Nearly 7 in 10 Medicare Beneficiaries Did Not Compare Plans During Medicare’s Open Enrollment Period
Issue Brief
Each year, people with Medicare can review their coverage options and change plans during the annual Open Enrollment Period (October 15 to December 7). Medicare beneficiaries with traditional Medicare can compare and switch Medicare Part D stand-alone drug plans or join a Medicare Advantage plan, while enrollees in Medicare Advantage can compare and switch Medicare Advantage plans or elect coverage under traditional Medicare with or without a stand-alone drug plan. Beneficiaries have no shortage of plans to choose from: in 2024, the average Medicare beneficiary can choose among 43 Medicare Advantage plans and 21 Part D stand-alone prescription drug plans (PDPs).
The marketplace of Medicare private plans operates on the premise that people with Medicare will compare plans during the open enrollment period to select the best source of coverage, given their individual needs and circumstances. Coverage and costs vary widely among both Medicare Advantage plans and Part D prescription drug plans and can change from one year to the next, which could lead to unexpected and avoidable costs and disruptions in care for beneficiaries who do not review their options annually. For example, changes in Medicare Advantage provider networks could mean beneficiaries lose access to their preferred doctors, while changes in the list of covered drugs and cost-sharing requirements could result in higher out-of-pocket drug costs. Further, beneficiaries’ health care needs can change from one year to the next. Even without a change made by their plan or a change in health status, beneficiaries may be able to find a plan that better meets their individual needs or lowers their out-of-pocket costs.
In focus groups conducted by KFF, Medicare beneficiaries highlighted many of these factors, including out-of-pocket costs, access to specific doctors, and coverage of prescription drugs, as important in choosing their Medicare coverage. Yet, Medicare beneficiaries also expressed difficulty understanding and comparing the various plan options and being overwhelmed by a barrage of television ads – mostly for Medicare Advantage plans.
In this analysis, KFF examines the share of Medicare beneficiaries who reviewed their coverage and compared plans during the 2021 open enrollment period for coverage in 2022, and who made use of Medicare’s official information resources, as well as variations by demographic groups, based on an analysis of the 2022 Medicare Current Beneficiary Survey (the most recent year available).
Key Takeaways
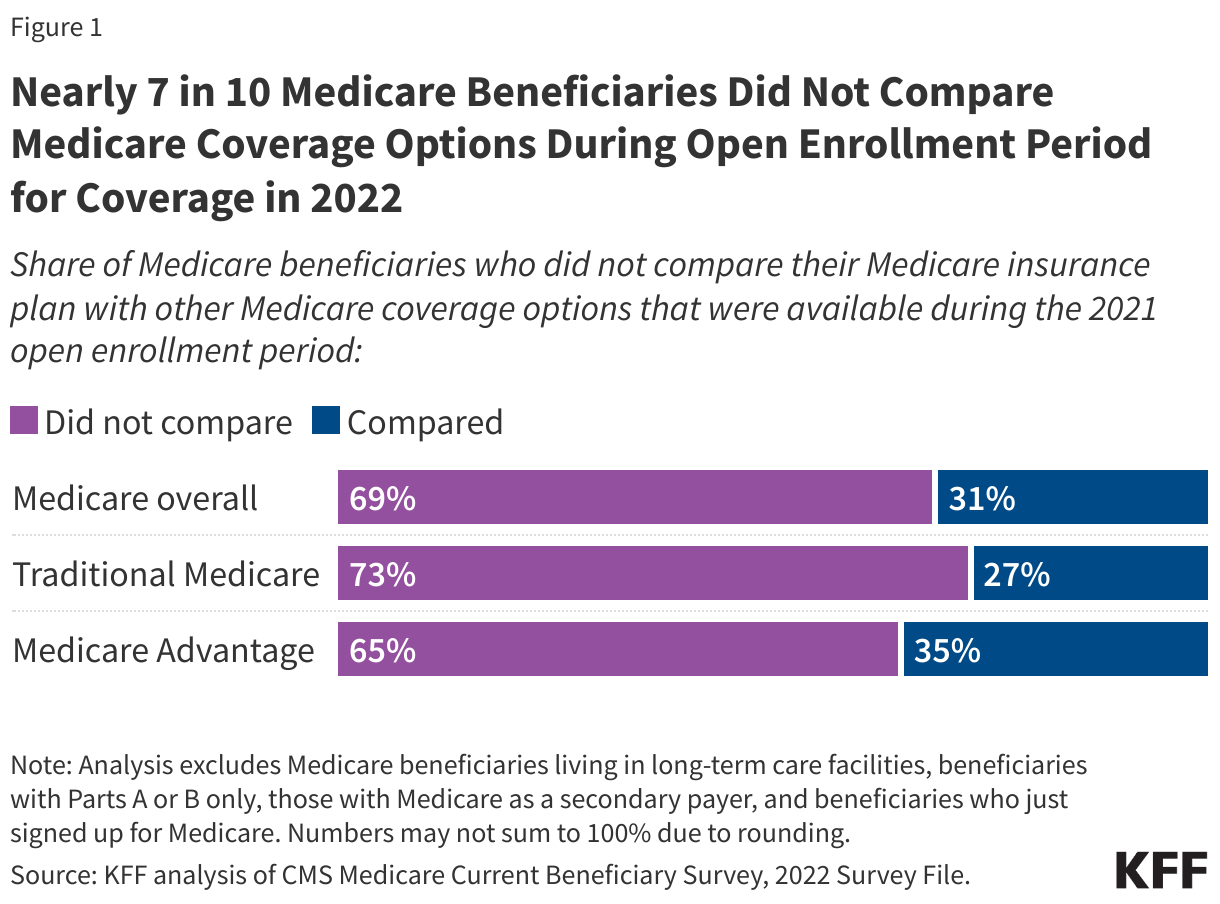
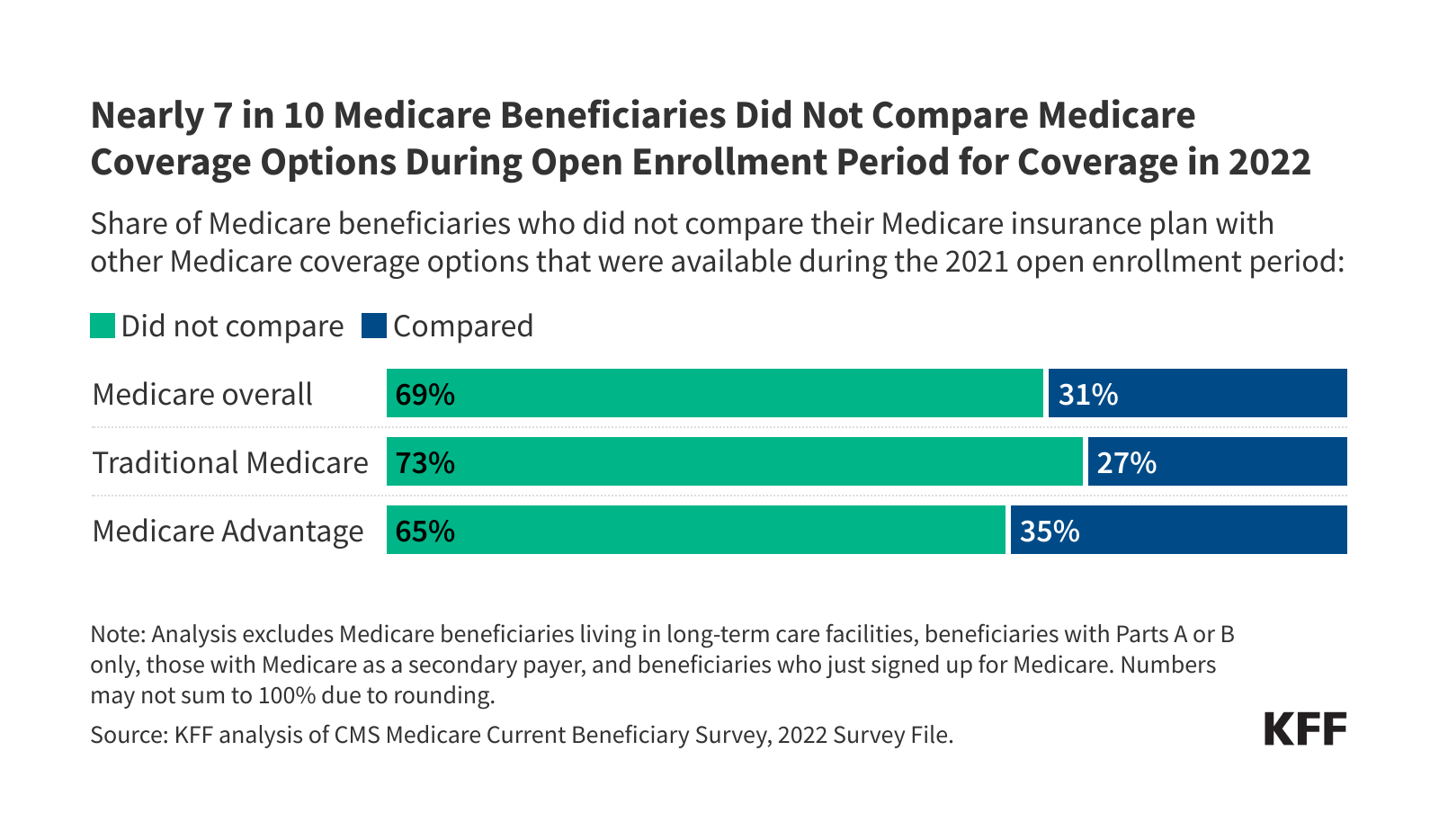
- Overall, nearly 7 in 10 (69%) Medicare beneficiaries did not compare their own source of Medicare coverage with other Medicare options offered in their area during the 2021 open enrollment period, while 31% did so. A larger share of beneficiaries in traditional Medicare than in Medicare Advantage did not compare their own source of coverage with other plans (73% vs 65%).
- Among Medicare Advantage enrollees, more than 4 in 10 (43%) did not review their current plan’s coverage to check for potential changes in their plan’s premiums or other out-of-pocket costs, while the remainder (57%) did so. A similar share (44%) did not review their current plan for potential changes in the kinds of treatments, drugs, and services that would be covered in the following year.
- Most enrollees in Medicare Advantage prescription drug plans (82%) and stand-alone prescription drug plan (PDPs) (69%) did not compare their plan’s drug coverage with drug coverage offered by other plans in their area.
- Medicare’s official information resources are used by half or fewer of Medicare beneficiaries, with just a quarter (26%) reporting calling the toll-free number, 4 in 10 (42%) reporting visiting the Medicare website, and slightly more than half (54%) reporting reading some or parts of the Medicare & You handbook.
Nearly 7 in 10 Medicare Beneficiaries Did Not Compare Medicare Coverage Options During the Open Enrollment Period for 2022
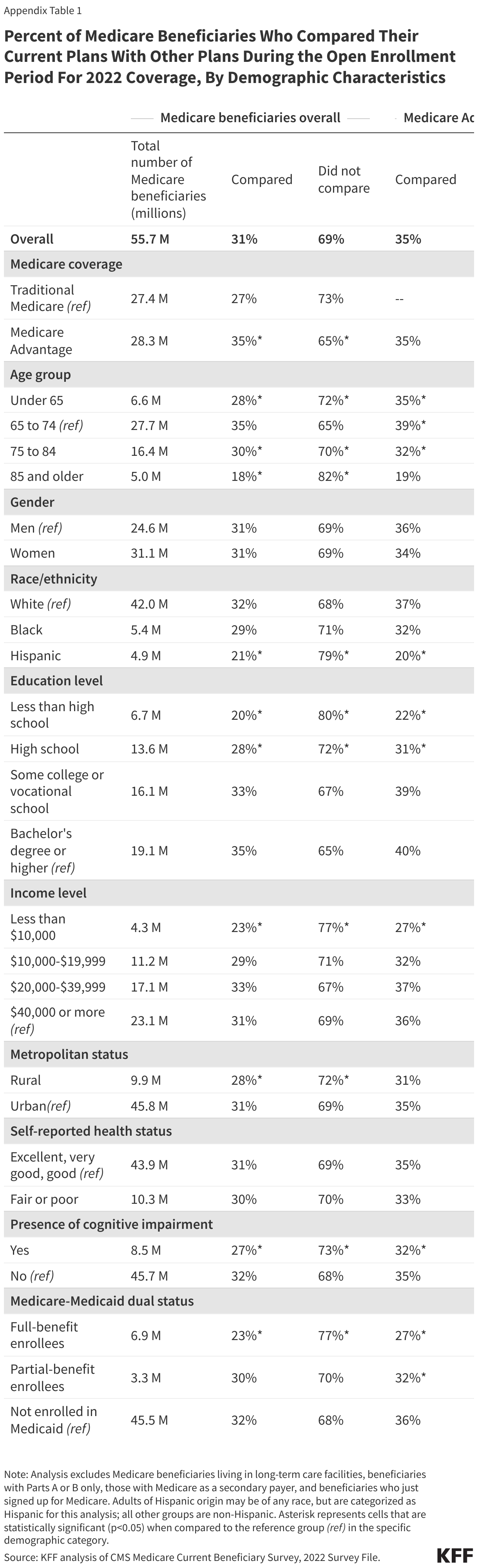
Overall, most (69%) Medicare beneficiaries reported that they did not compare their current Medicare plan to other Medicare coverage options that were available during the 2021 open enrollment period for coverage in 2022 (Figure 1, Table 1). Among Medicare Advantage enrollees, nearly two-thirds of enrollees (65%) did not compare coverage options for 2022, even though year-to-year changes in Medicare Advantage plans, such as changes in provider networks or prior authorization requirements can affect enrollees’ access to care.
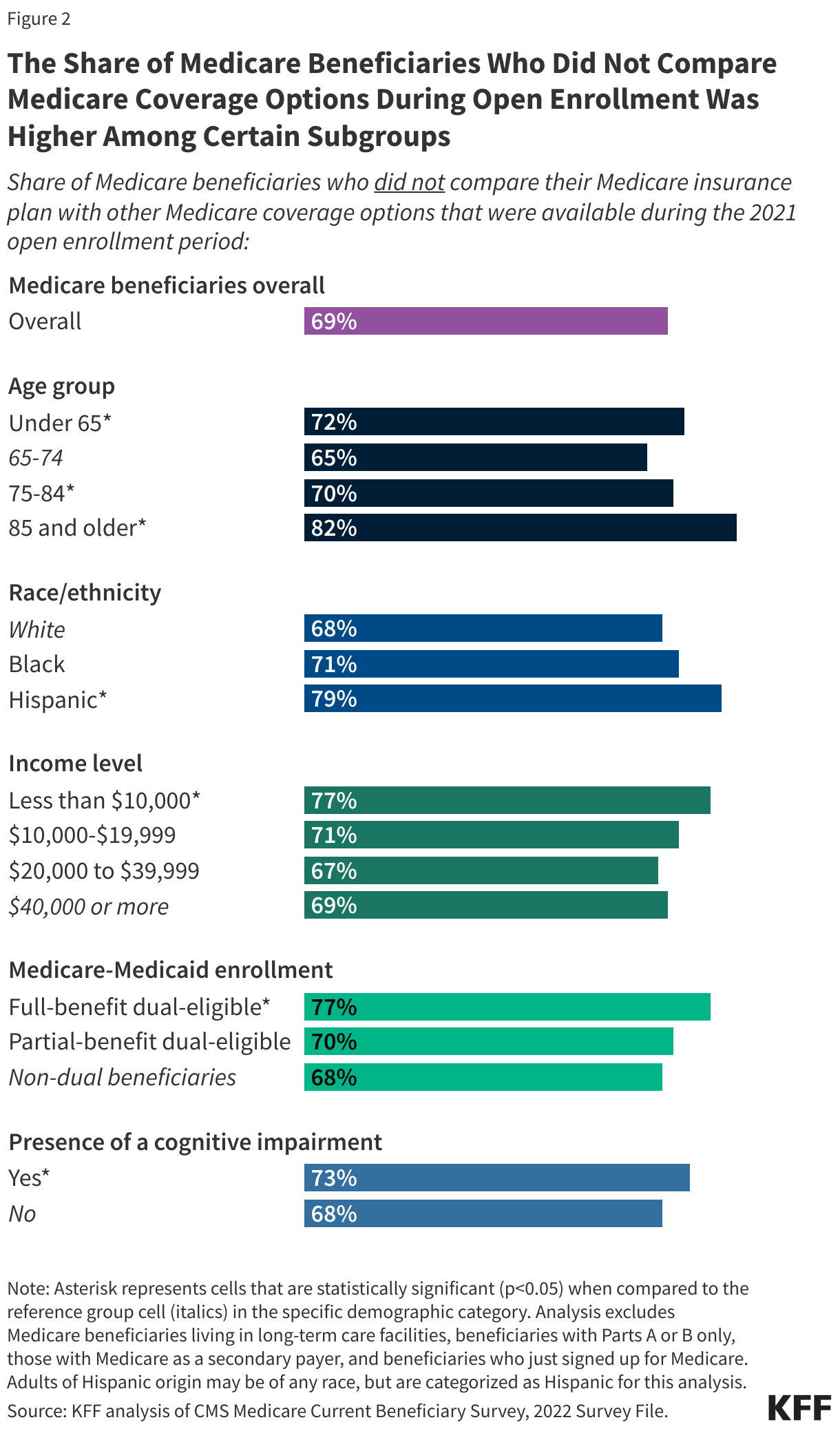
The share of Medicare beneficiaries who did not compare Medicare coverage arrangements was higher among certain subgroups, including beneficiaries with lower incomes and education levels, Hispanic beneficiaries, those dually-enrolled in Medicare and Medicaid, under age 65 with disabilities or ages 85 and older, and beneficiaries with a cognitive impairment (Figure 2, Appendix Table 1).
More Than 4 in 10 Medicare Advantage Enrollees Did Not Review Their Own Plan for Potential Changes in Covered Costs or Services for the Coming Year
For Medicare Advantage enrollees, premiums, cost sharing, and out-of-pocket limits can vary from year to year and across plans, with Medicare Advantage plans having the flexibility to modify cost sharing for most services, subject to limitations. Medicare Advantage plans may provide extra (“supplemental”) benefits that are not covered in traditional Medicare, but the type and scope of specific services often varies from one year to the next. Additionally, virtually all Medicare Advantage enrollees are in plans that impose prior authorization requirements for certain services, and these plans can alter the list of covered drugs, and broaden or narrow their network of physicians and other providers from one year to the next, subject to federal standards.
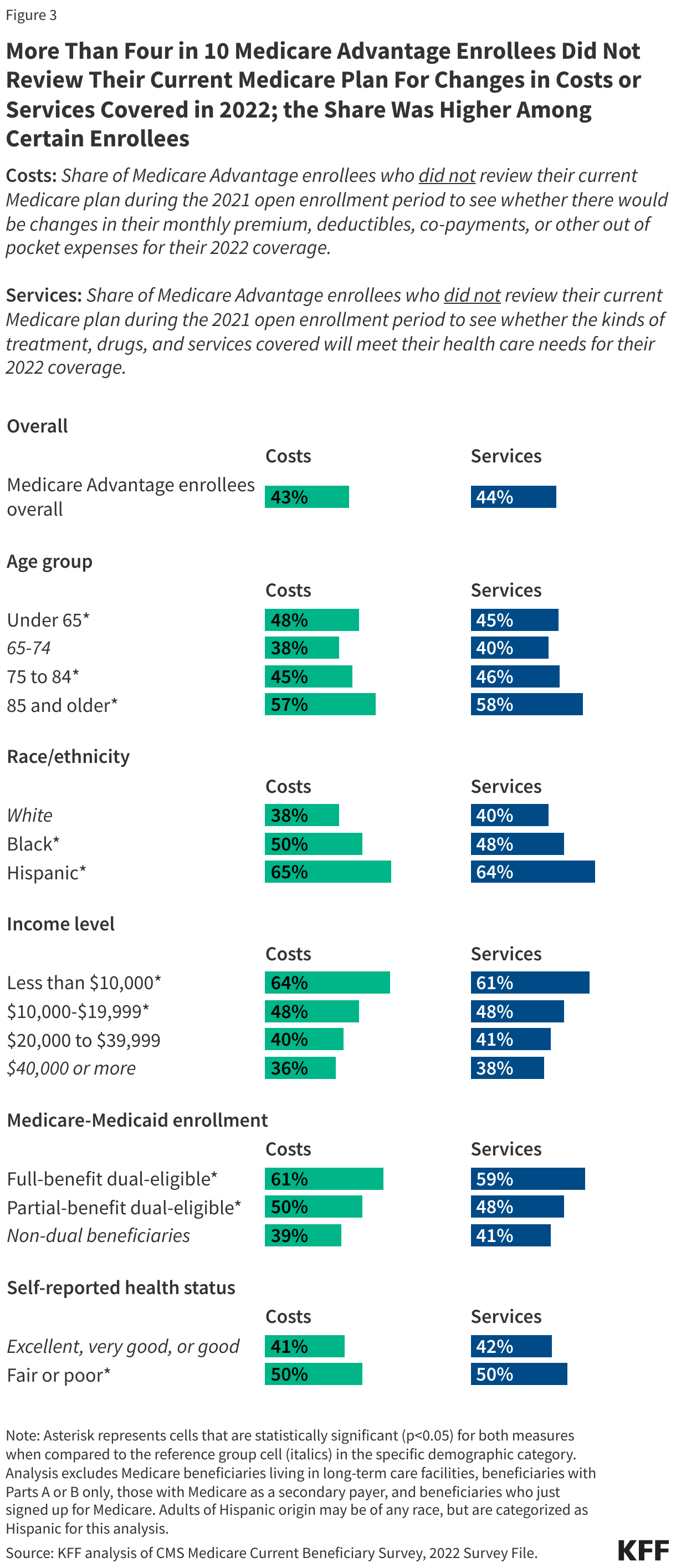
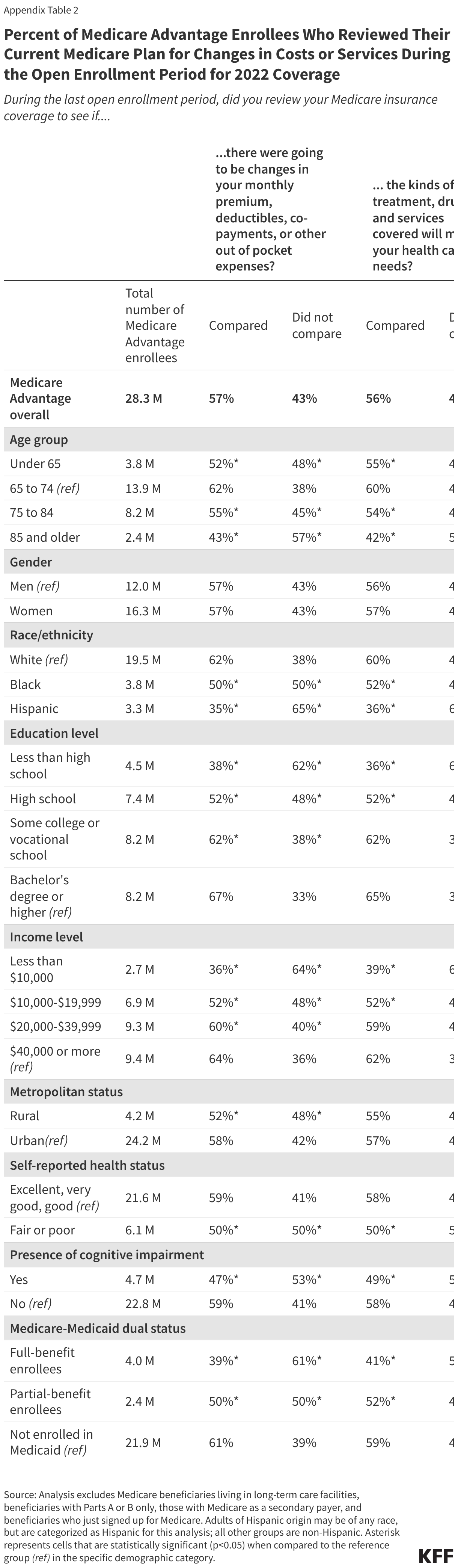
More than 4 in 10 (43%) Medicare Advantage enrollees did not review their current plan during the open enrollment period to see whether there would be changes for 2022 to their monthly premiums, deductibles, co-payments, or other out-of-pocket expenses, but the remaining 57% reported doing so (Figure 3, Appendix Table 2). Similarly, 44% of Medicare Advantage enrollees did not review their current plan for changes to the kinds of treatments, drugs, and services offered for their coverage in 2022.
The share of Medicare Advantage enrollees who did not review their own plan for changes in costs or services was higher among certain enrollees, including those with lower incomes and education levels, Black and Hispanic enrollees, individuals self-reporting fair or poor health, enrollees ages 85 and older, and those dually-eligible for Medicare and Medicaid coverage (Figure 3, Appendix Table 2).
For example, half of all Medicare Advantage enrollees reporting fair or poor health did not check to see if there was going to be a change in monthly premiums, deductibles or co-payments in their coverage, or any change in the kinds of treatments, drugs and services that would be covered. Nearly two-thirds of Hispanic (65%) and half of Black (50%) Medicare Advantage enrollees did not review their plan for changes in costs, with a similar pattern for changes in services (64% vs 48%, respectively). Additionally, nearly 60% of adults ages 85 and older did not review their plan for changes in costs (57%) or services (58%).
Most Medicare Beneficiaries with Part D Prescription Drug Coverage Did Not Compare Their Plan’s Drug Coverage to Other Drug Coverage Options
Part D plan costs, including premiums, deductibles, and cost-sharing requirements can change from year to year and vary by plan. Additionally, Part D plans can also modify their formularies, including adding or dropping drugs from coverage, and adding or modifying utilization management requirements that apply to specific drugs, such as prior authorization and step therapy.
The prescription drug provisions of the Inflation Reduction Act include changes that will lower out-of-pocket costs for all Part D enrollees, including a new $2,000 cap on out-of-pocket spending starting in 2025. In response to these changes, it is possible that Part D plan sponsors may make changes to plan premiums, formularies and cost sharing, making it particularly important for beneficiaries to compare their prescription drug options during open enrollment.
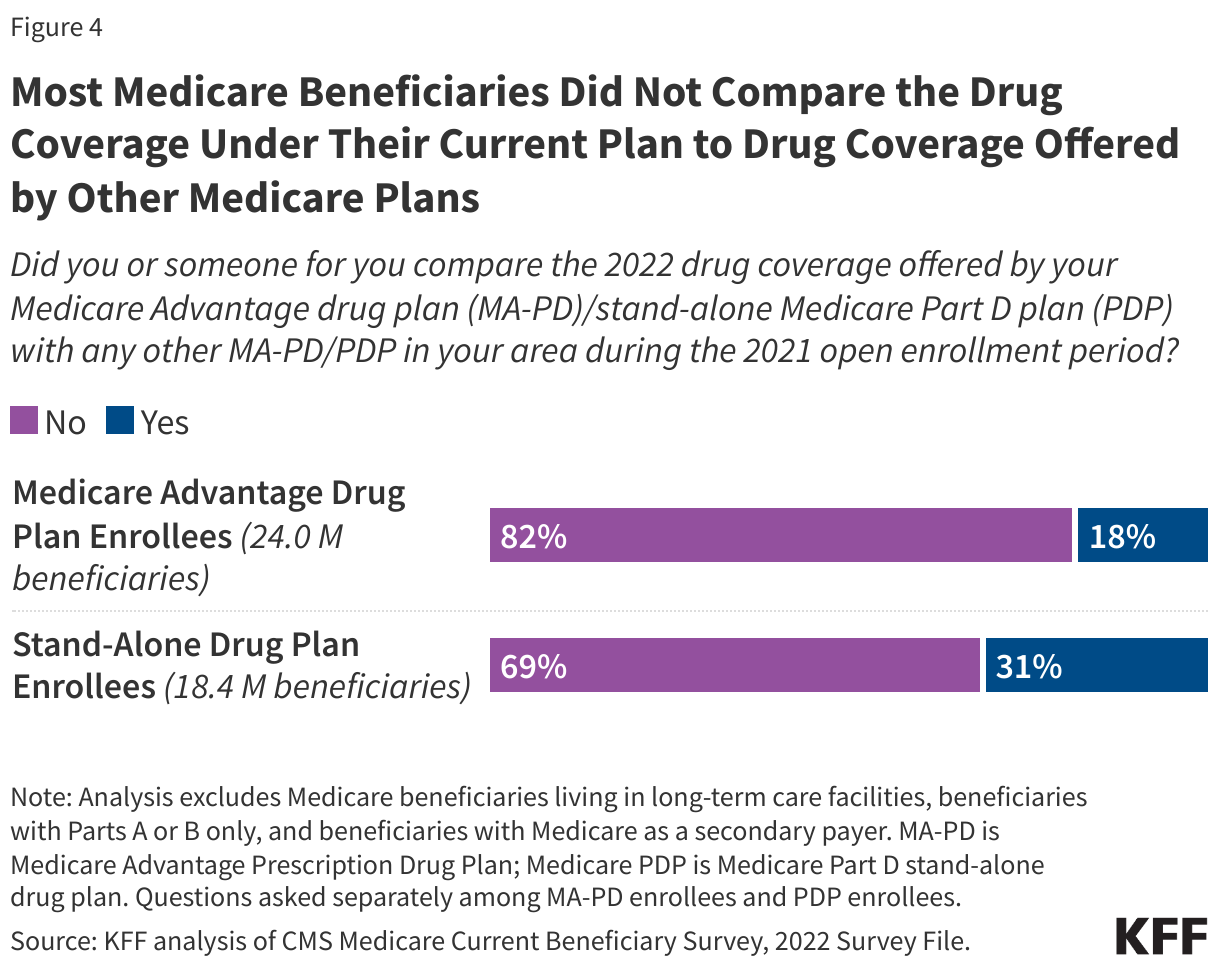
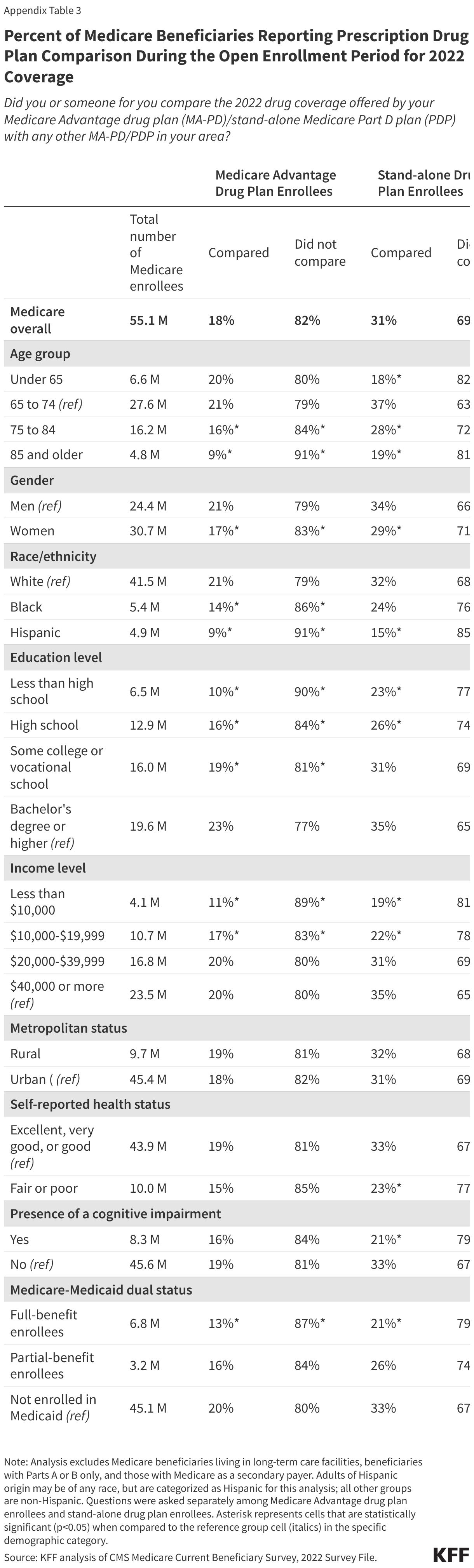
About 8 in 10 (82%) enrollees in Medicare Advantage plans with prescription drug coverage (MA-PDs) did not compare the drug coverage offered by their own MA-PD to other MA-PDs in their area during the 2021 open enrollment period (Figure 4; Appendix Table 3). Among stand-alone prescription drug plan (PDP) enrollees, a lower share, 69% of enrollees, said they did not compare drug coverage offered by their current PDP to other PDPs.
The share of beneficiaries with coverage under MA-PDs or PDPs who did not compare drug coverage offered for coverage in 2022 was higher among women, beneficiaries with lower incomes and education levels, Hispanic beneficiaries, beneficiaries ages 85 and older, and dual-eligible individuals (Appendix Table 3).
Medicare’s Information Resources Are Used by Half or Even Fewer Beneficiaries
Medicare provides information resources to help beneficiaries understand their Medicare benefits, coverage options, and costs, including the 1-800 Medicare toll free number, the Medicare.gov website, and the Medicare & You handbook that is provided each year to all Medicare beneficiaries. But these resources are not widely used, particularly the toll-free number (Figure 5, Appendix Table 4).
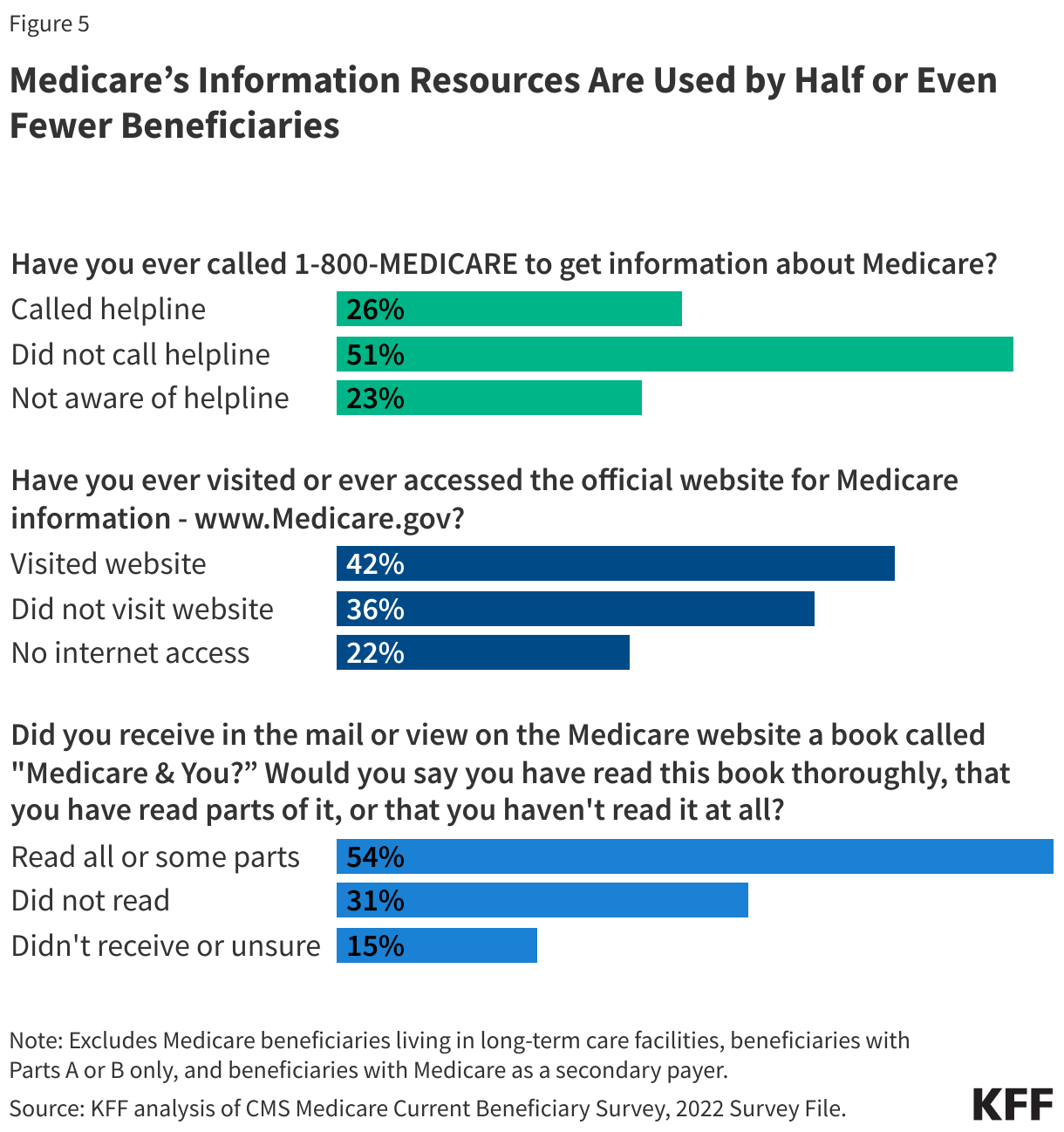
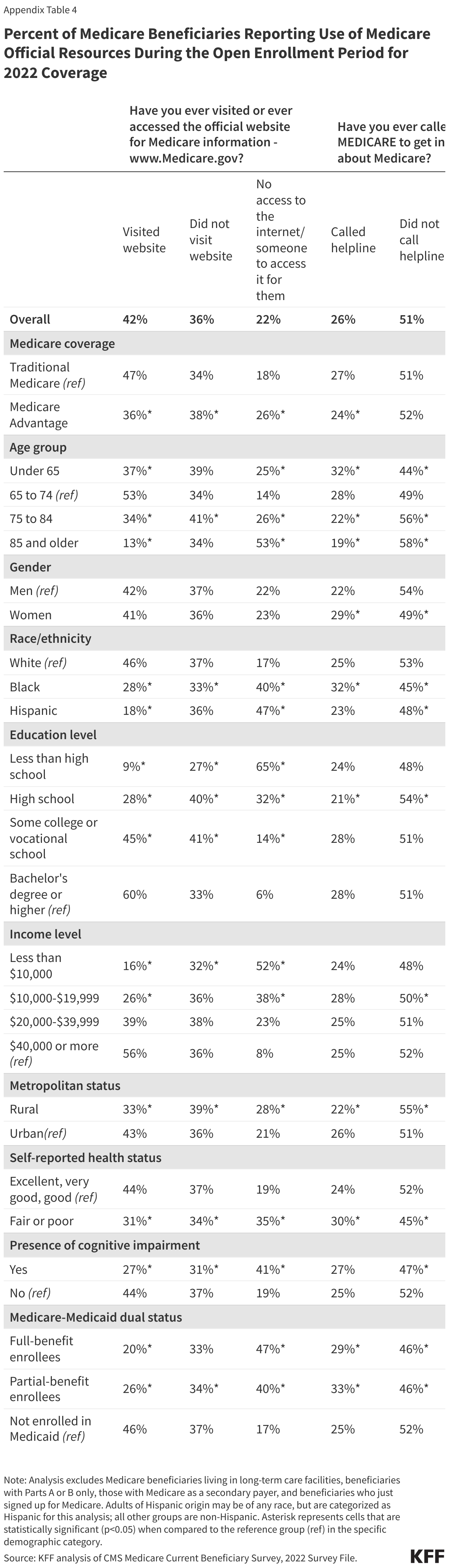
- About a quarter (26%) of Medicare beneficiaries reported calling the 1-800-MEDICARE helpline for information, but the remaining three-quarters (74%) of Medicare beneficiaries reported either never calling the helpline for information (51%) or being unaware that this helpline existed (23%).
- Four in 10 (42%) Medicare beneficiaries said they (or someone on their behalf) visited the official Medicare website for information, but more than half (58%) said they either never visited the website (36%) or they did not have access to the internet or had no one to access it for them (22%).
- More than half (54%) of Medicare beneficiaries reported that they had read the Medicare & You handbook (thoroughly or some parts of the handbook), but 46% reported that either they did not read the handbook (31%) or they did not receive it or did not know if they had received it (15%).
The share of Medicare beneficiaries who used Medicare information sources was lower among certain subgroups, including Black beneficiaries, individuals ages 75 to 84, and dual-eligible individuals (Appendix Table 4).
Methods
This analysis uses survey data for community-dwelling Medicare beneficiaries from the Centers for Medicare & Medicaid Services (CMS) Medicare Current Beneficiary Survey (MCBS) 2022 Survey File.
The analysis of 1) the share of beneficiaries who compared Medicare plans during the open enrollment period for 2022 coverage, 2) the share of Medicare Advantage enrollees who reviewed their current coverage for changes in costs or services, and 3) the share of beneficiaries who used Medicare’s official information sources used questions from the Medicare Plan Beneficiary Knowledge topical segment. This analysis was weighted to represent the ever-enrolled Medicare population in 2022 using the topical survey weight KNSEWT and relevant replicate weights. The analysis of the share of beneficiaries who compared Medicare plans and the share of Medicare Advantage enrollees who reviewed their current coverage for changes in costs or services excluded beneficiaries who reported just enrolling in Medicare.
The analysis of MA-PD/PDP drug plan comparison used questions from the Rx Medication topical segment; similar as above, the analysis was weighted to represent the ever-enrolled Medicare population in 2022 using the topical survey weight RXSEWT and relevant replicate weights.
Both analyses excluded beneficiaries with Part A or Part B only, those with Medicare as secondary payer, and those living in long-term care facilities. All reported differences in the text are statistically significant at p<0.05.
Appendix


 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma