KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
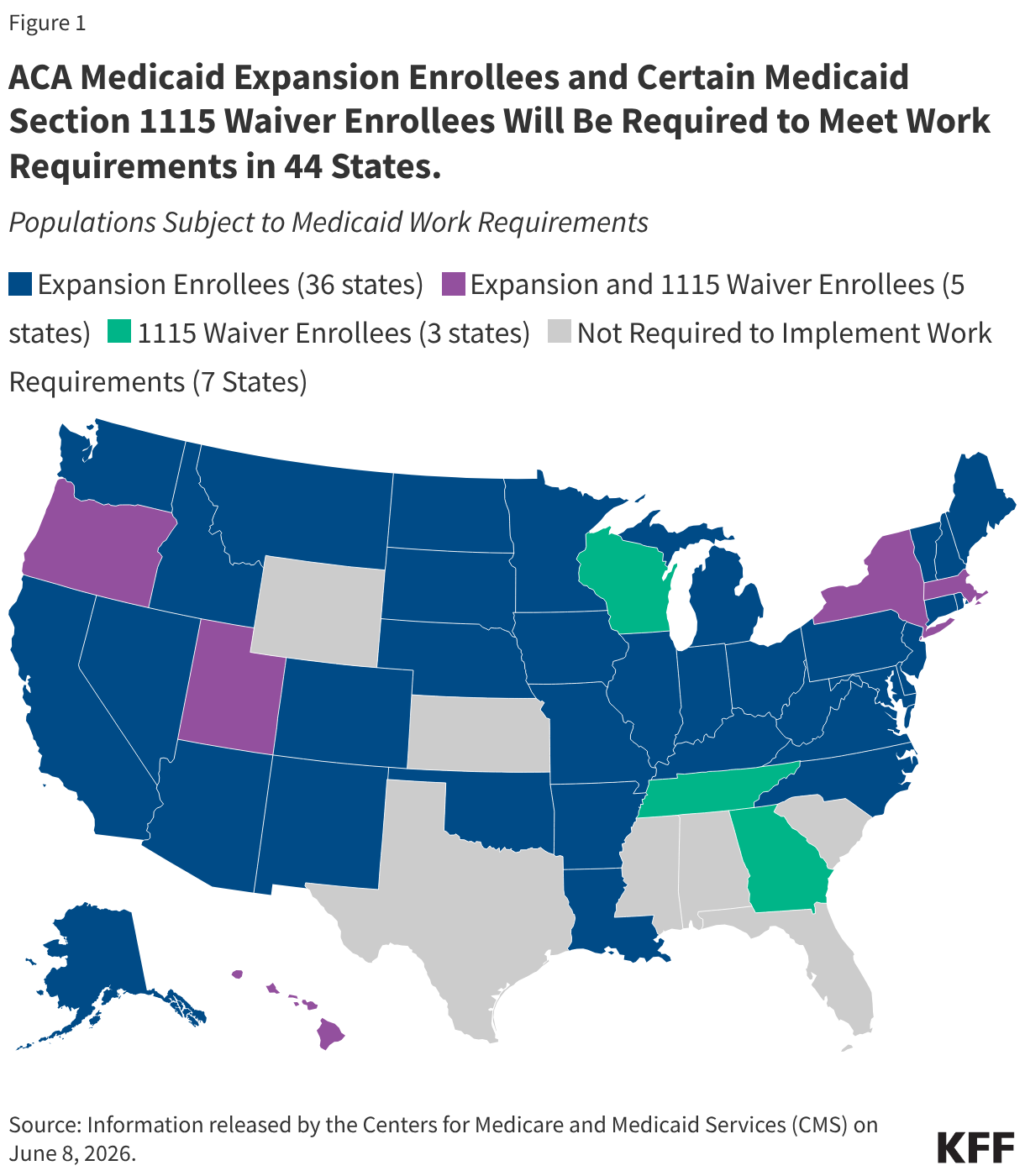
The 2025 reconciliation law, once called the “One Big Beautiful Bill,” signed by President Trump on July 4, 2025, requires 44 states (including DC) to condition Medicaid eligibility for adults in the Affordable Care Act (ACA) Medicaid expansion group and certain enrollees in 1115 waiver programs on meeting work requirements starting January 1, 2027. Currently, 41 states (including DC) have expanded their Medicaid programs under the ACA to nearly all adults with income up to 138% FPL ($21,597 for an individual in 2025). In June 2026, CMS released a list of states with 1115 waiver programs that include individuals who will be subject to work requirements. The list identifies waiver programs in three non-expansion states Georgia, Tennessee, and Wisconsin, as well as in five expansion states, Hawaii, Massachusetts, New York, Oregon, and Utah (Figure 1).
To implement Medicaid work requirements, states will need to make important policy and operational decisions, implement needed system upgrades or changes, develop new outreach and education strategies, and hire and train staff, all within a relatively short timeframe. The information tracked here can serve as a resource to understand Medicaid work requirements and state options, gauge readiness, and track implementation of the requirements, including:
NEW: State reported plans and policies related to implementing Medicaid work requirements and county-level unemployment rate data, as well as state and national data on Medicaid enrollment, renewal outcomes, and application processing times;
A compilation of KFF issue briefs and other resources on Medicaid work requirements.
This resource will be updated to include guidance from the Centers for Medicare and Medicaid Services (CMS), information on state policy decisions as they are made, and new data when available.
Continue scrolling to learn more about the Medicaid work requirements in the 2025 reconciliation law.
Editorial note: Originally published on June 11, 2026, this brief has been updated to reflect additional information about carriers’ plans for 2027.
As of June 22, 2026, six carriers have announced that they will exit the ACA Marketplaces in plan year 2027, either in some or all states that they are currently offering plans; four carriers have announced they will enter new state Marketplaces. These changes in insurer participation follow the expiration of the enhanced premium tax credits at the end of 2025, which drove sign-ups to fall by over a million from the 2025 to 2026 Open Enrollment Periods—with further membership declines in the ACA Marketplaces expected as the year progresses. ACA Marketplace enrollment declines affect the size of the potential market for insurers, and, potentially, the risk pool—to the extent that healthier than average enrollees are more likely to drop coverage.
As people leave the Marketplace, insurers may reassess the profitability of their Marketplace participation and decide to pull out in the future. Cigna has decided to leave the individual market in 2027 to focus on other segments given the lack of potential to grow their ACA Marketplace business. Cigna, which reported first-quarter on-exchange enrollment of over 350,000 individuals, will exit the 11 states in which it currently participates both on- and off-exchange. In some cases, multiple insurers are announcing exits in the same state. In some states, with fewer insurers participating in the ACA Marketplaces, remaining insurers will have less competition and consumers will be left with fewer choices.
KFF Poll Shows Three in Ten Adults Turn to Social Media or AI for Health Information, with Lower-Income Adults More Likely to Cite Cost and Access Barriers as a Reason
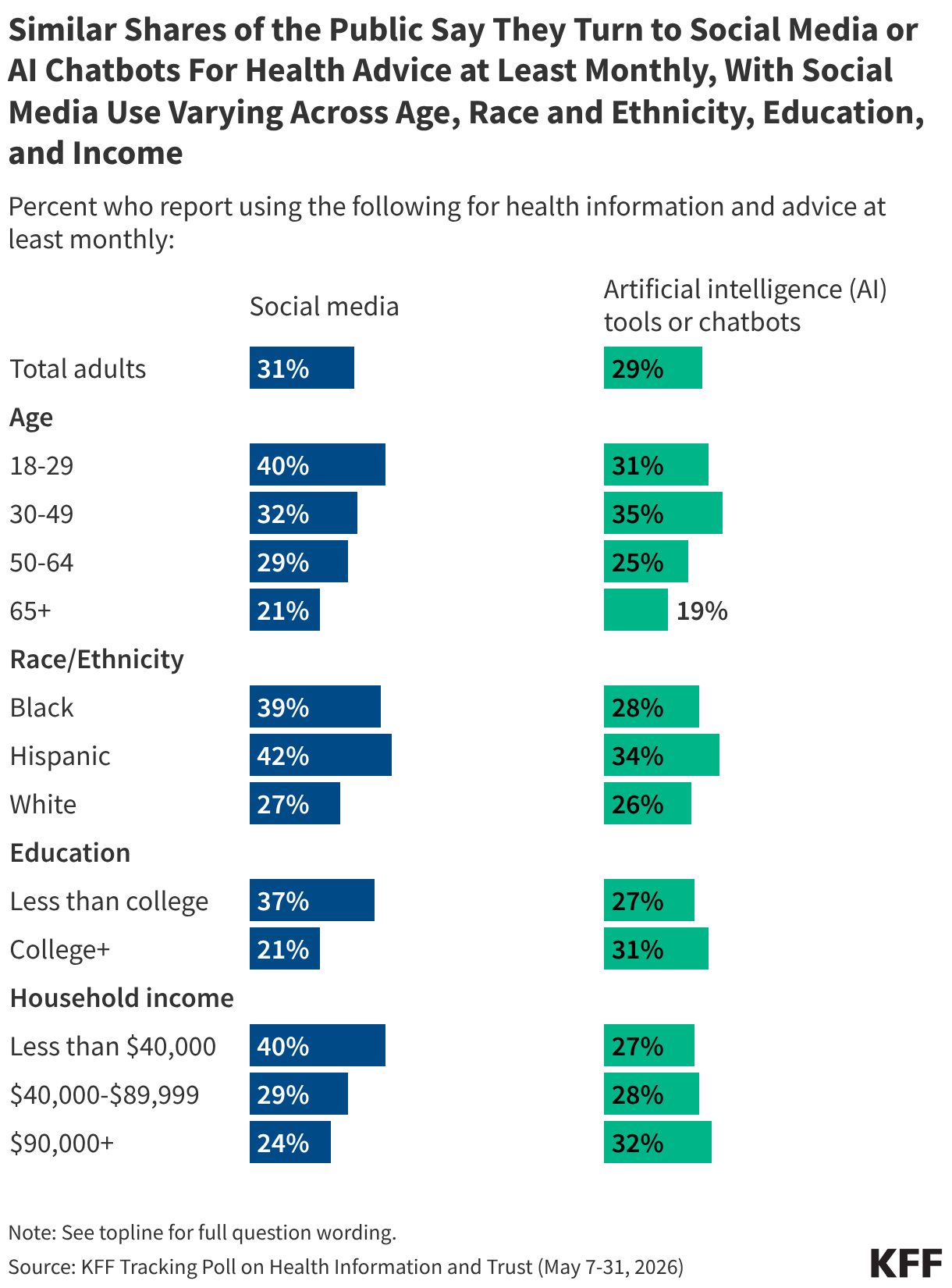
The latest KFF Tracking Poll on Health Information and Trust finds roughly three in ten adults report turning to social media (31%) or AI chatbots (29%) at least monthly for health information and advice. The top reasons people report turning to social media for health advice are wanting to hear from those with similar experiences or a desire for quick information. But nearly one in five say they turned to social media due to difficulties accessing or affording care, similar to the shares who cited access and cost as reasons for turning to AI for health information in a previous KFF poll.
KFF Poll Shows Three in Ten Adults Regularly Turn to Social Media or AI For Health Advice, With Similar Shares of Social Media and AI Users Citing Barriers to Accessing Care as a Reason for Using These Platforms
KFF’s latest Tracking Poll on Health Information and Trust examines the public’s use of social media and AI for health information. Overall, three in ten (31%) adults say they use social media at least monthly for health information and advice, similar to the share (29%) who say they use artificial intelligence (AI) tools or chatbots at least monthly for health. Larger shares of adults under 30, Black and Hispanic adults, those without a college degree, and those with lower incomes say they turn to social media for health information at least monthly.
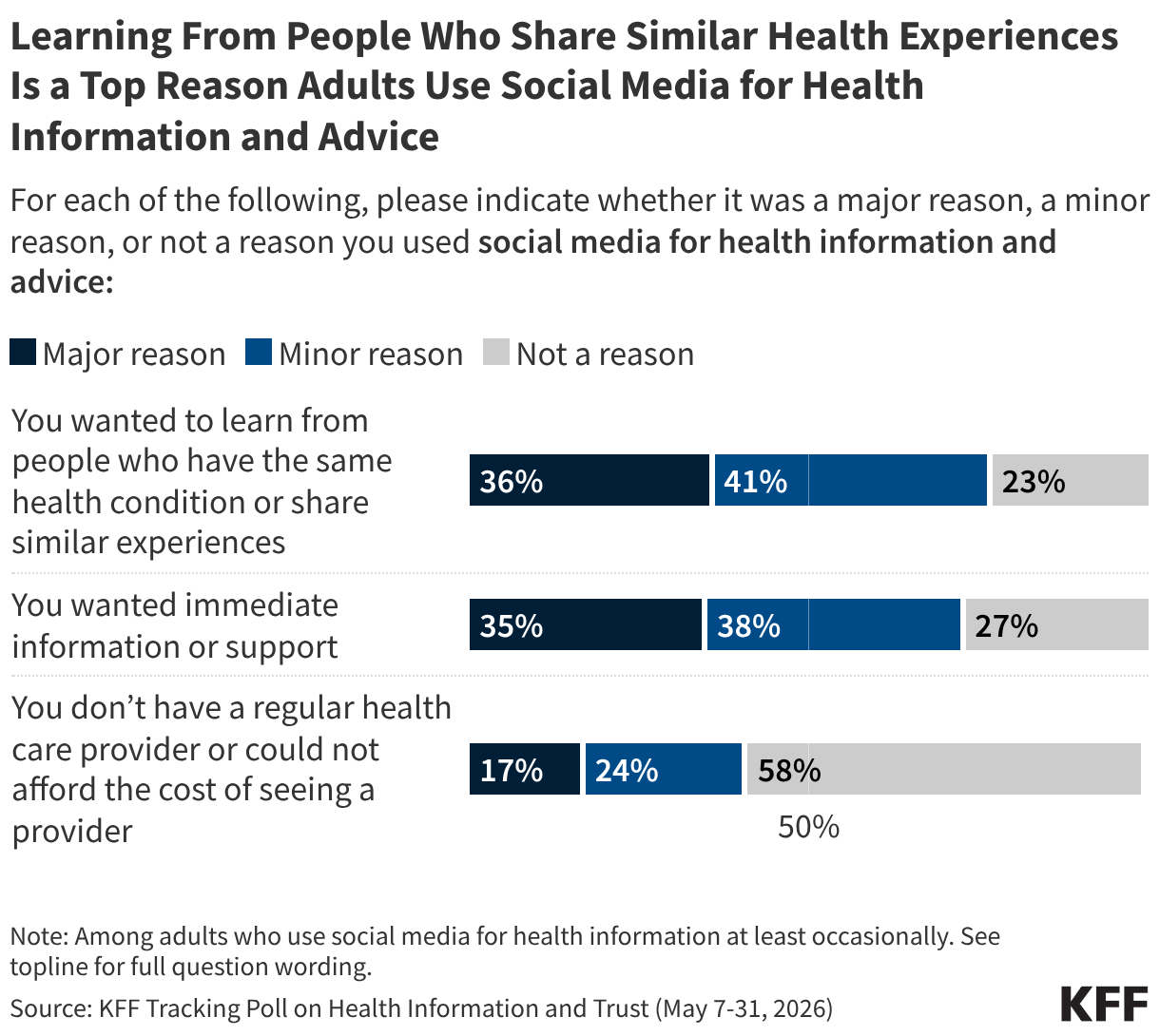
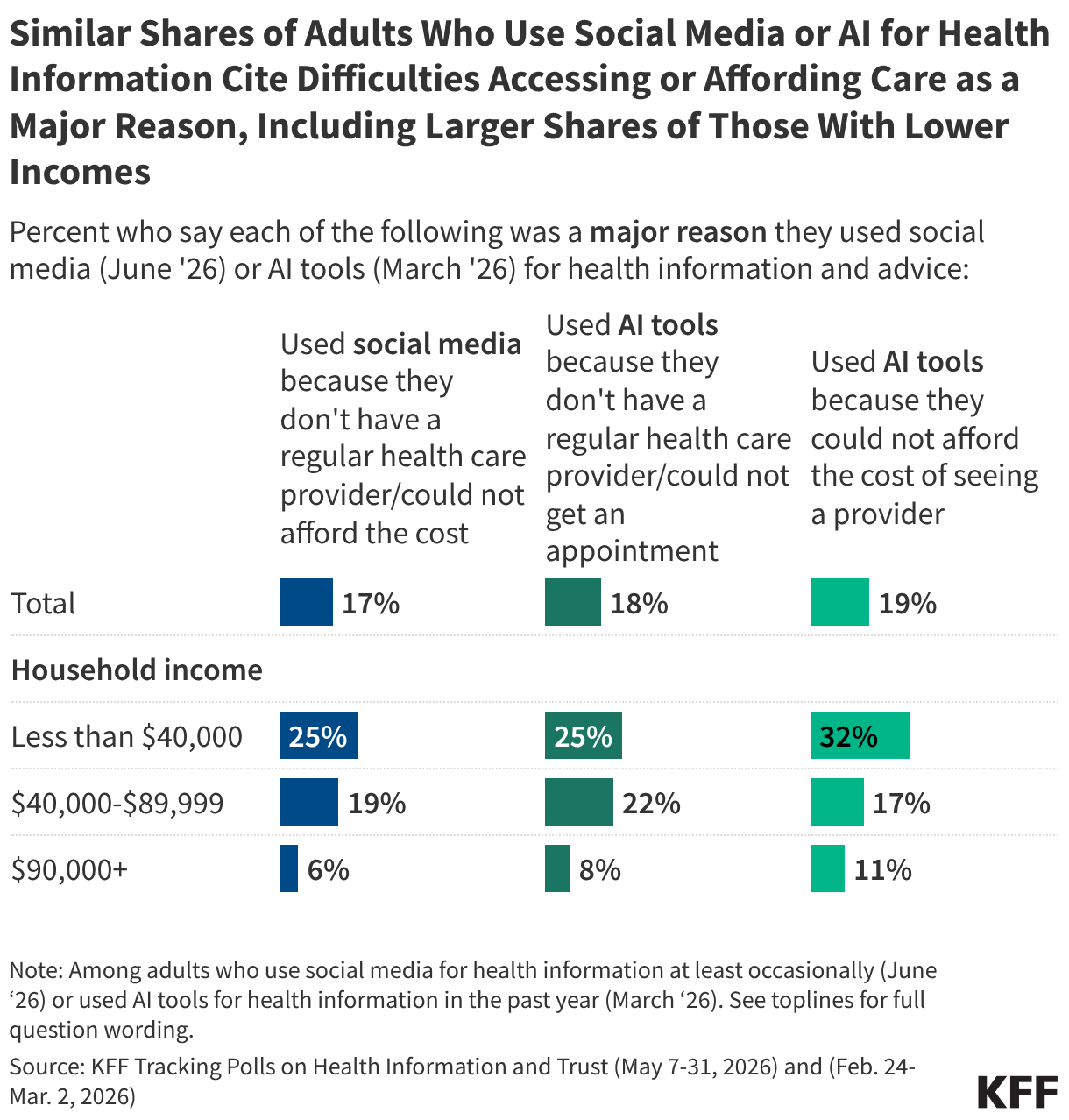
Among people who use social media for health information at least occasionally, over a third say a “major reason” they did so was to learn from others with similar experiences or conditions (36%) or because they wanted immediate information or support (35%). A smaller share of users (17%) say a “major reason” they relied on social media was because they don’t have a health care provider or couldn’t afford to see one.
While cost and access problems may not be the top reason people turn to either social media or AI for health information, nearly one in five users are turning to each of these mediums for these reasons, including even higher shares among those with lower incomes. Among adults who use social media for health, this reason is also more commonly cited among uninsured adults (32%) and some groups that have historically had a harder time accessing health care, including Hispanic adults (29%) and LGBT adults (30%).
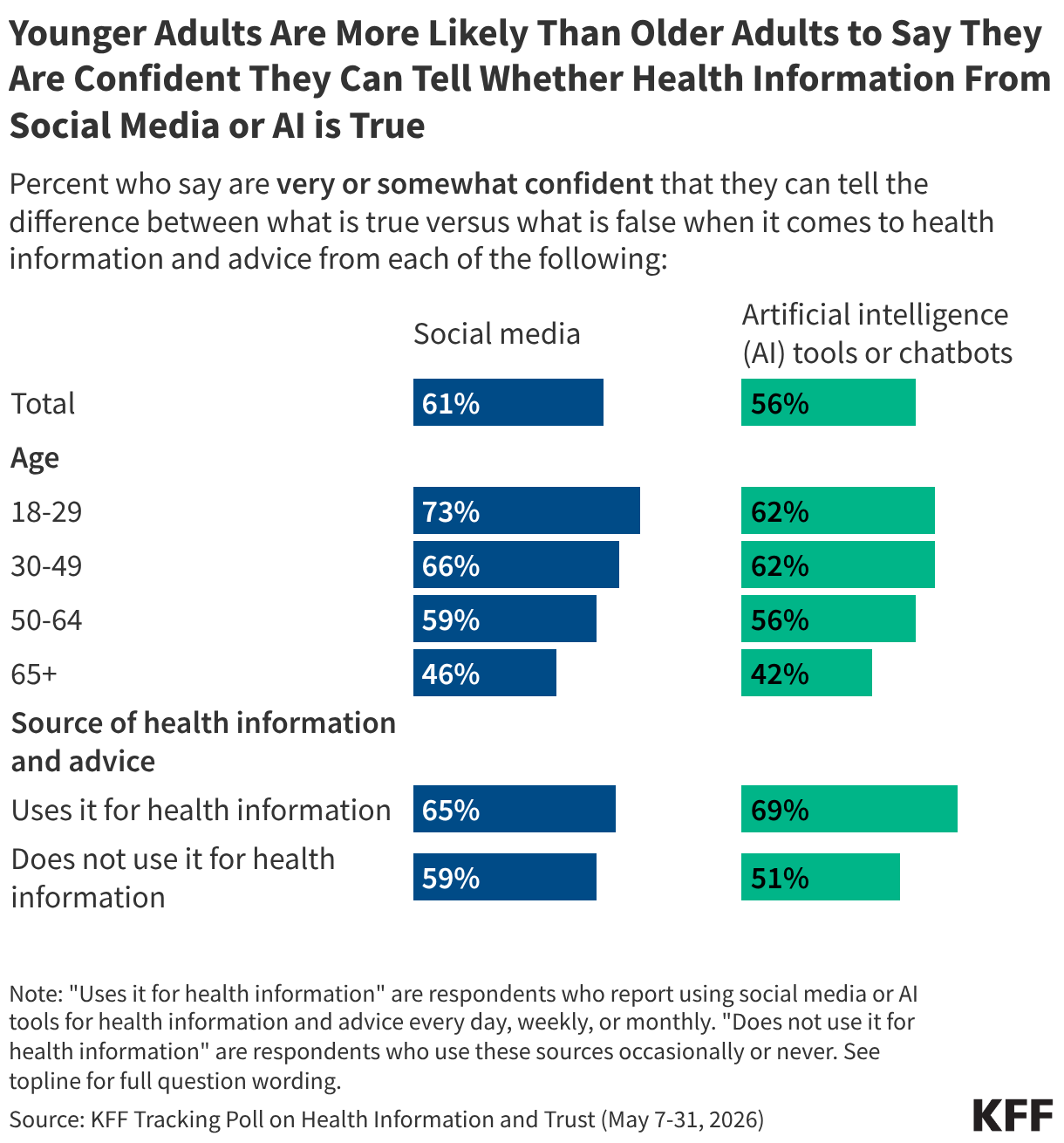
While a slim majority of adults express confidence in their ability to tell whether health information from social media or AI tools is true or not, about four in ten lack confidence in this regard. Adults who use social media and AI for health information are more likely than those who don’t to express confidence in their ability to discern whether health information on these platforms is true or not, as are younger adults compared to older adults.
AI & Emerging Tech
Understanding the Role of AI in Spreading and Creating Faulty Research
A correspondence published in The Lancet in May identified more than 4,000 fabricated references across nearly 2.5 million biomedical papers published between 2023 and early 2026. Researchers found that papers containing at least one fabricated citation became substantially more common during the study period, rising from roughly one in 2,800 papers in 2023 to one in 277 papers in early 2026. Many of the fabricated references appeared legitimate, citing real researchers, plausible publication years, and topic-specific article titles, but pointed to studies that did not exist.
The authors note that large language models (LLMs) are known to generate fabricated citations that appear authentic, and that the sharp rise in fabricated references coincided with the period following widespread adoption of generative AI tools. While the study could not determine what caused the increase, researchers note that fabricated references can emerge through multiple pathways, including AI-generated citations, paper mills, and other forms of research misconduct.
Here’s the big picture:
AI systems can amplify inaccurate or fabricated information. Large language models sometimes generate information that sounds plausible but is unsupported or entirely false, a phenomenon often referred to as "hallucination." A 2025 study found that when fictional medical terms were included in health questions, chatbots elaborated on them in nearly two-thirds of cases, generating explanations and treatments for conditions that do not exist. Researchers demonstrated a similar dynamic in an experiment involving a fictional skin condition called "bixonimania." After uploading fake papers about the condition to a preprint server, they found that several major AI chatbots described the made-up disorder as real and, in some cases, recommended medical care. The fabricated papers were later cited in a peer-reviewed article before being retracted.
AI systems increasingly interact with scientific literature that contain fraudulent or unreliable research. Researchers have documented the growing presence of "paper mills," operations that produce and sell fraudulent academic manuscripts. A study in BMJ found that nearly 10% of cancer research papers showed signs of paper mill involvement, with the proportion increasing over time. Because AI systems are trained on large volumes of publicly available content, including scientific literature, concerns have emerged that low-quality or fraudulent research may influence the information these systems retrieve, summarize, or generate. Some research has shown that even when fraudulent papers make up just 0.01% of an AI system's training data, they can contribute to errors in as many as 10% of responses.
Generative AI is also lowering barriers to producing convincing scientific content. Researchers have identified AI-generated manuscripts circulating through academic publishing and scholarly databases, sometimes without disclosure of AI assistance. The ability to rapidly generate text, references, and literature reviews raises concerns that AI could accelerate the production of papers that appear credible but contain errors, unsupported claims, or fabricated citations. As a result, some researchers and publishers are calling for stronger screening, reference verification, and disclosure requirements throughout the publication process.
Why This Matters: AI is increasingly involved at multiple stages of the scientific information ecosystem, from generating content and citations to retrieving and summarizing published research. As fabricated references, fraudulent papers, and other forms of low-quality research become harder to distinguish from legitimate scholarship, weaknesses in one part of the system can affect others. New efforts to detect paper mills, verify references, and improve AI reliability are underway, but people are already using AI tools to answer health questions.
What We’re Watching
A Closer Look at the State Level: New Jersey Poll Finds Broad Concern About Misinformation, Alongside Use of Search and Social Platforms
A Rutgers-Eagleton Poll commissioned by the New Jersey Civic Information Consortium found that concerns about misinformation are widespread among New Jersey voters, with 60% describing the spread of false or misleading information as a "very big problem" and another 22% calling it a "moderately big problem." The survey also found that New Jerseyans frequently rely on digital channels for news, including search engines (77%), friends and family (75%), and national news outlets (71%). At the same time, about one-third of voters (34%) said local news coverage in their area has decreased over the past five years. Rutgers researchers noted that concern about misinformation was shared across demographic and political groups, suggesting a rare point of bipartisan agreement.
Why This Matters: The findings are consistent with 2023 KFF polling among the general public, which found that a vast majority of adults (83%) say the spread of false and inaccurate information in the United States is a “major problem.” At the same time, the Rutgers-Eagleton survey sheds light on the role that search engines, social networks, and interpersonal connections play in how people access information and evaluate its credibility.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.
The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The data shared in the Monitor is sourced through media monitoring research conducted by KFF.
Medicaid Program Integrity: Tracking State-Specific and Nationwide Federal Action
The Trump Administration and Congress continue to focus on rooting out fraud, waste, and abuse in federal programs, including Medicaid. Those efforts include 50-state initiatives and targeted actions that focus on issues in specific states. Given the quickly evolving Medicaid program integrity landscape, this page tracks emerging developments in the federal government’s approach to program integrity in Medicaid, along with the implications of those actions for different states. For more detailed analyses and context, see ‘Related Resources’ in Section 2.
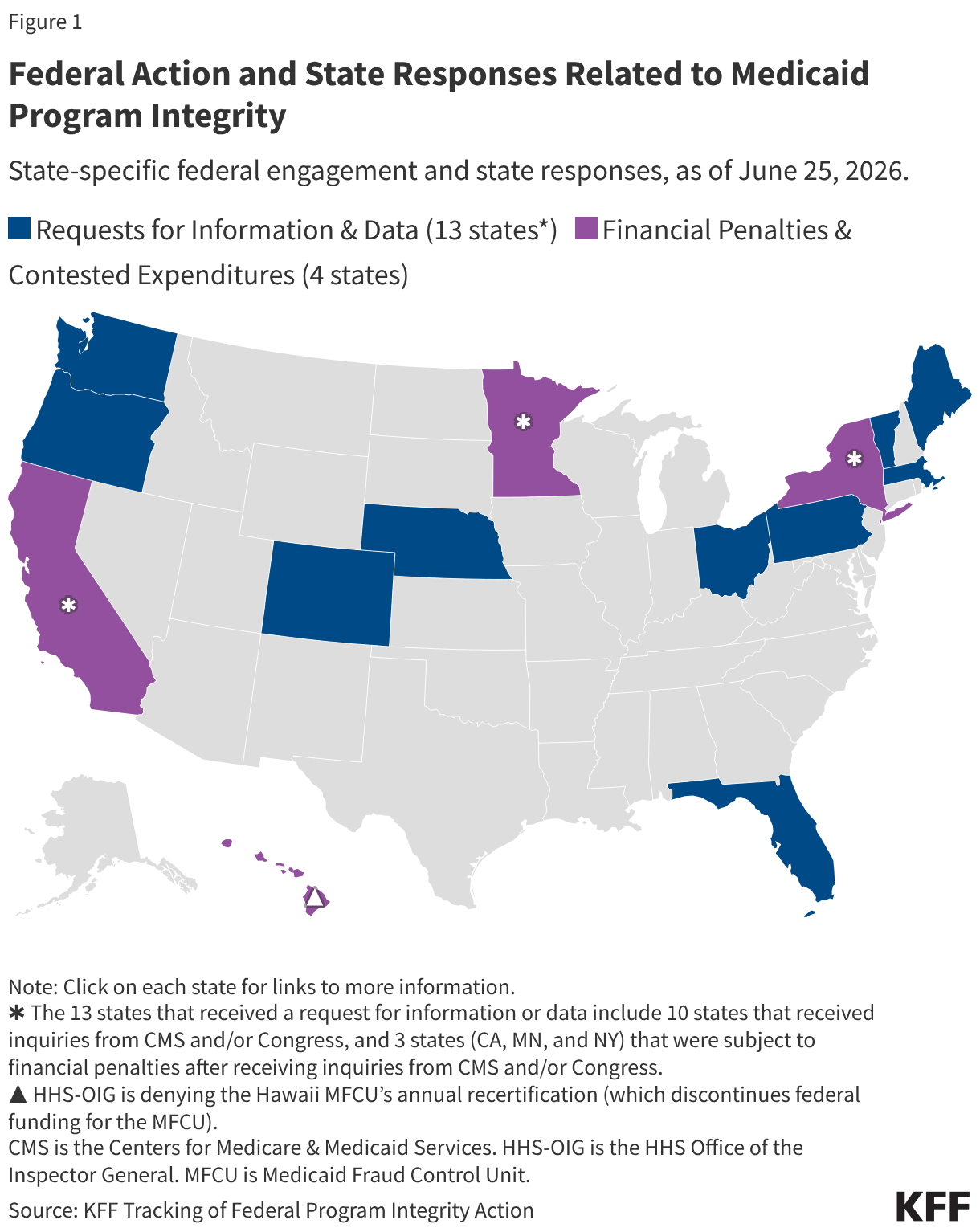
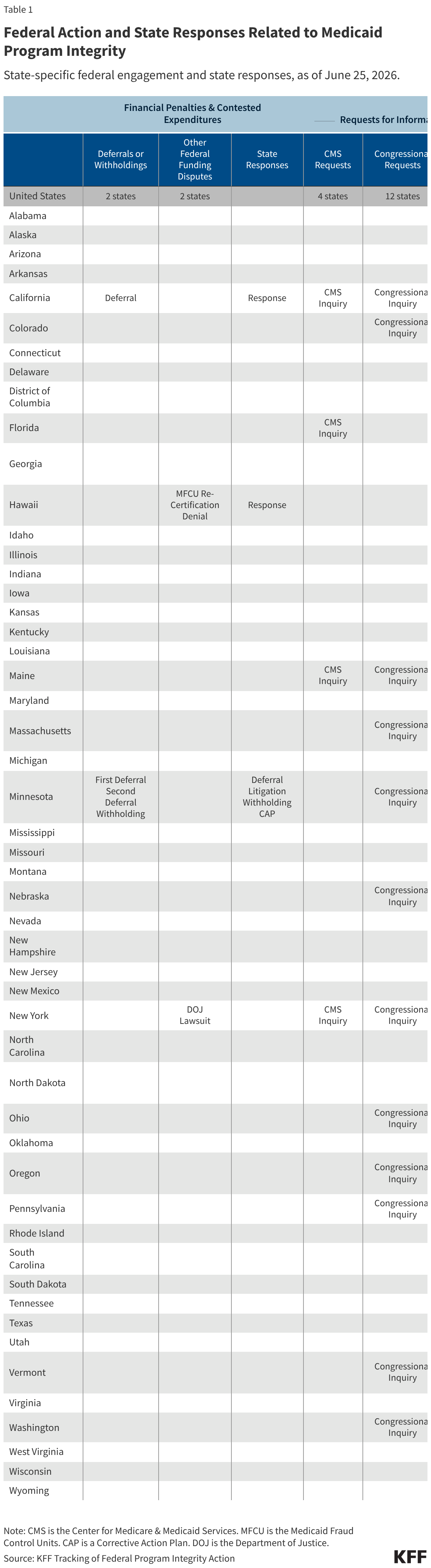
This page tracks the federal government’s 50-state initiatives and targeted actions focused on Medicaid program integrity (Figure 1 and Table 1). The map and tracker include federal actions towards states and exclude actions towards providers (such as those governing providers’ ability to participate in Medicaid and civil or criminal charges).
The following federal actions are included when materials are publicly available, along with states’ publicly available responses:
Financial penalties and contested expenditures including:
Notices of potential or actual withholding, deferrals, or disallowances of federal funding expressly tied to program integrity concerns; and
Other federal Medicaid funding in dispute (e.g., Health and Human Services (HHS)-Office of the Inspector General (OIG) funding for Medicaid Fraud Control Units or Department of Justice (DOJ)-contested state Medicaid program expenses).
Requests for state information and state responses, including formal inquiries, probes, or other materials that investigate specific state Medicaid programs or require states to respond with new information or an action plan.
The figure and table exclude the following actions:
Routine deferrals/disallowances (i.e., deferrals/disallowances only for longstanding disputed Medicaid claims and/or are not identified by CMS as expressly tied to concerns about fraud/waste/abuse);
HHS-OIG audits that are initiated as part of planned work and are more narrow or targeted in scope, and/or are not expressly tied to broader concerns about fraud/waste/abuse;
Routine DOJ proceedings (i.e., proceedings which target specific instances of fraud/waste/abuse against a Medicaid program but do not name a state Medicaid official as party to the case nor tie state claims for federal Medicaid funds to a case outcome); and
State or federal actions that do not have publicly available documentation (i.e., actions that may be referenced or announced in reporting or on social media but without documentation from federal or state governments).
Related Resources
KFF issue briefs related to Medicaid program integrity or fraud, waste, and abuse.
On June 9, 2026, the Medicare Trustees issued the annual report on the financial status of the Medicare program for 2026. The Trustees highlighted that the Medicare Part A trust fund is projected to be depleted in 2033, the same year but one quarter earlier than last year’s projection. In addition to discussing the status of the Part A trust fund, the report also provides substantial additional details on federal spending for Medicare Part B and Part D benefits, the distribution of spending for traditional Medicare and Medicare Advantage, and revenue sources for Medicare, along with updated spending and revenue projections and a detailed discussion of factors that have contributed to changes in the program’s financial outlook. This brief provides an overview of key trends in Medicare spending and spending growth, as well as the impact of these trends on out-of-pocket costs for Medicare beneficiaries and Medicare program solvency, as projected by the Medicare Trustees.
Physician Services and Other Outpatient Services Account for Roughly Half of Total Medicare Benefits Spending
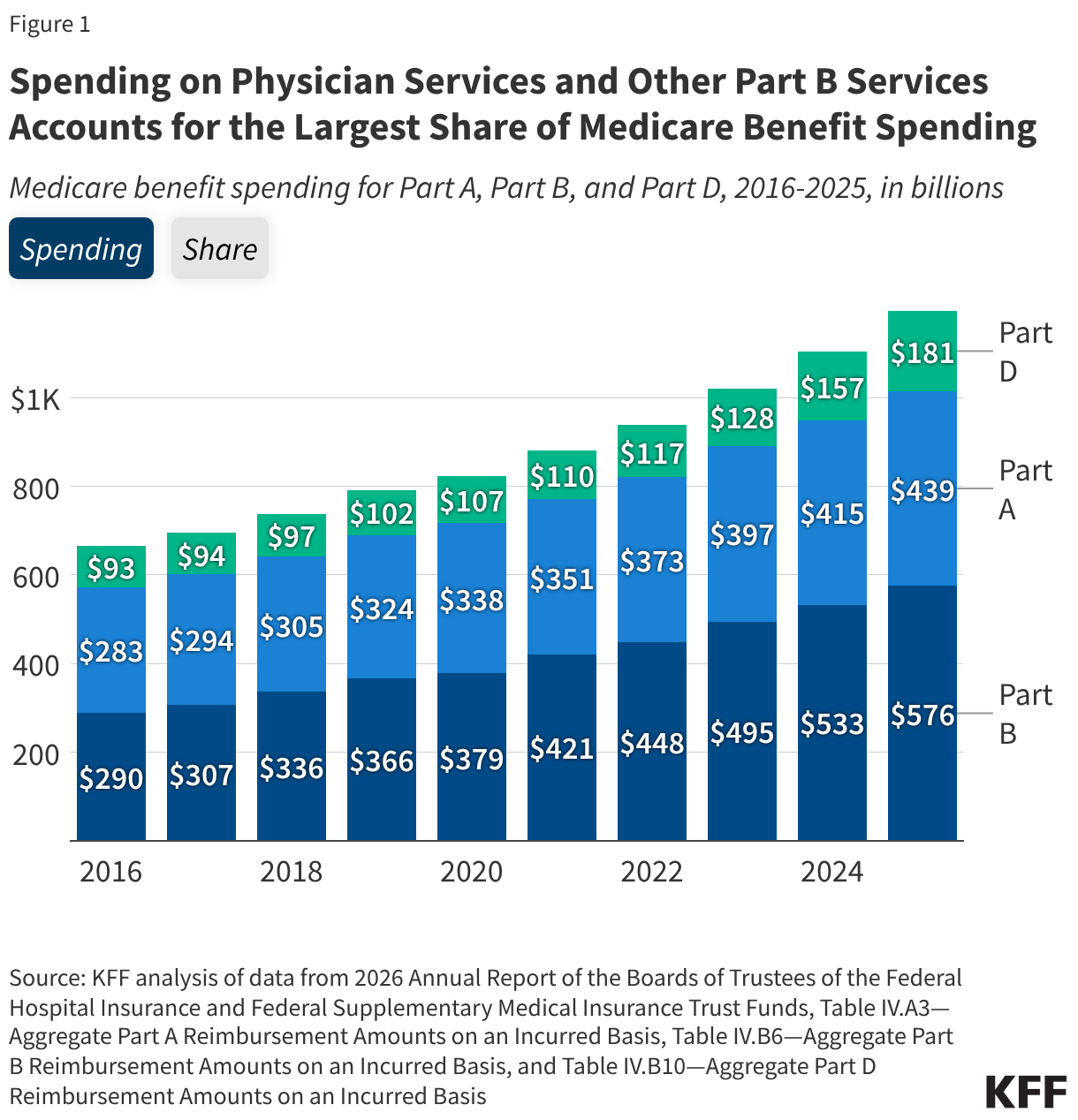
In 2025, Medicare benefit payments totaled $1.2 trillion, up from $666 billion a decade earlier (Figure 1). Spending on Part B services (including physician services, outpatient services, and physician-administered drugs) accounts for the largest share of Medicare benefit spending (48% in 2025), as it has since 2015. In contrast, spending on Part A services (including inpatient hospital services, skilled nursing facility services, and hospice care) has declined as a share of Medicare benefit spending (from 43% in 2016 to 37% in 2025). Over time, this decline has been driven in part by a shift of some services from inpatient to outpatient settings reflecting changes in practice patterns, along with increases in spending on services covered under Part B, including high-cost physician-administered drugs. Spending on Part D prescription drugs has accounted for a relatively constant share of Medicare benefit spending for much of the past decade (12-13%) but rose to 15% in 2025 and is projected to continue growing in the coming years.
Spending on Part A and Part B Benefits in Traditional Medicare Was $481 Billion in 2025
Looking at spending by type of service in traditional Medicare, the single largest category of benefit spending in 2025 was for inpatient hospital services covered under Part A (spending by type of service for Medicare Advantage enrollees is unavailable). Although a relatively small share of beneficiaries use inpatient hospital services, these services accounted for roughly one-third of total benefit spending in traditional Medicare ($159 billion or 33%), followed by outpatient hospital services covered under Part B ($76 billion or 16%) (Figure 2). This means that combined spending on hospital services (both inpatient and outpatient) accounted for nearly half of spending on Part A and Part B benefits in traditional Medicare in 2025. Services covered under the Medicare Part B physician fee schedule accounted for $71 billion (15%), and the remaining $174 billion (36%) consisted of payments for all other Part A and Part B services, including physician-administered drugs (8%), skilled nursing facility services (6%), and hospice care (6%), among others.
Figure 2
Spending on the Medicare Part D Prescription Drug Benefit is Projected to be Significantly Higher Over the Coming Decade Compared to Last Year’s Projections
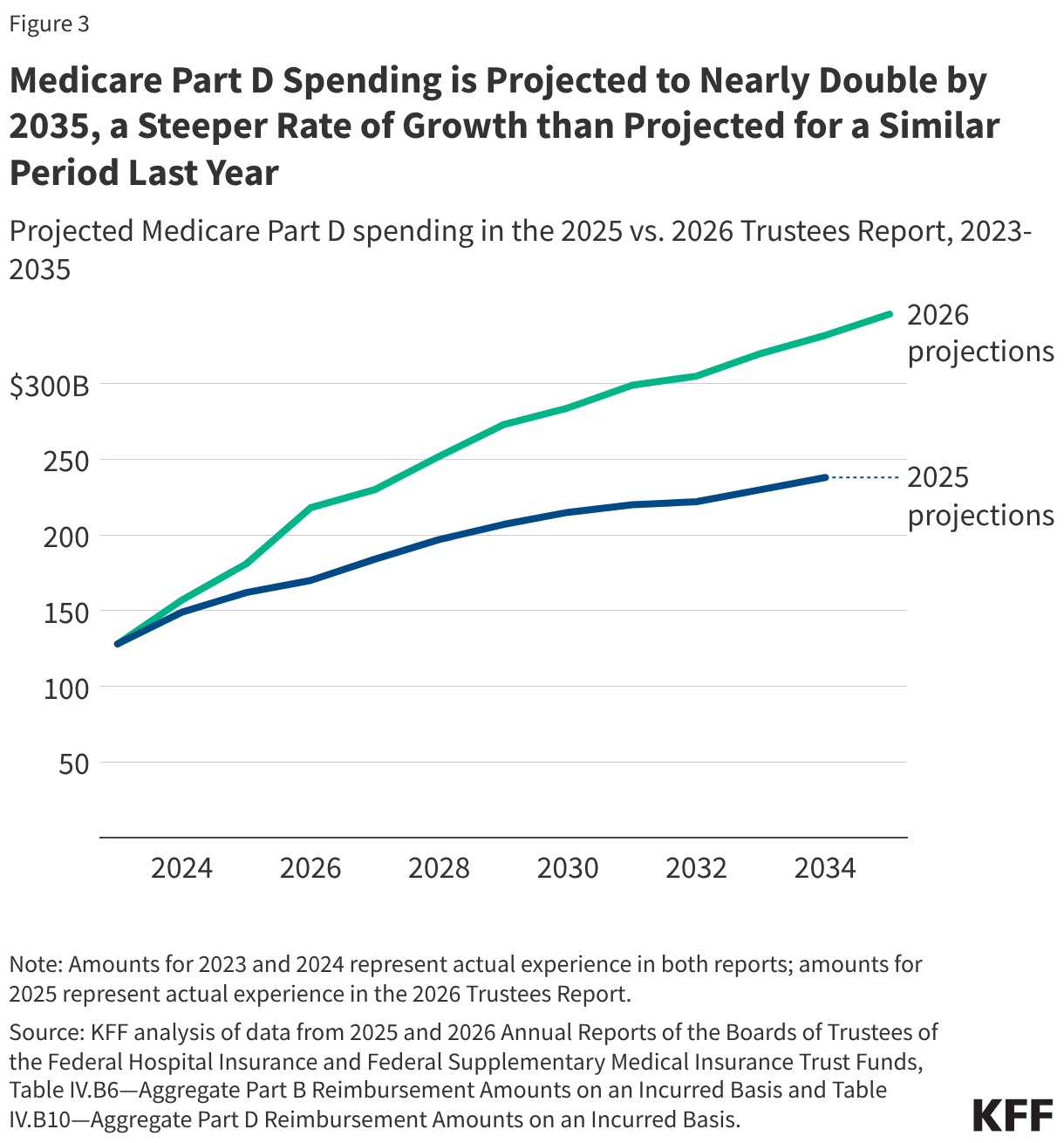
The Medicare Trustees currently project that Medicare Part D spending will nearly double from 2025 ($181 billion) to 2035 ($346 billion), representing an average annual growth rate of 6.7% compared to the 4.8% that was projected for a similar period last year (Figure 3). The Trustees indicate that higher spending projections for Part D in the 2026 report are due to increased use of GLP-1s and other high-cost specialty drugs. The Trustees also point to other factors that have contributed to changes in Part D spending in recent years, including the pharmacy price concessions policy that lowers point-of-sale prices for beneficiaries but reduces rebate revenue to Part D plans, which leads to higher federal Part D spending; the exemption of more orphan drugs from drug price negotiation in the 2025 budget reconciliation bill (H.R. 1), which will lower federal savings from negotiation; and the redesigned Part D benefit that improved the generosity of coverage while shifting more liability onto plans and increased the level of federal subsidies for coverage. These higher spending trends are offset somewhat by the effect of drug price negotiations and inflation rebates established by the Inflation Reduction Act.
Spending on Medicare Advantage was $534 Billion in 2025, Over Half (53%) of Total Medicare Program Spending
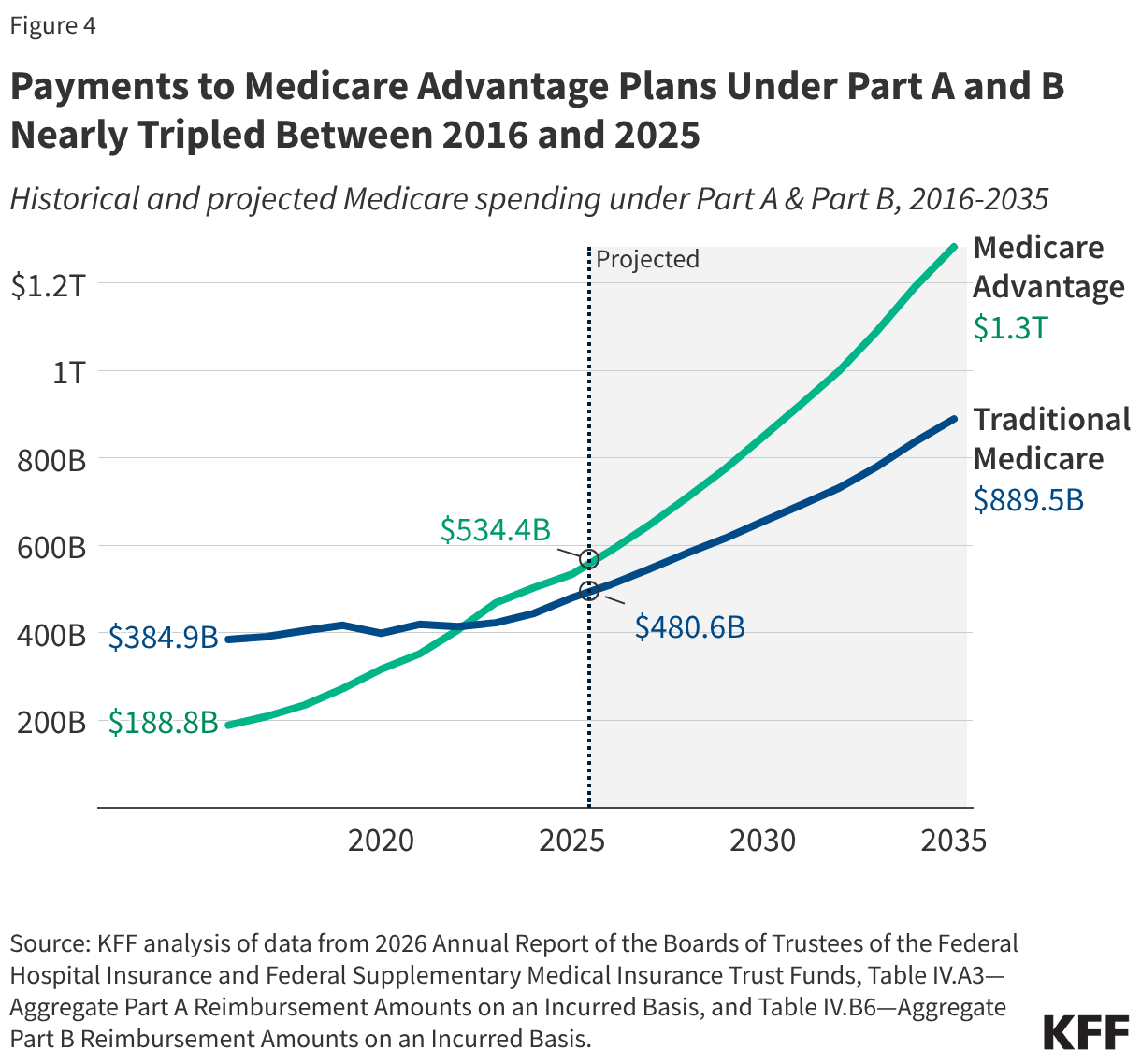
Payments to Medicare Advantage plans under Medicare Part A and Part B nearly tripled as a share of total Part A and Part B spending between 2016 and 2025 (from $189 billion to $534 billion), including payments for the cost of Part A and Part B services, as well as rebates, which must be used to reduce cost sharing, pay for extra benefits, or buy down the Part B and/or Part D premium (Figure 4). This growth is partly due to increased enrollment in Medicare Advantage plans, which rose from 33% to 54% of all eligible beneficiaries over this same period. At the same time, Medicare pays an estimated 14% more per enrollee in Medicare Advantage than it would if the same beneficiary were covered by traditional Medicare, resulting in $76 billion in additional Medicare spending in 2026. Those higher payments largely reflect the impact of higher coding intensity and favorable selection into Medicare Advantage. Growth in Medicare Advantage spending is projected to continue into the next decade, with payments to Medicare Advantage plans under for Part A and B benefits projected to increase to $1.3 trillion in 2035, or 59% of total Part A and Part B spending.
The Medicare Part A Trust Fund is Projected to be Depleted in 2033, Seven Years from Now
The depletion of the reserves in the Medicare Hospital Insurance (Part A) trust fund, which pays for inpatient hospital, skilled nursing facility, home health, and other Part A services, is projected to occur in the second quarter of 2033, based on the latest projections from the Medicare Trustees (Figure 5). This is one quarter earlier than the projection in last year’s report. According to the Medicare Trustees, the earlier depletion date is primarily the result of updated estimates of Social Security tax revenue (one source of Part A funding) that are lower than previously projected due to changes in the 2025 budget reconciliation bill (H.R. 1). If the reserves in the Part A trust fund are fully depleted, Medicare would not have sufficient funds to cover Part A benefit spending for the full year without additional revenues or reductions in spending on benefits or payments to providers.
Figure 5
Projected Increases in Medicare Spending Will Lead to Higher Medicare Premiums and Cost-Sharing Requirements
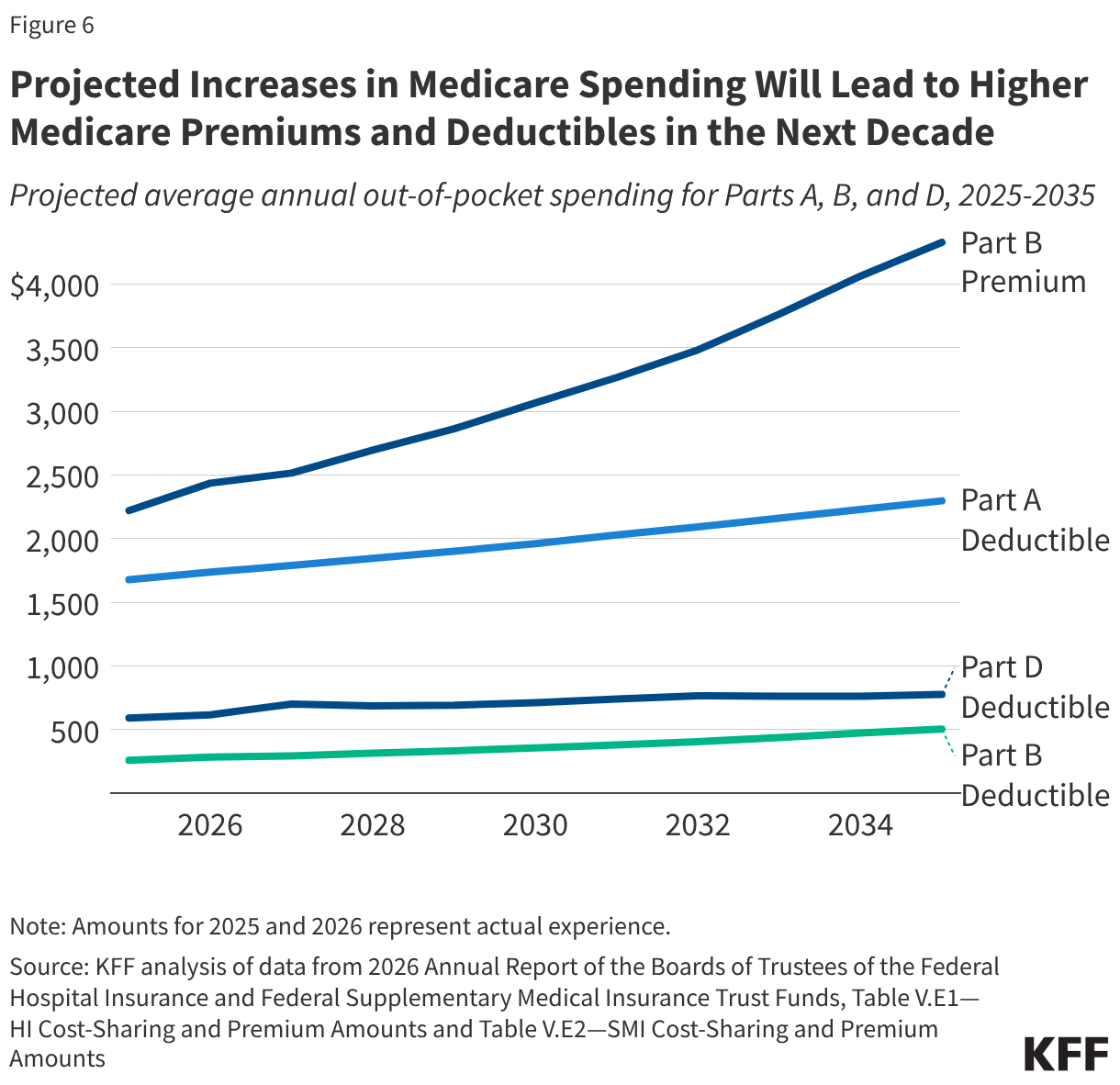
Medicare’s premium and cost-sharing requirements are determined annually based on expected growth in Medicare benefit costs for the coming year (though the exact approach to determining these amounts is different in each part). For 2027, the Trustees project that the monthly Part B premium will increase from $203 to $210 (3.3%), after increasing from $185 to $203 between 2025 and 2026 (9.7%). Likewise, the Part A hospital deductible is projected to increase from $1,736 to $1,788, and the Part D deductible from $283 to $292 in 2027. Further increases are estimated for the duration of the 10-year projection period in the 2026 Trustees report (Figure 6). These amounts may not reflect the costs that all beneficiaries face, particularly enrollees in Medicare Advantage plans, where cost sharing is generally different from the standard cost-sharing requirements for traditional Medicare beneficiaries. In 2024, seven million Medicare beneficiaries spent more than 10% of their income on the Part B premium alone. Increases in Medicare premiums and other out-of-pocket costs may represent a growing burden for many beneficiaries if income growth does not keep pace.
This tracker provides a listing of global health-related legislation being considered by the 119th Congress (Jan. 3, 2025 – Jan. 3, 2027). Currently, there are more than 50 pieces of legislation related to global health. They address topics ranging from global health security to reproductive health to the World Health Organization (WHO). Sometimes a bill may address broader topics, but this tracker focuses on the global health aspects of the legislation.
The tracker includes the bill title, sponsor(s), current status, and topic, as well as a short description of its global health-related provisions. The tracker includes bills only; resolutions are not included. Legislation is listed in alphabetical order by short title. In certain cases, identical bills have been introduced in both chambers of Congress (often referred to as companion bills). For example, the Global Health, Empowerment and Rights Act and the WHO is Accountable Act were each introduced in both chambers. Such companion bills are listed separately in the tracker.
The tracker will be updated periodically.
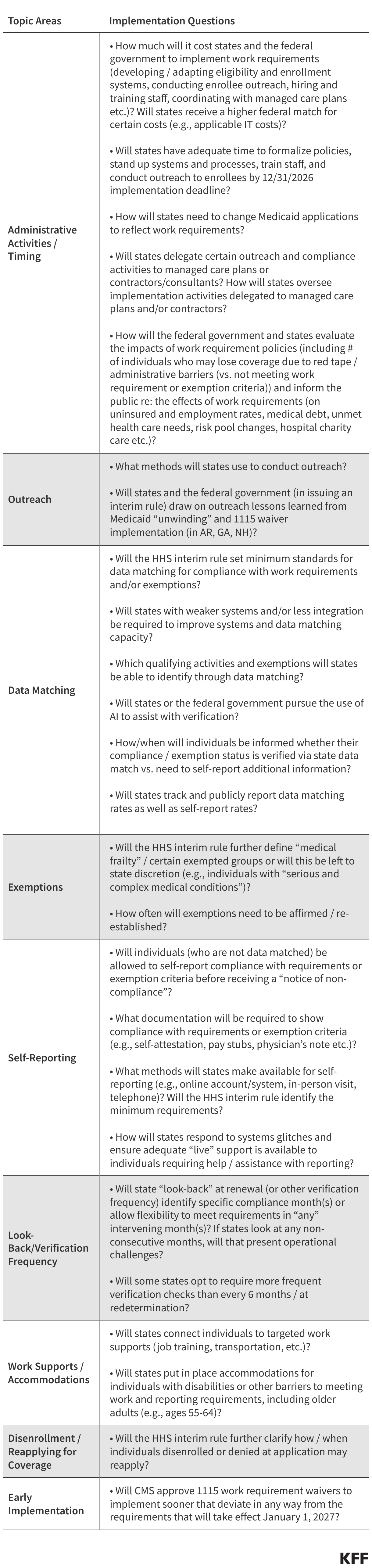
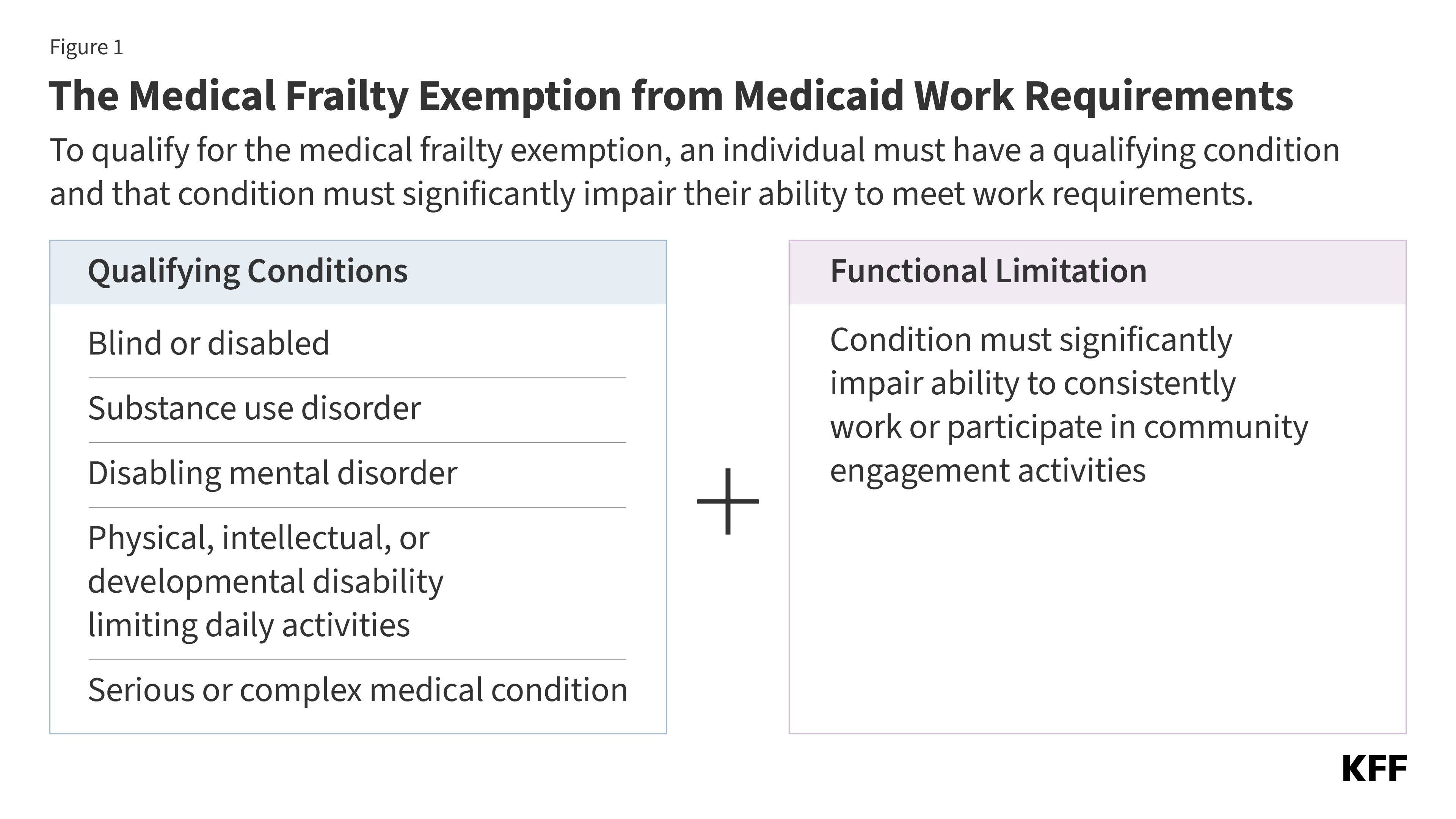
The Medical Frailty Exemption from Medicaid Work Requirements: Key Takeaways from the CMS Interim Final Rule
On June 1, 2026, the Centers for Medicare and Medicaid Services (CMS) issued a long-anticipated interim final rule that will guide state implementation of Medicaid work requirements. The 2025 reconciliation law requires 44 states to condition Medicaid eligibility for adults in the Affordable Care Act (ACA) Medicaid expansion group and enrollees in certain waiver programs, including in non-expansion states (Georgia, Tennessee, and Wisconsin), on meeting work requirements starting January 1, 2027, or sooner at state option. The law specifies mandatory exemptions, including individuals who are “medically frail.” Given the abbreviated implementation timeline, states had tentatively moved forward with key decisions over how to implement the medical frailty exemption even as they waited for formal guidance from CMS.
Significantly, the rule adopts a restrictive definition of medical frailty that differs from states’ early expectations and ties medical frailty to an individual’s ability to meet the community engagement requirements, including work or volunteer activities. The 2025 law specifies the medically frail exemption includes five categories of individuals who: are blind or disabled; have a physical, intellectual, or developmental disability that limits their ability to perform one or more activities of daily living (ADL); have a substance use disorder; have a “disabling” mental disorder; or have a “serious or complex” medical condition. The new rule requires states to consider not just whether the individual falls into one of the five categories described in the statute, but also whether the individual’s condition impairs their ability to engage in community engagement activities (including but not limited to work). States will likely need to pivot from earlier implementation plans and approaches to accommodate the new guidance.
States were already facing challenges in preparing to implement complex new requirements by January 1, 2027 and the provisions in the rule will amplify operational challenges, with added risks for states due to the potential for audits and financial penalties. The rule also may increase barriers for individuals to obtaining and maintaining coverage, leading to more people falling through the cracks and becoming uninsured. In addition, more complicated definitions of medical frailty may be difficult for states to explain as they conduct outreach with enrollees and potential applicants. This brief describes the new guidance and potential challenges states will face in operationalizing this exemption.
How Does the Interim Final Rule Define Medical Frailty?
For all categories of medical frailty, states are expected to develop a list of diagnosis and other codes to identify people who could potentially qualify for the exemption. States will be required to create lists of conditions that could potentially qualify someone as medically frail (generally in the form of health care code sets), which they must revise on a regular basis to reflect implementation experiences. CMS notes that the lists states use will be auditable, and if states are found to have determined an individual to be medically frail with little to no support for the conclusion that their physical, mental, or other behavioral health condition significantly impairs their ability to comply with the community engagement requirement, states would not be in compliance with the regulation and could be subject to financial penalties.
The rule relies heavily on existing definitions for the five medically frail categories and generally provides little additional clarification to help states develop the list of conditions for each category. In the rule, CMS said it did not believe it would be appropriate to include an exhaustive list of conditions in regulation, although they did provide examples of conditions across the various categories that could reasonably be expected to cause an individual to be medically frail. The rule acknowledges multiple existing definitions for several categories and ultimately defersto states the exact process of capturing individuals in these groups, explaining it “would be incredibly difficult to set one standard.” Notable details in the new rule include:
In the case of individuals with an SUD, the rule clarifies that the medical frailty category applies regardless of whether they are in an active treatment program but does not include individuals who have been in active recovery for 5 or more years.
For those with a serious or complex medical condition, the rule provides a new definition that requires a severe level of acuity for a condition to be considered serious or complex, which stands in contrast to other conceptions of “serious or complex” medical conditions that include individuals for whom maintaining access to health coverage is necessary to protect against serious health consequences if treatment is interrupted.
For all five categories, the rule makes clear that states must consider both if an individual’s condition meets the medical frailty definition and also if it significantly impairs their ability to work or engage in qualifying activities (Figure 1).
How Does the CMS Guidance Direct States to Verify Medical Frailty?
States are required to use claims and encounter data from the preceding 12 months to verify medical frailty status before requesting information from the individual; however, it will be difficult to use claims data alone to verify an individual’s ability to work. To ease the burden on individuals, the law directs states to use available information “where possible” to verify compliance with Medicaid work activities or exemption status, without requiring additional documentation from individuals. States are required to use claims or encounter data from the preceding 12 months as a data source. States are told they cannot consider information older than 12 months as this information “may not reflect the individual’s current condition.” The rule also encourages states to incorporate concise, plain language screening questions for use at application and renewal to identify individuals who may be medically frail. The rule is explicit that diagnosis alone cannot be used to verify medical frailty (because states must also consider whether an individual is sufficiently impaired from being able to work), limiting the ability of states to verify medical frailty on an ex parte (i.e., automatic) basis.
The rule does not provide details on criteria states should use for measuring severity of conditions or ability to meet new requirements. The rule only provides high-level examples of processes states may adopt to verify that an individual’s condition impairs their ability to work, such as algorithms that use administrative claims data to assign acuity scores, or using lists of qualifying diagnosis codes combined with utilization and other data. States may need to use combinations of data such as utilization data (e.g., hospitalizations), prescription drug data, and durable medical equipment (DME) prescription data. These approaches require states to implement even more complicated systems changes within the next six months that they were not anticipating based on earlier informal guidance. In addition, while these examples suggest states may be able to use acuity as a proxy for an individual’s ability to work, the rule is not clear on how states are expected to make these determinations. With the potential for audit, states may struggle to operationalize the medical frailty exemption in a way that protects them from financial penalty and minimizes administrative burden, without denying coverage to individuals who should qualify for the exemption.
Data limitations make it likely that medical frailty determinations will not be automated for many individuals. Examples of limitations include lack of data on file for new applicants and recent enrollees, or providers not consistently coding conditions or not using codes identified by the state. Certain individuals, such as those with functional limitations or behavioral health conditions, may also be more difficult to identify using claims data. States are also not provided with clear guidance on how to assess whether an individual is able to work or engage in community engagement activities, including what type of work activities states must consider. The more individualized the required assessment is, the more difficult it will be for states to auto-exempt individuals using data.
While states may need to rely on confirmation from treating providers to verify medical frailty conditions and ability to participate in community engagement activities, the rule offers little information on what information states need to collect from providers. States choosing to accept provider documentation are told that lists of who they choose to be allowable practitioner types must be shared with CMS if requested as part of oversight and data monitoring activities. Relying on provider confirmation could increase administrative burden (on the clinical workforce, individuals, and states), particularly for providers that treat large shares of Medicaid patients. Relying on providers or eligibility workers to determine whether an individual is able to work will likely require a subjective decision and could raise ethical concerns among providers. New Hampshire had previously implemented work requirements with a requirement that individuals needed to be deemed unable to work by providers to qualify for an exemption; enrollees with physical and behavioral health problems struggled when applying for exemptions, often because primary care providers resisted signing forms declaring that their patients were unable to work. Research also shows that physician attitudes to assisting patients who request exemptions from work requirements can vary substantially. In addition, because providers receive Medicaid payments and, therefore, have an interest in their patients maintaining health coverage, requesting information from them to confirm a medical frailty exemption could raise conflict of interest issues.
While states are permitted to use self-attestation to verify medical frailty, the rule limits reliance on self-attestation starting in January 2028. Given the limitations of existing data sources and the difficulty of identifying whether an individual is medically frail, accepting self-attestation of medical status or ability to work could relieve the administrative burden for states as well as applicants and enrollees. Acknowledging data limitations states face particularly for new applicants, the rule allows states to accept self-attestation throughout 2027 in cases where there is no reliable information available to the state. However, starting January 1, 2028, states may only accept self-attestation of medical frailty status one time during an individual’s enrollment period. States would then be expected to verify individuals using available data or require documentation or other information from individuals for future renewals.
The rule requires states to verify medically frail exemption status at least every 12 months. States must reverify medical frailty even for people whose health condition or disability status is unlikely to change every 12 months; however, the rule gives states the option to reverify medical frailty more frequently (such as at each 6-month renewal period). For states that elect to verify compliance between regular renewals (e.g., quarterly), the rule specifies that individuals identified as specified excluded individuals during their most recent verification, including those who meet medical frailty exemptions, are not subject to more frequent verifications.
Episode 9, AI Series: In this episode, Dr. Ziad Obermeyer joins Chip to talk about AI bias in patient management, including how far the health care industry has come since his groundbreaking research that revealed alarming biases in a widely used algorithm that underestimated the health needs of Black patients. The discussion emphasizes that while AI can analyze data with remarkable precision, it is the context surrounding that data that ultimately determines its efficacy, usefulness, and fairness. Dr. Obermeyer is an emergency department physician, researcher, co-founder of Nightingale Open Science and Dandelion, and associate professor at the UC Berkeley School of Public Health and the College of Computing, Data Science, and Society.
Charles N. Kahn III is a senior visiting fellow at KFF. He is also a visiting senior fellow at the American Enterprise Institute and a nonresident senior scholar at the University of Southern California’s Schaeffer Center for Health Policy & Economics. He serves as co-chair of the international Future of Health collaborative.
Blue Cross of California Distinguished Associate Professor of Health Policy and Management, UC Berkeley School of Public Health
Dr. Ziad Obermeyer is Associate Professor and Blue Cross of California Distinguished Professor in UC Berkeley’s School of Public Health and College of Computing, Data Science, and Society. His work, grounded in clinical practice, uses AI and data to improve clinical decisions, accelerate medical discovery, and bring computational innovations into patient care. His research on algorithmic bias has influenced hospital AI practices worldwide and informed public accountability efforts. He co-founded Nightingale Open Science and Dandelion and is a Chan–Zuckerberg Biohub Investigator and a Research Associate at the National Bureau of Economic Research. A Harvard Medical School faculty member and McKinsey consultant, he was named to TIME Magazine’s 100 most influential people in AI.
This weekly podcast features insightful conversations between host Chip Kahn and his guests, who discuss the business of health care, connecting the dots between the health care business, policy, and patients.
The podcast’s first series on AI in health care illuminates how AI is changing health care, and features guests who are deploying this technology, managing its consequences, and designing policy around it.