Key Takeaways
The COVID-19 pandemic created unprecedented health and education challenges for children with disabilities, many of whom receive special education services. Recently, the Omicron variant, slowing vaccination rates among children, and state bans on school mask mandates have impacted school operations during the new year as well as the health, safety, and educational progress of children with special education plans. Many children receiving special education services have substantial health care needs, and services available through a child’s health insurance plan, such as Medicaid, can complement special education services. This brief describes how Medicaid and special education services work in meeting children’s needs, explores how the pandemic has affected children who receive special education services, and identifies key issues to watch moving forward. Key findings include the following:
- If a child is eligible for both special education services and Medicaid, federal law requires state Medicaid programs to pay for services that are both educationally and medically necessary.
- Medicaid/CHIP covers half of all children with special education plans. Children with special education plans covered by Medicaid/CHIP are more likely to have greater health needs compared to those with private insurance only.
- The onset of the pandemic and ensuing school closures created disruptions and challenges in how children received special education services. Many children with special education plans experienced missed or delayed services and loss of instructional time during the pandemic.
Students with special education plans may be entitled to compensatory services to make up for lost skills due to pandemic related service disruptions, and some children, such as those with disabilities related to long COVID, may be newly eligible for special education services. Medicaid can play an important role in ensuring that children receive preventive services that may have been delayed during the pandemic and access services to address needs that may have arisen due to the pandemic.
Introduction
The COVID-19 pandemic has had a disproportionate impact on people with disabilities, including children, whose health and functional needs place them at increased risk of severe illness or death from COVID-19 and who may require special education services that may not be adequately provided in education settings modified by the pandemic. There are an estimated 6.7 million children1 , or 9% of all children in the U.S., who currently have special education plans2 , and over two-thirds of these children have special health care needs.3 Throughout the pandemic, these children have experienced delayed or missed services and losses in instructional time, which can have implications for their ability to continue to progress in their education. As a major health insurance provider for children with special education plans, Medicaid can provide important services to these children as well as ensure that children receive other preventive services that may have been delayed during the pandemic and access services to address needs that may have arisen due to the pandemic, such as mental health treatment.
While students have largely returned to in-person learning this school year, challenges for children receiving special education services remain. A number of lawsuits are challenging state bans on school mask mandates, arguing that these bans violate the right of children with disabilities to safely attend school. Further, the recent, rapid spread of the Omicron variant has created additional instability for students and some schools have temporarily switched to remote learning, a move that may make it difficult to provide all needed services to children with special education plans. While the Pfizer-BioNTech COVID-19 vaccine is now authorized for school-aged children, vaccination among young children is not yet widespread. This brief explains how Medicaid and special education services intersect, explores the pandemic’s implications for children receiving special education services, and identifies key issues to watch moving forward. For additional context, the appendices provide information on what is required under federal special education law and includes supporting data tables.
What is the intersection between Medicaid and special education services?
If a child is eligible for both special education services and Medicaid, federal law requires state Medicaid programs to pay for services that are both educationally and medically necessary. This is an exception to the general rule that usually makes Medicaid the payer of last resort when other sources of coverage are available. If a device or service included in a child’s special education plan under the Individuals with Disabilities Education Act (IDEA) is also medically necessary, then Medicaid is obliged to pay before the school district.4 For more on what is required under the federal IDEA, see Appendix A. Children also may qualify for additional services covered by Medicaid, beyond what is required by the IDEA. For example, a child with cerebral palsy may need physical therapy to improve mobility and manage muscle contractures. The IDEA might require the school district to provide physical therapy so that the child can access and progress in their education, such as therapy targeted to moving around the school or developing skills related to their educational goals. If the child requires additional physical therapy for other purposes, such as to facilitate their ability to transfer in and out of a wheelchair at home or skills needed to access the community outside of school, such services could be “medically” but not “educationally” necessary and therefore available under Medicaid.
The scope of services that must be provided to children under federal Medicaid law is broader than what is required under the IDEA’s definition of “related services.” The Early Periodic Screening Diagnostic and Treatment (EPSDT) provision requires state Medicaid programs to cover all services that are “necessary. . . to correct or ameliorate. . . physical and mental illnesses and conditions. . . .”5 Like the IDEA, EPSDT applies to Medicaid enrollees from birth through age 21. To receive federal matching funds, state Medicaid programs must cover a minimum set of services for adults (such as inpatient hospitalization and physician services) and can choose to cover additional services (such as private duty nursing and rehabilitative services). However, EPSDT means that there are no “optional” services for children; instead, if medically necessary, all services must be covered for children, regardless of whether the state chooses to cover them for adults.
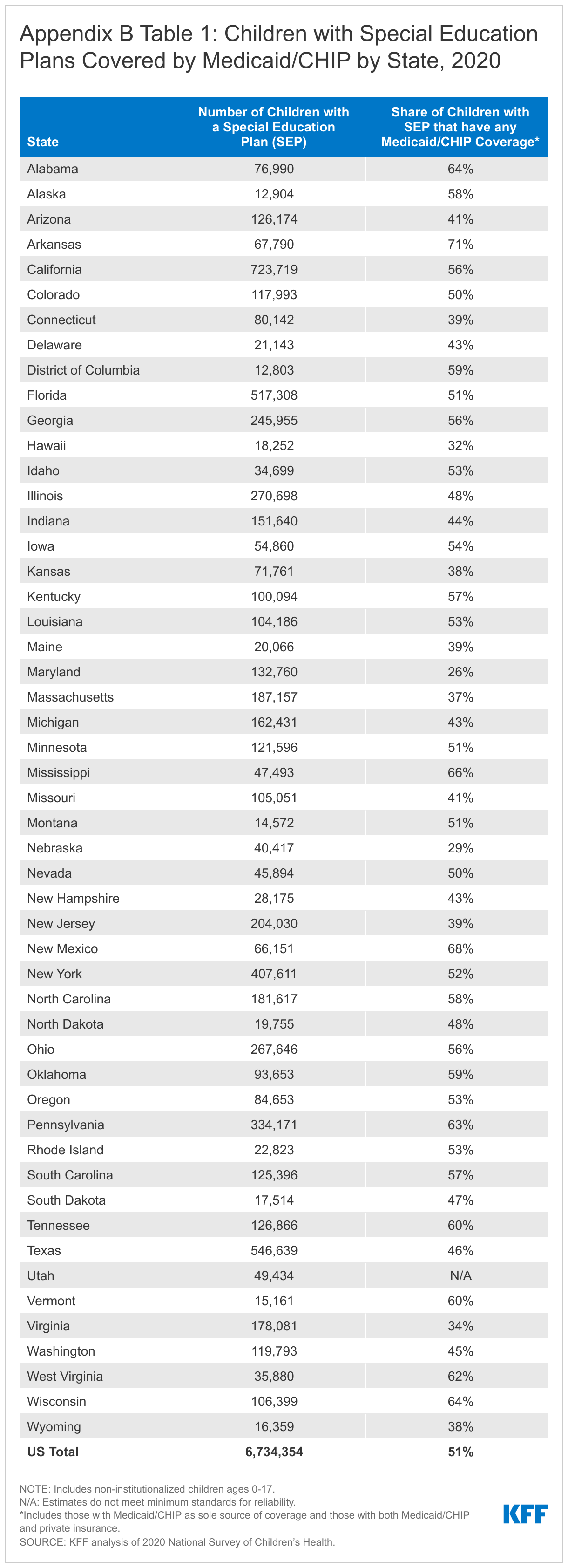
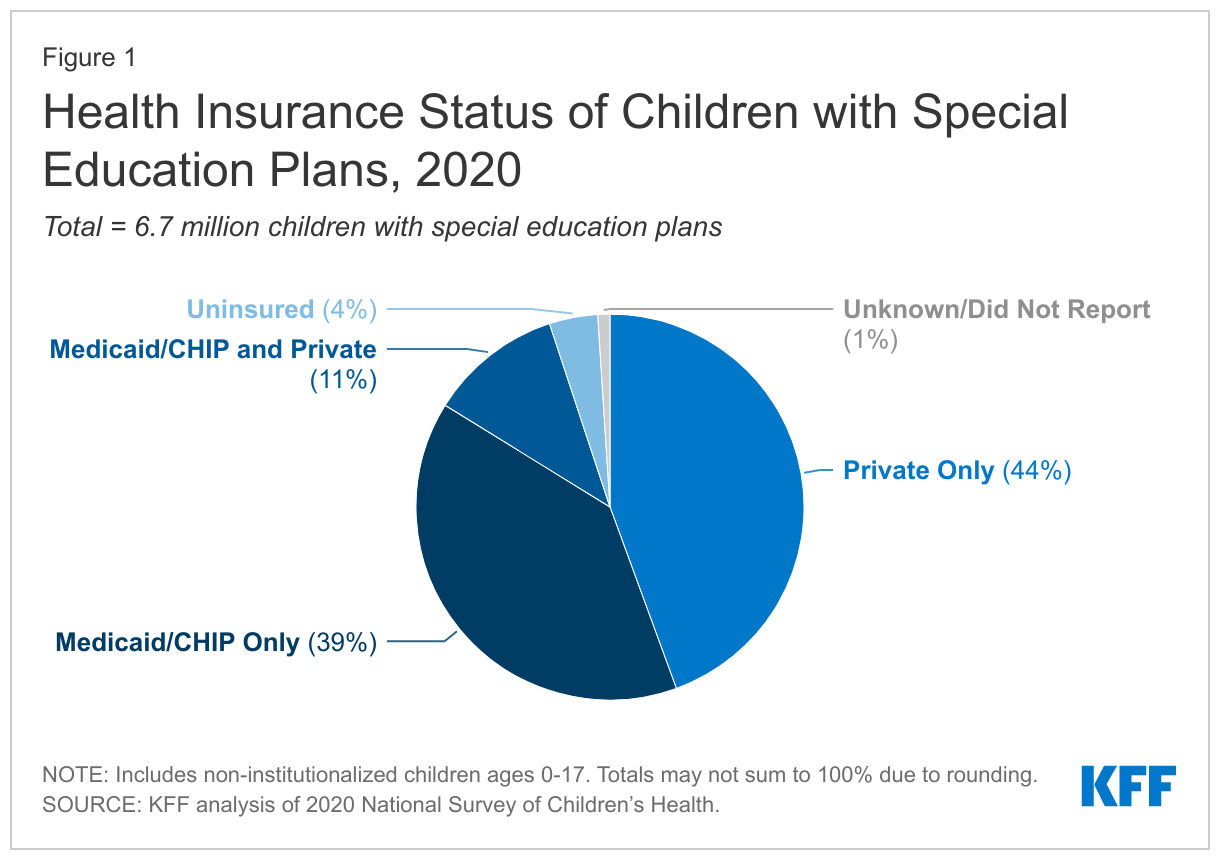
Medicaid, together with the Children’s Health Insurance Program (CHIP), covers half of all children with current special education plans (Figure 1). Medicaid/CHIP is the only source of coverage for nearly four in 10 children nationwide receiving special education services, while over one in 10 have Medicaid/CHIP to supplement private insurance. Medicaid covers services that private insurance typically does not, including long-term services and supports (LTSS) and home and community-based services (HCBS), and has cost-sharing protections that help keep health care affordable for families. The share of children with special education plans covered by Medicaid/CHIP varies by state, ranging from 26% to 71%, reflecting variation in state choices about optional Medicaid eligibility pathways for children with disabilities (Appendix B Table 1).
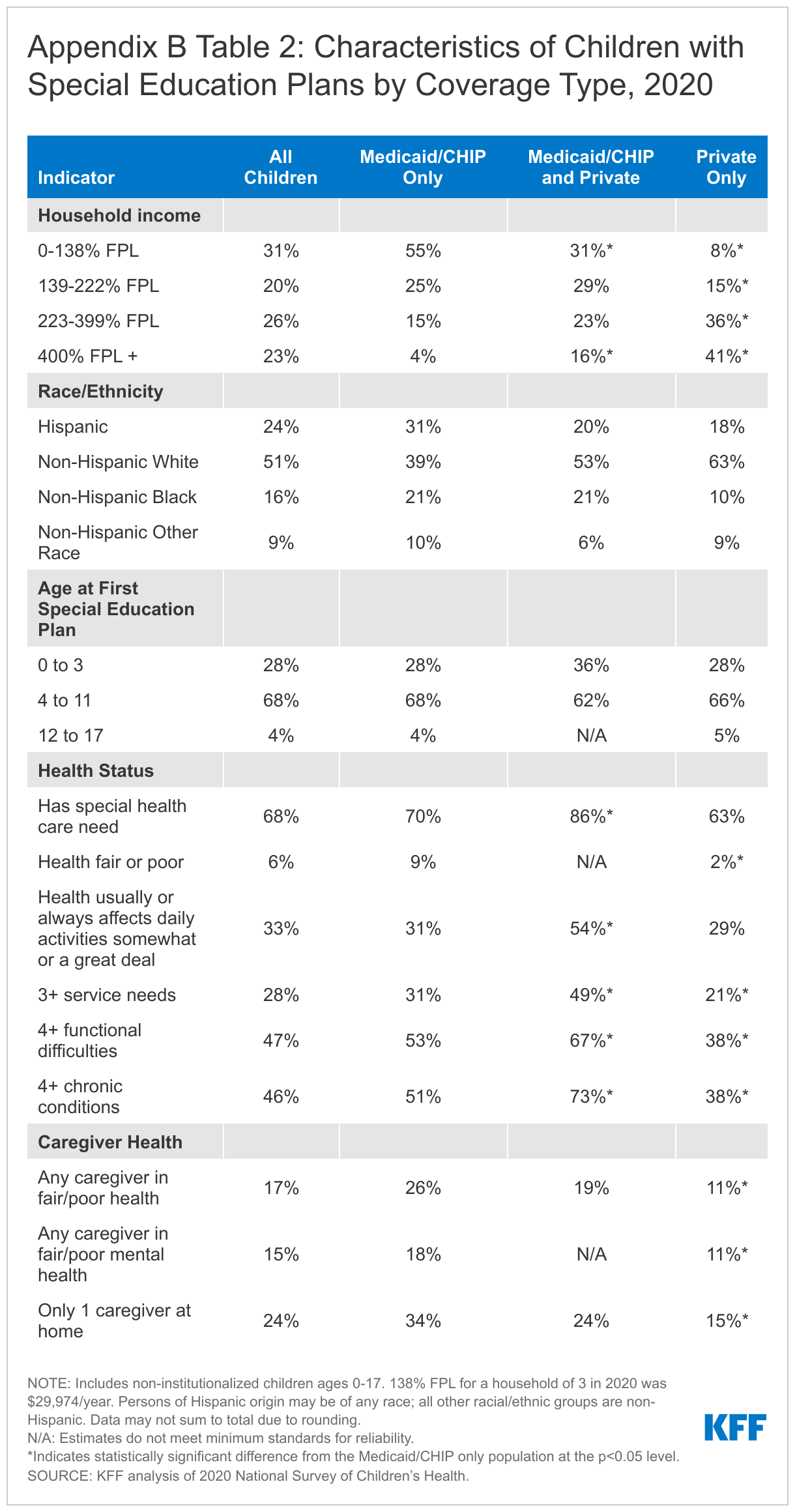
A majority of children with special education plans covered by Medicaid/CHIP alone are children of color and live in low-income households (Appendix B Table 2). Medicaid/CHIP-only children with special education plans are more likely to be non-Hispanic Black or Hispanic compared to children with private coverage only. Medicaid/CHIP-only children with special education plans also are more likely to live in a household with an income at or below 138% of the federal poverty level (FPL, less than $29,974/year for a family of three in 2020) when compared to those with private insurance only. Additionally, most children (68%) receive their first special education plan between the ages of 4 and 11 regardless of health coverage type.
Children with special education plans covered by Medicaid/CHIP are more likely to have greater health needs compared to those with private insurance only. Medicaid/CHIP-only children with special education plans are more likely to have multiple chronic conditions and multiple functional difficulties, with over half of the Medicaid/CHIP-only group reporting four or more functional difficulties or four or more chronic conditions, compared to 38% of those with private insurance only (Appendix B Table 2). Further, children with special education plans covered by both Medicaid/CHIP and private insurance are more likely than children covered by Medicaid/CHIP alone to have four or more functional difficulties, four or more chronic conditions, or three or more service needs. These children are also more likely than children with Medicaid/CHIP alone to have special health care needs and health that usually or always affects daily activities somewhat or a great deal. Medicaid coverage can address gaps in private coverage, and children covered by both Medicaid/CHIP and private insurance often have complex health needs and are more likely to be eligible for Medicaid through a disability-related pathway. Further, parent/caretakers of Medicaid/CHIP-only children with special education plans are also more likely to parent alone and face challenges with their own physical and mental health compared to those with private insurance only.
How has COVID-19 affected children’s access to special education services?
Many children with special education plans experienced missed or delayed services and loss of instructional time during the pandemic. One report estimates that school attendance and engagement has declined since the start of the pandemic, with early data suggesting larger declines for children with disabilities. A survey released early in the pandemic (May 2020) found 40% of parents of students with special education plans reported their child was not receiving any support, and only 20% reported their child was receiving all the services they required. School districts reported it was more or substantially more difficult to provide hands-on instruction accommodations and services such as speech, physical, or occupational therapy during pandemic school closures. Students with disabilities experienced a loss of instructional time, and may have started the 2021 school year up to one year behind. Remote learning may have also been hindered by a lack of access to the internet and assistive technology to which students with disabilities have access when attending school in-person. Low-income children and children of color faced increased health and economic challenges during the pandemic, and children with special education plans within these groups, many of whom are covered by Medicaid/CHIP, likely faced additional barriers to learning and accessing services during the pandemic.
Students with special education plans may be entitled to compensatory services to make up for lost skills due to school closures or other pandemic related service disruptions. The Department of Education (DOE) guidance advises special education teams to make individualized decisions about the needs for additional services as schools return to normal operations. The American Academy of Pediatrics noted the “critical” role of school-based services such as physical, occupational, and speech-language therapies and mental health services which often were disrupted during the pandemic. Other researchers have found service disruptions in these areas during the pandemic, noting that some services “may be challenging or even impossible to deliver virtually,” leaving children with special health care needs who could not receive in-person services with unmet needs. Further, according to DOE guidance, some children may be newly eligible for special education services, as those with disabilities related to long COVID can qualify for services under the IDEA or Section 504. For more information about eligibility under both laws, see Appendix A.
What are key issues to watch going forward?
As most schools returned to in-person learning in the fall of 2021, lawsuits have been filed in a number of states challenging government bans on school mask mandates as violating the rights of children whose health conditions put them at increased risk of severe illness or death from COVID-19. Although the CDC recommends distancing and masks for all staff and students regardless of vaccination status for in-person learning, some state and local governments have prohibited school districts from adopting school mask mandates. Multiple lawsuits have been filed arguing that these bans prevent children with disabilities from attending school safely in person, in violation of the Americans with Disabilities Act and Section 504. Federal district courts in Iowa, South Carolina, and Tennessee have granted preliminary injunctions blocking governors’ bans on school mask mandates. On the other hand, the 5th Circuit Court of Appeals has put on hold a Texas federal district court’s permanent injunction that blocked a governor’s ban on school mask mandates, which means that the ban will go into effect while the appeal is pending. Additionally, a Florida federal district court denied a motion for a preliminary injunction in a case seeking to block a similar governor’s ban. All of these cases are currently on appeal.
Some school districts are struggling to stay open amid the rapid spread of the Omicron variant. Despite calls from the Biden Administration, governors, and mayors for schools to remain open, many school districts have decided to temporarily return to remote learning following the recent spike in COVID-19 cases. School districts are facing high case rates among students and staff, making it difficult to re-open and maintain student safety. At the same time, returning to virtual learning makes it more difficult for school districts to provide all needed services to students with special education plans and may put these children at further risk for falling behind.
COVID-19 vaccine uptake among young children has slowed. Children ages 5 and older are now eligible to be vaccinated against COVID-19. Following an initial wave of enthusiasm and a slight uptick for a period in December, vaccine uptake among 5-11 year-olds, who recently became eligible, has declined. As of January 12, 2022, 27% of 5-11 year-olds and 64% of 12-17 year-olds have received at least one dose of the COVID-19 vaccine. There may be unique challenges to vaccinating young children, particularly those from low-income families who may face additional barriers to access, and Medicaid can play a role in facilitating access to vaccines for these children. Further, the US Food & Drug Administration’s (FDA) recently authorized booster shots of Pfizer-BioNTech’s COVID-19 vaccine for children ages 12 to 15.
Children who receive special education services already faced disparities compared to their non-disabled peers and lost instructional time and disruptions in access to related services during the pandemic have exacerbated those differences. Medicaid, together with CHIP, covers half of children with special education plans, and these children have greater health needs compared to children with special education plans covered by private insurance. This means Medicaid supports children with special education plans by providing both educationally and medically necessary services as well as ensuring that children receive the other medical and preventive services they need.
Methods
The data in this analysis draw from the 2020 National Survey of Children’s Health (NSCH), the most current data available. Parent responses to the questions “Has this child EVER had a special education or early intervention plan?...Children receiving these services often have an Individualized Family Service Plan or Individualized Education Plan” and “Is this child CURRENTLY receiving services under one of these plans?” were used to identify children who have a current special education plan. Children were determined to have a current special education plan if they have ever had a special education or early intervention plan and indicate they are currently receiving services under one of these plans. The NSCH and this analysis use the CSHCN Screener to identify children with special health care needs. To meet the criteria for having a special health care need, a child must experience a health consequence that is due to a medical or other health condition that has lasted or is expected to last for 12 months or longer. This analysis breaks down indicators by health insurance coverage status for children with special health care needs but does not include estimates for uninsured children or children who did not report coverage status. This is due to many of the estimates for these children not meeting the minimum standards for reliability.