KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Use of telehealth, which allows patients to see health care providers without being in the same location, has grown rapidly in recent years, among both privately-insured patients and Medicare beneficiaries. Prior to the COVID-19 pandemic, telehealth utilization in traditional Medicare was very low, but it rose dramatically in 2020 following temporary measures put in place at the start of the COVID-19 public health emergency that greatly expanded the scope of Medicare coverage of telehealth. Since early 2021 telehealth use has declined steadily, but it remains higher than pre-pandemic levels, with considerable variation by income level, race and ethnicity, and urban versus rural location, among other factors.
Congress has extended a number of pandemic-era flexibilities around Medicare coverage of telehealth beyond the COVID-19 public health emergency, which ended on May 11, 2023, but most of these flexibilities are due to expire in December 2024. There is bipartisan support for proposedlegislation to extend these provisions for another two years, and Congress is weighing the potential benefits, risks, and costs of permanently expanding Medicare coverage of telehealth services. Medicare beneficiaries are generally satisfied with their telehealth visits, and many health care providers are supportive of keeping these services accessible, but questions remain about the longer-term impact on patient care, Medicare spending, and program integrity.
These FAQs provide answers to key questions about the current scope of Medicare telehealth coverage, including both temporary and permanent changes adopted through legislation and regulation, and policy considerations that lie ahead.
What is the current scope of Medicare telehealth coverage and how did it change at the start of the COVID-19 pandemic?
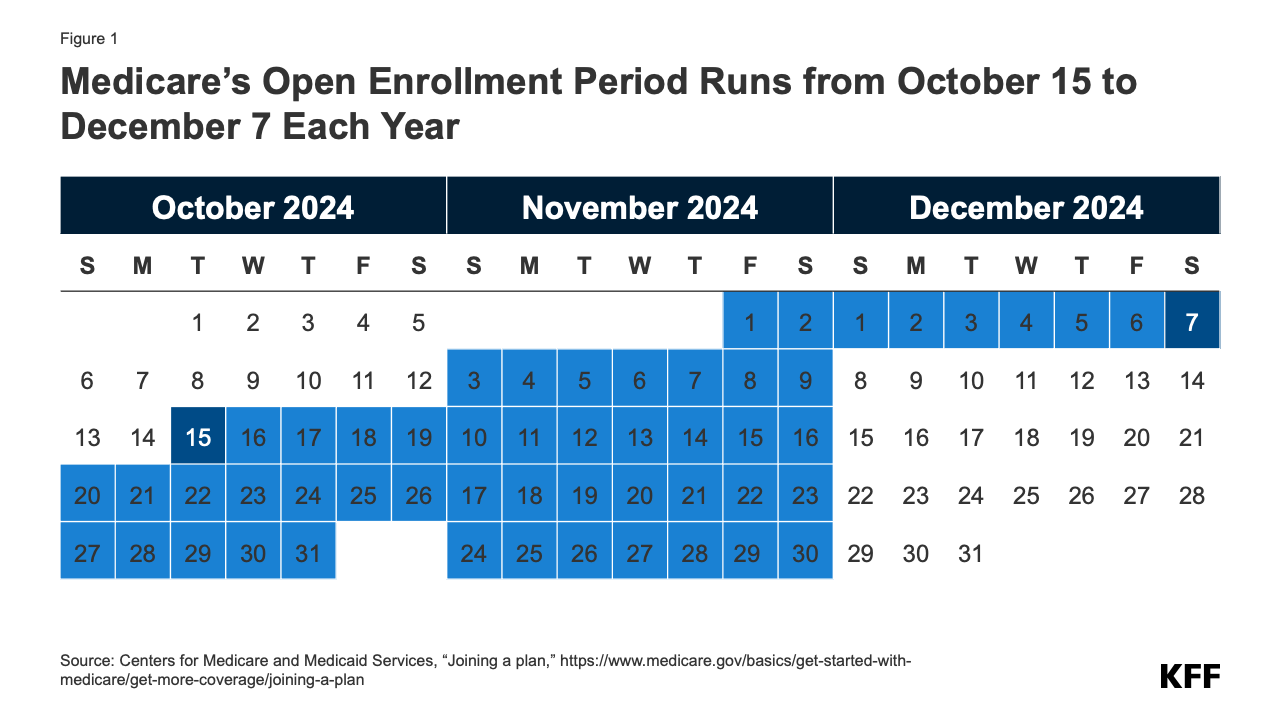
Prior to the declaration of the COVID-19 public health emergency, Medicare coverage of telehealth was largely restricted to beneficiaries in rural areas and to certain types of providers, facilities, and services. At the time, beneficiaries were typically required to travel from their homes to approved clinical sites where they could receive care from providers at other locations. To make it easier and safer for beneficiaries to seek medical care during the pandemic, the Secretary of the Department of Health and Human Services (HHS) waived many of these restrictions in March 2020, enabling broader use of telehealth services for all Medicare beneficiaries. While the pandemic-related expansion of telehealth coverage under Medicare was initially due to expire at the end of the COVID-19 public health emergency, subsequent legislation extended many of these flexibilities through December 2024 and incorporated others into the program on a permanent basis (Figure 1).
The following list summarizes key provisions of current law related to coverage of telehealth in traditional Medicare, both temporary and permanent. (See section below for a discussion of telehealth coverage by Medicare Advantage plans.)
Temporary telehealth provisions (currently due to expire after December 31, 2024)
Waiver of geographic and “originating site” requirements: Telehealth is currently available to Medicare beneficiaries in both urban and rural areas, and patients can receive telehealth services from any location, including their home as the “originating site.” Prior to the expansion, telehealth coverage in traditional Medicare was limited to rural areas (with certain exceptions), and patients were required to travel to an approved originating site, such as a clinic or doctor’s office, when receiving telehealth services. (Providers participating in select accountable care organizations (ACOs) are permitted to waive these requirements under the Bipartisan Budget Act of 2018, and may continue to provide telehealth services without geographic restrictions, and to beneficiaries in their homes, should the current flexibilities expire.)
Expansion of covered telehealth services: Medicare currently offers coverage for an expanded set of telehealth services, including physical and occupational therapy, emergency department visits, and nursing facility care. Prior to the expansion, Medicare offered coverage for a more limited set of telehealth services, such as preventive health screenings, office visits, and psychotherapy. The Centers for Medicare & Medicaid Services (CMS) has the authority to expand the list of allowable telehealth services when there is a demonstrable clinical benefit and continues to evaluate select services for permanent inclusion on this list.
Coverage of audio-only services: Medicare currently allows a limited set of telehealth services to be provided to patients via audio-only platforms, such as a telephone or a smartphone without video. Prior to the expansion, Medicare required all telehealth services to be provided via a two-way audio/video connection, such as an interactive audio-video system or a smartphone with video enabled.
Expansion of eligible “distant site” telehealth providers: Currently, any health care provider who is eligible to bill for Medicare-covered services can provide and bill for telehealth as a “distant site” telehealth provider and may conduct an initial telehealth visit whether or not they have treated the beneficiary previously. Additionally, federally qualified health centers (FQHCs) and rural health clinics (RHCs) are now authorized to provide and bill for telehealth. Prior to the expansion, only physicians and certain other providers (e.g., physician assistants, clinical social workers, and clinical psychologists) were permitted to bill for telehealth services as the distant site provider and must have treated the beneficiary receiving those services within the last three years. FQHCs and RHCs were not authorized to serve as distant site providers but could serve as originating sites if located in a qualifying area.
Waiver of in-person visit requirement for behavioral health: Currently, Medicare beneficiaries receiving behavioral health services may opt to receive these services via telehealth with no in-person visit requirements. The Consolidated Appropriations Act of 2021 made numerous changes to Medicare coverage of behavioral telehealth (see below), including a provision that beneficiaries must have an in-person visit with their behavioral health provider no more than six months before their initial telehealth appointment and annually thereafter. Subsequent legislation delayed this requirement until January 2025.
Use of telehealth for hospice recertification: Patient recertification for the Medicare hospice benefit can currently be conducted via telehealth, provided there is a two-way audio/video connection that allows for real-time interaction between the patient and hospice provider. Prior to the expansion, only in-person encounters could be used for the purposes of hospice recertification.
Permanent telehealth provisions
Behavioral health: The Consolidated Appropriations Act of 2021 permanently removed geographic and originating site restrictions for any telehealth service used to diagnose, evaluate, or treat a mental health disorder. (These restrictions had already been lifted for treatment of substance use disorders and co-occurring mental health disorders in 2018). While many other provisions related to telehealth coverage expire at the end of 2024, Medicare beneficiaries may continue to receive behavioral health services from their homes, in both urban and rural areas, and may do so via audio-only platforms if they are unable to access a video connection or do not consent to video use. Additionally, FQHCs and RHCs are permanently allowed to serve as telehealth providers for behavioral health services.
What trends have emerged in Medicare beneficiaries’ use of telehealth services?
Telehealth use in traditional Medicare increased dramatically at the start of the COVID-19 public health emergency, with nearly half (46.7%) of all eligible beneficiaries receiving at least one telehealth service in the second quarter of 2020, compared to just 6.9% in the first quarter (Figure 2). While use has declined since that time, it remains nearly two times higher than pre-pandemic levels, with more than one in ten (12.7%) eligible beneficiaries receiving a telehealth service in the final quarter of 2023.
Use of telehealth services varies by geography, race and ethnicity, reason for Medicare eligibility, and dual enrollment in Medicare and Medicaid (Figure 3).
Geography: Rates of telehealth use in 2023 were higher among beneficiaries living in urban areas than those in rural areas (27% vs. 19%), which may be due in part to disparities in access to broadband and other communication technologies. Beneficiaries in rural or underserved areas may lack the infrastructure to support reliable video telehealth visits or the means to afford internet access, which may further impede access to telehealth if coverage of audio-only services is reduced or eliminated.
Race and ethnicity: Rates of telehealth use in 2023 were highest among Asian and Pacific Islander (31%) and Hispanic (30%) beneficiaries, and somewhat lower among Black (26%), American Indian or Alaska Native (25%), and non-Hispanic White beneficiaries (24%). Given that beneficiaries of color are more likely than non-Hispanic White beneficiaries to report difficulty accessing needed health services, telehealth use may help to improve access to care for certain groups.
Reason for Medicare eligibility: Rates of telehealth use in 2023 were higher among beneficiaries who qualify for Medicare based on having end-stage renal disease (ESRD) (37%) or a long-term disability (37%), relative to those who qualify based on age (23%). This may be due in part to higher overall rates of service use among people with ESRD and disabilities (whether in-person or via telehealth) but may also reflect a preference for telehealth services among these populations, or a greater ease of accessing care via telehealth relative to in-person care. Beneficiaries under age 65 who qualify for Medicare based on having long-term disabilities are more likely than older beneficiaries to report having three or more limitations in activities of daily living, and may be more likely to benefit from the increased flexibility of receiving health care services from their home via telehealth.
Dual-eligible individuals: Rates of telehealth use in 2023 were higher among beneficiaries dually eligible for both Medicare and Medicaid compared to Medicare beneficiaries who were not Medicaid-eligible (34% vs. 23%). Dual-eligible individuals are four times more likely than other Medicare beneficiaries to live on incomes of less than $20,000. Prior studies have found that having lower income or living in a socioeconomically deprived neighborhood is associated with higher rates of telehealth use, suggesting that telehealth may have the potential to improve health care access for beneficiaries with limited access to in-person services.
How does Medicare pay providers for telehealth services?
Medicare currently pays providers for telehealth services, both video and audio-only, at the same rate that would be paid if the service were delivered in person. As with most services paid under the Medicare physician fee schedule, payment rates for telehealth services currently vary based on the location of the provider, with services furnished by providers based in a non-facility setting, such as a doctor’s office, reimbursed at a higher rate than services furnished by providers based in a facility setting, such as a hospital outpatient department.
Prior to the COVID-related temporary expansion, Medicare paid for all covered telehealth services at the lower facility rate, regardless of provider location. This means that providers in non-facility settings currently receive higher payment for telehealth services than they did before the temporary expansion. However, assuming no change to current law, Medicare will resume paying for most telehealth services (with the exception of behavioral health services) at the lower facility rate beginning in January 2025. The Consolidated Appropriations Act of 2021 permanently established payment parity between in-person and telehealth services in the context of behavioral health. Should the current flexibilities expire, Medicare will continue to pay providers for behavioral telehealth services at the same rate they would receive if the service were delivered in person.
CMS permanently authorized FQHCs and RHCs to provide and bill for behavioral telehealth services in 2022. As with other types of providers, clinicians in these settings are paid the same rate for behavioral telehealth services as they would receive if the service were delivered in person on a permanent basis. However, for all other types of telehealth services, FQHCs and RHCs are only eligible for reimbursement through December 2024. Medicare currently pays FQHCs and RHCs at rates comparable to those set under the physician fee schedule, which are lower than what they would receive for comparable in-person care, since Medicare typically pays more for clinician services provided by FQHCs and RHCs than those provided in other types of settings.
How do Medicare Advantage plans cover telehealth?
Medicare Advantage plans are required to cover all Part A and Part B benefits covered under traditional Medicare, and have some flexibility to offer additional benefits as well, including telehealth benefits not routinely covered by traditional Medicare (outside of the current telehealth expansion), such as telehealth services provided to enrollees in their own homes, services provided outside of rural areas, and services provided through audio-only platforms.
Since 2020, Medicare Advantage plans have been permitted to include the costs associated with select telehealth services in their basic Medicare Part A and B benefit package, and may continue to do so after December 2024 regardless of the status of the temporary telehealth expansions in traditional Medicare. Telehealth services may be included in a plan’s basic benefits package if they meet certain requirements, such as coverage under Medicare Part B when the same service is provided in person. When these requirements are not met, plans may continue to offer supplemental telehealth benefits via remote access technologies and/or telemonitoring services, but must cover the cost of these benefits using rebates or supplemental premiums.
What additional steps have been proposed to expand Medicare coverage of telehealth?
Options to extend or make permanent many of the current flexibilities around Medicare coverage of telehealth have been the subject of a number of hearings in both the U.S. Senate and the House of Representatives. Bipartisan bills such as the Preserving Telehealth, Hospital, and Ambulances Act and the Telehealth Modernization Act of 2024 include provisions that would temporarily extend the current flexibilities through December 2026. However, outside of select changes, such as permanently allowing FQHCs and RHCs to provide non-behavioral telehealth services, neither bill provides for a permanent expansion of Medicare telehealth coverage.
The Biden-Harris Administration has announced additional measures to preserve telehealth access for Medicare beneficiaries, such as a grant program to support the development of an interstate licensure compact that would make it easier for licensed social workers to practice across state lines, and provisions in a recent CMS proposed rule that would permanently extend certain telehealth flexibilities, such as coverage of audio-only services that meet all other conditions for Medicare telehealth coverage. However, in the absence of Congressional action, implementation of these provisions will be limited to the types of providers, services, and settings where telehealth was permitted before the current flexibilities were put in place (with the exception of behavioral health flexibilities, which have been made permanent).
Related to licensure, Medicare providers are generally required to be licensed in any state where they are practicing, and this requirement extends to telehealth. In most cases, a distant site telehealth provider must be licensed in the state where the beneficiary receiving services is located when the telehealth visit takes place. However, certain states have taken action to develop multi-state licensure compacts, which has allowed for additional flexibility related to licensure in participating states. These compacts are formed when states agree upon a uniform standard of care and enact state laws which allow qualified providers to practice across state lines while maintaining a single license or to maintain multiple licenses or which expedite the process of gaining additional licensure across member states. These compacts may be continued beyond December 2024, though other restrictions may limit their use if the current flexibilities are allowed to expire.
What are the implications of telehealth for Medicare program integrity?
As policymakers weigh whether to extend or make permanent current flexibilities around Medicare coverage of telehealth, several questions have been raised about the impact of telehealth services on patient care quality and program spending, as well as the potential for fraud and overuse.
Since the current flexibilities were introduced, state and federal agencies have filed several lawsuits regarding the submission of fraudulent claims by telehealth companies to Medicare and other insurers. However, investigations by the HHS Office of the Inspector General (OIG) into provider billing patterns during the first year of the COVID-19 pandemic found that just 0.2% of providers who billed for a telehealth service during the period engaged in excessive billing patterns that posed a high risk to the Medicare program, and clinicians generally complied with Medicare requirements when providing Evaluation and Management services through telehealth, suggesting little evidence of widespread misuse to date. MedPAC has recommended that CMS take certain precautions if the current telehealth flexibilities are extended, such as applying additional scrutiny to “outlier” clinicians who deliver more telehealth services than others and requiring in-person visits before high-cost tests and medical equipment are paid for.
What is the expected impact of telehealth use on Medicare spending and the estimated cost of expanding coverage?
Expanding telehealth coverage is expected to lead to an increase in Medicare spending, but the overall magnitude in the long term is uncertain. Some telehealth services may replace in-person care, as in the case of behavioral health visits, but easier access to telehealth may also lead to an overall increase in use of services and higher costs. Prior research has found modest increases in clinical encounters and spending per person among Medicare beneficiaries in geographic areas and health systems with higher rates of telehealth use. At the same time, there is evidence to suggest that beneficiaries with greater access to telehealth services may have fewer emergency department visits and improved adherence to certain medications. Additional research would help policymakers and other interested parties determine whether any increases in Medicare spending as a result of expanded telehealth coverage are offset by improvements in quality of care or decreases in other costs, such as spending on preventable hospital admissions and other types of acute care services.
As policymakers weigh the implications of legislation to maintain or broaden Medicare coverage of telehealth, a key consideration is how to set payment rates for telehealth services across different care settings and provider types. Payment parity between in-person and telehealth services may encourage providers to invest more time and resources into telehealth, but some have raised questions about how to ensure that this investment does not come at the expense of patient care quality or access to in-person services for beneficiaries who prefer them. MedPAC has recommended that CMS return to paying the lower facility rate for most telehealth services, including those furnished by FQHCs and RHCs, and collect data on practice costs in order to adjust telehealth payment rates in the future. Where policymakers end up on these issues would likely affect the overall cost of extending or making permanent Medicare coverage of telehealth beyond 2024.
While the implications of the election on the future of abortion access have received extensive attention, the stakes are also high for the future directions of Medicaid, a program that seven in ten women have a connection to. Vice President Harris and former President Trump hold vastly different views on abortion and Medicaid, key issues affecting women’s health, particularly for women in their reproductive years and with lower incomes. With regard to Medicaid, the Biden-Harris Administration policy proposals have generally focused on efforts to “protect and strengthen Medicaid and the Affordable Care Act (ACA)”, as well as repealing the Hyde Amendment, which limits federal spending on abortion; in contrast, Former President Trump supported plans to repeal or weaken the ACA, cap and reduce Medicaid financing, and restrict Medicaid eligibility while he was president. In a recent column, KFF President and CEO Drew Altman pointed out that Medicaid is the program most likely to be in the crosshairs if Republicans take control this November is Medicaid.
Changes related to Medicaid could have major consequences for health coverage of women with low incomes as well as pregnancy, postpartum and other reproductive health care for women. Here are the top five things to know about women and Medicaid ahead of the election.
Medicaid is a major source of coverage for women with low incomes (and their children). Medicaid provides coverage to one in five non-elderly adult women, the largest source of coverage after employer coverage (Figure 1). Medicaid covers 43 percent of non-elderly women with low incomes (income below 200% FPL) and over half (52%) of poor women (income below 100% FPL). Medicaid also covers four in ten children and eight in ten poor children..
Medicaid provides coverage to women across the lifespan, including women who are older and those with chronic disabilities. Medicaid provides coverage to women with low incomes who qualify because they meet one of the eligibility categories (pregnancy, parent, disability, or age 65+), or have income less than 138% of poverty through the ACA expansion pathway. Nearly two-thirds (64%) of adult women who are covered by Medicaid are of child-bearing age. Medicaid also covers over four in ten (44%) nonelderly women with a broad range of physical and mental disabilities, including physical impairments and severe mental illnesses. Medicaid finances over half (54%) of all long-term care spending, which is critical for many frail elderly women and women who qualify on the basis of disability. In 2021, 20% of women with Medicare were also enrolled in Medicaid. For these women, Medicaid helps to pay Medicare premiums, deductibles and cost-sharing as well as pay for services not typically covered by Medicare such as long-term care..
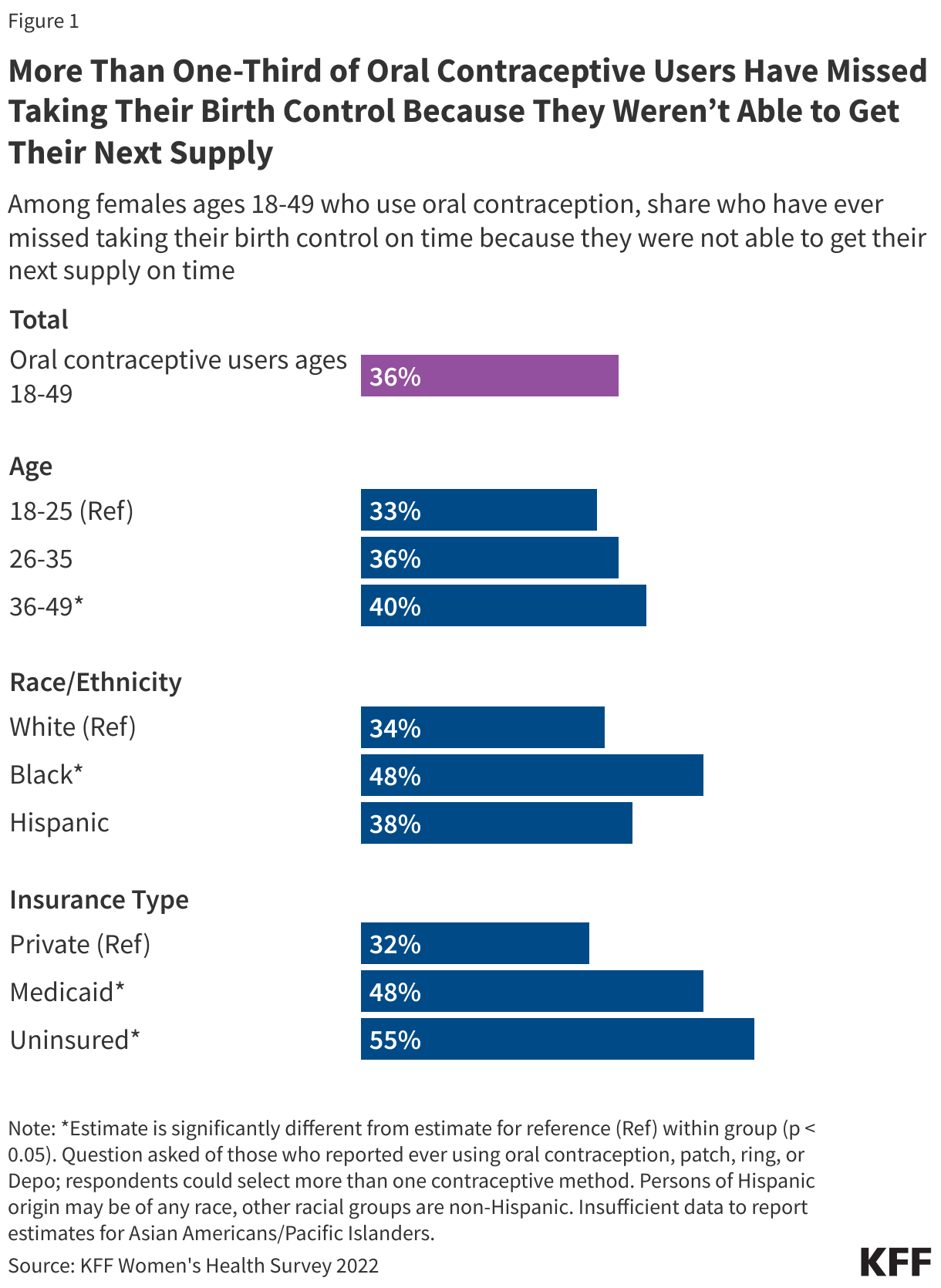
Medicaid is a key source of coverage for pregnant and postpartum women and births as well as access to family planning and preventive services. Medicaid covers over 4 in 10 births nationally and the majority of births in many states. Medicaid has also been used as a lever to help address disparities in access and outcomes in maternal and infant health. KFF research has found that the ACA’s Medicaid expansion promotes continuity of coverage in both the prenatal and postpartum periods. Furthermore, as a result of a provision in the American Rescue Plan Act of 2021, nearly all states now allow pregnancy-related coverage to continue through one year postpartum. Over half of the states have established programs that use Medicaid funds to cover the costs of family planning services for low-income women who remain uninsured and Medicaid accounts for 75% of all publicly funded family planning. Most states have limited scope Medicaid programs to pay for breast and cervical cancer treatment for certain low-income uninsured women..
Medicaid provides very limited access to abortion services. The federal Hyde Amendment prohibits federal spending on abortions, except when the pregnancy is a result of rape or incest, or when it jeopardizes the life of the pregnant person. However, states may use their own unmatched funds to pay for abortions for Medicaid enrollees in other circumstances and 19 states currently do so..
Medicaid has broad support and the majority of enrollees prefer to keep it as it is today. The public’s views of Medicaid are also largely positive. KFF public opinion polling shows Medicaid has broad support across political parties, with majorities of Democrats, independents, and Republicans expressing a favorable view of the program. In addition, the majority of the public and Medicaid enrollees prefer to keep Medicaid as it is today, with the federal government guaranteeing coverage for low-income people, setting standards for who states cover and what benefits people get, and matching state Medicaid spending as the number of people on the program goes up or down. Seven in ten women have a personal connection to Medicaid (including health insurance, pregnancy-related care, home health care, or nursing home care, coverage for a child, or to help pay for Medicare premiums for themselves, a family member or close friend). Eight in ten adult women (79%) have a favorable opinion of the program (Figure 5)..
Major outbreaks of mpox – the infectious disease previously called monkeypox – are ongoing in a number of African countries, in particular the Democratic Republic of the Congo (DRC). In addition, several mpox cases linked to the DRC outbreak have now been identified in some non-African countries, including Sweden and Thailand. Due to these circumstances, in mid-August 2024, the World Health Organization (WHO) and the Africa Centres for Disease Control and Prevention (Africa CDC) each declared mpox to be a public health emergency requiring a globally coordinated response.
This is the second time mpox has been declared an international emergency, with the first spanning 2022-2023. The current mpox outbreak centered in the DRC is being driven by the “clade I” strain of the virus, with a clade Ia variant that is primarily affecting children and a more recently identified clade Ib variant that is spreading primarily via sexual contact among adults. The previous international emergency was driven by a “clade II” strain, and primarily affected adult gay and bisexual men. Currently, there is ongoing transmission of both clades affecting mostly different geographic areas.
The U.S. government has provided technical and financial assistance for mpox response in DRC and elsewhere for years. Following the emergency declarations it has increased this support, including by delivering 50,000 doses of mpox vaccine to the DRC and 10,000 doses to Nigeria, as well as providing $10 million in mpox response-specific funding. On September 24, President Biden also pledged to donate up to 1 million more vaccine doses and an additional $500 million in funding to support mpox response across Africa.
Since the emergency declarations, the Africa CDC, WHO, and governments of affected countries have accelerated efforts to respond to the situation by developing updated response plans, mobilizing more funds and attention from policymakers, and working to obtain more mpox vaccine doses. Still, the response faces a number of challenges including an uncertain path to delivering mpox vaccines at scale, lack of access to prevention tools, poor health infrastructure in many affected areas along with ongoing conflicts and instability, and high levels of distrust and misinformation in affected communities.
No cases of clade I mpox have been identified in the U.S. as of September 26, 2024, and the CDC estimates the risk to the general public in the U.S. from the current outbreak in African countries is very low. However, clade II mpox infections continue to occur in the U.S. primarily among adult gay and bisexual men, though case numbers have declined since the previous mpox emergency in 2022-2023.
Introduction
Major outbreaks of mpox are again raising significant international concern. The DRC in particular has reported a large increase in cases driven by the “clade I” strain of the mpox virus, including a “clade Ia” variant that is primarily affecting children and a more recently identified “clade Ib variant” that is spreading primarily via sexual contact among adults. Clade I cases are also being reported in some other African nations, and several cases of the clade Ib variant have now been identified in non-African countries. At the same time, there continue to be mpox cases caused by “clade II” mpox, which was the variant that led to an earlier public health emergency in 2022-2023 in many different regions and countries around the world, including in the U.S. The recent circumstances led to two public health emergency declarations: the Africa Centres for Disease Control and Prevention (Africa CDC) declared mpox to be a “public health emergency of continental security” (PHECS) for Africa on August 13, 2024, and the WHO Director-General declared the mpox outbreaks a “public health emergency of international concern” (PHEIC) on August 14, 2024.
This explainer answers key questions about the international response to date, including the U.S. government’s role globally, and identifies issues and challenges that may affect the response going forward. It also discusses how the global emergency might affect the U.S. and the current status of mpox circulation within the U.S. It will be updated as needed.
Key Questions
What is mpox?
Mpox is a disease caused through infection with the mpox virus (MPXV). The first human case of mpox was identified in 1970, and since then, the virus has caused intermittent outbreaks. It is considered endemic in several Central, East, and West African countries, where infections have traditionally occurred through exposure to rodents or other animals carrying the virus. Human-to-human spread is also possible, primarily through close contact such as skin-to-skin contact and sexual or other contact with infected body fluids. Mpox can also pass from mother to fetus during pregnancy and during or after birth. Mpox infections can lead to symptoms such as fever, headaches, and body aches, and the development of a rash with lesions. Some infections can cause severe illness and even death, and there is a higher risk for severe outcomes in those with weaker immune systems such as people with HIV who are not virally suppressed and children. In areas with poor health care infrastructure and a lack of access to prevention tools, testing, treatment, and supportive care, mpox can be more difficult to identify, treat, and contain.
In recent years, more sustained human-to-human transmission and larger mpox outbreaks have been recorded from two genetic families of mpox virus (known as clade I and clade II mpox viruses; see Box 1). Most notably, in 2022, an outbreak of clade II mpox virus emerged from West Africa and spread globally, eventually affecting more than 100 countries and causing over 100,000 reported cases, including over 30,000 cases in the U.S. alone. That global outbreak was declared a PHEIC by WHO between July 2022 and May 2023 , and also declared a public health emergency in the U.S. in August 2022, marking the first time mpox had become a significant public health threat in non-endemic countries. Adult gay and bisexual men, especially men of color, made up the vast majority of cases during that outbreak in the U.S.
Strains of mpox virus (MPXV) from both clades have continued to circulate in largely geographically separate sets of endemic African countries, with clade II mpox infections primarily found in West African and Southern African countries and clade I infections found in Central African countries, the DRC in particular. In addition, clade II infections continue to be identified in many countries outside endemic regions, including in the U.S., primarily in gay and bisexual men, though the number of reported cases has declined significantly since the 2022 global outbreak.
Box 1: Epidemiology of Mpox Virus (MPXV) Clades I and II
There are two main genetic families of MPXV, known as clade I and clade II, and each clade is divided into sub-clades (clade Ia, clade Ib, clade IIa, and clade IIb) based on genetic similarities and differences.
Historically, clade I MPXV infections have been identified primarily in Central African countries, the DRC in particular, while clade II MPXV infections have been identified primarily in West African countries. In 2022, clade II MPXV emerged from West Africa to cause a global outbreak, primarily spread via sexual contact among adult gay and bisexual men. While that outbreak subsided following its 2022 peak, new cases of clade II MPXV infection continue to be reported in a number of countries worldwide, including African countries and the U.S.
In recent years, clade Ia and clade Ib MPXV have been circulating concurrently in the DRC and in Africa, and some clade Ib infections have also been identified outside of Africa:
Clade Ia MPXV: Infections continue to occur mostly in central DRC, affecting children exposed to infected animals with some additional ongoing human-to-human transmission due to close contact among family members or caregivers.
Clade Ib MPXV: Firstdescribed in 2023; infections have been found primarily in eastern DRC and neighboring African countries. This includes several countries reporting mpox cases for the first time ever, such as Burundi, Kenya, Rwanda, and Uganda. In areas affected by clade Ib, the majority of cases have occurred in adults and transmission appears to be sustained “largely, but not exclusively, through transmission linked to sexual contact and amplified in networks associated with commercial sex and sex workers.”
Available data suggest clade Ia MPXV infections are more likely to be severe cases and cause deaths than infections from clade IIa or clade IIb MPXV. While there is limited data on the severity of clade Ib, early indications are that it may not be as severe as clade Ia. Still, more data and studies are needed to fully understand the extent of biological and epidemiological differences across mpox sub-clades.
Why has mpox again been declared a public health emergency this year?
WHO and Africa CDC issued the emergency declarations due to the recent rapid rise in case numbers and expanded geographic reach of mpox. Of primary concern has been mpox in the DRC. In 2023, the DRC reported more than 14,000 suspected cases (three times as many as in 2022) and over 500 deaths from mpox. In 2024, these trends have accelerated, and in only the first half of this year, the country has reported over 14,000 suspected cases across 23 different provinces, with over 450 deaths. Children have been heavily affected in the DRC outbreaks, with an estimated 70% of mpox cases and 85% of mpox deaths in the country since 2022 occurring in children under 15.
Moreover, the emergence and rapid spread of a new strain of the mpox virus (known as clade Ib; see Box 1) that “appears to be spreading mainly through sexual networks” was first identified in eastern DRC in 2023 has not only caused a growing number of cases in the DRC, it has been found in a number of other countries in the region and outside Africa with one case detected in Sweden and one in Thailand. There are concerns that clade Ib virus may be more readily transmissible (including via sexual contact) compared to clade Ia, which could be contributing to the increased numbers of cases and the cross-border spread of the disease.
What has been the global response to the current mpox emergency?
Alongside its PHEIC declaration on August 14, WHO released $1.45 million from its Contingency Fund for Emergencies to help scale up the response in affected countries. On August 26, WHO issued a Global Mpox Strategic Preparedness and Response Plan (SPRP) that outlined a set of global, regional, and country level response steps and needs to address the spread of clade Ib in eastern DRC and to control outbreaks of clades I and II in the DRC and other African countries. The plan emphasized the need for better mpox surveillance, strengthening clinical care for the disease, more global cooperation to increase vaccine access, implementation of strategic vaccination efforts in populations at highest risk, and public health communication efforts and community empowerment.
Along with its declaration on August 13, Africa CDC requested $20 million for immediate mpox response needs (and reported it had been granted $10.4 million) from the African Union, and initially requested an additional $16 million from WHO and other international partners for a continent-wide response. The Africa CDC and WHO also launched a joint plan, the Mpox Continental Preparedness and Response Plan for Africa, covering the September 2024 through February 2025 period identifying the following:
10 “pillars” for the continental response including coordination and leadership, case management, vaccination, and logistics and financing;
roles and responsibilities for the primary international organizations involved in the response, including Africa CDC, WHO, Gavi, the Vaccine Alliance, and UNICEF;
the need for approximately $600 million to address the outbreak on the continent during the plan period (with 55% to be allocated to the mpox response in 14 affected countries and to boost readiness in 15 other countries at risk and 45% to be allocated to operational and technical support through partners), calling on donor governments, philanthropic organizations, and the private sector to provide this funding. Recent pledges from the U.S. and other donors totalled
In addition, Africa CDC activated its Public Health Emergency Operations Centre (PHEOC), initiated negotiations with pharmaceutical manufacturers and others to obtain mpox vaccines for use in outbreak response on the continent (see Box 2 for more on mpox vaccines), began supporting laboratory testing capacity building for mpox, and deployed epidemiologists to affected areas, among other activities.
Are mpox vaccines available, and are they getting to affected countries quickly?
There are several vaccines that can be used to prevent mpox (see Box 2). Africa CDC and WHO consider vaccines to be a key prevention tool for the response, and the joint Africa CDC and WHO continental response plan calls for enough vaccine doses to vaccinate 10 million people in African countries from September 2024 through February 2025. However, there are a limited number of vaccine doses available other than those already stockpiled by high-income countries.
Some high-income countries have agreed to donate vaccine doses from their existing stockpiles in support of the global response. For example, the European Commission announced a donation of 175,000 doses to Africa CDC, and Japan agreed to donate up to 3.5 million doses for response in the DRC. The U.S. has pledged to provide 1 million doses for the response, and has already delivered 50,000 doses to the DRC and 10,000 doses to Nigeria (see more on the U.S. role in mpox response below). In addition, Bavarian Nordic, the company that manufactures one of the mpox vaccines, pledged to donate 40,000 of the doses it has on hand to the DRC and to ramp up production of more doses for use in African countries in the coming months. Taken together, donors have pledged to provide a total of over 5.4 million doses of mpox vaccine for this response, according to WHO.
UNICEF and Gavi are also assisting in the process of acquiring vaccine doses and implementing vaccination in affected areas. Gavi announced it would redirect $2.9 million in funding to support mpox vaccinations in the DRC, and also is talking with vaccine manufacturers to help purchase doses directly, using funds drawn from its First Response Fund. Gavi is also helping coordinate the delivery of donated vaccines to countries in need. UNICEF reports that it is providing vaccination supplies and logistics support, health worker trainings, transportation, storage, and vaccine administration in the country.
As of September 24, 2024, 250,000 doses – 200,000 doses from the European Commission and Bavarian Nordic, along with the 50,000 doses from the U.S. – have arrived in the DRC. However, this is just a small fraction of the over 3 million doses that health authorities say are needed in the country in the near term. The DRC government announced it expects mpox vaccinations to begin in the country in the first week of October.
In other nearby countries reporting recent clade I mpox cases (such as Burundi, Rwanda, and Uganda), there is little information so far about if mpox vaccines will be provided in-country and when vaccinations may begin.
Box 2: Mpox vaccines and the international response
There are three vaccines, initially developed for smallpox prevention, that are considered effective in preventing mpox infection:
MVA-BN: Also known under the brand names Jynneos, Imvamune, and Imvanex, it is manufactured by Bavarian Nordic in Denmark and licensed by a number of countries for use in adults for the prevention of mpox.1 The MVA-BN vaccine is administered in a two-dose series.
ACAM2000: Manufactured by Emergent in the U.S., it has been made available for mpox prevention in adults under expanded access by the FDA in the U.S. The ACAM2000 vaccine is administered as a single dose.
LC16m8: Manufactured by KM Biologics in Japan, it has been licensed by Japan for smallpox prevention in children and adults and authorized by Japan for use against mpox since 2022. The LC16m8 vaccine is administered as a single dose.
Africa CDC has primarily focused on acquiring MVA-BN and LC16m8 doses for African countries, and estimates that enough doses to vaccinate 10 million people on the continent are needed.1 In the U.S., a 2022emergency use authorization issued by the FDA allows for the use of MVA-BN (JYNNEOS) vaccine in children and adolescents under some circumstances. WHO representatives have stated that the same vaccine could be used “off label” to vaccinate children and adolescents on the African continent during the current emergency response.
What assistance has the U.S. provided to the DRC for mpox response?
The U.S. government has long provided support to help DRC address mpox. For example, CDC has supported mpox research and response efforts in country for decades. Over the last few years, U.S. support for mpox response has included efforts to build laboratory testing capacity in-country, conduct mpox vaccine research, and training health care workers.
With the growth in mpox cases in the DRC and the emergency declarations from Africa CDC and WHO, the U.S. government has announced a number of additional actions. This includes a U.S. commitment to provide over $55 million in emergency health assistance through USAID and the U.S. CDC for mpox response in DRC and other affected countries in Africa, including $10 million in additional funding announced in August specifically for clade I mpox response efforts. Also, the U.S. donated 10,000 doses of mpox vaccine to Nigeria in August and delivered 50,000 doses of mpox vaccine to the DRC in September, along with additional support for vaccine delivery.
On September 24, President Biden stated the U.S. would increase its support over the coming months, and expects to provide over $500 million in additional assistance for the mpox response in African countries as well as donate as many as 1 million mpox vaccines in support of the response.
Besides its mpox-specific support, the U.S. government has also long provided significant amounts of global health and humanitarian assistance to the country, and recently stated it would be expanding assistance for broad humanitarian efforts in the DRC.
What are key challenges in responding to the current mpox emergency?
Addressing the current mpox emergency in the DRC and other affected countries in Africa poses a number of challenges, including:
Limited testing, surveillance, and epidemiological capacity. There is a lack of point of care testing and laboratory capacity in many affected areas, which means many suspected cases of mpox may be undiagnosed and suspected cases unconfirmed. This is particularly true in regard to genomic sequencing. This hampers epidemiological investigations and leaves many questions unanswered about the current state of mpox in the DRC and elsewhere. More testing and epidemiological information on modes of disease transmission, risk factors, and disease severity associated with the different MPXV clades, as well as outcomes of pregnancy in women infected with different MPXV clades, would help authorities target response efforts.
Difficulties with obtaining and distributing mpox vaccines at scale. There is currently a limited global supply of mpox vaccines, with many of the existing doses found only in national stockpiles of high-income countries so the response relies in large part on donations. Also, there is a lack of formal authorization to use these vaccines in a number of the affected countries in Africa and little data on the effectiveness of these vaccines against clade I mpox or their effectiveness in children. A new, large-scale vaccination campaign to reach the populations at greatest risk for mpox is also a challenge.
Stigma and overlapping risks of mpox and HIV infection. There are relatively high rates of HIV infection in some mpox-affected countries in Africa, which raises concerns about the potential overlap in risks between these infectious diseases. Unsuppressed HIV infection could raise the risk for mpox transmission, especially in the context of sexual contact, and for development of more severe outcomes from mpox infection. In addition, both infections can lead to stigma for those affected, making the response more challenging. Therefore, ensuring public health authorities plan to address HIV and mpox in a coordinated fashion will be important.
Health systems and health care workforce. Lack of access to health care and a limited health care workforce increase risks from mpox for individuals and communities. Linking mpox cases to health care services as early as possible and ensuring the health care workforce is adequately trained and supplied to address mpox improves outcomes.
Travel restrictions. To date, countries have not put into place harsh restrictions on travel to and from areas affected by this mpox emergency. However, if the outbreak worsens and spreads to more countries, there is the potential for countries to impose travel bans or other restrictions, as has occurred during past outbreaks. There is little evidence to support the effectiveness of such restrictions in interrupting international transmission of mpox.
Competing priorities amid instability, conflict, and community distrust. Many of the affected countries – the DRC in particular – face multiple simultaneous humanitarian crises, health emergencies, and other urgent issues in addition to mpox. This makes focusing attention on and implementing a response to mpox more challenging, especially in the context of limited resources. For example, in some affected areas in the DRC, there is a history of instability and conflict and an ongoing lack of trust in authorities in many communities, which complicates response and risk communication efforts particularly those focused on reaching the most at-risk populations.
How might this latest outbreak affect people in the U.S.?
Although cases of mpox due to clade II infections continue to occur in the U.S. (see below), so far no cases of mpox due to clade I infections – the genetic family linked to the current DRC outbreak – have been identified in the U.S. The U.S. CDC estimates that the risk to the general public from the current mpox outbreak in African countries remains very low. The CDC also estimates there is a low to moderate risk from the current DRC-based clade I outbreak for U.S. gay, bisexual and other men who have sex with men (MSM) who have more than one sexual partner as well as for people who have sex with MSM, regardless of gender, particularly if there is a history of travel to any of the African countries affected in the current mpox emergency.
In light of the evolving mpox situation in parts of Africa and the potential risk of imported cases, CDC has issued a travel warning for the DRC and has issued severalhealth alerts for U.S. clinicians, which provide guidance on prevention strategies and also suggest a “heightened index of suspicion” for mpox in patients recently arriving from affected areas in Africa who demonstrate signs and symptoms consistent with the disease.
Given the rise in anti-immigrant rhetoric and a history of charged debates about travelers entering the U.S. during health emergencies, there is the potential for mpox to become politicized this election year, especially if cases linked to the ongoing outbreaks in Africa are eventually identified in the U.S.
What is the status of ongoing mpox circulation in the U.S.?
As mentioned above, in 2022-2023, the U.S. had over 30,000 mpox cases during the global outbreak of clade II mpox, which had initially emerged from West African countries. While case numbers have declined in the U.S. since 2022, some clade II mpox cases continue to be identified, with CDC reporting 1,968 mpox (clade II) cases so far this year nationwide as of September 1, 2024. These cases have primarily occurred among adult gay, bisexual and other men who have sex with men (MSM) who have multiple sexual partners, especially men of color and with people with HIV being disproportionately impacted. According to CDC, during the peak of the epidemic in 2022 over 99% of mpox clade II cases in the U.S. occurred among men, and of those, 94% were among men who had sexual contact with other men.
The 2024 election is the first Presidential election since the Supreme Court’s ruling in Dobbs v. Jackson Women’s Health Organization, and abortion access and reproductive health more broadly, are front and center in this election (Figure 1). The two candidates, Vice President Kamala Harris (D) and former President Donald Trump (R) have widely different positions on reproductive health. Vice President Harris has been and is an outspoken leader and advocate for reproductive freedom, while former President Trump celebrates the overturning of Roe v Wade, which ended the constitutional right to abortion and allowed states to completely ban or severely restrict abortion access. The candidates’ Vice-Presidential running mates, Governor Tim Walz (D) and Senator JD Vance (R) also have divergent records on reproductive health issues. Governor Walz points to his support for Minnesota’s Protect Reproductive Freedom Act, which codified abortion rights in the state, as well as his family’s own experience with fertility care. Senator Vance has expressed support for a national abortion ban via the Comstock Act and voted against a Senate bill that would have established a national right to IVF, a position that his running mate, Donald Trump, has said he supports.
While abortion is the most prominent health care campaign issue, the election could also have large implications for contraceptive care and maternal health. This brief summarizes the positions, records, and potential priorities of the two major party candidates for the 2024 Presidential election on three major issues in women’s health policy – abortion, contraception, and maternal health. The information presented is derived from the candidates’ records from their time as elected officials, their proposals or statements, and the Democratic and Republican party platforms. We have also included discussion of proposals from the Heritage Foundation’s Project 2025. While former President Trump has distanced himself from this proposal, its authors are influential in Republican circles and include several individuals who served in the Trump Administration. A separate side-by-side from KFF compares the candidates’ positions across a broad range of health care issues.
Abortion
Abortion access is one of the most prominent issues in the 2024 election, and the candidates have widely divergent records and positions. Vice President Harris has been an outspoken advocate for reproductive freedom and has endorsed the restoration of the prior federal standard under Roe v. Wade, which would guarantee a right to abortion until the point of fetal viability. In contrast, Trump expresses his support for letting states set their own abortion policy, including banning abortion, as allowed under the Dobbs Supreme Court ruling.
Vice President Harris has been vocal in her disagreement with the Supreme Court’s 2022 decision in Dobbs v. Jackson Women’s Health Organization, which overturned Roe v. Wade and allowed states to set their own policy on abortion legality. In stark contrast, Trump has repeatedly taken credit for the overturning of Roe and giving states decision-making authority on abortion because he appointed three conservative justices to the Supreme Court with the explicit goal of overturning Roe. Since the Dobbs ruling, 14 states have banned abortion with very few exceptions and several other states have limited abortion availability to very early in pregnancy.
Abortion Access
Vice President Harris has been the leading voice for the Biden/Harris Administration on reproductive health and has said she supports restoring the protections of Roe v. Wade and eliminating the filibuster to do so. In the wake of the Dobbs ruling, the Biden-Harris administration has tried to limit the impact of the bans through executive actions as well as in the courts. This includes reiterating federal protections for abortion care under EMTALA in cases of pregnancy-related emergencies, reinforcing requirements for pharmacies to fulfill their obligation to provide access to reproductive health pharmaceuticals, enforcement of non-discrimination policies for health care providers, promulgating policies to strengthen data privacy to protect those seeking reproductive health care, and defending the FDA decision to approve mifepristone (one of the drugs used in the medication abortion regimen) and changes in how the drug can be dispensed. Vice President Harris opposes the Hyde Amendment, which limits federal spending on abortions to cases of rape, incest, or life of the pregnant person.
In 2016, Trump ran on the promise that he would appoint Supreme Court judges that would overturn Roe v. Wade, a promise he kept. Most recently, he has stated that he believes that abortion regulation should be left up to states and tweeted that he would veto a federal ban. At times earlier in the campaign he has suggested that he would support some type of federal standard, such as 15 or 16 weeks gestation, that would apply in all states. He has said that he believes in exceptions for cases of rape, incest, and life of the mother. Despite stating that he believes that abortion bans or limits at 6 weeks are “too early,” he also said he will vote against the ballot initiative that would expand abortion legality in Florida, where he resides (currently limited to six weeks of pregnancy). In terms of penalties for violation of bans or gestational limits, he has said that they should be also decided by states, even leaving open the possibility of allowing states to prosecute people in states with bans if they obtain abortions.
Trump has repeatedly stated that Democrats support abortion up to and after birth, which is false. There are no abortions at birth or after. During the 2016 campaign, he pledged to make the Hyde Amendment abortion funding ban a permanent law.
Medication Abortion
Medication abortion pills account for the majority of abortions in the U.S. The Biden-Harris Administration has implemented policies that expand access to medication abortion, particularly via telehealth, and has been fighting lawsuits brought by anti-choice clinicians and policymakers to further restrict abortion access. Former President Trump’s statements about medication abortion have been inconsistent, at times suggesting he would not block their availability and at other times suggesting the opposite. His support for leaving abortion policy to the states allows states to prohibit access to all abortions, including medication abortion. Project 2025—the detailed conservative policy treatise that was spearheaded by many former Trump Administration leaders—is clear in its opposition to the FDA’s approval of mifepristone and endorses the Comstock Act, which would effectively prohibit the mailing and distribution of abortion pills.
The Comstock Act is an existing 1873 anti-vice law banning the mailing of obscene matter and articles used to produce abortion. The Biden-Harris Administration’s Department of Justice maintains that the Comstock Act should not be interpreted literally and therefore has not enforced it. Based on over a century of Federal Court rulings, they determined the Comstock Act only applies when the sender intends for the material or drug to be used for an illegal abortion, and there are legal uses of abortion drugs in every state and no way to determine the intent of the sender. However, that would not preclude an Administration that is hostile to abortion from doing so. Former President Trump has not articulated his stance on enforcement of the Comstock Act, but some Republican leaders, including his running mate Senator Vance, have called for enforcement of the law and a halt on the mailing of all abortion medications and supplies within the country (which would be a de facto national ban) and even limiting access in states that currently allow abortion without restrictions.
Pregnancy-Related Emergency Care
Health exceptions to abortion bans is an issue that Vice President Harris has spoken about extensively. In addition to reiterating the federal EMTALA requirements for hospitals to provide health-stabilizing emergency care that includes abortion in cases of pregnancy-related emergencies, the Biden-Harris administration defended their policy in a case that reached the Supreme Court. This challenge was spearheaded by Republican-led states that ban emergency abortion care, even when it is the standard of care to preserve or stabilize health. President Trump says he believes in exceptions for “life of the mother.” Project 2025 authors say that emergency abortion denials are not a problem and call for the reversal of the Biden-Harris Administration’s EMTALA guidance and withdrawal of lawsuits challenging state abortion bans without health exceptions.
Access to contraception has emerged as another health care issue in this year’s election where Vice President Harris and former President Trump have different records. Vice President Harris’ call for reproductive freedom includes access to contraception, and her support on this issue extends back to her time before she became Vice President. Since the Dobbs decision, the Biden-Harris Administration issued executive orders reiterating support for contraception and directing various federal agencies and regulators to assure that access to the full range of contraceptive services and supplies is safeguarded. Trump’s Administration issued multiple regulations that placed restrictions on the availability of funding for contraception. During his campaign, he initially expressed that states could restrict access to contraceptives, but shortly afterwards, also said that he would not support this.
Right to Contraceptives
Vice President Harris is a strong supporter of contraceptive care, including coverage of over-the-counter methods, encouraging broader access under Medicare and at colleges and universities, and for the proposed federal Right to Contraception Act, which is pending in Congress. Although Trump has not spoken extensively about contraception during this campaign, the Republican party platform states support for “access to birth control;” however, there is no detail on the policies that they would implement to promote access. The majority of the Republican members of Congress (including Senator Vance) either opposed or abstained from voting on the Right to Contraception Act. Project 2025 characterizes some emergency contraception pills—a contraceptive that prevents pregnancy after sex by preventing or delaying ovulation, as a “potential abortifacient.”
Title X Federal Family Planning Program
While in office, Trump’s Administration rewrote the rules governing the federal Title X program, the federal family planning program that supports contraceptive access for people with lower incomes. Title X funds have never been used to pay for abortion services, but Trump’s Administration rewrote the regulations to disqualify family planning clinics from participating in the program if they also offered abortion services (with separate funding); additionally, they prohibited participating clinics from offering referrals to abortion services at other clinics to pregnant patients seeking abortion information. These changes resulted in a reduction of about 1,300 of the 4,000 sites participating in the network of clinics receiving federal support from the Title X program. His Administration also provided federal family planning funding through Title X funds to clinics that did not provide contraceptive methods, which had been a requirement of the program until that time. The Biden-Harris Administration reversed the Trump Administration changes to the program. Project 2025 calls for the restoration of the Trump-era rules and focusing the program on fertility-awareness based methods (FABM).
Medicaid and Family Planning
For decades, the Medicaid program has required coverage for family planning services, including contraceptives. The Biden–Harris Administration has reiterated support for this policy as well as the program’s “free choice of provider” policy which commits to inclusion of all qualified providers (including Planned Parenthood) that offer both contraception and abortion services, although federal Medicaid funds are not used for abortion care. Former President Trump allowed federal Medicaid funds to be used in a Texas Medicaid program that excluded Planned Parenthood and did not cover the full range of contraceptives, excluding emergency contraception. Eliminating Planned Parenthood from Medicaid provider networks has long been a priority of some Republican lawmakers and conservative organizations and is reiterated by Project 2025.
Contraceptive Coverage and the ACA
Private insurance coverage for contraceptives and other evidence-based preventive services such as cancer screenings and prenatal care is required under the ACA and has been championed and expanded by the Biden-Harris Administration. While President, Trump issued regulations that expanded facilitated employer claims to an exemption from the contraceptive coverage requirement, allowing employers with religious or moral objections to completely exclude contraceptives from their employee health plans.
The outcome of a pending federal lawsuit, Braidwood Management Inc v Becerra, which specifically challenges the ACA preventive services requirements, could put contraceptive coverage at risk. The Biden-Harris Administration is defending the ACA requirement and fighting the case. Former President Trump has not publicly voiced an opinion on the case, but Project 2025 calls for the federal government to issue new requirements for contraceptives and other women’s preventive services because of the pending case.
In recent years, there has been increased awareness and attention to the poor state of maternal health in the U.S., particularly stark racial and ethnic disparities in mortality and morbidity, as well as limited access and coverage for fertility assistance, particularly in vitro fertilization (IVF), under private insurance and Medicaid. While in the Senate and as Vice President, Harris has been a champion on improving maternal health, with a particular focus on eliminating persistent racial and ethnic disparities. Recently, has called for insurance coverage of IVF.
Equity, Quality, and Access to Care
Vice President Harris has a history of advocating for improvements in maternal health and care. As Senator, she sponsored the MOMNIBUS, a package of bills aimed at improving quality of and access to maternity care. After becoming Vice President, the American Rescue Plan Act (ARPA) of 2021, which the Administration supported, allowed states to extend postpartum coverage under Medicaid from 60 days to 12 months. Since it took effect, nearly all states have adopted the extension.
The Biden-Harris Administration has also taken other actions, including the launch of a maternal mental health hotline and a new Medicaid payment model for better coordinated maternity homes. Their Maternal Health Blueprint presents future priorities, such as coverage for a broader range of services, improving data collection, diversifying the maternity workforce (including with midwives and doulas), and improving treatment of pregnant people, particularly communities of color.
Trump also issued a maternal health plan near the end of his term that called for action on many of the same issues, including more research and technological investments in maternal health. The former President signed federal legislation that provided funding for maternal mortality review committees. The Project 2025 document supports broader access to doulas, as long as no federal funds support training related to abortion care.
Fertility Assistance and IVF
In February 2024, the Alabama Supreme Court ruled that embryos created through in vitro fertilization (IVF) are “unborn children” under the state’s law. Since the state court’s ruling, both Vice President Harris and former President Trump have expressed their support for IVF care. Trump has also said that if elected, his administration would provide access to full coverage of IVF services by requiring insurance companies or the government to pay, but he has not provided any details on how this would be funded or operationalized.
Both party platforms express support for IVF, however the Republican platform also invokes the 14th Amendment, which can be used to promote fetal personhood policies that could threaten and criminalize IVF care. Additionally, the Project 2025 authors refer to embryos as “aborted children” and oppose research using embryonic stem cells (which can be derived from the IVF process). Senators in both parties introduced federal legislation related to IVF. The Democratic-sponsored proposal would have established a federal right to IVF as well as other fertility assistance services, while the Republican-backed bill would have prohibited states from banning IVF care. Both bills failed to pass.
Paid Leave
Despite strongpublicsupport, the U.S. is one of the few industrialized nations that does not have national requirements for paid family leave for most workers. Vice President Harris supports guaranteeing 12 weeks of paid leave for new parents, caregivers, cases of domestic violence, or military deployment. The Republican Party platform does not address paid leave. During former President Trump’s time in office, he signed the 2020 National Defense Authorization Act, which provided 12 weeks paid parental leave to federal employees for the birth or arrival of a child.
National health spending totaled $4.5 trillion in 2022—17% of gross domestic product (GDP)—and is projected to grow faster than GDP through 2032, contributing to higher costs for families, employers, states, and the federal government. As policymakers consider a variety of strategies to make health care more affordable, they have been increasingly attentive to the effects of consolidation in health care markets and the potential implications for cost and quality of care. Hospital consolidation has been a subject of particular focus in part because nearly one third of all health spending goes towards hospital care. Consolidation may allow providers to operate more efficiently and help struggling providers keep their doors open in underserved areas, but often reduces competition. A substantial body of evidence has found that consolidation can contribute to higher prices, with unclear effects on quality.
This analysis examines the competitiveness of markets for hospital care, based on RAND Hospital Data—a cleaned and processed version of cost reports from Medicare-certified hospitals—and American Hospital Association (AHA) survey data. This piece describes competition among independent hospitals and health systems, referring to both as “health systems” throughout for brevity. Competition is measured in three ways: the share of metropolitan statistical areas (MSAs) controlled by a small number of health systems, the level of market concentration in MSAs based on the Herfindahl-Hirschman Index (HHI), and the share of hospitals affiliated with health systems over time. Using hospital data from 2022 (the most recent year available), this analysis focuses on general short-term or general medical or surgical hospitals depending on the dataset and excludes federal hospitals (see Methods for more details).
Key Takeaways
One or two health systems controlled the entire market for inpatient hospital care in nearly half (47%) of metropolitan areas in 2022.
In more than four of five metropolitan areas (82%), one or two health systems controlled more than 75 percent of the market.
Nearly all (97% of) metropolitan areas had highly concentrated markets for inpatient hospital care when applying HHI thresholds from antitrust guidelines to MSAs.
One or Two Health Systems Controlled the Entire Market for Inpatient Hospital Care in Nearly Half (47%) of Metropolitan Areas in 2022
Nearly one in five (19%) metropolitan statistical areas (MSAs) were controlled by a single health system, and more than one in four (27%) markets were controlled by two systems in 2022 (see Figure 1). In more than four of five metropolitan areas (82%), one or two health systems controlled more than 75 percent of the market. These markets all met the definition of highly concentrated markets based on thresholds in current antitrust guidelines (see below). One health system controlled at least half of the market in three out of four MSAs (75%) and at least a quarter of the market in nearly every MSA (98%).
The number of health systems in a given MSA tends to increase with the population of the region. For example, in 79% of MSAs with a population of less than 200,000, one or two health systems controlled the entire market for inpatient hospital care in 2022, as in the Muncie, IN; Napa, CA; and Amherst Town-Northampton, MA MSAs (Figure 2). MSAs with one or two health systems account for nearly half (47%) of all MSAs but 12% of the U.S. population living in metropolitan areas.
Conversely, virtually all (53 of 54) MSAs with a population of at least one million people had at least four health systems, as in the MSAs encompassing Detroit, Miami, and Phoenix. MSAs with four or more health systems accounted for 35% of all MSAs but 79% of the U.S. population living in metropolitan areas.
However, in nine of these relatively large MSAs with four or more health systems, the two largest health systems controlled at least 75% of the market, and in 37 of these areas, they controlled at least 50% of the market. For example, in the MSA encompassing Austin, TX, with 2.4 million residents, two systems (HCA Healthcare and Ascension Health) controlled 85% of the inpatient hospital care market, though Austin is home to more than four health systems. The metropolitan area encompassing Portland, OR, with 2.5 million residents and more than four health systems, is a less concentrated market than Austin’s, but the two largest systems (Legacy Health and Providence) still control a combined 56% of the market. (See Methods for discussion about MSAs as geographic hospital markets).
Nearly all (97% of) metropolitan areas had highly concentrated markets for inpatient hospital care in 2022 based on thresholds used in current antitrust guidelines
Another way to assess market competitiveness is to evaluate a measure of concentration known as the Herfindahl-Hirschman Index (HHI), which is based on the number of participants in a market and their respective shares. The measure runs from 0 (perfectly competitive) to 10,000 (monopoly market). Based on current merger guidelines from the Federal Trade Commission (FTC) and Department of Justice (DOJ), markets can be grouped into three categories: not concentrated (HHI < 1,000), moderately concentrated (1,000 – 1,800), and highly concentrated (HHI > 1,800). This analysis calculates HHIs for MSAs and groups these regions accordingly, though there are other ways of defining the boundaries of hospital markets (see Methods).
Nearly all (97% of) MSAs had highly concentrated markets for inpatient hospital care in 2022 based on thresholds used in current merger guidelines (Figure 3). These guidelines reflect updates in 2023 that lowered the HHI thresholds for moderately concentrated and highly concentrated markets. Based on the thresholds used in prior guidelines, a large majority but somewhat smaller share (93%) of MSAs were highly concentrated markets for inpatient hospital care in 2022, closer to an estimate from an earlier study (90%) that used data from 2016.
As was the case when looking at counts of health systems in MSAs, larger metropolitan areas tended to be less concentrated and more competitive than less populated metropolitan areas, although this was not always the case. All 13 MSAs that were identified as either not concentrated or moderately concentrated had more than one million residents, such as the MSAs encompassing Cincinnati, Oklahoma City, and Miami. However, 41 MSAs with more than one million residents—including the MSAs encompassing Houston, Denver, and Atlanta—had highly concentrated hospital markets. Overall, 70% of people living in metropolitan areas lived in highly concentrated hospital markets.
The share of hospitals affiliated with health systems increased from 56% in 2010 to 67% in 2022, with the share growing in both rural and nonrural areas
About two thirds of hospitals (67%) are now part of a larger system, an increase from 56% in 2010 (Figure 4). A smaller share of rural than nonrural hospitals were part of a health system in 2022 (52% versus 83%), though shares have increased over time for both rural and nonrural regions: from 43% in 2010 to 52% in 2022 among rural hospitals and from 69% in 2010 to 83% in 2022 among nonrural hospitals.
Most system-affiliated hospitals in 2022 (53%) were part of a system with at least 15 hospitals, and 22% were in a system with at least 50 hospitals. Systems with at least 100 hospitals accounted for 13% of system-affiliated hospitals.
Hospitals joining larger systems may not always reduce local market competition, for example, if an independent hospital is acquired by a larger system that does not own facilities in the same market. However, mergers between hospitals that operate in different geographic markets for patient care—also known as “cross-market” mergers—may nonetheless lead to higher prices in some cases.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Methods
Analyses of market shares and HHI (e.g., Figures 1 through 3) were based on RAND Hospital Data. RAND Hospital Data are a cleaned and processed version of annual cost reports that Medicare-certified hospitals are required to submit to the federal government. Although limited to Medicare-certified hospitals, in 2022, our analysis of RAND data included the vast majority (97%) of non-federal general medical and surgical hospitals in US metropolitan areas included in our analysis of the AHA Annual Survey Database (see below). Cost reports were assigned to years based on the end of the reporting period and were scaled up or down to reflect a 365-day period, as necessary.
Analyses of market shares and HHI were restricted to non-federal, general short-term hospitals. Market shares were calculated as the share of inpatient discharges in an MSA that occurred within a given health system or independent hospital. One percent of hospitals that met our other sample restrictions had missing values for inpatient discharges and were excluded. Hospitals were grouped into health systems, as applicable, based on the 2022 AHRQ Compendium of US Health Systems. MSAs reflect 2023 geographic definitions from the Census Bureau calculated based on data from the 2020 decennial census. HHIs were calculated as the sum of squared market shares for all health systems in a given MSA (e.g., an MSA divided evenly between two systems would have an HHI of 502 + 502 = 5,000). We obtained 2022 MSA population estimates from the Census Bureau.
We used MSAs as a proxy for hospital markets, which is one approach used by other studies summarizing hospital market competition across the country. There are other ways of defining markets that would yield different results when calculating the level of competition. For example, one relatively recent report also evaluated MSAs but focused on where residents received their care, including at hospitals outside of a given MSA. As another example, some have defined markets based on Hospital Referral Regions (HRRs) and USDA Commuting Zones. More precise market definitions, such as those used to define competition in antitrust cases, were not feasible. This study did not exclude MSAs with populations of at least three million as some others have done, because the analysis sought to describe competition across all metropolitan areas.
Analyses of the share of hospitals affiliated with systems are based on the AHA Annual Survey Database, which includes its own measure of system affiliation. We restricted this analysis to nonfederal, general medical and surgical hospitals. Hospitals were designated as rural if they were located in a ZIP code that is eligible for Rural Health Grants through the Federal Office of Rural Health Programs.
Nearly half (47%) of metropolitan areas across the country had only one or two hospitals or health systems providing general inpatient hospital care in 2022, a new KFF analysis finds.The analysis examines the extent of competition among hospitals amid a wave of hospital consolidation that has drawn the attention of state and federal regulators. About one in five (19%) metropolitan statistical areas have only one hospital or health system providing hospital care, and more than a quarter (27%) are controlled by two hospitals or systems. In a large majority of metro areas (82%), one or two hospitals or health systems were responsible for at least three quarters of all inpatient hospital discharges in their area, thereby meeting the definition for highly concentrated markets based on current federal antitrust guidelines.
The number of hospitals or health systems in a metro area tends to increase with the population of the region, with a large majority of smallest metro areas (less than 200,000 residents) having only one or two hospitals or health systems providing inpatient hospital care, while nearly all of the largest areas (at least one million people) having at least four hospitals or health systems.Other findings include:
Nearly all (97%) metropolitan areas had highly concentrated markets for inpatient hospital care in 2022 based on the Herfindahl-Hirschman Index, which takes into account the market shares of the participants in a given market. The Federal Trade Commission and Department of Justice include this measure of competitiveness in their current guidelines for evaluating mergers between hospitals or health systems
Two thirds (67%) of hospitals nationwide were affiliated with health systems in 2022, up from 56% in 2010. The rise in affiliated hospitals affected both rural and nonrural areas, though nearly half (48%) of hospitals in rural areas remain unaffiliated with larger health systems.
The share of individuals identifying as LGBTQ+ in the United States has increased over time, rising from just 4% in 2012 to 8% in 2023. In addition, support for same-sex marriage has also grown (27% in 1996 v. 69% as of 2024) and fewer believe there should be less acceptance for LGBTQ+ people (26% in 2001 v. 8% in 2020). Increases in identity and acceptance have been punctuated by several Supreme Court decisions providing new civil rights for LGBTQ+ people. Still, widespread stigma and discrimination persist for many LGBTQ+ people, including in health care as well as across a range of social institutions. These experiences can fuel significant health care disparities among LGBTQ+ people, challenging well-being and affecting health outcomes. Further, LGBTQ+ rights and health care access have become increasingly politicized at the federal and state levels, especially when it comes to young people.
All people’s health and health care experiences are informed by the socioeconomic context in which they live, including the policy environment. Federal and state policy can facilitate or impede access to health care for LGBTQ+ people. At the federal level, there have been both expansions as well as restrictions in protections and access, and pending legal cases may decide the extent to which protections remain. At the state level, there has been a rapid increase in the number of laws and policies impacting LGBTQ+ people’s health, especially, though not exclusively, that of young people. This chapter provides an overview of LGBTQ+ people’s identities, experiences with health and health care, and the related health policy landscape.
A Note on Language
Throughout this chapter, whenever possible, we use the term LGBTQ+ to represent the full spectrum of non-heterosexual, non-cisgender people. Additionally, people who are asexual, questioning, or intersex are sometimes included under the LGBTQ+ umbrella. However, at times, the reader may encounter differences in terminology (e.g., LGBT, LGB, etc.). In these circumstances, we use language to reflect the specific data being cited. It is important to note that the language used to describe LGBTQ+ people has evolved considerably over time and will likely continue to do so.
The concepts of sex, gender, and sexual orientation are discreet. However, they are often thought of as interrelated and dependent on one another, though their actual relationship is more diverse and complex:
Sex is often described as one’s biological categorization of being male or female based on anatomical, hormonal, and genetic factors. At birth, individuals are typically assigned a sex based on external genitalia. While sex is often thought of as a binary, as many as 1.7% of the population has been estimated to have some intersex trait, with population estimates of people with anatomical variations being lower (less than 0.5% of the population).
Gender identity is an individual’s sense or experience of being male, female, transgender (trans), non-binary, gender non-conforming, or something else. Gender identity may or may not align with the sex that was assigned at birth. Gender expression is the public expression of gender identity, which may occur through attire, body characteristics (e.g., hair), voice, etc. Gender expression may or may not align with traditional assumptions related to sex or gender identity.
Sexual orientation refers to emotional, romantic or sexual attraction to other people, often in relationship to one’s own sex and/or gender identity.
While many people and institutions historically considered these three concepts to be inseparably linked and linear (e.g., assigned the male sex at birth, identifies as male, and is attracted to women), there is wide variation in how these concepts relate, and they can be dynamic over time.
It is estimated that 7.6% of U.S. adults identify as LGBTQ+, as of 2023, more than double the share in 2012 (3.5%), and LGBTQ+ identity is expected to continue to increase over time. This increase may reflect changes in behavior and desire and an increased willingness to self-identify and disclose as societal acceptance has grown. Indeed, these two factors are likely interrelated. LGBTQ+ identity is strongly associated with age; younger generations self-identify at higher rates than older generations (one in five of those aged 18-26 identify as LGBTQ+ compared to just 1% among those aged 78 and older). In addition as of 2021, 1 in 4 high school students identifies as LGBTQ+. As the LGBTQ+ population ages and new generations identify at higher rates, it is expected that the share of adults who identify as LGBTQ+ will increase as well.
As such, the LGBTQ+ population is younger than the U.S. population overall. Almost half (47%) of LGBT adults are under age 30, compared to 18% of non-LGBT adults. Just 6% are 65 or older, compared to nearly one-quarter (24%) of non-LGBT adults (see Figure 1). LGBT adults are also more likely to have lower incomes and be living on less than $40,000 per year than non-LGBT adults (42% v. 33%), which may reflect their lower age. (See Table 1.)
Within the LGBTQ+ community, identity is complex and multifaceted. Among adults who identify as LGBTQ+, the majority identify as bisexual (57%), a finding driven by younger adults, followed by gay (18%), and lesbian (15%). Smaller shares identify as transgender (12%), pansexual (2%), or in some other way (3%).
It is estimated that 1.6 million people living in the U.S. identify as transgender or trans, which, as noted, translates to 12% of the LGBTQ+ population but less than 1% of all adults. A 2023 KFF/Washington Post Survey of a nationally representative sample of transgender adults in the U.S shows the trans adult population is younger than the larger cisgender adult population, with the majority of trans adults under the age of 35, echoing trends seen in the larger LGBTQ+ population. Additionally, most (70%) trans adults identify as lesbian, gay, or bisexual, compared to one in ten cisgender adults. Trans adults and cisgender adults do not notably differ when it comes to race and ethnicity or income. (See Table 2.)
Most trans adults, or about 6 in 10, describe themselves as “trans, gender non-conforming” or “trans, nonbinary,” while smaller shares say they would describe themselves as a “trans woman” (22%) or a “trans man” (12%). (See Figure 1.)
In addition to sexual orientation and gender identity, the lives of people who are LGBTQ+ are also shaped and informed by a range of other intersectional sociodemographic factors, including race/ethnicity, income, geography, educational opportunities, language, citizenship status, disability status, and other variables, which, together, affect health access and outcomes in both positive and negative ways.
Data Collection
Having an understanding of who the LGBTQ+ community is, what challenges they face, what their health needs are, and how those differ from non-LGBTQ+ people allows policymakers, providers, and others to meet the community’s needs better. While the share of people who identify as LGBTQ+ has increased over time, the community is still a relatively small share of the overall population (approximately 8%). This makes representative data collection more difficult, particularly for sub-group analysis, since obtaining a representative sample of a small population requires a relatively larger sample size, which can be both challenging to obtain and costly. In addition to methodological challenges, in many cases, researchers, systems, and surveys simply haven’t asked about sexual orientation and gender identity. While this is improving, including through efforts by the federal government, collecting data about sexual orientation and gender identity is still not routine in federal, state and local surveys, or in health systems, providers’ offices and employment, among other settings.
How data are collected is also important for reaching and understanding the needs and experiences of LGBTQ+ people. Best practice suggests data should be collected in ways that align with tested standards, conducted in culturally sensitive ways (accompanied by adequate training), secured responsibly, and then used to improve the lives of the people it represents. (See section on policy impact on LGBTQ+ people’s health.)
Many LGBTQ+ people report having experienced stigma and discrimination in health care and other social institutions due to their actual or perceived sexual orientation, gender identity, and/or gender expression.
KFF polling has shown that LGBT adults face higher rates of discrimination and unfair treatment in their daily lives compared to others, with about two-thirds (65%) saying they have experienced at least one type of discrimination at least a few times in the past year, compared to four in ten non-LGBT adults. (See Figure 2.) These experiences are higher among LGBT adults who are younger and lower income.
The KFF/Washington Post Trans survey found that many trans adults say they feel discriminated against at least “sometimes” due to their gender identity or expression, with trans adults of color even more likely to report multiple types of discrimination, including because of their race or ethnicity, income level or education, or sexual orientation, reflecting how discrimination can cut across intersecting identities. (See Figure 3.)
Experiences of stigma and discrimination also occur in health care settings, in part because pathologizing LGBTQ+ identity, behavior, and desire has a long history in medicine. Indeed, much of the early language of LGBTQ+ identity has its origins in 19th-century psychiatry, which defined LGBTQ+ people in opposition to heterosexual people (and health). The early medical literature promotedthe idea that individuals with LGBTQ+ behavior or desire needed treatment, a notion that persisted for more than a century in dominant medical literature and, in 1952, homosexuality was defined as a psychiatric disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM), the tool for classifying mental health conditions in the United States; it was not removed as such until 1974 (though as a compromise APA added “sexual orientation disturbance” as diagnosis which was then replaced with “ego dystonic homosexuality” which was not removed until 1987.) While mainstream medicine has evolved from the view of needing to treat LGBTQ+ identity as a medical or psychological disorder, stigma and discrimination within medicine persist.
KFF polling shows that 6 in 10 LGBT adults report at least one of several negative experiences with a health care provider in the past three years – about twice the share of non-LGBT adults who report this. (See Figure 4.)
Additionally, about 3 in 10 trans adults say they have had to teach a doctor or other health care provider about trans people to receive appropriate care, had a doctor refuse to acknowledge their preferred gender identity, or been asked unnecessary or invasive questions about their gender identity that were unrelated to their care. (See Figure 5.)
Experiences of stigma, discrimination, and mistreatment based on sexual orientation or gender identity occur in multiple non-health care environments and institutions as well, and these also negatively affect health and well-being.
Hate crimes, defined as “bias against people or groups with specific characteristics that are defined by the law,” have negative effects on health, including both physical and psychological harm, and LGBTQ+ people are more likely to experience hate crimes than non-LGTBQ+ people. According to the FBI, in 2022, more than 1 in 5 hate crimes were related to being LGBTQ+. Of these, 17% were based on sexual orientation and 4% on gender identity, accounting together for 2,416 crimes in total. Hate crimes against gay men accounted for nearly half (45%) of these, followed by crimes against a combined group of LGBT people (26%), and then transgender people (14%). A smaller share were reported against lesbians (8%), gender non-conforming people (5%), bisexual people (1%), and heterosexual people (1%). (Notably, whether a hate crime gets reported to the FBI and how it is defined are highly variable so these statistics are likely an underrepresentation of actual crimes that occur.) (See Figure 6.)
Sexual violence, in particular, is a common experience among LGBTQ+ people relative to non-LGBTQ+ people and is especially high among bisexual women and gay and bisexual men. Bisexual women report higher lifetime experiences with rape, other sexual violence and stalking, and lesbian women report higher rates of sexual violence and unwanted sexual contact across their lifetimes than heterosexual women. Gay and bisexual men report higher rates of sexual violence, unwanted sexual experiences, and sexual coercion than heterosexual men, with gay men also reporting higher rates of stalking across their lifetimes than heterosexual men.
Transgender people also face higher rates of intimate partner violence and are more likely to be the victim of a violent crime, with surveys finding that trans people report high rates of violence across a range of measures. KFF polling shows that a majority of trans adults (64%) say they have been verbally attacked and 1 in 4 say they have been physically attacked because of their gender identity, gender expression, or sexual identity. The share of trans adults who have been physically attacked because of their gender identity increases to 31% among trans people of color.
Young LGBTQ+ people are also impacted by higher rates of bullying and violence, including sexual violence, compared to their non-LGBTQ+ peers. LGBTQ+ high school students report higher rates of being bullied than non-LGBTQ+ students, with LGBTQ+ students about twice as likely as non-LGBTQ+ students to report that they have been bullied on school property (29% v. 16%) or to report electronic bullying (25% v. 13%). Additionally, LGBTQ+ high school students are twice as likely to report having been injured or threatened with a weapon at school compared to non-LGBTQ+ students (14% v. 7%). Experiences with sexual violence generally (20% v. 8%) and forced sex in particular (17% v. 6%) were also more common among LGBTQ+ high school students than non-LGBTQ+ high school students. (See Figure 7.)
LGBTQ+ people’s disproportionate experiences of maltreatment, stigma, and discrimination can have a significant and negative impact on present and future mental health. Indeed, LGBT adults who had recent experiences with at least one form of discrimination in the past year are more likely to report feeling always or often lonely (42% v. 15%), depressed (38% v. 21%) or anxious (65% v. 34%) than those who rarely or never experienced discrimination in daily life. Additionally, larger shares of LGBT women, younger LGBT adults, and lower-income LGBT adults report regular feelings of anxiety, loneliness, or depression. While other underlying factors beyond discrimination may contribute to these differences, the relationship between feelings of loneliness, anxiety, and depression and experiences with discrimination among LGBT adults remains significant even after controlling for race/ ethnicity, education, income, gender, and age (see section on mental health below). (See Figure 8.)
Overall, LGBT people report similar rates of being uninsured as non-LGBT people (9% v. 10%). LGBT adults, who are notably both younger and lower income than the general population, have higher rates of Medicaid coverage (25% v. 15%) and lower rates of Medicare coverage (8% v. 22%). They are slightly more likely to be covered by private insurance than non-LGBT adults (57% v. 51%). (See Figure 9.)
Research has found that having a usual source of care is associated with increased use of preventive care and better health outcomes, but LGBT people are more likely to report not having a usual source of care than non-LGBT people (19% v. 12%). (From KFF’s Survey of Racism, Discrimination, and Health). One study found that LGBTQ people were more likely to lack access to providers, delay care, face issues taking medications due to cost, and have fewer routine checkups than heterosexual cisgender people.
KFF polling has also found that many LGBT adults say negative health care experiences have affected their willingness to seek care, their health care coverage, and their physical health. For example, LGBT adults are significantly more likely than non-LGBT adults to report that having a negative health care experience in the last three years caused their health to get worse (24% v. 9%), made them less likely to seek health care (39% v. 15%), or caused them to switch health care providers (36% v. 16%).
While in some areas, the health experiences of LGBTQ+ people mirror those of non-LGBTQ+ people, in other areas, LGBTQ+ people face disparities in health outcomes due to their sexual orientation and gender identity, as well as other factors such as race/ethnicity, class, nationality, and age. Disparities related to mental health, substance use, and sexual health are especially apparent, and LGBTQ+ people also experience certain chronic conditions at higher rates than heterosexual and cisgender people. In some cases, these are driven by social factors such as the biosocial impact of experiencing stigma and discrimination, higher rates of alcohol use and smoking, and obesity. They may also stem from fear of engaging with the health system, including from past experiences of discrimination, which may lead to forgoing routine screening or needed care.
There may also be a link between health care access, competency, and affordability (discussed above) and the ability to detect, control and treat disease. For example, research has found that transgender and gender-diverse people are both less likely to receive cancer screenings and also have a higher incidence of HIV- and HPV-associated cancers.
Overall Health Status
Despite being a younger population, a group traditionally reporting higher levels of well-being, LGBT people are more likely to report being in fair or poor physical health than non-LGBT people (26% v. 19%).
LGBT+ people also report that they are managing chronic conditions and living with disabilities that impact daily life at higher rates than non-LGBT+ people. Half (50%) of LGBT+ people reported that they had an ongoing health condition that requires regular monitoring, medical care, or medication, compared with 45% of non-LGBT+ people. Additionally, one-quarter (25%) of LGBT+ people reported having a disability or chronic disease that keeps them from participating fully in work, school, housework, or other activities, compared with 16% of non-LGBT+ people.
Likewise, a larger share of LGBT+ people report taking at least one prescription medication on a regular basis than non-LGBT+ people (62% v. 55%). This includes more than half (54%) of young LGBT+ adults (ages 18 to 24) who reported regularly taking a prescription compared to just over one-third (36%) of non-LGBT+ adults in the same age group.
Chronic Conditions
Studies have found disparities in certain chronic conditions among LGBTQ+ people, including reports of higher rates of diabetes among lesbians and gay and bisexual men and higher rates of cardiovascular diseases and cancers in certain populations. One study found LGBTQ+ survey respondents were more likely to report having asthma, arthritis, diabetes, kidney disease, hypertension, cardiovascular disease, heart attack, stroke, and chronic obstructive pulmonary disease (COPD) than non LGBTQ+ respondents.
HIV and STIs
There are significant HIV and STI-related disparities among gay and bisexual men, other men who have sex with men, and transgender women compared to other groups and the population as a whole. These disparities may arise for a range of reasons, including sexual networks, differences in behavior, and biological or social factors. In addition, increased incidence of HIV and STIs can, in turn, put these groups at higher risk for other comorbid conditions like other STIs and certain cancers. Nearly three-quarters (71%) of people diagnosed with HIV in 2022 were gay and bisexual men or other men who have sex with men, and of those, young Black and Latino men were disproportionately represented. (See Figure 10.)
A meta-analysis estimated that 14% of transgender women and 3% of transgender men are HIV positive. Black and Hispanic transgender women are disproportionately impacted, with prevalence estimates of 44% and 26%, respectively.
Among those seeking care at STD clinics, gay and bisexual men are more likely to test positive for gonorrhea and chlamydia than women or heterosexual men. An estimated 34% of cases of primary and secondary syphilis cases reported in 2022 were among gay and bisexual men and other men who have sex with men, and cases have increased significantly over the past decade. Additionally, the 2022 mpox outbreak occurred almost exclusively among gay and bisexual men and other men who have sex with men, with Black and Hispanic men being especially impacted. While data are limited on gender identity and STIs, studies have indicated that incidence and prevalence levels of gonorrhea and chlamydia among transgender women are similar to those among cisgender gay and bisexual men.
Mental Health and Substance Use
LGBTQ+ people face greater mental health challenges and disparities than non-LGBTQ+ people, including in accessing mental health care. The drivers of these disparities are complex and may relate, in part, to widespread experiences of stigma and discrimination (as described above). Current attempts to institute anti-LGBTQ+ policies in many states and communities may contribute to poor mental health outcomes and increase the need for care.
LGBT adults are more likely than non-LGBT adults to describe their mental health and emotional well-being as either “fair” or “poor” (39% v. 16%). LGBT adults with household incomes below $40,000 are about twice as likely as LGBT adults with higher incomes to report fair or poor mental health (55% v. 27%), as are LGBT adults ages 18-29 compared to those ages 50 and older (56% v. 24%). Across racial and ethnic groups, about 4 in 10 Black (40%), Hispanic (35%) and White (41%) LGBT adults describe their mental health as fair or poor. (See Figure 11.)
More specifically, about half (54%) of LGBT adults report feeling anxious either “always” or “often” in the past year, while a third report feeling lonely (33%) or depressed (32%) “always” or “often” – more than twice the shares of non-LGBT adults who report the same. As noted earlier, those who experienced recent discrimination were more likely to report these feelings than those who did not.
LGB adults also report having serious thoughts of suicide, making a suicide plan, or attempting suicide at higher rates than non-LGB adults, with disparities especially pronounced among bisexual adults. LGB adults also report higher rates of substance use and substance use disorder (SUD) than non-LGB adults, with rates especially high among bisexual adults.
KFF’s polling of trans adults shows that many struggle with serious mental health issues, including 4 in 10 (43%) who say they have had suicidal thoughts in the past year. Trans adults are about six times as likely as cisgender adults to say they have engaged in self-harm in the past year, and more than twice as likely to say they have had an eating disorder in the past year or had suicidal thoughts in the past year. (See Figure 12.)
Mental health disparities are especially significant among young LGBTQ+ people. In 2023, more than half (53%) of LGBTQ+ high school students reported poor mental health in the past 30 days compared to 1 in 5 (21%) non-LGBTQ+ students and more than twice as many reported persistent feelings of sadness or hopelessness over the past year (65% among LGBTQ+ students compared to 31% among non-LGBTQ+ students). In addition, 41% of LGBTQ+ high school students reported having seriously considered suicide during the past year, with 20% having attempted suicide, rates that are substantially higher than for non-LGBTQ+ students (13% and 6%, respectively). (See Figure 13.)
Substance use rates were also higher among LGBTQ+ high school students than their non-LGBTQ+ peers. LGBQ+ students and students with any same-sex partners were more likely to engage in a range of substance use behaviors than their peers, including use of alcohol, marijuana, any illicit drug, vaping, and prescription opioids.
In addition to higher reported rates of mental health challenges, LGBT people, particularly those in fair or poor mental health and younger adults, report greater challenges accessing mental health care and are more likely to report forgoing needed mental health care than non-LGBT adults. About half (46%) of LGBT adults say there was a time in the past three years when they thought they might need mental health services but didn’t get them, more than twice the share of non-LGBT adults who say so (20%). Reported challenges to care include affordability and accessibility of providers, including finding a provider who can relate to their background and experiences.
Access to competent and inclusive health care that meets the needs of LGBTQ+ people can improve engagement with the health system and, ultimately, health outcomes.
The American Medical Association (AMA) provides recommended standards of practice with LGBTQ patients and resources to help make medical practices LGBTQ-friendly, such as including posters, brochures, and other materials that are LGBTQ-inclusive, revising intake materials to be affirming and inclusive, and participating in further provider education.
Similarly, the American Psychiatric Association also provides guidance, including acknowledgment of the role the association played in perpetuating stigma for LGBTQ+ people in the past and guiding practitioners to not make assumptions about sexual orientation or gender identity in gathering medical information, reminding providers that families can be helped to move towards more acceptance of LGBTQ+ children to improve their mental health, and explicitly coming out against ‘conversion or reparative’ therapy. Indeed, the use of “conversion therapy” is condemned among all major health groups, 28 of which signed a 2023 joint statement against its use, stating that such interventions are both ineffective and harmful, and about half of states have enacted a ban on coverage therapy for minors.
Other resources highlight the importance of language use in caring for LGBTQ+ people, including when it comes to how sexual orientation and gender are discussed and described and how patients are addressed with respect to names and pronoun use. Leadership “buy-in” and the role of LGBTQ+ champions are also highlighted, as are the benefits of inclusive policies. Data collection used to improve health outcomes, staff training, and partnering locally with the LGBTQ+ community are also noted as ways to be a more affirming practice.
Providing health care services or competent referrals for health services that are disproportionately needed by the LGBTQ+ community is another way to offer inclusive care. This might include behavioral health services, STI care and screening, or inclusive family planning services. Another such service is gender affirming care (see below).
Gender affirming care is a model of care which includes a spectrum of “medical, surgical, mental health, and non-medical services for transgender and nonbinary people” aimed at affirming and supporting an individual’s gender identity.Gender affirmation is highly individualized. Not all trans people seek the same types of gender affirming care or services and some people choose not to use medical services as a part of their transition. Gender affirming care is tailored to an individual’s needs across the lifespan.
There is no one way to transition. KFF polling finds commonly utilized gender affirming activities are related to a social transition, such as changing the types of clothes worn (77%), changing hairstyles/grooming habits (76%), or going by different pronouns (72%). Slightly fewer, but still a majority, of trans adults use a different name than the one on their birth certificate (57%). Fewer than half of trans adults report attending counseling or therapy as a part of their gender transition (38%) (which is sometimes a requirement for other gender affirming care), legally changing their name on identifying documents (24%), or using hormone treatments or puberty-blocking hormones (31%) Despite common rhetoric, surgical care is a rare component of gender affirming care, with just 16% of trans adults reporting having received gender-affirming surgery. While the number of young trans people using puberty blockers or hormone therapy has increased modestly in recent years, the overall number of those using these prescriptions remains fairly low and multiplestudies have shown gender affirming surgery is extremely rare among minors.
Lack of insurance coverage for gender affirming care is a barrier to receiving these services. KFF’s polling finds, for example, that among trans adults with health insurance, about a quarter (27%) say their insurance covers gender affirming treatment or health care, while 14% say their health insurance does not cover this and 6 in 10 (58%) are unsure. One in 5 trans adults say they have had health insurance that would not cover gender affirming treatments or health care (22%). About 1 in 7 trans adults have changed jobs or health insurance in order to get gender affirming treatments or health care. (See Figure 14.)
Despite the evidence around the role gender affirming care can play in promoting well-being for young people and support from the medical community, some have argued against this care claiming that the services are experimental and lack an evidence base or that young trans people commonly change their minds about their gender identity. To date, more than half (26) of US states (as of September 2024) have enacted restrictions on gender affirming care for minors. As a result, young people may be unable to get medically necessary care depending on where they live and research has demonstrated that young transgender people’s mental health is negatively impacted when this care is denied including leading to an increased risk of suicidality. Further, claims around lack of evidence and changing identity are not borne out by the data and, in fact, the very same services are provided to young people in other medical circumstances without controversy.
Policymaking, including in health care, can both facilitate and hinder access to care and coverage, and ultimately, health outcomes, for LGBTQ+ people. Recent examples of how policymaking addresses LGBTQ+ people’s health include:
Supreme Court of the United States (SCOTUS) Decisions: Several recent Supreme Court decisions have impacted the health and well-being of LGBTQ+ people. SCOTUS decisions regarding marriage equality have been particularly far reaching with both the Windsor (2013) and Obergefell (2015) decisions providing same-sex married couples with legal access to spousal health insurance benefits for the first time, among other changes. In Bostock (2019), SCOTUS ruled that in the context of employment, discrimination based on sex encompasses sexual orientation and gender identity—a decision that was subsequently used to support extending sex protections in health care to LGBTQ+ people (see discussion of Section 1557 below). In the fall of 2024, SCOTUS will hear arguments over a Tennessee law that bans gender affirming care for minors based on a petition brought by the Biden administration arguing against the ban and examine whether the law violates the 14th Amendment’s Equal Protection clause. A decision is expected in the summer of 2025.
Section 1557: One area that has received significant attention over the last decade is Section 1557 of the Affordable Care Act (ACA). Section 1557 prohibits discrimination on the basis of a range of factors, including sex, and applies to health programs and activities receiving federal financial assistance (referred to as covered entities). Specifically, it prevents covered entities from discriminating against certain protected groups in providing health care services, insurance coverage, and program participation. Across different Presidential administrations, lengthy rulemaking and court challenges have affected the application of Section 1557, particularly around whether sexual orientation and gender identity should be encompassed in sex protections. The Obama administration interpreted the statute to include protections on the basis of gender identity and sex-stereotyping, laying out specific protections for trans people, while the Trump administration removed such protections. The Biden administration has since restored and expanded on protections, including by also interpreting sex protections to protect against discrimination on the basis of sexual orientation, following the Bostock decision.
Mental Health: Policy can also positively or negatively impact the mental health of the LGBTQ+ community. For example, 988, the federally-mandated suicide and crisis line, supported by the Substance Abuse and Mental Health Services Administration (SAMHSA), includes specific services to meet the needs of LGBTQ+ young people. SAMHSA also released a “road map” for supporting LGBTQ+ youth, an LGBTQI+ Family Support Grant providing nearly $2 million in funding for programs that address behavioral health for LGBTQ youth, and more than $5 million for “Family Counseling and Support for Lesbian, Gay, Bisexual, Transgender, Queer/Questioning, Intersex+ Youth and their Families,” The agency also funds the Center of Excellence: LGBTQ+ Behavioral Health Equity aimed at supporting “implementation of change strategies within mental health and substance use disorder treatment systems to address disparities impacting the LGBTQ+ community.” The Biden administration issued a rule to better protect LGBTQ+ youth in foster care. In addition to federal efforts, some states are also electing to highlight and address the behavioral health needs of LGBTQ+ people, sometimes through the use of federal funds. On the other hand, there is evidence that the promulgation of state laws and policies restricting access to LGBTQ+ health and other services negatively affects the mental health of the community.
Data collection: (See also callout box on data collection.) Better understanding of who the LGBTQ+ community is and what challenges they face, allows policymakers, providers, and other individuals and groups to meet their needs better and provide care and coverage that is culturally competent. Addressing care needs may happen in the provider’s office, at the health system level, or in the policy arena. Research on LGBTQ+ people and health has increased over time, and the federal government has implemented a range of efforts to improve collection and reporting of data on LGBTQ+ people. For example, in 2016 the NIH formally designated sexual and gender minorities (SGMs) as a health disparity population for research purposes. In doing so, NIH recognized the health disparities faced by this population and that “the extent and causes of health disparities are not fully understood, and research on how to close these gaps is lacking.” Many federal surveys now ask sexual orientation and gender identity questions, including the Behavioral Risk Factor Surveillance System Survey, the National Survey on Drug Use, the National Health Interview Survey, and the Youth Risk Behavior Survey. However, data collection is not routine in federal surveys and systems and is sometimes an optional variable for states or a restricted variable for researchers. Data collection efforts have also been subject to partisan politics, with the Obama administration working to expand SOGI data collection, the Trump administration seeking to roll efforts back, and the Biden administration again working to enhance these efforts. The Biden administration issued an executive order calling for agencies to enhance routine collection of sexual orientation and gender identity data to improve outcomes and address disparities, and an implementing roadmap in a Federal Evidence Agenda. Data collection efforts are variable at state and health system levels.
State and Local Policymaking: While federal policymaking plays an important role in individuals’ lives, so too does state and local policymaking, perhaps, especially so in health care. Over the past few years, there has been a rash of policymaking addressing LGBTQ+ people’s health. Policies have both aimed to expand protections and well-being for LGBTQ+ people and sought to restrict access to care or loosen antidiscrimination standards. For example, as of August 2024, half of states have enacted policies aimed at limiting or prohibiting youth access to gender affirming care and most of this policymaking took place within a recent 18-month period. Other states have enacted “refuge laws” (also known as “shield laws”) that generally aim to protect individuals, families, and providers living in states where these bans have been enacted. State policymaking has also focused on LGBTQ+ people and access to services through private and public insurance coverage. For example, while some states expressly prohibit insurers from discriminating against people based on sexual orientation and gender identity, others are silent on the issue. Similarly, some state Medicaid programs explicitly cover gender affirming care, others have exclusions, and some have no clear policy; even those that do cover this care may not cover all the services an individual needs. Another example of protections is that about half of states have enacted laws banning conversion therapy for minors. Finally, some LGBTQ+ related policy is not overtly health-related but has the potential to impact well-being. For example, preventing schools from adopting LGBTQ+ anti-bullying policies or enacting laws that require school staff to out transgender youth to their families stand to negatively impact health outcomes.
Despite the increase in the share of people identifying as LGBTQ+ and in public support for LGBTQ+ relationships and protections against discrimination, LGBTQ+ people continue to face health disparities and worse health outcomes in several areas. In many cases, these are directly related to ongoing experiences of stigma, discrimination, and violence. Policy efforts to address health disparities among LGBTQ+ people, including those tied to experiences of stigma and discrimination, have increased over time. Still, there has been growing partisanship in some areas of LGBTQ+ rights and access, particularly for LGBTQ+ youth, and a rise in policies and laws that restrict access to recommended care. Monitoring these policies and better understanding the actual experiences of LGBTQ+ people will help inform efforts to address and mitigate health disparities for this population moving forward.
Note: This brief was updated on October 21, 2024 to incorporate new federal policy developments on contraceptive coverage.
Oral contraceptives are the most commonly used method of reversible contraception in the U.S. Oral contraceptive pills were first approved for prescription use by the U.S. Food and Drug Administration (FDA) in 1960. Over 60 years later, on July 13, 2023, the FDA approved Opill, the first daily oral contraceptive pill to become available over-the-counter (OTC) without a doctor’s prescription. It has been available online and in stores since March 2024 to people of all ages. The formulation in Opill was initially approved for prescription use by the FDA in 1973 (by a different manufacturer and with a different brand name). This issue brief provides an overview of OTC oral contraceptives and laws and policies related to insurance coverage.
Safety and Efficacy
Oral contraceptive pills are highly effective at preventing pregnancy with “perfect use”, with a failure rate of less than 1%. However, the failure rate with “typical use,” which accounts for inconsistent or incorrect use, is 9%. Oral contraceptive pills must be taken once per day and are primarily used for pregnancy prevention, but they can also be used to address other health conditions such as menstrual pain, irregular menstruation, fibroids, endometriosis-related pain, menstrual-related migraines, and acne management. Oral contraceptives, especially progestin-only pills, are safe for most women.
Oral contraceptive pills, especially progestin-only pills, are safe for most people to use and have a very low risk of serious side effects or contraindications. Possible side effects from the pill include headache, nausea, breast tenderness, and breakthrough bleeding. Research has found that people, including those under the age of 18, are able to understand label instructions and contraindications for OTC contraception without clinician involvement.
Although it is not as far along in the FDA approval process, another pharmaceutical company, Cadence, is working toward FDA approval of an OTC version of its combined (progestin and estrogen) oral contraceptive pill, Zena. Combined oral contraceptive pills have more contraindications and small, but higher, risks of serious side effects than progestin-only pills like Opill. They are believed to be slightly more effective at preventing pregnancy than progestin-only pills and while they also must be taken every day, there is more flexibility on the precise timing.
Research on Over-the-Counter Access
Over-the-counter (OTC) status is an FDA designation meaning that a drug or product is available without a prescription from a health care provider. The ability to access oral contraceptives without a prescription from a clinician can save time spent on travel, at a doctor’s office, and off work. Studies suggest that OTC access to oral contraceptives could increase the use of contraception, facilitate continuity of use, and reduce the risk of unintended pregnancy.
Additionally, previous KFF research found that more than one-third (36%) of reproductive-age female respondents who use oral contraception have missed taking it on time because they were not able to get their next supply (Figure 1). The added convenience and time saved by obtaining oral contraception OTC instead of having to visit a doctor could reduce the share of women who miss taking their contraception on time.
Consumer Awareness and Use of Over-the-Counter Contraceptive Pills
The nationally representative 2024 KFF Women’s Health Survey found that awareness of Opill is generally low, with just a quarter (26%) of women 18 to 49 saying they have heard of the new daily oral contraceptive pill (Figure 2). Compared to women ages 36 to 49 (24%), significantly larger shares of women ages 26 to 35 say they have heard of Opill. Smaller shares of Black (21%) and Hispanic (23%) women say they have heard of the new oral contraceptive compared to White women (29%).
Research suggest that OTC oral contraceptives can especially benefit populations who have historically faced barriers to accessing contraceptive care, such as young adults and adolescents, those who are uninsured, and those living in contraceptive deserts or areas with limited access to health centers offering the full range of contraceptive methods. However, smaller shares of women who are uninsured (17%) and who live in rural areas (21%) have heard of Opill compared to those with private insurance (29%) and those living in urban or suburban areas (27%).
Among women 18 to 49 who have ever heard of Opill, just 4% say they have ever purchased the over-the-counter contraceptive pill for themselves or for someone else (Figure 3). An even smaller share (3%) say they have used or taken Opill since the contraceptive became available in stores and online earlier in 2024.
Other OTC Contraception
Levonorgestrel emergency contraceptive (EC) pills, known as “the morning after pill” and marketed as Plan BOne-Step and other brands, are a form of backup birth control intended to be taken several days after unprotected sex or contraceptive failure. Levonorgestrel EC pills were the first hormonal contraception to have switched from prescription to OTC status, in 2006. Unlike daily oral contraceptives, emergency contraception is not intended for daily use and is FDA approved for use by women within 72 hours (3 days) after unprotected intercourse or contraceptive failure to prevent pregnancy.
Other contraceptive products that are available over the counter without a prescription include male and female condoms, spermicides, and contraceptive sponges. These contraceptive methods are less effective than oral contraception at preventing pregnancy. FDA’s approval of Opill makes it the most effective form of contraception available over the counter intended for regular use.
Federal Laws on OTC Contraceptive Coverage
Private Insurance
The Affordable Care Act (ACA) requires most private health plans (group and individual) to cover, without cost sharing, the full range of FDA-approved contraceptive methods, which includes oral contraceptive pills. The ACA tasks the Health Resources and Services Administration (HRSA) with coverage requirements for a range of preventive services for women, which now includes contraception, that must be covered by insurance. Right after the ACA was passed, HRSA tasked the Institute of Medicine (IOM) to identify gaps in preventive recommendations. This committee identified contraceptive services and supplies as one of the eight gaps in preventive health services to promote women’s health. The IOM recommended that all FDA-approved contraceptives be included as preventive services, and the HRSA coverage requirement for contraception included that they be covered “as prescribed,” which was reflected in the original guidance issued by the Obama administration in 2013.
Currently, HRSA has commissioned the Women’s Preventive Services Initiative (WPSI) as the expert body it relies on to update and expand preventive services coverage recommendations, which WPSI last updated in 2021. The current coverage requirement posted by HRSA no longer includes a prescription requirement for coverage of contraception, but the U.S. Departments of Labor, Health and Human Services, and Treasury (federal tri-agency) guidance has not been revised to drop the “as prescribed” requirement.
The prescription requirement is currently only mentioned in federal FAQs clarifying ACA coverage requirements, with the most recent one issued by the Biden administration in July 2022. The FAQ references coverage of emergency contraception and states that plans must cover OTC contraceptives when the product is prescribed. It also states that plans are “encouraged to cover OTC emergency contraceptives with no cost sharing when they are purchased without a prescription.” In October 2024, the Biden administration proposed a new rule that would build on the ACA’s coverage requirements and expand coverage of contraception without cost-sharing for those with private insurance. If finalized, most private insurers would be required to cover OTC contraceptives without a prescription from a clinician, and insurers would also be required to disclose to enrollees that OTC contraceptives like Opill and emergency contraception are included in this coverage. The proposed rule also addresses new coverage requirements for other OTC contraceptive methods, such as male condoms.
OTC medications and products do not require a prescription for purchase, but most people wishing to avoid cost-sharing for them need to obtain one. The prescription requirement re-introduces some of the same barriers that were intended to be reduced with OTC status such as eliminating the need to make and wait for a doctor appointment or find a pharmacy whose pharmacists are licensed and available to prescribe contraception (where permitted by state law).
Medicaid
Medicaid is the public health insurance program that covers approximately 20% of low-income children, adults, seniors, and people with disabilities. Medicaid is jointly financed by the federal government and the states. Federal statute sets broad minimum standards in exchange for federal matching funds and states have flexibility in determining other aspects of their Medicaid programs such as covered services and provider payment models.
Coverage for contraceptives is a key element in Medicaid coverage of family planning services. All states cover prescription drugs, even though it is technically an “optional” benefit category under federal law. Federal rules require state Medicaid programs that cover prescription drugs (including OTC drugs with a prescription) to cover all prescription drugs from manufacturers that have entered into a federal rebate agreement with the U.S. Secretary of Health and Human Services, though states may determine whether and how to employ utilization management controls. In order to obtain federal matching funds, a prescription is required for over-the-counter drugs and products.
Federal law also requires state Medicaid programs to cover family planning services and supplies without cost-sharing to enrollees. The federal Medicaid law does not define what services must be included and also does not explicitly cite OTC contraceptives as part of the coverage requirement, but most state Medicaid programs cover a range of contraceptive methods, and some cover OTC methods. The ACA requires states to cover at least one form of all 18 FDA-approved contraceptive methods for enrollees who qualify through the ACA’s Medicaid expansion. In general, these services are defined and determined by the states within broad federal guidelines.
With few exceptions (such as prenatal vitamins, fluoride preparations for pregnant people, and tobacco cessation products), federal law does not require states to cover OTC drugs and products in their Medicaid programs. However, state Medicaid programs can opt to cover them by submitting a state plan amendment (SPA) to CMS, the federal agency that administers Medicaid in partnership with state Medicaid agencies. For example, CMS approved SPAs from Delaware, Montana, andFlorida requesting to cover select OTC drugs generally. After obtaining approval from CMS to cover OTC products generally, states can choose which OTC products their program will cover. However, even when a drug is available to purchase without a prescription, enrollees usually need a prescription to obtain coverage and states cannot obtain federal matching dollars unless it is prescribed. If states wish to include coverage for OTC products without a prescription, state Medicaid programs may opt to use state-only funds.
State Laws on OTC Contraceptive Coverage
State-regulated private health insurance
To reduce access barriers to OTC contraception while also avoiding cost sharing, seven states (CA, CO, MD, NJ, NM, NY, and WA) have laws or regulations requiring state-regulated private health insurance plans (individual, small group, and large group markets) to cover, without cost sharing, at least some methods of OTC contraception without a prescription(Figure 3). With the exception of New York, which applies only to emergency contraception, the language of these laws is broad enough to encompass an OTC daily oral contraceptive such as Opill without a change in policy. (See KFF State Health Facts for more details on each state’s law, including contraceptive methods covered.)
Illinois and Oregon require private health plans to cover OTC contraception; however, while the laws do not state that a prescription is required in order for it to be covered by insurance, the laws also do not explicitly stipulate that plans must cover them without a prescription. Delaware and Massachusetts require private plans to cover OTC emergency contraception with a prescription or pursuant to a standing order or protocol. A standing order allows a physician of a state health department or other state agency to authorize pharmacists to prescribe drugs or provide care under certain conditions set forth in the order.
While federal law applies to all plans, state law applies to only individual plans and fully-insured group plans. Therefore, many people who live in states that require coverage of OTC contraception without a prescription may not have this coverage if they are enrolled in a self-funded employer-sponsored health plan (65% of covered workers nationally).
Medicaid
To increase access to contraception, eight states (CA, IL, MD, MI, NC, NJ, NY, and WA) have opted to use state-only funds to cover at least some methods of OTC contraception for their Medicaid enrollees (primarily emergency contraception) without a prescription (Figure 3). With the exception of California and North Carolina, the language of these state-level policies does not appear broad enough to encompass an OTC daily oral contraceptive pill such as Opill without a change in policy. (See KFF State Health Facts for more details on each state’s policy, including contraceptive methods covered.)
Challenges to the Broad Adoption of OTC Oral Contraception
There are some limitations to the potential reach of an over-the-counter progestin-only pill (POPs). While both progestin-only pills and combined pills (COCs) are safe and effective at preventing pregnancy, POPs are believed to be slightly less effective than COCs. It is recommended that users of POPs take the pill at the same time every day, which could be a barrier for people who are not able or would forget to do this. However, there is limited evidence that adhering to this precise timeframe actually reduces the efficacy of POPs.
Opill’s reach may be limited because few women who use oral contraceptive pills use POPs and instead opt to use COCs. Currently, the primary users of POPs are breastfeeding women because they are safe for this population, and they are not advised to use COCs during this time. Whether users of COCs will opt to switch to Opill for reasons such as convenience or cost is not yet known.
Additionally, retailers can choose whether and how to stock Opill. Retailers who choose to sell it will also decide which supply option (one, three, or six-month packs) to stock. As is the case with emergency contraception at many retailers who stock it, Opill could be kept in a locked case on the shelf or behind the pharmacy counter to reduce the chance of theft, which could create access barriers.
The extent to which over-the-counter oral contraception is accessible will depend, in large part, on affordability and coverage. The suggested retail price for Opill is $19.99 for one month’s supply or $49.99 for three month’s supply. KFF’s 2022 Women’s Health Survey found that 11% of women would not be willing or able to pay anything for an OTC oral contraceptive, and 39% would pay $1-$10 per month. Only 16% said they would pay more than $20 a month. Other research that asked specifically about a progestin-only pill found that adult women would be willing to pay $15 per month and teens ages 15-17 would pay $10.
Insurance coverage of OTC oral contraception without a prescription would eliminate out-of-pocket costs, but for those who prefer not to use their insurance or those who do not have insurance, the price point will matter. Furthermore, while some states require private plans and Medicaid to cover non-prescribed OTC contraception, not everyone in those states is guaranteed this coverage. Absent federal guidance, guaranteed coverage of OTC oral contraception without a prescription will continue to depend on where people live and their type of health plan.
This document was updated on Oct. 4, 2024 to clarify that a new Special Enrollment Period (effective Jan. 1, 2025), which allows individuals who are dually-eligible for Medicare and full Medicaid benefits to make certain changes to their Medicare coverage outside of open enrollment, applies on a monthly basis, not quarterly as was previously stated.
Medicare is the federal health insurance program for 67 million people ages 65 and over and younger adults with long-term disabilities. The program helps to pay for many medical care services, including hospitalizations, physician visits, and prescription drugs, along with post-acute care, skilled nursing facility care, home health care, hospice care, and preventive services.
People with Medicare may choose to receive their Medicare benefits through traditional Medicare or through a Medicare Advantage plan, such as an HMO or PPO, administered by a private health insurer. People who choose traditional Medicare may sign up for a separate Medicare Part D prescription drug plan for coverage of outpatient prescription drugs and may also consider purchasing a supplemental insurance policy to help with out-of-pockets costs if they do not have additional coverage from a former employer, union, or Medicaid. People who opt for Medicare Advantage can choose among dozens of Medicare Advantage plans, which include all services covered under Medicare Parts A and B, and often include Part D prescription drug coverage as well.
Each year, Medicare beneficiaries have an opportunity to make changes to how they receive their Medicare coverage during the nearly 8-week annual open enrollment period. This brief answers key questions about the Medicare open enrollment period and Medicare coverage options.
1. When is the annual Medicare open enrollment period?
The annual Medicare open enrollment period runs from October 15th to December 7th each year (Figure 1). During this time, people with Medicare can review features of Medicare plans offered in their area and make changes to their Medicare coverage, which go into effect on January 1st of the following year. These changes include switching from traditional Medicare to a Medicare Advantage plan (or vice versa), switching between Medicare Advantage plans, and electing or switching between Medicare Part D prescription drug plans.
2. What changes can Medicare beneficiaries make during the annual open enrollment period?
People in traditional Medicare can use the Medicare open enrollment period to enroll in a Medicare Part D prescription drug plan or switch between Part D plans. Traditional Medicare beneficiaries who did not sign up for a Part D plan during their initial enrollment period can enroll in a Part D plan during the annual open enrollment period, though they may be subject to a late enrollment penalty if they did not have comparable prescription drug coverage from another plan before signing up for Part D. Traditional Medicare beneficiaries with Medicare Parts A and B can also use this time to switch from traditional Medicare into a Medicare Advantage plan, with or without Part D coverage.
People who are enrolled in a Medicare Advantage plan can use the Medicare open enrollment period to choose a different Medicare Advantage plan or switch to traditional Medicare. Medicare Advantage enrollees who switch to traditional Medicare can enroll in a Part D plan if they want outpatient prescription drug coverage, which is not covered under Medicare Parts A and B. They may also consider purchasing a Medicare supplemental insurance policy (Medigap) if the option is available to them (see question 4 for details about Medigap and potential limits on enrollment).
Medicare beneficiaries are encouraged to review their current source of Medicare coverage during the annual open enrollment period and compare other options that are available where they live. Because an individual’s medical needs can change over the course of the year, and from one year to the next, this may influence their priorities when choosing how they want to get their Medicare benefits. Medicare Advantage and Medicare prescription drug plans typically change from one year to the next and may vary in many ways that could have implications for a person’s access to providers and costs. Despite this, a KFF analysis of a nationally representative survey of people with Medicare found that nearly 7 in 10 (69%) did not compare their Medicare coverage options during a recent open enrollment period (Figure 2).
3. Are there other opportunities for Medicare beneficiaries to make coverage changes outside of the open enrollment period?
Some Medicare beneficiaries can make certain changes to their coverage at other times of the year. For example, beneficiaries who experience disruptions to existing coverage (such as a cross-county move or a loss of employer- or union-sponsored coverage) or changes in eligibility for Medicaid or other programs, may qualify for a Special Enrollment Period at any time of year. People who are enrolled in both Medicare and Medicaid (i.e., dual-eligible individuals) or who qualify for the Medicare Part D Extra Help program, can currently change their Medicare Advantage or Medicare Part D coverage once per quarter. People living in nursing homes and certain other facilities may change their Medicare Advantage or Medicare Part D coverage once per month.
Beginning on January 1, 2025, new rules go into effect related to the type and frequency of changes dual-eligible individuals and those who qualify for Extra Help can make to their Medicare coverage. Beneficiaries in this group will be allowed to disenroll from a Medicare Advantage plan into traditional Medicare on a monthly basis and may choose to enroll in a stand-alone Part D drug plan at that time. People who receive full Medicaid benefits will only be allowed to switch between Medicare Advantage plans on a monthly basis if switching to a Fully Integrated Dually Eligible Special Needs Plan (FIDE SNP), a Highly Integrated Dually Eligible Special Needs Plan (HIDE SNP), or a coordination-only D-SNP that is an Applicable Integrated Plan (AIP) that is aligned with their Medicaid managed care enrollment. People who receive partial Medicaid benefits, or who qualify for the Extra Help program but do not receive Medicaid benefits, will no longer be allowed to switch between Medicare Advantage plans outside of open enrollment.
Medicare Advantage enrollees who wish to change plans or switch to traditional Medicare may do so between January 1st through March 31st each year, during the Medicare Advantage Open Enrollment Period. (This is in addition to the open enrollment period that runs from October 15th to December 7th.) Additionally, those who have a Medicare Advantage or Medicare Part D plan with a 5-star quality rating available in their area may switch into a 5-star plan between December 8th and November 30th of the following year.
The annual open enrollment period and other opportunities to switch coverage are distinct from the initial enrollment period for people who are newly enrolling in Medicare, which begins three months before a person’s 65th birthday and ends three months after it. For more information on initial enrollment, see the Medicare Open Enrollment FAQ.
4. How does supplemental coverage, like Medigap and employer-sponsored retiree health benefits, factor into Medicare coverage decisions?
Many Medicare beneficiaries have some form of additional coverage, such as a Medicare Supplemental Insurance policy (Medigap) or coverage offered by an employer or a union, that helps with Medicare’s cost-sharing requirements. Enrollment in these plans and programs is not tied to the open enrollment period, though beneficiaries may wish to take them into account when considering their options for Medicare coverage.
Medigap. People in traditional Medicare with both Part A and Part B can apply for a Medigap policy at any time of the year. Medigap policies are designed to help beneficiaries in traditional Medicare with Medicare’s deductibles and cost-sharing requirements and have standard benefits to allow for apples-to-apples comparisons across insurers. Traditional Medicare beneficiaries with a Medigap plan that covers most deductible and cost-sharing requirements may have lower out-of-pocket spending for Medicare-covered services than people with other coverage, including a Medicare Advantage plan. Medigap policies are designed to wrap around traditional Medicare, and do not work with Medicare Advantage. People enrolled in Medicare Advantage do not need (and can’t buy) a Medigap policy.
While Medigap insurers are required to issue policies to people age 65 or over, without regard to health status or diagnosed medical conditions when they first enroll in Medicare, those with pre-existing conditions may be denied a Medigap policy or face higher premiums in most states if they apply for Medigap coverage after their first six months of enrollment in Part B. People who disenroll from Medicare Advantage within 12 months of first enrolling in Medicare Advantage have a right to purchase a Medigap policy without regard to medical history, but after 12 months, they are not guaranteed Medigap coverage and may be denied a policy due to a pre-existing condition or face higher Medigap premiums if they are offered a policy.
Medigap guaranteed issue rights are different for people under age 65 who qualify for Medicare due to long-term disability. Federal law does not require Medigap insurers to sell a policy to people with Medicare under age 65, although several states do require insurers to offer at least one kind of Medigap policy to people under 65. Premiums for Medigap policies sold to people under age 65 are typically higher than policies sold to those age 65 or older. People under age 65 with disabilities who are already enrolled in Medicare will qualify for the 6-month Medigap open enrollment period when they turn 65 and become age eligible for Medicare. At this point, they can buy any Medigap policy they want without facing higher premiums or denials of coverage based on their existing medical conditions.
Employer-sponsored coverage. While employer-sponsored retiree health benefits are on the decline, more than 14.5 million people with Medicare have retiree health coverage (distinct from people with Medicare Part A only who continue to work and have health insurance through their current employer or a spouse’s current employer). Retiree health benefits may be designed to supplement either traditional Medicare or Medicare Advantage. Some employers that offer benefits to retirees on Medicare offer retiree health benefits exclusively through a Medicare Advantage plan. Beneficiaries with retiree health coverage offered exclusively through a Medicare Advantage plan may lose retiree health benefits if they choose to switch to traditional Medicare during the annual open enrollment period. Similarly, employers may only offer a retiree health benefit that supplements traditional Medicare. If a person with such coverage switches from traditional Medicare to Medicare Advantage during an open enrollment period, they may lose their retiree health benefits. In fact, if a Medicare beneficiary drops their employer or union-sponsored retiree health benefits for any reason, they may not be able to get them back.
5. How does additional support for low-income people factor into Medicare coverage decisions?
Low-income Medicare beneficiaries who meet their states’ Medicaid eligibility criteria qualify for additional coverage of services not covered under Medicare, such as long-term services and supports. Additionally, Medicare beneficiaries with modest incomes may qualify for assistance with Medicare premiums and out-of-pocket costs from the Medicare Savings Programs (MSP) and Part D Low-Income Subsidy (LIS) if their income and assets are below certain amounts. Medicare beneficiaries who are eligible for Medicaid, the Medicare Savings Programs, or Medicare Part D Low-Income Subsidies, but not yet enrolled in these programs, can enroll at any time of the year. This additional coverage and assistance may factor into how people choose to receive their Medicare benefits.
Medicaid. For people who qualify for full Medicaid benefits, the choice of Medicare coverage can impact how they receive those benefits and the degree to which those benefits are coordinated with Medicare. In general, Medicaid wraps around Medicare coverage, with Medicare as the primary payer and Medicaid paying for costs and services not covered by Medicare. People dually eligible for Medicare and Medicaid can enroll in a Medicare Advantage plan designed for this population, such as a dual-eligible special needs plan (SNP), and depending on the state and the plan, experience a higher level of coordination of their benefits. People who qualify for full Medicaid benefits can currently switch their Medicare coverage outside of the open enrollment period, up to once per quarter. Beginning on January 1, 2025, new rules go into effect related to the type and frequency of changes dual-eligible individuals can make to their Medicare coverage (see Q3 for further details).
Medicare Savings Programs. State Medicaid programs pay Medicare premiums and, in many cases, cost sharing for Medicare beneficiaries who have income and assets below certain amounts (though some states have lifted their income and/or asset thresholds above the federal limits). Specifically, states cover the Medicare Part B premium for people who qualify and may also provide assistance with Medicare deductibles and other cost-sharing requirements. People who receive MSP assistance and are enrolled in a Medicare Advantage plan may still have cost sharing associated with non-Medicare covered services offered by the plan. People who qualify for MSP can also switch their coverage outside of the open enrollment period, up to once per quarter.
Part D Low-Income Subsidy. People who qualify for the Part D Low-Income Subsidy (LIS) receive varying levels of assistance toward their Part D prescription drug coverage premiums and cost sharing, depending on their income and asset levels. Dual-eligible individuals and people enrolled in the Medicare Savings Programs automatically qualify for full LIS benefits, and Medicare automatically enrolls them into a stand-alone Part D drug plan in their area with a premium at or below the regional average (the Low-Income Subsidy benchmark) if they do not choose a plan on their own. Other beneficiaries are subject to both an income and asset test and need to apply for the LIS through either the Social Security Administration or Medicaid. People who receive LIS assistance can select any Part D plan offered in their area, but if they enroll in a plan that is not a so-called “benchmark plan” (that is, plans available without a premium to enrollees receiving full LIS), or their current plan loses benchmark status, they may be required to pay some portion of their plan’s monthly premium, which would diminish the value of the subsidy.
6. How do the features of traditional Medicare compare to those of Medicare Advantage?
Traditional Medicare and Medicare Advantage both provide coverage of all services included in Medicare Part A and Part B, but certain features, such as out-of-pocket costs, provider networks, and access to extra benefits vary between these two types of Medicare coverage. When deciding between traditional Medicare and Medicare Advantage, Medicare beneficiaries may want to consider a variety of factors, such as their own health and financial circumstances, preferences for how they get their medical care, which providers they see, and their prescription drug needs. These decisions may involve careful consideration of premiums, deductibles, cost sharing and out-of-pocket spending; extra benefits offered by Medicare Advantage plans; how the choice of coverage option may affect access to certain physicians, specialists, hospitals and pharmacies; rules related to prior authorization and referral requirements; and variations in coverage and costs for prescription drugs.
People may prefer traditional Medicare if they want the broadest possible access to doctors, hospitals and other health care providers. Traditional Medicare beneficiaries may see any provider that accepts Medicare and is accepting new patients. People with traditional Medicare are not required to obtain a referral for specialists or mental health providers. Additionally, prior authorization is rarely required in traditional Medicare and only applies to a limited set of services. With traditional Medicare, people have the ability to choose among stand-alone prescription drug plans offered in their area, which tend to vary widely in terms of which drugs are covered and at what cost.
People may prefer Medicare Advantage if they want extra benefits, such as coverage of some dental and vision services, and reduced cost sharing offered by these plans, often for no additional premium (other than the Part B premium). Additionally, Medicare Advantage plans are required to include a cap on out-of-pocket spending, providing some protection from catastrophic medical expenses. Medicare Advantage plans also offer the benefit of one-stop shopping (i.e., people who enroll have coverage under one plan and do not need to sign up for a separate Part D prescription drug plan or a Medigap policy to supplement traditional Medicare).
7. How do Medicare Advantage plans vary?
The average Medicare beneficiary can choose from 43 Medicare Advantage plans (Figure 3) offered by 8 insurance companies in 2024. These plans vary across many dimensions, including premiums and out-of-pocket spending, provider networks, extra benefits, prior authorization and referral requirements, and prescription drug coverage. As a result, enrollees face different out-of-pocket costs, access to providers and pharmacies, and coverage of non-Medicare benefits (such as dental, vision and hearing) based on the Medicare Advantage plan they choose.
Premiums and out-of-pocket spending. Medicare Advantage enrollees may be charged a separate monthly premium (in addition to the Part B premium). In 2024, the average enrollment-weighted premium for Medicare Advantage plans was $14 per month, though three quarters (75%) of enrollees were in plans that charged no additional premium (apart from the Part B premium).
Medicare Advantage plans are generally prohibited from charging more than traditional Medicare, but vary in the deductibles, co-pays and co-insurance they require. For example, plans typically charge a daily co-pay for hospital stays, which vary both in the amount and the number of days for which they apply.
Medicare Advantage plans are required to include a cap on out-of-pocket expenses. In 2024, this cap may not exceed $8,850 for in-network services or $13,300 for all covered services. Most plans have an out-of-pocket limit below this cap, averaging $4,882 for in-network services and $8,707 for in-network and out-of-network services combined. Out-of-pocket limits only apply to services covered under Medicare Parts A and B.
Provider networks. Medicare Advantage plans are permitted to limit their provider networks, the size of which can vary considerably for both physicians and hospitals, depending on the plan and the county where it is offered. Medicare Advantage plans that include prescription drug coverage may also establish pharmacy networks or designate preferred pharmacies, where enrollees will have lower out-of-pocket costs. If a Medicare Advantage plan provides coverage of out-of-network providers, it may require higher cost sharing from enrollees for these services.
Extra benefits. Medicare Advantage plans may choose to offer extra benefits not covered by traditional Medicare, such as some coverage of dental, vision, and hearing services. Virtually all Medicare Advantage enrollees are in a plan that offers extra benefits, including some coverage of eye exams and/or eyeglasses (more than 99%), dental care (98%), hearing exams and/or aids (96%), and a fitness benefit (95%). Additionally, a majority of Medicare Advantage enrollees are in plans that provide an allowance for over-the-counter items (88%) and meals following a hospital stay (74%). While extra benefits are common, the scope of coverage varies widely from plan to plan. For example, in 2021, more than half (59%) of Medicare Advantage enrollees were in a plan with a maximum dental benefit of $1,000 or less, while nearly one-third (30%) were in a plan with a limit between $2,000 and $5,000.
Prior authorization and referral requirements. Medicare Advantage plans may require enrollees to receive prior authorization before a service will be covered. In 2022, more than 46 million prior authorization requests were submitted to insurers on behalf of Medicare Advantage enrollees, and in 2024, virtually all Medicare Advantage enrollees were in plans that required prior authorization for some services, such as inpatient hospital stays, diagnostic tests and procedures, or stays in a skilled nursing facility. Prior authorization may also be required for some services included in a plan’s extra benefits, such as hearing and eye exams or comprehensive dental services. In addition, Medicare Advantage plans may require enrollees to obtain a referral from a primary care provider in order to see a specialist or mental health provider.
Prescription drug coverage. Medicare Advantage enrollees who want prescription drug coverage must choose a plan that offers this coverage, as they are not permitted to enroll in a stand-alone prescription drug plan while enrolled in Medicare Advantage. Medicare Advantage plans that include prescription drug coverage may also charge a drug deductible. Drug coverage in Medicare Advantage plans varies along the same dimensions as drug coverage in stand-alone Part D plans (described below).
8. How do Part D plans vary?
The average Medicare beneficiary has 21 stand-alone Part D plans to choose from in 2024 (Figure 4) (in addition to a large number of Medicare Advantage drug plans, if they want to consider Medicare Advantage for all of their Medicare-covered benefits). For traditional Medicare beneficiaries who want to add Part D coverage, stand-alone Part D plans vary in terms of premiums, deductibles and cost sharing, the drugs that are covered and any utilization management restrictions that apply, and pharmacy networks. These differences can affect enrollees’ access to prescription drugs and out-of-pocket costs.
Premiums. People in traditional Medicare who are enrolled in a separate stand-alone Part D plan generally pay a monthly Part D premium unless they qualify for full benefits through the Part D Low-Income Subsidy (LIS) program and are enrolled in a premium-free (benchmark) plan. In 2024, the average enrollment-weighted premium for stand-alone Part D plans was $43 per month. Changes to the Part D benefit in the Inflation Reduction Act, such as the new $2,000 cap on out-of-pocket drug spending for Part D enrollees, will mean lower out-of-pocket costs for many Medicare beneficiaries but higher costs for Part D plans overall, leading to concerns about possible premium increases for 2025 (see Q9 for further discussion of the Inflation Reduction Act).
Deductibles and cost sharing. Deductibles and cost-sharing requirements for prescription drug coverage are variable. Plans generally impose a tier structure to define cost sharing requirements and cost sharing amounts charged. Plans typically charge lower cost-sharing amounts for generic drugs and preferred brands and higher amounts for non-preferred and specialty drugs, and charge a mix of flat dollar copayments and coinsurance (based on a percentage of a drug’s list price) for covered drugs.
Drugs covered and utilization management restrictions. Part D plans include a list of drugs they cover (also referred to as a plan’s formulary). In addition, plans may also impose utilization management restrictions on covered prescription drugs, including prior authorization, quantity limits, and step therapy, which can affect beneficiaries’ access to medications. In 2024, around 30% of covered drugs are subject to prior authorization.
Pharmacy networks. Part D prescription drug plans may establish pharmacy networks or designate preferred pharmacies, where enrollees will have lower out-of-pocket costs.
9. Do the Medicare prescription drug changes in the Inflation Reduction Act differ across Medicare coverage options?
No. The prescription drug provisions in the Inflation Reduction Act of 2022 that aim to lower out-of-pocket costs apply to all Part D plans, including both stand-alone Part D plans and Medicare Advantage Prescription Drug plans. Regardless of whether beneficiaries get their drug coverage from a stand-alone Part D plan or a Medicare Advantage drug plan, they will benefit from these changes.
As of 2023, cost sharing for insulin is now capped at $35 per month per prescription. All Medicare Part D plans, both stand-alone drug plans and Medicare Advantage drug plans, will be required to charge no more than $35 for whichever insulin products they cover, although plans will not be required to cover all insulin products. Beneficiaries who use a specific insulin product should verify coverage of their product before enrolling in a specific plan.
Also as of 2023, adult vaccines covered under Medicare Part D that have been recommended by the Advisory Committee on Immunization Practices (ACIP) must now be covered at no cost to enrollees. This change does not impact the small number of vaccines covered under Medicare Part B (such as the flu, pneumonia, and COVID-19 vaccines), many of which were already covered free of cost. Finally, drug companies are now required to pay rebates to the Medicare program if the cost of drugs used by Medicare beneficiaries rises faster than the rate of inflation each year, similar to the rebate system used by the Medicaid program.
Additional provisions came into effect at the start of 2024, which include phasing in a cap on out-of-pocket costs for prescription drugs covered under Medicare Part D by eliminating cost sharing above the catastrophic threshold in 2024 and expanding eligibility for full benefits under the Medicare Part D Low-Income Subsidy Program, which assists qualifying beneficiaries with their Part D premiums, deductibles, and cost-sharing expenses.
Starting in 2025, Medicare beneficiaries will pay no more than $2,000 out of pocket for the prescription drugs they take that are covered under Medicare Part D. Other changes to the Medicare Part D program will be introduced in future years.
10. What resources are available to assist Medicare beneficiaries in understanding their coverage options?
People with Medicare can learn more about Medicare coverage options and the features of different plan options by reviewing the Medicare & You handbook. In addition, people can review and compare the Medicare options available in their area by using the Medicare Plan Compare website, a searchable tool on the Medicare.gov website, by calling 1-800-MEDICARE (1-800-633-4227), or by contacting their local State Health Insurance Assistance Program (SHIP). SHIPs offer local, personalized counseling and assistance to people with Medicare and their families. Contact information for state SHIPs can be found by calling 877-839-2675 or by checking the listing provided on the Medicare.gov website.
Additionally, many people use insurance agents and brokers to navigate their coverage options. While helpful, agents and brokers are financially compensated by private insurers for enrolling people in their plans, and often receive higher commissions if people choose a Medicare Advantage plan rather than remaining in traditional Medicare and purchasing a supplemental Medigap policy and stand-alone Part D plan.
Each year, people with Medicare can review their coverage options and change plans during the annual Open Enrollment Period (October 15 to December 7). Medicare beneficiaries with traditional Medicare can compare and switch Medicare Part D stand-alone drug plans or join a Medicare Advantage plan, while enrollees in Medicare Advantage can compare and switch Medicare Advantage plans or elect coverage under traditional Medicare with or without a stand-alone drug plan. Beneficiaries have no shortage of plans to choose from: in 2024, the average Medicare beneficiary can choose among 43 Medicare Advantage plans and 21 Part D stand-alone prescription drug plans (PDPs).
The marketplace of Medicare private plans operates on the premise that people with Medicare will compare plans during the open enrollment period to select the best source of coverage, given their individual needs and circumstances. Coverage and costs vary widely among both Medicare Advantage plans and Part D prescription drug plans and can change from one year to the next, which could lead to unexpected and avoidable costs and disruptions in care for beneficiaries who do not review their options annually. For example, changes in Medicare Advantage provider networks could mean beneficiaries lose access to their preferred doctors, while changes in the list of covered drugs and cost-sharing requirements could result in higher out-of-pocket drug costs. Further, beneficiaries’ health care needs can change from one year to the next. Even without a change made by their plan or a change in health status, beneficiaries may be able to find a plan that better meets their individual needs or lowers their out-of-pocket costs.
In focus groups conducted by KFF, Medicare beneficiaries highlighted many of these factors, including out-of-pocket costs, access to specific doctors, and coverage of prescription drugs, as important in choosing their Medicare coverage. Yet, Medicare beneficiaries also expressed difficulty understanding and comparing the various plan options and being overwhelmed by a barrage of television ads – mostly for Medicare Advantage plans.
In this analysis, KFF examines the share of Medicare beneficiaries who reviewed their coverage and compared plans during the 2021 open enrollment period for coverage in 2022, and who made use of Medicare’s official information resources, as well as variations by demographic groups, based on an analysis of the 2022 Medicare Current Beneficiary Survey (the most recent year available).
Key Takeaways
Overall, nearly 7 in 10 (69%) Medicare beneficiaries did not compare their own source of Medicare coverage with other Medicare options offered in their area during the 2021 open enrollment period, while 31% did so. A larger share of beneficiaries in traditional Medicare than in Medicare Advantage did not compare their own source of coverage with other plans (73% vs 65%).
Among Medicare Advantage enrollees, more than 4 in 10 (43%) did not review their current plan’s coverage to check for potential changes in their plan’s premiums or other out-of-pocket costs, while the remainder (57%) did so. A similar share (44%) did not review their current plan for potential changes in the kinds of treatments, drugs, and services that would be covered in the following year.
Most enrollees in Medicare Advantage prescription drug plans (82%) and stand-alone prescription drug plan (PDPs) (69%) did not compare their plan’s drug coverage with drug coverage offered by other plans in their area.
Medicare’s official information resources are used by half or fewer of Medicare beneficiaries, with just a quarter (26%) reporting calling the toll-free number, 4 in 10 (42%) reporting visiting the Medicare website, and slightly more than half (54%) reporting reading some or parts of the Medicare & You handbook.
Nearly 7 in 10 Medicare Beneficiaries Did Not Compare Medicare Coverage Options During the Open Enrollment Period for 2022
Overall, most (69%) Medicare beneficiaries reported that they did not compare their current Medicare plan to other Medicare coverage options that were available during the 2021 open enrollment period for coverage in 2022 (Figure 1, Table 1). Among Medicare Advantage enrollees, nearly two-thirds of enrollees (65%) did not compare coverage options for 2022, even though year-to-year changes in Medicare Advantage plans, such as changes in provider networks or prior authorization requirements can affect enrollees’ access to care.
The share of Medicare beneficiaries who did not compare Medicare coverage arrangements was higher among certain subgroups, including beneficiaries with lower incomes and education levels, Hispanic beneficiaries, those dually-enrolled in Medicare and Medicaid, under age 65 with disabilities or ages 85 and older, and beneficiaries with a cognitive impairment (Figure 2, Appendix Table 1).
More Than 4 in 10 Medicare Advantage Enrollees Did Not Review Their Own Plan for Potential Changes in Covered Costs or Services for the Coming Year
For Medicare Advantage enrollees, premiums, cost sharing, and out-of-pocket limits can vary from year to year and across plans, with Medicare Advantage plans having the flexibility to modify cost sharing for most services, subject to limitations. Medicare Advantage plans may provide extra (“supplemental”) benefits that are not covered in traditional Medicare, but the type and scope of specific services often varies from one year to the next. Additionally, virtually all Medicare Advantage enrollees are in plans that impose prior authorization requirements for certain services, and these plans can alter the list of covered drugs, and broaden or narrow their network of physicians and other providers from one year to the next, subject to federal standards.
More than 4 in 10 (43%) Medicare Advantage enrollees did not review their current plan during the open enrollment period to see whether there would be changes for 2022 to their monthly premiums, deductibles, co-payments, or other out-of-pocket expenses, but the remaining 57% reported doing so (Figure 3, Appendix Table 2). Similarly, 44% of Medicare Advantage enrollees did not review their current plan for changes to the kinds of treatments, drugs, and services offered for their coverage in 2022.
The share of Medicare Advantage enrollees who did not review their own plan for changes in costs or services was higher among certain enrollees, including those with lower incomes and education levels, Black and Hispanic enrollees, individuals self-reporting fair or poor health, enrollees ages 85 and older, and those dually-eligible for Medicare and Medicaid coverage (Figure 3, Appendix Table 2).
For example, half of all Medicare Advantage enrollees reporting fair or poor health did not check to see if there was going to be a change in monthly premiums, deductibles or co-payments in their coverage, or any change in the kinds of treatments, drugs and services that would be covered. Nearly two-thirds of Hispanic (65%) and half of Black (50%) Medicare Advantage enrollees did not review their plan for changes in costs, with a similar pattern for changes in services (64% vs 48%, respectively). Additionally, nearly 60% of adults ages 85 and older did not review their plan for changes in costs (57%) or services (58%).
Most Medicare Beneficiaries with Part D Prescription Drug Coverage Did Not Compare Their Plan’s Drug Coverage to Other Drug Coverage Options
Part D plan costs, including premiums, deductibles, and cost-sharing requirements can change from year to year and vary by plan. Additionally, Part D plans can also modify their formularies, including adding or dropping drugs from coverage, and adding or modifying utilization management requirements that apply to specific drugs, such as prior authorization and step therapy.
The prescription drug provisions of the Inflation Reduction Act include changes that will lower out-of-pocket costs for all Part D enrollees, including a new $2,000 cap on out-of-pocket spending starting in 2025. In response to these changes, it is possible that Part D plan sponsors may make changes to plan premiums, formularies and cost sharing, making it particularly important for beneficiaries to compare their prescription drug options during open enrollment.
About 8 in 10 (82%) enrollees in Medicare Advantage plans with prescription drug coverage (MA-PDs) did not compare the drug coverage offered by their own MA-PD to other MA-PDs in their area during the 2021 open enrollment period (Figure 4; Appendix Table 3). Among stand-alone prescription drug plan (PDP) enrollees, a lower share, 69% of enrollees, said they did not compare drug coverage offered by their current PDP to other PDPs.
The share of beneficiaries with coverage under MA-PDs or PDPs who did not compare drug coverage offered for coverage in 2022 was higher among women, beneficiaries with lower incomes and education levels, Hispanic beneficiaries, beneficiaries ages 85 and older, and dual-eligible individuals (AppendixTable 3).
Medicare’s Information Resources Are Used by Half or Even Fewer Beneficiaries
Medicare provides information resources to help beneficiaries understand their Medicare benefits, coverage options, and costs, including the 1-800 Medicare toll free number, the Medicare.gov website, and the Medicare & You handbook that is provided each year to all Medicare beneficiaries. But these resources are not widely used, particularly the toll-free number (Figure 5, Appendix Table 4).
About a quarter (26%) of Medicare beneficiaries reported calling the 1-800-MEDICARE helpline for information, but the remaining three-quarters (74%) of Medicare beneficiaries reported either never calling the helpline for information (51%) or being unaware that this helpline existed (23%).
Four in 10 (42%) Medicare beneficiaries said they (or someone on their behalf) visited the official Medicare website for information, but more than half (58%) said they either never visited the website (36%) or they did not have access to the internet or had no one to access it for them (22%).
More than half (54%) of Medicare beneficiaries reported that they had read the Medicare & You handbook (thoroughly or some parts of the handbook), but 46% reported that either they did not read the handbook (31%) or they did not receive it or did not know if they had received it (15%).
The share of Medicare beneficiaries who used Medicare information sources was lower among certain subgroups, including Black beneficiaries, individuals ages 75 to 84, and dual-eligible individuals (Appendix Table 4).
Methods
This analysis uses survey data for community-dwelling Medicare beneficiaries from the Centers for Medicare & Medicaid Services (CMS) Medicare Current Beneficiary Survey (MCBS) 2022 Survey File.
The analysis of 1) the share of beneficiaries who compared Medicare plans during the open enrollment period for 2022 coverage, 2) the share of Medicare Advantage enrollees who reviewed their current coverage for changes in costs or services, and 3) the share of beneficiaries who used Medicare’s official information sources used questions from the Medicare Plan Beneficiary Knowledge topical segment. This analysis was weighted to represent the ever-enrolled Medicare population in 2022 using the topical survey weight KNSEWT and relevant replicate weights. The analysis of the share of beneficiaries who compared Medicare plans and the share of Medicare Advantage enrollees who reviewed their current coverage for changes in costs or services excluded beneficiaries who reported just enrolling in Medicare.
The analysis of MA-PD/PDP drug plan comparison used questions from the Rx Medication topical segment; similar as above, the analysis was weighted to represent the ever-enrolled Medicare population in 2022 using the topical survey weight RXSEWT and relevant replicate weights.
Both analyses excluded beneficiaries with Part A or Part B only, those with Medicare as secondary payer, and those living in long-term care facilities. All reported differences in the text are statistically significant at p<0.05.
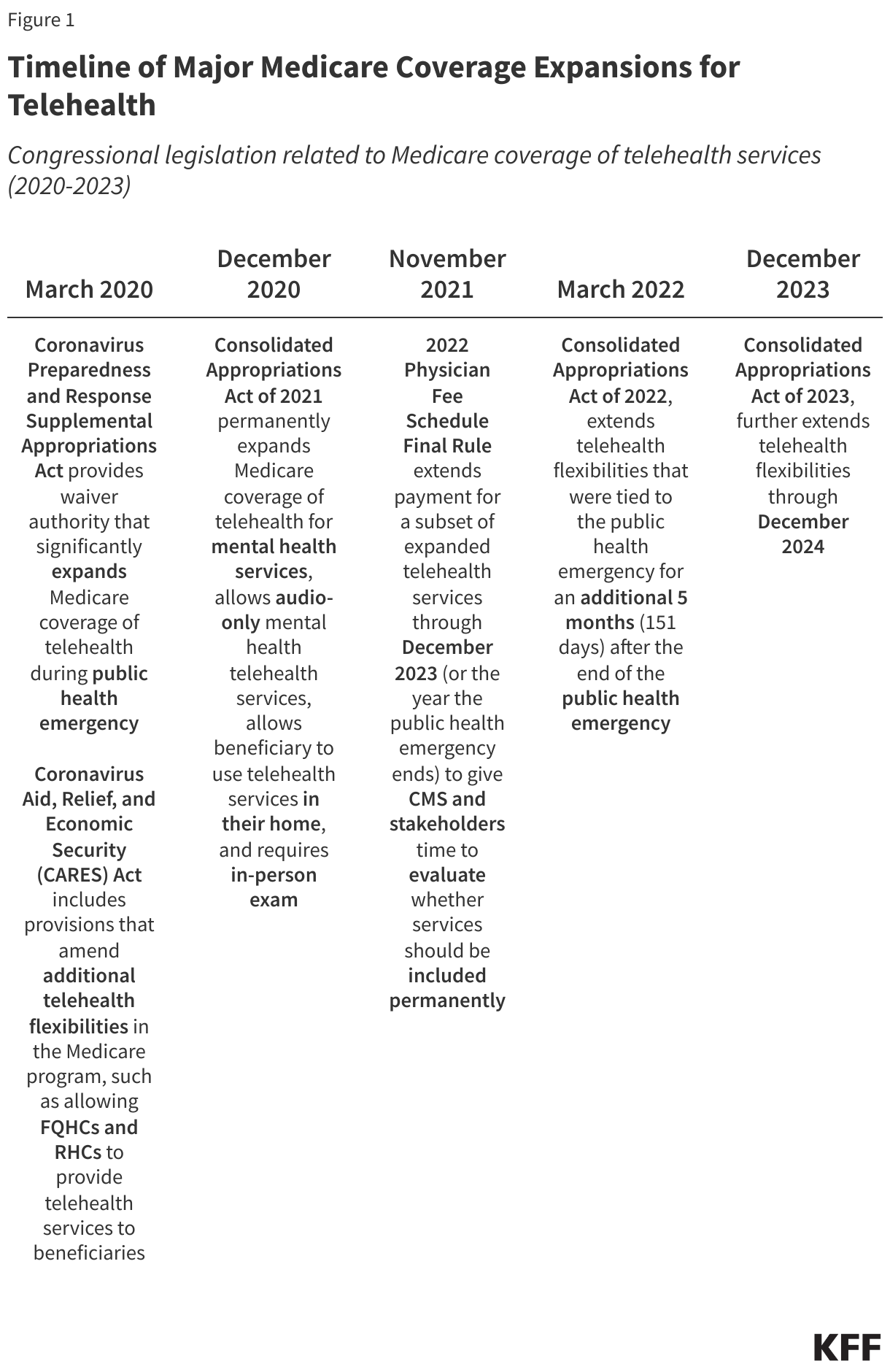
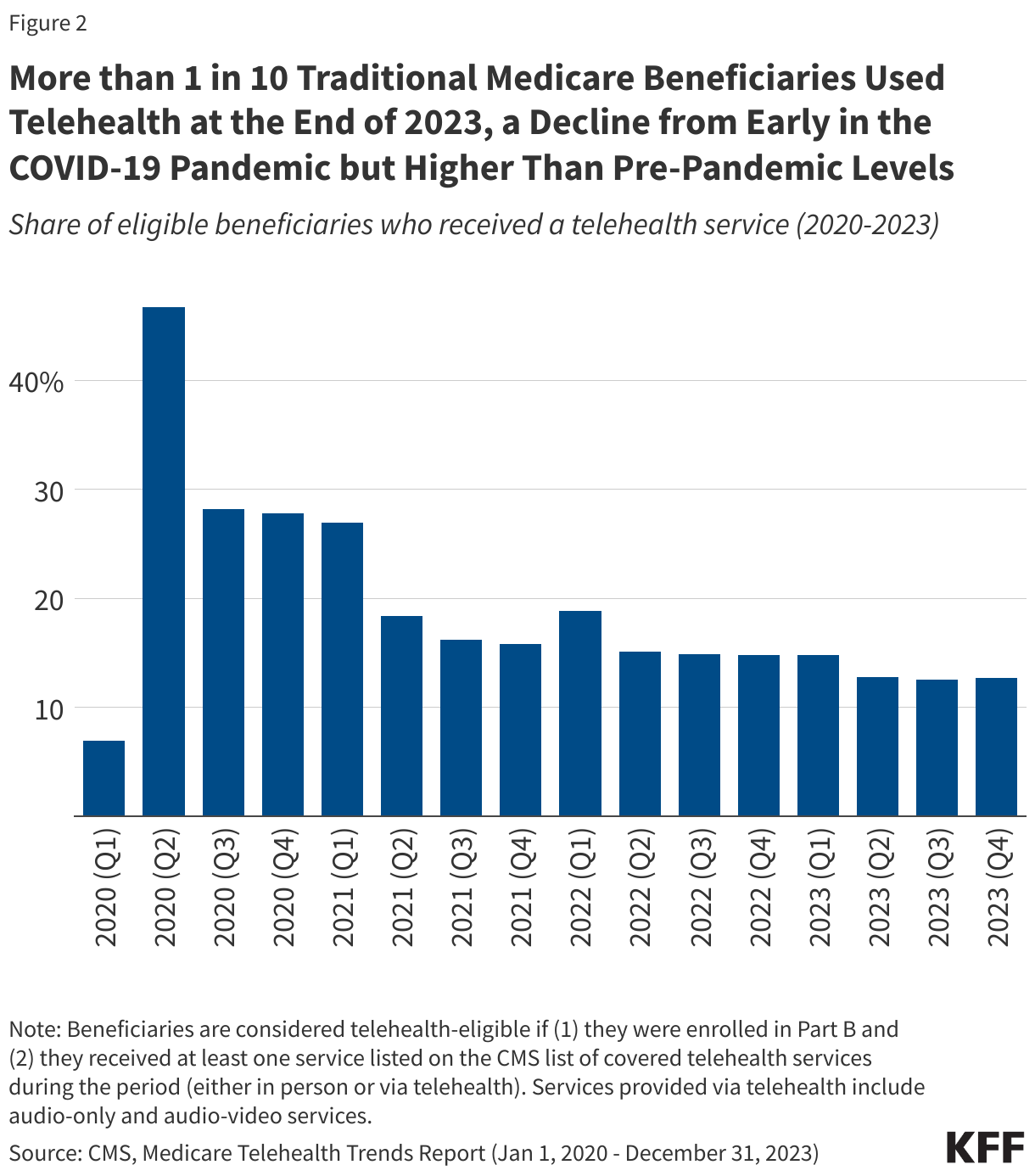
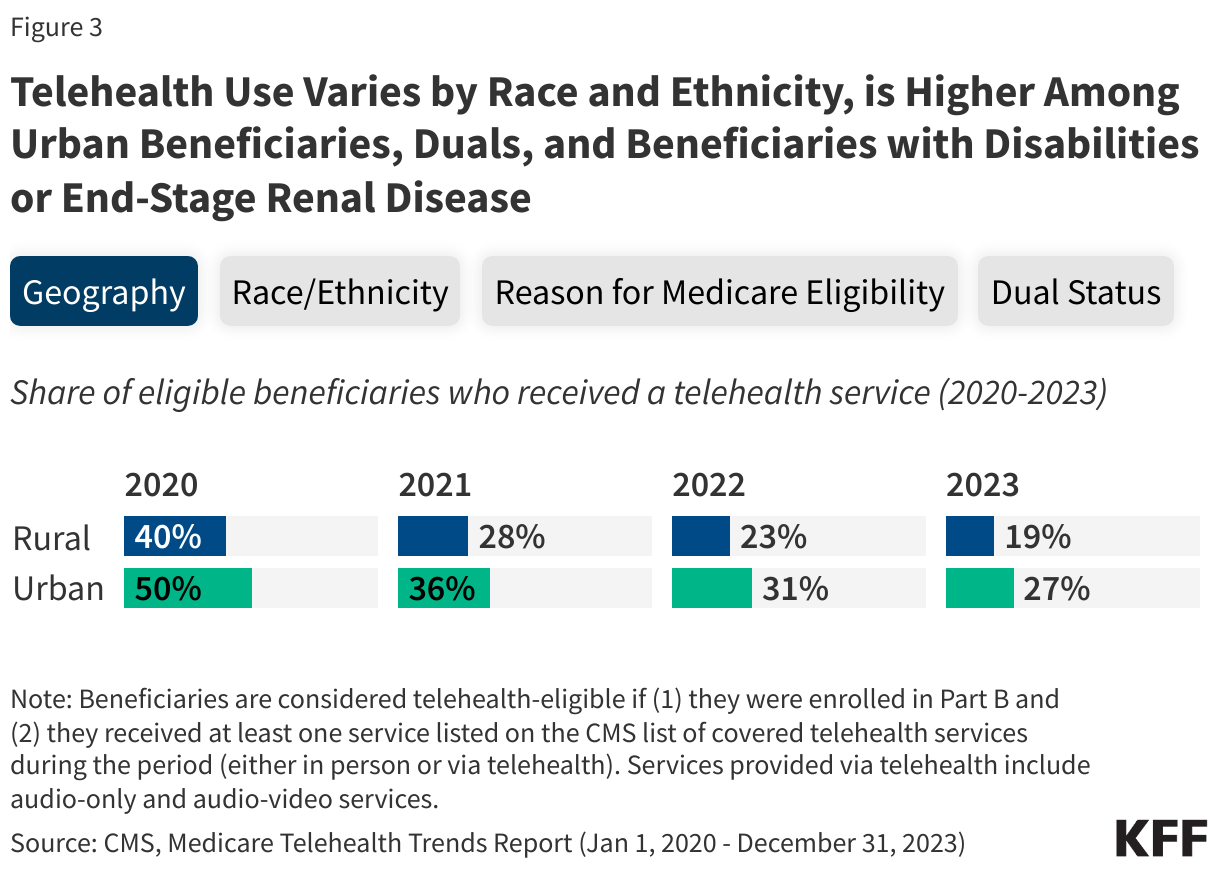
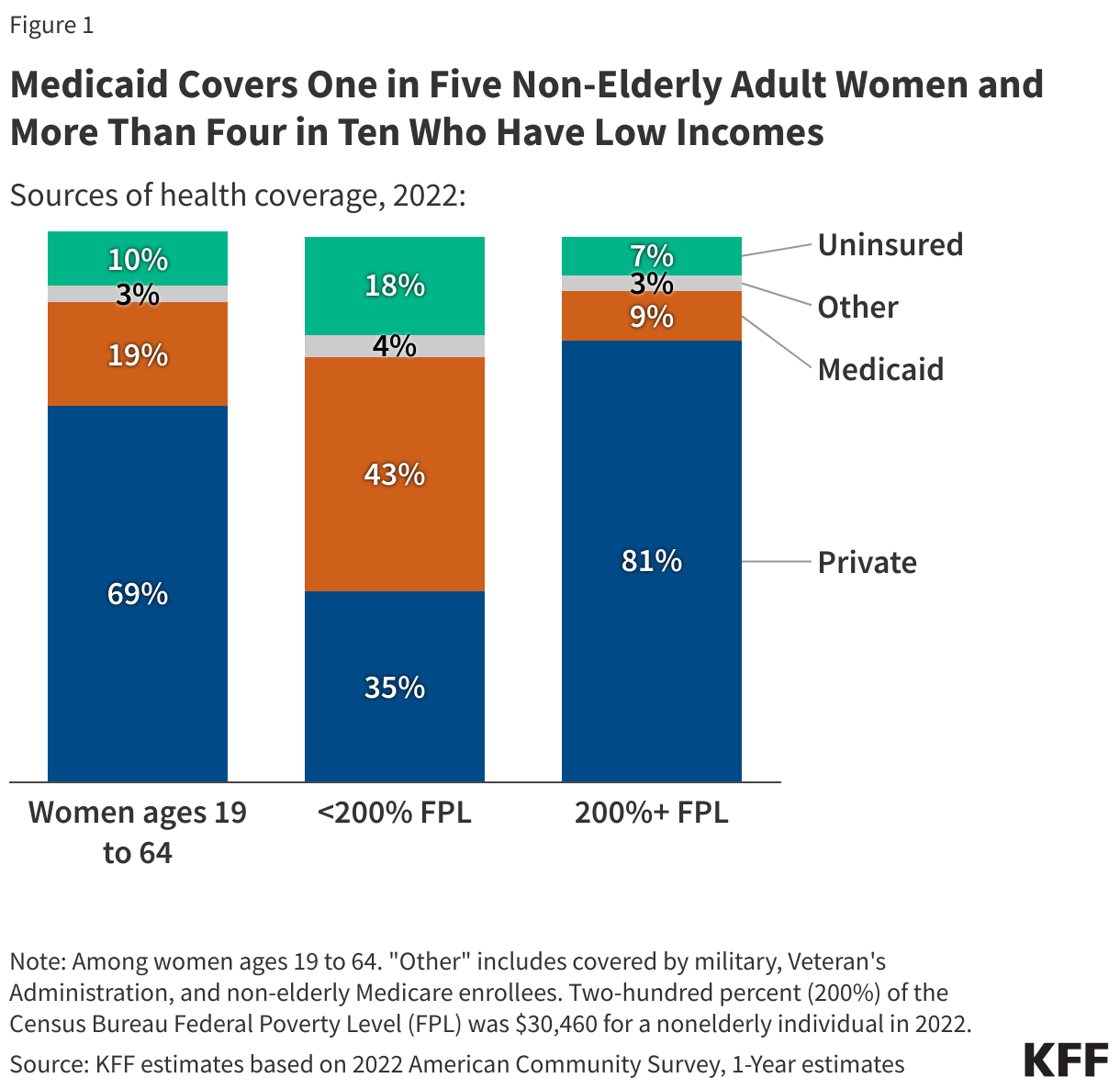
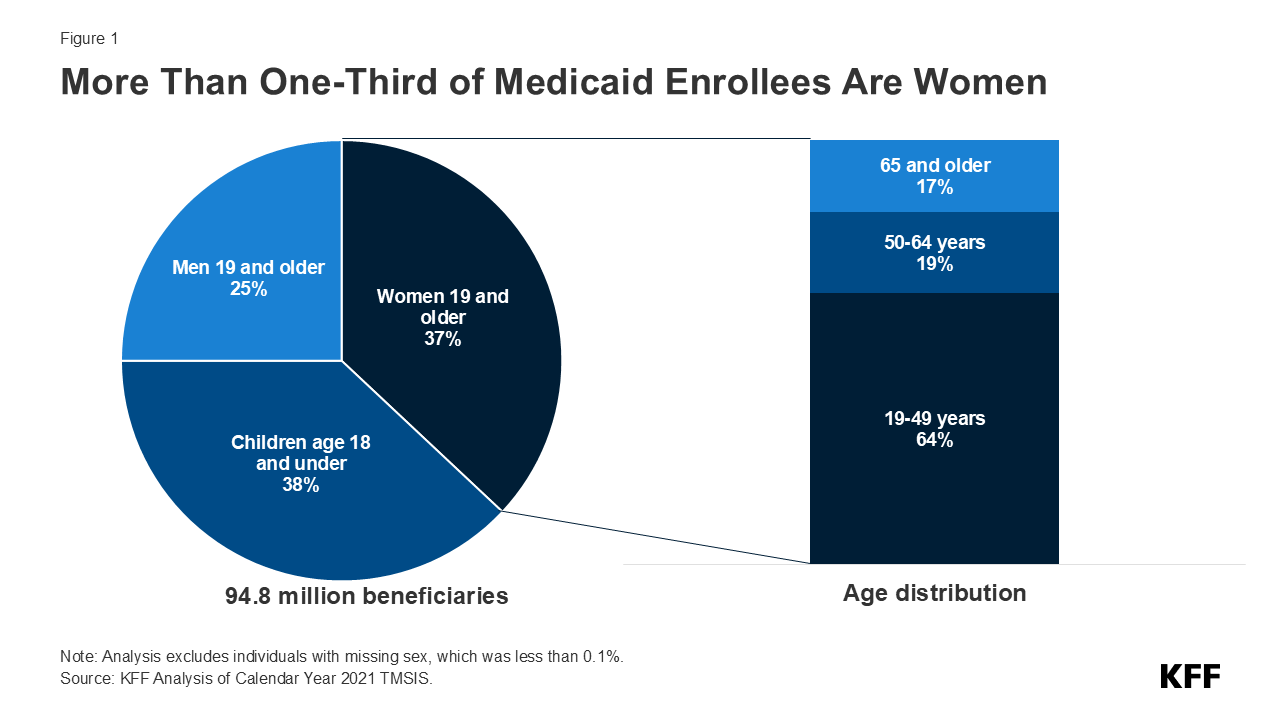
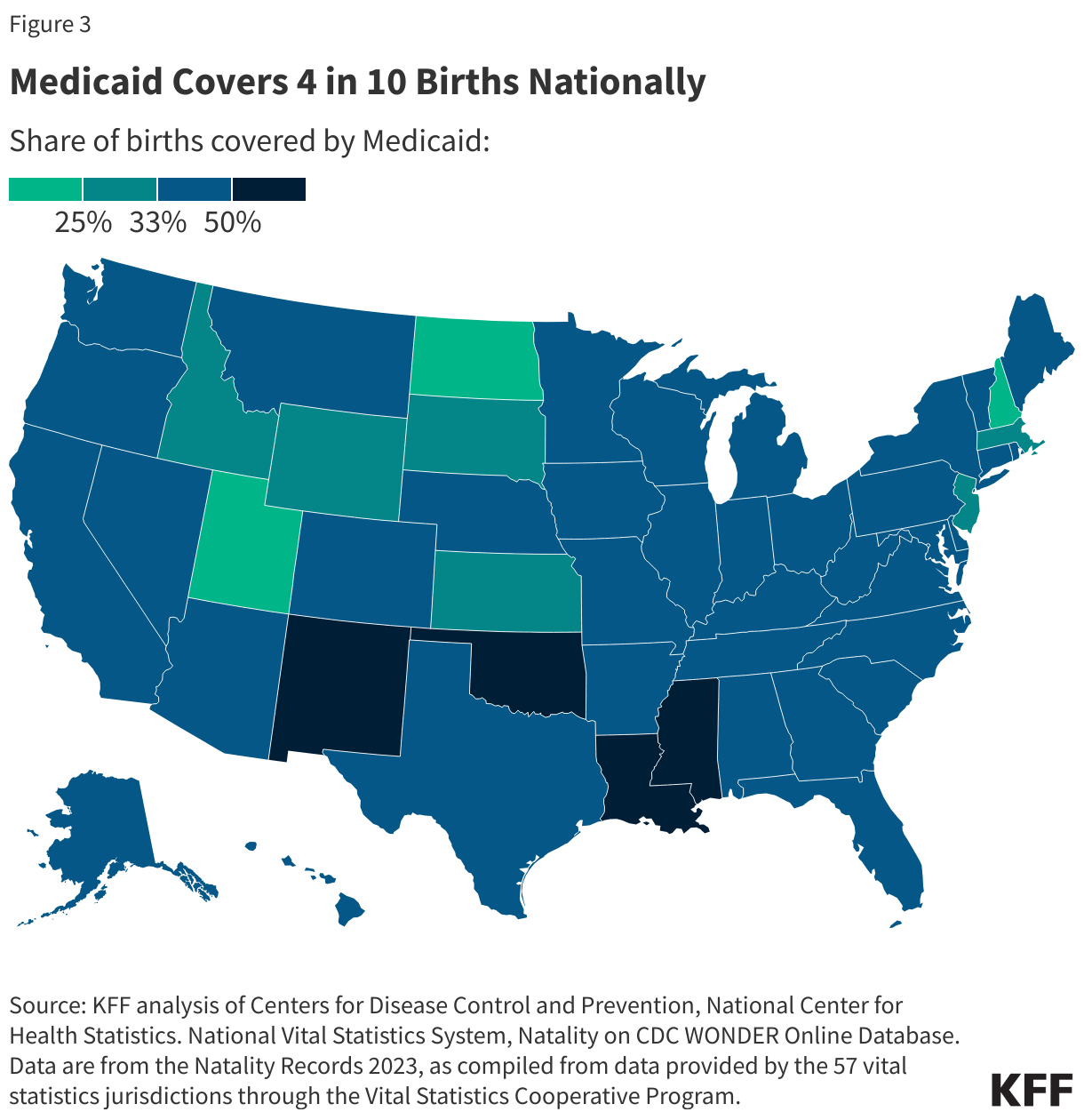
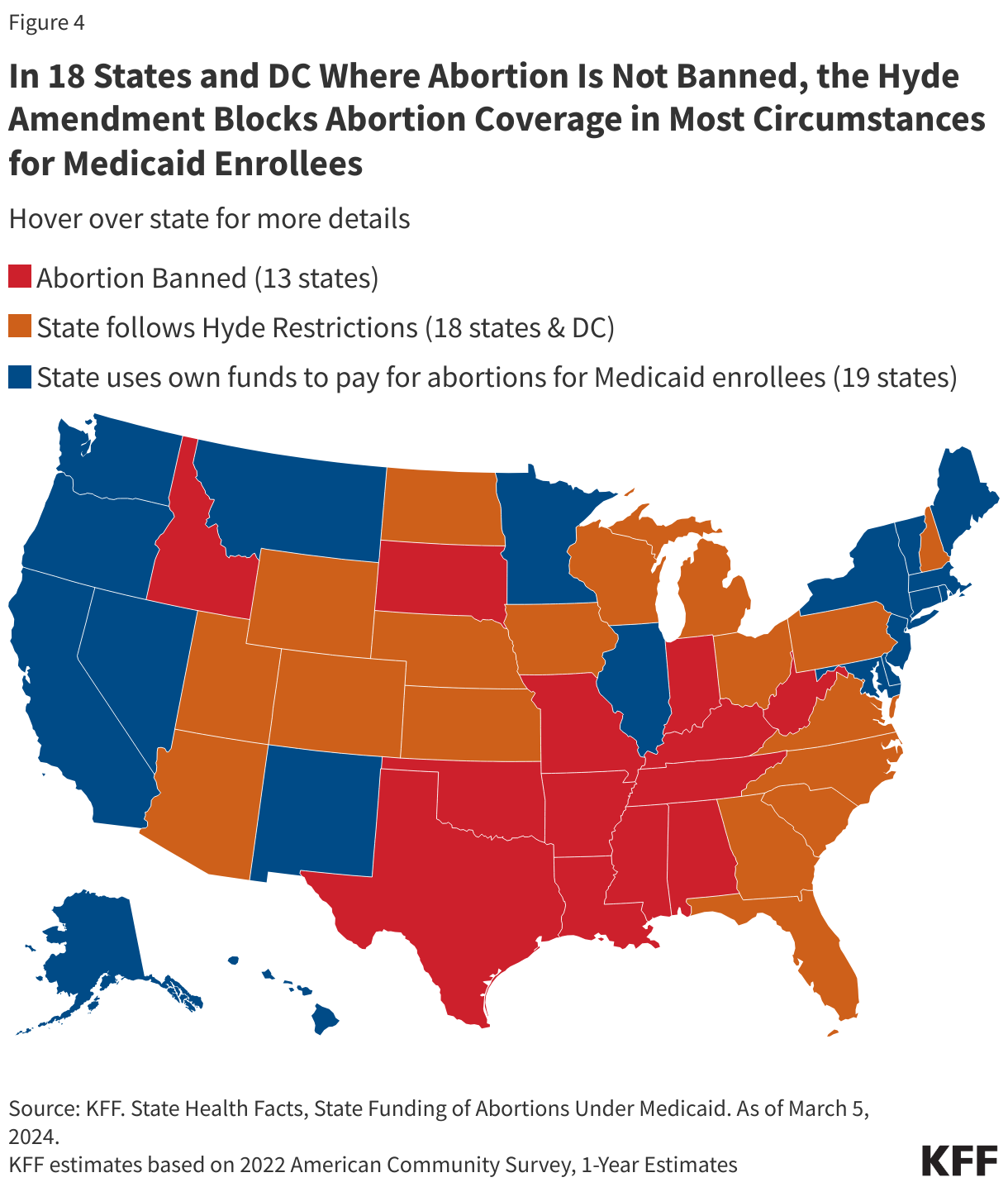
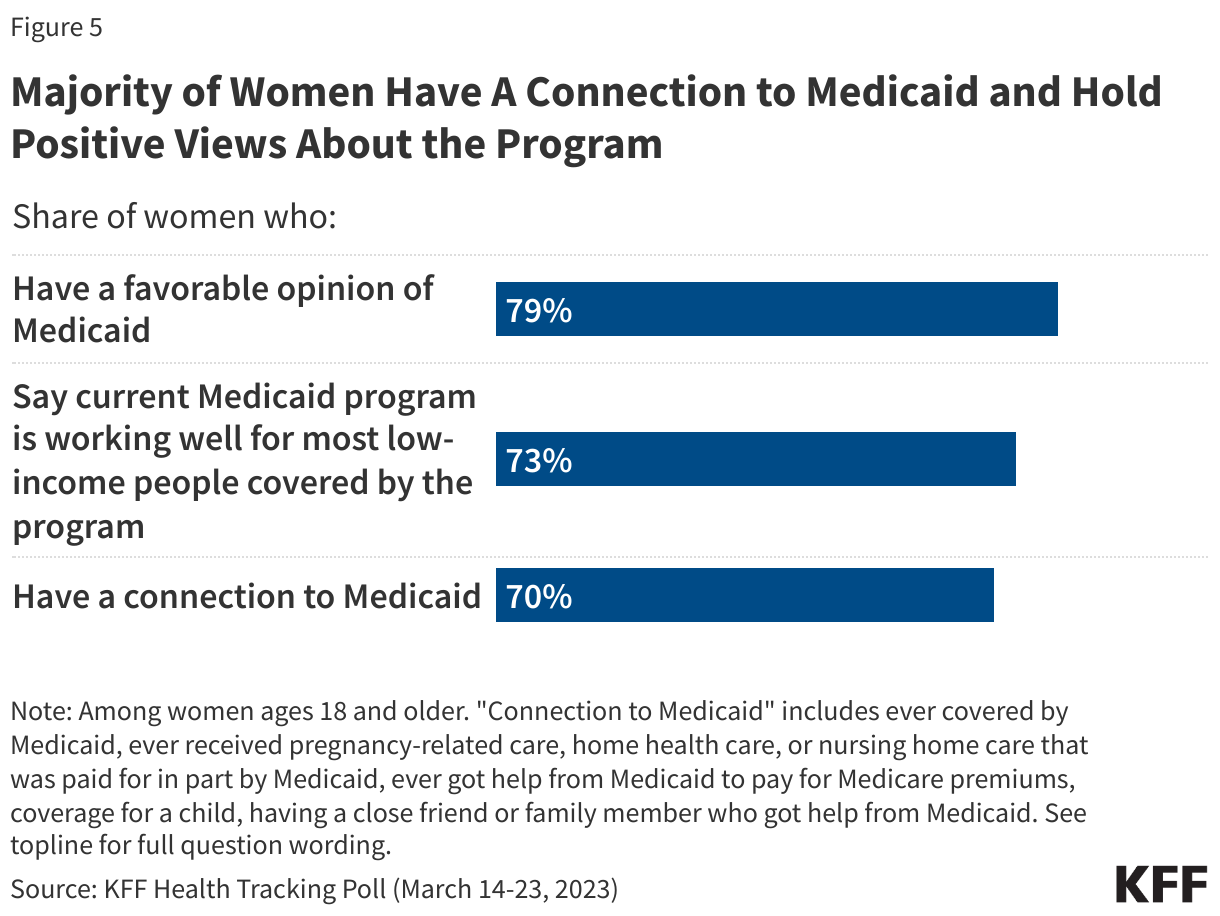
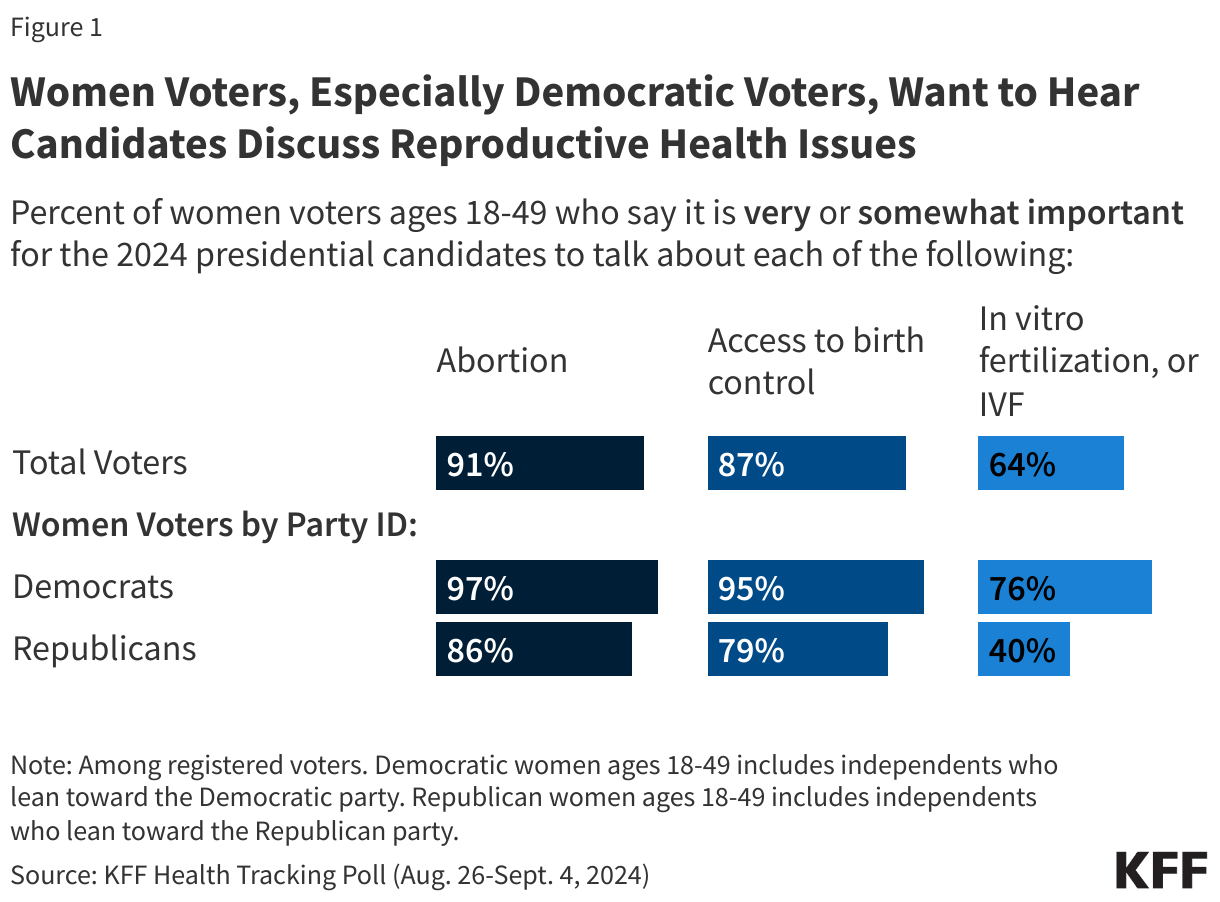

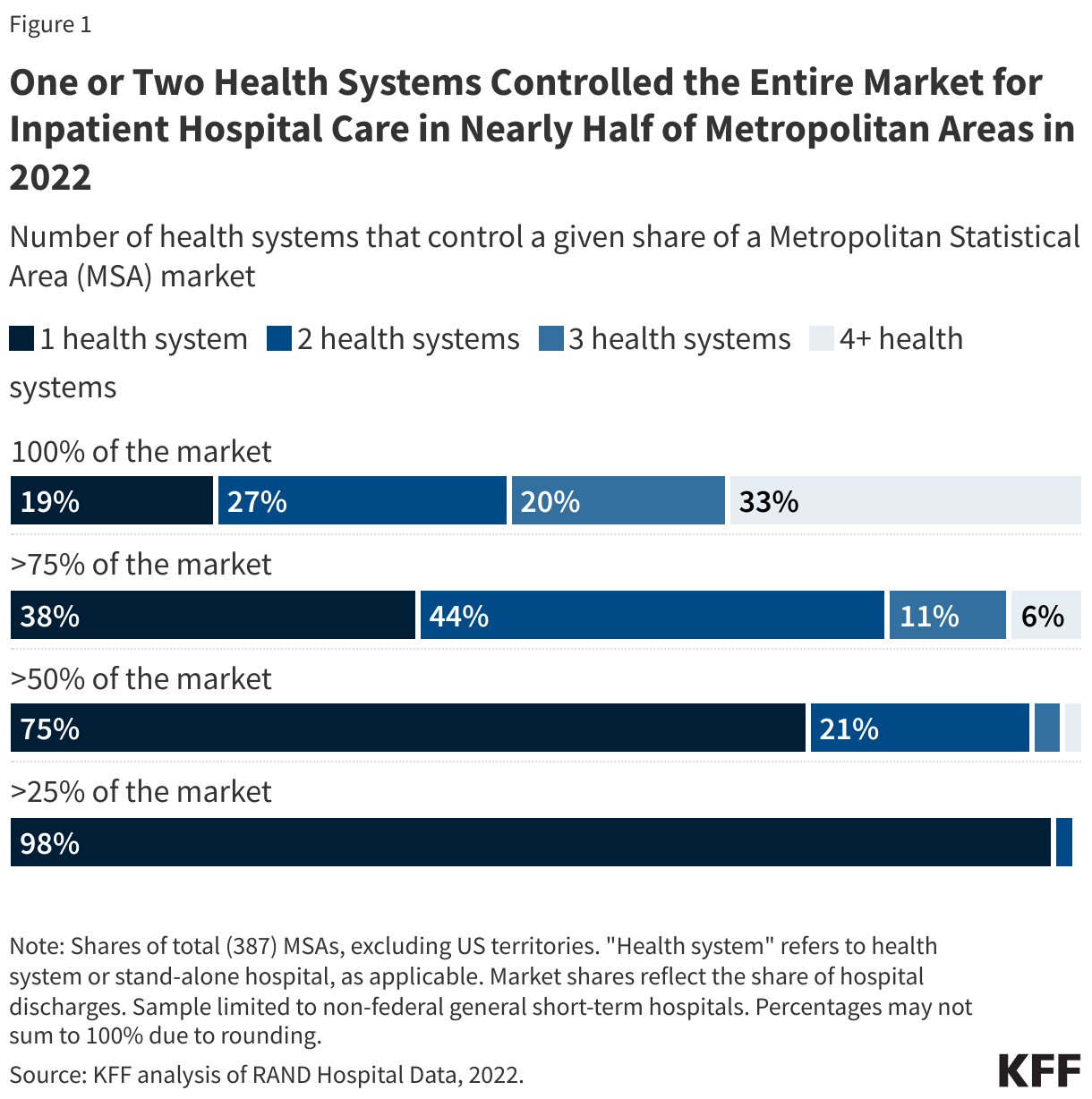
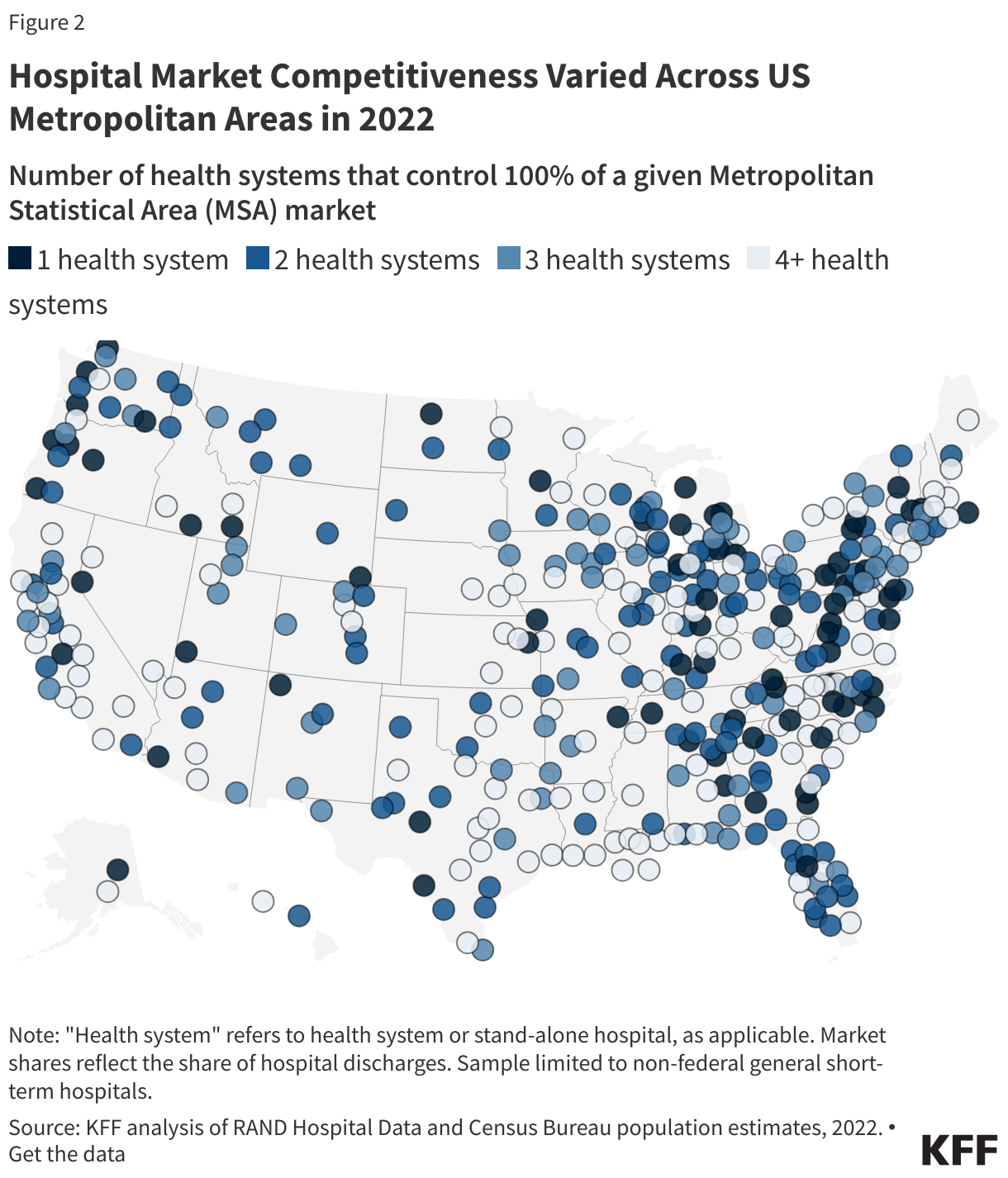
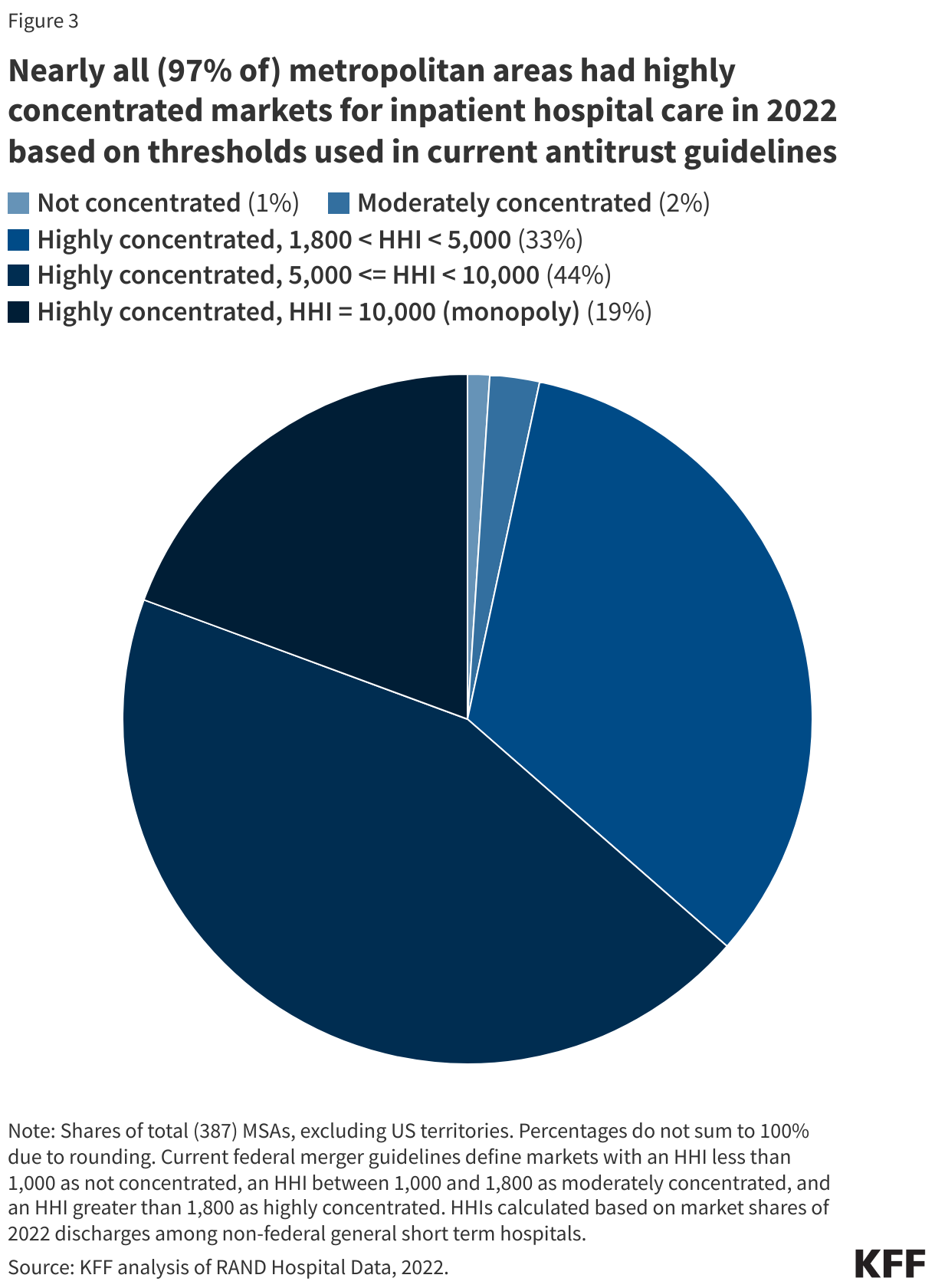
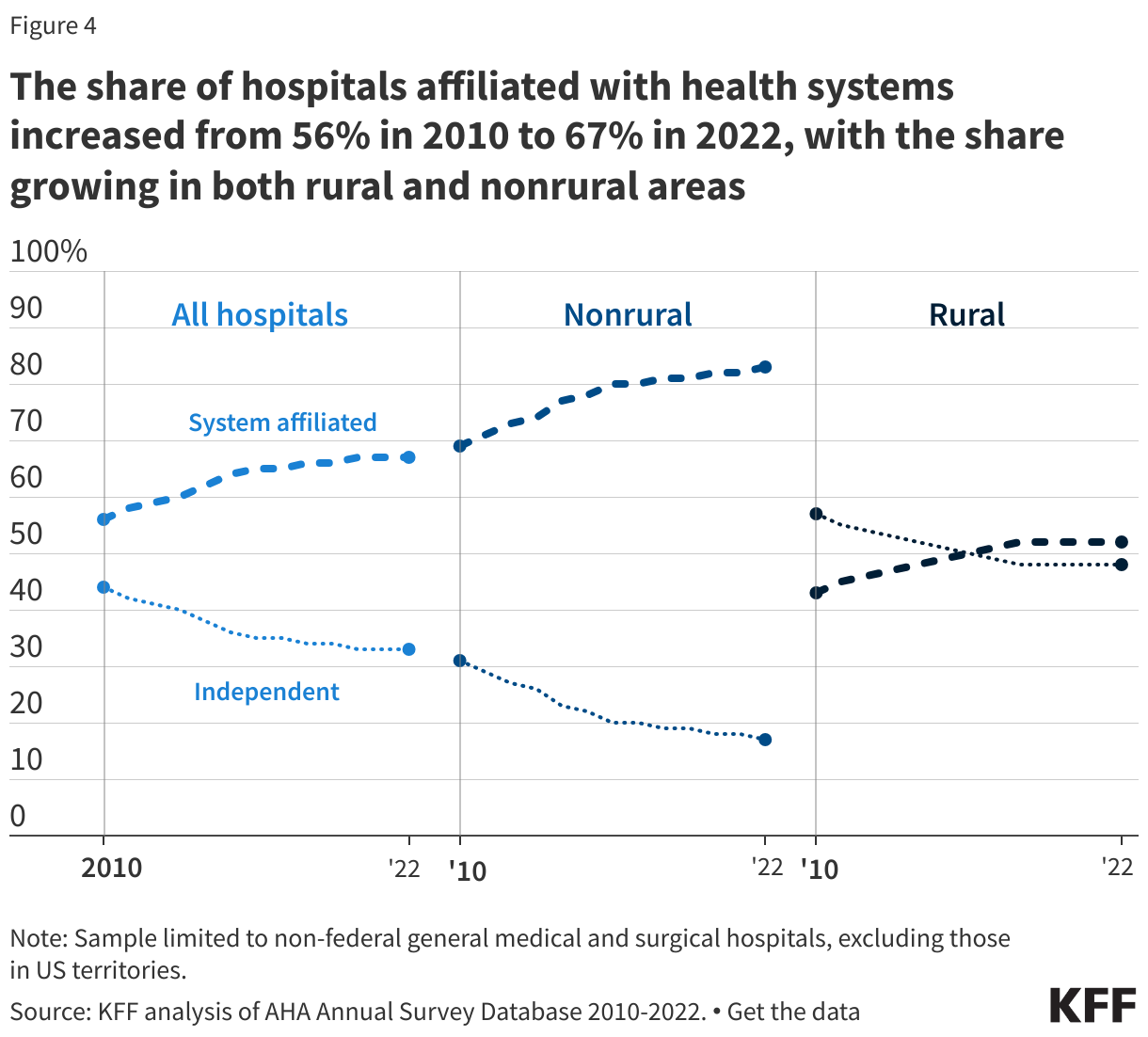


 Lindsey Dawson
Lindsey Dawson  Jennifer Kates
Jennifer Kates  Alex Montero
Alex Montero  Ashley Kirzinger
Ashley Kirzinger