Note: Originally published in Jan. 2017, this resource is updated as needed, most recently on Feb. 12, 2025, to reflect the latest developments.
Key Points
- On January 24, 2025, President Trump reinstated the Mexico City Policy, marking the resumption of the expansion of the policy from his first term.
- First announced in 1984 by the Reagan administration, the policy has been rescinded and reinstated by subsequent administrations along party lines and has been in effect for 22 of the past 41 years.
- When in effect, the policy has required foreign non-governmental organizations (NGOs) to certify that they would not “perform or actively promote abortion as a method of family planning” using funds from any source (including non-U.S. funds) as a condition of receiving U.S. government global family planning funding. In 2017, President Trump reinstated the policy but also significantly expanded it to encompass the vast majority of U.S. bilateral global health assistance, and in 2025, he reinstated this expanded application of the policy.
- The expanded policy applies to all of global health, including PEPFAR, maternal and child health, malaria, nutrition, and other U.S. programs. When last in effect, it potentially encompassed $7.3 billion in FY 2020 alone, to the extent that such funding was ultimately provided to foreign NGOs, directly or indirectly (family planning assistance accounted for approximately $600 million of that total).
- The Trump administration’s recent reinstatement of the policy calls for the Secretary of State, in coordination with the Secretary of Health and Human Services, to implement a plan to extend the requirements of the policy to global health assistance provided by all departments or agencies.
What is the Mexico City Policy?
The Mexico City Policy is a U.S. government policy that – when in effect – has required foreign NGOs to certify that they will not “perform or actively promote abortion as a method of family planning” using funds from any source (including non-U.S. funds) as a condition of receiving U.S. global family planning assistance and, when in place under the Trump administration, most other U.S. global health assistance.
The policy was first announced by the Reagan administration at the 2nd International Conference on Population, which was held in Mexico City, Mexico, on August 6-14, 1984 (hence its name; see Box 1).1 Under the first Trump administration, the policy was renamed “Protecting Life in Global Health Assistance” (PLGHA). Among opponents, it is also known as the “Global Gag Rule,” because among other activities, it prohibits foreign NGOs from using any funds (including non-U.S. funds) to provide information about abortion as a method of family planning and to lobby a foreign government to legalize abortion.
Box 1: The Original Language of the Mexico City Policy, 1984
“[T]he United States does not consider abortion an acceptable element of family planning programs and will no longer contribute to those of which it is a part. …[T]he United States will no longer contribute to separate nongovernmental organizations which perform or actively promote abortion as a method of family planning in other nations.”2
When first instituted in 1984, the Mexico City Policy marked an expansion of existing legislative restrictions that already prohibited U.S. funding for abortion internationally, with some exceptions (see below). Prior to the policy, foreign NGOs could use non-U.S. funds to engage in certain voluntary abortion-related activities as long as they maintained segregated accounts for any U.S. money received, but after the Mexico City Policy was in place, they were no longer permitted to do so if they wanted to receive U.S. family planning assistance.
The first Trump administration’s application of the policy to the vast majority of U.S. bilateral global health assistance, including funding for HIV under the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), maternal and child health, malaria, nutrition, and other programs, marked a significant expansion of its scope, potentially encompassing $7.3 billion in FY 2020 alone, to the extent that such funding was ultimately provided to foreign NGOs, directly or indirectly (family planning assistance accounted for approximately $600 million of that total).3 The Trump administration also moved to further tighten restrictions, reaching other areas of U.S. development assistance beyond global health and other non-U.S. funding streams. See “What is the definition of ‘financial support’?” below.4
Although President Biden rescinded the policy during his administration, President Trump’s reinstatement of the policy during his second term will once again require agencies involved in foreign assistance to apply the policy going forward. In addition, the Trump administration has also issued an executive order to re-evaluate foreign aid, including a 90-day review of all programs and pause on new obligations and disbursements as well as freeze of current program implementation; how the reinstated Mexico City Policy intersects with these other actions is not yet clear.
When has it been in effect?
The Mexico City Policy has been in effect for 22 of the past 41 years, primarily through executive action, and has been instated, rescinded, and reinstated by presidential administrations along party lines (see Table 1).
The policy was first instituted in 1984 (taking effect in 1985) by President Ronald Reagan and continued to be in effect through President George H.W. Bush’s administration. It was rescinded by President Bill Clinton in 1993 (although it was reinstated legislatively for one year during his second term;5 see below).6 The policy was reinstated by President George W. Bush in 2001,7 rescinded by President Barack Obama in 2009,8 and reinstated and expanded by President Trump in 2017.9 It was rescinded by President Biden at the beginning of his term in 2021,10 and again reinstated, in its expanded form, by President Trump at the beginning of his term in 2025.11
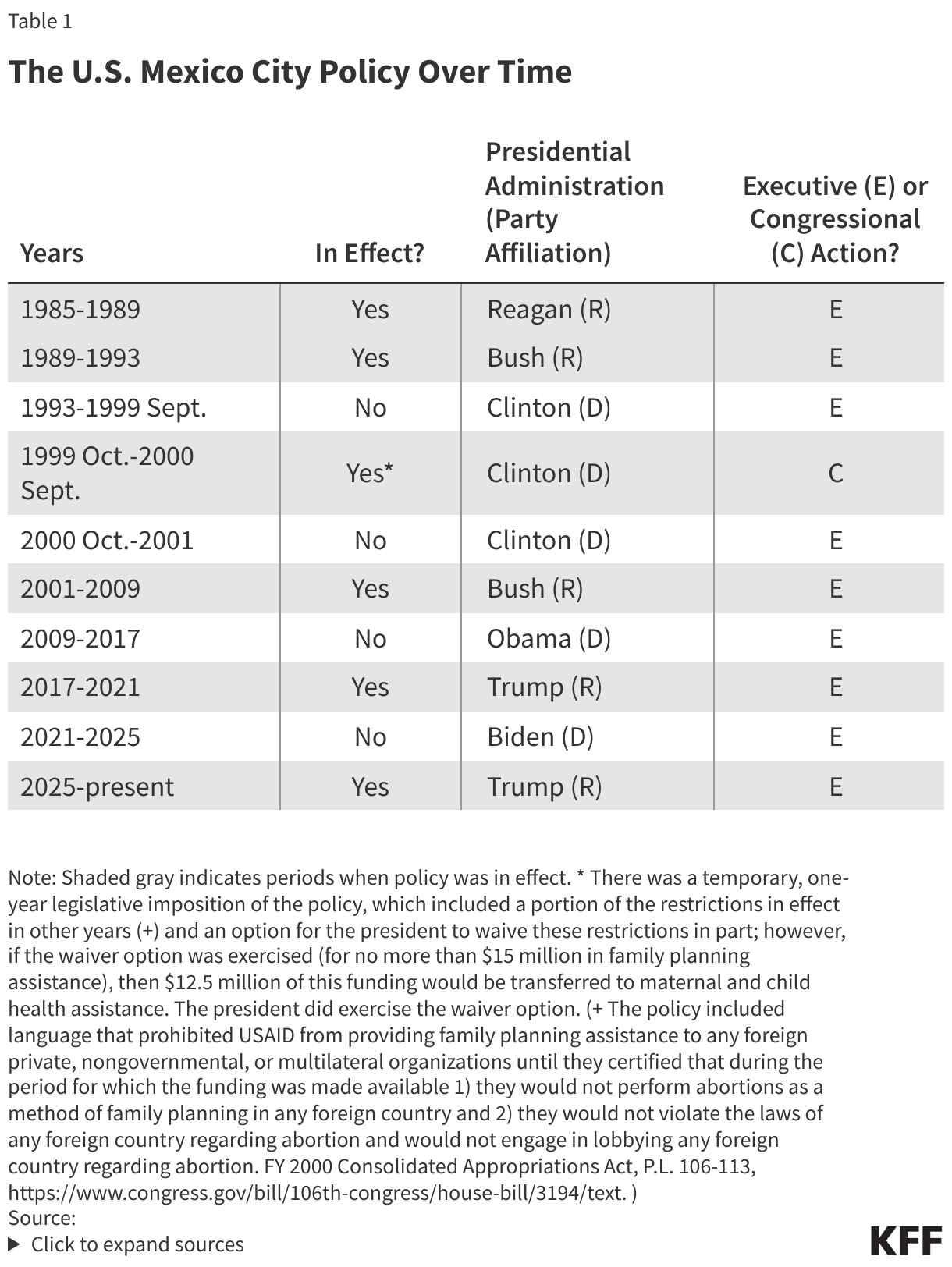
The Mexico City Policy has, for the most part, been instituted or rescinded through executive branch action (typically via presidential memoranda12 ). While Congress has the ability to institute the policy through legislation, this has happened only once in the past: a modified version of the policy was briefly applied by Congress during President Clinton’s last year in office as part of a broader arrangement to pay the U.S. debt to the United Nations.13 (At that time, President Clinton was able to partially waive the policy’s restrictions.14 ) Other attempts to institute the policy through legislation have not been enacted into law,15 nor have legislative attempts to overturn the policy.16 See Table 1.
Who does the policy apply to?
When in effect, the policy applies to foreign NGOs as a condition of receiving U.S. family planning support and, as expanded under President Trump, most other bilateral global health assistance, either directly (as the main – or prime – recipient of U.S. funding) or indirectly (as a recipient of U.S. funding through an agreement with the prime recipient; referred to as a sub-recipient). Specifically, a foreign NGO “recipient agrees that it will not, during the term of this award, perform or actively promote abortion as a method of family planning in foreign countries or provide financial support to any other foreign non-governmental organization that conducts such activities.”17
Foreign NGOs include:
- international NGOs that are based outside the U.S.,
- regional NGOs that are based outside the U.S., and
- local NGOs in assisted countries.18
U.S. NGOs have not been directly subject to the Mexico City Policy but, when in place, must also agree to ensure that they do not provide funding to any foreign NGO sub-recipients unless those sub-recipients have first certified adherence to the policy. Specifically, a U.S. NGO “recipient (A) agrees that it will not furnish health assistance under this award to any foreign non-governmental organization that performs or actively promotes abortion as a method of family planning in foreign countries; and (B) further agrees to require that such sub-recipients do not provide financial support to any other foreign non-governmental organization that conducts such activities.”19
Certain recipients of U.S. assistance have always been exempt from the policy, including foreign governments (national or sub-national) and public international organizations and other multilateral entities, such as the Global Fund to Fight AIDS, Tuberculosis and Malaria and Gavi, the Vaccine Alliance.20 However, as expanded by President Trump, this funding is subject to the policy if it flows through a foreign NGO that has accepted the policy;21 see “What is the definition of ‘financial support’?” below.
To what assistance does it apply?
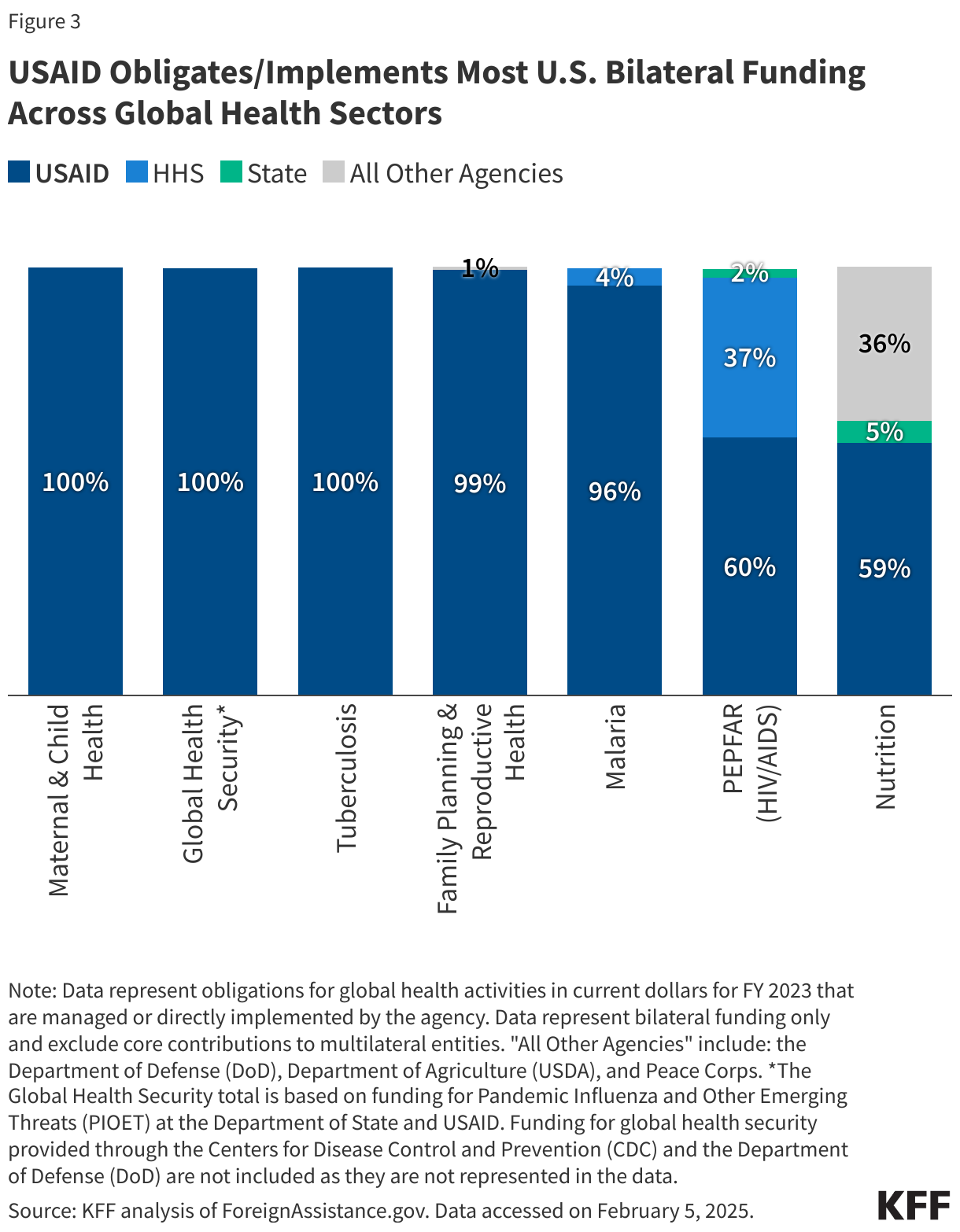
“Assistance” includes “the provision of funds, commodities, equipment, or other in-kind global health assistance”.22 In the past, foreign NGOs have been required to adhere to the Mexico City Policy – when in effect – as a condition of receiving support through certain U.S. international funding streams: family planning assistance through the U.S. Agency for International Development (USAID) and, beginning in 2003, family planning assistance23 through the U.S. Department of State. In the 2003 memorandum announcing the policy’s expansion to include the Department of State, President Bush stated that the policy did not apply to funding for global HIV/AIDS programs and that multilateral organizations that are associations of governments are not included among “foreign NGOs.”24 However, the first Trump administration greatly expanded – and the second Trump administration reinstated – the policy to apply to the vast majority of U.S. bilateral global health assistance furnished by all agencies and departments, including:25
- family planning and reproductive health
- maternal and child health (including household-level water, sanitation, and hygiene (WASH))26
- nutrition
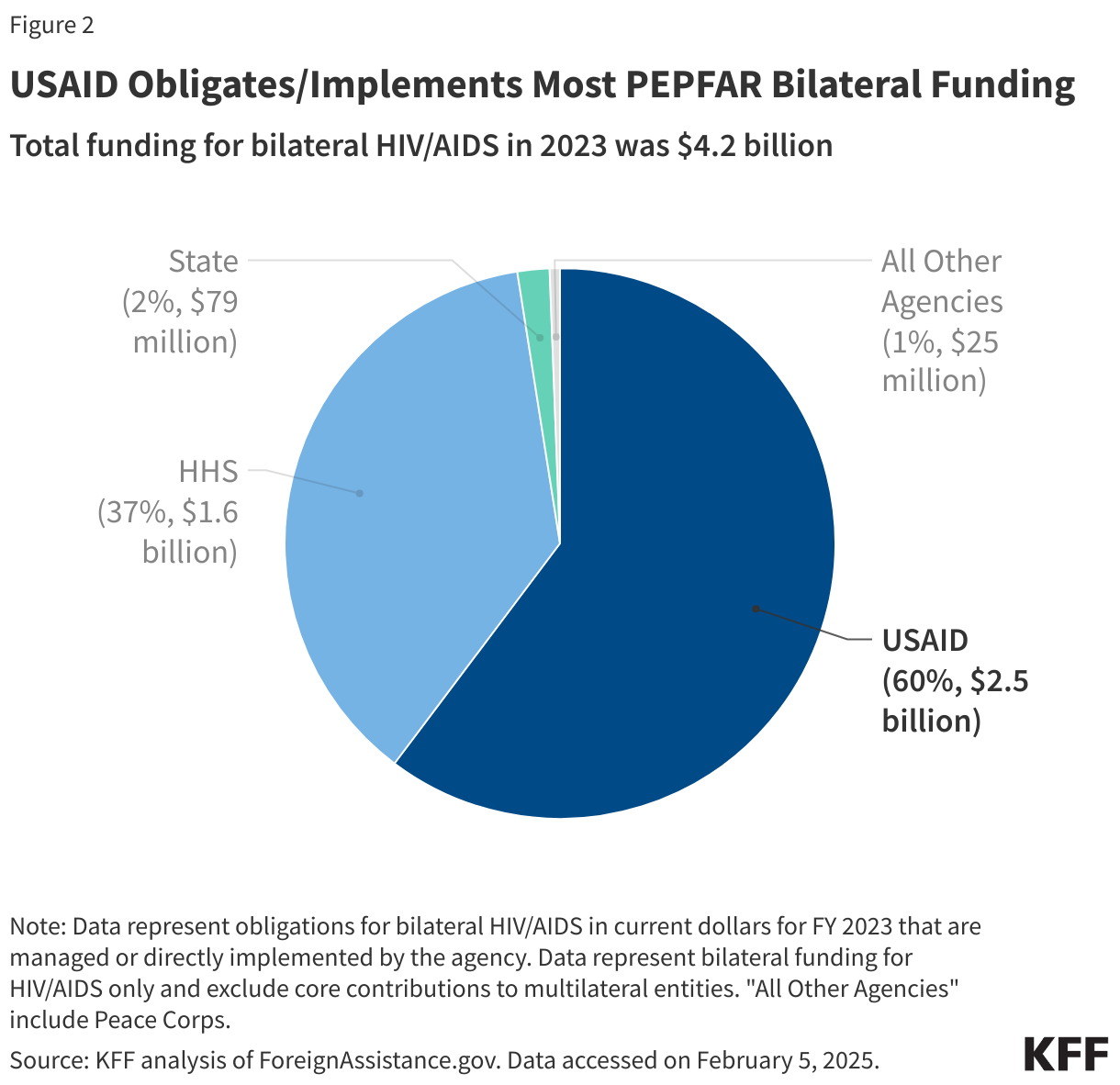
- HIV under PEPFAR
- tuberculosis
- malaria under the President’s Malaria Initiative (PMI)
- neglected tropical diseases
- global health security
- certain types of research activities27
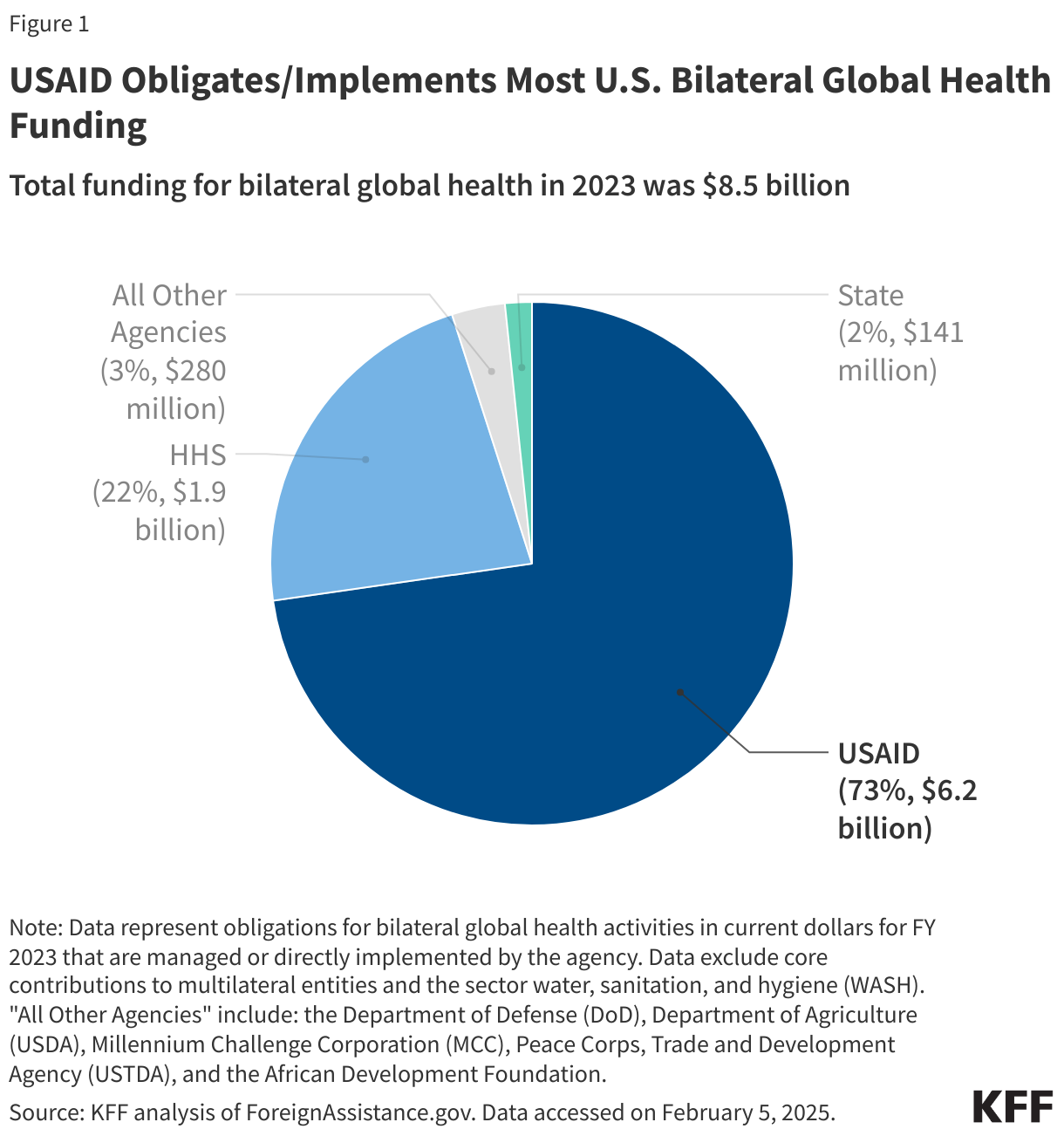
The policy applies to the assistance described above that was appropriated directly to three agencies and departments: USAID; the Department of State, including the Office of the Global AIDS Coordinator, which oversees and coordinates U.S. global HIV funding under PEPFAR; and for the first time, the Department of Defense (DoD).28 When such funding is transferred to another agency, including the Centers for Disease Control (CDC) and the National Institutes of Health (NIH), it remains subject to the policy, to the extent that such funding is ultimately provided to foreign NGOs, directly or indirectly.
The policy applies to two types of funding instruments: grants and cooperative agreements.29 The first Trump administration had sought to apply the policy to contracts and issued a proposed rule to this effect, but it was not finalized;30 it is not clear whether the second Trump administration will also seek to do so.
The policy does not apply to U.S. assistance for: water supply and sanitation activities, which is usually focused on infrastructure and systems;31 humanitarian assistance, including activities related to migration and refugee assistance activities as well as disaster and humanitarian relief activities; the American Schools and Hospitals Abroad (ASHA) program; and Food for Peace (FFP).32 However, this funding is subject to the policy if it flows through a foreign NGO that has accepted the policy;33 see “What is the definition of ‘financial support’?” below.
What activities does it prohibit?
The policy prohibits foreign NGOs that receive U.S. family planning assistance and, as expanded by President Trump, most other U.S. bilateral global health assistance from using funds from any source (including non-U.S. funds) to “perform or actively promote abortion as a method of family planning.” In addition to providing abortions with non-U.S. funds, restricted activities also include the following:
- providing advice and information about and offering referral for abortion – where legal – as part of the full range of family planning options,
- promoting changes in a country’s laws or policies related to abortion as a method of family planning (i.e., engaging in lobbying), and
- conducting public information campaigns about abortion as a method of family planning.
The prohibition of these activities is why the policy has been referred to by its critics as the “Global Gag Rule.”
Additionally, for the first time, the expanded policy during the first Trump administration prohibited foreign NGOs from providing any financial support with any source of funds (including non-U.S. funding) and for any purpose to other foreign NGOs that perform or actively promote abortion as a method of family planning;34 see “What is the definition of ‘financial support’?” below.
When in effect, the policy, however, does not prohibit foreign NGOs from:
- providing advice and information about, performing, or offering referral for abortion in cases where the pregnancy has either posed a risk to the life of the mother or resulted from incest or rape;35 and
- responding to a question about where a safe, legal abortion may be obtained when a woman who is already pregnant clearly states that she has already decided to have a legal abortion (passively providing information, versus actively providing medically-appropriate information).
In addition, the expanded policy during the Trump administrations does not apply to healthcare providers who have an affirmative duty required under local law to provide counseling about and referrals for abortion as a method of family planning.
Does it restrict direct U.S. funding for abortion overseas?
U.S. funding for abortion was already restricted and remains restricted under several provisions of the law.36 Specifically, before the Mexico City Policy was first announced in 1984, U.S. law already prohibited the use of U.S. aid:
- to pay for the performance of abortion as a method of family planning or to motivate or coerce any person to practice abortion (the Helms Amendment, 1973, to the Foreign Assistance Act);
- for biomedical research related to methods of or the performance of abortion as a means of family planning (the Biden Amendment, 1981, to the Foreign Assistance Act); and
- to lobby for or against abortion37 (the Siljander Amendment, first included in annual appropriations in 1981 and included each year thereafter).
Then, shortly after the policy was announced in 1984, the Kemp-Kasten Amendment was passed in 1985, prohibiting the use of U.S. aid to fund any organization or program, as determined by the president, that supports or participates in the management of a program of coercive abortion or involuntary sterilization (it is now included in annual appropriations).
Before the Mexico City Policy, U.S. aid recipients could use non-U.S. funds to engage in certain abortion-related activities but were required to maintain segregated accounts for U.S. assistance.38 The Mexico City Policy reversed this practice: no longer were foreign NGOs allowed to use non-U.S. funds, maintained in segregated accounts, for voluntary abortion-related activities if they wished to continue to receive or be able to receive U.S. family planning funds.
Does the policy prohibit post-abortion care?
The Mexico City Policy does not restrict the provision of post-abortion care, which is a supported activity of U.S. family planning assistance. Whether or not the Mexico City Policy is in effect, recipients of U.S. family planning assistance are allowed to use U.S. and non-U.S. funding to support post-abortion care,39 no matter the circumstances of the abortion (whether it was legal or illegal).
What has been the impact of the policy?
A KFF literature review of studies examining the policy, from 2001 to 2024, identified a range of impacts associated with the policy, including: increases in abortion rates and reductions in contraceptive prevalence (among other health outcomes); disruption and gaps in services; reduction in service integration; over-implementation and chilling effects; confusion about the policy; loss of civil society/NGO coordination and partnerships; and increased administrative burden. In addition, several studies sought to calculate or estimate the reach of the policy, as measured by amount of funding, countries, and/or NGOs affected (see Box 2).
Box 2: Impacts Associated with the Mexico City Policy in the Literature
- Increased abortion rates
- Increased pregnancy
- Decreased contraceptive prevalence
- Disruption in family planning and other services
- Gaps in family planning and other services
- Reduced service integration
- Over-implementation and chilling effect
- Confusion
- Loss of civil society/NGO coordination and partnerships
- Increased administrative burden
KFF analyses have also found that during the first Trump administration, the expanded policy applied to a much greater amount of U.S. global health assistance, and greater number of foreign NGOs, across many program areas.40 KFF found that more than half (37) of the 64 countries that received U.S. bilateral global health assistance in FY 2016 allow for legal abortion in at least one case not permitted by the policy and that had the expanded Mexico City Policy been in effect during the FY 2013 – FY 2015 period, at least 1,275 foreign NGOs would have been subject to the policy. In addition, at least 469 U.S. NGOs that received U.S. global health assistance during this period would have been required to ensure that their foreign NGO sub-recipients were in compliance. Additional foreign NGOs were likely impacted by the policy due to the revised interpretation of “financial support” announced in March 2019 and implemented beginning June 2019;41 see “What is the definition of ‘financial support’?” below.
During the first Trump administration, two official assessments by the U.S. Department of State were released (see below).42 Additionally, a report released in March 2020 by the U.S. Government Accountability Office (GAO) provided new information on the number of projects (awards) and NGOs affected by the expanded policy during the first Trump administration. It found that from May 2017 through FY 2018:
- the policy had been applied to over 1,300 global health projects, with the vast majority of these through USAID and CDC, and
- NGOs declined to accept the policy in 54 instances, totaling $153 million in declined funding – specifically, seven prime awards amounting to $102 million and 47 sub-awards amounting to $51 million (more than two-thirds of sub-awards were intended for Africa) – across USAID and CDC; the Department of State and DoD did not identify any instances where NGOs declined to accept the policy conditions.
What did the U.S. government’s reviews of the expanded policy during the first Trump administration find?
During the first Trump administration, the U.S. government published two reviews of the expanded policy, with the first examining the initial six months of the policy released in February 2018 and the second examining the first 18 months of the policy released in August 2020.
First Review
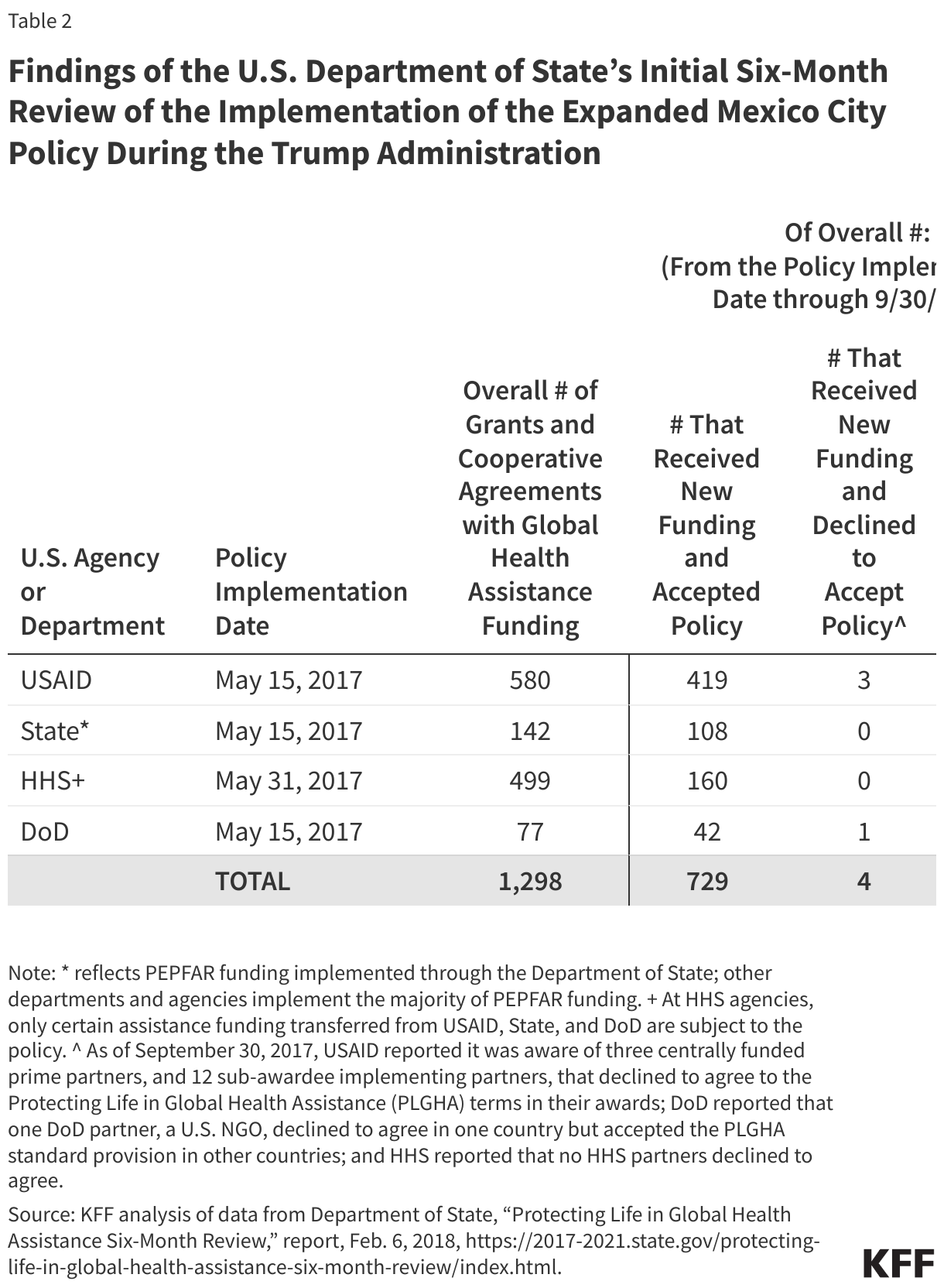
In February 2018, the Department of State announced the findings of an initial six-month review of implementation of the policy through the end of FY 2017 (September 2017).43 The report directed agencies to provide greater support for improving understanding of implementation among affected organizations and provided guidance to clarify terms included in standard provisions of grants and cooperative agreements. In the six-month review report, the Department of State report identified a number of “actions” for implementing agencies, such as a need for:
- more central and field-based training and implementation tools,
- a clearer explanation of termination of awards for NGOs found to be in violation of the policy, and
- a clarification of “financial support,” which was not defined in the standard provisions (see “What is the definition of ‘financial support’?” below).
- The six month review also identified the number of affected agreements with prime implementing partners and the number of those that have accepted the Mexico City Policy as part of their agreements through September 2017 (see Table 2).
Second Review
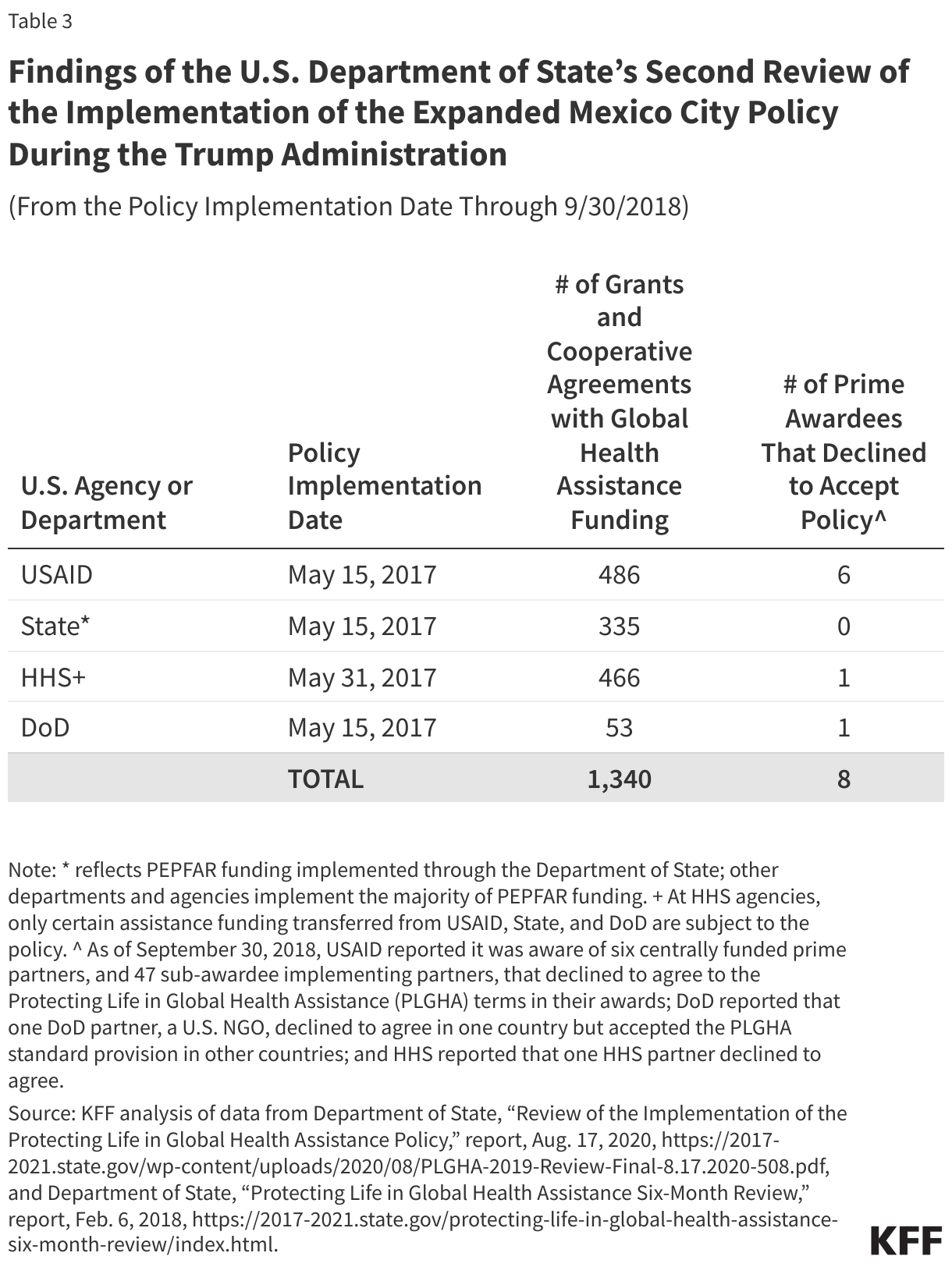
On August 17, 2020, the Department of State released its second review of the policy, updating its initial six-month review (as an action item in the six-month review report, the department stated it would “conduct a further review of implementation of the policy by December 15, 2018, when more extensive experience will enable a more thorough examination of the benefits and challenges”). The long-anticipated review, which examines the period from May 2017 through September 2018, found:
- the awards declined spanned a variety of program areas, including family planning and reproductive health (FP/RH), HIV and AIDS (HIV/AIDS), maternal and child health (MCH), tuberculosis (TB), and nutrition, in addition to cross-cutting awards;
- the awards declined spanned geographic areas but many were for activities in sub-Saharan Africa;
- agencies and departments made efforts to transition projects to another implementer in order to minimize disruption; but
- nevertheless, among USAID awards involving health service delivery where prime and sub-award recipients declined to accept the policy, gaps or disruptions in service delivery were sometimes reported.
The second review also identified the number of affected agreements with prime implementing partners and the number of those that have accepted the Mexico City Policy as part of their agreements through September 2018 (see Table 3).
Additionally, the review reported that 47 sub-awardees, all under USAID awards, declined to accept the policy. It is important to note that the review also stated that information on sub-awards is not systematically collected by departments and agencies and that DoD was not able to collect information on sub-awards.
What is the definition of “financial support”?
The first Trump administration also expanded (and the second Trump administration reinstates) the interpretation of “financial support” to apply to more funding and organizations, albeit indirectly. In February 2018, in the initial six-month review issued when then-Secretary of State Tillerson led the department, the Department of State report included an “action” statement to clarify the definition of “financial support” as used in the standard provisions for grants and cooperative agreements. At issue was whether it applied more narrowly to certain funding provided by foreign NGOs (i.e., funding other than U.S. global health funding) to other foreign NGOs specifically for the purpose of performing or actively promoting abortion as a method of family planning or if it applied more broadly to certain funding provided by foreign NGOs to other foreign NGOs for any purpose, if that foreign NGO happened to perform or actively promote abortion as a method of family planning. The State Department clarified that it was the more narrow interpretation.44
However, on March 26, 2019, then-Secretary of State Pompeo reversed this interpretation, announcing further “refinements” to the policy to clarify that it applied to the broader definition of financial support.45 Specifically, under the policy, U.S.-supported foreign NGOs agree to not provide any financial support (global health-related as well as other support), no matter the source of funds, to any other foreign NGO that performs or actively promotes abortion as a method of family planning. In June 2019, USAID provided additional information to reflect this broader interpretation of the standard provisions.46
This marked the first time the policy had been applied this broadly, as it could then affect funding provided by other donors (such as other governments and foundations) and non-global health funding provided by the U.S. government for a wide range of purposes if this funding was first provided to foreign NGOs who had accepted the policy (as recipients of U.S. global health assistance) that then in turn provided that donor or U.S. non-global health funding for any purpose to foreign NGOs that perform or actively promote abortion as a method of family planning. For example, under the prior interpretation, a foreign NGO recipient of U.S. global health funding could not provide any non-U.S. funding to another foreign NGO to perform or actively promote abortion as a method of family planning but could provide funding for other activities, such as education, even if the foreign NGO carried out prohibited activities. Under the broader interpretation, a foreign NGO could not provide any non-U.S. funding for any activity to a foreign NGO that carried out prohibited activities. Similarly, while under the prior interpretation a foreign NGO recipient of U.S. global health funding could provide other U.S. funding (such as humanitarian assistance) to another foreign NGO for non-prohibited activities, even if the foreign NGO carried out prohibited activities, under the subsequent broader interpretation, it could not do so.
What has happened since President Trump reinstated the expanded policy during his second term?
Since President Trump reinstated his 2017 memorandum on the Mexico City Policy in January 2025 and also directed the Secretary of State and HHS Secretary to implement a plan to extend its requirements to global health assistance furnished at all agencies or departments, no additional specifics about what actions have been taken to implement the expanded policy have been announced. This is, in part, due to the recent executive actions affecting the operation of USAID and freezing foreign aid.



 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma