Key Questions About Nursing Home Cases, Deaths, and Vaccinations as Omicron Spreads in the United States
Staff and residents at long-term care facilities were hit hard by the pandemic, reporting over 195,000 deaths as of the end of 20211 , or about 23% of all COVID-19 deaths in the U.S. After a dramatic surge, cases and deaths in long-term care facilities (including nursing homes, assisted living facilities, ICF/IIDs, and other settings) dropped following the vaccine rollout in the Winter of 2020-2021, according to a KFF analysis. Since then, nursing home cases and deaths have mostly risen and fallen in tandem with national cases and deaths, although they are once again on the rise as Omicron has taken hold in the U.S.
This data note analyzes federal nursing home data as of January 2nd, 2022 to determine the impact of the pandemic on COVID-19 cases and deaths among staff and residents, amid the recent surge of national cases due to the Omicron variant. The data on overall U.S. and nursing home cases and deaths in this analysis reflects data reported over the holiday season, which may include delayed, disrupted, or otherwise anomalous reporting. Additionally, since increases in deaths lag increases in cases, it is not yet clear the extent to which the surge in Omicron will affect mortality. See methods box for more details.
What are the recent trends in COVID-19 cases and deaths in nursing homes?
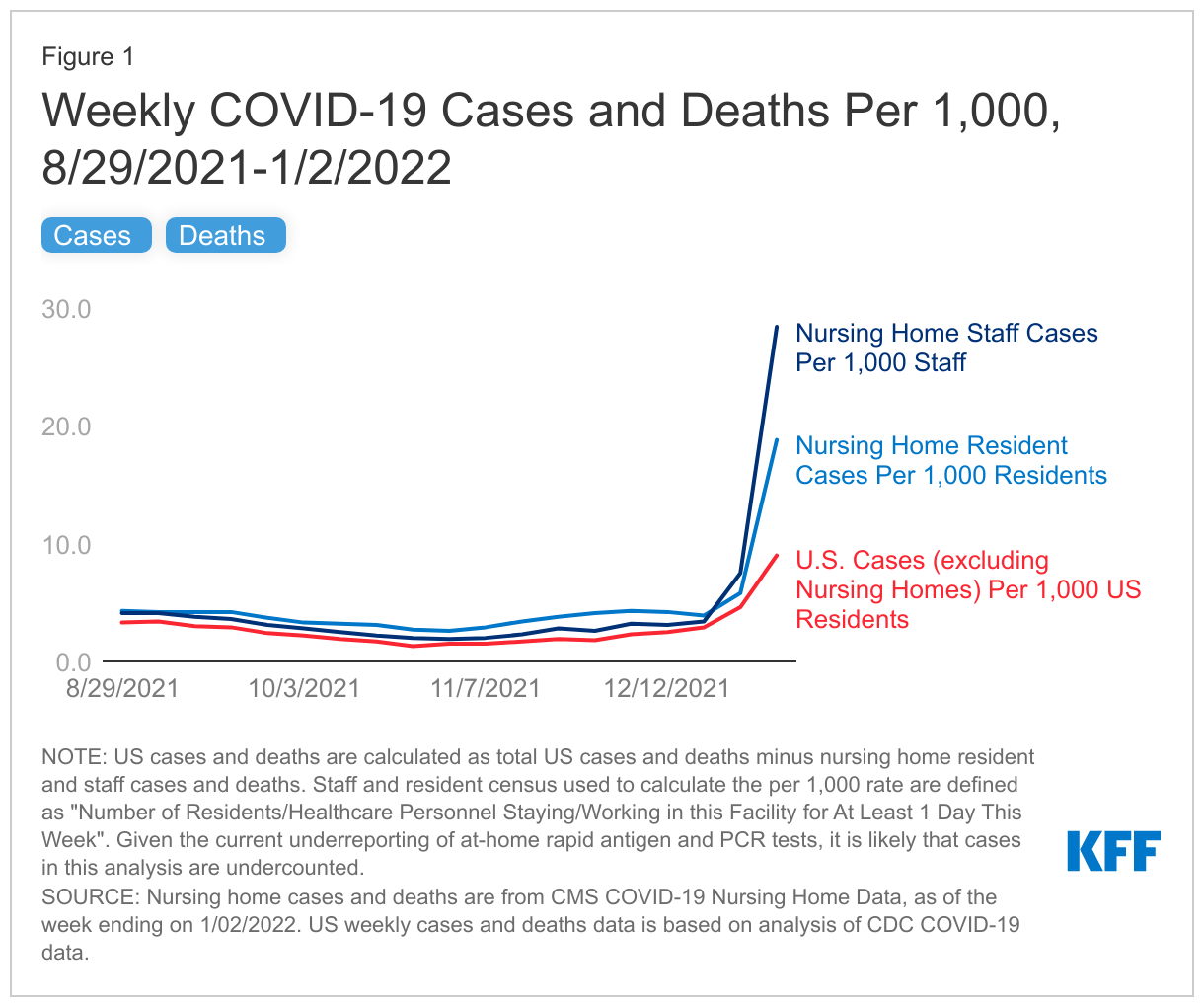
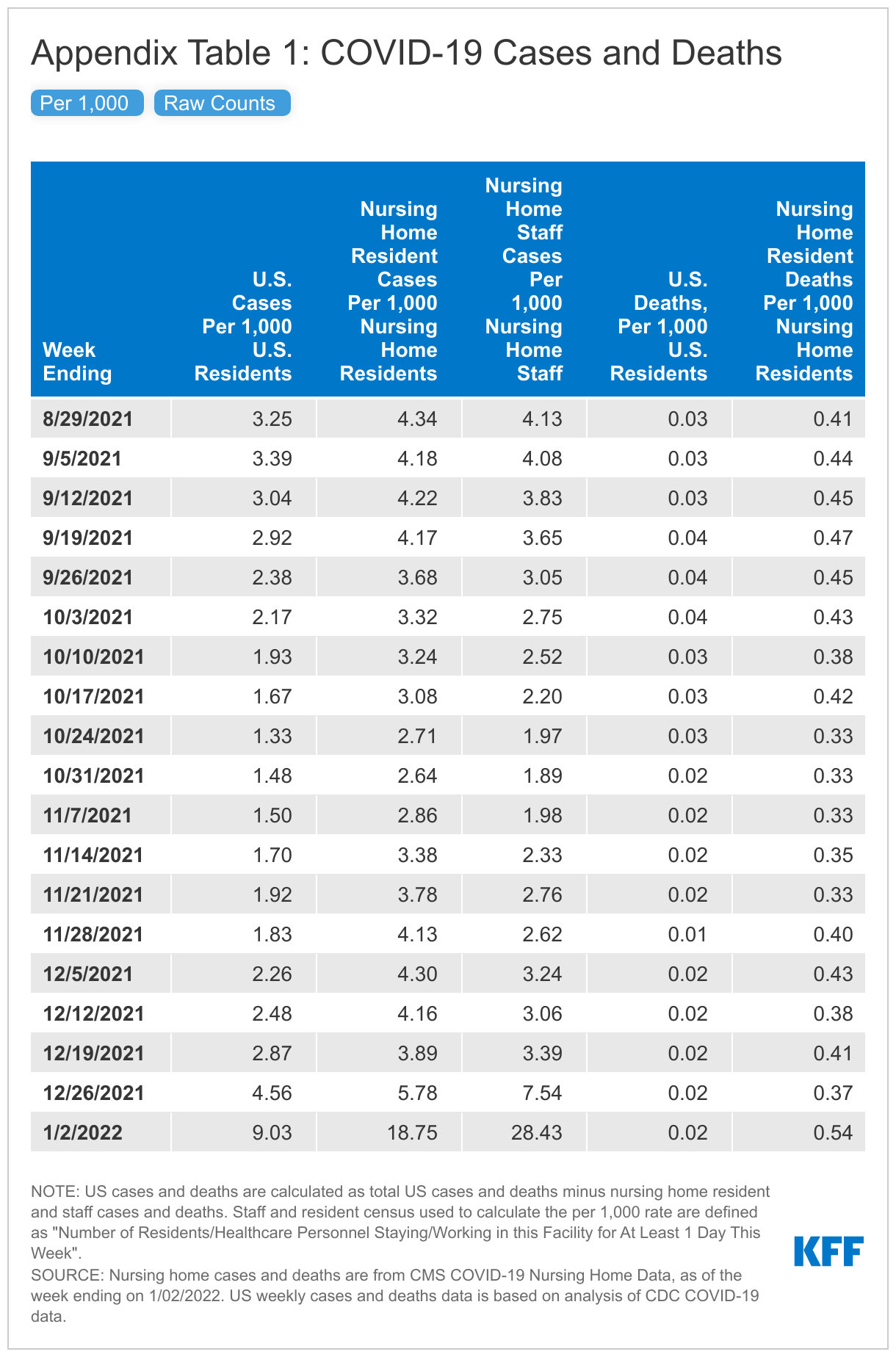
Cases and deaths in nursing homes are rising, generally mirroring current trends in the overall U.S., though rates have recently started to rise faster in nursing homes (Figure 1 and Appendix Table 1). In the week ending January 2nd, 2022, nursing homes reported 18.75 resident cases per 1,000 residents, a 225% increase from the week prior, and 0.54 resident deaths per 1,000 residents, a 48% increase from the week prior.
Cases among nursing home staff have increased at an even steeper rate, with staff cases per 1,000 staff increasing by 277%. These patterns look mostly similar to the current rise in cases and deaths across the U.S., aligning with the general pattern observed over the course of the pandemic.
In the week ending January 2nd, nursing home residents and staff reported higher case rates (per 1,000) than the overall U.S. population, and higher death rates (per 1,000) among nursing home residents (Figure 1 and Appendix Table 1). According to the most recent data available, the case rate was higher for nursing home staff (28.43 per 1,000) than for nursing residents (18.75 per 1,000), both of which were higher than the overall U.S. average (9.03 cases per 1,000). Nursing homes reported 0.54 resident deaths per 1,000 residents, which is over 25 times the death rate reported in the general population (0.02 deaths per 1,000). Higher case rates may be attributed to the highly transmissible nature of Omicron and the nature of congregate care settings. Higher death rates may be attributed to the high-risk status of those who reside in nursing homes.
How have vaccination rates changed over time for nursing home residents and staff?
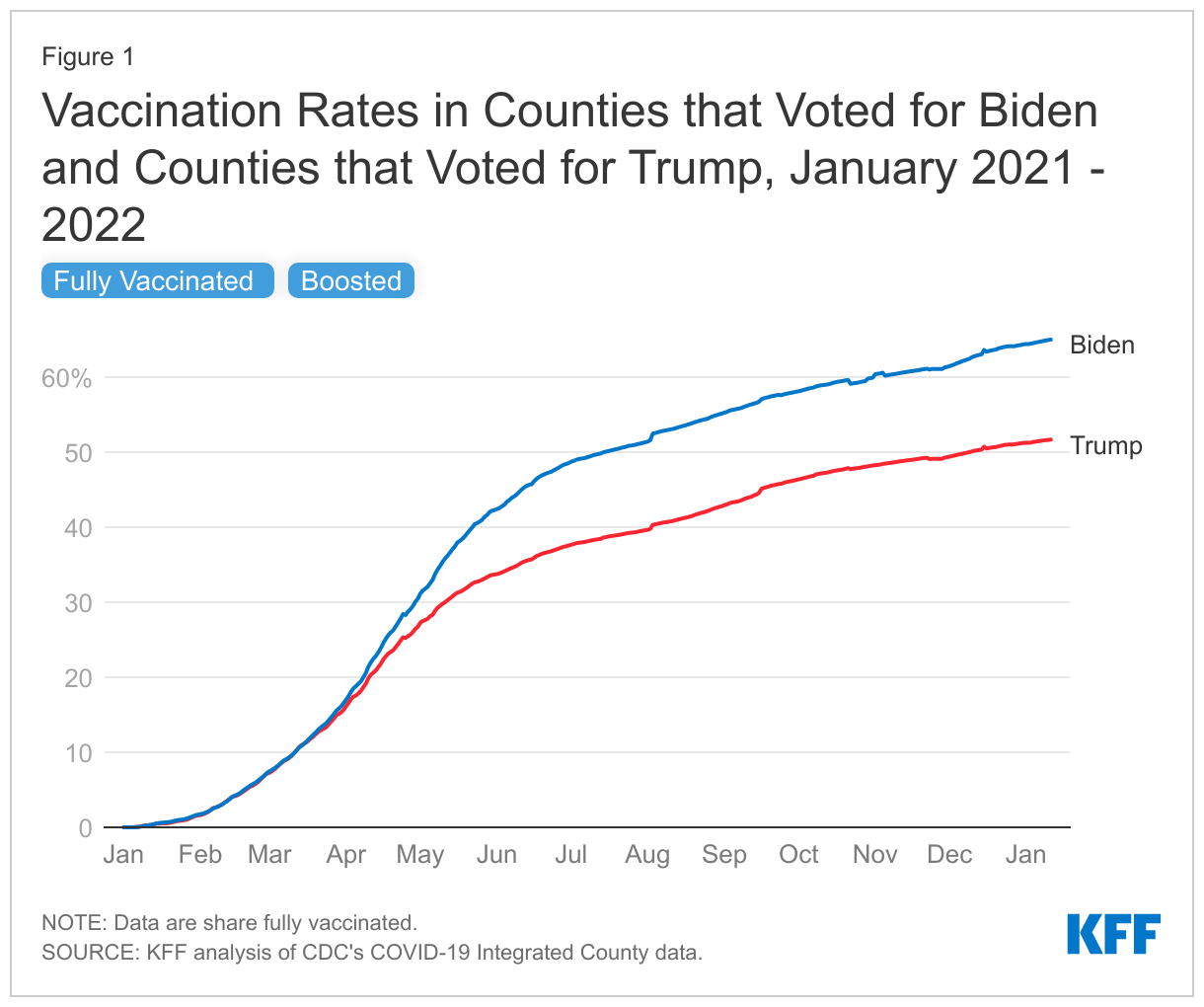
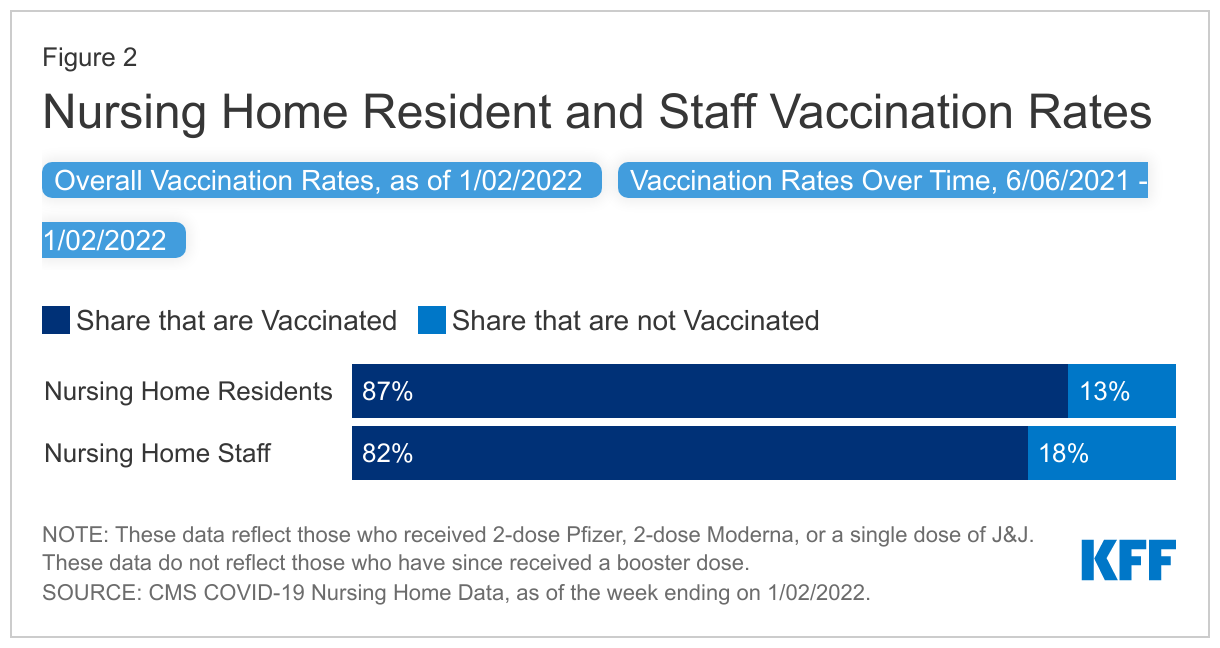
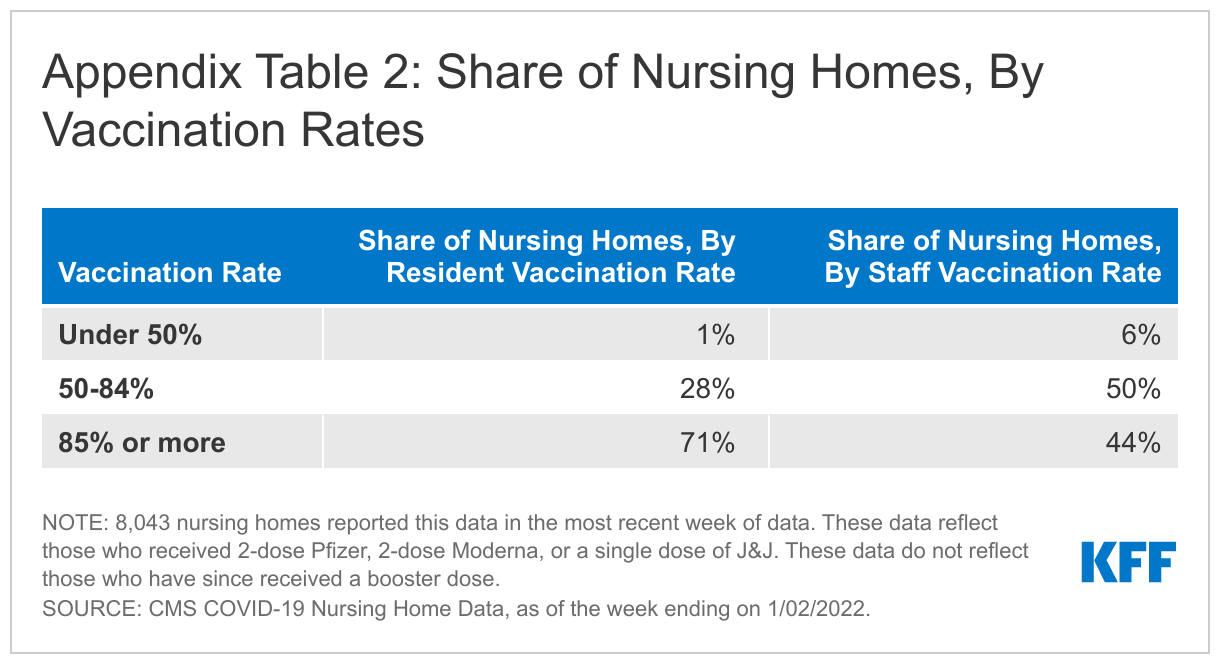
Staff vaccination rates remained five percentage points lower than resident vaccination rates as of the week ending January 2nd (87% vs. 82%), though staff vaccination rates increased by nearly 26 percentage points between June and early January 2022 (Figure 2). Residents and staff started receiving vaccinations in December 2020 through the Pharmacy Partnership for Long-Term Care. Resident uptake was initially higher than that of staff, leading to higher early vaccination rates. When nursing home vaccination data first became available in June 2021, a much larger share of residents (79%) than staff (56%) were vaccinated. A key reason staff vaccination may have increased since June 2021 is that the Biden administration announced a nursing home staff vaccine mandate in August 2021 as a condition for facilities to continue receiving Medicare and Medicaid funding2 . Lawsuits have been filed challenging the mandate, but Supreme Court has ruled that the mandate can take effect while the cases play out in the lower courts. The increase in staff vaccination rates may also be partially attributed to unvaccinated staff leaving their positions. For the most recent period, a larger share of facilities reports very high (85%+) vaccination rates among residents (in 71% of facilities) than among staff (in 44% of facilities) (Appendix Table 2).
What do we know about the boosters for nursing home residents and staff?
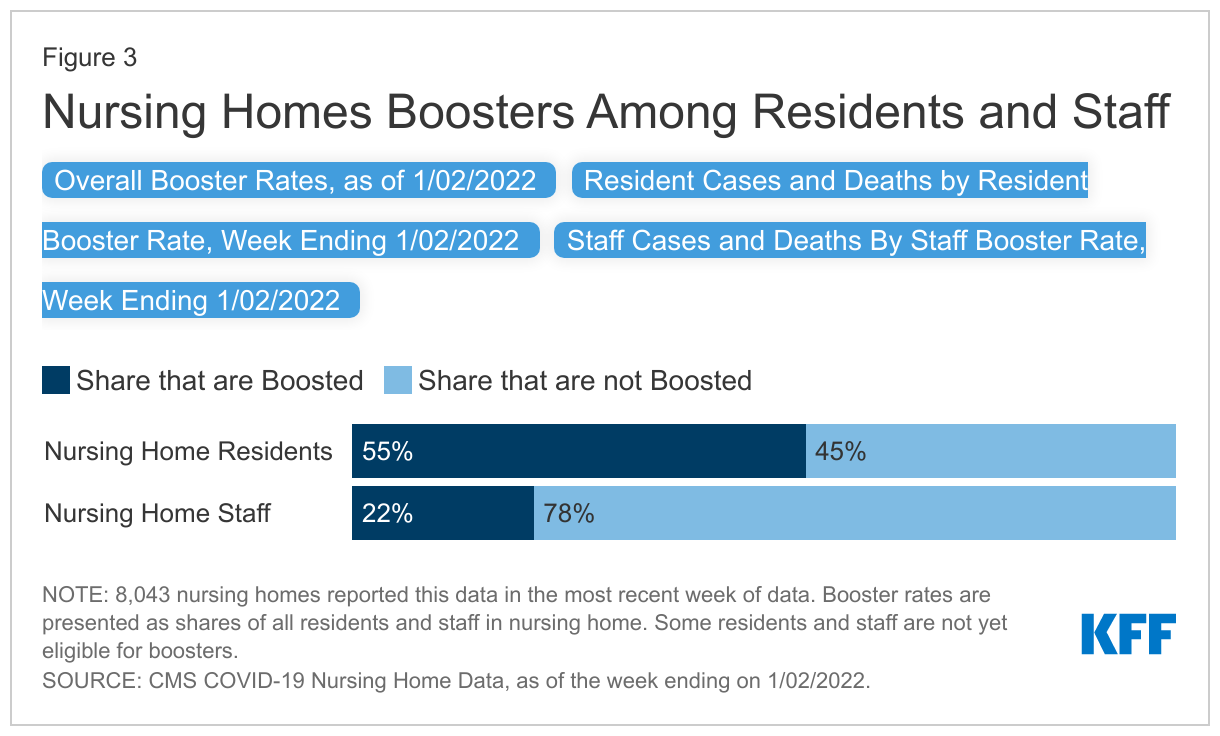
In the week ending January 2nd, about 54% of nursing homes (8,043) reported data on cases, deaths, and boosters. In this sample of nursing homes, about 55% of residents had received a booster compared to just 22% of staff (Figure 3). These values represent the share of all residents and staff who have received their booster, although some may not have been eligible for their booster by January 2nd. Individuals who received the Pfizer-BioNTech or Moderna vaccines become eligible for boosters five months after completing their primary vaccination series. Individuals who received Johnson & Johnson’s Janssen vaccine are eligible for boosters two months after receiving their shot. Since many residents received their vaccinations earlier than the staff, residents were likely eligible and received their booster earlier than staff. The share of residents and staff who are boosted will continue to increase as more residents and staff become eligible, though data on vaccinations suggests that staff booster rates may not reach levels of resident boosters regardless of eventual eligibility.
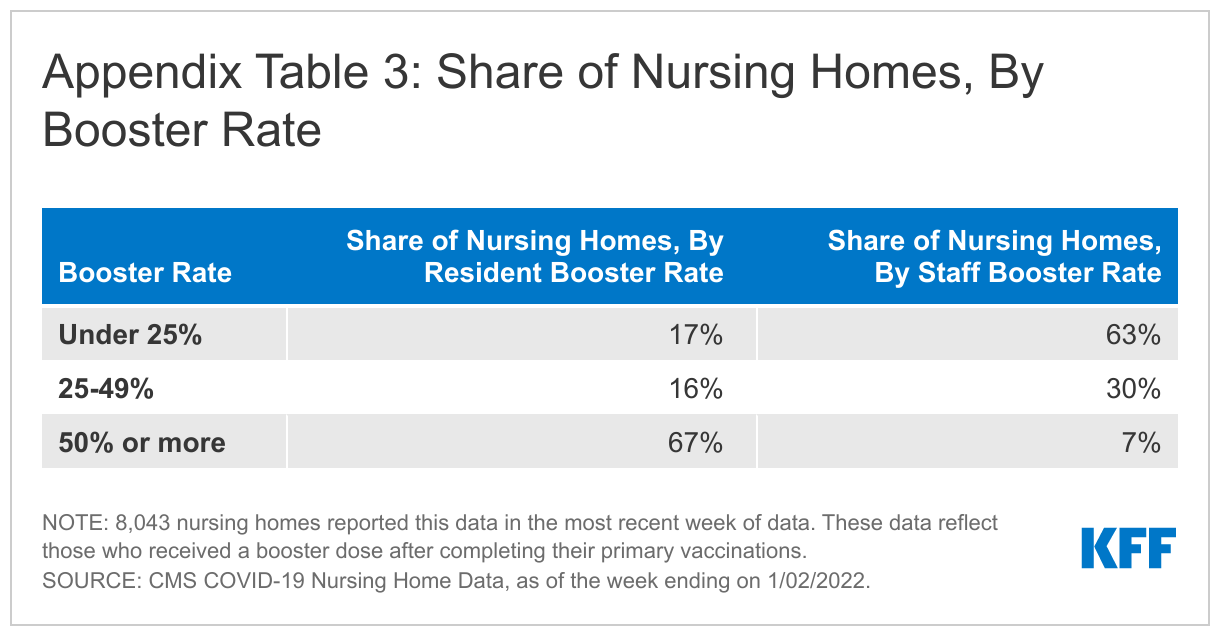
Among the nursing homes in the sample reporting data for the week ending January 2nd, a small share (7%) reported staff booster rates of 50% or higher, while over two thirds (67%) of these nursing homes reported resident booster rates of 50% or higher (Appendix Table 2). Previous research suggests a myriad of factors impact cases and deaths in nursing homes including, but not limited to, resident acuity, surrounding community spread, and facility size. Recent hospital data showing higher levels of severe illness and death among those who are unvaccinated suggests that vaccination and booster rates may be a key consideration as well. Our analysis found that nursing homes with low resident booster rates reported higher average resident cases and higher average resident deaths in the week of data analyzed. Similarly, facilities with low staff booster rates reported higher average staff cases (Figure 3). While vaccination and booster rates should be considered alongside other factors, they likely play a key role in protecting those who live and work in these congregate care settings.
Looking Ahead
This data notes suggests that the Omicron variant has made its way into nursing homes, once again raising concerns about the impact on residents and staff. While there is growing evidence that Omicron is less likely to cause severe illness than previous variants, older adults and those with other health conditions are still at greater risk. Given the particularly high-risk nature of residents in these settings and the experience of residents and staff earlier in the pandemic, nursing homes may see a significant increase in deaths following this increase in cases. Numerous studies have shown that those that are fully vaccinated and boosted are highly protected against the new variant, a finding which increases the urgency to increase vaccination and booster rates among unvaccinated and unboosted residents and staff in nursing homes. Lawsuits have been filed challenging the vaccine mandate for health care staff, a key policy lever that policymakers and other stakeholders can use to increase vaccination rates among unvaccinated staff. However, the Supreme Court has ruled that the mandate can take effect while the cases play out in lower courts. As Omicron continues to break case and hospitalization records, increasing vaccination and booster rates will be an important protection against illness and death for nursing home residents and staff.
Appendix Tables
Methods
This analysis uses federal data on coronavirus cases and deaths in nursing homes, which includes weekly data as of mid-May 2020 through January 2nd, 2022. These data are updated regularly to reflect revised data from previous weeks, so future versions of this dataset reflecting the same time period may output different values. This analysis excludes suspected cases from the definition of nursing home cases among residents and staff. Data on U.S. cases and deaths are calculated based on the number of nationwide cases and deaths from the CDC minus nursing home cases and deaths; we make this adjustment to account for possible endogeneity (that is, cases or deaths in nursing homes contributing to the patterns in COVID-19 cases and deaths nationwide). Given the current underreporting of at-home rapid antigen and PCR tests, it is likely that cases in this analysis are undercounted. The federal data includes only data on federally certified nursing homes. This analysis therefore does not include data on other long-term care settings, such as assisted living facilities, residential care facilities, group homes, or intermediate care facilities.
Previous analysis used state-reported data on long-term care facility cases and deaths, which represented a more comprehensive set of facilities. Due to a drop-off in reporting regularity and lack of consistency in states overtime, this analysis uses federal data to be able to trend cases and deaths in nursing homes since June 2020.
- This statistic was calculated by adding the nearly 187,000 long-term care COVID-19 deaths identified from KFF data collection efforts that ended June 30th, 2021 with the approximately 8,700 COVID-19 deaths nursing homes have reported to CMS since June 30th, 2021. This death count is an undercount since CMS data does not account for deaths in non-nursing home settings and not all nursing homes report complete data. ↩︎
- The new rule applies to Medicare and Medicaid providers that are directly regulated by CMS and therefore does not reach all Medicaid providers, such as certain home and community-based services (HCBS) providers. The rule applies to nursing homes, hospitals, outpatient rehab facilities, federally qualified health centers, rural health centers, and home health agencies, among other provider types. ↩︎