Key Takeaways
- With childhood vaccination rates in the U.S. continuing to decline as measles cases rise across the U.S., KFF’s latest Tracking Poll on Health Information and Trust shows that several commonly circulated vaccine myths remain pervasive among the public. Many adults say they have heard false claims about the measles and COVID-19 vaccines, including that the measles, mumps, and rubella (MMR) vaccines have been proven to cause autism in children (66%), that more people have died from the COVID-19 vaccines than the virus (46%), that mRNA vaccines can alter DNA (36%), or that measles vaccines are more dangerous than measles itself (29%).
- While many have heard of these myths, smaller shares are convinced they are true. Fewer than one in ten adults express ardent belief in each myth, while larger shares (between 31% and 44%) say each are “definitely false” and at least half fall in the “malleable middle,” saying each of these claims is either “probably true” or “probably false.”
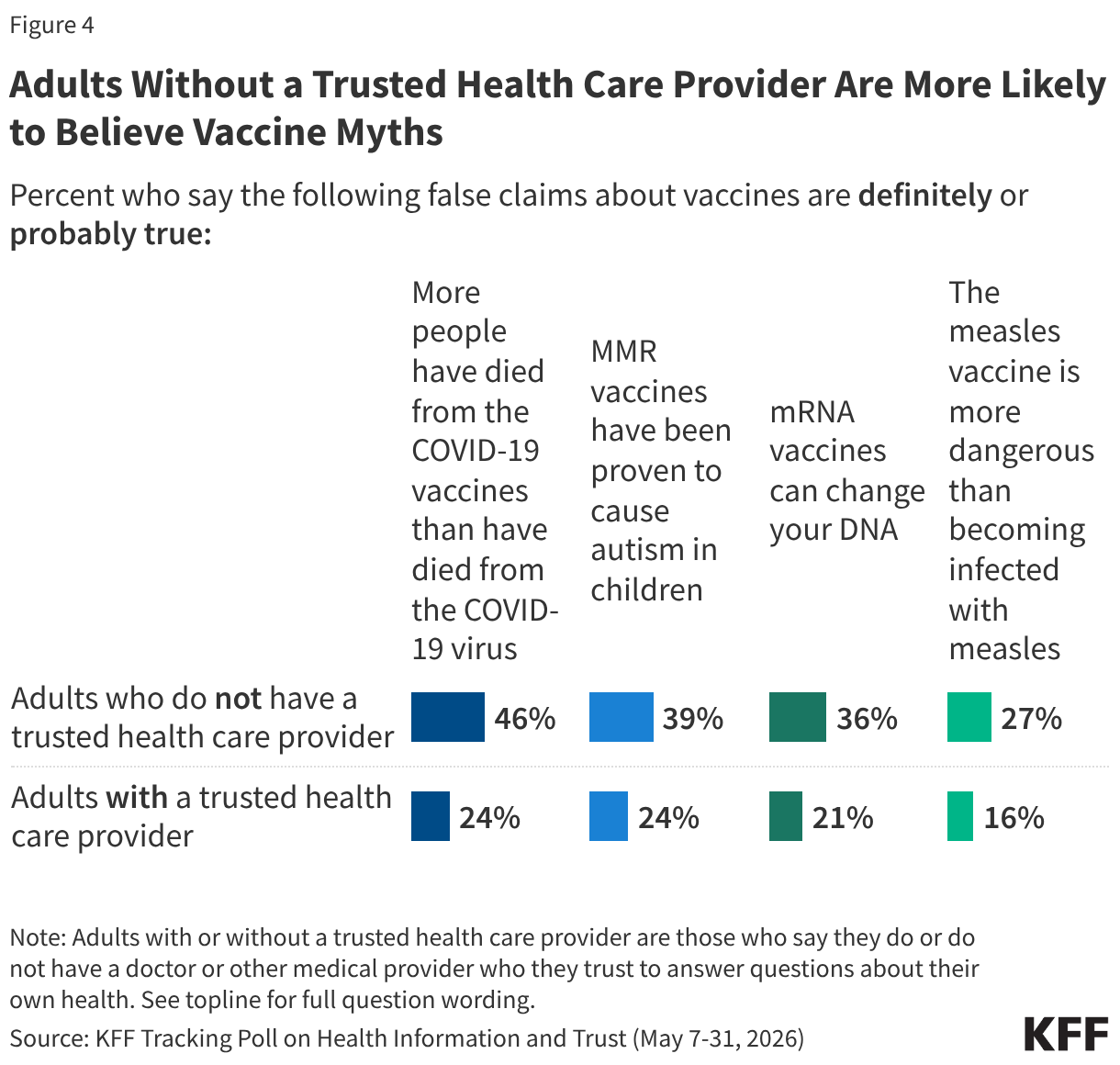
- Adults who have a relationship with a trusted health care provider are less likely than those who don’t have such a relationship to believe or lean toward believing vaccine falsehoods. For instance, nearly half (46%) of adults who say they do not have a health care provider they trust to answer questions about their health say it is “probably” or “definitely true” that more people have died from COVID-19 vaccines than from the virus, which is nearly twice the share among those with a trusted provider (24%). While younger adults, Hispanic adults, and uninsured adults are more likely than their counterparts to say they don’t have a trusted provider, the connection between lacking a trusted provider and belief in vaccine myths holds even when controlling for factors like age, race and ethnicity, education, partisanship, and insurance coverage.
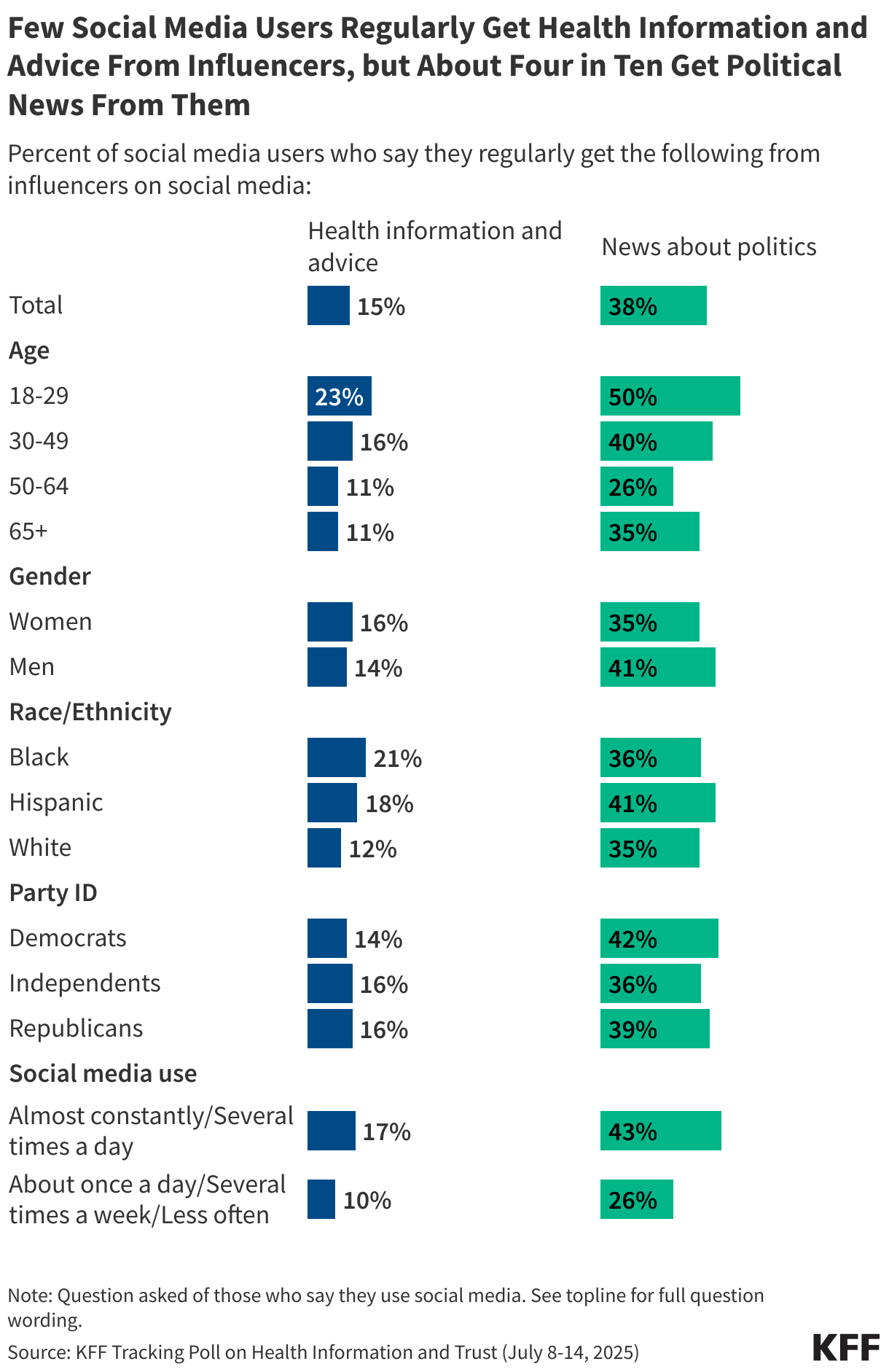
- Those who use social media and artificial intelligence (AI) chatbots for health information are also more likely to endorse many of these vaccine myths. For example, adults who use social media for health information at least weekly are more than twice as likely as those who don’t use social media for health to say the myth linking MMR vaccines to autism is “probably” or “definitely true” (37% v. 16%). Use of artificial intelligence (AI) for health information is also correlated with views on some of these myths, with adults who regularly use AI for health information more likely than non-users to believe or lean toward believing myths about the MMR and mRNA vaccines. While younger adults, Black and Hispanic adults, and those without a college degree are all more likely to use to social media for health information, the connection between frequent use and belief in vaccine myths holds even when controlling for factors like age, race and ethnicity, education, and partisanship.
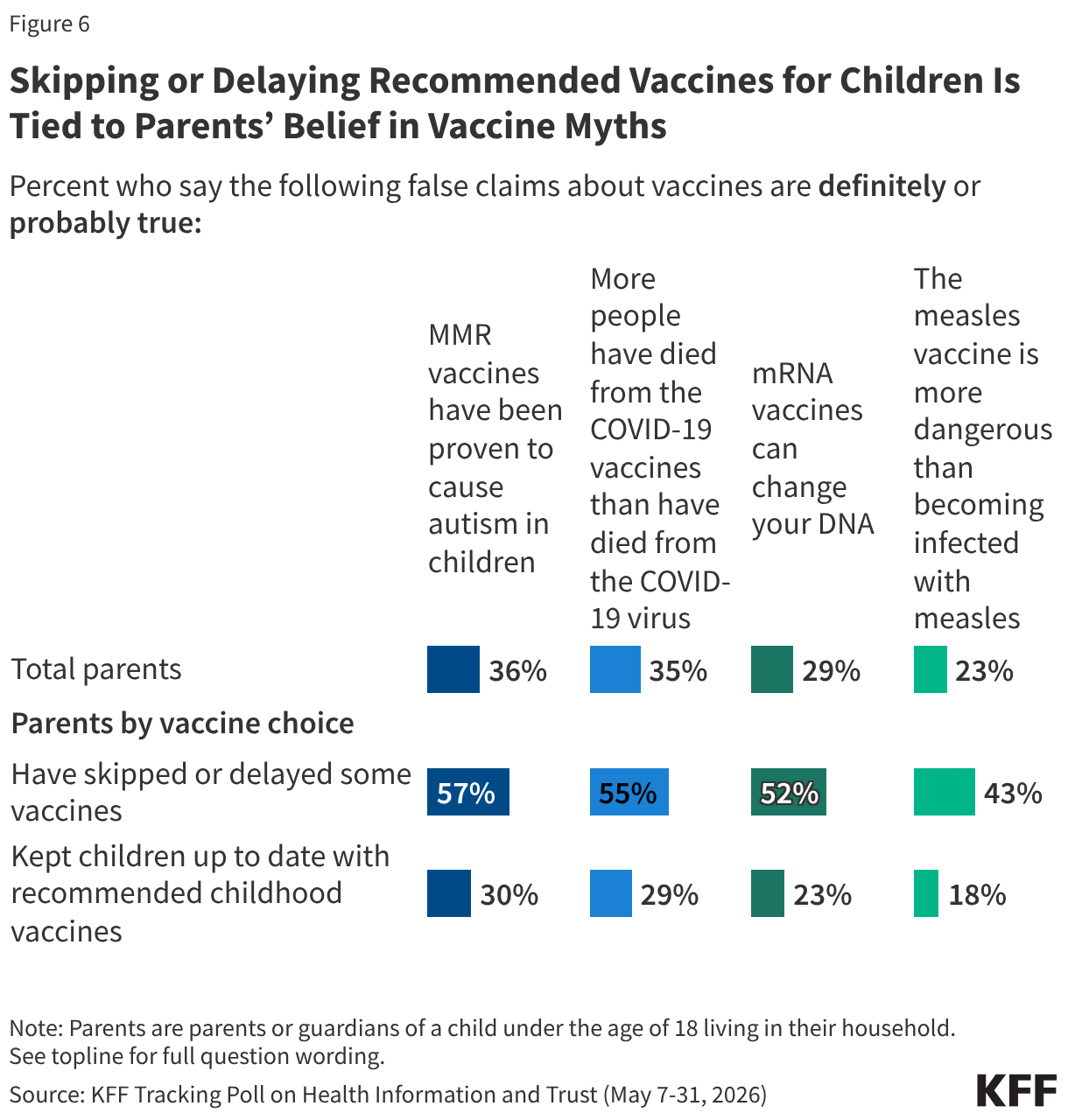
- Parents’ views on vaccine myths are also correlated with their decisions about childhood vaccinations. Parents who report skipping or delaying recommended childhood vaccines are consistently at least 25 percentage points more likely than those who keep their children up-to-date to say vaccine myths are “definitely” or “probably true,” including the false claims that MMR vaccines cause autism in children (57% v. 30%), that more people died from COVID-19 vaccines than the virus itself (55% v. 29%), that mRNA vaccines alter DNA (52% v. 23%), and that measles vaccines are more dangerous than measles (43% v. 18%). This relationship remains significant even when controlling for factors like age, education, and partisanship.
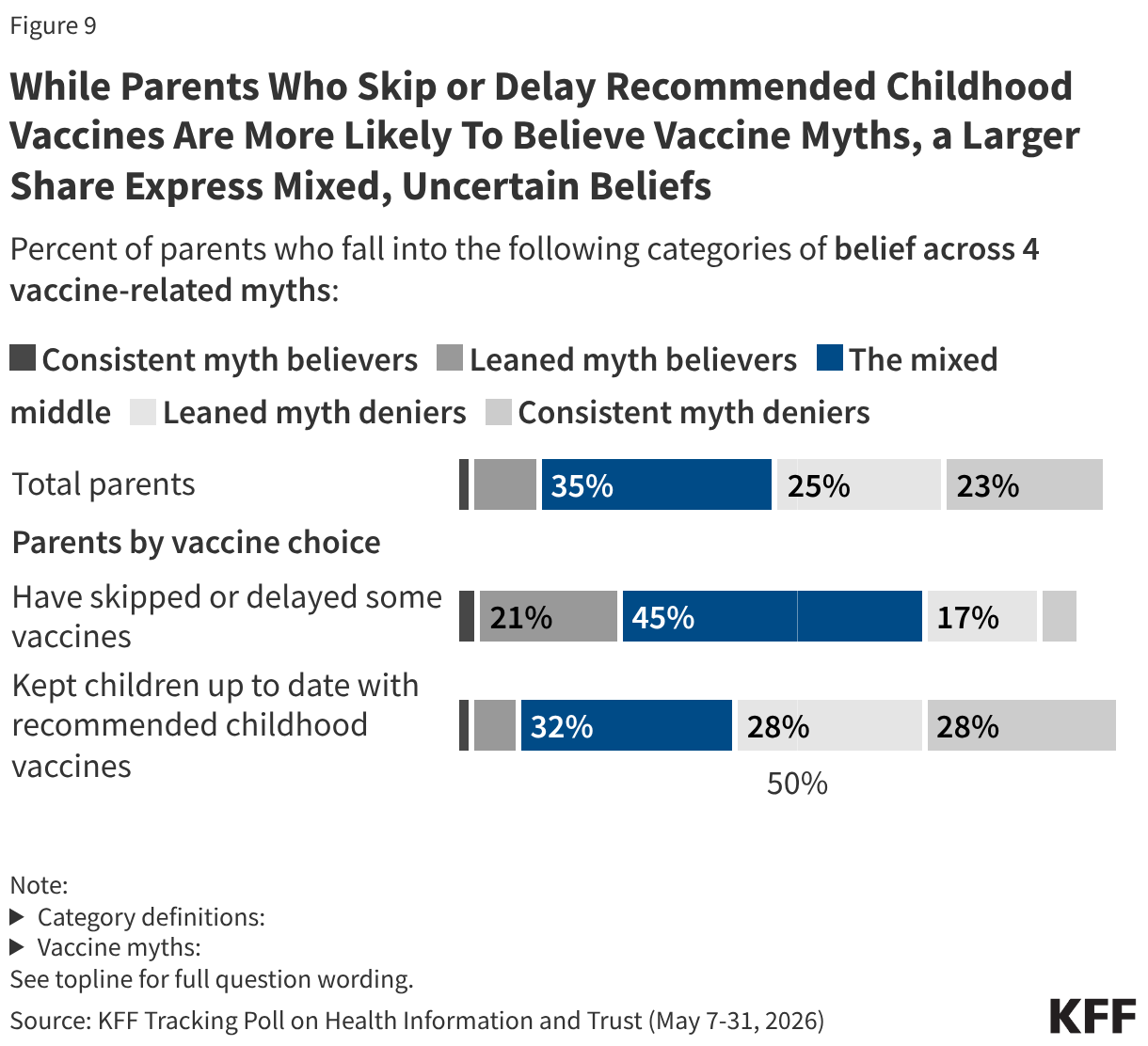
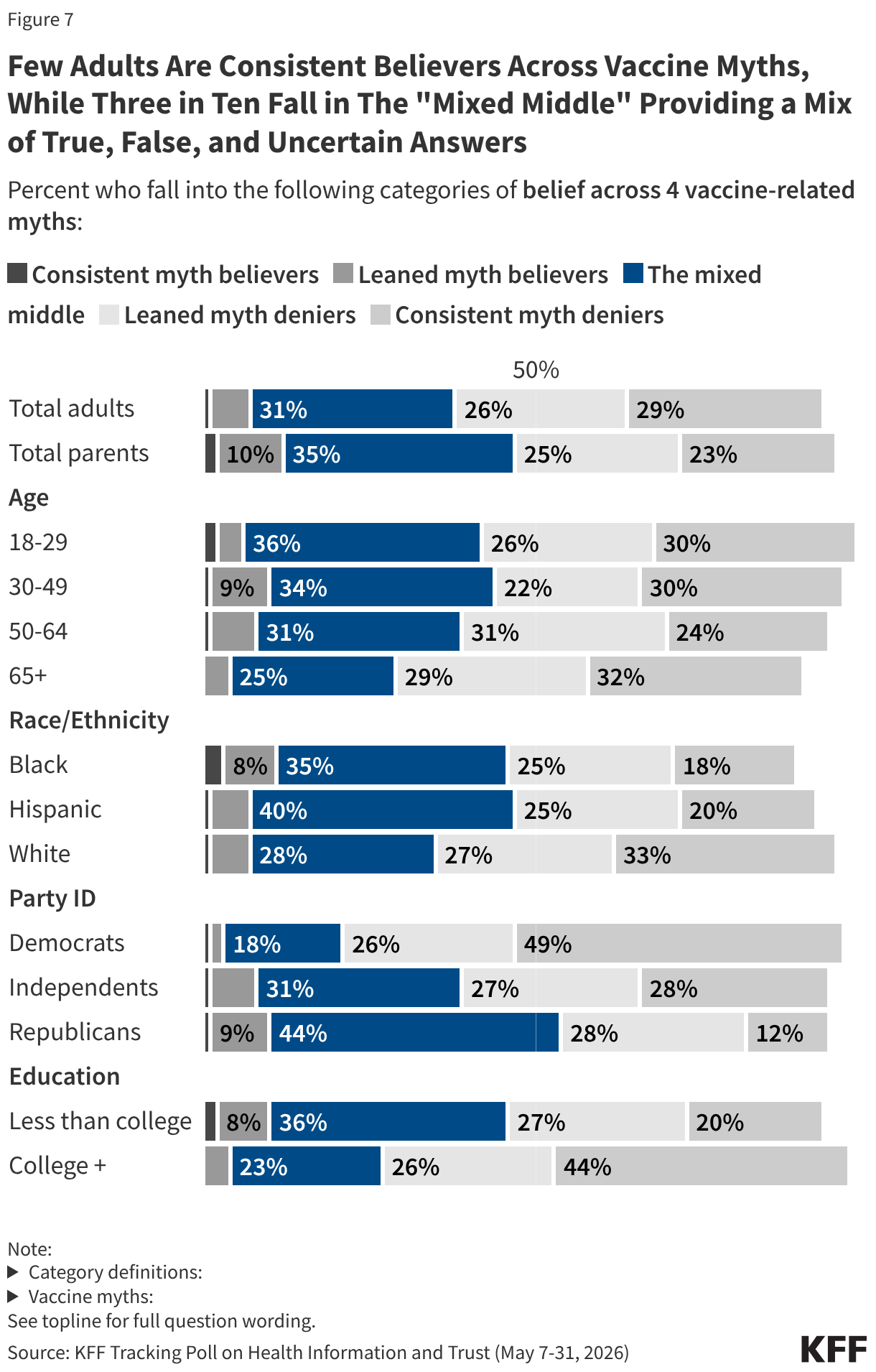
- When looking at patterns of belief across the four false vaccine claims, a new analysis shows that some adults are consistent or leaned myth believers (8% who say all four claims are either “probably” or “definitely true”), or myth deniers (55% who deny all four claims, saying they are either “probably” or “definitely false”). At the same time, about three in ten (31%) fall in a “mixed middle” group, providing a range of true and false answers across the four vaccine myths and lacking certainty on at least half of the false claims. This group may be an important focus for those looking to counter vaccine misinformation and dispel confusion. Black adults, Hispanic adults, Republicans, younger adults, and those without a college degree are all more likely than their counterparts to fall into this “mixed middle” group, as are individuals who go to social media or AI for health information. Notably, nearly half of parents who report skipping or delaying recommended vaccines for their children fall in the “mixed middle,” indicating that these parents’ decisions may be driven, at least in part, by uncertainty and confusion.
Exposure to Common Vaccine Myths
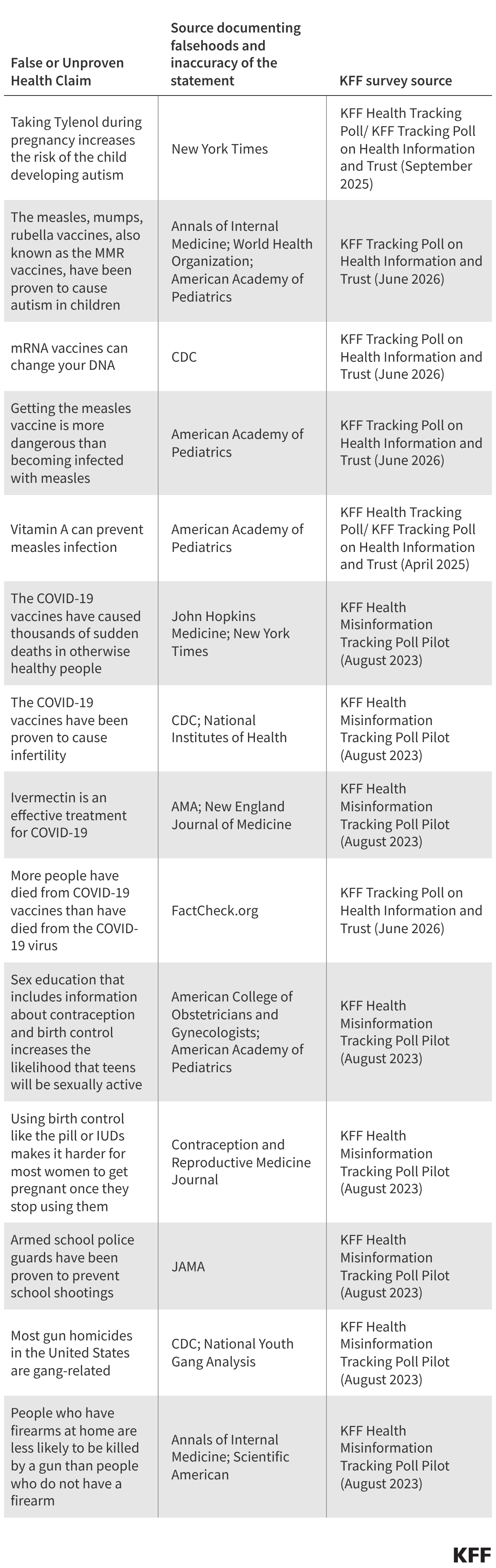
The latest KFF Tracking Poll on Health Information and Trust examines the pervasiveness of several commonly circulated vaccine myths. These false or unproven claims about vaccines have remained persistent in terms of exposure over the past several years, with little change to the share of the public have heard most of these myths.
The false claim that MMR vaccines have been proven to cause autism in children – a myth associated with a since retracted study from the 1990s – remains one of the most widely heard vaccine myths, with two-thirds of adults saying they have heard or read this. Nearly half (46%) of adults say they have heard the false claim that more people have died from the COVID-19 vaccines than the virus itself, and about one third of adults (36%) say they have heard the myth that mRNA vaccines can change your DNA (mRNA is a vaccine technology utilized by some COVID-19 vaccines and others under development). About three in ten adults (29%) say they have heard the false claim that measles vaccines are more dangerous than measles infections.
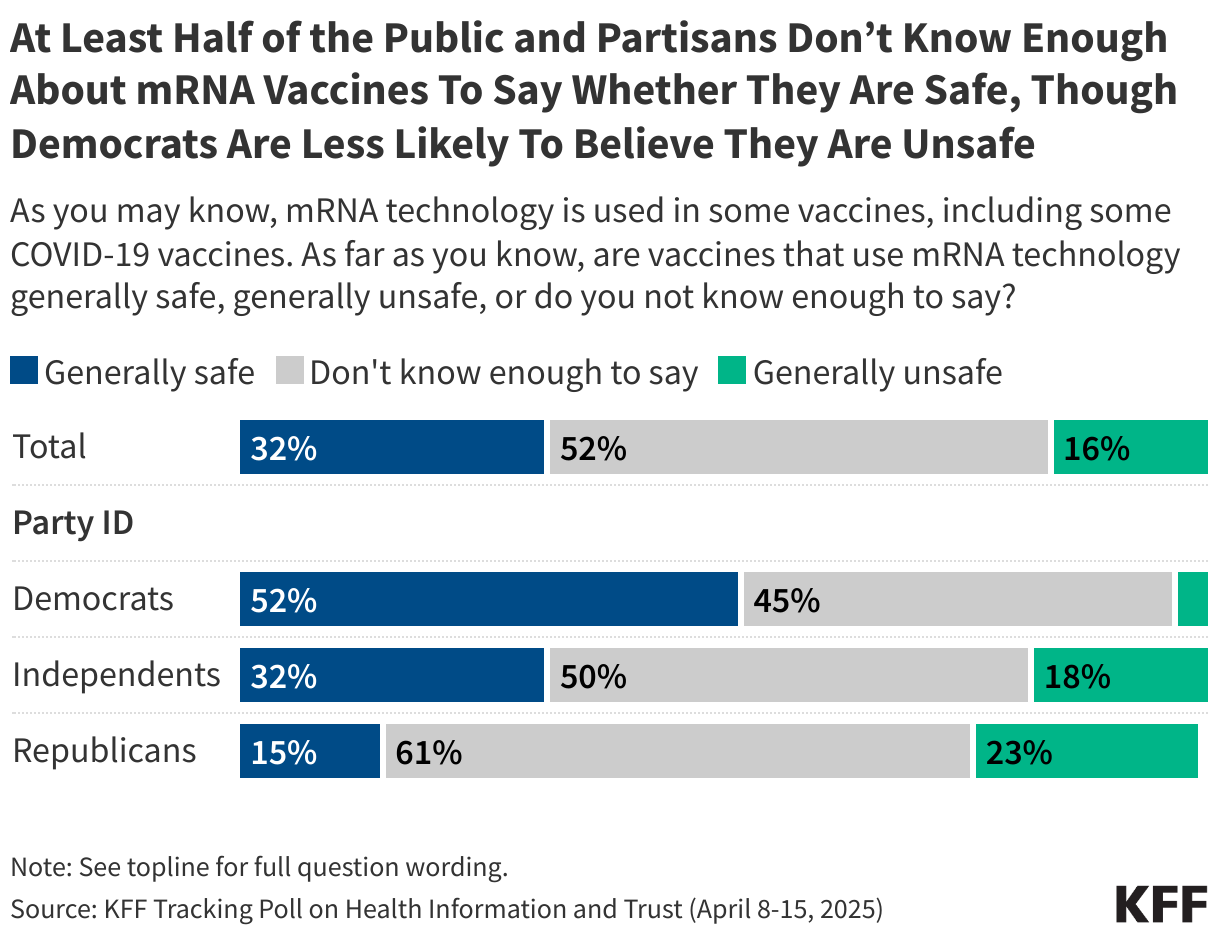
Exposure to each of these false claims has been fairly steady in KFF polls over the past several years, though the share who report hearing the myth that mRNA vaccines can alter a person’s DNA dropped by 9 percentage points since April 2025 (from 45% to 36%). Exposure to the myth that measles vaccines are more dangerous than measles rose between 2024 and 2025, but has remained steady since then.
Figure 1
Uncertainty Surrounding False Vaccine Claims
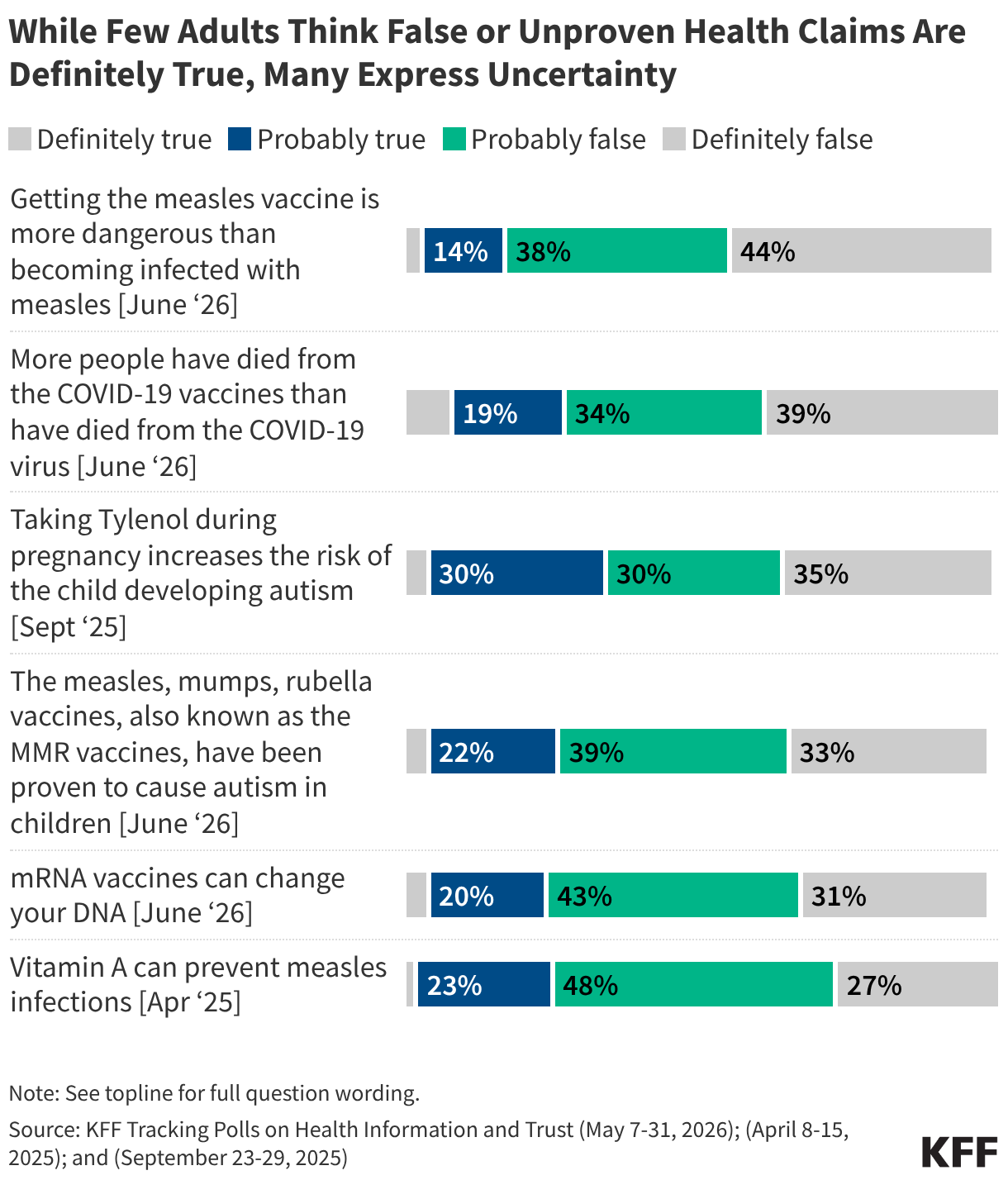
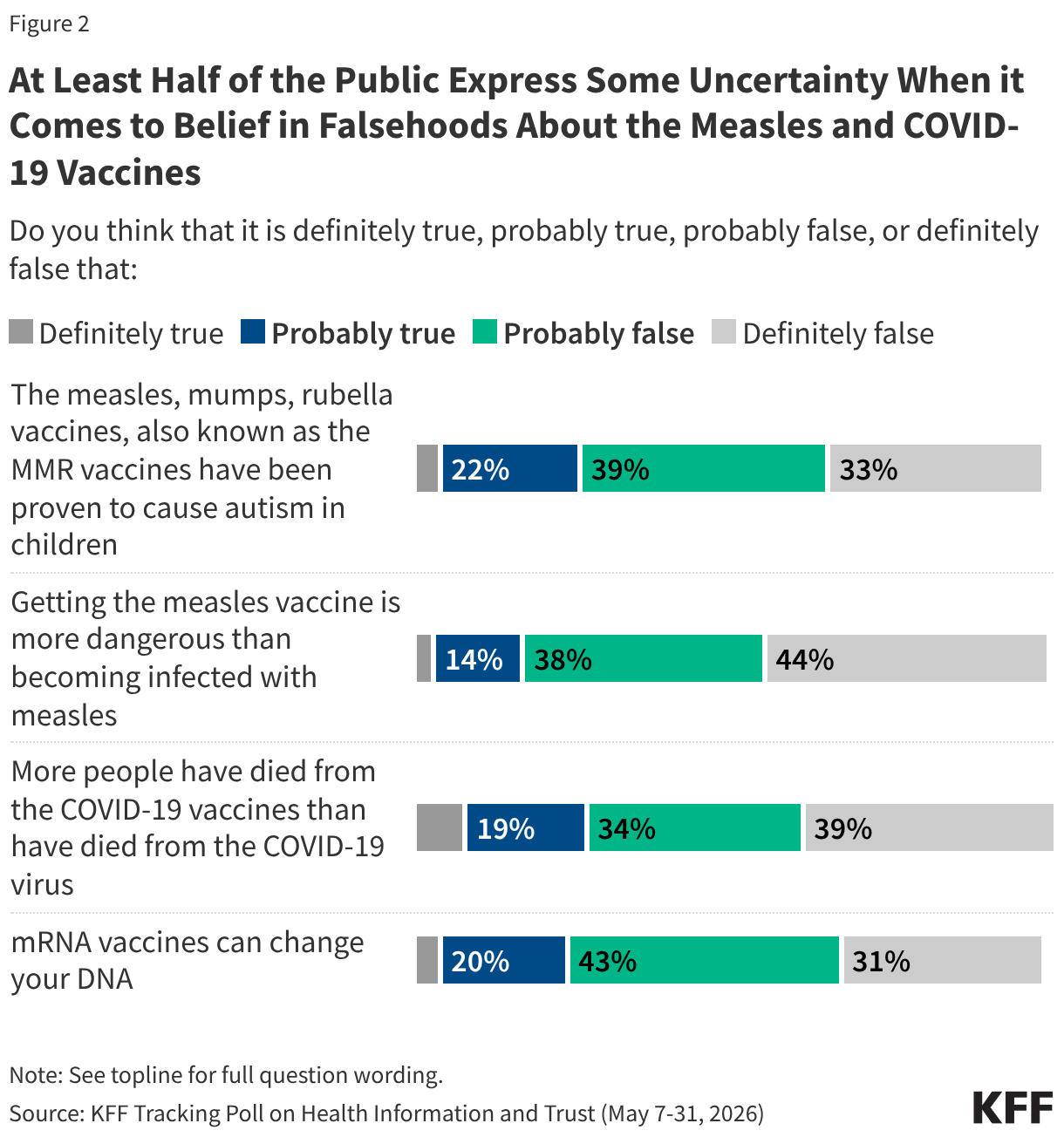
While many report having heard some false claims about vaccines, very few adults are ardent believers in these myths, with larger shares (but fewer than half) stating the myths are “definitely false.” At the same time, and consistent with past KFF polling, at least half of adults fall into the “malleable middle” across the myths, expressing some uncertainty and saying these vaccine myths are either “probably true” or “probably false.” Across these four vaccine falsehoods, most parents fall into the malleable middle, expressing some uncertainty for each claim.
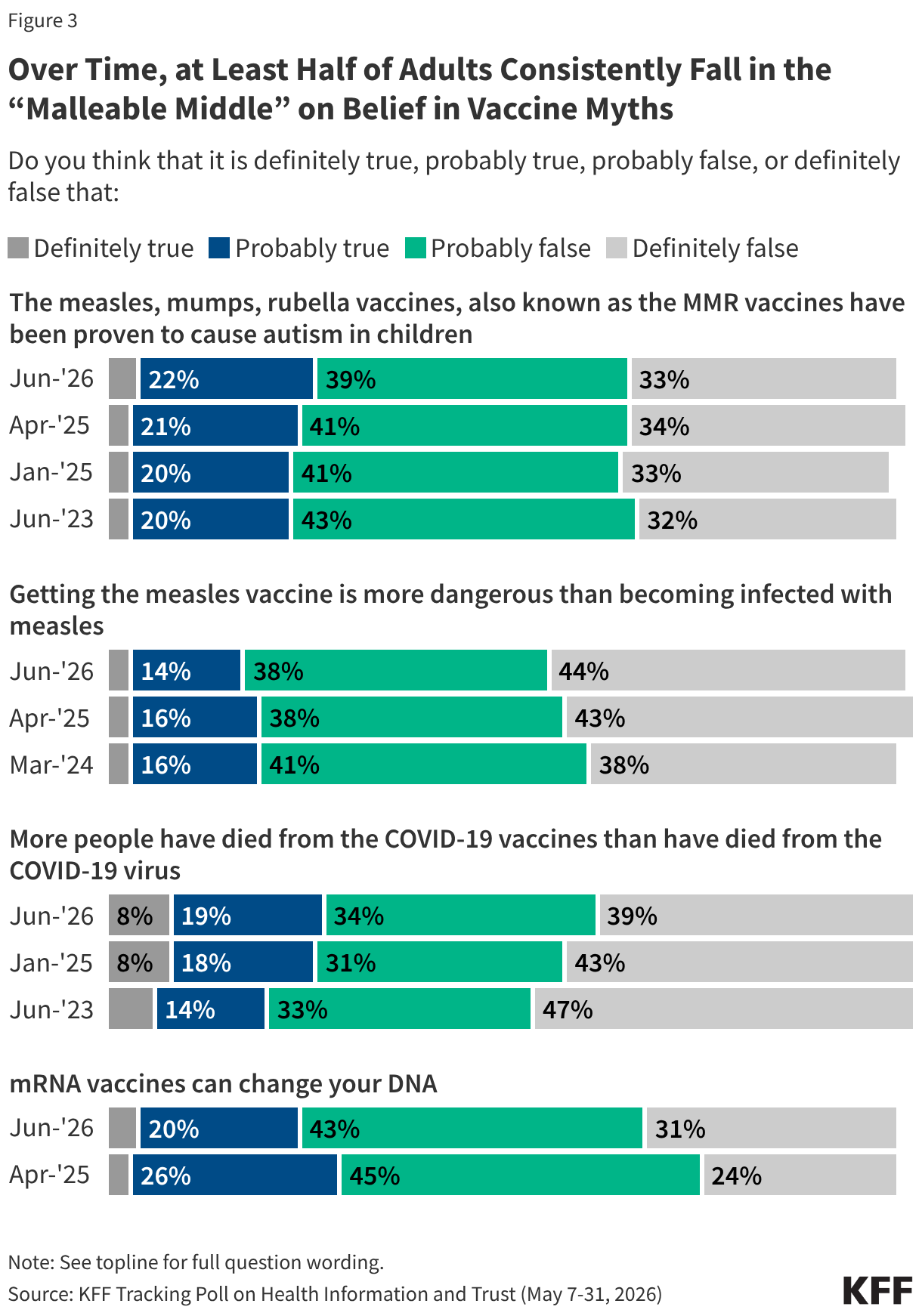
Over time, the share who fall in the “malleable middle” for these vaccine myths has been relatively stable, with at least half saying each is either “probably true” or “probably false.” At the same time, there have been some minor shifts in the share who view some of these myths as “definitely false” over the past few years, underscoring how the public’s willingness to endorse vaccine falsehoods is not completely static. Somewhat larger shares of adults now say it is “definitely false” that mRNA vaccines can change your DNA (31% now v. 24% in April 2025), and that measles vaccines are more dangerous than getting infected with measles (44% now v. 38% in March 2024). Conversely, the share of adults who think it is “definitely false” that more people have died from COVID-19 vaccines than from the virus has declined (39% now compared to 47% in June 2023) alongside a 5-percentage point jump in the share who say this myth is “probably true.” There have been no notable changes in views of the long-standing myth that MMR vaccines cause autism.
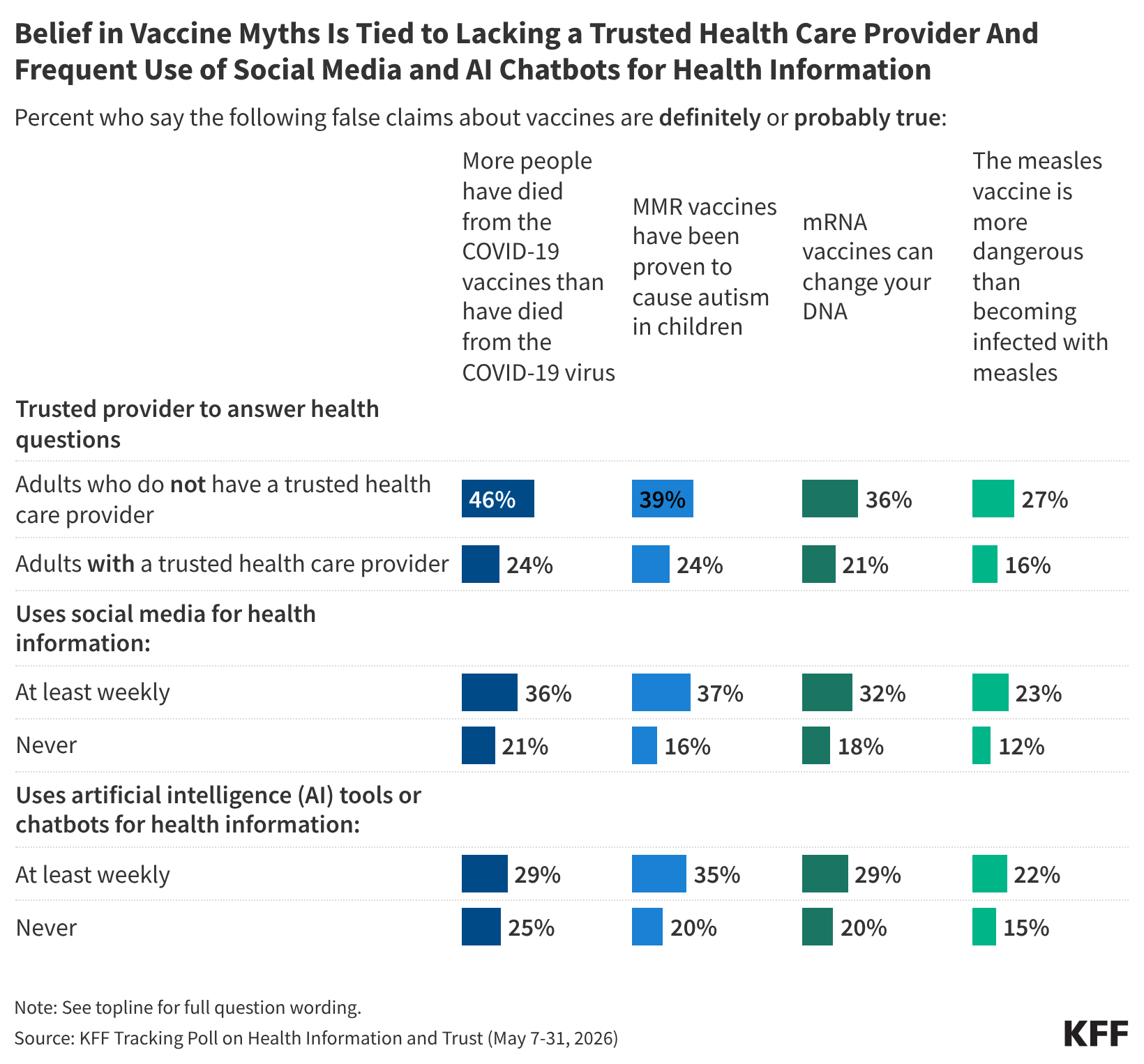
Previous KFF polls have shown that health care providers are the most trusted source of health information among the public, and this latest poll shows that individuals who have a trusted provider are less likely than those without a trusted provider to endorse vaccine-related myths. For example, among adults who say they do not have a doctor or health care provider they trust to answer questions about their health (16% of all adults), nearly half (46%) say it is either “definitely” or “probably true” that more people have died from COVID-19 vaccines than from the COVID-19 virus, compared to a quarter (24%) among those who say they have a trusted health care provider.
Unsurprisingly, adults who say they do not have a trusted health care provider to answer their health questions are much more likely to be uninsured than those who have a provider they trust (36% v. 7%). At the same time, lacking a trusted provider could be related to low trust in providers and doctors more broadly and not necessarily related to health care access. Across demographics, adults under age 50, LGBT adults, and Hispanic adults are all more likely than their counterparts to say they don’t have a provider they trust to answer questions about their health. However, the connection between not having a trusted provider and belief in vaccine myths remains significant even when controlling for factors like age, race and ethnicity, education, partisanship, and insurance coverage.
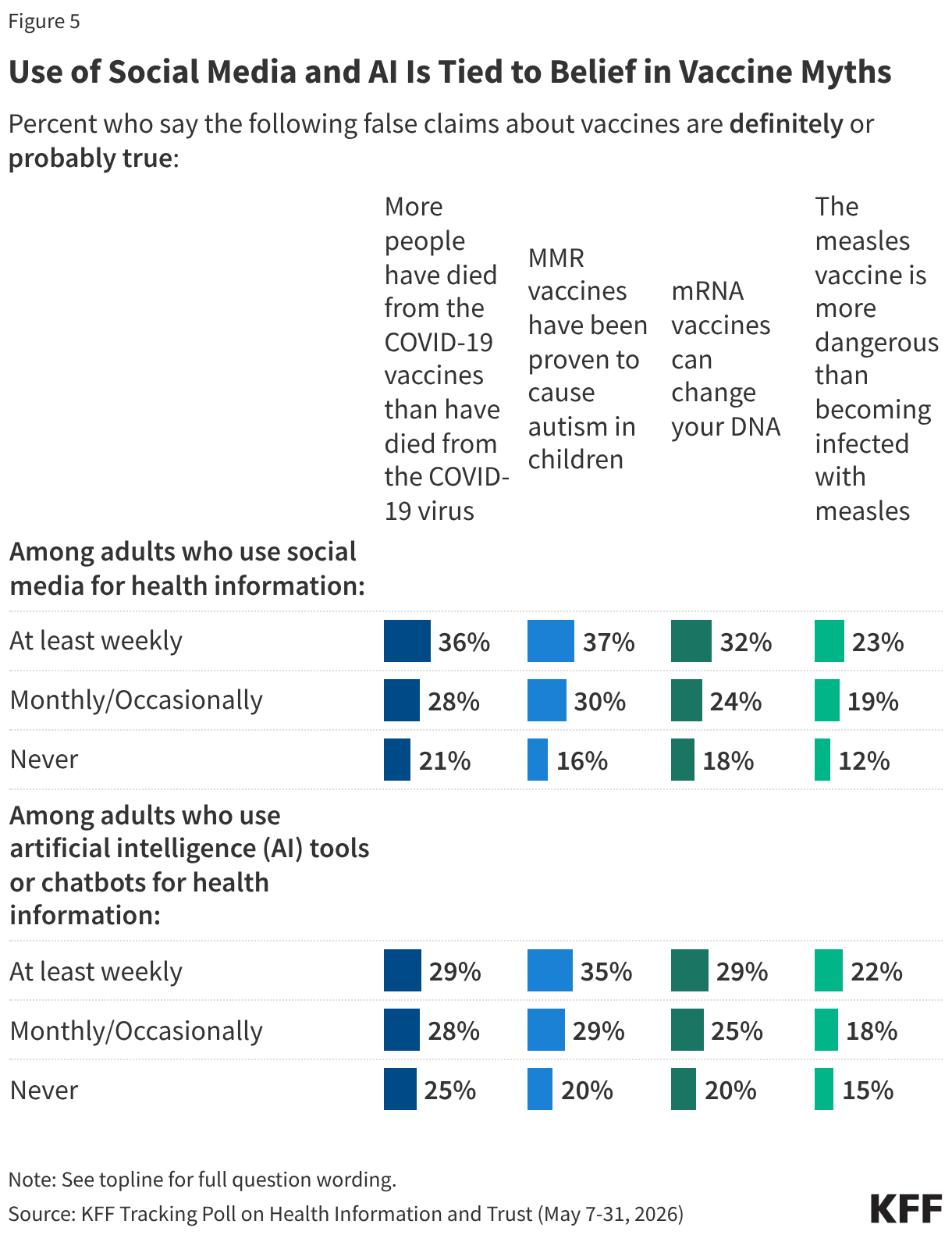
Frequent health information-seeking on social media and via artificial intelligence (AI) chatbots is also tied to a tendency to believe vaccine myths. Adults who say they use social media for health information and advice at least weekly (26% of all adults) are more likely than those who never use social media for health to say each false vaccine claim is “probably” or “definitely true.” Similarly, adults who report using AI tools or chatbots at least weekly for health advice (20% of all adults) are more likely than those who never use these chatbots to endorse myths about the measles vaccines and mRNA vaccines. For example, the share who say it is “probably” or “definitely true” that MMR vaccines have been proven to cause autism is higher among adults who seek health advice at least weekly from social media (37%) or AI (35%) compared to those who never use social media (16%) or AI (20%) for health advice.
The relationship between belief in vaccine myths and use of social media or AI for health information continues to be significant even when controlling for factors like age, race and ethnicity, education, and partisanship.
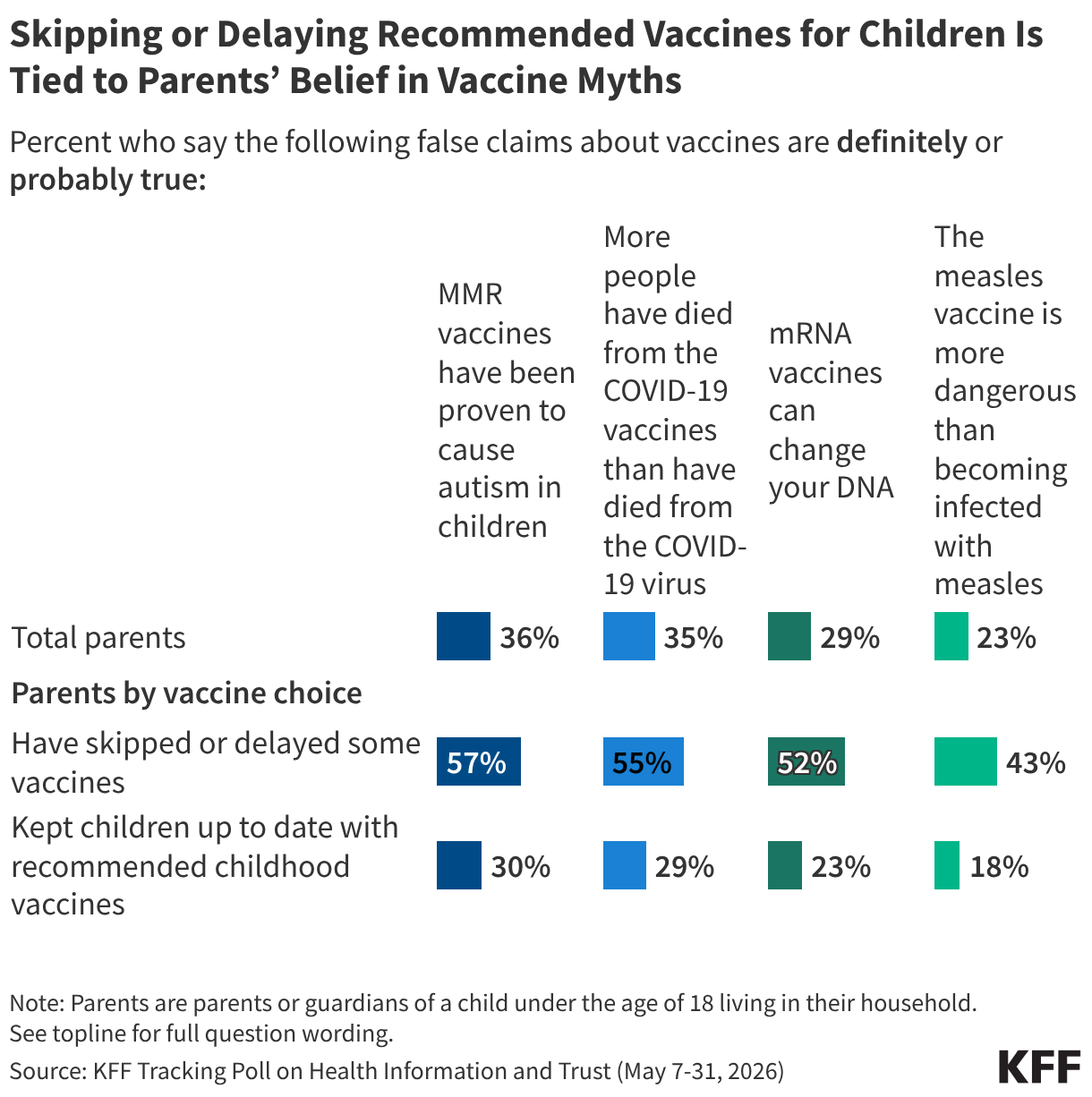
Parents who skip or delay recommended vaccines for their children are about twice as likely as parents who keep their children up to date on vaccines to believe or lean toward believing false claims about the measles and COVID-19 vaccines, underscoring how false health claims may shape parents’ decisions.
Overall, at least three in ten parents say it is “probably” or “definitely true” that MMR vaccines have been proven to cause autism in children (36%), that more people have died from COVID-19 vaccines than the virus (35%), or that mRNA vaccines can alter DNA (29%). About one in four (23%) parents believe or lean toward believing the myth that measles vaccines are more dangerous than measles.
The tendency to endorse these false vaccine claims, however, rises substantially among parents who report not keeping their children up to date on recommended vaccines. Six in ten (57%) parents who report having skipped or delayed recommended childhood vaccines (excluding seasonal vaccines for COVID-19 and flu), say it is either “definitely true” or “probably true” that the MMR vaccines have been proven to cause autism in children, while around half believe or lean toward believing that the COVID-19 vaccines killed more people than the virus (55%), or that mRNA vaccines alter DNA (52%). About four in ten (43%) parents who skipped or delayed childhood vaccines say it is true that the measles vaccines are more dangerous than measles itself. Each of these shares is at least 25 percentage points higher than among parents who report keeping their children up to date on recommended childhood vaccines, a relationship that remains significant even when controlling for factors like age, education, and partisanship.
Digging Deeper on The Malleable Middle: Patterns of Belief Across Vaccine Myths
While KFF polling has routinely found that at least half the public fall in the “malleable middle” when it comes to a wide variety of false health claims, there are nuances within this group that can be examined by looking at patterns of belief across multiple myths rather than examining a single question.
This new typology identified five groups based off patterns of belief across the four false vaccine claims included in this survey:
- Consistent myth believers (1% of the public) say all four vaccine myths are true, including at least three out of four as “definitely true.”
- Leaned myth believers (6% of the public) say all four vaccine myths are true but are somewhat uncertain in their beliefs, saying at least two of the four myths are “probably true.”
- The mixed middle (31% of the public) provide a range of true and false responses and at least half of the time provide a “probably” response (in either the true or false direction).
- Leaned myth deniers (26% of the public) say all four vaccine myths are false but are somewhat uncertain, saying at least two of the four myths are “probably false.”
- Consistent myth deniers (29% of the public) say all four vaccine myths are false, including at least three out of four as “definitely false.”
The “mixed middle” group, making up 31% of all adults, reflects a portion of the “malleable middle” that expresses the most uncertainty and does not routinely land on one side when it comes to commonly circulating vaccine falsehoods. The share who fall in the “mixed middle” differs by partisanship, education, race and ethnicity, and age. For example, four in ten Hispanic adults and about a third (35%) of Black adults are part of this group compared to fewer than three in ten white adults (28%). Republicans (44%) are more than twice as likely as Democrats (18%) to be part of this group, while independents (31%) fall in between the two. Those without a college degree (36%) are also 10 percentage points more likely than college graduates (23%) to fall into this mixed middle group. These findings suggest these groups who disproportionately fall in the “mixed middle” may be an important focus for those looking to counter vaccine misinformation and dispel confusion.
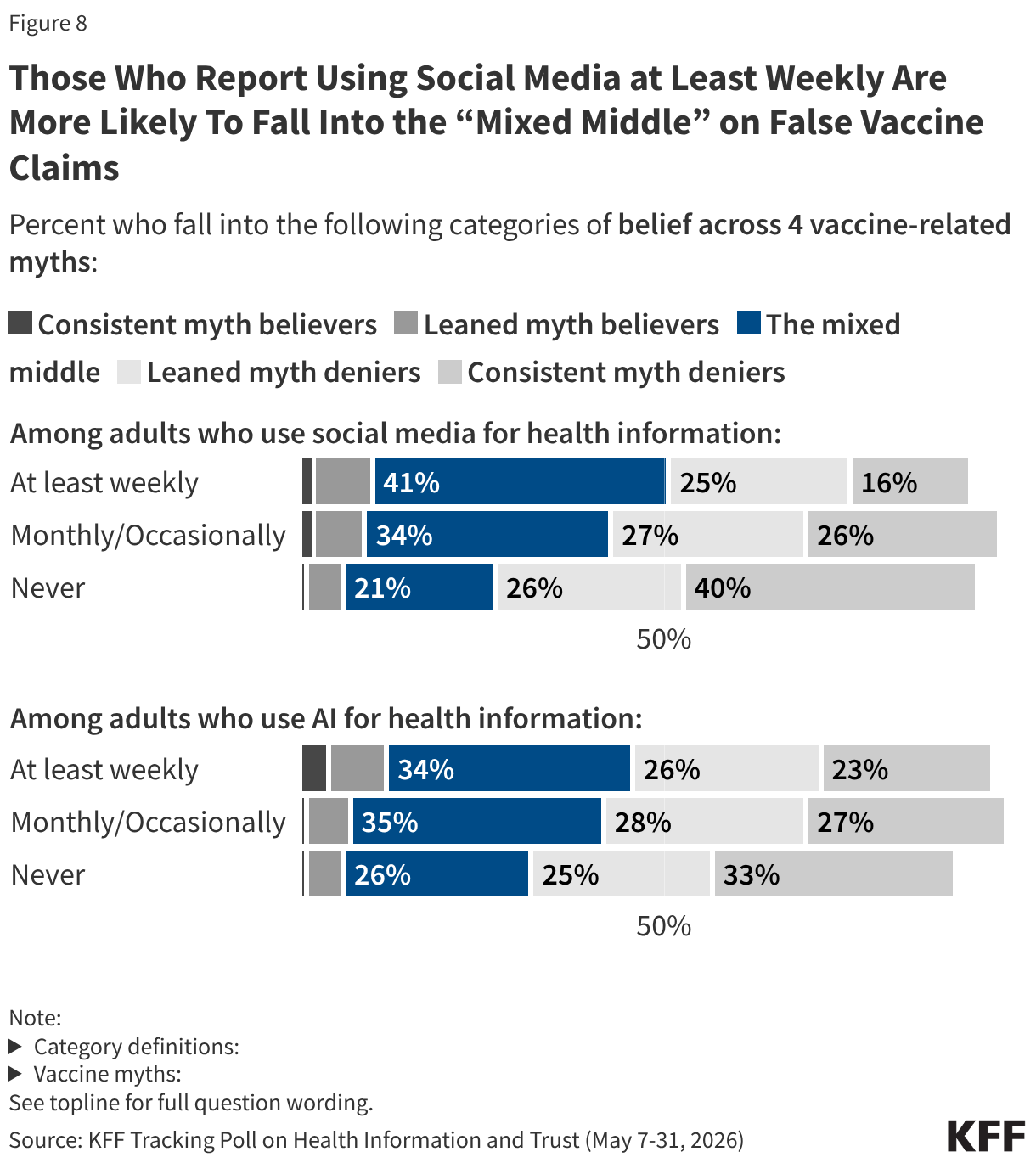
Adults who are frequently using social media for health advice are also more likely to lack certainty across vaccine myths, providing a range of mixed answers and saying at least half of the four myths are either “probably true” or “probably false.” When looking at belief across different vaccine myths, adults who report using social media for health information on at least a weekly basis are twice as likely to fall in the “mixed middle” group as those who never use social media for health (41% v. 21%). Adults who use AI tools for health information at least occasionally are also somewhat more likely to fall into the “mixed middle” compared to those who never use AI for health, but the difference is smaller for AI than it is for social media use.
Nearly half (45%) of parentswho have skipped or delayed recommended vaccines for their children fall in this “mixed middle” group, underscoring the connection between confusion, uncertainty and parents’ decisions to forgo recommended vaccines for their children.