Key Takeaways
- Voters who say abortion is the most important issue to their vote are disproportionately younger, Democratic-leaning, and want abortion to be legal in all cases. In the two years post Dobbs, there seems to be a new generation of abortion voters largely made up of those who want abortion to be legal in all cases. Voters who say abortion is the “most important issue” in their 2024 vote (12% of all voters) are disproportionately made up of Black voters, Democratic voters, women voters, and the youngest voting bloc – voters ages 18 to 29.
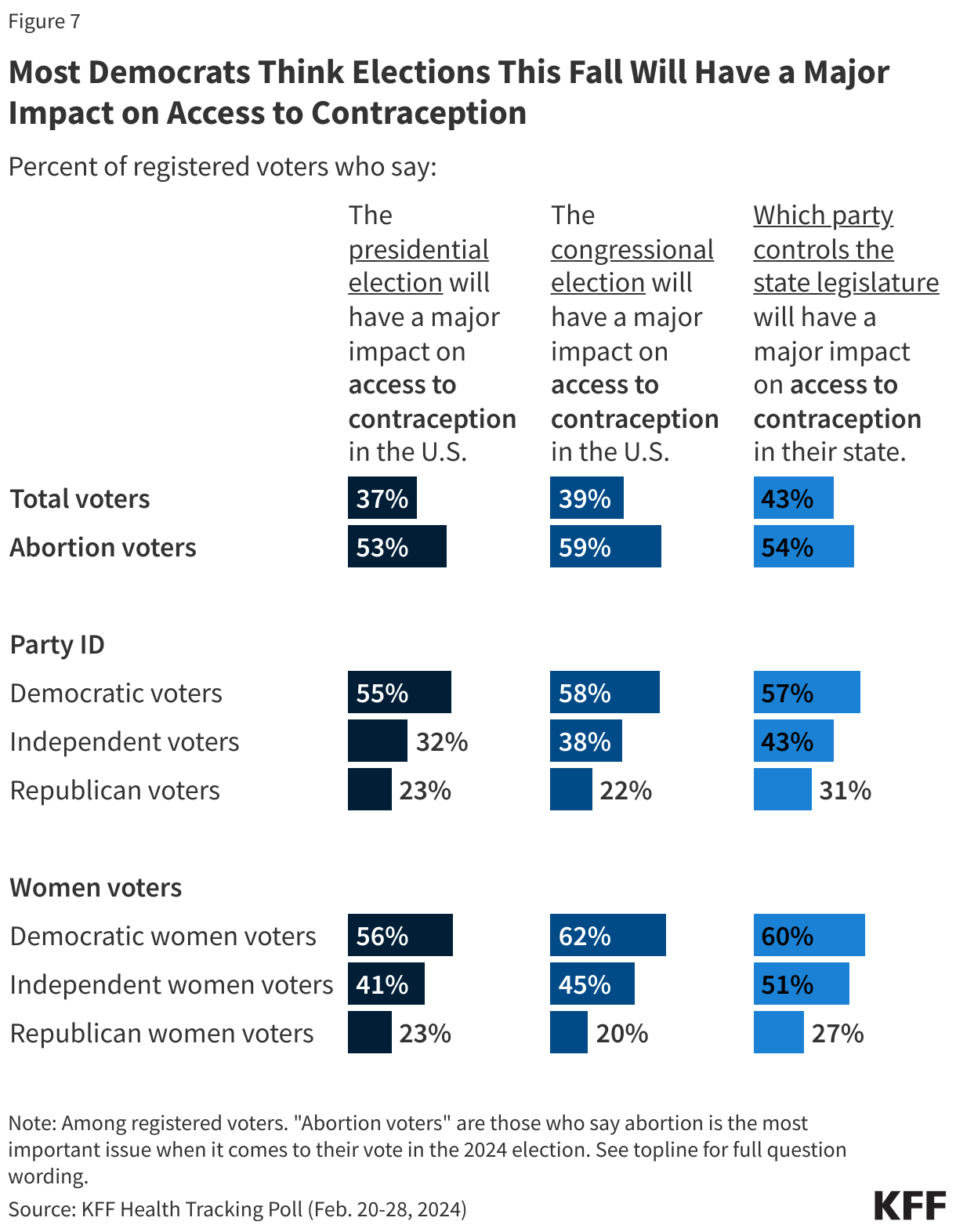
- Many voters, especially Democrats, see the 2024 election as a high-stakes election for determining the future of access to abortion and contraception. Half of voters say they think the elections for president, Congress, and state legislatures will have a “major impact” on access to abortion, rising to two-thirds of Democratic voters and seven in ten voters who say abortion is their most important voting issue. About four in ten voters overall say the same about the perceived impact of the elections on access to contraception, though there are stark partisan divides on this outlook. At least half of Democratic voters say they think the elections will have a “major impact” on access to contraception, whereas three in ten or fewer Republican voters say the same.
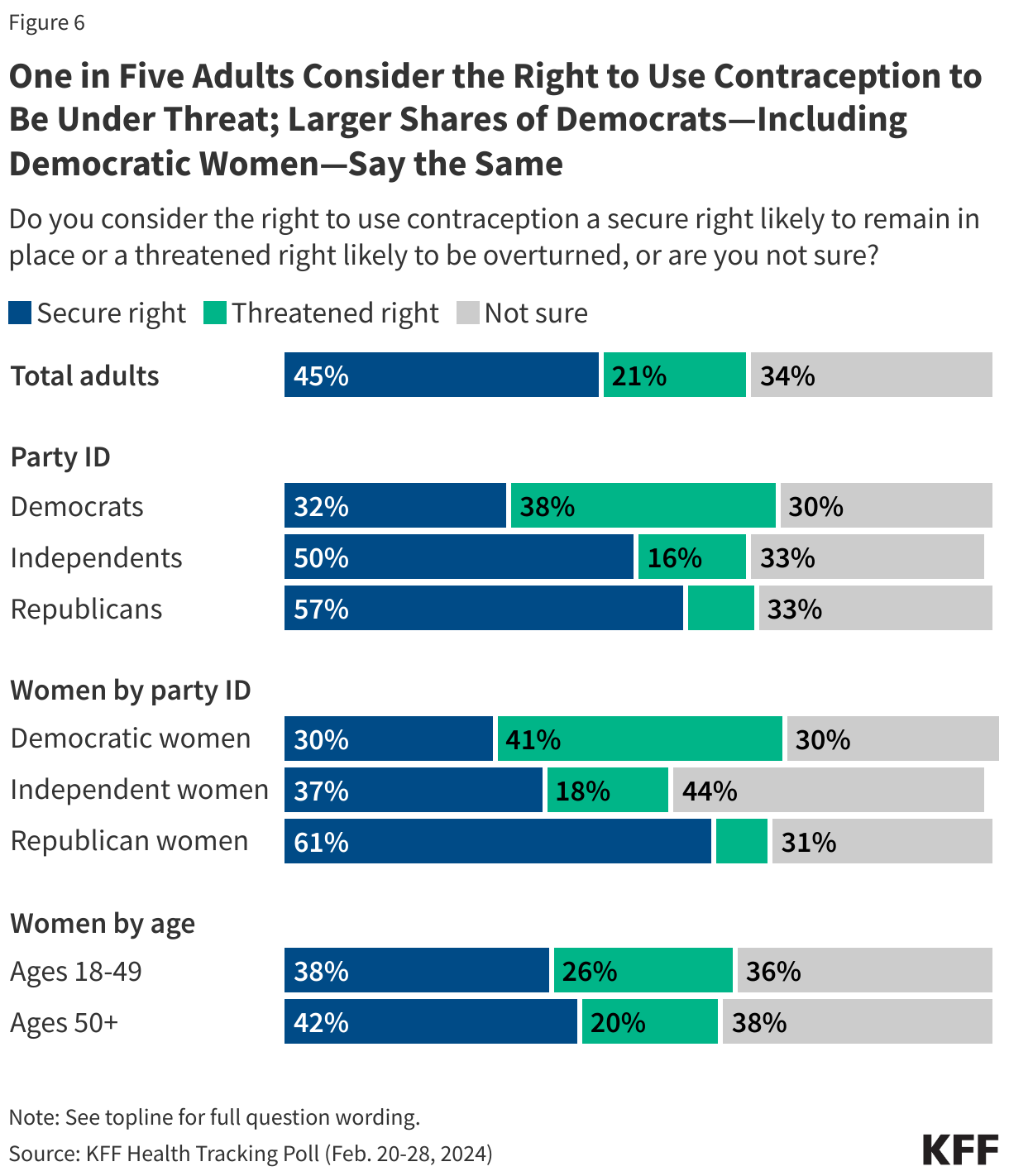
- Less than half of adults say the right to use contraception is a “secure right.” Following the Dobbs decision, uncertainty around people’s ability to access contraception emerged, while the recent Alabama Supreme Court ruling on IVF further ignited public debate on the impact of abortion bans on access to other health services. Less than half of adults (45%) say they consider the right to contraception a “secure right likely to remain in place,” about one in five (21%) adults consider the right to use contraception a threatened right likely to be overturned, and an additional third (34%) are “not sure” if the right is threatened or secure. Views on this topic diverge widely by partisanship, with Democrats nearly four times more likely to say they view the right to use contraception as threatened than are Republicans (38% vs. 10%).
- There is broad support, even among partisans, for protecting access to abortions for patients who are experiencing pregnancy-related emergencies and protecting patients’ right to travel to access abortions, but partisans disagree on other policy proposals such as whether there should be a federal right to abortion or a nationwide 16-week abortion ban. Two-thirds of the public, including majorities of Democrats (86%) and independents (67%), support a law guaranteeing a federal right to abortion. Yet, this is opposed by nearly six in ten Republicans (57%). In addition, while among the public overall about six in ten (58%) oppose a 16-week abortion ban, a majority of Republicans (63%) adults support this proposal, while most Democrats (75%) and independents (59%) oppose it.
- The group most impacted by reproductive health policy in this country – women ages 18 to 49 – see the upcoming election as a pivotal moment and largely support laws protecting access to abortions. One in six (16%) women of reproductive age (18-49) say abortion is the most important issue in their 2024 vote and about half say the 2024 elections will have a “major impact” on abortion access in the country and their own state. Women of reproductive age overwhelmingly say decisions about abortions should be made by a woman, in consultation with her doctor (86%), two-thirds (65%) want the federal government to pass laws to protect abortion nationwide, and at least two thirds support laws protecting access to abortions for patients experiencing pregnancy-related emergencies (88%), protecting a patient’s right to travel to get an abortion (79%), and guaranteeing a federal right to abortion (76%).
- Reflecting strong Trump support, Republicans trust former President Trump on abortion policy, regardless of their own views on the issue. While 85% of Republican voters who want abortion to be illegal in all or most cases say they trust former President Trump more than President Biden on the issue of abortion, half of Republican voters who want abortion to be legal in all or most cases also say they trust Trump more than Biden on this issue, suggesting that former President Trump is able to connect with many Republican voters regardless of their own views on abortion, including many of those who are more supportive of abortion access. This may be largely because few (4%) of Republicans who want abortion to be legal see abortion as the most important issue to their vote.
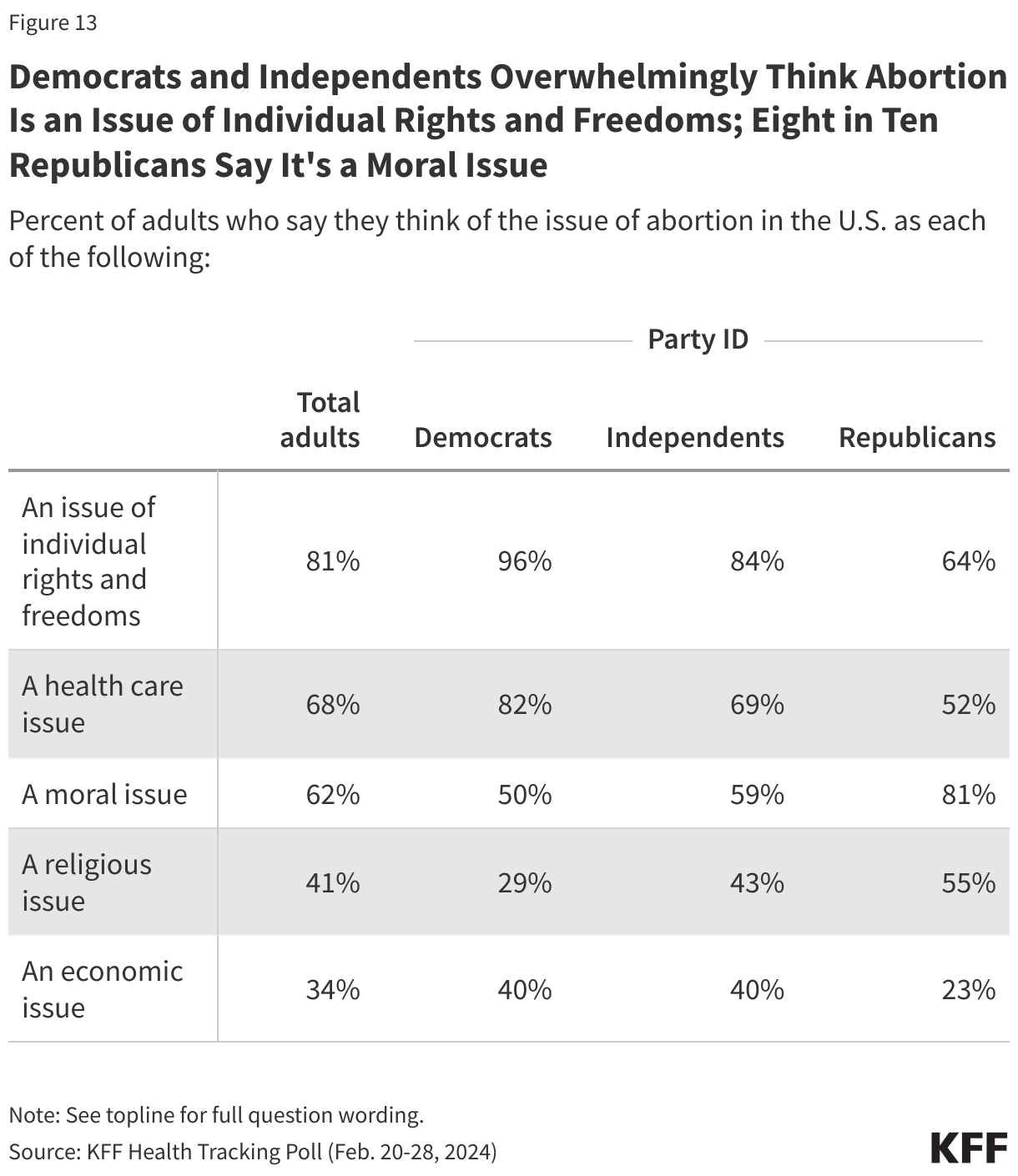
- Democrats and Republicans hold very different views on how they see the issue of abortion. The large partisan disagreement on proposals aimed at legislating abortion access may be driven by how differently Democrats and Republicans view the issue. Democrats overwhelmingly view the issue of abortion as an issue of individual rights and freedom (96%) as well as a health care issue (82%). Republicans, on the other hand, are more likely to view it as a moral issue (81%) and more than half (55%) of Republicans also say it is a religious issue.
- About two-thirds of the public have not heard anything about an upcoming Supreme Court case that may impact if and how patients can access mifepristone (medication abortion). In addition, many adults are at least somewhat confused by the abortion laws in their state and uncertain about the legality and use of mifepristone.
How Voters See Abortion as a Voting Issue
With former President Trump and President Biden now the presumptive presidential nominees for both parties, the focus of voters has shifted from the presidential primaries to the 2024 general election and how the candidates’ positions on key voting issues could impact voters’ decisions. Last month’s KFF Health Tracking Poll showed that partisans supported their own candidates when it came to two key health care issues: affordability and the ACA. This month’s poll explores voters’ preferences on another key voting issue: abortion.
Abortion Voters Are More Likely to be Women Voters, Black Voters, Younger Voters, and Democratic Voters
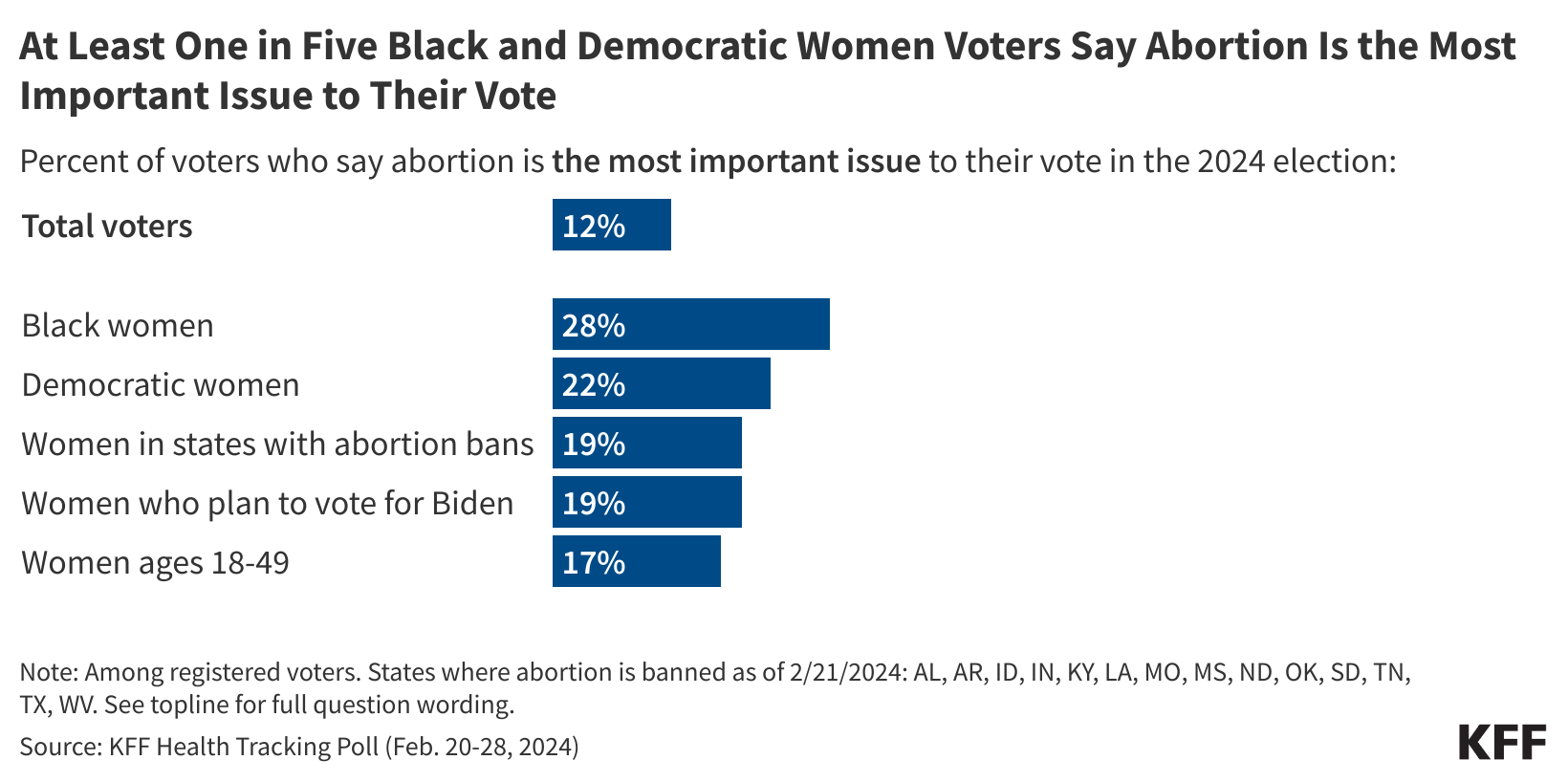
With many issues competing for voters’ attention during this election cycle, one in eight voters (12%) say abortion is the “most important issue” to their vote in the 2024 election while half of voters (52%) say it is a “very important issue but not the most important.” About one in three voters say either abortion is “somewhat important” (22%) or “not an important issue” (14%) to their 2024 vote.
The share saying abortion is the “most important issue” includes 16% of all women voters and rises to more than one in four Black women voters (28%), and about one in five in other key voting groups of women including Democratic women (22%), women who currently live in states where abortion is banned1 (19%), women voters who say they plan to vote for President Biden (19%), and women of reproductive age (ages 18 to 49) (17%). At least two-thirds of each of these groups say they think abortion should be legal in all or most cases.
Prior to the Supreme Court decision overturning Roe v. Wade, pro-life proponents and Republicans were the voters most likely to identify as “single issue abortion voters.” In fact, twenty years ago pro-life adults were nearly three times as likely as pro-choice adults to describe themselves as single-issue voters on abortion. And in 2020, prior to the 2022 Dobbs decision, a larger share of pro-life voters than pro-choice voters said abortion was important to their vote.
Yet, post Dobbs, there seems to be a new generation of abortion voters. These voters are largely made up of those who want abortion to be “legal in all cases.” They also are disproportionately made up of Black voters, Democratic voters, women voters, and the youngest voting bloc – voters ages 18 to 29. In contrast, about one in three voters who say abortion is the most important issue to their vote think abortion should be “illegal in all or most cases.”
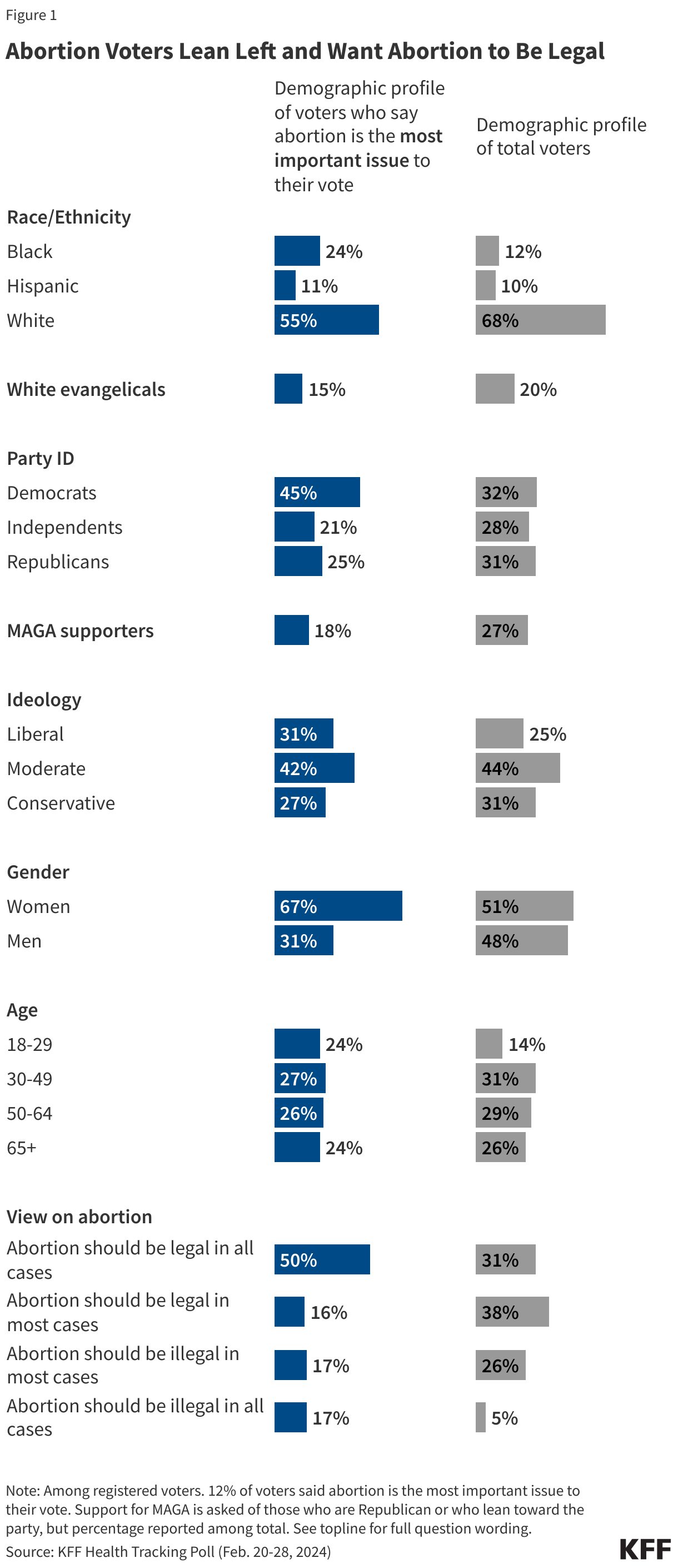
Reflecting their Democratic leaning, about half of abortion voters say if the 2024 presidential election was held today, they would vote for Democrat Joe Biden (48%) while one in four (26%) say they would vote for Republican Donald Trump. A quarter of these voters say they would either vote for some other candidate (16%) or they wouldn’t vote (9%). This group also went for President Biden over President Trump in the 2020 election by a nearly two to one margin (50% v. 27%). About one in five in this group say they didn’t vote in the 2020 presidential election.
Slightly less than half of abortion voters (45%) say they are “more motivated” to vote in this presidential election compared to previous ones while about a quarter (23%) say they are “less motivated” to vote. Similarly, overall, 44% of voters say they are more motivated to vote in this year’s presidential election.
While abortion may not be a top voting issue for independent voters or Republican voters, the issue may move small numbers within these groups to vote for President Biden – which could matter in tight races. While just five percent of independent voters identify abortion as their most important issue and say if the election was held today, they would vote for Biden, overall one-third of independent voters want abortion to be legal and plan on supporting Biden. Among Republicans, less than 1% identify abortion as their most important issue and plan on crossing the political aisle to vote for Biden, but overall 3% of Republicans want abortion to be legal and say that if the election was held today, they would vote for President Biden.
Partisan Voters Trust Their Own Party More on Abortion Policy, But Significant Shares Say They Trust Neither Party nor Either Presidential Candidate
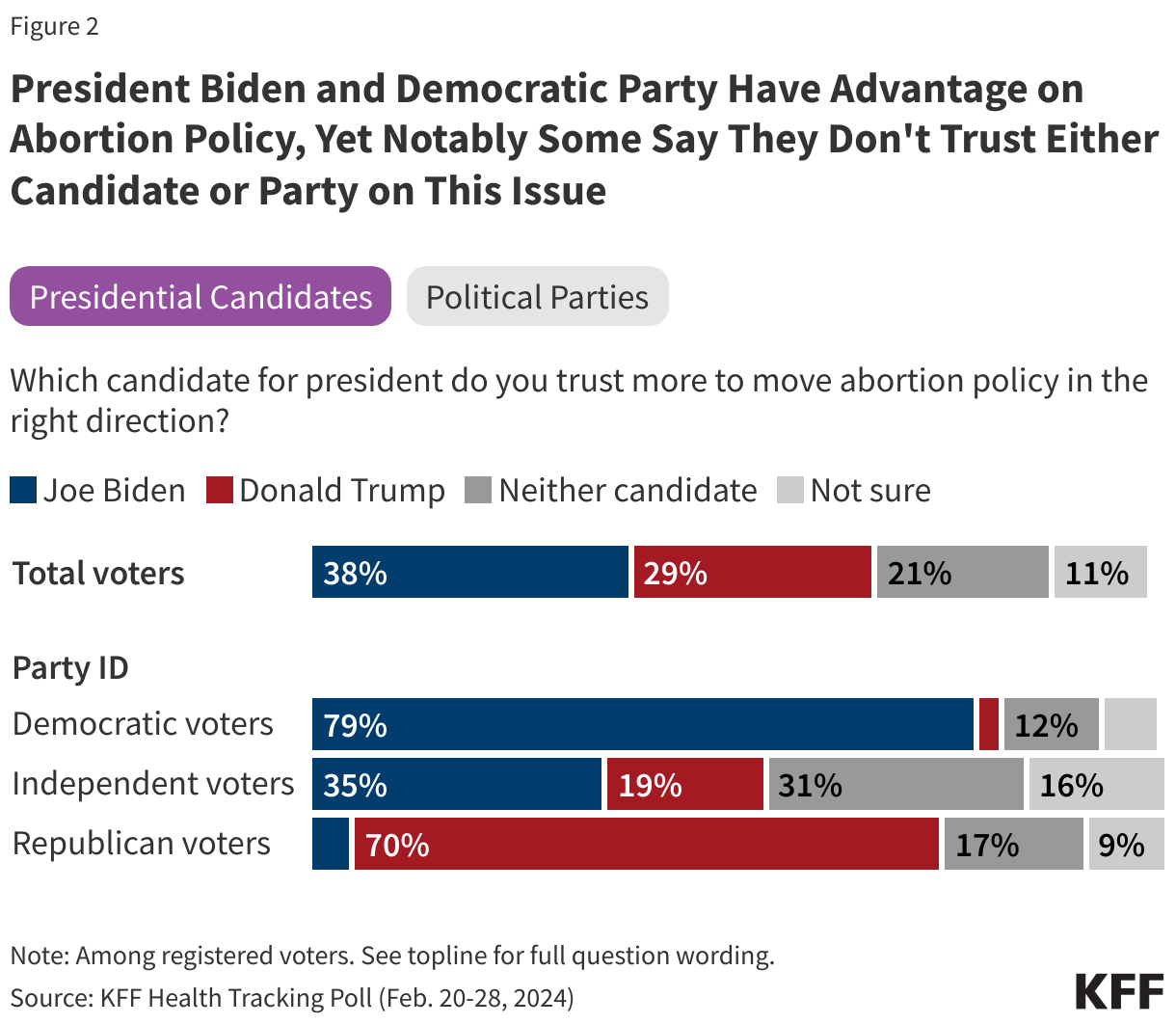
While voters overall are split largely by their partisan identification in who they are planning on supporting in the upcoming presidential election, President Biden has an advantage over former President Trump on who voters trust more to move abortion policy in the right direction. Four in ten voters (38%) say they trust Biden, compared to three in ten (29%) who say they trust Trump. A notable share of voters say either that they don’t trust either candidate to move abortion policy in the right direction (21% of voters) or that they are unsure (11%).
Partisans largely say they trust their own party’s candidate on abortion. Eight in ten (79%) Democratic voters say they trust President Biden, and seven in ten (70%) Republicans say they trust former President Trump. Independent voters give President Biden the advantage on the issue of abortion with a third saying they trust him on this issue (35%) compared to 19% who say they trust former President Trump. However, one in three independent voters (31%) say they don’t trust either candidate on this issue as do more than one in ten Democratic voters (12%) and one in six Republican voters (17%).
The same trends emerge when examining which political party voters trust more on abortion policy. The Democratic Party overall garners more trust among voters on abortion policy than the Republican Party (41% vs. 27%) – but still don’t have a majority of voters’ trust. And while each party garners majority support from their own partisan voters and the Democratic Party has a more than two to one advantage among independent voters (38% v. 15%), a significant share of independent voters (39%) say they trust neither party. One in four (24%) Republican voters say they trust neither party on the issue of abortion, which is more than twice the share of Democratic voters who say the same (10%).
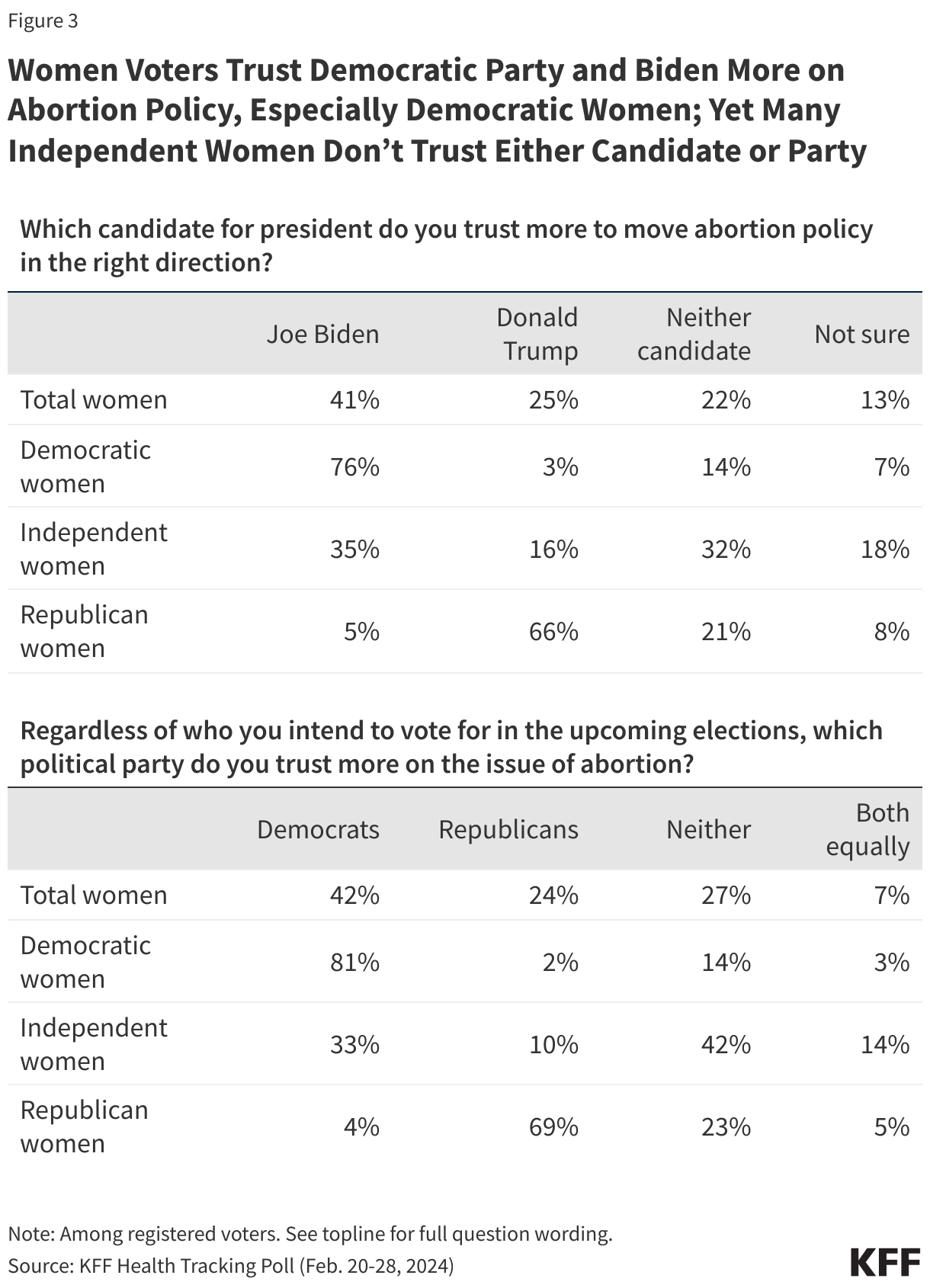
Women voters overall say they trust both the Democratic Party and President Joe Biden more on abortion policy in this country, but trust varies depending on partisanship and age. In fact, neither candidate nor party garners majority of support from women of reproductive age.
Most Republican women voters trust former President Trump and the Republican Party to move abortion policy in the right direction, but one in five say they don’t trust either candidate or they don’t trust either party. On the other side of the political aisle, at least three-fourths of Democratic women voters say they trust President Biden and the Democratic Party more on abortion policy and about one in seven say they don’t trust either candidate or political party.
Independent women voters are more than twice as likely to say they trust Biden (35%) than Trump (16%) to move abortion policy in the right direction. Similarly, a larger share of independent women voters give the Democratic Party an advantage over the Republican Party (33% v. 10%), but neither candidate nor party gets a majority of independent voters saying they trust them more on this issue. In addition, about a third of independent women voters say they trust neither candidate (32%) and four in ten say they trust neither party (42%) on this issue. This suggests at least some independent women voters may be looking for different leadership from the political parties and the party’s candidates for president on this key issue.
Half of Republicans Who Want Abortion to be Legal Trust Trump and Republican Party on this Issue, Most Don’t Associate Trump with the Overturning of Roe
About four in ten Republican voters (43%) say they think abortion should be legal in all or most cases. Among this group of voters, half (52%) say they trust the Republican Party more on the issue of abortion, 8% say they trust the Democratic Party, and one in three (33%) say they don’t trust either political party on this issue.
Similarly, half of these Republican voters (those who want abortion to be legal) say they trust former President Trump more to move abortion policy in the right direction, while 9% say they trust President Biden, and more than a quarter (28%) say they don’t trust either candidate. Among Republicans who say abortion should be illegal in all or most cases, both former President Trump and the Republican Party garner majorities of trust on this issue (85% and 80%, respectively). Republicans who say abortion should be illegal are more likely to be single-issue abortion voters (14%, 8% of total Republican voters) than those who say abortion should be legal (4%, 2% of total Republican voters).
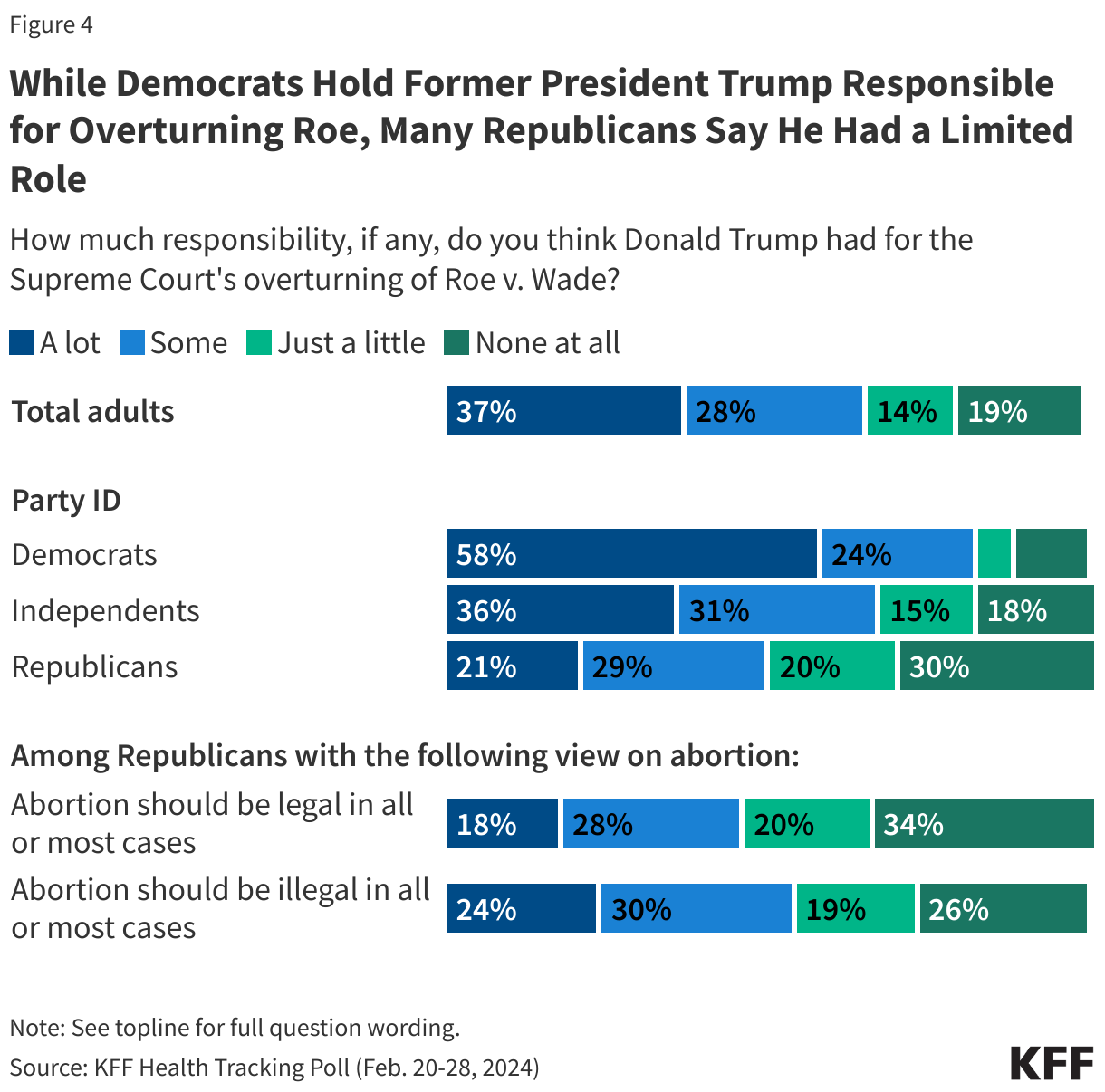
Republican voters, regardless of their views on whether abortion should be legal or illegal, are divided in former President Trump’s role in the overturning of Roe v. Wade – though leaning in slightly different directions. While former President Trump has taken credit for the 2022 Dobbs decision in past speeches because he had appointed three conservative judges which led to the ruling, a majority of Republican voters who want abortion to be legal (56%) say Trump had “just a little” or “no responsibility” in the overturning of Roe v. Wade. On the other hand, more than half of Republican voters who want abortion to be illegal (54%) say he has at least some responsibility.
Overall, two-thirds of voters (65%) say former President Trump had at least some responsibility for the overturning of Roe v. Wade, but this is largely driven by the views of Democrats (83%) and independents (64%).
Half Of Voters Say The Elections This Fall Will Have A “Major Impact” On Access To Abortion
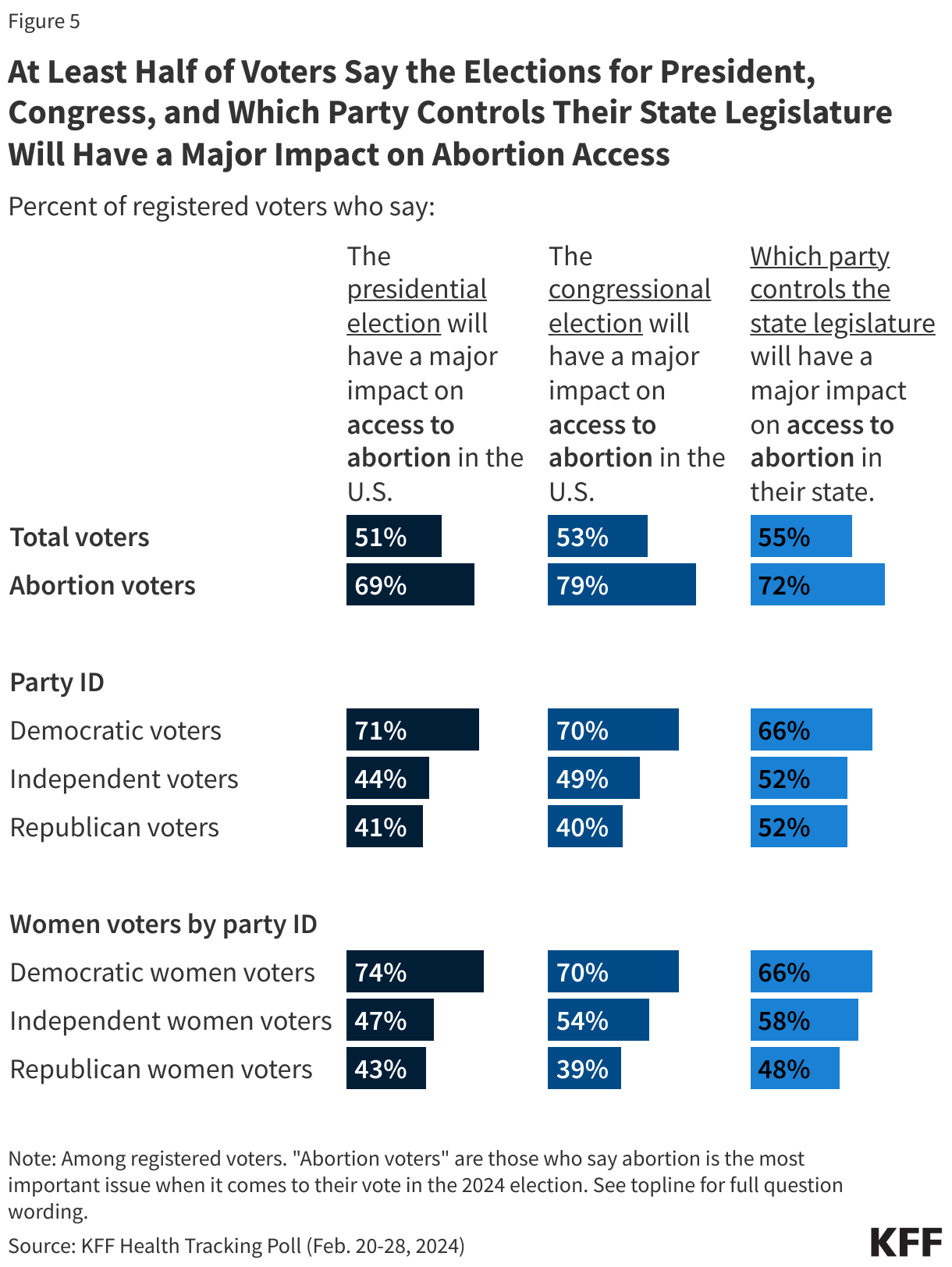
Large shares of the public say they think the elections this fall will impact access to abortion both in this country and in their own states. At least half of voters overall say this year’s elections for president (51%), Congress (53%), as well as which party controls their state legislature (55%) will have a “major impact” on access to abortion in the U.S. and their state, respectively. At least seven in ten single-issue abortion voters say each of these elections will have a “major impact” on abortion access in the U.S. or their state.
Other than single-issue abortion voters, Democratic voters are the most likely to say the elections will matter, with at least two-thirds saying they think the elections will have a “major impact” on abortion access in the U.S. and their state. About four in ten Republican voters say the same when considering the presidential (41%) and Congressional (41%) elections, rising to about half (52%) who say which political party controls the legislature in their state will have a “major impact” on access to abortion in their state. The views of women voters by partisanship largely mirror the patterns on these questions among partisans overall.
One In Five Adults Consider the Right to Use Contraception Threatened, And Most Democratic Voters Say the Upcoming Election Will Have a Major Impact on Access to Contraception
Following the Dobbs decision and Justice Clarence Thomas’ concurrence opinion which questioned the basis for a prior Supreme Court case granting the right to contraception, many predicted that contraception access also could be affected. The recent Alabama Supreme Court ruling that frozen embryos can be considered children further ignited public debate on the impact of abortion bans on access to other health services.
Just under half (45%) of adults say they consider the right to use contraception “a secure right likely to remain in place,” while one in five (21%) say they consider the right to use contraception “a threatened right likely to be overturned.” A third (34%) are “not sure” if the right to use contraception is threatened or secured.
Partisans are split, with Democrats more likely to see the right to contraception as threatened, while Republicans see it more as a secure right. About four in ten Democrats (38%) – including four in ten (41%) Democratic women – consider the right to contraception threatened, whereas about six in ten Republicans (57%) – including six in ten Republican women (61%) – say they consider contraception access secure. At least three in ten across partisans say they are not sure about the future of the right to contraception. Similar shares of women of reproductive age (18 to 49) and women ages 50 and older consider the right to use contraception secure, with about four in ten saying so.
When asked specifically about how the elections this fall may impact access to contraception in the U.S., about four in ten voters overall say the elections for president (37%), Congress (39%), and which party controls the legislature in their state (43%) will have a “major impact.” About half or more of single-issue abortion voters say the presidential election (53%), Congressional election (59%) or which party controls the legislature in their state (54%) will have a “major impact” on access to contraception. And majorities of Democratic voters say they think the three elections will have a “major impact” on access to contraception, whereas three in ten or fewer Republican voters say the same.
Majorities Say Abortion Decisions Should Be Made by Women and Their Health Care Providers
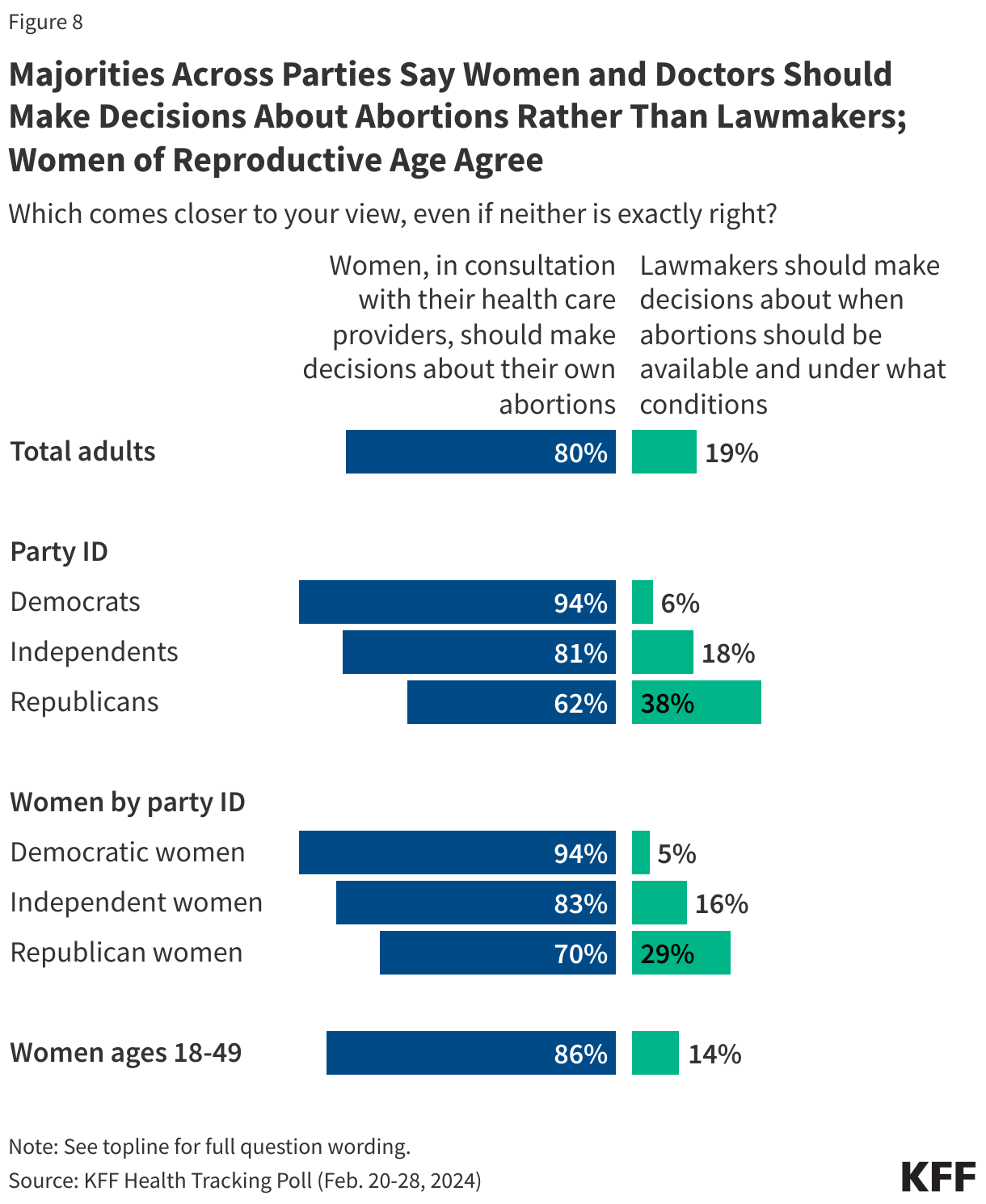
The public overwhelmingly thinks decisions about abortions should be made by women in consultation with their health care providers (80%), while 19% say lawmakers should make decisions about when abortions should be available and under what conditions. The share who say the decision-making should fall to women remains unchanged since the Dobbs decision and includes large majorities of Democrats (94%) and independents (81%), and most Republicans (62%).
Nearly nine in ten (86%) women between the ages of 18 and 49 say decisions about abortion should be made by women and their health care providers, as do almost all Democratic women (94%), eight in ten independent women (83%), and seven in ten Republican women (70%).
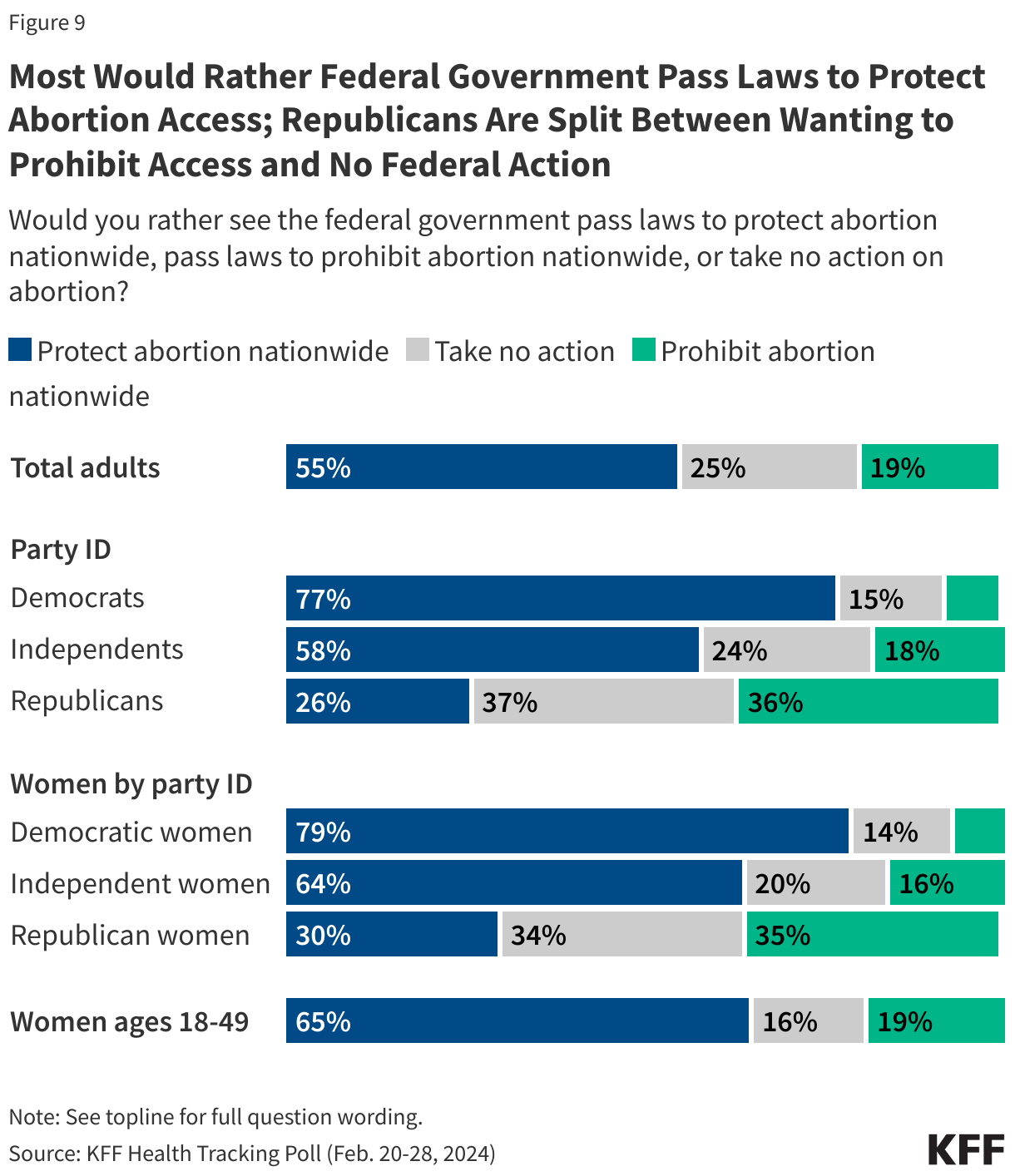
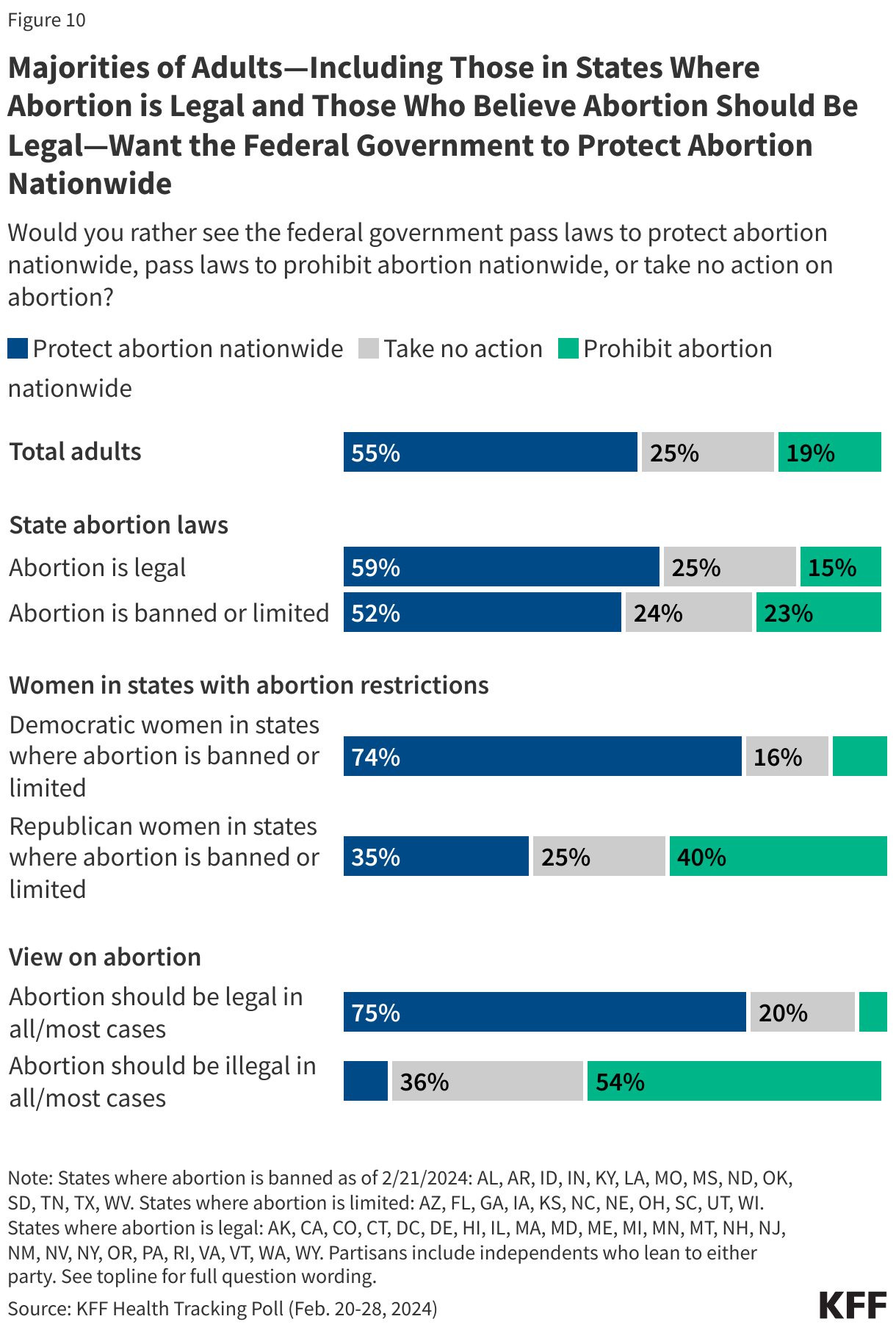
While most of the public doesn’t think lawmakers should decide when abortions should be available, many states are passing laws regulating abortion access and there has been public debate about whether the federal government should take action on this issue. Overall, a majority of the public (55%) say they would rather see the federal government pass laws to protect abortion access nationwide, while a quarter (25%) say they want to see the federal government take no action, and a fifth (19%) want the federal government to pass laws prohibiting abortions.
Three in four Democrats (77%) say they would rather see the federal government pass laws to protect abortion access, as do six in ten (58%) independents. Republicans, on the other hand, are divided between wanting the federal government to pass laws prohibiting abortions nationwide (36%) and wanting the federal government to not act on this issue (37%). About a quarter (26%) of Republicans want the government to pass laws to protect abortion nationwide.
Women of reproductive age want the federal government to pass laws to protect abortion nationwide (65%), as do large majorities of Democratic women (79%) and independent women (64%). Republican women are more divided with similar shares wanting the government to pass laws prohibiting abortion (35%), take no action (34%), and pass laws to protect abortion (30%).
In states where abortion is either banned or limited, half of adults (52%) say they would rather see the federal government pass laws to protect abortion nationwide including three-fourths (74%) of Democratic and Democratic-leaning women living in those states. Republican and Republican-leaning women living in states where abortion is banned or limited are divided with similar shares who say they want the federal government to pass laws prohibiting abortion nationwide (40%) as say they want laws protecting abortion nationwide (35%).
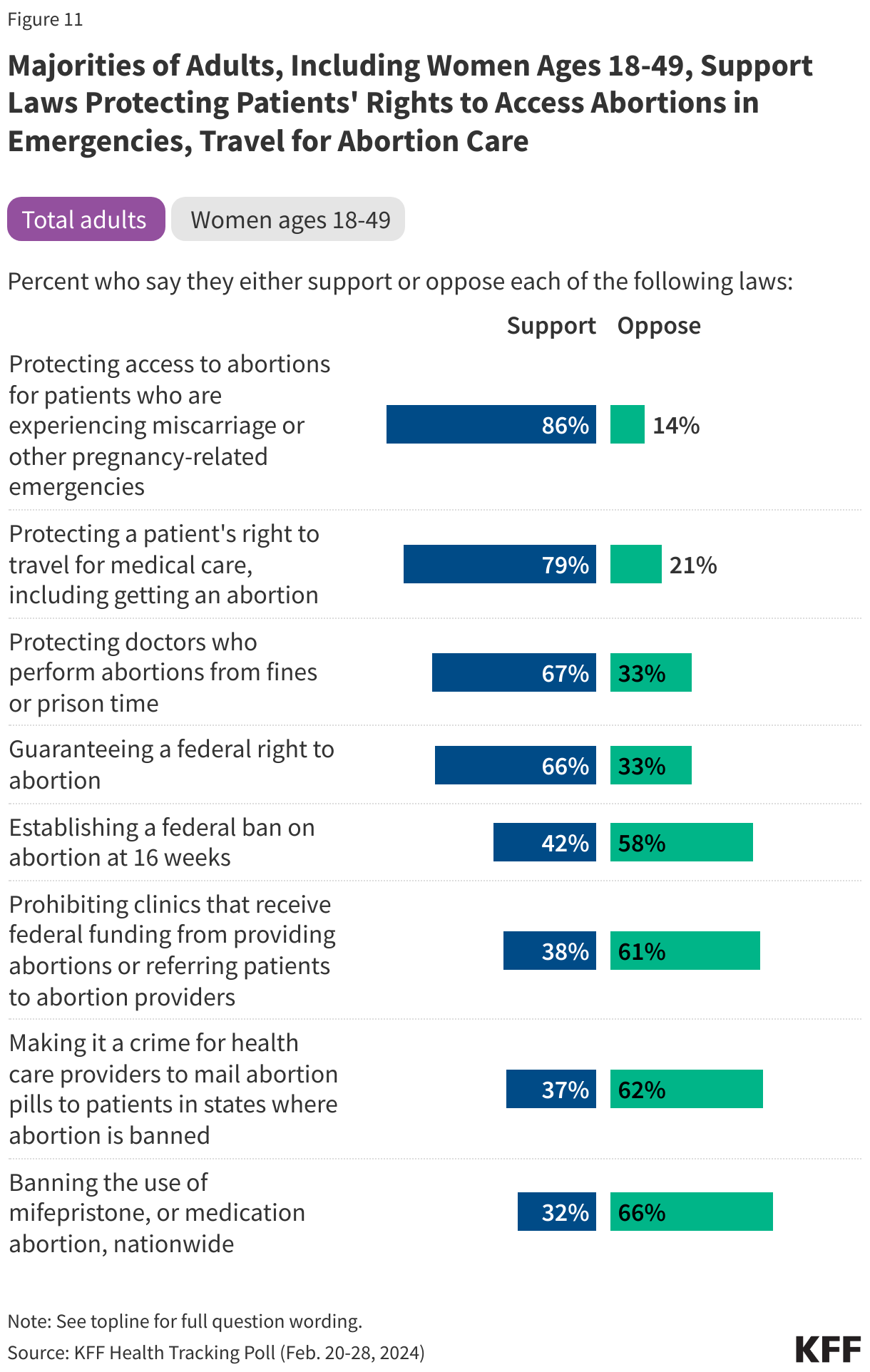
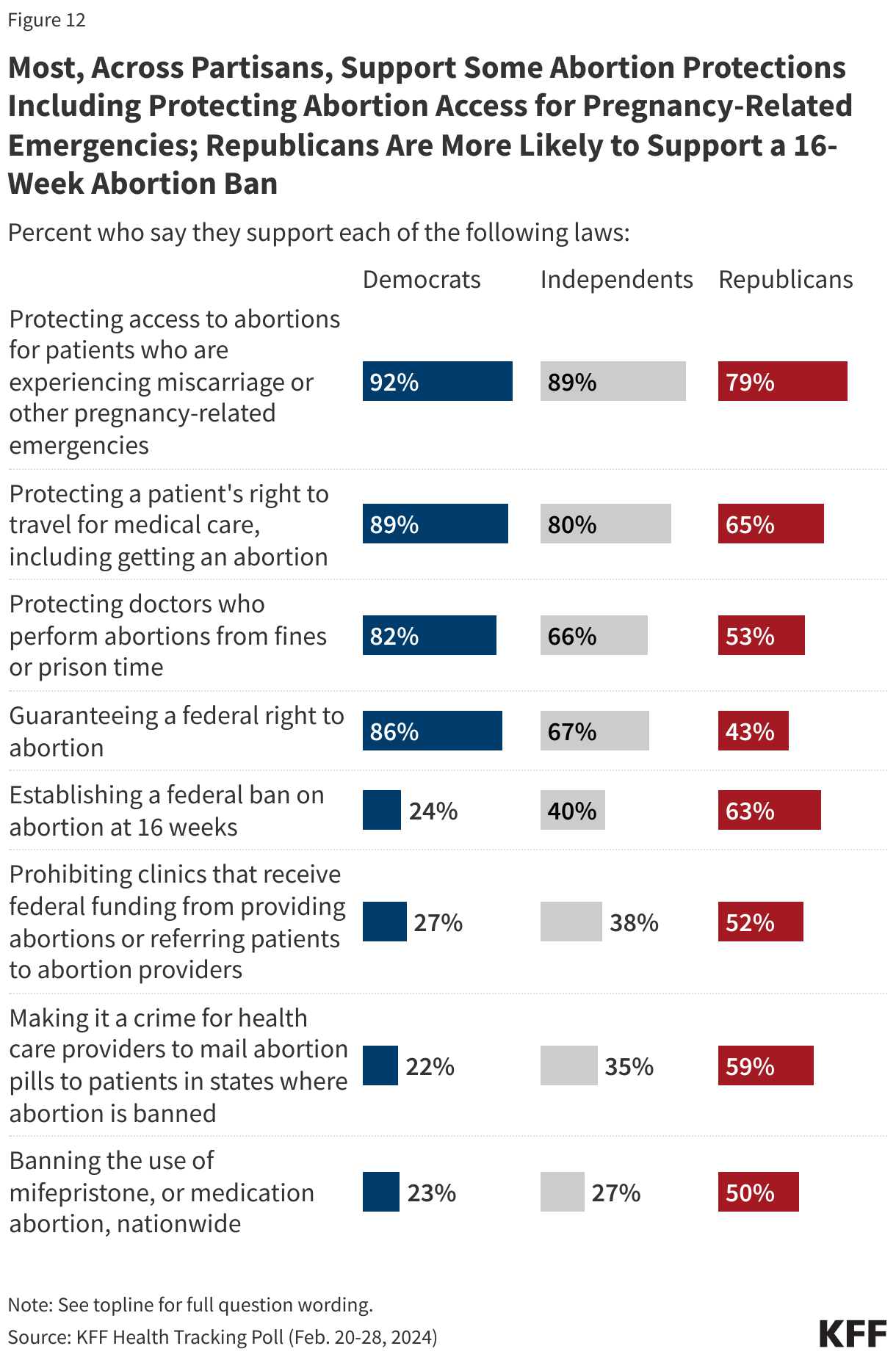
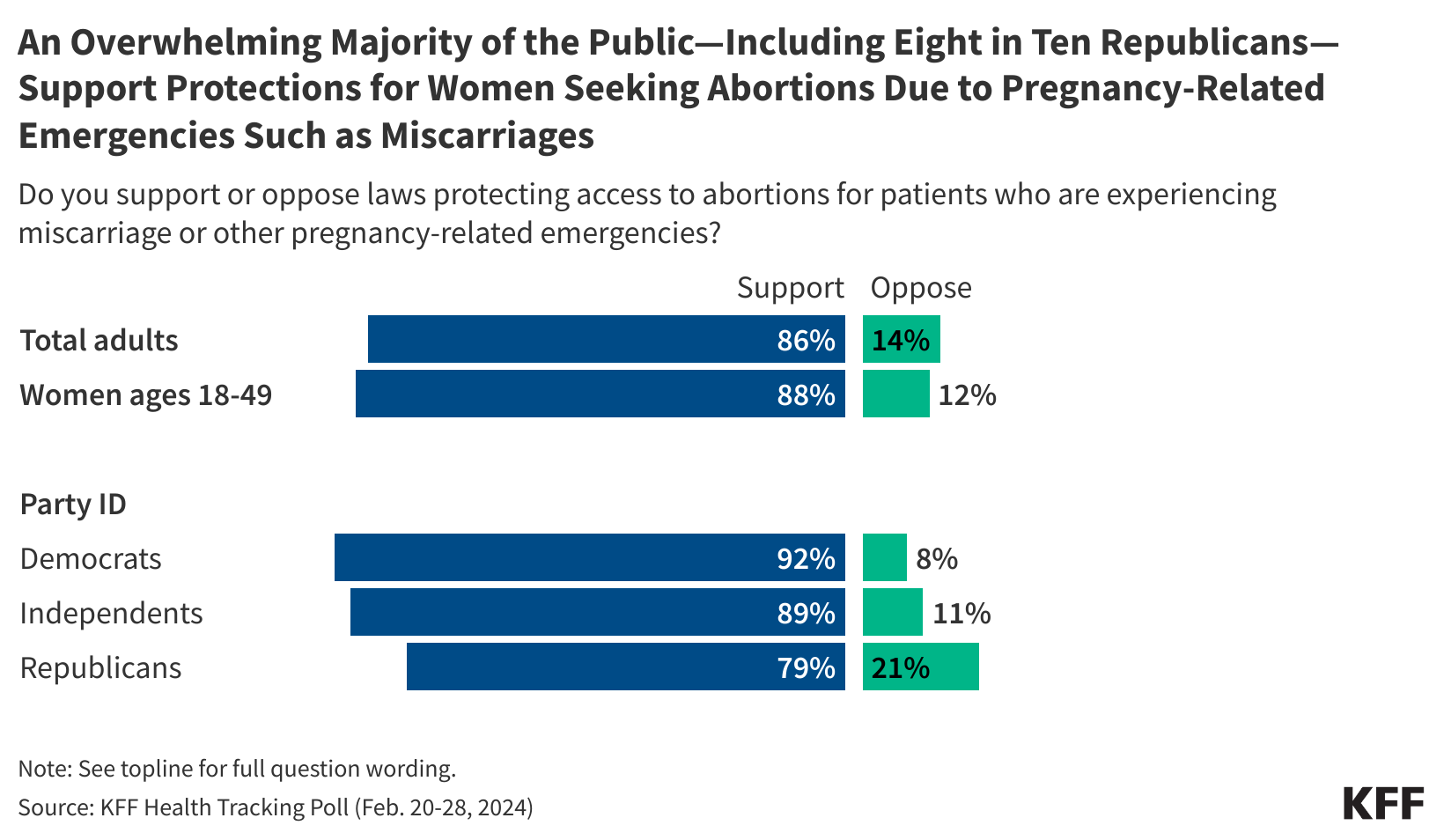
Overall, a majority of the public supports protecting access to abortions for patients who are experiencing pregnancy-related emergencies, such as miscarriages (86%), protecting a patient’s right to travel in order to get an abortion (79%), and protecting doctors who perform abortions from receiving fines or facing prison time (67%). Two-thirds of the public also support a law guaranteeing a federal right to abortion. Less than half (42%) of the public support a law establishing a 16-week ban on abortion.
In addition, most of the public opposes many of the policies anti-abortion groups are advocating for aimed at restricting or banning medication abortion such as making it a crime for health care provider to mail medication abortion to patients living in states where abortions are banned (62%) or banning the use of medication abortion nationwide (66%). Most of the public (61%) also opposes policies that prohibit clinics that receive federal funds from providing abortions or referring patients to abortion providers.
The group that stands to be impacted most by these proposals, women of reproductive age (18-49), also support protecting access to abortion including opposing laws restricting access to medication abortion. Three-fourths (76%) of women between the ages of 18 and 49 support laws guaranteeing a federal right to abortion while four in ten (38%) support a 16-week abortion ban.
There is consensus support across partisans for some reproductive health proposals such as protecting access to abortions for patients who are experiencing miscarriages, protecting a patient’s right to travel in order to get an abortion, and protecting doctors who perform abortions from receiving fines or facing prison time. But support for other proposals, including both a federal right to abortion and a 16-week abortion ban, vary widely depending on partisanship.
While majorities of Democrats (86%) and independents (67%) adults support a law guaranteeing a federal right to abortion, this is opposed by nearly six in ten Republicans (57%). In addition, while a majority of Republicans (63%) support a federal 16-week abortion ban, a policy that former President Trump has quietly supported in recent weeks, a majority of Democrats (75%) and independents (59%) oppose this proposal.
The large partisan disagreement on proposals aimed at legislating abortion access may be driven by how differently Democrats and Republicans view the issue. Democrats overwhelmingly view the issue of abortion as an issue of individual rights and freedom (96%) as well as a health care issue (82%). Republicans, on the other hand, are more likely to view it as a moral issue (81%) and more than half (55%) of Republicans also say it is a religious issue.
Knowledge, Use, and Legality of Mifepristone
Since the overturning of Roe, medication abortion has been the focus of policy debates at the state and federal level, yet there is extensive uncertainty on whether medication abortion is legal or illegal, given that its legality depends on state laws.
Overall, more than one in three (36%) adults say they understand the abortion laws in their state less than “somewhat well,” including one-third (32%) of women of reproductive age (ages 18 to 49). And while a slim majority (54%) of the public has heard of mifepristone, the medication abortion pill, the legality and use of the medication continues to be misunderstood across the public.
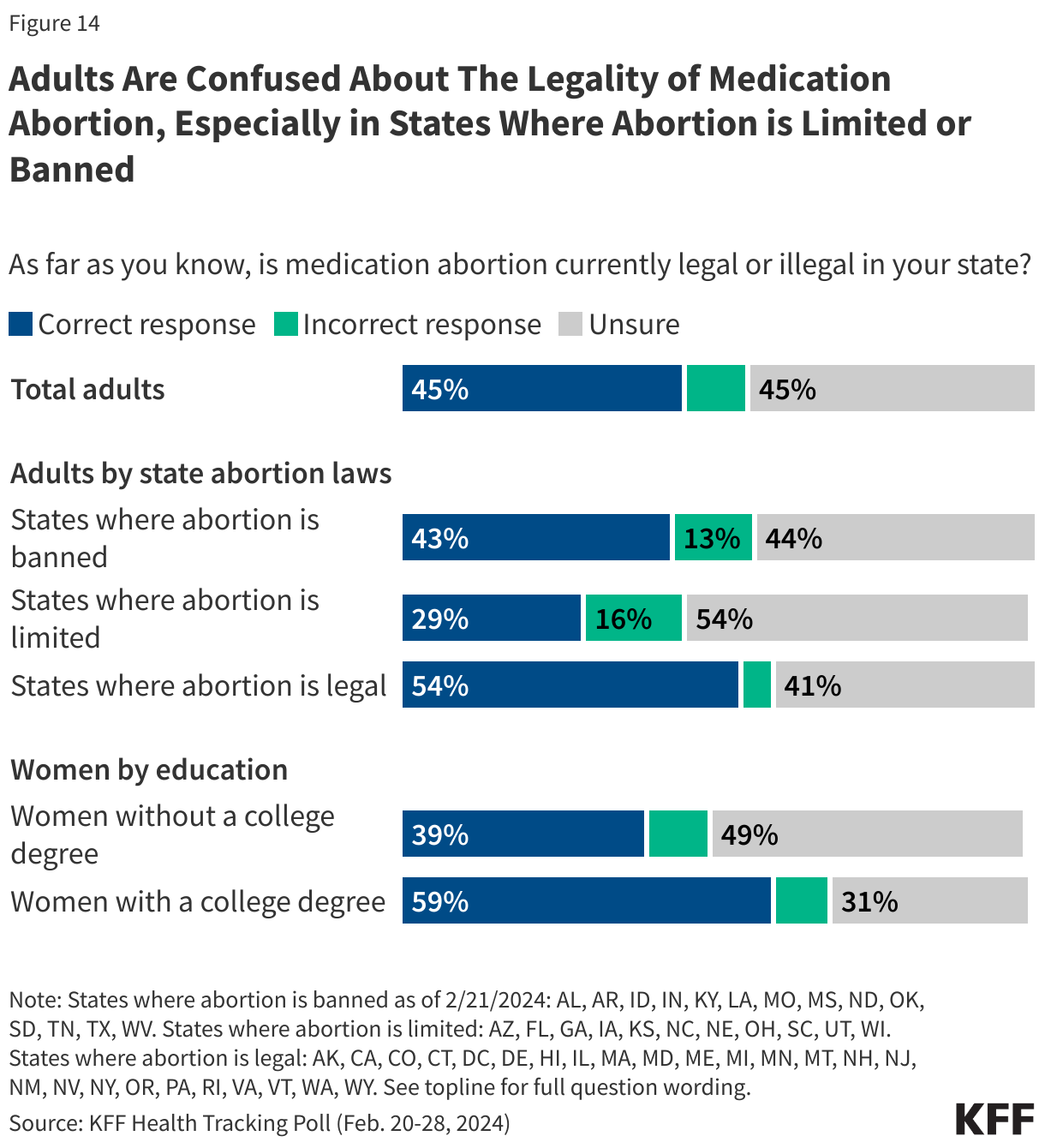
About four in ten women (43%) are “unsure” whether medication abortion is legal in the state they live in, including 38% of women ages 18-49. Nationally, at least four in ten U.S. adults say they are not sure whether the medication is legal where they live regardless of whether they live in a state where abortion is limited (54% say they are unsure), banned (44%), or available (41%). In addition, about one in eight adults (13%), including a similar share (11%) of women, living in states where abortion is currently banned, incorrectly believe medication abortion is legal in their state.
Women without a college degree are more likely to say they are “unsure” about the legality of medication abortion in their state, with half (50%) of women without a college degree saying they are unsure, compared to about one in three (32%) of women with a college degree.
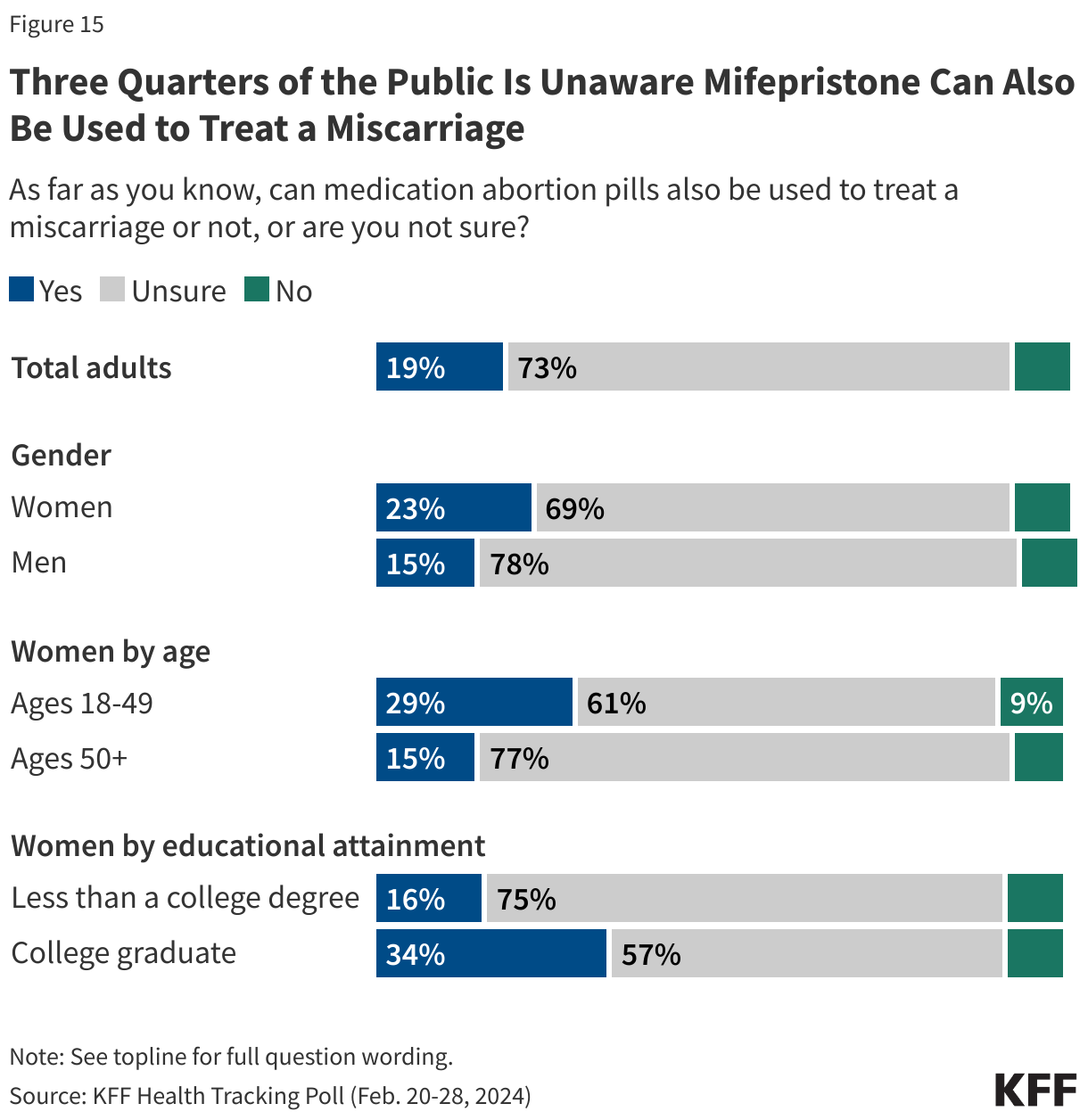
In addition to confusion around state abortion laws and whether mifepristone is legal or not, there is also a general lack of understanding of what the pill is used for. About one in five (19%) adults correctly say that mifepristone can be used to treat a miscarriage, while about one in ten (8%) incorrectly say it cannot be used for this purpose and about three in four (73%) are “unsure” whether mifepristone can also be used to treat a miscarriage or not. Across gender, age, and education, at least six in ten adults say they are “unsure” about whether mifepristone can also be used to treat a miscarriage. However, women with a college degree (34%) and women of reproductive age (29%) are the groups most likely to be aware that mifepristone can also be used to treat a miscarriage.
Most of the public is unaware that few abortions occur after 20 weeks of pregnancy
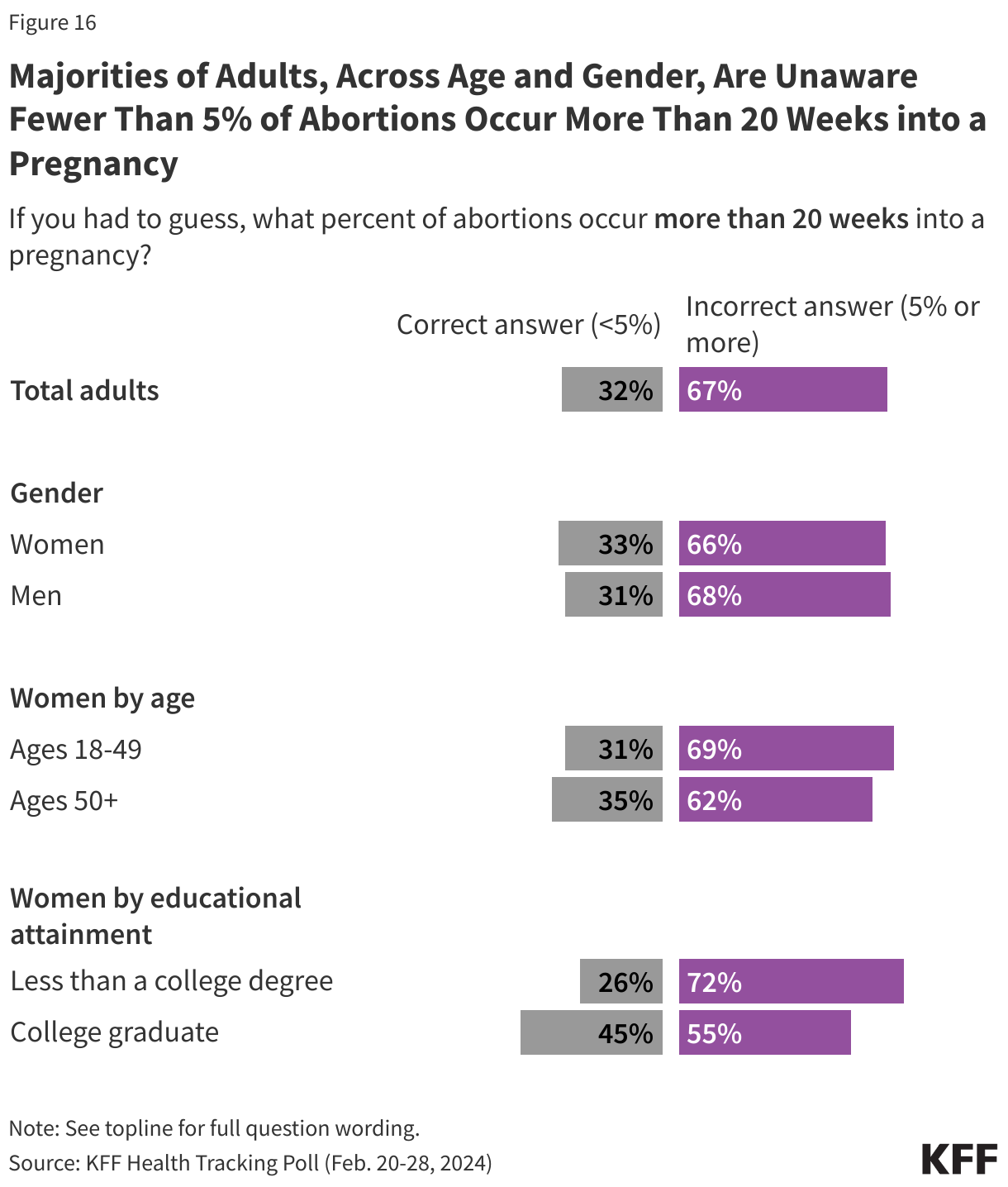
There is also widespread misunderstanding about when most abortions occur. Public debate continues to circulate around so-called “late-term” abortions, which typically refer to abortions obtained at or after 21 weeks. The latest KFF Health Tracking Poll finds that two-thirds (67%) of adults are unaware that less than 5% of abortions occur more than 20 weeks into a pregnancy, while one-third of adults (32%) correctly say that five percent or fewer abortions occur before this point. Indeed, abortions at or after 21 weeks are uncommon and represent 1% of all abortions in the U.S. And, despite claims of abortions occurring “moments before birth” or “after birth,” scenarios like these do not occur nor are they legal in the United States.
Similar majorities of adults across age and gender are unaware of this statistic. However, women who are college graduates are more likely to correctly say less than five percent of abortions occur after 20 weeks than are women with lower levels of education (45% vs. 26%).
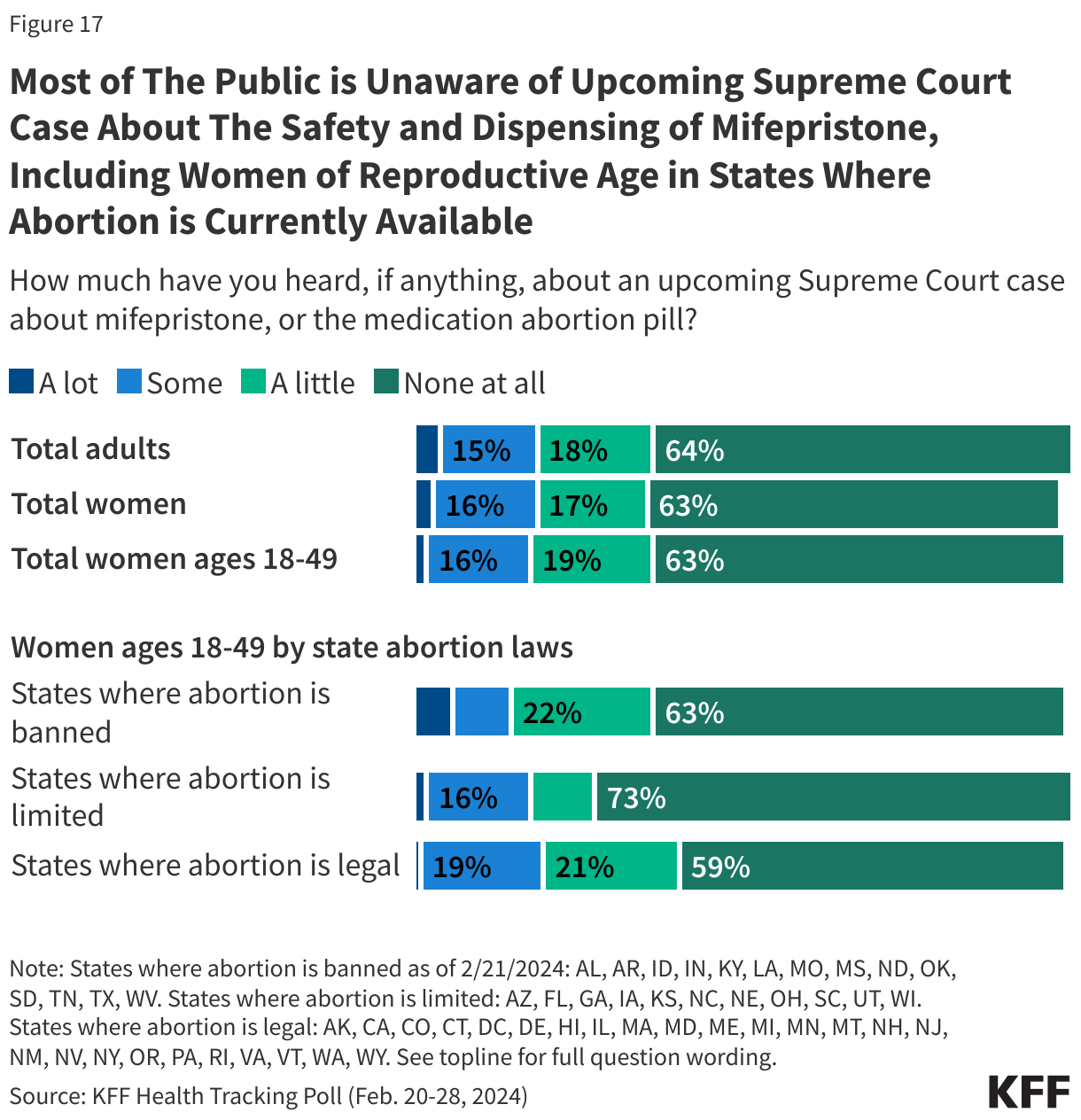
Two-thirds of the public has not heard about the upcoming Supreme Court case challenging mifepristone use
Currently, FDA policy allows mifepristone pills to be prescribed via telehealth, mailed to patients, and dispensed at in-person pharmacies. However, this policy update is currently being legally challenged by anti-abortion groups. On March 26, 2024 the Supreme Court is set to hear oral arguments challenging the safety and the conditions in which the Mifepristone can be dispensed which may impact if and how patients can access the drug, including in states where abortion is currently available. About two-thirds (64%) of adults have not heard anything in the news regarding this court case, while 18% have heard “just a little,” 15% have heard “some” and few (4%) have heard “a lot.” About six in ten (59%) women under the age of 50 living in states where abortion is currently available, a group that could also be affected if the court rules to restore limits on dispensing mifepristone, are unaware of the case.