KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Health Care Costs Tops the Public’s Economic Worries as the Runup to the Midterms Begins; Independent Voters Are More Likely to Trust Democrats than Republicans on the Issue
Two Thirds of Public Say Congress "Did the Wrong Thing" by Not Extending ACA Enhanced Tax Credits, But Republicans Largely Say Congress “Did the Right Thing”
Heading into this midterm election year, the cost of health care tops the public’s economic anxieties and more than 4 in 10 voters say the issue will have a major impact on their vote, a new KFF Health Tracking poll finds. Voters, including independents, currently trust Democrats more than Republicans to address the cost of health care and most other health care issues, though neither party has an advantage on addressing the overall cost of living, the poll finds.
The poll provides an early look at how the public and voters view health care issues, including costs, following a year of substantial debate and changes. Congress last year enacted major Medicaid changes expected to cut federal spending and increase the number of uninsured and allowed the Affordable Care Act’s enhanced tax credits to expire, sharply increasing the premium payments for most ACA Marketplace enrollees.
Across a range of measures, the poll finds significant concerns about health care costs:
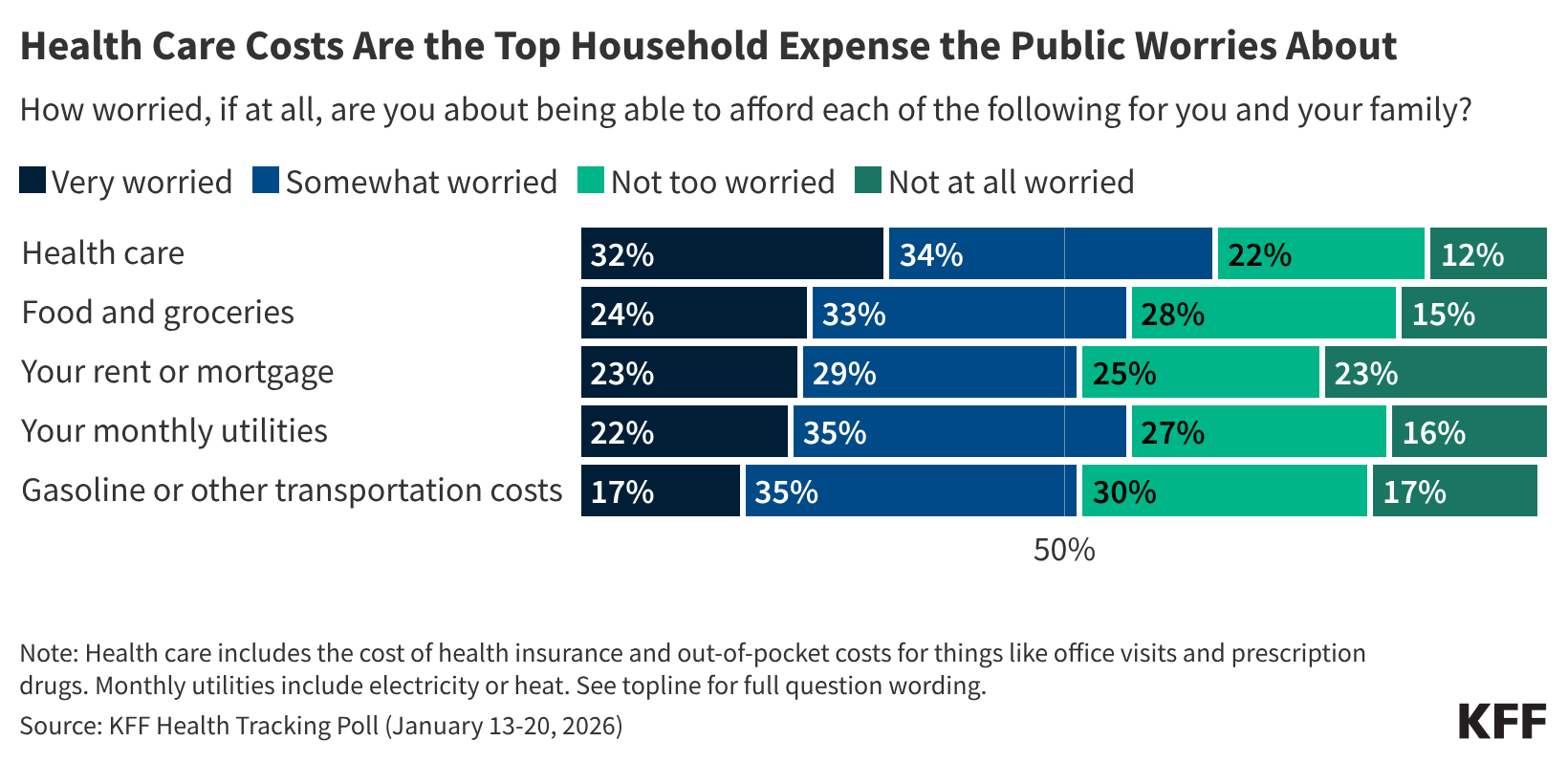
The public was given a list of household expenses families worry about. A third (32%) say that they are “very worried” about their ability to afford health care for them and their families – more than say the same about affording food and groceries (24%), rent or mortgage (23%), monthly utility bills (22%), or gasoline and other transportation costs (17%).
Health care costs are the top economic worry for Democrats, independents, Republicans, and supporters of President Trump’s “Make America Great Again” movement.
A majority (56%) of the public expect health care costs for their family to become less affordable in the coming year. About 1 in 5 say that their health care costs have increased more quickly than other necessities such as monthly utilities (23%) and food and groceries (21%).
Among independent voters, more trust the Democratic Party (35%) than the Republican Party (15%) to address health care costs. Independent voters also give Democrats an advantage over Republicans on Medicaid, the ACA, Medicare, and the cost of prescription drugs, though sizeable shares say they trust neither party. Among all voters, trust in Republicans (30%) is within 5 percentage points of Democrats (35%) on drug prices, an issue President Trump has championed.
More than 4 in 10 voters say that health care costs will have a “major impact” both on their decision to vote in the midterm elections (44%) and on which party’s candidates they will support (43%). This includes two thirds of Democrats, more than 4 in 10 independents, and about a fifth of Republicans.
“Republicans won the legislative battle to let the enhanced ACA tax credits expire, but that helped make health costs more of an economic worry and voting issue, and Democrats are well positioned to capitalize on that in the midterms,” KFF President and CEO Drew Altman said.
Most Continue to View ACA Favorably, But Support Falls Among Republicans After Debate
The poll also gauges the public’s views on the ACA after Congress allowed the law’s enhanced tax credits to expire after extensive debate.
Two thirds (67%) of the public say that Congress did “the wrong thing” by allowing the tax credits to expire, twice the share (33%) that says Congress did “the right thing.”
Large majorities of Democrats (89%) and independents (72%) say that Congress did the wrong thing. While most Republicans (63%) and MAGA supporters (64%) say Congress did the right thing, about a third of each group says that Congress did the wrong thing.
Most (58%) of the public continues to hold favorable views of the ACA, though support this month is down 6 percentage points since September (64%).
The shift reflects a drop in favorability among Republicans (22% now vs. 36% in September) and among MAGA supporters (16% now vs. 31% in September).
Designed and analyzed by public opinion researchers at KFF, this survey was conducted January 13-20, 2026, online and by telephone among a nationally representative sample of 1,426 U.S. adults in English and in Spanish. The margin of sampling error is plus or minus 3 percentage points for the full sample. For results based on other subgroups, the margin of sampling error may be higher.
Finding on other topics including prior authorization will be reported separately.
On January 27, 2026, the Trump administration released details of the latest expansion of the Mexico City Policy, a policy he reinstated in January of last year. The policy, which has been in effect, depending on the party of the President, since 1984, has required foreign non-governmental organizations (NGOs) to certify that they would not “perform or actively promote abortion as a method of family planning” using funds from any source (including non-U.S. funds) as a condition of receiving U.S. government global family planning funding. In 2017, President Trump reinstated the policy but also significantly expanded it to encompass the vast majority of U.S. bilateral global health assistance. The latest expansion, now part of a broader set of restrictions known as the “Promoting Human Flourishing in Foreign Assistance (PHFFA)” Policy, applies to significantly more funding, many more organizations, and new services and activities. Specifically, it now applies to most non-military foreign assistance and most recipients of foreign aid (not just foreign NGOs). And, in addition to abortion, it prohibits activities related to diversity, equity, and inclusion (DEI) and promoting or providing gender affirming care, legal protections based on gender identity, and other related services and activities. This analysis assesses the potential reach of the latest expansion of the policy by examining foreign assistance funding provided in FY 2024, the most recent year with complete information, to identify the amount of funding, number of organizations, and range of foreign assistance sectors that stand to be affected. The analysis looks at total funding that would be subject to restrictions, and although not all recipients are necessarily currently engaging in activities subject to the restrictions, all would have to decide whether they accept the policies’ terms. Among the key findings:
In FY 2024, $39.8 billion in U.S. foreign aid, spanning 160 countries, was obligated to prime recipients, funding that would be subject to the latest expansion (additional funding could be subject to the policy if it was ultimately provided, directly or indirectly, to recipients or sub-recipients).
Notably, this is tens of billions more than the amount of global health assistance subject to the policy under the Trump administration’s previously expanded policy ($7.3 billion in FY 2020), and significantly more than the amount of family planning assistance subject to the policy during earlier administrations (between $300-$600 million).
By recipient type, the largest share (41%) of the $39.8 billion was provided to multilateral organizations, recipients that are newly subject to the policy under the latest expansion. The second largest (29%) was provided to private sector organizations, including the newly-subject U.S. private sector.
By sector, humanitarian assistance accounted for the largest share of funding (29%), followed by health (26%) and economic development (22%); two of these sectors (humanitarian assistance and economic development) are among the several sectors newly subject to the policy under the latest expansion.
There were almost 2,600 prime recipients of U.S. foreign aid in FY 2024, a significantly higher number than for health alone (756 prime recipients). This number should be considered a floor, since prime recipients must “flow-down” the policy to any sub-recipients. The majority of prime recipients were foreign entities (62%); U.S.-based entities accounted for 34%, with multilateral recipients accounting for 4%.
Whether or not the full extent of the expansion will be instituted (there are likely to be legal challenges to some aspects of the policy, which could limit its reach, and some additional rule-making has yet to occur), it represents a significant expansion in terms of funding, number of organizations, and content and services restricted, well beyond the reach of what was in place during the first Trump administration.
Background
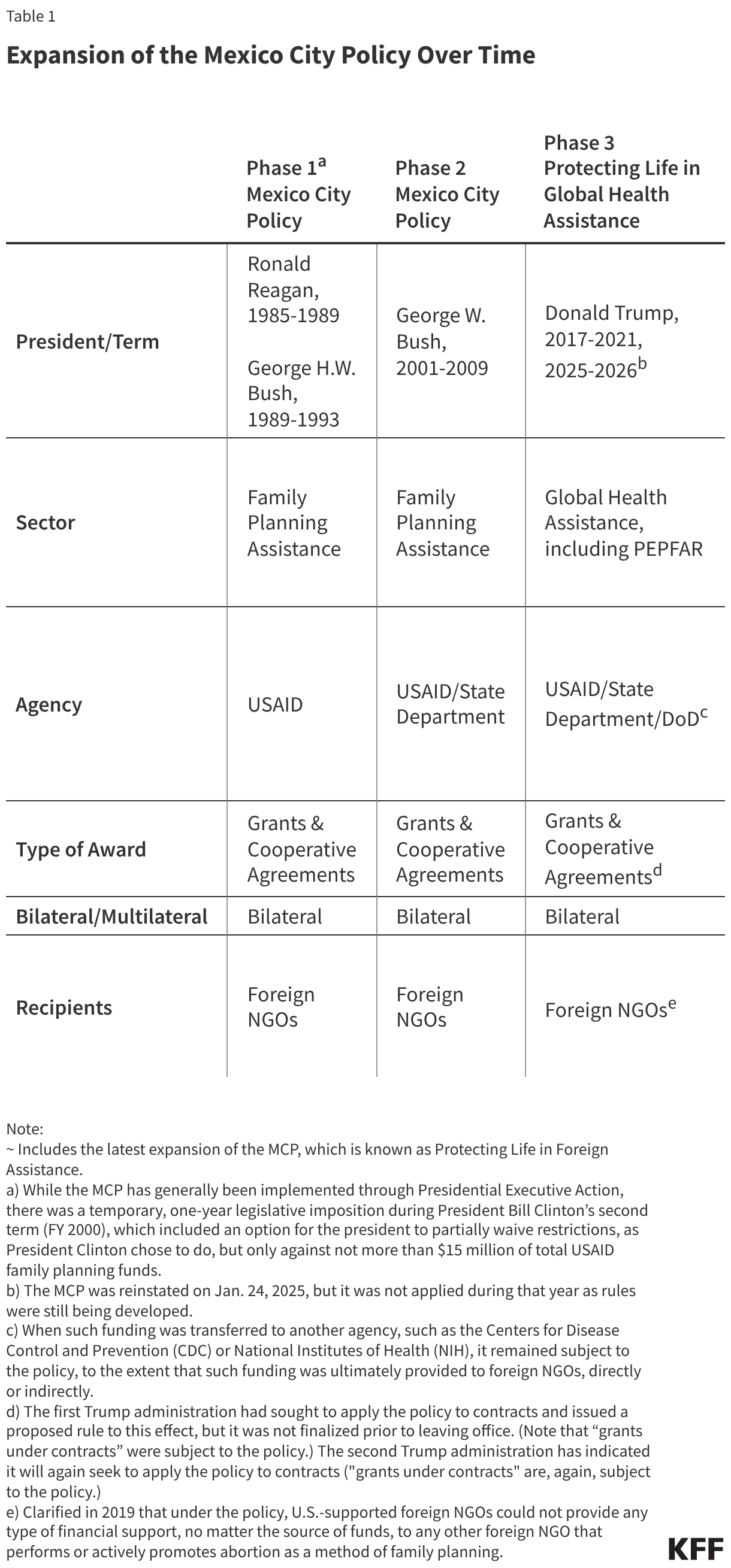
The Mexico City Policy (MCP) is a U.S. government (USG) policy that – when in effect – has required foreign NGOs1 to certify that they will not “perform or actively promote abortion as a method of family planning” using funds from any source (including non-U.S. funds) as a condition of receiving U.S. global family planning assistance and, in 2017 under the first Trump administration, most other U.S. global health assistance. First announced in 1984 by the Reagan administration, the policy has been rescinded and reinstated by subsequent administrations along party lines since and has been in effect for 23 of the past 42 years. It has also been steadily expanded over time (see Table 1). Under the first Trump administration, the policy was renamed “Protecting Life in Global Health Assistance” (PLGHA). Among opponents, it has also been known as the “Global Gag Rule,” because among other activities, it prohibited foreign NGOs from using any funds (including non-U.S. funds) to provide information about abortion as a method of family planning and to lobby a foreign government to legalize abortion.
The second Trump administration reinstated the MCP through a Presidential Memorandum on January 24, 2025, noting that the policy would be expanded even further. On January 27, 2026, the policy details were released under three separate, but inter-related final rules (interim final rules were first posted on January 23), now called the “Promoting Human Flourishing in Foreign Assistance (PHFFA) Policy” (see Box 1).
Box 1: Promoting Human Flourishing in Foreign Assistance (PHFFA) Policy
The Trump administration released details of its new Promoting Human Flourishing in Foreign Assistance (PHFFA) Policy, which includes the latest expansion of the Mexico City Policy, via three separate, but related, final rules on January 27, 2026. Each rule applies to the same funding streams, types of organizations, and award mechanisms but restricts different activities and services:
Protecting Life in Foreign Assistance (PLFA): prohibits recipients from performing or actively promoting abortion as a method of family planning; the latest expansion of the Mexico City Policy.
Combating Gender Ideology in Foreign Assistance: prohibits recipients from providing or promoting gender affirming care, legal protections based on gender identity, and other related activities; defines sex as “person's immutable biological classification as either male or female.”
This marks the most significant expansion of the policy to date. Specifically, it:
expands to all non-military U.S. foreign assistance (not just global health) administered by the State Department2 (with an intention for the State Department to work with other agencies that administer foreign assistance to also incorporate these provisions);
expands the types of recipients, and consequently the number of organizations, subject to the policy to also include multilateral organizations, foreign governments, and U.S.-based NGOs (not just foreign NGOs);3
expands to prohibit additional content areas and services newly subject to the policy: DEI-related activities as well as support for gender affirming care and services, information, and legal protections based on gender identity, among other related activities (referred to as promoting “gender ideology”); and
expresses an intent to expand to include funding provided through contracts (not just grants and cooperative agreements), although this will be the subject of future rule-making.
Findings
To assess the potential reach of the latest expansion, this analysis looks at U.S. government foreign assistance obligation data for FY 2024 (the most recent year for which complete obligation data by sector are available) to quantify the amount of funding and number and type of prime recipients that could be affected. While not all recipients are necessarily currently engaging in activities subject to the restrictions, all would have to decide whether they accept the policies’ terms. Obligations were analyzed because the policy applies to funding once newly obligated to a recipient (either through an existing or a new award). Data were obtained from ForeignAssistance.gov, the U.S. government’s centralized data portal for budgetary and financial data provided by more than 20 federal agencies that manage foreign assistance programs. The analysis is based on the funding identified in the PHFAA rules, which includes all non-military foreign assistance4 appropriated to the State Department or U.S. Agency for International Development (USAID) under Title III and four other accounts under Department of State, Foreign Operations, and Related Programs (SFOPs)/National Security, State Department, and Related Programs (NSRP) appropriations acts (specifically, “International Narcotics Control and Law Enforcement,” “Nonproliferation, Anti-Terrorism, Demining and Related Programs,” “Peacekeeping Operations,” and “International Organizations and Programs”). The analysis also includes funding provided through contracts (not just grants and cooperative agreements) for two reasons: first, the rules indicate that further rule-making will be undertaken to add these policy restrictions to contracts; and second, it is not possible to disaggregate obligations by funding instrument in ForeignAssistance.gov (see Box 2 for key terms, Methodology for more detail, and Appendix for detailed data).
Box 2: Key Terms
Obligation: A binding agreement that will result in outlays of funds immediately or at a later date.
Prime Recipient: The main recipient, or those that receive funding directly from the U.S. government to carry out foreign assistance work.
Sub-Recipient: Those that receive funding indirectly from the U.S. government through an agreement with the prime recipient.
Non-Governmental Organization (NGO): a for-profit or not-for-profit organization that is not part of the U.S. government, a foreign government, or a multilateral organization; includes private sector organizations, non-profit organizations, and educational institutions.5
Multilateral Organization: an organization that is jointly supported by multiple governments and, often, other partners (versus bilateral efforts, which are carried out on a country-to-country basis); includes specialty agencies of the United Nations (U.N.) and international financing mechanisms that pool and direct resources from multiple public and private donors for specific causes.6
Foreign Government: any department, agency, independent establishment, or other entity of the government of a foreign country.
Parastatal: foreign-government-owned organization operated as a commercial company or other organization, including non-profits, or enterprises in which foreign governments or foreign government agencies have a controlling interest.
In FY 2024, $39.8 billion in U.S. foreign aid was obligated to prime recipients, funding that would be subject to the latest expansion. This includes funding provided to U.S. and foreign NGOs, international organizations, foreign governments, and parastatals (additional funding could be affected if it was ultimately provided, directly or indirectly, to recipients or sub-recipients subject to the policy).
Notably, this is tens of billions more than the amount of global health assistance subject to the policy under the first Trump administration’s previously expanded policy ($7.3 billion in FY 2020), and significantly more than the amount of family planning assistance subject to the policy during earlier administrations (between $300-$600 million). See Box 3.
Box 3: Funding Newly Subject under the Latest Expansion of the MCP
By Recipient Type:
Multilateral organizations: $16.3 billion
Foreign governments: $1.3 billion
U.S. NGOs: $16.5 billion^
Foreign NGOs: $3.5 billion in non-health sectors
By Sector:
Non-health sectors: $29.2 billion, including (for example):
Humanitarian assistance: $11.5 billion
Economic development: $8.7 billion
Democracy, human rights, and governance: $2.6 billion
Peace and security: $2.2 billion
Education and social services: $1.2 billion
Health sector: $8.3 billion in U.S. NGO,^ multilateral, and foreign government funding
Note: Amounts by recipient type and sector are not mutually exclusive categories. ^ Any foreign NGO that was a sub-recipient of U.S. global health assistance from a U.S. NGO would have been subject to the previously expanded MCP, PLGHA, when in place.
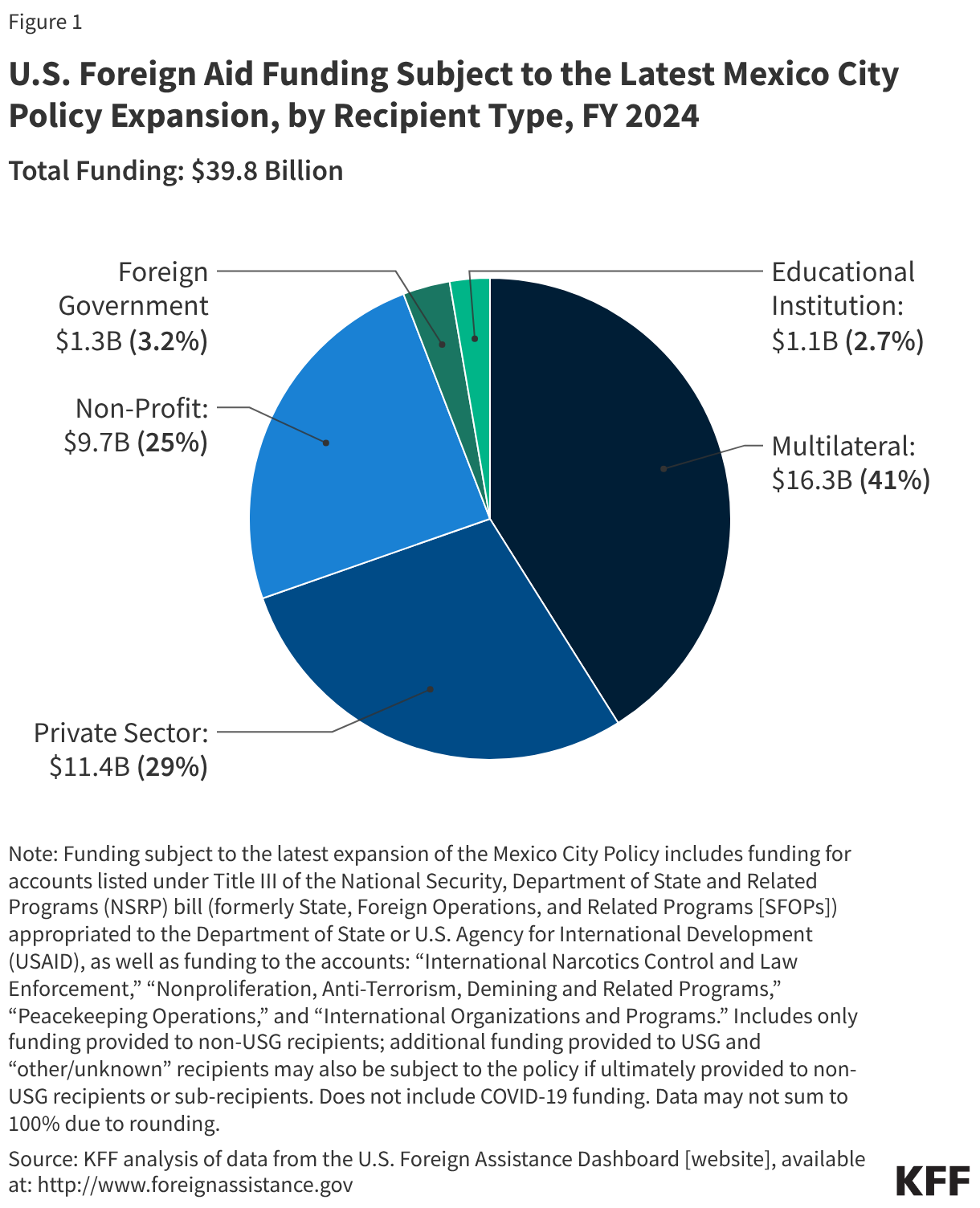
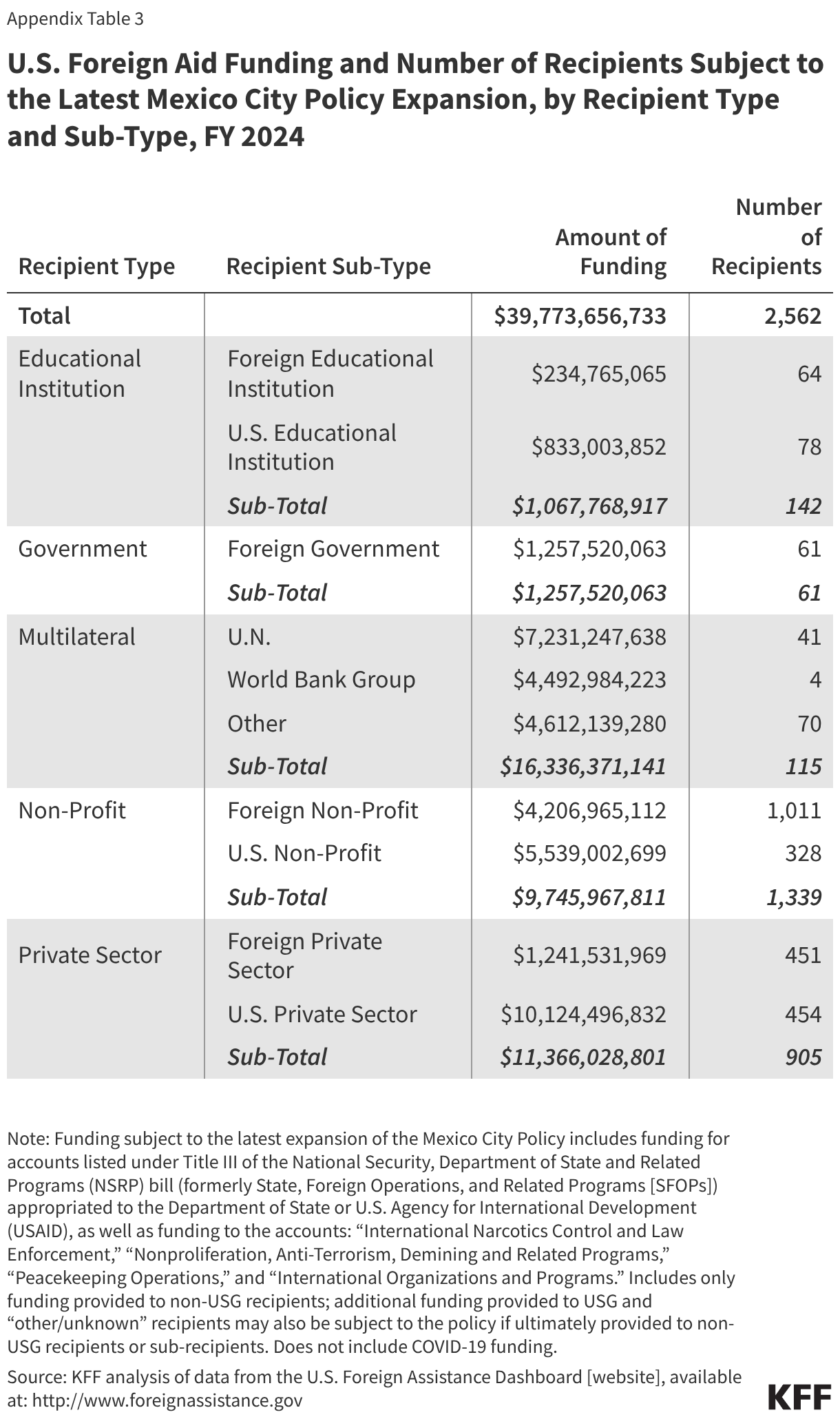
By recipient type, the largest share of funding was provided to multilateral organizations ($16.3 billion, or 41%), entities that are newly subject to the policy. The private sector received the next largest amount of funding ($11.4 billion, or 29%), followed by the non-profit sector ($9.7 billion, or 25%). Smaller amounts were provided to foreign governments ($1.3 billion, or 3.2%) and educational institutions ($1.1 billion, or 2.7%) (see Figure 1).
U.S.-based recipients received $16.5 billion (41%). These included U.S. NGOs, specifically U.S. non-profits, private sector organizations, and educational institutions (all newly subject to the policy). Foreign recipients, both governments and NGOs, received $6.9 billion (17%); foreign governments are also newly subject to the policy.
Collectively, the $39.8 billion in foreign assistance was provided to 160 countries, with more countries likely reached through “regional” and “worldwide” activities.7 This is significantly more countries than would be reached with global health assistance alone (87 countries).
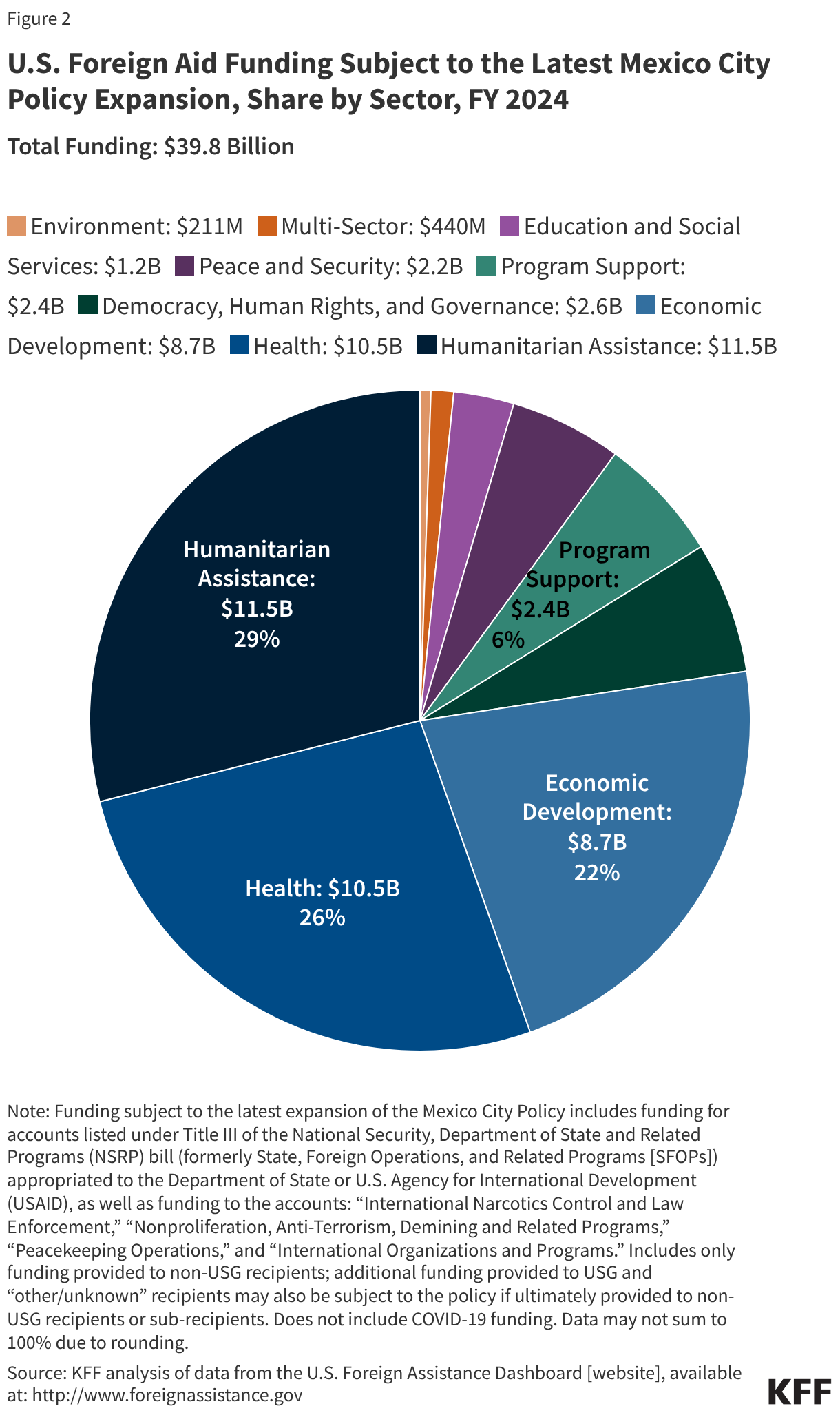
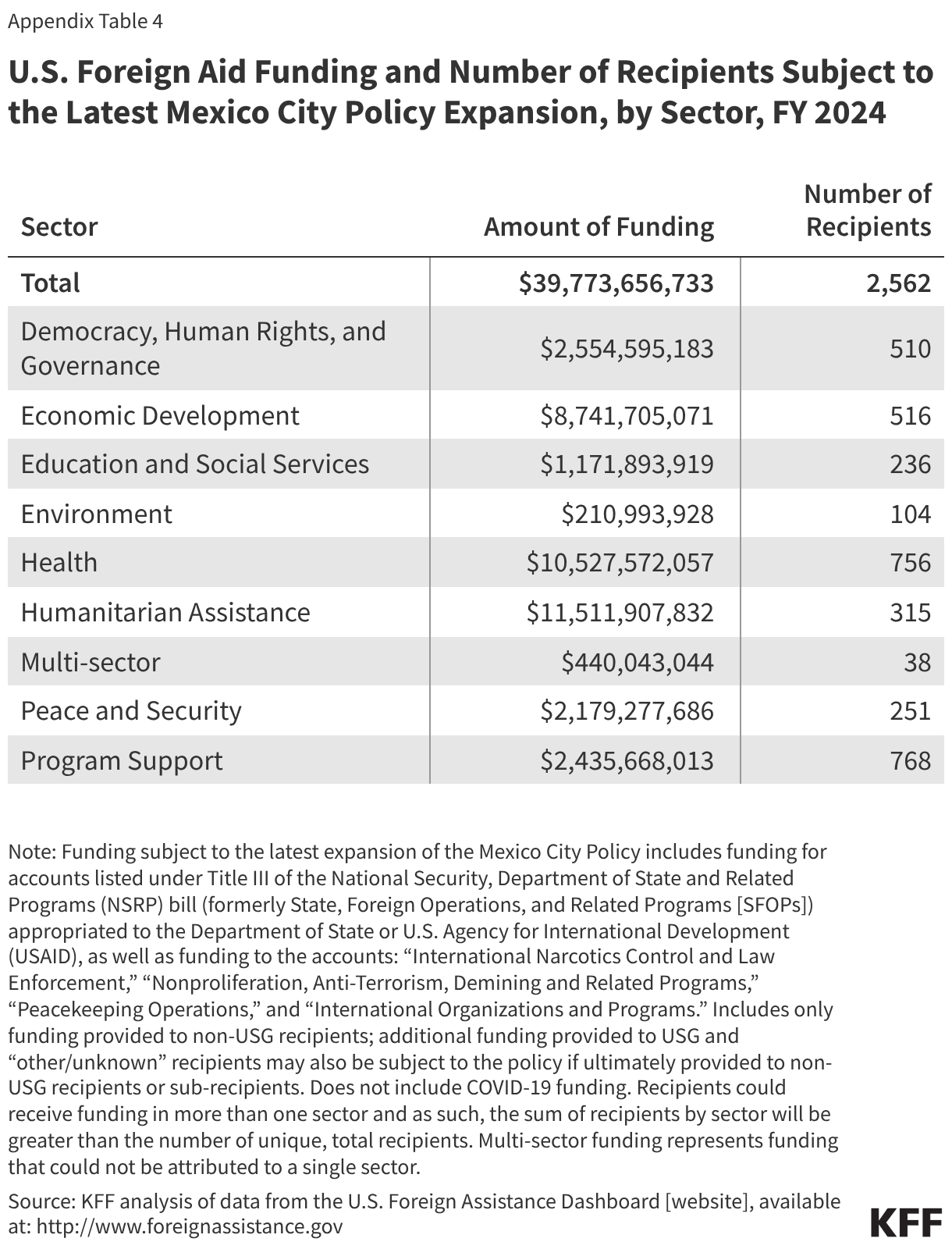
By sector, humanitarian assistance accounted for the largest share of funding ($11.5 billion, or 29%) in FY 2024, followed by health ($10.5 billion, or 26%) and economic development ($8.7 billion, or 22%). Two of these sectors (humanitarian assistance and economic development) are newly subject to the policy (see Figure 2). The remaining sectors each accounted for approximately $3 billion (6%) or less.
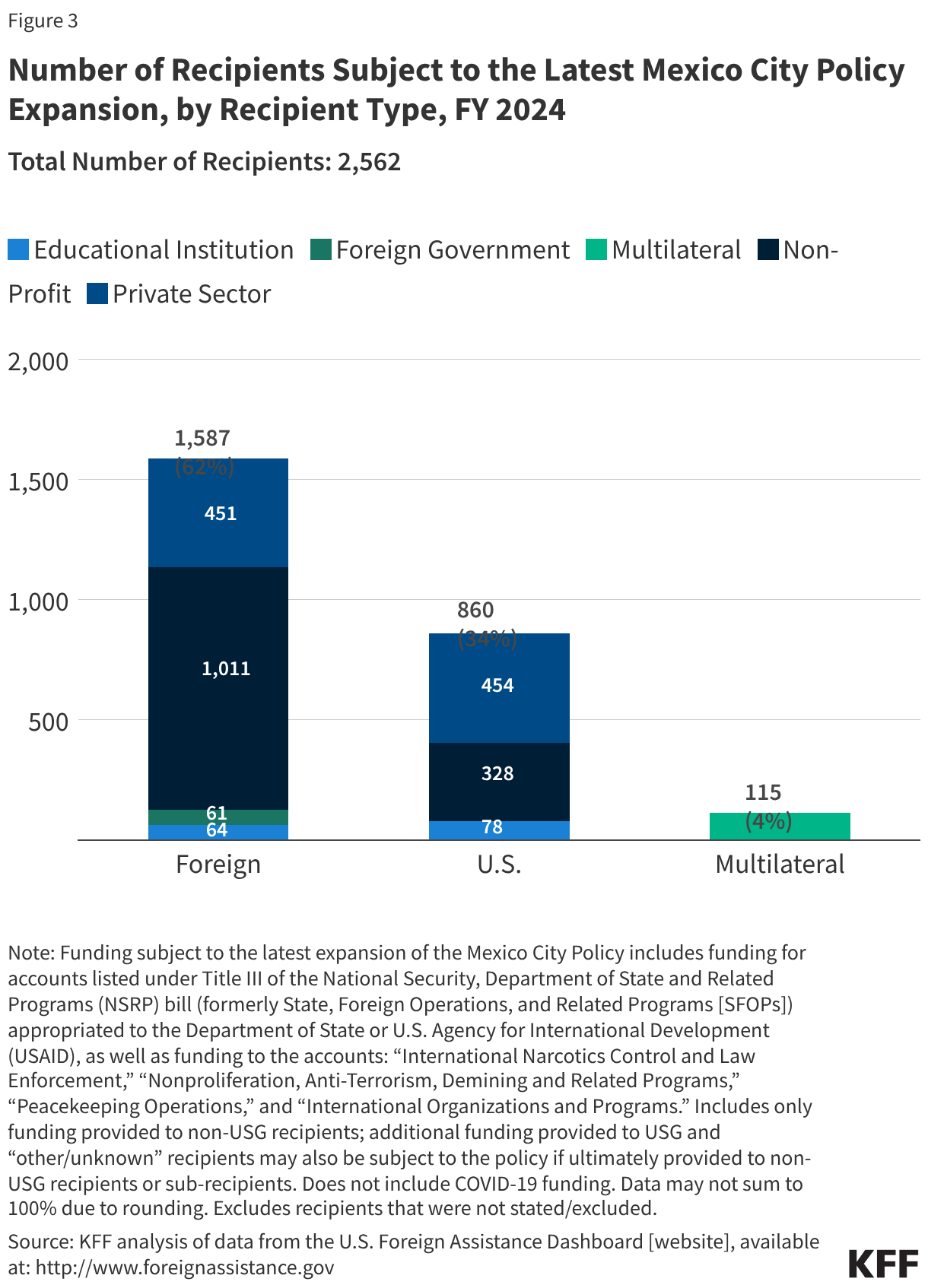
There were 2,562 non-USG prime recipients of U.S. foreign assistance in FY 2024, most8 of which (2,111 or 82%) would be subject to the policy for the first time. This number should be considered a floor, since any sub-recipients of U.S. foreign aid would also be subject to the policy.
Whereas most funding was provided to multilateral organizations, most recipients (62%, or 1,587) were foreign-based organizations. About a third (34%, or 860) were U.S.-based organizations. Multilateral organizations accounted for the remaining 4% (115) (see Figure 3).
NGOs (foreign- and U.S.-based) accounted for the vast majority (93%, or 2,386) of recipients. NGOs include:
non-profits (more than half – 52% - of all 2,562 recipients, or 1,339),
private sector organizations (more than a third – 35% - of all recipients, or 905), and
educational institutions (6% of all recipients, or 142).
Among the 2,386 NGO recipients, almost two-thirds (64%, or 1,526) were foreign NGOs, and the other third (36%, or 860) were U.S.-based NGOs.
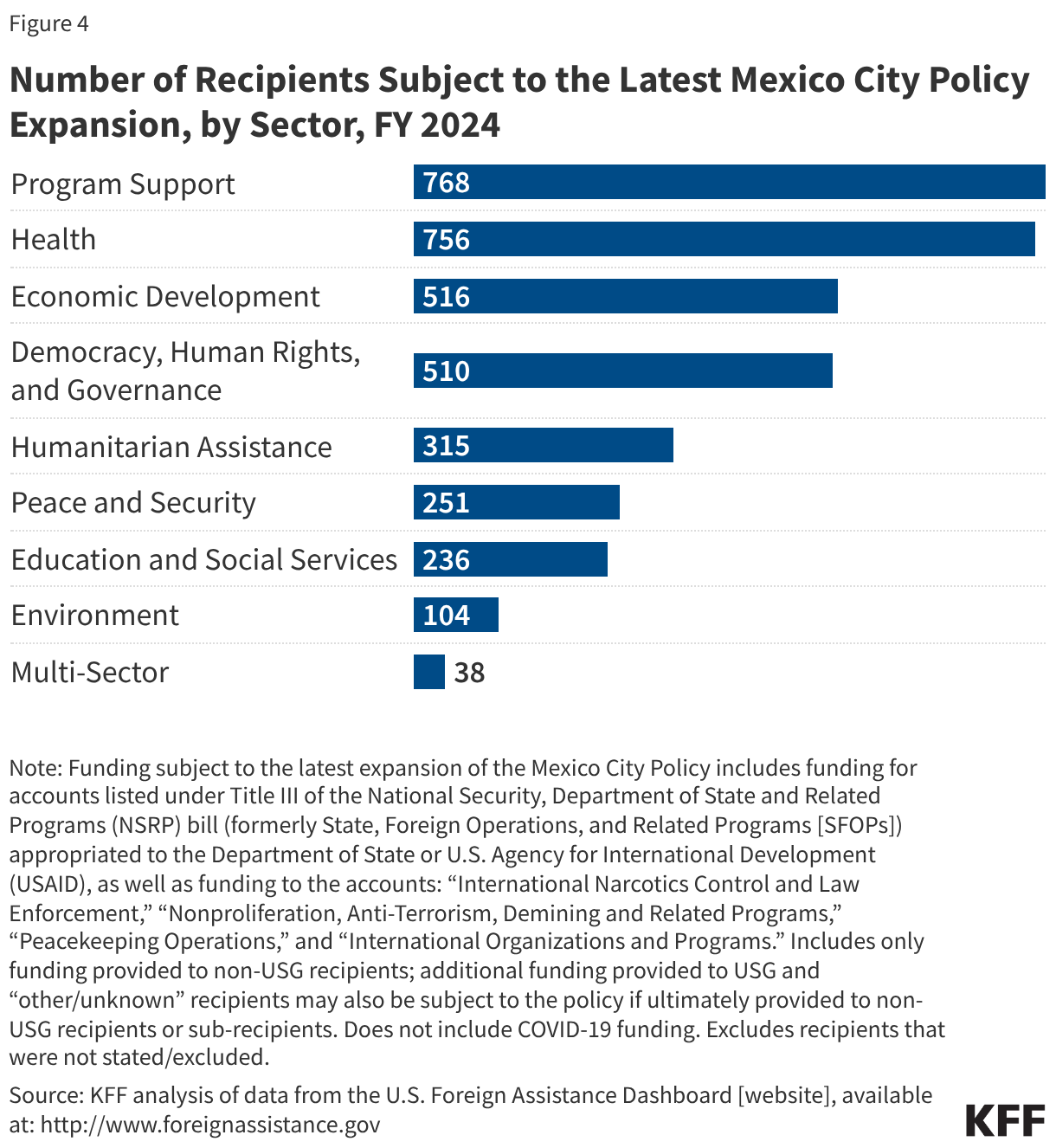
The sectors with the largest numbers of recipients in FY 2024 were program support9 (768), health (756), and economic development (516). The next largest sector was democracy, human rights, and governance (510), followed by humanitarian assistance (315) (see Figure 4).
Methodology
This analysis uses FY 2024 foreign assistance obligation data, downloaded from ForeignAssistance.gov on November 20, 2025. ForeignAssistance.gov is the U.S. government’s centralized data portal for budgetary and financial data provided by more than 20 federal agencies that manage foreign assistance programs. Obligations are binding agreements that will result in outlays of funding, immediately or sometime in the future. The policy, when in place, is applied to funding that is obligated to recipients either as part of an existing award or as part of a new award. Data on funding amounts and recipients were analyzed by agency, sector, location, and type of entity. To the extent possible, COVID-19 emergency funding was excluded from this analysis, as it represented one-time funding for a particular event.
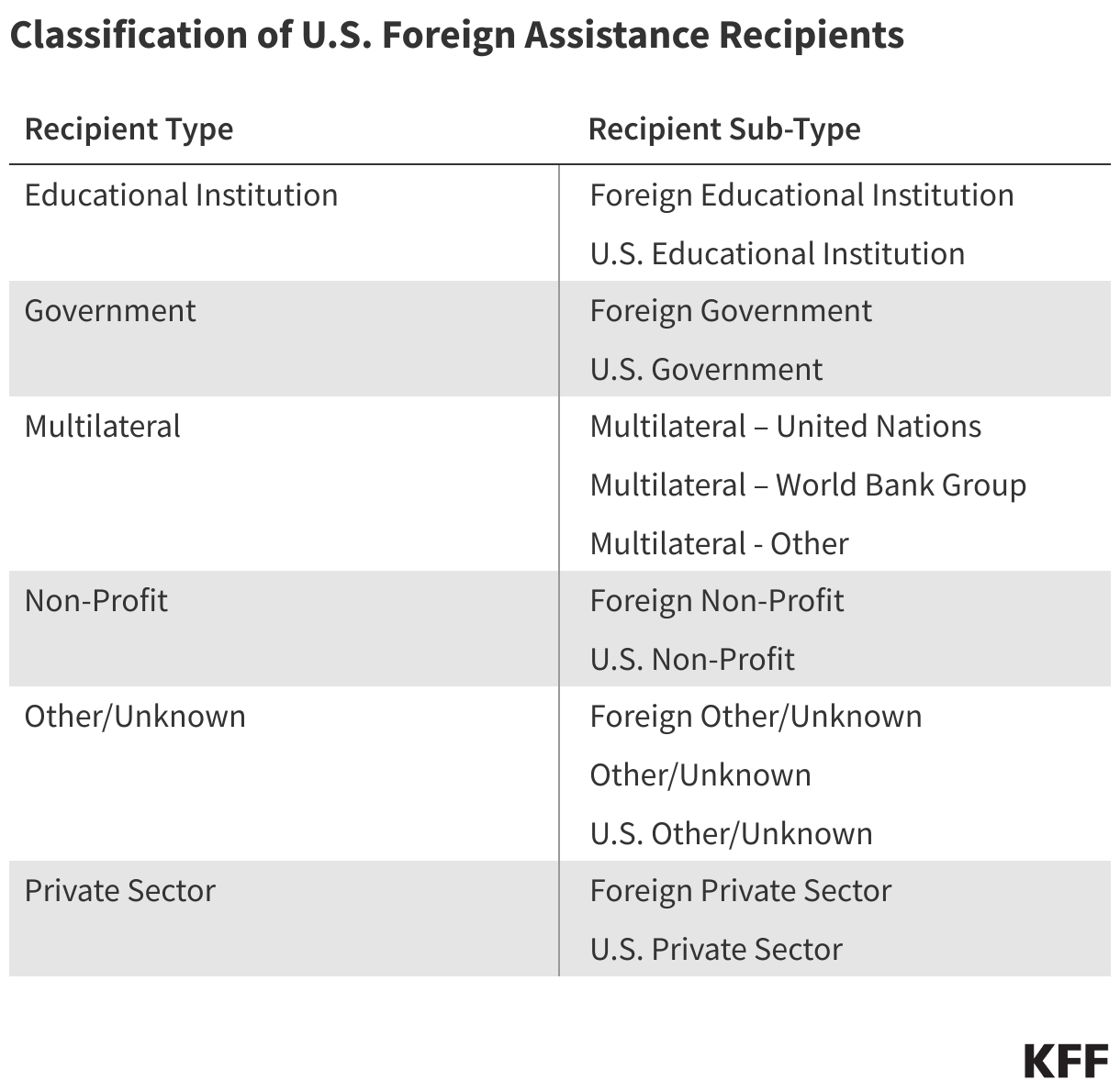
Recipients were categorized into the following groups (see table below) based on classifications already present in the ForeignAssistance.gov data as well as background research, where such classifications were not provided. Each recipient was reviewed, and the review sought to correct any mis-categorization in the original data and remove duplicates. “Other/Unknown” recipients were those that could not be easily identified as belonging to a particular recipient type/sub-type. Where it was not possible to identify a recipient as a single, implementing entity, they were excluded from analysis looking at the number of unique recipients.
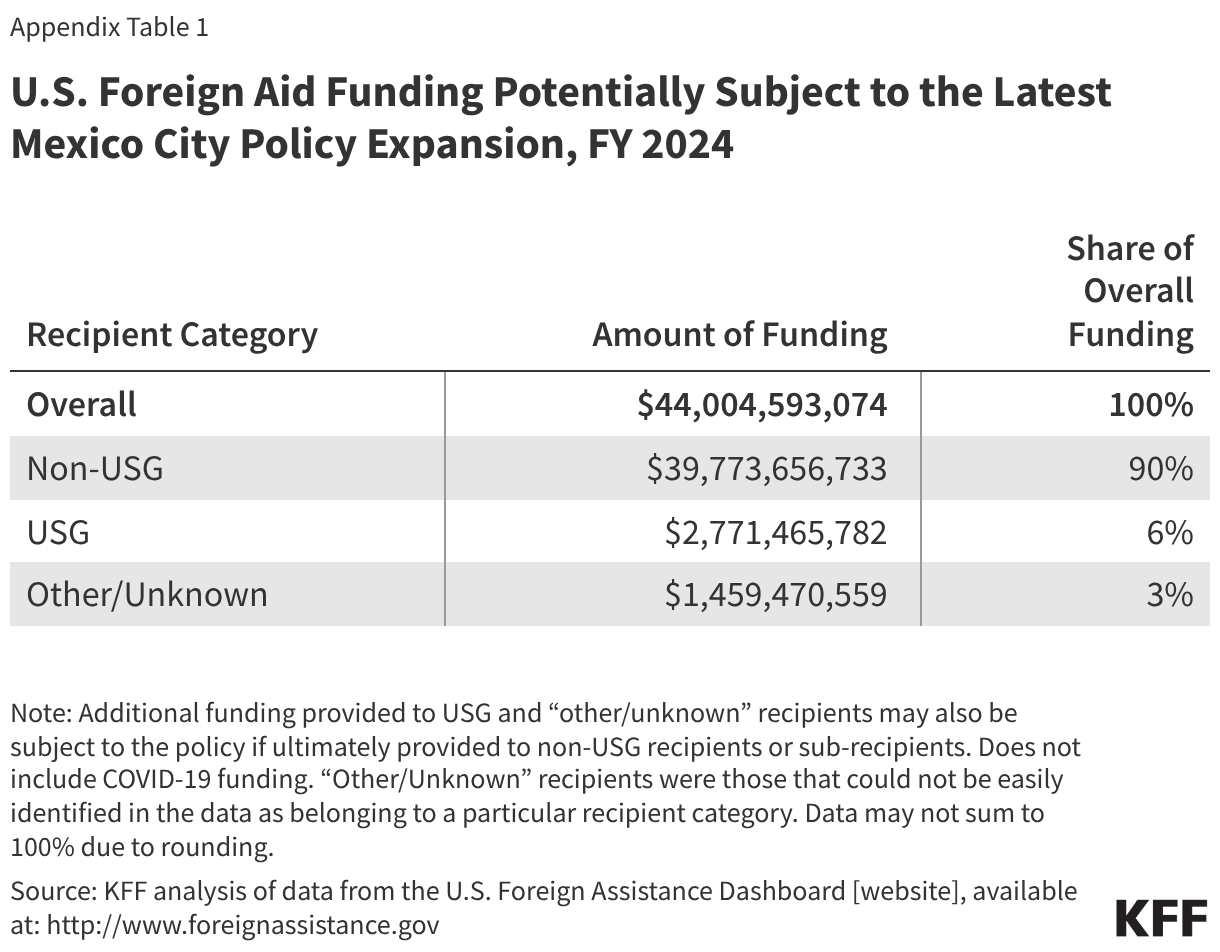
Funding included in the analysis was based on the specifications in the final rules and includes Title III funding appropriated to the State Department and USAID (now administered by the State Department) as well as funding appropriated to four other accounts under Department of State, Foreign Operations, and Related Programs (SFOPs)/National Security, State Department, and Related Programs (NSRP) appropriations acts (specifically, “International Narcotics Control and Law Enforcement,” “Nonproliferation, Anti-Terrorism, Demining and Related Programs,” “Peacekeeping Operations,” and “International Organizations and Programs”), whether or not these data were listed as "Economic" or "Military" funding. The analysis excluded the funding in these accounts that was directed to U.S. departments or agencies as prime recipients, which totaled $2.8 billion in FY 2024, as well as funding directed to “Other/Unknown” recipients, which totaled $1.5 billion in FY 2024 (although to the extent that this funding is ultimately provided to a non-USG sub-recipient, it too would be subject to the policy). The U.S. government has also indicated that its intention is to apply the latest MCP expansion to additional non-military foreign assistance at other U.S. agencies and departments, which would also increase the amount of funding and number of organizations subject to the latest expansion.
The analysis also includes funding provided through contracts (not just grants and cooperative agreements) for two reasons: first, the rules indicate that further rule-making will be undertaken to add these policy restrictions to contracts; and second, it is not possible to disaggregate obligations by funding instrument in ForeignAssistance.gov data.
Appendix Tables
Per the interim rules, a foreign non-governmental organization is defined as “any non-governmental organization or entity, whether non-profit or profit-making (including any commercial firm and educational institution), not organized or existing under the laws of the United States, any State of the United States, the District of Columbia, the Commonwealth of Puerto Rico, or any other territory or possession of the United States.” ↩︎
Specifically, funding appropriated to the U.S. Agency for International Development (USAID) and the State Department; this funding is “administered” by the State Department. USAID was dissolved by the Trump administration in 2025, with its remaining programs transferred to other agencies, including mainly but not solely the State Department. ↩︎
The policies apply differently to U.S. NGOs and foreign governments/parastatals than to foreign NGOs and multilateral organizations. ↩︎
The analysis excluded approximately $82 million in FY 2024 foreign aid funding that was identifiable as emergency COVID-19 assistance since it was one-time emergency funding. ↩︎
Each rule of PHFFA defines a foreign NGO as “any non-governmental organization or entity, whether non-profit or profit-making (including any commercial firm and educational institution), not organized or existing under the laws of the United States, any State of the United States, the District of Columbia, the Commonwealth of Puerto Rico, or any other territory or possession of the United States,” and it defines a U.S. NGO as “any non-governmental organization or entity, whether non-profit or profit-making (including any commercial firm and educational institution), organized or existing under the laws of the United States, any State of the United States, the District of Columbia, the Commonwealth of Puerto Rico, or any other territory or possession of the United States.” ↩︎
Each rule of PHFFA defines an international organization as “(A) Any organization designated as being entitled to enjoy the privileges, exemptions, and immunities under the International Organizations Immunities Act; (B) Any organization treated as a public international organization pursuant to the regulations or policies of the Department of State; (C) Any organization established by international agreement and whose governing body is composed principally of representatives of national governments; or (D) Any other multilateral entity in which sovereign nations participate.” ↩︎
Number of countries represents countries that received funding directly from the U.S. government; additional countries may be reached through regional and worldwide programming. ↩︎
Includes number of foreign governments, multilaterals, and U.S. NGOs that received foreign assistance as well as the number of foreign NGOs that received non-health assistance only. ↩︎
Program support is “general management support required to ensure completion of U.S. foreign assistance objectives by facilitating program management, accounting and tracking for costs” according to the State Department, Standardized Program Structure and Definitions (SPSD) [Updated Foreign Assistance Standardized Program Structure and Definitions], June 2017, uploaded Feb. 2023, available at: https://www.state.gov/wp-content/uploads/2023/02/The-New-SPSD-June-2017-Accessible-2.16.2023.pdf. ↩︎
Virtually all enrollees in Medicare Advantage (99%) are required to obtain prior authorization for some services – most commonly, higher cost services, such as inpatient hospital stays, skilled nursing facility stays, and chemotherapy. This contrasts with traditional Medicare, where only a limited set of services, including certain outpatient hospital services, non-emergency ambulance transport, and durable medical equipment, require prior authorization (see Box 1). Insurers often use prior authorization requirements to assess whether health care services are medically necessary before they are covered and to reduce unnecessary costs. At the same time, prior authorization processes and requirements, including the use of artificial intelligence to review requests, may result in administrative hassles for providers, delays for patients in receiving necessary care, and in some instances, denials of medically necessary services, such as post-acute care.
Prior authorization practices have gotten a fair amount of attention in recent years. KFF polling shows that most people view delays and denials of care by health insurance companies as a problem, with about two-thirds of Medicare beneficiaries reporting that they consider it to be a major problem. Last summer, the Trump Administration announced that private health insurers, including those that comprise a majority of Medicare Advantage enrollment, agreed to a voluntary initiative to improve the prior authorization process. Lawmakers in Congress have also been active on the issue, with bipartisan legislation introduced in both the House and Senate. Additionally, on January 1, 2026, the Administration launched the Wasteful and Inappropriate Spending Reduction (WISeR) model to test the use of enhanced technology to conduct prior authorization for an additional set of select services in traditional Medicare in six states.
This analysis uses data submitted by Medicare Advantage insurers to the Centers for Medicare and Medicaid Services (CMS) to examine the trends in the number of prior authorization requests, denials, and appeals for 2019 through 2024, as well as differences across Medicare Advantage insurers with the largest enrollment. It does not include requests or denials by type of service or type of plan because CMS does not collect or report this information, though such data could help inform consumers in choosing among plans. It also presents data from CMS about the use of prior authorization in traditional Medicare, including the number of requests and denials for fiscal years 2021 through 2024.
Key Takeaways
Nearly 53 million prior authorization requests were submitted to Medicare Advantage insurers on behalf of Medicare Advantage enrollees in 2024, an increase from 2023 (49.8 million) as the number of people enrolled in Medicare Advantage has grown. Substantially fewer prior authorization requests for traditional Medicare than Medicare Advantage beneficiaries were submitted to CMS – just over 625,000 in fiscal year 2024.
In 2024, there were 1.7 prior authorization requests on average per Medicare Advantage enrollee, a slight decline from 1.8 in 2023. In contrast, in 2024, about 2 prior authorization requests were submitted per 100 traditional Medicare beneficiaries – a rate of about 0.02 per enrollee – which reflects the limited set of services subject to prior authorization in traditional Medicare.
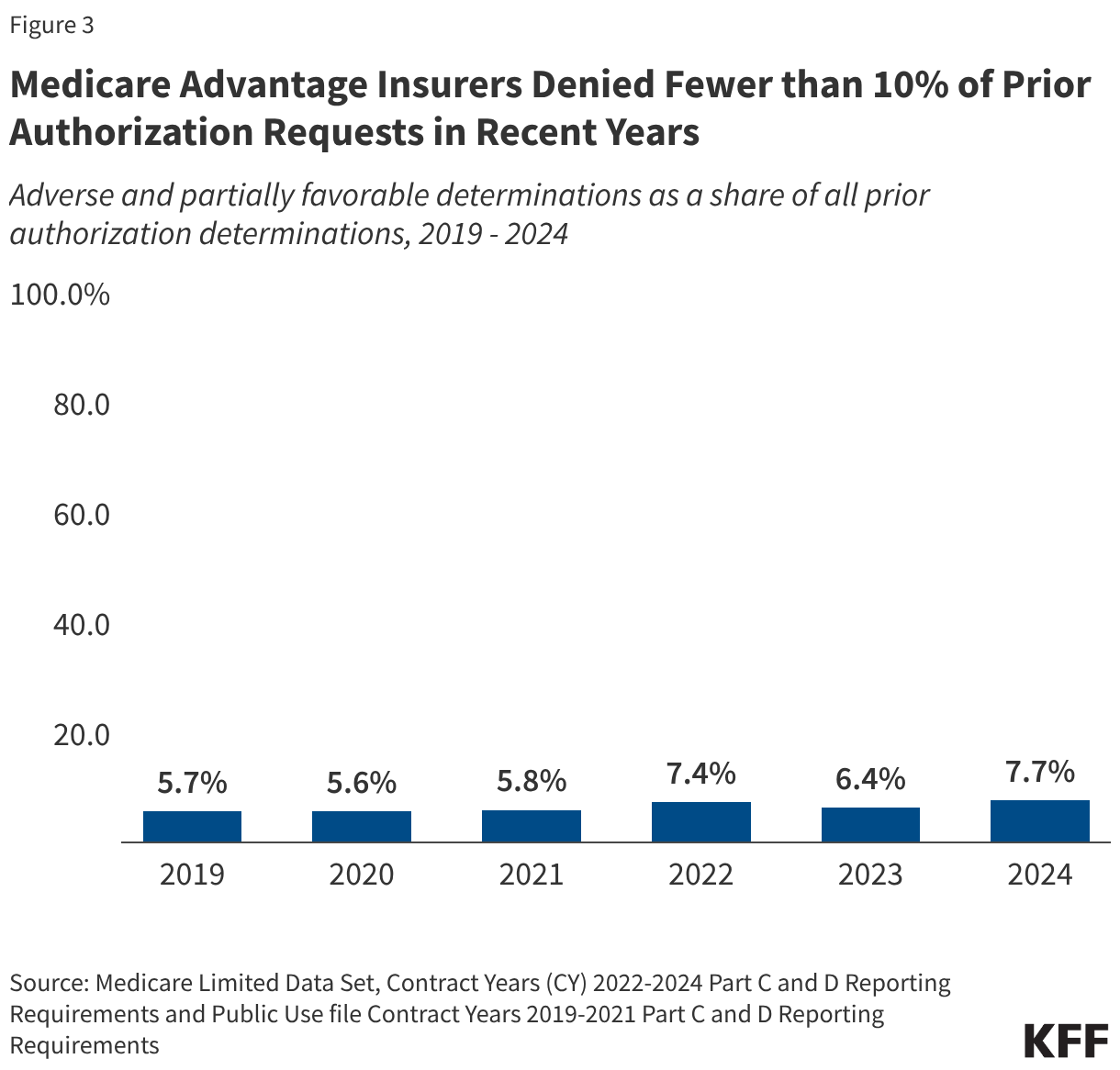
In 2024, Medicare Advantage insurers fully or partially denied 4.1 million prior authorization requests, which is a somewhat larger share (7.7%) of all requests than in 2023 (6.4%) and similar to 2022 (7.4%). Though there were substantially fewer prior authorization requests for traditional Medicare beneficiaries, a larger share was denied – 22.9% (less than 150,000) in 2024.
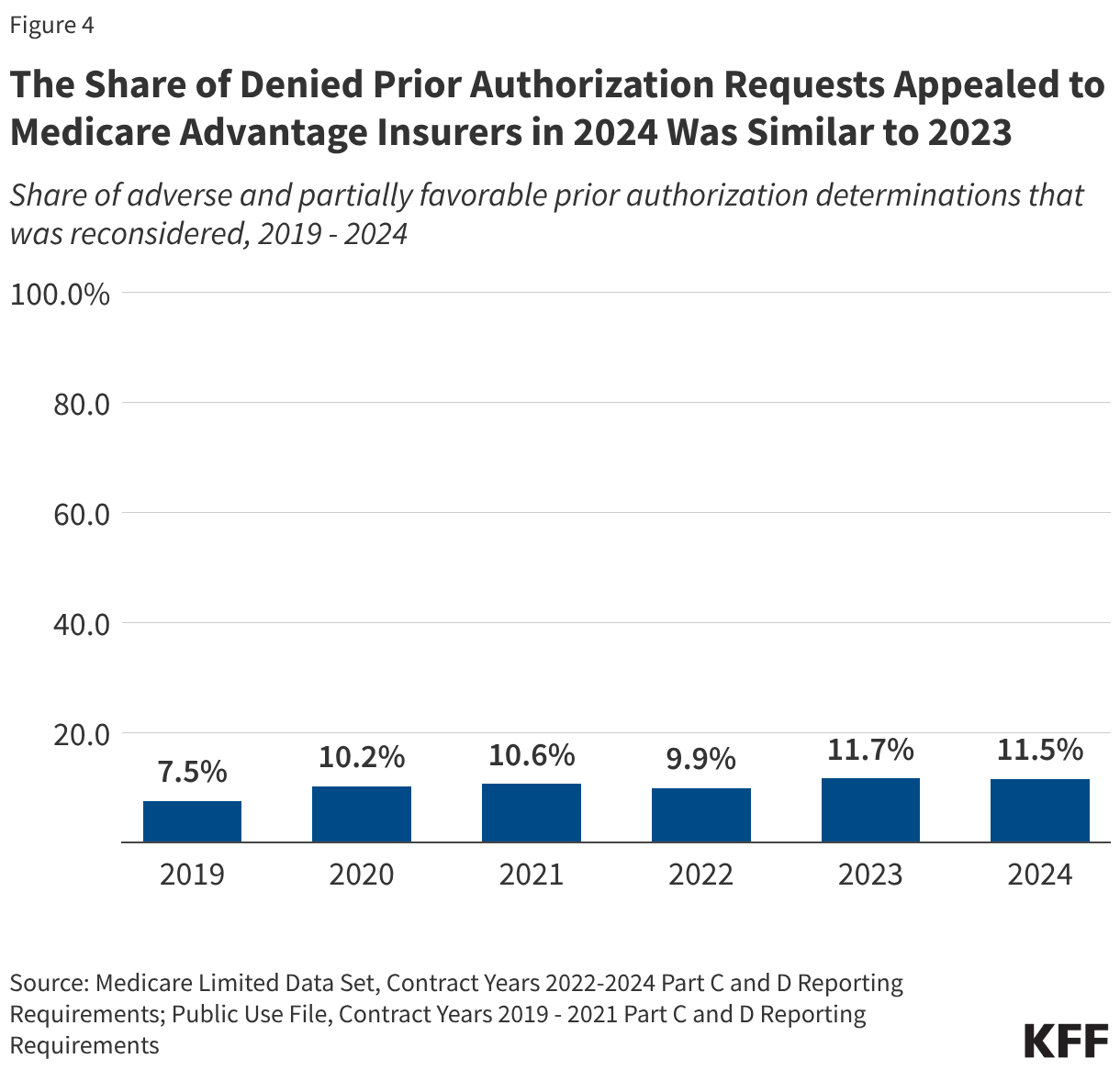
A small share of denied prior authorization requests was appealed in Medicare Advantage –11.5% in 2024, similar to 2023 (11.7%).That represents an increase since 2019, when 7.5% of denied prior authorization requests in Medicare Advantage were appealed. The traditional Medicare data do not include information on appeals for 2023 and 2024, but in 2022 a relatively small share of denied prior authorization requests was appealed in traditional Medicare (6.4% in 2022).
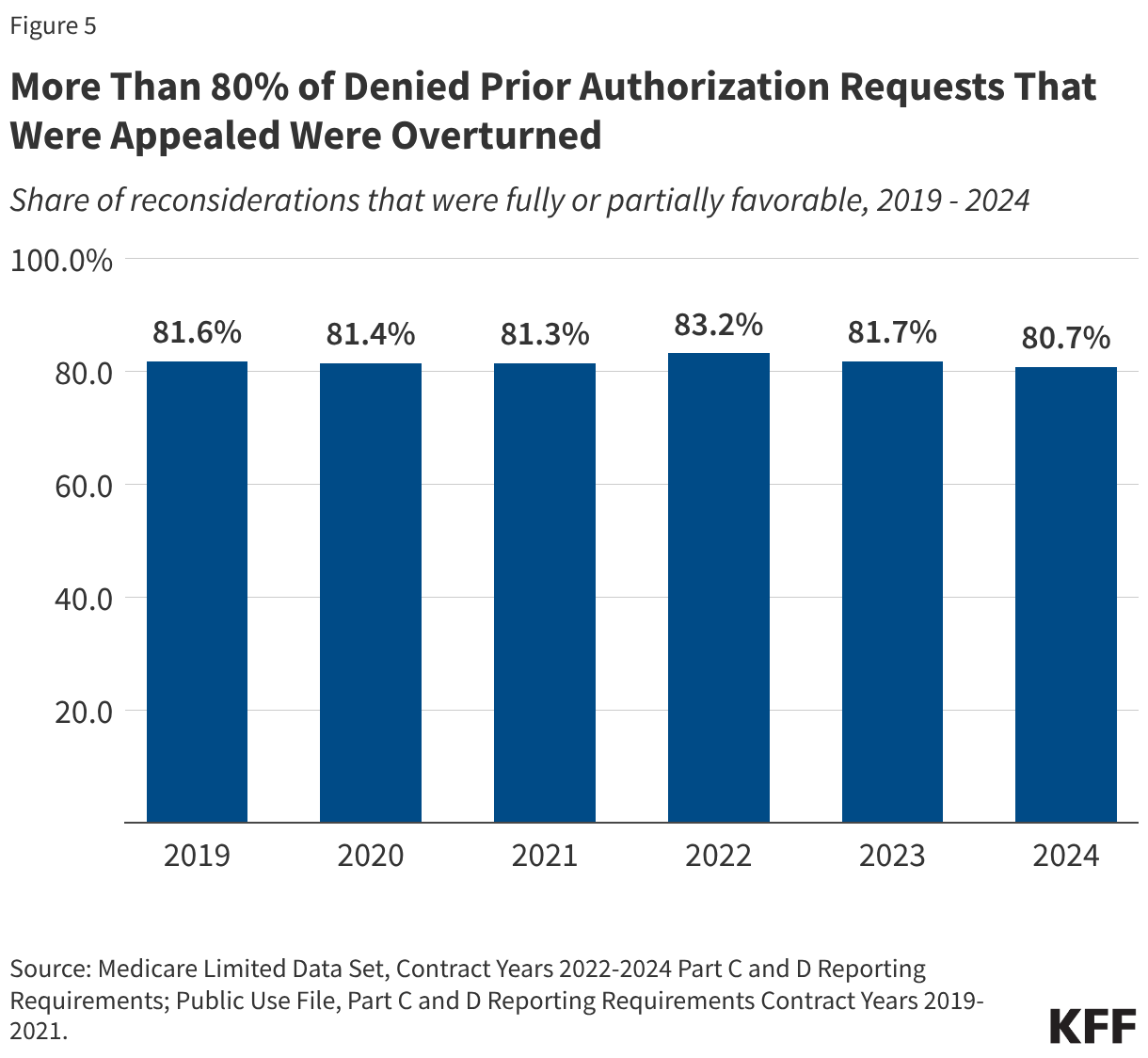
Though a small share of prior authorization denials were appealed to Medicare Advantage insurers, most appeals (80.7%) were partially or fully overturned in 2024. Across all years examined, more than eight in ten appeals overturned the initial denial. These requests represent medical care that was ordered by a health care provider and ultimately deemed necessary but was potentially delayed because of the additional step of appealing the initial prior authorization decision. Such delays may have negative effects on a patient’s health.
Use of Prior Authorization in Medicare Advantage
CMS requires Medicare Advantage insurers to submit data for each Medicare Advantage contract (which usually includes multiple plans) as part of its oversight of Medicare Advantage plans. Insurers are required to submit the number of prior authorization determinations made during a year and whether the request was approved. Insurers are additionally required to report the number of initial decisions that were appealed (reconsiderations) and the outcome of that process, including whether the initial decision was affirmed, partially overturned, or fully overturned. These data are useful for assessing overall trends and variations across insurers, but do not contain the information necessary to understand how the use of prior authorization varies by type of service or type of plan because they are aggregated to the contract level. CMS is implementing a pilot program to collect more detailed data at the plan and service level this year, which would help assess whether some enrollees bear a higher burden of prior authorization requirements or are more frequently denied requested services. CMS states that it anticipates expanding the requirement to all plans in 2027.
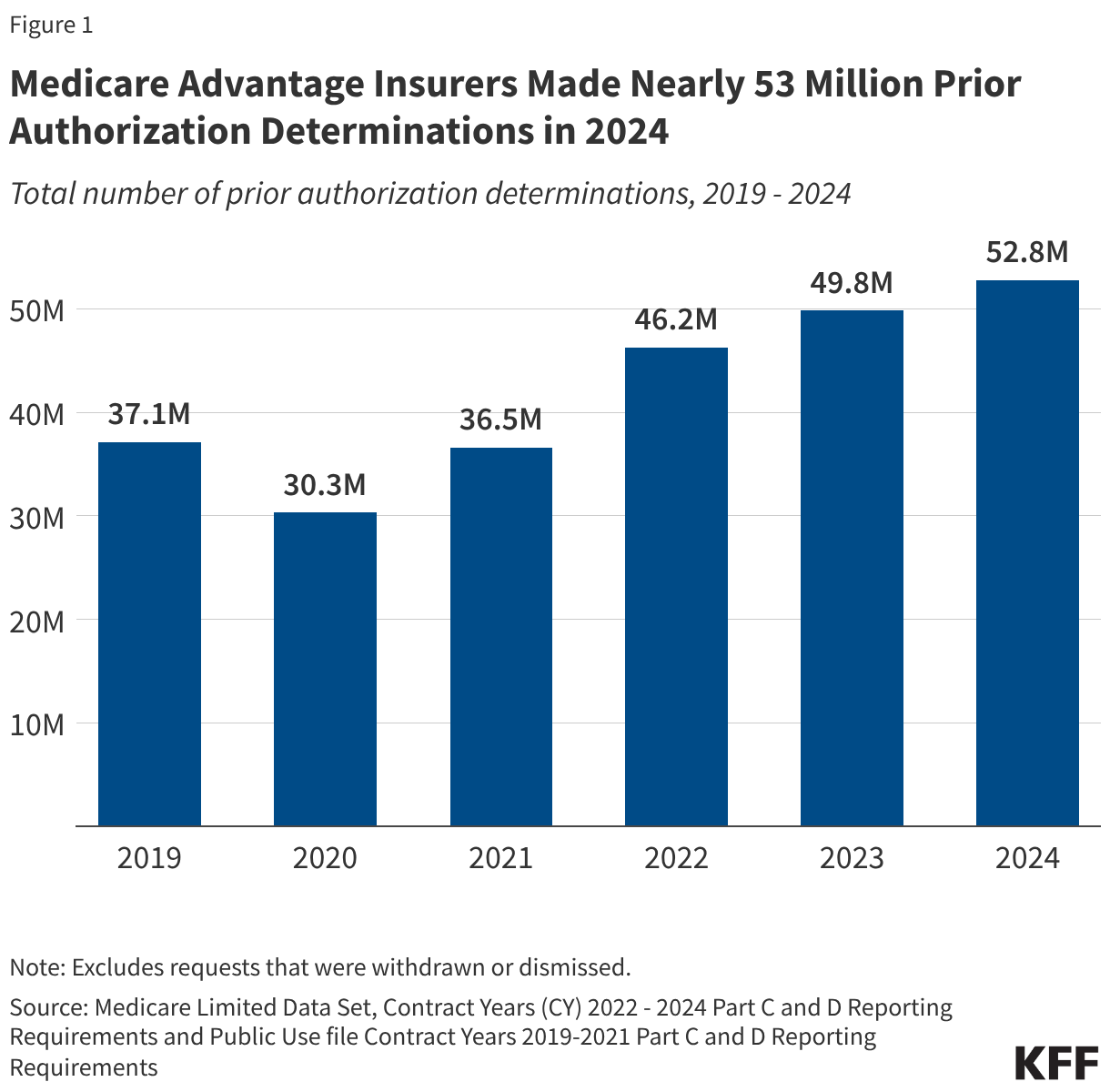
In 2024, nearly 53 million prior authorization requests were submitted to Medicare Advantage insurers.
After dropping in 2020 amid the initial phase of the COVID-19 pandemic, prior authorization requests increased steadily between 2021 and 2024 (Figure 1). The decline in 2020 was likely due to both a decline in utilization, as well as the option for insurers to temporarily pause prior authorization requirements during the public health emergency.
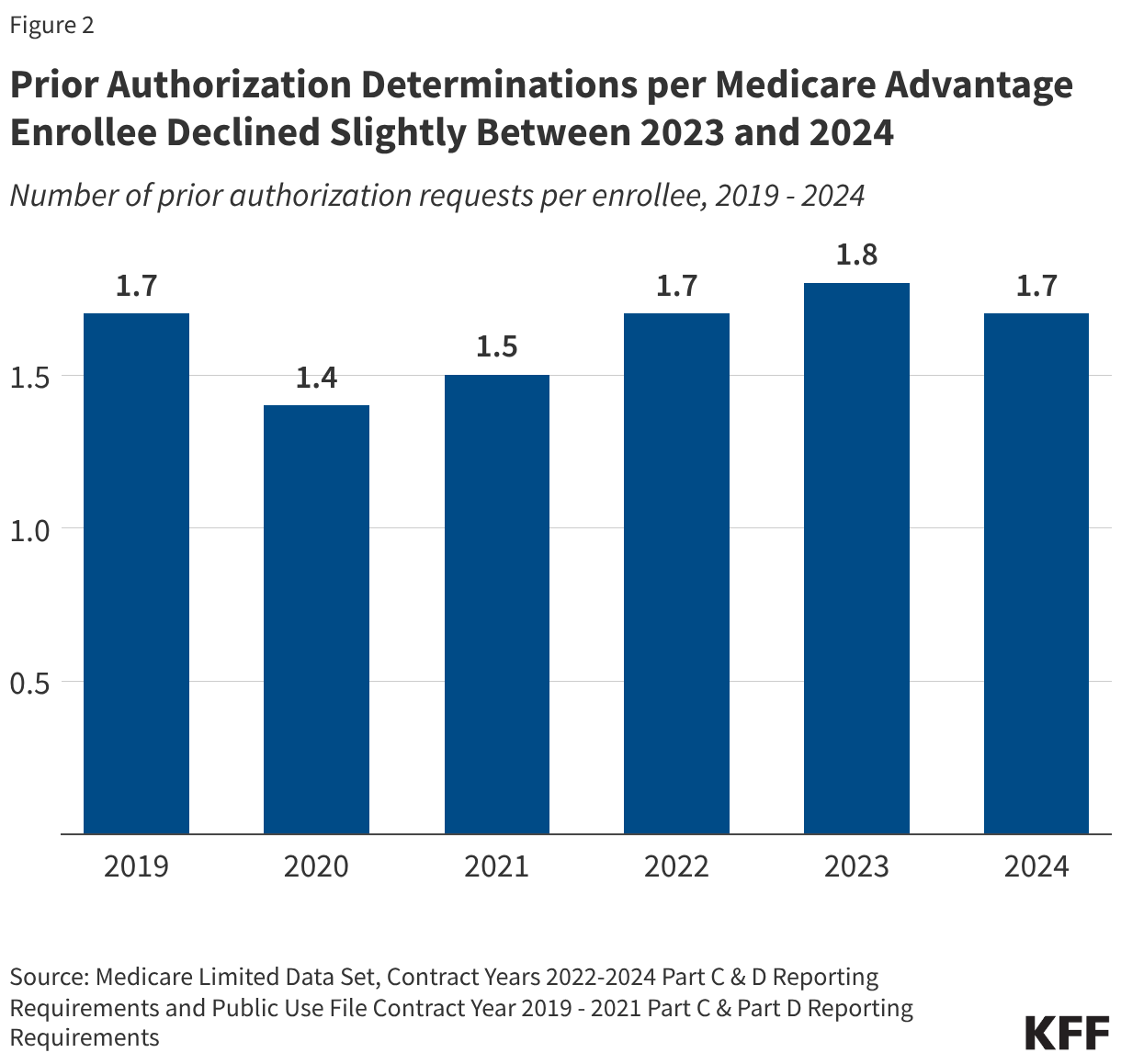
The increase in the total number of prior authorization requests since 2020 corresponds to an increase in Medicare Advantage enrollment. Between 2019 and 2024, the number of Medicare Advantage enrollees rose from 22 million people to 33 million people. Therefore, the number of prior authorization requests per enrollee has remained relatively constant in the past few years. In 2019, there were approximately 1.7 prior authorization requests per Medicare Advantage enrollee. That number dropped at the onset of the COVID-19 pandemic to 1.4 in 2020 and 1.5 in 2021, before returning to the pre-pandemic level of 1.7 requests per enrollee in 2022 and rising slightly to 1.8 in 2023. In 2024, Medicare Advantage enrollment growth outpaced the increase in the number of prior authorization requests, leading to a slight drop in the number of requests per enrollee to 1.7 (Figure 2).
The modest decline in the number of prior authorization determinations per enrollee corresponds with increased regulatory attention to prior authorization in Medicare Advantage which clarified the criteria that may be used by Medicare Advantage plans to establish prior authorization policies. In addition, certain Medicare Advantage insurers also announced changes to prior authorization practices in 2023 and 2024, such as UnitedHealth Group’s decision to reduce the number of services subject to prior authorization and launch a national “gold card” program that exempts certain providers from prior authorization requirements.
Medicare Advantage insurers denied 4.1 million (7.7%) prior authorization requests in 2024.
Of the 52.8 million prior authorization determinations in 2024, more than 90% (48.7 million) were fully favorable, meaning the requested item or service was approved in full. However, the remaining 4.1 million prior authorization requests (7.7%) were denied in full or in part by Medicare Advantage insurers. This is slightly higher than the 6.4% of requests that were denied in 2023 and similar to the share denied in 2022 (Figure 3). Across all years, most denials (73% in 2024, data not shown) were denied in full, while a minority of denials were determined to be partially favorable, meaning that only part of the request was approved. For example, the insurer may have approved 10 of 14 requested therapy sessions.
Just 11.5% of denied prior authorization requests were appealed to Medicare Advantage insurers in 2024.
As in previous years, the majority of the 4.1 million denied prior authorization requests were not appealed. Though the share of denied requests that are appealed is small at just 11.5%, similar to the share in 2023 (11.7%), it has risen over time, from 7.5% in 2019 (Figure 4). These include appeals of claims that were both fully and partially denied.
The vast majority of denied prior authorization requests that were appealed were subsequently overturned by Medicare Advantage insurers.
In each year from 2019 through 2024, more than eight in ten denied prior authorization requests that were appealed were overturned (Figure 5). This raises questions about whether the initial request should have been approved, although it could also indicate that the initial request was missing the required documentation to justify the service. In either case, patients potentially faced delays in obtaining services that were ultimately approved because of the prior authorization process.
Variation in Use of Prior Authorization Across Medicare Advantage Insurers in 2024
In 2024, the volume of prior authorization determinations varied across Medicare Advantage insurers, as did the share of requests that were denied, the share of denials that were appealed, and the share of decisions that were overturned upon appeal, meaning people may have different experiences depending on the Medicare Advantage plan in which they enroll.
Across most insurers, fewer prior authorization requests per enrollee were correlated with a higher share of requests being denied and vice versa. For example, prior authorization requests for UnitedHealth Group Inc. and Humana Inc., the two largest Medicare Advantage insurers, were among the lowest (UnitedHealth Group Inc., 1.0 requests per enrollee) and the highest (Humana Inc., 2.2 requests per enrollee) observed, and correspondingly, denial rates were above average (UnitedHealthcare, 12.8%) and below average (Humana, 5.8%) for these insurers.
While all Medicare Advantage insurers require prior authorization for at least some services, there is variation across insurers and plans in the specific services that are subject to these requirements. In addition, some insurers waive prior authorization requirements for certain providers, for example, as part of risk-based contracts or through “gold carding” programs that exempt providers with a history of complying with the insurer’s prior authorization policies.
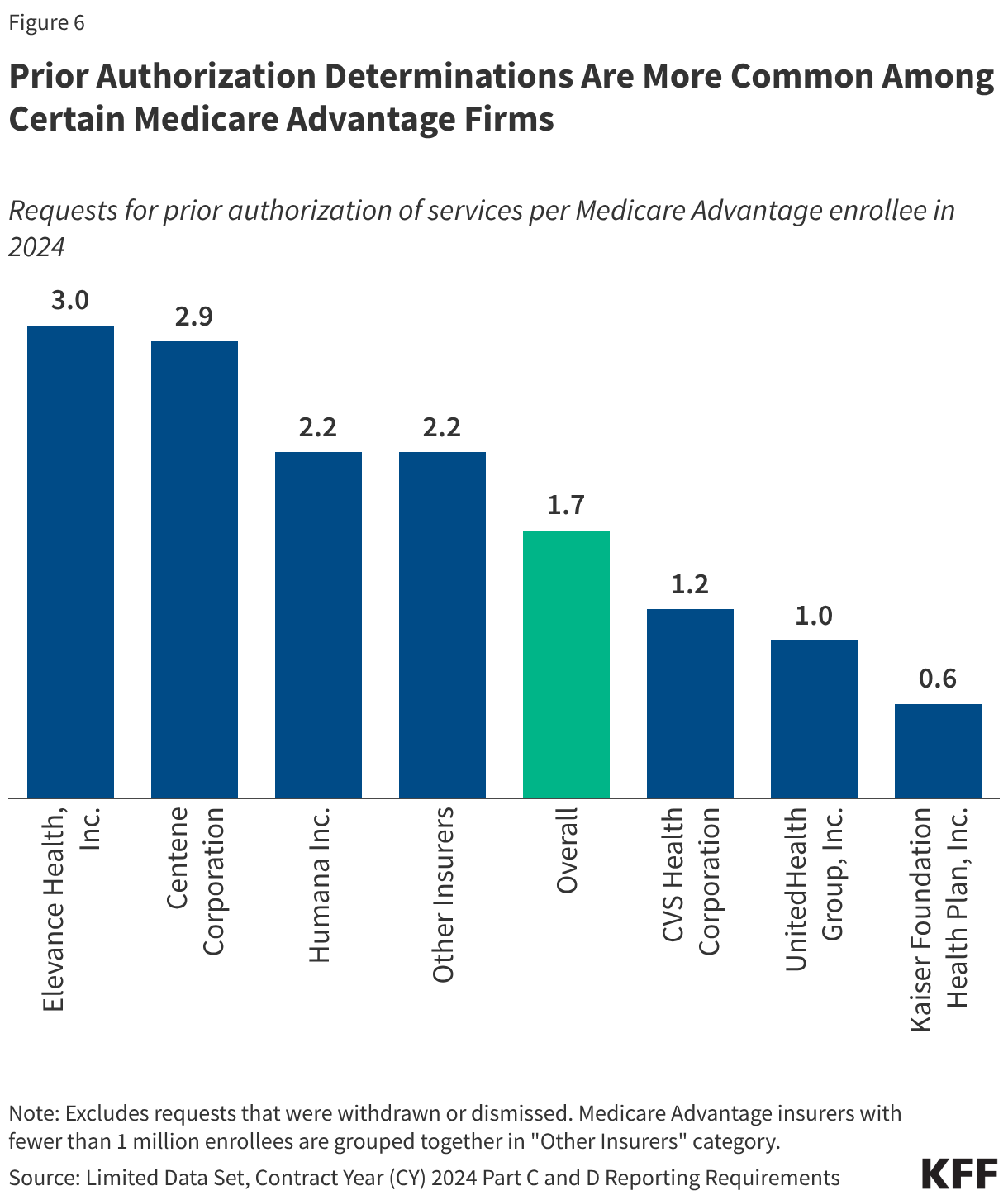
Prior authorization requests were most common among Elevance and Centene plans.
The number of prior authorization requests per enrollee ranged from a low of 0.6 requests per enrollee in plans sponsored by Kaiser Foundation Health Plan, Inc. to a high of 3.0 requests per enrollee in Elevance Health, Inc. and Centene Corporation plans (Figure 6). Kaiser is atypical among insurers in that it generally operates its own hospitals and contracts with an affiliated medical group. Looking across other insurers that are more similar, the low end of the range was 1.0 prior authorization requests per enrollee in UnitedHealth Group, Inc. plans. Differences across Medicare Advantage insurers in the number of prior authorization requests per enrollee likely reflect some combination of differences in the services subject to prior authorization requirements, the frequency with which contracted providers are exempted from those requirements (which may be related to the extent to which providers are affiliated with the insurer), how onerous the prior authorization process is for a particular insurer relative to others, and differences in enrollees’ health conditions and the health care services they use.
UnitedHealth Group denied the highest share of prior authorization requests while Elevance denied the fewest.
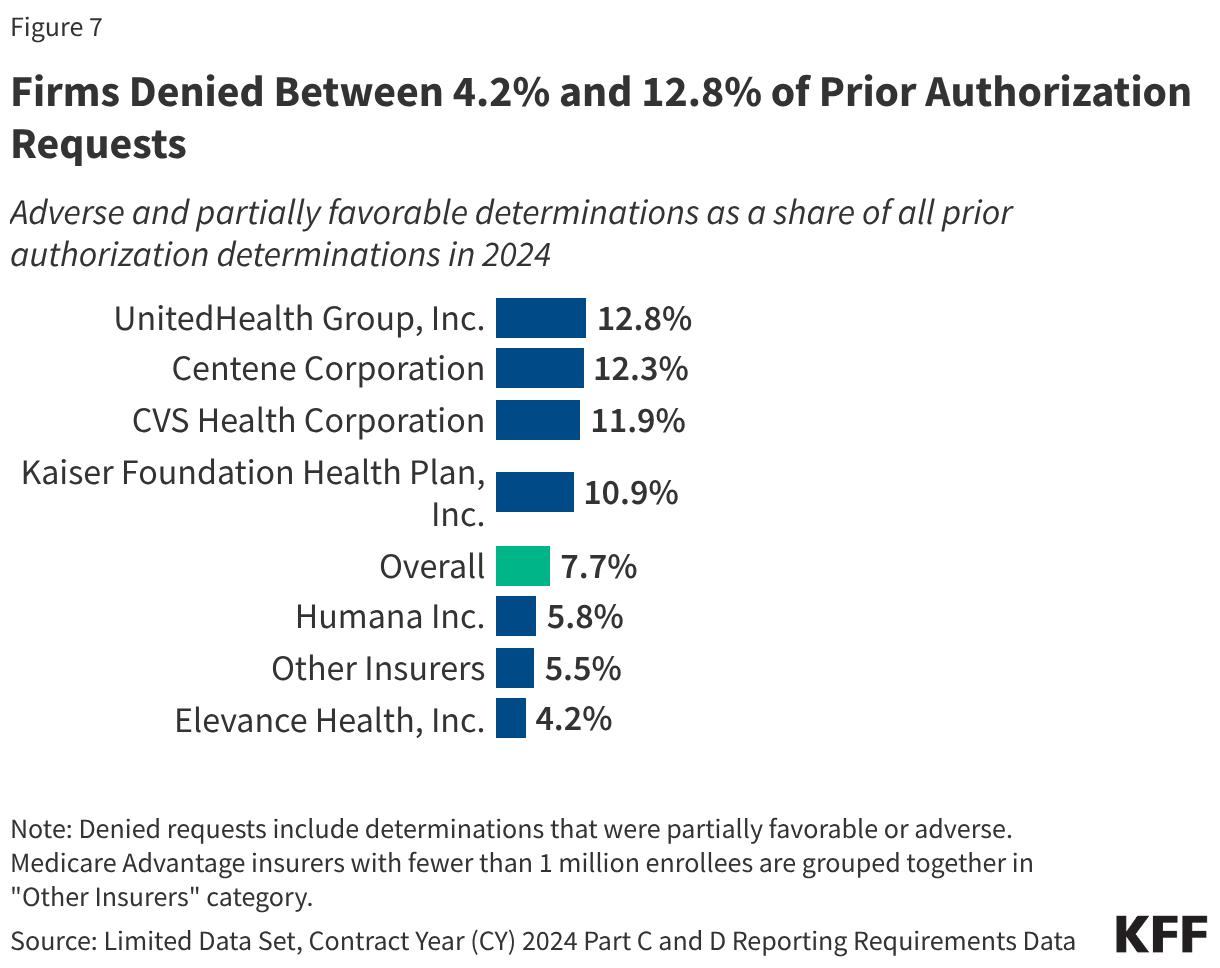
The denial rate ranged from 4.2% of prior authorization requests for Elevance Health plans to 12.8% of prior authorization requests for UnitedHealth Group plans (Figure 7). The overall denial rate includes requests that were both fully and partially denied (adverse and partially favorable determinations, respectively).
Most insurers that had more prior authorization requests per enrollee than average denied a smaller share of those requests than average, such as Elevance Health, which had 3.0 prior authorization requests per enrollee and a denial rate of 4.2%. Conversely, insurers with fewer prior authorization requests per enrollee denied a higher share of those requests, such as UnitedHealth Group, which had 1.0 prior authorization requests per enrollee and a denial rate of 12.8%. Centene Corporation was an exception with both a relatively high number of prior authorization requests (2.9 per enrollee) and a relatively high denial rate (12.3%).
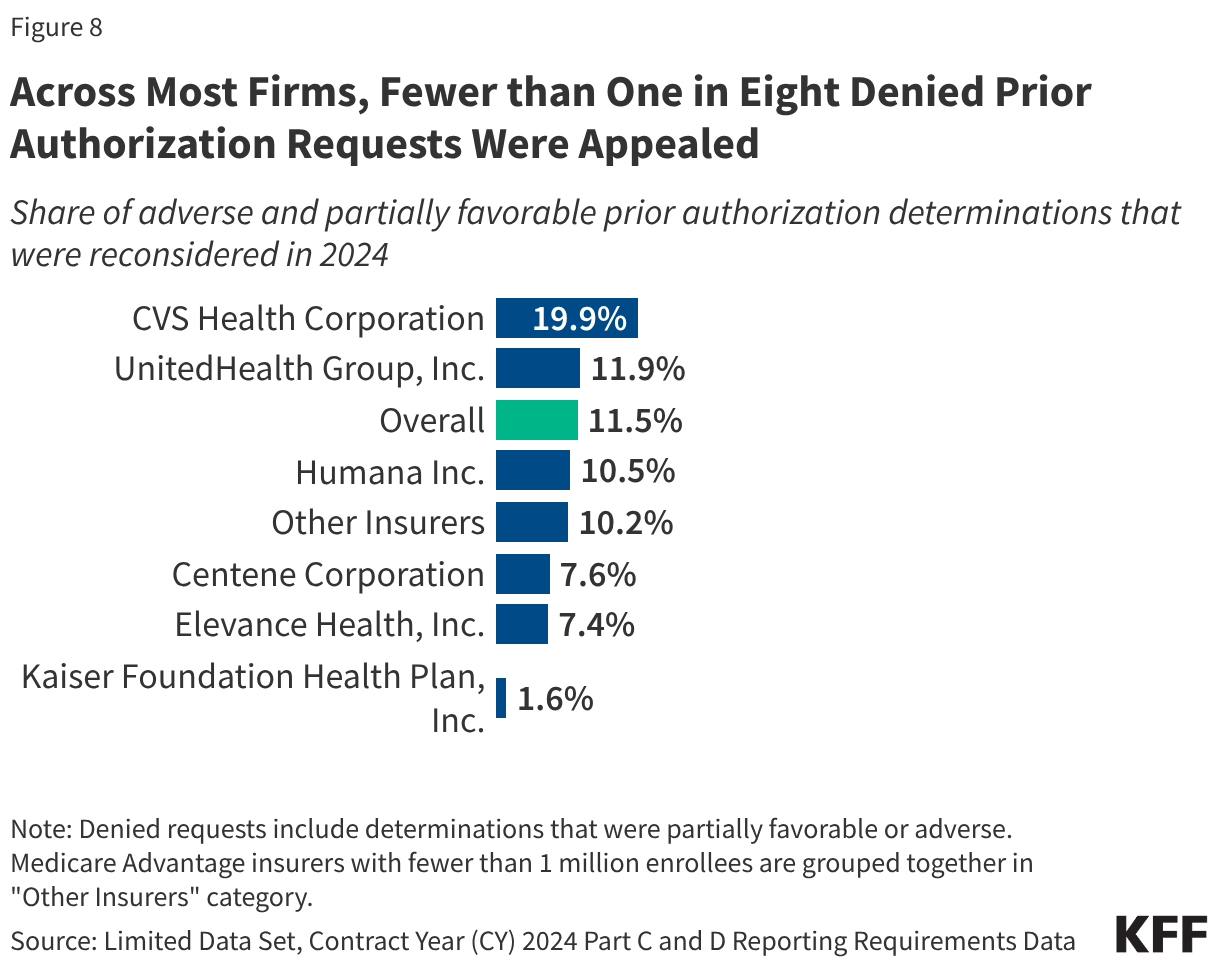
Across all insurers, a small share of denials was appealed.
Most denied prior authorization requests are not appealed to the Medicare Advantage insurer. The shares ranged from 1.6% for Kaiser Foundation Health Plan to 19.9% for CVS Health Corporation, with the appeal of fewer than one in twelve denials across all insurers except CVS Health Corporation (Figure 8).
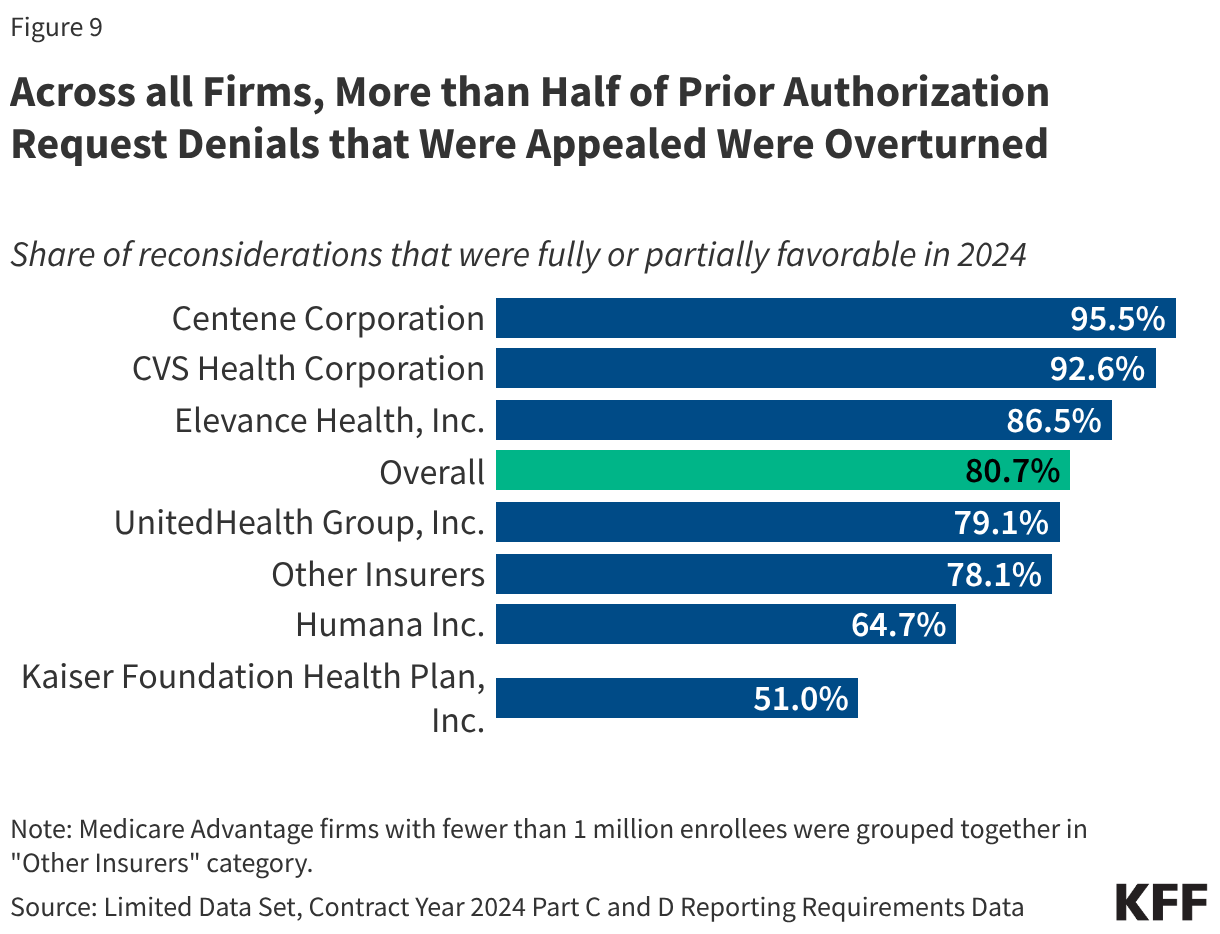
Across all firms, more than half of appeals were successful.
Even though most denials were not appealed, when they were, most of the initial decisions were partially or fully overturned. The share of appeals that resulted in favorable decisions overturning the initial denial was lowest for Kaiser Foundation Health Plan (51.0%) and highest for Centene Corporation (95.5%) (Figure 9), which also had the second highest share of requests initially denied.
The Use of Prior Authorization in Traditional Medicare
The use of prior authorization is relatively new to traditional Medicare and only used for a limited set of services, including certain outpatient hospital services, non-emergency ambulance transport, and durable medical equipment (see Box 1). The prior authorization process does not change any documentation requirements that are necessary for receiving Medicare payment – the confirmation that coverage requirements are met are required earlier in the review process. CMS has published reports presenting data on the use of prior authorization in traditional Medicare for fiscal years 2021, 2022, 2023, and 2024. These reports include information on the number of requests received, reviews completed, and the number and share of requests that were affirmed. For 2021 and 2022 only, the data also include information on appeals and the outcome of the appeal.
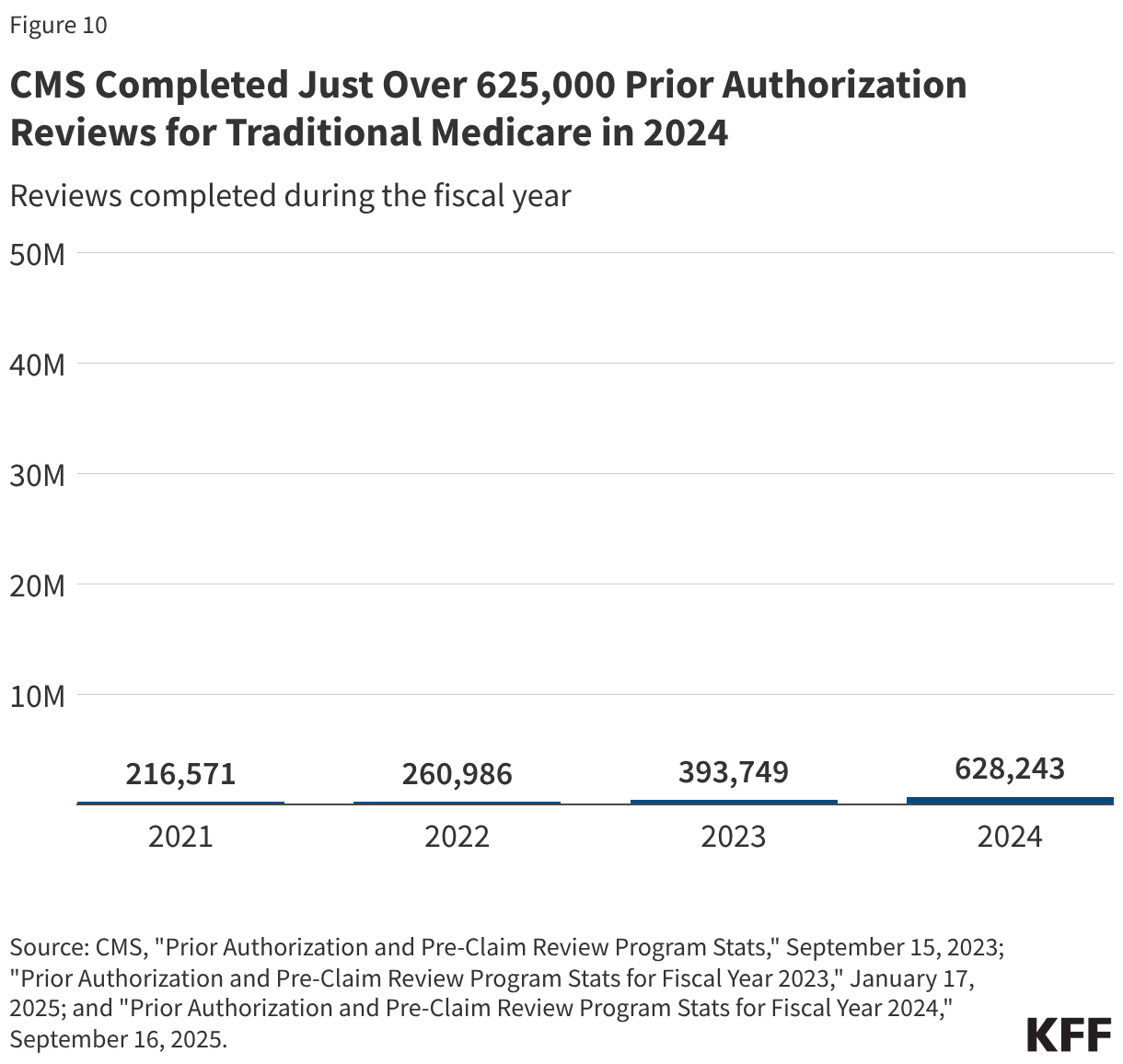
Just over 625,000 prior authorization reviews were completed by CMS for traditional Medicare in 2024.
Across the three categories of services that required prior authorization, there were 216,571 reviews completed in 2021, 260,986 reviews completed in 2022, 393,749 reviews completed in 2023, and 628,243 reviews completed in 2024 (Figure 10). This translates to about 2 prior authorization reviews per 100 traditional Medicare beneficiaries in 2024.
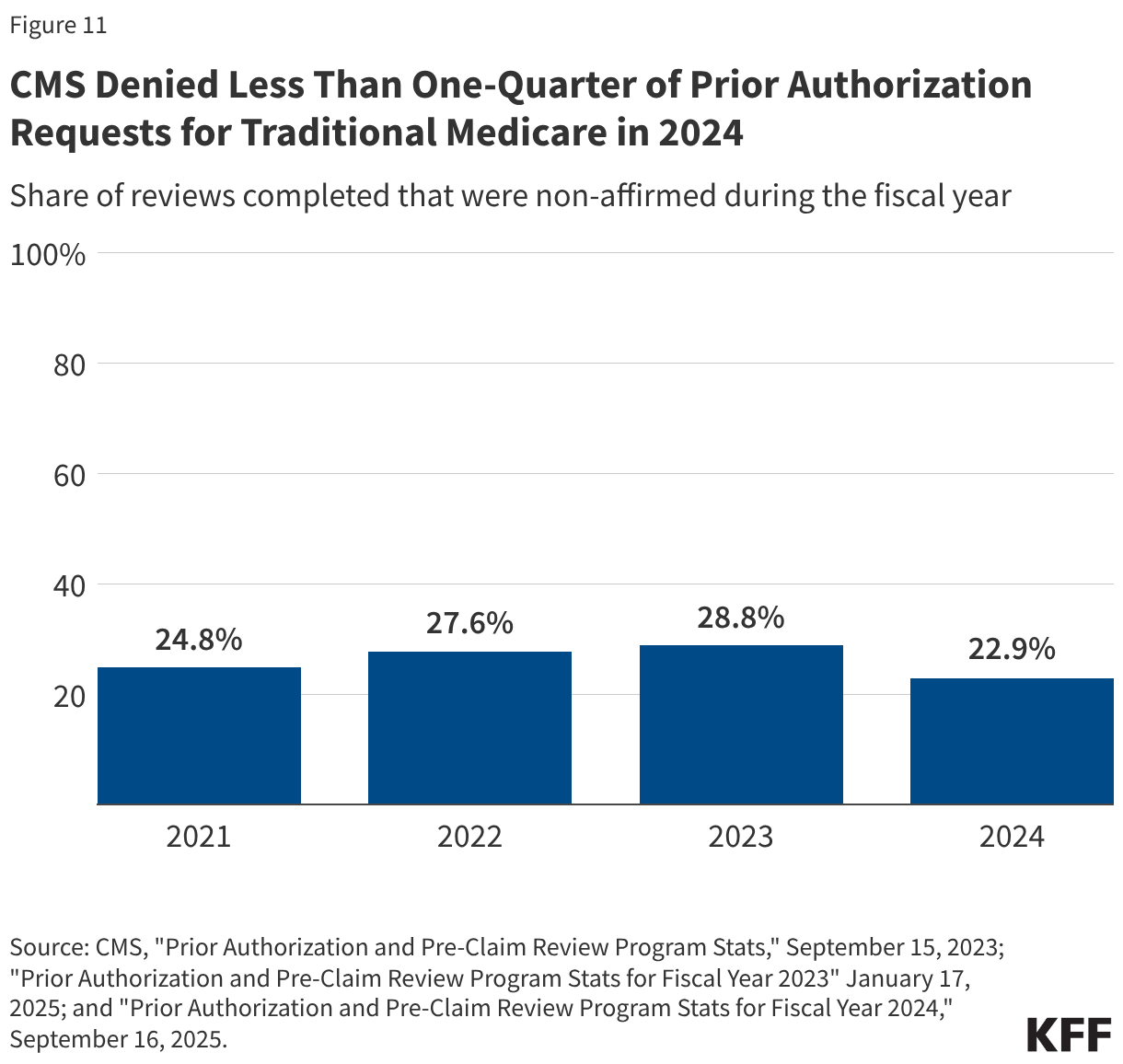
Less than one-quarter of prior authorization requests in traditional Medicare were denied.
CMS approved (or affirmed) the majority of prior authorization requests it reviewed. CMS reported that 24.8% of requests were denied (or non-affirmed) in 2021, 27.6% of requests were denied in 2022, 28.8% of requests were denied in 2023, and 22.9% of requests were denied in 2024 (Figure 11). This reflects 53,680 denied requests in 2021, 72,029 denied requests in 2022, 113,448 denied requests in 2023, and 143,705 denied requests in 2024.
In traditional Medicare, a small share of denied prior authorization requests was appealed to CMS and the share of prior authorization requests that were appealed and overturned upon appeal varied across service type.
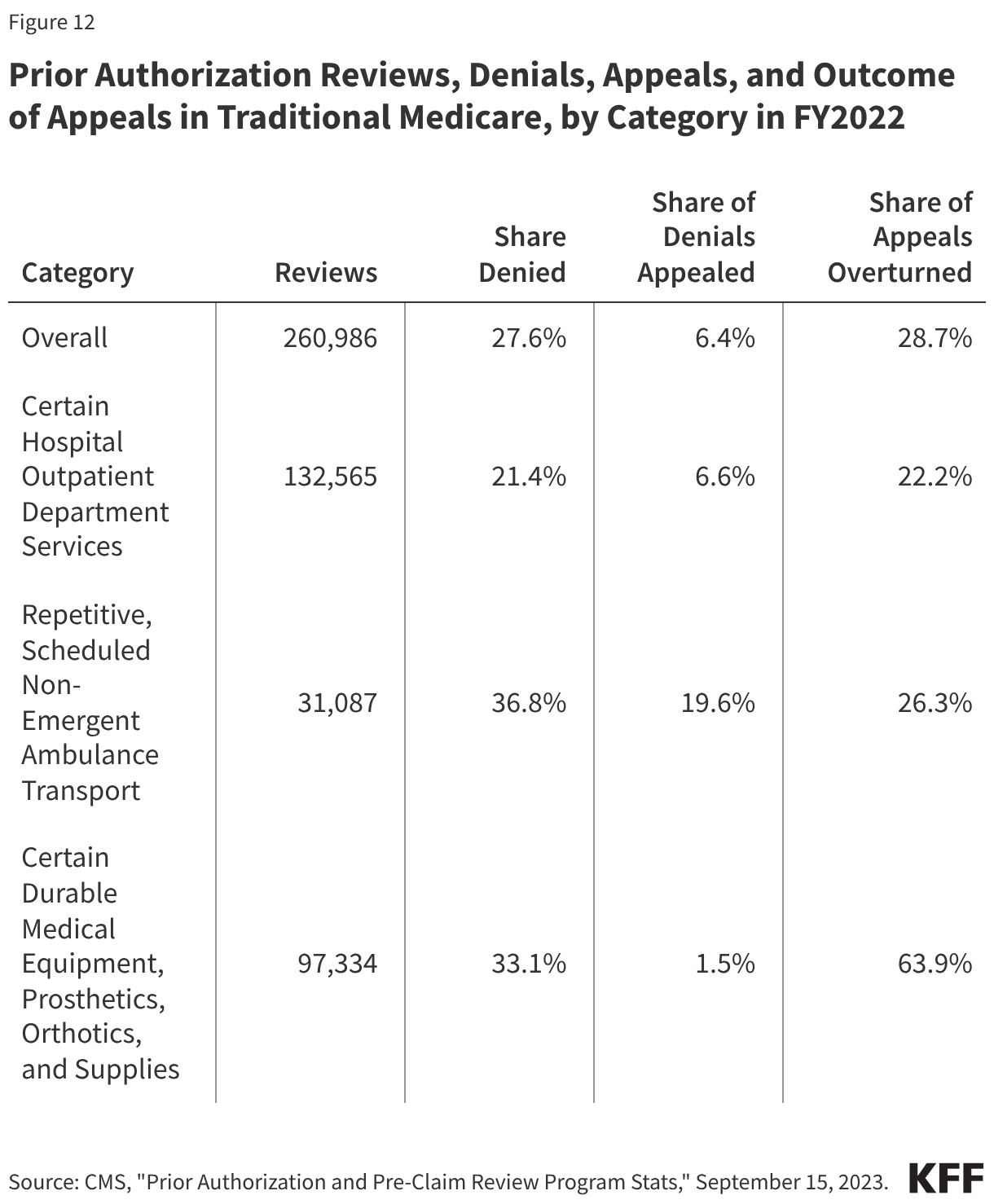
In 2022, fewer than 5,000 denied prior authorization requests in traditional Medicare were appealed to the first level. As a share of all denied requests that translates to 6.4% appealed in 2022. Of the denied requests, 1,323 prior authorization denials were overturned upon appeal, which represents 28.7% of all first level appeals (Figure 12). Appeals data in traditional Medicare are presented differently across the CMS reports. Specifically, the 2023 and 2024 reports include a separate claims and appeals section for each category of service, which appears to include a broader universe of reviews by Medicare Administrative Contractors, including those for payment of services rendered, than what is presented in the report for 2021 and 2022. Given the differences in the data reported, we present appeals and whether the decision was overturned on appeal for 2022 only.
Denied requests for the ambulance transport services were most often appealed (19.6%); just 6.6% of denials for certain hospital outpatient services and 1.5% of certain durable medical equipment, prosthetics, orthotics and supplies requests were appealed.
The share of appeals that resulted in overturning the initial decision also varied widely. Nearly two-thirds (63.9%) of appeals for durable medical equipment, prosthetics, orthotics and other supplies were successful. That compares to 26.3% of appeals for the ambulance transport services and 22.2% of appeals for certain hospital outpatient services.
Box 1: Prior Authorization Requirements in Traditional Medicare
In 2015, CMS issued a final rule that established a prior authorization process for certain Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) items, with the goal of reducing the use of items that had been frequently subject to unnecessary utilization. Initial implementation began March 20, 2017, and items have been added and subtracted to the list over the following years through subsequent rulemaking. As of January 13, 2026, the DMEPOS items prior authorizations list includes over 70 items, including for pressure reducing support surfaces, power mobility devices, and lower limb prosthetics. Additionally, in December 2025, CMS issued a rule which establishes a prior authorization exemption process for certain DMEPOS items, allowing qualifying suppliers, such as those who show an affirmation rate of 90% or higher, to be exempt from prior authorization.
In a 2019 final rule (effective July 1, 2020), CMS established national prior authorization requirements for a set of hospital outpatient department services which had experienced significant increases in utilization and that are likely to be cosmetic procedures and not covered by Medicare, but may be combined with other therapeutic services, including blepharoplasty, botulinum toxin injections, panniculectomy, rhinoplasty, and vein ablation. In further rulemaking (effective July 1, 2021), CMS added implanted spinal neurostimulators and cervical fusion with disc removal to the list of services requiring prior authorization, and another rule (effective July 1, 2023) added facet joint interventions.
On January 1, 2026, the Center for Medicare and Medicaid Innovations (CMMI) launched the Wasteful and Inappropriate Service Reduction (WISeR) Model that establishes new prior authorization requirements in traditional Medicare for select services in six states (New Jersey, Ohio, Oklahoma, Texas, Arizona, and Washington). These services include skin substitutes (synthetic products used in the treatment of severe or chronic wounds), orthopedic pain management services, electrical nerve stimulator implants, incontinence control devices, and services related to the diagnosis and treatment of impotence. According to CMS, the model will test the use of enhanced technologies, such as artificial intelligence, to conduct prior authorization for services vulnerable to fraud or abuse.
Box 2: Recent Administrative Actions and Proposed Legislation on Prior Authorization
The Administration recently finalized three rules related to prior authorization.
The first rule (effective date: June 5, 2023) issued by the Biden Administration clarifies the criteria that may be used by Medicare Advantage plans in establishing prior authorization policies and the duration for which a prior authorization is valid. Specifically, the rule states that prior authorization may only be used to confirm a diagnosis and/or ensure that the requested service is medically necessary and that private insurers must follow the same criteria used by traditional Medicare. That is, Medicare Advantage prior authorization requirements cannot result in coverage that is more restrictive than traditional Medicare. The rule also describes how private insurers may consider additional information when traditional Medicare does not have fully established coverage criteria. The rules apply to coverage beginning with plan year 2024.
The second rule (effective date: April 8, 2024) issued by the Biden Administration is intended to improve the use of electronic prior authorization processes, as well as the timeliness and transparency of decisions, and applies to Medicare Advantage and certain other insurers. Specifically, it shortens the standard time frame for insurers to respond to prior authorization requests from 14 to 7 calendar days starting in January 2026 and standardizes the electronic exchange of information by specifying the prior authorization information that must be included in application programming interfaces starting in January 2027. It also requires that beginning in 2026, insurers post all items and services subject to prior authorization and the share of prior authorization requests that were approved, denied, and approved after appeal. A bipartisan bill has also been introduced to codify pieces of this rule.
The third rule (effective date: June 3, 2024) also issued by the Biden Administration would have required Medicare Advantage plans to evaluate the effect of prior authorization policies on people with certain social risk factors (“health equity analysis”) starting with plan year 2025, but the Trump Administration announced in June 2025 that it would not enforce these requirements.
Additionally, lawmakers in Congress have introduced several bills aimed improving the prior authorization process, including codifying changes made through recent rulemaking, and requiring written clinical criteria for prior authorization requirements, which were both introduced on a bipartisan basis. Other legislation would penalize insurers when initially denied requests are overturned upon appeal too often, require plans to include prior authorization information in plan advertisements, and one proposal would prohibit the use of prior authorization altogether.
Methods
The analysis of Medicare Advantage uses organization determinations and reconsiderations – Part C data from the Centers for Medicare and Medicaid Services (CMS) Part C and D reporting requirements public use file for contract years 2019 – 2021 and the limited data set for contract years 2022 through 2024. Medicare Advantage insurers submit the required data at the contract level to CMS and CMS performs a data validation check.
Data for Medicare Advantage contracts is aggregated to the parent company level. Insurers with less than 1 million enrollees into “other insurers”.
This analysis reflects data on service determinations and does not include claims determinations (for payment for services already provided). We also do not include withdrawn or dismissed determination requests in this analysis.
The enrollment data are from the CMS Medicare Advantage enrollment file for March of each year at the contract-plan-county level. We then sum up to the contract level to merge with the determination and reconsideration data. Contract-plan-county combinations are not included if there are fewer than 11 enrollees. The traditional Medicare analysis uses data included “Prior Authorization and Pre-Claim Review Program Stats,” published by CMS on September 15, 2023, which reflects prior authorization reviews completed in fiscal years 2021 and 2022, “Prior Authorization and Pre-Claim Review Program Stats for Fiscal Year 2023,” published on January 17, 2025, and “Prior Authorization and Pre-Claim Review Program Stats for Fiscal Year 2024,” published on September 16, 2025. The total number of traditional Medicare beneficiaries is from the Medicare Monthly Enrollment Dashboard for 2021 through 2024. While CMS published data on the use of prior authorization in traditional Medicare for FY2023 and FY2024, the information for appeals are not comparable to FY2021 and FY2022 data and are therefore not included in this analysis.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
At the start of 2026, many issues are at play that could affect Medicaid coverage, financing, and access to care. Medicaid, which is administered by states within broad federal rules, provides comprehensive health and long-term care coverage to one in five low-income Americans. A more tenuous fiscal climate in 2026 coupled with implementation of the 2025 reconciliation law will put pressure on state Medicaid programs. While major legislative changes to Medicaid at the federal level are unlikely in 2026, key areas to watch include federal policy actions such as new regulations or guidance related to work requirements, implementation guidance for other components of the 2025 reconciliation law, and states’ policy actions in response to federal policy changes and state budget pressures.
Medicaid issues are likely to intersect with broader health care coverage and affordability debates, including the expiration of the enhanced premium tax credits for Affordable Care Act (ACA) coverage and efforts by the administration to control drug prices and hold insurance companies accountable, leading up to the mid-term elections in November 2026. At the federal level, these elections could affect the make-up of Congress and at the state level, they could affect control of state legislatures and governors’ offices. There will be 39 gubernatorial elections (18 incumbent governors running for reelection and 21 incumbent governors who are either term-limited or not seeking reelection).
Medicaid Coverage
In 2026, states will begin implementing Medicaid policy changes that are estimated to increase the number of people without health insurance by 7.5 million in 2034. Over half (5.3 million) of people newly uninsured from Medicaid changes would come from new work requirements for Medicaid enrollees in the ACA Medicaid expansion group or enrollees in partial expansion waiver programs (Georgia and Wisconsin) starting January 1, 2027. Beyond work requirements, the 2025 reconciliation law made other Medicaid eligibility changes, including pausing implementation of some provisions in two Biden-era eligibility and enrollment rules (that aimed to streamline complex processes), restricting Medicaid eligibility for certain lawfully-present immigrants, and requiring states to conduct more frequent eligibility redeterminations for ACA expansion adults.
States will need to make major policy decisions and systems upgrades, likely in advance of formal federal guidance, to be ready to implement work requirements in January 2027. Operationalizing new Medicaid work requirements will require changes to state eligibility systems and processes, enhanced data sharing infrastructure, and targeted enrollee outreach and education, all of which will demand staff resources and funding that will limit attention to other Medicaid priorities. The short timeline for making these changes means states will need to move forward with key decisions before formal guidance from the Centers for Medicare and Medicaid Services (CMS) may be available, increasing the risk that they will have to make adjustments to align with federal policy, which could increase costs. Despite these challenges, some states have indicated a desire to implement work requirements before the January 2027 deadline. To date, Nebraska is the first to announce it will begin enforcing federal work requirements early, starting May 1, 2026.
Federal immigration policies and state policy choices could have implications for Medicaid coverage in 2026. In addition to federal legislative changes, broader immigration policies, such as changes to the public charge rules, new agreements for CMS to share Medicaid data with Department of Homeland Security (DHS) and Immigration and Customs Enforcement (ICE), and continued public immigration enforcement activity could result in fewer legal immigrants obtaining or maintaining Medicaid coverage. In the face of increasing fiscal pressure, several states have announced they are rolling back state-funded coverage for immigrants who are not eligible for federally-funded Medicaid, which will further limit coverage options for immigrants. States may also adopt other eligibility restrictions in an effort to reduce state costs.
Medicaid Financing
Cuts to federal Medicaid spending will exacerbate the fiscal challenges states are experiencing because of slowing revenue growth and increasing spending demands. The 2025 reconciliation law made historic cuts to federal Medicaid financing, which are estimated to reduce federal Medicaid spending by $911 billion over 10 years. Although the most significant changes to federal Medicaid financing don’t take effect until October 2027 or later, some states will experience more immediate effects resulting from changes to federal requirements governing provider taxes. One of the most immediate effects is that states are prohibited from establishing any new provider taxes or increasing existing taxes. Historically, states have used provider taxes as a means of sustaining Medicaid funding in times of slowing revenue growth or increasing spending demands, but that tool is no longer available because of the new prohibition.
Some states may also face reductions to states’ budgeted revenues for 2026 because of more immediate changes to federal provider tax rules. This would occur in two types of cases:
States that had adopted new provider taxes for state fiscal year (FY) 2026 may not be able to implement those taxes if they had not done so by July 4, 2025, and
States that have implemented provider taxes with a special waiver from CMS known as a “uniformity waiver,” may need to revise their taxes as early as April 1, 2026 because of new limits on the use of such waivers (estimated to affect at least seven states including California, Illinois, Massachusetts, Michigan, Ohio, New York, and West Virginia).
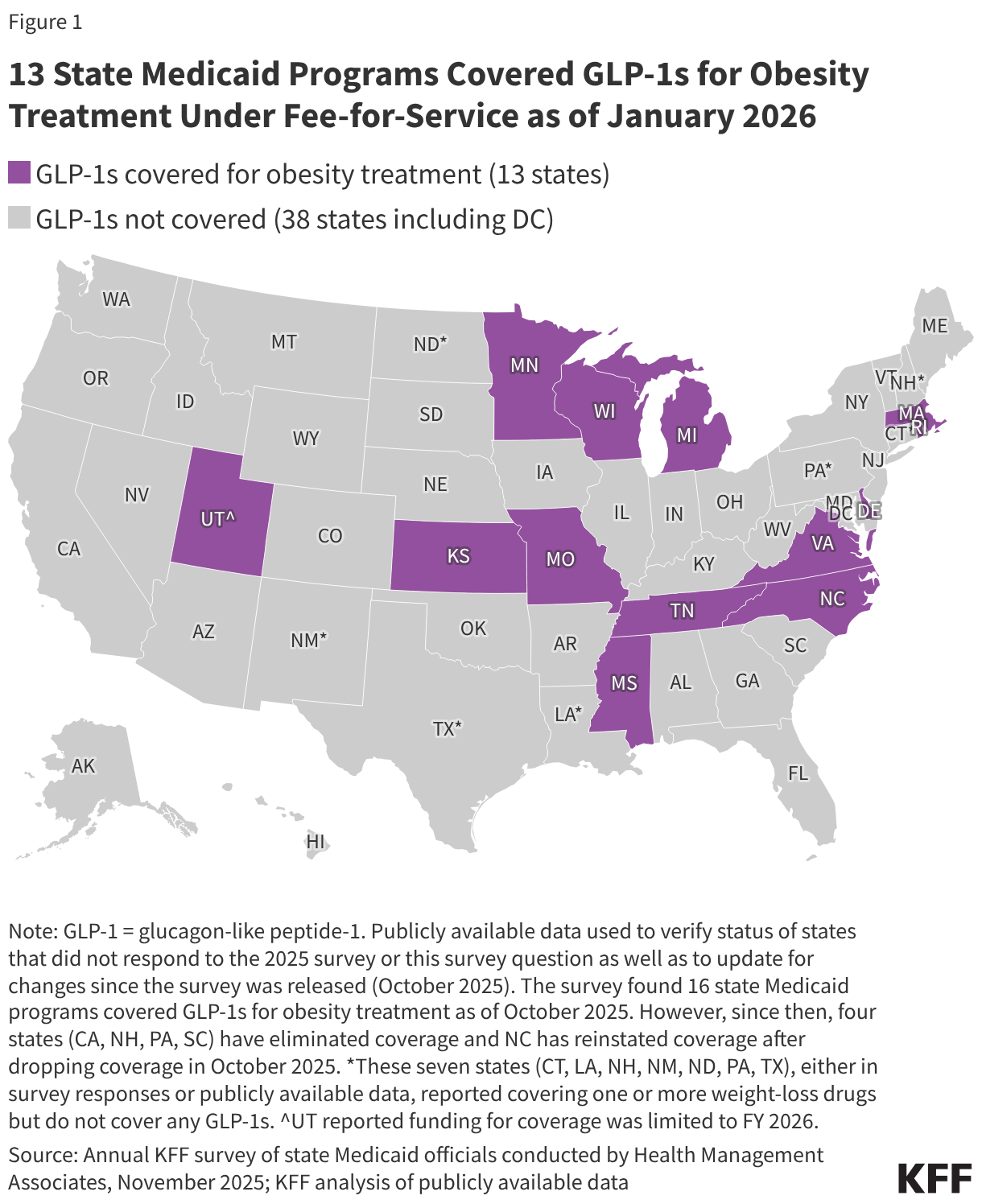
To address slowing revenue growth and increasing spending demands, states may seek to restrict Medicaid provider reimbursement rates, benefits, or eligibility to reduce state Medicaid spending. For example, four states eliminated GLP-1 coverage for obesity treatment in late 2025 likely reflecting recent state budget challenges and fiscal uncertainty. While state Medicaid programs must cover nearly all drugs, a long-standing statutory exception allows states to choose whether to cover weight-loss drugs under Medicaid, resulting in limited state coverage of GLP-1s for obesity treatment. Recent governors’ budgets have included restrictions for other Medicaid benefits including dental and home care. States’ fiscal challenges in 2026 stem from factors other than the 2025 reconciliation law, but the law may exacerbate such challenges. Beyond limiting revenues in states affected by the provider tax provisions, states will need to spend more to implement the law’s requirements, most notably the new work requirements that start January 1, 2027. While the 2025 reconciliation law included some resources to implement policy changes, states may need to make additional investments in systems or workforce to comply with multiple and complex policy changes. Because states pay less than 50% of total Medicaid costs, reductions in state funding will have even larger effects on total Medicaid spending. For example, on average, states accounted for 35% of total Medicaid spending in federal fiscal year 2024. At that rate, a decrease of $100 million in state Medicaid spending would decrease total Medicaid spending by $286 million.
Recent Trump administration prescription drug initiatives could result in savings for state Medicaid programs, though questions remain about the implementation and impact of the deals. In fall 2025, the Trump administration announced reaching agreements with some drug manufacturers, including Pfizer and AstraZeneca, to provide most-favored nation (MFN) prescription drug pricing in Medicaid. MFN prices will be available to state Medicaid programs through the GENEROUS (GENErating cost Reductions fOr U.S. Medicaid) Model, a voluntary drug payment model through which CMS will negotiate supplemental drug rebates based on prices paid in other countries. The Trump administration also recently announced the BALANCE (Better Approaches to Lifestyle and Nutrition for Comprehensive hEalth) Model, another voluntary model that intends to expand access to obesity drugs in Medicaid and Medicare by negotiating lower GLP-1 prices with manufacturers. While lower prices for state Medicaid programs through the recently announced models could result in reduced Medicaid prescription drug spending and potentially expanded coverage of obesity drugs, how the new lower costs under the models compare to the net prices state Medicaid programs currently pay and how states or manufacturers will respond remain unclear. Due to the design of the Medicaid Drug Rebate Program (MDRP), Medicaid programs already typically pay lower prices, net of rebates, than other payers. Further, the recent announcements will not impact costs for Medicaid enrollees as they already pay little or no copays for prescription drugs.
Medicaid Access to Care
State decisions to restrict provider reimbursement rates or benefits in response to federal Medicaid spending cuts could limit access to care for some Medicaid enrollees in 2026. Changes to Medicaid financing will make it difficult for states to increase payment rates to providers and may create pressure for states to restrict payment rates. Reduced or stagnant payment rates to providers coupled with rising costs and increases in the number of people who are uninsured (from Medicaid and Marketplace coverage changes) could pressure providers to reduce staff, services or potentially close. Some providers already struggling financially, such as rural hospitals or hospitals serving a high share of Medicaid enrollees, could face more challenges. An influx of funding from the Rural Health Transformation Program may help to mitigate some challenges in the near term, but those funds are temporary and not expected offset the full magnitude of Medicaid funding cuts over the next ten years. Restricting Medicaid coverage of “optional” services (like behavioral health or home care) could result in less access to care for people with complex health conditions. This may be particularly likely for home care services, where existing tools for managing spending such as caps on total spending or enrollment make it easier for states to limit spending in the future.
The administration may shape Medicaid access through actions to curtail or approve new Section 1115 Medicaid demonstration waivers. Such waivers allow states an avenue to test new approaches in Medicaid if the Department of Health and Human Services (HHS) Secretary determines the waiver is likely to “promote the objectives of the Medicaid program.” Waiver priorities may shift from one presidential administration to another. For example, the Trump administration has rescinded Biden-era 1115 waiver guidance on covering health-related social needs (HRSN) services, indicated plans to phase out certain waiver financing tools (related to use of “Designated State Health Programs” (DSHP), notified states that it does not anticipate approving or extending waivers with continuous eligibility provisions for children and adults or workforce initiatives. While the Trump administration has indicated the phase out or rescission of certain Biden-era waiver policies, the administration has not provided details about its priorities for the use of 1115 waivers. The 2025 reconciliation law included a new provision that requires the Chief Actuary at CMS to certify that 1115 waivers are not expected to result in an increase in federal expenditures compared to federal expenditures without the waiver. While “budget-neutrality” for waivers has been required under long-standing policy and practice, typically the calculations are determined on a per enrollee basis over the course of the waiver and are negotiated between states and the administration.
Workforce challenges tied to reimbursement rate policies and changes in immigration policy could also exacerbate access challenges. KFF survey data finds that 13% of immigrants have avoided going to work since January 2025 because of concerns about drawing attention to someone’s immigration status, a number which rises to 40% among people who are likely to be undocumented immigrants. Such concerns are most significant for the long-term care workforce because Medicaid is the dominant payer for care and more than one in four long-term care workers are immigrants. Beyond long-term care, immigrants constitute a large share of workers in other health care fields, including over one in four physicians in US hospitals.
What to Watch
The issues identified in this policy watch could have major implications for Medicaid coverage, financing, and access to care. Key questions for each of these areas will be important to monitor as debates evolve leading up to the mid-term elections, which will have significant implications for Medicaid and health policy in general in the years ahead.
Medicaid coverage changes:
How will federal guidance shape implementation of work requirements and other eligibility changes in the reconciliation law?
How will states implement Medicaid work requirements? How many states will implement work requirements ahead of the January 2027 deadline? Will any states be granted good faith waivers to delay implementation?
Will states adopt additional eligibility restrictions in budgets for FY 2027?
How will aggregate and state enrollment trends evolve during 2026?
Medicaid financing changes:
How will federal Medicaid financing changes affect state budgets and provider rates in 2026?
How will state financing challenges affect the development of their FY 2027 budgets?
Will states be able to offset reduced federal funding with state funding or will states adopt policies to restrict Medicaid? What policies will states adopt to reduce state Medicaid spending?
Will states be able to sustain recent increases in provider rates or expansions in services, particularly for long-term care and behavioral health?
Medicaid access changes:
How will broader changes in Medicaid coverage affect access to care?
How will changes in Medicaid 1115 waiver policy affect access to care?
Will changes in financing result in hospital or other provider closures and what will that mean for access to care? Will funding for providers from the rural health transformation fund offset restrictions from other federal and state policies?
How will broader immigration policies affect the long-term care workforce and access to services that are predominantly funded by Medicaid?
As states begin budget debates for state fiscal year (FY) 2027, many states are facing a more tenuous fiscal climate. Slowing revenue growth and heightened spending demands coupled with anticipated federal Medicaid cuts under the 2025 reconciliation law, changes to the Affordable Care Act (ACA) enhanced Marketplace subsidies, and economic changes are contributing to tighter budget conditions and fiscal uncertainty for states. Medicaid is often central to state fiscal decisions as it is simultaneously a significant spending item as well as the largest source of federal revenues for states.
States projected Medicaid enrollment to remain flat for FY 2026 in KFF’s 2025 budget survey of Medicaid officials and total Medicaid spending was expected to increase 7.9%, though there was substantial variation across states. States reported a variety of cost pressures including provider and managed care rate increases, greater enrollee health care needs, and increasing costs for long-term care, pharmacy benefits, and behavioral health services. Some states have already implemented Medicaid spending cuts to address recent budget challenges, and others may follow as they contend with budget gaps and prepare for the implementation of the Medicaid changes in the 2025 reconciliation law.
Now in January 2026, halfway through FY 2026, governors are beginning to release proposed budgets for state legislatures to consider for FY 2027. Most states will be adopting FY 2027 budgets this year and another 16 states enacted biennial budgets last year, though some of these states may adopt a supplemental budget for FY 2027. The state budget cycle in most states runs from July to June, and governors typically release their budget proposals early in the calendar year followed by a convening of the legislature to finalize and enact a budget. While most states have not yet released budget proposals, implementation of the 2025 reconciliation law will put pressure on state Medicaid programs and states such as Colorado and Idaho have already announced Medicaid cuts. Medicaid issues are also likely to intersect with broader health care coverage and affordability debates leading up to the mid-term elections in November 2026. There will be 39 gubernatorial elections (18 incumbent governors running for reelection and 21 incumbent governors who are either term-limited or not seeking reelection) and control of state legislative bodies could also be affected. This brief describes current state fiscal conditions as states begin FY 2027 budget debates and highlights key areas to watch for Medicaid policy changes as states respond to fiscal challenges and the 2025 reconciliation law.
State Fiscal Pressures
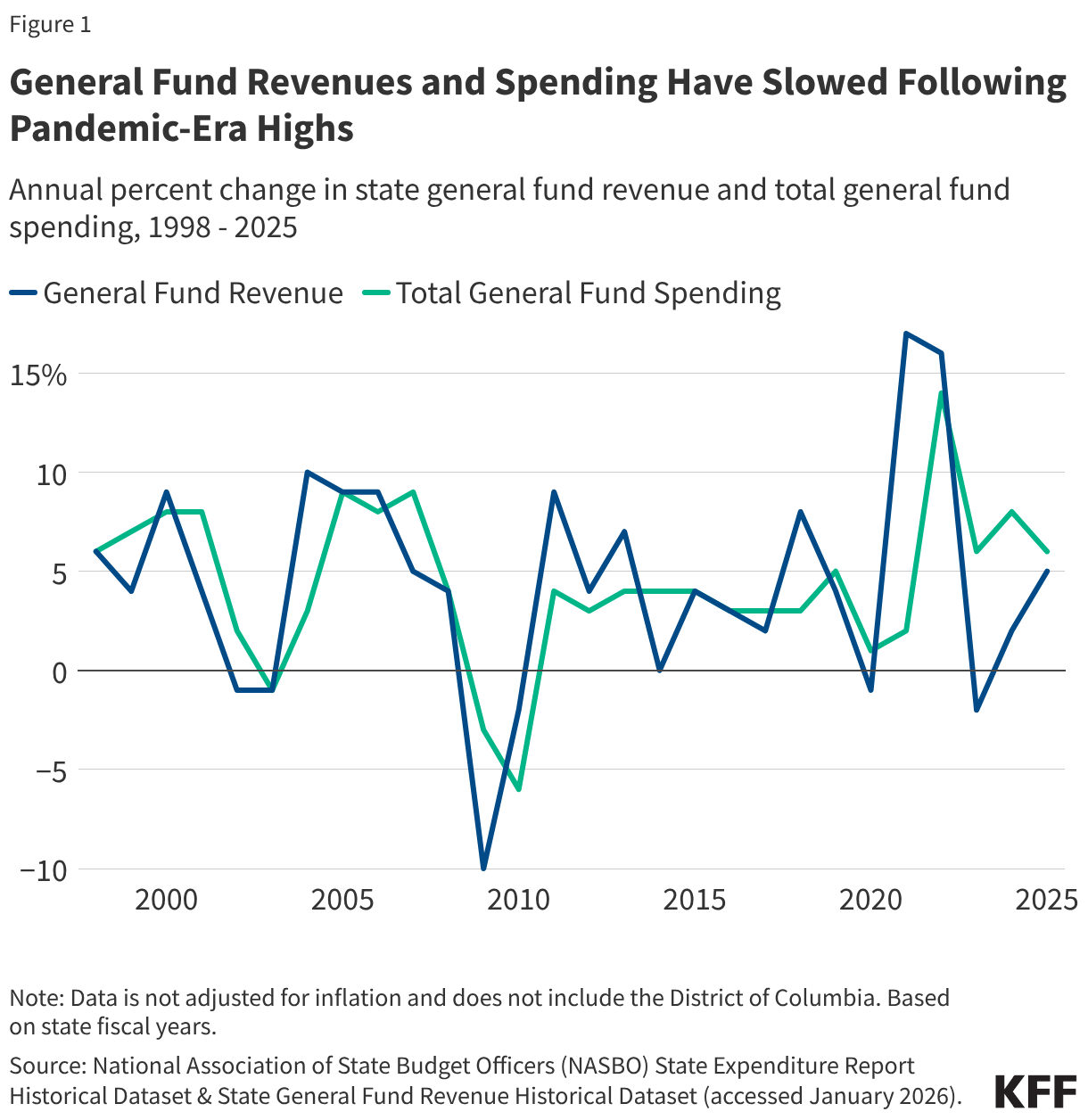
States are facing a more tenuous fiscal climate as they prepare for FY 2027 budget debates. In recent years, tax cuts combined with changes in inflation and consumer consumption patterns has led to slowing state revenue growth following a period of record-breaking revenue and expenditure growth for states after the initial pandemic-induced economic downturn (Figure 1). General fund spending has also slowed, and data show state rainy day fund capacity is also beginning to decline following all-time highs (though funds remain stronger than before the pandemic). States are also contending with increasing spending demands from Medicaid, employee health care, education, housing, and disaster response, though state fiscal conditions vary widely across states. Due to tightening budget conditions, some states have begun implementing more budget management strategies, like spending cuts or other cost containment measures.
Recent federal actions, including the passage of the 2025 reconciliation law, may intensify state budget pressures for FY 2027. States are preparing for significant policy changes and federal funding cuts in the 2025 reconciliation law, including tax code changes as well as Medicaid and SNAP cuts. The new law is expected to reduce federal Medicaid spending by $911 billion (or 14%) over the next decade, though the impact varies by state. States may offset some of the reductions with state funds, though the challenging fiscal climate and the magnitude of federal funding cuts in the new law may make it difficult. For example, states may consider filling in funding gaps created by losses in federal funding for Planned Parenthood or providing state funded coverage for lawfully present immigrants who lose health coverage due to new eligibility restrictions. Some states are also moving to subsidize ACA Marketplace premiums with state funds following the expiration of the enhanced subsidies. The expiration of the enhanced subsidies as well as federal workforcecuts, tariff changes, and shifts in economic conditions contribute to heightened fiscal uncertainty for states. While not expected to offset rural hospitals’ losses under the reconciliation law and funding amounts will vary, states will be receiving additional federal funding through a new rural health fund. Given state budget challenges and fiscal uncertainty, at least 14 states, including Arizona, California, Colorado, Delaware, Maryland, New Mexico, and Rhode Island, have already forecasted budget gaps for FY 2027.
State Medicaid Changes
In response to mounting state budget pressures and the passage of the 2025 reconciliation law, FY 2027 state budget debates may include efforts to reduce Medicaid spending. Even though many provisions of the reconciliation law do not take effect immediately, a few states have already implemented Medicaid spending cuts for FY 2026 and, heading into the FY 2027 budget cycle, states may continue to propose Medicaid policy changes in key areas (Figure 2). This brief includes Medicaid changes from recently announced governors’ budget proposals, though most states have not yet released detailed budget proposals yet. The state budget landscape will likely continue to evolve as revenue forecasts and spending demands become clearer and as more states release their budgets. Given the timing and disparate impact of the reconciliation law across states as well as variation in state fiscal conditions, FY 2027 Medicaid policy changes will vary by state and some Medicaid cuts may not begin until FY 2028 or later.
Figure 2
Provider Rates
States have substantial flexibility to establish Medicaid provider reimbursement methodologies and amounts, especially within a fee-for-service (FFS) delivery system where a state Medicaid agency pays providers or groups of providers directly. Historically, during times of weak state revenue collections, states have typically turned to provider rate restrictions to contain costs. KFF’s 2025 Medicaid budget survey found that adopted FY 2026 budgets included more rate increases than cuts, but there was a notable uptick in states reporting provider rate restrictions compared to previous years. Some notable restrictions in FY 2026 included 4% across the board reductions for all provider types and services in Idaho, and a reversal of 1.6% across the board provider rate increases to address budget shortfalls in Colorado.
State budget pressures and the 2025 reconciliation law may result in additional rate cuts in FY 2027 budgets. While the 2025 reconciliation law did not directly make changes to how states set provider rates, the law imposes new limits on managed care state-directed payments for inpatient hospital and nursing facility services and new restrictions on states’ ability to generate Medicaid provider tax revenue. Some provider tax provisions in the new law have already been implemented, and some states may be anticipating the effect of future provider tax limits that will be phased on over time, which could exacerbate state budget challenges and result in reimbursement rate cuts. Some early FY 2027 governors’ budget proposals include provider rate restrictions: Colorado proposed reducing Medicaid provider rates to 85% of Medicare rates, along with rate reductions for certain home health, dental, behavioral health, and other services, and Idaho proposed extending their 4% provider rate reductions. Texas has also proposed reimbursement rate reductions for FY 2027 for substance use treatment facilities and durable medical equipment. North Carolina has not yet passed their biennial budget for FY 2026 and FY 2027; while this stalemate resulted in rate cuts that were eventually restored in FY 2026, the legislature may consider additional cuts as they finalize their budget.
Benefits
State Medicaid programs must cover a comprehensive set of “mandatory” benefits, including items and services typically excluded from traditional insurance, but may also cover a broad range of optional benefits. For example, all states cover prescription drugs as an optional benefit, and most states cover other optional services such as physical therapy, eyeglasses, and adult dental care. KFF’s 2025 Medicaid budget survey found that benefit expansions continued to far outweighed benefit restrictions and limitations in FY 2026 (consistent with prior survey years), particularly for behavioral health. However, some states had plans to restrict coverage of GLP-1s for obesity treatment, including California, New Hampshire, Pennsylvania, and South Carolina, which all eliminated coverage of GLP-1s for obesity treatment in January 2026, likely reflecting recent state budget challenges and fiscal uncertainty.
As states enter FY 2027 budget debates, it may be challenging to sustain recent benefit expansions and states may face increased pressure to cut or limit optional benefits. While the 2025 reconciliation law does not directly change Medicaid benefits, states may have to cut or limit optional benefits to offset federal funding cuts in the new law or respond to existing budget challenges. Colorado’s recently released governor’s budget proposal for FY 2027 includes capping dental benefits, and Rhode Island’s Medicaid program FY 2027 budget proposal considers ending GLP-1 coverage. Idaho governor’s budget proposal includes suggested cuts to dental, pharmacy, and various medical service benefits.
Home Care
Medicaid pays for almost 70% of all home care spending in the U.S., and most Medicaid home care is provided through optional services, giving states flexibility to manage costs. Most states use various mechanisms to limit home care spending under waiver programs, including caps on enrollment, total spending, and per-participant costs, as well as restrictions on specific services like personal care. Nearly a third of states reported planning to adopt new strategies in FY 2026 to contain home care costs, according to data from KFF’s 2025 survey of officials administering Medicaid home care programs.
State budget challenges and federal funding cuts in the 2025 reconciliation law could result in additional pressure to reduce optional home care services in FY 2027 budgets. The 2025 reconciliation law does not directly change home care benefits, but significant Medicaid spending on home care and the availability of mechanisms for limiting such spending could spur states to make home care cuts. When faced with fiscal pressures in the past, all states reduced spending on home care by either serving fewer people (40 states) and/or by cutting benefits or payment rates for long-term care providers (47 states). Recently released governors’ budget proposals from Colorado and Idaho include suggested cuts to home care services, although specifics of these proposals are not available and may evolve during the legislative process.
Eligibility and Work Requirements
Since the pandemic, many states have expanded Medicaid eligibility or taken steps to remove administrative barriers to enrollment for certain groups. States have also built on post-pandemic unwinding strategies to automate eligibility and renewal processes, improve communication with members, and reduce administrative barriers. However, in FY 2026, some states reduced Medicaid spending through eligibility restrictions, reflecting tighter budget conditions. As of January 2026, California reinstated asset limits for Medi-Cal eligibility for long-term care benefits for adults 65 and older or with a disability, and D.C. reduced Medicaid income limits to 138% of the federal poverty limit for certain enrollees. Some states have also rolled back state-funded health coverage programs that expand coverage to immigrants regardless of status. In addition, KFF’s 2025 Medicaid budget survey found that a few states planned to cancel or postpone one or more projects or initiatives due to uncertainty at the federal level, including federal waiver policy changes such as pre-release coverage for individuals who are incarcerated or continuous enrollment for children.
Upcoming FY 2027 budget debates may consider Medicaid eligibility restrictions to address state budget challenges. States will also begin the implementation of the 2025 reconciliation law’s Medicaid eligibility policy changes, including pausing implementation of some provisions in the Biden-era Eligibility and Enrollment Final Rule (that aimed to streamline complex processes), restricting Medicaid eligibility for certain immigrants, conducting more frequent eligibility redeterminations for ACA expansion adults, and imposing Medicaid work requirements for ACA expansion adults. Operationalizing these new policies will require significant changes to state eligibility systems and processes, which may displace staff, funding, and resources from implementing other Medicaid priorities. Increased costs associated with implementing the changes in addition to state budget pressures and federal funding cuts could mean more states consider restricting coverage of optional eligibility groups. For example, Idaho’s legislature has signaled that it may consider repealing the Medicaid expansion to address budget shortfalls.
The implementation of Medicaid work requirements may have a significant impact on state Medicaid program budgets and systems capacity in FY 2027. The 2025 reconciliation law requires states to implement work requirements for individuals enrolled through the ACA Medicaid expansion pathway or certain state waivers beginning January 1, 2027 (with the option for states to implement requirements earlier). The Congressional Budget Office (CBO) estimates that this requirement will have the largest effect on spending and coverage compared to other provisions, reducing federal Medicaid spending by $326 billion over ten years and resulting in 5.3 million more people who are uninsured. In KFF’s 2025 Medicaid budget survey, states reported a number of implementation challenges including the significant eligibility systems changes needed, the short timeframe, staff capacity concerns, and issues for applicants and enrollees. States also reported fiscal challenges tied to systems changes, hiring additional staff, and conducting outreach to enrollees. Even with implementation funds and federal matching payments for administrative costs, some states cited the increased costs of implementing work requirements on a short timeline as a concern, which may factor into FY 2027 budget debates. For example, among recently released FY 2027 governors’ proposed budgets, Utah includes $16.5 million, Colorado includes over $50 million, Kentucky includes $35.6 million, and Wyoming includes $7.4 million in funding for the new law’s Medicaid eligibility redetermination changes. In addition, some states are planning to move forward with work requirements before the federal deadline, which could have additional implications for state budgets. To date, Nebraska is the first state to announce it will implement early, starting May 1, 2026.
This chart collection explores National Health Expenditure (NHE) data from the Centers for Medicare and Medicaid Services (CMS), including the latest data from 2024. These data offer insights into changes in health spending over time in the U.S., as well as the driving forces behind spending growth. A related interactive tool contains more of the latest NHE data.
The slideshow is part of the Peterson-KFF Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
In anticipation of federal changes to vaccine policy by the Trump administration, last year, some states began to de-couple their own vaccine recommendations from the federal government. This marked a departure from prior practice where, historically, states typically relied on Centers for Disease Control and Prevention (CDC) and its Advisory Committee on Immunization Practices (ACIP) for such recommendations. Starting in May of last year, HHS Secretary Kennedy and the CDC/ACIP began to make changes to the federal vaccine schedule for children, culminating in an announcement on January 5 of this year with the most wide-ranging changes to date (see Table 1). Collectively, these changes have resulted in reducing the number of diseases targeted from 17 to 11 and the number of routine vaccines from 13 to 7. As part of these changes, six vaccines are no longer recommended for routine use by all children in the United States.
This policy brief tracks the number of states that have announced they are no longer following federal government recommendations for childhood vaccines as of January 20, 2026, updating an analysis from September of last year (while the current analysis focuses on state sources for childhood vaccine recommendations, our earlier analysis also looked at state actions regarding insurance coverage requirements and pharmacist administration). Overall, the number of states that have taken such an action has increased significantly since last September, with a majority of states (28) now departing from federal guidelines for some or all childhood vaccines compared to 22 states in September of last year (see Table 2). Moreover, the number of states decoupling their vaccine recommendations for all childhood vaccines has risen from just nine in September to 25. The red-blue divide across the country continues to grow, with all blue states1 (those with Democratic governors) having announced that they will no longer follow federal guidelines, though four states with Republican governors have also done so.
Findings
As of January 20, 2026, the majority of states (28 states, including DC) have announced that they will not follow the new CDC childhood vaccine recommendations for at least some childhood vaccines, instead relying on prior recommendations, state recommendations, and/or those of external entities. Most of these states have indicated that they will follow the recommendations of the independent medical association, the American Academy of Pediatrics (AAP). Among these are two inter-state public health alliances which previously formed to develop shared recommendations and have reaffirmed their intent to follow AAP guidelines: the West Coast Health Alliance, which includes California, Hawaii, Oregon, and Washington, and the Northeast Public Health Collaborative, which includes ten states and New York City.
Almost all of these states (25 of 28) have announced that they will do so for all childhood vaccines. Most of these states are choosing to follow non-federal guidelines for all childhood vaccines. The three states that are more limited are Alaska and Mississippi, which announced that they would continue to recommend the Hepatitis B vaccine at birth for all infants, even those whose mothers test negative (no longer recommended as routine by the CDC), and Arizona, which has announced that it will continue to recommend Hepatitis B at birth and COVID-19 vaccines consistent with guidelines from external entities.
This marks a significant increase since September when only nine states had announced that they would not follow CDC/ACIP vaccine recommendations for all childhood vaccines (some also did so for adults). In September, most states that had announced changes did so for COVID-19 only (13), which at that time, was the only vaccine for which changes had been made by the federal government (removing the routine vaccination recommendation generally, including for children). With the changing recommendation regarding Hepatitis B vaccine in December of 2025 and additional vaccines in early January 2026, many more states have expanded this scope to include all childhood vaccines.
The red-blue divide in vaccine policy continues with all blue states (those with Democratic governors) departing from federal guidelines. As in September, there is a significant political divide in vaccine policies across the country, which is even sharper today. While all blue states have departed from federal recommendations (one exception is Virginia which just swore in a new Democratic Governor this week and may choose to change their position regarding vaccine recommendations soon), four states with Republican governors have also done so for at least some childhood vaccines (Alaska, Mississippi, New Hampshire, and Vermont). This divide in state policy mirrors a growing divide in public opinion).
Looking ahead, it is possible other states will join this group and de-couple their own childhood vaccine recommendations from the federal government. Regardless of future state decisions, the current landscape – with diverging recommendations from the federal government, many states, and physician organizations — represents a challenging one for parents and providers to navigate, which could dampen already falling vaccination rates. Moreover, much of this divide is likely to play out in the next school season, when states have to decide whether and how to translate their vaccine recommendations into school attendance requirements or revise existing exemption allowances.
Table 1: Trump Administration Changes to Childhood Vaccine Recommendations
Table 2: State Childhood Vaccine Recommendations: Reliance on Non-Federal Sources
State
Party of Governor
Relies on non-Federal Source for Routine Childhood Vaccine Recommendations
As of September 22, 2025 All Vaccines: 9 States COVID-19 only: 13 States
As of January 20, 2026 All Vaccines: 25 States COVID-19/Hepatitis B: 1 State Hepatitis B only: 2 States
Alabama
R
Alaska
R
Hepatitis B
Arizona
D
COVID-19 Only
COVID-19/Hepatitis B
Arkansas
R
California
D
All Vaccines
All Vaccines
Colorado
D
All Vaccines
Connecticut
D
COVID-19 Only
All Vaccines
Delaware
D
COVID-19 Only
All Vaccines
District of Columbia
D
All Vaccines
All Vaccines
Florida
R
Georgia
R
Hawaii
D
All Vaccines
All Vaccines
Idaho
R
Illinois
D
All Vaccines
All Vaccines
Indiana
R
Iowa
R
Kansas
D
All Vaccines
Kentucky
D
All Vaccines
Louisiana
R
Maine
D
COVID-19 Only
All Vaccines
Maryland
D
All Vaccines
All Vaccines
Massachusetts
D
All Vaccines
All Vaccines
Michigan
D
COVID-19 Only
All Vaccines
Minnesota
D
COVID-19 Only
All Vaccines
Mississippi
R
Hepatitis B
Missouri*
R
Montana
R
Nebraska
R
Nevada*
R
New Hampshire
R
All Vaccines
New Jersey
D
COVID-19 Only
All Vaccines
New Mexico
D
COVID-19 Only
All Vaccines
New York
D
COVID-19 Only
All Vaccines
North Carolina
D
COVID-19 Only
All Vaccines
North Dakota
R
Ohio
R
Oklahoma
R
Oregon
D
All Vaccines
All Vaccines
Pennsylvania
D
All Vaccines
All Vaccines
Rhode Island
D
COVID-19 Only
All Vaccines
South Carolina
R
South Dakota
R
Tennessee
R
Texas
R
Utah
R
Vermont
R
COVID-19 Only
All Vaccines
Virginia**
D
Washington
D
All Vaccines
All Vaccines
West Virginia
R
Wisconsin
D
COVID-19 Only
All Vaccines
Wyoming
R
Notes: *While news reports for Missouri and Nevada indicate that these states do not anticipate making changes to their vaccine recommendations, despite CDC changes, these were not attributed to specific officials or other documentation and were therefore not included here. **As of January 17, 2026, Virginia’s governor is now a Democrat, the state may choose to change its position regarding vaccine recommendations soon.
One exception is Virginia, which just swore in a new Democratic Governor on January 17th and may choose to change their position regarding vaccine recommendations soon. ↩︎
New features from AI companies, like ChatGPT Health and Claude for Healthcare, aim to provide personalized health guidance as OpenAI reports more than 40 million daily users seek health information from its chatbot, but concerns remain about AI providing wrong or dangerous health advice, particularly around mental health.
And as the U.S. experiences its highest flu levels in 25 years, a vaccine-strain mismatch may be contributing to claims that flu vaccines are ineffective, despite evidence that vaccines still reduce severe illness and death and protect against other circulating strains.
AI & Emerging Technology
AI Companies Launch Health Products as Millions Seek Medical Advice From AI
KFF/ Getty Images
What’s happening?
Two artificial intelligence (AI) companies announced new health-related features this month, with “ChatGPT Health” and “Claude for Healthcare” both allowing users to connect their medical records and wellness apps to the chatbots for personalized health guidance. The companies say the features are not intended to be used for diagnosis or treatment, but rather aim to help users navigate everyday health questions by grounding responses in users’ own health data.
The new tools come as OpenAI reports that more than 40 million people globally turn to ChatGPT daily for health information, with users asking 1.6 to 1.9 million health insurance questions per week about comparing plans, handling claims, billing, and coverage. According to a report from OpenAI which draws from anonymized conversations and a survey of ChatGPT users, Americans are using ChatGPT to decode medical bills, appeal insurance denials, and at times self-diagnose or manage their care. More than 5% of all ChatGPT messages globally are about health care, according to OpenAI’s report. KFF will continue to monitor how the public reports using AI tools for health information.
Why this matters
ChatGPT and other generative AI models can give wrong and potentially dangerous advice, particularly in conversations about mental health. OpenAI faces multiple lawsuits from people who say loved ones harmed or killed themselves after interacting with the tool, and several states have passed laws banning chatbots from providing mental health and therapeutic decision making.
KFF polling has shown that only about one in three adults (32%) say they would trust an online health tool that uses AI to access their medical records to provide personalized health information. Despite this low level of trust, the use of AI chatbots for health questions and the expansion into more personalized health features by leading AI companies suggests that the convenience offered by these tools may outweigh concerns about accuracy and safety, or that some users may not be aware of gaps in these areas. Health communicators and providers should be aware of how patients are using these tools and provide guidance on their appropriate use.
Social Media and AI Policy Roundup
Study Shows Team-Based Content Moderation Improves Consensus
A common challenge in content moderation of incorrect or harmful information is people do not agree on what is true. A December study from the Annenberg School for Communication found that content moderators working in teams reached higher levels of agreement on controversial content moderation decisions compared to working alone. The experiment involved over 600 politically diverse moderators and found that “structured social interaction” strengthened accuracy and agreement in content moderation decisions. The findings come as some major platforms have scaled back content moderation efforts to prioritize free speech and diverse thinking, with Meta ending its third-party fact-checking program in 2025 and X reducing its trust and safety teams. Even before these changes, a 2023 KFF poll found that most adults (69%) said social media companies were not doing enough to limit the spread of false and inaccurate health information.
Visa Restrictions Target Content Moderators and Fact-Checkers
A December directive from the State Department instructed immigration officers to deny H-1B visas to individuals who worked in fact-checking, content moderation, trust and safety, or other activities the administration considers censorship of Americans’ speech. In response, the International Fact-Checking Network issued a statement calling the policy a misunderstanding of fact-checking, arguing that the practice strengthens public debate rather than censoring it. Imran Ahmed, the CEO of the Center for Countering Digital Hate, was among European figures barred from receiving a visa and has sued the Trump administration, claiming the denial is “punishment” for his organization’s work combatting misinformation.
Grok’s Explicit Images Highlight Legal Ambiguities in AI Liability
Reports indicate that X’s Grok chatbot is being used to create AI-generated nonconsensual intimate imagery (NCII) of women and children, which can harm victims’ mental health through depression, anxiety, PTSD, and suicidal ideation. X has since announced that it would restrict Grok from generating explicit images of real people in jurisdictions where such content is illegal, but these reports have raised questions about who is liable when AI causes documented psychological harm. International regulators have warned of investigations and other actions, and lawmakers in the U.S. have expressed concern. Legal observers have characterized the AI-generated images as a testing ground for whether Section 230 of the Communications Decency Act, which provides legal immunity to online platforms for user-generated content, extends to harmful or illegal AI-generated content. Legal efforts to regulate AI have largely stalled in the U.S., but a bill signed into law last year criminalizes sharing NCII, including AI-generated images, and requires platforms to remove them.
Recent Developments
Flu Vaccine Misconceptions Spread During One of the Worst Flu Seasons in Decades
Lauren Bishop / CDC
What’s happening?
Misleading claims that flu vaccines are ineffective or weaken the immune system have circulated during the ongoing respiratory virus season, which has seen the highest flu levels in 25 years. The surge in cases is largely driven by a new mutation of the virus, called subclade K, that emerged after the season’s vaccine formulation was finalized in March. Each year, scientists predict what strains to include in the coming season’s flu vaccine, but subclade K only became the dominant strain after those decisions were made, creating a mismatch between the vaccine and the circulating virus.
Where confusion about flu vaccines is emerging
The vaccine-strain mismatch may be contributing to claims that the vaccine is ineffective. Senator Rand Paul, for example, questioned the vaccine’s effectiveness on a podcast in mid-January, specifically citing the strain mismatch and suggesting that claims about crossover protection are “inflated.” While this season’s vaccine was not specifically designed to target subclade K, evidence from prior influenza seasons shows that flu vaccines can still provide some protection from infection when they are mismatched to the dominant circulating strain. Vaccination also helps to protect against severe outcomes, including hospitalization and death.
Statements by health officials may also contribute to concern over the safety of the flu vaccine. For example, a video clip of Health and Human Services (HHS) Secretary Robert F. Kennedy Jr. appearing on a podcast in 2020 has been shared widely online recently. In the clip, Kennedy says he would not take a flu shot “in a million years” and claims that the vaccine can make people susceptible to other infections. Other HHS officials have claimed that randomized controlled trials do not show that the flu vaccine protects against influenza, but fact-checkers note that flu vaccines are designed primarily to reduce the risk of hospitalization and death. Although clinical trials are typically too small to reliably measure these relatively rare outcomes, meta-analyses have demonstrated that flu vaccines reduce these risks.
Others have claimed that the flu vaccine increases the risk of being infected with flu. While flu vaccines can cause some side effects that may resemble flu-like illness, they contain inactivated or attenuated versions of the virus that cannot cause flu infection, and vaccination is not associated with higher rates of other, non-influenza infections. Because flu vaccines do not fully protect against infection and multiple strains can circulate in the same season, vaccinated individuals can still become infected with influenza, but this does not mean the vaccine caused the infection.
Conflicting guidance may contribute to further confusion
Guidelines published by the Centers for Disease Control and Prevention (CDC) in August 2025 recommended that everyone aged six months or older receive routine annual influenza immunization. However, as part of broader changes to federal vaccine policy, HHS issued a memo in January reducing the number of vaccines recommended for all children and moving six vaccines, including influenza, from routine recommendations to “shared clinical decision making,” a process where health care providers and parents decide individually whether vaccination is appropriate.
Physician organizations, including the American Medical Association (AMA) and American Academy of Pediatrics (AAP), have criticized the changes and reaffirmed their support for routine childhood vaccinations, including flu vaccines. KFF polling has shown that larger shares of the public trust their own health care providers and physician associations like the AMA and AAP than the CDC for reliable vaccine information.
Why this matters
The misleading narratives about flu vaccines and the shifting federal guidance come as flu vaccination rates have already declined from pre-pandemic levels to around 43% for both adults and children. Older adults, pregnant people, and people with underlying health conditions face the highest risk of severe illness, hospitalization, or death from influenza. While these groups typically have higher flu vaccination rates than the general public, the ongoing severe season and the vaccine-strain mismatch may create an environment that allows misleading claims about the flu vaccine to spread, potentially impacting vaccine uptake and hesitancy among these vulnerable groups.
For children, the federal government’s decision to move pediatric flu vaccines to the shared clinical decision making category could introduce additional barriers to vaccine access and potentially result in lower vaccination rates. The move comes as smaller shares of parents view flu vaccination as important. The KFF/Washington Post Survey of Parents found that while about nine in ten parents view routine immunizations for measles, mumps, and rubella (MMR) and polio as important for children in their community to get, a much smaller share (56%) said the same for the flu vaccine. Similarly, while at least eight in ten parents express confidence in the safety of MMR and polio vaccines for children, smaller shares (65%) say they are confident the flu vaccines are safe for children. HHS framed the decision as part of an effort to restore trust, but it remains unclear what effect the changes will have. KFF will continue to monitor how changing federal guidance impacts trust in vaccines and public health efforts.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.
The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The data shared in the Monitor is sourced through media monitoring research conducted by KFF.
Quiz: Test Your Knowledge of the Affordable Care Act
The Affordable Care Act (ACA) affects virtually all aspects of the U.S. health system, including insurers, providers, state governments, employers, taxpayers, and consumers. The ACA introduced regulated health insurance exchange markets, or Marketplaces, which offer financial assistance for ACA-compliant coverage to those without traditional insurance sources.
Take this ten-question quiz to see how much you know about how the ACA affects health insurance coverage and costs as well as who is eligible for financial assistance.
GLP-1 (glucagon-like peptide-1) drugs were originally developed to help people with type 2 diabetes manage blood sugar levels but have gained widespread attention for their effectiveness as a treatment for obesity. Due to their cost, however, coverage of GLP-1s for obesity treatment in Medicaid, ACA Marketplace plans, and most large employer firms remains limited, and GLP-1 coverage in Medicare for treatment of obesity is prohibited under current law. While state Medicaid programs must cover nearly all Food and Drug Administration (FDA) approved drugs, a long-standing statutory exception allows states to choose whether to cover weight-loss drugs under Medicaid. As a result, Medicaid coverage of GLP-1 drugs for obesity treatment is optional for states, while coverage for other indications (diabetes, cardiovascular disease, and sleep apnea) is required.
The upfront costs of GLP-1s are an ongoing concern for both public and private payers, and some employers and state Medicaid programs are now restricting coverage, despite recognizing their effectiveness at treating obesity. Expanded obesity drug coverage can increase Medicaid spending and put pressure on overall state budgets, and states are now facing tighter budget conditions and longer-term fiscal uncertainty, due in part to the federal Medicaid cuts in the 2025 reconciliation law, causing state Medicaid programs to re-evaluate their obesity drug coverage. However, almost four in ten adults and a quarter of children with Medicaid have obesity, meaning expanding Medicaid coverage of these drugs could provide access to effective obesity treatments for millions. In the longer term, reduced obesity rates among Medicaid enrollees could also result in reduced Medicaid spending on chronic diseases associated with obesity, though the evidence is mixed. Any savings on health spending because of obesity drugs may take many years and may not accrue to the Medicaid program if individuals experience shifts in coverage, so states may not be factoring long-term savings into coverage decisions.
At the federal level, the Trump administration decided not to proceed with a Biden administration proposal to allow Medicare and require Medicaid to cover obesity drugs but recently launched their own obesity drug coverage initiatives to reduce costs and increase access (see Box 1). While lower prices for state Medicaid programs could help alleviate cost concerns for states and result in expanded coverage of obesity drugs, how the new lower costs compare to the net prices state Medicaid programs currently pay and how states will respond amid tightening budget conditions remain unclear. Further, the recent announcements will not impact costs for Medicaid enrollees as they already pay little or no copays for prescription drugs, and the costs of purchasing drugs directly from manufacturers through TrumpRx will likely still be prohibitive for people on Medicaid who must have a low income to qualify for the program. Unless Medicaid covers obesity medications, enrollees are unlikely to have access to them given the high out-of-pocket cost even at lower prices.
This brief discusses the current landscape of Medicaid GLP-1 coverage and examines recent trends in Medicaid prescriptions and gross spending on GLP-1s. Key takeaways include:
Obesity drug coverage in Medicaid remains limited, with 13 state Medicaid programs covering GLP-1s for obesity treatment under fee-for-service (FFS) as of January 2026.
The number of Medicaid prescriptions and gross spending on GLP-1s have both increased substantially since 2019.
Increased utilization of Ozempic and Wegovy (semaglutide) as well as Mounjaro and Zepbound (tirzepatide) have contributed substantially to recent growth.
Box 1: Recent Trump Administration Obesity Drug Initiatives
In November 2025, the Trump administration announced reaching a deal with Eli Lilly and Novo Nordisk to lower the cost of their GLP-1s for Medicare, Medicaid, and those purchasing the drugs directly from the manufacturers through a new TrumpRx website. In December 2025, the administration also introduced the BALANCE (Better Approaches to Lifestyle and Nutrition for Comprehensive hEalth) model, a five year CMS Innovation Center (CMMI) model that intends to expand access to obesity drugs in Medicaid and Medicare by negotiating lower GLP-1 prices with manufacturers. The new model will include standardized coverage criteria as well as lifestyle supports and is voluntary for state Medicaid programs, Medicare Part D plans, and manufacturers. State Medicaid programs and manufacturers were requested to submit their intentions to participate by January 8, 2026, and the model is expected to begin in May 2026. For Medicare Part D, this model will be implemented in January 2027, following a separate short-term demonstration that will allow Medicare Part D enrollees to access obesity drugs beginning in July 2026.
Does Medicaid cover GLP-1s for obesity treatment?
States can decide whether to cover obesity drugs under Medicaid. Under the Medicaid Drug Rebate Program, Medicaid programs must cover nearly all of a participating manufacturer’s FDA-approved drugs for medically accepted indications. However, weight-loss drugs are included in a small group of drugs that can be excluded from coverage1 (though the statutory exception refers to agents used for “weight loss”, “obesity drugs” is used to refer to this group of medications in this analysis). As a result, coverage of GLP-1 drugs for the treatment of obesity remains optional for states, while coverage is required for drugs approved for the treatment of diabetes and, since March 2024 and December 2024, for the treatment of cardiovascular disease (Wegovy) and moderate to severe obstructive sleep apnea in adults with obesity (Zepbound), respectively (Table 1). Coverage is also required if deemed medically necessary for children under Medicaid’s Early and Periodic Screening, Diagnostic and Treatment (EPSDT) benefit.
Obesity drug coverage in Medicaid remains limited, with 13 state Medicaid programs covering GLP-1s for obesity treatment under FFS as of January 2026 (Figure 1). When covered, GLP-1s are typically subject to utilization controls such as prior authorization, which can further limit access. Notably, KFF’s 2025 Medicaid budget survey found 16 state Medicaid programs covered GLP-1s for obesity treatment as of October 2025; however, since then, four states (California, New Hampshire, Pennsylvania, and South Carolina) have eliminated coverage of GLP-1s for obesity treatment, likely reflecting recent state budget challenges and the significant costs associated with coverage. North Carolina eliminated GLP-1 coverage beginning October 2025 due to a budget stalemate in the legislature, but coverage was reinstated in December 2025, bringing the total number of states covering GLP-1s for obesity to 13 as of January 2026. A few other states are planning or considering obesity drug restrictions in state fiscal year 2026 or 2027, and state interest in expanding coverage of obesity drugs is also waning according to this year’s survey, with states continuing to report cost as the key factor contributing to obesity drug coverage decisions. The state obesity drug coverage landscape will continue to evolve as states respond to the recent announcement of the BALANCE model (see Box 1) and as states contend with budget challenges and the federal Medicaid spending cuts in the 2025 reconciliation law.
How have Medicaid prescriptions and gross spending on GLP-1s changed in recent years?
The number of Medicaid prescriptions and gross spending on GLP-1s have increased substantially since 2019 (Figure 2). Not all GLP-1s are approved for obesity treatment, and this analysis includes all FDA-approved GLP-1s, including those approved for obesity (Saxenda, Weogvy, Zepbound) as well as those approved for type 2 diabetes (see Table 1). Overall, the number of GLP-1 prescriptions increased sevenfold, from about 1 million in 2019 to over 8 million in 2024. At the same time, gross spending increased ninefold, from about $1 billion in 2019 to almost $9 billion in 2024, and gross spending per GLP-1 prescription reached $1,000 in 2024. Preliminary trends through June 2025 (data not shown) show rapid growth will continue in 2025. Those prices and spending numbers do not account for rebates, and states typically receive substantial rebates on brand drugs. In response to growing criticism of the cost of their drugs, Novo Nordisk, the company that manufactures Ozempic and Wegovy, reported last year that rebates and other fees (across all payers) accounted for about 40% of the cost of the two drugs and that they expected rebates to grow. GLP-1s still account for a relatively small share of the total number of Medicaid prescriptions, accounting for about 1% of all Medicaid prescriptions in 2024 (up from about 0% in 2019). However, GLP-1s accounted for over 8% of all Medicaid prescription drug spending before rebates in 2024 (up from 1% in 2019).
Specifically, increased utilization of Ozempic and Wegovy (semaglutide) as well as Mounjaro and Zepbound (tirzepatide) have contributed substantially to recent growth. Prescriptions and spending on Ozempic, approved for type 2 diabetes (not obesity) in 2017, have grown considerably over the period. By 2024, Ozempic had surpassed Trulicity, also approved for type 2 diabetes (not obesity) to make up the largest share of GLP-1 prescriptions and spending (39% in 2024). Looking from 2023 to 2024, the latest year of data available, prescriptions and gross spending for Wegovy (first approved for obesity in 2021, approved for cardiovascular disease in 2024) and Mounjaro (approved for type 2 diabetes in 2022) more than doubled, and prescriptions and gross spending for Zepbound (first approved for obesity in 2023, approved for sleep apnea in 2024) increased more than fivefold. These drugs are produced by Novo Nordisk and Eli Lilly, which both recently announced agreements with the Trump administration to lower prices. From Medicaid data publicly available, there is no way yet to disentangle how much of the growing use of GLP-1s is related to treatment for diabetes, cardiovascular disease, or sleep apnea versus obesity, or a combination.
Methods
Number of Prescriptions and Gross Spending Data: This analysis uses 2019 through 2024 State Drug Utilization Data (SDUD) (downloaded in January 2026). The SDUD is publicly available data provided as part of the Medicaid Drug Rebate Program (MDRP), and provides information on the number of prescriptions, Medicaid spending before rebates, and cost-sharing for rebate-eligible Medicaid outpatient drugs by NDC, quarter, managed care or fee-for-service, and state. It also provides this data summarized for the whole country. The data do not include information on the number of days supplied in each prescription. CMS has suppressed SDUD cells with fewer than 11 prescriptions, citing the Federal Privacy Act and the HIPAA Privacy Rule. This analysis used the national totals data because less data is suppressed at the national versus state level.
Identifying GLP-1s: This analysis includes all Medicaid prescriptions and gross spending for any FDA-approved GLP-1s. KFF links each drug’s NDC in the dataset to a drug class using the World Health Organization’s (WHO) Anatomical Therapeutic Chemical (ATC) classification system. GLP-1s are then identified as those classified under “A10BJ” or glucagon-like peptide-1 (GLP-1) analogues. The analysis also includes tirzepatide (Mounjaro and Zepbound), which is a dual glucose-dependent insulinotropic polypeptide (GIP) and GLP-1 agonist (and classified under “A10BX” or other blood glucose lowering drugs, excl. insulins). This method results in the inclusion of Medicaid prescriptions and gross spending for: Ozempic, Rybelsus, Mounjaro, Victoza, Trulicity, Wegovy, Zepbound, Saxenda, and generic liraglutide as well as a small number of prescriptions and spending for Adlyxin, Byetta, Bydureon BCise, and Tanzeum (now discontinued).
Limitations: There are a few limitations to the estimates of Medicaid prescriptions and gross spending found in this analysis, including:
This analysis examines the number of Medicaid prescriptions in the data and does not adjust for days supplied by each prescription.
Gross spending and spending per prescription numbers do not account for rebates.
The SDUD are updated quarterly; a new quarter of data is typically released, and the prior five years of data are also updated. This means utilization and gross spending totals can vary depending on when the data is downloaded, and totals may not match other outside sources or prior KFF analysis for this reason.
Drugs that may be excluded from coverage under the MDRP include drugs used for: a) anorexia, weight loss, or weight gain, b) promoting fertility, c) cosmetic purposes or hair growth, d) symptomatic relief of cough and colds, e) prescription vitamins and mineral products except prenatal vitamins and fluoride preparations , f) nonprescription drugs, g) a manufacturer’s covered outpatient drug in which tests and monitoring services have to be purchased from that manufacturer, h) sexual or erectile dysfunction unless used to treat a condition. For more information see, 42 U.S.C. § 1396r-8. ↩︎