influence resonate with a larger share of the public beyond those who identify as supporters. Majorities of the public say there is not enough regulation of chemical additives in food (75%) or of pesticides used in agriculture (64%) in the U.S., and most adults express distrust in agricultural, food, and pharmaceutical companies to act in the public’s best interest. At the same time, confidence in the government agencies that are tasked with regulating these industries is low across partisans; about a third of the public express confidence in the FDA (36%) and the EPA (36%) to act independently without outside interference.
Even as MAHA issues resonate, the cost of health care is a more prominent focus for voters than issues like food and vaccine policy. Most voters say health costs will have a “major impact” on their decision to vote (55%) and who they vote for (61%) in November, compared to about four in ten who say the same of vaccine or food policy. Even among voters who support the MAHA movement, health care costs are the dominant priority by a wide margin when compared with other areas of health. When asked to select the most important health priority for the federal government, four in ten MAHA voters (42%) choose lowering health costs, twice the share who choose restricting chemical additives in the food supply (21%) and far outranking other MAHA priorities like reevaluating vaccine safety (10%), limiting corporate influence in U.S. food policy (8%), or restricting pesticide use in agriculture (8%).
Voters overall give the Trump administration low approval ratings on two key health areas elevated by the MAHA movement; about four in ten approve of the administration’s handling of vaccine policy (38%), and fewer than half approve of the administration’s handling of food policy (46%). The Democratic Party holds the advantage over the Republican Party in who voters trust to handle vaccine policy (41% vs. 25%) and to ensure federal health agencies act independently without corporate influence (33% vs. 24%). Voters are more evenly divided on whether they trust Democrats (31%) or Republicans (27%) to handle the safety of food additives and pesticides, or neither party (31%).
Who Are MAHA Supporters?
Make America Healthy Again (MAHA) is the political and public health movement promoted by the Trump administration and led by Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. The movement has elevated issues such as vaccine safety, the role of corporate interests in federal health agencies, and the presence of chemical additives and pesticides in the food supply. KFF’s latest Health Tracking Poll shows about four in ten adults say they are supporters of the MAHA movement, but some of the concerns elevated by the MAHA movement resonate well beyond its core supporters.
Overall, about four in ten (41%) adults – and a similar share of voters (43%) – say they are supporters of the MAHA movement, with support closely tied to partisanship and support of the Make America Great Again (MAGA) movement. Two-thirds of MAHA supporters identify as Republican or Republican-leaning independents, including about half (52%) who are supporters of the MAGA movement. Far fewer MAHA supporters are Democrats or Democratic-leaning independents (21%) or independents who do not lean toward either political party (10%). Among registered voters who support MAHA, the partisan composition is similar.
Among MAHA-supporting voters, just over half say they “strongly” support the movement (55%) and 45% say they “somewhat” support it, translating to about one in four voters overall as strong MAHA supporters (24%) and one in five who “somewhat” support it (19%).
When asked specifically why they support the MAHA movement, supporters give a range of answers, with the two most common relating to generally wanting people to be healthier (19%) and removing or regulating harmful substances in food (15%). Some MAHA supporters mention improving nutritional habits for Americans (7%) or lowering obesity rates (7%). Five percent of MAHA supporters cite health care access and affordability as their reasons for supporting the movement, despite the MAHA movement’s lack of focus on these issues. Just 4% of MAHA supporters cite vaccines and medical choice as their reason for supporting the movement. Few MAHA supporters specifically express support for President Trump or HHS Secretary Robert F. Kennedy Jr. (2%) as their reasoning for supporting the movement.
In Their Own Words: What is the Main Reason You Support the MAHA Movement?
“It is morally correct. We don’t want to poison our kids with vaccines they don’t need. We don’t want to eat food that leads to morbidity to make companies’ profit margins higher,” 43-year-old Republican man, Pennsylvania
“America uses far too much harmful ingredients that most other countries ban,” 28-year-old independent man, Indiana
“To get people healthier so taxpayers don’t have to pay for their health care,” 58-year-old Republican woman, Kentucky
“We should be promoting healthier lifestyles in the country,” 29-year-old Republican woman, Iowa
“The MAHA movement gives patients more freedom to choose the doctors they actually want to see…While I support it for now, I'll be waiting to see how these policies are actually implemented,” 39-year-old independent man, Washington
“It’s about making the next generation healthy,” 27-year-old independent woman, Arizona
“I followed Kennedy before he was in office and I’m hoping that he will continue with what he stood for before,” 51-year-old independent woman, Tennessee
“Health care should be a right,” 65-year-old Democratic man, New York
Where MAHA Concerns Resonate With the Public: Food Safety, Pesticides, and Industry Influence
Among the public, there is broad, bipartisan agreement that there is not enough government regulation of chemical additives in food and pesticides in agriculture in the U.S. Three-quarters of adults say there is not enough government regulation of chemical food additives, and about two-thirds (64%) say the same about pesticides used in agriculture. Majorities across partisan lines and among both MAHA supporters and those who do not support the movement agree, suggesting this is an area where MAHA’s concerns align with broader public sentiment.
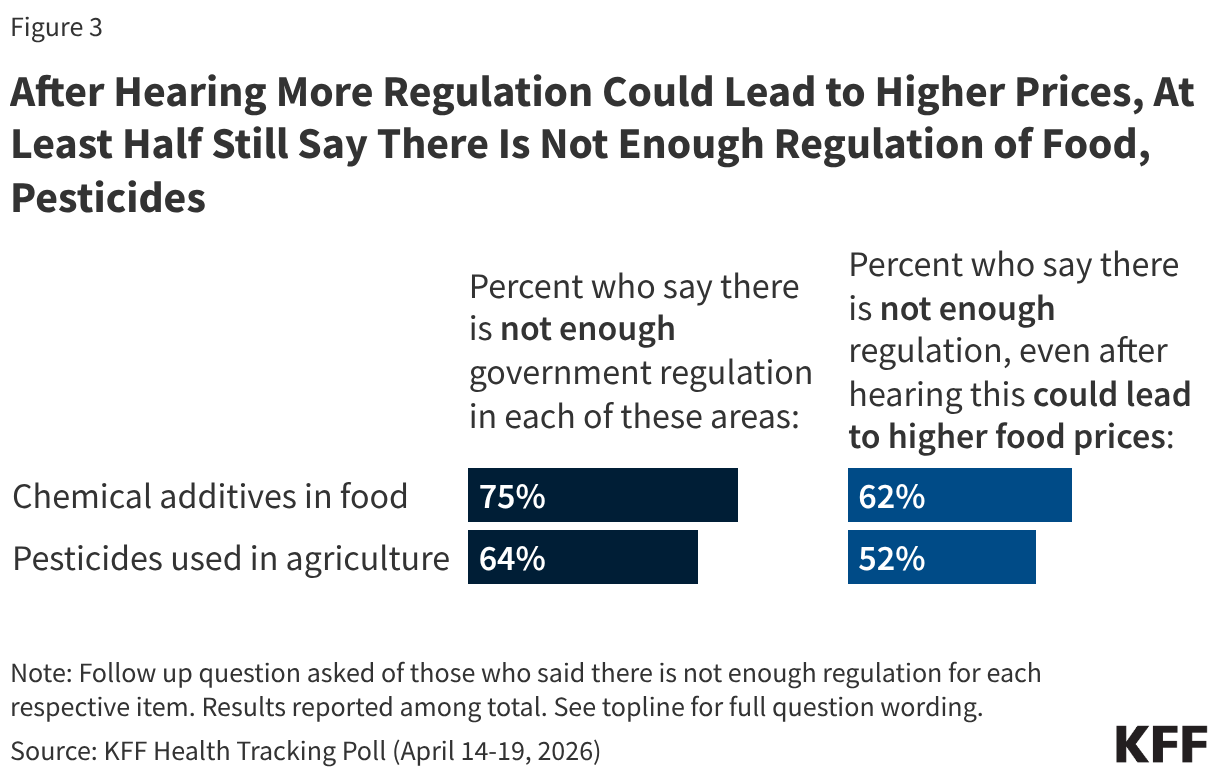
Some food industry groups and public health experts have argued that restrictions on approved food ingredients could limit access to affordable groceries for families in the U.S. When those who originally said there is “not enough regulation” of chemical additives in food or pesticides used in agriculture are presented with the caveat that increased regulation could lead to higher food prices for consumers, most still support increased regulation. But the possibility of increased costs does move some people. The share saying there is not enough regulation of food additives drops by 13 percentage points after hearing that increased regulation could increase costs (from 75% to 62%), with a similar drop in the share who maintain that there is not enough regulation of pesticides (from 64% to 52%).
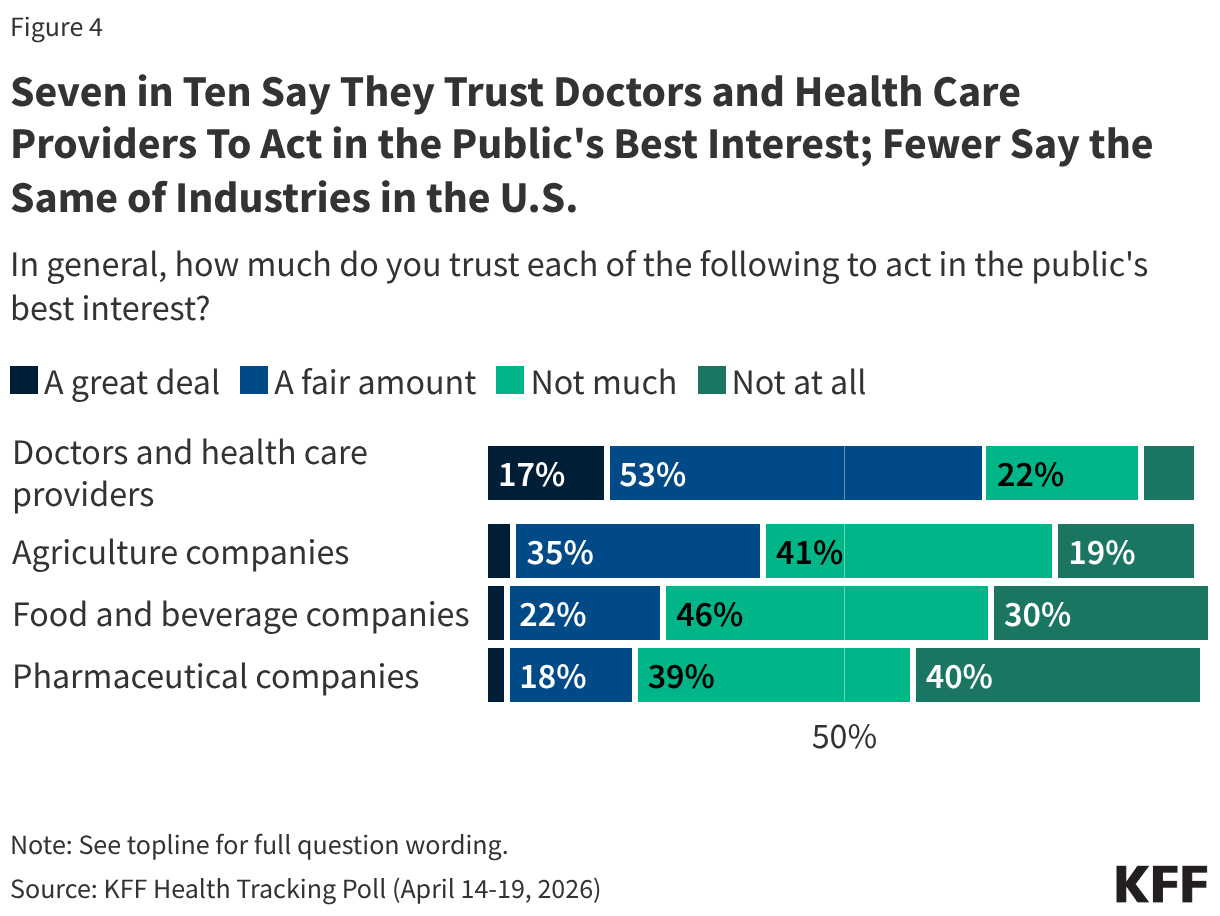
The public perception that there is not enough regulation may be rooted in broader skepticism toward the industries themselves. Most U.S. adults do not trust pharmaceutical companies, food and beverage companies, or agricultural companies to act in the public’s best interest. One in four or fewer adults say they trust food and beverage companies (25%) or pharmaceutical companies (21%) “a great deal” or “a fair amount” to act in the public's best interest, while a somewhat larger share (40%) trust agricultural companies on this measure. Very small shares – fewer than 5% – trust each of these groups “a great deal” to act in the public’s best interest.
By contrast, seven in ten adults say they trust doctors and health care providers at least “a fair amount” to act in the public’s best interest.
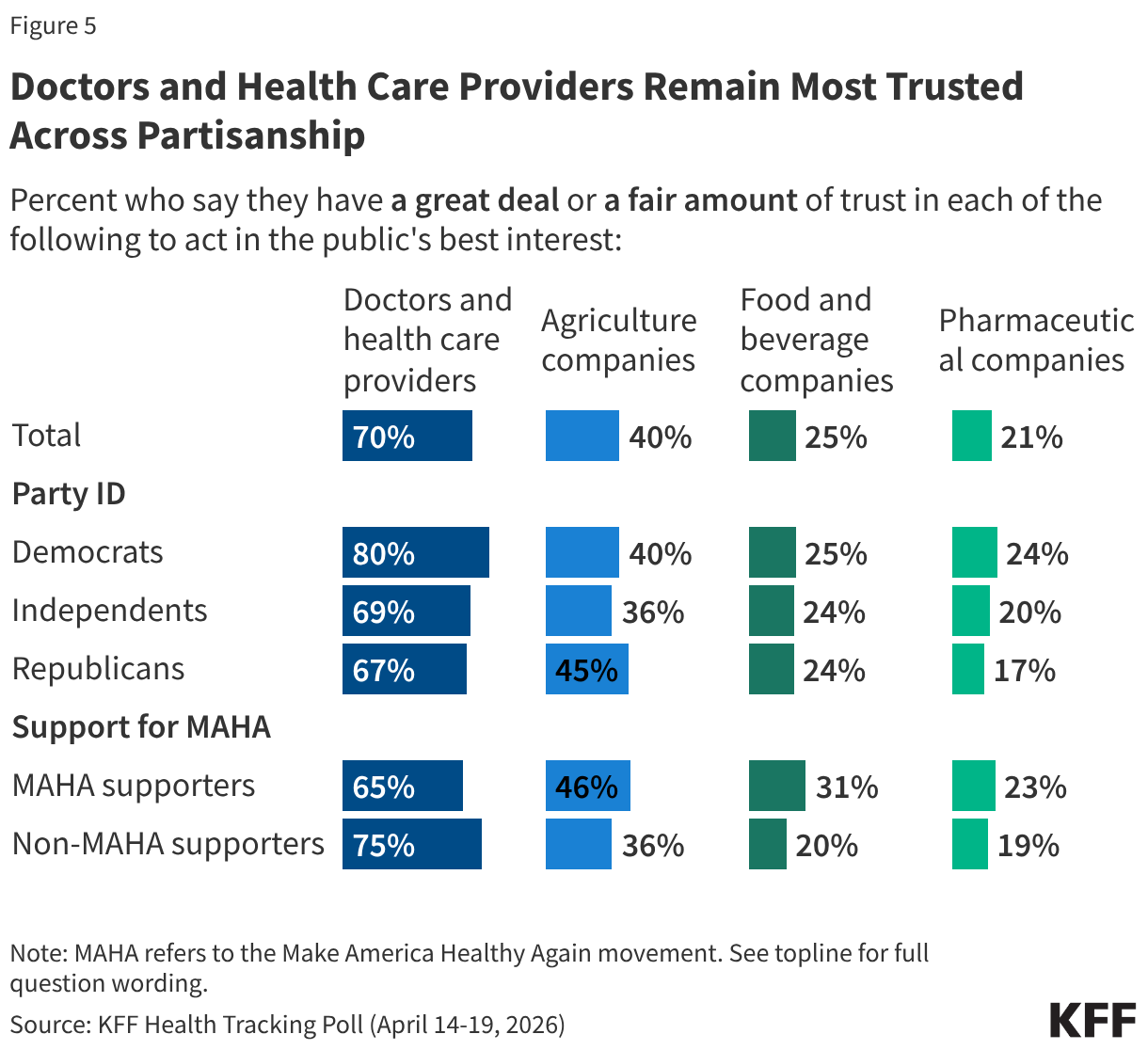
Across partisanship, and among those who do and do not support the MAHA movement, fewer than half trust agricultural companies, food and beverage companies, or pharmaceutical companies to act in the public’s best interest. However, most Democrats (80%), independents (69%), and Republicans (67%) have a great deal or a fair amount of trust in doctors and health care providers to act in the public’s best interest.
Confidence in the government agencies with major responsibilities for food safety and public health is low across partisans. Four in ten or fewer adults say they have “a lot” or “some” confidence in the U.S. Centers for Disease Control and Prevention (CDC) (40%), U.S. Food and Drug Administration (FDA) (36%), or the U.S. Environmental Protection Agency (EPA) (36%) to act independently without interference from outside interests. Democrats are slightly more likely than Republicans or independents to express confidence in the CDC (47% vs. 37% and 38%, respectively), but partisan differences largely disappear when it comes to confidence in the FDA and EPA.
U.S. adults who support the MAHA movement and those who do not are similarly skeptical. Four in ten MAHA supporters say they are confident in each of these agencies to act independently, leaving six in ten MAHA supporters who have “a little” or “no confidence at all.”
MAHA and Other Health Care Issues in the Election
Despite the resonance of these issues elevated by the MAHA movement, health care costs overshadow these concerns for voters heading into the 2026 midterm elections. Previously released findings from the April 2026 KFF Health Tracking Poll show health care costs remain a primary economic concern for the public. Reflecting that, costs are voters’ top health concern heading into the 2026 midterm elections, outweighing policy areas elevated by the MAHA movement, such as vaccines or food safety.
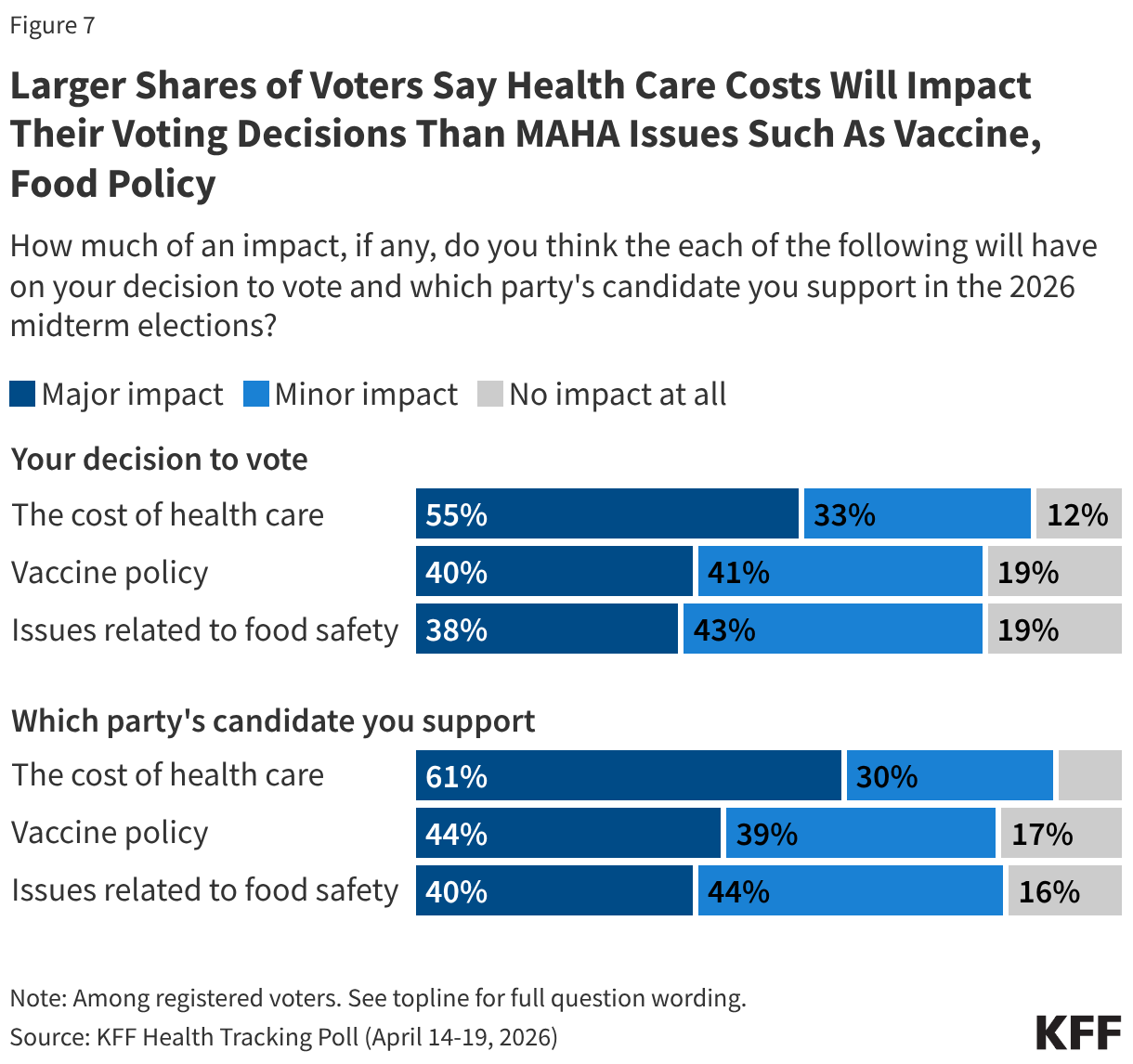
More than half of voters say health care costs will have a “major impact” on their decision to vote (55%) or which party’s candidate they will support (61%). When it comes to vaccine policy and food policy, about four in ten voters say these issues will have a “major impact” on their decision to vote or which party’s candidate they will support, at least 15 percentage points lower than the share who say the same about health care costs.
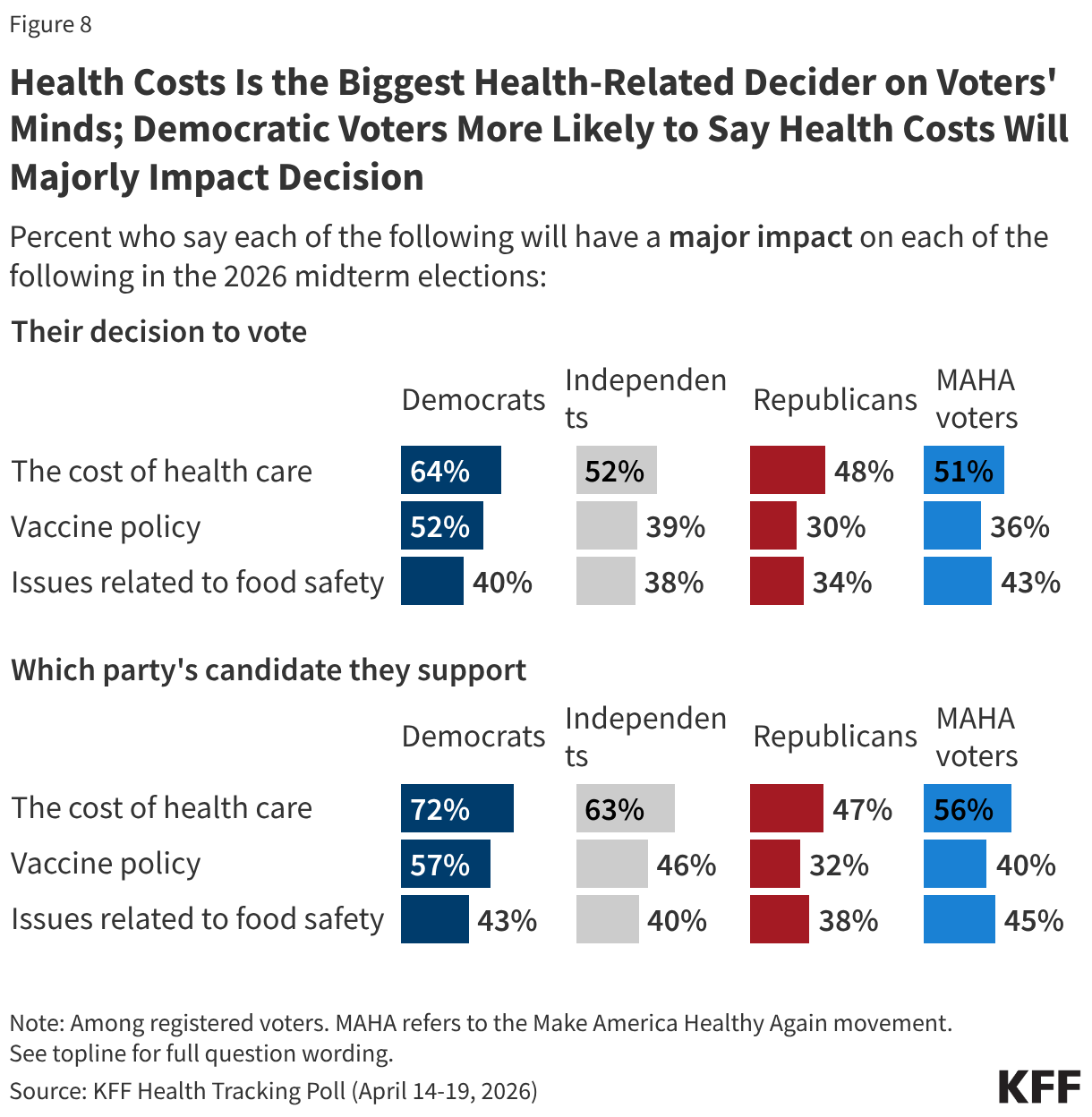
While the issue of health costs is more salient for Democratic voters than for Republicans, larger shares across partisans say health costs will have a major impact on their voting decisions than say the same about vaccine policy or food safety. For example, about half of independent voters (52%) say health care costs will have a major impact on their decision to turn out in November, compared to about four in ten who say the same about vaccine policy (39%) and food safety (38%). Patterns are similar for Republican voters (48%, 30%, and 34%, respectively) and Democratic voters (64%, 52%, and 40%, respectively).
Among voters who say they support the MAHA movement – a majority (56%) of whom identify as MAGA Republicans – at least half say the cost of health care will have a major impact on their decision to vote (51%) or which party’s candidate they support (56%). Despite the MAHA movement elevating issues such as vaccine and food safety, fewer MAHA voters – about four in ten – say vaccine policy or issues of food safety will majorly impact their voting decisions.
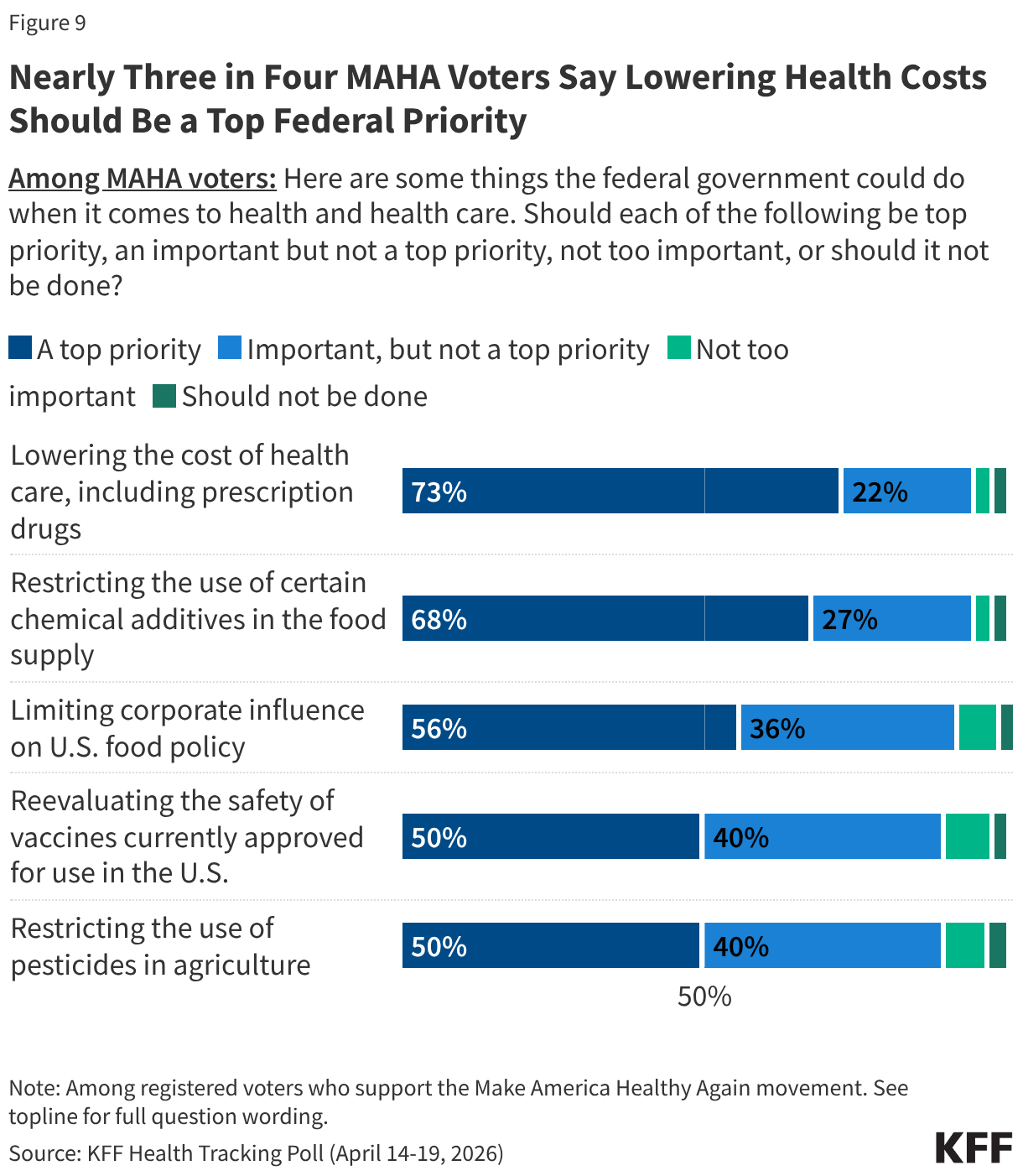
MAHA-supporting voters express broad enthusiasm for federal action across the movement’s core agenda, but once again, health care costs remain the dominant priority. Nearly three-quarters of MAHA voters (73%) say lowering the cost of health care, including prescription drugs, should be a top priority for the federal government. This is followed by restricting the use of certain chemical additives in the food supply (68%) and limiting corporate influence on U.S. food policy (56%). Half of MAHA voters say reevaluating the safety of vaccines currently approved for use or restricting the use of pesticides in agriculture should be top priorities. Across all five items, one in ten or fewer MAHA voters say any of these efforts are “not too important” or “should not be done.”
When asked to choose the single most important health priority to them, about four in ten MAHA-supporting voters (42%) choose lowering the cost of health care, including prescription drugs—twice the share who say the same of restricting chemical additives in the food supply (21%). Fewer cite reevaluating vaccine safety (10%), limiting corporate influence in U.S. food policy (8%), or restricting pesticide use in agriculture (8%) as their single top priority.
The cost of health care tops the list of health care priorities for MAHA voters regardless of partisanship. Among voters who support the MAHA movement, six in ten Democrats (57%) and four in ten independents (43%) and Republicans (40%) say lowering the cost of health care is the most important priority. For each of these groups, health care costs rank at least 14 percentage points ahead of restricting the use of chemical additives in food, and even further ahead of issues like reevaluating vaccine safety and restricting pesticide use.
Trump Administration Approval and Party Preference on MAHA Health Issues
Voters give the Trump administration low approval ratings on two key policy areas elevated by the MAHA movement. Just under half (46%) of voters approve of the administration’s handling of food policy, and a larger share (54%) disapprove. Just a few months after the changes made to the childhood vaccine schedule by HHS, about four in ten voters approve of the administration’s handling of U.S. vaccine policy (38%) and six in ten (61%) disapprove, including about half (47%) who “strongly disapprove.”
As the head of the MAHA Commission and Secretary of Health and Human Services, Robert F. Kennedy Jr. is the spokesperson for many of the administration’s federal health policies. About four in ten voters say they approve of the way Secretary Kennedy is handling his job (39%) and six in ten disapprove, including nearly half (46%) who “strongly disapprove.”
Unsurprisingly, voters are split along partisan lines, with the Trump administration receiving high approval ratings from Republicans on food and vaccine policy as well as Secretary Kennedy’s handling of his job at HHS, and most Democrats disapproving.
Despite Secretary Kennedy’s leadership at HHS and recent changes focused on MAHA priorities, approval of the administration’s handling of issues like vaccine policy is far from unanimous among the movement’s supporters. About seven in ten MAHA voters approve of the administration’s handling of food policy (72%) and vaccine policy (67%), and Secretary Kennedy’s handling of his job as Health Secretary (69%). On each of these areas, just a third “strongly” approve of the administration and a similar share disapprove: tepid ratings for a group that aligns with Kennedy’s signature movement.
With about six months until the 2026 midterm elections, the Democratic Party has a strong edge over the Republican Party when it comes to who voters trust to address vaccine policy, and a narrower edge on ensuring federal agencies act independently. Voters are split over who they trust to do a better job ensuring food additives are safe. Democrats have a double-digit advantage over Republicans when it comes to who voters trust to handle vaccine policy (41% vs. 25%). While the Democratic Party has a smaller advantage among voters on which party they trust to ensure that federal health agencies act independently without corporate influence (33% vs. 24%), nearly four in ten (37%) say they trust “neither party.”
Similar shares of voters say they trust the Democratic Party (31%), the Republican Party (27%), or “neither party” (31%) more when it comes to doing a better job ensuring food additives and pesticides in the U.S. are safe.
Methodology
This KFF Health Tracking Poll was designed and analyzed by public opinion researchers at KFF. The survey was conducted April 14 – April 19, 2026, online and by telephone among a nationally representative sample of 1,343 U.S. adults in English (n=1,251) and in Spanish (n=92). The sample includes 1,023 adults (n=81 in Spanish) reached through the SSRS Opinion Panel either online (n=999) or over the phone (n=24). The SSRS Opinion Panel is a nationally representative probability-based panel where panel members are recruited randomly in one of two ways: (a) Through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Groups (MSG) through the U.S. Postal Service’s Computerized Delivery Sequence (CDS); (b) from a dual-frame random digit dial (RDD) sample provided by MSG. For the online panel component, invitations were sent to panel members by email followed by up to three reminder emails.
Another 320 (n=11 in Spanish) adults were reached through random digit dial telephone sample of prepaid cell phone numbers obtained through MSG. Phone numbers used for the prepaid cell phone component were randomly generated from a cell phone sampling frame with disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity groups within each frame. Among this prepaid cell phone component, 140 were interviewed by phone and 180 were invited to the web survey via short message service (SMS).
Respondents in the prepaid cell phone sample who were interviewed by phone received a $15 incentive via a check received by mail or an electronic gift card incentive. Respondents in the prepaid cell phone sample reached via SMS received a $10 electronic gift card incentive. SSRS Opinion Panel respondents received a $5 electronic gift card incentive (some harder-to-reach groups received a $10 electronic gift card). In order to ensure data quality, cases were removed if they failed two or more quality checks: (1) attention check questions in the online version of the questionnaire, (2) had over 30% item non-response, or (3) had a length less than one quarter of the mean length by mode. Based on this criterion, no cases were removed.
The combined cell phone and panel samples were weighted to match the sample’s demographics to the national U.S. adult population using data from the Census Bureau’s 2024 Current Population Survey (CPS), September 2023 Volunteering and Civic Life Supplement data from the CPS, and the 2025 KFF Benchmarking Survey with ABS and prepaid cell phone samples. The demographic variables included in weighting for the general population sample are gender, age, education, race/ethnicity, region, civic engagement, frequency of internet use and political party identification. The weights account for differences in the probability of selection for each sample type (prepaid cell phone and panel). This includes adjustment for the sample design and geographic stratification of the cell phone sample, within household probability of selection, and the design of the panel-recruitment procedure. Initial coding for open-ended questions was done using BT Insights AI Platform and then reviewed, edited, and finalized by KFF researchers.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available on request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. KFF public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Episode 2, AI Series: The data is good enough, the technology is getting better, the computing is becoming more available, and the use cases are getting clearer—but is AI truly a revolutionary technological advancement yet for health care? With a 30-year perspective on what digital technology has done and failed to do in health care, Dr. John Halamka, President of the Mayo Clinic Platform, joins Chip in discussing whether AI is actually disruptive or another wave of incremental change.
Charles N. Kahn III is a senior visiting fellow at KFF. He is also a visiting senior fellow at the American Enterprise Institute and a nonresident senior scholar at the University of Southern California’s Schaeffer Center for Health Policy & Economics. He serves as co-chair of the international Future of Health collaborative.
Dwight and Dian Diercks President, Mayo Clinic Platform
Dr. Halamka is an emergency medicine physician, medical informatics expert and president of Mayo Clinic Platform, a digital initiative that brings together solution developers, data partners and healthcare service providers to transform healthcare. Dr. Halamka has been developing and implementing healthcare information strategy and policy for more than 40 years. Previously, he was executive director of the Health Technology Exploration Center for Beth Israel Lahey Health, chief information officer at Beth Israel Deaconess Medical Center, and International Healthcare Innovation Professor at Harvard Medical School. He is a member of the National Academy of Medicine.
AI Usage Disclosure: This transcript was created with assistance from AI tools. It was reviewed and edited by KFF Staff.
Chip Kahn: Last week Eric Larson gave us the strategic landscape, the case that AI is a general-purpose technology on the order of the steam engine and the Internet, and that American health care is uniquely exposed to its disruption and largely unprepared for it. This week we go from the roadmap to the road. Our guest is John Halamka. There may be no one in American medicine who has had a longer or closer view of what digital technology has done and failed to do in health care over the last 30 years. He ran IT at Beth Israel Medical center for more than two decades, advised the Bush and Obama administrations on national health IT, and lived through high tech, meaningful use and, and the rise of telehealth. He has watched every wave of digital innovation promise to transform American medicine and deliver something less. Today, he is president of Mayo Clinic Platform. So, when John says, as he did recently, that the data’s good enough, the technology’s getting good enough, the compute is getting available enough, and the use cases are getting clearer, that this time really may be different, it carries the weight of three decades of having heard this time is different before. The mission critical question for this conversation is whether AI is genuinely a disruptive revolution that has to be navigated or another wave of incremental change. And if it is a revolution, what makes it categorically different, and what does it take to navigate it? There is no better person to take us from the big picture to the operational reality. John Halamka, welcome to KFF’s Business of Health.
John Halamka: It is extraordinary to be with you because we’ve worked together for 25 years. This is going to be fun.
Chip Kahn: Great. John, one thing striking me, and at least for our YouTube viewers, you’ve got two grandfather clocks in the back of the room that I can see, and that’s an actual room, it’s not a virtual site. What’s that all about?
John Halamka: So, Eric Schmidt, who is on the board of Mayo, would tell you the following, that there are certain technological principles you should follow because the technology is going to change very fast, but the principles will not. And so, the two clocks behind me illustrate a bit of guidance as we start to talk about AI. So, in 1905 a guy in Armonk, New York had this idea. Could he take modular componentry knowing that technology would change? But you know, for the moment, take the technology you had, put it together in a novel way and create something of value. And so, the clock that you see over there was assembled to wind itself in 1905 using a singer sewing machine motor and Mercury switches. But of course, you could change it out as technology changed. The notion of modular replaceable technology was rolled into a company that the inventor called the International Time Recording Company. But then he said, “I wonder if I could work on other business machines.” So, he renamed the company IBM. So, the clock on the left is the pitch deck for the startup company of Thomas J. Watson, IBM. The clock on the right is exactly the opposite. And every component is hand-tooled, not replaceable, not maintainable, and locked in the technology of the mid-1700s. That’s Paul Revere’s clock. And the only way to maintain it is to be a silversmith in Boston. So, there you go. I think Thomas J. Watson had the right idea.
Chip Kahn: What a way to start. Let’s look at you for a moment. I mean you’ve spent decades on it. Whether it was your years at Beth Israel, whether it’s all the advice and guidance you’ve given to people here in Washington over that time, you’ve been there for it all. The advent of the EHR, the advent of high tech, meaningful use, the beginning of telehealth. Let’s look at it and just keep AI out of it for a moment. Why did all of that have an effect but then had so many unintended consequences and on the one hand got us somewhat advancing and we can call it a transformation, but we surely can’t call it a revolution in terms of health care.
John Halamka: Chip, you were there. I mean again, this is the great thing, isn’t it, a line from Hamilton, that we were there when these events happened in the room.
Chip Kahn: Yes.
John Halamka: And so, what happened in the room? Take us back to 2009. And as you remember, I was the chair of the Healthcare Information Technology Standards Panel. We had policy and we had standards and I was charged by Obama of figuring out all of these questions of how technology would revolutionize medicine. So, I said, well Mr. Obama, what should I do? He said well go talk to the FDA, see what they want. The FDA said oh, post market surveillance device and implantables. We need universal device identifiers. So just simply have every doctor at every visit type in every device in the patient’s body and be able to track it for quality and safety and recalls. Wow, who could argue with that? And then I said well, what should I do next? He said go talk to CMS. And CMS, we care about quality. In fact, 40 different quality measures. So what we just simply want is every doctor at every visit to record 40 numerators and denominators. So we can measure quality. Are we going to argue against quality? And then I talked to the CDC and they said, we want to look at epidemiology, and we want to look at emerging diseases or trends in violence. So all we have to do is ensure that every doctor at every visit and every nurse a complete understanding of every infectious agent that could be entering the community. By the time we were done, every doctor and every nurse had to enter 140 data elements while seeing the patient, being empathetic, never committing malpractice, in 11 minutes. It’s impossible. So, as you suggest, all of the best people with all of the best intent created a set of burden for our clinicians that unfortunately has these unintended consequences of burnout and less working at the top of your lists.
Chip Kahn: John, I think last year you said, and I’ll quote you here, the data is good enough, the technology is getting good enough, the compute is getting available enough, and the use cases are getting clearer. Is it really different this time?
John Halamka: It really is. And so, I am just turning 64. And so, I know this sounds a bit odd, but I have been working on these issues for 50 years. And 50 years ago, what did I do? Oh, well, we didn’t have compute, so I actually did something called wire-wrapped something called an Altair 8080. I actually built a computer 50 years ago. I was the very first student at Stanford University to have a computer because I built it. Well, today you could go get teraflops for pennies in an instant. Mayo wanted to do an algorithm that required 20,000 GPUs running for two weeks. No problem. You could order it like you order a Happy Meal, right? I mean, it was very easy in 2025 and 2026 to get the compute, the storage that you need that wasn’t there 50 years ago. And I actually don’t have to write a lot of code to do these things. Many of the tools are low code or no code kinds of tools. And data. Think about it. I mean, we’ve both been on this journey for decades to reduce the friction for interoperability and data standards and aggregation of information to turn it into wisdom. And today at Mayo Clinic, as we’ll talk about, I work with eight countries on sovereign AI looking at hundreds of millions of birth-to-death multimodal records so that we can create the models for the patients of the future. So yes, 2026 is the perfect storm for innovation.
Chip Kahn: So, it’s categorically different.
John Halamka: It is categorically different. How about this, sometimes I’m asked, what is the best era that you would want to relive? Oh, did you like the 60s, the 70s, the 80s? I’ll tell you the answer to the question is today. Today is the best era to be alive.
Chip Kahn: So, let’s go to Mayo and walk us through the AI applications that are generally operational right now that you have strong feelings about and that are not piloting, that are actually affecting patients at the bedside.
John Halamka: Well, sure. So, Bob Wachter, who I’m sure you know very well and you’ll be chatting with, visited Mayo for a week. And I actually took him to the bedside and saidI’m going to show you how a patient, how a doctor uses this stuff day to day, and how it materially changes the way we are delivering a service.
John Halamka: So, for example, in cardiology. And again, I’m just going to give you some real examples. And you know, I have no privacy of any kind. And it’s all okay. So I have a supraventricular tachycardia. And that means my heart rate, which is about 50 or so at rest, sometimes goes to 170. It’s irritating. It is not life threatening. Mayo Clinic said, wow, John, maybe you have a cardiomyopathy, maybe you have pulmonary hypertension, maybe you have valvular disease. I mean, we’re not sure. So you have two choices. You know, you could come to Mayo. We could spend four days doing expensive invasive procedures, or we could just run 14 algorithms on the Lead 1 ECG you gather over a consumer device in your living room. Your choice. What did I do? Again, I’m not, of course, endorsing any product or service here, but I literally bought like a $50 device on Amazon that was able to gather either, a one-lead or a six-lead ECG. And then I sent it to Mayo that ran all the algorithms, and they came back and said, John, your heart is that of a 17-year-old. It is amazing. But you have a conduction defect. Take 25 cents of Diltiazem every day and your SVT will disappear forever. I did all that literally from my living room. And I am cured. And I didn’t have a single invasive procedure. And this is what Mayo does. Take every specialty. Radiology, radiation oncology, early detection of breast cancer, prostate cancer, all of these things in production today, augmenting the workflow of our clinicians, so that those clinicians can see more patients with greater quality and safety than ever before.
Chip Kahn: Boy, that’s really significant. You know, obviously Ambient AI in doing charting is one of the big areas of progress. And I know that you do a lot, both in Arizona and Florida, with the nurses. Actually, almost all their charting is done by voice. How does that all work? And how are the nurses working with that? And then, what are the efficiencies that come from that?
John Halamka: You may remember in Bob Wachter’s first book, the Digital Doctor, the first page is a crayon drawing done by a 7 year old called “A Visit to the Doctor,” where the doctor and the nurse are staring at a computer at one side of the room and the patient and the family are on the other side of the room. And that’s unfortunately, as we have moved from an analog to digital world, that’s unfortunately, we’ve lost the hearts and the minds of our doctors and nurses by turning them into administrative typists. And so, what ambient listening can do is several things. Well, first I mentioned those 140 data elements that need to be gathered. Those 140 data elements can actually be automagically—I know that’s not a word, right—
Chip Kahn: but it sounds good, though.
John Halamka: Yeah, yeah. from the doctor and the patient having a dialogue. So, you know, have you been sleeping okay? How’s your weight, how’s your mood? How’s your family? Right? You start to populate all of that and then the clinician just goes back and edits or signs off on the result. It is a substantial reduction burden with nurses especially, right? You’ve got nursing care plans and you’ve got progress notes, and the nurse and the patient have a dialogue. And that, in effect, inpatient record is created automatically so that the goal that our Chief Nursing Officer has is that a nurse will not touch a keyboard during a shift. And what a noble goal that is. I’m going to give you an analogy to ambient listening that you’re going to find kind of funny. Take you back to 2011. There was a product called Google Glass. And you remember, you put on the glasses, they had a camera, they had capacity to run software. Beth Israel at the time was the pilot site for that product. And what did we do? Well, we displayed the patient’s chart and their vital signs and their problem list on the glasses. So, we said, hey, patient, how did you like that experience? They said, the doctor was looking at me instead of a computer the whole time. Well, of course, the reality is the doctor was just reading the computer on the glasses in front of them. But the patient experience was better. And that’s the goal of ambient listening, compliance and accuracy with a patient focus.
Chip Kahn: I guess it also affects literally the nurse’s time because she or he is not stuck at a desk anymore…
John Halamka: I mean, you’ve talked to our clinicians. Approximately 50% of nursing days are spent at a keyboard. And so now, as you say, reduce that from 50% to 5%. It means that the reason they went into nursing was active listening, empathy, contact with patients, service. They can now work at the top of their lessons.
Chip Kahn: So, the issue of whether to go with an app or a technology that’s AI driven, you’ve said that they ought to be evaluated similarly to a pharmaceutical. What do you do at Mayo? What’s the process that you have and how much rigor do you want in evidence before you’ll pilot or experiment even with a new technology?
John Halamka: Sure. So you, of course know Micky Tripathi, and Micky served as ASTP ONC lead. When he retired from the Biden administration, he actually came to Mayo and is now the Chief AI Implementation Officer. You say, “Wow, that’s a weird title.” Well, so Micky obviously had spent a career in safety and quality and data, and is charged with making sure that we deploy AI, we do it rapidly. Right. We don’t want to constrain innovation, but we also understand its implications, you know, it’s safety and consequence. So here’s what we do for every algorithm, and I’m going to start with predictive AI because predictive, generative, and agentic AI, they all have slightly different characters. Predictive AI. What data set did you use to develop it? So suppose. And of course, Chip I’m making this up.
Chip Kahn: Sure.
John Halamka: I create an algorithm from the 10 million patients that Mayo has in Minnesota, lots of Scandinavian Lutherans, and then I run that algorithm in rural Georgia. Fewer Scandinavian Lutherans. Will it be good? Will it be bad? Do you know? So a data card tells you who phenotype, genotype, exposome was put into the training set for the algorithm. So every algorithm at Mayo has a data card. Then a model card tells you actually how does it run in practice? So here’s a fun one. I don’t know if you spent time with Eric Horvitz, chief scientist at Microsoft, but back in the day, Microsoft bought Amalga, I think it was, Craig Feied, Mark Smith and MedStar created this thing, I don’t know, 20 years ago, MedStar, Washington D.C., typically insured patients. The folks at Microsoft took the algorithms developed at MedStar and moved the algorithm six blocks away to a largely Medicaid population clinic. It didn’t work at all. Right, because your insured population in Georgetown has maybe a different diet or, or a different set of medication adherence than does a Medicaid clinic. So a model card tells you a bit about how the model actually works on each patient, given stratifications of race, ethnicity, zip code, age, gender, et cetera. So Mayo does that. But then here’s the biggest issue. I am going to develop an algorithm that is going to tell Chip whether you should eat more vegetables for dinner and whether you should walk 10,000 steps a day. Suppose that algorithm is wrong. Maybe you eat too many vegetables, and you walk too much. The likelihood of harm to you probably zero. Right? So, you have to do what we call qualification. If the algorithm is wrong, what is the consequence? Suppose I have an algorithm that is actually going to automatically go, back to device integration here, automatically inject insulin into your bloodstream. Aha. that algorithm’s wrong. You could be in hypoglycemic coma. So what you see is for every algorithm, not only data card and model card, but, but a stratification of six different ranks of risk if the algorithm goes bad. And once we do that, then in a—don’t worry, this is a relatively quick process, I mean, a week or two turnaround time—we then get the approval to put it in production.
Chip Kahn: This is causing big changes. And what this podcast is all about is how do we get to, good patient outcomes with the notion that at the end of the day, the business model is what’s going to be right to get there? And so how are the economics of running a health system affected by all the kinds of apps and adaptation of these new technologies that you’re bringing into place in your health system and recommending for other health systems?
John Halamka: Well, and of course you ask the best question, but also a complicated question. And, sometimes I say with a bit of levity, the United States is actually five countries. You know, the East coast, the West coast, the Midwest, the South, and Texas, which is its own country. I say this because the reimbursement models and the incentives in each region of the United States are different. I mean, again, just knowing your career, would you say that in the Midwest in general, of course, heads in beds is a good idea, but let’s take the East coast to the West coast. Heads in beds. Oh my God, no. You don’t want that. You want wellness, you want home care, you want value-based purchasing, et cetera. So here’s the question for you, right? Depending on your reimbursement model, what is it that you’re going to do with AI that is going to ensure the best patient care? That’s of course what you want to do first. But also reimbursement, is going to cover some kinds of costs. Here’s why it’s hard. I think we probably all listened to Dr. Oz say, let’s move from sickness to wellness. Let’s move from hospital tertiary, quaternary referral to community and home, and let’s move from analog to digital. But ask yourself this question. What’s the reimbursement today for chemotherapy delivered in a hospital facility versus the home? Right. So, the incentives are slightly misaligned to do that end delivery in a non-traditional setting. So anyway, I say all this because your question is so complicated. I, mean, right, with AI, I can deliver right care, right patients, right time, right setting. But you know, hospital systems have to keep the lights on and so they will also have to reflect, “is there reimbursement for what activity that they use AI to automate?” Don Berwick, our mutual friend, said, if you automate a bad process, you just achieve a bad result faster. So, imagine you and I design a system that is great and unreimbursed. We’ll go bankrupt quicker. So again, this is not about letting revenue drive what it is we do. We have to be realistic when we deploy these things. We’re not building a CPT code for every use of AI. We’re trying to achieve efficiencies that are aligned with the reimbursement we get from delivering the service.
Chip Kahn: One of the issues, to me, I should say with pay-for-performance as an area, is that if it’s been successful at all in all the areas around the country you talked about up to this point, it’s given the payers an edge so that maybe they can get a cheaper price, maybe it’s used effectively, sometimes maybe inappropriately in terms of controlling volume, but it doesn’t really have any kind of outcomes measurement. It has all these measurement requirements that really don’t tell you much other than the hospital or the physician followed the right process or the right structure was in place. Can AI be a game changer here to begin to reform the structure you just described, which is sort of hostile to evolution that is appropriate because it’s so complicated?
John Halamka: Well, sure. So let me ask you an interesting question again. You’ve done this for decades how easy is it for you to order and get an echocardiogram on a patient? Well, here’s a problem. We don’t have a lot of echo techs and the supply and the demand has a mismatch. So, you’re going to wait six weeks to get an echo? I mean, unless you’re in some sort of life-threatening situation. Well, and again, I’m not endorsing any product or service here. I’m just telling you my experience. There are companies that are now creating AI driven devices so that a person who’s never done an echo in their lives with a minimal amount of training, as in a couple of hours, can produce an echo with the same quality as an echocardiographer with 30 years of experience. Wow. That means I’m actually be able to see more patients and deliver more services with more quality in more regions than ever before. Okay. Again, it’s going to always be in the interest of the patient and doing the right thing and it’s appropriate. But I will now be able to increase volume. But there’s another aspect of all this which is that a primary caregiver who’s utterly overwhelmed may say, ah, I am not really sure if I should refer this patient to a cardiologist or not. And how about this? I have doubt. So let me just refer them to cardiologists, which as you know, especially referrals and result in increased expense, obviously increased testing. What if the AI says actually the person in front of you right now has an ejection fraction of 70% based on their Apple Watch? (Not endorsing Apple). Oh, you don’t actually need to refer this person to a cardiologist. Well, and of course what I’m referring to is the Mayo Eagle and Beagle study, right, which actually took 125,000 EKGs from consumer devices and actually had primary care givers be able to now decide who to refer and not to refer based on AI interpretation of patient device data. And it had two interesting implications. First, those who needed cardiology referral got it 30% faster. And a whole lot of patients were actually not in need of a cardiology referral and fully managed by the PCP, resulting in the substantial increase in job satisfaction for the PCP. So again, you can hear this. We have in the United States a limited number of specialists. And if I can ensure that the right care is delivered by the right person in the right setting and AI helps us figure that out, everybody wins.
Chip Kahn: There has been a lot of discussion about AI hallucinations and other issues that are raised by the complexity and the mystery in some ways of the technology. How do you deal with that? One of my interviews the other day mentioned something, I think he used the word wobble or some word like that that said, that over time, even though their technology’s approved, it’s validated, it works over time, there’s an evolving of the way it works, so they’ve got to constantly recalibrate it. How do you make sure all of that is appropriately in place so that the AI results you’re talking about will be as assured a month from now as today?
John Halamka: Right. So what you’re talking about is data drift or data shift. And I’ll give you a real example. Think back. January 2020. Mayo was asking, how do we start delivering care in the home? How do we do telemedicine? In January of 2020, we are going to create an algorithm based on every person who is seeking remote care in January of 2020. And it will help us figure out who will benefit from remote care. And then we deployed it in March of 2020. So again, think back. How many of your patients were seeing their doctors through telemedicine in 2019 or January of 2020 versus say March or April of 2020, we literally went from 3% of the population to 93% of the population. And so, the algorithm developed back when it was 3% is completely useless when you get to the 93% because of this thing we call COVID. Right. And so, it requires, and this is what I would argue like a pharmaceutical post market surveillance on every use of the technology to say, did it work? Did it not work? Was there benefit? Was there harm? And then constant fine tuning. And so, here’s again a sort of interesting challenge. And again, I’m just going to be realistic because I get to live this every day. I went to medical school in the 1980s, and so I recently had the opportunity to speak with one of my colleagues who is the director of National Library of Medicine, Lister Hill. And I said, I’m curious, if you look back at the literature that I mastered in the 1980s, how much of it is wrong? And she did do an analysis. 60% of what I learned in medical school is wrong. I just don’t know which 60%. Right. So isn’t it interesting? Although AI, as you say, has hallucination, the AUCs aren’t perfect, but it’s probably a whole lot better than somebody who trained in medical school in the 1980s. So where does society draw the line? If my AUC is 0.6 and the algorithm AUC is 0.8, I’m betting you probably want the algorithm over me, even though it’s imperfect.
Chip Kahn: So, what you’re describing in some ways is the Waymo problem. When they hit a cat, it’s a big scandal. But if you compare them to all of us driving, they have a lot fewer accidents, if they have any at all. And we are a big risk. But the public doesn’t look at it that way. So, this is something that is an issue for technology generally.
John Halamka: So let me just give you another dark side to this. So, a few months ago, I was in Dublin and I met with all of the world’s radiology chairs. And they told me they hate AI. I said, well, why is that? And they say, well, let’s imagine that it has a positive predictive value of 95%. I mean, wow, that’s wildly better than any human. But here’s the problem. If I’m going to argue against the AI, right, there’s 5% false positives. The amount of time it takes me to document that I disagree with the AI, and I’m going to actually go a different direction from a medical legal perspective outweighs the benefit of the 95% of good advice that it offered me. And as you suggest, this is a cultural issue, that we are not allowing AI to have any margin of error, despite the fact that our human doctors and nurses have an amazing level of error.
Chip Kahn: If we look at, FDA, I think they’ve authorized roughly 950 AI enabled medical devices. How many of them actually clear your bar, for deployment at Mayo? And what does the ratio tell us about the gap between authorization and real clinical research readiness?
John Halamka: So isn’t it interesting, as you look at adoption of AI across health care systems, the radiologists and the cardiologists tend to adopt it first. And so as you look at the FDA approvals, the vast majority of these are in the field of radiology, cardiology devices, and that kind of thing. So then you start to ask the question, where is there a human nearby? Right? And that is, is it an autonomous decision where the AI looks at something and takes an action? Or is it that it’s that smart consultant that’s telling the human, hey, you know, I saw this fracture here. You may want to recheck that. So I would tell you where Mayo has been an early adopter of this stuff is, especially in the field of imaging, right? So radiology or digital pathology, radiation oncology, where it’s augmenting human behavior by helping them focus their attention. And at the moment I don’t think there’s a single case, I mean maybe we could find one in supply chain that orders Band Aids or something, but a single case where the AI itself is running autonomously without a human nearby.
Chip Kahn: I think that’s important. And if AI is generally disruptive, the question is whether health care’s decision making structures are designed for incremental change. And here I’m speaking generally not of Mayo specifically, can they actually navigate well, this revolution, I mean you’ve got a very contained shop, you know, you’ve got your implementer staff. Everyone’s not going to have the facility or the knowledge that you’re bringing. How is the average health care system, the individual or small group physician going to deal with the kinds of issues we’re talking about in terms of navigating this?
John Halamka: It’s a brilliant question, right? And there’s several ways you could look at it. I mean when you talk to Marty Makary, FDA has said it’s going to take a bit of a light touch for regulation. So you’re probably not going to see this rigorous premarket testing and such. So what that means it’s probably going to be up to the marketplace, the innovators and provider organizations, to figure out what to use and how to use it. So here’s what Mayo’s done. Although we have three destination medical centers, Minnesota, Florida, Arizona, we actually have around the world, about 50 affiliates that are typically community hospitals, some critical access hospitals. And they’ve said, hey Mayo, help us figure out what AI to deploy. So what Mayo will do is look at all these products and services built by Mayo, built by third parties, qualify them, and once we think they’re good enough, then we will go out to the community hospitals and say, oh, we’ve actually found this particular solution to be reasonable in terms of its positive, predictive value, its risk, its post market surveillance and that kind of thing. So maybe I would argue those who have the sophistication to develop and test these things have a societal responsibility to spread them to those who don’t. And certainly that’s the work that I do at Mayo Clinic Platform is I’ve been given an interesting KPI and that is Gianrico Farrugia said, John, I want you by 2030 to have touched the lives of 4 billion people by ensuring these algorithms that are qualified are disseminated globally to every Android phone, every HER, and every country on the planet.
Chip Kahn: Well, I guess along those lines, you’re also a chair of the Coalition for Health AI. What should AI governance look like inside a health system? And does that exist today? I mean, do the institutions even have the kind of structure to get the information from you and those who can provide guidance to make the kind of decisions they need to make?
John Halamka: And so, one of the challenges, and about four years ago we put this coalition together because there was not a community standard. As you and I know, malpractice isn’t a good or bad outcome. It’s, did you deviate from the community standard of care? So our thought was if we could put 4,000 organizations together across government, academia and industry and define what’s good enough, what are the best practices, what are the right safeguards, what is a standard data card or model card or qualification schema, then others would say, oh, I don’t have to define a data card myself. I can adopt the community standard of care for the evaluation of a given AI algorithm. And that’s really the purpose of the Coalition for Health AI. It’s a nonprofit organization bringing people together just to decide what will we, as a society ,accept and not. I mean, it was very funny. Eric Schmidt, who I mentioned, you know, he’s a board member of Mayo. When he created Waymo, he said, we actually did a cultural analysis and we found that the public wanted self-driving cars to be 10,000 times better than a human driver. Wow. Okay. The community standard of care is that a Waymo will have one accident in a million miles. Fascinating. I mean, somebody had to decide what’s good enough. So as you pointed out, if suddenly, I mean, there’s one tiny accident, it’s news, front page news. Despite the fact that we all agreed it’s wildly safer than any other transportation alternative. That’s why we need the standard for how you test, how you govern, and what is good enough.
Chip Kahn: One of the things that all of us face and see whenever we have any kind of interaction with the health care system is the health care workforce shortage. Sort of hits us in the face. You’ve said that AI is essential to closing that gap from a policy standpoint and then from a practical, real-world standpoint, how is AI going to do that and how fast can it do it?
John Halamka: So, let me give you a couple of statistics. I don’t know if you have, spent time in Davos at the World Economic Forum, but in 2025, the theme was AI and all the government leaders in Davos said, we have a problem. The birth rates in many industrialized countries are, are less than replacement. And in some places like Japan and South Korea, I mean looking at birth rates of 0.6, 0.7, but yet we have societies that are living into their 80s. So, lifespan may be in the 80s, but health span is probably in the 60s. So, what that means is we have a 20 year period where we’re going to need more care. Oh, but wait, our birth rates are so low there’s no one to deliver that care. And so, what I have heard from societal leader after societal leader and I just flew in from three days in Rochester where I hosted 28 international companies, including many government officials from Japan. What they said is we have decided that unless we deploy AI as part of extending the license of our mid-levels, helping our specialists see the right patient, delivering care in the home, an autonomous fashion, robotics, all these other things, we’re never going to meet the demand of an aging society with a birth rate that’s 0.6 or 0.7. So this becomes kind of a John Carter problem, right? That is there’s an urgency to change and it’s up to us to figure out how. And so I think the vision is this, that we assess as we’ve been talking about levels of risk and if we can build AI that will help a mid-level, a nurse practitioner, a PA deliver a higher quality of care to more patients with more serious disease, suddenly we are going to have a healthier society. And I’m seeing this sovereign AI notion that is country scale adoption of this stuff to meet the societal problems of supply, demand, mismatch. And I don’t see a lot of other arrows in our quiver because we’re not going to graduate enough nurses and doctors over the next 20 years to solve this problem for us without AI.
Chip Kahn: Well, I think your echo example is a good one in that respect. And I’m sure there are other areas with techs and other aspects of the workforce where literally, you know, having AI can change the whole aspect of that kind of care. And I assume that’s coming. And that gets to my sort of the overall question from a regulatory and policy framework, what do you think we need to assure the public that is risk averse, and I’ll use the word in a sense, and I think it comes from our discussion, not risk illiterate, but has a notion of risk that frankly reflects a nervousness that doesn’t reflect the reality of everyday life. I mean when you cross the street, you’re at risk. And people don’t compare that to other aspects of risk. What kind of structure do we need for AI deployment so that it can achieve, on the positive side, all the kinds of outcomes you’re describing?
John Halamka: Of course, you’ve asked the $64,000 question, so let me frame it in an unusual way. I was speaking with a prominent industry leader the other day about a paradox, and here’s the paradox is, say there are AI products, I’m sure you use several of them that go out and summarize the literature or summarize clinical data for you, and let’s say they’re 80% good. There are products that use different technologies and get actually higher levels of accuracy. And this leader told me the paradox is people trust the output of an LLM because it’s so compelling. Right? It makes you happy. And even if it’s telling you information that’s completely false, you feel good about it. So I asked the question, how many people do you know that are uploading their medical record or their wearable device information to ChatGPT or to Claude and then are asking questions of it and actually feel really good about the advice they are getting back, not only because it’s compelling and it’s well phrased, but because they’re instantaneously getting information that could take a couple of days for their PCP to synthesize and respond to. So, wow, there’s a cultural question that you ask. If people say, I am actually more interested in, immediacy and comfort than I am in complete accuracy and delay, we have to decide as a society if that’s okay or not. We’re replacing Dr. Google with Dr. Claude. And so, I guess here would be my dream. We’re not there yet. What if for every generative AI product, we could figure out an accuracy score? And remember, every time you give a prompt to a generative AI product, you get a different answer. So you actually need a score on every single answer that you get. Again, I’m going to hypothesize here. Let’s say that, the National Library of Medicine, working with industry innovators, creates a knowledge graph, and every generative AI response is checked, error checked against a knowledge graph of the world’s literature or clinical observations, then gets a score. You can say, wow, Claude just synthesized your medical record and gave you advice, and the confidence level is 0.9 as opposed to 0.1. Then you’ll decide as a human. Yes, it’s comforting and compelling. But you want to believe it. So here’s where I’m getting a little bit speculative. I have no question that people are going to use these products to guide their care journeys because they feel like it’s democratized access to knowledge and it’s reduced burden of navigation. But data cards, model cards, qualification, that all helps. But the individual patient, I’m betting is not going to go look at a data card or model card. They’re going to need something that says, oh, you, you know, this is believable or not believable. And we haven’t as a society built that yet, but we must to sort of close out.
Chip Kahn: Clearly, five years from now, ten years from now, the world is going to be different because of this technology. What keeps you up at night when you think about the prospects of that? Obviously, we’ve talked about the positive, but just in terms of how it could affect health care, is there an aspect that keeps you up at night when you think about how this is all going to work out?
John Halamka: Well, a couple of things keep me up at night. I’m sure you talk to many medical school deans. Generally for the last 30 years or so I’ve been able to lecture to conferences of the medical school deans of not only the U.S. but internationally. They are not preparing the next generation of students to be AI interpreters. Unfortunately, our medical schools tend to be fairly conservative and haven’t changed the curriculum to move away from memorization to data science or to tool assessment. And we need to. So, you know, I do not want the next generation of doctors to blindly accept the advice of an AI without having the training to decide if that AI is credible or not. That’s certainly one issue I do worry in agentic AI. We didn’t talk a lot about it, but I have recently had discussions with some of the chief information security officers of the largest hyperscalers in the world. They are really concerned that as we use agentic AI, in effect say AI can now take action on your own, that if a bad actor takes over that agentic AI, they could literally shut down your company in a few seconds. So we’re going to be really careful about cybersecurity and the potential for some of these tools that we create to actually have an effect that was never intended and, and one that could be extraordinarily harmful to our care delivery system. Again, I told you, I will never mention a product or service, but there is an open-source stack called OpenClaw which you may have looked at.
Chip Kahn: Yes, I’M familiar with it.
John Halamka: It’s a lovely open-source software system with no security of any kind. So if you say hey OpenClaw, you can now go answer all of Chip’s emails or order all of Chip’s groceries and operate the entire home ecosystem of locks and lights and heating. Just think about what happens when a bad actor has taken control of everything in your life. We just need to ensure that doesn’t happen.
Chip Kahn: John, this has been terrific and I just appreciate you spending the time with us and I think our audience will clearly have learned a lot today from our conversation.
John Halamka: Well, and I live this every day and as I said I’m approaching 64 but I’ve been a vegan for 25 years, so I got like 30 more years of working through this. So, you and I, 30 years from now we’ll say and here’s what we said in 2026 and here’s what came to pass.
Chip Kahn: John, I want to be with you 30 years from now. Thanks.
This weekly podcast features insightful conversations between host Chip Kahn and his guests, who discuss the business of health care, connecting the dots between the health care business, policy, and patients.
The podcast’s first series on AI in health care illuminates how AI is changing health care, and features guests who are deploying this technology, managing its consequences, and designing policy around it.
Health coverage plays a major role in enabling people to access health care and protecting families from high medical costs. There have been longstanding racial and ethnic disparities in health coverage that contribute to disparities in health. Due to Medicaid and Affordable Care Act (ACA) cuts in the 2025 reconciliation law and the expiration of the ACA’s enhanced premium tax credits, the number of uninsured is expected to increase by more than 14 million by 2034, potentially exacerbating racial disparities in coverage. This brief examines trends in health coverage by race and ethnicity from 2010 through 2024 and discusses the implications for health disparities. It is based on KFF analysis of American Community Survey (ACS) data for people under age 65. All noted differences between groups and years described in the text are statistically significant at the p<0.05 level. Key takeaways include:
Since 2010, there have been large gains in health coverage across racial and ethnic groups but racial and ethnic disparities in coverage persisted. The largest gains occurred after implementation of the ACA coverage expansions in 2014, with increases continuing until 2016. Hispanic people under age 65 had the largest percentage point increase in coverage, with their uninsured rate falling from 32.6% in 2014 to 19.1% as of 2016. Black, Asian, and American Indian or Alaska Native (AIAN) people also had larger percentage point increases in coverage compared to White people over that period. Despite these larger gains, Hispanic, Black, AIAN, and Native Hawaiian or Pacific Islander (NHPI) people under age 65 remained more likely than their White counterparts to be uninsured as of 2016. Beginning in 2017, coverage gains began reversing, and the overall number of uninsured increased for three consecutive years, coinciding with the first Trump administration. Pandemic-era policies drove broad coverage gains and reduced uninsured rates across most racial and ethnic groups between 2019 and 2023.
In 2024, the overall uninsured rate increased for the first time since 2019 as pandemic-era continuous enrollment in Medicaid came to an end, with significant increases among Hispanic, Black, and White people under age 65. Asian, AIAN and NHPI people did not have statistically significant changes in coverage over this period. As of 2024,AIAN and Hispanic people under age 65 had the highest uninsured rates at 18.9% and 18.4%, respectively. Uninsured rates for NHPI (12.3%) and Black people (10.1%) under age 65 also were higher than the rate for their White counterparts (6.8%). Asian people had the lowest uninsured rate at 5.7%.
Coverage disparities have persisted over time and, in some cases, widened despite earlier gains under the ACA. For example, between 2010 and 2024, the uninsured rate for AIAN people grew from 2.4 to 2.8 times higher than the uninsured rate for White people, the Hispanic uninsured rate grew from 2.5 to 2.7 times higher than the rate for White people, and Black people remained 1.5 times more likely to be uninsured than White people.
Recent policy changes are projected to lead to increased coverage losses in coming years, which will likely widen racial and ethnic coverage disparities. The 2025 reconciliation law makes significant changes to Medicaid and the ACA Marketplaces, which are projected to lead to large coverage losses. It also further restricts access to health coverage for lawfully present immigrants across public health insurance programs. Additionally, the expiration of enhanced premium tax credits for ACA Marketplace enrollees has led to substantial out-of-pocket premium increases and further growth in the uninsured population. The Congressional Budget Office estimates that the combined impact of the reconciliation law with the expiration of the ACA’s enhanced premium tax credits will increase the number of uninsured by more than 14 million in 2034. Medicaid and ACA Marketplace coverage losses will likely widen racial disparities in coverage given that disproportionately large shares of Hispanic, Black, AIAN, and NHPI people are covered through these sources. Coverage losses, in turn, would likely contribute to widening disparities in health.
Trends in Uninsured Rates by Race and Ethnicity, 2010-2024
Prior to the enactment of the ACA in 2010, Hispanic, Black, Asian, AIAN, and NHPI people under age 65 were more likely to be uninsured compared to their White counterparts, with Hispanic and AIAN people at the highest risk of lacking coverage (Figure 1). Their higher uninsured rates reflected more limited access to affordable health coverage options. Although the majority of individuals have at least one full-time worker in the family across racial and ethnic groups, there are ongoing racial disparities in employment and income that result in some groups having more limited access to coverage offered by an employer or having greater difficulty affording private coverage when it is available. While Medicaid helps fill some of these gaps in private coverage, prior to the ACA, Medicaid eligibility for parents in most states was limited to those with very low incomes (often below 50% of the poverty level), and adults without dependent children—regardless of how poor—were ineligible under federal rules.
Between 2010 and 2016, there were large gains in coverage across racial and ethnic groups under the ACA, but racial and ethnic disparities in coverage persisted. The ACA created new coverage options for low- and moderate-income individuals. These included provisions to extend dependent coverage in the private market up to age 26 and prevent insurers from denying people coverage or charging them more due to health status. Further, beginning in 2014, the ACA expanded Medicaid coverage to nearly all adults with incomes at or below 138% of poverty in states that adopted the expansion and made tax credits available to people with incomes up to 400% of poverty to purchase coverage through a health insurance Marketplace. Following the ACA’s enactment in 2010 through 2016, coverage increased across all racial and ethnic groups, with the largest increases occurring after implementation of the Medicaid and Marketplace coverage expansions in 2014. Hispanic people under age 65 had the largest percentage point increase in coverage, with their uninsured rate falling from 24.8% to 19.1% between 2014 and 2016. Black, Asian, and AIAN people also had larger percentage point increases in coverage compared to White people over that period. Despite these larger gains, Hispanic, Black, AIAN, and NHPI people under age 65 remained more likely than their White counterparts to be uninsured as of 2016.
Beginning in 2017, coverage gains began reversing, and the number of uninsured increased for three consecutive years. The uninsured rate for the total population under age 65 increased from 10.0% in 2016 to 10.9% in 2019. Hispanic people had the largest statistically significant increase in their uninsured rate over this period (from 19.1% to 20.0%) although the absolute change was small. There were also small but statistically significant increases in the uninsured rates among White and Black people under age 65, which rose from 7.1% to 7.8% and 10.7% to 11.4%, respectively, between 2016 and 2019. Rates for AIAN, NHPI, and Asian people under age 65 did not have a significant change. These coverage losses likely reflected policy changes made by the first Trump administration after taking office in 2017. These changes included decreased funds for outreach and enrollment assistance, guidance encouraging states to seek waivers to add new eligibility requirements for Medicaid coverage as well as to increase the frequency of eligibility verifications, and changes to public charge immigration policy that made some immigrant families more reluctant to participate in Medicaid and the Children’s Health Insurance Program (CHIP) (which were later reversed by the Biden administration).
Pandemic-era policies drove broad coverage gains and reduced uninsured rates across most racial and ethnic groups between 2019 and 2023. After rising in the years before the pandemic, uninsured rates declined between 2019 and 2023, with 3.6 million more people under age 65 gaining coverage as the uninsured rate fell from 10.9% to 9.5%. Declines occurred across most racial and ethnic groups, with the largest drop among AIAN people (21.7% to 18.7%), alongside smaller but significant declines among Hispanic (20.0% to 17.9%), Black (11.4% to 9.7%), Asian (7.2% to 5.8%), and White people (7.8% to 6.5%), while changes for NHPI people were not statistically significant. These gains were driven largely by increased Medicaid coverage, which offset declines in employer-sponsored insurance, and reflected pandemic-era policies that stabilized and expanded coverage. These policies included the Families First Coronavirus Response Act’s continuous enrollment provision for Medicaid, which required states to pause disenrollments from Medicaid during the COVID pandemic in exchange for increased federal funding to states, enhanced ACA Marketplace subsidies under the American Rescue Plan Act and Inflation Reduction Act, increased outreach and enrollment efforts, and low Marketplace attrition.
After years of decline, the overall uninsured rate among people under age 65 increased in 2024, with significant increases among Hispanic, Black, and White people. The total number of people under age 65 without health coverage increased by more than 1.3 million to 26.7 million in 2024, and the uninsured rate for the population under age 65 increased from 9.5% to 9.8%.Hispanic people experienced the largest increase in uninsured rates between 2023 and 2024 (17.9% to 18.4%), followed by Black (9.7% to 10.1%) and White people (6.5% to 6.8%).Asian, AIAN andNHPI people did not have statistically significant changes in coverage over this period.
Coverage disparities have persisted, and in some cases widened, over time even with recent gains and the large earlier gains in coverage under the ACA. For example, in 2010, the uninsured rate for AIAN people was 2.4 times higher than the uninsured rate for White people; however, in 2024, the gap had increased to 2.9 times higher than the rate for White people. Similarly, the Hispanic uninsured rate grew from 2.5 to 2.8 times higher than the rate for White people from 2010 to 2024, while Black people remained 1.5 times more likely to be uninsured than White people.
Coverage by Race and Ethnicity as of 2024
Hispanic, Black, AIAN, and NHPI people under age 65 were more likely than their White counterparts to be uninsured as of 2024(Figure 2). AIAN and Hispanic people had the highest uninsured rates at 18.9% and 18.4%, respectively, as of 2024. Uninsured rates for NHPI (12.3%) and Black people (10.1%) also were higher than the rate for their White counterparts (6.8%). Asian people had the lowest uninsured rate at 5.7%, although uninsured rates vary among subgroups of the Asian population. The higher uninsured rates among some groups are driven by lower rates of private coverage. Medicaid coverage helps to narrow these differences but does not fully offset them.
Medicaid and CHIP coverage help fill gaps in private coverage and reduce coverage disparities for children, but some disparities in children’s coverage remain (Figure 2). Medicaid and CHIP cover larger shares of children than adults, reflecting more expansive eligibility levels for children. This coverage helps fill gaps in private coverage, with over half of Hispanic, Black, AIAN, and NHPI children covered by Medicaid and CHIP. However, there remain some disparities in children’s coverage. For example, AIAN children are about three times as likely as their White counterparts to lack coverage (13.6% vs. 4.4%). Moreover, Hispanic children are more than twice as likely as White children to be uninsured (9.8% vs. 4.4%).
Among people under age 65, uninsured rates in states that have not expanded Medicaid are higher than rates in expansion states across most racial and ethnic groups as of 2024 (Figure 3). While uninsured rates for children are lower than for adults across groups, these differences between expansion and non-expansion states persist among children. For example, 16.0% of Hispanic children in non-expansion states are uninsured compared to 6.7% of Hispanic children in expansion states. The differences in coverage rates between Black and Hispanic people compared with White people are larger in non-expansion states compared with expansion states. However, the relative risk of being uninsured for Black, Hispanic, Asian and NHPI people compared with White people is similar in expansion and non-expansion states. For example, Hispanic people under the age of 65 years old are roughly 2.6 times as likely as their White counterparts to lack coverage in both expansion and non-expansion states. Uninsured rates for AIAN people are similar in expansion and non-expansion states.
Eligibility for Coverage Among The Uninsured as of 2024
Overall, about half of uninsured people are eligible for Medicaid or Marketplace coverage, but eligibility varies across racial and ethnic groups, with smaller shares of Hispanic and Asian uninsured people eligible for assistance due to these groups having larger shares of ineligible noncitizen immigrants. Overall, over half (52.2%) of people who were uninsured in 2024 were eligible for financial assistance either through Medicaid or through subsidized Marketplace coverage, while the remaining half (47.8%) were not eligible because they fell in the Medicaid coverage gap in states that have not expanded Medicaid, had income too high to qualify for Marketplace premium tax credits, , were eligible for employer coverage, or had an ineligible immigration status. However, the share of the remaining uninsured eligible for assistance varied by race and ethnicity. For example, uninsured Black people under age 65 were more likely than their uninsured White counterparts to fall in the Medicaid coverage gap, reflecting that most of the 10 states that have not expanded Medicaid, are in the South where a higher share of the Black population resides. Uninsured Hispanic and Asian people under age 65 were also less likely than White people to be eligible for coverage options, in part, due to higher shares of noncitizens who face immigrant eligibility restrictions including eligibility restrictions for lawfully present immigrants and ineligibility for undocumented immigrants. (Figure 4).
Editorial Note: Originally published in June 2011, this resource is updated as needed to reflect the latest developments.
Section:
0/0
Key Facts
Gavi, the Vaccine Alliance (Gavi) is an independent public-private partnership and multilateral funding mechanism that aims to expand global access to and use of vaccines, particularly among vulnerable children.
Since its launch in 2000, Gavi has provided approximately $29 billion to support immunization efforts in low- and middle-income countries, not including funding for COVAX.
The U.S. government (U.S.) has supported Gavi since its creation through direct financial contributions, participation in Gavi’s governance as a member of the Board, and technical assistance; it had been its third largest contributor in recent years, providing 13% of its funding since its inception (not including funding for COVAX, the global COVID-19 pandemic vaccine response), reaching $300 million in FY 2024. In addition, the Biden administration had pledged that the U.S. would provide approximately $1.6 billion to Gavi over its 2026-2030 funding period.
While Congress again appropriated $300 million for Gavi in both FY 2025 and FY 2026, the Trump administration has not provided this funding to the organization, citing concerns about vaccine safety despite Gavi following globally recognized scientific standards and evidence.
Gavi’s latest replenishment summit secured pledges of more than $9 billion, towards a target of $11.9 billion, for the 2026-2030 period, as well as additional financing from development finance institutions and manufacturers to support country recipients. Still, the loss of U.S. funding in the context of a constrained financing environment globally presents new challenges for reaching children in low- and middle- income countries with life-saving vaccines.
Gavi Overview
Created in 1999 and formally launched in January 2000, Gavi, the Vaccine Alliance (Gavi) is an independent public-private partnership and multilateral funding mechanism that “aims to save lives and protect people’s health by increasing coverage and equitable and sustainable use of vaccines.” Gavi’s main activities include supporting low- and middle-income countries’ access to new and underused vaccines for vulnerable children through financial support, technical expertise, and market-shaping efforts, such as negotiating with manufacturers, to help lower the cost of procuring vaccines. Gavi operates in five-year funding cycles, with a revised strategy and goals for each cycle. Each five-year strategy is accompanied by a vaccine investment strategy, which determines which vaccines will be made available to countries.
strengthen health systems to increase equity in immunization,
improve sustainability of immunization programs, and
ensure healthy markets for vaccines and related products.
The current strategy emphasizes reducing the number of ‘zero-dose’ children with the goal of reaching no zero-dose children by 2030, in alignment with Immunization Agenda 2030; prioritizing programmatic and financial sustainability of country immunization programs; supporting targeted countries that have phased out of Gavi support or have never been eligible for Gavi support to maintain immunization progress; and providing more tailored approaches for Gavi countries to reach under-vaccinated populations, such as those living in remote or conflict settings, by encouraging countries to adopt strategies that reduce potential barriers to vaccination.
In addition to Gavi’s role in routine childhood immunizations, Gavi was one of the organizations leading COVAX, a multilateral effort that supported the equitable development, procurement, and delivery of COVID-19 vaccines globally that began in 2020 and ended in 2023. Gavi’s role in COVAX was to facilitate the procurement and delivery of COVID-19 vaccines, with particular emphasis on low- and middle-income countries. Provision of COVID-19 vaccines and funding support to countries was integrated into Gavi’s regular programming from 2024-2025 (COVID-19 vaccine support has been discontinued).
Organization
Gavi’s Secretariat, with its main headquarters in Geneva and an office in Washington, D.C., carries out the day-to-day operations of the partnership. Gavi does not have program offices or staff based in recipient countries but rather relies on country health ministries and World Health Organization (WHO) regional offices to implement programs. Gavi is led by a Chief Executive Officer (CEO), currently Sania Nishtar.
The 28-member Gavi Board sets Gavi’s funding policies and strategic direction, and monitors program implementation. It includes 18 “representative” seats, nine seats for independent individuals, and one ex-officio non-voting seat for Gavi’s CEO. The 18 representative seats, as specified in Gavi’s statutes, are as follows: donor country governments (5), implementing country governments (5), the WHO, the United Nations Children’s Fund (UNICEF), the World Bank, and the Gates Foundation, and one seat each for civil society groups, the vaccine industry in industrialized countries, the vaccine industry in developing countries, and technical health/research institutes. Additionally, several Board committees guide and advise the Board and the CEO on Gavi activities under their purview. The U.S. government was represented on Gavi’s Board as the Board member for the donor country government constituency until the end of 2025. With the suspension of U.S. support, the U.S. lost eligibility to hold a seat on the Gavi Board.
Funding
Since its 2000 launch, Gavi has received approximately $30 billion in financing, not including funding for COVAX (see Table 1).1 Approximately four-fifths (80%) of Gavi’s funding came from contributions provided by donor governments and private organizations and individuals. The top three government donors were the United Kingdom, the U.S. and Norway, while the largest private donor was the Gates Foundation.
Donors support Gavi through direct contributions as well as funding commitments to innovative financing mechanisms, the proceeds of which help support Gavi’s overall financing. These innovative financing mechanisms include the International Finance Facility-Immunisation (IFFIm) and the Pneumococcal Conjugate Vaccine (PCV) Advance Market Commitment (AMC). The IFFIm was created in 2006 and uses donor funding commitments to back the issuance of special bonds in capital markets, essentially providing “up-front” financing to Gavi. The PCV AMC began in 2010, and though it ended in 2020, it supported accelerated access to pneumococcal vaccines through up-front funding commitments from donors and continues to do so through contracts with manufacturers that extend until 2029. The U.S. does not provide support to either of these mechanisms.2
In addition to financing Gavi’s regular activities, donors pledged additional resources to support the Gavi COVAX Advance Market Commitment (COVAX AMC), a financial mechanism within COVAX that supported low- and middle-income countries through procurement and distribution of COVID-19 vaccines; through 2024, Gavi received $12.6 billion from donor governments, private philanthropy, and innovative financing mechanisms for the COVAX AMC for vaccine procurement, delivery, and logistics.3
Country Eligibility and Support
Eligibility
Only low- and middle-income countries with a Gross National Income (GNI) per capita below or equal to $1,8204 are eligible for Gavi support. In 2025, 54 countries were eligible for Gavi support.
Recipient countries’ governments are expected to share responsibility for funding their national immunization efforts through Gavi’s co-financing requirements (introduced in 2008), determined according to country income level and transition status. As countries develop economically, they are expected to contribute a greater share of the funding required for immunization programs. Countries classified as low-income by the World Bank are initial self-financing countries, while countries between the low-income threshold and Gavi eligibility threshold ($1,820 GNI per capita) are in preparatory transition. Initial self-financing countries are responsible for co-financing the equivalent of $0.20 per dose each year. Countries in preparatory transition gradually increase their co-financing contribution each year.5 When a country’s income rises above the GNI per capita threshold, it moves into an eight-year “accelerated transition” period of increasing domestic financing share, after which the country is expected to fully fund its own immunization programs.6 As of 2025, 19 countries have transitioned out of Gavi financial support.
Additionally, Gavi offers limited support for countries that have transitioned out of Gavi eligibility and for middle-income countries that have never been eligible for Gavi support.7 Recognizing that many formerly and never Gavi-eligible countries experience low coverage rates and have yet to make key vaccine introductions, eligible countries can apply for “catalytic” funding to support the introduction of key missing vaccines (HPV, PCV, or rotavirus) or mitigation of backsliding.8
Country Support
Gavi provides grant financing to country programs in the following two support types:
Vaccine support, including for vaccine introduction, targeted and routine campaigns, and
Country allocation formulas for HSIS support are based on the following metrics: number of zero-dose children, coverage of essential vaccines,10 GNI per capita, and if a country is considered fragile or conflict-affected.11 For vaccines, all countries are required to pay a share of the cost of their Gavi-supported vaccines.
Additionally, Gavi has provided country support through emergency response funding, including for Ebola vaccination during Ebola outbreaks12 and for COVID-19, allowing for up to $200 million in reprogrammed Gavi support for the COVID-19 response in Gavi-eligible countries, and other support for the COVID-19 response including through the creation of COVAX (which helped expand access to COVID-19 vaccines in lower-income countries) and the COVID-19 Vaccine Delivery Partnership (CoVDP, which aimed to improve COVID-19 vaccine coverage in certain COVAX countries, with a particular emphasis on countries that were below 10% coverage in January 2022).13 In 2022, Gavi supported 50 outbreak response vaccination campaigns. Gavi currently funds several emergency vaccine stockpiles, allowing for rapid deployment of vaccines during outbreaks, including for cholera, Ebola, meningitis, mpox,14 and yellow fever. In 2024, Gavi deployed vaccines from these emergency stockpiles to 20 countries.15
Since its launch in 2000, Gavi has provided approximately $29 billion to support country immunization programs (not including funding for COVAX).16 Over the past three years, 2023-2026, more than $8.1 billion has been disbursed, most of which has been for vaccine support (62%), followed by health systems strengthening (23%) (see Table 2).
Results
Gavi reports it has helped to immunize more than 1.2 billion children in supported countries, including more than 72 million in 2024 alone, and supported 58 different vaccine introductions and preventive campaigns and 50 outbreak response campaigns in 2024. Additionally, Gavi support has helped avert more than 20.6 million deaths and contributed to more than $280 billion in economic benefits, since its launch in 2000. Additionally, according to Gavi, its support has led to improved child health and immunization indicators across its supported countries. For example, the average vaccine coverage across multiple key Gavi-supported vaccines – including the human papillomavirus (HPV) vaccine, inactivated polio vaccine, and pentavalent vaccine (the vaccine providing protection against diphtheria, tetanus, pertussis, hepatitis B, and Hib),17 among others – was 63% in Gavi-supported countries in 2024, up from 48% in 2019.18 Lastly, Gavi’s work has contributed to vaccine market-shaping; for example, Gavi reports that its influence has helped lower the cost of the HPV vaccine from a price per dose of $4.50 in 2015 to $2.90 in 2022.19
U.S. Engagement with Gavi
The U.S. government has supported Gavi since its creation. President Clinton made the initial U.S. pledge to the newly formed partnership in 2000, and the U.S. provided its first contribution in 2001. Prior to the second Trump administration, the U.S. supported Gavi through financial contributions, participation in Gavi’s governance, and by providing technical assistance, but the current administration has not provided funding to the organization (see below).
Additionally, the U.S. had supported other global immunization activities that complemented Gavi’s efforts, providing bilateral (country-to-country) support for immunization through USAID (before its dissolution), CDC, and other agencies, focusing on strengthening routine immunization systems to deliver vaccines. However, the U.S. government is currently reorganizing how it supports global health programs, including immunization activities, under its “America First Global Health Strategy” which includes the development of bilateral agreements with countries. Given that Gavi was the mechanism through which the U.S. supported vaccine procurement, it is not yet clear how these agreements will support procurement going forward. See also the KFF fact sheet on the Trump administration’s foreign aid review and the proposed reorganization of U.S. global health programs.
Financial Support
The U.S. supported Gavi with direct contributions starting in 2001, with funding reaching $300 million in FY 2024, its highest level. Additionally, in response to the COVID-19 pandemic, the U.S. provided $4 billion in FY 2021 emergency funding to Gavi for COVID-19 vaccine procurement and delivery support under COVAX, making the U.S. the largest donor to COVAX (32% of $12.6 billion received overall).20In addition to its financial support for COVAX, the U.S. donated the largest number of COVID-19 vaccines to other countries. While Congress appropriated $300 million for U.S. contributions to Gavi in FY 2025 and FY 2026 (see Figure 1), the current administration has not provided funding to Gavi after citing concerns about vaccine safety despite Gavi following globally recognized scientific standards and evidence.21 See the KFF budget tracker and the KFF fact sheet on the U.S. Global Health Budget: Maternal & Child Health (MCH) for details on historical appropriations for Gavi, and also the KFF fact sheet on the Trump administration’s foreign aid review and the status of U.S. support for Gavi.
Governance Activities
The U.S. had historically played a role in Gavi’s governance, including as a Board and committee member, but with the suspension of U.S. funding by the Trump administration, the U.S. is no longer eligible to hold a Board seat.
Technical Support
The U.S. had historically provided Gavi with technical support and expertise in the design, implementation, and evaluation of its programs in the field through partnerships with several U.S. agencies. For example, Gavi’s accelerated vaccine introduction programs had been conducted with technical support from the Centers for Disease Control and Prevention (CDC) and the now-dissolved U.S Agency for International Development (USAID), along with other partners.
Endnotes
This amount includes proceeds for 2000-2024 and pledges for 2025. ↩︎
For further information about restrictions on U.S. support for these innovative financing mechanisms, see KFF, Innovative Financing Mechanisms for Global Health: Overview and Considerations for U.S. Government Participation, Sept. 2011. ↩︎
For countries to be eligible for Gavi support, their most recent GNI per capita must be at or below $1,820, or the country’s average GNI per capita over the last three years must be at or below $1,820. ↩︎
Countries in the first year of the accelerated transition phase co-finance the equivalent of the prior year’s total fraction plus 15%, the same as countries in preparatory transition. For each year after, the amount per dose increases linearly until the country is fully financing each vaccine after the eighth year and end of Gavi support. Gavi, “Co-financing policy,” https://www.gavi.org/sites/default/files/programmes-impact/our-impact/01_Gavi-Alliance-Co-financing-Policy-60.pdf. ↩︎
KFF analysis of data provided by Gavi on disbursements by program area and year. KFF personal communications with Gavi, March 19, 2026. ↩︎
The vaccines included in Gavi’s breadth of protection measure include: the third dose of the pentavalent vaccine, third dose of the pneumococcal conjugate vaccine, first dose of the rubella-containing vaccine, last dose of the rotavirus vaccine, second dose of the measles-containing vaccine, yellow fever, meningococcal A, Japanese encephalitis, and last dose of the HPV vaccine. Gavi, “Gavi 2024 Annual Progress Report,” https://www.gavi.org/sites/default/files/programmes-impact/our-impact/apr/Gavi-2024-Annual-Progress-Report.pdf#page=17. ↩︎
The U.S. announced it would donate 500 million Pfizer doses to COVAX at the G7 Summit in June 2021. However, a portion of these doses were purchased using funds appropriated to Gavi ($2 billion for 300 million Pfizer doses), while the remaining 200 million doses were purchased using $1.5 billion in other emergency funds from the American Rescue Plan Act. To avoid double-counting, Gavi counts the U.S. funding that was contributed to Gavi under its COVAX funding contributions, with only 200 million of the doses – those purchased directly by the U.S. – counted as COVAX vaccine dose donations. KFF personal communication with Gavi, Nov. 12, 2021; White House, “FACT SHEET: President Biden Announces Historic Vaccine Donation: Half a Billion Pfizer Vaccines to the World’s Lowest-Income Nations,” June 10, 2021; Gavi, “COVAX AMC Donors Table,” Apr. 7, 2022, https://www.gavi.org/sites/default/files/covid/covax/COVAX-AMC-Donors-Table.pdf; Gavi, “Cash Receipts 31 December 2024,” https://www.gavi.org/news-resources/document-library/cash-receipts. ↩︎
The Temporary Protected Status (TPS) program was established in 1990 and allows the Secretary of Homeland Security to designate a country for TPS if there is an ongoing armed conflict, environmental disaster, epidemic, or other conditions that may “temporarily prevent the country’s nationals from returning safely.” Eligible individuals from TPS designated countries can receive TPS, which protects them from deportation and allows them to work in the U.S. for temporary, extendable periods.
The Trump administration has carried out numerous immigration policy changes focused on increasing immigration enforcement and reducing immigration into the country, including seeking to end TPS designations for many countries. Further, under the 2025 reconciliation law, TPS holders will lose access to subsidized ACA Marketplace coverage starting January 1, 2027, and Medicare starting no later than January 4, 2027, while they already are ineligible for Medicaid and the Children’s Health Insurance Program (CHIP). This brief provides an overview of the TPS program, recent changes to TPS designations announced by the Trump administration, and potential implications of loss of TPS for individuals on health and health care. It includes KFF analysis of Congressional Research Service reports to assess changes in the number of individuals and countries with TPS designations over time and of 2024 American Community Survey (ACS) data to estimate the number of noncitizen immigrant workers likely to have TPS, who could be impacted by the elimination of TPS designations.
According to federal data, as of March 2025 (the latest data available), nearly 1.3 million individuals from 17 countries had TPS. As of March 2026, the Trump administration has ended or attempted to end TPS designations for 13 of 17 countries with active TPS designations at the time he took office, which could impact over one million TPS holders. However, implementation of some of these changes is subject to ongoing litigation. Individuals who lose TPS lose their work authorization and become at risk for deportation, which may negatively impact their health and access to health coverage and care. Moreover, termination of TPS designations could negatively impact the U.S. economy and workforce by putting hundreds of thousands of immigrant workers at risk of deportation. Immigrants likely to have TPS from 16 of the 17 countries for which data are available made up about 740,000 workers ages 18 and older in the U.S. as of 2024, including about 53,000 workers in the health care industry.
Overview of the TPS Program
The TPS program was established under the Immigration Act of 1990 to allow eligible immigrants from designated countries to live and work in the U.S. The program is administered by U.S. Citizenship and Immigration Services (USCIS) within the Department of Homeland Security (DHS). DHS has the authority to designate a country for TPS for periods of 6 to 18 months and can extend these periods if conditions in the country continue to prevent its nationals from returning safely, such as due to armed conflict or environmental disasters. TPS provides immigrants with employment authorization and protection from deportation but it does not provide a pathway to citizenship. A TPS holder can only obtain permanent status by separately qualifying for another immigration status, such as lawful permanent residence through a family-based or employment-based visa petition.
As of March 2025, close to 1.3 million noncitizen immigrants from 17 countries had TPS with five countries, Venezuela, Haiti, El Salvador, Ukraine, and Honduras, accounting for approximately 97% of all recipients. The remaining 12 countries include over 39,000 individuals with TPS. The number of people with TPS has grown in recent years, from under 500,000 in 2017 to about 1.3 million in 2025, driven by new country designations, particularly for Venezuela and Ukraine, as well as redesignations for countries like Haiti that continue to face ongoing humanitarian crises (Figure 1).
Recent Changes to TPS Designations
The Trump administration has ended or attempted to end TPS designations for 13 of 17 countries that had designations when he took office, which could impact about one million TPS holders, but implementation is subject to ongoing litigation (Appendix Table 1). As of March 31, 2026, termination of TPS designations for Afghanistan, Cameroon, Honduras, Nepal, Nicaragua, and certain Venezuelan TPS holders had already taken effect, impacting close to 320,000 TPS holders from these countries. Termination of TPS designation for Yemen is expected to take effect in May 2026, and termination of TPS designation as well as work authorization for remaining Venezuelan TPS holders is expected to take effect in October 2026, which could impact over 350,000 immigrants from these countries. Further, the Trump administration has taken steps to end TPS designations for Burma (Myanmar), Ethiopia, Haiti, Somalia, South Sudan, and Syria, but these terminations were on hold as of March 31, 2026, due to court challenges. If allowed to proceed, these terminations could lead to an additional 330,000 immigrants losing TPS status.
Potential Implications of Loss of TPS
Individuals who lose TPS lose their work authorization and become at risk of deportation, which may negatively impact their access to health coverage and care. The Trump administration’s attempts to end TPS designations for 13 of 17 countries put a vast majority of TPS holders at risk of losing their status and becoming subject to deportation as well as losing access to health coverage. As of 2026, TPS holders are eligible for subsidized ACA and Medicare coverage if they meet other program eligibility requirements. They are not eligible for Medicaid and CHIP. TPS holders who lose their status would become undocumented and lose access to any federally funded coverage. Under longstanding policy, undocumented immigrants are ineligible for all forms of federally funded health coverage including Medicaid, CHIP, Medicare, and coverage through the ACA Marketplace. Further, loss of TPS would result in immigrants losing their work authorization, leading to employment loss and, consequently, potential loss of access to employer-sponsored health coverage. At the same time, lost income due to job loss may make it difficult for impacted immigrants to afford health care. Based on KFF analysis of ACS data, as of 2024, over four in ten (44%) of likely TPS workers 18 and older from 16 of 17 countries with active TPS designations at the time had employer-sponsored health coverage compared to 45% of other noncitizen workers and 70% of U.S. citizen workers 18 and older.
Loss of TPS may also negatively affect people’s health by increasing their immigration-related worries and making them more reluctant to access health care. People losing TPS status become undocumented, putting them at risk for deportation and likely increasing their immigration-related worries. Data from the 2025 KFF Survey of Immigrants show that over three in four (77%) of likely undocumented immigrants say they have experienced negative health impacts due to immigration-related worries since January 2025, and about half (48%) say that they have avoided seeking medical care since January 2025 due to immigration-related concerns.
Termination of TPS designations may also have negative impacts on the U.S. workforce, which included about 740,000 likely TPS workers overall as of 2024. KFF analysis of ACS data show that, as of 2024, noncitizen immigrants likely to have TPS from 16 of the 17 countries with active designations at the time made up about 740,000 workers in the U.S., including about 53,000 health care workers. These include noncitizen immigrants ages 18 and older who were born in a country with an active TPS designation as of December 2024 and whose year of entry in the U.S. is on or before the most recent continuous residence requirement for their country as specified by USCIS (see methods for more details). Data for immigrants from South Sudan were not available separately in ACS. Among noncitizen immigrants ages 18 and older likely to have TPS from the 16 countries with data available, about three in four (74%) report being employed compared to about two-thirds (67%) of other noncitizen immigrants and about six in ten (62%) U.S. citizens ages 18 and older.
Methods
This analysis is based on KFF analysis of the 2024 American Community Survey (ACS) 1-year Public Use Microdata Sample. Individuals likely to have TPS were identified in ACS as those who report being noncitizen immigrants, were born in a country with an active TPS designation as of December 2024 for which data are available namely, Afghanistan, Burma (Myanmar), Cameroon, El Salvador, Ethiopia, Haiti, Honduras, Lebanon, Nepal, Nicaragua, Somalia, Sudan, Syria, Ukraine, Venezuela, or Yemen (country of birth data for South Sudan is not available separately in ACS); arrived in the U.S. on or before the year of the most recent continuous residence requirement for their country as specified by USCIS; do not receive Medicaid, Supplemental Nutrition Assistance Program (SNAP), or Social Security; and do not work for the U.S. government or military since TPS holders are excluded from these benefits and are generally excluded from government and military service. Workers were further identified as those ages 18 and older who report being employed and currently at work in the U.S. civilian labor force and health care workers were identified as a subset of all workers who worked in the health care industry (industry codes 7970 through 8290).
Appendix
Table 1
Country
Initial Designation
Latest Designation
Status as of March 2026
Number of TPS Holders as of March 2025
Afghanistan
5/20/2022
11/21/2023
Terminated effective 7/14/2025
8,105
Burma (Myanmar)
5/25/2021
5/26/2024
Terminated effective 1/26/2026, but restored subject to court order
3,670
Cameroon
6/7/2022
12/8/2023
Terminated effective 8/4/2025
4,920
El Salvador
3/9/2001
Active
170,125
Ethiopia
12/12/2022
7/13/2024
Terminated effective 2/13/2026, but restored subject to court order
4,540
Haiti
1/21/2010
8/4/2024
Terminated effective 2/3/2026, but restored subject to court order
330,735
Honduras
1/5/1999
Terminated effective 9/8/2025
51,225
Lebanon
11/27/2024
Active
140
Nepal
6/24/2015
Terminated effective 8/20/2025
7,160
Nicaragua
1/5/1999
Terminated effective 9/8/2025
2,910
Somalia
9/16/1991
9/18/2024
Terminated effective 3/17/2026, but restored subject to court order
705
South Sudan
11/3/2011
11/4/2023
Terminated effective 1/5/2026, but restored subject to court order
210
Sudan
11/4/1997
10/20/2023
Active
1,790
Syria
3/29/2012
4/1/2024
Terminated effective 11/21/2025, but restored subject to court order
3,860
Ukraine
4/19/2022
10/20/2023
Active
101,150
Venezuela (2021 desig.)
3/9/2021
Terminated effective 11/7/2025, small number of individual cases on hold pending court activity
252,825
Venezuela (2023 desig.)
9/20/2023
Terminated effective 10/3/2025, with work authorization for some beneficiaries valid until 10/2/2026 subject to court order
CMS recently finalized policies as part of the 2027 Medicare Advantage final rule that both enhance consumer protections and roll back changes to the Medicare Advantage program that were intended to protect consumers. These changes have gotten less attention than payment issues and changes to the star ratings system, which also affect plan payments, but could have implications for Medicare beneficiaries (See Table 1):
CMS will enhance some consumer protections by requiring Medicare Advantage plans to post eligibility criteria for Special Supplemental Benefits for the Chronically Ill (SSBCI), making it easier for prospective enrollees to assess their eligibility for these benefits, which include food and produce, pest control, and transportation for non-medical needs, among others. CMS also added guardrails for debit cards issued by plans to administer supplemental benefits, so enrollees can better understand how to use these cards to obtain their benefits and also to prevent the purchase of non-covered items.
CMS rolled back some changes to the Medicare Advantage program that were intended to protect consumers, including rescinding a requirement that plans notify enrollees of unused supplemental benefits mid-year, as well as eliminating a number of marketing requirements, such as provisions aimed at increasing the separation between marketing activities from educational events and a prohibition on the use of superlatives in marketing materials, and removes the State Health Insurance Assistance Programs (SHIPs) from the list of resources that brokers must offer to beneficiaries for further information during sales calls.
In addition, CMS did not finalize a proposal that would have modified a special enrollment period to make it easier for enrollees to switch coverage if one of their providers is no longer part of their Medicare Advantage’s plan network.
CMS Finalized a Few Changes to the Medicare Advantage Program That Enhance Some Consumer Protections
Improving SSBCI Eligibility Transparency. Medicare Advantage plans offer supplemental benefits to Medicare Advantage plan enrollees, such as dental, vision, and hearing, which are considered primarily health related (e.g., preventing or treating an illness). Beginning in 2020, Medicare Advantage plans have also been able to offer supplemental benefits that are not primarily health related for chronically ill beneficiaries, known as Special Supplemental Benefits for the Chronically Ill (SSBCI). These benefits include food and produce, general supports for living (i.e. assistance with housing and utilities), pest control, and transportation for non-medical needs, among others. To receive these benefits, Medicare Advantage enrollees must have one or more comorbid and medically complex chronic conditions that meet all of the following criteria:
is life threatening or significantly limits the overall health or function of the enrollee;
has a high risk of hospitalization or other adverse health outcomes; and
requires intensive care coordination.
Additionally, Medicare Advantage plan must determine that the benefit has a reasonable expectation of improving or maintaining the health or overall function of the chronically ill enrollee.
The final rule requires Medicare Advantage plans to post on their websites the eligibility criteria they use to determine whether an enrollee qualifies for SSBCI to increase transparency for potential enrollees, including both the criteria for meeting the “chronically ill” definition as well as the specific criteria for each benefit. Previously, plans were not required to post eligibility criteria publicly. CMS noted that in response to a prior rule, they had received many comments requesting that plans post their specific SSBCI criteria on a public-facing website. CMS expects this change will provide greater transparency for Medicare Advantage enrollees and improve their ability to assess whether they are eligible for these benefits and make an informed decision when they are deciding whether to enroll in a plan.
Moreover, CMS added regulatory language to ensure plans apply the eligibility criteria to Medicare Advantage enrollees in an objective and consistent manner. The rule clarifies that Medicare Advantage plans must verify all statutory criteria for "chronically ill" status through an objective process such as a health risk assessment or a claims review, rather than allowing self-attestation alone.
Enhancing Guardrails for Debit Cards that Administer Supplemental Benefits. Medicare Advantage plans are permitted to use debit cards to administer supplemental benefits, such as helping cover the cost of dental or vision services, the purchase of over-the-counter products, or the purchase of food and produce at participating retailers. CMS requires that Medicare Advantage plans administer these benefits in a way that ensures the debit card only be used towards plan-covered items and services. CMS noted, however, that enrollees frequently express confusion about what can be purchased with their plan debit card, and that stakeholders have raised concerns that these cards could be used to purchase items that are not covered by Medicare Advantage plans, particularly at large retailers. CMS also indicated that debit cards may be subject to fraud in the absence of stronger guardrails applied to non-covered items.
The final rule codifies existing regulations and adds requirements regarding the use of debit cards for supplemental benefits. Beginning in 2027, Medicare Advantage plans that choose to use debit cards to administer supplemental benefits must provide cards that are electronically linked to plan-covered benefits through a real-time identification mechanism that verifies eligibility at the point of sale. CMS states that real-time verification will ensure ease of access to benefits, increase transparency, and help eliminate fraud by preventing unauthorized purchases of non-covered items. Plans are also required to provide instructions to enrollees on how to use the debit card, provide customer support service to enrollees who have questions about how to use the debit card, and maintain an alternative reimbursement process for circumstances where enrollees are not able to use their debit card. CMS explained that it expects these changes will make Medicare Advantage enrollees more aware of their debit card benefits and how to use them.
The rule does not finalize a proposed change that would have prohibited marketing materials from listing the dollar value of supplemental benefits or the method by which these benefits are administered (e.g., debit cards or “Medicare flex cards”). In the proposal, CMS raised concerns with marketing tactics related to debit cards, including that some Medicare Advantage plans had been marketing the debit cards in inaccurate and misleading ways, using terms like "flex card" with an enticing dollar value attached to them, which might imply enrollees will automatically receive unrestricted spending money just by enrolling in the plan. However, CMS declined to finalize this proposal, citing concerns that this change would reduce informed decision-making before beneficiaries enroll in a plan.
CMS Also Rolled Back Changes to the Medicare Advantage Program That Were Intended to Protect Consumers
Mid-Year Supplemental Benefits Notice Rescinded. Medicare Advantage plans offer an array of supplemental benefits, but there is little data yet available to examine how frequently enrollees are using the benefits available to them. Medicare beneficiaries often highlight the availability of extra benefits as a reason they choose to enroll in Medicare Advantage plans, and CMS has also observed beneficiaries make enrollment decisions on these benefits, but that enrollees are often unaware of the benefits available to them and are not using them. The April 2024 final rule required Medicare Advantage plans to send enrollees a mid-year notice, between June 30 and July 31 of each plan year, listing any supplemental benefits the enrollee had not yet used during the first six months of the year, which was set to take effect January 1, 2026.
CMS rescinded this requirement before it took effect, citing several reasons: more recent survey data showing that 70 percent of Medicare Advantage enrollees reported using at least one supplemental benefit in the past year, which CMS suggests means beneficiaries are aware of these benefits, (though CMS notes there are still data gaps on utilization of these benefits); the administrative and financial burden on plans, particularly on smaller Medicare Advantage plans; and that this information is duplicative of information in the Annual Evidence of Coverage document that is already sent to enrollees. They also note this recission is consistent with the administration’s priorities to reduce unnecessary regulatory burdens, laid out in its Executive Order, Unleashing Prosperity Through Deregulation.
Marketing Requirements Rolled Back. CMS regulates how Medicare Advantage insurers, as well as agents, brokers, and other third parties who sell Medicare Advantage plans may communicate with beneficiaries. In recent years, CMS has documented patterns of aggressive and misleading marketing behavior, based on reports from state insurance commissioners, State Health Insurance Assistance Programs (SHIPs), and beneficiary advocacy groups, and has made a number of changes in prior rules to provide additional oversight of Medicare Advantage plan marketing. The recent final rule eliminates many of these provisions, with the stated goal of streamlining regulatory requirements for agents and brokers, and making the services offered by these groups more accessible to beneficiaries.
Limitations on Marketing at Educational Events Rolled Back: CMS requires that Medicare Advantage insurers, agents, and brokers clearly distinguish between educational and marketing events, and prohibits the discussion of specific plan costs or benefits at events promoted as educational. The April 2023 final rule reinforced this separation by prohibiting the collection of scope of appointment forms at educational events, requiring a 48-hour waiting period between the collection of scope of appointment forms and personal marketing appointments, and requiring a 12-hour waiting period between educational and marketing events at the same location. These provisions were intended to prevent beneficiaries from feeling pressured into attending marketing events or making coverage decisions on the spot when seeking out educational information.
The current final rule rolls back these provisions, citing stakeholder feedback that waiting periods create unnecessary delays and may be burdensome to beneficiaries who must travel for multiple events and appointments that could otherwise take place in a single session. Agents and brokers may now collect scope of appointment forms at educational events, and may conduct a personal marketing appointment at any point afterwards, with no waiting period. Further, educational and marketing events may now be held back-to-back in the same location, provided that beneficiaries are notified of the transition and offered the opportunity to leave if they prefer. CMS noted that some commenters opposed these changes due to concern that they may leave beneficiaries more vulnerable to aggressive sales tactics and may blur the line between educational and marketing information.
Prohibition on Use of Superlatives in Marketing Materials Eliminated: The final rule eliminates certain requirements around the language used in marketing materials, such as a prohibition on the use of superlatives (e.g., “best” or “most”) without supporting documentation. CMS first introduced this requirement in the April 2023 final rule, citing concern that these claims may be misleading when taken out of context, and may encourage beneficiaries to enroll in a plan based on information that is misrepresented or misunderstood. The current rule revises this stance, stating that existing CMS requirements already prohibit the use of misleading or inaccurate claims in marketing materials, while the prohibition on superlatives represents an undue burden for insurers, agents, and brokers that does not meaningfully expand on these other protections.
Mandatory Disclaimer Requirements Modified: CMS requires that brokers and other third parties who represent multiple Medicare Advantage insurers begin all sales calls with a mandatory disclaimer stating that they do not represent every plan available in the area and providing beneficiaries with a list of resources they may reach out to for further information. CMS introduced this requirement in the May 2022 final rule to ensure that beneficiaries had access to complete, unbiased information about their coverage options, as many brokers only represent a subset of available plans and may have a financial incentive to steer beneficiaries towards some plans over others. The current final rule preserves this requirement, but allows the disclaimer to be provided later in the call as long as it is stated before any discussion of specific plan benefits, rather than in the first minute of the call as previously required.
Notably, the rule also removes the State Health Insurance Assistance Programs (SHIPs) from the list of resources that must be included in the disclaimer, now limited to official CMS resources such as 1-800-MEDICARE and Medicare.gov. SHIPs are federally-funded, state-based programs that offer free, unbiased counseling and education to Medicare beneficiaries. This change prompted criticism from some commentors, who noted that 1-800-MEDICARE is not generally equipped to provide the same level of in-depth counseling or local information that SHIP counselors are trained to provide. However, CMS states that SHIP volunteers may not always have the expertise to help beneficiaries navigate increasingly complex Medicare Advantage options and that the standardized training and 24/7 availability of customer service representatives at 1-800-MEDICARE make it a more appropriate resource in this context, while also noting that 1-800-MEDICARE may still refer callers to their local SHIP on a case-by-case basis.
CMS Declined to Finalize a Proposal to Streamline the Medicare Advantage Special Enrollment Period for Provider Terminations
Medicare Advantage plans have networks of providers, and beneficiaries must see providers in their plan’s network or potentially pay higher cost sharing. KFF analysis has shown that Medicare Advantage enrollees have access to about half of the physicians available to traditional Medicare beneficiaries in their area, on average. Medicare beneficiaries say having access to their preferred providers is an important factor when selecting their Medicare coverage. With this in mind, the Trump administration recently launched a new provider search tool on the Medicare plan finder to help beneficiaries identify if their doctors are in a plan’s network, though it experienced issues during its initial rollout.
While Medicare beneficiaries may select plans based on access to their preferred doctors and hospitals, providers can leave Medicare Advantage networks at any time during the year, potentially disrupting coverage for plan enrollees. Currently, a special enrollment period (SEP) for Significant Change in Provider Network allows Medicare Advantage enrollees to switch plans or return to traditional Medicare when CMS determines there were "significant" changes to their plan's provider network – for example, the termination of a contract with a large hospital system. When CMS makes that determination, Medicare Advantage plans must send a separate notice to affected enrollees explaining their SEP eligibility to select different coverage, including guaranteed issue rights to purchase a Medigap policy regardless of pre-existing conditions.
CMS proposed to eliminate the significance determination, making the SEP available to any "affected enrollee" of a provider termination, defined as someone assigned to, currently receiving care from, or having received care within the past three months from a terminated provider. Rather than waiting for CMS to review and approve a significance finding, plans would include SEP eligibility information in the standard provider termination notice already sent to enrollees. Enrollees could then attest directly to the plan that they meet the affected enrollee definition and are eligible for a special enrollment period to change their Medicare coverage.
This proposal would have put the decision in the hands of Medicare beneficiaries – allowing them to decide whether a provider termination was significant enough to warrant switching coverage, rather than waiting for that determination from CMS. However, CMS declined to finalize this proposal and did not explain its rationale for its decision. CMS does note that this topic generated broad interest and may be addressed in further rulemaking.