U.S. Department of Health and Human Services Report on Pediatric Gender Dysphoria and Gender Conversion Efforts
On May 1, 2025, the Department of Health and Human Services (HHS) released Treatment for Pediatric Gender Dysphoria: Review of Evidence and Best Practices, a report issued following the Executive Order, “Protecting Children From Chemical and Surgical Mutilation,” which directed the HHS Secretary to publish an evidence review related to gender dysphoria in young people within 90 days.
Access to gender affirming care has becoming increasingly contested political territory in the United States. A growing number of states have laws that ban youth access (27 to date), and there are numerous legal challenges underway, including a case that is before the Supreme Court. The issue also figured prominently in the presidential election cycle, with President Trump campaigning on promises to end access to such care. The Executive Order and report are in line with a range of other executive actions that question evidence around gender affirming care, aim to limit access to these medical services, particularly for youth, and, in some cases, promote misinformation or deny the existence of transgender people.
The report states that it is a review of the evidence and best practice regarding information about treatment of gender dysphoria. Its main conclusion is that the quality of evidence on the effects of any intervention is low, and evidence on harms is “sparse.” Still the report cites what it identifies as significant risks of medical transition, marking a departure from most medical associations and widely used guidelines in the U.S. Instead, the report supports the use of psychotherapeutic approaches, including an approach termed “exploratory therapy”, which can include conversion therapy.
Shortly after its release, the review received criticism by researchers, advocates, and medical association for its methods, lack of alignment with current guidance, promotion of misinformation, support of certain practices, and decision not to disclose the authors. A particular concern was raised about the review’s support of “exploratory therapy” Other groups including the Christian legal advocacy group Alliance for Defending Freedom and the Center for American Liberty supported the review’s assessment.
This policy brief reviews the main points raised by the report regarding its emphasis on psychotherapy, and recommendations around “exploratory therapy”, which could include gender conversion practices, as well as the current legal and policy environment across the country.
What does the report say about psychotherapy as treatment for gender dysphoria and conversion practices?
Psychotherapy is one of five dedicated parts in the review and a theme that receives significant attention is support for gender identity conversion based practices, sometimes called “conversion” or “reparative” “therapy,” which the report calls “exploratory therapy.” The report counters this description stating that “equating ‘exploratory therapy’ with ‘conversion therapy’ is misguided and that equating any “approach focused on reducing a minor’s distress about their body or social role [with conversion therapy] is a problematic.” Other reasons provided include: pointing to Dutch practices, stating that all therapy is exploratory, and noting that the label “conversion therapist” is damaging.
Conversion practices aim to “suppress or alter an individual’s sexual orientation or gender to align with heterosexual orientation, cisgender identity, and/or stereotypical gender expression. [These]…efforts are premised on or motivated by the belief that diversity in sexual orientation and/or gender identity and expression is a deficit, mental illness, or pathology.” Major medical associations (described in detail below) in the U.S. conclude that conversion practices lack evidence and are, at best, unfair or ineffective and at worst, harmful. The United Kingdom’s Cass Review, like the HHS report, reviewed evidence around gender affirming care for minors and made recommendations to the National Health Service. While it ultimately led to restrictions on access to this care in the UK, in discussing psychotherapy, it stated “that no LGBTQ+ group should be subjected to conversion practice.”
The review describes “exploratory psychotherapy,” in part, as “trying to help children and adolescents come to terms with their bodies” and goes on to equate the distress related to gender dysphoria with general “discomfort with the sexed body or with societal sex-based expectations is common during puberty and adolescence.” This goes against identified best practice which encourages clinicans to recognize to recognize that transgender and gender non-conforming people “are more likely to experience positive life outcomes when they receive social support or trans-affirmative care.”
The report promotes therapeutic approaches as first line treatment and suggests that they can be an “alternative to endocrine and surgical interventions for the treatment of pediatric gender dysphoria.” This runs contrary to guidelines which suggest a range of approaches to gender affirming care, which is highly individualized, to be delivered as clinically appropriate. The review presents therapeutic modalities and describes how they can be applied to treat gender dysphoria, noting especially their potential to interrogate the wish for gender transition. For example, of psychodynamic therapy, the review states that this modality “can help patients gain deeper understanding of their personal identity, including any external factors that may contribute to their cross-sex identification and desire for medical/surgical interventions…”
The report, and the Executive Order, also question Standards of Care issued by the World Professional Association for Transgender Health (WPATH), which are widely relied on guidelines that providers look to in delivering evidence based best practice gender affirming care. These standards are regularly referenced by major medical associations including the American Psychological Association. While the report suggests that psychotherapy is not common in delivering gender affirming care to minors, psychological wellbeing is promoted within WPATH’s guidance. WPATH recommends “health care professionals working with gender diverse adolescents undertake a comprehensive biopsychosocial assessment of adolescents who present with gender identity-related concerns and seek medical/surgical transition-related care, and that this be accomplished in a collaborative and supportive manner.”
What is the aim of conversion efforts and what does evidence say about them?
Gender conversion practices are based on the premise that non-cisgender identities are a pathology and that transgender people would benefit from changing their gender identity. Medical evidence does not support this and, as noted below, most major medical associations have concluded that such interventions stand to cause harm. Yet, the efficacy of and ability to provide these services, due to local regulations, remains somewhat contested.
Research has shown that lifetime exposure to gender identity conversion efforts are associated with adverse mental health outcomes, including higher odds of depression, suicidality, and suicide attempts and substance abuse.
Where does the medical establishment stand on conversion practices?
Sexual orientation and gender identity have a long history of being pathologized, including in the mental health field. It was not until 1994 that “transsexualism” was removed from the Diagnostic and Statistical Manual of Mental Disorders (DSM) when it was replaced with “gender identity disorder.” This diagnosis was then replaced with “gender dysphoria” in 2013. Today, it is widely accepted by established medical groups that the full spectrum of sexual orientations and gender identities are not pathologies and do not need treatment. The American Academy of Pediatrics, for example writes “variations in gender identity and expression are normal aspects of human diversity, and binary definitions of gender do not always reflect emerging gender identities.” Rather, some gender diverse people experienced distress “caused by the body and mind not aligning and/or societal marginalization of gender-variant people.” Thus, care is typically provided to relieve distress, not to try to treat certain gender identities.
Broadly, gender affirming care is supported by practically all major medical associations in the U.S., including, the American Medical Association, American Academy of Pediatrics, and the American Psychological Association. It is also supported through guidance from the Endocrine Society and the World Professional Association for Transgender Health (WPATH).
Specifically, conversion approaches to gender dysphoria contrast with recommendations from these medical associations, which criticize conversion practices, stating that they lack evidence, are ineffective, and can create harm. In August 2023, 28 medical and mental health associations signed onto a joint statement opposing conversion practices. Additionally, many have provided independent statements addressing their concerns regarding these practices. For example:
- An American Academy of Pediatrics (AAP) policy statement (reaffirmed in 2023) states that “reparative approaches have been proven to be not only unsuccessful but also deleterious and are considered outside the mainstream of traditional medical practice. The AAP described reparative approaches as ‘unfair and deceptive.’”
- In a 2018 policy statement The American Academy of Child and Adolescent Psychiatry (AACAP) wrote of “conversion therapies” that “these interventions are provided under the false premise that homosexuality and gender diverse identities are pathological. They are not; the absence of pathology means there is no need for conversion or any other like intervention. Further, there is evidence that ‘conversion therapies’ increase risk of causing or exacerbating mental health conditions in the very youth they purport to treat…AACAP asserts that such ‘conversion therapies’ (or other interventions imposed with the intent of promoting a particular sexual orientation and/or gender as a preferred outcome) lack scientific credibility and clinical utility. Additionally, there is evidence that such interventions are harmful. As a result, ‘conversion therapies’ should not be part of any behavioral health treatment of children and adolescents.”
- The American Psychological Association (APA) writes that “to consider …[gender identity change efforts (GICE)]…as therapies or treatments is inaccurate and inappropriate because, the incongruence between sex and gender in and of itself is not a mental disorder…so, any behavioral health or GICE technique or treatment that seeks to change an individual’s gender identity or expression is not indicated; thus, any behavioral health or GICE effort that attempt to change an individual’s gender identity or expression is inappropriate.”
- National Association of Social Workers (NASW) states that “NASW upholds that sexual orientation, gender identity, and gender expression are real and irrefutable forms of identity. Thus, NASW condemns any and all forms of conversion practices, as they are harmful to the mental health and well-being of LGBTQIA2S+. These practices stand in direct conflict with NASW’s professional code of ethics, and these practices represent a significant risk of harm by subjecting individuals to forms of treatment.”
How common is it for transgender people to experience conversion practices?
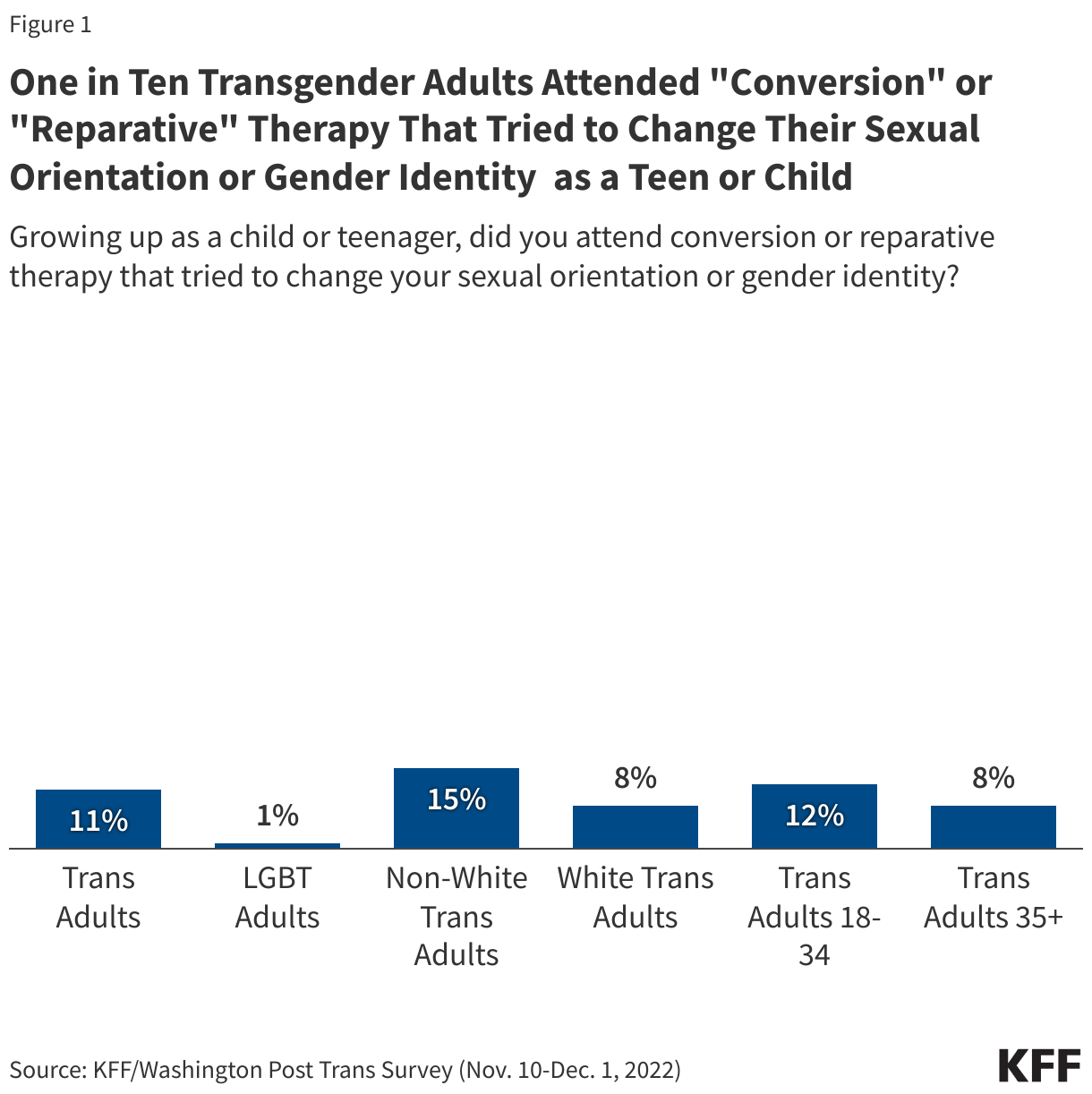
While conversion practices are widely discredited, KFF polling finds that one-in-ten transgender adults report having attended “conversion” or “reparative” therapy that tried to change their sexual orientation or gender identity as a teen or child. Since the share is much lower among LGBT adults as a group (1%), it is likely that many of these experiences were aimed at gender identity. Similarly, the Trevor Project finds that “13% of LGBTQ+ young people reported being threatened with or subjected to conversion therapy.”
What is the policy and legal landscape regarding conversion practices?
As noted, while medical consensus is against the use of conversion practices, this matter has not been settled in the policy realm. States have increasingly stepped in to regulate the practice in clinical settings, with almost half banning it in full or in part. According to data from the Movement Advancement Project, currently:
- 19 states and DC have bans on the practice of conversion therapy.
- 4 states have a partial ban in their state (e.g. banning the practice among those with only certain licenses or banning the use of state funds in the provision conversion therapy).
- 4 states prohibit local level bans on conversion therapy either via state law or a court ruling.
- 19 states have no policy.
Beyond these state actions, some cities and counties have enacted policies prohibiting at least certain conversion practices.
Notably, states currently have the ability to regulate therapeutic practice and prohibit conversion efforts by certain mental health professionals but conversion efforts also take place within religious settings and those are not included in these prohibitions. KFF polling finds that 25% of transgender adults report that they attended religious services that tried to change their sexual orientation or gender identity as a child or teen.
The ability of states to ban conversion therapy will soon be reviewed by the Supreme Court, which, on March 10, 2025, granted certiorari in Chiles v. Salazar, a case challenging Colorado’s conversion therapy ban for minors. The state’s ban, which prohibits mental health professionals from attempting or purporting to change a minor’s sexual orientation or gender identity, was upheld by the Tenth Circuit Court of Appeals in September 2024. Chiles, a Christian counselor, has appealed this decision and asked the Supreme Court to review “whether a law that censors certain conversations between counselors and their clients based on the viewpoints expressed regulates conduct or violates the Free Speech Clause.” A decision in Chiles’ favor could limit the ability of states to regulate such practices.
This review could be used as support for other actions the administration seeks to take (some described here) aimed at limiting minor access to gender affirming care. With respect to therapeutic practices, it could shift how some practitioners approach gender affirming care or potentially provide support to those using conversion related approaches. The report could also fuel misinformation in other areas, particularly around regret rates and the share of transgender young people seeking a medical transition.