KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
The latest report from the KFF COVID-19 Vaccine Monitor examines how the COVID-19 pandemic has impacted the lives of lesbian, gay, bisexual and transgender (LGBT) people and finds that larger shares of LGBT adults report economic losses and mental health struggles than their non-LGBT counterparts.
Based on data gathered on self-identified LGBT and non-LGBT individuals over two months, some of the key differences include:
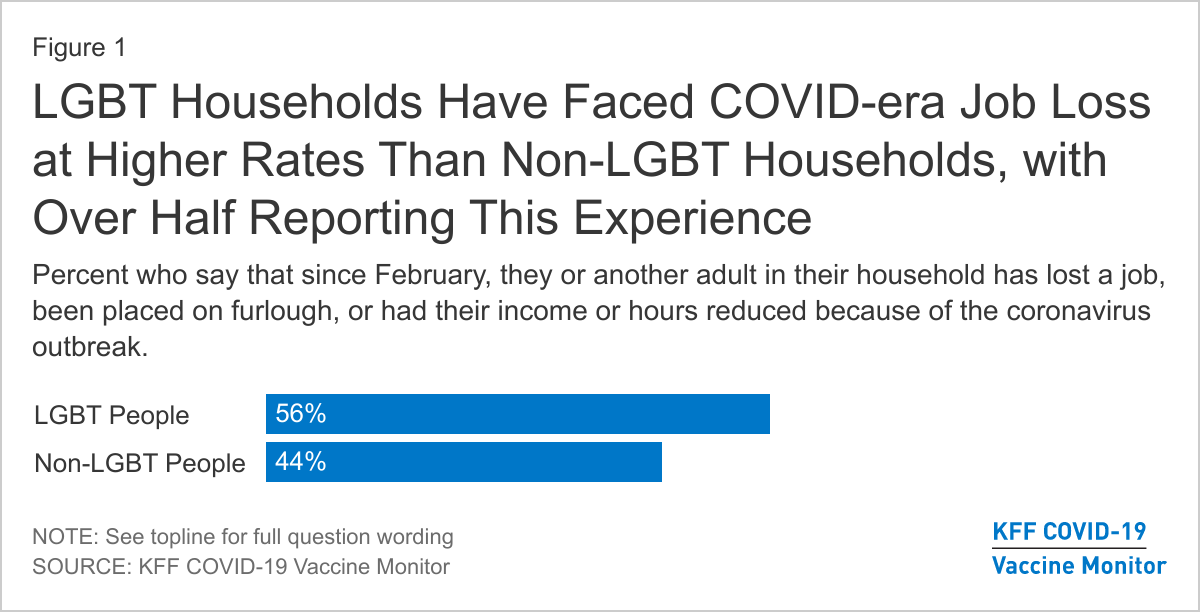
Economic impact. Most LGBT adults say that they or a household member lost a job or income due to the pandemic (56%), which compares to 44% of non-LGBT adults.
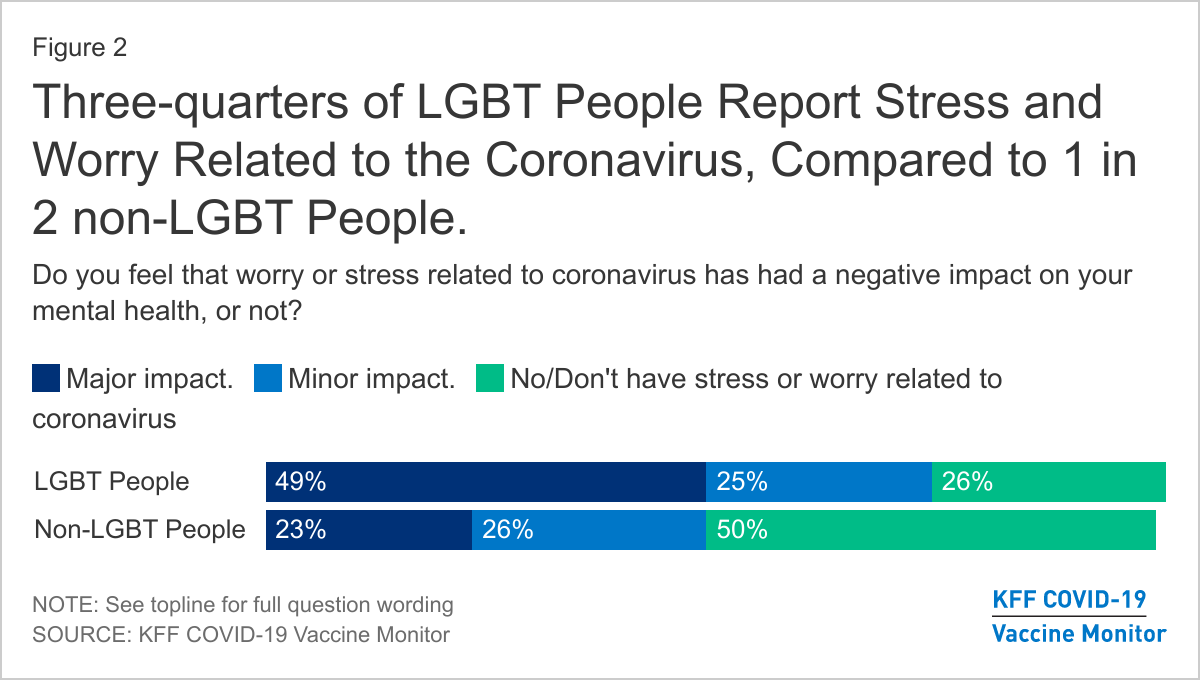
Mental health. Three quarters (74%) of LGBT people say worry and stress from the pandemic has had a negative impact on their mental health, compared to half (49%) of non-LGBT people. LGBT people are also more than twice as likely to say this negative impact has been major (49% to 23%).
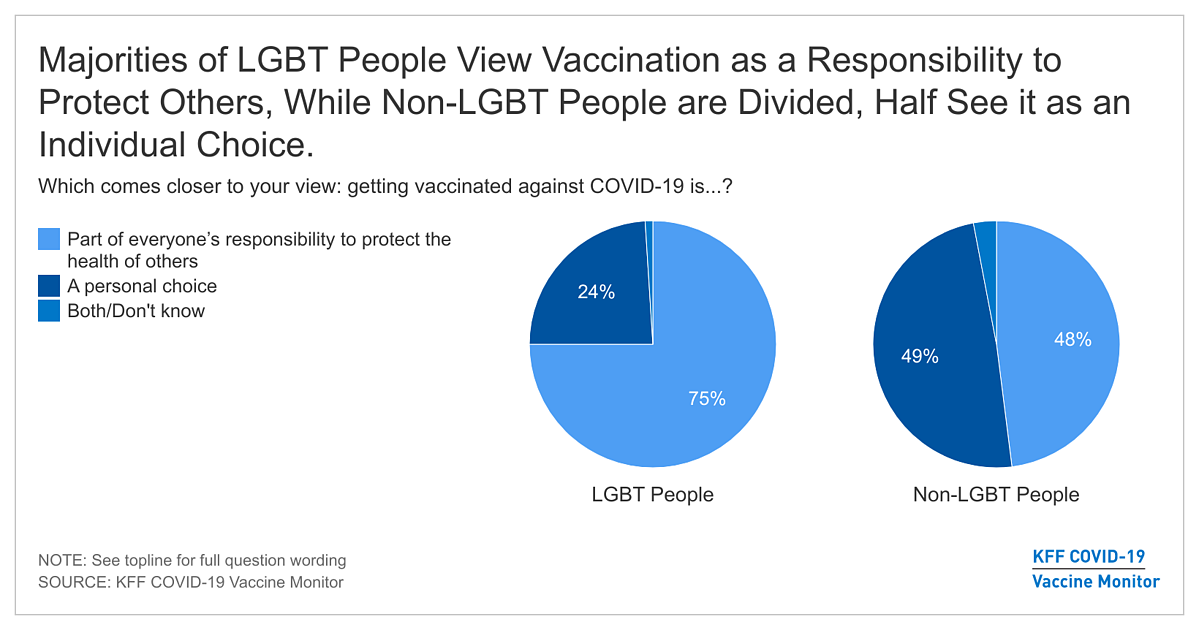
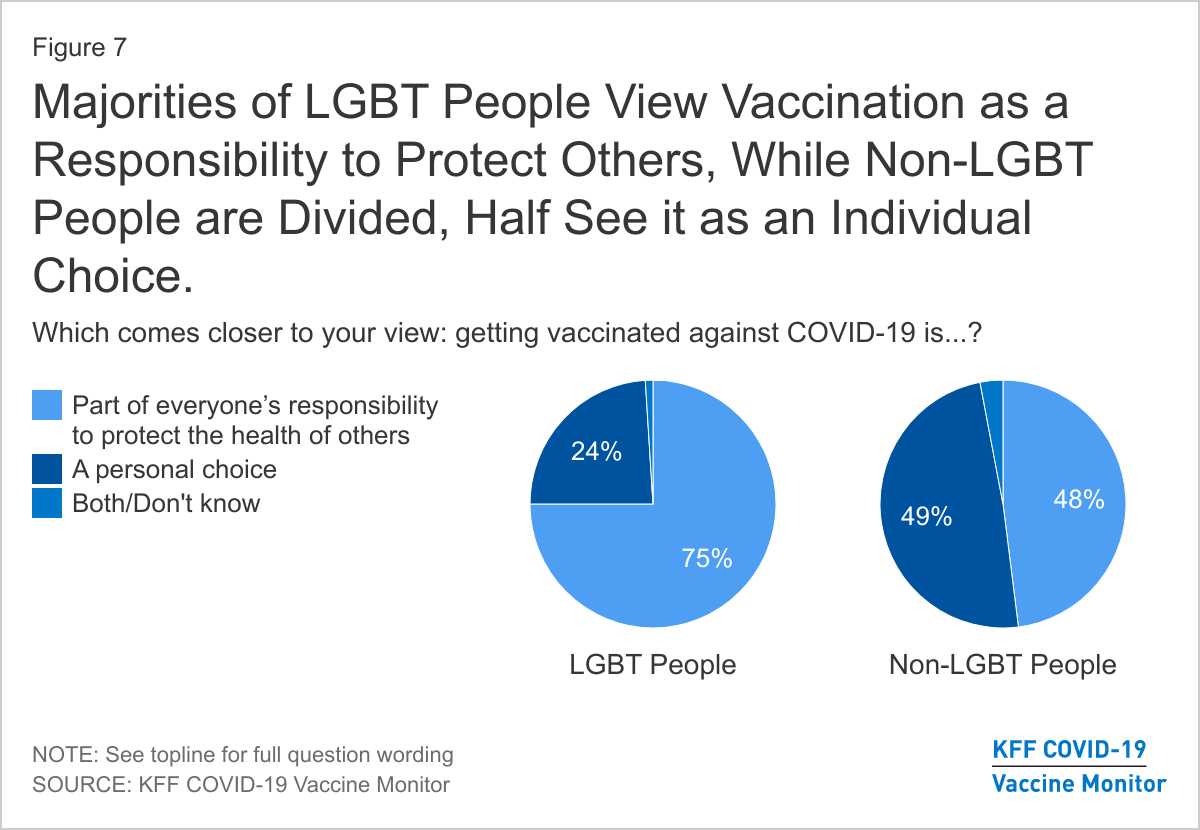
Vaccine intentions. LGBT people are about as eager to get vaccinated as other Americans but more view it as a part of everyone’s responsibility to protect the public health (75%) rather than a personal choice (24%). Non-LGBT individuals are about as equally likely to say it is part of everyone’s responsibility (48%) and a personal choice (49%).
Differences in the experiences of LGBT and non-LGBT individuals likely reflect a number of factors. Other research has found that LGBT individuals are more likely to work in health care, restaurants and other industries highly impacted by the pandemic; have lower average incomes; and may experience discrimination and stigma, including in accessing health care.
This analysis is based on interviews conducted in December and January among a nationally representative random digit dial telephone sample of 3,239 adults, including 174 who identified as lesbian, gay, bisexual, or transgender. The margin of sampling error is plus or minus 9 percentage points for the full LGBT sample and 2 percentage points for the non-LGBT sample. For results based on subgroups, the margin of sampling error may be higher. Detailed methodology can be found in the toplines for the December and January KFF COVID-19 Vaccine Monitor.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and acceptance, information needs, trusted messengers and messages, as well as the public’s experiences with vaccination.
There has been little data on how the coronavirus pandemic has impacted the lives of lesbian, gay, bisexual, and transgender individuals (LGBT) in the U.S. Drawing on previous research indicating that LGBT individuals are at greater risk of both COVID-19 health and economic outcomes, this analysis examines the reported experiences from self-identified LGBT individuals from two months of the KFF COVID-19 Vaccine Monitor and finds that LGBT people have experienced the COVID-19 pandemic differently than non-LGBT people, including being harder hit in some areas:
Economic: A larger share of LGBT adults compared to non-LGBT adults report that they or someone in their household has experienced COVID-era job loss (56% v. 44%).
Mental health: Three-fourths of LGBT people (74%) say worry and stress from the pandemic has had a negative impact on their mental health, compared to 49% of those who are not LGBT, and are more likely to say that negative impact has been major (49% v 23%).
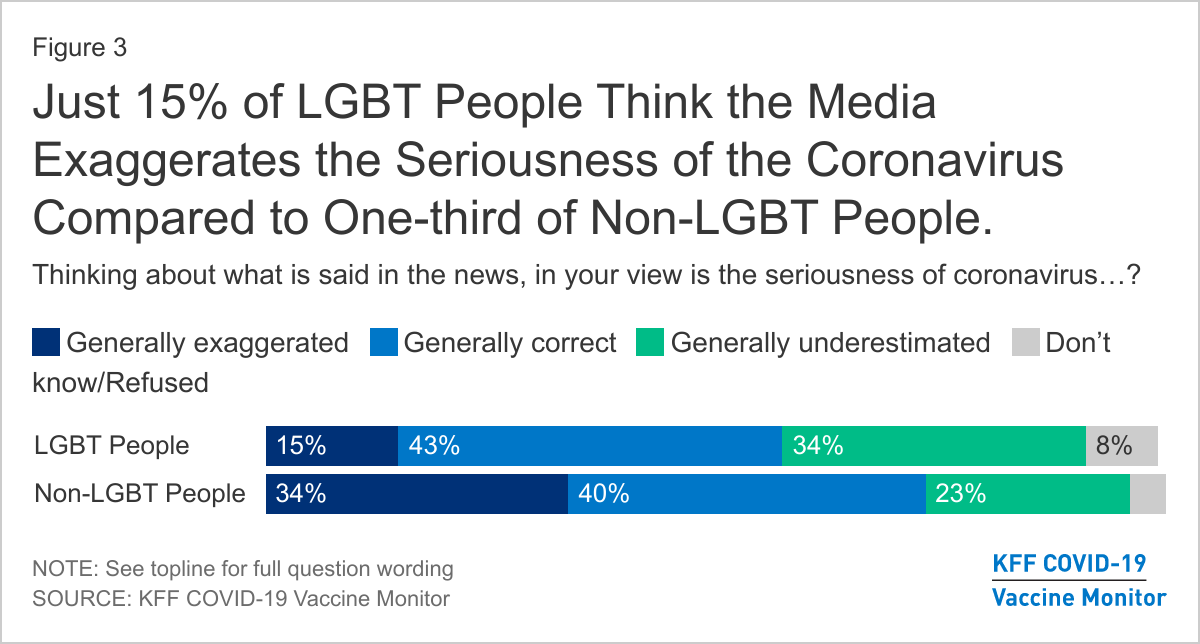
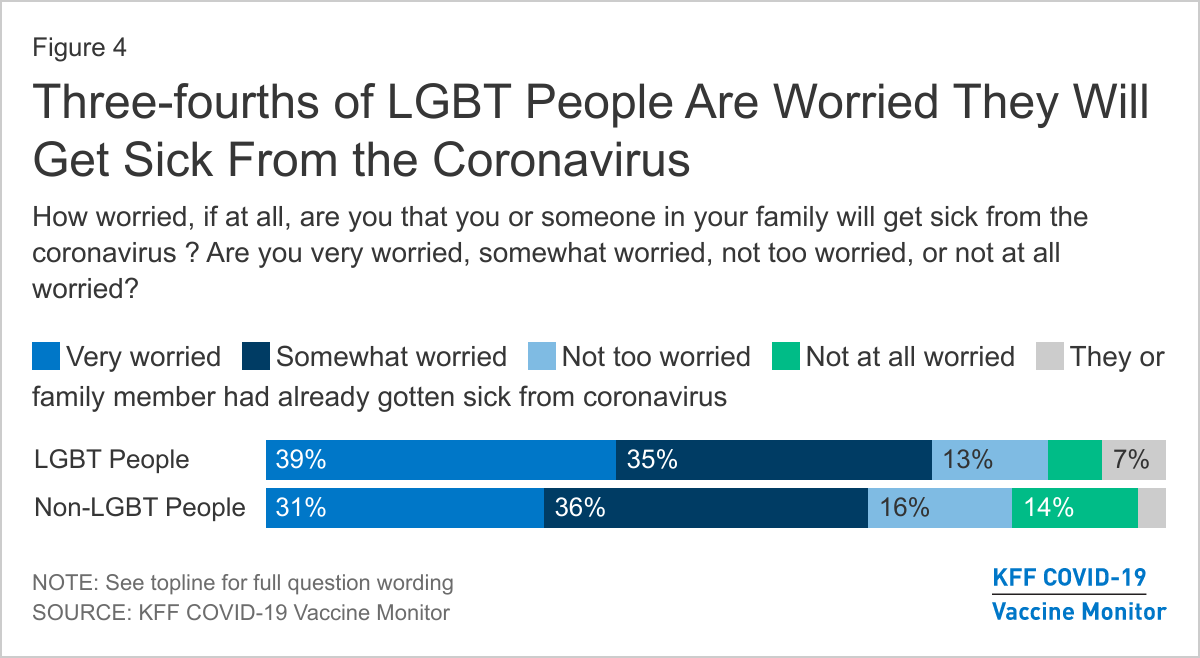
Views: One-third (34%) of LGBT adults say the news has generally underestimated the seriousness of the pandemic (compared to 23% of non-LGBT adults). Three-fourths of LGBT adults (74%) are either “very worried” or “somewhat worried” that they or someone in their family will get sick from the coronavirus, similar to responses from, non-LGBT adults (67%). A large share of LGBT adults report being willing to take CDC recommend steps to avoid acquisition/transmission of the virus.
Vaccine: While LGBT people report wanting to get vaccinated at a similar pace as non-LGBT people, a greater share of LGBT adults see doing so as part of everyone’s responsibility to protect the health of others (75% v. 48%), while greater shares of non-LGBT people see vaccination as a personal choice (49% v 24%).
Why Examine COVID-19 Views and Experiences of LGBT Populations?
Limited early data available on how LGBT people have experienced the COVID-19 pandemic in the United States (U.S.) has suggested that this group may be disproportionately impacted. The reasons are far-reaching and may include: LGBT individuals being at greater risk of worse COVID-19 outcomes due to higher rates of comorbidities; working in highly affected industries such as health care and restaurants/food services; living on average on lower incomes than non-LGBT people; experiencing stigma and discrimination related to sexual orientation/gender identity, including in accessing health care; and, for transgender individuals, being less likely to have health coverage. As the pandemic continues to take a toll nationwide, our analysis from the KFF COVID-19 Vaccine Monitor explores self-identified LGBT people’s COVID-19 experiences and offers comparisons to the non-LGBT population. We find that LGBT adults have experienced the pandemic differently than non-LGBT people in some key domains including with respect to their risk of COVID-19, mental health, employment loss, vaccine attitudes, and willingness to engage in risk-reduction behavior such as social distancing.
The analysis is based on findings from the December and January KFF COVID-19 Vaccine Monitor and building on previous research conducted early on, offers a new look at experiences nearly a year into the pandemic.
COVID-19 Economic and Health Impacts
Echoing previous research conducted earlier on in the pandemic, we find that LGBT adults and their household members report facing COVID-era job loss at higher rates than non-LGBT adults. Since February 2020, 56% of LGBT people report that they or another adult in their household have lost a job, been placed on furlough, or had their income or hours reduced because of the coronavirus outbreak, compared to 44% of non-LGBT people. Separate research has found that LGBT people are more likely to work in industries hard hit by the pandemic, such as restaurants or food services, than their non-LGBT peers.
In addition to personal or familial experience with job loss, the COVID-19 pandemic has been hard hitting for LGBT people in terms of mental health. Prior to the pandemic, LGBT people experienced certain mental health conditions at higher rates than non-LGBT people. In this analysis, we find three-fourths of LGBT people (74%) say worry and stress from the pandemic has had a negative impact on their mental health, compared to 49% of non-LGBT people. In addition, LGBT people more than twice as likely to say this negative impact has been major (49% compared to 23%).
Views Of the COVID-19 Pandemic
LGBT people have a different perspective on some aspects of the pandemic compared to non-LGBT people, including regarding the media’s portrayal and their own level of concern. They also have different views on COVID-19 risk mitigation efforts.
One-third (34%) of LGBT adults say the news has generally underestimated the seriousness of the pandemic (compared to 23% of non-LGBT adults).A much smaller share of LGBT people say the seriousness of coronavirus is exaggerated in the news compared to non-LGBT people (15% vs 34%). Previous KFF COVID-19 Vaccine Monitor analysis finds that these views are largely driven by partisanship, with larger shares Republicans saying the seriousness of the pandemic has been “generally exaggerated” compared to Democrats and independents.
Three-fourths of LGBT adults (74%) say they are either “very worried” or “somewhat worried” that they or someone in their family will get sick from the coronavirus. While this share is not statistically different than those of non-LGBT adults (67%), it demonstrate the high level of concern among LGBT individuals which may be correlated to taking more precautions to protect themselves and family members.
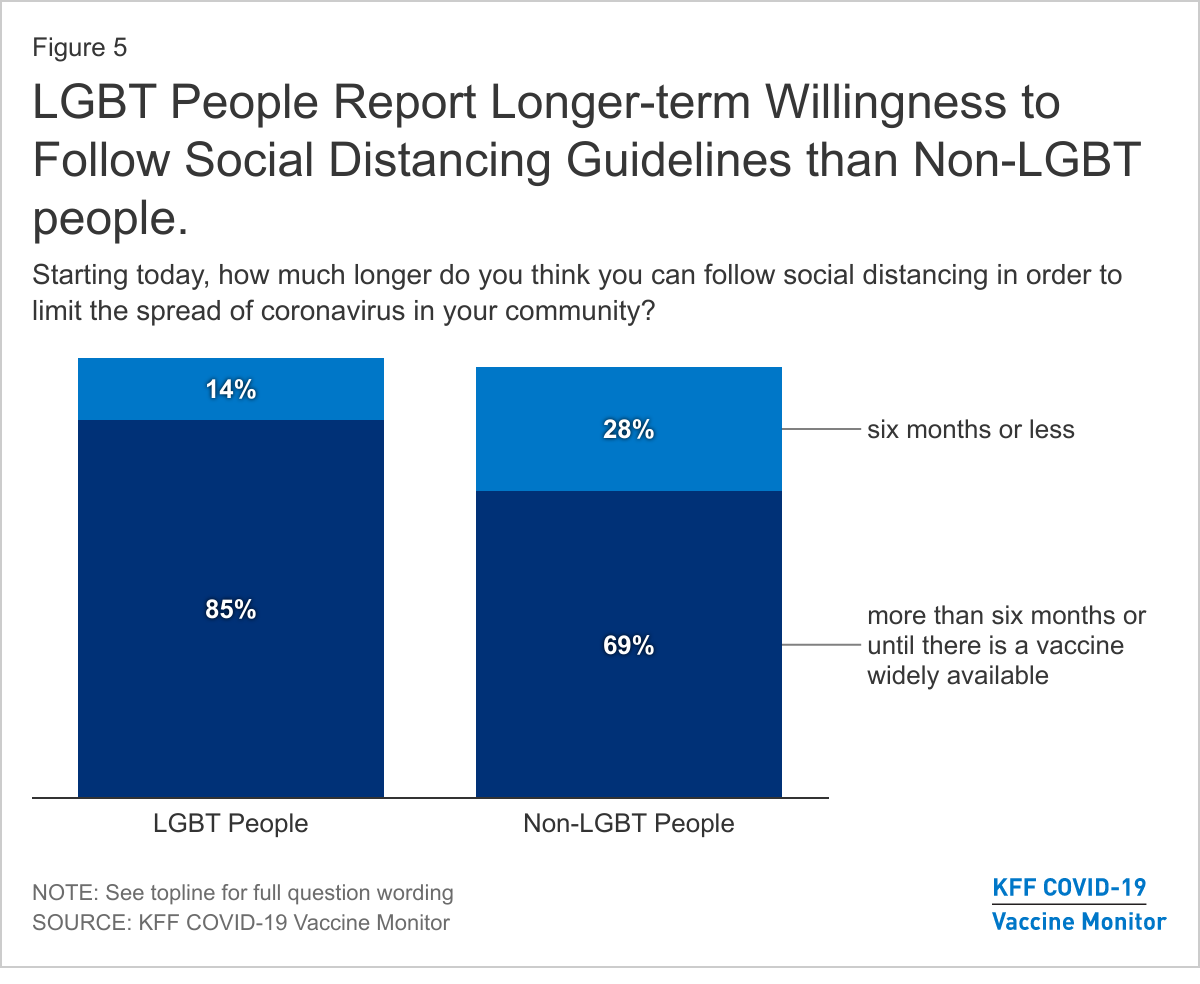
In addition to worry surrounding the virus, large shares of LGBT people report being willing to take CDC recommend steps to avoid acquisition/transmission of COVID-19. Larger shares of LGBT people say they could follow social distancing guidelines for more than six months or until there is a vaccine widely available than non-LGBT people (85% v 69%). Conversely, larger shares of non-LGBT people say they could follow social distancing guidelines for only up to six months compared to LGBT people (28% v. 14%). Additionally and similarly to non-LGBT people, vast majorities of LGBT people also say they wear a mask every time or most of the time when they leave the house (97%) and accurately believe masks limit the spread of coronavirus (90%).
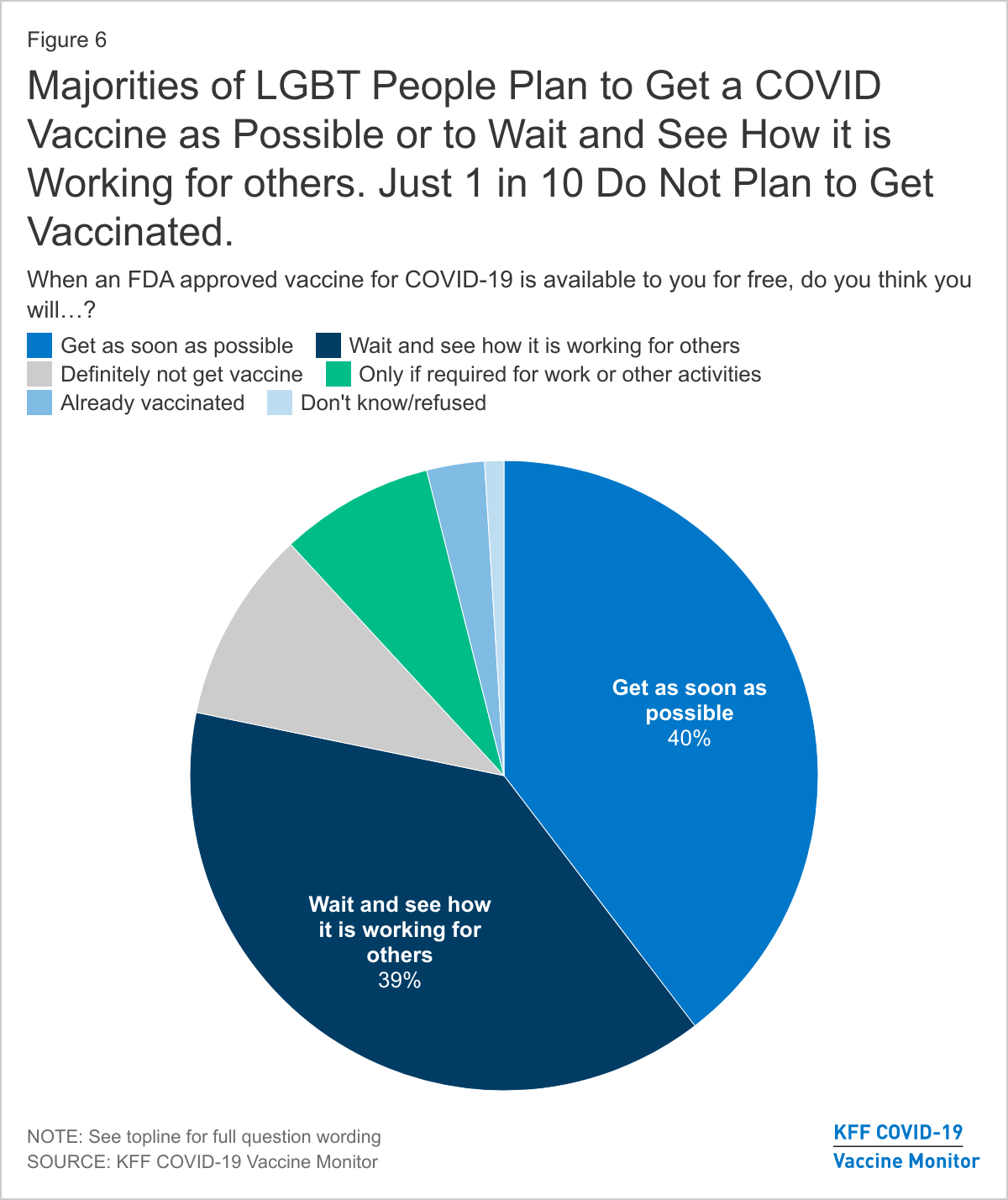
While LGBT people report wanting to get vaccinated at the same rate as non-LGBT people, LGBT people hold different views on whether getting vaccinated is public health imperative or individual choice. LGBT people report wanting to get the vaccine as soon as possible (40%) or take a wait and see approach (39%) at similar rates as non-LGBT people (36% and 36%, respectively). One in ten LGBT people (10%) say they definitely do not plan to get the vaccine, statistically similar to 15% of non-LGBT people.
In Their Own Words.
We asked LGBT people to explain in their own words, “What is the biggest concern you have about getting a COVID-19 vaccine?” Select responses follow:“My biggest concern is actually getting the vaccine on a timely manner and then the second dose. With so much chaos in this country” – Male, white, transgender, California
“Honestly, I just think that the vaccine was "rushed", but I'll probably consider it later on the future for any side affects of any kind.” – Female, black, bisexual, Florida
“Know what really it contains? Is it trustworthy?” – Female, Hispanic, bisexual, Florida
However, a larger share of LGBT people believe getting vaccinated is part of everyone’s responsibility to protect the health of others (75% v. 48%) and a smaller share sees it as a personal choice (24% v. 49%) compared to non-LGBT people.
Implications
Compared to non-LGBT adults, larger shares of LGBT people report experiencing COVID-era job loss, say the pandemic has had a negative impact on their mental health, and report being worried about getting COVID-19. As such it may not be surprising that smaller shares believe the media has overstated the seriousness of the pandemic and with more saying it has been understated. The greater levels of concern and negative experiences with the pandemic in certain domains may also play a role in LGBT people’s willingness to take recommend steps to avoid acquisition/transmission of the virus. Finally, a larger share of LGBT people view COVID-19 vaccination as a collective responsibility than as an individual choice, potentially reflecting the community’s experience with HIV, another infectious disease that requires community level buy-in of public health strategies to curb. While sexual orientation and gender identity may drive some of the differences we find between LGBT and non-LGBT adults, it is also important to note the two populations differ markedly in other key areas. Compared to non-LGBT adults, larger shares of LGBT adults are younger, live on lower incomes, and identify as Democrats, factors that may also contribute to the difference observed. Targeted vaccine outreach to LGBT people could be helpful in reaching a group that has high rates of comorbidities that place them at elevated risk for COVID-19 but has traditionally faced barriers to accessing medical care.
Methods
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and acceptance, information needs, trusted messengers and messages, as well as the public’s experiences with vaccination.
Designed and analyzed by researchers at KFF, this analysis is based on interviews conducted in December and January among a nationally representative random digit dial telephone sample of 174 adults who identified as lesbian, gay, bisexual, or transgender. The margin of sampling error is plus or minus 9 percentage points for the full LGBT sample and 2 percentage points for the non-LGBT sample. For results based on subgroups, the margin of sampling error may be higher. Detailed methodology can be found in the toplines for the December and January KFF COVID-19 Vaccine Monitor. Methods for the qualitative “in their own words” findings can be found at KFF COVID-19 Vaccine Monitor: In their Own Words.
This work was supported in part by the Elton John AIDS Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. KFF paid for all costs associated with the survey.
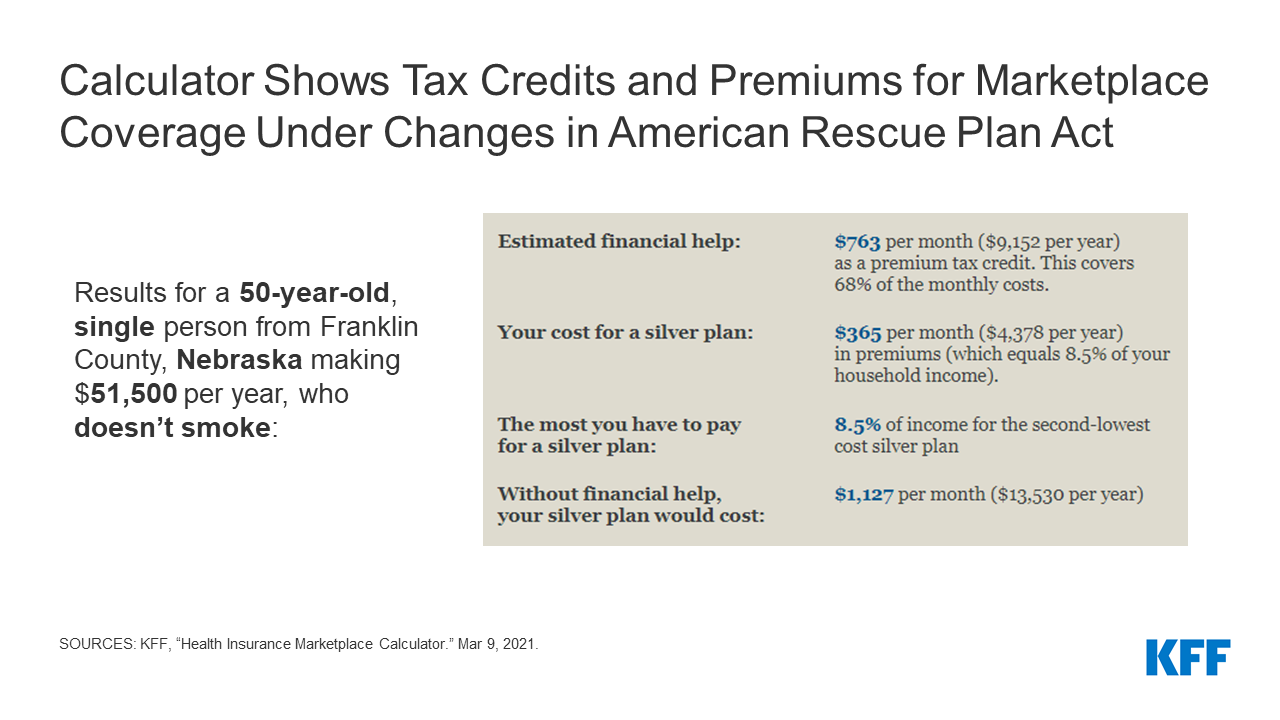
KFF has updated its 2021 Health Insurance Marketplace Calculator to reflect the expanded premium tax credits available to people who purchase their own coverage through their state’s health insurance exchange as passed by Congress in the American Rescue Plan Act and expected to be signed into law soon.
The calculator allows users to enter their age, income, family size, and zip code to assess their eligibility for tax credits and how much they can expect to spend on premiums for coverage purchased through the Affordable Care Act’s marketplaces. It reflects the actual cost of health plans in the region and the changes to how the tax credits are calculated under the legislation’s provisions.
The American Rescue Plan Act increases the premium tax credits available both to people previously eligible and to those at higher incomes who had been ineligible before but face high premiums. The enhanced tax credits will expire after two years and are projected to increase federal deficits by $34.2 billion.
A previous KFF analysis found that the changes would result in premium savings for the vast majority of the nearly 14 million people already insured through the individual market, while millions of uninsured Americans would become eligible for new or bigger tax credits that could make marketplace coverage more affordable.
Those likely to see the biggest drop in what they pay in premiums include those who make just above 400% of the federal poverty rate ($51,040 for an individual), who were not previously eligible for tax credits and would have had to pay the full cost of coverage.
Some examples from the calculator:
A 50-year-old in Franklin County, Nebraska making $51,500 annually is newly eligible for tax credits under the legislation that would lower what they would pay in premiums for a benchmark plan from $1,127 per month to $365 per month.
A 50-year-old in Jefferson County, Oklahoma making $18,000 annually is now eligible for a benchmark plan with significant help to lower deductibles. Previously, they would have had to pay $54 per month for that plan, or enroll in a less generous plan with a large deductible for no premium.
HealthCare.gov, the federal health insurance marketplace serving 36 states, last month began a special enrollment period that runs through May 15. All state-based marketplaces also launched their own special enrollment periods, though the exact dates vary.
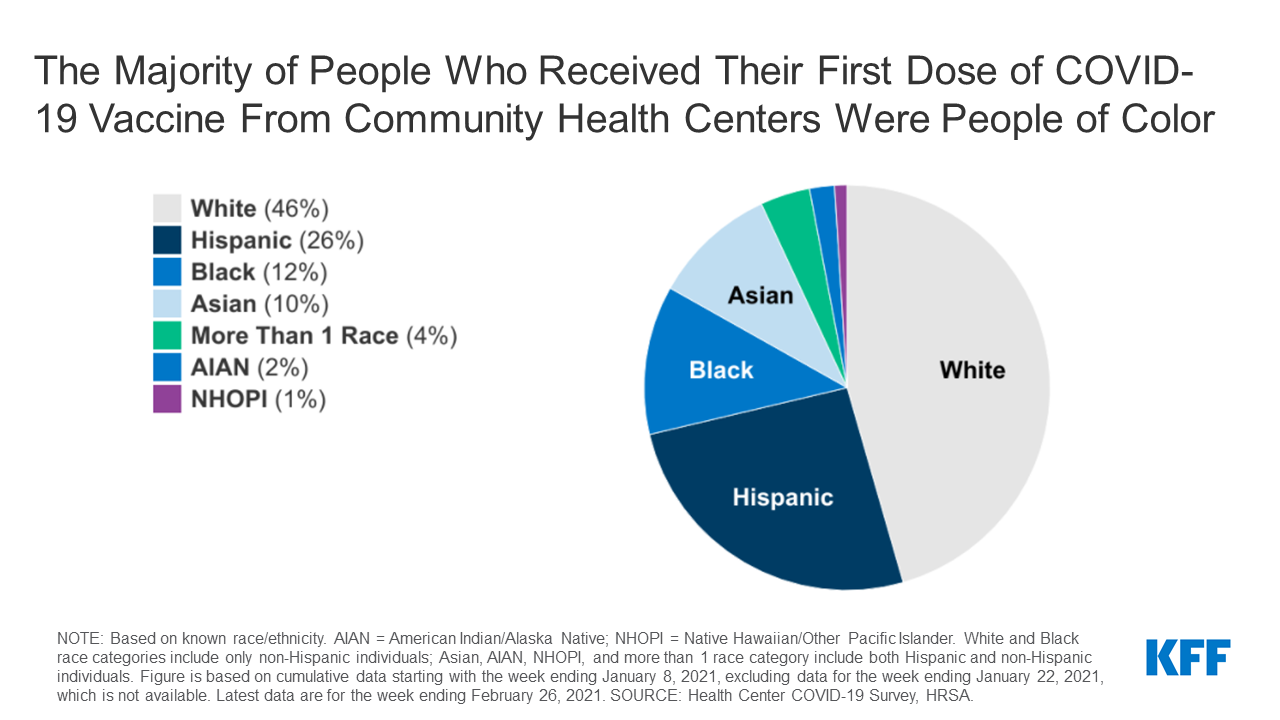
More than half of those who received their first dose of a COVID-19 vaccine through a community health center were people of color, suggesting that health centers appear to be doing a better job of reaching people of color than are overall vaccination efforts, finds a new KFF analysis.
People of color accounted for 54 percent of people who got their first dose of the vaccine through a health center, the analysis finds, including 26 percent who were Hispanic and 12 percent who were Black. The analysis is based on weekly surveys of health centers by the Health Resources and Services Administration starting the week of January 8 through February 26.
In contrast, Centers for Disease Control data show that, as of March 7, just 9 percent of people receiving one or more doses of a COVID-19 vaccine nationally were Hispanic and 7 percent were Black.
As part of an effort to increase vaccination rates among people of color, the Biden administration recently announced an initiative to provide health centers with direct access to vaccine supply. The more than 1,300 health centers in the U.S. are a national network of primary care providers serving nearly 30 million patients annually, many of them low-income and living in underserved communities.
The analysis finds that, among those receiving the 1st dose of the vaccine, health centers appear to be vaccinating people of color at similar or higher rates than their shares of the total population. However, their shares were similar or slightly lower than that of the health center patient population. It also finds that patterns of health center vaccinations by race/ethnicity and population distributions varied widely by state. People of color appear to be receiving a larger share of vaccinations at health centers in recent weeks compared to vaccinations at health centers in January.
As COVID-19 vaccine distribution continues and expands to larger segments of the population, early KFF analysis of state-reported data raise concerns about disparities in vaccinations for Black and Hispanic people. Ensuring equitable access to the vaccines will be important to mitigate the disproportionate impacts of the pandemic for underserved populations, prevent widening disparities going forward, and achieve broad population immunity. The Biden administration’s national COVID-19 response strategy outlines equity as a key priority, including as part of vaccine distribution efforts. Some states have also emphasized equity as a priority in their vaccine distribution plans and, in some cases, have taken responsive action to address disparities in vaccinations revealed by early data.
This brief reviews information available through state websites and publicly available vaccine distribution plans as of February 2021 to provide greater insight into how states are addressing equity through vaccine allocation and distribution strategies, outreach and communications efforts, and data collection and reporting. The review seeks to provide a snapshot and examples of state efforts in these areas. However, this review does not provide a fully exhaustive summary of all state actions, and given the rapidly evolving nature of state vaccination efforts, it may not reflect the latest developments in state approaches. Beyond the state-level strategies highlighted in this review, efforts to advance equitable access to the vaccines are also underway at the city and county level, among health systems and providers, and in the private sector. Moreover, the federal government is implementing a range of approaches to expand vaccine access and uptake — including direct distribution through community health centers — with a particular focus on reaching underserved areas and communities hardest hit by the pandemic.
Vaccine Allocation and Distribution
Where and how people can sign-up for and access vaccines has direct implications for who will receive them. People living in underserved and disproportionately affected areas may face increased challenges accessing vaccines due to more limited resources available to navigate online sign-up systems, lack of transportation, and other access challenges. States are employing a range of strategies to increase the availability and accessibility of vaccines for disproportionately affected areas and people.
Some states are allocating additional vaccine doses to enhance vaccine supplies in underserved and disproportionately affected areas. About half the states indicated in their vaccine distribution plans that they planned to use the Center for Disease Control and Prevention’s (CDC’s) Social Vulnerability Index (SVI) or similar indices to inform their vaccine allocation strategies. States varied in the level of detail they provided in their plans on how they would use these resources to inform their allocation approach, although some states have provided more specific implementation details. For example, in December, Governor Baker of Massachusetts pledged to allocate 20% additional vaccines to communities with high social vulnerability to help address the pandemic’s disproportionate impact on people of color. New Hampshire has indicated that it will reserve 10% of its vaccine supply for allocation to communities that have been hard hit by the pandemic. Connecticut reports providing an additional roughly 10% of the state’s allocation to areas that have high vulnerability based on the SVI. North Carolina also reports allocating additional doses to counties with larger older populations and historically marginalized populations. They indicate that vaccines will be invested into projects and events that promote increased access and partnerships in the community, with a particular focus on achieving equitable access to the vaccine. California will begin reserving 40% of vaccines for residents in the most disadvantaged areas of the state.
Some states are prioritizing vaccine appointments or eligibility for certain groups or areas. In response to early data showing gaps in vaccinations in certain wards of the city, Washington DC changed its vaccine appointment system to prioritize people living in these low-income, underserved areas. Residents in these wards are given the opportunity to register for vaccine appointments 24 hours before they become available to people living in other areas of the city. California provided codes that would provide access to vaccine appointments to community organizations that were intended to be distributed to people living in largely Black and Hispanic communities, although media reports pointed to problems with the initial rollout of this approach. Rhode Island has taken a different approach of prioritizing eligibility for broader groups of residents in certain geographic areas that have an increased risk for COVID-19 hospitalizations and deaths, including Central Falls and certain other areas of the state. Montana and Utah include people of color in their initial vaccine priority groups. With Montana vaccinating American Indians and people of color who may be at elevated risk for COVID-19 complications in Phase 1b, and Utah including people living in Tribal reservation communities and racial/ethnic groups at increased risk in Phase 1c.
Nineteen states have established call centers or provided text options to facilitate access to vaccine appointments for people who may not be able to navigate online sign-up systems. For example, Mississippi and Alabama have set up vaccine appointment scheduling hotlines for residents who cannot or do not want to use the web-based booking programs. In Maryland, the Departments of Health and Aging collaborated to create a telephone-based support line and appointment system designed to assist those without internet access. Connecticut is working with the United Way to provide a call center to schedule appointments that is available 12 hours a day and 7 days a week. However, many states have also encountered initial challenges with this approach, due to overwhelming demand. For example, New Jersey opened up a phone line to schedule vaccine appointments, but it was quickly stretched beyond its initial capacity. Some states are using text-based approaches to provide notifications of when appointments become available. Oklahoma is piloting a text-based notification system that sends second dose appointment updates to individuals who have registered for the vaccine through their scheduling portal.
Some states are deliberately locating vaccine clinics in underserved or disproportionately affected areas. For example, Tennessee is partnering with pharmacies and community health centers to add more than 100 vaccination sites, with a particular focus on rural and underserved areas. Colorado has outlined several strategies to increase the accessibility of vaccines, including partnering with counties to host community clinics, establishing community partnerships to reach communities of color, and coordinating with transportation providers to assist people without vehicles in getting to appointments. The state has also established a goal of having vaccines available through a community-based clinic in “50% of the top 50 census tracts with a high-density of low-income and minority communities.” Alaska is using an Area Deprivation Index to identify areas to provide targeted efforts to ensure equitable access to the vaccine through partnerships with Federally Qualified Health Centers and other community and locally-led organizations. While placing vaccine clinics in underserved or disproportionately affected areas can make vaccines more accessible to people living in areas, location alone will not necessarily ensure access if people face barriers completing sign up processes, and appointments are taken by people living in other areas. As such, prioritizing or reserving appointments for people living in those areas is also important.
Outreach and Communications Strategies
In addition to ensuring individuals can access the vaccine, making sure people receive clear information that explains how and when they can obtain the vaccine and addresses any concerns or questions they have about the vaccine also is important. Moreover, it is key for this information to be provided in culturally and linguistically appropriate ways through trusted messengers.
Some states are collaborating with and supporting community-based organizations and health centers to conduct outreach, communication, and education. For example, Massachusetts launched a targeted outreach initiative through which the Department of Health will invest resources directly into the 20 cities and towns most impacted by COVID-19 to increase awareness of vaccine safety and efficacy by working with local leaders and community- and faith-based groups. The state has also invested $1 million in the Massachusetts league of community health centers to provide grants to health centers to assist in engaging patients and community members in vaccination discussions and increase vaccination rates in the states’ hardest hit communities. The state of Washington has Community Outreach Services Contracts with several community-rooted organizations and groups to assist with COVID-19 vaccine outreach and makes investments in community/ethnic media outlets and community based organizations for community-driven messaging efforts. Colorado announced it is working to schedule more than 175 vaccine equity clinics across the state in partnership with community based organizations, local public health agencies, and Tribes, with community organizations playing a key role in providing outreach to their community members and registering people for appointments.
Many states are launching their own vaccination communications campaigns, often with a focus on reaching people of color and other groups who may face heightened barriers to vaccination. As part of its GoVAX outreach campaign, Maryland launched a mobile public health education unit—or sound truck—to provide information about COVID-19 prevention and vaccination availability in Spanish and English in selected neighborhoods that have been hardest hit by the virus. Volunteers will also distribute informational flyers and face masks at designated stops. In Ohio, health officials are hosting virtual town halls that will be replayed weekly on television to tackle COVID-19 vaccine myths. The town halls are focused on addressing questions and concerns of Black, Hispanic, Asian, Pacific Islander, and rural residents. In addition to these outreach efforts, all states provide information through public-facing websites to address questions and concerns about the vaccine. For example, many prominently feature frequently asked questions (FAQ) sections that address common questions.
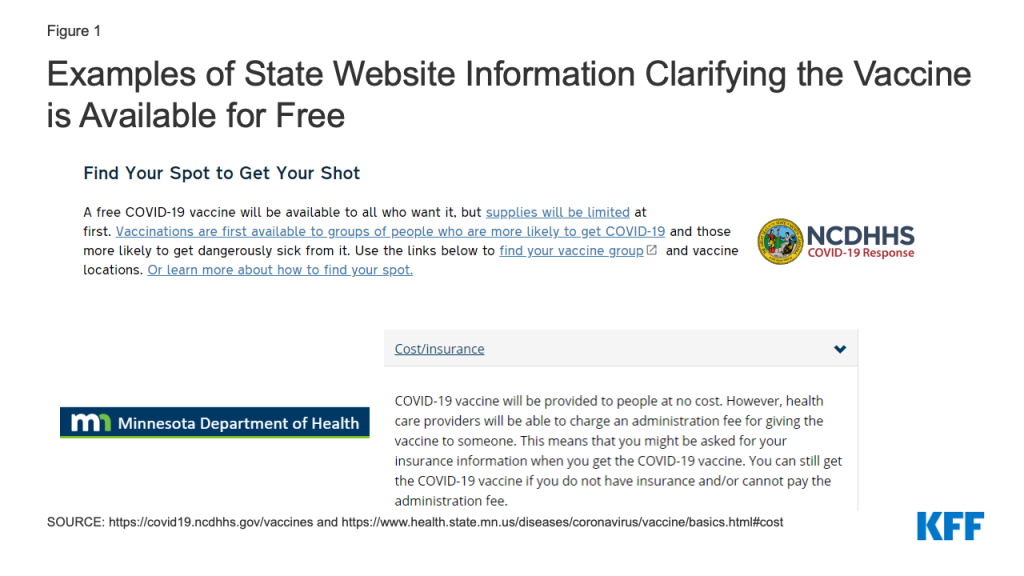
Most state websites include information clarifying that the vaccine is available for free, although the information is not always highlighted prominently. Some states highlight this information up front. For example, North Carolina clarifies that the vaccine is available for free to all who want it on its landing page for vaccine information (Figure 1). Similarly, Minnesota includes this information in the FAQs listed on its “vaccine basics” page. Clarifying that people can receive the vaccine at no cost regardless of insurance status is important for facilitating equity, as recent survey data show that Black and Hispanic adults have heightened concerns about potentially having to pay out-of-pocket costs. Possibly, even more important is whether vaccine providers clarify that the vaccine is available at no cost and ensure people are able to sign up for appointments without providing insurance information.
Figure 1: Examples of State Website Information Clarifying the Vaccine is Available for Free
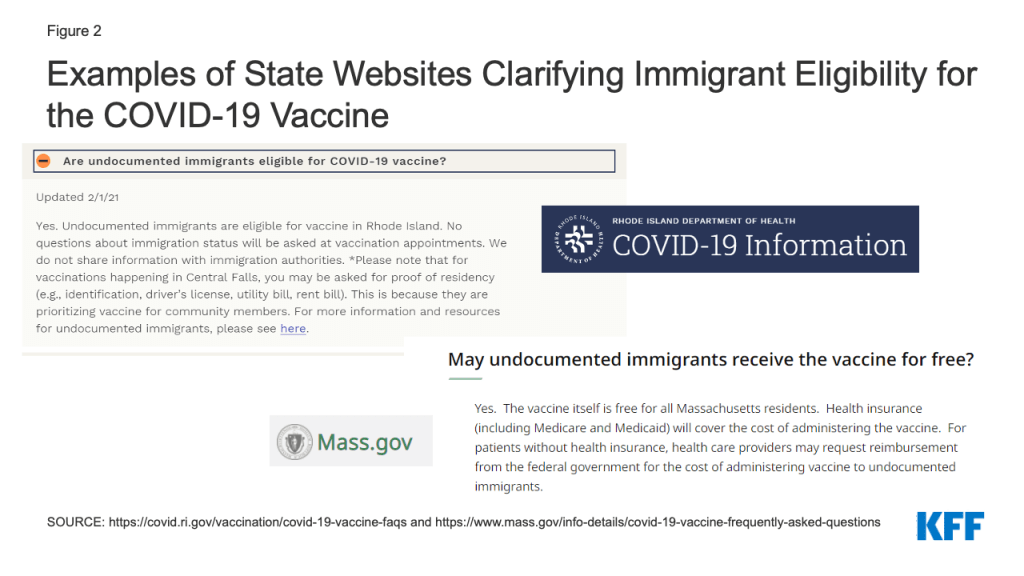
Fewer state websites clarify that individuals are eligible for that vaccination regardless of immigration status and/or that obtaining the vaccine will not negatively affect immigration status. Clarifying this information can help address fears and confusion that could present barriers to vaccination among immigrants. For example, Rhode Island clarifies that undocumented immigrants are eligible for vaccination and that information will not be shared with immigration authorities (Figure 2). In Massachusetts, they emphasize that the vaccine is free for all Massachusetts residents, and that health care providers may request reimbursement from the federal government to cover the administrative costs of providing vaccines to undocumented immigrants.
Figure 2: Examples of State Websites Clarifying Immigrant Eligibility for the COVID-19 Vaccine
All websites provide options to access information in different languages, but they vary in how they provide this access. Some states solely utilize google translate or similar translation software; others provide translated materials through downloadable resources, in some cases linking to translated materials provided by CDC. However, recent reporting finds that many vaccine registration and information websites at the federal, state, and local levels violate disability rights laws, hindering the ability of blind people to sign up.
Data Collection and Reporting
Collecting and analyzing COVID-19 vaccination data by race/ ethnicity is integral to gaining insight into who is and is not receiving vaccines and can be used to direct resources and efforts to address disparities as they are identified.
As of March 1, 2021, 41 states are publicly reporting COVID-19 vaccination data by race and/or ethnicity. While most states are reporting data, the quality, completeness, and timeliness of the data vary widely across states, which affects its usefulness. For example, as of March 1, 2021, in Minnesota and Washington D.C., race/ethnicity information was missing for over 40% of vaccinations, while North Carolina reported less than 1% as missing race/ethnicity information. States also vary in the extent to which they disaggregate data to allow an understanding of the experiences of specific groups. For example, Florida groups people who report their race as Asian, Native Hawaiian or Pacific Islander, or other into a single “Other race category.” In contrast, other states, like Maine, disaggregate data separately for racial and ethnic groups. Very few states report vaccination data by race/ethnicity and other demographic factors like age or gender. However, South Carolina and Washington provide data in these more detailed ways, allowing for a more nuanced understanding of who is being vaccinated that can inform efforts to address gaps.
Several states have taken actions designed to increase the completeness of race/ethnicity data. For example, North Carolina and Texas are requiring vaccine providers to collect race/ ethnicity data.Texas is updating its immunization registry system so that race and ethnicity must be entered to complete the data entry process. Michigan added a hand-entry field into their registry system to collect race and ethnicity data since the system had not previously collected this information. In addition, Virginia added language to its website to encourage individuals to report demographic data and clarifying how the data will be used (Figure 3).
Figure 3: Example of State Website Information on Importance of Reporting Demographic Data and How Data Will Be Used
Conclusion
In sum, early data pointing to racial disparities in COVID-19 vaccinations underscore the importance of intentional efforts focused on ensuring equity as the vaccine rollout continues. As highlighted in this brief, a number of states included a focus on equity in their vaccine distribution plans and are taking responsive action to try to address emerging disparities through vaccine allocation and distribution approaches, outreach and communications strategies, and data collection and reporting. Continued monitoring of data to understand who is and is not receiving the vaccine will be important for gauging the effectiveness of these approaches; and will help guide ongoing efforts to prevent and reduce disparities as distribution continues.
As noted, beyond the state-level strategies highlighted in this review, efforts to advance equitable access to the vaccines are also underway at the local level, among health systems and providers, and in the private sector. Moreover, at the federal level, the Biden administration has outlined equity as a key goal of its national COVID-19 response strategy, including as a part of vaccine distribution efforts. To that end, it has established a COVID-19 Health Equity task force; indicated plans to work with states to incorporate equity into their vaccine distribution processes; is taking steps to expand vaccine availability in underserved areas through federally-supported vaccination centers and allocations of vaccine doses directly to community health centers and retail pharmacies; is launching and vaccination communication plan; and is focused on expanding data collection and reporting. The American Rescue Plan Act includes additional funding that will further enhance these approaches.
High rates of preventable maternal mortality and morbidity and wide racial and ethnic disparities have caught the attention of clinicians, public health practitioners, advocates, and policymakers.1 In the closing days of the Trump Administration, HHS released an action plan to improve maternal health, and President-elect Biden has cited this topic as a key health care issue. Vice President-elect Harris has been an advocate in the Senate for improving maternal health, particularly stemming the disproportionately high rates of maternal mortality and morbidity among Black women, and may continue to champion this work at the Executive Branch. During the 2019-2020 Congressional session, more than a dozen bills across political lines related to maternal health outcomes, care, and coverage were introduced, and many could be re-introduced when the new Congress is seated. Several federal and state efforts aim to address the postpartum period, the time shortly after the birth of an infant, an important but often neglected element of maternity care. Birthing parents may be dealing with a host of medical conditions, such as complications from childbirth, pain, depression or anxiety, all while caring for a newborn. It can be a medically vulnerable period and many cases of maternal mortality occur in the postpartum period.
While Medicaid pays for more than four in ten births and must cover pregnant women through 60 days postpartum, after that period states can and have made very different choices regarding whether eligibility for Medicaid coverage is continued. In states that have not expanded Medicaid under the Affordable Care Act (ACA), many women are left without a pathway to coverage and become uninsured just two months after giving birth. Recently, there has been growing interest from federal and state policymakers, clinicians, and health advocates in expanding Medicaid’s postpartum coverage from 60 days to one year. This brief discusses Medicaid’s eligibility for pregnancy and postpartum care, describes gaps in coverage particularly for low-income women who live in states that have not expanded Medicaid under the ACA, and highlights several state and federal efforts to extend postpartum coverage for a longer period of time.
What is Medicaid’s role for pregnancy and postpartum care?
Medicaid has long prioritized coverage of pregnant women and now finances more than four in ten births in the United States.2 Federal law requires that all states extend eligibility for pregnant women with incomes up to 138% of the federal poverty level (FPL); however, most states (48 and DC) go beyond this minimum threshold, ranging from 138% to 380% FPL. Pregnancy-related coverage must last through 60 days postpartum and the infant is eligible for Medicaid for the first year after birth. For women who qualify for Medicaid on the basis of pregnancy, all states provide pregnant women with a wide range of Medicaid benefits, including prenatal care, childbirth and delivery services. States have discretion to determine specific maternity care benefits under Medicaid. For example, many states cover substance use treatment and home visiting services but fewer cover other services such as doula care and home births.
For pregnant women who are eligible for Medicaid under the ACA’s Medicaid expansion pathway, states must cover all preventive services recommended by the United States Preventive Services Task Force (USPSTF) including many pregnancy-related services, such as prenatal screening tests and folic acid supplements as well as services in the postpartum period, such as lactation consultation and breastfeeding supplies. Importantly, all states cover family planning services before and after pregnancy. Pregnancy-related services for those enrolled under any Medicaid pathway are exempt from cost-sharing. For low-income people in particular, the lower cost sharing and absence of deductibles under Medicaid can be a major advantage over private insurance.
Where are the gaps in coverage during the postpartum period?
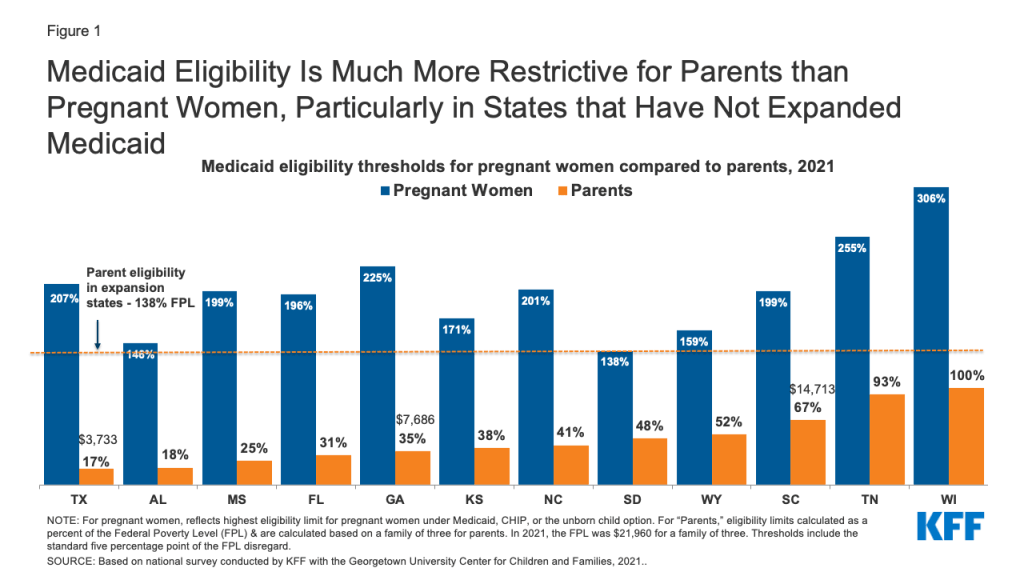
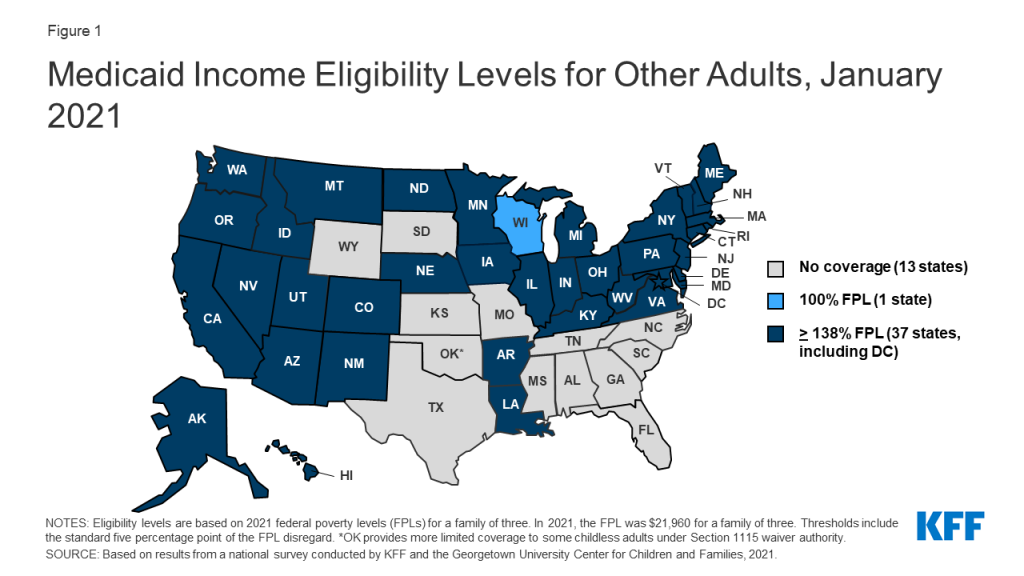
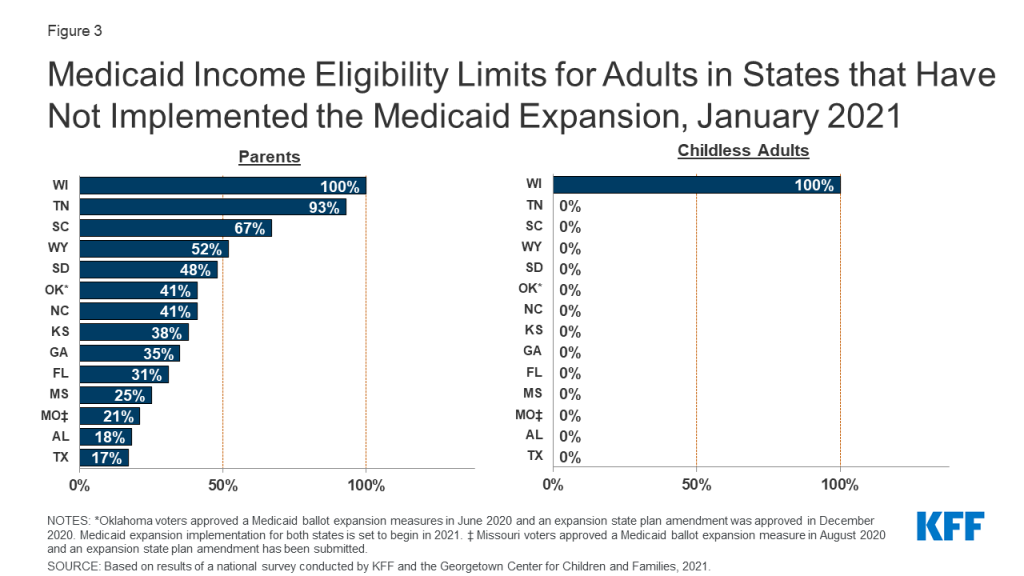
Following the 60 days postpartum period, mothers with incomes up to 138% FPL in the states that have expanded Medicaid under the ACA (38 states and DC) have a continued pathway to coverage. Those with incomes above 138% FPL may qualify for subsidized coverage through the ACA Marketplace. However, in the 12 states that have not adopted the ACA’s Medicaid expansion, postpartum women could qualify for Medicaid as parents to stay on the program, but Medicaid income eligibility levels for parents are much lower than for pregnant people in all of the states (Figure 1). As a result, many women in non-expansion states become uninsured after pregnancy-related coverage ends 60 days postpartum because, even though they are poor, their income is still too high to qualify for Medicaid as parents and too low to qualify for Marketplace subsidies. For example, in Texas, a married mother with a newborn loses Medicaid coverage two months after giving birth if she and her partner have an annual income above $3,733 (17% FPL).
Figure 1: Medicaid Eligibility Is Much More Restrictive for Parents than Pregnant Women, Particularly in States that Have Not Expanded Medicaid
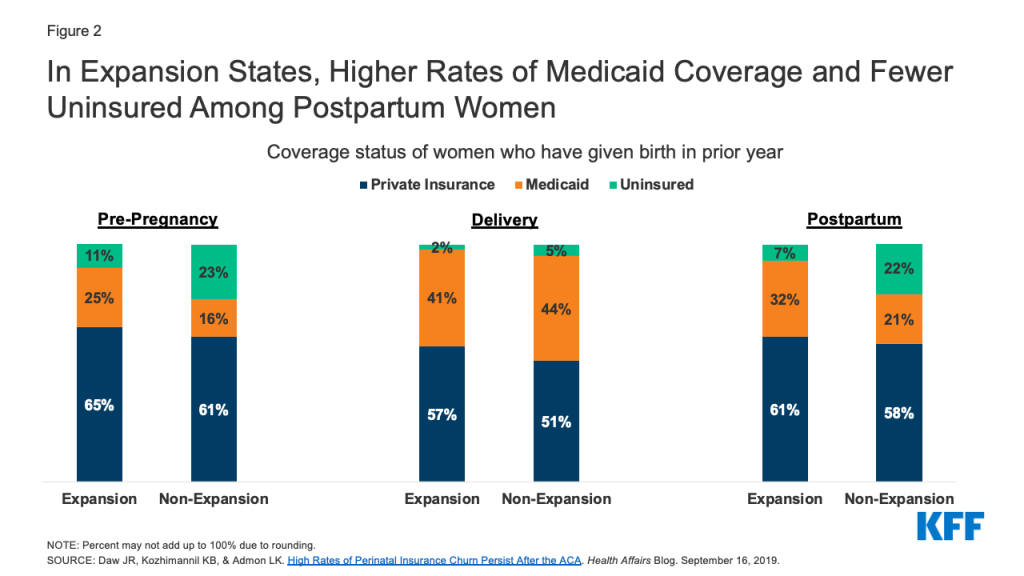
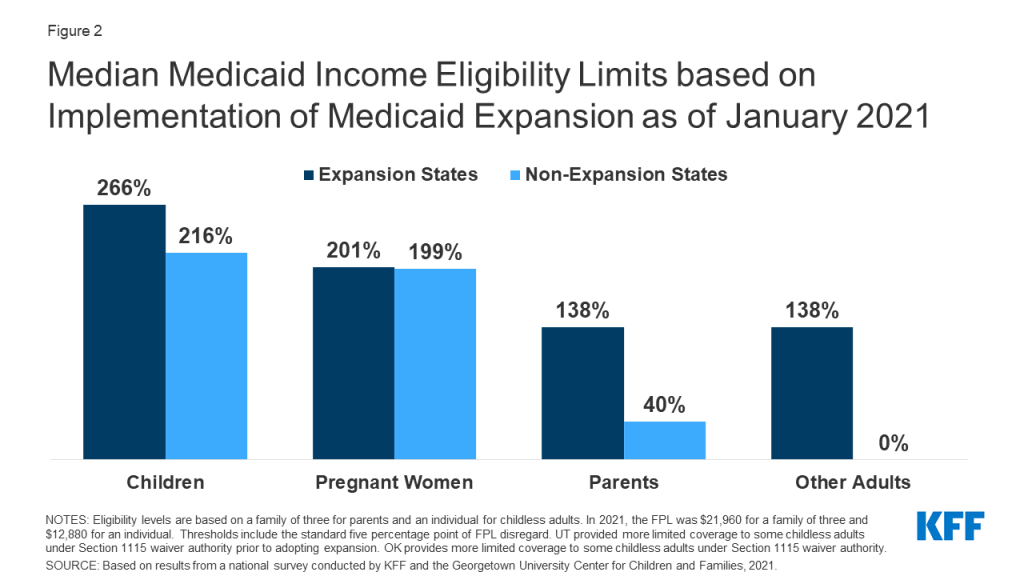
Research shows that Medicaid coverage is higher and uninsured rates are lower among women before and after pregnancy in expansion states compared to non-expansion states (Figure 2). As shown in Figure 2, coverage patterns are similar during pregnancy between expansion and non-expansion states. After pregnancy, however, Medicaid coverage declines and the uninsured rate climbs, with the effect more pronounced in non-expansion states.3
Figure 2: In Expansion States, Higher Rates of Medicaid Coverage and Fewer Uninsured Among Postpartum Women
Furthermore, many women in non-expansion states who do not qualify for Medicaid after 60 days postpartum may also not qualify for subsidies to assist with the purchase of private insurance in state Marketplaces because they have incomes between the income limit for parents and 100% FPL, leaving them in the “coverage gap” with few options for affordable coverage.
How has the coronavirus affected postpartum coverage?
The Families First Coronavirus Recovery Act (FFCRA) includes an enhanced federal match (FMAP) to states, contingent on meeting maintenance of eligibility (MOE) requirements that include ensuring continuous coverage for enrollees until the end of the month in which the public health emergency (PHE) is in place. Under earlier guidance issued by the Centers for Medicare and Medicaid Services (CMS), someone qualifying on the basis of pregnancy would remain enrolled in that group, even after the 60 days postpartum period. Under a new interim final rule effective on November 2, states can move a pregnant woman from the pregnancy group to another eligibility pathway if eligible for another full benefit group, such as ACA expansion, and the benefit package for the new group is the same or more generous than the pregnant woman benefit package, move to new group. However, if the pregnancy benefit package is more generous than another pathway or the person is ineligible for any other full benefit group, they would remain enrolled in pregnancy group.
In addition to changing eligibility for coverage, the coronavirus pandemic has changed the way pregnancy and postpartum care is provided. New mothers may be more isolated from postpartum support, such as family members or doulas and women may be accessing services such as lactation consultations or postpartum checkups via telehealth. Continuity of coverage may be even more valuable given the other disruptions in care that new parents may be facing during the pandemic.4
Why is coverage for postpartum care important?
Postpartum care encompasses a range of important health needs, including recovery from childbirth, follow up on pregnancy complications, management of chronic health conditions, access to family planning, and addressing mental health conditions. While postpartum care has traditionally centered around one clinical visit six to eight weeks after delivery, there has been a paradigm shift to emphasize that postpartum care is an ongoing process that typically requires multiple visits and follow up care that may last a year or even longer. This is particularly important for those who experience pregnancy complications or have chronic conditions, such as hypertension or diabetes.
Mental health is a major concern during and after pregnancy. Suicidality among pregnant and postpartum people has risen over the past decade. At least one in ten women experience perinatal depression, and some studies suggest higher rates but poorer access to treatments among some communities of color and low-income women. ACOG recommends screening during the postpartum visit and initiation of treatment or referral to a mental health provider when a woman is identified with depression. This kind of care may be provided over a long duration, often lasting beyond 60 days.
Addressing pregnancy-related deaths (typically defined as death within one year of pregnancy)5 , particularly the substantially higher rates among Black and American Indian and Alaska Native (AIAN) women, is an urgent health challenge.6 At least one-third of maternal deaths occur in the postpartum period. Identifying the causes of maternal mortality and morbidity is complex, and coverage is only one factor, but research strongly indicates that access to health care throughout a woman’s reproductive years, is essential for prevention, early detection, and treatment of some of the conditions that place women at higher risk for pregnancy-related complications, including cardiovascular disease, diabetes, and chronic hypertension. Coverage disruptions during the perinatal period disproportionately affect Black, AIAN, and Hispanic women. Furthermore, a wide array of conditions that may present or persist through the postpartum period, including mental health challenges, intimate partner violence, and substance use, all play a role in maternal mortality and broader maternal health outcomes.
What can states do to extend postpartum coverage under Medicaid?
Assuring that low-income women have continuous coverage after pregnancy would support improvements in infant and maternal outcomes. States have several main pathways for broadening coverage in the postpartum period to Medicaid beneficiaries. These would all involve some increase in state spending, but with substantial federal matching funds available as well. Potential approaches, in decreasing order of scope and reach, include:
Expand full scope Medicaid–Expanding Medicaid eligibility under ACA would provide the most comprehensive approach to broadening postpartum coverage, and the federal government would pay 90% of the costs for the expansion population. Postpartum women with incomes up to 138% FPL would be able to retain Medicaid past 60 days postpartum, providing greater continuity of coverage and care. Furthermore, other individuals with incomes up to 138% FPL would also qualify for Medicaid coverage, expanding Medicaid benefits to mothers and fathers as well as people without children, including those who intend to become pregnant and need preconception care. Research demonstrates the impact of Medicaid expansion on pregnancy-related coverage and care to date. One study found that Medicaid expansion was associated with lower maternal mortality rates compared to non-expansion states.7 Full Medicaid expansion would also narrow the coverage gap in non-expansion states for poor parents who do not qualify for either Medicaid or subsidies in the Marketplace. Research from the Urban Institute suggests that at least a quarter of uninsured new mothers would likely newly qualify for Medicaid postpartum if their state expanded Medicaid.
Raise parental income eligibility levels under Medicaid– Short of full expansion, non-expansion states have another tool at their disposal to narrow the postpartum coverage cliff– raising income eligibility thresholds for parents, which is one of the pre-ACA eligibility categories. States set income eligibility levels for Medicaid. Raising the eligibility thresholds for parents could extend Medicaid eligibility to more low-income mothers and fathers and partially close the coverage gap in non-expansion states. Currently, Wisconsin sets eligibility thresholds for parents at 100% FPL and Tennessee is not far behind at 93% FPL (Table 1). The rest of the non-expansion states are much more restrictive however and currently have large gaps in coverage for parents. States would receive their regular federal match rate for any new enrollees who qualify as a result of higher parental eligibility levels.
Extend pregnancy-related Medicaid coverage beyond 60 days postpartum– A number of states, both expansion and non-expansion, are taking action to try to extend the period of Medicaid postpartum eligibility, but the initiatives vary in scope.8,9 Some states are applying for Section 1115 waivers from CMS to extend Medicaid beyond 60 days postpartum. Georgia, a non-expansion state, enacted legislation to extend postpartum coverage from 60 days to six months for those who had a Medicaid funded birth, and the state has submitted a waiver application to CMS. Even in Medicaid expansion states, postpartum women may lose Medicaid coverage postpartum, particularly if their incomes are above 138% FPL, and need to transition to Marketplace insurance. Even with a premium subsidy, some may find the out of pocket costs unaffordable and they may have to change providers with a coverage transition. Some expansion states, such as Illinois and New Jersey, are also seeking waivers from CMS to extend Medicaid’s postpartum period so that low-income postpartum women at income levels above 138% FPL keep their Medicaid coverage beyond two months postpartum.
Expand coverage for specific postpartum services or specific populations- There has been some interest in broadening Medicaid postpartum coverage for specific health needs. The HHS maternal health action plan recommends supporting policies that allow states to maintain coverage for pregnant and postpartum people with substance use disorders. The postpartum period can be a particularly susceptible time for substance use relapse, with loss of coverage and access to care considered a potential trigger for relapse. Missouri and Indiana have submitted waiver applications to CMS that propose Medicaid postpartum extension to 12 months for postpartum women in need of services for substance use. Missouri’s waiver would allow postpartum women to continue to receive substance use and mental health services for a year, while Indiana’s proposal would extend full Medicaid coverage for those with opioid use disorder. Additionally, both states participate in CMS’ Maternal Opioid Misuse (MOM) model, a funding initiative that the agency offers for states to develop and improve programs to care for pregnant and postpartum people with opioid use disorder..Some states have used state dollars to extend postpartum coverage to certain populations. California enacted legislation and is using state funds to extend Medicaid coverage to a year for postpartum individuals diagnosed with a maternal mental health condition. Since September 2020, the state of Texas has been using state funds to provide a limited package of postpartum services for one year to those enrolled in the state’s Healthy Texas Women program, which is for uninsured reproductive age women. The state has submitted a Section 1115 waiver application to CMS to draw down federal funds for this program.
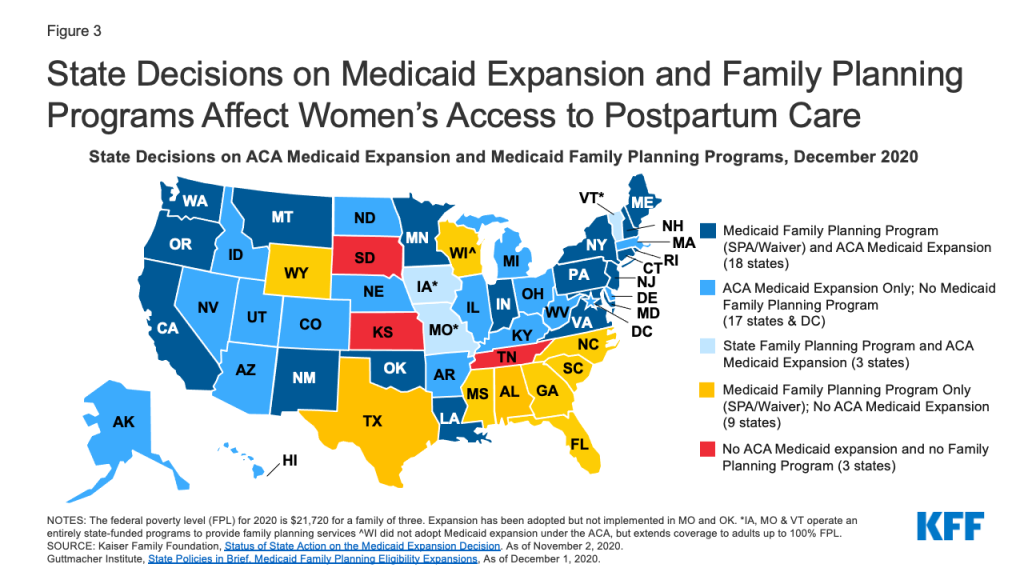
Provide postpartum coverage for family planning services – Outside of lengthening the postpartum period under Medicaid, half of states provide Medicaid coverage for just family planning services to individuals who do not qualify for full Medicaid coverage. While these programs do not provide coverage that is as comprehensive as full scope Medicaid, they provide access to postpartum and intrapartum contraceptive services, which is important for pregnancy planning and healthy birth spacing. Most of the non-expansion states have a Medicaid or state-funded family planning program (Figure 3). However, in three states – Tennessee, Kansas, and South Dakota – postpartum individuals who were covered by Medicaid for pregnancy likely become uninsured after 60 days because the state has not expanded Medicaid under the ACA, and may not even have access to contraceptive services after pregnancy because the state does not have a Medicaid-funded family planning program.
Figure 3: State Decisions on Medicaid Expansion and Family Planning Programs Affect Women’s Access to Postpartum Care
What legislative proposals are currently being considered at the federal level to broaden postpartum coverage and strengthen maternity care?
In the 2019-2020 Congressional session, a number of federal bills related to maternal health care coverage, access, and quality are pending. Major themes across these bills include extension of Medicaid postpartum coverage to 12 months, coverage of doulas, greater support for state maternal mortality review committees, broadening provider networks in rural areas, and training on health equity and implicit bias for providers. Some notable federal bills that have garnered attention include:
H.R. 4996 Helping Medicaid Offer Maternity Services (MOMS) Act of 2019 (sponsored by Rep. Robin Kelly), would amend the Medicaid program to allow states the option to extend continuous coverage with full benefits for postpartum individuals through one year postpartum. The bill was approved unanimously by voice vote in the House, and while many advocates and policymakers called for the Senate to pass the bill before the end of the 2019-2020 session, it was not passed.
H.R. 1425, Patient Protection and Affordable Care Act Enhancement Act – This bill focuses on strengthening the ACA, but also includes a change to the postpartum period under Medicaid from 60 days to a full year. This differs from the Helping MOMS Act, which proposes a state option, while this bill requires mandatory 12 months postpartum coverage in all states. There would likely be significant differences in financing and access to care between proposals that create a mandatory expansion versus a state option, which some states would not adopt.10 A CBO analysis of the coverage extension in HR 1425 estimates a resulting $6 billion increase in the deficit over ten years. The bill passed the full House of Representatives in June 2020.
H.R. 6142 – The MOMNIBUS is a package of nine bills sponsored by the Black Maternal Health Caucus in the House of Representatives and Vice-President elect Kamala Harris in the Senate. It is intended to improve different aspects of maternal health care for pregnant people, with a focus on health equity. Key components in the package include an extension of WIC benefits for one year postpartum, measures to diversify the perinatal workforce, funding to enhance maternal mortality committees and data collection, and mitigating the impact of social determinants of health. The MOMNIBUS has not yet been heard in a House committee.
Conclusion
As President-elect Biden, Vice President-elect Harris, and a new Congress come into office, maternal health, particularly large and persistent racial and ethnic inequities, continues to be a major health challenge. Coverage changes alone cannot address these issues, but given Medicaid’s large role in maternity financing and health coverage for communities of color, an extension of postpartum coverage for the full year after a Medicaid birth could provide stable coverage and care to more low-income birthing parents in both non-expansion and expansion states. For birthing parents, the need for health care services does not end two months after childbirth.
The ACA offers states the option to extend Medicaid eligibility to low-income parents with incomes up to 138% of the federal poverty level. However, in the 12 states that have not adopted full scope Medicaid expansion, most postpartum women lack a pathway to coverage and are at greater risk of becoming uninsured and losing access to critical health services in the postpartum and intrapartum periods. Some federal and state-level initiatives are in place to provide coverage for family planning or other more limited services to some reproductive age and postpartum people, but they do not provide the same level of coverage afforded by full scope Medicaid. Absent federal action, these decisions will continue to be in the hands of the states to decide whether to choose from among a number of pathways to expand coverage for new parents.
Many Relied on Another Person’s Help to Try to Get a Vaccine Appointment
As many states and local authorities ramp up their COVID-19 vaccination efforts, the latest KFF COVID-19 Vaccine Monitor report provides the first in-depth look at Americans’ experiences trying to gather relevant information and sign up to get vaccinated.
The report shows that many older Americans have been able to navigate the system successfully to get vaccinated, though a significant minority are frustrated and have been unable to sign up for a shot.
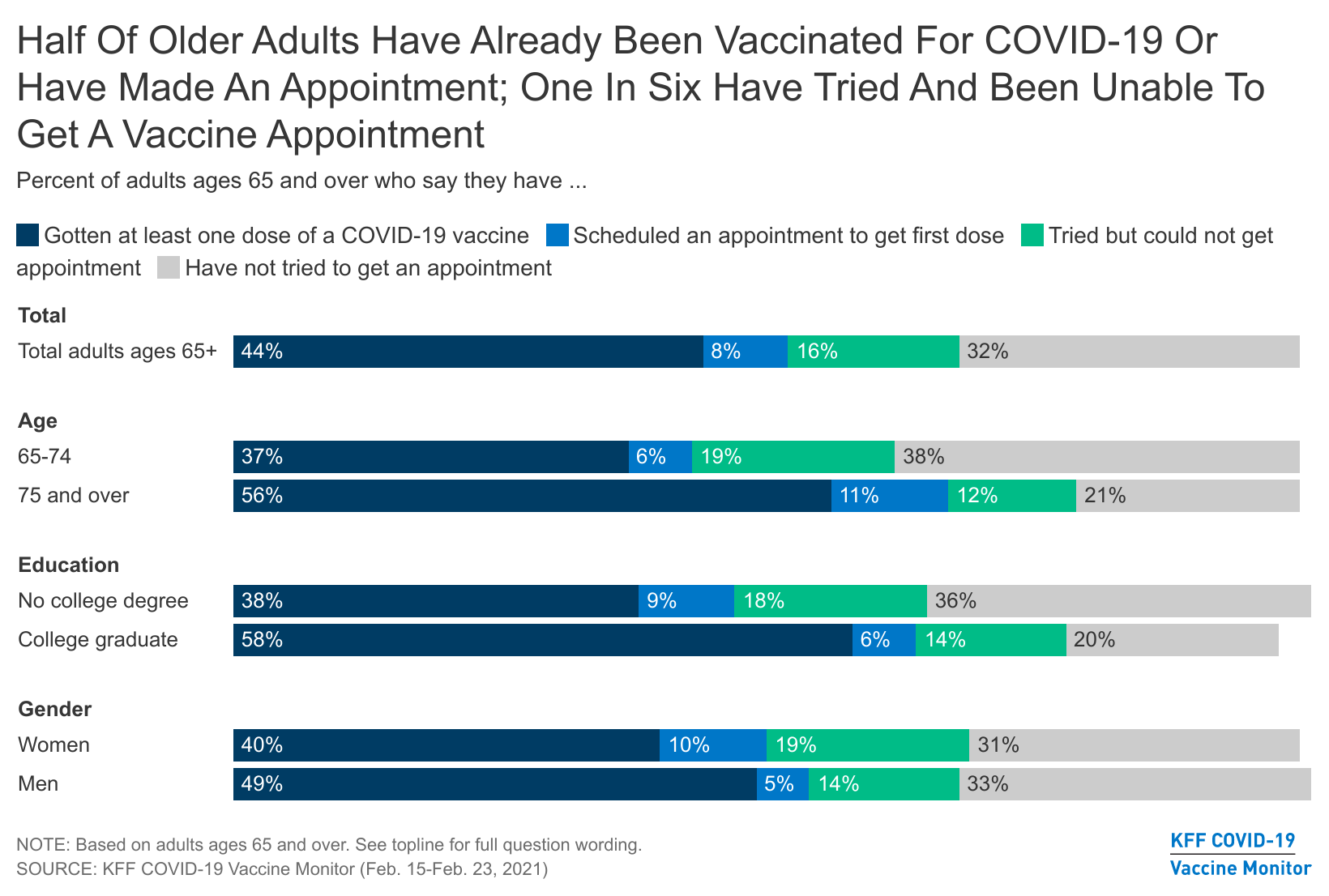
Among those at least 65 years old – a group eligible to get vaccinated in nearly all states – about half have either already received at least one dose of a COVID-19 vaccine (44%) or have an appointment to get vaccinated (8%). An additional 16% say they tried to make an appointment but could not.
Most of the older adults who got vaccinated or attempted to get an appointment say the process was easy to navigate, but 43% say it was difficult. This could be due to difficulties navigating the sign-up system or to the demand for vaccine exceeding supply in their area.
Older adults with college degrees, who may be better able to navigate the sign-up systems, are more likely than those who have not graduated from college to say they have received or scheduled their first dose (65% compared to 46%).
Available through the Monitor’s online dashboard, the new report also examines other aspects of people’s experiences trying to get a COVID-19 vaccine and accessing relevant information. Key takeaways include:
Among adults of any age who have gotten vaccinated, 39% say someone else helped them get the appointment. On the flip side, a third (33%) of all adults say they helped someone else find information about when and where to get vaccinated, and nearly a quarter (23%) say they helped someone make a vaccine appointment.
Although anecdotes abound about children and grandchildren helping older relatives get appointments, those at least 65 years old are more likely than younger adults to report assisting someone else (43% helped someone else find information and 32% helped someone get a vaccine appointment).
Among those who have not yet gotten the vaccine, nearly two thirds (63%) say they don’t have enough information about when they’ll be able to get the vaccine, and nearly half (45%) say they don’t have enough information about where to go. In addition, more than half (54%) say they don’t know enough about potential side effects.
Three-quarters of adults who are open to getting vaccinated say they would be very likely to get it at their doctor’s office, if available. Most also say they’d be very likely to get it at a local pharmacy (61%) or a hospital (55%), and about half say so about a community health clinic (49%) or their workplace (48%). When asked to pick their most preferred place, 38% chose their doctor’s office, followed by a local pharmacy (15%), hospital (9%), or their workplace (8%).
Designed and analyzed by public opinion researchers at KFF, the KFF Vaccine Monitor survey was conducted from February 15-23 among a nationally representative random digit dial telephone sample of 1,874 adults, including oversamples of adults who are Black (507) or Hispanic (506). Interviews were conducted in English and Spanish by landline (339) and cell phone (1,535). The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and acceptance, information needs, trusted messengers and messages, as well as the public’s experiences with vaccination.
The KFF COVID-19 Vaccine Monitor is an ongoing research project tracking the public’s attitudes and experiences with COVID-19 vaccinations. Using a combination of surveys and qualitative research, this project tracks the dynamic nature of public opinion as vaccine development and distribution unfold, including vaccine confidence and acceptance, information needs, trusted messengers and messages, as well as the public’s experiences with vaccination.
Key Findings
A little over two months into the U.S. efforts to distribute and administer the COVID-19 vaccine, and as many states and localities ramp up efforts and work out the kinks in their systems, the latest KFF COVID-19 Vaccine Monitor shows that while the scheduling process has been smooth for most of those who got vaccinated, some older adults have had difficulty getting a vaccination appointment and many others have had trouble finding information about where or when they will be able to get the vaccine.
Among adults ages 65 and over, who are now eligible to be vaccinated in nearly every U.S. state, about half say they have already received at least one dose of the vaccine (44%) or have scheduled an appointment to do so (8%). However, one in six older adults (16%) say they have tried but been unable to make an appointment to get vaccinated. Among older adults who got vaccinated or attempted to get an appointment, about half say the process was easy and about four in ten say it was difficult.
Among those who have gotten at least one dose of the COVID-19 vaccine, four in ten across age groups say someone else helped them get the appointment. About half of those who helped others try to get an appointment say it was difficult to get an appointment, while a similar share say it was easy.
Among those who have not been vaccinated, just over four in ten (44%) say they have tried to look for information about when or where to get the COVID-19 vaccine. About six in ten (57%) of this group say the information was easy to find and four in ten (42%) say it was difficult. Overall, nearly two-thirds (63%) of those who haven’t been vaccinated say they don’t have enough information about when they’ll be able to get vaccinated and nearly half (45%) say they don’t have enough information about where they can go to get the vaccine.
Asked where they would most like to go to get the COVID-19 vaccine, the largest share across demographic groups says they want to get it at their own doctor’s office (75% say they’d be very likely to get it there if it was available, and 38% pick their doctor’s office as the place they would most prefer to go among a range of options). Fifteen percent choose a pharmacy as the place they’d most like to get vaccinated, followed by a hospital (9%) or their workplace (8%). Others say they’d choose locations such as a community health clinic, a local school, a church or other religious site, or a large vaccination site run by the government, suggesting that having multiple distribution avenues will help in reaching different segments of the U.S. population with a trusted place to go to get vaccinated.
While there is variation across states and even counties in terms of who is currently eligible to receive the COVID-19 vaccine, most states have opened up vaccinations to those ages 65 and over. New analysis from the KFF COVID-19 Vaccine Monitor shows that about half of adults in this age range say they have either gotten their first vaccine dose (44%) or have scheduled an appointment to do so (8%). Another one in six (16%) say they tried to make an appointment to get vaccinated but were unable to get one.
Some states started vaccinating adults ages 75 and over before opening up vaccinations to other age groups, and this is reflected in a higher share of this group saying they have received or scheduled their first vaccine dose (67% of those ages 75 and over compared to 43% of those ages 65-74). In addition, older adults with college degrees, who may be better able to navigate the systems for signing up for vaccine appointments, are more likely than those who have not graduated from college to say they have received or scheduled their first dose (65% compared to 46%). About half of both men and women ages 65 and over say they have received or scheduled their first dose of the vaccine.
.Among older adults who either got the COVID-19 vaccine or tried to get an appointment, about half (52%) say it was easy to get an appointment while about four in ten (43%) say it was difficult. Combined with the fact that one in six older adults attempted to get a vaccination appointment but were unable, this suggests that while the process is working well for many of those among the first priority age group for vaccination, others are encountering difficulties and frustration when attempting to sign up.
.Ease Of Finding Information About When And Where To Get Vaccinated
Among adults of all ages who have not yet been vaccinated, just over four in ten (44%) say they have tried to look for information about when or where to get the COVID-19 vaccine. Among all those who were either vaccinated or tried to look for information, just over a third (36%) say that information was difficult to find while most (63%) say it was easy. Those who have gotten at least one dose of the vaccine are somewhat less likely to report difficulty finding information compared to those who looked for information but have not yet been vaccinated (24% vs. 42%).
Among those who are most eager to get the COVID-19 vaccine (those who say they will get it as soon as it’s available to them), about six in ten (63%) say they have looked for information about where or when they can get the vaccine, and nearly half that group (28% overall) say the information was difficult to find.
.Who Got Help? Who Is Helping?
Among those who have gotten at least the first dose of a COVID-19 vaccine, four in ten (39%) say that someone else helped them find or schedule a vaccine appointment while six in ten (59%) completed the process on their own. The share who report getting help signing up is similar among both older and younger adults who have gotten the vaccine (40% of those ages 18-64 and 39% of those ages 65 and over). Those without a college degree (50%) and those with household incomes under $40,000 (55%) are somewhat more likely than their counterparts with higher levels of income and education to report getting help with finding or scheduling a vaccine appointment.
.One third of adults overall say they have helped someone else find information about when and where to get vaccinated and close to a quarter (23%) report helping someone else get a vaccine appointment. While those with lower levels of income and education are more likely to report getting help finding vaccine appointments, the opposite is true when it comes to doing the helping. Nearly half of college graduates (47%) and those with incomes of $90,000 or more (45%) say they have helped someone else find information and about three in ten in these groups say they’ve helped someone get a vaccine appointment (32% and 30%, respectively). Although anecdotes abound about adult children and grandchildren helping older relatives get appointments, those ages 65 and over are in fact more likely than younger adults to report assisting someone else (43% say they’ve helped someone else find information and 32% have helped someone get a vaccine appointment).
.Those helping others report similar levels of difficulty finding information and getting appointments as those who completed these tasks on their own. Among those who helped someone else look for information about when and where to get vaccinated, six in ten (62%) say it was easy and four in ten (38%) say the information was difficult to find. Among those who helped someone else try to get a COVID-19 vaccination appointment, half (49%) say the process was difficult and a similar share (46%) say it was easy.
.Information And Outreach
At this point, a much larger share of the public reports seeing messages in the media urging people to get the COVID-19 vaccine than says they have asked a health care professional for information or received information via targeted outreach. Among those who haven’t been vaccinated, seven in ten (71%) say they’ve seen messages online or in the media, one-quarter have asked a health care provider for information, and about one in five (18%) have been contacted by a health organization or agency with information about how to get the vaccine.
While large shares across demographic groups report seeing messages online and in the media, older adults, women, and those with college degrees are both more likely to say they have asked a health care provider for more information and more likely to say they have been contacted by a health care provider, insurance company, or public health agency with information about how to get vaccinated for COVID-19.
Despite high visibility of outreach campaigns online and in the media, large shares of the public continue to say that they don’t have enough information about the potential side effects of the COVID-19 vaccine, or about when or where they will be able to get vaccinated. Among those who have not yet gotten the vaccine, awareness about where to get vaccinated increased somewhat over the past month; 55% now say they have enough information about this, up from 43% in January. Yet this leaves 45% saying they don’t have enough information about where to get vaccinated. In addition, 63% of those who haven’t been vaccinated say they don’t have enough information about when they’ll be able to get the vaccine and over half (54%) say they don’t know enough about the potential side effects of the vaccine, both essentially unchanged from last month.
.Among those who have not yet been vaccinated, adults with lower incomes are more likely than those with higher incomes to say they don’t have enough information about where they can get vaccinated as well as the potential side effects of the COVID-19 vaccine. In addition, Hispanic adults are more likely than White adults to say they don’t have enough information about where or when they can get the vaccine, and both Black and Hispanic adults are more likely than White adults to say they don’t have enough information about the potential side effects of the vaccine.
.Where People Want To Get Vaccinated
With COVID-19 vaccines increasingly becoming available at different locations across the U.S., we examined which locations people say they’d be willing to visit to get a COVID-19 vaccine, as well as the locations they would most prefer as vaccination sites. Individual doctor’s offices were at the top of both lists, but a range of locations were acceptable and preferred by different individuals.
Three-quarters of adults who are open to getting vaccinated (defined as those who say they will get the vaccine as soon as they can, after waiting to see how it works for others, or if required) say they would be very likely to get the COVID-19 vaccine at their doctor’s office, if it is available there. A majority also say they’d be very likely to get it at a local pharmacy (61%) or a hospital (55%) and around half say the same of a community health clinic (49%) or their workplace (48%). When asked to pick their most preferred place, 38% chose their own doctor’s office, followed by a local pharmacy (15%), a hospital (9%), or their workplace (8%). Fewer people say they’d most prefer to get the vaccine at a large vaccination site run by the government (5%), a community health clinic (4%), a local school (4%), a grocery store (4%), or a local church or religious center (3%).
.As previously reported, majorities of Black and Hispanic adults who are still deciding whether to get vaccinated are concerned that they won’t be able to get the vaccine from a place they trust. Given this, it’s important to understand preferred vaccination locations among Black and Hispanic adults.
Across racial and ethnic groups, the largest share says they would be “very likely” to get vaccinated at their own doctor’s office, though many are open to getting vaccinated at a range of other places as well. Black adults are somewhat less likely than White adults to say they’d be very likely to get vaccinated at work (39%), at a large vaccination site run by the government (31%), or at a local school (32%). However, the top choice three choices across Black, Hispanic, and White adults alike are their own doctor’s office, a local pharmacy, and a hospital.
.Concerns About Vaccine Effectiveness Against New Strains Of The Virus
Over half (53%) of adults are worried that the vaccines currently available against COVID-19 might not be effective against new strains of coronavirus, while another 47% aren’t worried. Adults who say they definitely won’t get the vaccine are the least likely to be worried, with 55% saying they are not worried at all.
The people who want the vaccine as soon as possible and those who are going to wait and see are the most concerned about the new strains, with seven in ten of those who plan to wait and see very or somewhat worried that it might not be effective, and 58% of those who want the vaccine as soon as possible who say the same.
Black and Hispanic adults are among the most concerned that the current vaccines might not be effective against new strains, with two-thirds of Hispanic adults (67%) and around three in five Black adults (61%) saying they are very or somewhat worried.
Methodology
This KFF COVID-19 Vaccine Monitor was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted February 15-23, 2021, among a nationally representative random digit dial telephone sample of 1,874 adults ages 18 and older (including interviews from 506 Hispanic adults and 507 non-Hispanic Black adults), living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). Phone numbers used for this study were randomly generated from cell phone and landline sampling frames, with an overlapping frame design, and disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity subgroups within each frame. Specifically, the cell phone frame was stratified as: (1) High Hispanic: Cell phone numbers associated with rate centers from counties where at least 35% of the population is Hispanic; (2) High Black: Cell phone numbers associated with remaining rate centers from counties where at least 35% of the population is non-Hispanic Black; (3) Else: numbers from all remaining rate centers. The landline frame was stratified as: (1) High Black: landline exchanges associated with Census block groups where at least 35% of the population is Black; (2) Else: all remaining landline exchanges. The sample also included 190 respondents reached by calling back respondents that had previously completed an interview on the KFF Health Tracking poll at least nine months ago. Another 387 interviews were completed with respondents who had previously completed an interview on the SSRS Omnibus poll (and other RDD polls) and identified as Hispanic (n = 180; including 50 in Spanish) or non-Hispanic Black (n=207). Computer-assisted telephone interviews conducted by landline (339) and cell phone (1,535, including 1,143 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. To efficiently obtain a sample of lower-income and non-White respondents, the sample also included an oversample of prepaid (pay-as-you-go) telephone numbers (25% of the cell phone sample consisted of prepaid numbers) Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the Census Bureau’s 2019 U.S. American Community Survey (ACS), on sex, age, education, race, Hispanic origin, and region, within race-groups, along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the January- June 2020 National Health Interview Survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample, and design modifications, namely, the oversampling of prepaid cell phones and likelihood of non-response for the re-contacted sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
This work was supported in part by a grant from the Chan Zuckerberg Initiative DAF, an advised fund of Silicon Valley Community Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Group
N (unweighted)
M.O.S.E.
Total
1,874
± 3 percentage points
COVID-19 Vaccination Status
Have gotten at least one dose of the COVID-19 vaccine
During the coronavirus pandemic, Medicaid has played a key role in providing coverage to millions of people who have lost their jobs or their health coverage. In addition, provisions included in the Families First Coronavirus Response Act (FFCRA) and the Coronavirus Aid, Relief and Economic Security (CARES) Act require states to maintain eligibility standards and provide continuous enrollment in Medicaid until the end of the public health emergency (PHE) in order to qualify for enhanced federal Medicaid funding. This report provides data on state Medicaid and CHIP eligibility levels and presents a snapshot of key aspects of state enrollment and renewal procedures in place during the COVID-19 PHE based on information from the 19th annual survey of Medicaid and CHIP program officials in the 50 states and DC. The report includes policies for children, pregnant women, parents and other non-elderly adults whose eligibility is based on Modified Adjusted Gross Income (MAGI) financial rules. Key findings from the survey include the following.
In 2021, Medicaid and CHIP eligibility is largely unchanged from 2020 as a result of maintenance of eligibility (MOE) requirements. State eligibility levels across all groups remained steady throughout 2020 due to the FFCRA’s increased FMAP and MOE provisions. Children and pregnant women continue to be covered at higher income levels while the coverage gap for low-income adults persists in the 14 states that have not implemented the expansion. In October 2020, Nebraska became the 37th state, including the District of Columbia, to implement the Medicaid expansion following its adoption through a ballot initiative in 2018. Voters in Missouri and Oklahoma approved similar initiatives in 2020 and will implement the expansion later in 2021.
Even with the MOE, most states are renewing coverage when possible and taking other steps to prepare for the end of the PHE. Most states are renewing coverage when they are able to confirm ongoing eligibility through electronic data sources. Two-thirds of states processing renewals also indicate they are sending renewal forms or requests for information when they are unable to renew coverage automatically through other data sources. Although states may not now terminate coverage for lack of response or ineligibility, sending renewal requests enables states to extend coverage for those who respond with proof that they remain eligible. In addition, just over a third of states have established a new 12-month renewal period when processing a change in circumstances that results in a new eligibility pathway. As states prepare for the end of the PHE, more than one-third are continuing or plan to take proactive steps to update enrollee mailing addresses. These actions will help to reduce backlogs and minimize coverage disruptions at the end of the PHE. Only 17 states reported an increase in new applications since the beginning of the COVID-19 PHE. This could be because of smaller than expected declines in employer-sponsored insurance, drops in applications at the beginning of the pandemic due to office closures, and the elimination of reapplications (where an individual loses coverage, often due to procedural reasons, then reapplies a short time later) due to the MOE requirements.
Administrative actions and Congressional proposals will have implications for Medicaid coverage and enrollment as well as for state efforts to plan for resuming normal operations after the PHE. In a letter to Governors, the Biden administration noted that the PHE is likely to extend for the entirety of 2021 and promised a 60-day notice before the PHE is terminated or is allowed to expire. In December 2020, CMS released guidance outlining how states are expected to unwind emergency authorities and resume normal eligibility and enrollment processing after the end of the PHE. Although the extension of the PHE gives states more time to prepare for it to end, it is possible CMS will issue additional clarifying guidance, which would affect states’ planning efforts. The administration also recently announced it will revise Medicaid waiver demonstration policy and rescind guidance related to work requirements and may also revise demonstration policy related to capped financing. In addition, the latest COVID relief legislative package includes provisions to provide states the option to extend coverage for pregnant women to 12 months postpartum in both Medicaid and CHIP and to provide financial incentives for non-expansion states to adopt the Medicaid expansion. The eligibility and enrollment policies presented here provide a baseline for assessing changes states may make in response to these federal policy shifts.
Report
Introduction
Since its emergence a year ago, the coronavirus has had implications for the health of the nation and our economy, exposing gaps in the public health infrastructure and further highlighting the importance of health coverage. During this time, enrollment in Medicaid has increased as people sought coverage after losing jobs or income because of the pandemic. Through the Families First Coronavirus Response Act (FFCRA) and the Coronavirus Aid, Relief and Economic Security Act (CARES), states are required to maintain eligibility standards and provide continuous enrollment in Medicaid until the end of the public health emergency (PHE) in order to qualify for a 6.2 percentage point increase in Federal Medical Assistance Percentage (FMAP). The continuous coverage provision, along with new applications, resulted in Medicaid enrollment growth of 6.7% between February and September 2020 (the most recently available data). States were also able to adopt a range of options through temporary changes in their state Medicaid plans (SPAs),through disaster-related waivers, and through other administrative authorities to streamline processes and connect individuals to coverage more quickly, such as expanding use of presumptive eligibility and allowing self-attestation of certain eligibility criteria.
This 19th annual survey of the 50 states and the District of Columbia (DC), provides data on state Medicaid and CHIP eligibility levels and presents a snapshot of key aspects of state enrollment and renewal procedures in place during the COVID-19 public health emergency. In light of the ongoing COVID-19 pandemic, the survey was scaled back in length and scope and focuses on state actions taken or planned in response to the pandemic. The report is based on a survey of state Medicaid and CHIP program officials conducted by the Kaiser Family Foundation (KFF) and the Georgetown University Center for Children and Families during January 2021. The report includes policies for children, pregnant women, parents and other non-elderly adults whose eligibility is based on Modified Adjusted Gross Income (MAGI) financial eligibility rules; it does not include policies for groups eligible through Medicaid pathways for adults over the age of 65 or on the basis of disability.
Medicaid and CHIP Eligibility
As of January 2021, Medicaid and CHIP eligibility is largely unchanged from 2020 due to maintenance of eligibility (MOE) requirements tied to enhanced federal funding. To help support states and promote stability of coverage amidst the COVID-19 pandemic, the FFCRA provides a 6.2 percentage point increase in the federal share (FMAP) of certain Medicaid spending if states meet certain MOE requirements. The MOE provisions prohibit states from tightening eligibility and enrollment standards beyond policies in place as of January 1, 2020 and require states to provide continuous coverage and to cover COVID-19 testing and treatment for Medicaid enrollees. The MOE continuous coverage requirement remains in place until the end of the month when the public health emergency (PHE) expires or is terminated. The MOE does not apply to CHIP programs, but other MOE requirements remain in place for CHIP.1 While states continue to have the flexibility to increase eligibility or implement new enrollment and renewal processes, the impact of the COVID-19 pandemic and the economic recession have limited states’ ability to do so, resulting in few changes in eligibility outside of temporary emergency authorities.
In October 2020, Nebraska implemented the ACA Medicaid expansion, the only major eligibility policy change in 2020. As of January 2021, 37 states extend coverage to adults without dependent children with incomes up to 138% FPL ($30,305 for a family of 3) (Figure 1). Also, in 2020, Missouri and Oklahoma voters approved ballot initiatives to implement Medicaid expansion in their states. When Medicaid expansion was first launched in January 2014, 26 states (including DC), participated. Since then, an additional 13 states have adopted the Medicaid expansion, six via state ballot initiatives. Following implementation in Missouri and Oklahoma, planned for mid-2021, the total number of expansion states will increase to 39.
Figure 1: Medicaid Income Eligibility Levels for Other Adults, January 2021
In states that have not implemented the Medicaid expansion, eligibility for parents and other adults remains extremely low (Figures 2 and 3). The median eligibility level for parents and caretakers in the 14 non-expansion states remains at 40% FPL ($8,784 annually for a family of three), ranging from a low of 17% FPL in Texas to 100% FPL in Wisconsin. Ten non-expansion states base eligibility on a fixed dollar threshold that is converted to the equivalent federal poverty level for comparison purposes. Over time, the equivalent eligibility level will decrease when annual updates adjust federal poverty levels upward to account for inflation. Wisconsin remains the only non-expansion state to cover adults without dependent children, extending eligibility up to 100% FPL for these adults through a waiver.
Figure 2: Median Medicaid Income Eligibility Limits based on Implementation of Medicaid Expansion as of January 2021Figure 3: Medicaid Income Eligibility Limits for Adults in States that Have Not Implemented the Medicaid Expansion, January 2021
Children’s upper income eligibility in Medicaid and CHIP continues to be the highest of all eligibility groups with 49 states covering children at or above 200% FPL (Figure 4). In 2020, the median eligibility level for children held steady at 255% FPL, ranging from a low of 175% FPL in North Dakota to a high of 405% FPL in New York. More than a third of the states (19) cover children at or above 300% FPL. The only change in eligibility levels for children’s coverage was in Kansas, where CHIP eligibility is linked to a dollar-based income level tied to the 2008 FPL. While the dollar value remains the same, over time, the equivalent eligibility level will decrease when the federal poverty level is adjusted upward to account for inflation.
Figure 4: Income Eligibility Levels for Children in Medicaid/CHIP, January 2021
The median eligibility limit for coverage for pregnant women in Medicaid and CHIP is stable at 205% FPL (Figure 5). Across states, eligibility levels for pregnant women in Medicaid and CHIP range from a low of 138% FPL (the federal minimum level) in Idaho and South Dakota to a high of 380% FPL in Iowa. A total of 35 states cover pregnant women at or above 200% FPL. Six states have expanded coverage for pregnant women through CHIP, an option for states that cover pregnant women in Medicaid up to at least 185% FPL.
Figure 5: Income Eligibility Levels for Pregnant Women in Medicaid/CHIP, January 2021
As of January 2021, 41 states have adopted federal options or use state-only funds to extend coverage or limited benefits to some immigrant children, pregnant women, or non-elderly adults. CHIP’s enactment in 1997 included the unborn child option that allows states to provide coverage from conception to birth, thereby extending coverage to pregnant women regardless of immigration status. A total of 17 states have adopted this option. Then, the 2009 CHIP Reauthorization Act (CHIPRA) offered a new option for states to receive federal funding to cover lawfully-residing children and pregnant women in Medicaid and CHIP without the five-year waiting period. Since then, two-thirds of states (35) have implemented the option for children in Medicaid and all of those states with separate CHIP programs (24 states) cover lawfully-residing children in CHIP (Figure 6). Twenty-five states have adopted the CHIPRA option to cover lawfully-residing pregnant women. Additionally, eight states use state-funds to cover children who are ineligible for federal funding due to immigration status, five states provide pre-natal or postpartum services to some immigrant pregnant women, and eight states cover other immigrant adults.
Figure 6: Medicaid/CHIP Coverage for Lawfully Residing Immigrant Children and Pregnant Women, January 2021
The median eligibility level for family planning services is 206% FPL, but eligibility levels range from 138% FPL in Louisiana and Oklahoma to a high of 306% FPL in Wisconsin. In 2020, Texas became the 30th state to provide family planning services using federal funds. Texas offers family planning services through a Section 1115 demonstration waiver, Healthy Texas Women, which includes restrictions on free choice of family planning providers.
Enrollment and Renewal Processes During the PHE
One third of states have experienced an increase in new applications since the beginning of the COVID-19 PHE (Figure 7) and few states reported application backlogs. Seventeen states report that the volume of new applications increased during the COVID-19 PHE compared to the same period in 2019. Seven of these states (Delaware, Hawaii, Illinois, Nebraska, New York, Nevada, and Tennessee) report increases of greater than 10%. Despite overall Medicaid enrollment growth, states may not be experiencing large increases in applications for a variety of reasons, including smaller than expected declines in employer-sponsored insurance, a drop in applications early in the pandemic due to office closures and the elimination of reapplications (where an individual loses coverage, often due to procedural reasons, then reapplies a short time later) due to the MOE requirements. Only five states report current delays in processing new applications beyond the current timeliness standards. Two of the five states with backlogs indicated their current backlogs were lower than in the prior year, while one state indicated that the backlog was the result of decreased administrative capacity due to the pandemic. CMS expects that states will resume timely processing of all applications within four months of the end of the PHE. Since most states are not currently experiencing application backlogs, they can potentially focus resources on processing renewals or changes in circumstances before the end of the PHE.
Figure 7: States Indicating an Increase in Applications by Percent Change in Application Volume, January 2021
Just over half of states (28) report a shift in how individuals are applying for Medicaid coverage, largely driven by an increase in online applications (Figure 8). The ACA required states to create a single streamlined application for Medicaid, CHIP, and Marketplace coverage and to provide options for individuals to apply for and renew coverage through multiple modes, including online and phone. Most states reporting a change in the primary mode of application experienced an increase in online applications, likely driven by limited access to in-person application assistance at state and local eligibility offices or through community-based assisters due to COVID-19.
Figure 8: States Reporting A Change in Primary Mode of Application, January 2021
CMS has recommended that states take steps to increase the share of online applications in a planning tool it developed to help states prepare for the end of the PHE. Electronic applications can expedite determinations and reduce both administrative costs and errors associated with manual data entry. As reported in the 2020 survey, the share of applications received online varies considerably among states, ranging from less than 10% to more than 90%. Both states that reported high and low shares of online applications in 2020 reported experiencing an increase in online applications. States can use a variety of strategies to increase the volume of online applications, including actively promoting the weblink in all outreach and marketing efforts and developing mobile-based apps and creating portals for assisters to facilitate applications.2
As of January 2021, most states (41) report processing ex parte (automated) renewals to extend coverage for individuals during the PHE (Figure 9) and two-thirds of those states (28 of 41) are sending renewal forms or requests for documentation when they are unable to confirm ongoing eligibility through electronic data sources. Under the ACA, states must seek to complete automated or ex parte renewals by verifying ongoing eligibility through available data sources, such as state wage databases, before sending a renewal form or requesting documentation from an enrollee. While some states suspended renewals as they implemented the MOE continuous coverage requirements and made other COVID-related adjustments to operations, most states are now actively processing renewals. Other states will likely restart the renewal process in response to CMS guidance that outlines actions states should take during the PHE to resume normal operations to the extent possible. When states are able to confirm ongoing eligibility on an ex parte basis, including the 41 states currently processing automated or ex parte renewals, they have the option to extend the renewal date out to 12 months from the original renewal date or 12 months from when the renewal was processed to stagger renewal dates, but this may result in renewal periods for enrollees that are shorter than 12 months. If an enrollee submits documentation to verify ongoing eligibility at renewal, the state must extend coverage for a full 12 months.
Figure 9: States Reporting Processing Renewals as of January 2021
Slightly more than a third of states (19) have established a new 12-month renewal period when processing a change in circumstances that results in a new eligibility pathway. In November 2020, CMS published an interim final rule that provided options for states to transition enrollees determined ineligible for their current coverage to different coverage pathways for which they are eligible if such a transition is in the same tier of coverage (though it may cover fewer benefits or have higher patient cost-sharing). States may then retain the original renewal date or extend a new 12-month eligibility period if they have information needed to confirm ongoing eligibility. Some states report that pregnant women and children aging out of coverage are most likely to be given a new 12-month renewal period, while other states say enrollees in all MAGI-based eligibility groups are given a new 12-month renewal period.
Just over one third of states (19) proactively take steps to update mailing addresses or plan to do so before the end of the PHE (Figure 10). Once the PHE expires and states resume normal operations under current federal rules, states may automatically terminate coverage without the advance ten-day notice when an enrollee cannot be located.3 Prior to the COVID-19 pandemic, a number of states terminated coverage when mail was returned as undeliverable, potentially contributing to enrollment declines. Ongoing issues with the United States Postal Service (USPS) and the impact of the COVID-19 economic crisis on housing may exacerbate difficulties in reaching enrollees by mail. In 2020, states that took proactive steps to keep mailing addresses current reported using the USPS National Change of Address Database or contracting with vendors to facilitate the process. States may also check other public programs for more updated information or engage Medicaid managed care organizations in updating addresses. Additionally, as of 2020, 43 states offered online accounts, which make it easier for enrollees to update addresses among other features. A few states also reported taking additional action, such as attempting to contact enrollees via telephone.
Figure 10: States Reporting Plans to Proactively Update Addresses Prior to The End of The PHE, January 2021
Most states are not planning changes to eligibility or enrollment that are currently disallowed when the PHE ends. While all states will phase out the continuous coverage requirement, five states are planning to make other changes. Two states reported plans to move forward with implementing work requirements and three states plan to charge premiums for some adults. The Biden Administration has announced it intends to rescind work requirements demonstration waivers and may take additional action to revise waiver guidance, impacting states’ ability to implement these policies.
Looking Ahead
State eligibility and enrollment policies in place as of January 2021 provide a baseline for assessing state actions after the PHE ends and in response to new Medicaid policy options that may be adopted at the federal level. Currently, states cannot implement more restrictive eligibility policies than those in place as of January 1, 2020 and must provide continuous coverage to Medicaid enrollees until the PHE ends in order to receive enhanced federal funding. Their policy choices at the end of the PHE and decisions around adopting potential coverage options will have coverage implications for those who are currently enrolled and those who may become eligible.
The Biden Administration’s recent announcement regarding the likely extension of the PHE gives states more time to prepare for the end the PHE. In a letter to Governors, the Biden administration noted that the PHE is likely to extend for the entirety of 2021 and promised a 60-day notice before the PHE is terminated or is allowed to expire. Advance notice before the end of the PHE was one of the top responses when states were asked what additional guidance they need from CMS to plan for resuming normal operations.
States are taking steps now to prepare for the end of the PHE, but some indicate additional guidance would be helpful to reduce backlogs and minimize coverage disruptions. While most states are processing automated renewals when possible, states will still have a backlog of renewals that were not able to be completed. Some states noted the need for additional guidance to avoid unevenly distributed workloads due to large numbers of renewals and other changes occurring in a short period of time. When the PHE ends, CMS guidance issued under the Trump administration allows states to send coverage termination notices to individuals who did not respond to requests for information, did not return renewal forms, or lost eligibility for other reasons within six months of the end of the PHE. This approach may result in coverage losses at the end of the PHE for individuals who remain eligible. CMS guidance also gives states six months to catch up on pending renewals and other changes once the PHE ends; however, several states indicated that 12 months would allow for a smoother resumption of operations. While states can use this guidance to help plan for the end of the PHE, it is possible the Biden administration could revise the guidance, which would affect states’ planning efforts.
As states prepare to return to normal operations at the end of the PHE, there are additional considerations beyond resuming routine eligibility and enrollment procedures. In addition to the MOE requirements, states implemented a variety of temporary strategies to deal with the pandemic including, but not limited to eligibility, enrollment or renewal. These changes were wide ranging, impacting all aspects of Medicaid from improving access to telehealth and easing prior authorization requirements to waiving premiums or cost-sharing and modifying appeals and fair hearing requirements. CMS has developed two planning tools to aid states in preparing for the end of the PHE. The first focuses on eligibility and enrollment pending actions and the second provides assistance in general planning to restore regular Medicaid and CHIP operations. Together, the tools prompt states to consider actions that will aid in a smooth return to normal operations, including how they communicate with beneficiaries and stakeholders and how to extend or permanently implement flexibilities adopted through Section 1135 emergency waivers or disaster-related temporary state plan amendments.
Administration actions and Congressional proposals would reduce some barriers to Medicaid enrollment and support targeted Medicaid coverage expansions. The Biden administration has already reopened the marketplace and will restore funding for outreach, marketing and consumer assistance that will help connect uninsured individuals with Medicaid and CHIP. The administration also recently announced it will revise waiver demonstration policy and rescind guidance related to work requirements and may also revise demonstration policy related to capped financing. In addition, the latest COVID relief legislative package includes provisions to provide states the option to extend coverage for pregnant women to 12 months postpartum in both Medicaid and CHIP and to provide financial incentives for non-expansion states to adopt the Medicaid expansion.
42 CFR §431.213 – Exception from advance notice. The agency may send a notice not later than the date of action if: (d) The beneficiary’s whereabouts are unknown and the post office returns agency mail directed to him indicating no forwarding address (See §431.231 (d) of this subpart for procedure if the beneficiary’s whereabouts become known). ↩︎
THE CONVERSATION: Between Us, About Us, A New Campaign By Black Health Care Workers for Black People about the COVID-19 Vaccines
W. Kamau Bell Joins Black Doctors, Nurses and Researchers to Dispel Misinformation and Provide Accessible Facts in this Video Series to be Featured on YouTube
March 4, 2021 – THE CONVERSATION: Between Us, About Us. is a new campaign to provide Black communities with credible information about the COVID-19 vaccines co-developed by KFF (Kaiser Family Foundation) and the Black Coalition Against COVID. Black doctors, nurses and researchers dispel misinformation and provide accessible facts in 50 FAQ videos that deliver the information Black people are asking for about the COVID-19 vaccines. More videos and voices will be added to this one-of-its-kind living video library as new questions arise and information becomes available.
The series debuts on YouTube today with a launch video featuring W. Kamau Bell in an open, honest conversation with Black health care workers that gets to the heart of Black people’s questions and concerns. YouTube is providing significant support for the campaign, including high visibility promotion across its platform.
Despite having one of the highest COVID-19 mortality rates in the U.S., Black Americans are among those least likely to get the vaccines. “As Black health academicians, researchers, and clinicians, we understand our empathy-based responsibility to provide our community with the resources and guidance on surviving this pandemic,” said Reed Tuckson, MD, Founding Member, Black Coalition Against COVID. “As such, we appreciate this partnership with KFF to produce one of the largest of its kind campaigns to creatively provide trustworthy information that will save Black lives.”
“We’re seeing more Black adults want to get vaccinated when their time comes, but still a sizeable percent say they are waiting to see others vaccinated first. Among this group, many share common concerns that are directly addressed in this campaign,” said Drew Altman, PhD, President & CEO, KFF, which produced the campaign as the first initiative in its Greater Than COVID public information response to the pandemic.
“The Biden Administration has made a commitment to prioritize equity, in policy and practice. As we work toward eliminating the severe and pervasive health and social inequities that have been exacerbated by this pandemic, we know we can’t do it alone. Honest and transparent communication about the vaccine is a critical piece of this work. That’s why, I’m proud to listen to and support THE CONVERSATION. This work truly exemplifies the power partnerships have to uplift the voices of Black health care workers and ensure that those most impacted by this pandemic have the resources they need to respond to it,” said Marcella Nunez-Smith, MD, MHS, Chair, COVID–19 Health Equity Task Force and Associate Dean, Yale University.
“There are two major barriers to Black folks receiving the COVID-19 vaccines. Neither one of them are vaccine hesitancy. The barriers are accessible facts about the COVID-19 vaccines and convenient access to receive a vaccine,” said Rhea Boyd, MD, MPH, a pediatrician and public health advocate, who co-developed the project with KFF and the Black Coalition Against COVID. “This is a comprehensive effort on behalf of Black health care workers across the country, to ensure every Black person in the United States has the credible information they need to make this critical choice. It is time for us to have a conversation, between us and about us.”
“Effective communication is as critical to the outcome of the vaccine program as manufacturing the shots. YouTube is where people are, and it’s where they are looking for information and support to guide them in health decisions. By partnering with KFF and the Black Coalition Against COVID, we are able to bridge the information gap between communities most at-risk and trusted health experts who are representative of those communities and make clinical topics like COVID vaccine development accessible and relatable in a way that only video can. Together, I believe we can reimagine how health information has traditionally been shared and make public health truly public,” explained Garth Graham, MD, Director and Global Head of Healthcare and Public Health at YouTube.
For more about THE CONVERSATION: Between Us, About Us., go to:
The California Health Care Foundation, Commonwealth Fund and Sierra Health Foundation have generously contributed funding to the production and are supporting distribution of the series.Through Greater Than COVID, KFF will also be working with partners to address information needs in other disproportionately affected communities.
* * *
Black Coalition Against COVID is a Washington, D.C.-based community initiative which seeks to provide trustworthy, science-based, information curated on behalf of and for the Black community about COVID-19 and the vaccine development process in an effort to help save Black lives at the national and local levels.
Greater Than COVID is a public information initiative from KFF to help individuals take charge of their health during the evolving COVID-19 public health crisis. Tailored media messages and community tools address information needs about the vaccines.