On June 27,2025, the U.S. Supreme Court issued the opinion for Kennedy v. Braidwood Management, finding that the ACA requirement that most private insurers and Medicaid expansion programs cover preventive services recommended by the United States Preventive Services Preventive Task Force (USPSTF) with no cost-sharing is constitutional. In its decision, the Court affirmed that USPSTF members are appointed constitutionally, and the Secretary of Health and Human Services can remove USPSTF members at-will and directly review and block Task Force recommendations before they take effect.
In this case, the Supreme Court narrowly considered whether the structure of USPSTF violates the Appointments Clause, but did not review the litigants’ other claims about the Advisory Committee on Immunization Practices (ACIP), and the Health Resources and Services Administration (HRSA). The federal district court will now resume briefing on the consideration of the plaintiffs’ claim that the Secretary of Health and Human Services’ ratification of HRSA and ACIP recommendations violates the Administrative Procedure Act. For more analysis of the Court’s decision please see Kennedy v. Braidwood: The Supreme Court Upheld ACA Preventive Services but That’s Not the End of the Story.
Since the enactment of the Affordable Care Act (ACA) in 2010, more than 2,000 legal challenges have been filed in state and federal courts contesting part or all of the ACA. The most recent challenge involves the ACA requirement that most private insurance plans cover recommended preventive care services without cost sharing. In this case, Braidwood Management v. Becerra, Christian owned businesses and six individuals in Texas assert that (1) the requirements in the law for specific expert committees and a federal government agency to recommend covered preventive services is unconstitutional, and that (2) the requirement to cover preexposure prophylaxis (PrEP), medication for HIV prevention, violates their religious rights. If the plaintiffs prevail on either the constitutional or the religious claims, the government’s ability to require insurance plans to cover evidence-based preventive services without cost-sharing may be limited.
On September 7, 2022, Judge Reed O’Connor at the US District Court in the Northern District of Texas ruled partly in favor of the plaintiffs and partly in favor of the Department of Health and Human Services (HHS), which is defending the ACA. On March 30, 2023, Judge O’Connor issued a ruling for the remedy in this case, Braidwood Management v. Becerra, striking down part of the ACA’s requirement for no cost coverage of preventive services recommended or updated by the U.S. Preventive Services Task Force (USPSTF) on or after March 23, 2010 and finding that the requirement to cover PrEP medications for HIV prevention violates the rights of the plaintiffs who have religious objections to PrEP. The federal government appealed this decision and on May 15, 2023 the 5th Circuit Court of Appeals issued an administrative stay of the district court’s ruling. This means that the federal government can continue enforcing the preventive services requirement while the 5th Circuit considers the Department of Justice’s motion for a stay pending appeal. This brief explains the preventive services coverage requirements, the basis of the lawsuit, next steps in the litigation, and the potential implications.
Preventive Services Provision
The ACA requires most private health insurance plans to cover a range of recommended preventive services without any patient cost-sharing. Preventive services include a range of services including screening tests, immunizations, behavioral counseling, and medications that can prevent the development or worsening of diseases and health conditions. The preventive services that private plans and Medicaid expansion programs must cover are based on those receiving an A or B level recommendation by the U.S. Preventive Services Task Force (USPSTF), vaccines recommended by the Advisory Committee on Immunization Practices (ACIP), and the Health Resources and Services Administration (HRSA) based on recommendations issued by the Women’s Preventive Services Initiative and issued by the Bright Futures for Children program. As new recommendations are issued or updated, coverage must commence in the next plan year that begins on or after exactly one year from the recommendation’s issue date.
Judge Reed O’Connor has heard multiple challenges to the ACA
U.S District Judge Reed O’Connor, an appointee of President George W. Bush, has been the “go-to” judge for plaintiffs challenging the ACA. In 2018, he ruled that the entire ACA was unconstitutional because Congress zeroed out the tax penalty. The Supreme Court ultimately ruled the other way and upheld the ACA. In June 2019, Judge O’Connor issued a permanent injunction against the ACA’s contraceptive coverage requirement, blocking the federal government from enforcing it against employers and individuals who object to contraceptive coverage. Judge O’Connor has also ruled in favor of the plaintiffs in challenges to the ACA Section 1557.
Preventive Services Litigation
In the current case, Braidwood Management Inc. v. Becerra, the plaintiffs claim that the preventive services requirements for private health insurance are unconstitutional and the requirement to cover PrEP-specific coverage requirement violates the Religious Freedom Restoration Act (RFRA) (Table 2). The plaintiffs are six individuals and Christian owned businesses. Braidwood Management, a for-profit closely held organization, owned by a trust, with Dr. Steven F. Hotze, a religious Christian, as the sole trustee and beneficiary. Braidwood is self-insured and provides health insurance to its 70 employees. The other plaintiff is Kelley Orthodontics, a Christian professional association owned by plaintiff John Kelley. The plaintiffs are asserting both economic harm for having to pay more money for a health plan that includes services they do not want or need, and religious harm for having to include services they object to.
Plaintiff Claims
Position 1: The Preventive Services Provision violates the Appointments Clause
The plaintiffs contend that the ACA provisions violate the Appointments Clause of the US Constitution, which provides that “officers of the United States” may only be appointed by the president, subject to the advice and consent of the Senate. They claim that the members of USPSTF, ACIP and HRSA are “officers of the United States” who have not been appointed in conformity with the Appointments Clause because they were not nominated by the President and approved by the Senate. Rather, members of these bodies are appointed by the heads of agencies within HHS (Table 1). The plaintiffs are asking the court to declare all preventive-care mandates based on recommendations or guidelines issued by USPSTF, ACIP or HRSA after March 23, 2010 (the day the ACA was signed into law) as unconstitutional. The plaintiffs contend that the ACA does not allow the Secretary of HHS or the directors of the agencies within HHS to reject the recommendations made by the committees and is thus insufficient oversight.
Conversely, HHS contends that “there are numerous statutes that incorporate by reference independent recommendation without creating any requirements that the heads of the recommending bodies be appointed as officers of the United States.” They cite examples such as a public health regulation related to water standards for consumer products that outsources the development of those standards to a non-governmental organization. Similarly, they cite a law requiring states and designated database providers to use a format for an electronic database approved by an expert panel that is not subject to approval by the head of a federal agency.
|
|---|
| Table 1: Committees Issuing Recommendations for Preventive Services |
| Recommending Entity | Role of the Agency | Process for Appointments and Oversight |
| United States Preventive Services Task Force (USPSTF) | The U.S. Preventive Services Task Force is an independent, volunteer panel of national experts in disease prevention and evidence-based medicine. The Task Force works to improve the health of people nationwide by making evidence-based recommendations about clinical preventive services. | USPSTF members appointed by the Director of AHRQ to serve 4-year terms.
USPSTF recommendations are not subject to AHRQ oversight or approval. |
| Advisory Committee on Immunization Practices (ACIP) | The ACIP shall provide advice and guidance to the Director of the CDC regarding use of vaccines and related agents for effective control of vaccine-preventable diseases in the civilian population of the United States. | The Secretary of the U.S. Department of Health and Human Services selects the members following an application and nomination process.
Recommendations made by the ACIP are reviewed by the CDC Director, and if adopted, are published as official CDC/HHS recommendations which determines insurance coverage policy. |
| Health Resources and Services Administration (HRSA) – Women’s Preventive Services Initiative | HRSA is an agency of the U.S. Department of Health and Human Services that operates programs intended to provide equitable health care to people who are geographically isolated and economically or medically vulnerable. | HRSA contracts with an external organization, currently ACOG, to convene a panel of experts, the Women’s Preventive Services Initiative (WPSI) to make and update recommendations for women’s preventive services.
HRSA can accept or reject recommendations which determines insurance coverage requirements. |
| HRSA — Bright Futures for Children | HRSA (see above) | HRSA uses the guidelines developed by The Bright Futures Program to identify evidence-informed guidelines for preventive care screenings and routine visits for newborns through adolescents up to age 21. The American Academy of Pediatrics (AAP) convenes experts in pediatric care with support from HRSA to review scientific evidence and recommend updates. |
Plaintiff Position 2: The Preventive Services Provision violates the Nondelegation Doctrine
The plaintiffs contend the ACA’s preventive services provisions violate the nondelegation doctrine – based on the theory that since Article I of the Constitution vests legislative power in Congress, there are limits to the authority that Congress can delegate to federal administrative agencies. The current caselaw precedent requires statutes that delegate authority to agencies to supply an “intelligible principle” to guide and provide a boundary or limit on the agency’s discretion. The plaintiffs contend that an “intelligible principle” is lacking: “Yet there is nothing in the text of section 300gg-13(a) that purports to guide the discretion of [US]PSTF, ACIP or HRSA when choosing the preventive care that private insurance must cover.” The plaintiffs contend that this constitutional nondelegation problem can be averted if the phrase “current recommendations is construed to refer to the recommendations that existed when the ACA was signed into law.”
The plaintiffs point to comments in the Supreme Court’s opinion in Little Sisters of the Poor, as evidence that the current majority believes there could be a constitutional issue with delegation to HRSA for preventive services for women, including contraception: “On its face, then, the provision grants sweeping authority to HRSA to craft a set of standards defining the preventive care that applicable health plans must cover. But the statute is completely silent as to what those “comprehensive guidelines” must contain, or how HRSA must go about creating them. The statute does not, as Congress has done in other statutes, provide an exhaustive or illustrative list of the preventive care and screenings that must be included.” While the Little Sisters case, challenging the contraceptive coverage regulations, was not decided based on the nondelegation doctrine, there is growing speculation that the Supreme Court is poised to revisit the nondelegation doctrine to make it more difficult for Congress to delegate authority to federal agencies to address major policy details.
Plaintiff Position 3: The Preventive Services Provision violates the Religious Freedom Restoration Act
The plaintiffs assert the requirements to cover PrEP violates the Religious Freedom Restoration Act. Relying on the Supreme Court’s ruling in Burwell v. Hobby Lobby, the plaintiffs contend that employers are left with a “Hobson Choice” to provide health insurance that covers these medications and services that violate their religious beliefs or refuse to offer any health insurance to its employees. Notably, the plaintiffs state the requirement to cover PrEP “imposes a substantial burden on the religious freedom of those who oppose homosexual behavior on religious grounds” claiming further that PrEP drugs “facilitate and encourage homosexual behavior, prostitution, sexual promiscuity, and intravenous drug use.” The plaintiffs also contend the provision violates individuals who have religious objections and wish to purchase health insurance without PrEP coverage.
District Court’s Decision
Finding that Braidwood has standing to pursue its claims, on September 7, 2022, Judge O’Connor ruled that that the ACA’s delegation to U.S. Preventive Services Task Force violates the Appointments Clause because the Secretary cannot direct USPSTF to give a specific preventive service an “A” or “B” rating . The Court finds that the Secretary does not have any authority to direct which services are covered under § 300gg-13(a)(1) and concludes that USPSTF members are officers of the United States and that their selection does not comply with the Appointments Clause procedures. However, the Court also found that the ACA’s delegation to ACIP and HRSA are not in violation of the Appointments Clause since the Secretary of HHS effectively has the authority to ratify or not the ACIP and HRSA recommendations.
The court rejected the plaintiff’s nondelegation doctrine claims stating that the preventive care law met the criteria set out in prior Fifth Circuit cases on when Congress has properly provided an “intelligible principle” to guide agency discretion. Judge O’Connor noted that the Supreme Court might soon “reexamine or revive” the nondelegation doctrine, but it’s too early to predict a change in the nondelegation criteria from comments made in the Little Sisters case.
Relying on the reasoning in the Supreme Court’s decision in Hobby Lobby, the District Court also found that the requirement to cover PrEP violates Braidwood’s religious rights under the Religious Freedom Restoration Act (RFRA).
On March 30, 2023, District Court Judge O’Connor issued a ruling for the remedy in the case, Braidwood Management v. Becerra, striking down part of the ACA’s coverage requirement for preventive services. Effective immediately nationwide, the ruling blocks the federal government from requiring health plans to cover services recommended or updated by the U.S. Preventive Services Task Force (USPSTF) on or after March 23, 2010. The ruling did not affect coverage requirements for USPSTF services recommended prior to that date and also did not affect the requirement for plans to cover Women’s Preventive Services recommended by Health Resources and Services Administration (HRSA) or vaccines recommended by the CDC’s Advisory Committee on Immunization Practices (ACIP). Additionally, the judge ruled that the requirement to cover PrEP medications for HIV prevention violates the rights of the plaintiffs who have religious objections to PrEP. The federal government has appealed this decision to the United States Court of Appeals for the 5th Circuit. On May 15, 2023 the 5th Circuit Court of Appeals issued an administrative stay of the district court’s ruling. This means that federal government can continue enforcing the preventive services requirement while the 5th Circuit considers the Department of Justice’s motion for a stay pending appeal.
Implications for Coverage and Access to Preventive Services in Private Health Insurance
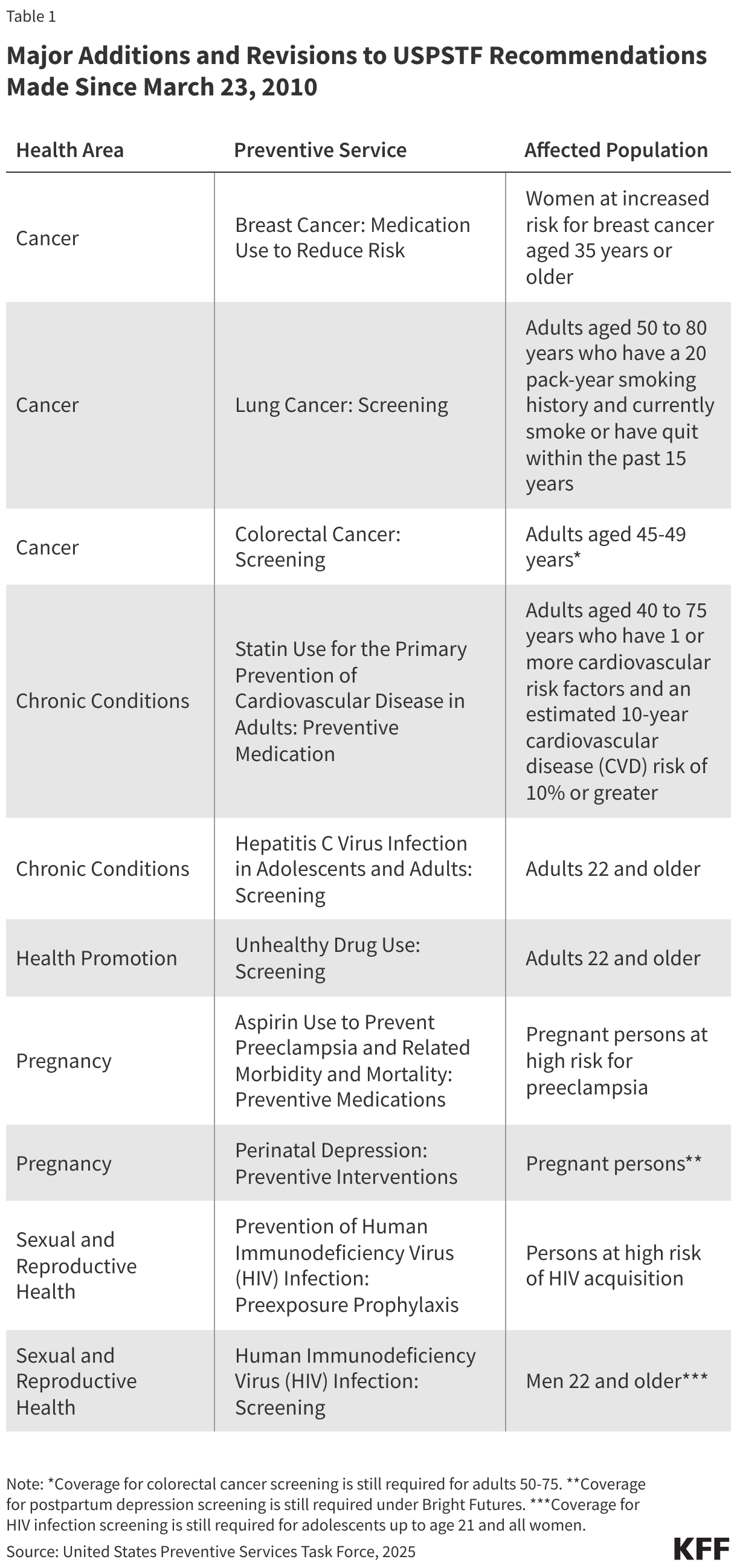
Even if the Court’s ruling upholds the authority of HRSA and ACIP, USPSTF recommendations include a broad range of services across multiple populations and health conditions. This includes cancer screenings, preventive medications for chronic conditions such as cardiovascular disease, counseling on health behaviors related to nutrition and weight management, alcohol and drug use, tobacco cessation services, screening for depression, and prenatal services, Elimination of the coverage requirements for USPSTF recommendations would invalidate the requirement to cover all of these services without cost sharing.
Religious Objections to PrEP Coverage
The ACA’s contraceptive coverage provision has been one of the most litigated parts of the law, with three cases brought by employers who object to the coverage on religious grounds reaching the Supreme Court. The Court’s ruling on the PrEP coverage requirement is the first time a court has ruled in favor of plaintiffs challenging another preventive service based on religious objections.
If employers who object to including coverage for PrEP in their plans are allowed to exclude the coverage, employees could lose coverage for a medication that could prevent the transmission of HIV and HIV related morbidity and mortality. PrEP reduces the risk of acquiring HIV by approximately 99% through sex and 74% through injection drug. Given that over 80% of PrEP users are covered by commercial insurers, this could have significant ramifications for cost and access should the ruling be applied broadly. The cash price for generic PrEP (Emtricitabine / Tenofovir), which is about 99% effective at preventing HIV through sex, is approximately $30 per month. This compares to an estimated lifetime HIV treatment cost of $420,285 ($1,079,999 undiscounted).
In addition, allowing employers to exclude PrEP because of religious objections has the potential to open the door to employers objecting to other services, such as vaccines.
Implications for Access to Preventive Services in Medicaid & Medicare
While the plaintiffs in Braidwood are only challenging the preventive services required in private health insurance plans, Medicaid and Medicare also have requirements for coverage of preventive services. States that have expanded Medicaid eligibility under the ACA must cover Essential Health Benefits (EHBs) as defined by the ACA. One of the categories of EHBs is preventive services, which CMS has defined to include the same services as required for private insurance plans. As a result, all states must cover the preventive services recommended by USPSTF, ACIP and HRSA for enrollees who qualify through the Medicaid expansion pathway. If this litigation is successful in challenging any of the preventive services required in private health insurance plans, the requirement for preventive services for enrollees who qualify through the Medicaid expansion pathway would be left to individual states to determine based on their state private insurance benchmark plan, which may not include all the services currently required.
While Medicaid relies on the same agencies to determine the recommended services as private insurance plans must cover, the process is slightly different under Medicare. In that case, under the national coverage determination process, the Secretary of HHS has the authority to determine coverage for preventive services for Medicare beneficiaries. The ACA eliminated Medicare cost sharing, including coinsurance and deductibles, for most preventive benefits that are rated A or B by the USPSTF, beginning in 2011, and authorized the Secretary of HHS to add coverage for new preventive services, using the national coverage determination process, if they are: reasonable and necessary for prevention or detection of illness; rated A or B by the USPSTF; and appropriate for Medicare beneficiaries. Coverage under Medicare for several preventive services, including some rated A or B by the USPSTF, predated the ACA and is specified in statute, and therefore would not be affected by any ruling on the current litigation.
The current litigation is brought by employers and individuals who allege economic and religious harm from the preventive services requirements in private health insurance. Any litigation challenging the preventive services requirements under Medicaid or Medicare would need to be brought by plaintiffs who suffer a tangible harm to establish legal standing.
Broader Implications
Overturning the preventive services requirement broadly would have significant implications for coverage of a broad range of clinical preventive services. Should the final decision for this case be found in favor of the plaintiffs, and applied nationwide, then millions of people may be vulnerable to loss of guaranteed coverage of preventive services without cost sharing. It will again be at the discretion of plans and employers to determine what preventive services will be covered and whether they will charge cost-sharing, lowering premiums in some cases, but likely creating a patchwork of coverage for these services. This could widen access barriers for groups that already face increased barriers dure to cost, including low-income people and people of color.
Should this case reach the US Supreme Court, the broader implications of a final decision in favor of the plaintiffs will depend on the basis for the ruling. The Court could rule in favor of the plaintiffs based on the Appointments Clause argument, similar to Judge O’Connor’s decision, finding that USPSTF members are officers of the United States who have not been properly appointed.
The potential implications are much broader, however, if the Supreme Court revisits and revises the nondelegation doctrine and restricts Congress’ ability to delegate the development of very precise standards to federal agencies. Without allowing the agencies to update the recommended preventive services, Congress would have to pass a new law every time the USPSTF recommends a new preventive service in order for it to be covered without cost-sharing. Any decision that changes the standard for Congress’ delegation could limit agency discretion to address a broad range of health and other issues through regulation.
Beyond preventive care, much of health policy and law has been developed through the delegation of authority to federal agencies to develop standards to address complex public policy and technical requirements—from the prescription drug approval process of the FDA to the apparatus set up to review and annually update the Medicare fee schedule. The ACA itself specifically left it up to the Secretary of HHS to define the essential health benefits that insurers must cover in the individual and small group insurance markets within the framework of the ten categories of items and services that Congress set out. The authority Congress gave to HHS to temporarily waive certain healthcare requirements during the COVID public health emergency is probably the best example of how delegated authority has functioned to benefit public health as well as access to public and private health insurance coverage. Any movement by the Court to restrict Congress’ authority to delegate in these areas could have a profound effect on the daily lives of Americans.
We do not know how quickly the United States Court of Appeals for the 5th Circuit will rule on this case. Ultimately, the parties are likely to appeal to the Supreme Court.
| Table 2: Braidwood v. Becerra: Litigation Challenging the ACA’s Preventive Services Provision: Summary of the Plaintiffs’ and Government’s Position |
Claim: The ACA preventive services provisions (42 U.S.C. § 300gg-13(a)(1)–(4)) Violate The Appointments Clause because the members of the committees act as “officers of the United States” and have not be properly appointed
The Appointments Clause provides: [The President] shall have Power, by and with the Advice and Consent of the Senate, to . . . appoint Ambassadors, other public Ministers and Consuls, Judges of the supreme Court, and all other Officers of the United States, whose Appointments are not herein otherwise provided for, and which shall be established by Law: but the Congress may by Law vest the Appointment of such inferior Officers, as they think proper, in the President alone, in the Courts of Law, or in the Heads of Departments.
U.S. Const. art. II § 2. Y |
Plaintiffs’ Position:
42 U.S.C. § 300gg-13(a)(1) – (4) allow the members of the U.S. Preventive Services Task Force, the Advisory Committee on Immunization Practices, and the Health Resources and Services Administration to unilaterally determine the preventive care that private insurers must cover.
These individuals are “officers of the United States,” because they “occupy a continuing position established by law” and exercise “significant authority pursuant to the laws of the United States.” Yet none of these officers have been appointed in conformity with the Appointments Clause. | Government’s Position:
The secretary’s ratification of the current preventive services coverage requirements defeats plaintiffs’ appointments clause claim
HRSA and the CDC (which ACIP Advises) are components of the HHS that exercise the secretary’s power and are under the secretary’s control.
The USPSTF is an independent body that does not exercise Executive Power. Its independent recommendations about the quality of evidence backing the effectiveness of certain preventive services is separate from any judgment about what should or should not be covered by health insurance, which latter judgment was made by Congress. |
| Claim: The ACA preventive services provisions (42 U.S.C. § 300gg-13(a)(1)–(4)) violate the nondelegation doctrine because Congress did not provide any details to guide the recommendations for preventive services |
Plaintiffs’ Position:
There is nothing in the text of section 300gg-13(a) that purports to guide the discretion of USPSTF, ACIP or HRSA when choosing the preventive care that private insurance must cover. | Government’s Position:
“Delegations are constitutional so long as Congress ‘lay[s] down by legislative act an intelligible principle to which the person or body authorized [to exercise the authority] is directed to conform.”
The grants of authority under 42 U.S.C. § 300gg-13(a) fall well within the wide range of delegations approved by the Supreme Court and the Fifth Circuit and are consistent with established limits on Congress’s power to delegate.
Congress did not “delegate” power to PSTF at all but instead incorporates its work. |
| Claim: Certain provisions of the ACA’s preventive services coverage requirements violate the Religious Freedom Restoration Act: requires the government to show the law in question, in this case the requirement that plans include coverage of PrEP without cost sharing, furthers a “compelling interest” in the “least restrictive means” when it “substantially burdens a person’s exercise of religion.” |
Plaintiffs’ Position:
The compulsory coverage of PrEP drugs, the HPV vaccine and the screenings and behavioral counseling for STDS and drug use violate the Religious Freedom Restoration Act (RFRA).
Plaintiffs are opposed for religious reasons to sexual activity outside of marriage between one man and one woman.
Requiring for providing Coverage of PrEP drugs facilitates and encourages homosexual behavior, intravenous drug use and sexual activity outside of marriage between one man and one woman. | Government’s Position:
The plaintiffs have failed to demonstrate the PrEP coverage requirement substantially burdens their religious beliefs.
The plaintiffs cannot identify any impact on their health insurance premiums arising from the requirement to cover PrEP drugs.
Even if the plaintiffs could show a substantial burden, the government has a compelling interest in countering the spread of HIV infections, and the plaintiffs have not argued that there is a less restrictive way of meeting this compelling interest (requiring private health insurance to cover PrEP without cost sharing). |