President Trump has made a slew of immigration policy changes focused on restricting entry at the border and increasing interior enforcement efforts to support mass deportation. These include rescinding protections against enforcement action in previously protected areas such as health care facilities and schools. While many of these actions focus on the estimated 11 million undocumented immigrants in the U.S., they will have ripple effects among the much larger number of people in immigrant families, including millions of U.S.-born citizen children. During the first Trump administration, restrictive immigration policies and increased enforcement activity led to increased fears among immigrant families across immigration statuses that had negative effects on health and well-being, employment, and daily life. They also could lead to family separations as well as mass detentions, which can have negative mental and physical health impacts on immigrants across statuses and their children. Mass deportations also could negatively impact the U.S. economy and workforce, given the role immigrants play, particularly in certain industries, including health care.
The extent to which President Trump will be able to carry out his plans without additional legislative action and in the face of potential court challenges remains uncertain. However, these plans are already affecting immigrants’ daily lives and increasing fears, with Immigrations and Customs Enforcement (ICE) agents carrying out raids across communities, and reports of nearly 1,000 people arrested in one recent day. This brief discusses the potential implications of increased enforcement actions under the Trump administration for the health and well-being of families and potential broader impacts for communities, the workforce, and the economy, including health care.
What actions is President Trump taking to increase interior enforcement and who may be affected?
Upon taking office, President Trump issued a series of executive orders focused on restricting immigration and increasing interior enforcement activity. These include orders limiting birthright citizenship, declaring a national emergency at the Southern border and restricting access at the border, expanding enforcement policies, suspending the refugee admissions program, and rescinding numerous Biden-era policies, including a policy that protected against enforcement in “sensitive areas,” including schools and health care facilities. Many of the changes outlined in the orders may require legislative or regulatory action to implement, and many are likely to be challenged in court. For example, a federal judge has already blocked the order to end birthright citizenship through a temporary restraining order. However, these changes are already increasing fears and uncertainty among families and communities. Other changes may put other groups with lawful status at risk of losing protections, including Deferred Action for Childhood Arrivals (DACA) recipients and people with Temporary Protected Status (TPS) designations from some countries. The administration recently revoked TPS for Venezuelans living in the U.S., which will make them at risk for deportation in coming months and eliminate their work authorizations.
While enforcement actions are focused on undocumented immigrants, they will have ripple effects across millions more people living in immigrant families, including U.S.-born citizen children. As of 2023, there were 47.1 million immigrants residing in the U.S., including 22.4 million noncitizen immigrants, of whom an estimated 11 million are undocumented. Additional immigrants that currently have lawful statuses may be at risk for enforcement actions under new policies if they lose protections, including nearly 1.2 million immigrants who either have or are eligible for TPS, the over 530,000 active DACA recipients, and individuals in the U.S. with pending asylum cases. Millions of additional individuals living in immigrant families also are likely to be impacted. Many undocumented immigrants live in families with mixed immigration statuses that may include people with lawful status and U.S. citizens. As of 2023, 19 million, or one in four, children in the U.S. had an immigrant parent, including one in ten (12%) who are citizen children with a noncitizen parent. An estimated 4.4 million U.S.-born children live with an undocumented immigrant parent.
What are the likely impacts of enhanced enforcement activity on the health and well-being of immigrant families?
Prior KFF focus groups with immigrant families during the first Trump administration found that restrictive immigration policies, including increases in detention and deportation, led to increased fears among immigrant families across immigration statuses that had negative effects on health and well-being. Immigrant families, including those with lawful status, reported experiencing resounding levels of fear and uncertainty. Some also reported changes in daily life such as increased difficulty finding employment, leading to increased financial strains on families. Some parents, particularly those who are undocumented or who have an undocumented family member, said they would only leave the house when necessary, such as for work; limit driving; or no longer participate in recreational activities, leading to children spending many hours inside. Parents and pediatricians reported a broad array of impacts of increased fears among children, including behavioral changes, such as problems sleeping and eating; psychosomatic symptoms, such as headaches and stomachaches; and mental health issues, such as depression and anxiety. Parents and pediatricians also felt that fears negatively affected children’s behavior and performance in school. Pediatricians expressed significant concerns about the long-term health consequences of these fears for children, including the damaging effects of toxic stress on physical and mental health over the lifespan, negative effects on children’s growth and development, and compounding social and environmental challenges that negatively impact health.
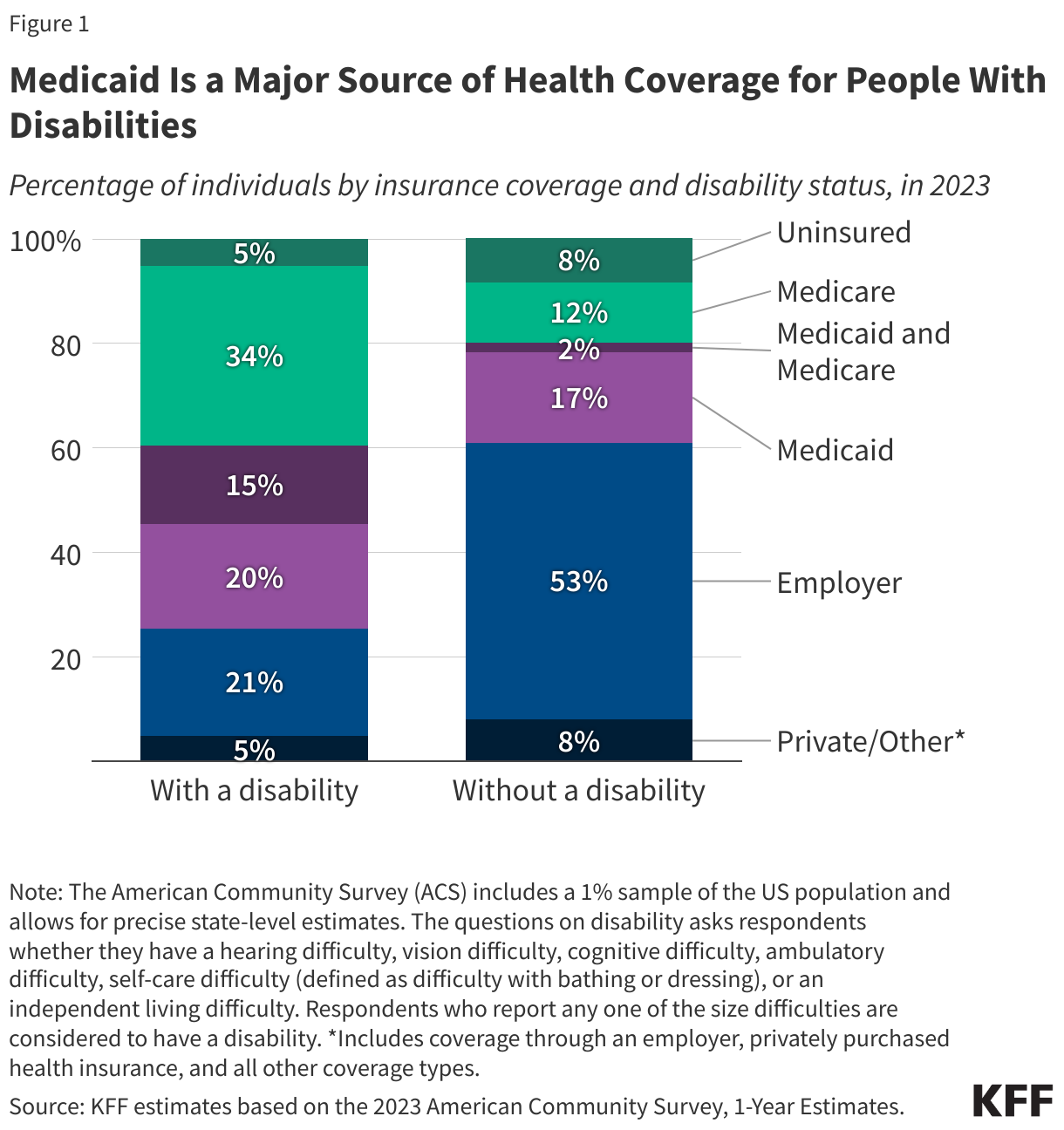
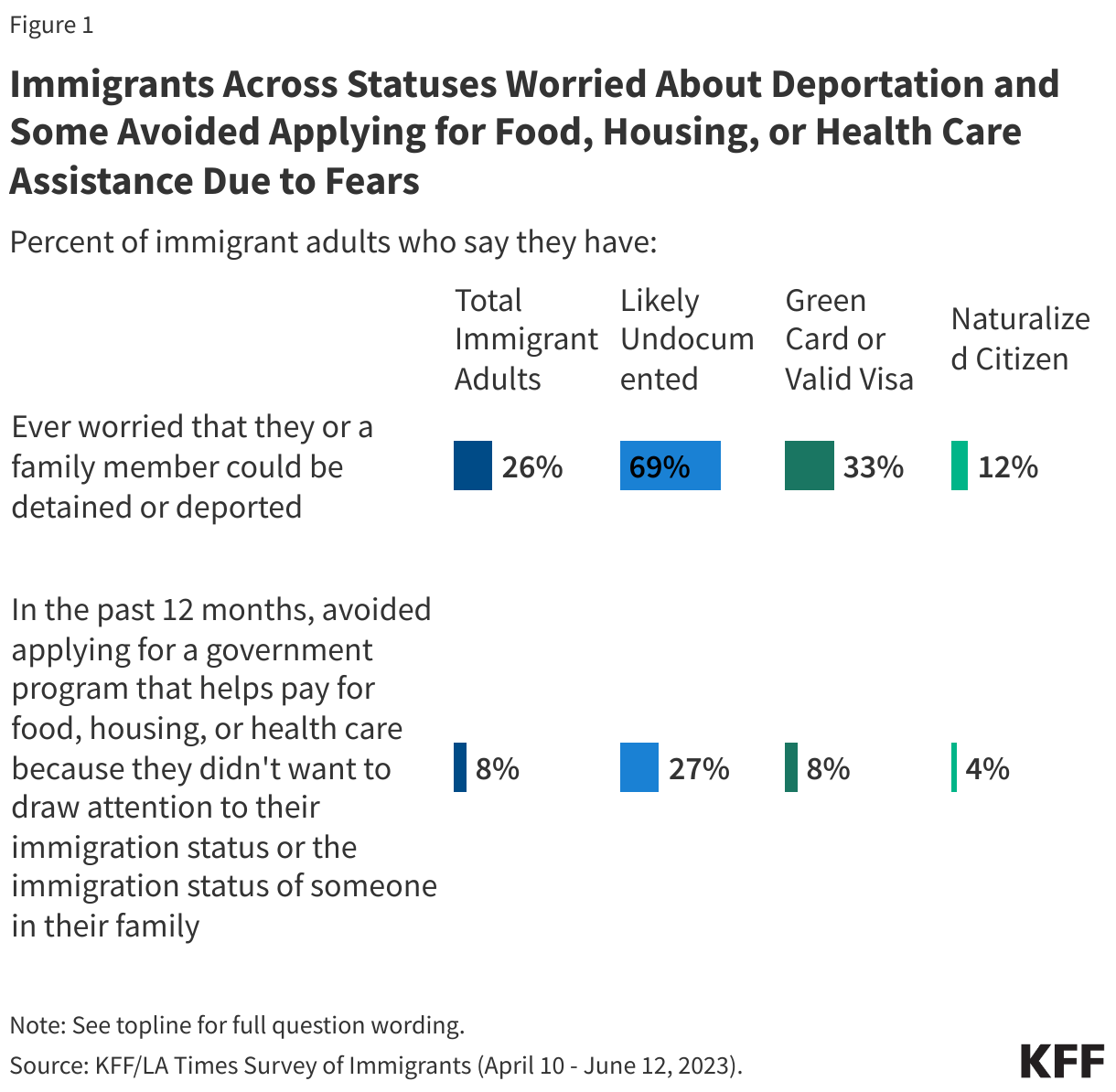
Increased fears under the first Trump Administration also led to growing reluctance among some families, including lawfully present immigrants and citizen children, about participating in programs and seeking services for which they are eligible, including health coverage and care. In KFF focus groups with immigrant families during the first Trump administration, parents noted that they highly prioritize their children’s health and generally viewed hospitals and doctors’ offices as safe spaces. However, there were some reports of changes in health care use, including decreased use of some care, and decreased participation in Medicaid and CHIP and other programs due to increased immigration-related fears. Despite efforts by the Biden administration to reduce these fears, data from the KFF/LA Times Survey of Immigrants showed that, as of 2023, nearly seven in ten (69%) likely undocumented immigrants, a third (33%) of lawfully present immigrants, and over one in ten (12%) naturalized citizen immigrants said they ever worried that they or a family member could be detained or deported. Moreover, about a quarter (27%) of likely undocumented immigrants and nearly one in ten (8%) lawfully present immigrants say they avoided applying for food, housing, or health care assistance in the past year due to immigration-related fears (Figure 1). Fears about accessing health care services may be enhanced under the second Trump administration, given the recission of a policy dating back to 2011, that protected against enforcement activity in sensitive areas, including health care facilities. Health care providers will face new challenges helping families feel safe accessing health care, protecting patient information, and establishing protocols to respond to potential encounters with ICE agents. Additionally, Florida and Texas have implemented policies that require hospitals to request immigration status from patients, which may further enhance fears about accessing care.
KFF interviews with individuals who had a family member detained or deported during the first Trump administration reported broad negative impacts on health and well-being. Respondents reported that detention and deportation of family members often occurred suddenly and unexpectedly, leaving families in shock and unprepared. One of the most immediate and significant effects on families was the loss of income, which left them struggling to pay their bills, including rent, food, and utilities. They further reported disruptions to children’s daily lives, and, in some cases, older children assuming new responsibilities and changing plans, such as no longer attending college, to support the family. Families also reported direct health impacts, including symptoms of depression and worsening chronic conditions. Some families reported losing health coverage and increased barriers to accessing coverage or care due to fears and increased financial challenges.
Other research shows that immigration enforcement raids and family separations can lead to worsened physical and mental health of both parents and children of deported parents. Exposing children to traumatic events and prolonged or toxic stress such as raids and separation from a parent disrupts a child’s healthy development and can result in short- and long-term negative effects on physical, mental, and behavioral health. Research has found that living near areas subject to immigration enforcement raids increased the risk of negative mental health among children of immigrants and worse birth outcomes among both Hispanic immigrant mothers as well as U.S.-born Hispanic mothers as compared to non-Hispanic White mothers. Education outcomes also worsened among Hispanic children in areas impacted by raids compared to White children. One potential consequence of raids and detentions and deportations is the separation of parents from their children. Studies have found that children and caregivers impacted by family separations experience worse mental health, including anxiety, depression, and posttraumatic stress disorder. Family separations can also lead to financial challenges for mixed-status households due to loss of income.
Prior experience suggests that immigrants held in detention facilities may not receive sufficient health care and face unsafe conditions. As the Trump administration escalates enforcement actions, the number of people held in detention facilities will grow likely beyond current capacity. Research showed that detainees, including children, experience poor conditions and inadequate care in detention facilities. An analysis found that most of the deaths of immigrants in detention occurred among “relatively young and healthy men” and were associated with ICE violating their own medical standards. Detention and solitary confinement can also worsen the mental health of immigrants. Studies show high levels of psychiatric distress, including depression and post-traumatic stress, among detained immigrants and their children, even after short detention periods. Research on immigrant detention centers have also found gaps in care for pregnant Hispanic migrants and that LGBT detainees experience higher rates of harassment than non-LGBT detainees.
What are the potential impacts of enhanced enforcement activity on the nation’s economy and workforce?
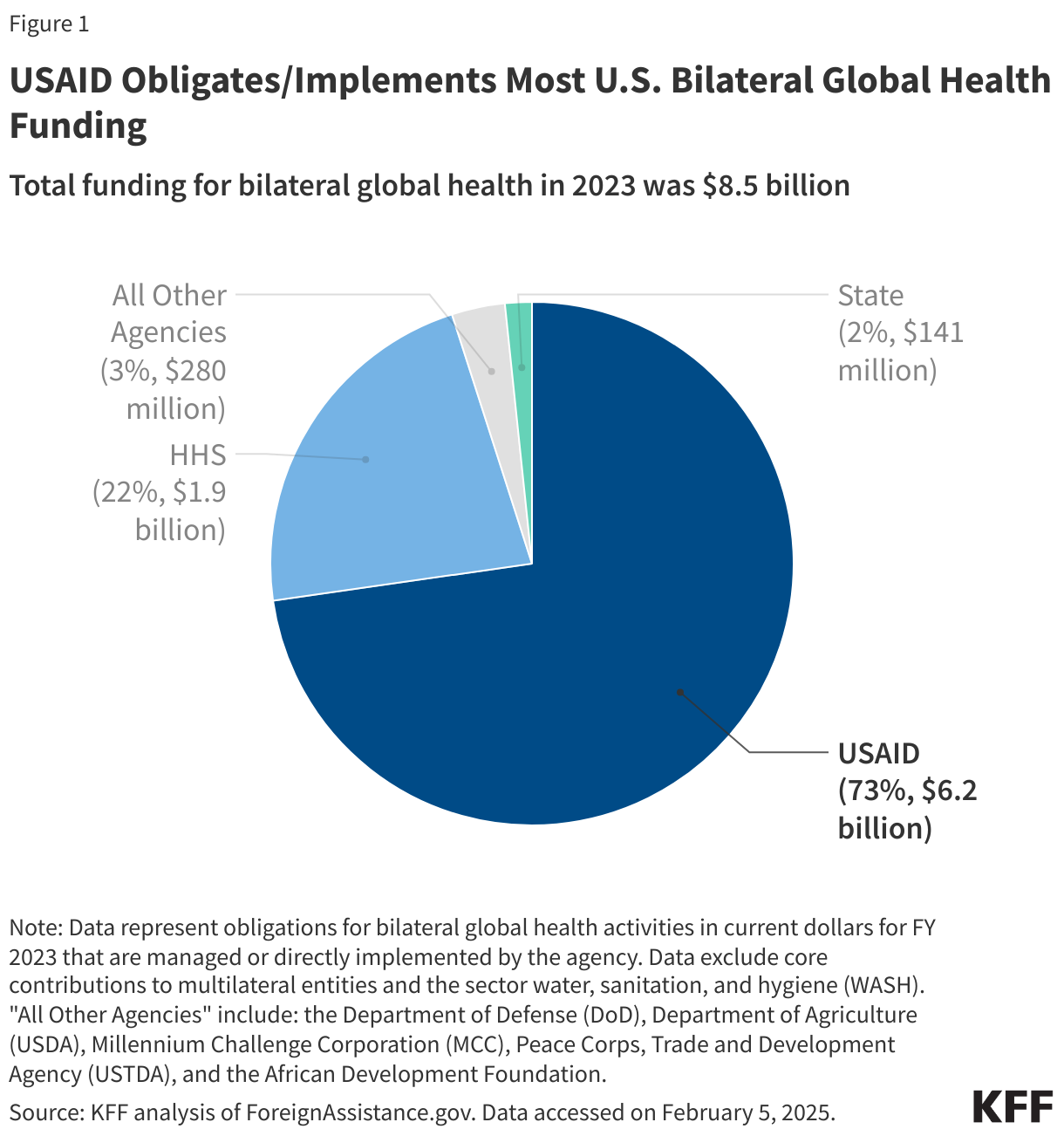
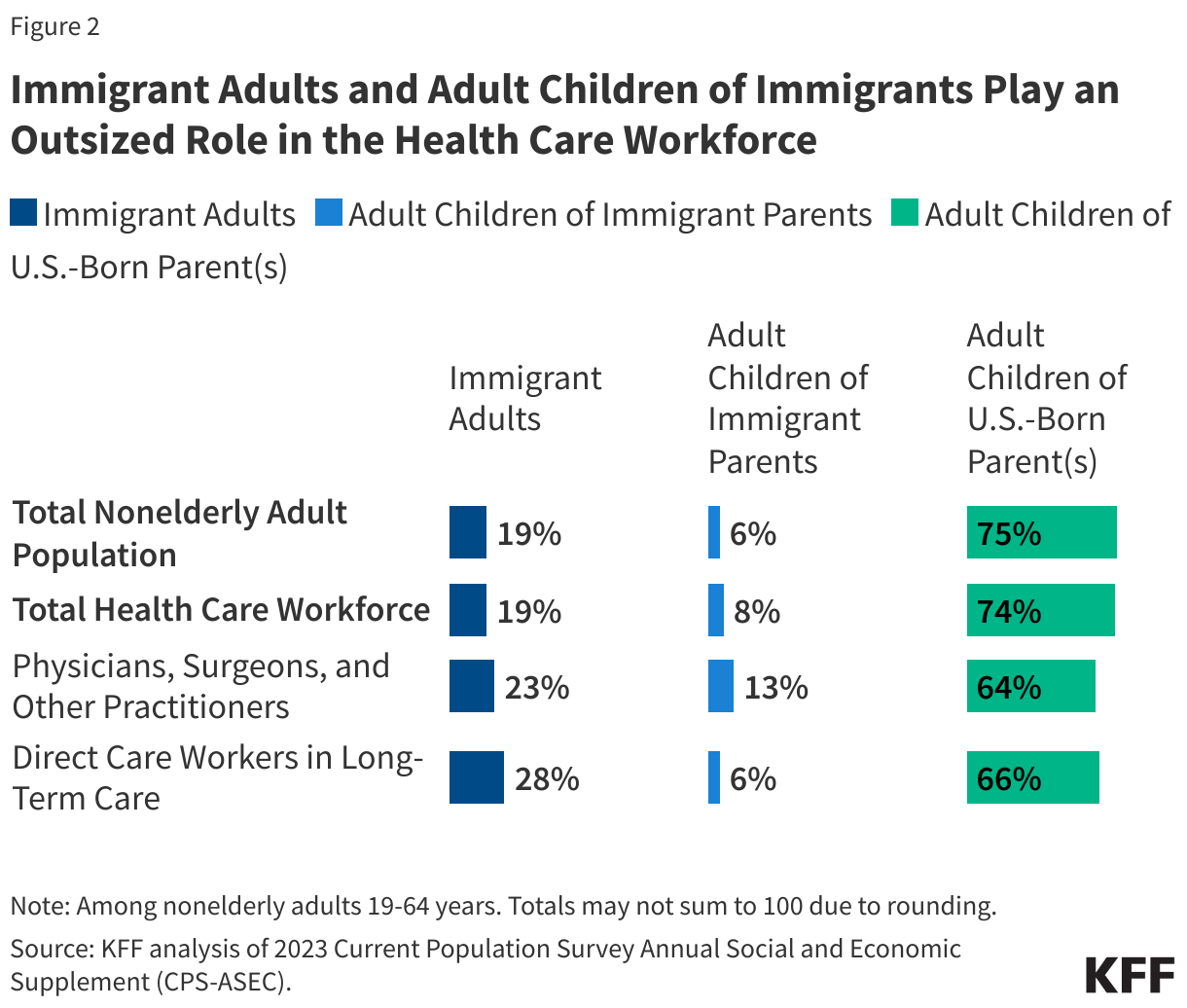
Mass deportations could also negatively impact the U.S. workforce, given the role immigrants play, particularly in certain industries, including health care. Most immigrants say they came to the U.S. for better work and educational opportunities. Immigrants and their U.S.-born children fill unmet labor market needs and have been the primary drivers of workforce growth, accounting for 83% of the growth in the U.S. labor force between 2010 and 2018. Research shows that immigration does not displace nor lead to more unemployment among U.S. born workers as they often do not compete for the same jobs. Immigrants and their adult children play outsized roles in certain occupations, including agriculture, construction, and health care (Figure 1). As the U.S. 65 and older population grows, deportation of immigrants may exacerbate the health care workforce shortage. Immigrants and their adult children make up a larger share of physicians, surgeons, and other health care practitioners than they do of the population and play a particularly large role as direct care workers in home and community-based settings.
Mass deportations may also reduce the billions of dollars immigrants, including undocumented immigrants, pay in federal, state, and local taxes, which help subsidize health care for U.S.-born citizens. It is estimated that more than a third of their tax dollars are payroll taxes that fund programs they cannot access, including Social Security, Medicare, and the federal share of unemployment insurance. Children of immigrants also contribute more in taxes on average than their parents or the rest of the U.S.-born population. The Congressional Budget Office (CBO) estimates that the recent immigration surge will reduce the federal deficit over the next decade. Research further finds that immigrants pay more into the health care system through taxes and health insurance premiums than they utilize, helping to subsidize health care for U.S.-born citizens. Earlier research found that without the contributions undocumented immigrants make to the Medicare Trust Fund, it would reach insolvency earlier, and that undocumented immigrants result in a net positive effect on the financial status of Social Security.
Expanding capacity to carry out mass deportations would likely be a significant cost to taxpayers and may require additional allocations by Congress. New estimates suggest that Trump’s plan to deport millions of undocumented immigrants could cost hundreds of billions of dollars. Trump’s selected border czar reported an estimated cost of $86 billion. Increases in enforcement activity would likely strain limited resources at ICE and the current system of detention centers, which is already at capacity. Expanding detention capacity to support large-scale deportations would require large investments in infrastructure, including setting up new detention facilities, expanding immigration court capacity, increasing the use of private contractors, and paying for more flights used for deportations.