5 Key Facts About Medicaid Eligibility for Seniors and People with Disabilities
Options under consideration in Congress to reduce Medicaid spending by nearly one-third in future years could have major implications for seniors and people with disabilities. Nearly 1 in 4 Medicaid enrollees are eligible for the program because they are ages 65 and older or have a disability, and they have higher per-enrollee costs than other enrollees. Within this group, there are multiple eligibility pathways, most of which are optional for states to cover, and all of which have more complex eligibility requirements than coverage for children and non-elderly adults. Proposals to limit federal spending on Medicaid may create incentives for states to drop or reduce their eligibility or coverage for seniors and people with disabilities in response to fewer federal revenues. Loss of Medicaid coverage poses unique challenges for seniors and people with disabilities, people who are likely to live on fixed incomes, have high health care spending, and rely on Medicaid for coverage of long-term care.
Considering the proposed reductions in Medicaid spending, this issue brief describes Medicaid eligibility pathways, enrollment, and spending among people eligible through the age and disability-related pathways (known as “non-MAGI” pathways because they do not determine eligibility based on Modified Adjusted Gross Income, as is the case for people covered under the Affordable Care Act Medicaid expansion and other groups). This analysis uses the most recent data available to KFF at the time of the analysis (Medicaid T-MSIS data, 2021, see Methods).
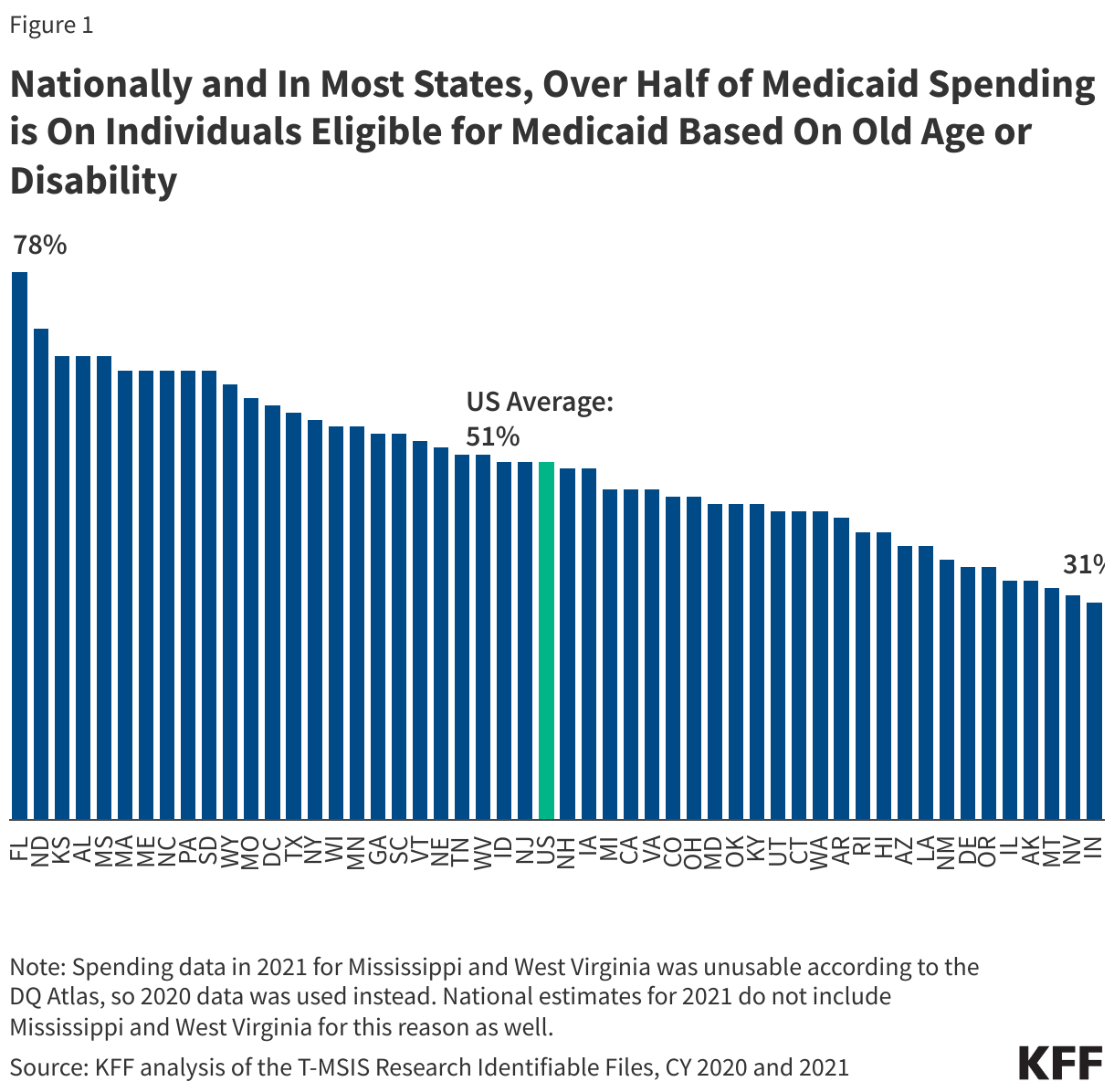
1. Over half of Medicaid spending is on people eligible for Medicaid because of old age or disability.
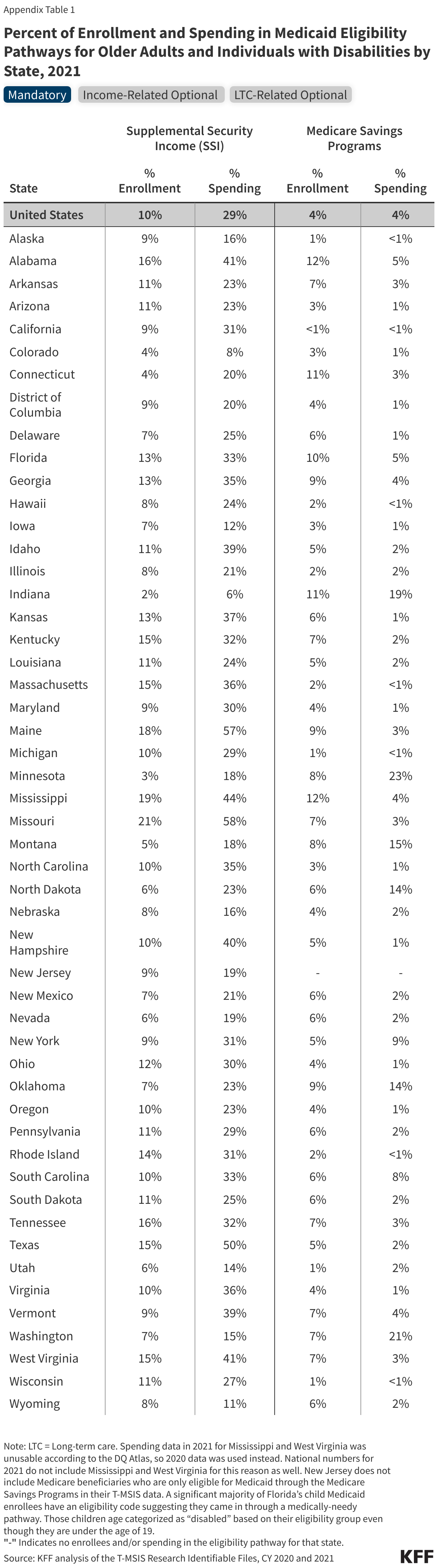
Over half of Medicaid spending ($339 billion in 2021) pays for care for people eligible through the non-MAGI pathways (Figure 1). Seniors and people with disabilities often have higher health care costs than other enrollees due to more complex health care needs, higher rates of chronic conditions and being more likely to utilize long-term care. There is significant state variation in the percentage of Medicaid spending that pays for non-MAGI enrollees (Appendix Table 1). In some states (Alaska, Nevada, Montana, Illinois and Indiana), only a third of spending went to these populations, and in five states (Alabama, Florida, Kansas, Mississippi, and North Dakota), care for seniors and people with disabilities accounted for at least two-thirds of spending (Figure 1). Differences in the percentage of spending across the states stem from differences in eligibility criteria for both MAGI and non-MAGI eligibility pathways, which also affects relative levels of enrollment in these pathways, as well as demographic variation across states.
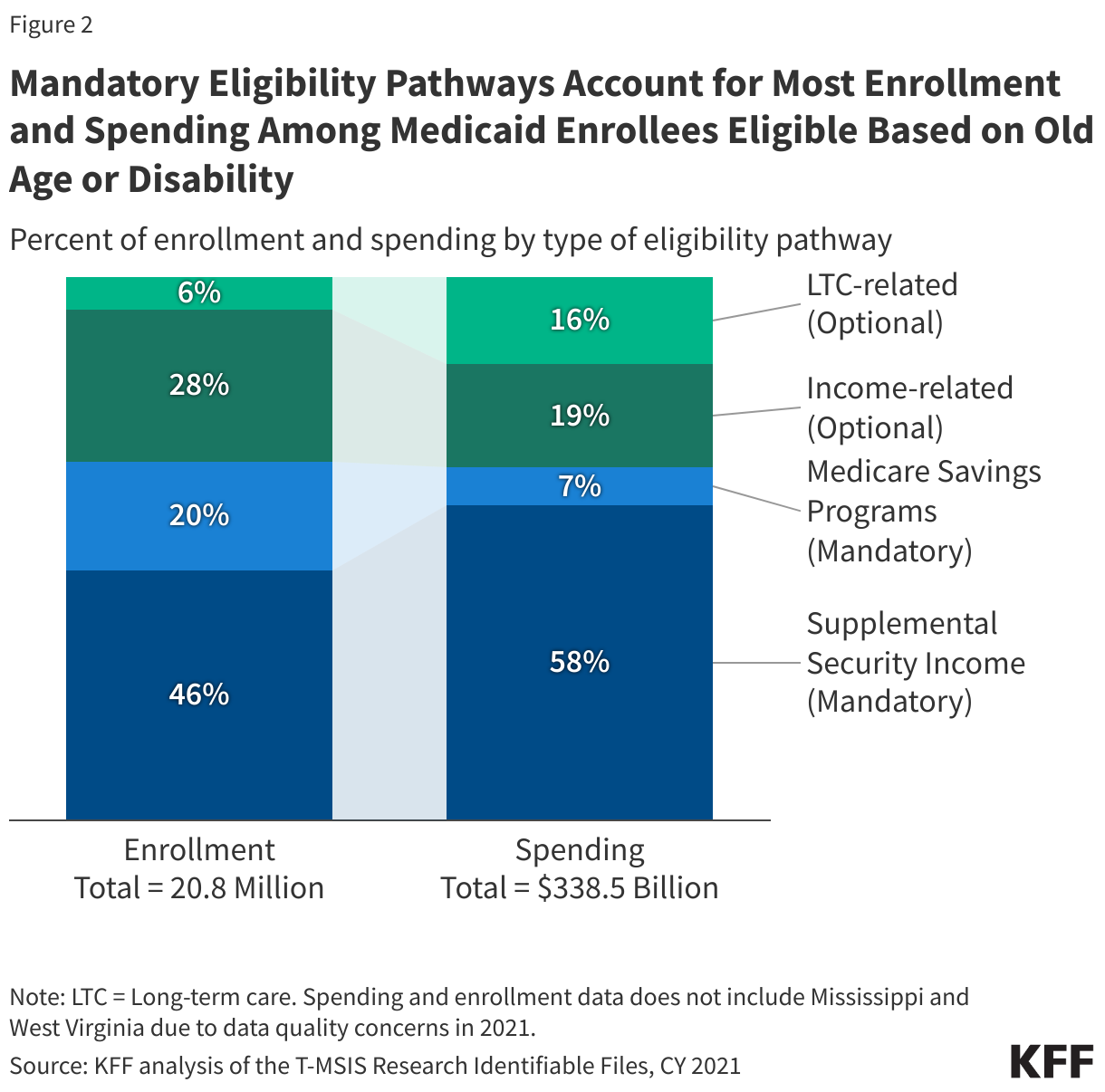
2. Most non-MAGI Medicaid enrollees are eligible through mandatory eligibility pathways that are tied to Medicare and Supplemental Security Income.
Federal statutes require states to enroll people who receive Supplemental Security Income (SSI) in Medicaid and to enroll eligible Medicare beneficiaries in the Medicare Savings Programs. SSI is a disability program that provides monthly income to people who are unable to work on account of a disability and who have income and financial resources below federal limits. The Medicare Savings Programs provide Medicaid coverage of Medicare premiums and in most cases, cost sharing to Medicare beneficiaries with limited financial resources. People who are eligible for the Medicare Savings Programs, but not full Medicaid, only receive Medicaid coverage for the costs of Medicare premiums and usually, cost sharing. Beyond these two “mandatory” eligibility pathways, there are optional Medicaid eligibility pathways that states may choose to offer for people who have disabilities or are ages 65 and older, including options to expand coverage beyond what is required under federal law to low-income seniors and people with disabilities and coverage for people who need long-term care.
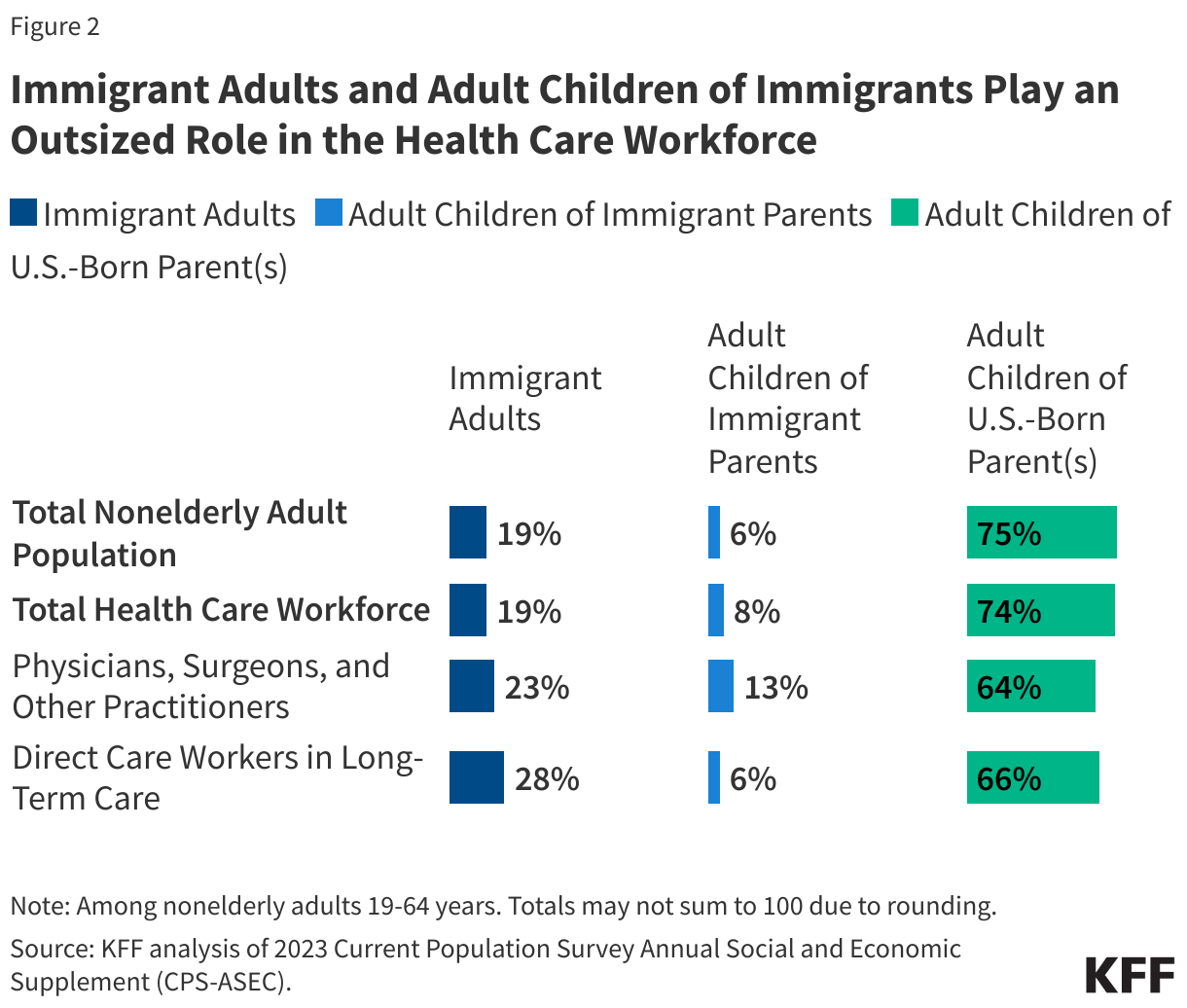
Roughly two-thirds of Medicaid enrollees who qualify based on old age or disability are eligible for Medicaid through a mandatory pathway and those enrollees account for about two-thirds of Medicaid spending on non-MAGI enrollees (Figure 2). The remaining third of enrollees includes people coming in through optional income-related pathways (28% of all non-MAGI enrollees and 19% of spending) and those coming in on account of their need for long-term care (6% of enrollees, 16% of spending).
Most seniors and people with disabilities who are eligible for non-MAGI Medicaid must demonstrate limited financial resources and go through an application process that requires documentation of their income and savings (Table 1). States that offer eligibility based on long-term care have higher income eligibility criteria for those eligibility pathways, but nearly all still require applicants to demonstrate having limited savings ($2,000 for an individual, $3,000 for a couple). Some assets, including the home, are excluded from the calculation of financial resources, but states are required to recoup the certain Medicaid costs after enrollees die through a process known as estate recovery. States that offer eligibility for seniors and people with disabilities based on income, have income limits generally little more than the federal poverty level with similarly low thresholds for applicants’ savings; and most states have more complicated eligibility processes for non-MAGI pathways than they do for MAGI pathways.

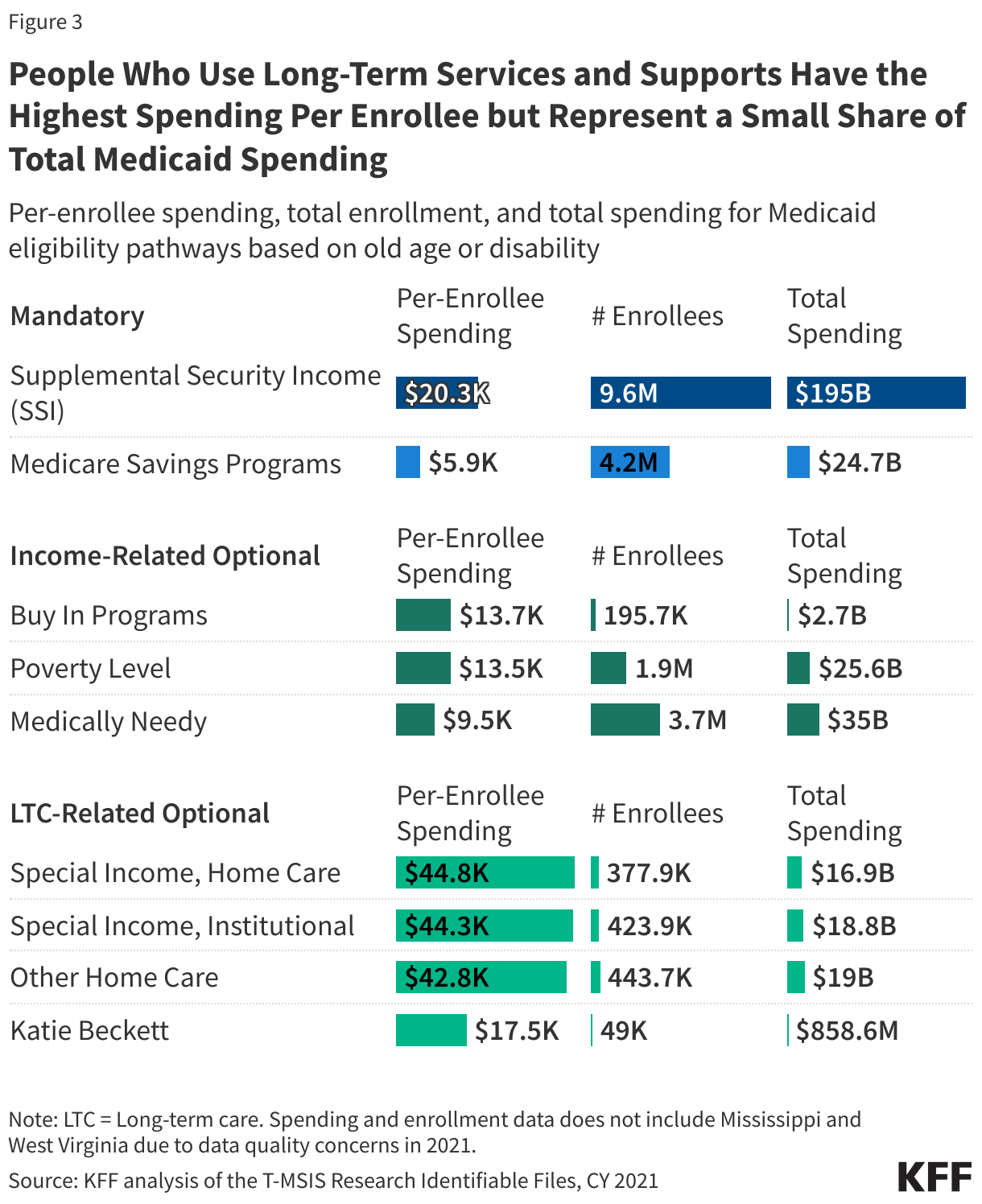
3. Enrollees eligible because they need long-term care have much higher spending per enrollee.
Among the four eligibility pathways specifically for people who use long-term care, per-enrollee spending is over $40,000 per year for three of the pathways (Figure 3). Per-enrollee spending for children with disabilities enrolled through Katie Beckett programs (which include Family Opportunity Act options too) is more similar to that of other eligibility pathways for seniors and people with disabilities (close to $20,000 per year) because many of those children also have private health insurance. In such cases, Katie Beckett coverage helps lower- and middle-income families cover the costs of long-term care for children, which are very difficult to save for. Although per-enrollee costs for people eligible through the long-term care pathways are high, they still represent a small share of total Medicaid spending because the number of people enrolled is so low.
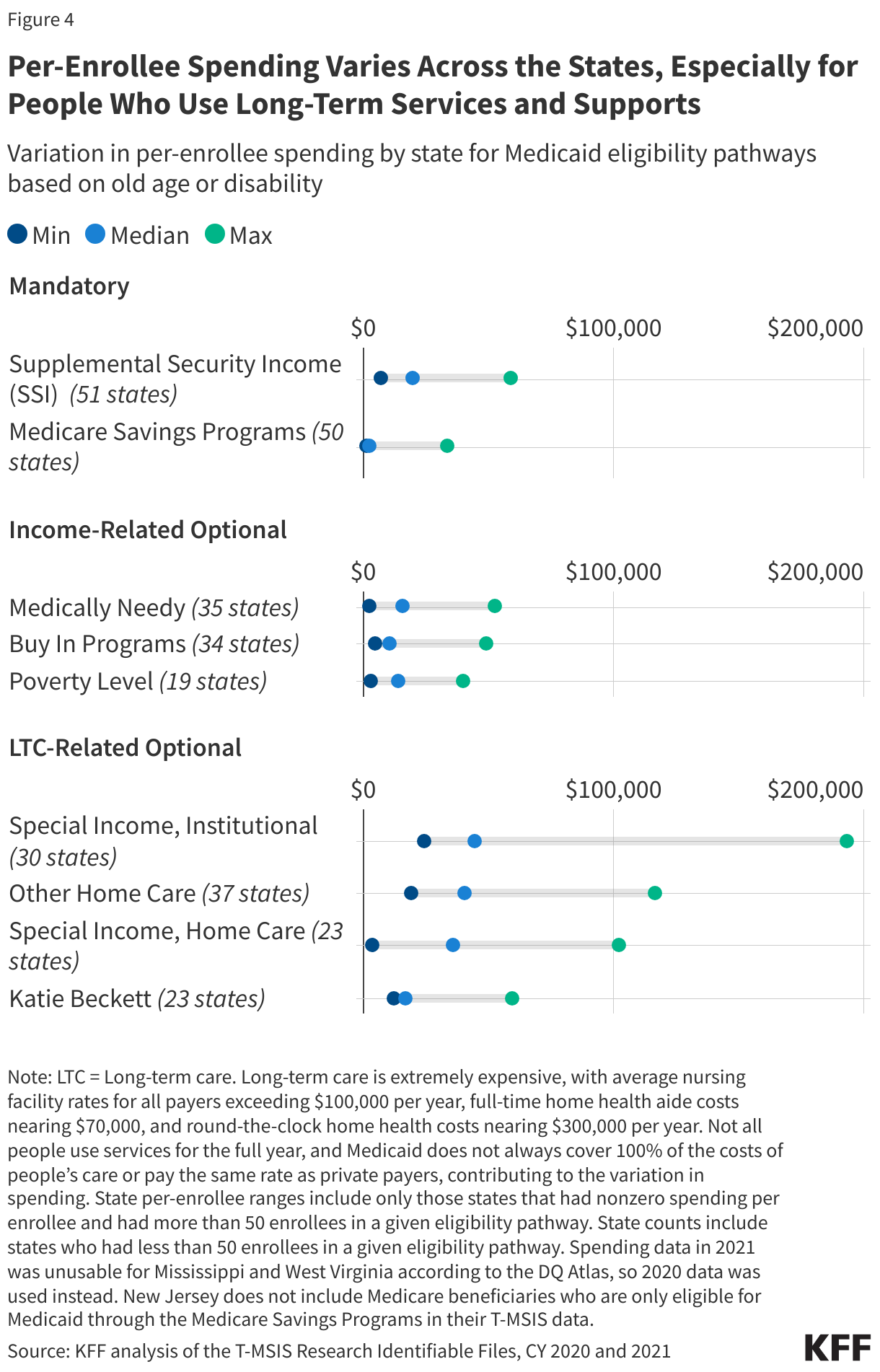
4. Per-enrollee spending varies across states, especially for enrollees who use long-term care.
For mandatory and income-related optional eligibility pathways, per-enrollee spending (including all services) varies from under $2,000 per enrollee to over $33,000 per enrollee for the Medicare Savings Programs and nearly $60,000 per enrollee for the SSI eligibility pathway (Figure 4). As large as that variation is, variation for the long-term care-related pathways is far greater: Variation in per-enrollee spending for people who use institutional care ranges from $24,000 to nearly $200,000 per year in Alaska. For people eligible through one of the two home care programs, per-enrollee spending ranges from about $3,000 to well over $100,000. in Washington, D.C. (Appendix Table 2).
The large variation in spending among the long-term care related pathways reflects states having considerable flexibility in determining who is eligible to receive optional benefits, what services to provide, and how much to pay providers. Long-term care is extremely expensive, with average nursing facility rates for all payers exceeding $100,000 per year, full-time home health aide costs nearing $70,000, and round-the-clock home health costs nearing $300,000 per year. Not all people use services for the full year, and Medicaid does not always cover 100% of the costs of people’s care or pay the same rate as private payers, contributing to the variation in spending. There is little information about how much states pay providers, but a KFF survey about payment rates for home care showed significant variation among states able to report. The Biden Administration finalized regulations that would require states to report payment rates for Medicaid, but Congress or the Trump administration may seek to undo that rule.
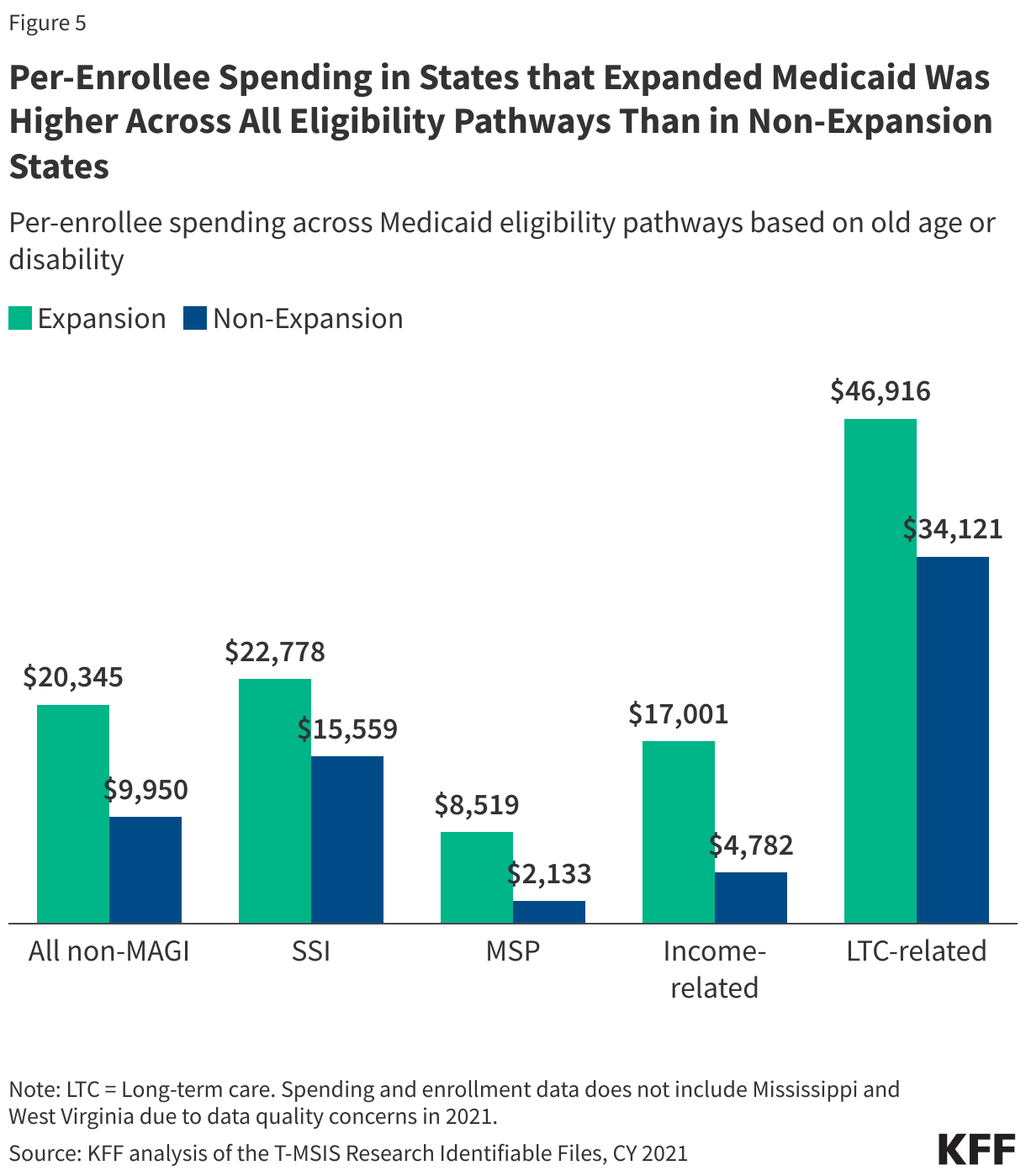
5. Across all non-MAGI eligibility pathways, per-enrollee spending is higher in ACA expansion states.
Although some researchers have criticized the ACA eligibility pathway as diverting resources away from Medicaid enrollees with disabilities, the data show per-enrollee spending for seniors and people with disabilities is two times larger in expansion states ($20,345 versus $9,950, Figure 5). The largest difference in per-enrollee spending stems from people eligible through optional income-related pathways, where spending is $17,000 per enrollee per year in expansion states but less than $5,000 per year in non-expansion states. Even in mandatory pathways, expansion states spent more per enrollee: Expansion states spent $6,386 more per enrollee eligible through the Medicare Savings Program pathway, and $7,219 more per enrollee through the SSI pathway.
Appendix Tables

Methods
Data: Data are from the 2021 and 2020 T-MSIS Research Identifiable Demographic-Eligibility and Claims Files (T-MSIS data). This analysis includes all Medicaid-eligible enrollees, with either full or partial benefits.
State Inclusion Criteria: National estimates include enrollees living in 48 states and DC and exclude residents in the U.S. territories. West Virginia and Mississippi enrollees were not included in the national estimates due to unusable data in 2021, according to the DQ Atlas. However, their reported state-level data in figures 1 and 4, and in the appendix tables, was calculated using 2020 T-MSIS data.
Medicaid non-MAGI eligibility pathways: Eligibility pathways for older adults and individuals with disabilities were identified using ELGBLTY_GRP_CD_LTST in the T-MSIS demographic-eligibility file.
Eligibility pathways for older adults and individuals with disabilities:
Supplemental Security Income (SSI) with values of 11-22, 37, 38, 40, 41
Medicare Savings Program (MSP) with values of 23-26.
Buy In Programs with values of 47, 48, 49.
Poverty Level with values of 46.
Medically Needy with values of 53-56, 59, 60.
Other Home Care with values of 39, 43, 51.
Special Income, Institutional with a value of 42.
Special Income, Home Care with a value of 52.
Katie Beckett with values of 45, 50.
Missingness: Approximately 0.36% (N=334,091) of Medicaid enrollees were missing a value for ELGBLTY_GRP_CD_LTST, representing 0.29% ($1.9 billion) of Medicaid spending, and were thus not included in this analysis.
Spending: Spending was calculated by summing the total Medicaid paid amount on all claims for each Medicaid-eligible enrollee with the desired ELGBLTY_GRP_CD_LTST code in the T-MSIS claims files.


 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma