KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
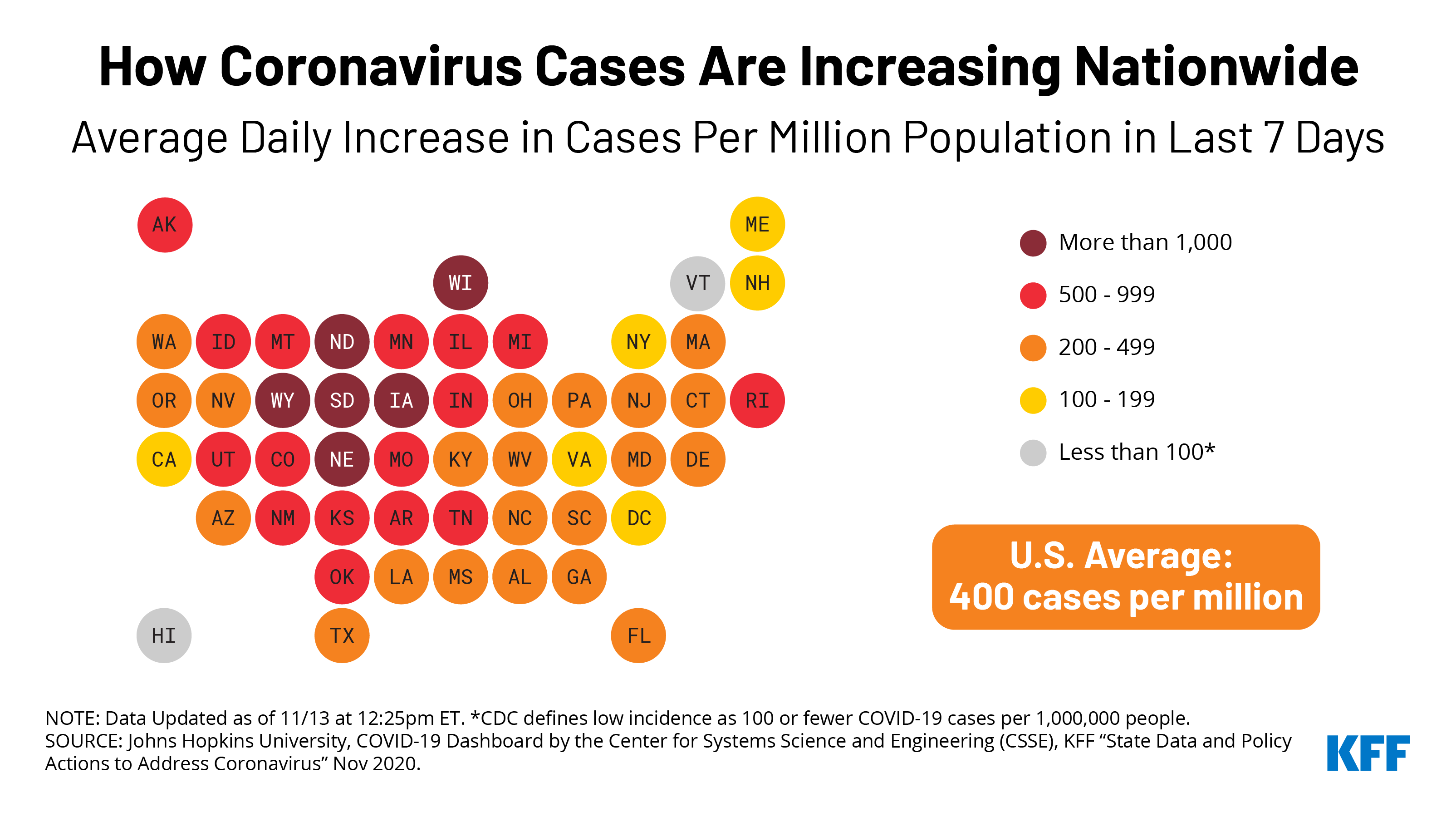
The total number of confirmed COVID-19 cases in the United States recently surpassed 10 million,and nationwide deaths are nearing 250,000. As we move into the holiday season, cases are rapidly growing across the country, putting pressure on health systems and providers. Currently, 49states and D.C.are categorized as COVID-19 hotspots,Hawaii is the only exception (see our COVID-19 dashboard for more data and a detailed definition of hotspots).
The chart shows daily new cases per million population in each state using a 7-day rolling average, which helps to account for fluctuations in reporting throughout each week.
By this metric, six states –North Dakota, South Dakota, Iowa, Wyoming, Wisconsin, and Nebraska — had an average daily increase of more than 1,000 cases per million people in the past week, and 13 additional states saw an averageof upwards of 500 new daily cases per million people. The alarming growth of COVID-19 cases in the Midwest and Mountain states,in particular,has led to urgent hospital capacity issues. Multiple hospitals in these states have reported being at full capacity, and COVID-19 hospitalizations nationwidehave reached their highest level since the start of the pandemic. Looking ahead, rising cases combined with holiday gatherings and travel have the potential to exacerbatehospital capacity concerns around the country.
KHN and Associated Press Investigation of Inadequate U.S. Public Health Infrastructure During the Pandemic Wins Top Journalism Award from the American Association for the Advancement of Science
The American Association for the Advancement of Science (AAAS) has awarded KFF’s Kaiser Health News and The Associated Press one of its top journalism prizes for a joint investigation that revealed the diminished state of the U.S. public health infrastructure in the face of the COVID-19 pandemic.
The AAAS gave the news organizations its Gold Award in science reporting for “Hollowed-Out Public Health System Faces More Cuts Amid Virus,” an investigation that found that the public health workforce in the U.S. is underfunded and under threat, lacking the basic tools to confront the worst pandemic in a century. The novel coronavirus has infected more than 10 million people in the U.S. so far and killed more than 238,000.
The AAAS is the world’s largest multidisciplinary scientific society, which also publishes research in the esteemed journal Science. Its Kavli Science Journalism Awards recognize distinguished science reporting for a general audience. The program, open to journalists worldwide, received entries from news organizations in 54 countries this year. Winners will receive their awards in a virtual ceremony held in conjunction with the 2021 AAAS Annual Meeting in February.
KHN and AP journalists interviewed more than 150 public health workers, policymakers and experts, analyzed state and federal financial records, and surveyed statehouses around the country. Their investigation found that governments at every level have failed to provide the public health system with the resources — both human and financial — that are required to protect the nation from pandemics.
AP and KHN also shared data and offered guidance to news organizations that are AP members and customers to help them localize the findings of the investigation for their regions.
The full list of award winners is available on the AAAS website.
About KFF and Kaiser Health News
Filling the need for trusted information on national health issues, KFF (Kaiser Family Foundation) is a nonprofit organization based in San Francisco, California. KHN (Kaiser Health News) is a nonprofit news service covering health issues. KHN is an editorially independent program of KFF and, along with Policy Analysis and Polling, is one of the three major operating programs of KFF. KFF is not affiliated with Kaiser Permanente.
About AP
The Associated Press is an independent global news organization dedicated to factual reporting. Founded in 1846, AP today remains the most trusted source of fast, accurate, unbiased news in all formats and the essential provider of the technology and services vital to the news business. More than half the world’s population sees AP journalism every day. Online: https://apnews.com/
Senate Appropriations Committee Releases FY 2021 State and Foreign Operations (SFOPs) and Labor Health and Human Services (Labor HHS) Appropriations Bills
The Senate Appropriations Committee released its FY 2021 State, Foreign Operations, and Related Programs (SFOPs) (links to bill and report) and Labor, Health and Human Services, Education, and Related Agencies (Labor HHS) (links to bill and report) appropriations bills and accompanying reports on November 10, 2020. The SFOPs bill includes funding for U.S. global health programs at the State Department and the U.S. Agency for International Development (USAID), while the Labor HHS bill includes funding for global health programs at the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health (NIH).[i]
Key highlights are as follows (see table for additional detail):
Funding provided to the State Department and USAID under the SFOPs bill and through the Global Health Programs (GHP) account, which represents the bulk of global health assistance, totals $9.3 billion in the bill, $161 million above the FY20 enacted level, $3.3 billion above the President’s FY21 request, and $96.5 million above the FY21 House level. Funding for most global health programs at State and USAID either increased or remained flat compared to the FY20 enacted level, except for family planning and reproductive health (including UNFPA), which declined; by far, the largest increase is for global health security. The biggest differences between the House and Senate FY 2021 bills is related to family planning (the House would provide more) and global health security (the Senate would provide more). Details on specific programs are as follows (unless otherwise specified, totals represent funding through the Global Health Programs account):
Bilateral HIV funding through the President’s Emergency Plan for AIDS Relief (PEPFAR) is $4,700 million in the Senate FY21 bill, matching the FY20 enacted and FY21 House bills, and $1,520 million (48%) above the FY21 Request ($3,180 million).
The bill includes $1,560 million as the U.S. contribution to the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), matching the FY20 enacted and FY21 House level, and $902 million (137%) above the FY21 Request ($657.6 million).
Funding for tuberculosis (TB) totals $325 million, $15 million (5%) above the FY20 enacted and FY21 House level ($310 million), and $50 million (18%) above the FY21 Request ($275 million).
Funding for malaria totals $785 million, $15 million (2%) above the FY20 enacted level ($770 million), $76.5 million (11%) above the FY21 Request ($708.5 million), and $30 million (4%) above the FY21 House level ($755 million).
The bill includes $865 million for maternal and child health (MCH), an increase of $14 million (2%) above the FY20 enacted level ($851 million), $205 million (31%) above the FY21 Request ($659.6 million), and $15 million (2%) above the FY21 House level ($850 million). Specific areas under MCH include:
Gavi, the Vaccine Alliance funding totals $290 million, matching the FY20 enacted, FY21 Request, and FY21 House level.
Polio funding through the GHP account totals $65 million, $4 million (7%) above the FY20 enacted and FY21 House level ($61 million). The President’s FY21 Request did not specify funding for polio.
The bill includes $139 million for the U.S. contribution to the United Nations Children’s Fund (UNICEF) provided through the International Organizations and Programs (IO&P) account, matching the FY20 enacted and FY21 House level. While the FY21 Request did not specify a funding amount for UNICEF and proposed to eliminate the IO&P account, it is possible that organizations such as UNICEF could receive funding through other accounts.
Funding for nutrition totals $150 million, matching the FY20 enacted level, $60 million (67%) above the FY21 Request ($90 million), and $5 million (3%) above the FY21 House level ($145 million).
Bilateral family planning and reproductive health (FP/RH) funding totals $461 million and is one of the only areas that is a decrease compared to the prior year total ($63 million or 12% below the FY20 enacted level of $524 million). The Senate FY21 FP/RH total is $224 million (95%) above the FY21 Request ($237 million) and $124.5 million (21%) below the FY21 House level ($585.5 million).
The bill does not include any funding for the United Nations Population Fund (UNFPA) similar to the FY21 Request; funding for UNFPA in FY20 totals $32.5 million and the FY21 House bill included $55 million. The Senate FY21 bill includes the Kemp Kasten amendment, which the Trump Administration has used in each year between FY17 and FY20 to withhold funding from UNFPA (learn more about the Kemp Kasten amendment here). By contrast, the House FY21 bill did not include the Kemp Kasten Amendment.
Funding for the vulnerable children program totals $30 million, $5 million (20%) above the FY20 enacted level ($25 million) and $6 million (25%) above the FY21 House level ($24 million); the FY20 Request proposed eliminating funding for this program.
Funding for neglected tropical diseases (NTDs) totals $102.5 million, matching the FY20 enacted and FY21 House level, and $27.5 million (37%) above the FY21 Request ($75 million).
Funding for global health security is the largest increase in the bill totaling $275 million, which is $175 million (175%) above the FY20 enacted level, $185 million (206%) above the FY21 Request ($90 million), and $150 million (120%) above the FY21 House level ($125 million).
The FY21 Senate bill states that up to $25 million made available under the GHP account may be made available for the Emergency Reserve Fund.
Funding for the World Health Organization (WHO) through the International Organizations and Programs (IO&P) account declined but is based on the assessed contribution (see KFF fact sheet on the WHO). WHO funding in the FY21 Senate bill totals $118.9 million, $3.8 million (3%) below the FY20 enacted level ($122.7 million), $61 million (105%) above the FY21 Request ($57.9 million), and $200 million (63%) below the FY21 House level ($200 million through the GHP account and $118.9 million through the IO&P account).
The Senate SFOPs bill also includes the Mexico City Policy (MCP) (see the KFF MCP explainer), while the House SFOPs bill includes a prohibition on using any current or prior SFOPs appropriations to implement the MCP.
Funding provided to CDC for global health through the Labor HHS bill totals $615.8 million, an increase of $45 million (8%) above the FY20 enacted level ($570.8 million), $83.6 million (16%) above the FY21 Request ($532.2 million), and $43 million (8%) above the House FY21 level ($572.8 million). All of the increase at CDC is for global public health protection, and the Senate would direct more to this area than the House. Global health funding at CDC includes:
$128.4 million for global HIV/AIDS, matching the FY20 enacted and FY21 House level and $58.9 million (85%) above the FY21 Request ($69.5 million).
$7.2 million for global tuberculosis (TB), matching the FY20 enacted and FY21 Request level and $2 million (22%) below the FY21 House level ($9.2 million).
$226 million for global immunization, matching the FY20 enacted and FY21 House level and $20 million (10%) above the FY21 Request ($206 million). Within this total are the following:
Funding for polio totals $176 million, matching the FY20 enacted and FY21 House level and $11 million (7%) above the FY21 Request ($165 million).
Funding for CDC’s other global vaccines/measles program totals $50 million, matching the FY20 enacted and FY21 House level and $9 million (22%) above the FY21 Request ($41 million).
$26 million for parasitic diseasesand malaria, matching the FY20 enacted and FY21 House level and $1.5 million (6%) above the FY21 Request ($24.5 million).
The entire increase at the CDC is for the global public health protection program which totals $228.2 million, $45 million (25%) above the FY20 enacted and FY21 House level and $3.2 million (1%) above the FY21 Request ($225 million).
Funding for the Fogarty International Center (FIC) at NIH totals $83.5 million, $2.7 million (3%) above the FY20 enacted level ($80.8 million), $9.9 million (14%) above the FY21 Request ($73.5 million), and $3 million (4%) below the FY21 House level ($86.5 million).
Resources:
FY2021 State, Foreign Operations, and Related Programs Appropriations Bill – Bill
FY2021 State, Foreign Operations, and Related Programs Appropriations Bill – Report
FY2021 Labor, Health and Human Services, Education, and Related Agencies Appropriations Bill – Bill
FY2021 Labor, Health and Human Services, Education, and Related Agencies Appropriations Bill – Report
The table (.xls) below compares global health funding in the FY 2021 Senate SFOPs and Labor HHS appropriations bills to the FY 2020 enacted funding amounts as outlined in the “Consolidated Appropriations Act, 2020” (P.L. 116-94; KFF summary here), the President’s FY 2021 request (KFF summary here), and the House FY 2021 SFOPs and Labor HHS bills (KFF summary here and here).
Table: KFF Analysis of FY21 Senate Appropriations for Global Health
Department / Agency / Area
FY20 Enacted(millions)
FY21Requesti(millions)
FY21House(millions)
FY21Senateii(millions)
Difference(millions)
FY21 Senate– FY20 Enacted
FY21 Senate– FY21 Request
FY21 Senate– FY21 House
SFOPs – Global Health
HIV/AIDS
$4,700.0
$3,180.3
$4,700.0
$4,700.0
$0 (0%)
$1519.7 (47.8%)
$0 (0%)
State Department
$4,370.0
$3,180.3
$4,370.0
$4,370.0
$0(0%)
$1189.7(37.4%)
$0(0%)
USAID
$330.0
$0.0
$330.0
$330.0
$0(0%)
$330.0(N/A)
$0(0%)
of which Microbicides
$45.0
$0.0
$45.0
$45.0
$0(0%)
$45.0(N/A)
$0(0%)
Global Fund
$1,560.0
$657.6
$1,560.0
$1,560.0
$0 (0%)
$902.4 (137.2%)
$0 (0%)
Tuberculosisiii
–
–
–
–
–
–
–
Global Health Programs (GHP) account
$310.0
$275.0
$310.0
$325.0
$15(4.8%)
$50(18.2%)
$15(4.8%)
Economic Support Fund (ESF) account
Not specified
Not specified
Not specified
Not specified
–
–
–
Malaria
$770.0
$708.5
$755.0
$785.0
$15 (1.9%)
$76.5 (10.8%)
$30 (4%)
Maternal & Child Health (MCH)iv
–
v
–
–
–
–
–
GHP accountvi
$851.0
$659.6
$850.0
$865.0
$14(1.6%)
$205.4(31.1%)
$15(1.8%)
of which Gavi
$290.0
$290.0
$290.0
$290.0
$0(0%)
$0(0%)
$0(0%)
of which Poliovi
$61.0
Not specified
$61.0
$65.0
$4(6.6%)
–
$4(6.6%)
UNICEFvii
$139.0
Not specified
$139.0
$139.0
$0(0%)
–
$0(0%)
ESF account
Not specified
Not specified
Not specified
Not specified
–
–
–
of which Poliovi
vi
Not specified
Not specified
Not specified
–
–
–
Nutritionviii
–
–
–
–
–
–
–
GHP account
$150.0
$90.0
$145.0
$150.0
$0(0%)
$60(66.7%)
$5(3.4%)
ESF account
Not specified
Not specified
Not specified
Not specified
–
–
–
Family Planning & Reproductive Health (FP/RH)ix
$607.5
–
$805.5
$461.0
$-146.5 (-24.1%)
–
$-344.5 (-42.8%)
Bilateral FPRHix
$575.0
–
$750.0
$461.0
$-114(-19.8%)
–
$-289(-38.5%)
GHP accountix
$524.0
$237.0
$585.5
$461.0
$-63(-12%)
$224(94.5%)
$-124.5(-21.3%)
ESF accountix
$51.1
Not specified
$164.5
$0.0
$-51.1(-100%)
–
$-164.5(-100%)
UNFPAx
$32.5
$0.0
$55.5
$0.0
$-32.5(-100%)
$0.0(N/A)
$-55.5(-100%)
Vulnerable Children
$25.0
$0.0
$24.0
$30.0
$5 (20%)
$30.0(N/A)
$6 (25%)
Neglected Tropical Diseases (NTDs)
$102.5
$75.0
$102.5
$102.5
$0 (0%)
$27.5 (36.7%)
$0 (0%)
Global Health Security
$100.0
$90.0
$125.0
$275.0
$175 (175%)
$185 (205.6%)
$150 (120%)
GHP account
$100.0
$90.0
$125.0
$275.0
$175(175%)
$185(205.6%)
$150(120%)
Emergency Reserve Fund
xi
$25.0
xi
xi
–
–
–
World Health Organization (WHO)xii
$122.7
$57.9
$318.9
$118.9
$-3.8 (-3.1%)
$61 (105.4%)
$-200 (-62.7%)
GHP accountxii
Not specified
Not specified
$200.0
Not specified
–
–
–
Contributions to International Organizations (CIO) account
$122.7
$57.9
$118.9
$118.9
$-3.8(-3.1%)
$61(105.4%)
$0(0%)
SFOPs Total (GHP account only)
$9,092.5
$5,998.0
$9,157.0
$9,253.5
$161 (1.8%)
$3255.5 (54.3%)
$96.5 (1.1%)
Labor Health & Human Services (Labor HHS)
Centers for Disease Control & Prevention (CDC) – Total Global Health
$570.8
$532.2
$572.8
$615.8
$45 (7.9%)
$83.6 (15.7%)
$43 (7.5%)
Global HIV/AIDS
$128.4
$69.5
$128.4
$128.4
$0(0%)
$58.9(84.7%)
$0(0%)
Global Tuberculosisxiii
$7.2
$7.2
$9.2
$7.2
$0(0%)
$0(0%)
$-2(-21.5%)
Global Immunization
$226.0
$206.0
$226.0
$226.0
$0(0%)
$20(9.7%)
$0(0%)
Polio
$176.0
$165.0
$176.0
$176.0
$0(0%)
$11(6.7%)
$0(0%)
Other Global Vaccines/Measles
$50.0
$41.0
$50.0
$50.0
$0(0%)
$9(22%)
$0(0%)
Parasitic Diseases
$26.0
$24.5
$26.0
$26.0
$0(0%)
$1.5(6.3%)
$0(0%)
Global Public Health Protection
$183.2
$225.0
$183.2
$228.2
$45(24.6%)
$3.2(1.4%)
$45(24.6%)
Global Disease Detection and Emergency Response
$173.4
Not specified
Not yet known
$218.4
$45(26%)
–
–
of which Global Health Security (GHS)
$125.0
$175.0
Not yet known
Not yet known
–
–
–
Global Public Health Capacity Development
$9.8
Not specified
Not yet known
$9.8
$0(0%)
–
–
National Institutes of Health (NIH) – Total Global Health
Not yet known
Not yet known
Not yet known
Not yet known
–
–
–
HIV/AIDS
Not yet known
Not yet known
Not yet known
Not yet known
–
–
–
Malaria
$208.0
Not yet known
Not yet known
Not yet known
–
–
–
Fogarty International Center (FIC)
$80.8
$73.5
$86.5
$83.5
$2.7(3.3%)
$9.9(13.5%)
$-3(-3.5%)
Notes:
i – In the FY21 Request, the administration proposed to consolidate the Development Assistance (DA), Economic Support Fund (ESF), the Assistance for Europe, Eurasia, and Central Asia (AEECA), and the Democracy Fund (DF) accounts in to one new account — the Economic Support and Development Fund (ESDF). ESF funding for the FY21 Request reflects the amounts requested by the administration for ESDF.
ii – The FY21 Senate bill states that funding from Global Health Programs, Development Assistance, International Disaster Assistance, Complex Crisis Fund, Economic Support Fund, Democracy Fund, Assistance for Europe, Eurasia and Central Asia, Migration and Refugee Assistance, and Millennium Challenge Corporation may be used to address an infectious disease or public health emergency as determined by the Secretary of State and not to exceed $50,000,000 in total funding.
iii – Some tuberculosis funding is provided under the ESF account, which is not earmarked by Congress in the annual appropriations bills and determined at the agency level (e.g. in FY18, TB funding under the ESF account totaled $4 million).
iv – Some MCH funding is provided under the ESF account, which is not earmarked by Congress in the annual appropriations bills and determined at the agency level (e.g. n FY18, MCH funding under the ESF account totaled $15.5 million).
v – It is not possible to calculate total MCH funding in the FY21 request because UNICEF, which has historically received funding through the International Organizations and Programs (IO&P) account, was not specified in the FY21 request.
vi – The minority summary of the FY20 conference agreement states that part of the increase in MCH funding is “due to a shift of $7.5 million for polio prevention programs from the Economic Support Fund account to the Global Health Programs account.”
vii – UNICEF funding in the FY20 Conference Agreement both include an earmark of $5 million for programs addressing female genital mutilation.
viii – Some nutrition funding is provided under the ESF account, which is not earmarked by Congress in the annual appropriations bills and determined at the agency level. (e.g. in FY17, nutrition funding under the ESF account totaled $21 million).
ix – The FY21 Senate bill text states that “not more than $461,000,000 shall be made available for family planning/reproductive health.”
x – The FY21 House bill text states that if this funding is not provided to UNFPA it “shall be transferred to the ‘Global Health Programs’ account and shall be made available for family planning, maternal, and reproductive health activities.”
xi – The explanatory statement accompanying the FY20 Conference Agreement states that the “agreement includes authority to reprogram $10,000,000 of Global Health Program funds to the Emergency Reserve Fund if necessary to replenish amounts used during fiscal year 2020 to respond to emerging health threats.” The House FY21 appropriations bill states that “up to $50,000,000 of the funds made available under the heading ‘Global Health Programs’ may be made available for the Emergency Reserve Fund.” The FY21 Senate bill text states that “up to $25,000,000 of the funds made available under the heading ‘Global Health Programs’ may be made available for the Emergency Reserve Fund.”
xii – The House FY21 appropriations bill states that of the GHP funding provided to USAID, “not less than $200,000,000 shall be available for grants or contributions to the World Health Organization, which shall be allocated and allotted not later than 60 days after the date of enactment of this Act.”
xiii – In FY20, the administration proposed to formally transfer $7.2 million from the “HIV/AIDS, Viral Hepatitis, STI and TB Prevention” account to “Global Tuberculosis” activities under “Global Health Programs” at CDC. The FY20 conference agreement formalizes this transfer.
[i] Total funding for global health is not currently available as some funding provided through USAID and DoD is not yet available.
New coronavirus cases in the United States have hit daily records multiple times in the past week and hospitalizations are rising in several areas of the country. Health care workers face some of the greatest risk of exposure to the coronavirus and a new KFF brief examines the composition of the workforce and how the risks and the impact of the pandemic on this workforce vary across racial/ethnic groups. With prospects for a successful vaccine in the coming months, the brief also examines the overall impact the pandemic is having on health care workers as well as their attitudes towards taking a COVID-19 vaccine.
While 60% of health workers are White, people of color accounted for the majority of COVID-19 cases and deaths among health workers based on available data.
Studies suggest that, among health care workers, people of color are more likely to be in roles and settings that pose particularly high risk of exposure to coronavirus, including providing direct patient care or support in inpatient hospital or residential or long-term care settings and reporting inadequate access to PPE.
While over half (54%) of health care workers say they would definitely get a free, safe and effective vaccine, Black adults with a health worker in their household are much less likely than comparable White adults to say they would definitely get vaccinated (24% vs. 46%).
Health care workers face potential COVID-19 exposure through their job. Data suggest that at least 200,000 health care workers have been infected with coronavirus as of November 2020, but this estimate likely vastly underestimates the number affected due to major gaps in data collection. Data further show that people of color account for the majority of COVID-19 cases and deaths known among health care workers, and that they are more likely to be in health care worker roles and settings that have particularly high risks of workplace exposure. This analysis provides greater insight into COVID-19 risks and impacts among health care workers and how they vary by race and ethnicity. It is based on a KFF analysis of 2019 American Community Survey and publicly available information on COVID-19 impacts among health care workers (see Methods for more details). It finds:
In 2019, there were over 18.6 million people working in the health care industry across a range of occupations and settings. Overall, 60% of health care workers were White and 40% were people of color, including 16% who were Black, 13% who were Hispanic, and 7% who were Asian. However, the racial/ethnic composition of health care workers varied across occupations and settings. Black and Hispanic health care workers made up relatively larger shares of aides and personal care workers and direct contact support workers. Black and Hispanic workers also accounted for larger shares of health care workers in home health care, and Black workers made up a relatively larger share of workers in skilled nursing facility or other residential care settings.
People of color account for the majority of COVID-19 cases and/or deaths known among health care workers for which race/ethnicity data are available. The Centers for Disease Control and Prevention (CDC) reported over 200,000 cases and just over 790 deaths among health care personnel as of November 9, 2020. However, this estimate likely vastly underestimates the number of health care workers affected as health care personnel status was known for only a quarter (25%) of total cases. CDC further found that, as of July 2020, more than half (53%) of confirmed cases among health care personnel were among people of color, including 26% who were Black, 12% who were Hispanic, and 9% who were Asian. Data collected by states, the media, and other organizations similarly find that people of color account for the majority of COVID-19 cases and/or deaths known among health care workers.
Research suggests that health care workers face increased risks of coronavirus exposure and infection, with certain health care workers facing particularly high risks that disproportionately affect people of color. Studies show that health care workers are at increased risk for exposure and infection relative to the general population, with particularly high risks for health care workers who provide direct patient care, work in inpatient hospital or residential or long-term care settings, are in nursing or direct support staff roles, or do not have adequate access to PPE.1 Research further suggests that, among health care workers, people of color are more likely to report reuse of or inadequate access to PPE and to work in clinical settings with greater exposure to patients with COVID-19. CDC analysis of antibody evidence of previous infection among health care personnel further found higher rates of seropositivity among people or color compared to their White counterparts (9.7% vs. 4.4%), suggesting higher rates of previous infection.
A recent KFF/The Undefeated Survey suggests that the pandemic is taking a disproportionate toll on health care workers, especially Black health care workers and their families. It finds that health care workers are more likely than others to worry about being exposed to the virus through the workplace, to know someone who has died from the virus, to say it has negatively impacted family relationships, and to report someone in their household lost a job or experienced a cutback in hours or income due to the pandemic. Black health care workers and their families are particularly likely to report certain impacts, including knowing someone who has died from the virus and a negative impact on their ability to pay for basic needs.
KFF/The Undefeated Survey data also show that, while health care workers are more likely than others to say they would definitely get a COVID-19 vaccine, substantial shares express vaccine hesitancy, particularly among Black health care workers and their families. Overall, 54% of health care workers say they would definitely get vaccinated if it was available for fee and determined safe and effective by scientists, compared to 33% of adults who do not have a health care worker in their household. However, among adults who are health care workers or who live in a household with a healthcare worker, Black adults are much less likely to say they would definitely get vaccinated compared to White adults (24% vs. 46%), mirroring greater vaccine hesitancy among Black adults more broadly.
Together these findings highlight the importance of focusing on health care workers as part of response efforts to help protect against COVID-19 infection and spread. They can also help target response efforts and distribution of treatments and vaccines as they become available to prioritize health care workers who are facing the highest risks of exposure and infection. Targeting these efforts will also have important implications for health disparities given the disproportionate risks and impacts among health care workers who are people of color, which may compound broader increased health and economic risks that are contributing to the pandemic’s disproportionate toll on people of color overall. This analysis also shows that there remain significant gaps in data to understand COVID-19 impacts by industry and occupation. Increased data would allow for better understanding of work-related risks and outbreaks to help guide response efforts and resources going forward.
Issue Brief
Overview of Health Care Workers
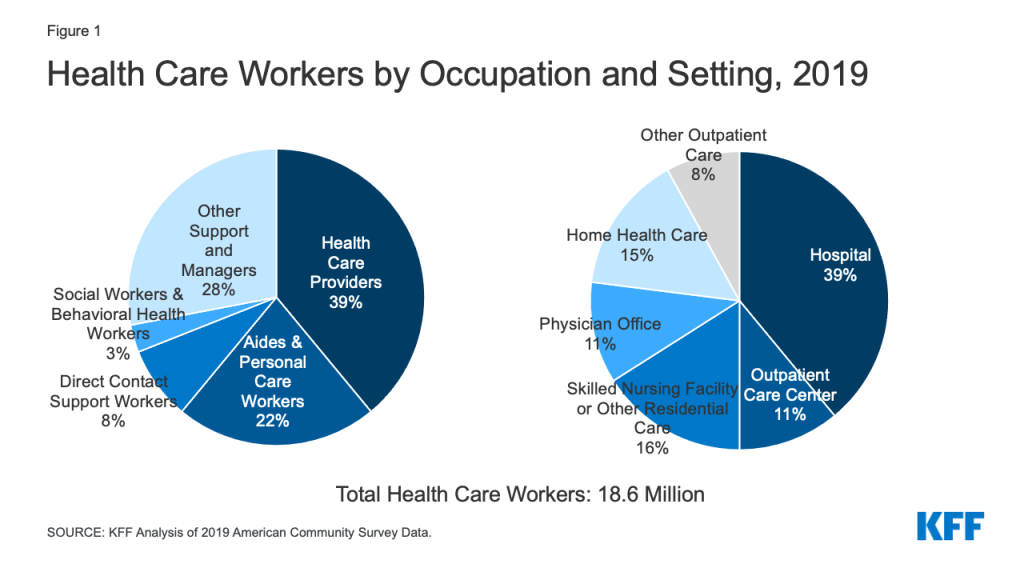
As of 2019, there were over 18.6 million people working in the health care industry. Health care workers face potential risk of exposure to COVID-19 through their job, but this risk may vary based on the type and setting of their work. Overall, nearly four in ten (39%) health care workers were health care providers such as nurses, physicians, technicians, and therapists; 22% were aides and personal care workers, such as certified nursing assistants, home health aides, and medical assistants; 8% were direct contact support workers, such as housekeeping and kitchen and cafeteria staff; and 3% were social workers and behavioral health workers (Figure 1). The remaining 28% were other support workers and managers, such as office and administrative managers and staff, who may have less direct contact with patients. Nearly four in ten (39%) worked in a hospital, 16% worked in a skilled nursing facility or other residential care, 11% worked in an outpatient care center, 11% worked in a physician office, 15% worked in home health care, and the remaining 8% worked in other health care service settings such as a dentist, optometrist or chiropractor offices.
Figure 1: Health Care Workers by Occupation and Setting, 2019
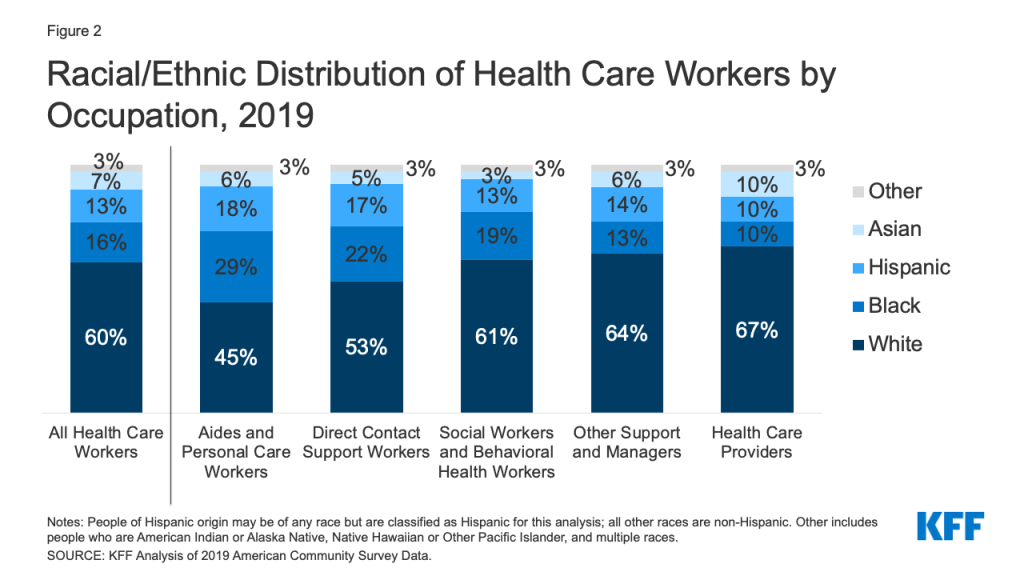
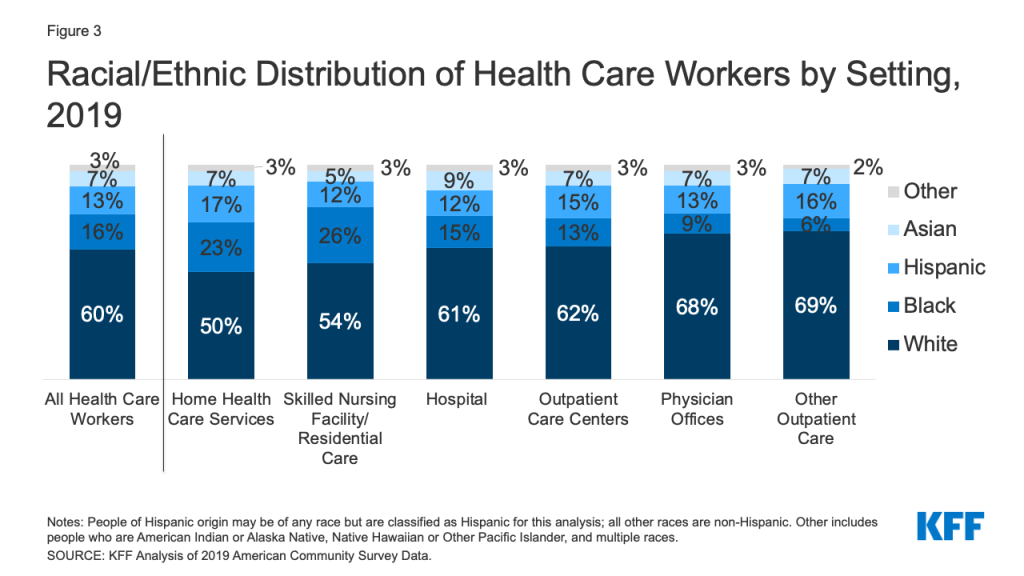
The racial/ethnic make-up of health care workers varied by occupation and health care setting. Overall, 60% of health care workers were White and 40% are people of color, including 16% who were Black, 13% who were Hispanic, and 7% who were Asian. However, Black and Hispanic health care workers made up relatively larger shares of aides and personal care workers and direct contact support workers and accounted for fewer health care providers (Figure 2). Similarly, Black and Hispanic workers made up larger shares of health care workers in home health care (23%), and Black workers accounted for over a quarter of workers in skilled nursing facility or other residential settings (26%) (Figure 3).
Figure 2: Racial/Ethnic Distribution of Health Care Workers by Occupation, 2019Figure 3: Racial/Ethnic Distribution of Health Care Workers by Setting, 2019
COVID-19 Among Health Care Workers
Cases, Hospitalizations, and Deaths
Some federal, state, and other data are available on COVID-19 infections and deaths among health care workers, but significant data gaps remain:
The Centers for Disease Control and Prevention (CDC) reported over 200,000 cases and just over 790 deaths among health care personnel as of November 9, 2020. However, health care personnel status was only known for less than a quarter of total cases, and death status was available for less than three-quarters of cases among health care personnel.
KFF review of state websites identified 16 states reporting over 144,000 COVID-19 cases among health care workers as of November 2020.2 However, states varied widely in how they defined and identified health care workers. Further, in most cases, it was not clear what share of total cases had health care worker status known. Some counties also report data for health care workers. For example, Los Angeles County reported over 17,000 positive cases and 105 deaths among health care workers and first responders as of October 29, 2020.
Media and other organizations have also undertaken efforts to track COVID-19 deaths among health care workers. For example, reporting by Kaiser Health News and the Guardian has identified over 1,300 likely deaths among health care workers related to COVID-19 as of November 9, 2020. National Nurses United estimated that, as of September 16, 2020, 1,718 health care workers, including 213 registered nurses, had died of COVID-19 and related complications based on media reports, social media, obituaries, union memorials, federal and state reporting, and internal reporting.
These data likely underestimate COVID-19 impacts among health care workers given that the majority of cases and deaths are missing information on health care worker status. CDC analysis of antibody evidence of previous infection further suggests that a high proportion of COVID-19 infections among health care personnel go undetected.
People of color accounted for a majority of COVID-19 infections, hospitalizations, and deaths known among health care workers for which race/ethnicity data is available. CDC found that, as of July 2020, more than half (53%) of confirmed cases among health care personnel were among people of color, including 26% who were Black, 12% who were Hispanic, and 9% who were Asian. Separate CDC analysis of hospitalization data, found that most health care personnel hospitalized with COVID-19 were people of color, including over half (52%) who were Black and nearly 9% who were Hispanic. Data from Los Angeles County show that, among the over 17,000 health care workers and first responders who were identified as positive for COVID-19 as of late October 2020, 50% were Hispanic, 15% were Asian, and 7% were Black. Moreover, among the 105 health care workers and first responders who died, 45% were Hispanic and 37% were Asian. Kaiser Health News and the Guardian tracking of health care worker deaths associated with COVID-19 further finds that a majority of deaths were among people of color. Similarly, National Nurses United found that over half (58%) of the 213 registered nurses it had identified as dying due to COVID-19 and related complications were nurses of color, including nearly a third (32%) who were Filipino nurses and 18% who were Black nurses.
Risks of Exposure and Infection
Analysis suggests health care workers are at increased risk for COVID-19 infection relative to the general population and that certain health care workers are at particularly high risk. A United States and United Kingdom study found higher prevalence of COVID-19 infections among frontline health care workers (i.e., those who reported direct patient contact) compared to the general community, with the highest risks for those working in inpatient hospital settings and nursing homes, reporting inadequate personal protective equipment (PPE), and caring for patients with documented COVID-19. CDC analysis of health care providers in Minnesota found that two-thirds (66%) of higher-risk exposures to COVID-19—defined as close contact for 15 minutes or more or during an aerosol-generating procedure—involved direct patient care, while roughly one-third (34%) were through nonpatient contacts, such as interactions with coworkers and social or household contacts. It also found that health care personnel working in congregate living or long-term care settings, including skilled nursing facilities, were less likely to wear appropriate PPE, worked more often while symptomatic, and were more likely to test positive following a higher-risk exposure compared to those working in acute care settings. Other CDC analysis found that more than two-thirds (67%) of health care personnel who were hospitalized with COVID-19 were in roles that likely required direct patient contact, and over one-third (36%) were in nursing-related occupations. Similarly, Kaiser Health News and the Guardian tracking of COVID-19 deaths among health care workers found that nurses and support staff accounted for the largest numbers of deaths.
Research further suggests that, among health care workers, people of color are more likely to face elevated risks of workplace exposure. As noted earlier, Black and Hispanic workers make up relatively larger shares of aides and personal care workers and direct contact support workers who typically are engaged in direct patient care, which is associated with increased risk of infection. Moreover, Black workers make up over a quarter of workers in skilled nursing facility or other residential settings, which pose higher risks of infection and have been sources of a significant share of cases. The United States and United Kingdom study also found that, among frontline health care workers, people of color were at especially high risk of infection and were disproportionately likely to report reuse of or inadequate access to PPE and to work in clinical settings with greater exposure to patients with COVID-19. Further, it found that Black, Asian, and other frontline workers of color had increased risk of a positive COVID-19 test compared to their White counterparts. CDC analysis of antibody evidence of previous infection among health care personnel also found higher rates of seropositivity among people or color compared to their White counterparts (9.7% vs. 4.4%), suggesting higher rates of previous infection.
Health and Financial Impacts of the Pandemic
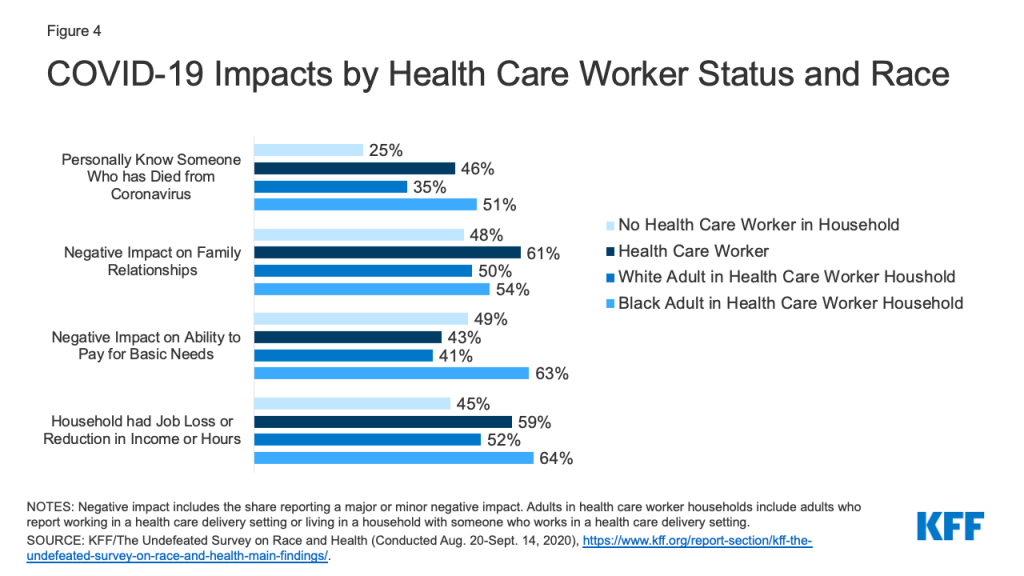
A recent KFF/The Undefeated Survey suggests that the pandemic is taking a disproportionate toll on health care workers, especially among Black health care workers and their families. Health care workers were more likely than adults who live in a household without any health care workers to be worried that they might be exposed to coronavirus at work (67% vs. 50%), to personally know someone who has died from coronavirus (46% vs. 25%), and to say the pandemic has had a negative impact on their relationships with family members (61% vs. 48%) (Figure 4). Health care workers also were more likely than adults living in a household without a health care worker to say that someone in their household has lost a job, been placed on furlough, or had their hours or income reduced as a result of the pandemic (59% vs. 45%), but they were not more likely to say it had a negative impact on their ability to pay for basic needs (43% vs. 49%). Among adults who are health care workers or who live in a household with a health care worker, Black adults were more likely compared to their White counterparts to report knowing someone who has died from coronavirus (51% vs. 35%) and to say that the pandemic negatively affected their ability to pay for basic necessities (63% vs. 41%).
Figure 4: COVID-19 Impacts by Health Care Worker Status and Race
COVID-19 Vaccine Attitudes
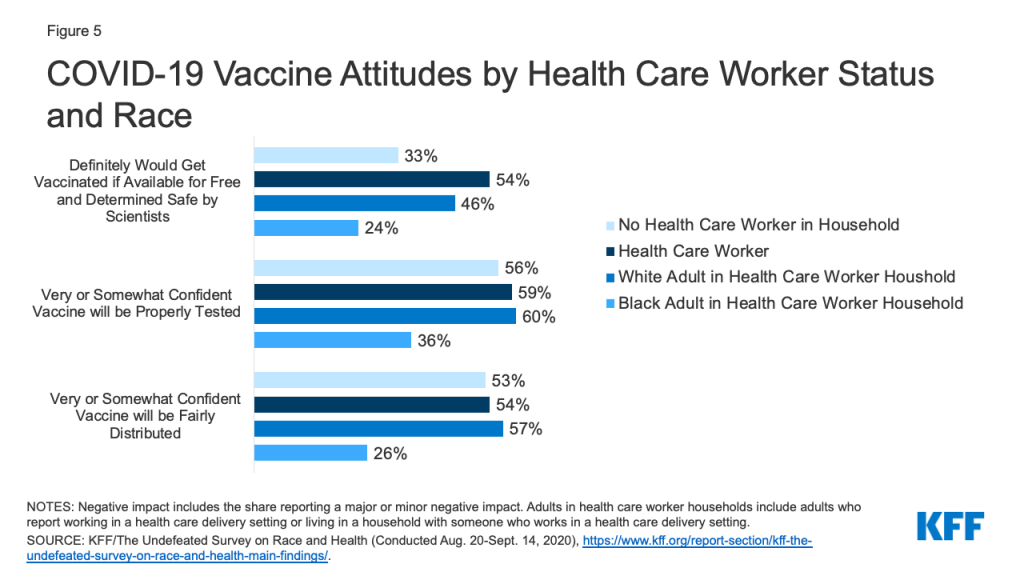
The KFF/The Undefeated survey also found that health care workers are more likely than others to say they would definitely take a vaccine if it was available for fee and determined safe and effective by scientists, but there are still substantial shares who say they would probably or definitely not get vaccinated, particularly among Black adults. Overall, 54% of health care workers say they would definitely get vaccinated, compared to 33% of adults who do not have a health care worker in their household (Figure 5). However, among adults who are health care workers or who live in a household with a healthcare worker, Black adults are much less likely to say they would definitely get vaccinated compared to White adults (24% vs. 46%), mirroring greater vaccine hesitancy among Black adults more broadly. Among health care workers and their family members, Black adults also express less confidence that a vaccine will be tested properly and distributed fairly compared to their White counterparts.
Figure 5: COVID-19 Vaccine Attitudes by Health Care Worker Status and Race
Implications
Health care workers face risk of COVID-19 exposure through their workplace. Data provide some estimates of cases and deaths among health care workers and show that people of color account for the majority of health care workers affected by COVID-19. However, the data likely vastly underestimate impacts among health care workers. Research suggests that health care workers are at increased risk of exposure and infection compared to the general population and that most high-risk exposures among health care workers occur through the workplace. However, risks are not equally shared across health care workers. Analysis suggests that frontline workers providing direct care in certain settings and those with inadequate access to PPE face particularly high risks. Moreover, among health care workers, people of color are more likely to face these elevated workplace risks, which may compound broader increased health and economic risks that are contributing to the pandemic’s disproportionate toll on people of color.
Together these findings highlight the importance of focusing on health care workers as part of response efforts to help protect against infection and spread. They can also help target response efforts and distribution of treatments and vaccines as they become available to prioritize health care workers who are facing the highest risks of exposure and infection. Targeting these efforts will also have important implications for health disparities given the disproportionate risks and impacts among health care workers who are people of color. This analysis also shows that there remain significant gaps in data to understand COVID-19 impacts by industry and occupation. Increased data would allow for better understanding of work-related risks and outbreaks to help guide response efforts and resources going forward.
Methods
This analysis is based on KFF analysis of the 2019 American Community Survey (ACS), 1-year file. The ACS includes a 1% sample of the US population, the subset used here includes over 170,000 observations. The health care industry is defined as industry codes 7970 through 8290, and does not include the childcare or vocational training industries. For more information see here.
Industry Classification
Industry Code
Title
Classification
7970
Offices of physicians
Offices of physicians
7980
Offices of dentists
Other Outpatient
7990
Offices of chiropractors
Other Outpatient
8070
Offices of optometrists
Other Outpatient
8080
Offices of other health practitioners
Other Outpatient
8090
Outpatient care centers
Outpatient care centers
8170
Home health care services
Home health care services
8180
Other health care services
Home health care services
8191
Hospital
General or MH Hospital
8192
Psychiatric and substance abuse hospitals
General or MH Hospital
8270
Skilled nursing facilities
SNF & Care Facility
8290
Residential care facilities
SNF & Care Facility
We define the healthcare workforce as all individuals who earned at least $1,000 during the year and indicated that their job was in one of the industry codes listed above. Within these industry groups, we grouped people’s occupations into five different categories based on type of work and level of contact with patients:
Aides and personal care workers includes certified nursing assistants (CNAs), personal care aides, home health aides, licensed practical nurses (LPNs), OT and PT assistants, medical assistants, and other aides.
Direct contact support workers includes non-clinical support staff, such as housekeeping and janitorial staff, kitchen and cafeteria staff, recreation workers, laundry workers, security guards, shuttle drivers, clergy, and first-line supervisors of support workers.
Health care providers includes registered nurses (RNs), physicians, dental assistants, physician therapists, occupational therapists, nurse practitioners, dentist, radiologist, phlebotomists, and various types of technicians that provide direct patient care.
Other support workers and managers includes office and administrative managers and staff, receptionists, nutritionists, laboratory technicians, office clerks, billing clerks, medical records specialist, human resources, groundskeeping and facilities workers, who are likely to come into regular direct contact with patients less often than other types of health care workers.
Social Workers and Behavioral health workers includes health professions such as Social workers, Mental health counselors and substance abuse counselors
Note, that this analysis only includes those in the healthcare industry, therefore healthcare professionals working in other care settings, such as school nurses are not included.
States reporting COVID-19 cases among health care workers include: AL, AR, CO, GA, ID, MA, MN, NH, OH, OK, OR, SC, UT, VT, VA, and WA. Dates for which cases are reported through vary across states. Total cases among Colorado health care workers includes confirmed COVID-19 cases among staff in any health care setting, based on active and resolved outbreak data. ↩︎
Recent trends in maternal and infant health and persistent racial disparities in these measures have led to a growing focus on improving health and reducing disparities in these areas, which has been heightened by the COVID-19 pandemic and growing racial justice movement. As a primary source of coverage for pregnant women and children, particularly among people of color, Medicaid can play a key role in helping to improve maternal and infant health and reducing racial disparities. This brief provides a summary of Medicaid’s role for pregnant women and infants and current Medicaid initiatives to improve maternal and infant health. It finds:
Medicaid, along with the Children’s Health Insurance Program (CHIP), provide a nationwide base of coverage for low-income pregnant women and children. Reflecting this coverage, nearly half of births (45%) are covered by Medicaid and nearly half of all infants (46%) are covered by Medicaid or CHIP. The programs play an even larger role for people of color given that they have more limited access to private coverage and lower incomes compared to their White counterparts. For example, Medicaid covers about two-thirds of births among Black, American Indian or Alaska Native (AIAN), and Native Hawaiian or Other Pacific Islander (NHOPI) women and over six in ten Black, Hispanic, and AIAN infants are covered by Medicaid or CHIP.
The Affordable Care Act (ACA) Medicaid expansion has led to improvements in and narrowed racial disparities in maternal and infant health. Through the ACA Medicaid expansion to low-income adults, states have increased coverage options for pregnant women who would otherwise lose eligibility at the end of the 60-day postpartum period, although some still may lose coverage at the end of the period. Studies show that the Medicaid expansion has had positive impacts on maternal and infant access to and use of care and health outcomes and narrowed racial disparities in certain measures including health coverage, maternal mortality, infant mortality, low birthweight, and preterm birth.
There are a range of Medicaid initiatives underway at the state and federal level to improve maternal and infant health. There has been interest at the state and federal level in extending the postpartum Medicaid eligibility period to further reduce coverage losses for women at the end of the period. In addition, there are efforts to expand benefits and implement new payment and delivery models. These efforts may not only contribute to improvements in maternal and infant health but also reduce racial disparities in these areas due to the large role the program plays for people of color.
Issue Brief
Introduction
Despite continued advancements in medical care, rates of maternal mortality and morbidity and pre-term birth have been rising in the U.S. Maternal and infant mortality rates in the U.S. are far higher than those in similarly large and wealthy countries and stark racial disparities in maternal and infant health persist. Improving maternal and infant health is key for preventing unnecessary illness and death and advancing overall population health. Moreover, growing calls for racial justice and the disparate impact of the COVID-19 pandemic for people of color have brought a heightened focus to health disparities, including the inequities in maternal and infant health. In particular, there has been broader recognition of the principles of reproductive justice, which emphasize the role that the social determinants of health and other factors play in reproductive health for communities of color.
A range of initiatives are underway that are designed to improve maternal and infant health and reduce disparities. Medicaid is key in these efforts given the substantial role the program plays in covering low-income pregnant women and children, particularly among people of color. This brief provides a summary of Medicaid’s role for pregnant women and infants and key Medicaid initiatives to improve maternal and infant health.
Medicaid’s Role for Pregnant Women and Infants
Medicaid provides a nationwide base of coverage for low-income pregnant women and children. Under federal rules, all states must extend Medicaid eligibility for pregnant women and children to at least 138% of the federal poverty level (FPL) ($29,974 per year for a family of three as of 2020). States can extend eligibility to higher levels through options in Medicaid as well as CHIP. As of January 2020, nearly all states (49 including DC) cover infants with family incomes up to at least 200% FPL ($43,440 per year for a family of three) through Medicaid and CHIP. Moreover, nearly all states (49) extend eligibility for pregnant women beyond the federal minimum of 138% FPL, with 35 extending eligibility to at least 200% FPL. Infants born to mothers on Medicaid are automatically covered for their first of life, while coverage for pregnant women ends after 60 days postpartum.
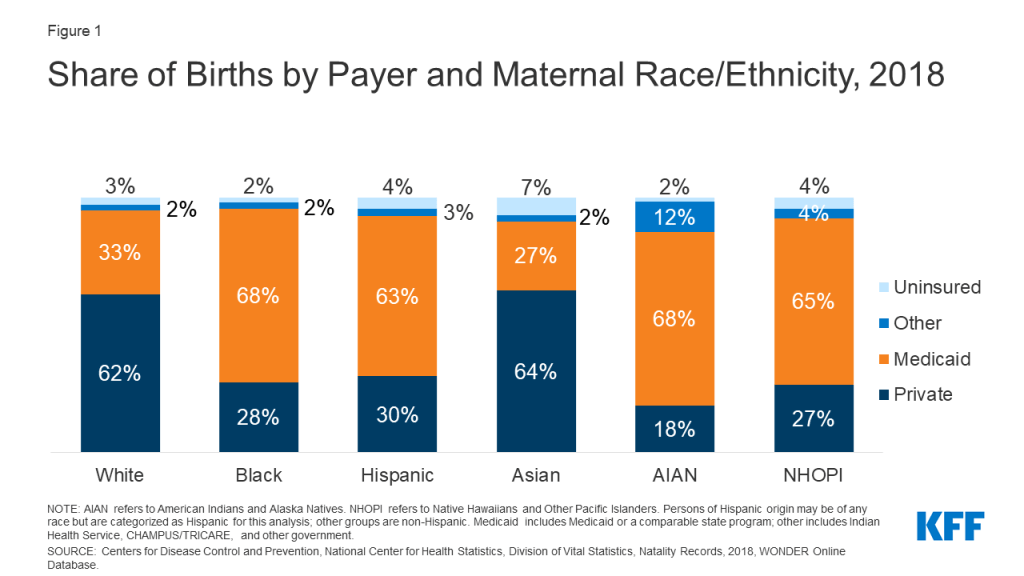
Reflecting this broad base of eligibility for pregnant women, Medicaid covers 45% of all births. The programs play an even larger role in covering births for women of color given their lower incomes and more limited access to private coverage. Medicaid covers about two-thirds of births among Black, AIAN, and NHOPI women and six in ten births among Hispanic women, compared to one in three births among White women (Figure 1).
Figure 1: Share of Births by Payer and Maternal Race/Ethnicity, 2018
Medicaid, along with CHIP, also cover nearly half (46%) of all infants, and the programs play a particularly large role covering infants of color. Over six in ten Black, Hispanic, and AIAN infants are covered by Medicaid and CHIP compared to one-third of White infants (Figure 2). Even with these higher rates of Medicaid and CHIP coverage, Hispanic and AIAN infants remain more likely to be uninsured compared to White infants.
Figure 2: Health Coverage among Infants (Ages 0-1) by Race/Ethnicity, 2019
Medicaid Expansion Effects on Maternal and Infant Health
Through the ACA Medicaid expansion to low-income adults, states have increased coverage options for pregnant women who would otherwise lose eligibility at the end of the postpartum period. As noted, under federal rules, states must extend Medicaid eligibility to pregnant women with incomes up to at least 138% FPL and provide this coverage through 60 days postpartum. Nearly all states have expanded pregnant women eligibility beyond the minimum level, with the median eligibility level at 255% FPL as of January 2020. Prior to the ACA, many pregnant women would lose coverage at the end of the 60-day postpartum period because state eligibility levels for parents were much lower compared to the levels for pregnant women—below half of poverty in many states. The ACA expanded Medicaid eligibility to nearly all adults with incomes up to 138% FPL, increasing coverage options for pregnant women at the end of the postpartum period in expansion states. As of August 2020, 39 states, including DC, have adopted the Medicaid expansion.
Studies suggest that the ACA Medicaid expansion has had positive impacts on maternal and infant access to and use of care and health outcomes and helped to narrow racial disparities in certain measures. For example, one study found increased coverage stability and use of postpartum care during the six months postpartum in a Medicaid expansion state compared to a neighboring non-expansion state.1 Another study found that infants in non-expansion states are approximately two and half times more likely to be born into a household without health insurance compared to infants in expansion states.2 Several studies suggest that Medicaid expansion has narrowed disparities for Black and Hispanic people in certain measures of maternal and infant health, including health coverage, maternal mortality, infant mortality, low birthweight, and preterm birth.3,4, 5,6
Even with the ACA Medicaid expansion, many women still may lose coverage at the end of the 60-day postpartum coverage period. Eligibility levels for pregnant women remain higher than those for parents in both expansion and non-expansion states, with the starkest differences in non-expansion states (Figure 3). Analysis finds that nearly half of women in non-expansion states and nearly one in three women in expansion states experience an insurance disruption from pre-pregnancy to postpartum.7 Another study on maternal insurance status during the preconception, delivery, and postpartum periods found that women of color experienced higher uninsured rates during each period compared to White women, and that disruptions in coverage disproportionately affected Hispanic, Black, and AIAN women.8
Figure 3: Median Medicaid Income Eligibility Limits based on Implementation of Medicaid Expansion as of September 2020
Medicaid Efforts to Improve Maternal and Infant Health
There has been interest at the state and federal level in extending the postpartum Medicaid eligibility period to further reduce coverage losses for women in the postpartum period. Extending the postpartum Medicaid eligibility period would increase state and federal spending, but could help reduce preventable maternal deaths and improve maternal health outcomes considering that approximately 30% of maternal deaths (excluding those caused by suicide or overdose) occur 43 to 365 days postpartum.9 One analysis estimates that approximately 217,000 uninsured low-income new mothers would benefit from the extended postpartum period.10
As of November 2020, several states are pursuing action to extend the postpartum period. In many cases, this activity is still in the planning stage or has been set aside as the COVID-19 pandemic response takes fiscal priority in state budgets. However a few states have developed specific proposals. As of August 1, 2020, California has allocated $34.3 million in state funds to extend postpartum coverage for women diagnosed with a mental health condition. Georgia has allocated $19 million in state funding to extend coverage to 6 months postpartum, and Texas is offering a set of postpartum care services for up to 12 months for women who are eligible for the state’s family planning program. Indiana is requesting Section 1115 waiver authority to extend postpartum coverage to one year for mothers with opioid use disorder.
Federal legislative proposals also have emerged. The Helping Medicaid Offer Maternity Services (MOMS) Act of 2020, which was passed by the House in September 2020, would provide a new state option to extend coverage for one year postpartum and increase the federal matching rate for states to take up the option. The Congressional Black Maternal Health Caucus has introduced a package of bills known as the Momnibus aimed at stemming maternal health disparities that includes measures such as diversifying the perinatal workforce and greater investment in social determinants of health. Notably, as part of COVID-19 response efforts, legislation requires states to provide continuous enrollment to Medicaid enrollees as a condition of receiving enhanced federal funding. This provision is designed to help protect against coverage losses during the pandemic, and states cannot disenroll pregnant women at the end of the postpartum period for during the public health emergency.
Most state Medicaid programs report being engaged in efforts to advance maternal and infant health. In a recent KFF survey, about two-thirds of states reported new or expanded Medicaid initiatives in FY 2019 or planned for FY 2020 to improve birth outcomes and/or address maternal mortality, with over a quarter of states focused on pregnant women with substance use disorder (SUD). These include efforts to expand eligibility for pregnant women, expand Medicaid coverage for perinatal services, and implement payment and delivery models that incentivize improvements in maternal care and outcomes.11 Some state Medicaid programs also offer benefits specifically for pregnant women such as behavioral health services, dental services, and home visiting services.12 Several states are engaged in efforts to include Medicaid coverage for doula services. Research suggests that doula services can improve health outcomes for women and infants, reduce interventions during delivery, and facilitate communication between pregnant women and health care providers.13 Having a trained advocate can be particularly important for women of color, who are more likely to encounter discrimination in the health care system. Currently, two states (Oregon, Minnesota) allow doulas to participate in their Medicaid networks statewide and other states are testing pilot programs to assess the feasibility of broader coverage. An important component for incorporating doulas in the Medicaid program is assuring adequate and timely reimbursement, which has been a challenge in some pilot programs.14
The Centers for Medicare and Medicaid Services (CMS) has launched recent initiatives focused on addressing maternal and infant health. In 2019, the Center for Medicare and Medicaid Innovation (CMMI) awarded grants to ten states (Colorado, Indiana, Louisiana, Maryland, Maine, Missouri, New Hampshire, Tennessee, Texas, and West Virginia) for its new Maternal Opioid Misuse Model, which is intended to address the fragmented care of pregnant and postpartum persons with opioid use disorder.15 It also recently released a request for information seeking input on opportunities to improve health care access, quality, and outcomes for women and infants in rural communities before, during, and after pregnancy. Further, CMS recently released its 2020 Maternity Core Set of 11 measures for voluntary reporting by state Medicaid and CHIP agencies to help evaluate maternal and perinatal health in Medicaid and CHIP.
Outside of Medicaid, the federal government, states, providers and health systems, foundations, and communities also are engaged in a broad range of efforts to advance maternal and child health and reduce disparities. For example, some Medicaid initiatives are part of broader statewide approaches to advance maternal health and reduce disparities. Moreover, outside of Medicaid, the federal government provides funding for and engages in efforts to advance maternal and infant health through the Maternal and Child Health Block Grant, the Health Resources and Services Administration, the CDC, and other agencies. The CDC recently launched the Hear Her campaign to support improved communication between pregnant and postpartum women and maternity providers, which is particularly important given the growing recognition of the role racism plays in contributing to adverse maternal health outcomes. Several states have perinatal and maternal quality collaboratives as well as maternal mortality review committees that collect and analyze data on maternal and infant health outcomes and work to improve health care delivery for women and infants. Several of these committees have focused on collecting local data by race and ethnicity, highlighting differences by both race/ethnicity and geography. Improved data collection and analysis are important tools for identifying and understanding the disparate outcomes between different subpopulations as well as for developing and targeting quality improvement initiatives within the delivery system.16 In 2019, California became the first state to require perinatal providers to obtain training on implicit bias. Further, the city of San Francisco recently launched a project that gives a group of Black and Pacific Islander pregnant persons an income supplement during pregnancy and through the infant’s first six months of life to help address some of the known health and income inequities.17
Conclusion
Maternal and infant mortality rates in the U.S. are far higher than those in similarly large and wealthy countries, and stark racial disparities in maternal and infant health persist. The COVID-19 pandemic further highlights the urgency and importance of addressing health disparities in health care more broadly, and maternal and infant health specifically.
Healthy birth outcomes and early identification and treatment of health conditions among mothers and infants helps to prevent death and illness and advance overall population health. Healthy People 2030, which provides 10-year national health objectives to set the national public health agenda, identifies the prevention of pregnancy complications and maternal deaths and improvement of women’s health before, during, and after pregnancy as a public health goal.18 Pregnancy and birth provide opportunities to identify health risks in women and children. Moreover, early identification and treatment of health conditions or complications can prevent death and disability in both mother and child, enable children to reach their full potential, as well as improve overall population health. Recent research finds that as many as 60% of all maternal deaths in the U.S. are preventable and that increasing access to preconception, prenatal, and interconception care can reduce pregnancy-related complications.19
As a primary source of coverage for pregnant women and infants, particularly among people of color, Medicaid is key to improving maternal and infant health and reducing racial disparities. A number of efforts are underway through Medicaid to improve maternal and infant health, including efforts to provide more continuous coverage, expand benefits, and implement new payment and delivery models. However, coverage is only one factor affecting maternal and infant health, and there is growing recognition that it is important for efforts to improve health and reduce racial disparities to address broad social and economic factors that influence health and racism and discrimination.
Endnotes
Sarah H. Gordon, Benjamin D. Sommers, Ira B. Wilson, and Amal N. Trivedi, “Effects Of Medicaid Expansion On Postpartum Coverage And Outpatient Utilization,” Health Affairs 39, no. 1 (January 2020): 77-84, https://doi.org/10.1377/hlthaff.2019.00547↩︎
Scott R. Sanders et al., “Infants without health insurance: Racial/ethnic and rural/urban disparities in infant households’ insurance coverage,” PLOS One 15, no. 1 (January 2020): e0222387, https://doi.org/10.1371/journal.pone.0222387↩︎
Clare Brown et al., “Association of State Medicaid Expansion Status With Low Birth Weight and Preterm Birth,” Journal of the American Medical Association 321, no. 16 (April 2019), https://jamanetwork.com/journals/jama/fullarticle/2731179↩︎
Erica Eliason, “Adoption of Medicaid Expansion Is Associated with Lower Maternal Mortality,” Women’s Health Issues 30, no. 3 (May-June 2020): 147-152, https://doi.org/10.1016/j.whi.2020.01.005↩︎
Donna L. Hoyert and Arialdi M. Miniño, “Maternal Mortality in the United States: Changes in Coding, Publication, and Data Release 2018,” National Vital Statistics Reports 69, no. 2 (January 2020): 1-18, https://www.cdc.gov/nchs/data/nvsr/nvsr69/nvsr69-02-508.pdf↩︎
Amy Chen, Alexis Robles-Fradet, and Helen Arega, Building A Successful Program for Medi-Cal Coverage for Doula Care: Findings from A survey of Doulas in California, National Health Law Program, May 21, 2020, https://healthlaw.org/resource/doulareport/↩︎
Here’s our recap of the past week in the coronavirus pandemic from our tracking, policy analysis, polling, and journalism.
The U.S. saw an increase of over 662,000 cases and about 6,300 deaths this week and crossed its highest daily total for new cases since the pandemic began on Wednesday at 102,831.
While we waited to see whose administration may manage the coronavirus response in 2021, our new analysis looks at the challenge of distributing a COVID-19 vaccine across states by examining last season’s flu vaccination rate variation. Rhode Island had the highest vaccination rate at 61%, while Nevada had the lowest at 44%.
An examination of Medicaid and CHIP enrollment trends this year shows that that total enrollment in the programs grew to 75.5 million in July 2020, an increase of 4.3 million from actual enrollment prior to the coronavirus pandemic in February 2020. This likely reflects changes in the economy and provisions in the Families First Coronavirus Response Act that require states to ensure continuous coverage to current Medicaid enrollees in order for the states to access a temporary increase in the Medicaid match rate.
Here are the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: Total cases worldwide are over 48 million this week – with an increase of approximately 3.7 million new confirmed cases in the past seven days. There were over 52,000 new confirmed deaths worldwide and the total for confirmed deaths is over 1.2 million.
U.S. Cases and Deaths: Total confirmed cases in the U.S. is over 9.6 million this week. There was an increase of roughly 662,400 confirmed cases between October 30 and November 5. Approximately 6,300 confirmed deaths in the past week brought the total in the United States to nearly 235,000.
State Variation in Seasonal Flu Vaccination: Implications for a COVID-19 Vaccine (News Release, Issue Brief)
Analysis of Recent National Trends in Medicaid and CHIP Enrollment (Issue Brief)
Updated: COVID-19 Coronavirus Tracker – Updated as of November 5 (Interactive)
Updated: State Data and Policy Actions to Address Coronavirus (Interactive)
WHO Resumes World Health Assembly Cut Short In May, Hears Calls To Include Taiwan, Votes To Hold December Summit On COVID-19 Pandemic (KFF Daily Global Health Policy Report)
New analysis shows that, in 2019, the number of uninsured continued to increase for the third year in a row, rising to 28.9 million people. Much of the coverage loss between 2018 and 2019 was among Hispanic people, who already were at increased risk of being uninsured. These losses erode earlier coverage gains under the Affordable Care Act (ACA) that had narrowed longstanding disparities in health coverage. Since 2019, coverage losses have likely continued due to the economic downturn associated with the COVID-19 pandemic, which has taken a disproportionate toll on Hispanic people and other people of color. Together these data point to significant increased barriers to health care for Hispanic people, including children, that will likely lead to widening health disparities looking forward.
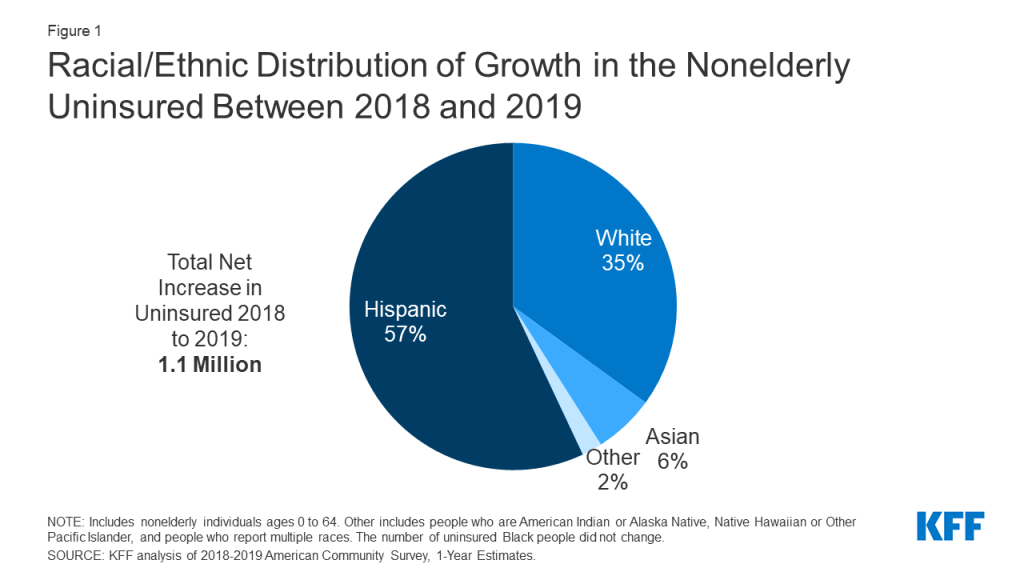
Between 2018 and 2019, the number of nonelderly uninsured Hispanic people grew by over 612,000, including nearly 217,000 children, from 10.3 to 10.9 million, accounting for over half (57.0%) of the 1.1 million increase in the total nonelderly uninsured(Figure 1). This coverage decline was primarily driven by a decline in Medicaid coverage. Between 2018 and 2019, the number of nonelderly Hispanic people covered by Medicaid fell by over 980,000 people, including 557,000 children, from 17.4 to 16.4 million, offsetting smaller gains in employer-sponsored coverage. Reflecting this coverage decline, the share of the total nonelderly uninsured who were Hispanic rose slightly from 36.9% to 37.6%. However, as of 2019, White people still made up the largest share of the total nonelderly uninsured (41.1%), while 13.4% were Black, 3.9% were Asian, and the remaining 4.0% were people of other races.
Figure 1: Racial/Ethnic Distribution of Growth in the Nonelderly Uninsured Between 2018 and 2019
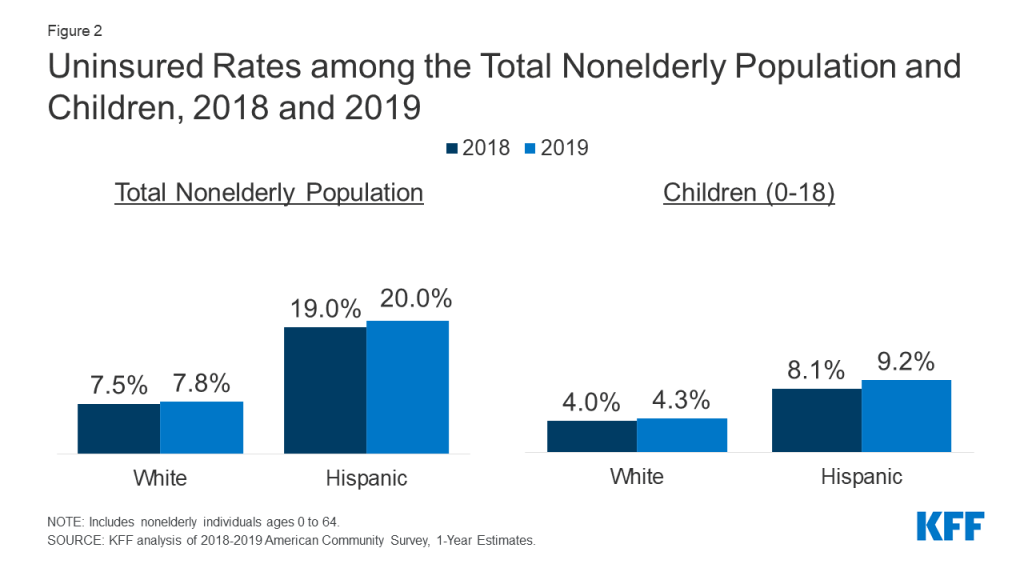
Reflecting these losses in coverage, the uninsured rate among nonelderly Hispanic people rose from 19.0% to 20.0% between 2018 and 2019 (Figure 2). As of 2019, their uninsured rate and was 2.5 times higher than the uninsured rate among the White nonelderly population (20.0% vs. 7.8%) (Figure 2). In addition, Hispanic children had the largest increase in their uninsured rate, which grew from 8.1% in 2018 to 9.2% in 2019, and was over twice as high as the rate for White children as of 2019 (9.2% vs. 4.3%).
Figure 2: Uninsured Rates among the Total Nonelderly Population and Children, 2018 and 2019
These coverage losses erode previous coverage gains under the ACA that had helped narrow longstanding disparities in coverage. Between 2010 and 2016, Hispanic individuals had the largest percentage point decrease in their uninsured rate, which fell from 32.6% to 19.1% among the nonelderly population, although they remained over 2.5 times more likely than their White counterparts to be uninsured (19.1% vs. 7.1%). These coverage gains stalled and began to reverse for some groups between 2016 and 2018.
Recent coverage losses among Hispanic people likely, in part, reflect growing immigration-related fears due to changes in immigration policy. The recent growth in the number of uninsured is likely due to a combination of factors, including rollback of outreach and enrollment efforts for ACA coverage, changes to Medicaid renewal processes, and elimination of the individual mandate penalty for health coverage. In addition, research suggests that recent changes to immigration policy, particularly changes to public charge policy, are contributing to growing fears among immigrant families about participating in public programs, including health coverage. In response to these fears, some immigrant families are avoiding enrolling themselves and/or their children in Medicaid or the Children’s Health Insurance Program (CHIP) or are disenrolling from or declining to renew their coverage despite being eligible.
The COVID-19 pandemic has likely contributed to additional coverage losses that will further widen disparities in coverage for Hispanic people. Data suggest that Hispanic people have been particularly hard hit by the economic fallout of the pandemic. Hispanic people have experienced large increases in unemployment, particularly among women, leading to widening gaps in employment compared to White people. Between the third quarter of 2019 and the third quarter of 2020, the unemployment rate for Hispanic people rose from 4.2% to 11.2%, while for White people it increased from 3.4% to 7.9%. Among Hispanic women, it rose from 4.8% to 12.5%, while the rate for White women rose from 3.7% to 8.6%. As people lose jobs, many may face disruptions in their health coverage since most people in the U.S. get their insurance through their job. While the ACA has provided coverage options for people losing employer-sponsored coverage who might otherwise become uninsured, enrollment in these options may be more limited among Hispanic people due to fears among immigrant families and other enrollment barriers. As such, Hispanic people face disproportionate risks of losing health coverage amid the pandemic that may exacerbate and further widen their gaps in health coverage.
Together these data show that Hispanic people experienced large coverage losses even before the economic upheaval of the pandemic. It is likely that they have had additional losses in coverage amid the pandemic because of high rates of job loss and increased barriers to enrolling in coverage, including immigration-related fears. These coverage losses come at the same time they are bearing a disproportionate burden of the health impacts of COVID-19 and may contribute to increased difficulties accessing testing and treatment. Looking ahead, people of color would likely face further disproportionate losses in coverage if the ACA is overturned by the Supreme Court. Coverage losses will lead to increased barriers to care and worse health outcomes, widening disparities in health at a time when there is a growing focus on prioritizing and advancing health equity and in the middle of a pandemic that has disproportionately affected people of color in the US.
The coronavirus pandemic has dominated the nation’s attention for about nine months, recently rivaled only by the Presidential election. But, there’s another thing many people may want to pay attention to right now, especially with historic job losses: How to maintain health insurance coverage at a time they may need it most.
The combination of extraordinary job losses and a historic pandemic are likely to test the Affordable Care Act (ACA) health insurance safety nets in a way not yet seen since the law’s passage. On one hand, people losing job-based coverage now may be more motivated than before to access ACA insurance programs like expanded Medicaid and Marketplace subsidies because of the pandemic. On the other hand, awareness of these key ACA programs has fallen over time, and people losing job-based coverage now may never have had a need to learn about the ACA’s programs since the 2014 implementation.
Here, we detail ten ways in which the 2021 ACA open enrollment period differs from enrollment periods in past years. We also provide links to a number of KFF resources for more information.
1. More people than ever before may need to know about coverage options through the Marketplace or Medicaid Expansion. Ten years ago, the ACA passed in the wake of the last financial crisis to hit the United States, when job losses left millions without access to insurance coverage. While most people in the U.S. still rely on employer coverage, the ACA creates and expands programs (specifically, the Marketplaces and Medicaid Expansion), through which people without job-based benefits can access health coverage with financial help. Since these programs went into effect in 2014, though, the economy has been relatively strong until early 2020. As such, this year’s Open Enrollment period could be the first real test of how well the ACA works to maintain coverage when large numbers lose their job-based health insurance.
Heading into 2021, continued widespread economic dislocation during this COVID-19 emergency could mean millions of people may need Medicaid or private health insurance through the Marketplace who haven’t needed that before. There are few, if any, reliable real-time data sources that would allow us to know exactly how many of the people losing employment have also lost health insurance. In an analysis of insurer-reported enrollment through June, we found employer group enrollment had dropped by 1.3%, indicating that many employers had kept furloughed workers on coverage at least temporarily. However, as more job losses become permanent, more coverage loss is possible, even likely. KFF has estimated that as many as 85% of people who are at risk of becoming uninsured due to loss of job-based coverage could be eligible for Medicaid or subsidized marketplace coverage.
2. Consumer awareness of ACA coverage options is limited. Although the vast majority of people at risk of losing coverage may be eligible for help, KFF polling finds that public awareness about ACA coverage options has fallen somewhat since the law passed a decade ago. For example, 59% of the public knows the ACA offers subsidies for marketplace health plans, compared to 75% ten years ago. Among uninsured consumers today, understanding of ACA options and enrollment rules is more limited. Less than half (43%) know Open Enrollment is the time to sign up for Marketplace plans; and 14% of uninsured individuals living in states that have expanded Medicaid eligibility under the ACA know about this expansion. KFF also finds many consumers are unsure about the current status of the ACA; as of this spring, just 22% of the uninsured know the law remains in effect. Uncertainty may result in part due to public debate and news coverage about a pending Supreme Court case to overturn the law.
The Trump Administration has reduced funding for Open Enrollment marketing and outreach by 90 percent. In this environment, news coverage of Open Enrollment and the availability of financial assistance could have an even more significant impact on public education.
3. The importance of health coverage is even greater as coronavirus cases are surging. In recent days, the number of new coronavirus infections reached record highs in the U.S., and the pandemic is worsening rapidly in parts of the country that had previously been spared. A KFF analysis earlier this year showed that the cost of COVID-19 treatment for those requiring hospitalization could easily top ten thousand dollars, with more severe cases costing tens of thousands of dollars. Many private insurers have waived out-of-pocket costs for people needing COVID-19 treatment. At the very least, people with ACA-compliant private insurance are protected by out-of-pocket maximums, limiting how much enrollees must pay for a hospitalization. There is currently no guarantee that hospitals waive COVID-19 treatment costs for uninsured patients, meaning those without coverage could be on the hook for large medical bills.
4. Changes are taking place for 2021: premiums are dropping in many areas, as new insurers enter the Marketplaces. On average, marketplace benchmark premiums are declining by more than 2% in 2021 across the country (Table 1). In addition, new insurers are entering the Marketplace or expanding their service area in many states next year. These changes can increase plan choices and improve affordability for people who don’t qualify for Marketplace subsidies. People already enrolled in Marketplace plans with subsidies who want to renew coverage for 2021 are strongly advised to actively renew coverage, and not rely on Marketplace automatic renewal procedures. Changes in 2021 premiums and plan participation can affect the amount of a person’s tax credit from year to year. Actively renewing coverage lets people update their income information and review new plan choices, ensuring they receive the most accurate subsidy for 2021.
Table 1: Change in the Average Lowest-Cost Premium by Metal Level Before Tax Credit, 2020-2021 for a 40-year-old
2020
2021
% Change
Lowest Cost Bronze Premium
$331
$328
-0.9%
Lowest Cost Silver Premium
$442
$436
-1.4%
Lowest Cost Gold Premium
$501
$481
-4.0%
Benchmark Premium
$462
$452
-2.2%
SOURCE: KFF analysis of premium data from Healthcare.gov and review of state rate filings.
5. For many people, incomes are particularly volatile this year, which can affect program eligibility and financial assistance. During the pandemic, many people have or will experience changes in income that could complicate their application for subsidies. Those who have previously been told they were ineligible for Marketplace financial assistance or Medicaid may now find out they are eligible if their income or other household circumstances have changed. An earlier KFF brief explored the various ways changes in wage income and unemployment benefits affect eligibility for Medicaid and Marketplace subsidies. Our newly released 2021 FAQs also review rules for income changes mid-year including potential tax consequences for those who mis-estimate their 2021 income. People who received Marketplace subsidies this year, will also have to report on income and sources when they file their 2020 tax return next year; FAQs provide information about how to count the $1,200 Recovery Rebate and federal supplements to weekly unemployment benefits that many received this year.
6. New State Actions: State Based Exchanges, Medicaid Expansions, and Public Options. Other new developments this year include new state-run insurance marketplaces and the first public option program. Residents of two states that have been using HealthCare.gov – Pennsylvania and New Jersey – will need to sign up through new state-run Marketplaces for 2021 and will have a longer Open Enrollment period than they’ve been used to. Currently, 37 states have adopted and implemented Medicaid expansion and both Oklahoma and Missouri plan to implement expansion by mid-2021. Additionally, the Washington state exchange has implemented a new quasi-public option, called Cascade Care, which will be offered in half of the state’s counties this year. KFF’s FAQs also provide updated information on four states that supplement marketplace subsidies with state funding.
7. Recent Trump Administration policy changes and court rulings may affect eligibility and covered benefits for some people. The KFF FAQs also include updated information related to recent Trump Administration actions and court rulings that may affect eligibility or covered benefits for some consumers. These include expanded exemptions for employers who refuse to cover contraceptive services based on religious or moral objections, and changes to the “public charge” test for certain individuals applying for green card status who use certain government services. The FAQs also provide information about private websites offering alternative enrollment pathways for people seeking marketplace plans and subsidies, and about short-term policies.
8. Enrollment help is available, though may be in short supply. Consumers in most states can get help from trained experts (Navigators) who won’t try to sell them anything. However, federal government funding for Navigators remains limited, with no funding for Navigators in South Carolina or Utah. In several other states, including Texas, Ohio, Illinois, Kansas, and Michigan, many counties will not be served by federal navigator programs. KFF finds nearly 5 million consumers tried to find enrollment help during the last Open Enrollment but could not. Among those who found help, about one in five heard about it through an advertisement or news coverage.
9. People affected by natural disasters or the COVID-19 disaster can apply for extended time to sign up for 2021 coverage. As in past years, people who live in FEMA-designated areas affected by hurricanes, wild fires, or other disasters – can get more time to sign up for 2021 coverage if you are unable to enroll by the end of Open Enrollment. This extension may also be available to residents throughout the US who are unable to sign up on time due to the COVID-19 disaster. The time extension is not automatic, and must be requested from the Marketplace call center.
10. There is still time to sign up for 2020 coverage. Even as this year winds down, people who lost coverage earlier this year due to the pandemic can still sign up for 2020 coverage because of a time extension for special enrollment periods (SEP). Normally, people have just 60 days to apply for a special enrollment period after they lose other coverage, but during the pandemic, those who lost coverage at any time during 2020 can still apply for an SEP to get coverage for the remainder of this year. In 3 states (Maryland, New York, and the District of Columbia), all residents who are uninsured, no matter the reason, can still sign up for 2020 coverage.
With so much changing this year, there is no shortage of reasons why the public needs to know about ACA open enrollment. KFF features more than 300 Frequently Asked Questions about the Health Insurance Marketplace and the Affordable Care Act (ACA). Spanish-language translations are also available. KFF Open Enrollment information materials also include an ACA Marketplace Subsidy Calculator, a subsidy explainer, and state-level data on premium changes. FAQs also focus on information of particular interest to young adults, women, immigrants, early retirees, non-traditional households, and people with employer-based health benefits.
A new chart collection examines what we know about the cost of common health services in the U.S.
The analysis shows that costs for many common health services have risen more rapidly than inflation; for example, the average cost of hospital admission among large employer plans increased by about $10,000 (68%) between 2008 and 2018. Additionally, there are large geographic variations in the cost of the same health services across the U.S. A lower back MRI in the Las Vegas, NV area costs $404 on average; in the Houston, TX area, the average price is $1,106.
The chart collection is available on the Peterson-KFF Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.