KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Poll: Nearly Half of Adults Expect to Get the New COVID-19 Vaccine, But Most Parents Don’t Expect to Get It for Their Children; More Eligible Adults Expect to Get a Flu Shot and the New RSV Vaccine
Republicans are Much Less Likely than Democrats to View Fall Vaccines as Safe Or Expect to Get Them, though COVID-19 Sparks the Greatest Split in Intentions and Views
Nearly half of adults say that they will “definitely” or “probably” get the newly recommended COVID-19 vaccine, though most parents are not planning to get the shot for their children, according to the latest KFF COVID-19 Vaccine Monitor poll.
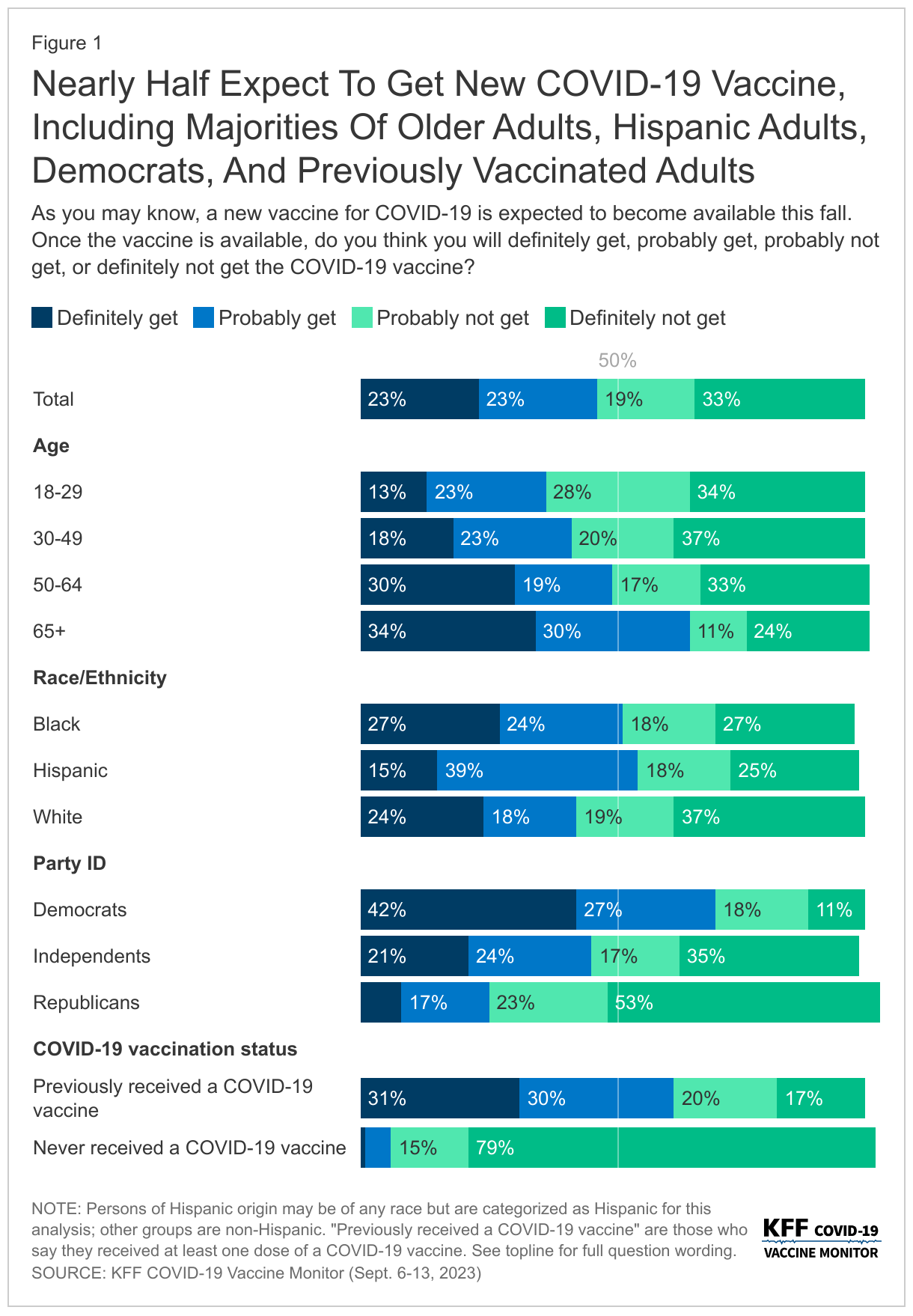
Among all adults, 23% say they will definitely get the new vaccine, 23% say they will probably get it, while 19% say they will probably not get it and 33% say they definitely not get it.
The share of the public who intend to get the new COVID-19 vaccine is higher than the share who have received previous booster shots, but not as high as initial vaccine uptake back in 2020. Almost four in ten (37%) people who previously received a COVID-19 vaccine say that they probably or definitely won’t get the new shot. Reflecting patterns from earlier vaccine rollouts during the pandemic, the groups most likely to say they definitely or probably will get the new vaccine include people at least 65 years old (64%) and Democrats (70%).
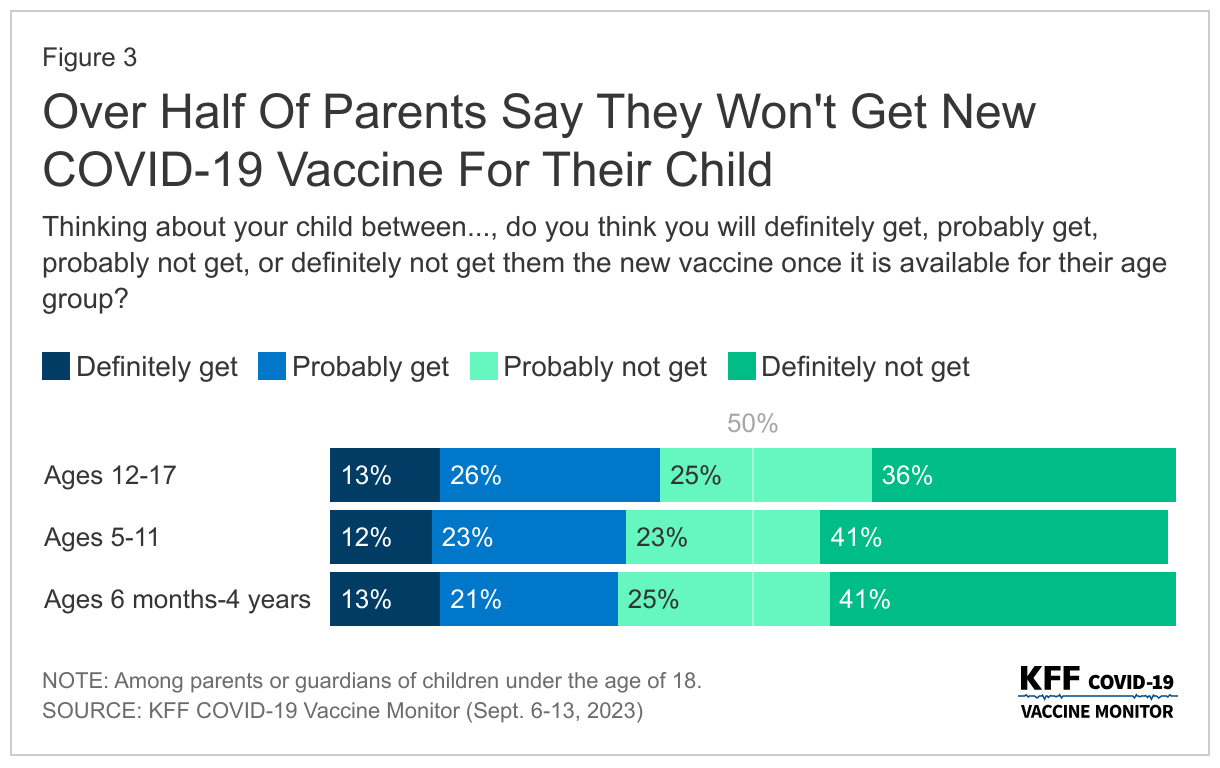
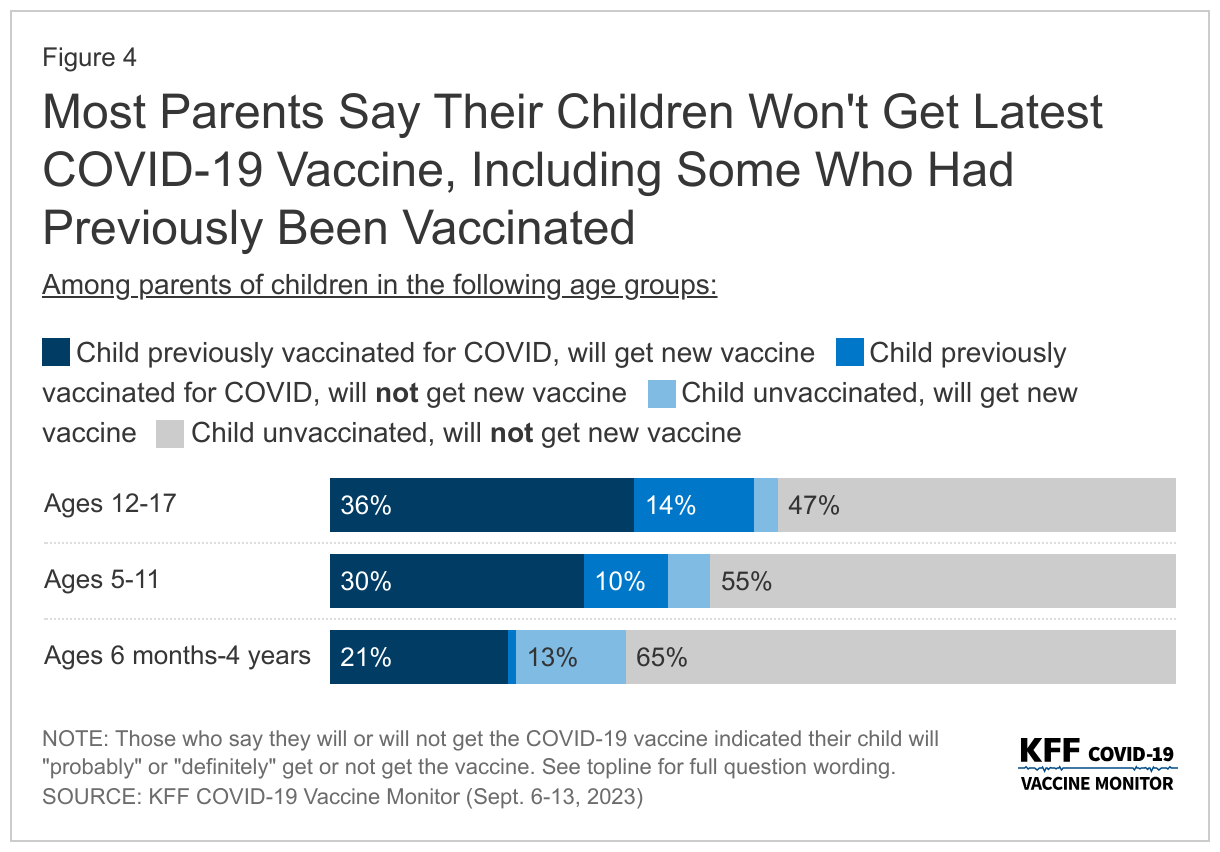
While the new COVID-19 vaccine is recommended for children ages 6 months and up, fewer than four in ten parents say they expect to get the vaccine for their children ages 12-17 (39%), ages 5-11 (36%), and ages 6 months through 4 years (34%). More than half of parents with children in each age group say they probably or definitely won’t get their children vaccinated.
The latest survey also shows that somewhat larger shares of eligible people expect to get an annual flu shot and a newly recommended vaccine for RSV (respiratory syncytial virus) than plan to get the COVID-19 vaccine. For example, most adults (58%) say that they have already gotten or expect to get a flu shot, and most adults ages 60 and older (60%) say they have already gotten or expect to get the new RSV vaccine (recommended for their age group).
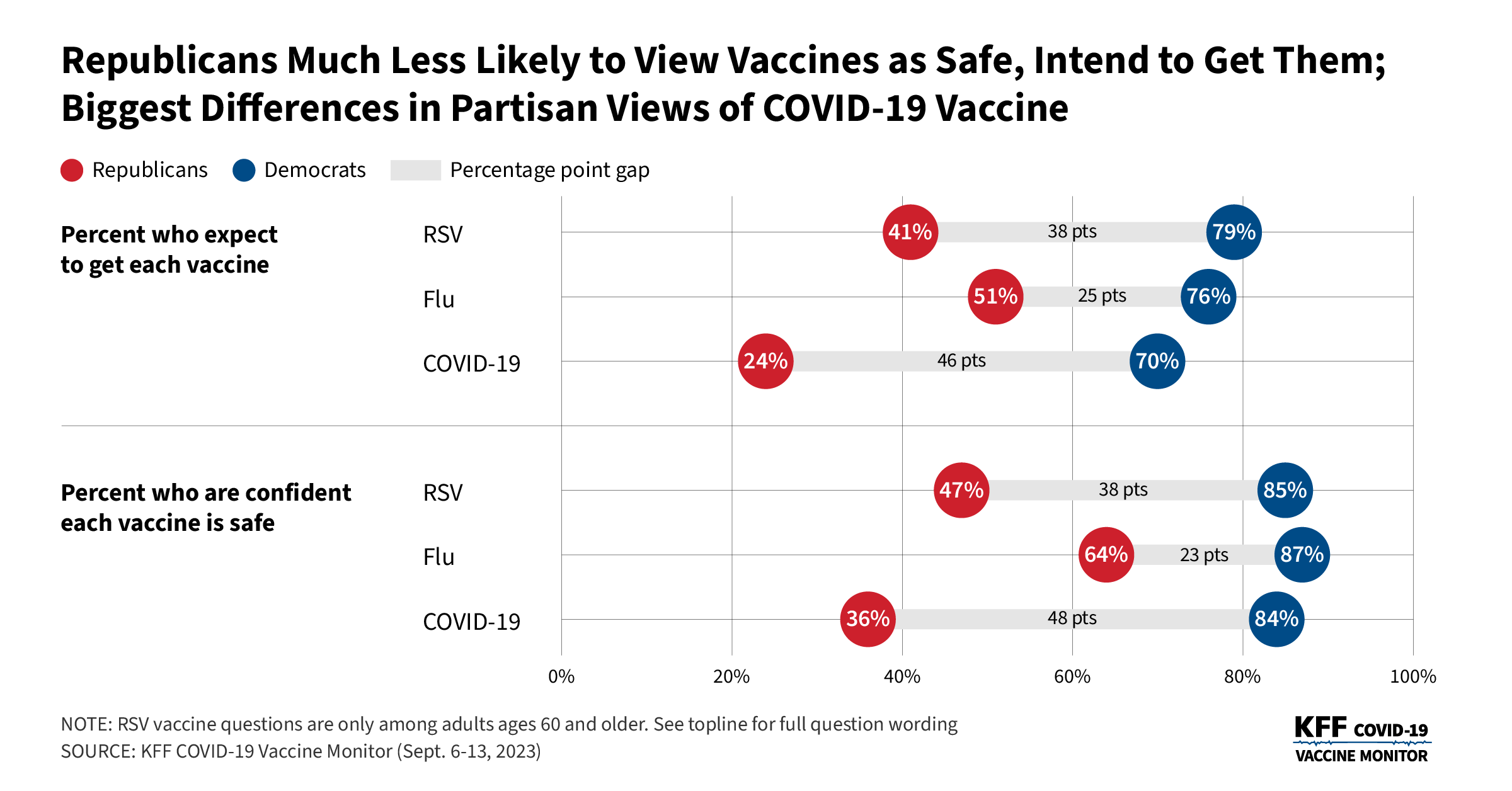
As has been true throughout the pandemic, a much smaller share of Republicans (24%) than Democrats (70%) expect to get the new COVID-19 vaccine – 46 percentage point gap.
There are smaller, but still considerable, partisan divisions in intentions for these vaccines than for the COVID-19 shot: for example, 76% of Democrats and 51% of Republican expect to get or have already gotten a flu shot this fall (a 25-point gap), while among those ages 60 and older, 79% of Democrats and 41% of Republicans expect to get or having already gotten an RSV vaccine (a 38-point gap)
Republicans are also less likely than Democrats to be confident that each of three vaccines are safe, with the biggest divide for the COVID-19 vaccine (84% of Democrats and 36% of Republicans are confident it is safe).
The partisan divides persist across a wide range of measures related to vaccines and the COVID-19 pandemic. Some examples:
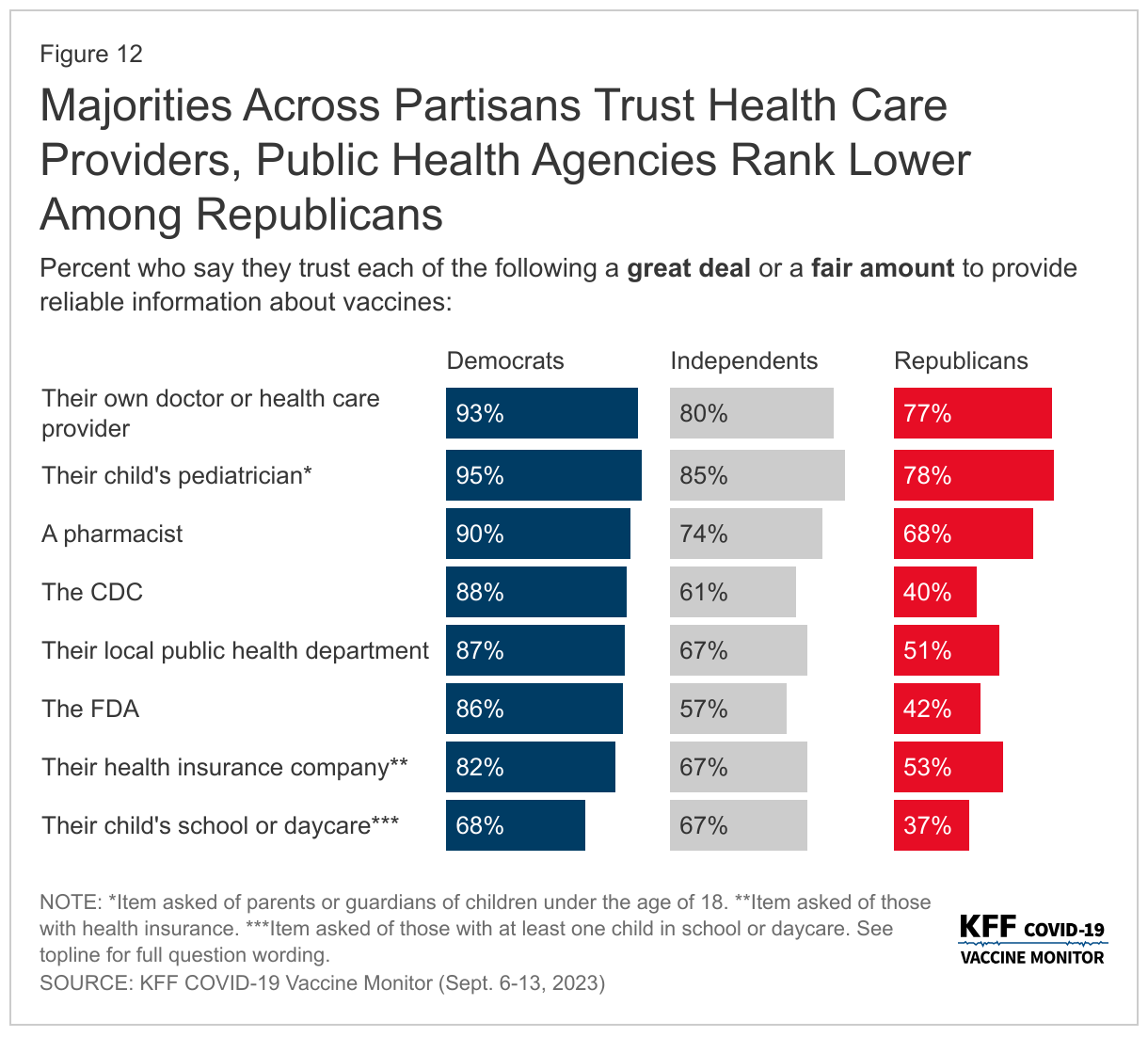
Trust in public health agencies. Overall, 63% of the public trust the Centers for Disease Control and Prevention (CDC) a great deal or a fair amount when it comes to providing reliable information about vaccines, and 61% trust the Food and Drug Administration (FDA).Much larger shares of Democrats than Republicans have at least a fair amount of trust in vaccine information from the CDC (88% vs. 40%), their local public health departments (87% vs. 51%), and the Food and Drug Administration (86% vs. 42%).
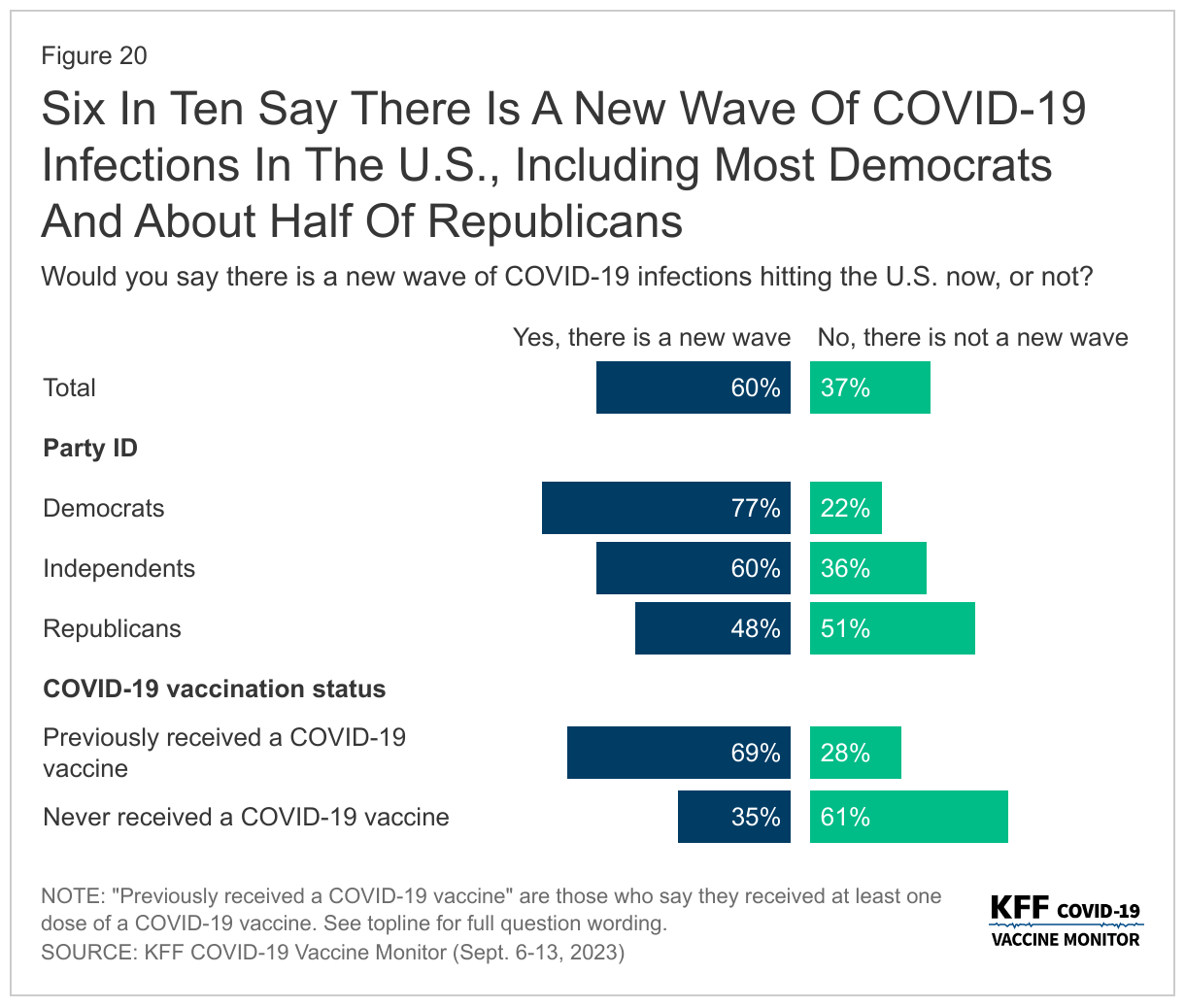
Perceptions about threat. Three quarters (77%) of Democrats say that there is a new wave of COVID-19 infections across the country. In contrast, similar shares of Republicans say there is (48%) and isn’t (51%) a new wave.
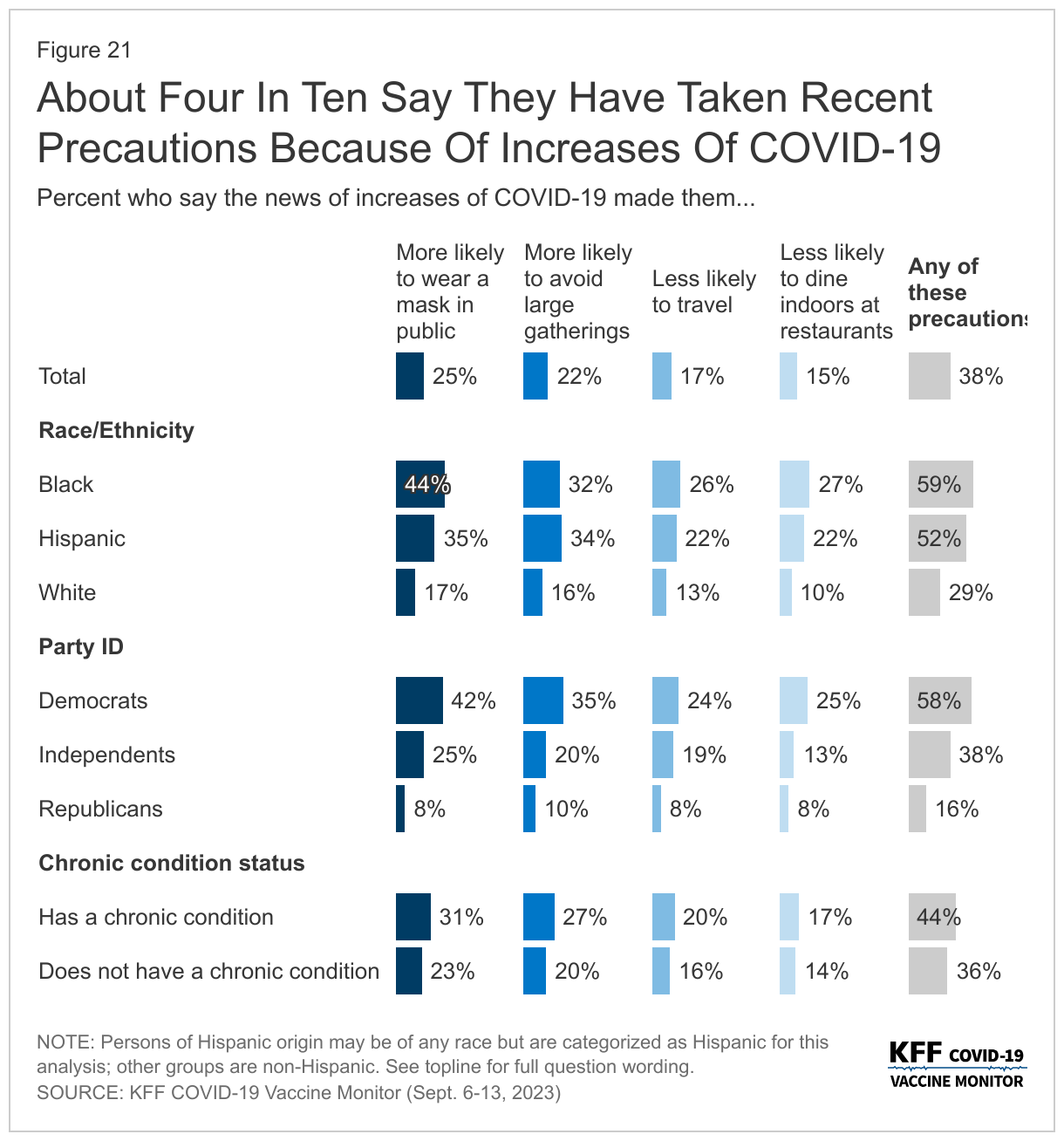
Taking precautions. Democrats are more than three times as likely as Republicans (58% vs. 16%) to say that news about the new COVID-19 wave has led them to take extra precautions, including being more likely to wear a mask in public or avoid large public gatherings, or being less likely to travel or to dine indoors at restaurants.
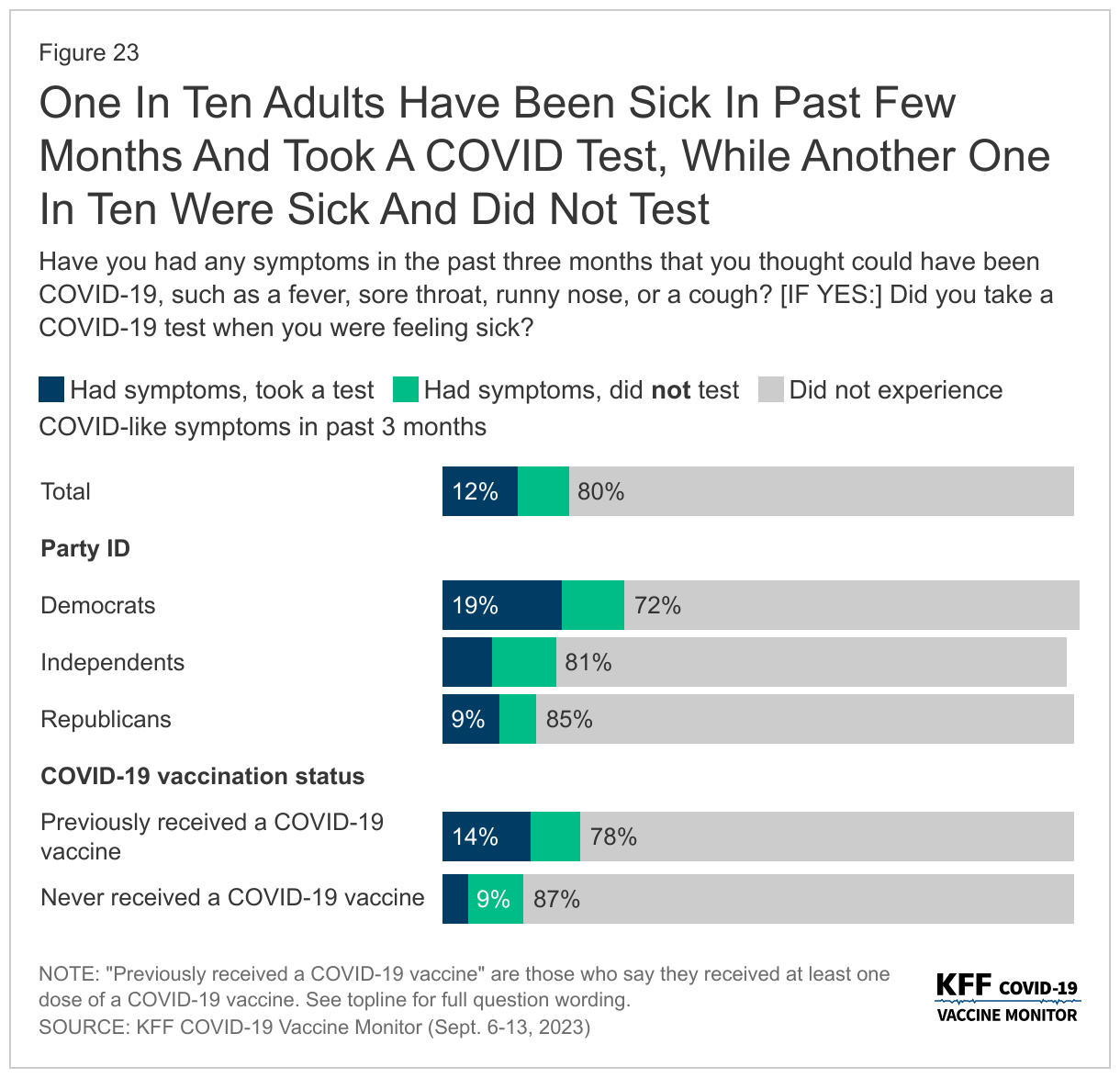
Getting tested. Republicans are half as likely as Democrats (9% vs. 19%) to say that they were sick in recent months and got a COVID-19 test.
“The poll shows that most of the nation still trusts the CDC and the FDA on vaccines – but there is a partisan gap, and most Republicans don’t trust the nation’s regulatory and scientific agencies responsible for vaccine approval and guidance,” KFF President and CEO Drew Altman said.
One area where partisans agree is that their personal doctors, including their children’s pediatricians, are their most trusted sources of vaccine information.
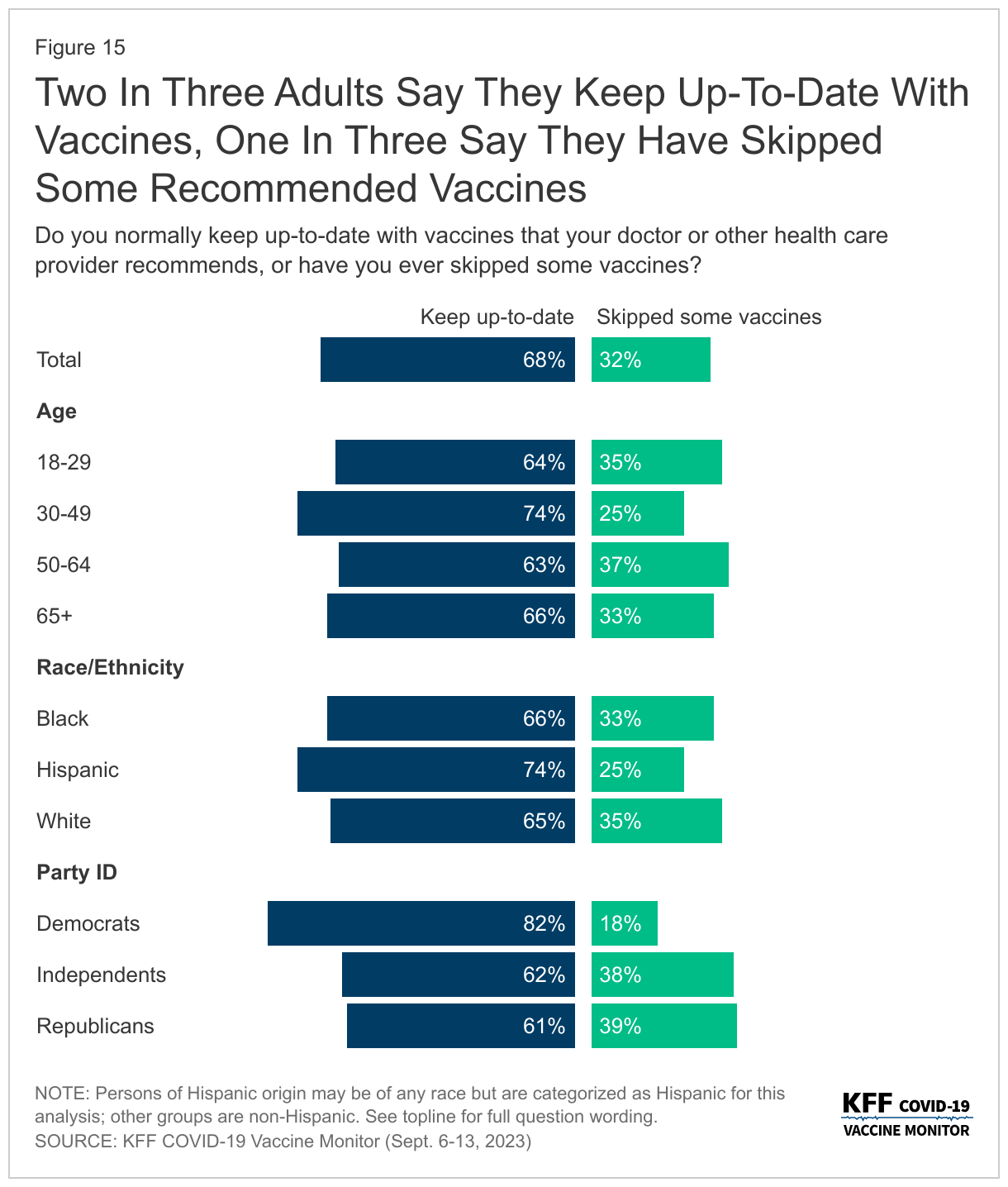
Most adults (68%) also say they normally keep up-to-date with the vaccines that are recommended by their own doctor, including 82% of Democrats and 61% of Republicans. Large majorities of parents – regardless of partisan identification – say they keep their children up to date on recommended childhood vaccines, with just 10% saying they delayed or skipped some vaccines.
Other poll results include:
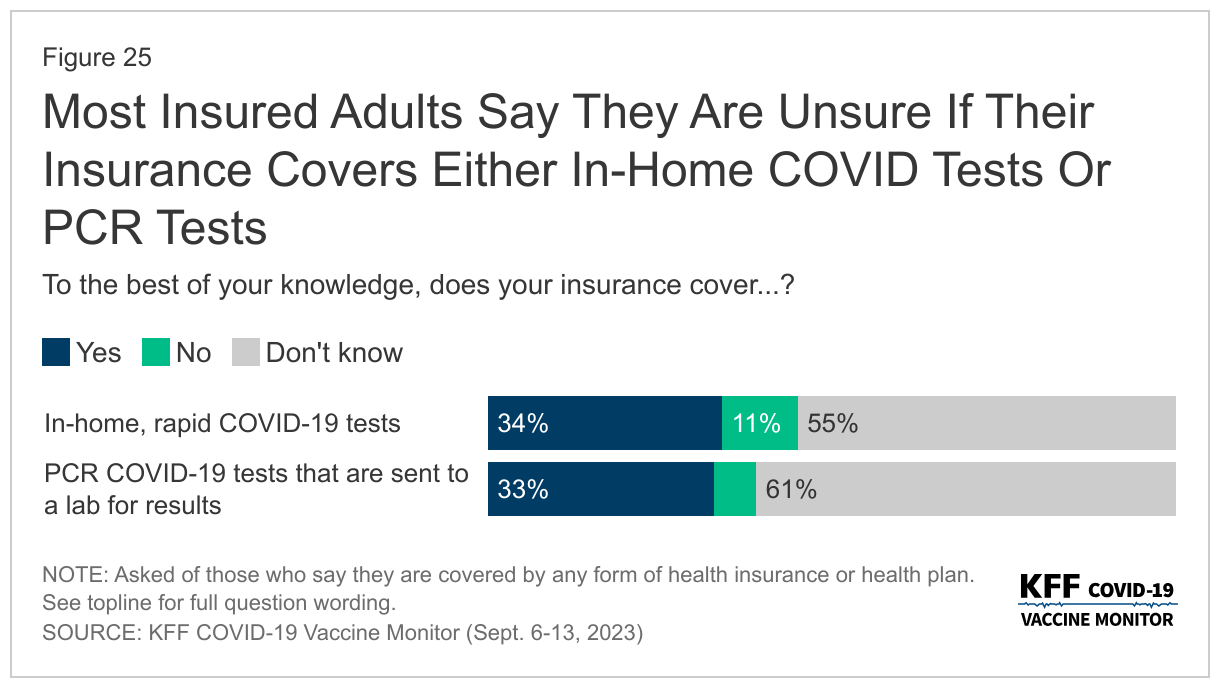
Following the end of the COVID-19 public health emergency in May, most insured people now say they are unsure whether their health insurance covers either in-home, rapid COVID-19 tests (55%) or PCR COVID-19 tests that are sent to a lab for results (61%).
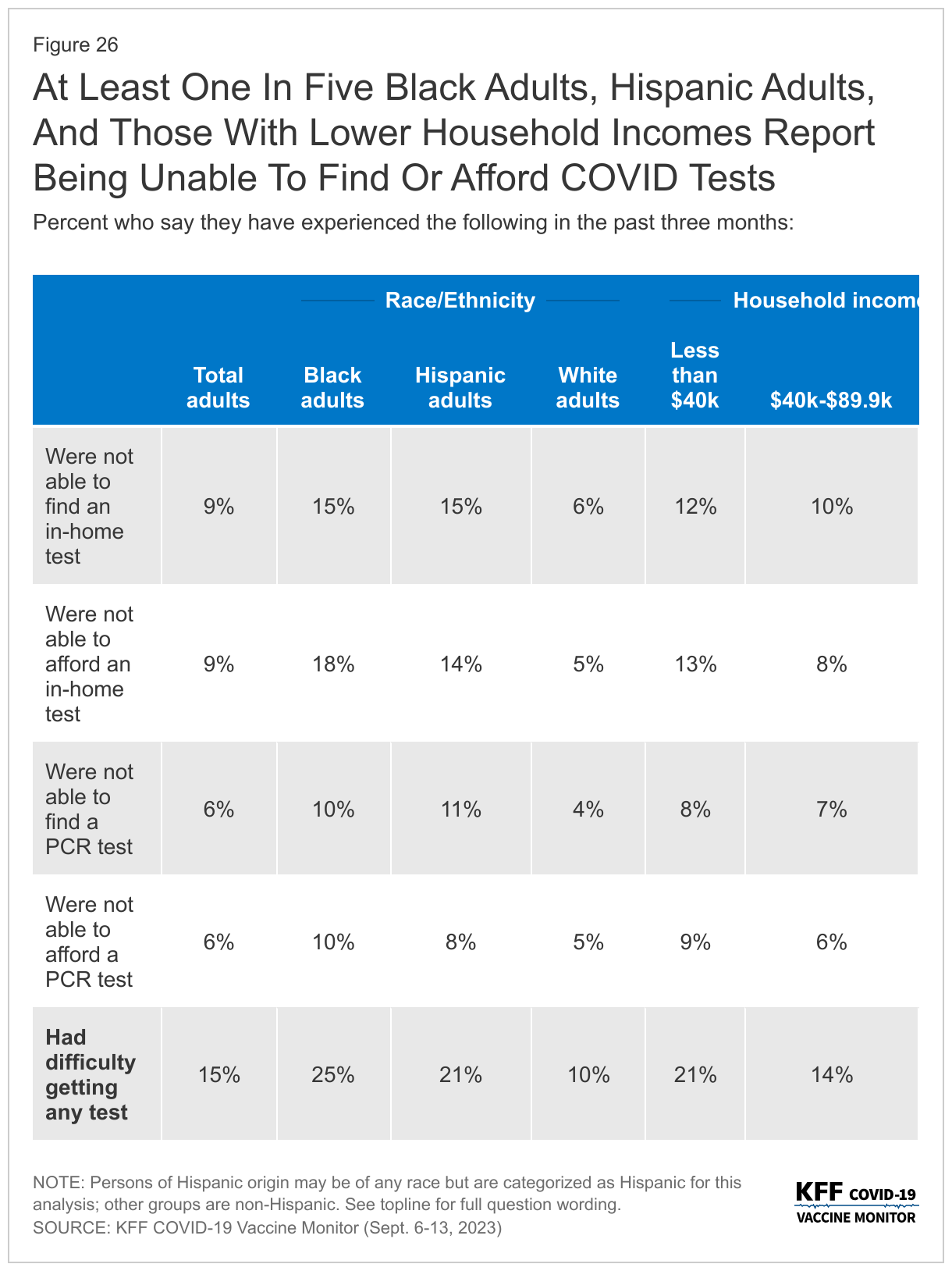
In addition, one in seven (15%) say they’ve wanted to get a COVID-19 test but were not able to find or afford one. Those most likely to report difficulties obtaining a COVID-19 test includes at least one in five Black adults (25%), Hispanic adults (21%), and people with household incomes under $40,000 annually (21%).
Most adults (68%) and parents (55%) – say that healthy children should be required to be vaccinated against measles, mumps, and rubella to attend public school; fewer adults (31%) and parents (43%) say that parents should be able to decide not to vaccinate their children even if that may create health risks for others.
Designed and analyzed by public opinion researchers at KFF, the survey was conducted from September 6-13, 2023, online and by telephone among a nationally representative sample of 1,296 U.S. adults. Interviews were conducted in English and in Spanish. The margin of sampling error is plus or minus four percentage points for the full sample. For results based on other subgroups, the margin of sampling error may be higher.
The fall season has become synonymous with increased concerns over the spread of three respiratory viruses: COVID-19, the flu, and RSV. A “tripledemic,” the scenario in which all three of these viruses peak at the same time, could strain the country’s health care system and impact millions of people with, for some, life-threatening illnesses. Yet, there are vaccines available, including an updated COVID-19 vaccine and a new RSV vaccine, to help prevent people from getting seriously sick. In the latest COVID-19 Vaccine Monitor, a majority of adults (58%), including three-quarters of adults ages 65 and older, say they will get a flu shot this year including some who say they have already received it. In addition, 58% of adults 60 and older say they will either “definitely get” or “probably get” the new RSV vaccine recommended for their age group.
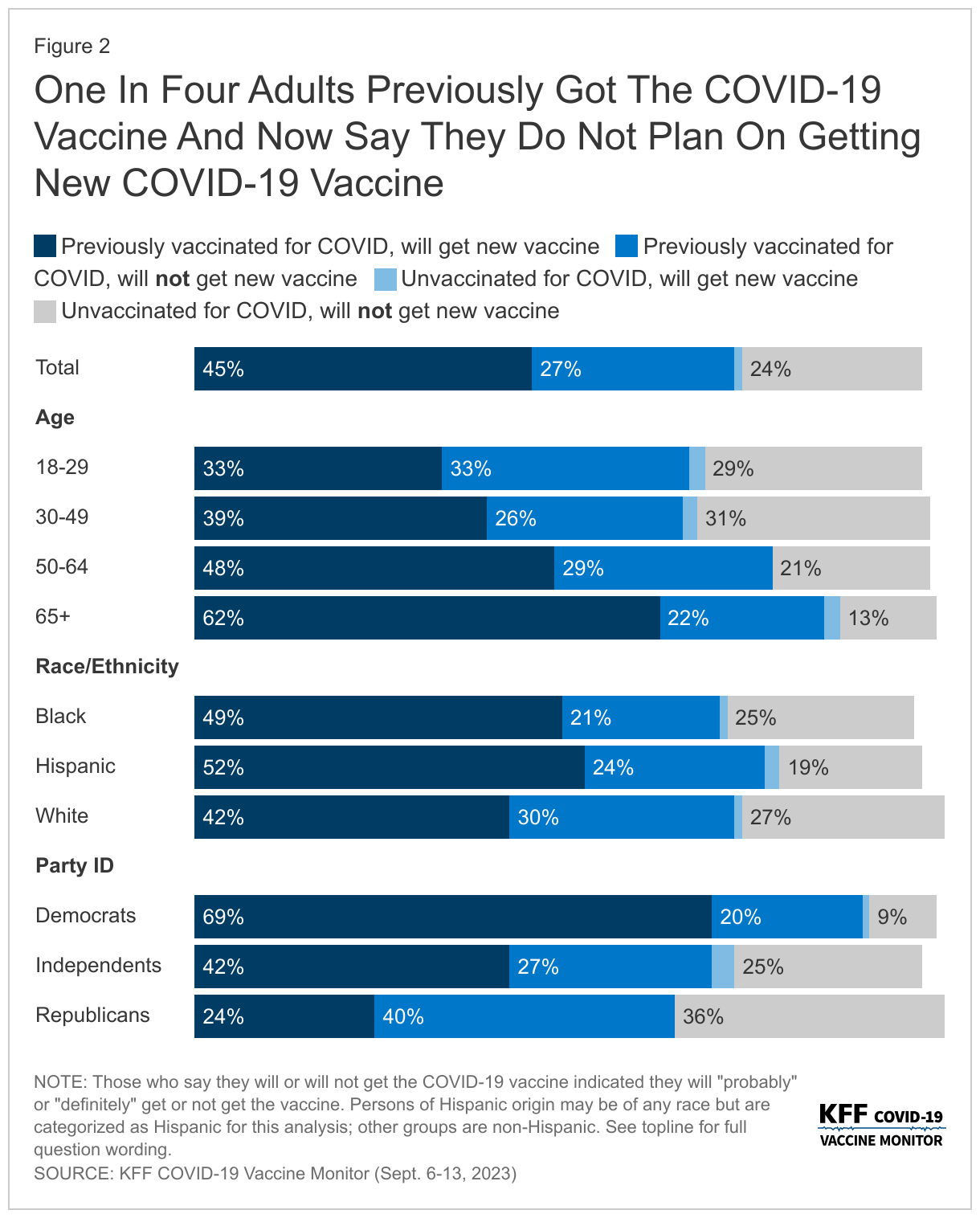
Compared to the flu and RSV vaccines, a somewhat smaller share of adults (47%) say they plan to get the new COVID-19 vaccine, which was recommended by the CDC on September 12th while the poll was in the field. While most (61%) of those who were previously vaccinated for COVID-19 say they will get the new vaccine, almost four in ten (37%) of this group say they “probably” or “definitely” will not get the new vaccine. This means one quarter (27%) of all adults have previously received a COVID-19 vaccine and say they will not get the new vaccine. The vast majority of previously unvaccinated adults say they also will not get the latest COVID-19 vaccine, with just 5% of this group saying they may get the new vaccine. One in four (24%) of all adults have not received any previous COVID-19 vaccine and do not intend to get the newest vaccine available.
Reflecting patterns seen throughout the COVID-19 pandemic, intended uptake is largely divided along party lines. Seven in ten Democrats say they will get the latest COVID-19 vaccine compared to about a quarter of Republicans. Confidence in safety of the new vaccine is also largely partisan. More than eight in ten Democrats (84%) say they are confident in the safety of the COVID-19 vaccine, compared to one in three (36%) Republicans. Overall views of the safety of the COVID-19 vaccine (57%) lag behind the other two vaccines (RSV, 65%; flu, 74%) – largely driven by the views of Republicans who are more confident in the safety of the other two vaccines.
Majorities of groups who are most at risk for getting seriously sick from COVID-19 say they intend to get the latest vaccine available including two-thirds (64%) of adults ages 65 and older and most (56%) of those with a serious health condition. In addition, at least half of Hispanic adults (54%) and Black adults (51%) say they will get the COVID-19 vaccine compared to four in ten (42%) White adults.
Since COVID-19 vaccines first became available for children, uptake has lagged behind that of adults, particularly at younger ages. In the latest survey, most parents say they will not get their child the new COVID-19 vaccine including six in ten parents of teenagers (those between the ages of 12 and 17), and two-thirds of parents of children ages 5 to 11 (64%) and ages 6 months to 4 years old (66%). One in seven (14%) parents of teenagers say their teen was previously vaccinated but they aren’t planning on getting them the most recent vaccine. More than half of parents of children ages 5 and younger say their child has never received a COVID-19 vaccine and they do not plan on getting them the newest COVID-19 vaccine. Similar to adults overall, larger shares of parents say they are confident in the safety of both the flu vaccine (68%) and the RSV vaccine (63%) compared to the COVID-19 vaccine (48%).
Mirroring the partisan differences in views on vaccines, there is a persistent partisan divide on overall views of COVID-19, the current caseload in the U.S., whether they could be sick from COVID, and changes to behavior – including willingness to take a diagnostic test when sick. Democrats are more likely to report changing their behaviors because of recent news of increases in COVID-19. More than half of Democrats (58%) say they’ve recently modified their behavior to be more COVID-conscious compared to 16% of Republicans. Democrats (19%) are also more than twice as likely as both independents (8%) and Republicans (9%) to say that in the past three months they have had symptoms they thought could be COVID-19, and therefore took a COVID-19 diagnostic test. Most Democrats (77%) also say there is a new wave of COVID-19 infections hitting the U.S. now, while half of Republicans (51%) disagree.
Most insured people now say they are unsure whether their health insurance covers either in-home, rapid COVID-19 tests (55%) or PCR COVID-19 tests that are sent to a lab for results (61%). This confusion likely reflects the changing coverage landscape for tests since the public health emergency ended more than three months ago as most people no longer have coverage of in-home tests and will likely face cost-sharing for PCR tests. And while most adults do not report difficulty accessing testing, 15% overall say there was a time in the past three months when they wanted a COVID-19 test and they were not able to find or afford one, rising to more than one in four Black adults and one in five Hispanic adults. HHS announced on September 20th that free in-home tests will soon be available again on a limited basis from the federal government.
COVID-19, Flu, and RSV Vaccine Intentions and Perceived Safety
The September KFF COVID-19 Vaccine Monitor asks the public about their intention to get the flu vaccine and the updated COVID-19 vaccine, both of which are recommended by the CDC for people ages 6 months and older. The poll was in the field when the latest COVID-19 vaccine was recommended by the Centers for Disease Control and Prevention (CDC) but largely before it was available to the public. The CDC issued recommendations for everyone 6 months and older to get the annual flu vaccination on June 29th. Older adults, those 60 and older, were also asked questions about other vaccines recommended for their age group including the pneumonia vaccine, the shingles vaccine, and the new RSV vaccine which the CDC also recently recommended for this group.
Intentions To Get New COVID-19 Vaccine Lags Behind Initial Vaccine Uptake Among Adults And Children
Half of adults say they either will “definitely get” (23%) or “probably get” (23%) the new vaccine for COVID-19 that was approved by the CDC on September 12th. One in three adults say they will “definitely not get” the new COVID-19 vaccine, and another 19% say they will “probably not get” the vaccine. Reflecting patterns in COVID-19 vaccine uptake throughout the pandemic, the share who say they will get the new COVID-19 vaccine is largest among adults age 65 and older (64%) and Democrats (70%). In addition, at least half of Hispanic adults (54%) and Black adults (51%) say they will get the COVID-19 vaccine compared to four in ten (42%) White adults.
Larger shares of those with a serious health condition (56%), such as high blood pressure, heart disease, lunch disease, cancer, or diabetes, say they will get the new COVID-19 vaccine compared to 42% of those who do not have a chronic condition. Similar to previous trends, almost half (44%) of those with insurance who are under the age of 65 report that they will get the new COVID-19 vaccine compared to three in ten (30%) of those who are uninsured and under 65 years old.
While most (61%) of those who were previously vaccinated for COVID-19 say they will get the new vaccine, almost four in ten (37%) of this group say they probably or definitely won’t get it. Very few (5%) of those who have not received a previous COVID-19 vaccine dose say they will get the new vaccine.
Intentions to get the initial booster, the bivalent booster, and now the latest vaccine available measured in the KFF COVID-19 Vaccine Monitor have not matched initial vaccine uptake. And while a smaller share of adults say they intend to get the latest vaccine compared to initial vaccine rollout (in which more than three in four adults received at least one dose), intentions to get this vaccine outpaces both intentions to get previous boosters and actual vaccine uptake measured by the CDC. Overall, about half of adults (45%) have received a COVID-19 vaccine and say they plan to get the latest vaccine, but about a quarter of adults (27%) say they have previously received a COVID-19 vaccine and now say they will not be getting the new vaccine available.
COVID-19 vACCINE Intent Among Parents Of Teenagers anD Kids
The KFF COVID-19 Vaccine Monitor has been tracking vaccine uptake for children across various age groups since the vaccines became available. The surveys have consistently shown COVID-19 vaccine uptake has been higher among older kids with about half of parents of teenagers saying their child has received at least one dose of the COVID-19 vaccine, compared to about a quarter of parents of kids between 6 months and 4 years old. Parents have cited safety concerns, lack of testing or research, and side effects as their main reasons for not getting the youngest cohort vaccinated.
The new version of the COVID-19 vaccine is recommended for all children ages 6 months and older and unlike previous COVID-19 vaccines, most parents say they will either “probably not get” or “definitely not get” their child, regardless of age, vaccinated. Six in ten parents of teenagers (those between the ages of 12 and 17) say they will not get their child the new COVID-19 vaccine as do two-thirds of parents of children ages 5 to 11 (64%) and ages 6 months to 4 years old (66%).
About a third of parents of teenagers say their child was previously vaccinated and they will get their child vaccinated with the most recent vaccine available, while a notable share (14%) say their teenager was previously vaccinated but they aren’t planning on getting them the most recent vaccine. More than half of parents of children younger than five years old say their child has never received a COVID-19 vaccine and they do not plan on getting them the newest COVID-19 vaccine.
Majority Of Adults Say They Will Get Annual Flu Shot And Most Older Adults Plan To Get RSV Vaccine
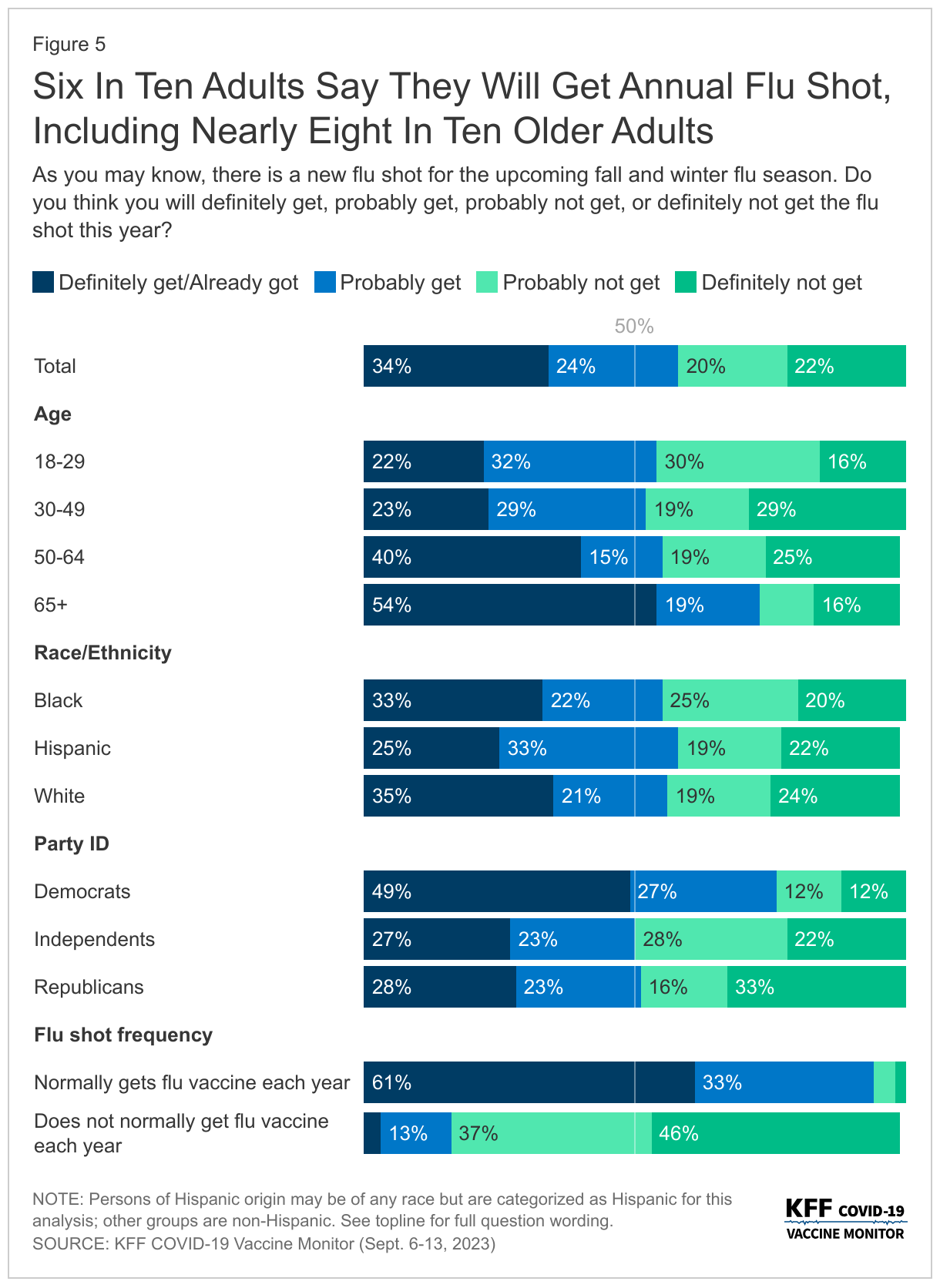
Six in ten adults (58%) say they will get a flu shot this year including 2% who say they have already gotten their flu shot. This includes nearly eight in ten adults ages 65 and older, as well as three in four Democrats. Those who report normally getting a flu shot (53% of all adults) are nearly six times as likely as those who do not normally get a flu shot to say they will get it this year. About half of Republicans (51%) and independents (49%) say they will get their annual flu shot or have already gotten it.
While public health officials say getting the flu vaccine and the COVID-19 vaccine at the same time is safe and initially thought to be preferred in order to reduce burden, only about half (53%) of those who intend to get both say they plan to get it at the same time.
Most Older Adults Say They Will Get RSV Vaccine
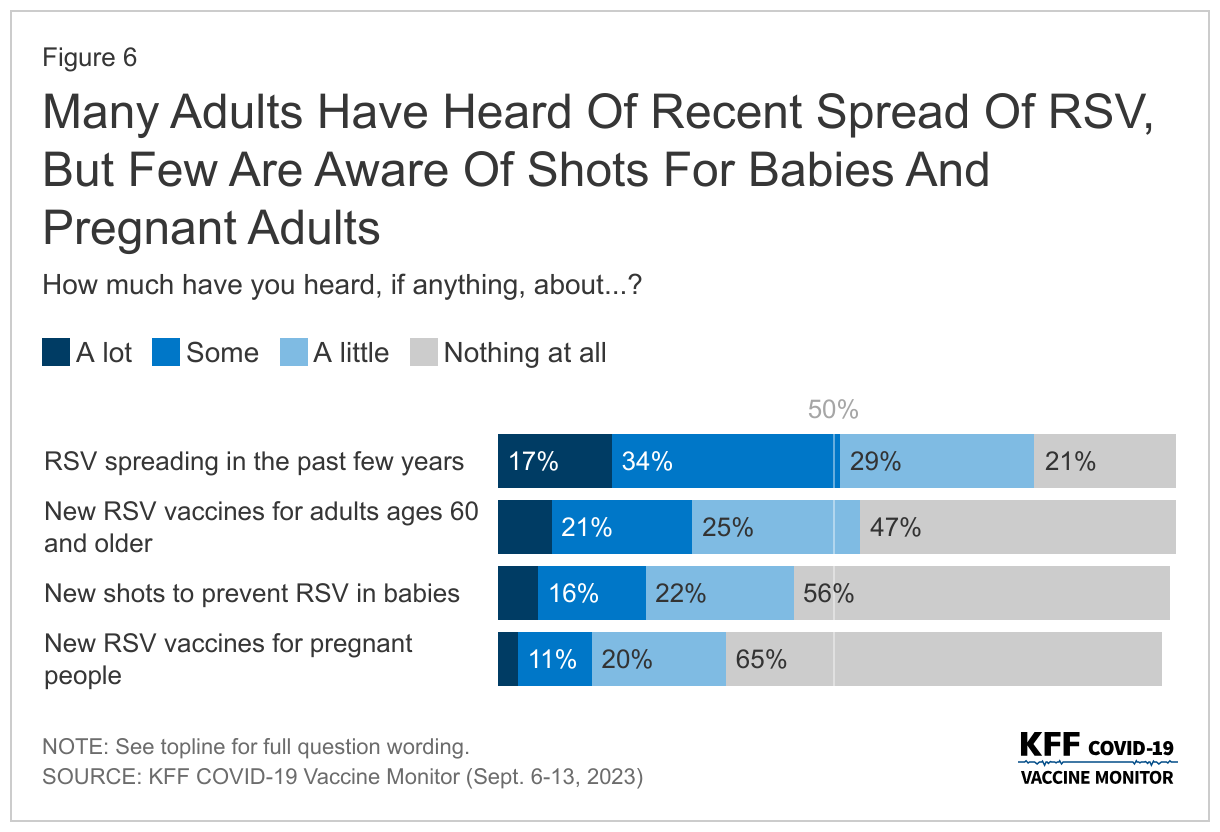
Half of people say they have heard either “a lot” or “some” about RSV spreading in the past few years, but considerably smaller shares have heard about the vaccines aimed at preventing at-risk groups from getting seriously sick from the respiratory virus. Three in ten adults (28%) say they have heard at least some about the new RSV vaccine for adults 60 and older, one in five (22%) say they have heard about the new shots to prevent RSV in babies, and one in seven (14%) have heard about the new recommended RSV vaccines for pregnant people.
Awareness of both the vaccines for adults ages 60 and older, and the new shots to prevent RSV in babies is higher among groups that are at risk. Four in ten adults ages 60 and older say they have heard about the new RSV vaccines for their age group and one in three parents of children less than two years old say they have heard about the shots for this age group.
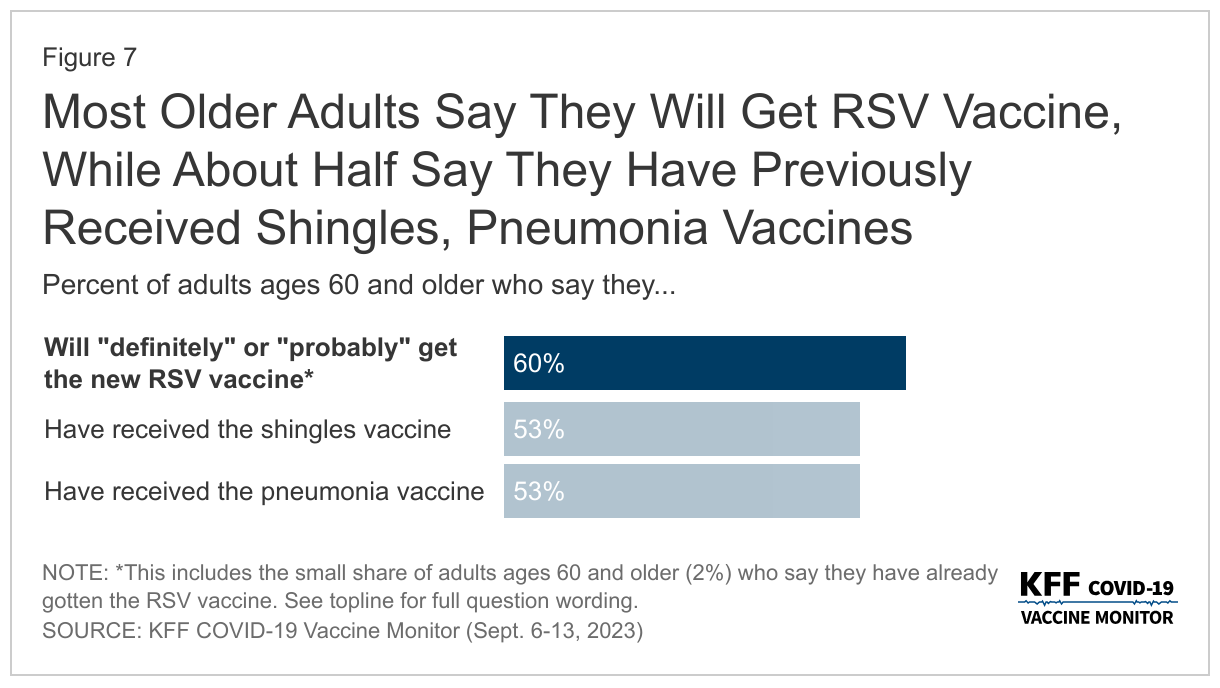
The share of adults ages 60 and older who say they will either “definitely get” or “probably get” the new RSV vaccine matches vaccine uptake for other key vaccines for this age group, notably the shingles vaccine and the pneumonia vaccine. More than half of older adults say they have received the pneumonia vaccine (53%), the shingles vaccine (53%), and plan to get the new RSV vaccine (58%). An additional 2% of older adults say they have already gotten the RSV vaccine.
As Virus Season Approaches, Most Are Confident In Vaccine Safety
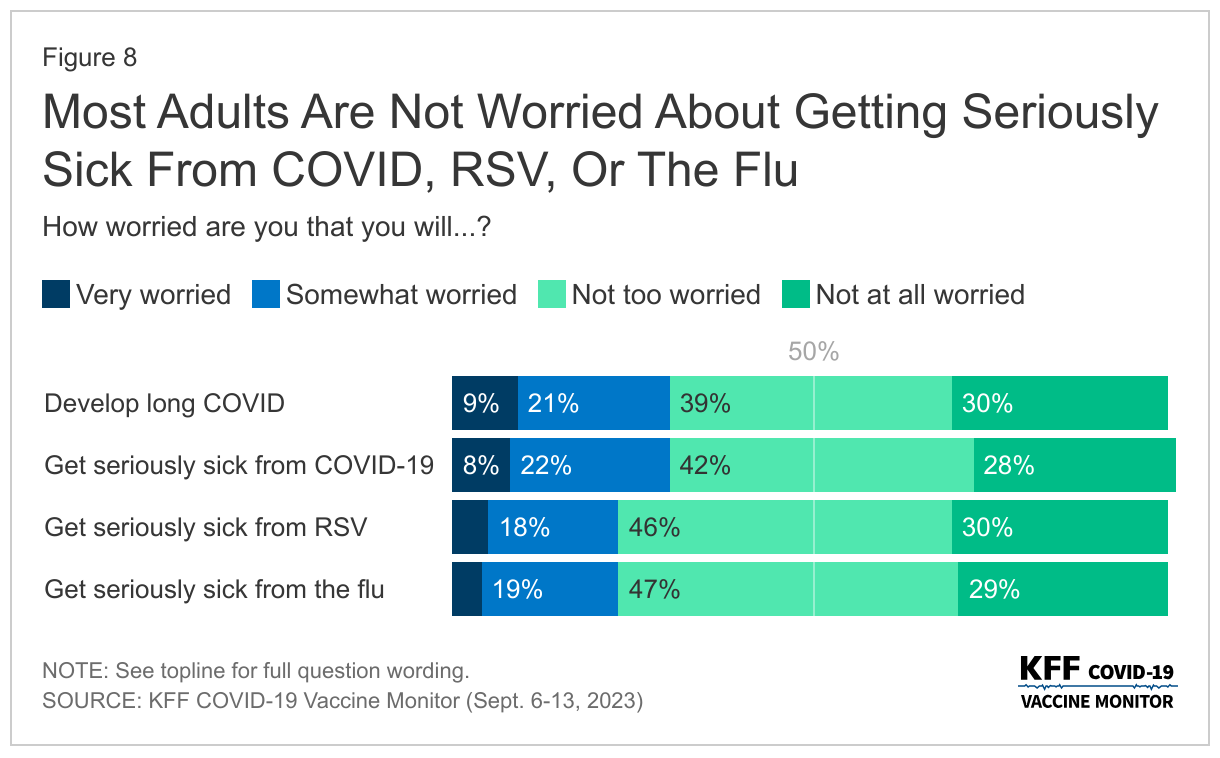
Public health officials have raised concerns about a possible “tripledemic” with COVID-19, the respiratory illness RSV (respiratory syncytial virus), and the flu all hitting peaks this fall as people are more likely to be indoors and gathering together. About three in ten adults say they are worried about developing long COVID (31%) or getting seriously sick from COVID-19 (30%). About one in four are worried about getting seriously sick from the flu (23%) or from RSV (23%).
Those with a serious health condition (such as high blood pressure, heart disease, lung disease, cancer, or diabetes) are more likely than those without a serious health condition to be worried about the impending virus season. About four in ten of those with a chronic health condition say they are worried about getting seriously sick from COVID-19 (38%) or developing long COVID (38%), and three in ten are worried about getting seriously sick from RSV (29%) or the flu (28%).
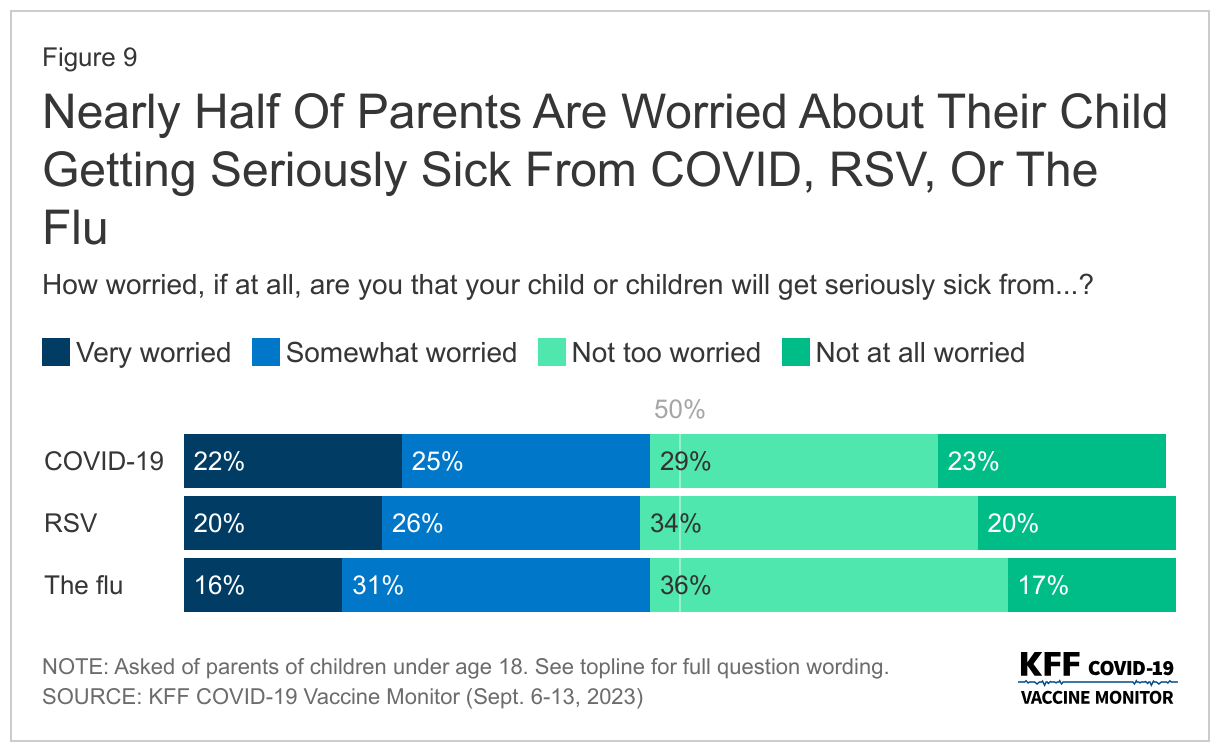
Nearly half of parents say they are worried that their child or children will get seriously sick from COVID-19 (48%), the flu (47%), or RSV (46%).
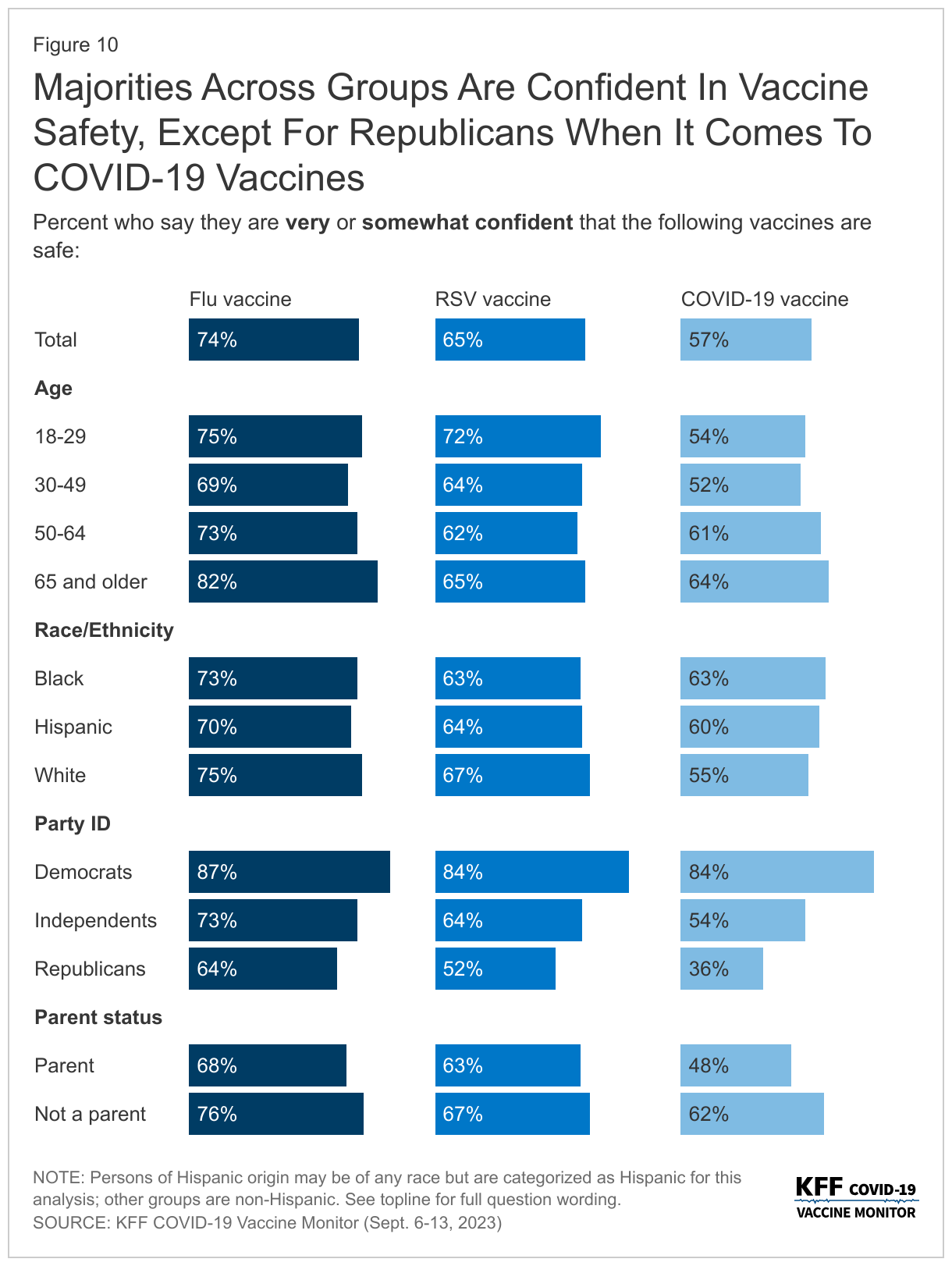
Amidst news of the impending virus season, most adults think that the vaccines developed to combat these viruses are safe. While a majority of adults are confident in the safety of the COVID-19 vaccine (57%), it lags slightly behind confidence in the RSV vaccine (65%) and the flu vaccine (74%).
Majorities across age groups, racial and ethnic identities, and partisanship are confident in the safety of all three vaccines – with one notable exception. About one in three Republicans say they are “very confident” or “somewhat confident” in the safety of the COVID-19 vaccine (36%), compared to more than half of Republicans who are confident the RSV vaccine is safe (52%) and nearly two-thirds who are confident in the safety of the flu vaccine (64%). These views reflect the partisan gap in COVID-19 vaccine confidence throughout the more than two years of COVID-19 vaccine rollout.
Similarly to adults overall, parents are more confident in the safety of both the flu vaccine (68%) and the RSV vaccine (63%), than the COVID-19 vaccine (48%).
Trust In Vaccine Information
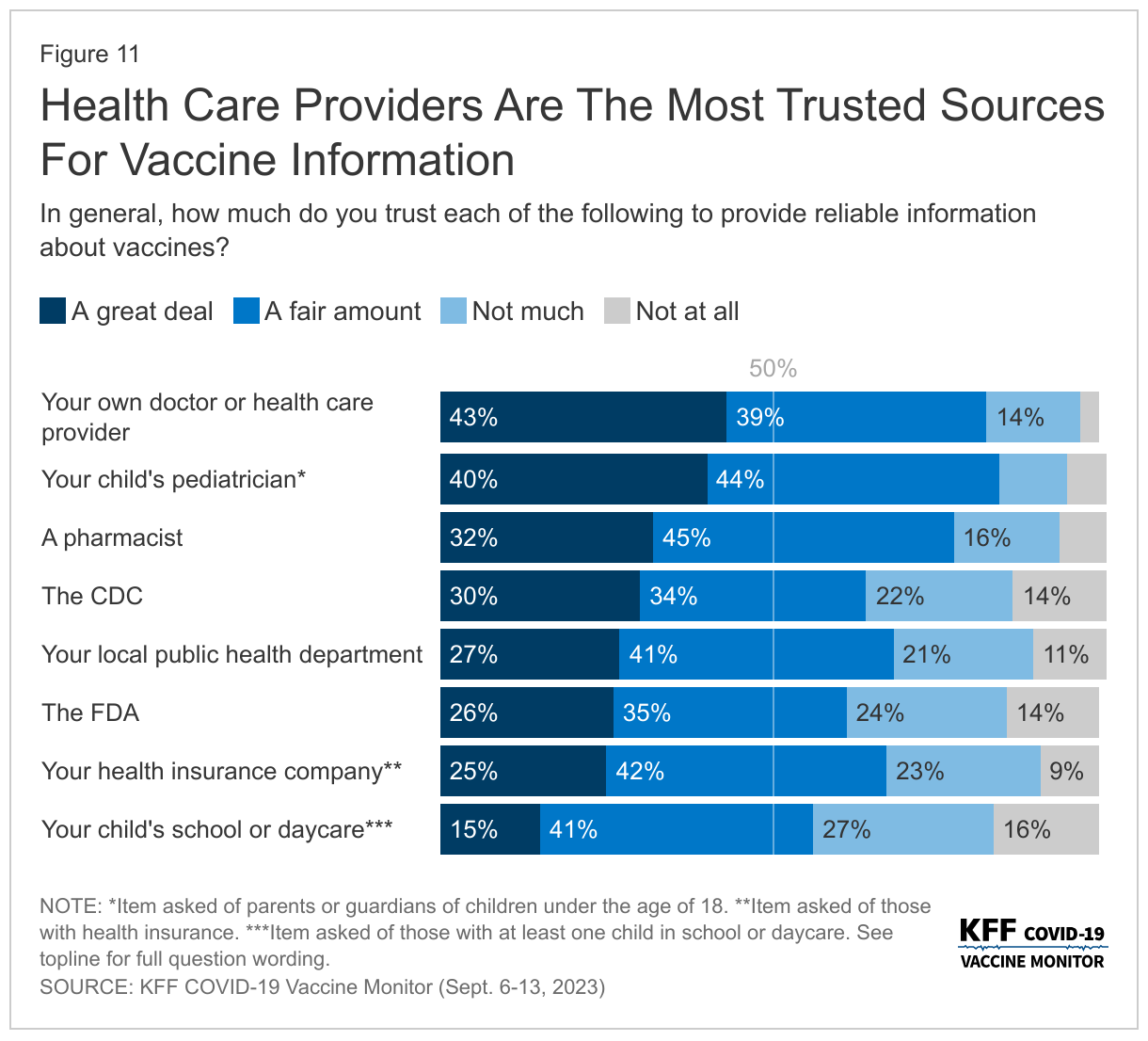
As the CDC Director Mandy Cohen continues her efforts to combat the lingering vaccine skepticism from the COVID-19 pandemic, the public continues to rank their own doctors as the most trusted source of information about vaccines. More than eight in ten adults (82%) say they trust their own doctor or health care provider at least a fair amount when it comes to providing reliable information about vaccines. A similar share of parents (84%) has the same level of trust in their child’s pediatrician. About three-quarters of adults (77%) say they trust pharmacists to provide reliable information. A smaller share, but still a majority, say they trust public health government agencies like their own local public health department (68%), the Centers for Disease Control and Prevention (CDC) (63%), or the U.S. Food and Drug Administration (FDA) (61%). This is similar to the share of insured adults (68%) who say they trust their health insurance company. Schools and daycares rank below other groups asked about with slightly more than half (56%) of parents with children attending school or daycare saying they trust them to provide reliable information about vaccines.
The ranking of trusted sources on reliable information about vaccines is similar to the sources the public trusts specifically on COVID-19 vaccines measured last year, and partisan differences are still very apparent. While large majorities across partisans say they trust their own doctor or child’s pediatrician, government sources of information like the CDC, local public health departments, and the FDA fare much worse among Republicans. About four in ten Republicans say they trust the FDA (42%) or the CDC (40%) to provide reliable information about vaccines, and about half of Republicans (51%) say the same about their local public health departments. Large majorities of Democrats and more than half of independents say they trust each of these organizations at least a fair amount.
Understanding How And Why To Get Vaccines
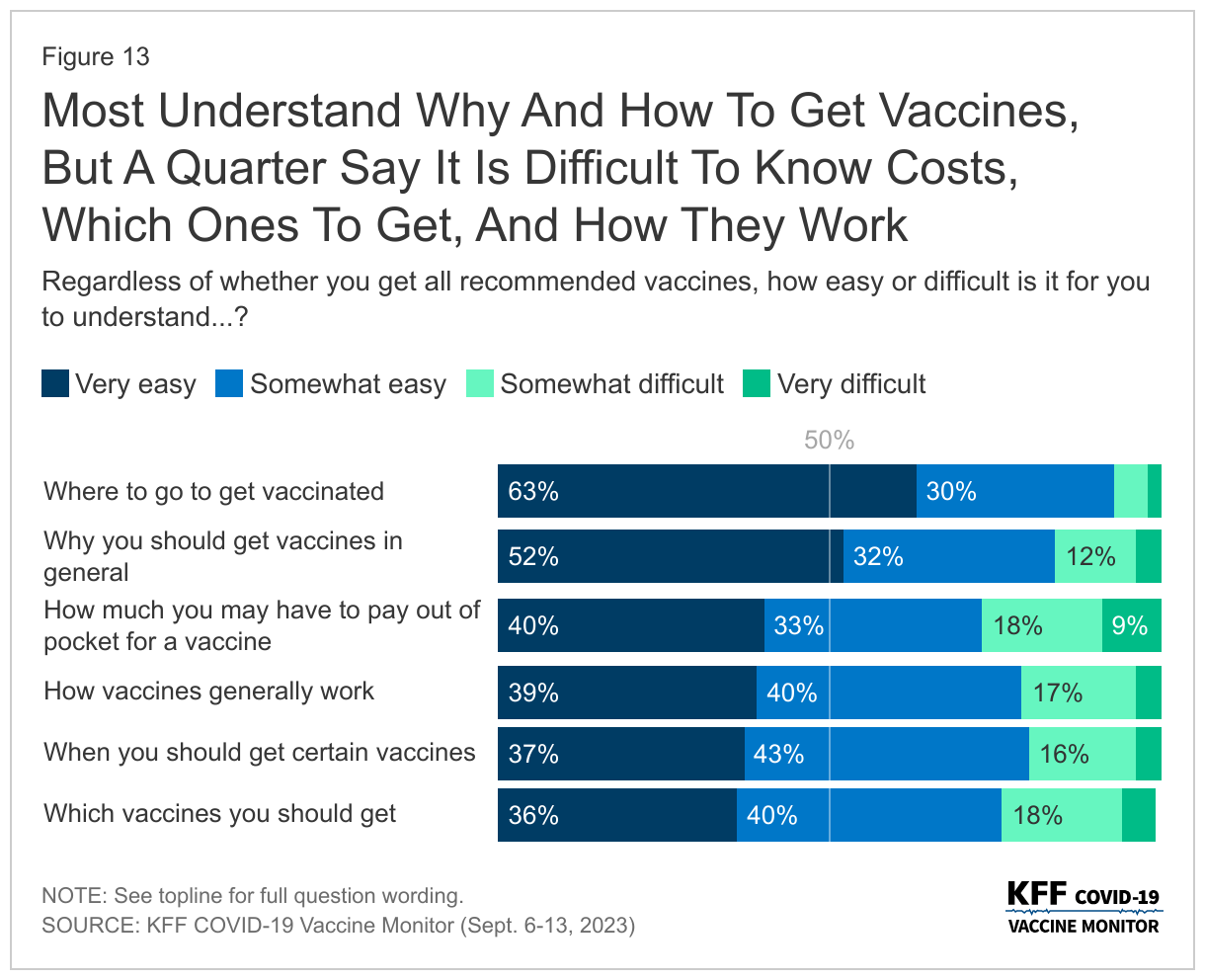
Nearly all adults (93%) say it is easy for them to understand where to go to get vaccinated, including six in ten (63%) who say it is “very easy.” At least three-quarters of adults also say it is easy for them to understand why they should get vaccines (84%), when they should get them (79%), how vaccines work (78%), which vaccines they should get (77%), and how much they may have to pay for a vaccine (63%).
While most adults say it is easy for them to understand the reasoning behind vaccines and the logistics of how to get them, at least one in five of adults still say some of these aspects are difficult to understand. This includes understanding which vaccines they should get (23%), how vaccines generally work (22%), or understanding when they need to get certain vaccines (20%). More than one in four adults say it is difficult to know how much they may have to pay out-of-pocket (27%), even as most people with health insurance will not have to pay any out-of-pocket costs for recommended vaccines.
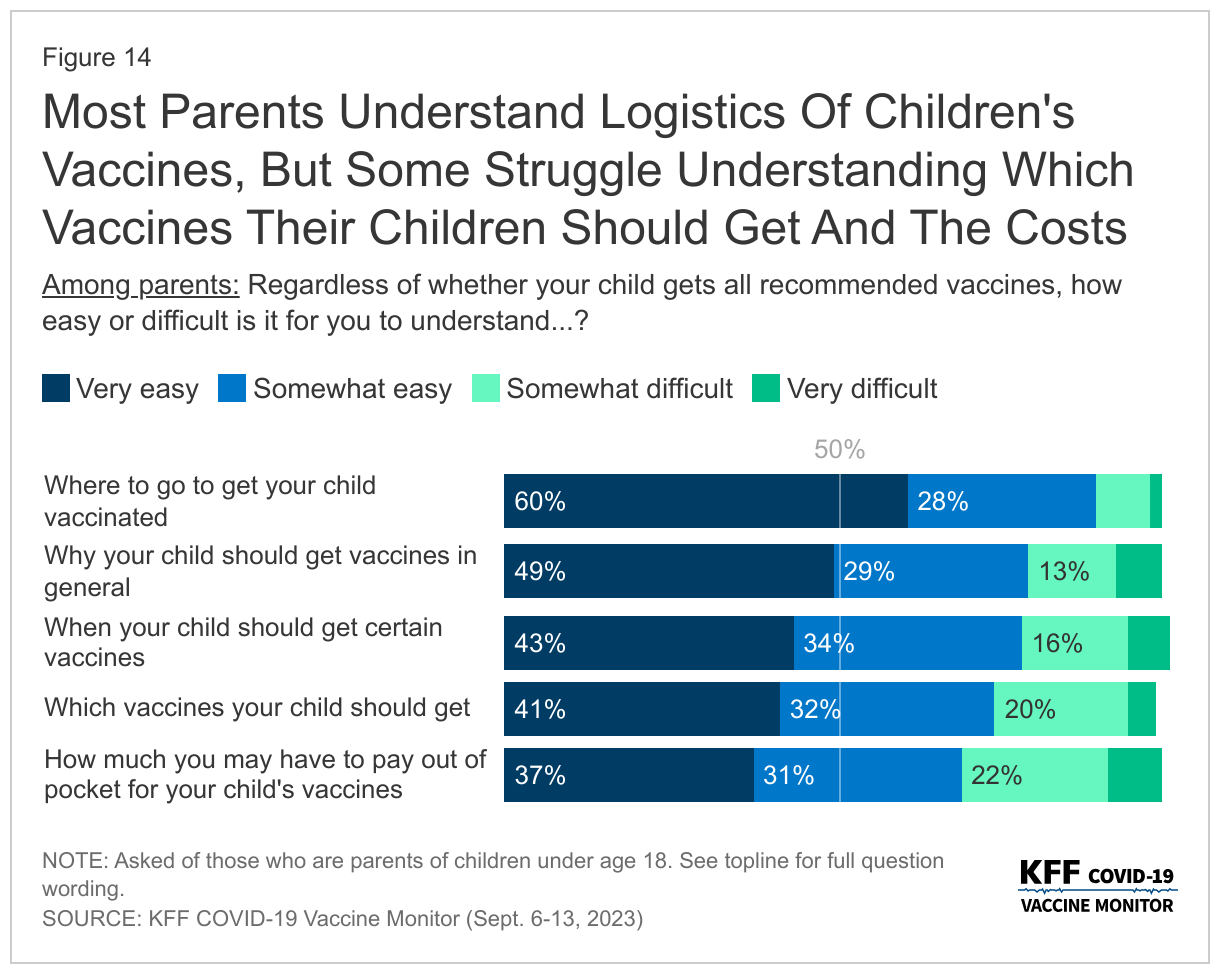
Similarly, most parents report that it is easy to understand the logistics of their vaccinations, such as when and where to get the shots and why their child should get vaccinated. Nearly nine in ten (88%) parents say it is easy to know where to go to get their children vaccinated and about three-fourths of parents say the same about why their children should get vaccines in general (78%), when their child should get certain vaccines (77%), or which vaccines their child should get (73%). Two-thirds (68%) say it is easy for them to understand how much they have to pay out-of-pocket for their child’s vaccines. Most insurance coverages require no out-of-pocket costs for recommended vaccines for children.
Most adults say they get vaccines recommended by Their doctors
With health care providers as the most trusted sources of information about vaccines, most adults (68%) say they normally keep up-to-date with the vaccines that their health care provider recommends for them, while one-third (32%) say they have skipped some recommended vaccines. The share who say they have skipped some recommended vaccines is lowest among Democrats with one in five (18%) saying they have skipped some vaccines, compared to four in ten independents (38%) and Republicans (39%). At least one in three Black adults (33%) and White adults (35%) say they have skipped some vaccines, as have one in four Hispanic adults.
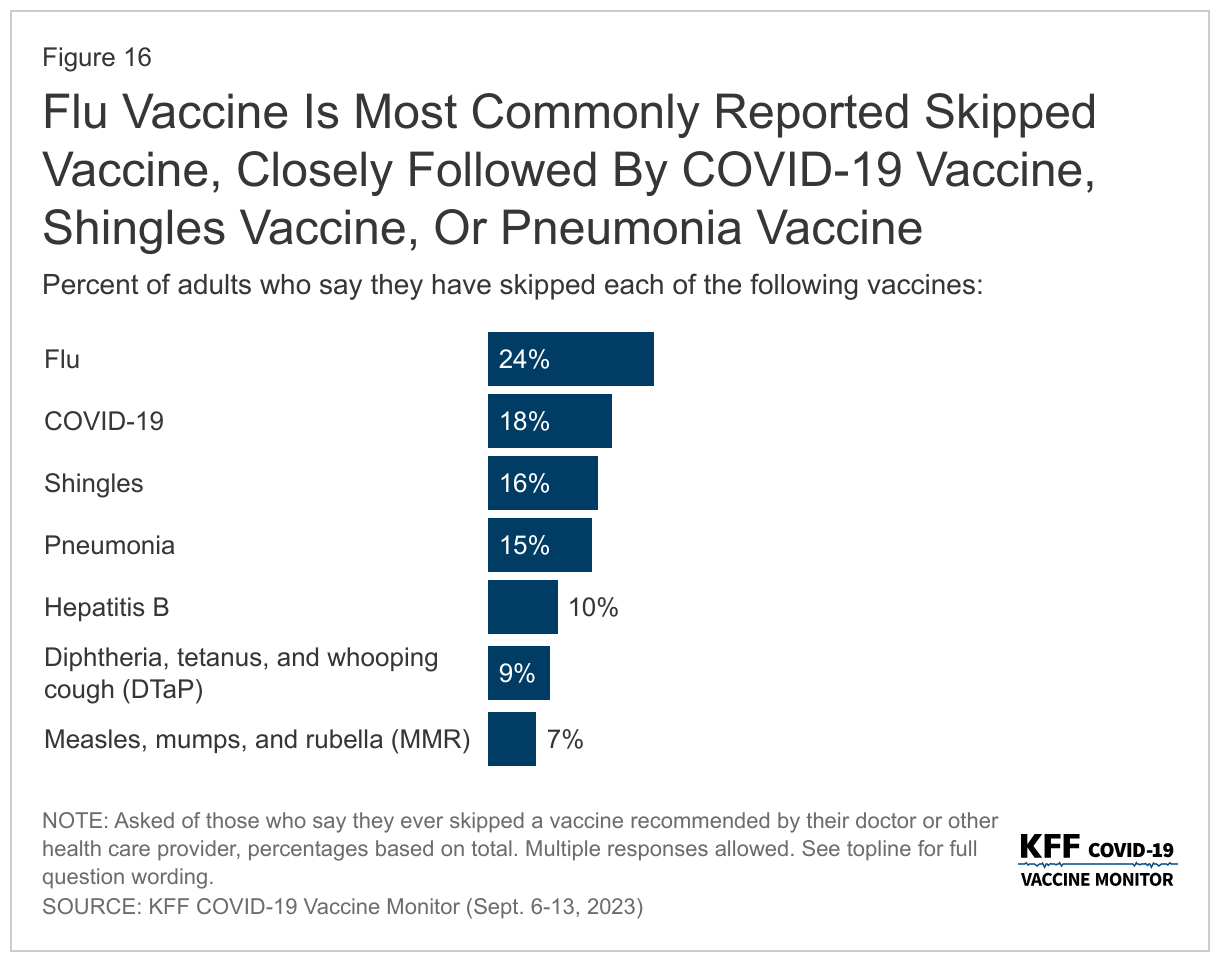
The flu vaccine is the most commonly reported skipped vaccine with one in four adults overall saying they have ever skipped a flu vaccine. About one in six adults say they have skipped a COVID-19 vaccine (18%), the shingles vaccine (16%), or the pneumonia vaccine (15%) when it was recommended by their provider. Previously, both the pneumonia and shingles vaccines were generally recommended for older adults and only recently has the shingles vaccine recommendations expanded to include some adults with certain ongoing health needs, and the pneumonia vaccine is now recommended for children as well as adults 65 and older. The flu vaccine and the COVID-19 vaccine are recommended for everyone age 6 months and older.
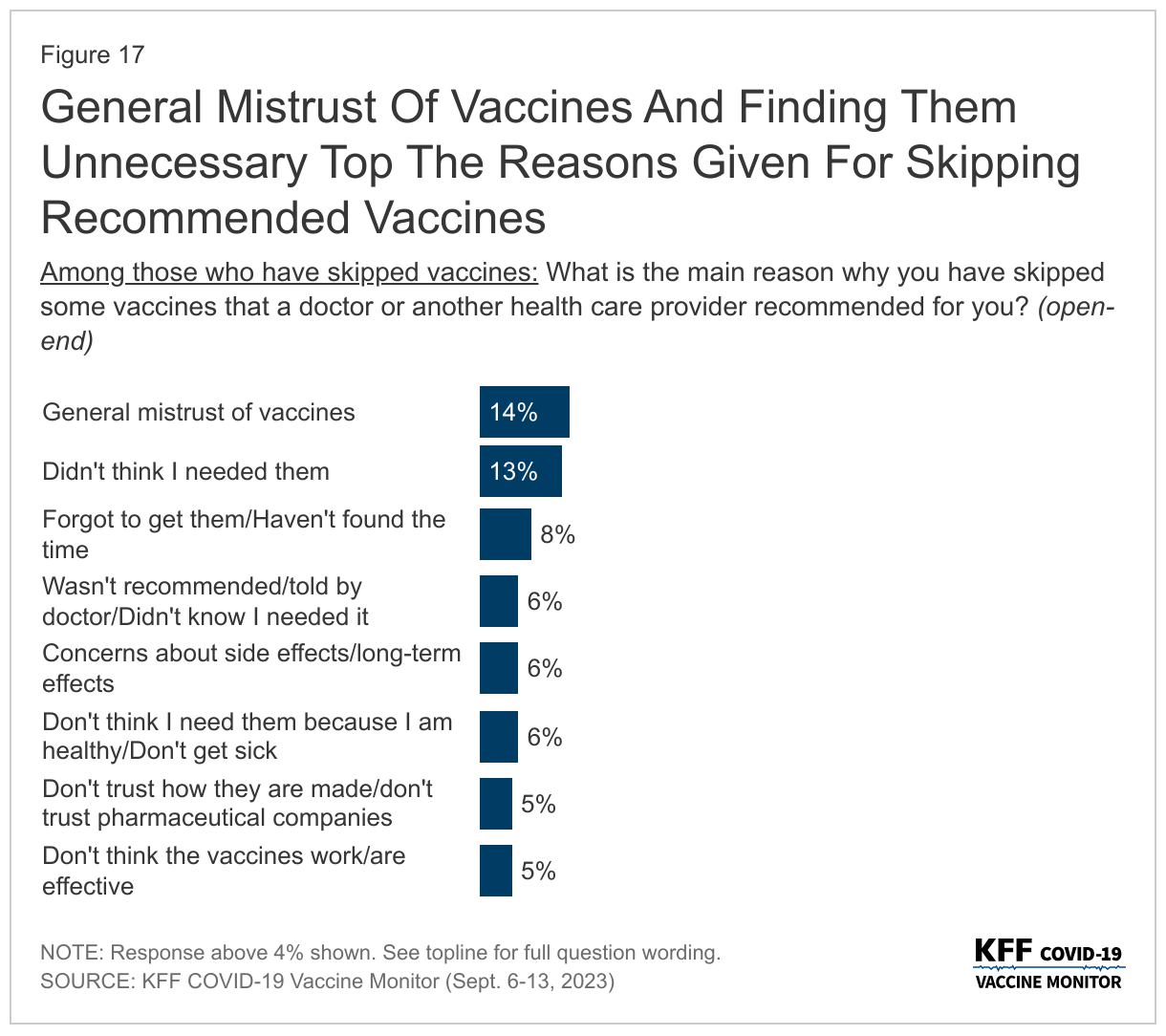
When asked the main reasons for skipping some recommended vaccines, the most commonly provided responses focus on general mistrust of vaccines (14%), or people not thinking they needed them (13%). Another one in ten offer responses focused on not finding the time or forgetting they needed to get them (8%). Other commonly reported responses include a doctor not recommending them or they not knowing they needed them (6%), concerns about side effects or long-term effects (6%), and not thinking they needed them specifically because they are healthy and do not typically get sick (6%). Small but significant shares also offer responses related to mistrust in the vaccines and pharmaceutical companies (5%) or thinking the vaccines do not work or are not effective (5%).
In Their Own Words: Why Have You Skipped Some Recommended Vaccines?
“I have no confidence in the safety or efficacy of vaccines. I believe they are unnecessary for generally healthy individuals.” – 62 year-old White woman, Florida
“Haven’t had a chance to go to local pharmacy to get one.” – 74 year-old Hispanic woman, New Jersey
“I don’t believe I will get sick, I don’t have insurance, visiting the doctors is a hassle, finding affordable or free healthcare assistance takes more time out of my schedule then I’ve had.” – 27 year-old Black individual (“other” gender selected), Georgia
“It’s inconvenient, and I’m completely broke.” – 24 year-old White woman, Missouri
“I trust my body to heal.” – 50 year-old White man, Montana
Most Parents get Recommended vaccines for children
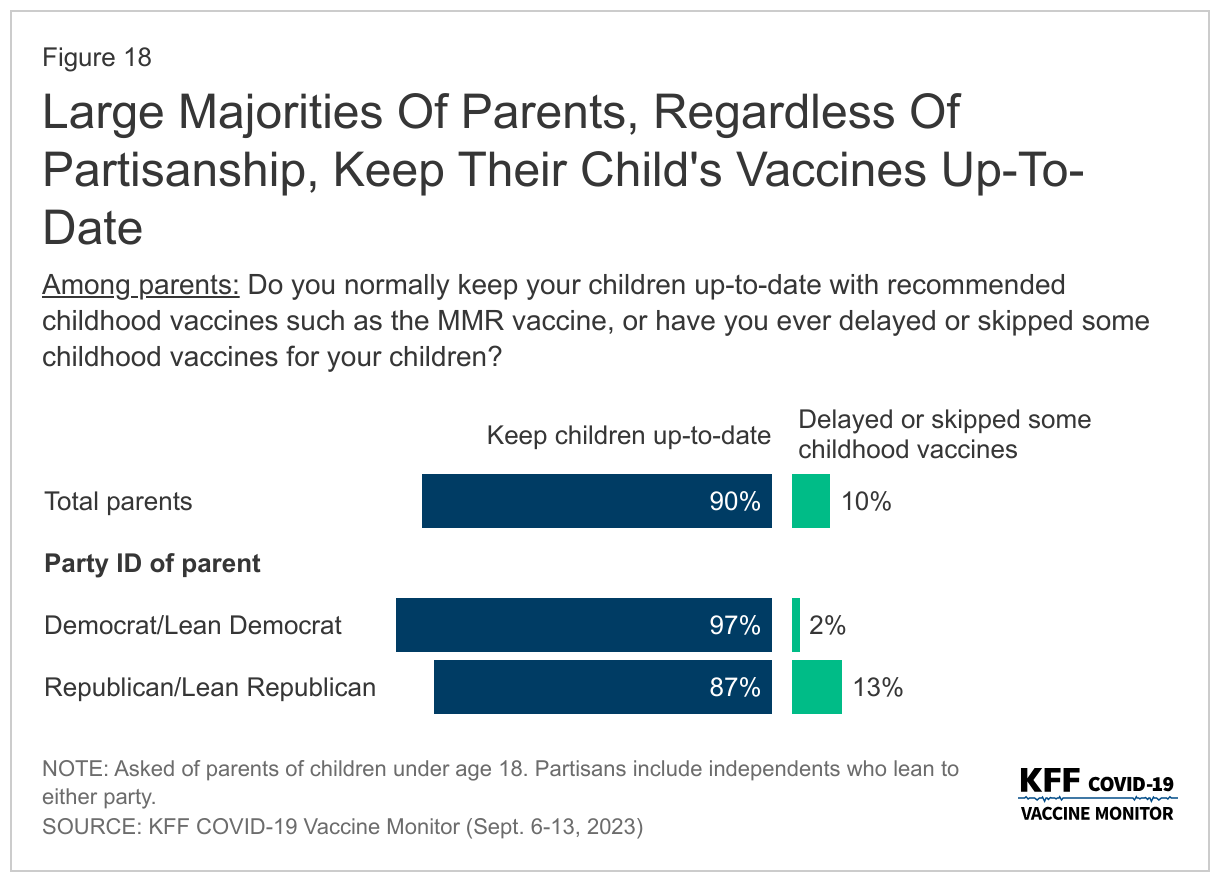
Adherence to recommended vaccines is higher among children than adults overall. Nine in ten parents say they normally keep their child or children up-to-date with recommended childhood vaccines, such as the MMR vaccine, while one in ten say they have delayed or skipped some of their child’s vaccines.
Large majorities of parents, regardless of partisanship, race and ethnicity and income, say they keep their child up-to-date including nearly all Democratic and Democratic-leaning parents (97%) and about nine in ten Republican or Republican-leaning parents.
The share of parents who report keeping their child updated with vaccines is unchanged since July 2021. While confidence in vaccines, such as the measles, mumps, and rubella, or MMR vaccine, remains high, the debate over COVID-19 vaccines and some government mandates has spilled over into attitudes towards requiring vaccines for public schools. Currently, all states and the District of Columbia require children to be vaccinated against certain diseases, including measles, mumps, and rubella, in order to attend public schools, though exemptions are allowed in certain circumstances.
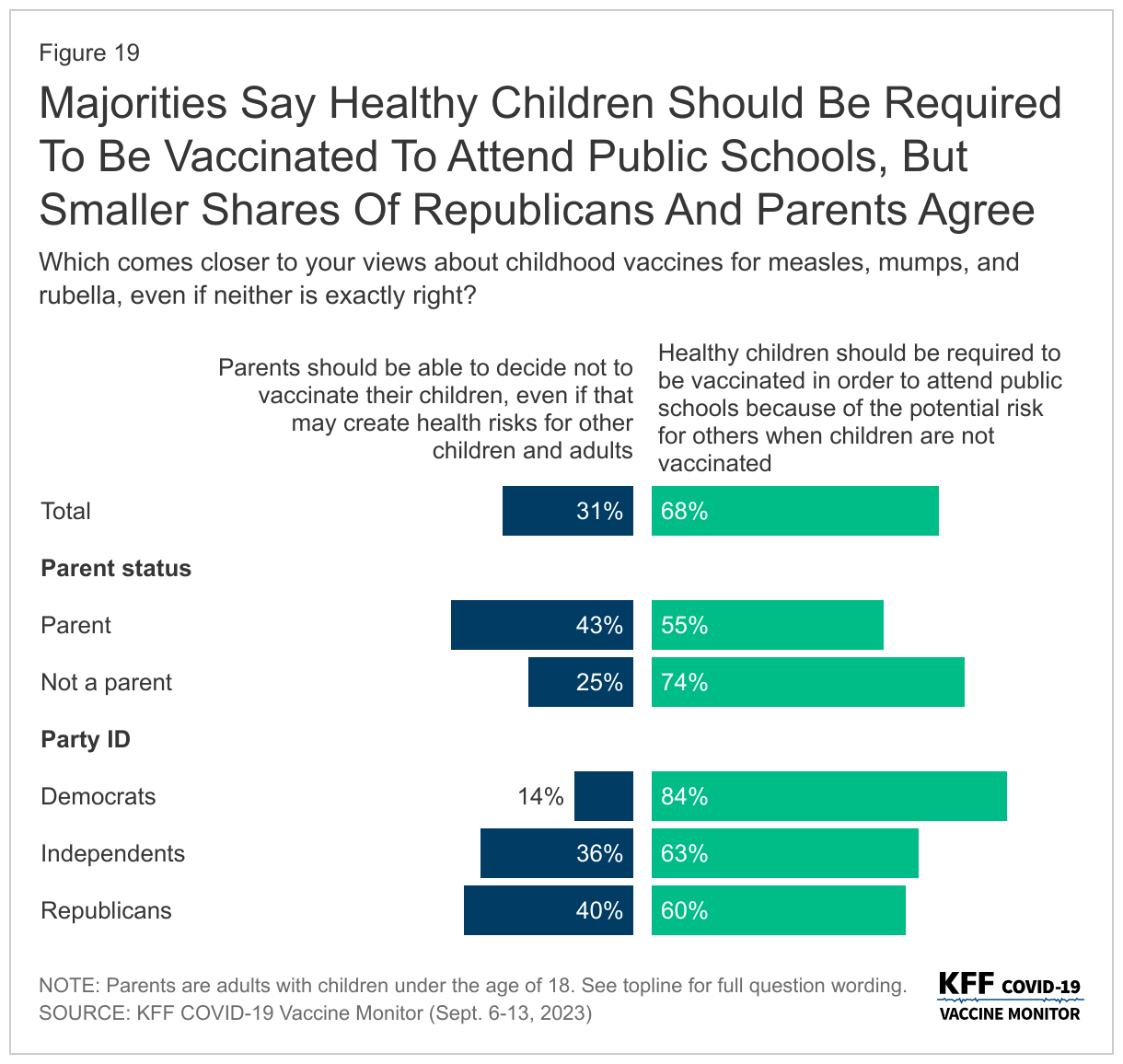
Most adults (68%)1 say healthy children should be required to be vaccinated against MMR in order to attend public schools because of the potential risk for others when children are not vaccinated, compared to three in ten (31%) who say parents should be able to decide not to vaccinate their children, even if that may create risks for other children and adults. Parents are more likely than adults without children under the age of 18 in their home to say parents should be able to decide whether or not to vaccinate their children (43% compared to 25%). A majority of parents (55%) still say vaccines should be required to attend public school.
Among all adults, a larger share but still a minority of Republicans (40%) say parents should be able to decide, while a large majority of Democrats say healthy children should be required to be vaccinated.
Late-Summer COVID-19 Wave and Who Is Still Taking COVID-19 Tests
Although the COVID-19 wave is difficult to track with the end of federal COVID-19 case tracking, earlier this month the CDC reported on an increase in virus-related hospitalization rates and deaths suggesting a late-summer COVID-19 wave.
Six in ten adults believe there is a new wave of COVID-19 infections hitting the U.S now, while nearly four in ten (37%) say there is not a new COVID-19 wave. Larger shares of Democrats and those who have received at least one COVID-19 vaccine say there is a new wave hitting the U.S., with three in four Democrats (77%) and seven in ten (69%) vaccinated adults saying they think there is a COVID-19 wave. Republicans are more equally divided with similar shares saying there is (48%) and is not (51%) a new COVID-19 wave. Most unvaccinated adults (61%) say there is not a new wave of COVID-19 infections hitting the U.S.
Groups that are more likely to say there is a current wave of COVID-19 cases are also more likely to report changing their behaviors because of the news of increases in COVID-19. Overall, four in ten (38%) adults say they have modified their behavior to be more COVID-conscious due to the news of the increases. This includes a quarter of adults who say they are more likely to wear a mask in public (25%) or avoid large gatherings (22%). Another one in six say the news of increases has made them less likely to travel (17%) or dine indoors at restaurants (15%).
Larger shares of Black adults (59%), Democrats (58%), Hispanic adults (52%), and people with a chronic condition (44%) say they have modified their behavior in at least one of these ways because of news of increases of COVID-19. Comparatively, smaller shares of White adults (29%), Republicans (16%), and people without a chronic condition (36%) report doing the same.
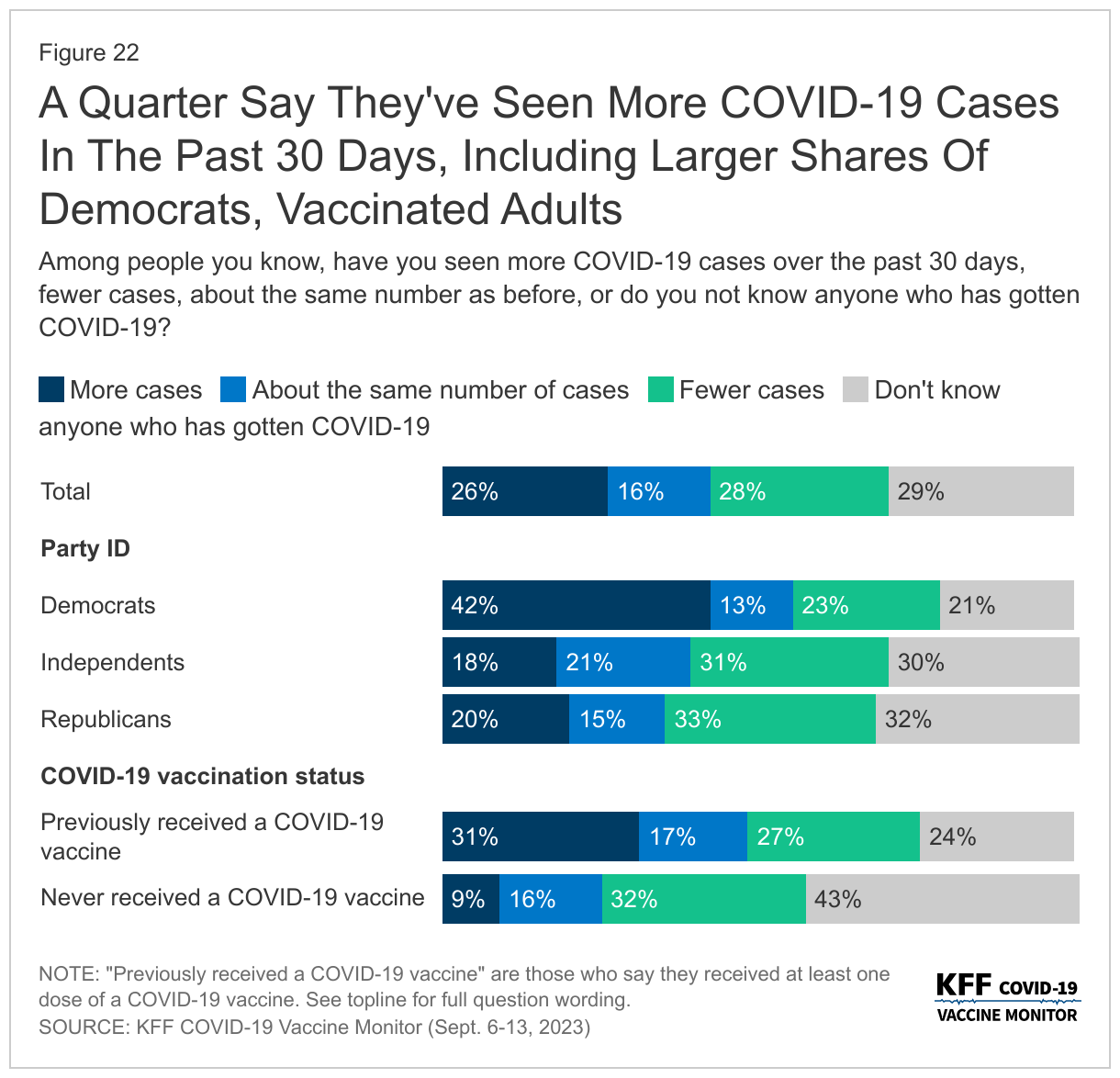
About a quarter (26%) of adults say they have personally seen “more cases” among people they know in the past 30 days. However, a similar share (28%) say they have seen “fewer cases” of COVID-19 in the past 30 days. About one in seven (16%) say they have seen the same number of cases among people they know, while three in ten (29%) say they do not know anyone who has gotten COVID-19.
Democrats (42%) and vaccinated adults (31%) are more likely to say they have seen more COVID-19 cases among people they know in the past 30 days, compared to one in five Republicans and a small share (9%) of those who have never gotten a COVID-19 vaccine.
COVID-19 Testing
Partisanship and vaccine status are also strong drivers in the share of people who say they have taken a COVID-19 test, most likely because they are more likely than their counterparts to identify any possible symptoms of COVID. One in five adults say they have had symptoms in the past three months they thought could be COVID-19, such as a fever, sore throat, runny nose, or a cough. Among those who had such symptoms, over half say they took a test (12% of all adults), and a similar share did not take a test (8% of all adults). Democrats are more than twice as likely as both independents and Republicans to say they felt like they had COVID-19 symptoms and took a test, 19% compared to 8% and 9% respectively.
These partisan and vaccine status differences in perceptions of cases and testing for the virus are consistent with overall views of the pandemic that KFF has been tracking for the past three years. Republicans are more than three times as likely as Democrats to say the news has “generally exaggerated” the seriousness of the coronavirus (71% compared to 18%), while most Democrats say either that the news of the seriousness of COVID-19 has been generally correct (65%) or even “generally underestimated” (18%).
Some Concerns Over Costs Of Diagnostic COVID-19 Tests
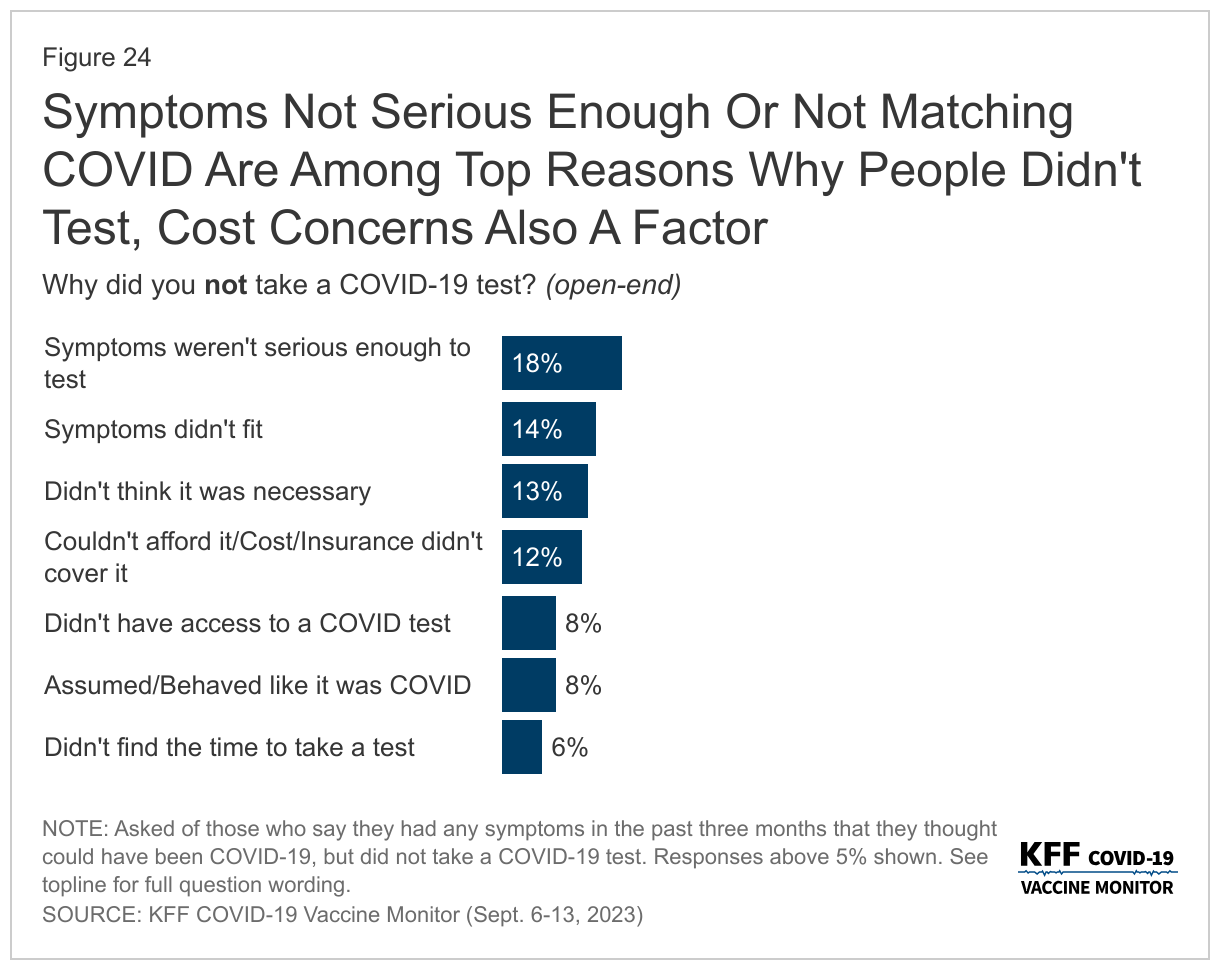
When those who said they were experiencing symptoms and did not take a test were asked why they did not get tested, the most common reasons provided were that they didn’t feel like their symptoms were serious enough to test (18%), they did not think their symptoms fit COVID-19 (14%), they did not think it was necessary for them to test (13%), or they had costs concerns about tests (12%).
These concerns over the costs of COVID-19 tests come more than three months since the end of the public health emergency and national emergency declarations related to the COVID-19 pandemic, which were put in place in early 2020 and provided some free COVID tests for people regardless of health insurance status.
Most insured people now say they are unsure whether their health insurance covers either in-home, rapid COVID-19 tests (55%) or PCR COVID-19 tests that are sent to a lab for results (61%).
While most adults do not report difficulty accessing COVID-19 tests, 15% say there was a time in the past three months when they wanted either an in-home rapid COVID-19 test or a PCR COVID-19 test and they were not able to find or afford one. The shares who report difficulty accessing and affording testing are even higher among Black and Hispanic adults and those with lower incomes. A quarter (25%) of Black adults and two in ten (21%) Hispanic adults say they had difficulty getting a test in the last three months, a larger share than the one in ten (10%) White adults who say the same. Similarly, another two in ten (21%) of those with a household income of less than $40,000 a year had difficulty, compared to smaller shares of those with higher incomes.
Overall, more than one in three adults say they would use a test they already have at home if they wanted to take a COVID-19 test (37%), while one in five say they would purchase one at a pharmacy (22%) or get one at a doctor’s office (19%). One in ten adults (11%) say they are unsure where they could get a COVID-19 test.
Note: The title on Figure 5 was updated on November 29, 2023, to better characterize the data on older adults’ intentions for getting a flu shot.
Methodology
This KFF COVID-19 Vaccine Monitor was designed and analyzed by public opinion researchers at KFF. The survey was conducted September 6-13, 2023, online and by telephone among a nationally representative sample of 1,296 U.S. adults in English (1,210) and in Spanish (86). The sample includes 1,014 adults (n=57 in Spanish) reached through the SSRS Opinion Panel either online or over the phone. The SSRS Opinion Panel is a nationally representative probability-based panel where panel members are recruited randomly in one of two ways: (a) Through invitations mailed to respondents randomly sampled from an Address-Based Sample (ABS) provided by Marketing Systems Groups (MSG) through the U.S. Postal Service’s Computerized Delivery Sequence (CDS); (b) from a dual-frame random digit dial (RDD) sample provided by MSG. For the online panel component, invitations were sent to panel members by email followed by up to three reminder emails. 988 panel members completed the survey online and 26 panel members who do not use the internet were reached by phone.
Another 282 (n=29 in Spanish) interviews were conducted from a random digit dial telephone sample of prepaid cell phone numbers obtained through MSG. Phone numbers used for the prepaid cell phone component were randomly generated from a cell phone sampling frame with disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents. Stratification was based on incidence of the race/ethnicity groups within each frame.
Cases that failed both attention check questions, those with over 30% item non-response, and cases with a length less than one quarter of the mean length by mode were flagged and reviewed. Cases were removed from the data if they failed two or more of these quality checks. Based on this criterion, no cases were removed. Respondents in the phone samples received a $15 incentive via a check received by mail, and web respondents received a $5 electronic gift card incentive (some harder-to-reach groups received a $10 electronic gift card).
The combined cell phone and panel samples were weighted to match the sample’s demographics to the national U.S. adult population using data from the Census Bureau’s 2022 Current Population Survey (CPS). Weighting parameters included sex, age, education, race/ethnicity, region, and education. The sample was weighted to match patterns of civic engagement from the September 2021 Volunteering and Civic Life Supplement data from the CPS. The sample was weighted to match frequency of internet use and political party identification by race/ethnicity based on parameters derived from a KFF Benchmarking survey with ABS and prepaid cell phone samples. The weights take into account differences in the probability of selection for each sample type (prepaid cell phone and panel). This includes adjustment for the sample design and geographic stratification of the cell phone sample, within household probability of selection, and the design of the panel-recruitment procedure.
The margin of sampling error including the design effect for the full sample is plus or minus 4 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. KFF public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Group
N (unweighted)
M.O.S.E.
Total
1,296
± 4 percentage points
Party identification
Democrats
434
± 6 percentage points
Independents
347
± 7 percentage points
Republicans
321
± 7 percentage points
Endnotes
The share who say parents should be able to decide not to vaccinate their children has stayed steady since the beginning of the pandemic. When the question was asked by Pew Research Center, fewer adults said that parents should be able to decide not to vaccinate their children than now, with 16% who said so, compared to 30% now.
↩︎
Telehealth use surged with the COVID-19 pandemic as patients sought access to services while providers implemented social distancing protocols. An ongoing question is how the growth of telehealth will affect health spending. If payers reimburse services provided through telehealth at a lower rate, there could be cost savings. Alternatively, if telehealth encourages the use of more services, total spending could increase.
This analysis compares payments for physician medical service claims delivered via telehealth and in-person in 2021 using data from the Health Care Cost Institute (HCCI). It finds that private insurers paid similarly for telehealth and in-person physician claims for evaluation and management and mental health therapy services, on average, in 2021 as well as 2020. This is after accounting for variation across regions, providers, and severity level, among privately insured. Among providers who offered both telehealth and in-person care, the majority received similar payments for service provided in-person or through telehealth.
The analysis is available through the Peterson-KFF Health System Tracker, an online information hub that monitors and assesses the performance of the U.S. health system.
Medicare recently announced the first 10 Part D drugs selected for negotiation under Medicare’s new drug price negotiation program. These drugs were identified as the 10 top spending drugs covered under Medicare Part D without generic or biosimilar equivalents that have been on the market for at least seven years and also meet other selection criteria. The 10 drugs selected for the first round of negotiations include treatments for several medical conditions, including diabetes (Farxiga, Fiasp/NovoLog, Januvia, Jardiance), blood clots (Eliquis, Xarelto), heart failure (Entresto, Farxiga), psoriasis (Stelara, Enbrel), rheumatoid arthritis (Enbrel), Crohn’s disease (Stelara), and blood cancers (Imbruvica) (Appendix Table 1). Between June 2022 and May 2023, 8.3 million Medicare Part D enrollees used one or more of these medications. Negotiated prices for these 10 drugs will be available on January 1, 2026.
Much of the discussion around Medicare’s new drug price negotiation program has been about the details of the negotiation process, whetheror not it will impact future drug development, and the several lawsuits that have been filed by drug manufacturers seeking to block its implementation. But scant attention has been paid to the ways in which the new negotiation program could affect access to and utilization of selected drugs for Medicare Part D enrollees:
The law requires all Medicare Part D plans to cover each of the selected drugs, including all dosages and forms, when negotiated prices take effect in 2026.
The Centers for Medicare & Medicaid Services (CMS) will require Part D plans to justify formulary placement of selected drugs on non-preferred tiers, where cost sharing is typically higher than for preferred tiers.
CMS will scrutinize plans’ use of utilization management tools, such as prior authorization requirements, applied to selected drugs, which could remove administrative barriers to accessing these medications.
Along with improved access, Part D enrollees could see lower out-of-pocket costs due to lower negotiated prices, particularly for drugs with coinsurance requirements, which could increase utilization.
This brief examines how Part D enrollees’ access to and utilization of the first set of 10 selected drugs could be affected by the new Part D coverage and formulary requirements for selected drugs established by the Inflation Reduction Act and in CMS guidance, as well as the potential for lower out-of-pocket costs, based on analysis of current (2023) Part D formulary coverage, tier placement, and utilization management requirements for these 10 drugs.
The Inflation Reduction Act requires Part D plans to cover all selected drugs, including all dosages and forms, when negotiated prices are in effect
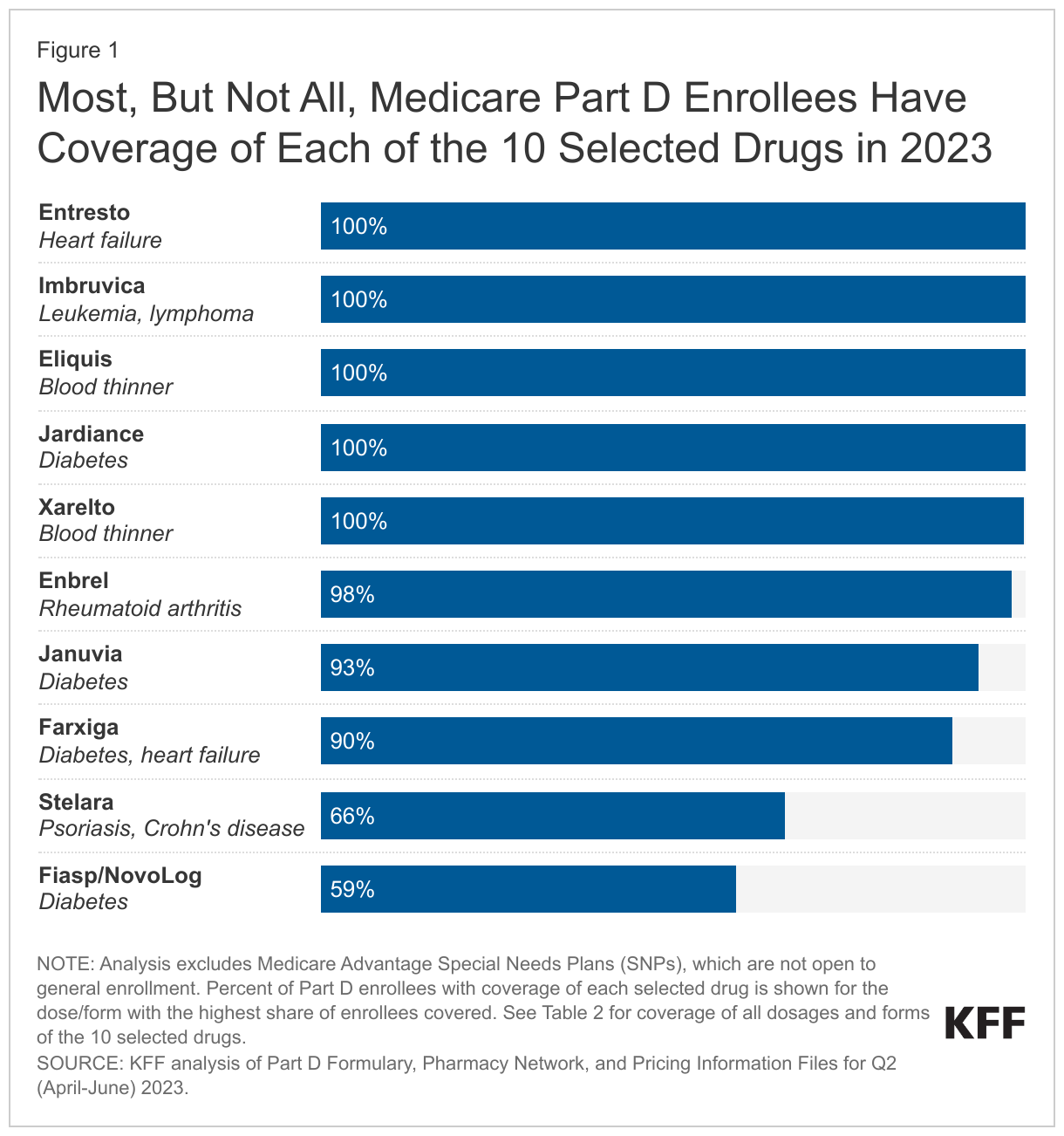
Not all Medicare Part D enrollees have coverage of each of the 10 selected drugs in 2023. The statutory coverage requirement will have the effect of improving access to the selected drugs that are not currently universally covered, in particular the insulin product Fiasp/NovoLog and the psoriasis drug Stelara. The share of Part D enrollees with coverage of any form of these 10 drugs ranges from less than 60% for Fiasp/NovoLog and 66% for Stelara to 100% for Eliquis, Entresto, Imbruvica, Jardiance, and Xarelto (Figure 1). (Imbruvica is an antineoplastic, a type of medication used to treat cancer, which is one of six so-called protected classes where all or substantially all drugs are required to be covered by all Part D plans.)
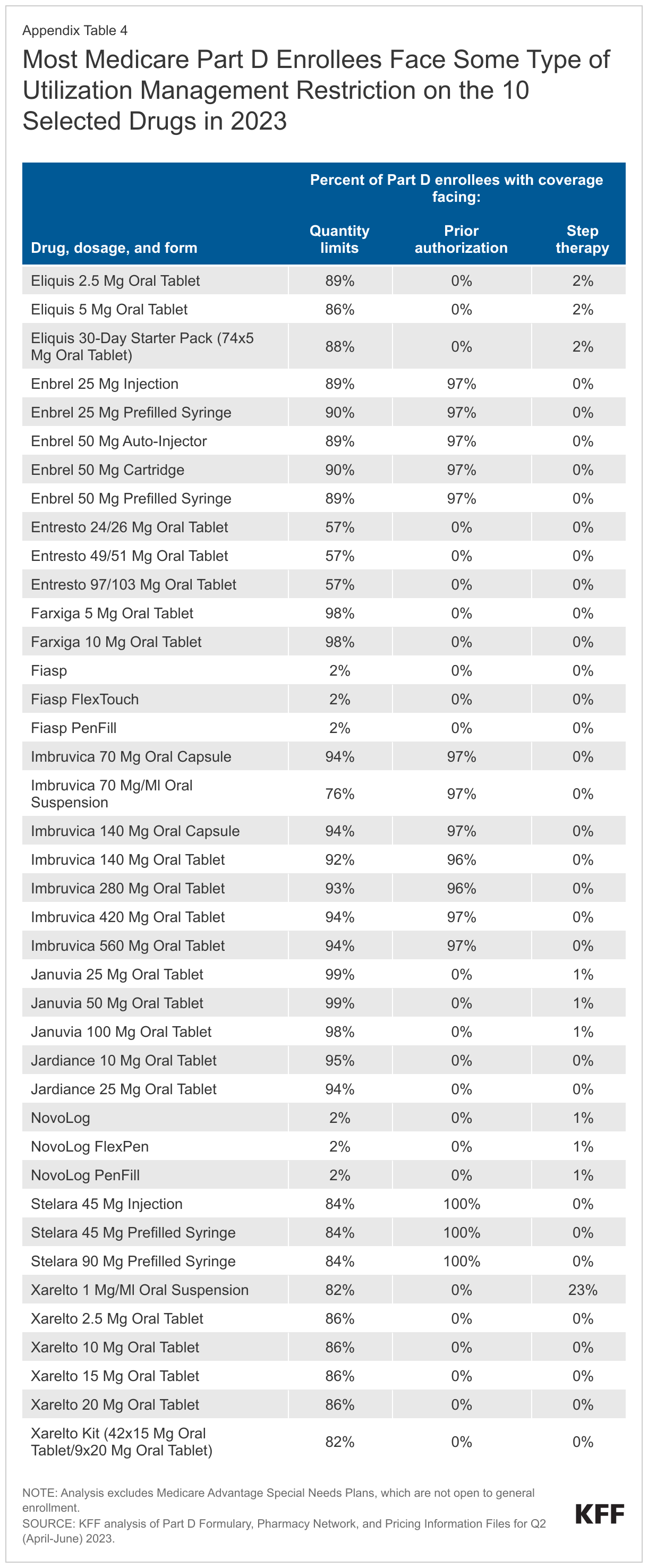
For Part D enrollees with coverage of the selected drugs in 2023, plans generally cover all or nearly all dosages and forms, but there is a small amount of variation in coverage for seven of the 10 selected drugs. For example, the blood thinner Xarelto is covered in tablet form for virtually all Part D enrollees, but the share of enrollees with coverage of the oral suspension falls to 78%. For the cancer drug Imbruvica, all enrollees have coverage of the 140mg oral capsule but that share drops to 77% for the 280mg oral tablet (Appendix Table 2).
CMS will require Part D plans to justify formulary placement of selected drugs on non-preferred tiers
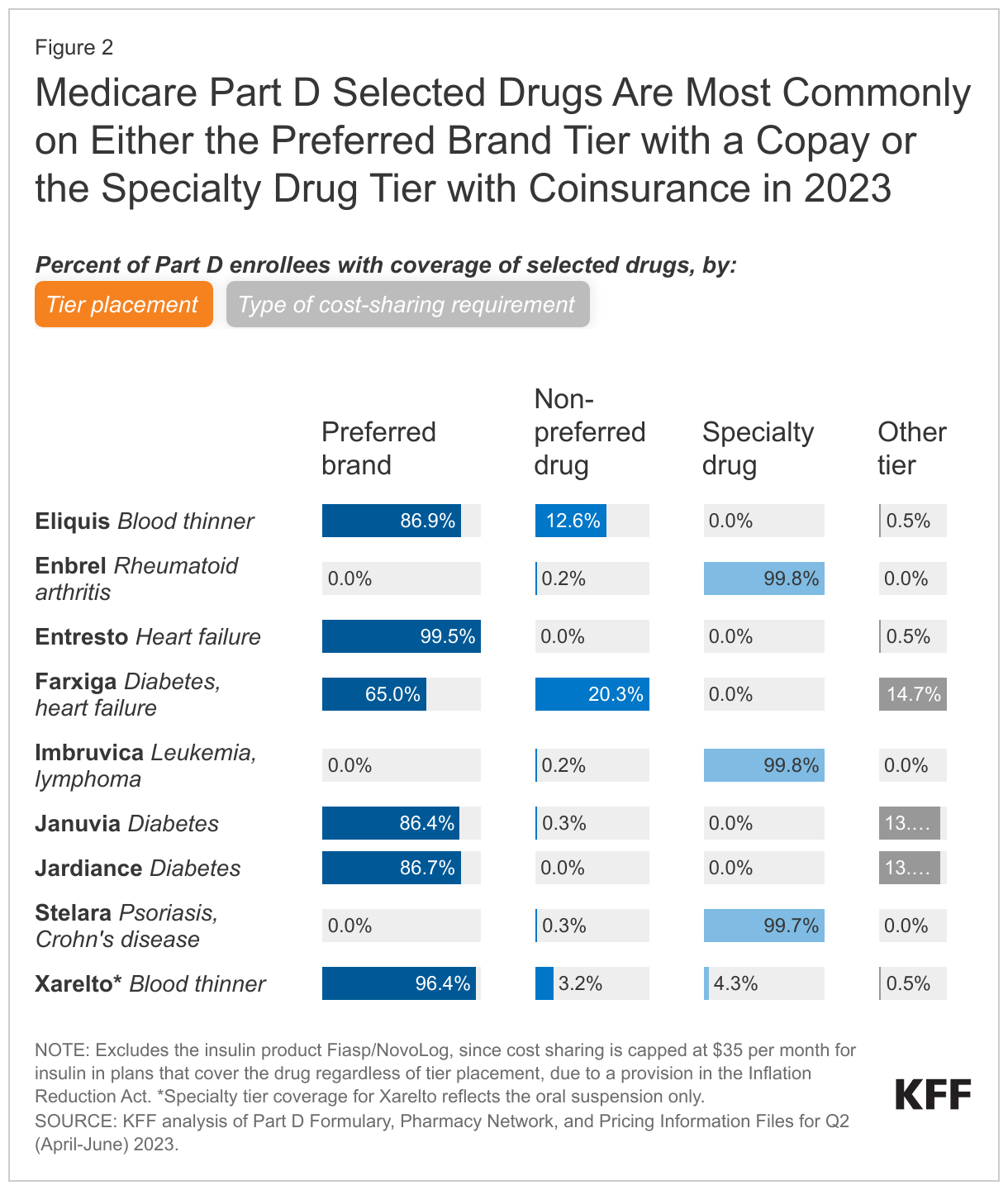
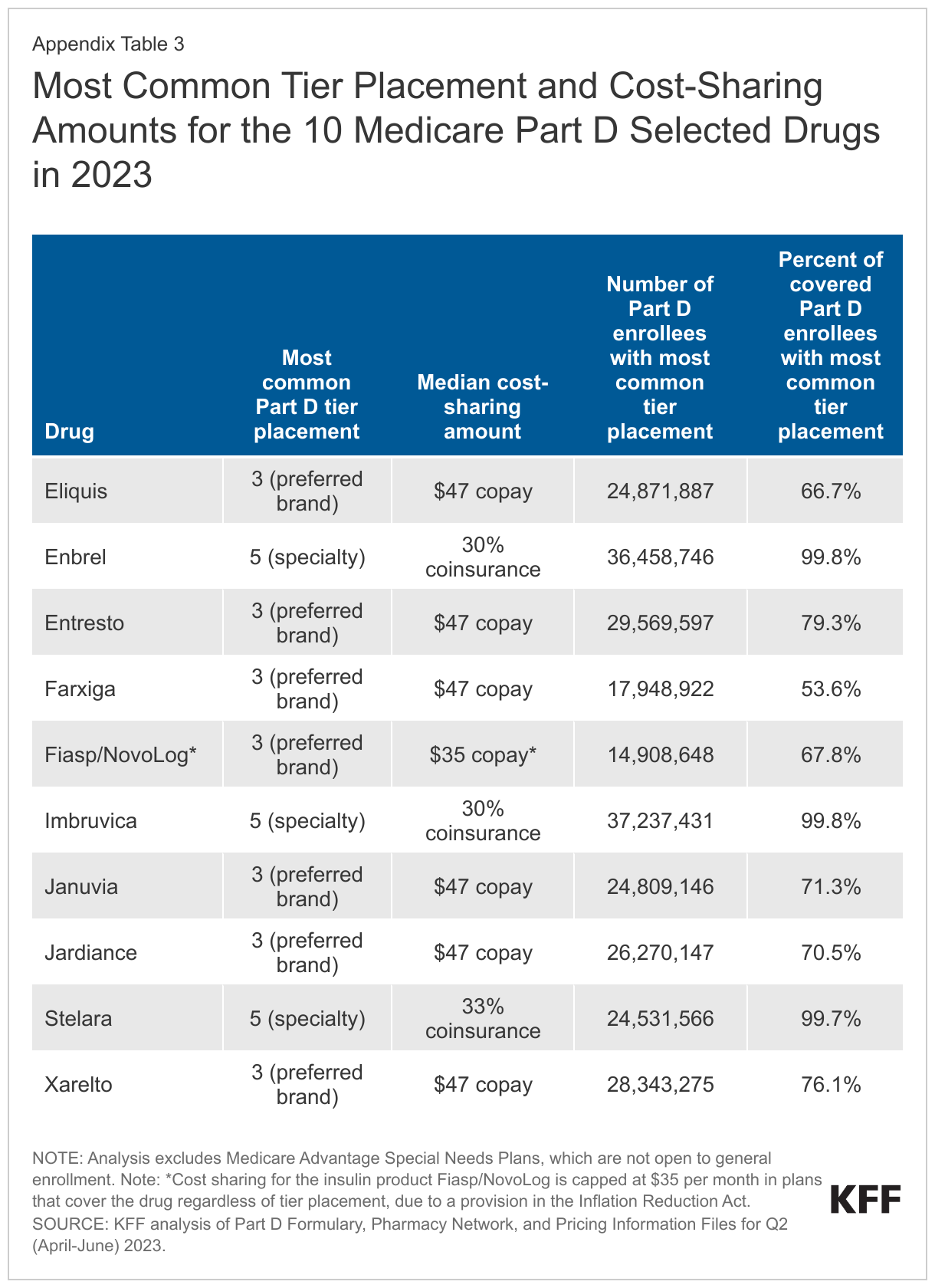
As of 2023, placement of the 10 selected drugs on non-preferred tiers is not common (although whether CMS will consider the specialty tier a non-preferred tier for this purpose is unknown); if coverage of selected drugs shifts to preferred tiers, that could lower Part D enrollees’ out-of-pocket costs. In 2023, three of the 10 selected drugs – the rheumatoid arthritis drug Enbrel, the cancer drug Imbruvica, and the psoriasis drug Stelara – are placed on the specialty tier in virtually all Part D plans that cover these drugs, with median coinsurance of 30-33% in the initial coverage phase (Figure 2, Appendix Table 3). This coinsurance rate is applied to the price of each drug to determine an enrollee’s monthly out-of-pocket cost. Currently, list prices, which do not take into account manufacturer rebates or other price concessions, are generally used in determining patient out-of-pocket costs for drugs with coinsurance. This means that a lower negotiated price would result in lower out-of-pocket costs for selected drugs with coinsurance requirements. In turn, lower out-of-pocket costs could lead to higher utilization of selected drugs.
Six of the 10 selected drugs (Entresto, Eliquis, Farxiga, Januvia, Jardiance, and Xarelto) are more commonly placed on a preferred brand tier in 2023, with a median copayment of $47 per month – an out-of-pocket amount that is fixed rather than being a percentage of the drug’s list price (Figure 2, Appendix Table 3).
But some Part D enrollees with coverage of these six drugs in 2023 have coverage on a non-preferred tier, where cost sharing is higher than for drugs on preferred tiers, and enrollees may face coinsurance of up to 50% rather than fixed copayments. For example, roughly 13% of Part D enrollees whose plans cover the blood thinner Eliquis have coverage on a non-preferred tier and face coinsurance of 50% (9.5% of enrollees) or a monthly copayment of $100 (3% of enrollees). If coverage of these drugs shifts to preferred tiers, that could lower Part D enrollees’ out-of-pocket costs.
For the insulin product Fiasp/NovoLog, the most common tier placement in 2023 is on a preferred brand tier, but regardless of tier placement, monthly cost sharing is capped at $35 in plans that cover this product. This is due to a provision of the Inflation Reduction Act, where, starting in 2023, Part D plans are not allowed to charge a copayment of more than $35 per month for covered insulin products.
CMS expects Part D plans to provide justification if more restrictive utilization management is applied to selected drugs relative to non-selected drugs in the same class
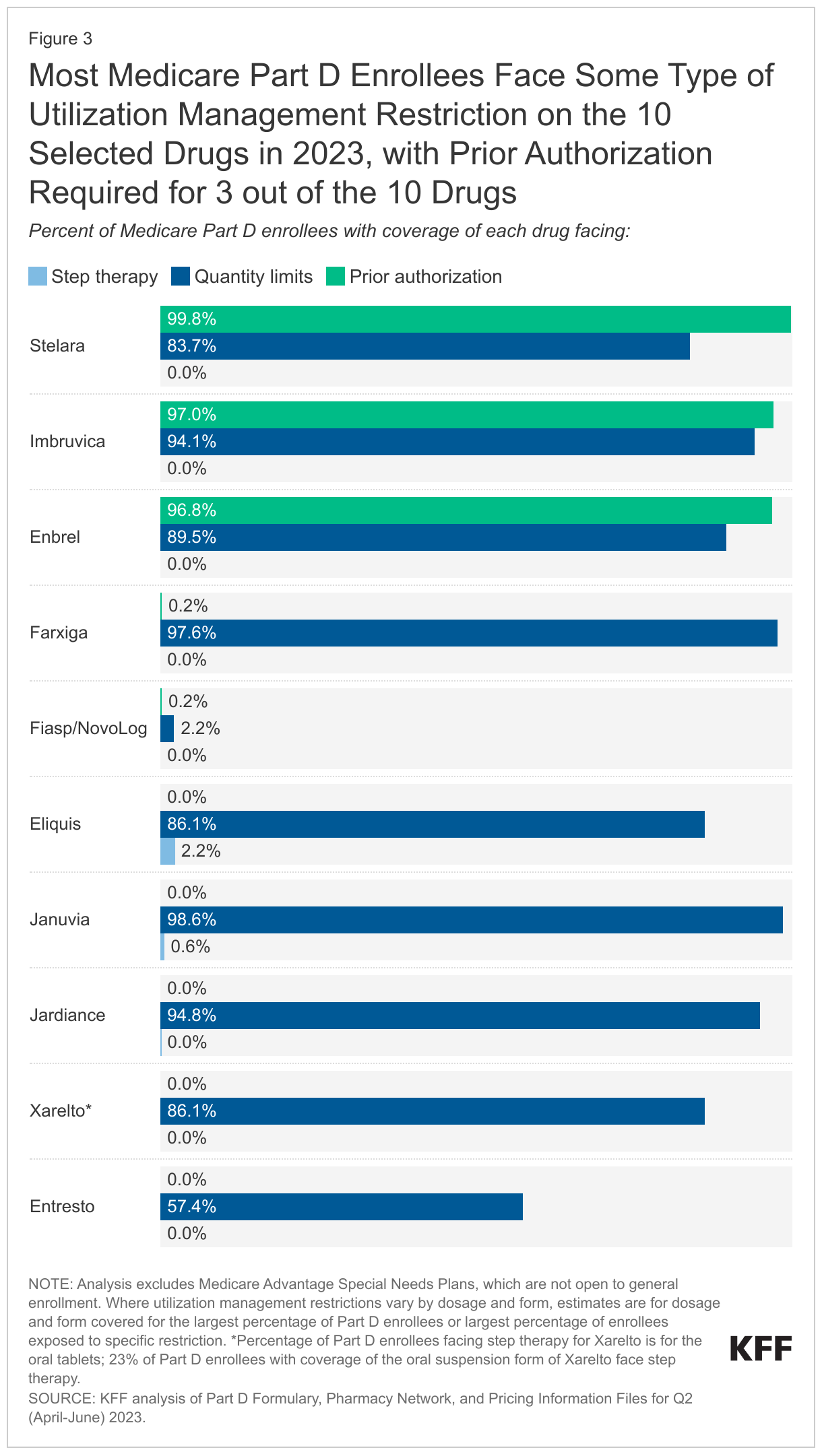
Most Part D enrollees face some type of utilization management restriction on the 10 selected drugs in 2023. Prior authorization requirements are applied to virtually all Part D enrollees who have coverage of Enbrel, Imbruvica, and Stelara in 2023, meaning that nearly all enrollees would need to get prior authorization from their plan prior to initiating treatment with any of these three drugs (Figure 3, Appendix Table 4). The most common utilization management restriction applied to the 10 selected drugs is quantity limits, ranging from around 2% of Part D enrollees who have coverage for the insulin product Fiasp/NovoLog to nearly all enrollees with coverage of Januvia and Jardiance. Step therapy requirements are rarely applied to these 10 drugs.
This analysis did not examine utilization management restrictions applied to other drugs in the same classes as selected drugs to assess whether utilization management applied to selected drugs in 2023 is comparatively more restrictive. But if CMS’s justification requirement leads to less frequent application of utilization management tools on selected drugs by Part D plans, utilization could increase.
Conclusion
While Medicare’s new drug price negotiation program is projected to lower Medicare spending on drugs selected for negotiation, less attention has been given to its potential to expand access to and utilization of selected drugs for Part D enrollees. In part, this could result from a requirement in the Inflation Reduction Act that all Part D plans cover all selected drugs once negotiated prices take effect. This requirement will have the effect of expanding coverage for the selected drugs that are not currently universally covered by all plans, in particular Fiasp/NovoLog and Stelara. This requirement could have a larger impact in future years, depending on formulary coverage of drugs selected for price negotiation in the future. CMS has also stated that it intends to use the annual formulary review process to ensure that all Part D plans cover all dosages and forms of selected drugs during the year that the negotiated prices apply. This level of coverage currently is not standard.
CMS has stated that it will also require plans to justify formulary placement of selected drugs on non-preferred tiers, where cost sharing is typically higher than when drugs are on preferred tiers. As of 2023, placement of the 10 selected drugs on non-preferred tiers is not common, but some Part D enrollees have coverage on a non-preferred tier and face higher cost-sharing requirements than for drugs on preferred tiers. If coverage of selected drugs shifts to preferred tiers, that could lower Part D enrollees’ out-of-pocket costs. And for drugs with coinsurance requirements, a lower negotiated price would result in lower out-of-pocket costs. In turn, lower out-of-pocket costs could lead to higher use of selected drugs.
Finally, CMS has stated that it expects plans to provide a justification if more restrictive utilization management is applied to selected drugs relative to non-selected drugs in the same class, or if utilization management restrictions that are not based on medical appropriateness are applied to selected drugs. If CMS’s justification requirement leads to less frequent application of utilization management tools on selected drugs by Part D plans, utilization could increase.
It should be noted that if manufacturers of selected drugs do not want to participate in price negotiations, they are required to withdraw their drugs from coverage under Medicare and Medicaid or face an excise tax on sales of the selected drug to Medicare beneficiaries. Withdrawal of products from coverage under the Medicare and Medicaid program would affect access to these medications, but would also mean that manufacturers would forfeit the revenue from sales of all of their products in these programs.
Taken altogether, the formulary and coverage requirements for selected drug in the Inflation Reduction Act and CMS guidance are likely to increase access to selected drugs for Medicare Part D enrollees and could also lower Part D enrollees’ out-of-pocket costs, which could increase utilization of these drugs and revenues for their manufacturers.
Juliette Cubanski and Tricia Neuman are with KFF. Anthony Damico is an independent consultant.
Methods
This analysis is based on KFF analysis of the Part D Formulary, Pharmacy Network, and Pricing Information Files for Q2 (April-June) 2023. Part D formulary files were used for analysis of formulary coverage, tier placement, cost-sharing amounts, and utilization management restrictions. The formulary analysis includes 4,281 Part D plans, both stand-alone prescription drug plans and Medicare Advantage drug plans, covering 37.3 million enrollees. Analysis excludes Medicare Advantage Special Needs Plans (SNPs), which are not open to general enrollment (1,144 plans covering 5.7 million enrollees).
Formulary tiers with tier number 3 were categorized as preferred brands, tier number 4 as non-preferred drugs, and tier number 5 as specialty drugs; all other tier numbers were categorized as other tier. Cost sharing is based on standard (i.e., non-preferred) 30-day cost-sharing requirements and is enrollment weighted.
Jennifer Kates, senior vice president and director of the Global Health and HIV Policy Program at KFFCynthia Cox, vice president and director of the Program on the ACA at KFF
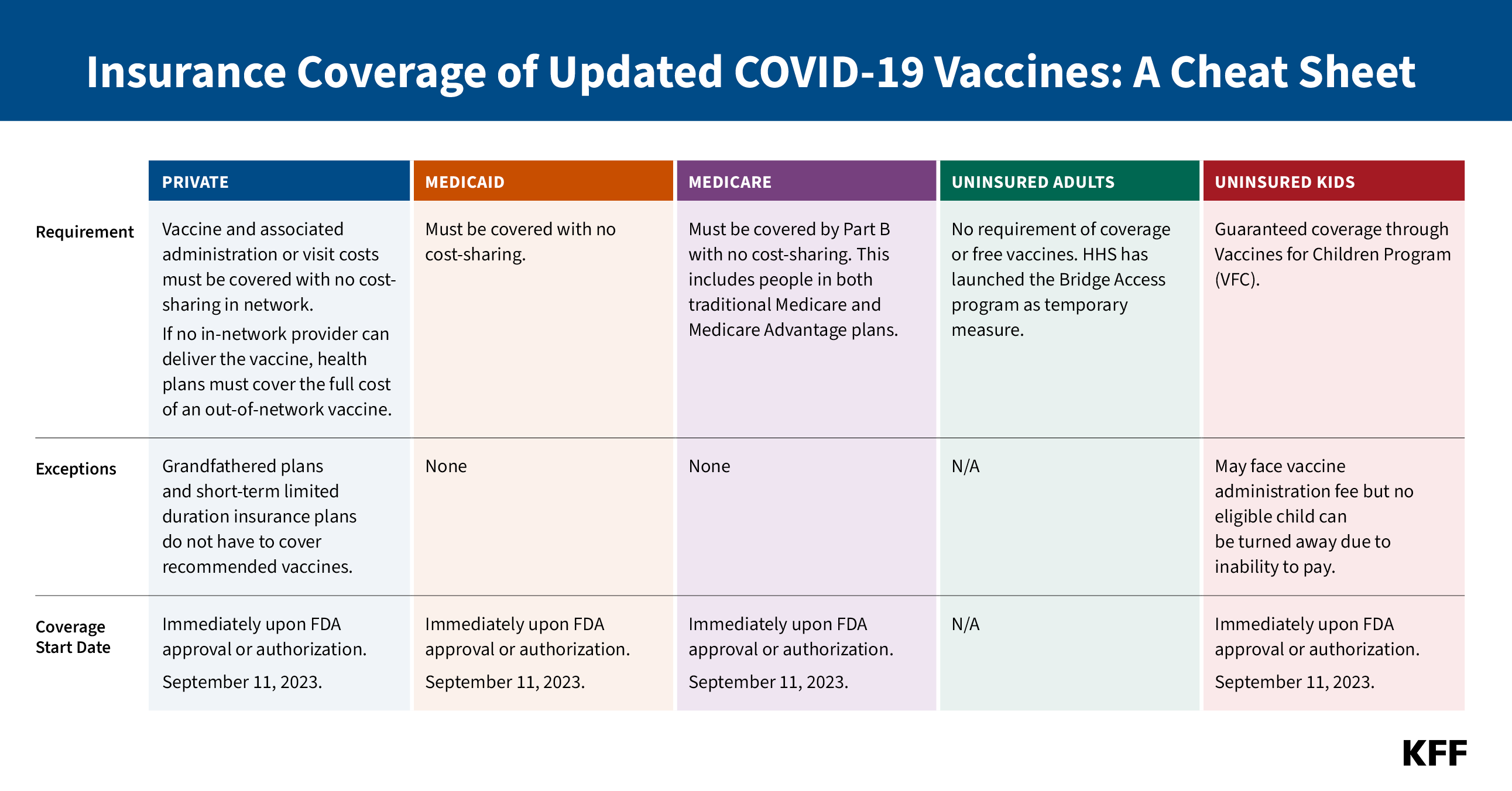
On September 11, 2023, the FDA approved and authorized updated COVID-19 vaccines from Pfizer and Moderna. The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP) recommended them for everyone from the ages of 6 months and older on September 12 and the CDC Director adopted this recommendation on the same day. This marks the first time that COVID-19 vaccines will be commercialized – that is, transitioned to the commercial market for their manufacturing, procurement and pricing. Up until this point, the federal government had purchased all COVID-19 vaccines and provided them free of charge to anyone, regardless of insurance coverage or ability to pay. The commercial price being charged by Pfizer and Moderna is $115 to $128 per dose, respectively, about 3-4 times higher than the price paid for by the federal government. In addition to the cost of the vaccine, there may be a cost associated with administering the vaccine and/or the cost of a provider visit.
With commercialization, the way in which vaccines are paid for and whether they are covered by insurance will now be dictated by insurance market rules and regulations. Because of the Affordable Care Act and laws passed during the COVID-19 pandemic, COVID-19 vaccines will continue to be free of charge to virtually everyone with private and public insurance coverage, although uninsured adults will have no guarantee of free vaccines. This cheat sheet provides details on coverage rules by insurance type and for people who are uninsured.
LEGAL BASIS
Private:
ACA: Requires private insurers to cover any ACIP recommended vaccine once the CDC Director adopts recommendation no later than one year later.
CARES Act: Expedited coverage requirement to 15 business days for COVID-19 vaccines
DOL FAQs: The 15-day requirement was already satisfied 15 days after first COVID-19 vaccine recommended in December 2020. As of January 5, 2021, any COVID-19 vaccine that is approved or authorized by the FDA must be covered immediately.
Medicaid:
ARPA: Requires no cost-sharing through September 2024
IRA: Requires Medicaid coverage of ACIP-recommended vaccines for adults with no cost sharing permanently.
Medicaid covers ACIP-recommended vaccines for children at no cost through the Vaccines for Children Program.
Medicare:
CARES Act: Requires no cost-sharing
Uninsured Adults:
There is no federal guarantee of free recommended vaccines for adults. Section 317 of the Public Health Services Act created a discretionary program that provides some limited support for recommended vaccines. The Biden administration has proposed creating a mandatory Vaccines for Adults Program, modeled on the Vaccines for Children Program
Uninsured Children:Section 1928 of the Social Security Act created the VFC program. Vaccines are automatically included in program if recommended by ACIP and included on the CDC’s vaccine schedule. COVID-19 vaccines were added to the vaccine schedule on October 19, 2022.
As Congress considers reauthorization of the President’s Emergency Plan for AIDS Relief (PEPFAR) for a fourth time, KFF explores the debate over abortion policy that has stalled the legislation and the potential implications if Congress does not reauthorize the program. PEPFAR spans more than 50 countries and has been reported to have saved 25 million lives since President George W. Bush created it in 2003. Funding for the program in FY 2023 was $6.9 billion, including funding for the Global Fund to Fight AIDS, Tuberculosis, and Malaria.
Despite a long history of broad and bipartisan support—and in the wake of the U.S. Supreme Court’s overturning of the constitutional right to abortion—the U.S. government’s signature global health effort in the fight against HIV has been drawn into a broader political debate about abortion, even though U.S. law prohibits the use of U.S. foreign assistance, including PEPFAR funding, for abortion.
In this new analysis, KFF provides an overview of the current debate and answers key questions about the role of the abortion debate in PEPFAR’s reauthorization, including:
What concerns about abortion have been raised?
What has been the response by PEPFAR and the U.S. government?
What U.S. government laws and policies regarding abortion apply to PEPFAR?
What are the implications if PEPFAR is not authorized?
Despite a long history of broad and bipartisan support, reauthorization of the President’s Emergency Plan for AIDS Relief (PEPFAR) is currently being held up by congressional debate around abortion. PEPFAR, first created in 2003 by President George W. Bush and reauthorized three times thus far, is the U.S. government’s signature global health effort in the fight against HIV. Widely regarded as one of the most successful programs in global health history, PEPFAR reports having saved 25 million lives due to its efforts, and KFF analyses have found a significant impact of the program beyond HIV, including large reductions in both maternal and child mortality and significant increases in some childhood immunization rates. Still, its fourth reauthorization has been drawn into broader U.S. political debate about abortion, in the wake of the Supreme Court’s Dobbs v. Jackson Women’s Health Organization decision (which overturned the nationwide right to obtain an abortion), even though U.S. law prohibits the use of U.S. foreign assistance, including PEPFAR funding, for abortion. This policy watch provides an overview of the current debate and issues.
What concerns about abortion have been raised?
Abortion was publicly raised as one of the discussion points in PEPFAR reauthorization in early May after a coalition of organizations opposed to abortion rights, a conservative think tank’s report, and a member of Congress raised their concerns that PEPFAR may be supporting abortion. Among the criticisms leveled were that the Biden administration had restored funding to the United Nations Population Fund (UNFPA), signaled its support for sexual and reproductive health and rights globally in the September 2022 Reimagining PEPFAR’s Strategic Direction strategy document and February 2023 PEPFAR operational guidance, and funded various recipients who expressed support for abortion generally. There was also a call for Congress to reinstate and apply the “Mexico City policy” to PEPFAR. The Mexico City policy – first instituted in 1984 but not currently in effect – is a policy that required foreign non-governmental organizations (NGOs) to certify that they would not perform or promote abortion as a method of family planning using funds from any source as a condition for receiving certain U.S. funding. Typically put in place through executive order, it first applied to PEPFAR in 2017 under an expanded version of the policy instituted by President Trump, which was rescinded by President Biden in 2021 (prior to that time, when it was in place, PEPFAR was not subject to this policy).
What has been the response by PEPFAR and the U.S. government?
There has been no evidence produced that PEPFAR has supported any prohibited abortion activities. In June, Ambassador John Nkengasong, the head of PEPFAR, publicly stated that PEPFAR does not provide a platform for abortion in Africa and that it is “implemented strictly within the context of the laws it was created [by].” PEPFAR also sent official communication to all its implementers regarding current law and policy in this area. Additionally, the PEPFAR program revised its earlier September 2022 document, Reimagining PEPFAR’s Strategic Direction, to clarify that “sexual and reproductive health services” has a specific meaning in the PEPFAR context and reiterated that “PEPFAR does not fund abortions, consistent with longstanding legal restrictions on the use of foreign assistance funding related to abortion.” The U.S. government also has training and compliance processes in place to monitor the adherence of funding recipients and sub-recipients with U.S. requirements.
What U.S. government laws and policies regarding abortion apply to PEPFAR?
PEPFAR is governed by several legal, policy, and programmatic requirements related to abortion (see the KFF fact sheet on these and other requirements), including:
theHelms Amendment (in place since 1973) – a legal ban on the direct use of U.S. funding overseas for the performance of abortion as a method of family planning or to motivate or coerce any person to practice abortion;
theLeahy Amendment (in place since 1994) – a legal requirement that clarifies the Helms Amendment language that uses the term “motivate” by stating that “motivate” shall not be construed to prohibit, where legal, the provision of information or counseling about all pregnancy options; and
theSiljander Amendment (in place since 1981) – a legal ban on the direct use of U.S. funding overseas to lobby for or against abortion.
In addition, while not currently in effect, the Mexico City policy was applied to PEPFAR for the first time during the Trump administration.
what are the implications if PEPFAR is not reauthorized?
If PEPFAR is not reauthorized this year, or in the near future, the program won’t end, but there are several practical and symbolic implications for the program and the people it serves.
PEPFAR is a permanent part of U.S. law and will continue, provided funds are appropriated. PEPFAR operates largely under permanent authorities of U.S. law that allow for ongoing funding and the continuation of the major structures of the program, such as the Office of the Global AIDS Coordinator at the Department of State as well as the position of Global AIDS Coordinator, U.S. participation in the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), and annual reporting on PEPFAR efforts.
Some requirements, however, are time-bound and would “sunset.” There are eight requirements that will end (seven after FY 2023 and one after FY 2024) if not addressed through PEPFAR reauthorization or another legislative vehicle. These include requirements related to Global Fund support, a funding directive for orphans and vulnerable children (OVC), and others.
The lack of reauthorization would mark a significant departure from PEPFAR’s long-time bipartisan support. PEPFAR has enjoyed strong bipartisan support across multiple Congresses and administrations. This has enabled the program to operate outside some of the policy debates that have stalled agreement on other issues related to both health care and foreign assistance in Congress. Despite the fact that funding for PEPFAR could continue absent reauthorization, the program may be more vulnerable in future funding debates.
Failure to reauthorize the program could send a message to partner countries and the people served by PEPFAR. Despite vocal administration support for the program as well as former President Bush and others calling on Congress to reauthorize PEPFAR, the lack of a congressional reaffirmation of the program may undermine efforts to demonstrate the depth of the U.S. government’s commitment to the global fight to end AIDS and broader leadership role in global health. It could also weaken PEPFAR’s partnering and diplomatic efforts, particularly conversations with partners about longer-term planning, financial sustainability, and country leadership of efforts.
KFF Research Shows that Medicare Open Enrollment TV Ads Are Dominated by Medicare Advantage Plans Featuring Celebrities, Active and Fit Seniors, and Promises of Savings and Extra Benefits Without Fundamental Plan Information
Beneficiaries Say They Are Confused— “Medicare” Hotlines and Other Tactics Often Give Viewers False Impressions
The annual blitz of ads for Medicare Advantage plans has become a rite of fall, as health insurers, brokers and other third parties seek to court enrollees for these private plans, which are offered to the 65 million people with Medicare during the program’s open enrollment season.
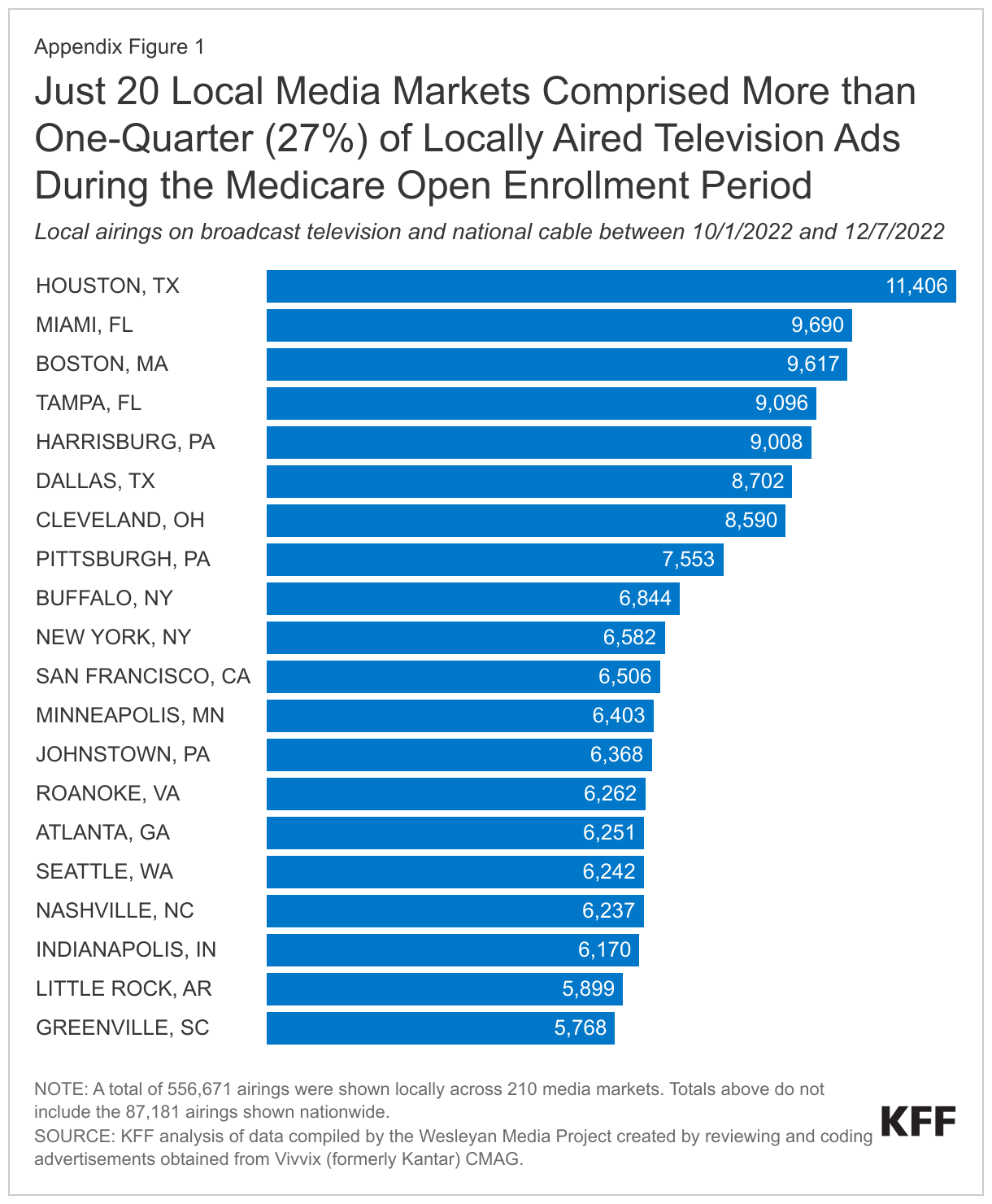
In advance of the open enrollment period starting on October 15, KFF reviewed more than 1,200 unique television ads that aired more than 643,000 times last year to examine these marketing strategies in depth.
Based on its research, KFF found a heavy reliance on celebrity endorsers, liberal use of what appear to be official hotlines and images of government-issued Medicare cards, and suggestions that seniors who do not sign up for a plan could miss out on benefits to which they are entitled.
More than 85 percent of airings, or 9,500 ads per day, were for Medicare Advantage, the private plans that now enroll more than half of all eligible people with Medicare. Most of the remaining ads were for Medicare drug plans or Medicare supplemental insurance (Medigap).
Ads rarely mentioned traditional Medicare, or potential limitations with plan coverage, such as provider networks or prior authorization requirements, leaving beneficiaries with an incomplete view of their coverage options and the tradeoffs among them. Open enrollment runs annually from Oct. 15 to Dec. 7, with advertising permitted to begin on Oct. 1.
“There’s no question that Medicare has become a lot more complex. As enrollment in Medicare Advantage plans has grown, the annual marketing madness can create confusion for people who are trying to make difficult decisions about coverage,” said KFF President and CEO Drew Altman. “We heard directly from seniors in focus groups that the ads were often perceived as misleading and left them feeling overwhelmed. This isn’t a good basis on which to make a choice that will affect your health and pocketbook.”
Key insights from the research include:
More than a quarter of all airings of Medicare Advantage ads (27%), included an official Medicare card or an image that resembled it. Additionally, more than 80% of airings sponsored by brokers and other third parties urged viewers to call a toll-free number described as “Medicare” hotline. But the number was not the official 1-800-Medicare hotline, and the entities behind such messages did not represent the government. New CMS rules in effect for the upcoming open enrollment period prohibit misleading use of the Medicare name, logo, or card in private marketing and communication materials, or any use of the Medicare card without prior approval from CMS.
Some ads suggest that seniors may miss out on financial savings, or benefits to which they are entitled, if they don’t sign up for a Medicare Advantage plan. While Medicare Advantage plans do typically offer extra benefits, that can leave viewers with the impression that they have incomplete coverage if they have traditional Medicare, and that they have an entitlement to extra benefits under Medicare Advantage.
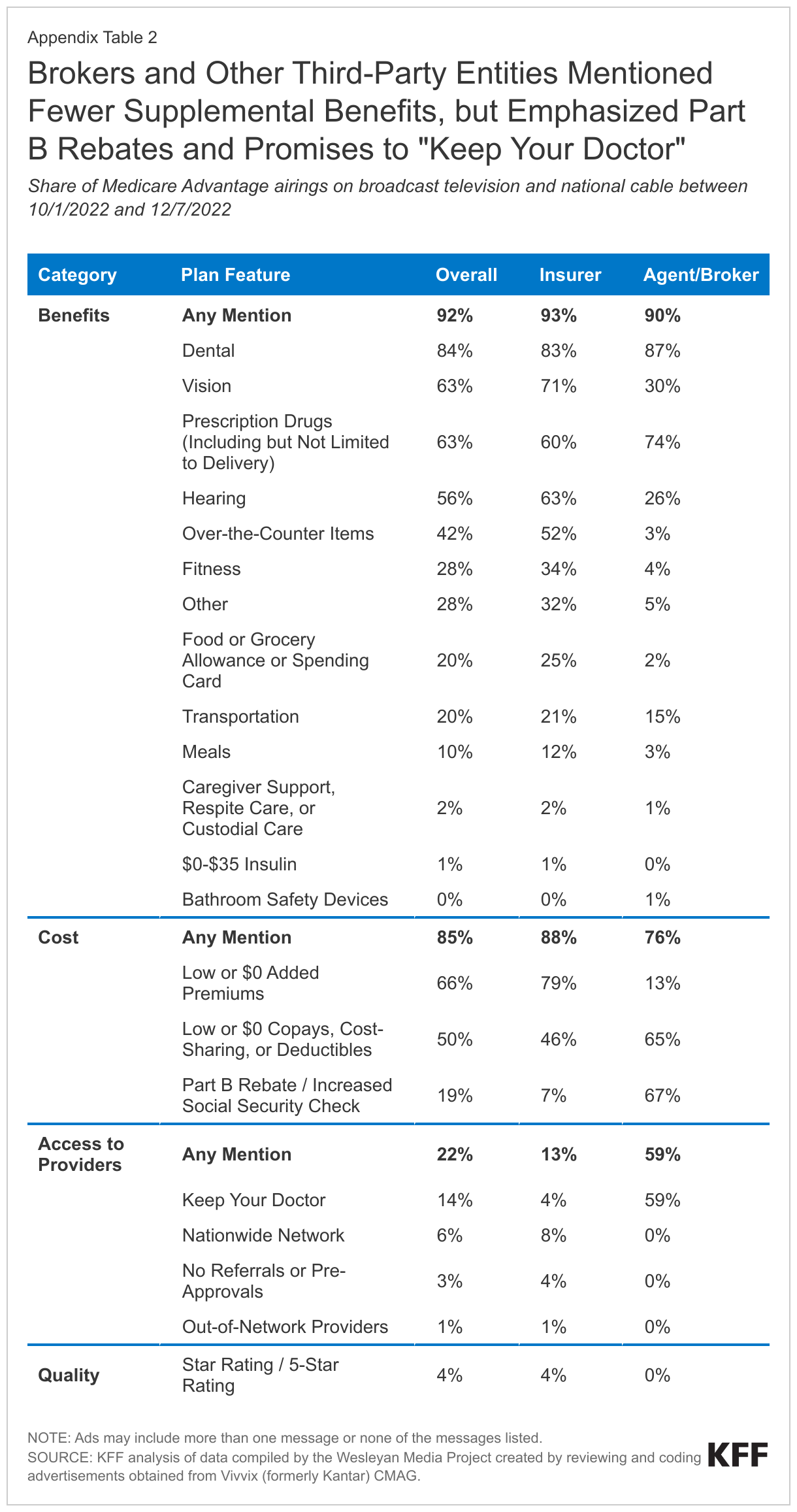
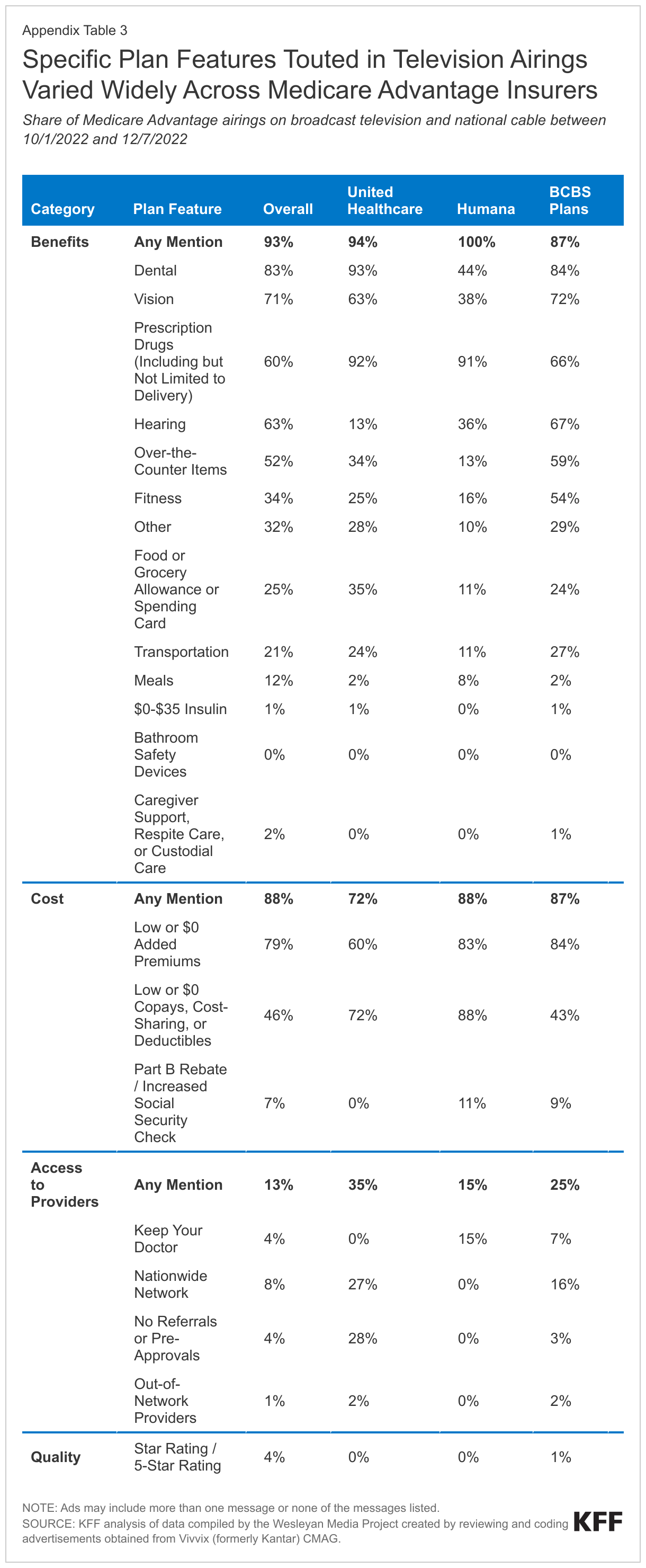
Nearly all Medicare Advantage ad airings emphasized extra benefits, such as dental, vision, and hearing (92%) or the potential for lower out-of-pocket spending (85%). Less than 4 percent of airings referenced quality star ratings, even though CMS created the ratings in part to help shoppers compare Medicare Advantage plans.
One-in-four Medicare Advantage ad airings (26%) showed physically robust seniors engaging in activities such as hiking, yoga, tennis, and even bouncing on a trampoline. This may suggest that they are targeting relatively healthy, lower cost enrollees. Few ads showed people with visible disabilities (4%) or the appearance of serious illness (1%), though one-fifth of Medicare beneficiaries are in fair or poor self-reported health.
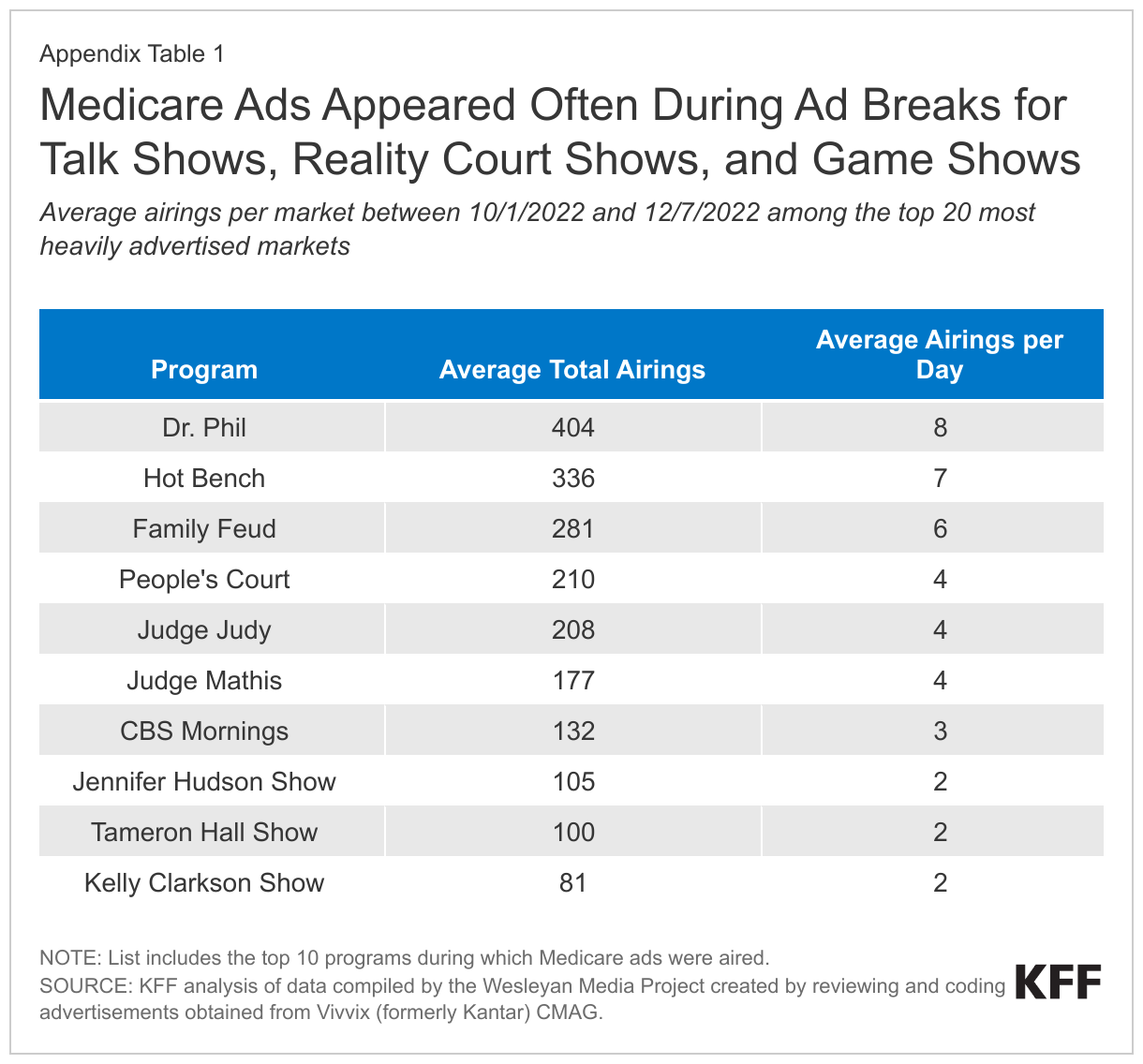
Celebrity endorsers, including actor William Shatner, comedian J.J. Walker and former Arkansas governor Mike Huckabee, appear more often in Medicare Advantage ads sponsored by brokers and other third-party entities than in ads sponsored by insurers. The celebrity endorsers are almost always men. Ex-NFL star Joe Namath was the most prolific, appearing in ads that aired nearly 56,000 times over the period, or about 10 percent of all airings of Medicare Advantage ads that season. More than two-thirds of ad airings sponsored by brokers and other third parties mentioned getting money back in your Social Security check, even though just 17% of Medicare Advantage plans offered in 2023 include this benefit.
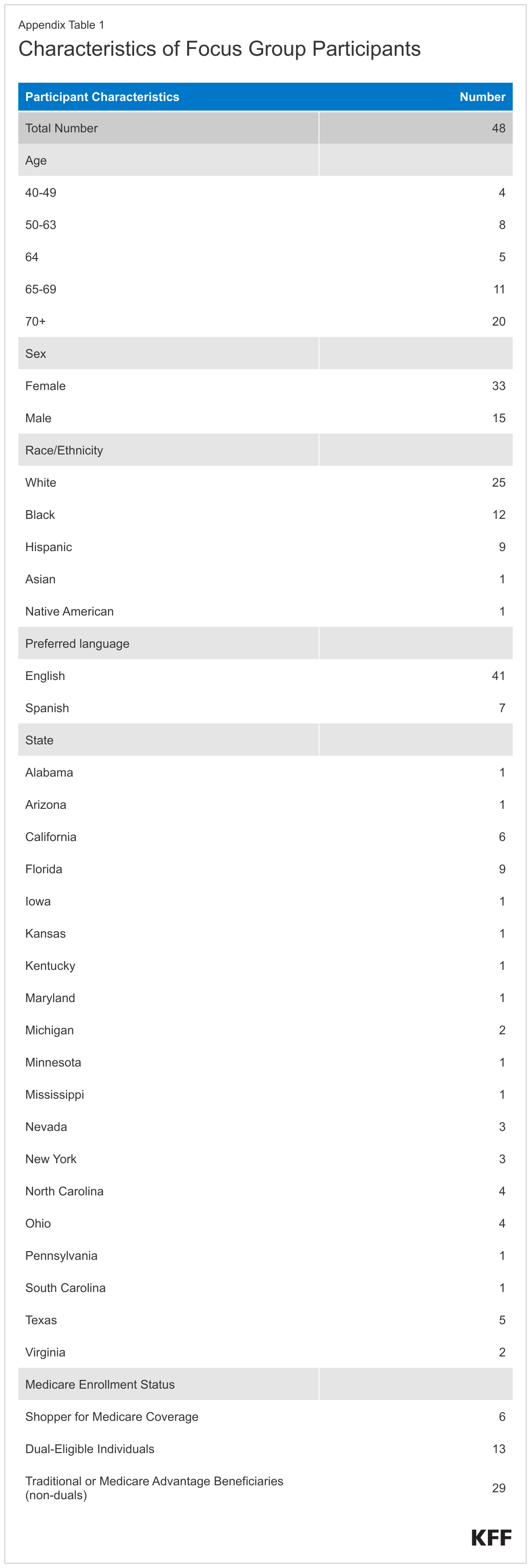
As part of this research, KFF also released a second report that was based on focus groups conducted in fall 2022, which confirms that many Medicare beneficiaries and their family members feel overwhelmed by the annual onslaught of TV ads and are sometimes confused about whether the government or private companies are behind them.
In the focus groups with beneficiaries and other Medicare plan shoppers, many participants thought TV advertisements were misleading and said they did not trust the content of the ads, particularly those that marketed a slew of “free” benefits. Many participants said they relied on agents and brokers when making coverage decisions. Few used government resources, such as the Medicare Handbook or 1-800 Medicare, but those who did generally found them helpful.
The two KFF reports come at a time when lawmakers in Congress, state insurance regulators and officials in the Biden administration are taking steps to address rising consumer complaints about deceptive marketing practices in Medicare ads. Such complaints, which numbered fewer than 16,000 in 2020, increased to nearly 40,000 in the first eleven months of 2021, according to the Centers for Medicare and Medicaid Services (CMS). The rise has coincided with an increase in advertising by third-party marketing organizations such as agents, brokers, lead generation businesses and media firms in recent years.
Finally, a third new KFF resource answers key questions about the Medicare open enrollment period. It addresses topics such as what sorts of changes beneficiaries can make during open enrollment; how features of traditional Medicare compare to Medicare Advantage; how supplemental coverage like Medigap plans or retiree health benefits factor into Medicare coverage decisions.
The Medicare ad study by KFF analyzed TV ad data that was compiled by the Wesleyan Media Project, which collaborated with KFF on the research. Ads were obtained from Vivvix (formerly Kantar) CMAG, a data analytics and consulting firm, and were coded by the Wesleyan Media Project and analyzed by KFF.
KFF also worked with PerryUndem to conduct focus groups with Medicare beneficiaries and other Medicare plan shoppers in the Fall of 2022, during the annual Medicare open enrollment period.
The full reports are available collectively here or individually at:
Most of the 65 million beneficiaries who receive health insurance coverage through the federal Medicare program are enrolled in some form of private plan. In 2023, 31 million Medicare beneficiaries are enrolled in Medicare Advantage (Medicare Part C) plans administered by private health insurers. The other 34 million beneficiaries are in traditional Medicare, including 22 million beneficiaries who are enrolled in a Medicare Part D prescription drug plan offered by private sponsors, and more than 14 million who have Medicare supplemental insurance (Medigap) offered by private insurers (traditional Medicare beneficiaries may be enrolled in a Part D plan, a Medigap plan, or both).
Private plan offerings have grown in recent years, most notably in the Medicare Advantage market. More Medicare Advantage plans are available in 2023 than in any prior year. Medicare Advantage enrollment has doubled since 2010, due in part to extensive marketing efforts and the draw of extra benefits and attractive cost features. Each year, beginning on October 1st, insurers, as well as brokers and other third-party entities, are permitted to begin marketing Medicare Advantage for the annual open enrollment period for coverage in the following year. The open enrollment period for Medicare Advantage and Medicare Part D plans runs from October 15th through December 7th. Television ads are one of many marketing activities used by insurers, brokers and other third-party entities to boost enrollment.
Recently, the Centers for Medicare and Medicaid (CMS) has reported a steep rise in beneficiary complaints related to the marketing of Medicare Advantage and Part D plans. Many of these complaints have centered on the activities of brokers and other third-party entities, referencing misleading claims and aggressive sales tactics. Concerns raised by the National Association of Insurance Commissioners and in a report released by the majority staff of the U.S. Senate Committee on Finance have also called attention to this issue. In response, CMS published updated regulations, effective June 2022, mandating stricter oversight of these third parties by the insurers they represent. Additional CMS requirements intended to curtail misleading marketing activities came into effect in June 2023, and will apply to the open enrollment period for 2024 coverage and beyond.
To capture the state of television marketing activities and consider the implications for people with Medicare, KFF analyzed ad data compiled by the Wesleyan Media Project, that were obtained from Vivvix (formerly Kantar) CMAG, a data analytics and consulting firm, and were coded by the Wesleyan Media Project in collaboration with KFF. The data set included all English-language TV ads that aired across national and local markets on broadcast television or national cable, from October 1st, 2022, through December 7th, 2022, the period that includes the Medicare open enrollment period for coverage in 2023. (see Methods).
Key Takeaways:
TV airways were flooded with ads for Medicare plans. Nearly 650,000 airings of Medicare ads appeared during the nine weeks of advertising, more than 9,500 airings per day. Most of these ads were aired in local media markets. While most TV ads were sponsored by health insurers, about one in every five TV ads were sponsored by brokers and other third-party entities, such as marketing firms.
TV ads for Medicare Advantage comprised more than 85% of all airings for the open enrollment period for 2023. The remaining ads focused on other types of plans, such as Medigap and stand-alone Part D prescription drug plans, or promoted the open enrollment period more generally. Medicare Advantage ads were disproportionately sponsored by health insurers who offer plans that comprise a relatively small share of Medicare Advantage enrollees.
TV ads for Medicare Advantage often showed images of a government-issued Medicare card or urged viewers to call a “Medicare” hotline other than the official 1-800-Medicare hotline. More than a quarter of all airings (27%) included a government-issued Medicare card or image that resembled it, including 28% of insurer-sponsored airings and 21% of airings sponsored by brokers and other third-party entities, a trend that CMS has flagged as potentially misleading to beneficiaries. Roughly 16% of airings featured a privately-run phone line described as a “Medicare” hotline, most of which were sponsored by brokers and other third-party entities.
Some ads suggested that people with Medicare miss out on benefits to which they are entitled if they are not enrolled in a Medicare Advantage plan. These TV ads were more common among ads sponsored by brokers and other third-party entities than those sponsored by health insurers, and used language that implied viewers were “missing out” on benefits they were “entitled to,” or receiving incomplete coverage under Medicare Parts A and B if they were not enrolled in a Medicare Advantage (Part C) plan
The vast majority of Medicare Advantage ad airings touted low costs and extra benefits, while few mentioned quality ratings. Nearly all Medicare Advantage ad airings emphasized extra benefits, such as dental, vision, and hearing (92%) or the potential for lower out-of-pocket spending (85%). Airings sponsored by brokers and other third-party entities often (67%) promoted the potential for enrollees to get money back in their Social Security check (or lower their Medicare Part B premium). Few airings (4%) mentioned quality star ratings.
Medicare Advantage ad airings often featured active seniors engaged in physical activities, but rarely showed people who appeared to have a serious health problem or visible disability. One in four Medicare Advantage ad airings (26%) showed seniors taking part in activities such as hiking or yoga, but few included people with visible disabilities (4%) or the appearance of serious illness (1%) for whom health insurance coverage and choice of providers may be a high priority.
TV ads sponsored by brokers and other third-party entities used celebrity endorsements more often than health insurers to promote Medicare Advantage. Celebrities, such as actors, athletes, and politicians, appeared in more than half of Medicare Advantage ad airings sponsored by brokers and other third parties (55%), but rarely appeared in airings sponsored by insurers (3%). Familiar figures included Joe Namath, Lionel Richie, William Shatner, and JJ Walker. Joe Namath was featured more than any other celebrity, appearing in nearly 56,000 airings.
Medicare beneficiaries have a wealth of choices for their health insurance coverage. While beneficiaries may appreciate the ability to select from multiple options, the variable costs, benefits, provider networks, and other characteristics of Medicare Advantage plans make the decision complex, especially in light of the barrage of advertising. Additionally, information about coverage under traditional Medicare is rarely included in television ads, leaving beneficiaries with an incomplete view of their coverage options and the tradeoffs among them. While CMS has issued new rules to address concerns about aggressive and misleading marketing tactics, ongoing monitoring and resources independent of commercial interests could help to improve beneficiary decision-making.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Jeannie Fuglesten Biniek, Alex Cottrill, Nolan Sroczynski, Meredith Freed and Tricia Neuman are with KFF. Breeze Floyd, Laura Baum, and Erika Franklin Fowler are with the Wesleyan Media Project. We thank Markus Neumann, Jielu Yao (Wesleyan University) and Sarah Gollust (University of Minnesota). We also thank the numerous undergraduate student research assistants at Wesleyan University for their efforts on this project.
Report
Introduction
During the annual Medicare open enrollment period that runs from October 15th through December 7th, Medicare beneficiaries can review the coverage options available in their area and make changes for the upcoming year. Drawn by the prospect of strong financial performance, buoyed by generous payments from the federal government, many insurers have expanded their Medicare Advantage offerings in recent years. In 2023, Medicare beneficiaries can choose from an average of 43 Medicare Advantage plans, offered by 9 different insurers, the highest number ever available. Traditional Medicare beneficiaries selecting prescription drug coverage can choose from an average of 24 stand-alone Part D plans.
Plans rely on TV advertising, among other marketing activities, to attract and retain enrollees during the open enrollment period. Recent years have seen an increase in print and television ads from third-party marketing organizations, such as agents and brokers, lead generation businesses, and media firms. At the same time, the Centers for Medicare and Medicaid Services (CMS) has reported a steep rise in beneficiary complaints related to the marketing of private Medicare plans, from less than 16,000 in 2020 to nearly 40,000 in the first eleven months of 2021, many of them centered on the marketing activities of these third-party entities.
In May 2022, the National Association of Insurance Commissioners (NAIC) sent a letter to Congress urging action on this issue, citing concerns about misleading claims and aggressive sales tactics. The following November, the majority staff of the Senate Finance Committee released a report detailing complaints and associated marketing materials from key stakeholders across 14 states. In response, CMS released new regulations, effective June 2022 and June 2023, tightening restrictions on health insurers and third parties who market Medicare Advantage and Part D plans.
This report describes the content and characteristics of all English-language TV ads focused on Medicare that aired on broadcast television or national cable between October 1, 2022 and December 7, 2022. Ads were obtained by the Wesleyan Media Project from Vivvix (formerly Kantar) CMAG, a data analytics and consulting firm, and coded by trained undergraduate student coders using an instrument developed jointly by the Wesleyan Media Project and KFF. The KFF analysis includes 1,267 unique ads that aired 643,852 times during the advertising period and focuses mainly on Medicare Advantage ads, the dominant Medicare plan type advertised during the period (see Methods).
Background
Trends in Medicare Coverage
More than 65 million people receive health insurance coverage through the federal Medicare program. Increasingly, this coverage is provided by private companies who contract with the federal government to offer Medicare Part A and Part B covered services (Medicare Advantage or MA), Part D prescription drug plan coverage (PDP), or both (MA-PD). Medicare Advantage enrollment has doubled since 2010, covering over half (31 million people) of eligible Medicare beneficiaries in 2023. Among traditional Medicare beneficiaries, 22 million are enrolled in a stand-alone PDP and most have some form of private supplemental coverage, including more than 14 million who purchase a private Medigap supplement policy.
The growth in Medicare Advantage enrollment is due, in part, to the extra benefits and attractive cost features offered by most Medicare Advantage plans. Virtually all Medicare Advantage plans offer some benefits not included in traditional Medicare, such as coverage of dental, vision, or hearing services. Additionally, unlike traditional Medicare, which places no cap on out-of-pocket spending for hospital or physician services, Medicare Advantage plans are required to set out-of-pocket limits for services covered by Parts A and B. At the same time, Medicare Advantage plans often have restrictions, such as prior authorization and referral requirements, rarely used in traditional Medicare, and most include networks that set limits on which providers enrollees may see. Close to 60% of Medicare Advantage beneficiaries are enrolled in HMO plans that typically do not cover out-of-network services.
Marketing Complaints and Regulatory Response
The report from the majority staff of the Senate Finance Committee documents numerous examples of beneficiary complaints about marketing practices used by Medicare Advantage insurers, as well as brokers and other third-party entities, including false or misleading information about plan costs and available benefits, concerns which have been raised by the National Association of Insurance Commissioners as well. For example, advertisements promising lower Part B premiums or higher Social Security checks were a common source of complaints. States frequently reported incidents in which agents or brokers used this claim to attract potential enrollees, even when advertising in service areas where no such plans were available, or when enrolling beneficiaries in a plan that offered this benefit would be an otherwise poor fit for their needs. In 2023, just 17% of Medicare Advantage plans offer a rebate toward the Part B premium.
Likewise, CMS has raised concerns that the prominent use of the word “Medicare” in company names or headers and images of the Medicare card or logo in print and TV ads creates confusion for beneficiaries and may lead them to believe that these organizations are speaking on behalf of the Medicare program. Focus groups conducted by KFF in the fall of 2022, suggest that beneficiaries find these ads to be misleading, often reporting uncertainty about who had sponsored the ads they saw on TV and whether they were endorsed by the Medicare program or the federal government.
CMS has moved to address these issues in several ways. Regulations that went into effect in June 2022, and apply to all Medicare Advantage and Part D ads discussed in this analysis, broaden the definition of third-party marketing organizations, mandate greater oversight by health insurers of the third parties who represent them, and require third parties to include a standard disclaimer in all communications and marketing materials informing beneficiaries that they do not represent every plan available in their area and advising them to contact official CMS resources for a complete list of their options (though CMS does not specify whether or not this disclaimer may be featured in fine print). In April 2023, CMS finalized additional requirements to address misleading marketing practices that will apply to the upcoming Medicare open enrollment period that begins in October 2023, for coverage in 2024. (See Appendix for details.)
TV Ads For the 2023 Medicare Open Enrollment Period
TV ads for Medicare Advantage often showed images of a government-issued Medicare card or urged viewers to call a “Medicare” hotline other than the official 1-800-Medicare hotline.
Some ads suggested that people with Medicare miss out on benefits to which they are entitled if they are not enrolled in a Medicare Advantage plan.
TV ads sponsored by brokers and other third-party entities used celebrity endorsements more often than health insurers to promote Medicare Advantage.
TV airways were flooded with ads for Medicare plans.
There were 643,852 airings of English-language Medicare ads run on broadcast television and national cable between October 1, 2022, and December 7, 2022, an average of more than 9,500 airings per day, more than were seen for any individual Healthcare.gov open enrollment period between 2013 and 2018. Just over 40,000 Spanish-language airings (not included in our analysis) bring the total number of Medicare-related airings close to 690,000.
Medicare ads were most common during the weekday afternoons. Across the top 20 markets, viewers of programs aired on Fox affiliates saw an average of at least 6 ads per day, viewers of programs aired on ABC and NBC affiliates saw an average of at least 5 ads per day and viewers of programs aired on CBS saw an average of at least 4 ads per day each weekday afternoon between October 1, 2022 and December 7, 2022 (data not shown).
The most common television programs during which Medicare ads were aired included talk shows, reality court shows and game shows. For example, across the top 20 markets, regular viewers of Dr. Phil saw an average of 404 Medicare ads, or 8 ads per day that were directed at the open enrollment period. Regular viewers of Hot Bench saw 336 ads on average, or 7 ads per day, and regular viewers of Family Feud saw 281 ads on average, or 6 ads per day (Appendix Table 1).
Local news broadcasts also often included commercials for Medicare plans. On December 1st, the day with the highest number of airings, a person watching News 5 at 5pm on ABC in Cleveland would have seen nine Medicare ads during the one-hour broadcast. Likewise, a person watching WCCO Mid-Morning on CBS in Minneapolis would have seen seven ads during the hour, and a person watching Eyewitness News 4 at Midday on NBC in Albuquerque would have seen six in the hour (data not shown).
Most Medicare ads aired in local media markets rather than nationally. Of the 643,852 Medicare ad airings analyzed, the vast majority (86%) aired locally, while 14% aired nationally. The targeting of TV ads to local media markets likely reflects a strategy to compete and grow enrollment in specific regions and service areas. (See Appendix for details.)
While health insurers sponsored the majority of Medicare TV ad airings, brokers and other third-party entities had a significant presence, especially with ads that aired nationally. Roughly 73% of all Medicare ad airings (468,808) were sponsored by health insurers, while more than one in five (21%, 135,699) were sponsored by brokers and other third-party entities. Just 3% (18,321) were sponsored by the Department of Health and Human Services or other government agency (Figure 1). Brokers and other third parties relied more on national airings than local markets, accounting for 50% of national airings but just 16% of all local airings.
Roughly 3% (21,024) of all Medicare ad airings did not identify the organization who sponsored the ad. Among national airings, nearly one in ten did not include this information, a pattern that may reflect the larger share of national ads sponsored by brokers and other third parties, who may have less to gain from brand recognition.
TV ads for Medicare Advantage comprised more than 85% of all airings for the open enrollment period for 2023.
Of the 643,852 airings of Medicare ads that ran during the nine-week advertising period for open enrollment for coverage in 2023, 556,068 (86%) promoted Medicare Advantage. Many of these airings also mentioned Part D benefits, but a review of the top 150 most-frequently aired ads (representing more than 80% of all Medicare ad airings) showed that nearly all of these were marketing Medicare Advantage plans that included Part D coverage, rather than offering stand-alone Part D plans as a separate product. Of the remaining 87,784 airings, 7,790 (1%) promoted Medigap plans and 465 (less than 1%) promoted stand-alone Part D plans with no mention of Medicare Advantage. Another 32,692 airings (5%) promoted multiple types of plans, while 46,837 (7%) did not mention any type of plan, instead offering general information on the open enrollment period or counseling on Medicare plan choice (Figure 2).
The emphasis on Medicare Advantage matches trends in Medicare enrollment. As of 2023, just over half of all eligible Medicare beneficiaries receive their Medicare Part A and Part B benefits through a Medicare Advantage plan, a twofold increase in the past decade that has outpaced the more modest growth seen in Medigap enrollment. Likewise, enrollment in stand-alone Part D plans has declined as a growing share of beneficiaries enroll in Medicare Advantage plans that include prescription drug coverage. At the same time, a KFF analysis of private Medicare advertising for the 2008 open enrollment period demonstrated that insurers have devoted the largest share of their advertising resources to Medicare Advantage plans for some time.
The remaining discussion is focused on Medicare Advantage, as these ads made up the vast majority of Medicare ad airings for the open enrollment period.
Four of every five Medicare Advantage ad airings were sponsored by health insurers, with the remaining sponsored by brokers and other third-party entities, such as marketing companies. Among the 556,068 ads promoting Medicare Advantage, health insurers sponsored a majority (79%) of ad airings while brokers and other third-party entities sponsored 19%. The remaining 2% of sponsors were not readily identifiable. Ads sponsored by brokers and other third parties rarely listed the specific Medicare Advantage organizations they represented or the plans they offered, though many advertised specific benefits and plan features that might be available. Brokers may contract with multiple insurers, and offer plans with varying benefits and costs, across many service areas, which may lead to confusion if beneficiaries are unaware which of the plan features advertised are available where they live. Further, brokers have a financial incentive to steer people towards Medicare Advantage plans over other coverage options. In the 2023 plan year, brokers receive $601 per new enrollee in most Medicare Advantage plans, substantially higher than for new enrollees in most Part D plans ($92). Though comparable data do not exist for Medigap plans, brokers report substantially lower commissions for Medigap enrollment.
Though not applicable to these ads, new regulations from CMS came into effect in June 2023 which prohibit brokers and other third parties from advertising specific plans or plan features without clearly identifying the insurers that offer them. Further, all groups are prohibited from marketing benefits in service areas where those benefits are not available (see Appendix for details).
UnitedHealthcare and Humana comprise nearly half of Medicare Advantage enrollment but sponsored just 20% of insurer-sponsored ad airings. Many TV ad airings promoting Medicare Advantage were sponsored by health insurers that enroll a relatively small share of Medicare Advantage enrollees. While UnitedHealthcare and Humana together comprise nearly 50% of Medicare Advantage enrollment in recent years, these two insurers sponsored less than 20% of airings for Medicare Advantage plans. In contrast, three insurers accounted for a larger share of airings than enrollment: Blue Cross Blue Shield affiliates (26% of airings vs. 14% of enrollment), Centene (12% vs. 4%), and Cigna (9% vs. 2%). Roughly one in five airings (24%) came from insurers that account for less than 2% of Medicare Advantage enrollment each, and 16% as a group (Figure 3). Despite rapid growth, Medicare Advantage enrollment remains concentrated among a small group of firms, and insurers with a smaller footprint in the Medicare Advantage market may rely more heavily on TV advertising to promote their plans and expand market share.
TV ads for Medicare Advantage often showed images of a government-issued Medicare card or advertised a “Medicare” hotline other than 1-800-Medicare.
Over one in four ad airings (27%) promoting Medicare Advantage showed a government-sponsored Medicare card or an image that resembled it, and 16% included a phone number other than 1-800-Medicare that was described as a “Medicare” hotline. Both CMS and the Senate Finance Committee have expressed concern that the use of the Medicare name, logo, or card in private marketing materials could confuse beneficiaries and lead them to believe they are contacting an official government resource. New regulations from CMS aim to address this issue by prohibiting the use of the Medicare card, except for educational purposes (see Appendix for details).
The Medicare card or a similar image appears on screen in more than one-quarter of ad airings for Medicare Advantage. Images of the Medicare card, or something that closely resembles it, appeared in more than one-quarter (27%) of all ad airings for Medicare Advantage, including 28% of insurer-sponsored airings and 21% of airings sponsored by brokers and other third-party entities. Some of these framed the screen with a red, white, and blue border that resembles the Medicare card design, in some instances, for the duration of the airing.
Though not applicable to these ads, new regulations, which will apply to the upcoming open enrollment period in October 2023, prohibit misleading use of the Medicare name, logo, or card in private marketing and communication materials, or any use without prior approval from CMS. CMS has stated that it will approve use for educational purposes only, such as a graphic showing beneficiaries how to tell the difference between their federally-issued Medicare card and their insurer-issued Medicare Advantage plan card. However, it is unclear whether images that are similar, but not identical, to a Medicare card will still be permitted in marketing materials, such as the use of a Medicare card design to frame the screen.
Most Medicare Advantage ad airings sponsored by brokers and other third parties featured a “Medicare” hotline that is not the official government-sponsored 1-800-Medicare hotline. A large majority of Medicare Advantage airings sponsored by brokers and other third-party entities (83%) featured a “Medicare” hotline other than the 1-800-Medicare line run by the federal government (Figure 4). These were often described using general names such as a “Medicare Helpline,” “Medicare Benefits Support Line,” or “Medicare Benefits & Questions Line,” with no reference to a specific company name. In contrast, airings sponsored by health insurers rarely included this type of “Medicare” hotline, instead directing viewers to call their own agents (data not shown). Virtually no ad airings promoting Medicare Advantage mentioned 1-800-Medicare, the official Medicare phone number, outside of fine print.
Among airings sponsored by brokers and other third parties, 19% included both an image of the Medicare card and mention of a privately-run “Medicare” hotline, increasing the possibility that beneficiaries will believe that the ad and its contents were sponsored by an official government agency.
VIDEO: Medicare Advantage ads often showed images of a government issued Medicare card or urged viewers to call a “Medicare” hotline other than 1-800-Medicare.
Focus groups conducted by KFF in the fall of 2022 suggest that beneficiaries are often overwhelmed by the volume and complexity of choices available to them, yet few make use of official Medicare resources such as 1-800-Medicare. Airings sponsored by brokers and other third parties often referenced this volume of choices, encouraging beneficiaries who felt “overwhelmed” or “confused” by their coverage options to call their privately-operated “Medicare” hotline for advice.
Under current rules that became effective in June 2022, and are applicable to the period examined, ads sponsored by brokers and other third-party entities are required to include a disclaimer explaining that they do not represent every plan available in a service area and advising beneficiaries to call 1-800-Medicare for a complete list of their coverage options. While this disclaimer was included in the subset of third-party airings we reviewed, it was often shown for just a few seconds or written in small font, potentially making it difficult for viewers to read.
In some cases, ads advised callers against giving their personal information to national hotlines or “1-800 numbers,” suggesting that local experts were more trustworthy. While these messages may be aimed at other broker-sponsored hotlines that operate at the national level, they may also discourage viewers from calling 1-800-Medicare for additional information.
Some ads suggest that people with Medicare miss out on benefits to which they are entitled if they are not enrolled in a Medicare Advantage plan.
More than 50,000 Medicare Advantage ad airings used language that suggested people with Medicare are “missing out” on important benefits if they are not enrolled in a Medicare Advantage plan. Additionally, some ads tell viewers that they are “entitled” to receive supplemental benefits or cost savings offered by some Medicare Advantage plans. Language such as “missing” or “entitled” may give some viewers the impression that they have incomplete coverage or have overlooked a necessary enrollment step if they receive their Medicare coverage from traditional Medicare.
Medicare Advantage plans often include low or $0 supplemental premiums and extra benefits not included in traditional Medicare, such as coverage of dental, vision, and hearing services. The language used in the TV ads refers to these benefits by emphasizing that they are not covered by Medicare Parts A and B, and beneficiaries “do not get these benefits automatically” without enrolling in Medicare Advantage (also referred to as Medicare Part C). For example, some common phrases included:
“It’s a new year, and you may be entitled to new benefits.”
“If you only have Medicare Parts A and B, you may be missing out on extra benefits.”
“That’s right! There are people on Medicare that don’t have a Medicare Part C plan!”
“You are now entitled to eliminate copays.”
This messaging may be especially confusing when paired with references to the Medicare name, logo, or card. Ads with this messaging were more commonly sponsored by brokers and other third-party entities. These third-party sponsored ads also included a privately-run “Medicare” hotline in four out of every five airings, often alongside images of (and references to) the Medicare card. While these references may be intended to alert Medicare beneficiaries that these ads are directed at them, they may lead some viewers to believe the ads were produced by a government source, creating the impression that the government is endorsing the message that Medicare Advantage is “missing” from traditional Medicare coverage.
The vast majority of Medicare Advantage ad airings touted low costs and extra benefits, while few mentioned quality ratings.
More than 90% of airings for Medicare Advantage promoted extra benefits, such as dental, vision, and hearing, and 85% promoted cost features, such as $0 co-pays, no additional premiums, or reductions to the standard Part B premium (Figure 5). A KFF analysis of private Medicare advertising in 2008 also found extra benefits to be the most common message appearing in TV, print, and radio ads for Medicare Advantage.
By contrast, only one in five airings (22%) mentioned plan features that promote flexible access to providers and services, such as nationwide networks and out-of-network coverage, and fewer than 4% made any reference to a plan’s quality star rating.
Ads promoting Medicare Advantage touted a range of supplemental benefits. Mentions of dental, vision, hearing, and prescription drug benefits each appeared in more than 50% of all airings promoting Medicare Advantage. Dental coverage was included in 84% of airings, more often than any other type of supplemental benefit or any cost-related message (Figure 6).
Benefits that may appeal to people in poorer health were marketed substantially less often, including allowances for food or grocery spending (20%), transportation services (20%), and meals (10%), though these were somewhat more common in insurer-sponsored airings than broker or other third-party airings (Appendix Table 2). Other benefits that are valuable to people with serious illnesses or mobility impairments were uncommon regardless of sponsor. Caregiver support, such as respite care or custodial care, was included in just 2% of airings, and bathroom safety devices such as bathtub rails and grab bars were included in less than 1%.
Supplemental benefits are a common feature of Medicare Advantage plans. In 2023, virtually all Medicare Advantage plans offer some supplemental benefits, most often dental, vision, hearing, gym memberships or other fitness benefits, and telehealth services, all of which were offered in at least 97% of available plans. Just 43% of plans included coverage for transportation services, and fewer than 15% included coverage for in-home support services, caregiver support, or bathroom safety devices, consistent with the smaller share of airings that mentioned these benefits.
More than two-thirds of airings sponsored by brokers and other third parties mentioned money back in your Social Security check. Two in three (67%) Medicare Advantage airings sponsored by brokers and other third-party entities included messaging about Part B premium rebates, compared to just 7% of insurer-sponsored airings and 19% overall (Figure 7; Appendix Table 2). While all Medicare Advantage enrollees must continue to pay the Part B premium (or in the case of dual-eligible individuals, have it paid on their behalf), Medicare Advantage plans can offer a rebate against the Part B premium as a supplemental benefit. This is sometimes referred to as the “give back” benefit and results in beneficiaries receiving higher Social Security payments each month.
Airings that included this message often featured endorsements from national celebrities. Joe Namath was featured more than any other celebrity (appearing in nearly 56,000 airings) and mentioned Part B premium rebates in 100% of his appearances.
Few airings, regardless of sponsor, stated that Medicare Advantage enrollees were required to pay the standard Part B premium, which may lead to confusion when plans are advertised as having “no premium.” Frequency of this message could not be measured precisely, due to the very small number of airings in which it appeared (see Methods for details).
Part B premium rebates are less common than many other supplemental benefits, offered by just 17% of plans available in 2023, with an even smaller share of enrollees (10%) opting for plans with this benefit. Though not applicable to these ads, new CMS rules, effective June 2023, prohibit marketing of benefits that are not available in the service area where the ad is aired, which may lead to fewer mentions of this benefit during the upcoming open enrollment period.
Low or $0 supplemental premiums were frequently mentioned among airings sponsored by Medicare Advantage insurers. Roughly two-thirds (66%) of airings promoting Medicare Advantage mentioned low or $0 supplemental premiums. Two-thirds of Medicare Advantage plans available in 2023 do not have a premium (other than the Part B premium) and among all plans the average premium is $15 per month. Mentions of low or $0 premiums were more common in airings sponsored by health insurers (79%) than those sponsored by brokers and other third-party entities (13%) (Appendix Table 2).
By contrast, airings promoting low out-of-pocket spending, including low or $0 co-pays, low cost-sharing, and low deductibles, were common among insurers and third-party sponsors, appearing in half (50%) of all Medicare Advantage airings (Figure 7; Appendix Table 2).
Messages about low premiums were often presented in contrast to the cost of supplemental plans such as Medigap. Traditional Medicare places no cap on out-of-pocket spending for hospital or physician services, and supplement plans can help to insulate beneficiaries from financial risk, but Medigap plans can be costly, with premiums ranging from less than $100 to more than $300 per month. Traditional Medicare beneficiaries may choose to purchase a Medicare supplement to assist with cost-sharing for services covered under Medicare Parts A and B.
VIDEO: Nearly all Medicare Advantage ads touted low costs and extra benefits.
Messages about low out-of-pocket spending sometimes featured estimates of savings that beneficiaries could expect to retain by enrolling in a Medicare Advantage plan. While not applicable to these ads, new regulations from CMS include a prohibition against advertising unrealized “savings” that are calculated relative to the expenses borne by uninsured individuals, the unpaid costs of beneficiaries dually eligible for Medicare and Medicaid, or other unrealized costs of a Medicare beneficiary. According to CMS, these savings estimates can be misleading, as they do not reflect the out-of-pocket costs paid by most Medicare beneficiaries and may give an unrealistic impression of the cost difference between plans.
About one in five Medicare Advantage TV airings emphasized access to doctors. Roughly one in five (22%) Medicare Advantage airings mentioned plan features that reflect flexible access to providers and services, such as promises to “keep your doctor” (14%), nationwide networks (6%), no referrals or pre-approvals for covered services (3%), or coverage for out-of-network providers (1%) (Figure 8). These messages were less common among TV ad airings sponsored by health insurers (13%) than brokers and other third-party entities (59%) (Appendix Table 2).
Health insurers may not choose to advertise access to providers as often as supplemental benefits because most plans employ networks, which place restrictions on which providers enrollees may see or offer more limited coverage for out-of-network services. Further, virtually all Medicare Advantage enrollees are in a plan that requires prior authorization for at least some services.
In contrast, 59% of Medicare Advantage airings sponsored by brokers and other third-party entities include the promise to “keep your doctor” (Appendix Table 2). Many brokers offer a range of plans with different networks, and may feel confident that they can offer a plan that includes a beneficiary’s current doctor, but it is unlikely that most beneficiaries would be able to keep their doctor regardless of the plan they choose. In 2023, 58% of Medicare Advantage plans are HMOs, which typically do not cover out-of-network services
Less than 4% of Medicare Advantage ad airings reference quality star ratings. CMS regularly publishes quality ratings of Medicare Advantage plans to assist beneficiaries in comparing the options available in their area. Plans are rated on a 5-star scale, with 1 star indicating poor performance, 3 stars indicating average performance, and 5 stars indicating excellent performance. While these ratings are intended, in part, to help consumers select a plan, they are very rarely used in TV advertising. Fewer than 4% of Medicare Advantage airings made any reference to a plan’s star rating (Figure 5).
An exception was Kaiser Permanente, which promoted the quality star rating of their plans in 86% of airings, while no other single insurer mentioned star ratings in more than 5% (Appendix Table 3). This may be due to the high ratings received by most Kaiser Permanente plans. Virtually all Medicare Advantage beneficiaries enrolled in Kaiser Permanente were in a plan with a quality rating of at least four stars in 2022, the highest share of any major insurer.
Focus groups conducted by KFF in the fall of 2022 suggest that beneficiaries do not generally take star quality ratings into account when choosing a plan. In 2023, 7 in 10 (71%) Medicare Advantage beneficiaries were enrolled in plans with a rating of 4 or more stars, which may make the rating system less meaningful to beneficiaries looking to distinguish between plans with similar scores. MedPAC has raised concerns about the star rating system in recent years, noting, among other things, that star ratings are reported at the contract rather than the plan level, which may make them less useful to beneficiaries interested in the quality of a specific plan.
Medicare Advantage insurers varied in whether they promoted particular supplemental benefits, the potential for savings, access to providers, or quality most often. Medicare Advantage insurers differed in the plan features they chose to emphasize (Appendix Table 3). UnitedHealthcare, Blue Cross Blue Shield affiliates, and CVS all touted dental coverage more often than any other supplemental benefit, consistent with the overall trend. In contrast, Humana mentioned dental coverage in just 44% of airings, but included mentions of cost features such as low or $0 premiums and low or $0 co-pays in more than 80% of airings. Centene mentioned less common offerings more often than other insururers, including benefits such as meals, transportation, and vouchers for food and groceries or over-the-counter items in more than 50% of airings.
UnitedHealthcare mentioned plan features related to access to providers more often than other insurers, promoting a nationwide network in 27% of airings and lack of referrals or prior authorization requirements in 28% (compared to just 8% and 4% of insurer-sponsored Medicare Advantage airings overall).
Medicare Advantage ad airings often featured active seniors engaged in physical activities, but rarely showed people who appeared to have a serious health problem or visible disability.
Most Medicare Advantage airings (78%) featured people in some capacity. While ads were diverse in terms of the race, ethnicity, gender, and age of people shown (data not shown), people were generally shown to be in good health and free from serious illness. A prior KFF analysis of private Medicare advertising found a similar pattern among print, radio, and TV ads for Medicare Advantage plans in 2008, with one in ten showing seniors engaging in physical sports, just 3% showing people under 65 with a visible disability, and none showing people with visible signs of illness or frailty (such as a walker or a cane).
About one-quarter (26%) of Medicare Advantage airings show seniors participating in physical activity. One in four Medicare Advantage airings (26%) (Figure 9), including 32% of those sponsored by health insurers, showed seniors engaging in some form of physical activity. While some ads featured wellness activities, such as yoga or stretching, others showed seniors engaging in activities that demand much greater health and fitness, such as mountain biking, ziplining, trampoline jumping, and other forms of vigorous exercise. These ads may be targeting healthier seniors who might find these activities appealing or aspirational, and may promote the message that these plans ensure a certain standard of health, but they may also signal to those in poorer health that the plans promoted in these ads are not designed to meet more serious health needs.
VIDEO: Medicare Advantage ads often featured active seniors engaged in physical activity.
Fewer than 5% of airings include a person with a physical disability or someone receiving treatment for a serious illness. People with physical disabilities were shown in less than 4% of airings promoting Medicare Advantage, while just 1% showed a person receiving treatment for serious illness (Figure 9). Nearly all of these airings were sponsored by health insurers, as virtually no airings sponsored by brokers or other third-party entities featured people in either demographic. While this may represent an effort by insurers to associate their plans with good health, this pattern does not represent the demographics of Medicare beneficiaries as a whole. One-fifth (22%) of Medicare beneficiaries are in fair or poor self-reported health, and more than one-quarter (28%) have at least one functional impairment. Among beneficiaries under 65 and living with a permanent disability, these shares are much higher, 57% and 52% respectively.
Just over one-fifth (22%) of Medicare Advantage airings show a senior using technology. One in five Medicare Advantage airings (22%) (Figure 9), including 25% of those sponsored by health insurers, showed seniors using technology such as laptops, smartphones, or tablets. As with ads that show physical activity or exercise, this may be an attempt to appeal to a younger, more engaged group of beneficiaries, rather than those who struggle with serious health issues such as cognitive impairment.
TV ads sponsored by brokers and other third-party entities used celebrity endorsements more often than health insurers to promote Medicare Advantage.
More than half (55%) of all Medicare Advantage airings sponsored by brokers and other third-party entities featured endorsements from celebrities such as actors, athletes, and politicians. Most featured celebrities who were seniors themselves, and virtually all national celebrities featured in these ads were men. In contrast, just 3% of insurer-sponsored ads featured celebrities. Brokers and other third parties may feel more of a need to give viewers a familiar name to catch their attention, while insurers may have more of an interest in establishing their own brand.
Focus groups conducted by KFF in the fall of 2022 suggest that beneficiaries are not swayed by celebrity endorsements and frequently disregard them. Nonetheless, many reported encountering these ads, suggesting that they are memorable, and that celebrities may help draw attention and promote a brand, even if beneficiaries do not regard them as credible.
Joe Namath was featured more often than any other celebrity, appearing in nearly 10% of all Medicare Advantage airings (55,839). One ad in which he appeared aired more often than any other single Medicare ad during the advertising period, and a second was in the top ten, with 41,252 airings and 14,421 airings respectively. No other celebrity appeared in more than 1% of Medicare Advantage airings. Other familiar figures included former sports stars such as David Ortiz, Magic Johnson, and Joe Montana, musicians such as Lionel Richie, politicians such as Mike Huckabee, and popular actors such as William Shatner, J.J. Walker, and William Devane.
VIDEO: Ads sponsored by brokers and other third parties often used celebrity endorsements to promote Medicare Advantage.
Every fall, Medicare beneficiaries are flooded with TV ads during the nine-week marketing period for open enrollment, most of which promote Medicare Advantage plans. The open enrollment period for 2023 coverage saw an average of more than 9,500 Medicare ad airings each day, nearly all of them from health insurers and third-party entities, such as brokers. This volume of advertising has been accompanied by a rise in beneficiary complaints related to aggressive and misleading marketing tactics, leading to heightened attention from CMS, the NAIC, and other policymakers.
New rules from CMS, effective June 2022 and June 2023, aim to address these issues by strengthening oversight of third-party marketing organizations, requiring greater transparency pertaining to the availability of advertised benefits and plan features, and prohibiting the use of certain language and images, such as the Medicare name, logo, or card, in ways that may be misleading to beneficiaries. While not all of these regulations applied to the ads discussed in this analysis, all will be in effect for the open enrollment period that begins in October 2023. Some of the observations described in this report, such as the use of a government-issued Medicare card, which may lead viewers to think the ads are sponsored by the government rather than a private company, may occur less frequently, if at all, in the future. While the new rules may address some concerns about aggressive and misleading marketing tactics, ongoing monitoring and resources independent of commercial interests could help to improve beneficiary decision-making.
Few if any ads mentioned the traditional Medicare program, the alternative to private Medicare Advantage plans, except in the context of the small number of ads promoting supplemental coverage, such as Medigap and stand-alone Part D plans. This is not surprising, since TV ads are sponsored by health insurers and brokers selling private plans, although it may leave beneficiaries without a clear understanding of their coverage options, and the tradeoffs that arise from one choice over another. Many beneficiaries may find it helpful to have support when making decisions about their Medicare coverage, including from financially disinterested sources such as State Health Insurance Assistance Programs, Social Security Administration district offices, and 1-800-Medicare. A recent survey found that many people age 65 and older would like to know more about the out-of-pocket costs and benefits of their Medicare coverage options and felt that they would benefit from one-on-one help. Adequate resources to meet the demands for assistance – beyond brokers, who have a financial interest in steering people to certain options — may help ensure Medicare beneficiaries are choosing the coverage option that best meets their needs.
Appendix
Additional Data and Figures
Time Slots, Concurrent TV Programs, and Broadcast Networks of Medicare Ad Airings: Medicare advertisements appeared at all times of day, and throughout the week, but airings were most frequent on weekday afternoons (24%), weekday mornings (19%), and in the hours leading up to prime time (16%). Airings were most often shown during local news broadcasts (data not shown), while court shows, game shows, and talk shows were among the top single programs during which Medicare ads were aired (Appendix Table 1). The largest number of airings appeared on the four major broadcast networks: the Fox Broadcasting Company (16%), the American Broadcasting Company (ABC) (16%), Columbia Broadcasting System (CBS) (15%), and the National Broadcasting Company (NBC) (14%). Local advertising was more concentrated in some areas than others, with the top 20 local media markets comprising 27% of all local airings (Appendix Figure 1).
Common Messages Featured in Medicare Ad Airings by Sponsor Type and Insurance Firm:
CMS Regulations
Rules Effective June 2022:Current rules from CMS, which came into effect in June 2022 and applied to all Medicare Advantage and Part D ads discussed in this analysis, include several changes aimed at tightening oversight of third-party marketing activities. The rules introduce a broad definition of third-party marketing organizations, encompassing all organizations and individuals paid to perform lead generation, marketing, sales, or enrollment functions on behalf of a private Medicare plan, either directly or indirectly through another third party.
Health insurance companies that offer Medicare plans are now responsible for ensuring that third-party marketing organizations adhere to any CMS requirements that apply to plans themselves (previously only required for direct contractors). In the context of TV advertising, some examples include existing rules that forbid ads from using the term “free” to describe a $0 premium, implying that a plan is recommended or endorsed by CMS or another government office, or implying that a plan is only available to seniors rather than all eligible Medicare beneficiaries. Health insurers are also required to add certain monitoring and oversight provisions to any direct contract with a third-party marketing organization, and keep track of any downstream relationships that organization is using to represent their plans.
Finally, third-party marketing organizations are now required to include a standardized disclaimer in all communications and marketing materials informing beneficiaries that they do not represent every plan available in their service area and encouraging them to contact Medicare.gov or 1-800-MEDICARE for a complete list of their options.
Rules Effective June 2023:Additional rules from CMS, which came into effect in June 2023 and will apply to the upcoming open enrollment period that begins in October, introduce several more provisions aimed at curtailing misleading marketing practices. While some of these provisions go beyond the scope of TV advertising, several will have a direct impact on TV ads in the fall and in future periods.
Ads are now prohibited from mentioning any benefits or plan features that are not available in the service area where the ad appears. Ads that air in media markets that cross multiple service areas are required to list which benefits apply to each service area (Medicare Advantage and Part D service areas are defined at the county level). The Washington, DC market, for example, includes not only DC itself but also surrounding counties in Maryland and Virginia, representing several distinct service areas for which an insurer may offer plans with different premiums, cost-sharing, and benefits.
Ads are also prohibited from using the Medicare name, logo, or card in ways that could be misleading to beneficiaries. Any use requires prior approval from CMS, and CMS has stated that it will only grant this approval in cases where it is serving an educational (as opposed to marketing) purpose. CMS defines marketing as any material or activity that meets certain standards for both intent (to influence enrollment decisions or draw attention to plans) and content (any mention of specific plan features such as benefits, costs, or quality rankings), standards which would likely apply to any ad targeting open enrollment.
Third-party marketing organizations, such as agents and brokers, are prohibited from advertising specific plans or plan features without identifying the Medicare Advantage organizations or Part D sponsors that offer them. CMS requires these names to be displayed in the same font size, or read at the same pace, as any benefits included in the ad. Third parties are prohibited from airing ads without the plan sponsors promoted in the ads agreeing to their content, and sponsors may be subject to penalties for endorsing ads that do not comply with CMS regulations.
Additional regulations include prohibiting the mention of unrealized “savings” calculated relative to the expenses borne by uninsured individuals, the unpaid costs of beneficiaries dually eligible for Medicare and Medicaid, or other unrealized costs of a Medicare beneficiary; prohibiting the use of superlatives such as “best” and “most” in marketing materials, taglines, or logos; and revising the disclaimer required for all third-party ads (described in the section above) to include State Health Insurance Assistance Programs (SHIPs) alongside Medicare.gov and 1-800-MEDICARE as a resource that beneficiaries can turn to for more information about their coverage options.
File & Use: Health insurers and third parties must submit all marketing materials to CMS for review before they can be aired, or in the case of some third parties, have them submitted by the insurer they represent. Until recently, CMS permitted TV ads to be submitted through its File & Use framework. Materials designated as File & Use may be aired five days after submission to CMS, though CMS reserves the right to review these materials for compliance both during and after this five-day window. Marketing materials that do not qualify for File & Use must be submitted forty-five days before they are aired, prospectively approved or disapproved during this timeframe, or “deemed approved” if no decision is reached within forty-five days. Beginning January 1st, 2023, in light of ongoing concerns, CMS no longer allows TV ads to be submitted as File & Use. Ads slated to air on October 1st, 2023 must be submitted to CMS by mid-August, allowing a longer window for prospective review.
Methods
Our data consist of 1,267 unique ads and 643,852 total airings, representing all English-language TV ads focused on Medicare that aired on broadcast television or national cable between October 1st, 2022 and December 7th, 2022. While the open enrollment period does not begin until October 15th each year, sponsors are permitted to advertise beginning October 1st. Ads were supplied to the Wesleyan Media Project by Vivvix (formerly Kantar) CMAG along with additional information on the timing of the airing, the media market, TV station, and broadcast network where it was aired, and the TV programming shown on the same station during that time slot. The Wesleyan Media Project compiled and processed all data flagged by Vivvix CMAG as relevant to our study, including ads classified as “Medical & Dental Insurance” or “Insurance Agencies & Brokers,” ads sponsored by the Department of Health and Human Services or AARP, and any ad with Medicare in the title.
In the first phase of processing, the Wesleyan Media Project used optical character recognition (OCR) to extract the textual information on screen and automatic speech recognition (ASR) to extract the audio into text for each video. Ads that did not contain the word Medicare in either OCR or ASR were removed from the set. The Wesleyan Media Project then assessed the degree of text similarity from the ASR data to identify advertising that was greater than 90% matching in audio content. Ads with 90% or higher similarity were grouped and only one ad per group was flagged for human coding (described below), along with any ads that did not match with others. Finally, the Wesleyan Media Project identified and removed Spanish-language advertising that ran on Spanish-language networks Telemundo, Unimas, and Univision. A secondary step to filter out Spanish-language advertising was conducted in the human coding stage. This left us with a final analytical set of 1,267 unique ads.
KFF and the Wesleyan Media Project then developed a coding instrument to analyze ad content. Key variables included in the instrument were those relevant to the evolving policy context surrounding Medicare marketing, such as the sponsor, Medicare products, and plans represented in each ad, as well as messaging on plan features, slogans or repeated phrases, activities and characteristics of people shown in the ad, websites and contact information, and use of the Medicare name, logo, or card.
Ten undergraduate student coders received training and completed four sets of practice ads prior to beginning live coding. A random sample of ads (20%) were double coded to assess intercoder reliability, and all Krippendorff’s alpha statistics were calculated for each variable. All results described in this report all met the 0.7 threshold for acceptable levels of reliability, with some exceptions noted below. For ads that included fine print, coders were asked to indicate whether they could read the fine print without pausing. While coder impressions are noted where relevant, this variable is not scientific, as monitor sizes vary, which affects readability. Coders were also asked to flag any ads that stood out to them as surprising, misleading, or notable in some other way and offer their qualitative impressions.
KFF analyzed the frequency of ad characteristics in the data as a whole, as well as by sponsor type, advertised product, and media market. Insurer sponsored ads were also analyzed by firm. KFF further reviewed a sample of ads in their entirety, including ads for which coders had given qualitative comments, to identify relevant examples of common messages, elements, and themes. Messages related to in-home support services, caregiver support, and bathroom safety devices were categorized as “other supplemental benefits” by our coding instrument. These were identified by coders in a free text field and reviewed by KFF as described, but were not formally assessed for intercoder reliability. Likewise, some characteristics, such as the message that beneficiaries were required to pay the standard Part B premium, appeared too rarely to meet the 0.7 threshold for acceptable intercoder reliability. In these cases, we noted that the characteristic was rare, but were not able to report its frequency with precision.
We focused much of our analysis on the substantial majority of ads promoting Medicare Advantage, the most common product advertised during the period.
Medicare is the federal health insurance program that covers over 65 million adults 65 and older and younger adults with long-term disabilities. Medicare is a very popular program, with 81% of the public holding favorable views of the program, and is viewed positively by large majorities of Democrats, Republicans, and Independents.
Over the past 15 years, the role of private plans in Medicare has increased dramatically. Today, more than half of all Medicare beneficiaries are enrolled in a Medicare Advantage plan, with an average of 43 plans to choose from in addition to traditional Medicare. Beneficiaries in traditional Medicare can choose among 24 stand-alone Part D plans, on average, and may choose supplemental coverage, such as Medigap, if they don’t have supplemental coverage under Medicaid or an employer or union-sponsored retiree health plan. This increasingly crowded marketplace has been accompanied by extensive marketing and advertising as well as agents and brokers competing to attract enrollees.
To capture Medicare beneficiaries’ views and experiences in choosing between traditional Medicare and private plans, and among private plans, and the factors that influence these decisions, KFF worked with PerryUndem to conduct focus groups with Medicare beneficiaries in the Fall of 2022, during the annual Medicare open enrollment period. This report summarizes first-hand accounts of participants’ reactions to phone calls, TV advertisements and other marketing activities they encounter during the open enrollment period, what influences their decision-making, including the role of licensed agents (also known as brokers), how much Medicare beneficiaries understand about their Medicare choices, what they think of the Medicare marketplace, and how well their Medicare coverage is working for them.
The focus group participants included Medicare beneficiaries ages 65 and older and younger adults with disabilities who make health coverage decisions for themselves and/or their spouse or family member. Some focus groups also consisted of people with both Medicare and Medicaid (also referred to as dual-eligible individuals or dual eligibles) as well as adults 64 years old who were approaching Medicare enrollment. Because the study focused on decisions pertaining to Medicare coverage, including Medicare Advantage and traditional Medicare supplemented by Medigap, we excluded people on Medicare with retiree coverage from a former employer or union.
Key Takeaways
Many participants reported experiencing aggressive marketing tactics pushing Medicare plans, including unsolicited phone calls. Many participants reported getting frequent phone calls from brokers or plan representatives advertising Medicare plans, though it was not always clear to participants who was calling.
Nearly all participants have seen TV advertisements that are marketing Medicare, most frequently Medicare Advantage plans. Participants reported they were often confused about who was sponsoring the ads. Some participants emphasized that who was sponsoring the ads was often unclear, noting many of the ads had the appearance of being sponsored by the government though they believed the ads were in fact sponsored by private companies.
Participants did not trust the content of the ads, particularly the ones that marketed a slew of “free” benefits. In general, many thought TV advertisements were misleading. Celebrities are often spokespeople for these advertisements, though participants did not seem to be swayed by them. Overall, participants said that Medicare private plan marketing and advertising did not play a role in their plan choices.
Most participants found the process of selecting their coverage to be confusing, difficult and overwhelming. As a result, many participants relied on a broker to assist them when choosing their coverage and valued their expertise. Participants who use brokers to help select and enroll in a Medicare plan say brokers are a trusted resource. Most of the participants who used brokers did not seem bothered by potential financial incentives to enroll them in a certain plan.
Few participants used government resources when making coverage decisions, such as the Medicare Handbook or 1-800 Medicare, but those participants who did use these government resources generally found them helpful. Most participants had not heard of or used State Health Insurance Assistance Programs (SHIPs), which provide local and objective insurance counseling to people on Medicare.
Focus group participants highlighted a number of factors that were important in choosing their coverage when they first enrolled in Medicare, including premiums and out-of-pocket costs, access to specific doctors, availability of extra benefits, and coverage of prescription drugs. Some participants who are enrolled in Medicare Advantage plans also said they enrolled in a particular plan because its name was familiar or because the company had a good reputation. Participants generally did not take into account Medicare’s star quality ratings of plans to inform their plan choices, though some did their own research on a plan’s quality using non-government resources.
Most focus group participants – whether in traditional Medicare or Medicare Advantage – said they were relieved to get on Medicare and are satisfied with their coverage.However, some participants cited specific issues with their coverage that varied based on their source of Medicare coverage.
Participants with traditional Medicare and a supplemental Medigap policy are generally pleased with their coverage, including low or no cost-sharing for Medicare services, protection against catastrophic expenses, broad access to providers since virtually all physicians take Medicare and Medigap, and feeling that have control over their health care, but some expressed concern about the cost of Medigap premiums.
Participants in Medicare Advantage are also generally satisfied with their coverage because of the zero or low premiums, and extra benefits offered by their plan, such as dental, vision, and hearing services, but some encountered high medical bills when using certain services, faced delays in care, such as having to wait weeks to see specific physicians due to prior authorization and referrals, and had issues in accessing preferred doctors due to network restrictions.
Dual-eligible participants – whether they had Medicare coverage through traditional Medicare or a Medicare Advantage plan – also reported being generally satisfied with their coverage, particularly due to the low out-of-pocket costs for their health care, such as no copays for doctor’s visits. However, some-dual eligible participants with Medicare Advantage had issues finding providers, such as primary care doctors, who would take both their Medicare and Medicaid coverage.
Participants enrolled in Medicare Advantage, including some dual-eligible individuals, also noted difficulty using some of their supplemental benefits, particularly dental benefits, due to network restrictions and certain providers not taking their coverage.
Participants in Medicare Advantage and Medicare Part D stand-alone drug plans reported being frustrated at the high out-of-pocket costs of some of their prescriptions.
The majority of participants do not review their coverage options every year, and even fewer switched plans because they felt they would not be better off with a different option. Participants generally feel they made the right choice – whether in traditional Medicare or Medicare Advantage – when selecting their coverage and feel it is working well enough for them. Therefore, participants do not see the need to look again at their coverage options; however, many wish they had had more information before enrolling.
Some participants with both Medicare and Medicaid were concerned about losing their Medicaid coverage, and were anxious about losing Medicaid during the redetermination process as states resume disenrollments after a three year pause during the pandemic.
This work was supported in part by the AARP Public Policy Institute. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Report
Introduction
The Medicare plan landscape has transformed markedly in recent years, with more than half of all Medicare beneficiaries enrolled in Medicare Advantage plans. When Medicare beneficiaries first enroll in Medicare and during the annual open enrollment period, they can choose traditional Medicare or enroll in a Medicare Advantage plan. If Medicare beneficiaries select traditional Medicare, they may also need to purchase a stand-alone Part D prescription drug plan (PDP), and potentially a supplemental Medigap plan, which fully or partially covers Part A and Part B cost-sharing requirements. In lieu of traditional Medicare, beneficiaries can get coverage through private Medicare Advantage plans, which are mainly HMOs and PPOs, that provide all Medicare Part A and B benefits, often for no additional premium for plans open for general enrollment (other than the Part B premium), typically include Part D drug coverage, and may cover other benefits such as dental, vision, and hearing. Some people with Medicare may otherwise receive supplemental coverage through an employer retiree health plan or Medicaid, which may supplement either traditional Medicare or a Medicare Advantage plan.
Dozens of private Medicare Advantage and Part D drug plans are available to people on Medicare. With a large number of plans and coverage options to review, beneficiaries have a myriad of choices to make when they enroll in the Medicare program, particularly as there may be tradeoffs for each of these decisions. For example, Medicare Advantage plans typically have lower premiums compared to traditional Medicare plus a Medigap policy and have extra benefits that traditional Medicare does not cover, such as dental, vision, and hearing. However, Medicare Advantage plans have limited provider networks and apply cost management tools such as prior authorization, which traditional Medicare does not.
Both people in Medicare Advantage and traditional Medicare also make choices about their prescription drug coverage, which can vary across numerous domains, including premiums, cost sharing, formularies, and pharmacy networks, among others.
Further, each year, plans may change their premiums, benefits, and other features, and beneficiaries have the opportunity to assess these changes and switch plans during the annual open enrollment period. At the same time, people with Medicare are often inundated with marketing and advertisements for private Medicare plans – typically Medicare Advantage plans – which can add to the complexity of decision-making around Medicare choices.
KFF research has shown, however, that few beneficiaries revisit their coverage decisions each year to determine which option is best for them based on their individual needs and the specific features of the plans available to them, and few change their coverage at all: during the open enrollment period for 2020, 10% of Medicare beneficiaries with Medicare Advantage switched plans. This could be because beneficiaries are satisfied with their current coverage selection, but also may also speak to the challenges of understanding and comparing the multitude of plan options.
To better understand Medicare beneficiaries’ experience with the Medicare program, how they make their Medicare coverage choices, the factors that influence these decisions, including the role of marketing and brokers, and whether they reconsider their plan choices, KFF worked with PerryUndem to conduct a series of focus groups to provide insight on these issues (see Appendix for more details on focus groups).
Perspectives from Beneficiary Focus Groups on Medicare Coverage, Marketing, and Plan Choice
Focus group participants said they were inundated by Medicare marketing, including unsolicited phone calls and TV ads, and believed the ads were often misleading and deceptive
Participants generally feel they made the right choice when selecting a plan, and most participants have not revisited their plan choices
Experiences Unique to Dual-Eligible Participants
Dual-eligible participants had varying experiences signing up for Medicaid coverage with some participants choosing coverage and others being assigned their coverage
Focus Group Participants Said They Were Inundated by Medicare Marketing, Including Unsolicited Phone Calls and TV Ads, And Believed the Ads were Often Misleading and Deceptive
Private Medicare plans are allowed to engage in a variety of Medicare marketing and communication activities, including over the phone, on television, and in-person, as long as they adhere to the Centers for Medicare & Medicaid Services (CMS) rules and regulations. However, there has been concern over misleading and deceptive marketing tactics by private Medicare plans as well as third-party marketing organizations who work for these plans. For example, CMS has seen a substantial increase in beneficiary complaints in recent years – they received more than twice as many beneficiary complaints related to marketing in 2021 (~40,000) compared to 2020 (~16,000). In response to these and other concerns, CMS finalized new marketing regulations in May 2022 and in April 2023 to help protect Medicare beneficiaries who are looking for Medicare coverage.
Focus group participants were asked to provide their reactions to Medicare marketing and advertising, including over the phone and on television, whether they could tell who was sponsoring these calls or ads, what they thought about the messaging, how they felt about celebrity spokespeople in many of the ads, and if any of these communications played a role in their Medicare choices. Dual-eligible participants had similar reactions to those enrolled only in Medicare.
Unsolicited phone calls
Many participants reported getting frequent unsolicited phone calls advertising Medicare plans. Participants said marketers promoting these plans used deceitful tactics, and participants usually ignored these calls.
For marketing solicitations over the phone, private Medicare plans are subject to a number of requirements and are not permitted to use telephone solicitation (that is, cold calling), as well as robocalls, text messages, or voicemail messages if unsolicited. However, a recent report from the majority staff of the Senate Finance Committee documented robocalls, telemarketing, and frequent phone calls as a common source of complaints among Medicare beneficiaries. Most focus group participants mentioned receiving unsolicited phone calls from marketers, some of whom were calling from insurance plans or were brokers or agents representing these plans, but many participants said it was not always clear who was calling.
“But lots of phone calls…but you know they are scam when they are coming in with a different number…faking to be from Cisco, T-Mobile, from AT&T, but when you pick up the phone they’re talking about Medicare…I get about eight of those calls a day.”
71-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy (San Jose, CA)
“They called me from a lot of (insurance) companies at that time and you don’t know if they are good or bad, to tell you the truth. They offer so much that you don’t know if it’s true, so I kept (my same) insurance.”
“I have had a lot of (marketing) calls, a lot of calls, but I don’t listen to them…The Medicare office doesn’t call you on the phone. They are fake to me. -68-year-old, female, Spanish speaking, Medicare Advantage Beneficiary”
“The issue is how you got to pick and choose and research, and then you get all these phone calls every day for the last two years from Medicare, Medicare, we’re Medicare specialist, we’re Medicare specialist”
61-year-old, female, Proxy on Behalf of Medicare Advantage Beneficiary (Petersburg, VA)
“They blow up my phone, too. And that’s really annoying. The Medicare Advantage insurance people. They constantly blow up your phone trying to; I don’t know if they’re trying to sell you a plan or exactly what they do. Or I don’t know if maybe, now that you mentioned…, a broker, maybe that’s what they are, but they’re constantly calling my phone. I get calls from all over the country and every time I answer the phone it’s somebody about Medicare Advantage, Medicare Advantage Plan”
56-year-old, female, Dual-Eligible Individual in Traditional Medicare (Benson, NC)
Confusion about TV ad sponsors
Nearly all participants have seen TV advertisements that are marketing Medicare, most frequently Medicare Advantage plans. However, many participants emphasized they were often confused who was sponsoring the ads and that many ads had the appearance of being sponsored by the government though they believed the ads were in fact sponsored by private companies.
One area of particular concern to CMS has been the use of the Medicare name and logo to give the appearance that advertisements or communications are being sponsored or endorsed by the Medicare program or the federal government, when they are actually sponsored by private Medicare plans or by representatives acting on behalf of these plans. The recent Senate Finance Committee majority staff report has also documented similar beneficiary complaints that highlight confusion over what is truly official correspondence and advertisements from the government. Likewise, a KFF analysis of Medicare TV advertising found that more than one in four ads aimed at the most recent open enrollment period, in the fall of 2022, included a government-issued Medicare card or an image that closely resembled it.
In order to address this issue, CMS has finalized changes to this type of marketing, which would prohibit the use of the Medicare name, CMS logo, or official products, including the Medicare card, in a misleading manner. Similar to these complaints, focus group participants also expressed confusion over who was sponsoring some of the ads. Many participants noted that the ads were clearly designed to give the impression they were coming from the government when they believe these ads were fact sponsored by private companies.
“…There is downright fraudulent stuff going on of people pretending to be part of the government…The Medicare hotline, the Medicare helpline; none of these people are from the government”
70-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy (Cleveland, OH)
“I’ve noticed that on the ads, they say you might get more money from Social Security if you apply for their coverage. And at the bottom of the screen, in small writing, they’ll tell you this is not a government offer.”
75-year-old, female, Traditional Medicare Beneficiary (Las Vegas, NV)
“(It’s not always clear who is sponsoring the ads), no, because I think sometimes the impression is that the ad is actually coming from the Social Security office or from Medicare or from the government, and I think some of them are designed that way.”
“(I have seen ads) for Medicare but I have read it but there is really small print that it says, this doesn’t have to do with Medicare. It has the Medicare name, but their identity doesn’t have to do with Medicare.”
One of the most common complaints among participants about TV marketing is that they often advertise that services and benefits are “free”, though this is not always true.
In many of the focus groups, participants mentioned their Medicare Advantage plans come with zero premiums and copays and access to many extra benefits, some of which give them additional money to spend, such as money for over-the-counter items. A KFF analysis of Medicare TV advertising aimed at the most recent open enrollment period, in the fall of 2022, confirmed that messaging about extra benefits was included in more than 90% of ads, while messaging about the potential for lower out-of-pocket costs was present in 85% of Medicare ads. Despite the fact that some beneficiaries report receiving these types of benefits at no cost, nearly all participants, regardless of the Medicare coverage they have, do not trust the content of these type of ads and are inclined to ignore it.
“Mine isn’t free, so even for my hearing aids, even though I appreciate that, I didn’t have to pay the whole $2,500, I still had to pay a copay of $500 to get my hearing aids. And I appreciate the fact that I didn’t have to pay the $2,000. The fact that, you know, I have the other copay with other issues, visits or prescriptions, I am greatly appreciative that I have the opportunity to be able to do so. But,…it’s not free. Silver Sneakers is free.”
“They’ll tell you no costs to have Medicare Advantage, but they don’t tell you that there’s copays…here’s limitations on where you go. All sorts of stuff that comes along with it, but you don’t pay a monthly fee. And that drives a lot of people to areas that’s not to their advantage, let’s put it that way.”
70-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy (Cleveland, OH)
“They try to tantalize you with some free bonus and then it feels like a scam.”
64-year-old, female, Shopping for Medicare (Lake Tahoe, CA)
“I was just going to say that they offer things like…free rides to appointments, free meals, free this, free that, and none of it’s actually true…Just give it to me straight and upfront and be honest you know and that’s one of the biggest reasons why I don’t even pay attention.”
56-year-old, female, Dual-Eligible Individual in Traditional Medicare (Benson, NC)
Participants feel inundated by TV ads
In general, participants feel inundated by TV ads. Most find them off-putting, misleading, and unhelpful, and say the ads did not influence their Medicare plan selections.
“I think some of them are misleading. It just seems to me that there should be more education for the consumer because some of these ads are so misleading. I don’t have any increased appreciation of the plan if there’s a celebrity endorsement. They can afford it.”
“I just want to say I find them (TV ads) very misleading, but because our Medicare and Medicaid systems in this country are so confusing to people that it’s easy to be misled by those ads. You know, I mean if it wasn’t so complicated to begin with, people would know that these ads are bogus.”
56-year-old, female, Dual-Eligible Individual in Traditional Medicare (Benson, NC)
“This is a serious subject. You know my health, our health and our well-being is the most important thing in the world, especially as we get older. And they make it all a big joke…and it grates on my nerves because they’re sing-songy, make a joke out of everything about this. It’s not a joke, it’s serious.”
60-year-old, female, Dual-Eligible Individual in Medicare Advantage (Largo, FL)
“We’re overrun with these commercials and, you know they just say the same thing over and over again you know, call this, call this. But it’s really, it’s kind of a comedy watching these commercials now about these, because they’re jokes. I mean to me they’re jokes… I mean the way they have it advertised it’s not really explaining anything.”
63-year-old, female, Dual-Eligible Individual in Traditional Medicare (Cleveland, OH)
Celebrity spokespeople
While celebrities are often spokespeople for Medicare Advantage plans, participants did not seem swayed by them and frequently disregarded them.
KFF analysis has found that celebrity endorsements are commonly featured in TV ads for Medicare Advantage, appearing most often in ads sponsored by brokers and other third-party organizations, such as marketing firms, who may contract with insurers to promote plans and boost enrollment. Participants reported encountering these ads but most did not find the endorsements helpful or persuasive.
“I saw one with the guy that played J.J., and I just thought, where has he been all of these years? I mean, I got nothing from it…I wasn’t in the market for it, I already had my plan, so it was just comical.”
66-year-old, female, Traditional Medicare Beneficiary with a Medigap Policy (Newport News, VA)
“I just think it’s comedy hour, because I think it’s some celebrity that’s trying to get a check”
“I think that some of (the sponsors) are very obscure. Like the celebrity ones, you really don’t know who the heck is they’re pushing there, to be quite honest.”
70-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy (Cleveland, OH)
“…I see them (ads) all the time but they kind of just come in one ear and out the other. Kind of yeah, like I’ve noticed J.J. Walker and the only thing that’s coming to my mind is God, man he looks good since “Good Times” that’s all I’m thinking.”
48-year-old, male, Dual-Eligible Individual in Traditional Medicare (New York City, NY)
Participants Found Selecting Medicare Coverage Overwhelming and Relied on Brokers to Assist Them with Their Choices While Few Used Official Medicare Resources
The average Medicare beneficiary has an average of 43 Medicare Advantage plans to choose from and 24-stand-alone prescription drug plans to choose from. Most participants said they were surprised to hear that was the average number of coverage options available and were overwhelmed at the idea of having to sort through so many plan options.
Many find the process overwhelming
Most participants said the process for selecting a plan was overwhelming and confusing to navigate. Some did try to sort through plan options themselves, but emphasized the process was challenging.
“There’s no getting around it, it’s a difficult decision because not only do you have those plans, but in each one of them there are so many different parameters that you need to look at… You’ve got the copay, you’ve got the premium, you’ve got the out-of-pocket max. I mean, I do it like I do everything else in my life, I build a spreadsheet. I have 15 or 20 columns of what’s important to me, and I could make it 50 column because there’s 50 different parameters you know, in each that you could look at. And so, it’s a little bit difficult and actually the Medicare or Social Security website is helpful, but if you really want to get to the details, you end up having to navigate out of it to get to the provider site…if you want to see the specific details like of dental coverage, how much is your allowance and all of that stuff, etc.”
“…It gets confusing after a while especially when you’re trying to do it looking at a book or looking on screen, it gets confusing when you’re trying to compare. And I just, you know, it’s just hard to understand to begin with, but it’s really hard when you’re trying to compare plans different plans and what they offer.”
“You got to do too much reading the fine print to find out what is covered, and what you’re going to get, and it’s really depending on what your illnesses are, say what your conditions are, if you have any condition, how you pick what’s going to be the best plan for you.”
61-year-old, female, Proxy on Behalf of Medicare Advantage Beneficiary (Petersburg, VA))
Use of Medicare insurance brokers
For this reason, many participants have used a broker at some stage to assist them when choosing their plan, and many found them helpful in sorting through the enrollment process. Many brokers were recommended by a friend or family members. For people who use brokers, they are seen as a trusted resource.
Many participants, including some dual-eligible individuals, relied on brokers to help narrow down their plan options. Medicare insurers contract with brokers to solicit and enroll beneficiaries in their plans, and in return, the brokers receive a commission from the insurer. Research has shown that people who received help making decisions about their Medicare coverage most commonly turned to brokers to help them compare and narrow down their Medicare plan options, and the focus group participants generally confirmed this trend.
Participants who used brokers said they liked that brokers simplify shopping, can ensure they choose a plan with their preferred providers, and can help navigate whether a plan covers their prescriptions. When dual-eligible participants used brokers, it was generally to help them choose a Medicare Advantage plan. In many cases, brokers were recommended to them by family and friends, who reported being happy with their plans, so participants see brokers as a trusted resource.
“If I had to do it myself, I would say very hard. But since I was blessed to have an agent to come and sit down and talk to me, and give me several plan options and go over with me what was there, and the physician that was in the plan that I chose, it made a world of difference.”
“Like I said, I went to a broker. And he told me look close, this is what you get, that’s what covered. Then he went through, I think, five programs. And I went to them, and I was thinking about it, and I decided to go with Medicare Advantage. And I trusted him, also, the broker, because he did it for some friends of mine and they were very happy with him”
“He wasn’t trying to force to sell me anything, he tried to give me the best plan for me, that fit my budget. Because a lot of times you get people that try to up-sell you stuff and I didn’t get that impression from him. And then he just cut out a lot of the excess fat, answered the questions I wanted.”
“I work with an agent that helps me and when I get dissatisfied I just call him up and say, we need to start looking again. And then he’ll sit down with me and, you know tell me like; okay you can with this company you can keep your rheumatologist. With this company you know, you can keep your oncologist. With this company you can keep your hematologist. And you know, whatever’s most important. I mean like for me it’s certain doctors are more important than others for me to keep. Because I bond with them and I trust them. So I couldn’t do this alone, honestly, it would make me nuts trying to figure this out without a broker, without an agent.”
60-year-old, female, Dual-Eligible Individual in Medicare Advantage (Largo, FL)
Beneficiaries not bothered by commissions that brokers received
Most of the participants who used brokers did not seem bothered by potential biases or financial incentives to enroll them in a Medicare Advantage plan and relied on their advice.
Medicare brokers receive a commission for enrolling beneficiaries in plans, whether they are for Medicare Advantage, stand-alone Part D plans or supplemental Medigap plans. Yet, researchhas shown that brokers tend to be paid more for enrolling beneficiaries in Medicare Advantage plans rather than Medigap plans, which could create conflicts for brokers who may have an incentive to recommend one type of plan over another based on their potential compensation rather than the needs of the beneficiary. In general, beneficiaries did not seem to be aware how brokers were paid – that they might be paid by a specific insurer or receive different fees for separate products. For example, in 2020, Medicare Advantage commissions were $510 nationally, while commissions were $322 for a Medigap supplement and $78 for a Part D plan, a total commission of $400 for Medigap plus a Part D plan. However, when asked if they had concerns about any potential biases or conflicts of interest, beneficiaries did not seem bothered by the commissions that brokers received as long as they felt they were getting good recommendations on their plan options.
“It doesn’t affect me that the agent makes more money recommending Medicare Advantage. I prefer for people to make their money, but I also like it because they come and explain everything as they should, so you understand it better.”
“Not in my case…He was a friend, but he took the information that I was giving him, for him to find the best plan for me. And I already knew that I wanted an Advantage Plan, so for my case…personally I don’t care what they get paid as long as I get what I need for me.”
71-year-old, female, Medicare Advantage Beneficiary (San Diego, CA)
“[Their commissions don’t] bother me because I don’t care what they’re getting paid as long as I’m getting what I’m asking for.”
64-year-old, female, Shopping for Medicare (San Antonio, TX)
Few have used official Medicare information resources
Few participants have used Medicare’s official information resources such as the 1-800 Medicare toll free number, the Medicare.gov website, and the Medicare & You Handbook that is provided each year to all Medicare beneficiaries, though for the few who did, some found these resources helpful.
Medicare has official information resources beneficiaries can turn to help with their coverage decisions, including the 1-800 Medicare toll free number, the Medicare.gov website, including the Medicare Plan Finder, and the Medicare & You Handbook. KFF research has shown that these resources are not widely used, and focus group participants generally confirmed this. Participants who used these resources, however, said the resources were mostly helpful and felt they could get answers to important questions, although some participants thought the toll-free phone number, in particular, was too slow. Further, most focus group participants had not heard of or used State Health Insurance Assistance Programs (SHIPs), which provide local, in-depth, and objective insurance counseling to people on Medicare.
“It was easy (to go to the Medicare website). In fact, I even looked to see and call someone. I went on the website and I took the phone number and I called, and I talked to someone there who could explain their benefits well…(We communicated) in Spanish, because my mom was next to me, so she had to authorize my call with them.”
46-year-old, female, Spanish speaking, Proxy on Behalf of Traditional Medicare Beneficiaries (Fort Lauderdale, FL)
“I use the healthcare, Medicare.gov website and do my comparison shopping there. I’m assuming that I am going on a correct route other than meeting with an agent. I dealt with, in my job, I dealt with health insurance for many years, so I feel pretty able to navigate that myself.”
“…We get a book from Social Security, so first I looked at that and…I had to see what was available in my area, then I had to screen out what I absolutely would not accept, and those were with extremely high premiums. And then I had to look at what was left to compare the features. Once I had done that, then I spoke with a one of those broker types.”
“I tried it out once (the 1-800-Medicare line), it’s kind of like calling the IRS, you better bring a lunch and a dinner because you going to be on hold for a long time no matter what.”
Participants Said They Considered Many Factors When Selecting Medicare Coverage, Including Premiums, Access to Doctors, Extra Benefits, and Coverage of Prescriptions
When Medicare beneficiaries first enroll in Medicare and select their coverage, they are encouraged to weigh a variety of factors, including premium costs, cost sharing for services, access to specific doctors, availability of extra benefits, coverage of prescription drugs, and quality ratings of plans, among others. Beneficiaries may revisit their choice of plan each year during the annual open enrollment period.
Focus group participants were asked what factors entered into their decision making when choosing a plan, how they viewed the process of selecting a plan, and why they ultimately chose Medicare Advantage or traditional Medicare.
Many confused by coverage options and how Medicare program works
Despite looking forward to going on Medicare, many said they were confused, stressed and overwhelmed by the various coverage options and how the Medicare program works.
Many participants lacked awareness or a good understanding about the different Medicare options available to them. They mentioned confusion with the different parts of Medicare – Parts A, B, C, D – and were unclear what makes them different from each other and which parts are mandatory or optional. They often did not know which parts of Medicare were included as part of a Medicare Advantage plan and if that was the same or different as a Medicare “supplement.”
“All the information that was coming through the mail…it stressed me out and I didn’t know what to do. I was like frozen…I ignored it and threw that stuff in the garbage.”
“I’ve got a mail, a pamphlet and a card already from MediCal that I have to read over the instructions. Basically my understanding is all I have to do is choose the plans I want, the A, the supplemental ones the A, B, C, or D, whichever ones I want. And I’m not sure how many of those are free, or how many I’m required to have, you know and what are optional ones.”
64-year-old, male, Shopping for Medicare (Bakersfield, CA)
“The prescription drug plans are hopelessly complicated. I don’t see how anybody could actually decipher what’s going to be paid unless you know what prescriptions you’ll already be getting through the year.”
70-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy (Cleveland, OH)
Zero or low premiums often cited as top reason for selecting a Medicare Advantage plan
For those who chose or were considering Medicare Advantage for their coverage, zero or low premiums was often cited as the top reason for selecting a Medicare Advantage plan, followed closely by low cost-sharing requirements for services.
People on Medicare are often concerned about the cost of health care because most live on fixed incomes with limited savings. When thinking about health care costs, the first thing that often comes to mind is a plan’s monthly premium, because it is monthly expense they will incur regardless of their health needs, and it is relatively easy to compare across plans. Many of the focus groups participants noted that they lived on tight budgets and could not afford to pay for coverage that required higher premiums, which may have led them to believe that Medicare Advantage seemed like a more affordable option than traditional Medicare plus a Medigap supplemental policy with an additional premium. Due to their budgets, they also looked closely at copay amounts, particularly for services that they thought they might use with some frequency.
“It was zero costs. It covered all of my meds, zero. My doctors were in the plan.”
“Well for us, when we first made the choice, we chose a Medicare Advantage [plan] which was…it was a zero premium, other than the basic Part B and the copays were $10, $20 for a specialist. So, the copays were very attractive and our doctors were in the network. So, yeah, the copays were a big part of it.”
“Well, (it was important for me) to be more comfortable financially (with my plan) without having to pay extra. Because, you are already paying for something in Medicare that they get from Social Security. (It’s important) to avoid paying more.”
Another factor that weighs heavily in their decision-making when selecting Medicare Advantage is whether their doctors are in the plan’s network.
For people considering Medicare Advantage plans, a top priority is whether their doctors are part of the plan’s network. In many cases, people are concerned about maintaining access to their primary care physician, but depending on their health needs, some are more concerned about having access to particular specialists.
“My reason for the Advantage Plan was that as far as my gynecologist, I can go once a year and get…a pap smear, exam, mammogram, and no payment whatsoever. With my primary care physician, I can go once a year…And also, for my dental I get two visits a year…with the cleaning and well the X-ray is once a year, but I get two cleanings and that. And with my eye care I get either glasses or contacts and $200 is what they pay towards that, and also…the exam is free. So basically, things like that that worked for me and having all my doctors there, it was really, it really worked for me financially to manage that.”
“When we pick a plan, we need to first verify the doctors that we are interested in treating us. Otherwise, they won’t take it. I pick the doctor who will treat me and if they are in the plan, perfect, otherwise I won’t get the plan.”
“It should be free, zero, zero cost to me. It should be convenient. I should be able to see doctors in town since we have you know, hospitals and specialists here in Bakersfield.”
64-year-old, male, Shopping for Medicare (Bakersfield, CA)
Availability of extra benefits in Medicare Advantage
An additional factor that influenced participants’ decision-making is the availability of extra benefits in Medicare Advantage such as dental and vision.
Medicare Advantage plans are able to offer extra benefits not available not offered by traditional Medicare, such as dental, vision, and hearing, as well as some that provide money to enrollees, such as over-the-counter benefits, and for this reason, many participants were attracted to Medicare Advantage plans.
“In general, compared to what other people are paying, I think ours is pretty good. You know, and you get $120 back every quarter, and over the counter drugs, and a $100 a quarter to cover copays, you’re getting back just as about as much as you pay, if not more.”
“The dental and the vision and stuff like that is important. Yes.”
64-year-old, female, Shopping for Medicare (San Antonio, TX)
“Because of the eyeglasses…I’ve still got to see a dentist to try to get dentures…the over the counter is a big help…this year we got a $65 cash card that you could use on groceries. I believe that next year they’re giving you $100 grocery card for food and that’s going to be a big help.”
67-year-old, female, Dual-Eligible Individual in Medicare Advantage (Homosassa, FL)
Reasons for choosing traditional Medicare
Those who ultimately chose or were considering traditional Medicare (and often a Medigap supplement) liked the relatively low cost-sharing requirements, comprehensiveness of their coverage, control over their health care, and ability to see any provider they wanted.
Medigap policies, sold by private insurance companies, are supplements to traditional Medicare and fully or partially cover Part A and Part B cost-sharing requirements, including deductibles, copayments, and coinsurance. Medicare beneficiaries with traditional Medicare, including those with a Medigap policy, can see any provider who accepts Medicare. Medigap insurance provided supplemental coverage to 36% of people in traditional Medicare (roughly 11.5 million beneficiaries) in 2020.
“Costs, and the coverage. We can afford the costs, so it’s not a problem of trying to get the cheapest, but we know that plan G is the most comprehensive coverage in the supplemental plans. And all the plans are the same by all insurance companies, it’s just the costs.”
77-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy (Kansas City, KS)
“I wanted to have what I thought was the best coverage for me…Like I say, for me when I started to sign up for Medicare, I had the days of the HMO’s ringing in my brain. People that had…cancer and other diseases and they were denying them medical care because for them it was the bottom line, it was…the dollars. And I didn’t want anybody to have that kind of control over my healthcare, which is why I chose the plan that I chose.”
66-year-old, female, Traditional Medicare Beneficiary with a Medigap Policy (Newport News, VA)
“(With traditional Medicare and Medigap) I can go anywhere I want. I can go out of state. If I don’t like this one doctor’s attitude, I don’t feel I’m getting the proper care, I can go somewhere else. For my medical supplies I can switch companies without an issue. I have the freedom to go wherever I choose to go.”
65-year-old, female, Shopping for Medicare (Chicago, IL)
Relationships with insurance providers
Some participants had relationships with insurance providers that they felt comfortable with or liked the reputation of the company.
“The reason I selected (my plan) was that I’ve seen that United Healthcare is very widely accepted, so I knew I wouldn’t have any problem with getting doctors. But also, I was dissatisfied with my prior insurance company, so this seemed like what I had been waiting for when I saw what the premium was and it was available, and that’s why I went with it.”
“…I was under Blue Cross Blue Shield most of my life. And then when I was in practice, I was Blue Cross BlueShield. So you get used to a certain standard of care, also by being in the healthcare field all those years, you’re very familiar with all of the healthcare companies, you know, who’s better at paying things so that factor in a lot as well. So, it’s better to go along with a brand name that’s been in the market for a while, those are easier to review, as opposed to some company you never heard of that has maybe a high deductible and doesn’t hardly cover anything. So those factored in a lot.”
Participants did not generally use Medicare’s star quality ratings when making coverage decisions, though some participants used other non-government sources to get information about plan quality.
On the Medicare plan finder, each Medicare Advantage plan has a star rating to provide beneficiaries with additional information about the quality of plans offered in their area. All plans are rated on a 1 to 5-star scale, with 1 star representing poor performance, 3 stars representing average performance, and 5 stars representing excellent performance. When asked whether these star ratings influenced their decision-making when choosing a plan, the majority of participants said no.
For the few participants who did look at ratings, they reported turning to other non-government sources for reviews on a plan’s quality.
“I went on…I forget what website it was. I went to check to see how good it was. I know there’s a place, but I can’t think of what it is right offhand. And they give you the ratings of the different health plans, Medicare Advantage plans…They give you the pros and the cons and how many stars…I just type into a search thing on the internet.”
67-year-old, female, Dual-Eligible Individual in Medicare Advantage (Homosassa, FL)
“I looked at reviews…. I think it helped me, I mean I think, and this may sound really, really crazy, but when I look at reviews, I don’t look at the highest ones, I look at the lowest ones…I look at those first because I want to find out if any of the issues, they’re having that pissed them off enough to give them a low rating, is going to affect me. And the high ones I want to look at because most people only review something if they’re mad. I mean it’s just, you know psychologically the way people work. Nine times out of 10 it’s not a good review that they put online to do. So if they did that means a lot. It would mean more to me than 10 bad ones. One good one actually means more than 10 bad ones.”
60-year-old, female, Dual-Eligible Individual in Medicare Advantage (Largo, FL)
“I didn’t look at the rating myself, but I did research through an organization called medicareschool.com and what they did when they were looking at the different plans and giving me some advice, was they looked at the companies and they would look at ten years back at the company, their ratings, how often they changed premiums and all of that stuff.”
66-year-old, female, Traditional Medicare Beneficiary (Newport News, VA)
Prescription drug coverage important factor in decision-making
Regardless of whether they selected or were going to select traditional Medicare with a stand-alone Part D plan or a Medicare Advantage plan with drug coverage, ensuring that their prescription drugs were covered was also an important factor in participants’ decision-making.
People with Medicare can get prescription drug coverage by enrolling in a stand-alone plan that provides Part D prescription drug coverage for people with traditional Medicare or by enrolling in a Medicare Advantage plan. Coverage of prescription drugs is based on each plan’s formulary, and depending on a plan’s formulary, beneficiaries can also be subject to prior authorization, step therapy, and quantity limits. Medicare beneficiaries with Part D coverage also face cost-sharing amounts for covered drugs and may pay an annual deductible ($505 in 2023) and depending on the plan, a monthly premium.
“(I chose my plan) for the prescriptions. They would give me the supplement plan to help with the prescriptions, even though I thankfully don’t take a lot of medications. And that was the one they recommended…if I went to the hospital, it would at least cover part of it, and then I would at least pay for the deductible, that is what made me make the decision”
“I would say number one is the cost of drugs, they’ve got me taking so much stuff it’s ridiculous…”
64-year-old, female, Shopping for Medicare (MN)
“I purposefully choose a plan that has no drug deductible. And so, fortunately, I take, I think it’s six or seven prescriptions, and through the mail order I pay zero, so I’m fortunate in that respect. The only issue I’m having is attempting to get that one medication prescribed, basically.”
Participants Overall Reported High Satisfaction with Their Medicare Coverage
Most participants satisfied with Medicare coverage
Most participants – whether in traditional Medicare or Medicare Advantage – were relieved to be on Medicare and reported being satisfied with their Medicare coverage.
Medicare continues to be a very popular program, with 81% of the public holding very or somewhat favorable views of the program. Most participants mentioned being excited or relieved to go on Medicare, often because of the lower costs compared to their previous insurance coverage or because of the security of having Medicare coverage. When asked on a scale of 1-10 how they would rate their Medicare coverage, with 10 being very satisfied, most participants gave their coverage an 8, 9 or 10, saying it is working well for them.
“Most of my life, well since age 21, we have not had insurance. So, it’s a blessing to finally turn 65 and have insurance, especially coming off a heart attack a few years earlier, which was very expensive. So yeah…we were doing a happy dance when we got that policy.”
“I have original Medicare and my supplement is G, which is the best of all the ratings. And other than the deductible that I have to pay every year for Medicare everything else is taken care of. I don’t have to worry about any billing. I never see a bill. I see a chiropractor every month and everything. That’s the only thing I do on a monthly basis and everything is taken care of.”
77-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy (Kansas City, KS)
“I was relieved, however, because I was…under the impression, I bought into the Medicare reputation in that it’s reliable insurance, medical insurance, that would always be there. So, I didn’t have to worry about not having medical insurance.”
Varied reasons for satisfaction depending on source of coverage
Participants cited a variety of reasons for their satisfaction, including costs, access to providers, and supplemental benefits, depending on their source of Medicare coverage.
Participants with traditional Medicare and a Medigap policy are generally happy with their coverage because they like the relatively low cost-sharing requirements, not having to deal with bills, protection against catastrophic expenses, ability to see any provider they want, and having control over their health care.
“I’m happy with what I have and I don’t want limitation on what doctors you can go to. That’s another generally limitation, I think, of the Medicare Advantage program.”
“I like that I don’t have to wait, if I feel like something is wrong or I need something to be checked out, I don’t have to wait on a doctor to get a referral to go and see…say I feel like I’ve got heart issues or something, I can find the cardiologist, call and make an appointment and go and see a cardiologist. Whereas, with my husband’s plan, he has to go to see his primary care doctor, get a referral to go see his cardiologist. I wanted control over my own health.”
66-year-old, female, Traditional Medicare Beneficiary with a Medigap Policy (Newport News, VA)
“To know that there is no hidden surprises down the road, like some were mentioning they might have to have a surgery, and all of a sudden find that their Advantage plan is not doing as much as they thought they would. And they come up with, maybe $5,000, $6,000, $7,000 bill, which maybe they’re not prepared to pay.”
77-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy (Kansas City, KS)
Medicare Advantage plan participants pleased with their coverage
Participants in Medicare Advantage plans are pleased with their coverage and noted that this was due to having zero or low premiums, and coverage of extra benefits, such as dental, vision, hearing, services and over-the-counter debit cards.
“In Medicare Advantage, I pay $0. In all the 10 years, I didn’t pay anything besides ultrasound on my legs. I used to get $50 over-the-counter medication. Next year it will be $75. That’s the only thing. I pay for nothing. So I believe in it.”
“For primary care, you know there’s zero copay and things like that…a decent copay for specialists, which I’m pleased with. And dental…for your cleaning…X-rays, you get once a year with zero copay and there’s a $200 allowance for eyes…if you want to get a pair of glasses every year, which I think that’s reasonable, in a sense…zero copay for the visit and things like that.”
Dual-eligible participants also generally satisfied with coverage
Dual-eligible participants – whether they had Medicare coverage through traditional Medicare or a Medicare Advantage plan – are also generally satisfied with their coverage, particularly due to the low cost of their health care.
Dual-eligible individuals feel their health care coverage is affordable and covers most services they need. Most referenced the low out-of-pocket costs for their health care, such as no copays for doctor’s visits and prescriptions, as the primary reasons they were satisfied with their coverage. Some who had their Medicare coverage through a Medicare Advantage plan also were pleased at having coverage of some extra benefits, such as an over-the-counter allowance or money to buy food and produce.
“It really works really well so that I almost have you know, no copays, almost zero deductibles. I’m paying very little out-of-pocket, so…I’m lucky.”
48-year-old, male, Dual-Eligible Individual in Traditional Medicare (New York City, NY)
“I have zero copay. I don’t need referrals to any specialists. And all my medicine is free. I also get $125 a month for over the counter or healthy food. So I’m very happy with that plan.”
72-year-old, female, Dual-Eligible Individual in Medicare Advantage (Delray Beach, FL)
“It paid good. You know paid for everything. I can choose one pair of glasses a year. I had cataract surgery and it paid for my cataract surgery. And if you can find a dentist around here that will take Medicaid, it will pay for a set of dentures and your dental work. And like I say, the county put me on the plan, and it worked really well for me and that’s why I just stayed on it and didn’t look for anything else.”
67-year-old, female, Dual-Eligible Individual in Traditional Medicare (NC)
Despite High Satisfaction, Participants Cited Specific Issues that Varied Depending on their Source of Medicare Coverage
Concerns about premiums
While participants with traditional Medicare and a Medigap policy are generally pleased with their coverage and access to physicians, they had concerns about the premium.
While Medigap limits the financial exposure of Medicare beneficiaries for services covered under Parts A and B, Medigap premiums can be costly and can rise with age, depending on the state in which they are regulated. Estimated average monthly premiums for Medigap policies can range from less than $100 per month to over $300 per month depending on the plan.
“I go right back into the AARP United Healthcare Plan F (when I got Medicare). It covers everything, but it’s not cheap. It’s very expensive. And I’m starting to look at some Advantage Plans and the reason for that is my plan doesn’t cover vision and dental. So, I may want to look at some Advantage Plans that will also cover those.”
71-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy (San Jose, CA)
“We can afford the extra money (for Medigap). What I’m seeking to avoid is a catastrophic medical bill that would basically jeopardize the money we’ve saved for retirement.”
70-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy (Cleveland, OH)
High medical bills for some participants in Medicare Advantage
While many participants with Medicare Advantage are satisfied with their coverage, some with serious medical conditions encountered high medical bills when using certain services.
“I had cancer two years ago and a lot of the bills that I got weren’t covered, some medication wasn’t covered and things like that. And the copays for, I had a lot of scans done, CT scans, MRIs and I had to pay a large co-pay to have those done. So, I did not realize that it was going to be like that until it happened, so I didn’t realize that I was going to have that much money to come out of pocket. But other than that, the plan is good, like I said it’s fine if you don’t get sick.”
“…I have problems paying my medical because I had so many over the last few years… But the hospital, and I still owe some now, but a lot of times the hospital has forgiven that bill. A couple times I’ve talked to a financial. Now I might have some bills from this surgery still coming up, but yeah, they had a program where they have forgiven. And there’s another issue where sometimes I can’t buy my prescriptions when the time comes and then I have to wait.”
“… I had to have cataract surgery in both eyes and surgery on my thumb, and the copays from United were like $350 for each surgery. And Aetna was 225, so I switched.”
Delay in care experienced by some participants in Medicare Advantage
Some participants with Medicare Advantage, including some dual-eligible individuals, experienced delays receiving care due to utilization management tools, such as prior authorization and/or referral requirements.
Medicare Advantage plans can require enrollees to get approval from the plan prior to receiving a service, and if approval is not granted, then the plan generally does not cover the cost of the service. Similarly, Medicare Advantage can impose referral requirements, in which a primary doctor must provide a written letter in order for a patient to see a specialist for services, and if not provided, then the plan generally does not cover the cost. In 2023, virtually all Medicare Advantage enrollees (more than 99%) are in plans that require prior authorization for some services. Health insurers use these utilization management tools to both contain spending and prevent enrollees from receiving unnecessary or low-value services, though there are some concerns these requirements may create barriers and delays to receiving necessary care. Some Medicare Advantage participants experienced delays receiving care, but nearly all ultimately got approval for their prior authorization and/or referral requests.
“So I went to my primary care originally when my knee first went, and I knew something was wrong. And then they did an X-ray and like the orthopedic doctor said later on, he said the X-ray showed how bad your knee was, why did they wait? They said because of insurance they had to, I have to have an MRI before they could refer me to orthopedic doctor. It took weeks to get the MRI, and then once they got the MRI, I think it was another two weeks before I actually got into the orthopedic doctor. He was ready to do the surgery immediately, but I had other things I needed to get done. But it could have been done months before. The damage to the bones in my knee where he had to shave it down to get the new knee to fit in, it wouldn’t have been that bad.”
“[…] I’ve been, was diagnosed 15 years ago with very severe rheumatoid arthritis. Every medication that I’ve been tried on, I’ve either had an anaphylactic shock reaction and almost died, or I had started vomiting blood copiously within hours of taking it, from stomach leaks. We finally found a medication that I was brave enough to try just one more, and we found one that is working. And it didn’t kill me, and it is helping. But Humana will not cover it, period. It’s expensive. But they’re injections that you get once a month, and two injections once a month, and they won’t pay for it. So they want me to try some other medications for R.A., that I haven’t tried yet, injectables and stuff.”
Dual-Eligible Individual in Medicare Advantage (Largo, FL)
“I have spinal stenosis and I was trying to see a pain management doctor and I had to get a referral from my primary care (doctor), and also my insurance had to approve it. And it took several weeks for me to get that. They were very slow with the process. And in the meantime, I was in pain every day. So I wasn’t happy about that. So I finally got (approval) and then it turns out the pain management doctor referred me to a neurosurgeon. So I had to get another referral for the neurosurgeon. So, the whole process it just took too long.”
While Medicare Advantage enrollees were generally aware of the importance of having their doctors in-network, many participants encountered situations when the doctor they wanted to see for a particular service was not in-network. Issues with provider networks was also a particular challenge for dual-eligible participants with a Medicare Advantage plan who sometimes could not find a provider who accepted both their Medicare and Medicaid coverage.
Unlike traditional Medicare, where Medicare beneficiaries can see any provider who accepts Medicare, beneficiaries enrolled in Medicare Advantage have a network of physicians and hospitals for their care. If providers are not in-network, Medicare Advantage enrollees typically must pay more to see out-of-network providers, or they may be responsible for the entire cost of seeing that provider. When beneficiaries select their Medicare Advantage plan, they are encouraged to check whether their preferred providers are in-network as provider networks vary across plans. However, evidence indicates provider directories might not always be accurate, and it may be difficult for beneficiaries to compare networks and providers across plans as they may be in different formats across insurers. Focus group participants noted situations when they could not see their preferred doctor because they were not in their plan network and were frustrated with having to see a different provider.
In addition, some dual-eligible participants with a Medicare Advantage plan, including participants with a dual-eligible Special Needs Plan (D-SNP), reported issues with doctors accepting their health insurance policy. D-SNPs are a specific type of Medicare Advantage plan designed for this population to better coordinate care, though these plans can also look different across states in terms of their levels of coordination. For example, some D-SNPs offer Medicaid and Medicare benefits through different organizations, while some have plans through the same parent company.
“Well, you have to go to the doctors that are in the plan. For example, I wanted to go see another doctor, because of (I needed) laparoscopy, and I had to go to a doctor that the insurance plan assigned. I couldn’t go to the doctor I wanted to go to.”
“My current insurance, I can’t find a psychiatrist in my area to go see to prescribe the anti-anxiety, so I’m dealing with that right now. I looked at, since we’re still in open enrollment, I looked at different plans, and there’s nobody here in my area that supports a psychiatrist who will be willing to prescribe those types of meds.”
Dual-Eligible Individual in Medicare Advantage (Largo, FL)
“You try to find a plan that takes your doctors and your medication and that was the most difficult. I must have gone through three or four different plans in the first year, because I didn’t understand how those plans worked and if they had what doctors I wanted on there.”
Dual-Eligible Individual in Medicare Advantage (Gainesville, FL)
“It’s been pretty much the same, although I have changed companies several times. Probably maybe four times altogether…Well one time was that my primary care doctor stopped accepting the Medicare policy, the company that I was using, and I didn’t want to lose my primary at that time. Another time was about paying bills and turning down things that should have been covered, copays and stuff that should have been covered under my Dual policy. And they kept trying to bill me for and threaten me about it, and it’s like no. So mostly just non-cooperation with the insurance company for the most part.”
Dual-Eligible Individual in Medicare Advantage (Largo, FL)
Frustration with using some supplemental benefits
Some Medicare Advantage enrollees also voiced frustration with using some supplemental benefits, particularly dental coverage, because cost sharing was higher than expected and due to network restrictions. Network restrictions for extra benefits were also challenging for dual-eligible participants who had a Medicare Advantage plan.
Many people are attracted to Medicare Advantage plans because they offer extra benefits that traditional Medicare does not offer, such as dental, vision, and hearing coverage. However, some participants raised concerns with the costs of these benefits, challenges using these benefits, or finding a provider who covered these services. Like accessing providers covered by Medicare Advantage plans, many Medicare Advantage plans have networks of providers who cover supplemental benefits, or the enrollee will be required to pay more to see someone out-of-network, such as for dental benefits.
“I am not happy because every year they charge more for copayment, for example, the dental…I had to leave my dentist because they don’t pay them enough, and I have to go to the one they want me to go.”
“I am not satisfied with my dental plan. It’s not very good, the coverage is bad and when we go to the dentist, they say there is a copayment. The plan I have it’s not very good.”
“When…my upper denture broke, nobody took the insurance that I had and I finally got it fixed. And my optometrist where I just get my eye exam and glasses every year, he just stopped taking Medicaid and Medicare, and I haven’t found a replacement yet.”
66-year-old, female, Dually Eligible Beneficiary in Medicare Advantage (Gainesville, FL)
“Yes, I’ve encountered problems with, you know, they’re like we’ll take regular CareSource, but we don’t take the Dual…I’ve had where, you know I was seeing, went to a dentist and then the next thing I know they’re just like, you know something’s going on with your insurance and I’m thinking it wasn’t the insurance, it was just like you know it was actually the provider, and having, you know having an issue, and it’s just like oh forget this and I’ve had to find somebody else. But it’s like it can be difficult with finding providers that take the Dual plan.”
43-year-old, female, Dual-Eligible Individual in Medicare Advantage (Youngstown, OH)
Frustration with high cost of certain medications
Some participants were also frustrated by the high cost of certain medications, particularly for those who need specific drugs to manage chronic conditions.
In recent years, many Medicare beneficiaries have experienced high out-of-pocket costs for their prescription drugs. Changes as part of the Inflation Reduction Act, including a $35 monthly copay on insulin that went into effect in 2023, as well as limits on out-of-pocket prescription drug spending in Part D beginning in 2024, and a $2,000 cap beginning in 2025, will help some Part D enrollees with their prescription drug costs.
“…I suffer from anxiety, and there is a medication that none of the insurances I have covers. I have to pay for it on my own. And that is a problem. None of the insurances I’ve had have wanted to pay for that medicine.”
“I’m diabetic. So, they wanted me to go on Trulicity and if you fill it, it puts you, right after one time, you’re in the donut hole. And I said, I just can’t afford it. I want medicines that don’t cost me anything.”
“Yes, (my parents have Part D) but there are certain medications that weren’t covered if it was the generic one, and they didn’t have that medication. So, we had we had to pay for it.”
46-year-old, female, Spanish speaking, Proxy on Behalf of Traditional Medicare Beneficiaries (Fort Lauderdale, FL)
Participants Generally Feel They Made the Right Choice When Selecting a Plan, and Most Participants Have Not Revisited Their Plan Choices
The marketplace of Medicare private plans is based on the idea that beneficiaries will compare their plan options to find plans that best meet their individual needs. CMS encourages beneficiaries to compare and review their plan options each year, which could enable them to receive care at a lower cost, ensure their preferred providers are in network, and that the prescription drugs they take are covered. However, KFF analysis has shown that most beneficiaries do not compare their plan options in each year.
Majority feel they made the right choice
The majority of participants in the focus groups confirmed this behavior – they explained that they felt that their coverage was comprehensive and did not need to reevaluate their coverage every year though some wish they had more information before enrolling. Additionally, many participants said they are unlikely to switch plans going forward because selecting a new plan would be too much work, and they did not feel confident they would be better off with another type of coverage. For dual-eligible participants who made a choice about their Medicare coverage, they also generally did not feel the need to switch plans going forward.
“I have no concerns about my coverage, everything works well for me. Even the co-payment, it’s not a large amount, but I can handle it…I like it because I can go to any doctor I want. Everything is great…I have no complaints about my coverage, none whatsoever.”
75-year-old, female, Traditional Medicare Beneficiary (Las Vegas, NV)
“Every year, right, I can always change, but I’ve never changed because like I said, for me if it ain’t broke don’t fix it. Why would I change because it’s been so nice, I’ve stayed with the same provider all the way through.”
48-year-old, male, Dual-Eligible Individual in Traditional Medicare (New York City, NY)
“I’m happy with the plan that I have now, and I haven’t looked at anything else. So, I don’t even know if I could (change) or not.”
74-year-old, female, Dual-Eligible Individual in Medicare Advantage (Cuyahoga Falls, OH)
But some say they shop around
However, a few of the participants said they do shop around, sometimes every year, to ensure they continue to have the best plan that meets their needs.
“We meet with an insurance man every year who looks at our prescriptions and then checks to see the best company that we can be with for those prescriptions that we have. And so we sometimes change companies every year based on the premium and the deductible and the prescription costs every time we order by mail order. And he’s looked…it pays to check every year to see what’s coming along.”
77-year-old, male, Traditional Medicare Beneficiary with a Medigap Policy(Kansas City, KS)
“I’m always looking for a better plan because I’m not that happy with what I have. But I’m just checking to see about the out-of-pocket and copays that other companies are charging as compared to what I have.”
“I take a legal pad and list two or three companies. And I itemize how many doctor visits, specialist visits, dental for the year and figure (the cost to me) – this company will cost me $1,000, this costs me $2,000, where I want to go. I’m pretty thorough about it.”
People with both Medicare and Medicaid, also referred to as dual-eligible individuals or dual eligibles are enrolled in both programs and must meet eligibility requirements for both programs. They receive their primary health insurance coverage through Medicare and some assistance from their state Medicaid program. Together, these two programs help to shield low-income beneficiaries from potentially unaffordable out-of-pocket medical and long-term care costs: Medicaid typically pays the Medicare Part B premium and may also pay for Medicare’s other cost-sharing requirements; Medicaid also helps pay for services that are not covered by Medicare, such as long-term services and supports. While nearly all dually eligible beneficiaries have low incomes and very modest savings, they are otherwise a diverse group in terms of age and physical and mental health.
To capture the unique experiences faced by dual-eligible individuals, we conducted two focus groups that consisted exclusively of these beneficiaries.
Dual-Eligible Participants Had Varying Experiences Signing Up for Medicaid Coverage With Some Participants Choosing Coverage and Others Being Assigned Their Coverage
As mentioned above, people with Medicare have the choice between traditional Medicare or a Medicare Advantage plan, which can include an individual plan open for general enrollment as well as a dual-eligible Special Needs Plan (D-SNP). Dual-eligible individuals who are eligible for full Medicaid may receive those Medicaid benefits through capitated managed care organizations (MCOs) or through fee-for-service (FFS). Options for Medicaid coverage vary depending on the state that the enrollee lives in as do the mechanisms for beneficiary enrollment. Some states provide dual-eligible individuals with the ability to choose their plans, others assign people to a plan, and still others assign enrollees to a plan but offer them the opportunity to disenroll and select a different option.
As a result, participants had varying experiences signing up for Medicaid coverage, often depending on the state they lived in and whether they had enrolled in Medicare or Medicaid first or at the same time.
Making a choice for Medicaid coverage
Some participants had to make a choice for their Medicaid coverage, and many had help from the state choosing their plan.
“I give full credit to the State of New York for the way that their coverage is set up here, because when you reenroll every year, you call a certain number and the person on the other end…I remember when I first enrolled they kind of walk you through the process, and they told you, they look for the providers that were the best and then just kind of walked you through it. So to answer your question, it’s always been very laid out very nicely.”
48-year-old, male, Dual-Eligible Individual in Traditional Medicare (New York City, NY)
“I went to the county, the office here in the county and applied. I had both knees were really bad and I knew I was getting to the point. They told me I was going to have to quit work and going to have to have knee replacements. So, I went to the county office here and applied, applied for the Medicaid here in the county.”
67-year-old, female, Dual-Eligible Individual in Traditional Medicare (NC)
Some participants did not have a choice
Some participants did not have a choice of their Medicaid coverage, or someone enrolled them in Medicaid coverage – often the state or county chose their Medicaid plan for them.
“I didn’t have a choice as to which (Medicaid) plan. You know the plan was chosen for me. It was out of my hands… I don’t know if it’s the state of Ohio, or the Summit County that I live in, whether they made the choice for me.”
74-year-old, female, Dual-Eligible Individual in Medicare Advantage (Cuyahoga Falls, OH)
“The state where I live, the county made the choice and I’ve not messed with anything, I let them do the choices. I get a lot of this stuff in the mail to change to Medicare this and Medicare that. I don’t touch anything, I let them do everything so it will stay the same. I’m afraid I would mess it up if I tried to go through and do something different.”
67-year-old, female, Dual-Eligible Individual in Traditional Medicare (NC)
“Initially when I first went on Medicaid there was just one state plan. In recent years they’ve gone to, where I could choose between, I don’t know I want to say like five different providers. And I didn’t choose, I just stayed on what I initially had, so I’m not exactly sure what provider I’m with when it comes to Medicaid. Now as far as the Medicare, the only choice I had was either traditional or the Advantage and I got traditional.”
56-year-old, female, Dual-Eligible Individual in Traditional Medicare (Benson, NC)
Some Medicare enrollees did not realize they might also be eligible for Medicaid
Some who were enrolled in Medicare did not realize they might also be eligible for Medicaid, but their state reached out to them to let them know they should apply for Medicaid coverage.
“I got Medicare A and B first and then Medicaid sent me a form telling me to apply for Medicaid.”
61-year-old, female, Dual-Eligible Individual in Traditional Medicare (Buffalo, NY)
“We enrolled her in Medicare first, and then we found out that she could supplement her Medicare with the Medicaid, and so we did that…She actually got a letter letting her know that she could apply for the additional Medicaid coverage. And here in Texas what it does is it basically covers what Medicare doesn’t, so like your doctor copays, remaining hospital and all that.”
46-year-old, male, Proxy on Behalf of Dual-Eligible Individual in Traditional Medicare (Odessa, TX)
Some Dual-Eligible Participants Were Concerned About the Possibility of Losing Medicaid Coverage Due to the Annual Redetermination Process
Concerns about redetermination process
Because of the importance of the Medicaid program for addressing their health care needs, some dual-eligible participants were concerned about the redetermination process and anxious about the possibility of losing that coverage.
Prior to the COVID-19 pandemic, states were required to renew Medicaid eligibility for dual-eligible individuals at least once per year. Since March 2020, states have provided continuous enrollment in Medicaid in exchange for enhanced federal funding. This continuous enrollment provision and enhanced federal funding were originally in place until the end of the COVID-19 public health emergency (PHE). In December 2022, the Consolidated Appropriations Act, 2023 (CAA) delinked the provision from the PHE and ended continuous enrollment on March 31, 2023. Beginning April 1, 2023, states have restarted disenrollments after conducting a full review of eligibility. As states begin to “unwind” the continuous enrollment provision, many people will likely be found to be no longer eligible for Medicaid. Others could face administrative barriers and lose coverage despite remaining eligible.
Focus group participants generally had not experienced a loss of Medicaid, but some participants mentioned being concerned with losing their Medicaid coverage in the future due to changes in their incomes, assets, or other eligibility requirements. Many were aware of the renewal requirements even though redeterminations had been on hold during the pandemic.
“You can’t have a lot of assets or a like a lot of money to get help. If you do, you don’t get a lot of help. You just got, you know you’re only allowed so much in the bank. You’re only allowed one track of property, two cars, and that’s it. If you go over, they will stop your Medicaid and cut it out.”
67-year-old, female, Dual-Eligible Individual in Traditional Medicare (NC)
“I have to renew it (my Medicaid) every year…I have to be poverty stricken in order to be qualified.”
72-year-old, female, Dual-Eligible Individual in Medicare Advantage (Delray Beach, FL)
“I also get the food stamps and now… that’s tied together with Medicaid that I renew every year.”
66-year-old, female, Dual-Eligible Individual in Medicare Advantage (Gainesville, FL)
Discussion
As more people on Medicare are enrolled in Medicare Advantage, CMS, policymakers, researchers, and the public have become more focused on how the program is serving people on Medicare. Participants across the spectrum of coverage noted that they experienced aggressive marketing tactics, including unsolicited phone calls, and felt inundated by Medicare television advertising, often for Medicare Advantage plans, that they believed to be both misleading and unhelpful.
Participants with Medicare found the process of selecting their coverage to be overwhelming and difficult, and often relied on brokers to help them review and understand their coverage options. Few participants used Medicare’s official resources to assist in their decision-making. When choosing their coverage, participants said they valued a variety of factors, including premiums and other costs, access to preferred providers, availability of extra benefits, and coverage of prescription drugs.
Participants in the focus groups – whether in traditional Medicare or Medicare Advantage – emphasized that they are generally satisfied with their Medicare coverage. Participants in Medicare Advantage plans were pleased with their coverage due to the low or no premium costs, as well as the availability of extra benefits, such as dental, vision, hearing, and debit cards. Participants with traditional Medicare and a Medigap policy were happy with their coverage due to the low or no cost-sharing requirements, no network restrictions on seeing their preferred providers, and the ability to control their own health care.
However, some participants, particularly in Medicare Advantage plans, also noted that there are elements of their coverage that caused them frustration, including delays receiving care due to prior authorization and referral requirements as well as facing limitations in seeing their preferred doctors due to limited networks. In recent months, CMS and policymakers have sought to address some of these issues through both legislation and rulemaking, including rules that would streamline the prior authorization process and place additional limitations on Medicare marketing.
Most dual-eligible participants who have both Medicare and Medicaid said they are satisfied with their coverage, whether in Medicare Advantage or traditional Medicare, though some in Medicare Advantage encountered problems finding a provider in their plan’s network. Further, some participants with Medicaid were uniquely concerned about maintaining their Medicaid eligibility and were anxious about losing Medicaid during the annual redetermination process. With Medicaid redeterminations having restarted April 1, states may have begun disenrollments, which could lead to some losing their coverage, though it is unclear how much that would impact focus group participants who generally had not experienced a loss of coverage prior to the pandemic.
In making coverage decisions, participants say they were annoyed by marketing calls and the number of ads marketing Medicare plans on TV, and generally ignored them. Few participants said they intend to review or switch their coverage. While focus group participants were generally satisfied with their Medicare coverage, most were also confused and frustrated by the complexity of the program and lacked confidence in their own ability to compare and choose a source of coverage to best meet their individual needs.
Appendix
The focus group participants included Medicare beneficiaries ages 65 and older and younger adults with disabilities who make health coverage decisions for themselves and/or their spouse or family member. Some focus groups also consisted of people with both Medicare and Medicaid (also referred to as dual-eligible individuals) as well as adults 64 years old who were not yet enrolled in Medicare. Participants included beneficiaries in traditional Medicare, some with and some without Medigap supplemental coverage, and beneficiaries enrolled in Medicare Advantage plans. Because the study focused on decisions around health plans, we excluded beneficiaries with retiree coverage from a former employer or union.
We conducted 7 focus groups with participants from across the country in November 2022, timed to coincide with the Medicare open enrollment period, which starts October 15 and ends December 7 of each year. Each focus group was conducted virtually by Zoom and included 5-8 participants, differing by age, gender, income, race/ethnicity, health status, and type of insurance coverage. Each focus group lasted one hour and forty-five minutes. Two of the seven focus groups consisted of people with Medicare and Medicaid, with one group consisting of adults 65 and older, and the other group adults younger than 65. One focus group included adults 64 years old who were not yet enrolled in Medicare, but who were starting to think about their Medicare coverage options. One focus group was conducted in Spanish. Individuals who were able to participate in the groups needed to know their Medicare coverage, and if applicable, Medicaid coverage, have two hours of time, a quiet space, a computer, and internet. These characteristics alone may not fully represent many people with Medicare, so the perspectives described in this report may not be generalizable to the entire Medicare population. See Appendix Table 1 for demographic details about the participants.
The analysis includes responses from participants across all 7 focus groups. There are also additional responses from dual-eligible participants that emphasize beneficiary experiences unique to this population.