KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Since 1970, the federal government has been funding Title X, a national grant program to support the delivery of family planning services to low-income individuals. On March 4, 2019, the Trump Administration finalized new regulations that made major changes to the program, which recently granted $255 million to fund approximately 4,000 clinics and service sites across the country. These new regulations prohibit any sites that receive Title X from providing abortion referrals, mandate referrals to prenatal services for all pregnant patients, and require complete financial and physical separation from abortion services. (Title X funds have never been permitted to be used to pay for abortions.) These regulations are a significant departure from the regulations that were in place, but mirror Reagan-era regulations that were upheld by the Supreme Court in Rust v Sullivan in 1991 but never fully implemented. Nonetheless, these new regulations are being legally challenged through 8 lawsuits representing 23 States and provider organizations (including the American Medical Association and Planned Parenthood). While several of the Federal District Courts hearing the cases initially issued preliminary injunctions blocking the implementation of the regulations, the 9th Circuit Court of Appeals ruled that the regulations can be implemented as the cases make their way through the courts.
Effective July 15, 2019, Title X projects can no longer provide abortion referrals and must refer all pregnant clients to prenatal care services regardless of their wishes. OPA required all grantees to submit a compliance plan by August 19, 2019, documenting the steps they will take to change their programs to comply with the final rule and have stated they will respond with questions two weeks after that date. While financial separation of all abortion services from other family planning services has been required in the past, effective March 4, 2020, all clinics must have full physical separation from abortion services and other grantees and providers may opt to leave after that date. This data note provides estimates of the status of the Title X network as of September 20, 2019. Grantees and sub-recipients are continuing to make decisions about their participation in the Title X program. The most up-to-date information on the status of the Title X network can be found on this interactive map.
Over one in five Title X sites will no longer be using program funding
The HHS Office of Population Affairs operates the Title X program and funds “grantees” (health care organizations, state health departments, or non-profits) that apply to oversee the distribution of federal dollars to safety-net clinics (sub-recipients) and other sites to provide family planning services to low-income, uninsured, and underserved clients. In 2019, OPA funded 90 grantees that supported approximately 4,000 clinics nationwide, including specialized family planning clinics such as Planned Parenthood centers, primary care providers such as federally qualified health centers (FQHCs), and health departments, school-based, faith-based, and other private nonprofits.
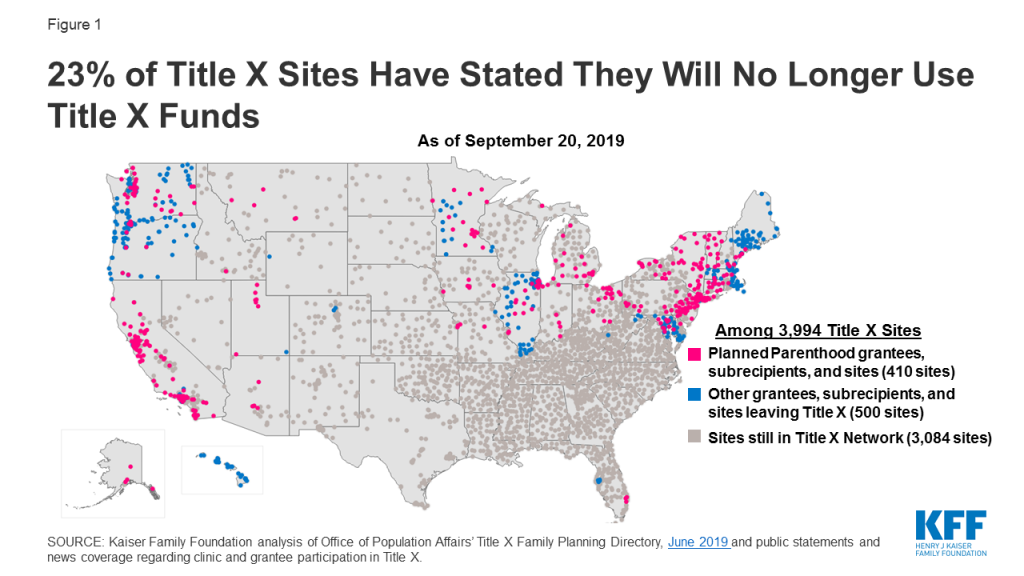
On August 19, 2019, Planned Parenthood informed OPA that all Planned Parenthood direct grantees and Planned Parenthood sub-grantees will withdraw from the Title X program. All eight direct Planned Parenthood grantees in the Title X program and the majority of sub-recipients have exited the program, while some sub-recipients are still in the process of withdrawing (Figure 1). The Planned Parenthood grantees that have withdrawn include: Planned Parenthood of Great Northwest and the Hawaiian Islands (Alaska), Planned Parenthood of Southern New England, Inc. (Connecticut), Planned Parenthood of Great Northwest and the Hawaiian Islands (Idaho), Planned Parenthood of Illinois (Illinois), Planned Parenthood of Minnesota, North Dakota, South Dakota (Minnesota), Planned Parenthood of Northern New England (New Hampshire), Planned Parenthood of Greater Ohio (Ohio), and Planned Parenthood of Utah (Utah).
Figure 1: 23% of Title X Sites Have Stated They Will No Longer Use Title X Funds
In Utah, Planned Parenthood is the only Title X grantee in the state and in Alaska, Connecticut, and Minnesota, Planned Parenthood is the largest Title X grantee.
In addition to Planned Parenthood, numerous grantees and sub-recipient clinics and networks have announced they will no longer use Title X funds (Table 1). These grantees have said that the new rules would require them to deny individuals needed care and accurate information to make informed medical decisions. In total, 23% of sites that were receiving Title X funds will no longer use Title X funds.
Table 1. Planned Parenthood sites by state and Title X grantees, sub-recipients, or sites that will no longer use Title X funds
State
Grantee or Sub-recipient Site
Number of Clinics
Alaska
Planned Parenthood of Great Northwest and the Hawaiian Islands (grantee)
Washington State Department of Health (only grantee in state)
93
West Virginia
Planned Parenthood site
1
Women’s Health Center of WV Inc. (service site of West Virginia Department of Health and Human Services)
1
Wyoming
Teton County Family Planning Clinic (service site of Wyoming Health Council)
1
NOTES: Planned Parenthood grantees, sub-recipients, and service sites are withdrawing from the Title X program; *HI has not officially withdrawn from the program but is not using Title X funds pending the outcome of the current lawsuit. **Located in KS, but a sub-recipient of Missouri Family Health Council, IncSOURCE: This analysis is based on KFF analysis of the June 2019 listing of Title X sites available from the HHS Office of Population Affairs and public statements and news coverage regarding clinic and grantee participation in Title X.
The loss of Title X funding will likely create access barriers to quality family planning services across the country and few new grantees have joined the program to take their place
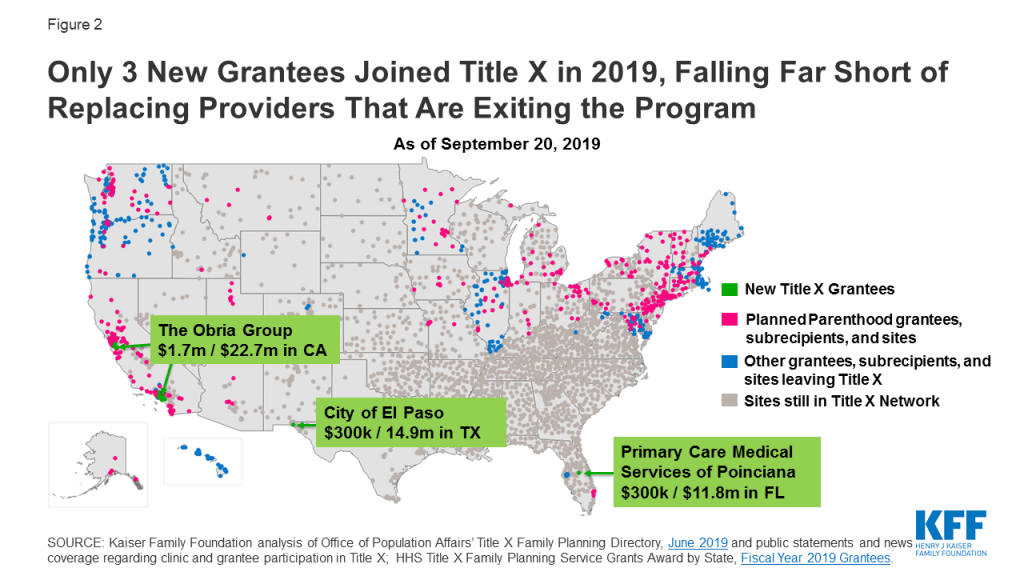
One of the Trump Administration’s aims with the new Title X regulations is to encourage participation by “non-traditional” organizations and broaden the network, but there have been very few additions to the Title X network of sites and grantees (Figure 2). Only three new grantees were added to the program as of April 1, 2019. One of the new grantees is the Obria Group, a Christian organization based in Southern California that does not provide contraceptive services based on religious objections to hormonal contraception, which is a key service that has been provided by Title X clinics, and is still required by the new regulations. These new grantees have been awarded a very small portion of the total Title X funds awarded in the states where they are located.
Figure 2: Only 3 New Grantees Joined Title X in 2019, Falling Far Short of Replacing Providers That Are Exiting the Program
Grantees and sites that are leaving the program will try to rely on state funds, reserves, or additional external funding to maintain their ability to serve the same number of individuals, but these funds may not be a replacement for the loss of federal dollars. As of August 30, 2019, Hawaii, Illinois, Maryland, Vermont, Washington, Massachusetts, Oregon, California and New York City have made some state or local funding available to replace some of the federal funds, but this may only be a short term solution and it is unclear whether these revenues will be available to compensate providers beyond this year.
Currently, 18 of 90 Title X grantees have said they will no longer use Title X funds and more grantees may leave in March 2020 when the requirement for complete physical separation from abortion takes effect.
Family planning providers that no longer have Title X support will likely face challenges in meeting the family planning needs of low-income residents in their communities without the federal program funds. This means that clinics may be forced to reduce hours, scale back or cut programs, reduce their stock of costly contraceptives like IUDs and implants, or decrease outreach and education efforts that have been supported by Title X. Many clinics may not be able to sustain their current staff without Title X funds, and could be forced to lay off medical staff, trainers, and educators. In addition, some of the sites may lose their eligibility for discount contraceptives under the 340B Drug Pricing Program. Historically, Title X funded sites are qualified to participate in this program, which allows clinics to obtain contraceptives and other drugs at considerably lower costs.
Certain parts of the country are more adversely impacted than others
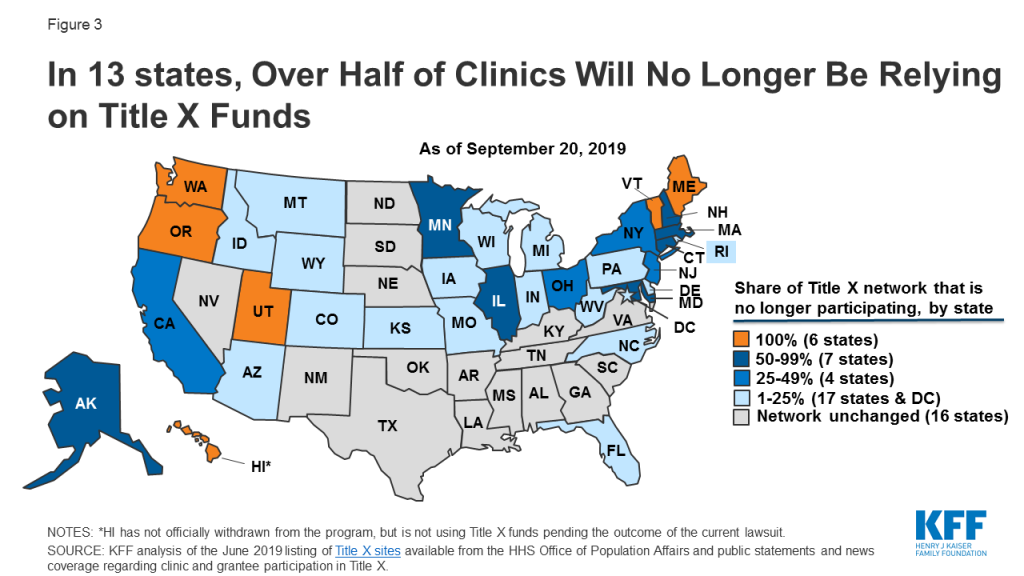
Title X has been a long-standing program that has offered federal family planning funding to all 50 U.S. states, D.C., and territories. There are entire states that are Title X grantees through their health departments or who have a single state-wide grantee that either have formally withdrawn or are in the process of, withdrawing from the Title X program. As of September 20, 2019, Hawaii, Maine, Oregon, Utah, Vermont, and Washington will no longer have Title X federally funded family planning clinics (Figure 3), even though some of these states have said they will use state dollars to offset some of the losses of federal funds to the clinics. Planned Parenthood clinics comprise a sizable share of the Title X network in Connecticut, Minnesota, California, and the Northeast that will no longer be participating in the Title X program.
Figure 3: In 13 states, Over Half of Clinics Will No Longer Be Relying on Title X Funds
Given the small numbers of new grantees that have recently joined the Title X program and the considerable reduction in the share of family planning providers that are participating in Title X, the result of the implementation of these regulations could be a significant reduction in the availability of free or low-cost family planning services to low-income women and men. It remains to be seen whether other organizations in these states will be able to absorb new clients and whether the existing sites and grantees will be able to serve the same number of clients with the level of comprehensive quality family planning services that the Title X program has facilitated since its inception in 1970.
The Senate Appropriations Committee released the draft FY 2020 Labor, Health and Human Services, and Education (LHHS) appropriations bill (and accompanying report) on September 18, 2019. The LHHS appropriations bill includes funding for U.S. global health programs provided to the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health (NIH).
Key highlights are as follows (see table for additional detail):
Funding provided to CDC for global health totaled $596 million, an increase of $100 million above the FY19 enacted level ($496 million), $139 million above the President’s FY20 request, and $65 million above the FY20 House level ($530.8).[i] This includes:
$128.4 million for global HIV/AIDS, matching the FY19 enacted and FY20 House levels and $58.9 million above the FY20 Request ($69.5 million).
$7.2 million for global tuberculosis (TB) through a shift in TB funding historically provided under the “HIV/AIDS, Viral Hepatitis, STD and TB Prevention” account to the “Center for Global Health” at CDC. This funding matches the FY19 enacted and FY20 Request levels, but is $10 million below the FY20 House level ($17.2 million).
$226 million for global immunization, matching the FY19 enacted and FY20 House levels and $20 million above the FY20 Request ($206 million). Within this total are the following:
Funding for polio totals $176 million, matching the FY19 enacted and FY20 House levels; the President’s FY20 request did not specify a funding amount for polio at CDC.
Funding for CDC’s other global vaccines/measles program totals $50 million, matching the FY19 enacted and FY20 House levels; the President’s FY20 request did not specify a funding amount for other global vaccines/measles at CDC.
$26 million for parasitic diseases and malaria, matching the FY19 enacted and FY20 House levels and $2 million above the FY20 Request ($24 million).
$208 million for the global public health protection program, $100 million above the FY19 enacted level ($108 million), $58 million above the President’s FY20 Request ($150 million), and $75 million above the FY20 House level ($133 million). This includes:
$198 million for the global disease detection and emergency response program, $100 million above the FY19 enacted level ($98 million) and $75 million above the FY20 House level ($123 million).
$9.8 million for the global public health capacity development program matching the FY19 enacted and FY20 House levels.
Funding for the Fogarty International Center (FIC) at NIH totaled $82 million, a $4 million increase above the FY19 enacted level ($78 million), $15 million above the President’s FY20 request ($67 million), and $3 million below the FY20 House level ($85 million).
Resources:
FY2020 Labor, Health and Human Services, and Education Appropriations Bill
FY2020 Labor, Health and Human Services, and Education Appropriations Report
The table (.xls) below compares global health funding in the FY 2020 Senate LHHS appropriations bill to the FY 2019 enacted funding amounts as outlined in the “Consolidated Appropriations Act, 2019” (P.L. 116-6; KFF summary here), the President’s FY 2020 request (KFF summary here), and the House FY 2020 LHHS bill (KFF summary here).
Table: KFF Analysis of FY20 Senate HHS Funding for Global Health
Department / Agency / Area
FY19 Enactedi(millions)
FY20 Requestii(millions)
FY20 House(millions)
FY20 Senate(millions)
Difference(millions)
FY20 Senate – FY19 Enacted
FY20 Senate – FY20 Request
FY20 Senate – FY20 House
Health & Human Services (HHS)
Centers for Disease Control & Prevention (CDC) – Total Global Health
$495.8
$457.0
$530.8
$595.8
$100 (20.2%)
$138.9 (30.4%)
$65 (12.2%)
Global HIV/AIDS
$128.4
$69.5
$128.4
$128.4
$0(0%)
$58.9(84.7%)
$0(0%)
Global Tuberculosisi
$7.2
$7.2
$17.2
$7.2
$0(0%)
$0(0%)
$-10(-58.1%)
Global Immunization
$226.0
$206.0
$226.0
$226.0
$0(0%)
$20(9.7%)
$0(0%)
Polio
$176.0
Not specified
$176.0
$176.0
$0(0%)
–
$0(0%)
Other Global Vaccines/Measles
$50.0
Not specified
$50.0
$50.0
$0(0%)
–
$0(0%)
Parasitic Diseases
$26.0
$24.5
$26.0
$26.0
$0(0%)
$1.5(6.3%)
$0(0%)
Global Public Health Protectionii
$108.2
$149.8
$133.2
$208.2
$100(92.4%)
$58.4(39%)
$75(56.3%)
Global Disease Detection and Emergency Response
$98.4
Not specified
$123.4
$198.4
$100(101.6%)
–
$75(60.8%)
of which Global Health Security (GHS)
$50.0
$99.8
Not specified
Not specified
–
–
–
Global Public Health Capacity Development
$9.8
Not specified
$9.8
$9.8
$0(0%)
–
$0(0%)
National Institutes of Health (NIH) – Total Global Health
$880.2
$760.1
Not specified
Not specified
–
–
–
HIV/AIDS
$590.1
$511.1
Not specified
Not specified
–
–
–
Malaria
$212.0
$182.0
Not specified
Not specified
–
–
–
Fogarty International Center (FIC)
$78.1
$67.0
$84.9
$82.3
$4.2(5.4%)
$15.3(22.9%)
$-2.6(-3%)
Notes:
i – CDC global health program totals have been adjusted to include the transfer of tuberculosis funding from the “HIV/AIDS, Viral Hepatitis, STI and TB Prevention” account at CDC. In FY20, the administration proposed to formally transfer $7.2 million from the “HIV/AIDS, Viral Hepatitis, STI and TB Prevention” account to “Global Tuberculosis” activities. The report accompanying the draft Senate FY20 appropriations bill states that the $7.2 million provided through the “HIV/AIDS, Viral Hepatitis, STI and TB Prevention” account for tuberculosis activities is shifted under this bill to the “Center for Global Health.”
ii – In the CDC FY20 congressional justification, this funding line is titled “Global Disease Detection and Other Programs”. The full breakdown in funding for “Global Public Health Protection,” which includes “Global Disease Detection and Emergency Response,” “Global Health Security,” and “Global Public Health Capacity” is not yet known for the draft House FY20 bill. However, the draft bill includes $99.8 million for “global public health protection,” and the committee report specifies $123.4 million for “Global Disease Detection and Emergency Response.” These totals will be updated as more information becomes available.
Posted: September 19, 2019
[i] CDC global health program totals have been adjusted to include the transfer of tuberculosis funding from the “HIV/AIDS, Viral Hepatitis, STI and TB Prevention” account at CDC. In FY20, the administration proposed to formally transfer $7.2 million from the “HIV/AIDS, Viral Hepatitis, STI and TB Prevention” account to “Global Tuberculosis” activities. The report accompanying the draft Senate FY20 appropriations bill states that the $7.2 million provided through the “HIV/AIDS, Viral Hepatitis, STI and TB Prevention” account for tuberculosis activities is shifted under this bill to the “Center for Global Health.”
Nearly 8 in 10 Immigrants Who Entered the U.S. Without Legal Permanent Resident Status Have At Least One Characteristic That Could Count Against Them under the New “Public Charge” Rule
Seventy-nine percent of noncitizen residents who originally entered the United States without legal permanent resident status have at least one characteristic that could count against them under the Trump Administration’s new “public charge” rule, according to an updated KFF analysis.
Such characteristics – including having an income below 125 percent of the federal poverty level or lacking a high school diploma or private health insurance — could make it harder for immigrants to obtain admission into the U.S. or get a green card under the administration’s final rule to change “public charge” inadmissibility policies scheduled to take effect on October 15. Under the changes, federal officials will deny entry or green cards to people who they determine are likely to rely on public programs such as Medicaid and certain housing and nutrition programs that were previously excluded from this “public charge” test. Many noncitizen residents have characteristics that would be considered positive under the rule as well, though immigration officials would have substantial discretion in assessing factors and applying the rule.
The new rule also will likely lead to decreased enrollment in Medicaid and other public programs among immigrant families beyond those directly affected by the rule due to fear and confusion about the changes. An estimated 13.5 million Medicaid or CHIP enrollees are citizens or noncitizens living in a household with a noncitizen. If the rule were to lead to disenrollment rates ranging from 15 percent to 35 percent among these enrollees – based on prior experience with welfare reform — then between 2 million and 4.7 million individuals could drop out of such programs, the analysis finds. Decreased participation in Medicaid would increase the uninsured rate among immigrant families and could decrease revenues and increase uncompensated care for providers.
In August 2019, the Trump Administration published a Department of Homeland Security (DHS) final rule to change “public charge” inadmissibility policies. Under longstanding immigration policy, federal officials can deny entry to the U.S. or adjustment to legal permanent resident (LPR) status (i.e., a “green card”) to someone they determine to be a public charge. The new rule redefines public charge and expands the programs that the federal government considers in public charge determinations to include previously excluded health, nutrition, and housing programs, such as Medicaid for non-pregnant adults. It also identifies characteristics DHS will consider as negative factors that increase the likelihood of someone becoming a public charge, including having income below 125% of the federal poverty level (FPL) ($26,663 for a family of three as of 2019). The rule is scheduled to go into effect as of October 15, 2019. Using the Survey of Income and Program Participation (SIPP) 2014 Panel and 2017 American Community Survey (ACS) data, this analysis provides estimates of the rule’s potential impacts:
Nearly eight in ten (79%) noncitizens who originally entered the U.S. without LPR status have at least one characteristic that DHS could weigh negatively in a public charge determination. Over one in four (27%) have a characteristic that DHS could consider a heavily weighted negative factor. The most common negative factors among the population are lacking private health insurance (56%), not having a high school diploma (39%), and having family income below the new 125% FPL threshold (32%).
If the rule leads to disenrollment rates ranging from 15% to 35% among Medicaid and CHIP enrollees who are noncitizens or live in a household with a noncitizen, between 2.0 to 4.7 million individuals could disenroll. Previous research and recent experience suggest that the rule will likely lead to decreased enrollment in public programs among immigrant families beyond those directly affected by the rule due to fear and confusion about the changes. Even before the rule was finalized, there were reports of parents disenrolling themselves and their children from Medicaid and CHIP coverage, choosing not to renew coverage, or choosing not to enroll despite being eligible. Beyond potential disenrollment, the rule may also deter new enrollment among some of the nearly 1.8 million uninsured individuals who are eligible for Medicaid and CHIP but not enrolled and are noncitizens themselves or live in a household with a noncitizen. Decreased participation in Medicaid would increase the uninsured rate among immigrant families, reducing access to care and contributing to worse health outcomes. Coverage losses also will likely decrease revenues and increase uncompensated care for providers and have spillover effects within communities.
Key Findings
Introduction
In August 2019, the Trump Administration published a DHS final rule to change “public charge” inadmissibility policies. Under longstanding immigration policy, federal officials can deny entry to the U.S. or adjustment to LPR status (i.e., a “green card”) to someone they determine to be a public charge. Based on Kaiser Family Foundation analysis of the SIPP 2014 Panel and 2017 ACS data, this analysis provides updated estimates of the:
Share of noncitizens who originally entered the U.S. without LPR status who have characteristics that DHS could potentially weigh negatively in a public charge determination; and
Number of individuals who might disenroll from Medicaid under different scenarios in response to the rule.
Background
Under longstanding policy, if authorities determine that an individual is likely to become a public charge, they may deny that person’s application for LPR status or entry into the U.S.1 Public charge determinations are a forward-looking test in which officials will assess the likelihood of someone becoming a public charge in the future. Specifically, DHS finds an individual “inadmissible” if officials determine that he or she is more likely than not at any time in the future to become a public charge.
The rule redefines public charge and broadens the programs that the federal government will consider in public charge determinations to include previously excluded health, nutrition, and housing programs (Table 1). Under previous policy, a person was considered a public charge if officials determined he or she was likely to become primarily dependent on the federal government as demonstrated by use of cash assistance programs or government-funded institutionalized long-term care. Guidance specifically clarified the exclusion of Medicaid and other non-cash programs from these decisions because of concerns that fears were limiting enrollment of families. Under the new rule, officials will determine someone to be a public charge if they determine an individual is more likely than not at any time in the future to receive one or more public benefits for more than 12 months in the aggregate within any 36-month period (such that, for instance, receipt of two benefits in one month counts as two months). Further, the rule defines public benefits to include federal, state, or local cash benefit programs for income maintenance and certain health, nutrition, and housing programs that were previously excluded from public charge determinations, such as non-emergency Medicaid for non-pregnant adults, the Supplemental Nutrition Assistance Program (SNAP), and several housing programs.
Table 1: Change in Public Charge Definition and Programs Considered
Previous Policy
Policy Under New Rule
Public Charge Definition
Likely to become primarily dependent on the federal government as demonstrated by use of cash assistance programs or government-funded institutionalized long-term care.
More likely than not at any time in the future to receive one or more public benefits for more than 12 months in the aggregate within any 36-month period (such that, for instance, receipt of two benefits in one month counts as two months).
Programs Considered in Public Charge Determinations
SSI
TANF
State/local cash assistance programs
Public assistance for long-term care in an institution (including Medicaid)
SSI
TANF
Federal, state, or local cash benefit programs for income maintenance
Non-emergency Medicaid for non-pregnant adults over age 212
SNAP food assistance
Housing assistance
Officials make public charge determinations based on the totality of the person’s circumstances. At a minimum, officials must take into account an individual’s age; health; family status; assets, resources, and financial status; and education and skills. The rule describes how DHS will consider each factor and identifies characteristics it will deem as positive factors that reduce the likelihood of an individual becoming a public charge and negative factors that increase the likelihood of becoming a public charge. DHS indicates that no single factor would govern a determination, and it appears officials would retain significant discretion in assessing factors and making determinations. The rule establishes a new income standard of 125% of the federal poverty level (FPL) ($26,663 for a family of three as of 2019) and specifies that family income below that standard is a negative factor. Some other negative factors include having a lower education level, a health condition, lacking private health insurance, not being employed or a primary caregiver, and having limited English proficiency. Examples of positive factors include being of working age, being in good health, having private health coverage, and having income at or above 125% FPL. The rule also specifies certain heavily weighted negative and positive factors.
The rule identifies previous or current use of public benefits as a negative factor, but most immigrants who would be seeking admission or adjustment to LPR status are already ineligible for these programs or are exempt from a public charge determination. For example, eligibility for the programs included in the rule for immigrants without LPR status is now largely limited to humanitarian immigrants such as refugees and asylees, who are exempt from the public charge test. However, since the public charge determination is a forward-looking test, even if an individual is not currently or has not previously used a public benefit, officials will assess the likelihood of an individual using those benefits in the future.
The new rule will likely lead to decreased enrollment in Medicaid and other programs among individuals in immigrant families beyond those directly affected by the rule, including their primarily U.S.-born children. Although few people directly affected by the rule are enrolled in Medicaid and the other public benefit programs, previous experience and recent research suggest that the rule will have chilling effects that would lead individuals to forgo enrollment in or disenroll themselves and their children from programs due to confusion and fear that their or their children’s enrollment could negatively affect their or another family member’s immigration status.3 For example, prior to the final rule, there were anecdotal reports of individuals disenrolling or choosing not to enroll themselves or their children in Medicaid and CHIP due to fears and uncertainty.4 Providers also reported increasing concerns among parents about enrolling their children in Medicaid and food assistance programs,5 and WIC agencies across a number of states have seen enrollment drops that they attribute largely to fears about public charge.6 A survey conducted prior to the final rule found that one in seven adults in immigrant families reported avoiding public benefit programs for fear of risking future green card status, and more than one in five adults in low-income immigrant families reported this fear.7
Characteristics of Noncitizens without LPR status
Using SIPP 2014 Panel data, we show characteristics that DHS could consider in a public charge determination under the rule among noncitizens who originally entered the U.S. without LPR status. Specifically, the analysis examines age, self-reported health status, family income, health insurance type, employment, education, and English proficiency (Appendix B). As noted, officials also will consider previous or current use of public benefits. However, because very few people without a green card are eligible for these programs who would be subject to a public charge test, this analysis does not include estimates of use of public programs.
These estimates illustrate the share of noncitizens living in the U.S. who might face barriers to adjusting to LPR status under the rule based on certain characteristics. Due to data limitations, they do not provide a precise count of the number of people within the U.S. who would be subject to public charge determinations. The estimates do not account for people who DHS could deny entry into the U.S. due to a public charge determination and do not account for all factors that DHS could consider in a public charge determination. As noted, officials would take into account the totality of an individual’s circumstances, and no single factor would govern a determination. How DHS would operationalize its assessment of factors may differ from SIPP’s measurement of characteristics. (See Appendix A: Methods for more detail.)
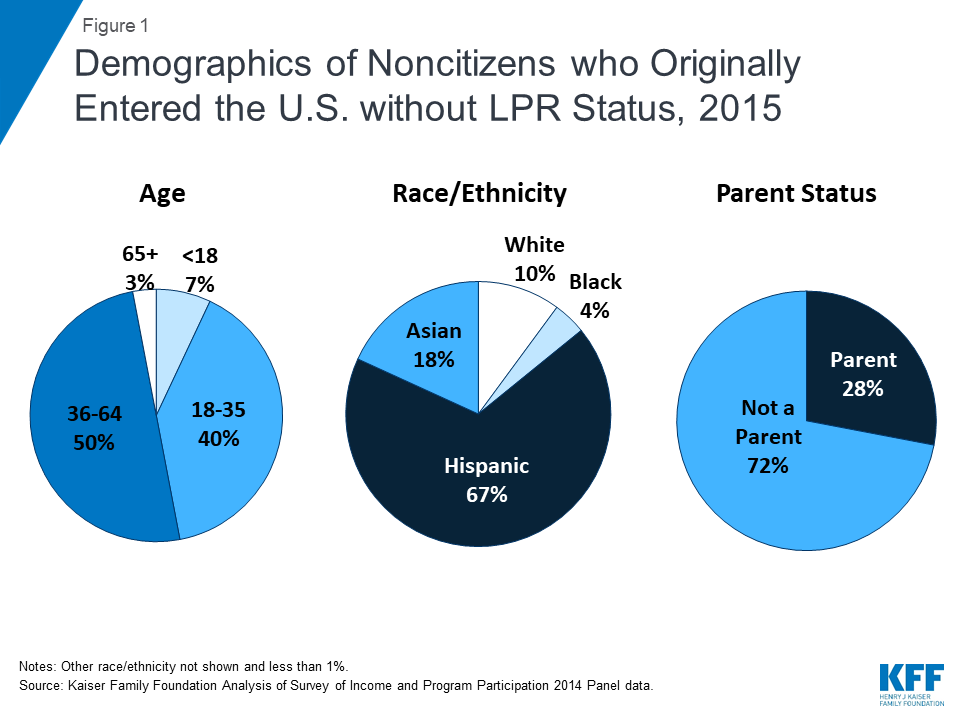
Noncitizens who entered the U.S. without LPR status include individuals across different ages, races/ethnicities, and family statuses. Although many were nonelderly Hispanic adults without a dependent child, 7% are a child, more than one in four is a parent (28%), and one-third (33%) is another race or ethnicity, including nearly one in five (18%) who is Asian (Figure 1).
Figure 1: Demographics of Noncitizens who Originally Entered the U.S. without LPR Status, 2015
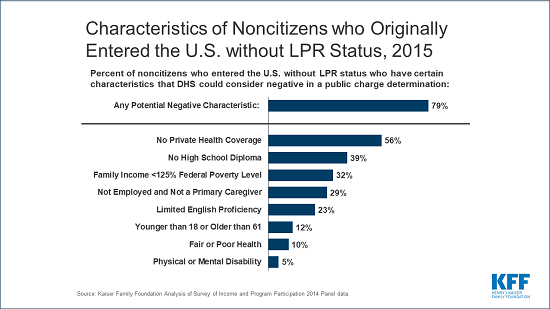
Nearly eight in ten (79%) noncitizens who entered the U.S. without LPR status have at least one characteristic that DHS could weigh negatively in a public charge determination under the rule. The most common characteristics examined that DHS could consider as negative factors include no private health coverage (56%), no high school diploma (39%), and having income below the new 125% FPL8 standard established by the rule (32%). (Figure 2 and Appendix B).
Figure 2: Characteristics of Noncitizens who Originally Entered the U.S. without LPR Status, 2015
More than one in four (27%) noncitizens who originally entered the U.S. without LPR status have a characteristic that DHS could consider a heavily weighted negative factor examined in this analysis. Potential heavily weighted negative factors examined in this analysis include not being employed and not a full-time student or primary caregiver (29%), and having a disability that limits the ability to work and lacking private health coverage (3%). The rule identifies other heavily weighted negative factors that were not included in this analysis, including receipt of a public benefit for more than 12 of the previous 36 months and being found previously inadmissible or deportable on public charge grounds. As noted, very few people without a green card are eligible for these programs who would be subject to a public charge test. SIPP data do not provide information on previous determinations of inadmissibility or deportability based on public charge grounds.
Nearly all of noncitizens who originally entered without LPR status have at least one characteristic that DHS could consider as a positive factor. The most common positive factors are no physical or mental health disability (95%), excellent, very good, or good health (90%), and being of working age (between age 18 and 61) (88%). Over half (55%) have a heavily weighted positive factor, which includes having private health insurance (44%) or having family income at or above 250% FPL (36%). Given the high prevalence of at least one positive factor among the population, it’s unclear how officials would weigh the presence of a positive factor in a public charge test. As noted, officials will make public charge determinations based on a totality of an individual’s circumstances. However, the rule does not specify how officials will weigh different factors against each other, leaving officials significant discretion in making determinations on a case-by-case basis.
Nearly seven in ten (68%) of U.S. citizens (U.S. born and naturalized) also had one or more characteristics that DHS could potentially weigh negatively if they were subject to a public charge determination. Citizens were more likely than noncitizens who entered the U.S. without LPR status to have certain characteristics that DHS could consider negative, including being a child or older than age 61 and reporting fair or poor health and having a physical or mental disability that limits their ability to work (Appendix B).
Impact on Medicaid Enrollment
We also illustrate the number of Medicaid and CHIP enrollees who are noncitizens or citizens living in a household with at least one noncitizen who could disenroll under different potential disenrollment scenarios. We use 2017 American Community Survey (ACS) data for this analysis as ACS provides more recent estimates of health coverage than available through SIPP. Although CHIP was not included as a public benefit in the rule, many individuals are not able to distinguish between their enrollment in Medicaid versus CHIP, and ACS data do not provide separate Medicaid and CHIP coverage measures. As noted, previous experience and recent research suggests that the proposed rule may lead to broader disenrollment among individuals in families with immigrants beyond those the rule directly affects.
We applied disenrollment rates of 15%, 25%, and 35% to the total number of Medicaid and CHIP enrollees who are noncitizens or citizens living in a household with at least one noncitizen. It is difficult to predict what actual disenrollment rates may be in response to the rule. These disenrollment rates illustrate a range of potential impacts and draw on previous research on the chilling effect welfare reform had on enrollment in health coverage among immigrant families.9 As noted, a 2019 survey fielded prior to finalization of the rule found that one in seven (13.7%) of adults in immigrant families reported avoiding public benefit programs for fear of risking future green card status, and more than one in five (20.7%) adults in low-income immigrant families reported this fear.10
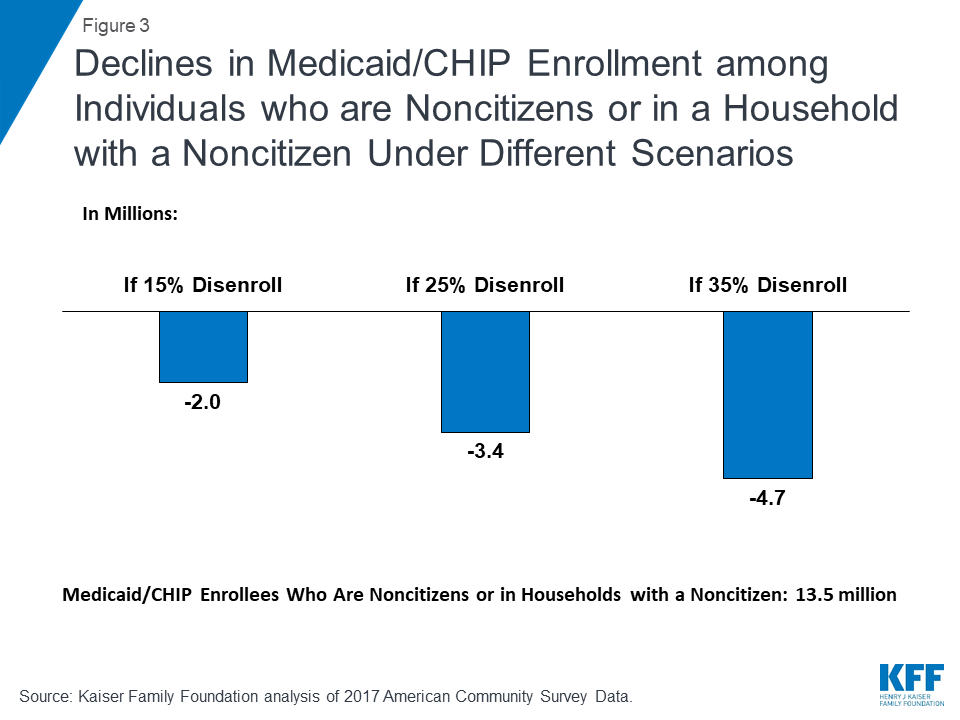
According to the ACS data, there were over 13.5 million Medicaid/CHIP enrollees who were noncitizens or citizens living in a household with at least one noncitizen, including 7.6 million children, who may be at risk for decreased enrollment as a result of the rule. If the proposed rule leads to disenrollment rates ranging from 15% to 35%, between 2.0 million and 4.7 million Medicaid and CHIP enrollees who are noncitizens or citizens living in a family with at least one noncitizen would disenroll (Figure 3). Because very few noncitizens are eligible for Medicaid would be subject to public charge, this disenrollment would primarily be due to chilling effects of fear and confusion. The estimates provide illustrative examples and, due to data limitations, may reflect both an undercount of noncitizens and an overestimate of noncitizens receiving Medicaid. (See Appendix A: Methods for more detail.)
Figure 3: Declines in Medicaid/CHIP Enrollment among Individuals who are Noncitizens or in a Household with a Noncitizen Under Different Scenarios
Beyond potential disenrollment, the proposed rule may also deter new enrollment among the nearly 1.8 million uninsured individuals who are eligible for Medicaid and CHIP but not enrolled and are noncitizens or live in a household with a noncitizen. Specifically, there are 652,200 noncitizen adults and 219,100 noncitizen children who are uninsured but eligible for Medicaid or CHIP. In addition, there are 366,800 uninsured citizen adults and 602,400 uninsured citizen children who are eligible for one of the programs and live in a household with a noncitizen.11 Given continually evolving immigration trends, potential effects of the new rule on lawful immigration in the future, and families’ increased fears of accessing programs, the number of people living in a household with a noncitizen who enroll in Medicaid and CHIP may continually decline over time.
Implications
The rule will make it more difficult for some individuals, particularly those with low incomes and health needs, to obtain LPR status or immigrate to the U.S. For example, a full-time worker in a family of three earning the federal minimum wage would not have sufficient annual income ($15,080) to meet the new income standard established in the rule, which would be $26,663 for a family of three. As such, the rule will affect future immigration opportunities for individuals and families. The rule may also increase barriers to family reunification and potentially lead to family separation, particularly among families with mixed immigration statuses. For example, if DHS denies an individual a green card and that individual loses permission to remain in the U.S due to a public charge determination, he or she may have to leave other family members, such as a spouse or child who is a citizen or who has LPR status, in the U.S.
Reduced participation in Medicaid and other programs would negatively affect the health and financial stability of immigrant families and the growth and healthy development of their children, who are predominantly U.S.-born. Coverage losses would reduce access to care for families, contributing to worse health outcomes. Reduced participation in nutrition and other programs would likely compound these effects. In addition, the losses in coverage would lead to lost revenues and increased uncompensated care for providers and have broader spillover effects within communities.
This brief was prepared by Samantha Artiga and Rachel Garfield, with the Kaiser Family Foundation, and Anthony Damico, an independent consultant to the Kaiser Family Foundation.
Appendices
Appendix A: Methods
The findings presented in this brief are based on Kaiser Family Foundation analysis of Wave 3 of the Survey of Income and Program Participation (SIPP) 2014 Panel and 2017 American Community Survey (ACS) data. SIPP enables us to directly measure individuals’ immigration status at the time they entered the U.S. and health status. SIPP also provides measures of health coverage, but 2015 is the most recent year of data available. Because 2015 was a year of substantial transition for Medicaid due to the implementation of the Affordable Care Act, we base our Medicaid and CHIP disenrollment analysis on 2017 ACS data.
We classified people as not having LPR status when originally entering the U.S. based on a SIPP question that asks, “What was [respondent’s] immigration status when he/she first moved to the United States?” In addition to measuring people who might adjust to LPR status in the future, who would be subject to a public charge determination (unless they fall into an exempt category), this measure includes noncitizens who have adjusted to LPR status since arriving into the U.S. It also includes nonimmigrants and undocumented immigrants who do not have a current pathway to adjust to LPR status. Our testing of different citizenship measures led to overall similar patterns. The 2014 SIPP shows 17.8 million noncitizens, including 7.4 million of whom originally entered the country without LPR status. Due to underreporting of noncitizens and legal immigration status in the SIPP, these estimates may reflect an undercount of the total noncitizen population and especially the undocumented population. Given this potential undercount—and that the group of noncitizens without LPR status includes some individuals who have since adjusted to LPR status as well as nonimmigrants and undocumented immigrants who do not have a pathway to adjust to LPR status— our analysis of characteristics that DHS could consider negative in public charge determinations focuses on shares rather than absolute numbers of affected individuals.
For the estimates of the share of noncitizens without LPR status living within the U.S. who have characteristics that DHS could weigh negatively in a public charge determination under the proposed rule, we used SIPP to measure age, poverty and work status, insurance status, education, English proficiency, and health status and classified each factor as positive or negative based on the rule’s description of how DHS would consider the characteristic. DHS’ implementation and operationalization of its assessment of factors may differ from SIPP’s measurement of characteristics.
In our analysis of household income, we use 125% of the Census poverty threshold, or $23,848 for a family of three in 2015. Census poverty thresholds are measured slightly differently than HHS poverty guidelines but lead to similar poverty levels for incomes of similar household size. In the rule, DHS provides a specific definition of a household to be used in the calculation of household income. Thus, the final income cutoff for a particular family to meet the 125% of poverty rule as implemented may differ from our measurement or that used by other programs.
We base the Medicaid and CHIP potential disenrollment analysis on 2017 ACS data. These data show that over 13.5 million Medicaid/CHIP enrollees were noncitizens or living in a household with at least one noncitizen. These data on Medicaid enrollees reflect both an undercount of noncitizens in the survey data (as noted above) as well as an overestimate of the share of noncitizens participating in Medicaid as it includes some who may be reporting emergency Medicaid or other state or local health assistance programs as Medicaid coverage.
For estimates of potential changes in coverage due to public charge policies, we present several scenarios using different disenrollment rates for Medicaid and CHIP. These disenrollment rates drew on previous research that showed decreased enrollment in Medicaid and CHIP among immigrant families after welfare reform.12 For example, Kaushal and Kaestner found that after new eligibility restrictions were implemented for recent immigrants as part of welfare reform, there was 25% disenrollment among children of foreign-born parents from Medicaid even though the majority of these children were not affected by the eligibility changes and remained eligible.13 Using this 25% disenrollment rate as a mid-range target, we assume a range of disenrollment rates from a low of 15% to a high of 35%. However, it remains uncertain what share of individuals may disenroll from Medicaid and CHIP in response to the proposed rule. Although the welfare reform experience is instructive of chilling effects among immigrant families broadly, it was associated with changes to program eligibility for immigrants. In contrast, this rule would change the potential consequences of participating in programs on an individual’s immigration status.
Appendix B
Characteristics that DHS Could Consider in Public Charge Determinations by Citizenship Status, 2015
Potential Positive or Negative Factor?
Heavily Weighted?
Non-LPR Noncitizen
Total Noncitizens
Citizens
Age
17 or younger
Negative
7%
8%
22%
18 to 61
Positive
88%
84%
58%
62 or older
Negative
6%
8%
21%
Health Status
No Physical or Mental Health Disability
Positive
95%
94%
86%
Physical or Mental Health Disability
Negative
5%
6%
14%
Excellent, Very Good, or Good Health
Positive
90%
90%
86%
Fair or Poor health
Negative
10%
10%
14%
Physical or Mental Health Disability and No Private Coverage
Negative
Y
3%
4%
7%
Family Income
Less than 125% Federal Poverty Level (FPL)
Negative
32%
28%
16%
125% to less than 250% FPL
Positive
32%
29%
22%
250% FPL or more
Positive
Y
36%
43%
62%
Health Coverage
Private Coverage
Positive
Y
44%
48%
71%
No Private Coverage
Negative
56%
52%
29%
Employment
Employed (and age 18+)
Positive
64%
62%
48%
Not employed and not a caregiver (and age 18+)
Negative
29%
30%
30%
Not employed and not a student (and age 18+)
Negative
Y
27%
28%
28%
Education
Has high school diploma or higher (and age 18+)
Positive
54%
56%
71%
No high school diploma (and age 18+)
Negative
39%
36%
8%
English Proficiency
Does Not Have Limited English Proficiency
Positive
77%
77%
99%
Limited English Proficiency
Negative
23%
23%
1%
Any Positive Factor
100%
100%
100%
Any Heavily Weighted Positive Factor
55%
60%
79%
Any Negative Factor
79%
78%
68%
Any Heavily Weighted Negative Factor
27%
29%
29%
Notes: For each individual subject to a determination, DHS would take into account the totality of his or her circumstances and would retain discretion on how to weigh specific circumstances and factors; no single factor would govern a determination. How DHS would implement and operationalize its assessment of factors under the rule may differ from how SIPP measures characteristics.Source: Kaiser Family Foundation Analysis of Survey of Income and Program Participation 2014 Panel data.
Endnotes
Becoming a public charge may also be a basis for deportation in extremely limited circumstances. “Public Charge Fact Sheet,” U.S. Citizenship and Immigration Services, https://www.uscis.gov/news/fact-sheets/public-charge-fact-sheet, accessed February 12, 2018. ↩︎
Services or benefits funded by Medicaid but provided under the Individuals with Disabilities Education Act and school-based services or benefits provided to individuals who are at or below the oldest age eligible for secondary education as determined under state or local law are not included as a public benefit. ↩︎
In our data analysis, we use the Census poverty threshold, which was $23,848 for a family of three in 2015. Census poverty thresholds are measured slightly differently than HHS poverty guidelines but lead to similar poverty levels for incomes of similar household size. See Methods for more detail. ↩︎
Medicare does not cover routine dental care, and two-thirds of the Medicare population have no dental coverage at all. With limited or no dental coverage, some incur high out-of-pocket costs, while others forgo need dental care because they can’t afford it. Policymakers in Washington and others are exploring ways to make dental care more affordable for the 60 million people on Medicare.
A new KFF brief examines five potential ways to make oral health care more available and affordable for the Medicare population, including two approaches that would add a new dental benefit under Medicare and others that would offer more limited help to people on Medicare, and have less of an impact on the federal budget. The five options include:
Adding a dental benefit to Medicare Part B
Creating a voluntary dental benefit under a new part of Medicare
Permitting greater access to medically necessary dental services under Medicare
Testing models for dental coverage
Offering dental discount cards
The brief reviews the limits of dental coverage permitted under current Medicare law, then describes each of the policy options, with an analysis of likely implications for key stakeholders, including Medicare beneficiaries, taxpayers, insurers, and dental professionals. It also examines trade-offs for the options, including increases in federal spending. The brief, Policy Options for Improving Dental Coverage for People on Medicare, is intended to inform policy discussions focused on improving oral health care and coverage for the Medicare population.
A previously released brief, Drilling Down on Dental Coverage and Costs for Medicare Beneficiaries, reviews the state of oral health for people on Medicare, describing the consequences of foregoing dental care, current sources of dental insurance, use of dental services, and beneficiaries’ out-of-pocket spending.
NOTE: This analysis has been updated to reflect data from 2019, available here.
Since its inception, Medicare, the national health insurance program for more than 60 million older adults and younger people with long-term disabilities, has explicitly excluded coverage of dental services, with limited exceptions. Some Medicare beneficiaries have access to dental coverage through other sources, such as Medicare Advantage plans, Medicaid, or private plans (either employer-sponsored retiree plans or plans purchased by individuals), but the scope of coverage under these plans varies widely and is typically quite limited.
Nearly half of the Medicare population – 24 million beneficiaries – have no dental coverage at all. Cost concerns and lack of dental coverage contribute to beneficiaries foregoing routine and other dental procedures. Lack of dental care can exacerbate chronic medical conditions, such as diabetes and cardiovascular disease, contribute to delayed diagnosis of serious medical conditions, and lead to preventable complications that sometimes result in costly emergency room visits.1 As a result, there is ongoing interest in policy options to make dental care more affordable by broadening dental coverage for people on Medicare.2
This issue brief begins with a review of dental coverage permitted under current Medicare law to set the context for understanding proposals that could improve oral health coverage for the Medicare population. It reviews a range of policy options that could make dental care more affordable, examines basic policy features associated with each proposal, and discusses potential implications for key stakeholders, including Medicare beneficiaries, taxpayers, insurers, and dental professionals.
This brief describes five potential ways to strengthen oral health care for older adults (Table 1). The first two options would create a new dental benefit under Medicare: one would add dental benefits to Medicare Part B, and the other would establish a separate dental benefit under a new part of Medicare, similar in some ways to the Part D benefit for prescription drugs. The other three options would be expected to provide less help in improving dental coverage and reducing out-of-pocket costs for dental care, and would have a more limited impact on Medicare spending.
Table 1. Potential Approaches for Improving Dental Coverage for People on Medicare
New Medicare Dental Benefit
Add a dental benefit to Medicare Part B
Create a voluntary dental benefit under a new part of Medicare
Other Approaches
Permit greater access to medically necessary dental services under Medicare
Test models for dental coverage
Offer dental discount cards
Overview of Current Rules for Medicare Coverage of Dental Care
Current law states that Medicare will not pay for dental services, except under very limited circumstances. Under Section 1862(a)(12) of the Social Security Act, Medicare will not make payments:
“…for services in connection with the care, treatment, filling, removal, or replacement of teeth or structures directly supporting teeth, except that payment may be made under Part A in the case of inpatient hospital services in connection with the provision of such dental services if the individual, because of his underlying medical condition and clinical status or because of the severity of the dental procedure, requires hospitalization in connection with the provision of such services.”3
Medicare does cover dental services if they are incident and integral to a covered procedure such as when the reconstruction of a ridge is performed as a result of and at the same time as the surgical removal of a tumor (for other than dental purposes). Medicare also specifies an exception to the “incident and integral to” rule when a dentist extracts teeth to prepare the jaw for radiation treatment for cancer.4
While the dental exclusion includes exceptions that allow coverage of limited medically-related services, current policy is not completely clear or consistent. For example, Medicare Part A will cover an oral examination for patients who are hospitalized for a comprehensive workup prior to a kidney transplant, but it will not cover an oral examination for patients prior to transplantation of organs other than kidneys.5,6,7 Even in this circumstance, there is no payment under Medicare Part B for the dentist’s service, just to the hospital for the service of an employed dentist.8 As a result of the lack of clarity and consistency in the dental exclusion, there has been ongoing discussion about whether the law can be interpreted to cover a wider range of medically necessary dental services.
Options for Strengthening Dental Coverage
Several approaches could make dental coverage more widely available and more affordable for Medicare beneficiaries. The first two options discussed in this brief would create a new Medicare dental benefit – one option would cover dental services under Part B and another option would offer dental services under a new voluntary part of the program, similar to the approach taken with the Part D prescription drug benefit. For either of these approaches to be implemented, the statutory dental exclusion would need to be modified. Each of these two approaches would require decisions about:
the scope of covered benefits;
cost sharing for specific services;
how premiums would be calculated;
provider rules for participation and payments;
assistance for low-income beneficiaries;
coordination with existing dental coverage; and
spillover effects on other payers and programs.
Other issues likely to emerge with each of these approaches include how to determine when dental services are reasonable and necessary (as required for all Medicare-covered benefits), how to measure and monitor the quality of dental care provided, and how to ensure patient access to dental services across the country, including in rural and other underserved areas.
Add a Dental Benefit to Medicare Part B
The Medicare statute could be amended to allow dental services to be covered under Medicare Part B. Under this approach, all Part B enrollees would be entitled to Medicare-covered dental services, just as they are covered for physician care and other defined outpatient services.9 While enrollment in Medicare Part B is voluntary, the vast majority of beneficiaries who are entitled to Part A are also enrolled in Part B.10
A new dental benefit under Part B would build upon the current structure of premiums, cost sharing, and low-income assistance of Part B. In general, Part B enrollees pay a standard monthly premium that covers 25 percent of Part B expenditures, with the other 75 percent covered by general revenues. Higher-income beneficiaries pay an additional income-related premium, and lower-income beneficiaries have their premiums, and in some instances, cost sharing, paid for by Medicaid through the Medicare Savings Programs. Most Part B services are subject to an annual deductible ($203 in 2021) and 20 percent coinsurance, with no cost sharing required for certain preventive services, such as cancer screenings.
Establishing a new dental benefit under Medicare Part B would require several policy decisions that would affect how much dental coverage beneficiaries get, the impact on premiums and out-of-pocket spending, beneficiaries’ access to dentists across the country, and health outcomes. These decisions will also directly affect federal spending, and could impact spending by other payers.
Scope of covered services. A key issue would be defining which dental services to cover. These decisions could be informed by a variety of sources, including surveys of beneficiary preferences, patterns of utilization among older adults, and current sources of dental insurance. Presently, the scope of covered dental benefits varies greatly across Medicare Advantage plans, Medicaid, and private dental insurance. A new Part B dental benefit could be structured in different ways, and could be defined to cover a relatively narrow scope of dental benefits (e.g., preventive services only), the full array of dental services, or something in between. For each of these approaches, coverage policies would need to be developed to determine when treatments are “reasonable and necessary.”.One approach could provide a comprehensive dental benefit that covers preventive services such as cleanings and x-rays, basic procedures such as fillings and extractions, and more extensive (and expensive) treatments, such as crowns, dentures, and implants. This approach would be parallel to the comprehensive nature of Part B medical benefits. A second and more limited approach could cover only preventive services and routine treatment. A third approach could cover all procedures once beneficiaries exceed a certain dollar threshold, essentially providing a catastrophic-only dental benefit, where beneficiaries pay the up-front costs of their dental care out-of-pocket (or obtain dental coverage to cover these front-end expenses) with Medicare picking up the cost for services above a certain dollar limit (similar to a high deductible health plan)..A fourth approach could be a doughnut-type benefit, with Medicare coverage of preventive services and catastrophic expenses, and beneficiaries responsible for expenses in the gap – similar to the structure of the Medicare Part D benefit when it was first implemented in 2006. Part D was initially designed in this fashion to meet budget targets, but over time, the law has been modified to close the so-called “doughnut hole” to provide better protection for beneficiaries..The scope of covered benefits would directly affect Medicare Part B premiums and Medicare spending. The structure and comprehensiveness of the benefit would also have spillover effects for other sources of coverage, including Medicare Advantage plans (discussed below).
Comprehensive dental benefit. A benefit that provides all reasonable and necessary dental services, including preventive and minor and major restorative services, would offer the most extensive coverage for beneficiaries. This approach would also be expected to significantly increase Part B premiums and program spending, much more than a more narrowly defined benefit package, and would likely replace other sources of dental coverage, such as private dental insurance plans and Medicaid, for those who have it (discussed below).
Preventive dental benefit. A more limited dental benefit that covers only preventive services could provide some help for the majority of Medicare beneficiaries, and may lead to earlier diagnosis of conditions that require follow-up medical attention. It would also have a lower price tag for the Medicare program and lead to smaller increases in Part B premiums than a more comprehensive benefit since preventive services tend to be less expensive. However, it would not cover the most expensive services that often cause beneficiaries to postpone or go without needed care. While Medicare Part B preventive dental benefit could duplicate dental coverage that some have today, it would create an opportunity for private dental insurers to offer supplemental dental benefits to cover more extensive and expensive services.
Catastrophic-only dental benefit. A catastrophic-only dental benefit package could be especially helpful for beneficiaries who need high-cost services but cannot afford the services on their own. However, it would offer no help to beneficiaries who are unable to cover the cost of routine dental hygiene or preventive care. Beneficiaries who are unable to afford these preventive services could go without needed care, which could result in potentially avoidable expensive dental or medical treatments, as occurs today. Further, a catastrophic-only dental coverage approach could create incentives for providers to increase volume for certain procedures or perform higher-cost procedures so that beneficiaries more quickly reach the catastrophic threshold where Medicare coverage begins, which could result in higher costs for both beneficiaries and the Medicare program.
Doughnut-type dental benefit. Like the more limited dental benefit and catastrophic benefit, a doughnut-type benefit would help to provide coverage for the preventive services most beneficiaries need while also helping those who require higher cost services. It would also increase Part B premiums and program spending less than a comprehensive benefit. However, this option would expose beneficiaries to high dental expenses in the coverage gap, potentially creating financial barriers to care for those who are unable to cover these costs before qualifying for catastrophic protection. Like the catastrophic-benefit, this option could also create incentives for providers to increase volume for certain procedures or perform higher-cost procedures so that beneficiaries move through the doughnut-hole more quickly to reach the catastrophic benefit.
Cost sharing. A dental benefit in Part B would be subject to the standard annual Part B deductible, 20 percent coinsurance on each service, and balance billing protections, if designed to track other Part B benefits. Preventive dental benefits could be provided with no cost sharing, similar to other Part B preventive benefits, and as envisioned in some legislative proposals.11 Currently, private dental plans often cover preventive services with limited (or no) cost sharing required. Other dental benefits could be covered with a 20 percent coinsurance. Private dental insurers typically impose coinsurance that varies by service, with higher coinsurance required for more expensive procedures if covered, which can range from 20%-50%.12 Imposing coinsurance rates for Part B dental services that exceed 20 percent would make dental services less affordable for beneficiaries, but less costly for the Medicare program.
Annual caps. Private plans that cover dental services, including employer-sponsored retiree and individually purchased plans, often cap the annual amount the plan will pay for covered dental services. The median limit for private plans (not exclusive to the Medicare population) that impose such limits is $1,500.13 Among Medicare Advantage plans that offer dental benefits, caps are also common, with an average limit of around $1,300, and the most common limit being $1,000.14 No Medicare Part B benefits are currently subject to an annual dollar limit..Imposing an annual dollar cap on Medicare payments for dental services would limit the financial exposure of the Medicare program, and limit the potential increase in beneficiaries’ Part B premiums. However, beneficiaries would be exposed to unlimited expenses once they exceed the annual cap on covered benefits. They would continue to be responsible for the cost of relatively expensive dental treatments, which could make certain procedures, such as crowns and implants, beyond the reach of beneficiaries with modest incomes. For example, for an individual living on an income of $29,650 (the median per capita income for people on Medicare in 2019) and subject to a $1,000 cap on covered dental benefits, out-of-pocket expenses could easily exceed 10 to 20 percent of his or her income for extensive dental services, such as crowns, implants and dentures.15
Frequency limits. Private dental plans and Medicare Advantage plans with dental coverage often impose limits on the frequency of obtaining certain procedures a plan will pay for during a defined timeframe. For example, Medicare Advantage plans typically limit oral examinations and cleanings to once every six months. Dental plans could also limit the number of a specific procedure (e.g., x-rays, fillings) that may be covered each year. Some procedures and treatments may require longer periods of time between covered services, such as a periodontal exam once every three years or dentures once every five years.16.Frequency limits on certain dental services would help constrain the costs associated with the new dental benefit, help limit the impact on beneficiary premiums, and could conform to dental standards of care. However, Medicare Part B does not generally impose frequency limits for diagnostic or therapeutic services that must be covered.
Provider participation. A new Medicare Part B dental benefit would only succeed if a sufficient and geographically dispersed number of dentists elected to participate in Medicare, and accept Medicare payment rates. Medicare law already includes dentists in the definition of physician,17 but most dentists are currently not enrolled in the Medicare program and would have to choose to enroll in order to receive Medicare payments for Medicare-covered dental services.18.A government outreach strategy would help to inform dentists about the new benefit, encourage them to enroll in the program, treat Medicare patients, and submit bills to get paid by Medicare. Without robust participation among dentists in Medicare, some beneficiaries would continue to have problems accessing affordable dental care or would pay high out-of-pocket costs for the dental services they receive. Beneficiary education would also be needed so that beneficiaries understand the implications of receiving covered services from a dentist who has not enrolled in Medicare.
Payment and fee schedules. Currently, for the very limited circumstances under which Medicare pays for some dental services, Medicare makes payments to dentists based on the physician fee schedule. For services not included on the fee schedule, regional Medicare Administrative Contractors (MACs), which are responsible for administering Medicare claims, determine the payment amount. If a dental benefit were to be added to Part B, Medicare would need to modify the physician fee schedule to include payment amounts for routine and other dental services that are not currently covered or establish a separate fee schedule for dental services.19 The specifics of the fee schedule would affect the cost of the new benefit and the willingness of dentists to participate in the Medicare program. The physician fee schedule amounts paid by Medicare for each service reflect the amount of physician time, technical skill and judgment required (“work values”), the associated practice expenses (e.g., non-physician clinical staff, supplies, a share of other staff and overhead costs), and professional liability expenses..To develop a fee schedule for dental services, research would be needed to determine appropriate work values, practice expense, and liability to assign values for the covered dental services. In considering the appropriate level of payment, the American Dental Association (ADA) Survey of Dental Fees or similar information may be a useful reference point. To ensure that payments are for diagnostic and therapeutic services that are “reasonable and necessary” as broadly required under Medicare law, coverage and coding policies would be needed to monitor that payments are made appropriately..In addition, it would be important to consider whether to include dentists in the Merit-based Incentive Payment System and, if so, what measures to use to assess performance of dentists on quality of care, cost, promoting interoperability of electronic health records, and practice improvement activities. If dentists are included, a particular focus would need to be identification or development of consensus-based quality measures that focus on the oral health needs of Medicare beneficiaries.
Low-income beneficiaries. If Part B is expanded to include a dental benefit, about 10 million low-income beneficiaries who are dually eligible for Medicare and Medicaid would have their premiums for the new Part B dental benefit automatically paid on their behalf by Medicaid (jointly funded by states and the federal government) through the Medicare Savings Programs, just as is done for other Part B benefits. Beneficiaries eligible for full Medicaid benefits and Qualified Medicare Beneficiaries (QMBs) could also have their cost sharing paid at least in part by Medicaid (depending on the fees otherwise paid by Medicaid relative to Medicare dental fees). Unlike a separate, voluntary benefit, the process for low-income beneficiaries would be automatic, without a separate process to determine eligibility for assistance..The financial assistance would help with the increase in Medicare Part B premiums associated with the dental benefit for low-income Medicare beneficiaries who qualify for Medicaid and the Medicare Savings Programs. However, this would mean additional costs for states and the federal government. Many low- and moderate-income people on Medicare would not qualify for premium and cost-sharing assistance because their income and assets exceed eligibility levels for those programs.
Interactions with other insurance. Adding coverage of dental services to Medicare Part B would affect other sources of dental insurance, including coverage provided under some Medicare Advantage plans, individually purchased dental policies, employer-sponsored retiree dental coverage, and Medicaid. It would also affect Medigap policies that cover the 20 percent coinsurance under Part B. These spillover effects are discussed below.
Medicare Advantage. Most Medicare Advantage plans offer dental services (or access to dental insurance) as an optional “extra” benefit. If a dental benefit were added to Part B, all Medicare Advantage plans would be required to cover the dental benefits provided by traditional Medicare. Depending on the scope of covered benefits under Part B (e.g., comprehensive or preventive only), Medicare Advantage plans could provide supplemental dental benefits that wrap around the new Part B benefit.
With a new Part B dental benefit, Medicare payments to Medicare Advantage plans would rise because payments are based on per capita spending in traditional Medicare, and traditional Medicare per enrollee spending would likely increase with the new benefit. As a result, plans that currently provide some dental coverage would receive higher payments by Medicare to provide dental benefits under Part B, even if the dental coverage is similar to what they currently provide as a supplemental benefit. Additionally, these Medicare Advantage plans would have extra money to spend on new supplemental benefits since plans would likely be providing fewer dental supplemental benefits.
Individually purchased dental plans. A new Part B dental benefit would potentially replace private dental coverage currently purchased by an estimated 7.8 million Medicare beneficiaries in 2019; this would shift costs to Medicare that are currently covered by private plans and enrollees and potentially affect Medicare Part B premiums. While private insurers are not permitted to duplicate benefits covered under Medicare under current law, they would be able to offer coverage that supplements the new Part B dental benefit. Total out-of-pocket dental spending, including premiums, could decrease for individuals who drop their current dental coverage, since the federal government pays 75% of Part B premiums.
Employer-sponsored retiree dental plans. With a new Medicare Part B dental benefit, employers that currently offer dental benefits as a supplemental benefit for their retirees would either offer dental coverage that wraps around the Part B benefit, or drop dental coverage altogether, unless the law was written in a way to encourage employers to maintain these benefits (e.g., favorable tax treatment or direct subsidies). If employers scale back or drop retiree dental coverage, the costs otherwise incurred would be shifted from employer plans to Medicare. This would affect retirees unevenly, depending on the comprehensiveness and cost of their former employer’s dental coverage, and the network of dentists in their employer plan relative to those who participate in the Medicare program.
Medicaid. Medicaid and the Medicare Savings Programs would automatically cover the incremental cost of dental benefits under Part B for low-income beneficiaries. For states that currently cover some dental benefits for dually eligible beneficiaries, the new Part B benefit would shift costs from the states to the Medicare program for dental benefits, resulting in lower spending for these states. In 2019, the majority (77 percent) of full dually eligible beneficiaries lived in states that offered some dental benefits to full dual eligibles, covering about 5.7 million beneficiaries.20 At the same time, Medicaid spending on behalf of dually eligible individuals could increase to cover the higher Part B premiums associated with the new Medicare dental benefit, and coinsurance, to the extent Medicaid pays the coinsurance for covered Medicare services.
To reduce federal costs, it would be feasible to establish a maintenance-of-effort requirement for states, which would have uneven effects across states; those that provide adult dental coverage under Medicaid would be required to make a maintenance of effort payment on behalf of dually eligible beneficiaries, but states without adult dental coverage would not be subject to this requirement.
For dually eligible Medicare beneficiaries, a new Medicare Part B dental benefit could help to improve access to dental professionals across the country.
Medigap. Medigap does not currently cover dental services, but Medigap policies that currently cover Part B coinsurance, which includes most Medigap policyholders, would also cover the coinsurance for a Part B dental benefit. Thus, a new Medicare Part B dental benefit could increase Medigap premiums for beneficiaries with Medigap policies that cover Part B coinsurance.
Monitoring the effects of the new dental benefit. In establishing a new Medicare Part B dental benefit, policymakers may want to consider ways to monitor the extent to which improved dental care contributes to better health outcomes for Medicare beneficiaries, assess how well the new benefit is meeting the needs of a growing Medicare population, and develop recommendations as needed.21,22
IMPLICATIONS
Adding a dental benefit to Part B would provide subsidized dental coverage to virtually all Medicare beneficiaries, addressing a widely recognized gap in Medicare coverage, and doing so in a way that integrates dental care with other Medicare-covered medical services. Today, nearly half of all Medicare beneficiaries do not have dental coverage, and either pay for the services they receive out-of-pocket, or forego needed care.23 A dental benefit under Part B has the advantage of using a structure in place, rather than setting up a new and separate part of Medicare that would require its own set of rules and would contribute to the complexity of Medicare for beneficiaries. Unlike a new voluntary, stand-alone dental benefit (described below), a Part B benefit would be relatively straightforward for beneficiaries because dental services would be integrated seamlessly with other covered medical benefits.
Integrating dental into Part B does present some tradeoffs, however. All beneficiaries would be required to pay for the new dental benefit through increased Part B premiums, regardless of whether they need or use dental services. However, some beneficiaries may prefer to go without dental coverage to avoid a higher Part B premium, even one that is heavily subsidized by the federal government. Or, they may prefer to choose their own private dental plan based on their individual needs and circumstances. The overall impact of a new Medicare Part B dental benefit on beneficiaries would depend on a number of factors, including the scope and comprehensiveness of covered dental services, cost-sharing requirements, how much Medicare pays providers under the fee schedule, the extent to which dentists choose to participate nationwide and in underserved areas, and other factors.
A new Part B dental benefit would also increase Medicare spending, the magnitude of which would also depend on a number of factors, including the scope of covered services, premium and cost-sharing requirements, and payments to providers. A comprehensive dental benefit under Part B with the usual beneficiary cost sharing would likely add substantial costs to the Medicare program since Medicare typically pays 80% of the fee for Part B services, and nearly 55 million people are currently enrolled in Part B.24 Additionally, this approach would shift some costs from employer and union-sponsored plans, and Medicaid to the Medicare program, and would increase federal payments to Medicare Advantage plans.
Create a Voluntary Dental Benefit under a New Part of Medicare
Another option for strengthening dental coverage under Medicare would be to create a new, separate voluntary dental benefit, similar to the approach taken to provide prescription drugs under Medicare Part D. A new, voluntary dental benefit, offered on its own under a new part of Medicare, could operate similarly to the Medicare Part D prescription drug benefit, where beneficiaries would have the option to sign up for a new freestanding dental benefit for an additional premium. This approach would not require all Part B enrollees to have dental coverage and incur a higher premium, so it would likely cover a somewhat smaller share of the Medicare population than would be provided under Part B.
To operationalize this approach, several key issues would arise, such as determining the scope of covered benefits and cost-sharing requirements, as with the Part B approach. Additionally, the benefit could be administered by the government, through private dental plans only (such as those offered to individuals for purchase), or through a mixture of private plans and a government-administered program. Since the benefit would be separate from Part B, other issues would arise such as how to set premiums and government subsidies, encourage enrollee participation, ensure plan participation (if using private plans), set payments to plans (if using private plans) and/or dentists (if using a government-administered program), and finance the new benefit.
Private plans versus a government-administered program. A key consideration for this approach is whether to use only private plans (as in the current Part D program), a government-administered program, or a combination of the two. This decision would have spillover effects for payments to oral health providers, since such payments would either be determined by the government or by private plans. It could also have spillover effects for federal spending and beneficiary out-of-pocket costs, although the directionality of the effect is not clear..There are important trade-offs associated with these approaches. If the notion is to essentially have a Part B-like benefit but make it optional to beneficiaries, a government-administered dental program might be desirable. If instead the goal is to allow more variation in benefits and rely on private plans, rather than broaden the government’s role directly, then having competing private plans might be desirable. A government-administered program would lessen the number of choices beneficiaries need to make about enrolling in various parts of Medicare (which can be complex), but may also limit the ability to choose among a number of dental plans, which some may prefer. Seniors have said that they find the process of choosing a Medicare Advantage or Part D plan to be a frustrating and confusing process, and they could likewise have a similar experience with private Medicare dental plans.25 Relying on private plans might require additional government oversight and consumer protections.
Financing. Regardless of whether a new dental benefit is provided by private plans and/or the government, a key consideration would be how to fund the benefit (e.g., the allocation of spending across beneficiary premiums and federal government spending). Following the Part D model, a separate account could be created within the Supplementary Medical Insurance Trust Fund for tracking the premiums or other targeted funding for this new part of Medicare as well as payments made for dental benefits.
Premiums. Another important decision in establishing a separate benefit under Medicare is the methodology for establishing premiums and government contributions. If the government administered the benefit, government actuaries would need to calculate the expected per beneficiary cost of the benefit and the beneficiary premium amount. If private plans administered the benefit, an approach similar to that of the Part D prescription drug benefit could be taken, whereby the federal subsidy is determined based on the national average bid across all plans; beneficiaries are then required to pay the difference between the bid of the plan they elect and the national average bid.
Beneficiary participation incentives. If the dental benefit is offered separately from Medicare Part B, policymakers would need to establish rules to determine when and how beneficiaries would sign up for coverage, and whether to apply penalties for late enrollment. One potential concern with applying a penalty is that it makes the stand-alone dental benefit less “voluntary.” At the same time, with a purely voluntary approach, some individuals might wait to enroll in the dental plan until they know they need services and disenroll after receiving treatment, leading to adverse selection and driving up program costs and premiums..Imposing a late enrollment penalty, such as was done for Medicare Parts B and D, would discourage this behavior. For example, under Medicare Part D, Medicare eligible beneficiaries who do not have “creditable coverage”, meaning they do not have drug coverage where the actuarial value equals or exceeds the actuarial value of standard prescription drug coverage under Medicare, face a penalty for late enrollment. Policymakers would need to determine if existing dental plans count as creditable coverage. Using this kind of approach would encourage beneficiaries to sign up when they are first eligible, and build in safeguards against adverse selection.
Low-income beneficiaries. Unlike a Part B dental benefit option, assistance for low-income beneficiaries would not automatically happen for a new voluntary dental benefit. Low-income subsidies could be offered in a manner similar to the Part D program, or a different model could be adopted. For example, under Part D, Medicare beneficiaries with incomes at or below 150% of the federal poverty level are provided with financial assistance to help cover their Part D monthly premiums, annual deductible, coinsurance and copayments. In contrast to the Medicare Savings Program where premiums and cost sharing for low-income beneficiaries are jointly financed by federal and state dollars, they are paid in full by the federal government under Part D, such that assistance for these low-income Part D enrollees does not directly affect Medicaid spending. Under Part D, federal expenditures are partially offset by Medicaid payments on behalf of dually eligible beneficiaries under a mechanism known as the “claw back.”
Provider payments. As with the Part B approach, if a government-administered separate voluntary dental program was offered, it would be necessary to determine the level of Medicare payments allowed for the services provided by dentists and other oral health providers. Given that it would be a new part of Medicare law, decisions would need to be made about which of the rules and operations currently used for providers under Part B would be extended to providers under this new part. If instead the new dental benefit was offered exclusively by private plans, then private dental plans would determine a methodology for making payments to dental providers on behalf of their enrollees.
Plan participation. If private plans were used to deliver a new voluntary dental benefit, payments to plans would need to be designed in a way that encourages participation of private insurers while also limiting costs. To discourage plans from selectively enrolling lower-cost beneficiaries and limiting losses due to higher than expected expenditures, policymakers could consider a number of approaches, including risk adjustment, reinsurance, marketing oversight, and other measures, as they did with Medicare Part D..These mechanisms are used to encourage plan participation and market stability, but can also increase the federal costs of such a benefit, as has occurred with Medicare Part D.26 However, such provisions may be unnecessary, particularly if the new dental benefit has an annual cap on coverage, which would limit plans’ liability and associated risk. Annual caps on coverage are common among private dental plans, as noted earlier.
Plan requirements. If a new Medicare dental benefit is administered through private plans, Medicare would need to develop requirements for dental plans contracting with the federal government, and establish a mechanism for oversight and enforcement. These requirements could mirror the approach used for sponsors Medicare Advantage and Medicare Part D plans that contract with the government to provide covered services. As with the Part B option above, dental plan requirements would need to address issues such as the scope of benefits, cost sharing, and coordination of benefits with other dental coverage, among others. However, some additional requirements would need to be assessed if contracting with private plans, such as standards for provider networks, oversight and audits, and the conditions under which Medicare Advantage plans can offer the dental benefit and integrate it with other medical benefits.
Coordination with current sources of dental coverage. A separate, voluntary dental benefit could be designed in a way to have fewer spillover effects than a Part D benefit if beneficiaries are able to maintain their current sources of dental coverage. To limit the increase in federal spending associated with dental coverage, policymakers could consider strategies to encourage other sponsors of dental coverage to maintain benefits..For example, when the Part D benefit was implemented, the retirement drug subsidy (RDS) program was enacted to encourage employers and unions to continue providing prescription drug benefits to their Medicare-eligible enrollees, which reduced Part D spending. Employer and union-sponsored plans that provided actuarially equivalent coverage to the Part D benefit were reimbursed for a portion of their qualifying employees’ costs for prescription drugs. Similarly, a new dental benefit could conceivably be designed to minimize substitution effects: for example, Medicare could deem qualified dental plans as creditable coverage and waive any late enrollment penalties for individuals enrolled in these plans. With an approach that allows for creditable dental coverage, policymakers would need to assess modifications to current law rules with respect to non-duplication of Medicare benefits. However, without such incentives to maintain other public and/or private sources of dental coverage, a Medicare dental benefit would likely replace other sources of coverage.
IMPLICATIONS
The approach of creating a voluntary dental benefit under a new part of Medicare, rather than including a dental benefit in Part B, would present trade-offs, which would impact coverage, spending and premiums. Unlike the Part B option, only beneficiaries who choose to enroll in this dental coverage would pay higher premiums. A voluntary dental benefit would likely cover fewer beneficiaries than a Part B approach, allowing beneficiaries to retain their current sources of dental coverage (if allowed under program rules), which could have a smaller impact on Medicare spending.
Under a voluntary approach separate from Part B, the program could be more likely to suffer from adverse selection, particularly in the absence of a penalty for late enrollment. This has the potential to increase premiums for beneficiaries who enroll in the new dental part of Medicare, and increase per capita Medicare spending. Also, if fewer people enroll because coverage is not integrated into Part B, many could continue to go without dental coverage and potentially forego needed care, or incur high costs.
An approach that creates a separate, optional benefit under Medicare would also add to the complexity of choices for Medicare beneficiaries, who currently face complicated decisions about enrolling in Medicare Parts A and B, choosing among Medicare Advantage plans or Medicare Part D plans, or Medigap policies. The complexity would be even greater if structured like Part D, with multiple competing private plan options available. At the same time, the availability of many private plan options would increase patient choice, and allow beneficiaries to shop for a dental benefit package that best suits their oral health needs.
As with an option to add a dental benefit to Medicare Part B, the impact on beneficiaries and program spending would depend on a variety of policy decisions, such as the scope of benefits, premiums and cost-sharing requirements, payment rates to providers (or plans), provider participation, and spillover effects on other sources of dental coverage.
Medicare spending could also be affected by whether the benefit is government-administered or administered by private plans that contract with the government to provide these services. A government-administered plan could constrain costs if Medicare fees for dental services are lower than the rates paid by private insurers, as is now the case for physician services.27 A more market-oriented approach, modeled on Part D, could also put downward pressure on costs and premiums through competition among private dental plans. Based on the available evidence, it is unclear whether private plans or a government-administered dental benefit would lead to lower prices and lower Medicare spending.
Permit Greater Access to Medically Necessary Dental Services under Medicare
Expanding the circumstances under which dental coverage is deemed medically necessary is another possible approach to broadening access to dental care for Medicare beneficiaries. While this approach would increase the number of people who could get some dental coverage through Medicare, fewer beneficiaries would qualify for dental coverage than by adding a comprehensive Part B benefit or a voluntary freestanding benefit.
Scope of current law. The Centers for Medicare & Medicaid Services (CMS) has interpreted the Medicare statute to cover only dental services that are “incident and integral to” a covered procedure and are performed by a dentist under Medicare Part B; routine dental services are excluded from Medicare coverage under current law except when the patient’s condition necessitates inpatient hospitalization for dental services otherwise excluded from coverage. In this case, only the hospital can be paid under Medicare Part A. CMS recognizes some exceptions to the dental exclusion, such as extractions done to prepare the jaw for cancer radiation treatment, and inpatient oral examinations (but not treatment) preceding kidney transplants or heart valve replacements in certain settings.28 Medicare also covers some dental-related emergency department visits and hospitalizations, but does not cover the cost of the dental care itself.29.The extent to which current law provides flexibility for Medicare to cover additional dental services, particularly services needed for the treatment or management of life-threatening medical conditions, is currently the subject of discussion. The Administrator of CMS has indicated that the agency is reviewing its statutory authority to broaden coverage for additional oral health services, the outcome of which is unclear.30 If the availability of Medicare coverage for dental treatment is not expanded as a result of the review, the law could be changed to broaden coverage for medically necessary dental services, and, for example, cover dental services for people with specific medical conditions or in certain clinical situations.
Medically necessary dental care. Under this option, and in the absence of a change in interpretation of Medicare statute by CMS, Congress could enact legislation to allow Medicare coverage for a wider range of clinical conditions that require dental treatment. For example, Medicare could cover treatment of any dental conditions that needs to be addressed in the context or management of organ transplant procedures, heart valve repair and replacement, stem cell transplantation, cancer chemotherapy, joint replacements, immunosuppression, and bisphosphonate therapy. Dental services could also be made available to individuals with specified chronic conditions, such as diabetes and cardiovascular disease, for which dental services have been associated with improved health outcomes..This option would provide dental coverage to fewer beneficiaries, but would require many of the same decisions as the two prior approaches. The clinical conditions and circumstances that would be covered (as exceptions to the current dental coverage exclusion) could be defined in the law. Alternatively, the Secretary or an independent scientific body, such as the National Academy of Medicine (NAM), formerly the Institute of Medicine (IOM), could be called upon to review clinical evidence and identify the appropriate contexts for medically necessary dental coverage under Medicare. Once these clinical contexts are identified, Medicare could use its normal process for determining which services would be covered..In 2000, the most recent review undertaken, the IOM/NAM assessed the dental exclusion under Medicare and the circumstances under which Medicare should “broaden the scope of the exceptions to include dental care needed to prevent or effectively manage systemic conditions, including the oral complications of specific illnesses or their medical treatment.” The IOM report noted a general lack of evidence regarding the medical necessity of dental services, and recommended further research to develop recommendations on a condition-by-condition basis for coverage of dental services needed in conjunction with surgery, chemotherapy, radiation or pharmacological treatment of a life-threatening condition.31 Despite IOM’s assertion that more direct evidence is needed to demonstrate the medical necessity of dental interventions, substantial additional research has not been generated on this topic and no formal recommendations have been produced.
Payment for dental services. Currently, payments by Medicare to dentists for the services covered are generally based on the physician fee schedule, with MACs determining the payment amount for services not on the fee schedule. If dental coverage was broadened, more comprehensive payment policies would likely need to be developed, similar to the option for adding a dental benefit to Part B. In addition, as with the Part B option, coverage policies (e.g., National Coverage Determinations) would need to be established to guide MACs and clarify the scope of Medicare coverage.
IMPLICATIONS
Broadening the definition of medically necessary dental care under current law would expand access to dental services for the subset of beneficiaries with the specified medical conditions or circumstances. This option could potentially help those who stand to gain the most in terms of health outcomes; however, it would not address the oral health needs of those whose dental issues do not meet a definition of “medically necessary.” The cost to the federal government would depend on the number of conditions and circumstances covered, the scope of services covered, the potential to reduce or prevent other medical costs, and Medicare payments for the services.32 The impact on Medicare spending and Part B premiums would likely be smaller than in the Part B approach, because fewer people would be expected to qualify for medically necessary services.
Test Models for Dental Coverage
Another option could be to use the demonstration authority through the Center for Medicare and Medicaid Innovation (CMMI) to test approaches to dental coverage for the Medicare population. A model would help to gather information about the potential costs and savings of adding a dental benefit to Medicare. The CMMI was created to test models and the Secretary can permanently authorize those that either achieve savings without reducing quality of care, or improve the quality of care without increasing spending.
Possible models could include testing the effects of providing dental coverage for Medicare beneficiaries on subsequent emergency department use and medical expenditures. Such a model could include Medicare beneficiaries broadly, target to specific geographic regions or states, or focus on those with specific clinical conditions, such as those with diabetes. Use of services under different cost-sharing designs could be tested as well. This type of model would provide useful data on the potential cost to the federal government of covering dental services. The CMMI could draw on data from Medicare Advantage plans that provide dental coverage in developing this model.
IMPLICATIONS
Innovative models are generally small in scale and relatively low-cost. By design, few beneficiaries would gain coverage unless the lessons learned evolved to broader policy change. However, models offer an opportunity to identify strengths and weaknesses of the approaches tested and, in this way, could inform future efforts to provide enhanced coverage more broadly.
Offer Dental Discount Cards
Another approach could be to provide Medicare beneficiaries with dental discount cards or another form of cash assistance to help cover the cost of oral health services, similar to what was done in the period before the Medicare Part D benefit was fully implemented. In that case, beneficiaries enrolled in Part A or B (except beneficiaries who received Medicaid drug coverage) were provided the opportunity to enroll in the Medicare Prescription Drug Discount Card program under which they could obtain negotiated discounts on retail prescription drug prices, with card sponsors taking into account rebates, discounts, and other subsidies in order to achieve these negotiated discounts.33
In the case of the temporary discount card program, drug card sponsors were required to cover at least one drug in 209 classes of drugs that were most commonly used by Medicare beneficiaries and were allowed to charge up to a $30 annual fee to purchase the card. A transitional assistance (TA) subsidy was also provided to low-income beneficiaries (those with incomes at or below 135% of the federal poverty level) of up to $600 per year, as long as these beneficiaries did not receive drug coverage from other sources, including Medicaid, TRICARE, group health insurance, or Federal Employee Health Benefit Plans. These cards primarily assisted people who did not currently have prescription drug coverage.
To operationalize a Medicare discount card approach for dental care, a number of factors would need to be considered, including whether to design and build such a program to be transitional (on the path to a Medicare dental benefit) or permanent. Other policy questions to consider include: which entities could administer the program, which dental services and procedures would be covered, including any service limits; how fees for each procedure would be determined and by whom, who would be eligible to purchase the cards, how the discount would be funded, how dentists would be encouraged to participate in this program, and how dental providers would receive reimbursement for services rendered. In addition, some consideration would need to be given to how such an approach could be structured to help low-income beneficiaries, including those who are currently eligible for dental benefits through Medicaid. Each of these decisions would affect the cost to the Medicare program, and the extent to which it provides meaningful improvements for beneficiaries in terms of out-of-pocket costs and access to dental care.
IMPLICATIONS
A discount card could reach a broad group of beneficiaries as most could be eligible to take advantage of this benefit. This approach could potentially make dental services somewhat more affordable for people who currently have limited or no dental coverage because the card would provide access to negotiated rates on dental services. However, the extent to which it could help improve access or reduce costs would depend on many factors, including the value of the discount for beneficiaries and the extent to which dental providers participate in the new arrangement.
Launching a temporary or permanent discount program would require many of the same administrative decisions as with the first two options, but would likely have less of an impact on beneficiaries’ oral health care. Medicare would have to establish the discount fee schedule, contract with a network of dentists who agree to provide services at those rates, establish and maintain other requirements for those participating dentists, and ensure provider compliance with the program requirements. If, instead, Medicare contracted with private plans to carry out these functions, it would need to establish rules for the contractors and provide oversight to ensure beneficiary protections are in place.
A dental discount card approach could be less expensive than the Medicare Part B or separate voluntary dental plan options discussed previously, depending on the level of funding allocated to the program. Low-income beneficiaries who are currently unable to afford to purchase dental coverage, or who live in a state with limited or no adult dental care provided under Medicaid, may also benefit if additional assistance was provided to these individuals, as was done under the Part D program. However, even with additional financial assistance, many low- and middle-income beneficiaries may still not be able to afford all the dental services they need with this approach. The scope of the network of participating dentists and the extent of the discounts would determine how useful this approach would be to improving beneficiary access to dental services.
A dental discount card approach could be designed in a way to be less costly to the Medicare program than the other approaches that establish a dental benefit covered by Medicare – a trade-off with direct implications for beneficiary spending. Even so, Medicare would still incur higher costs associated with providing access to discounted services. Depending on how these costs are financed, beneficiaries may also be expected to make a contribution to obtain access to the discounted fees, as was the case with the temporary prescription drug program. Costs aside, policymakers would need to resolve several operational issues, including whether to administer the discount card directly or through a private contractor and how to engage a sufficient number of dentists nationwide to make the program work.
Conclusion
Numerous studies confirm the importance of oral health as an integral component of medical care and improved health outcomes.34 Untreated oral health issues can negatively impact qualify of life, lead to serious health complications, and can exacerbate certain chronic conditions and diseases such as diabetes and cardiovascular disease. Lack of oral health care can also delay diagnosis of certain physical health conditions and result in costly emergency room visits.35 Since the start of the program, Medicare has not covered routine dental care. While about half of Medicare beneficiaries have coverage through other sources, such as Medicare Advantage, Medicaid, and private plans, most beneficiaries do not have any dental coverage at all. Lack of dental coverage means that dental care is out of reach for many beneficiaries who cannot afford to pay out-of-pocket for their care.
In light of these challenges, a number of options could be considered to broaden oral health coverage to Medicare beneficiaries. Two approaches would add a dental benefit under Medicare either by expanding dental benefits under Part B or by adding a new voluntary dental benefit under a new part of Medicare. Other approaches could include permitting greater access to medically necessary services, testing models to expanding dental care, and offering dental discount cards. Policy options could be designed to reach all beneficiaries or targeted to a subset of beneficiaries (e.g., those needing medically necessary treatments or low-income beneficiaries). These approaches would also have different financial effects on the federal government, beneficiaries, taxpayers, and other payers depending on the scope of services covered, required beneficiary contributions, and other factors. These approaches vary in the extent to which they would improve beneficiaries’ oral health care and improved health outcomes.
Meredith Freed, Gretchen Jacobson, and Tricia Neuman are with KFF.Lisa Potetz is with Health Policy Alternatives, Inc.This brief was funded in part by the AARP Public Policy Institute (PPI).KFF retains complete control over all of its policy analysis content.
Endnotes
U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General.
Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health, 2000; Schenkein HA, Loos BG. Inflammatory mechanisms linking periodontal diseases to cardiovascular diseases. J Clin Periodontol 2013;40 (Suppl. 14):S51–S69 https://onlinelibrary.wiley.com/doi/epdf/10.1111/jcpe.12060; Teeuw WJ, Gerdes VE, Loos BG. Effect of periodontal treatment on glycemic control of diabetic patients: a systematic review and meta-analysis. Diabetes Care 2010;33(2):421-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2809296/pdf/zdc421.pdf; Preshaw PM, Alba AL, Herrera D, et al. Periodontitis and diabetes: a two-way relationship. Diabetologia 2011;55(1):21-31. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3228943/#CR7; Allareddy V, Rampa S, Lee MK, et al. Hospital-based emergency department visits involving dental conditions. The Journal of the American Dental Association 2014;45(4):331–337. https://jada.ada.org/article/S0002-8177(14)60010-6/fulltext; Okunseri C, Okunseri E, Thorpe JM, Xiang Q, Szabo A. Patient characteristics and trends in nontraumatic dental condition visits to emergency departments in the United States. Clin Cosmet Investig Dent 2012;4:1-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3652363/↩︎
The original National Coverage Determination for renal transplant issued in 1979 provided for oral health examination. (Medicare National Coverage Determination Manual, 100-03, Section 260.6) However, subsequent Medicare coverage decisions for other organ transplantation procedures did not specify coverage of an oral examination prior to the procedure. ↩︎
Medicare law requires that to be covered, items and services must be reasonable and necessary. This means that if a dental benefit were added to Medicare, dental services would need to be medically necessary to be covered. Preventive services are only covered when specified by law. ↩︎
See National Association of Dental Plans. Dental Benefits Basics: What do dental plans normally cover? $1,500 is median annual limit in 2016 for dental preferred provider organization (PPO) plans. https://www.nadp.org/Dental_Benefits_Basics/Dental_BB_2.aspx↩︎
From the definition of physician at section 1861(r) of the Social Security Act: “… (2) a doctor of dental surgery or of dental medicine who is legally authorized to practice dentistry by the State in which he performs such function and who is acting within the scope of his license when he performs such functions…” ↩︎
If Medicare created a new dental benefit that followed existing law, in order for dentists to provide Medicare-covered dental services to Medicare beneficiaries, dentists would either have to 1) enroll in Medicare and submit claims on a beneficiary’s behalf for those services 2) opt-out of Medicare and enter into a private contract with the beneficiary for those services or 3) furnish Medicare-covered services for free. For more information, please see Christina Boccuti, “Paying a Visit to the Doctor: Current Financial Protections for Medicare Patients When Receiving Physician Services,” Kaiser Family Foundation, November 2016. https://modern.kff.org/medicare/issue-brief/paying-a-visit-to-the-doctor-current-financial-protections-for-medicare-patients-when-receiving-physician-services/↩︎
A small number of individuals who are eligible for Medicare Part A only if they pay a monthly premium are not eligible to enroll in Part B. More common are beneficiaries who become eligible for Part A at age 65 but delay enrollment in Part B at that time because they are working and have health insurance coverage through an employer plan. ↩︎
2019 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. ↩︎
Institute of Medicine. 2000. Extending Medicare Coverage for Preventive and Other Services. Washington, DC: The National Academies Press. https://doi.org/10.17226/9740↩︎
Inside Health Policy. Advocates Seek Medically Necessary Oral Health Care, CMS Eyes Issue. January 29, 2019. ↩︎
The 2000 IOM report also concluded that given limited evidence, “the severe consequences of radiation-induced osteoradionecrosis, and Medicare’s investment in treating patients with head and neck cancer, it is reasonable for Medicare to cover both tooth-preserving care and extractions, which may be medically appropriate for certain patients. The report further concluded that given limited evidence, “the severe consequences of septicemia and other complications of chemotherapy, and Medicare’s investment in treating leukemia patients, it is reasonable for Medicare to cover a dental examination, cleaning of teeth, and treatment of acute infections of the teeth or gums for a leukemia patient prior to chemotherapy.” ↩︎
Institute of Medicine. 2000. Extending Medicare Coverage for Preventive and Other Services. Washington, DC: The National Academies Press. APPENDIX C: Medically Necessary Dental Services. https://doi.org/10.17226/9740↩︎
See for example: U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health, 2000; IOM (Institute of Medicine) and NRC (National Research Council). 2011. Improving access to oral health care for vulnerable and underserved populations. Washington, DC: The National Academies Press. ↩︎
U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General.
Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health, 2000; Allareddy V, Rampa S, Lee MK, et al. Hospital-based emergency department visits involving dental conditions. The Journal of the American Dental Association 2014;45(4):331–337. https://jada.ada.org/article/S0002-8177(14)60010-6/fulltext; Okunseri C, Okunseri E, Thorpe JM, Xiang Q, Szabo A. Patient characteristics and trends in nontraumatic dental condition visits to emergency departments in the United States. Clin Cosmet Investig Dent 2012;4:1-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3652363/↩︎
A new KFF/Washington Post survey probes in depth what Americans know and think about climate change, their personal involvement with the issue, and their willingness to accept trade-offs to reduce its impact. A parallel survey of teens ages 13-17 explores how they view the potential effects of climate change on their generation.
The poll finds that a large majority of adults and teens believe that human activity is causing changes to the world’s climate. About half of adults believe people need to act within the next 10 years to prevent the worst effects of climate change or that it is already too late.
One in four adults say they personally have taken action to express their views on climate change, such as donating to a climate change charity, contacting a government official, or joining a protest, rally or other event.
Most adults say they would support higher taxes on the wealthy or on companies that burn fossil fuels to pay for policies aimed at reducing greenhouse gas emissions. Far fewer, however, say they would be willing to pay higher taxes at the gas pump or an extra $10 per month on their electricity bills.
Among teenagers, most say they feel that there are things they can do personally to make a difference when it comes to reducing the effects of climate change. About four in ten say they have taken action to reduce their own carbon footprint. And one in four say they personally engaged in political action on climate change – either participating in a school walkout, protest or rally, or contacting a government official about the issue.
As with adults, most teenagers see climate change as a major problem, though it does not stand out as a defining issue for their generation. About as many teens say climate change is “extremely important” to them personally as say the same about health care, gun policy and the economy.
The poll also probed support for specific policy solutions, perceptions of the urgency of the problem, frequency of discussions, and the politics of climate change. Additional findings related to the public’s knowledge and views of the major causes of climate change and the role climate change plays in severe weather events will be released in the near future.
This survey is the 34th in a series of surveys dating back to 1995 that have been conducted as a part of The Washington Post/KFF Survey Project. All surveys in the series are designed and analyzed jointly by survey researchers at KFF and The Washington Post. The survey was conducted online and by telephone July 9-Aug. 5 among a nationally representative sample of 2,293 adults ages 18 and over and 629 teens ages 13-17. The sample was drawn through the AmeriSpeak panel, the probability-based panel of NORC at the University of Chicago. Results have a margin of sampling error of plus or minus 3 percentage points for adults and plus or minus 5 percentage points for teens. A report highlighting key findings is available at kff.org. The Washington Post’s journalism drawing on the survey findings is available at washingtonpost.com.
As the debate over the future direction of our health care system heats up leading into the 2020 Presidential election, several Democratic proposals to create a single, federal, universal health insurance program known as Medicare-for-all have garnered significant attention. These proposals would replace most current public and private health insurance with a new federal program that would guarantee health coverage for all or nearly all U.S. residents. However, many details about how a new public program would be implemented and financed are not yet known. While much attention has focused on the implications of ending private insurance and Medicare, the debate has largely ignored the effects on the low-income and vulnerable populations covered by Medicaid and the broader implications for states of eliminating the Medicaid program. Key changes related to Medicaid under current proposals include:
The Medicare-for-all debate has largely ignored the effects on the low-income and vulnerable populations covered by Medicaid and the broader implications for states of replacing the Medicaid program. @KFF explores those issues in this brief.
Medicare-for-all proposals would generally eliminate current variation in eligibility, enrollment and renewal processes, benefits, and payment and delivery systems that are part of the current structure of Medicaid where states have considerable flexibility to design programs within broad federal rules.
Proposals would extend coverage for certain Medicaid services important to vulnerable populations (such as comprehensive benefits for children and non-emergency medical transportation) to other populations. The proposals would continue Medicaid protections against high out-of-pocket costs.
One of the most fundamental changes under Medicare-for-all would be uniform coverage of community-based long-term care services for all Americans. Medicaid is the primary payer for these services today, with substantial state variation in eligibility and coverage. Under current Medicare-for-all proposals, these services would be required and explicitly prioritized over institutional services. Medicare-for-all proposals vary as to whether they would include institutional long-term care, such as nursing homes, or instead continue the current Medicaid coverage of these services, locking in state spending, variation in benefits across states, and limited access to populations beyond Medicaid.
Some proposals would have the federal government assume all or a significant share of the nearly $222 billion in state spending on Medicaid, leading to significant state savings, while other proposals call for a maintenance of effort for all or some current state Medicaid spending.
The proposals would shift responsibility for designing and implementing much of health policy from states to the federal government, in contrast to states’ role under Medicaid today.
Introduction
As the debate over the future direction of our health care system heats up leading into the 2020 Presidential election, several Democratic proposals to create a single, federal, universal health insurance program known as Medicare-for-all have garnered significant attention. These proposals would replace most current public and private health insurance with a new federal program that would guarantee health coverage for all or nearly all U.S. residents, though many details about how a new public program would be implemented and financed are not yet known. While much attention has focused on the implications of ending private insurance and Medicare, the debate has largely ignored the effects on the low-income and vulnerable populations covered by Medicaid and the broader implications for states of eliminating the Medicaid program.
Multiple Medicare-for-all proposals have been introduced in Congress and advanced by Presidential candidates. Currently, the proposals are characterized by two main approaches: proposals that create a single-payer system and eliminate other forms of coverage, including employer-sponsored insurance, Medicare and Medicaid; and proposals that eliminate the Medicare and Medicaid programs but maintain a role for private insurance. Medicare-for-all bills proposed by Rep. Pramila Jayapal (HR 1384) and Sen. Bernie Sanders (S. 1129) and endorsed by Presidential candidates Sen. Elizabeth Warren, Sen. Cory Booker, and Andrew Yang adopt the former approach. A Medicare-for-all proposal offered by Sen. Kamala Harris takes the latter approach. Each of these proposals differs in some way from the others. However, for purposes of this brief, we refer to these proposals collectively as Medicare-for-all, though we note where important differences in the proposals may have different implications for Medicaid.
Medicaid is administered by the states, and each state’s program is unique, reflecting states’ use of existing program flexibility and waiver authority to design their programs. Because of this variation, the specific implications of a shift from Medicaid to a Medicare-for-all program would vary across states. However, in all states, Medicaid plays a key role by providing affordable health coverage for vulnerable populations that includes a wide range of medical, behavioral health, and long-term care benefits. It also is the largest source of federal funds to states. This issue brief explores key ways in which a shift to Medicare-for-all could affect current Medicaid enrollees, future enrollees (such as those who may need long-term care coverage at a later time), and states, which jointly finance the Medicaid program along with the federal government. Table 1 summarizes key similarities and differences regarding eligibility, benefits, affordability, provider payment and delivery systems, and state financing in the main Medicare-for-all proposals and Medicaid.
Medicaid covers a broad array of medical, behavioral health, and long-term care services. The Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) benefit for children provides comprehensive coverage including preventive screenings, vision, dental, and hearing services, and any other medically necessary care. Federal standards outline minimum benefits for adults, such as hospital, physician, and nursing facility services. States also can cover a variety of optional benefits, such as prescription drugs and private duty nursing. Medicaid is the principal source of coverage for long-term services and supports (LTSS), including nursing home care as well as home and community-based services that enable seniors and people with disabilities to live independently. While all state Medicaid programs cover a comprehensive set of services, because states have flexibility to provide optional services for adults, there is significant variation across states.
Medicaid provides affordable coverage for its low-income enrollees. Federal standards prohibit states from charging premiums to those with incomes less than 150% of the federal poverty level (FPL), though some states impose premiums for certain adults through a Section 1115 waiver. Federal rules also limit cost-sharing to nominal amounts and entirely exempt certain groups and services from any cost sharing. Aggregate out-of-pocket costs for an individual may not exceed 5% of family income.
Medicaid provides access to a broad range of providers, including many with unique expertise in treating vulnerable and low-income populations. States set provider payment rates within broad federal guidelines, and as a result, there is significant variation across states in how provider rates are determined and in payment levels. Despite lower payment rates in Medicaid and gaps in access to some types of specialists, national data show that access to services for children and adults is comparable to private insurance and exceeds access for the uninsured. Medicaid programs contract with a broad range of providers, including many safety net clinics, hospitals, and other providers that have experience in meeting the needs of Medicaid’s vulnerable enrollees. Managed care has become the dominant Medicaid delivery system, though states have substantial flexibility in designing their delivery and payment systems.
Medicaid is financed jointly by the federal government and the states, guaranteeing federal matching payments to states with no pre-set limit. The matching structure of the program provides states with resources that automatically adjust for demographic and economic shifts, rising health care costs, and changing state priorities. This structure also enables the program to respond to public health emergencies and natural and other disasters. Examples of this response include providing a coverage safety net to people affected by the HIV/AIDS epidemic and expanding eligibility and benefits for children and pregnant women exposed to high levels of lead during the Flint water crisis. Recessions, rising costs of prescription drugs, and increasing needs for long-term care and behavioral health services are factors that put upward pressure on Medicaid spending growth. However, over time, Medicaid growth per enrollee has been lower than private health spending. Medicaid is a significant spending item in state budgets, but also the largest source of federal revenues due to the matching structure.
Implications of Medicare-for-all for Medicaid
Eligibility, Coverage, and Enrollment
Medicare-for-all programs would establish universal national health coverage for all or nearly all U.S. residents, eliminating the need for the specific eligibility pathways in the current Medicaid program. Medicare-for-all programs would establish uniform eligibility criteria across all states that are tied to U.S. residency and not based on income. Notably, Medicare-for-all would eliminate the current variability in eligibility for health coverage across states and fill in coverage gaps in states that have not adopted the ACA’s Medicaid expansion. Under Medicaid, states must cover certain populations, such as very low-income parents and children, pregnant women, and poor people with disabilities who receive federal Supplemental Security Income (SSI) benefits. States then choose from a variety of optional coverage pathways and waiver authorities to expand coverage, especially for children with significant disabilities and seniors and adults with disabilities who need long-term care. While all states currently adopt at least one of these optional expansions, Medicaid eligibility criteria differ across states. Medicare-for-all programs would eliminate the need for specialized eligibility determinations based on disability or functional status. How current Medicaid enrollees, particularly those with complex health care needs, would be transitioned to a new coverage plan, is an important policy and implementation issue in the new proposals.
Immigrants’ eligibility for coverage under Medicare-for-all is unclear, while their coverage under Medicaid today is subject to limitations. Medicare-for-all proposals grant authority to the Health and Human Services Secretary to define residency when determining eligibility for coverage, so it is not yet known how undocumented immigrants would be treated, though some proposals specifically cover legal immigrants and certain undocumented immigrants. Many Democratic candidates running for President say they support coverage for undocumented immigrants. Most legal immigrants are barred from Medicaid coverage for five years after entering the United States (except in the 35 states that have taken up the option to eliminate the five-year waiting period for Medicaid/CHIP coverage for lawfully-residing immigrant children and/or pregnant women). Undocumented immigrants are not eligible for Medicaid coverage, although state Medicaid programs reimburse providers for emergency care for individuals who are otherwise eligible for Medicaid except for their immigration status.
A process for auto-enrolling individuals into coverage under Medicare-for-all programs would replace existing application and renewal processes in Medicaid. Once established, all of the Medicare-for-all proposals call for automatically enrolling individuals in coverage at birth. Auto-enrollment would result in higher coverage rates compared to the current Medicaid program, since not everyone who is eligible for Medicaid presently is enrolled. Each state administers its own Medicaid eligibility determination system. The ACA included new policies and strategies to streamline the eligibility and enrollment process, such as greater reliance on electronic data sources instead of paper verification, in an effort to keep eligible people enrolled in coverage. Nevertheless, the need to apply for and periodically renew Medicaid coverage can sometimes result in eligible individuals churning in and out of coverage.
Benefits
Medicare-for-all programs would cover a comprehensive set of health care services for adults that would eliminate the current variability in Medicaid benefit packages across states. For example, the Medicare-for-all proposals include some benefits that are optional in Medicaid for adults and consequently not available in all states, such as dental and vision care. The Medicare-for-all benefit package also would include mental health and substance use treatment services. While all state Medicaid programs cover mental health and substance use disorder services, the scope of coverage for adults can vary. Many states rely on Medicaid to cover specialized behavioral health services, and the Medicare-for-all proposals would include some of these benefits. For example, the Sanders and Jayapal proposals include day treatment and psychosocial rehabilitation for those with chronic mental illness. Also, although prescription drug coverage is not required by the Medicaid statute, all states cover this benefit. Medicaid must cover all drugs with a rebate agreement as medically necessary, but states may apply utilization controls such as prior authorization, a preferred drug formulary, or quantity limits on drug refills or pills per prescription, and those differ across states. While Medicare-for-all proposals would establish uniform coverage for prescription drugs across states, it is unclear if coverage would be as comprehensive. Under both Medicare-for-all and Medicaid, all covered services must be determined medically necessary.
Medicare-for-all would cover certain services important to vulnerable populations that currently are covered by Medicaid but not other payers. In current Medicare-for-all proposals, these include the EPSDT benefit that provides a comprehensive set of services for children as well as non-emergency medical transportation to access medical appointments, with the Sanders and Jayapal proposals limiting this benefit to those with low incomes and/or disabilities.
One of the most fundamental changes under Medicare-for-all would be uniform coverage of community-based long-term care services; Medicaid is the primary payer for these services today, with substantial state variation in eligibility and coverage. Medicare-for-all would cover many of the community-based long-term care services covered by Medicaid today. And, unlike Medicaid, where most community-based long-term care services are optional, these services would be required, and explicitly prioritized over institutional services, under Medicare-for-all. With community-based long-term care services included in the Medicare-for-all benefit package, everyone would be eligible to receive covered services without regard to income or assets, unlike in Medicaid today. The Jayapal proposal includes functional eligibility criteria (e.g. limitation in an activity of daily living) to qualify for LTSS; today, states set Medicaid LTSS functional eligibility criteria. Unlike other Medicaid services, states are allowed to cap enrollment for many community-based long-term care services, which means that some people who meet the eligibility criteria do not receive them. Including these services in Medicare-for-all could mean that individuals currently on state Medicaid waiver waiting lists as well as others who are not financially eligible for Medicaid could have access to these services. However, it could take time to develop adequate system capacity in terms of infrastructure and workforce to accommodate such an expansion in paid LTSS. Additionally, the cost of providing a universal long-term care benefit package could result in some limitations or restrictions on these benefits as more details are known and Medicare-for-all is implemented.
Medicare-for-all proposals vary as to whether they would include institutional long-term care, such as nursing homes, or instead continue the current Medicaid coverage of these services. Under a scenario where Medicare-for-all includes institutional long-term care, all enrollees would receive these services as part of their basic benefit package as medically necessary, without regard to income or asset limits. The Jayapal proposal includes functional eligibility criteria for institutional long-term care, as it does for HCBS. The Jayapal benefit package includes a range of institutional services, which could also include institutions for mental disease (IMDs) and intermediate care facilities for those with intellectual or developmental disabilities (ICF/DD). Medicaid currently covers ICF/DD services but generally does not cover services in IMDs for individuals ages 21-64. If institutional services are carved out of Medicare-for-all and instead continue to be provided through state Medicaid programs, as under the Sanders bill, then individuals would need to continue to meet current eligibility criteria for these services, which vary across states. Under this approach, states would also be required to continue to pay their state share of costs for these services based on the current federal Medicaid matching rules. Those not eligible for Medicaid would continue to have to pay for institutional long-term care out of their own income and assets or through private long-term-care insurance, or spend-down to be eligible for Medicaid. The Sanders Medicare-for-all program would require states to maintain their existing Medicaid eligibility standards and spending on institutional long-term care services and would continue to provide states with federal matching payments for these services, locking in variation in eligibility standards across states.
Premiums and Cost Sharing
Medicare-for-all would continue the protections that Medicaid provides against high out-of-pocket costs. Medicare-for-all programs would eliminate or reduce premiums and cost sharing. The Sanders and Jayapal proposals would eliminate premiums and deductibles, and the Jayapal proposal would eliminate cost sharing, while the Sanders proposal would include minimal copayments on prescription drugs for those with incomes above 200% FPL. Under these proposals, today’s Medicaid enrollees would continue to be protected from high out-of-pocket costs. While most Medicaid enrollees do not pay premiums and have limited out of pocket expenses, any who do would likely see these costs eliminated.
Payment and Delivery Systems
Similar to Medicaid, all licensed and certified providers would be eligible to participate in Medicare-for-all programs; however, given the scope of Medicare-for-all programs, it is likely a broader array of providers will participate, expanding the choice of providers for current Medicaid enrollees.State Medicaid programs are required to contract with federally qualified health centers, and most contract with other essential community providers, and consequently, these providers are an important source of care for Medicaid enrollees. While these contracting requirements are not part of current Medicare-for-all proposals, it is expected that health centers and other essential community providers would participate to the same extent they participate in Medicaid programs today.
Medicare-for-all programs would create a national fee schedule for paying providers, eliminating variation in payment rates across states and payers in Medicaid today. While few details are available, Medicare-for-all programs would establish payment rates for hospitals, physicians, and other providers, subject to a global budget process and negotiation under some proposals. In general, states have flexibility in setting Medicaid provider payment rates, leading for variation in payment rates across states. In general, Medicaid rates paid to physicians and some other providers are lower than Medicare rates, while other providers, such as safety net hospitals, may receive higher payments through Medicaid compared to Medicare due to supplemental payments. It is unclear whether payment rates under Medicare-for-all proposals would be based on Medicare rates or set using a different methodology. In addition, federal rules require special Medicaid payment rates for some providers, such as federally qualified health centers and rural health clinics that have contributed to their participation in the program. These providers are likely to see an increase in revenue from improved coverage under Medicare-for-all programs; however, given longstanding relationships Medicaid enrollees have with safety net providers, how they fare under a new program will matter.
The reliance on fee-for-service payments under current Medicare-for-all proposals may move away from current payment and delivery models adopted by state Medicaid programs. Medicare-for-all programs would pay physicians and other providers on a fee-for-service basis, while institutional providers would be paid through a global budget arrangement under some proposals or through fee-for-service under others. Medicaid initially relied on fee-for-service payments, but in recent years, states have experimented with innovative payment designs in their Medicaid programs that seek to improve quality of care, control costs, and address social determinants of health. In addition, through their contracts with managed care organizations as well as managed fee-for-service models, states have emphasized care management for people with complex health needs. Some proposals would allow for these types of payment and delivery models, including private managed care plans, while others would not. While moving to global budgets and a national fee schedule will likely lower costs, some of the benefits of care management strategies, particularly for people with multiple or complex conditions and other vulnerable patients, may be lost.
State Responsibilities
The state role in health care financing would change substantially under a Medicare-for-all program compared to Medicaid. The state share of spending for Medicaid was $222 billion in 2017. Medicare-for-all proposals vary in how much states could save and how much funding states would be required to contribute relative to current spending. For example, under the Jayapal proposal, states could see significant savings relative to current Medicaid spending because Medicaid would be eliminated, and there would be no state financing requirements. However, under other proposals, states would remain responsible through a maintenance of effort (MOE) requirement for all or part of current state spending on Medicaid. The Sanders Medicare-for-all program would require states to maintain their existing Medicaid eligibility standards and spending on institutional long-term care services and would continue to provide states with federal matching payments for these services, locking in variation in eligibility standards and financing across states. Long-term care accounts for more than one in five dollars of Medicaid spending and in 2016, community based long-term care services accounted for 57% of all Medicaid spending on long-term care nationally, although this varies by state. The level of state savings under the Sanders proposal will vary based on current state spending on institutional long-term care services. Under the Harris proposal, states would be required to make MOE payments to the new program equal to the amounts they currently spend on Medicaid and CHIP, increased over time by inflation. Since Medicaid costs have typically increased at higher rates than inflation, states could see some savings over time, but significantly less relative to the Jayapal and Sanders proposals. It is not clear in the Harris and Sanders proposals how state spending from provider fees or taxes (a mechanism used by nearly every state to finance the state share of Medicaid) would be factored in the MOE calculation.
In addition to transferring fiscal responsibility, the proposals would shift the role of designing and implementing much of health policy from states to the federal government. Under current programs, states have significant flexibility to design and administer Medicaid and other related health programs. Medicare-for-all programs would create more uniformity in eligibility and benefits and could result in state savings, but the proposals would also limit states’ ability to leverage Medicaid funding to implement innovative payment and delivery system reforms. Without a comprehensive Medicaid program – and the substantial financing of health care that comes along with it – state policymakers would have a much more diminished role in the health care system generally. Some role for states may remain. For example, the Sanders proposal calls for a regional administrative structure that would include state directors. While the proposals may open other avenues for innovation, the state role in administering all aspects of Medicaid and running insurance departments would diminish under Medicare-for-all programs as these functions shift to federal responsibility.
Looking Ahead
Many details about how a new Medicare-for-all program replacing all or most current public and private health insurance would be implemented and financed are not yet known. As proposals continue to emerge and develop, it is important to focus on the implications related to Medicaid, the program that currently covers 75 million low-income and vulnerable Americans. As with other parts of the health care system, there will be trade-offs. Medicare-for-all proposals would generally eliminate current variation in eligibility, enrollment and renewal processes, benefits, and payment and delivery systems that are part of the current structure of Medicaid, where states now have considerable flexibility to design programs within broad federal rules. However, the transition to a new program, even one with equally comprehensive benefits and cost sharing protections, could be particularly disruptive for current Medicaid enrollees who tend to be sicker with more complex health conditions, and for whom the ability to maintain relationships with current providers will be important. A smooth transition to any new system also will be critical for current Medicaid enrollees who rely on personal care and other services to meet daily self-care needs and maintain independent community living.
More broadly, Medicare-for-all programs would extend coverage for some Medicaid services to more Americans, most notably community-based long-term services and supports. For states, the role in health care financing would change substantially under a Medicare-for-all program. Some proposals would have the federal government assume all or a significant share of the nearly $222 billion in state spending on Medicaid, leading to significant state savings. However, other proposals call for a state maintenance of effort around spending broadly or for specific services. The details about how the MOE would be implemented are not clear. In addition, the proposals would shift responsibility for much of health policy from states to the federal government. As the debate continues and additional details emerge, it will be important to continue to evaluate how Medicare-for-all proposals affect coverage, benefits, out of pocket costs and access to care for the low-income and vulnerable populations currently covered by Medicaid.
Appendix
Appendix Table 1: Key Features of Medicare-for-all Proposals Compared to Medicaid
Feature
Medicare for All(Sanders, S. 1129)
Medicare for All(Jayapal, H.R. 1384)
Medicare for All(Harris)
Medicaid
Eligibility and Enrollment
All U.S. residents, to be defined by the HHS Secretary.
Individuals to be auto-enrolled at birth.
All U.S. residents, to be defined by the HHS Secretary.
Individuals to be auto-enrolled at birth.
All US residents Individuals to be auto-enrolled at birth.
States must cover low-income parents, children, pregnant women, seniors, and people with disabilities. State options to expand coverage to all adults up to 138% FPL and to cover seniors and people with disabilities at higher income levels.
Legal immigrants generally ineligible for coverage for 5 years. Undocumented immigrants only eligible for emergency services.
Individuals must apply and periodically renew eligibility.
Covered Benefits
Medically necessary services, including hospital services, ambulatory patient services, primary and preventive services, mental health and substance abuse services, laboratory and diagnostic services, comprehensive reproductive services, pediatrics, rehabilitative and habilitative services, emergency services are covered.
States are required to continue covering any services covered through a Medicaid state plan amendment that are not included in the Medicare-for-all benefit package, and they may provide additional benefits at state expense
Medically necessary services, including hospital services, ambulatory patient services, primary and preventive services, mental health and substance abuse services, laboratory and diagnostic services, comprehensive reproductive services, pediatrics, rehabilitative and habilitative services, emergency services are covered.
States may provide additional benefits at state expense
Covers all medically necessary services, including emergency room visits, doctor visits, mental health and substance use disorder treatment, and comprehensive reproductive health services
All medically necessary services covered for children. Core set of services covered for adults, with additional services covered at state option.
Vision, dental, hearing
Covered
Covered
Covered
Covered for children; at state option for adults
EPSDT
Covered
Covered
Covered
Covered
Non-emergency transportation
Covered for people with low incomes and/or disabilities
Covered
Not addressed
Covered
Institutional long-term care
Medicaid coverage for these services would continue.
Covered, subject to functional eligibility criteria
Covered
Covered with state option to expand financial eligibility up to 300% SSI and impose asset limit, subject to functional eligibility criteria.
Community-based long-term care
Covered
Covered, subject to functional eligibility criteria
Covered
Covered primarily at state option for adults, with state option to expand financial eligibility up to 300% SSI and impose asset limit, subject to functional eligibility criteria.
Prescription drugs
Secretary to establish a formulary that discourages use of ineffective, dangerous or excessively costly drugs when better alternatives are available and promotes use of generic drugs. Off-formulary drugs are covered subject to rules established by Secretary.
Covered
Covered
All drugs with rebate agreement covered as medically necessary. State option to apply utilization controls such as prior authorization, preferred drug formulary
Premiums and Cost Sharing
None.
Limited authority for Secretary to require cost sharing for prescription drugs for those with income above 200% FPL.
None
No deductibles, and no co-payments for high quality care
State option to charge premiums to those above 150% FPL. Nominal cost-sharing, with certain services and populations exempt from all cost sharing. Cost sharing cannot exceed 5% household income.
Covered Providers
All state-licensed and certified providers who meet applicable provider standards and file a participation agreement.
All state-licensed and certified providers who meet applicable provider standards and file a participation agreement.
All Medicare providers, and possibly others eligible to participate
States establish provider licensing or other criteria. States must contract with federally qualified health centers.
Provider Payment
Secretary to establish a fee schedule in a manner consistent with the processes for determining Medicare payments and a new process for updating fees.
Payments established through global budget process and negotiations
Hospitals/facilities paid quarterly lump sum to cover operating expenses under a global budget; amount of payments determined by annual negotiation
Physicians/clinicians in general paid fee-for-service based on a fee schedule determined by the Secretary, taking into account current Medicare fee schedule, expertise of providers, information from national data/tracking program and subject to annual review
Doctors, nurses, and other providers will be paid appropriate rates
States set provider payment rates and methodology subject to general federal standards.
Delivery System
Fee-for-service; global budget for institutional providers; would allow current payment and delivery system reforms to continue
Fee-for-service; global budget for institutional providers
Private insurers permitted to offer managed care plans, but must meet strict consumer protections.
Will accelerate delivery system reforms and value-based care that rewards meaningful outcomes
Fee-for-service, managed fee-for-service, or managed care at state option.
State Role in Financing
State maintenance of effort (MOE) on spending on institutional long-term care as well as any Medicaid benefit provided through a state plan amendment that is not covered in the Medicare-for-all benefit package.
No state financing requirement
State financing MOE required, equal to current payment amounts indexed for inflation.