Medicare Advantage Insurers Made Nearly 53 Million Prior Authorization Determinations in 2024
Introduction
Virtually all enrollees in Medicare Advantage (99%) are required to obtain prior authorization for some services – most commonly, higher cost services, such as inpatient hospital stays, skilled nursing facility stays, and chemotherapy. This contrasts with traditional Medicare, where only a limited set of services, including certain outpatient hospital services, non-emergency ambulance transport, and durable medical equipment, require prior authorization (see Box 1). Insurers often use prior authorization requirements to assess whether health care services are medically necessary before they are covered and to reduce unnecessary costs. At the same time, prior authorization processes and requirements, including the use of artificial intelligence to review requests, may result in administrative hassles for providers, delays for patients in receiving necessary care, and in some instances, denials of medically necessary services, such as post-acute care.
Prior authorization practices have gotten a fair amount of attention in recent years. KFF polling shows that most people view delays and denials of care by health insurance companies as a problem, with about two-thirds of Medicare beneficiaries reporting that they consider it to be a major problem. Last summer, the Trump Administration announced that private health insurers, including those that comprise a majority of Medicare Advantage enrollment, agreed to a voluntary initiative to improve the prior authorization process. Lawmakers in Congress have also been active on the issue, with bipartisan legislation introduced in both the House and Senate. Additionally, on January 1, 2026, the Administration launched the Wasteful and Inappropriate Spending Reduction (WISeR) model to test the use of enhanced technology to conduct prior authorization for an additional set of select services in traditional Medicare in six states.
This analysis uses data submitted by Medicare Advantage insurers to the Centers for Medicare and Medicaid Services (CMS) to examine the trends in the number of prior authorization requests, denials, and appeals for 2019 through 2024, as well as differences across Medicare Advantage insurers with the largest enrollment. It does not include requests or denials by type of service or type of plan because CMS does not collect or report this information, though such data could help inform consumers in choosing among plans. It also presents data from CMS about the use of prior authorization in traditional Medicare, including the number of requests and denials for fiscal years 2021 through 2024.
Key Takeaways
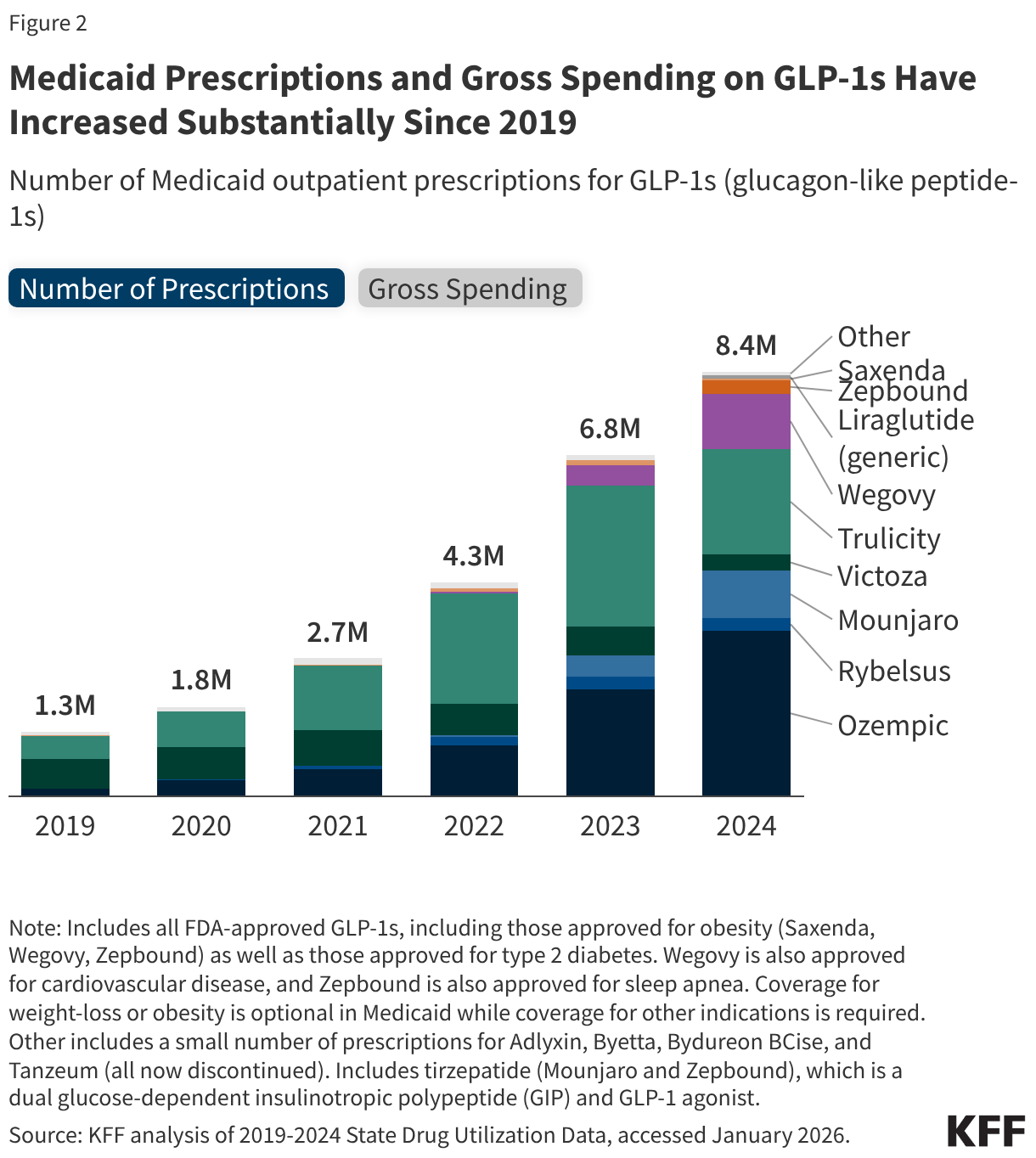
- Nearly 53 million prior authorization requests were submitted to Medicare Advantage insurers on behalf of Medicare Advantage enrollees in 2024, an increase from 2023 (49.8 million) as the number of people enrolled in Medicare Advantage has grown. Substantially fewer prior authorization requests for traditional Medicare than Medicare Advantage beneficiaries were submitted to CMS – just over 625,000 in fiscal year 2024.
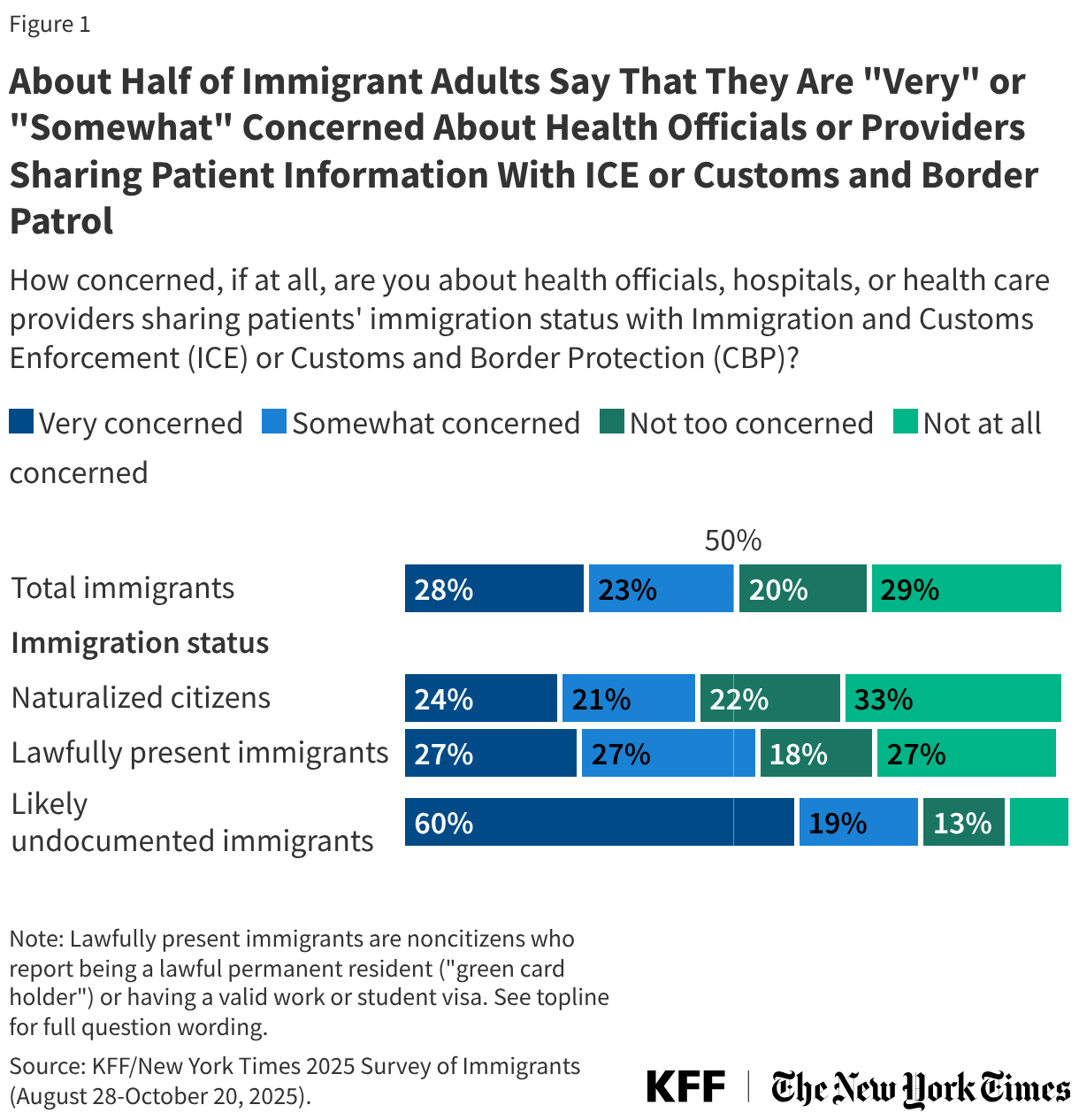
- In 2024, there were 1.7 prior authorization requests on average per Medicare Advantage enrollee, a slight decline from 1.8 in 2023. In contrast, in 2024, about 2 prior authorization requests were submitted per 100 traditional Medicare beneficiaries – a rate of about 0.02 per enrollee – which reflects the limited set of services subject to prior authorization in traditional Medicare.
- In 2024, Medicare Advantage insurers fully or partially denied 4.1 million prior authorization requests, which is a somewhat larger share (7.7%) of all requests than in 2023 (6.4%) and similar to 2022 (7.4%). Though there were substantially fewer prior authorization requests for traditional Medicare beneficiaries, a larger share was denied – 22.9% (less than 150,000) in 2024.
- A small share of denied prior authorization requests was appealed in Medicare Advantage –11.5% in 2024, similar to 2023 (11.7%).That represents an increase since 2019, when 7.5% of denied prior authorization requests in Medicare Advantage were appealed. The traditional Medicare data do not include information on appeals for 2023 and 2024, but in 2022 a relatively small share of denied prior authorization requests was appealed in traditional Medicare (6.4% in 2022).
- Though a small share of prior authorization denials were appealed to Medicare Advantage insurers, most appeals (80.7%) were partially or fully overturned in 2024. Across all years examined, more than eight in ten appeals overturned the initial denial. These requests represent medical care that was ordered by a health care provider and ultimately deemed necessary but was potentially delayed because of the additional step of appealing the initial prior authorization decision. Such delays may have negative effects on a patient’s health.
Use of Prior Authorization in Medicare Advantage
CMS requires Medicare Advantage insurers to submit data for each Medicare Advantage contract (which usually includes multiple plans) as part of its oversight of Medicare Advantage plans. Insurers are required to submit the number of prior authorization determinations made during a year and whether the request was approved. Insurers are additionally required to report the number of initial decisions that were appealed (reconsiderations) and the outcome of that process, including whether the initial decision was affirmed, partially overturned, or fully overturned. These data are useful for assessing overall trends and variations across insurers, but do not contain the information necessary to understand how the use of prior authorization varies by type of service or type of plan because they are aggregated to the contract level. CMS is implementing a pilot program to collect more detailed data at the plan and service level this year, which would help assess whether some enrollees bear a higher burden of prior authorization requirements or are more frequently denied requested services. CMS states that it anticipates expanding the requirement to all plans in 2027.
In 2024, nearly 53 million prior authorization requests were submitted to Medicare Advantage insurers.
After dropping in 2020 amid the initial phase of the COVID-19 pandemic, prior authorization requests increased steadily between 2021 and 2024 (Figure 1). The decline in 2020 was likely due to both a decline in utilization, as well as the option for insurers to temporarily pause prior authorization requirements during the public health emergency.
The increase in the total number of prior authorization requests since 2020 corresponds to an increase in Medicare Advantage enrollment. Between 2019 and 2024, the number of Medicare Advantage enrollees rose from 22 million people to 33 million people. Therefore, the number of prior authorization requests per enrollee has remained relatively constant in the past few years. In 2019, there were approximately 1.7 prior authorization requests per Medicare Advantage enrollee. That number dropped at the onset of the COVID-19 pandemic to 1.4 in 2020 and 1.5 in 2021, before returning to the pre-pandemic level of 1.7 requests per enrollee in 2022 and rising slightly to 1.8 in 2023. In 2024, Medicare Advantage enrollment growth outpaced the increase in the number of prior authorization requests, leading to a slight drop in the number of requests per enrollee to 1.7 (Figure 2).
The modest decline in the number of prior authorization determinations per enrollee corresponds with increased regulatory attention to prior authorization in Medicare Advantage which clarified the criteria that may be used by Medicare Advantage plans to establish prior authorization policies. In addition, certain Medicare Advantage insurers also announced changes to prior authorization practices in 2023 and 2024, such as UnitedHealth Group’s decision to reduce the number of services subject to prior authorization and launch a national “gold card” program that exempts certain providers from prior authorization requirements.
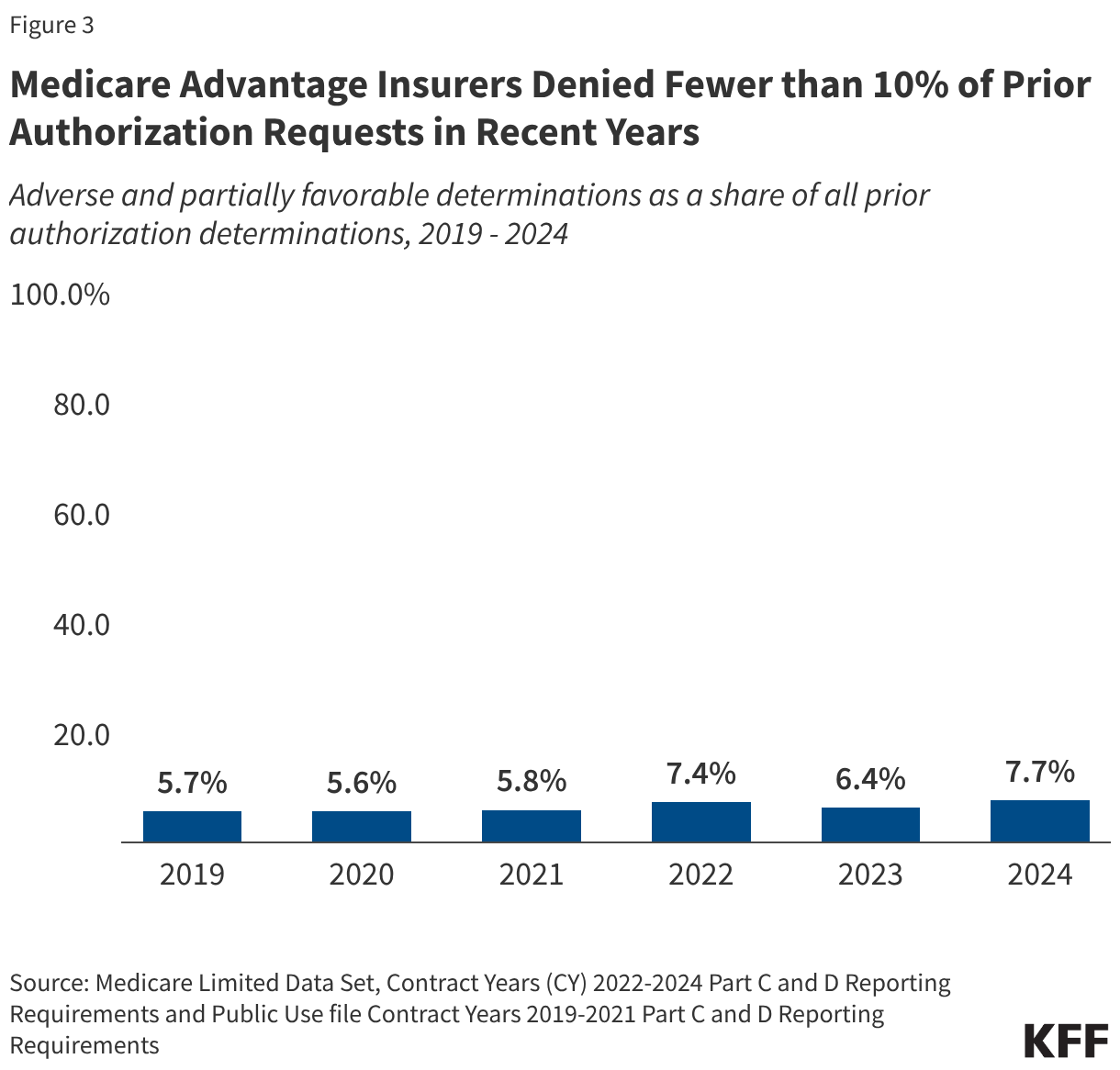
Medicare Advantage insurers denied 4.1 million (7.7%) prior authorization requests in 2024.
Of the 52.8 million prior authorization determinations in 2024, more than 90% (48.7 million) were fully favorable, meaning the requested item or service was approved in full. However, the remaining 4.1 million prior authorization requests (7.7%) were denied in full or in part by Medicare Advantage insurers. This is slightly higher than the 6.4% of requests that were denied in 2023 and similar to the share denied in 2022 (Figure 3). Across all years, most denials (73% in 2024, data not shown) were denied in full, while a minority of denials were determined to be partially favorable, meaning that only part of the request was approved. For example, the insurer may have approved 10 of 14 requested therapy sessions.
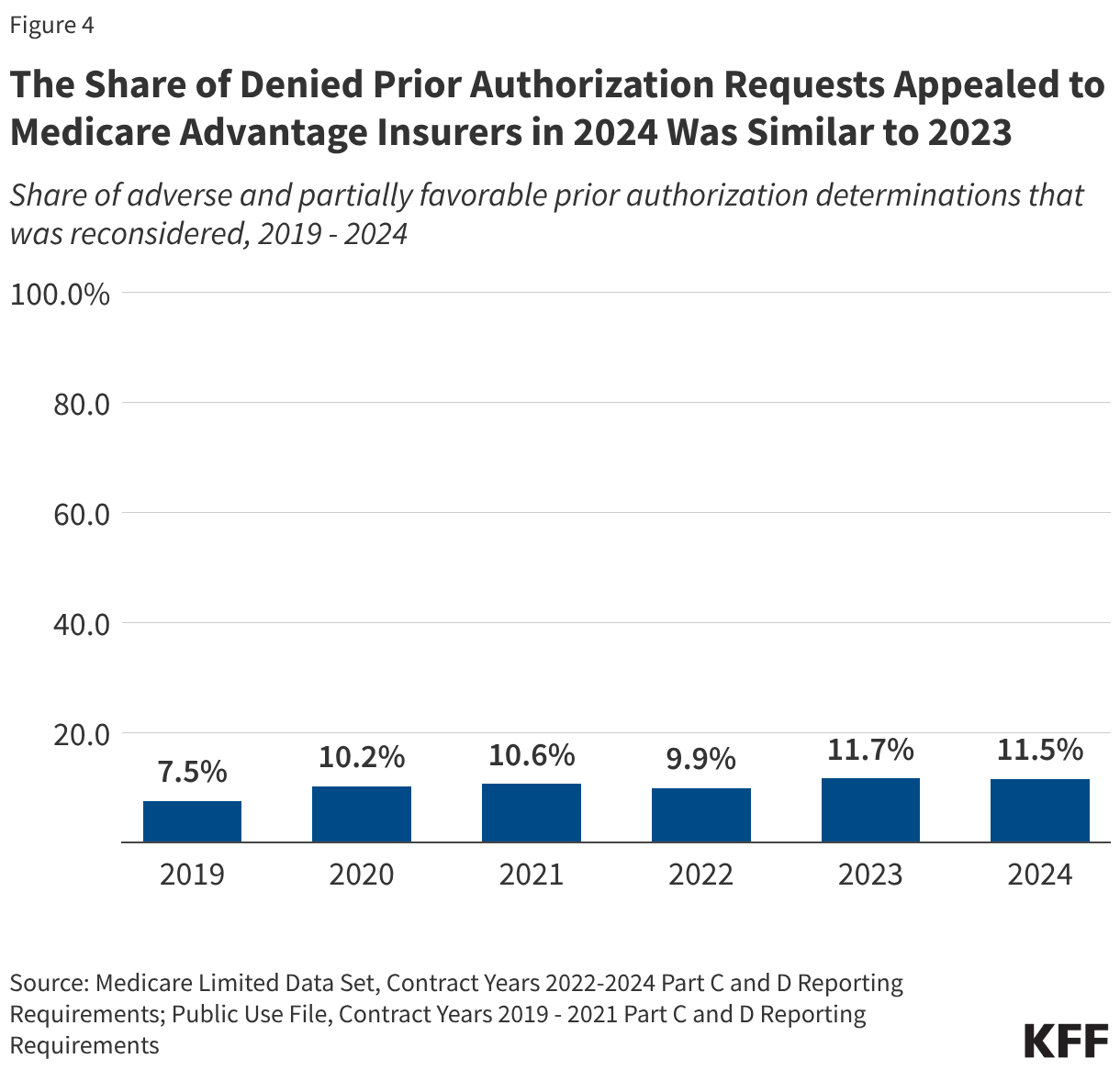
Just 11.5% of denied prior authorization requests were appealed to Medicare Advantage insurers in 2024.
As in previous years, the majority of the 4.1 million denied prior authorization requests were not appealed. Though the share of denied requests that are appealed is small at just 11.5%, similar to the share in 2023 (11.7%), it has risen over time, from 7.5% in 2019 (Figure 4). These include appeals of claims that were both fully and partially denied.
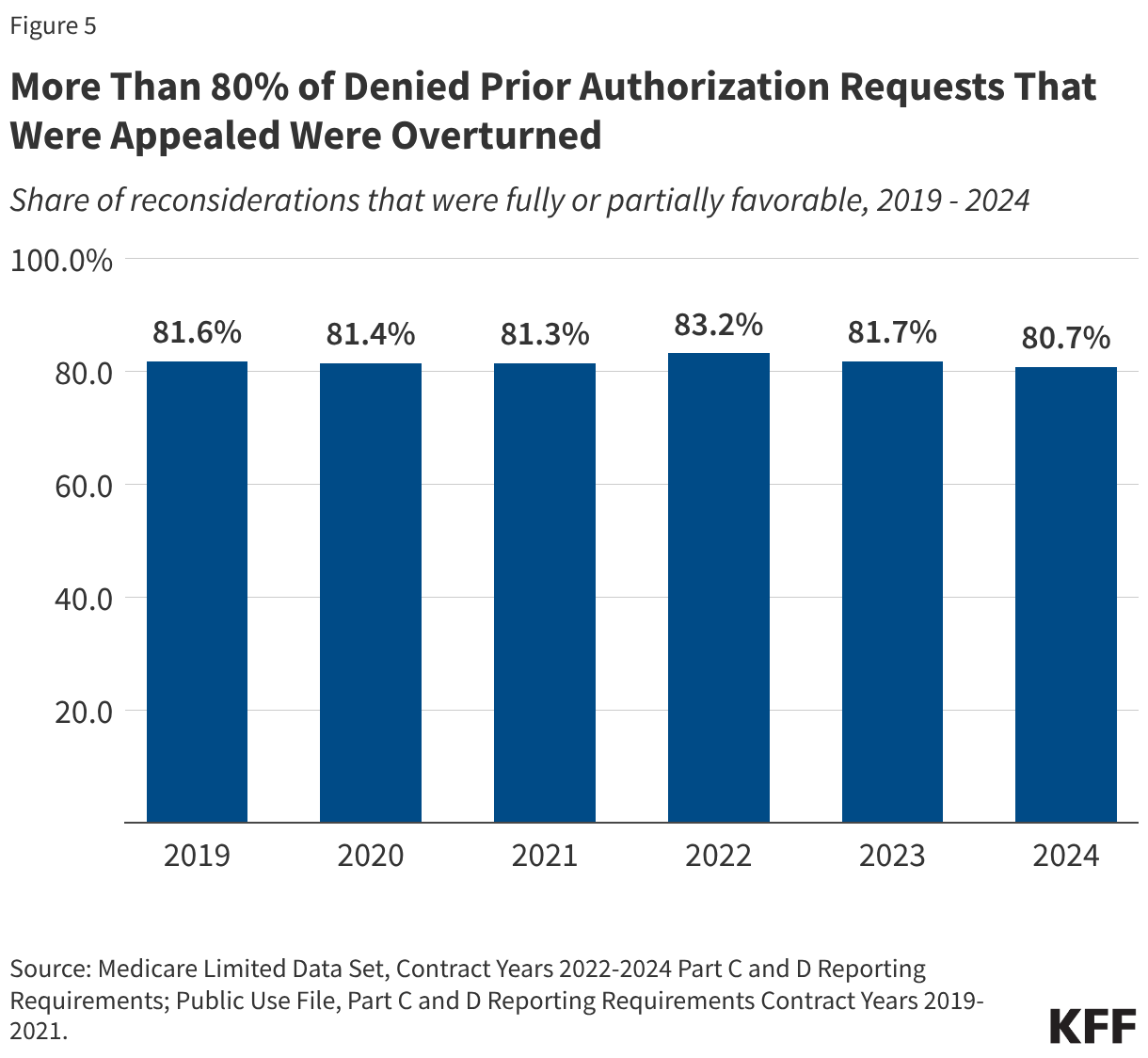
The vast majority of denied prior authorization requests that were appealed were subsequently overturned by Medicare Advantage insurers.
In each year from 2019 through 2024, more than eight in ten denied prior authorization requests that were appealed were overturned (Figure 5). This raises questions about whether the initial request should have been approved, although it could also indicate that the initial request was missing the required documentation to justify the service. In either case, patients potentially faced delays in obtaining services that were ultimately approved because of the prior authorization process.
Variation in Use of Prior Authorization Across Medicare Advantage Insurers in 2024
In 2024, the volume of prior authorization determinations varied across Medicare Advantage insurers, as did the share of requests that were denied, the share of denials that were appealed, and the share of decisions that were overturned upon appeal, meaning people may have different experiences depending on the Medicare Advantage plan in which they enroll.
Across most insurers, fewer prior authorization requests per enrollee were correlated with a higher share of requests being denied and vice versa. For example, prior authorization requests for UnitedHealth Group Inc. and Humana Inc., the two largest Medicare Advantage insurers, were among the lowest (UnitedHealth Group Inc., 1.0 requests per enrollee) and the highest (Humana Inc., 2.2 requests per enrollee) observed, and correspondingly, denial rates were above average (UnitedHealthcare, 12.8%) and below average (Humana, 5.8%) for these insurers.
While all Medicare Advantage insurers require prior authorization for at least some services, there is variation across insurers and plans in the specific services that are subject to these requirements. In addition, some insurers waive prior authorization requirements for certain providers, for example, as part of risk-based contracts or through “gold carding” programs that exempt providers with a history of complying with the insurer’s prior authorization policies.
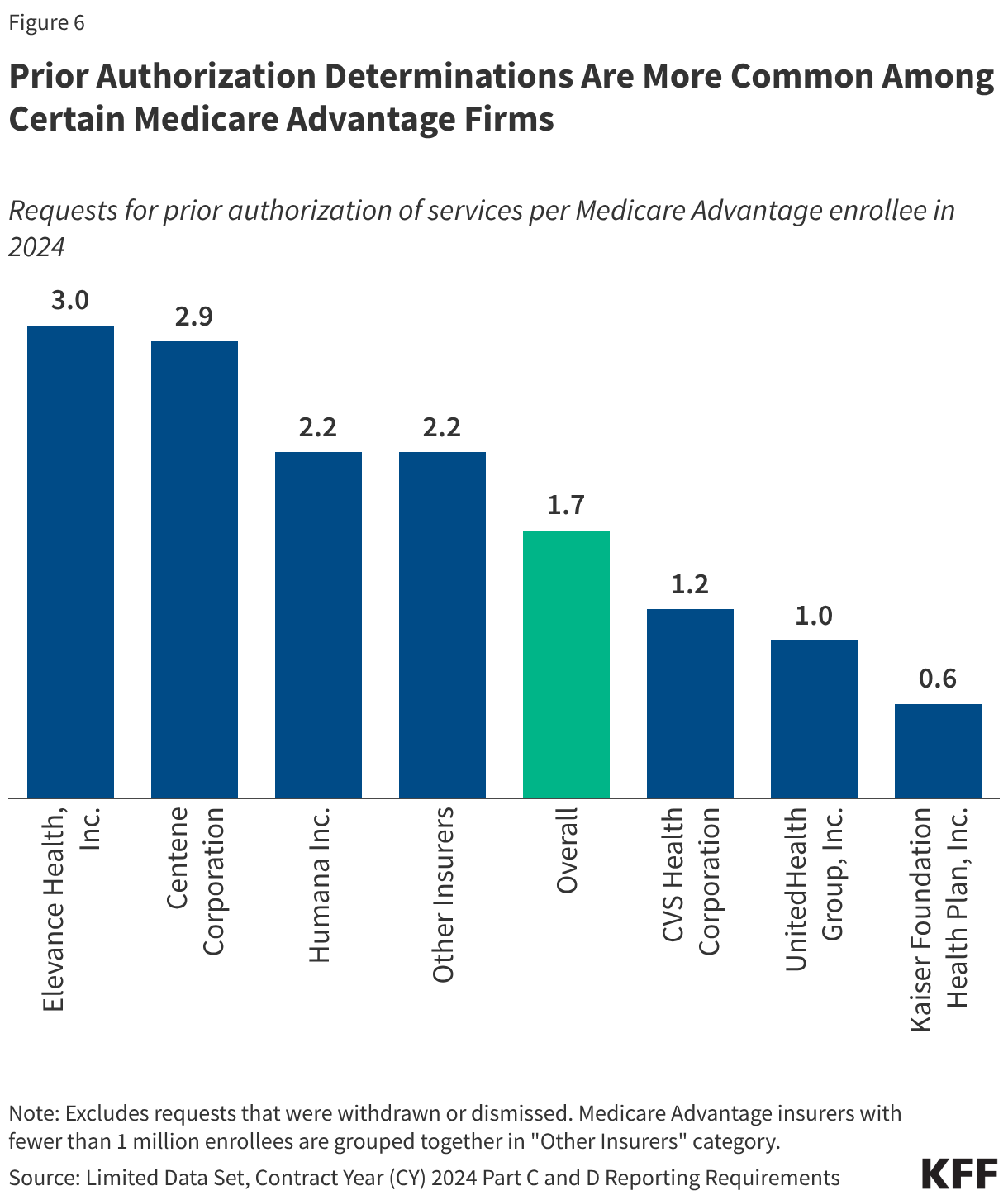
Prior authorization requests were most common among Elevance and Centene plans.
The number of prior authorization requests per enrollee ranged from a low of 0.6 requests per enrollee in plans sponsored by Kaiser Foundation Health Plan, Inc. to a high of 3.0 requests per enrollee in Elevance Health, Inc. and Centene Corporation plans (Figure 6). Kaiser is atypical among insurers in that it generally operates its own hospitals and contracts with an affiliated medical group. Looking across other insurers that are more similar, the low end of the range was 1.0 prior authorization requests per enrollee in UnitedHealth Group, Inc. plans. Differences across Medicare Advantage insurers in the number of prior authorization requests per enrollee likely reflect some combination of differences in the services subject to prior authorization requirements, the frequency with which contracted providers are exempted from those requirements (which may be related to the extent to which providers are affiliated with the insurer), how onerous the prior authorization process is for a particular insurer relative to others, and differences in enrollees’ health conditions and the health care services they use.
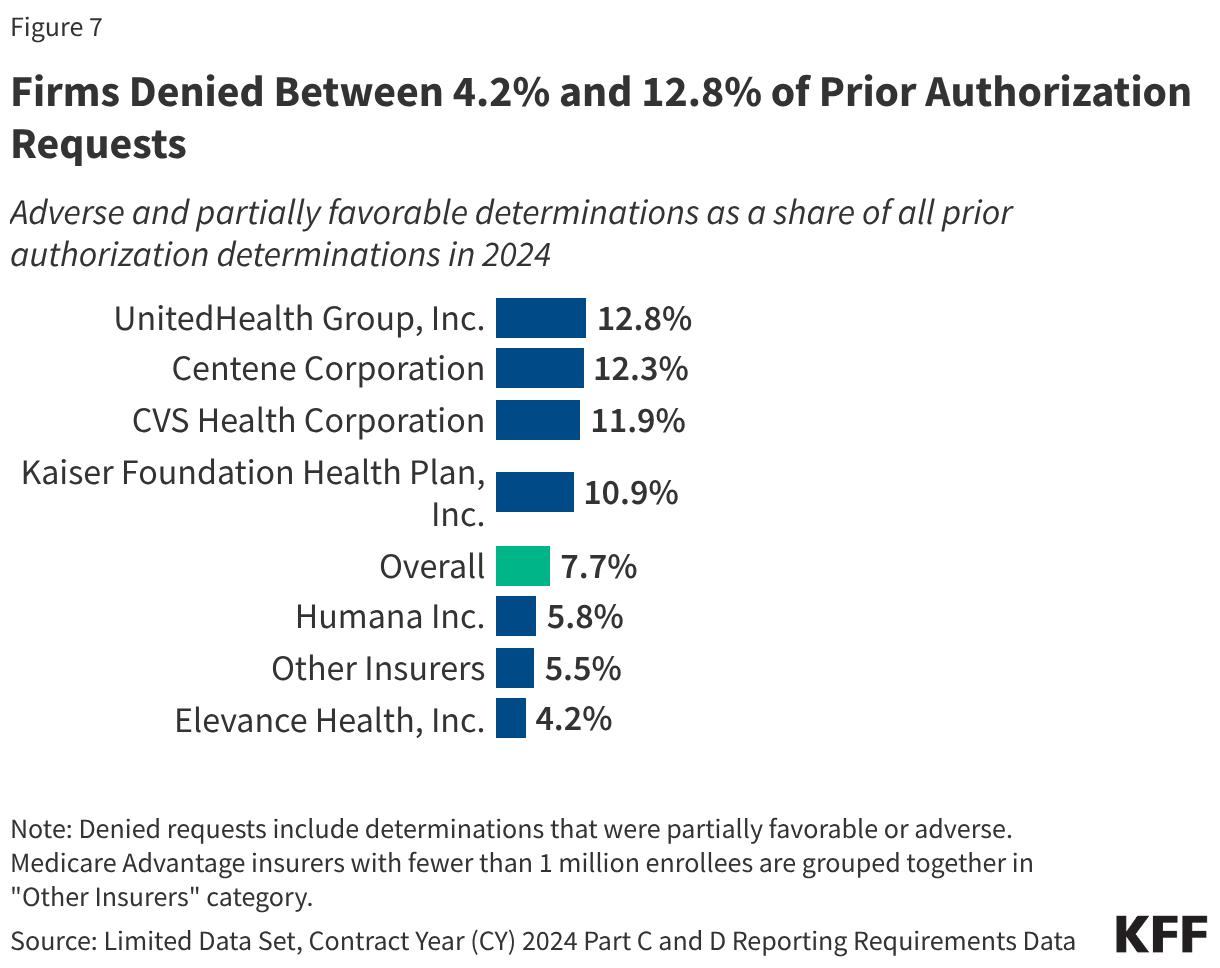
UnitedHealth Group denied the highest share of prior authorization requests while Elevance denied the fewest.
The denial rate ranged from 4.2% of prior authorization requests for Elevance Health plans to 12.8% of prior authorization requests for UnitedHealth Group plans (Figure 7). The overall denial rate includes requests that were both fully and partially denied (adverse and partially favorable determinations, respectively).
Most insurers that had more prior authorization requests per enrollee than average denied a smaller share of those requests than average, such as Elevance Health, which had 3.0 prior authorization requests per enrollee and a denial rate of 4.2%. Conversely, insurers with fewer prior authorization requests per enrollee denied a higher share of those requests, such as UnitedHealth Group, which had 1.0 prior authorization requests per enrollee and a denial rate of 12.8%. Centene Corporation was an exception with both a relatively high number of prior authorization requests (2.9 per enrollee) and a relatively high denial rate (12.3%).
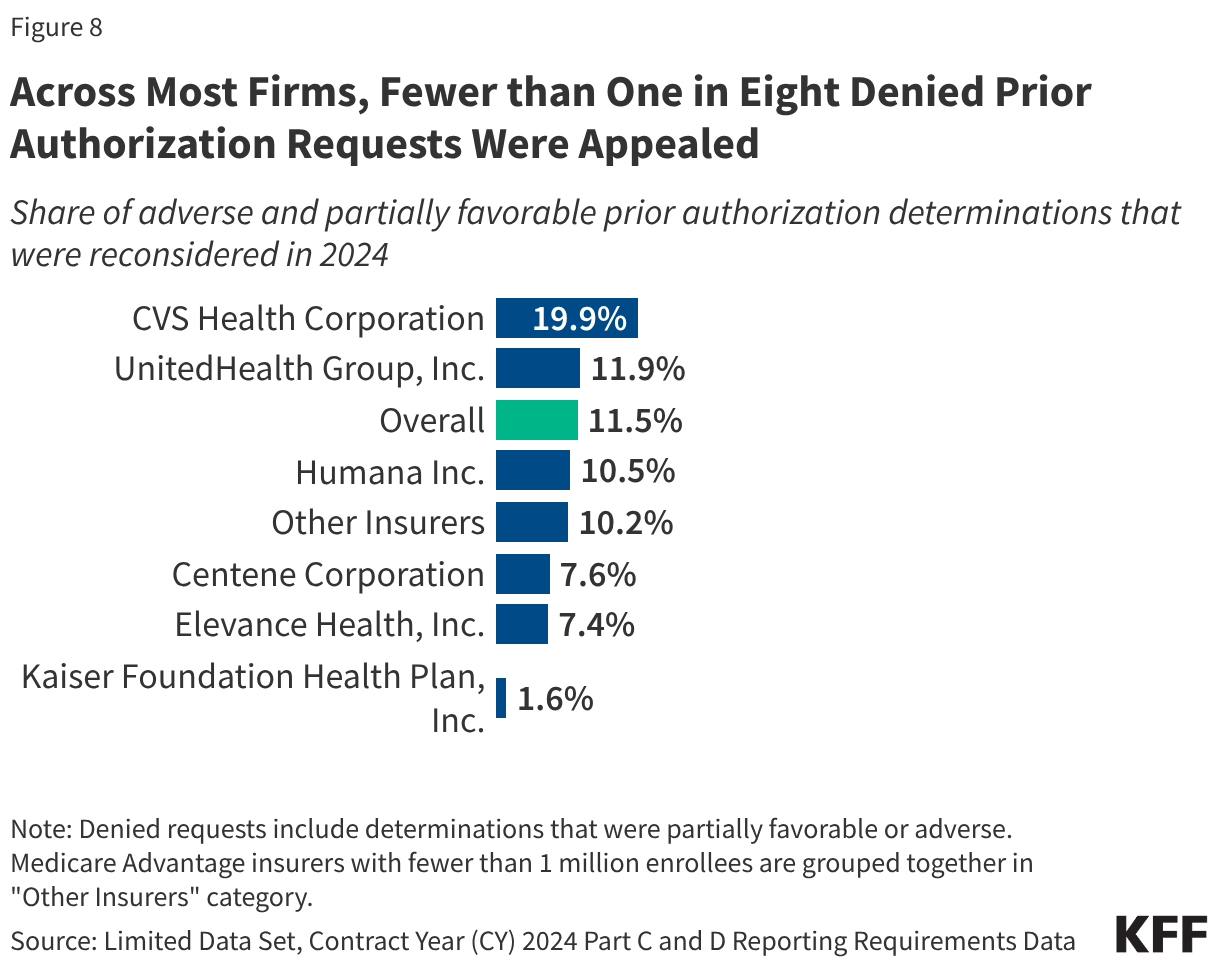
Across all insurers, a small share of denials was appealed.
Most denied prior authorization requests are not appealed to the Medicare Advantage insurer. The shares ranged from 1.6% for Kaiser Foundation Health Plan to 19.9% for CVS Health Corporation, with the appeal of fewer than one in twelve denials across all insurers except CVS Health Corporation (Figure 8).
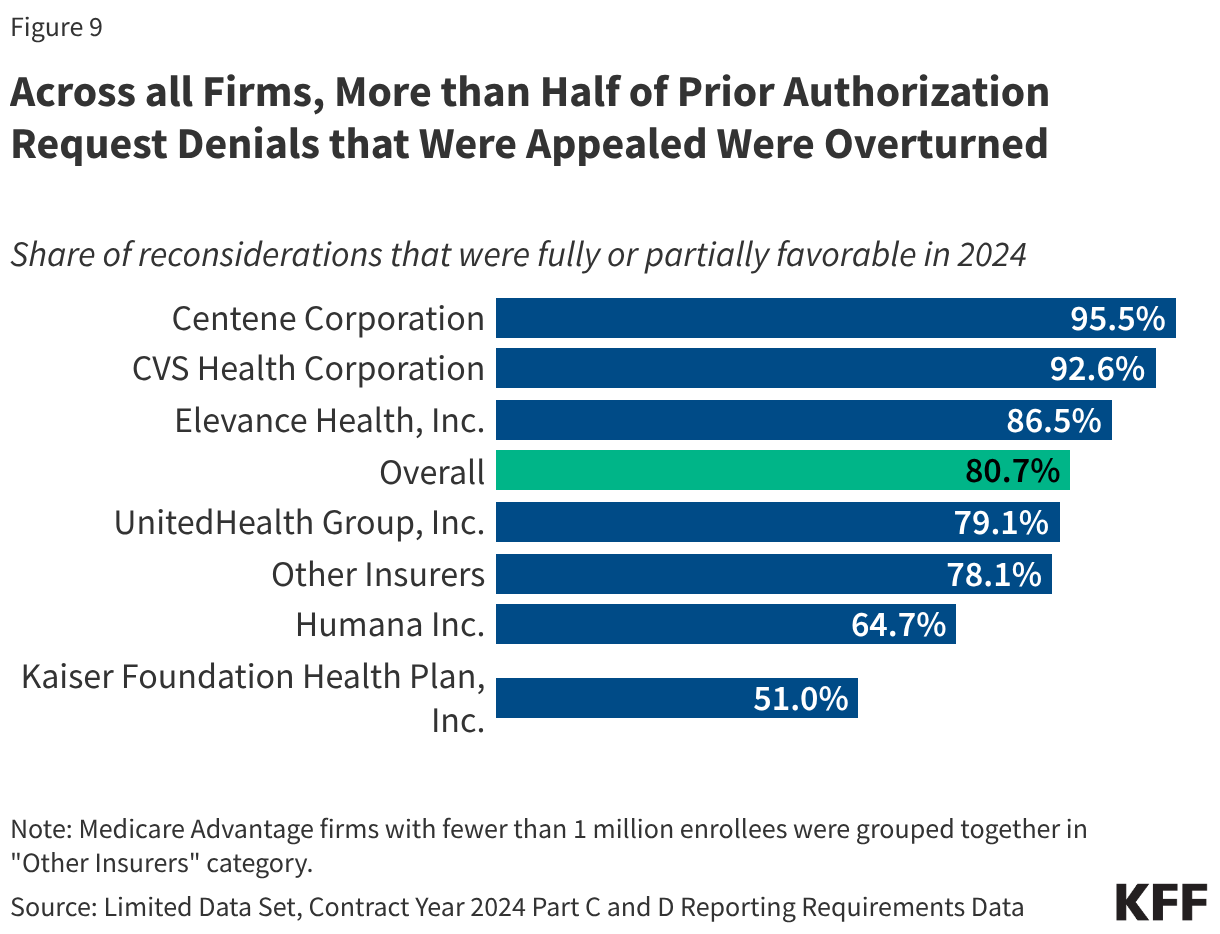
Across all firms, more than half of appeals were successful.
Even though most denials were not appealed, when they were, most of the initial decisions were partially or fully overturned. The share of appeals that resulted in favorable decisions overturning the initial denial was lowest for Kaiser Foundation Health Plan (51.0%) and highest for Centene Corporation (95.5%) (Figure 9), which also had the second highest share of requests initially denied.
The Use of Prior Authorization in Traditional Medicare
The use of prior authorization is relatively new to traditional Medicare and only used for a limited set of services, including certain outpatient hospital services, non-emergency ambulance transport, and durable medical equipment (see Box 1). The prior authorization process does not change any documentation requirements that are necessary for receiving Medicare payment – the confirmation that coverage requirements are met are required earlier in the review process. CMS has published reports presenting data on the use of prior authorization in traditional Medicare for fiscal years 2021, 2022, 2023, and 2024. These reports include information on the number of requests received, reviews completed, and the number and share of requests that were affirmed. For 2021 and 2022 only, the data also include information on appeals and the outcome of the appeal.
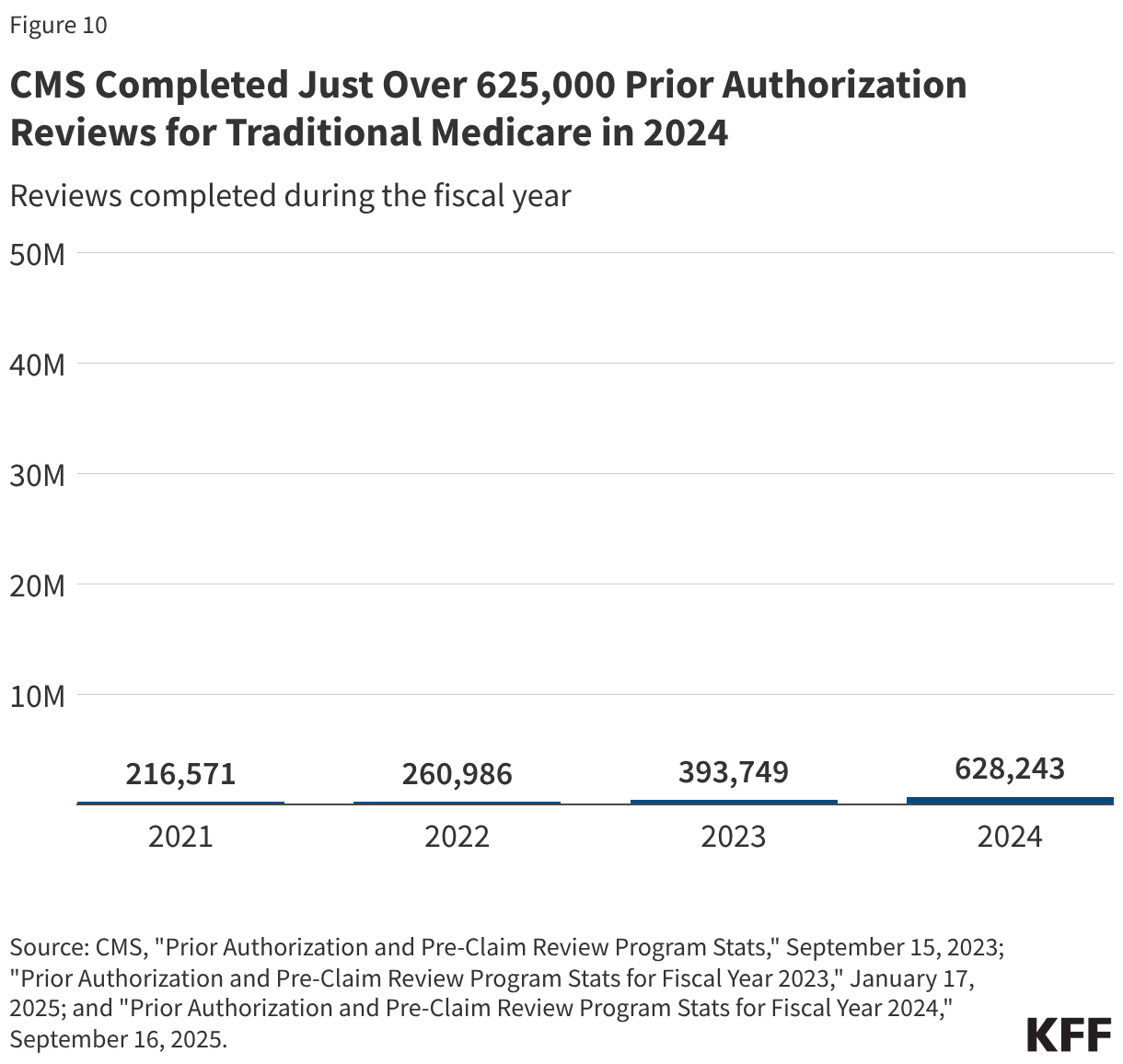
Just over 625,000 prior authorization reviews were completed by CMS for traditional Medicare in 2024.
Across the three categories of services that required prior authorization, there were 216,571 reviews completed in 2021, 260,986 reviews completed in 2022, 393,749 reviews completed in 2023, and 628,243 reviews completed in 2024 (Figure 10). This translates to about 2 prior authorization reviews per 100 traditional Medicare beneficiaries in 2024.
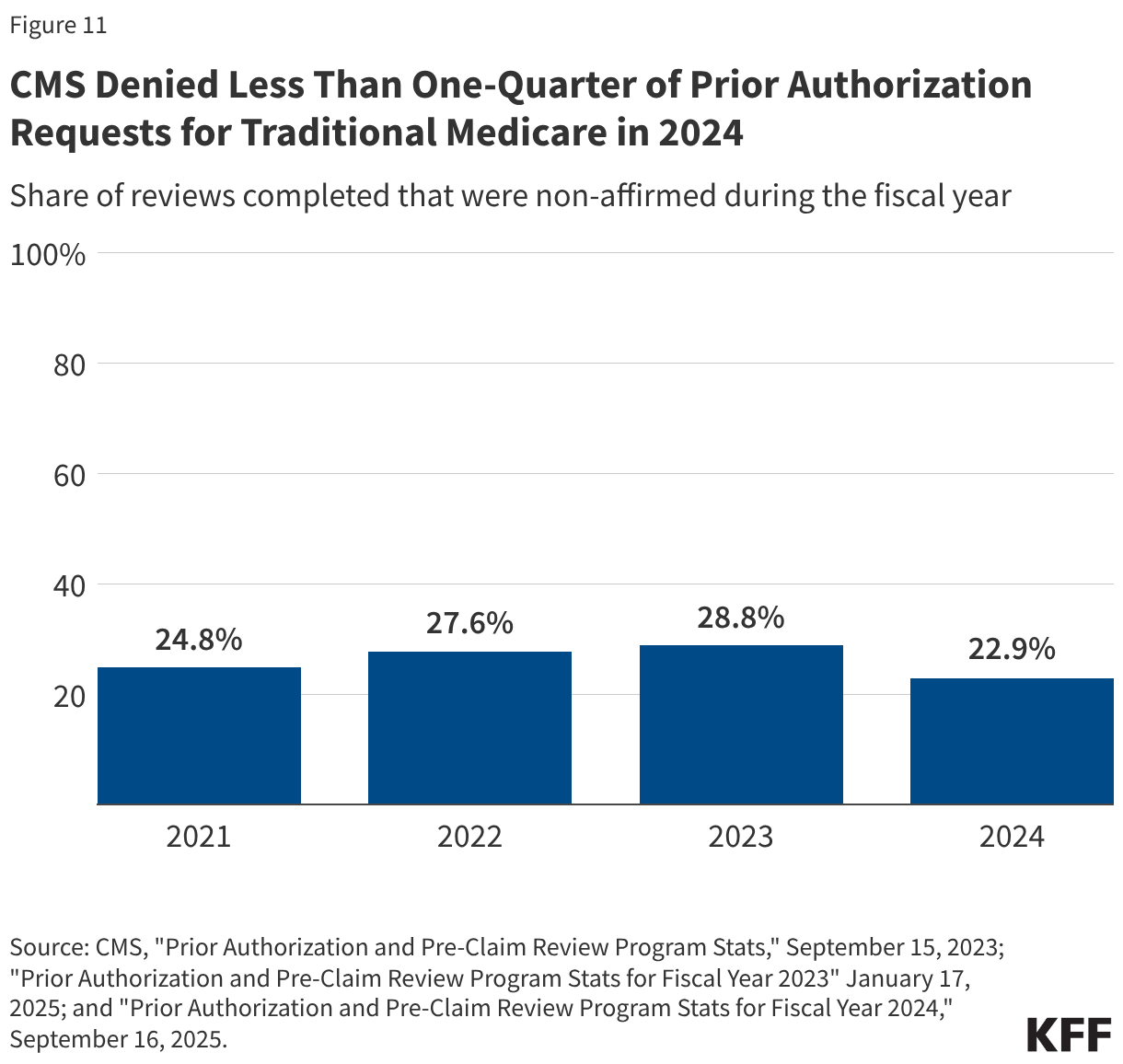
Less than one-quarter of prior authorization requests in traditional Medicare were denied.
CMS approved (or affirmed) the majority of prior authorization requests it reviewed. CMS reported that 24.8% of requests were denied (or non-affirmed) in 2021, 27.6% of requests were denied in 2022, 28.8% of requests were denied in 2023, and 22.9% of requests were denied in 2024 (Figure 11). This reflects 53,680 denied requests in 2021, 72,029 denied requests in 2022, 113,448 denied requests in 2023, and 143,705 denied requests in 2024.
In traditional Medicare, a small share of denied prior authorization requests was appealed to CMS and the share of prior authorization requests that were appealed and overturned upon appeal varied across service type.
In 2022, fewer than 5,000 denied prior authorization requests in traditional Medicare were appealed to the first level. As a share of all denied requests that translates to 6.4% appealed in 2022. Of the denied requests, 1,323 prior authorization denials were overturned upon appeal, which represents 28.7% of all first level appeals (Figure 12). Appeals data in traditional Medicare are presented differently across the CMS reports. Specifically, the 2023 and 2024 reports include a separate claims and appeals section for each category of service, which appears to include a broader universe of reviews by Medicare Administrative Contractors, including those for payment of services rendered, than what is presented in the report for 2021 and 2022. Given the differences in the data reported, we present appeals and whether the decision was overturned on appeal for 2022 only.
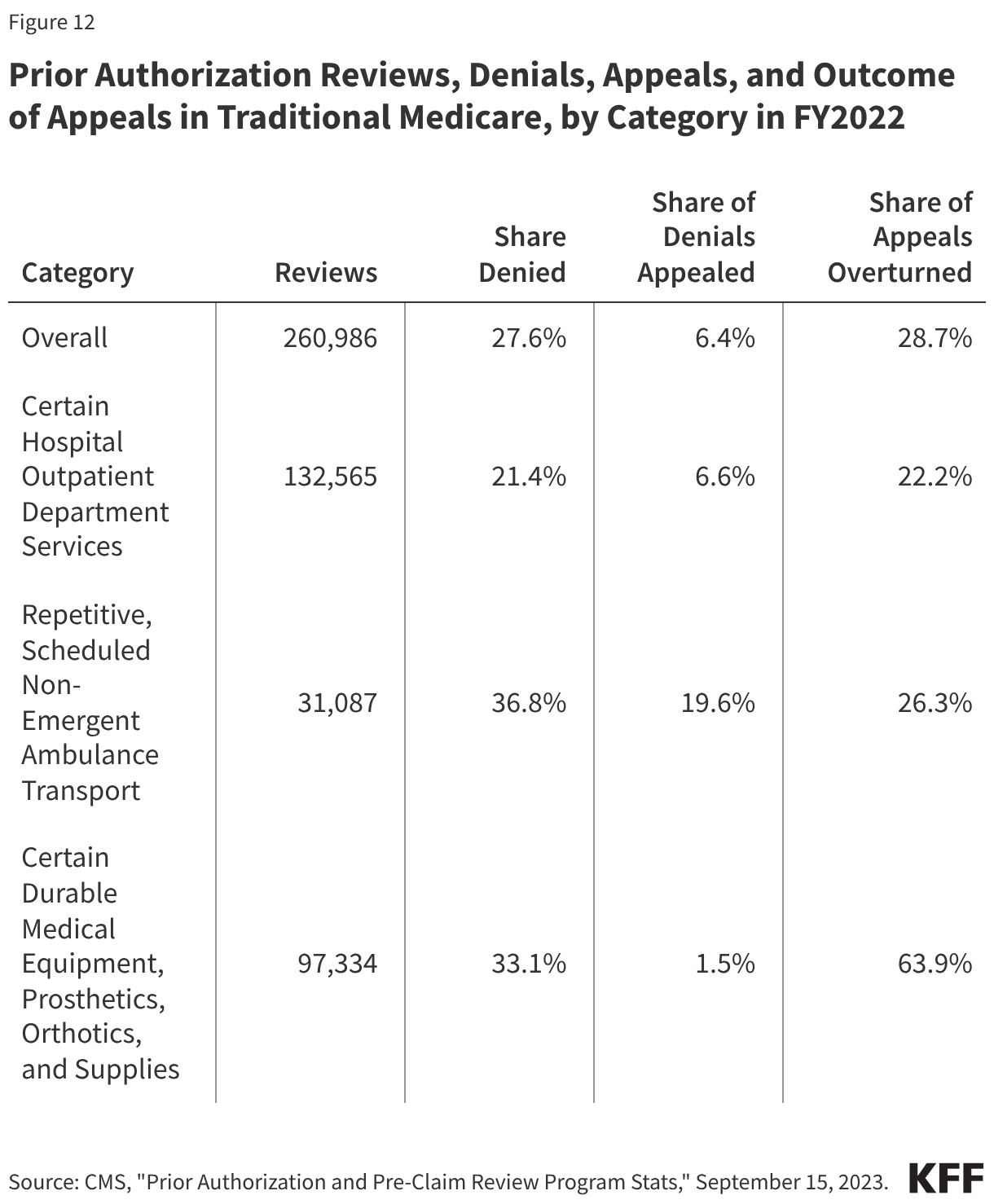
Denied requests for the ambulance transport services were most often appealed (19.6%); just 6.6% of denials for certain hospital outpatient services and 1.5% of certain durable medical equipment, prosthetics, orthotics and supplies requests were appealed.
The share of appeals that resulted in overturning the initial decision also varied widely. Nearly two-thirds (63.9%) of appeals for durable medical equipment, prosthetics, orthotics and other supplies were successful. That compares to 26.3% of appeals for the ambulance transport services and 22.2% of appeals for certain hospital outpatient services.
Box 1: Prior Authorization Requirements in Traditional Medicare
In 2015, CMS issued a final rule that established a prior authorization process for certain Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) items, with the goal of reducing the use of items that had been frequently subject to unnecessary utilization. Initial implementation began March 20, 2017, and items have been added and subtracted to the list over the following years through subsequent rulemaking. As of January 13, 2026, the DMEPOS items prior authorizations list includes over 70 items, including for pressure reducing support surfaces, power mobility devices, and lower limb prosthetics. Additionally, in December 2025, CMS issued a rule which establishes a prior authorization exemption process for certain DMEPOS items, allowing qualifying suppliers, such as those who show an affirmation rate of 90% or higher, to be exempt from prior authorization.
In a 2019 final rule (effective July 1, 2020), CMS established national prior authorization requirements for a set of hospital outpatient department services which had experienced significant increases in utilization and that are likely to be cosmetic procedures and not covered by Medicare, but may be combined with other therapeutic services, including blepharoplasty, botulinum toxin injections, panniculectomy, rhinoplasty, and vein ablation. In further rulemaking (effective July 1, 2021), CMS added implanted spinal neurostimulators and cervical fusion with disc removal to the list of services requiring prior authorization, and another rule (effective July 1, 2023) added facet joint interventions.
The CMS Repetitive, Scheduled Non-Emergent Ambulance Transport (RSNAT) Prior Authorization Model uses the authority provided through the Center for Medicare and Medicaid Innovation (CMMI, or Innovation Center) to test whether prior authorization for non-emergent ambulances for certain medical appointments would save money for Medicare while maintaining access and quality of care. The model was first implemented in select states in December 2014 and was ultimately expanded nationwide in September 2020 as it met the model requirements, saving Medicare about $650 million over four years.
On January 1, 2026, the Center for Medicare and Medicaid Innovations (CMMI) launched the Wasteful and Inappropriate Service Reduction (WISeR) Model that establishes new prior authorization requirements in traditional Medicare for select services in six states (New Jersey, Ohio, Oklahoma, Texas, Arizona, and Washington). These services include skin substitutes (synthetic products used in the treatment of severe or chronic wounds), orthopedic pain management services, electrical nerve stimulator implants, incontinence control devices, and services related to the diagnosis and treatment of impotence. According to CMS, the model will test the use of enhanced technologies, such as artificial intelligence, to conduct prior authorization for services vulnerable to fraud or abuse.
Box 2: Recent Administrative Actions and Proposed Legislation on Prior Authorization
The Administration recently finalized three rules related to prior authorization.
The first rule (effective date: June 5, 2023) issued by the Biden Administration clarifies the criteria that may be used by Medicare Advantage plans in establishing prior authorization policies and the duration for which a prior authorization is valid. Specifically, the rule states that prior authorization may only be used to confirm a diagnosis and/or ensure that the requested service is medically necessary and that private insurers must follow the same criteria used by traditional Medicare. That is, Medicare Advantage prior authorization requirements cannot result in coverage that is more restrictive than traditional Medicare. The rule also describes how private insurers may consider additional information when traditional Medicare does not have fully established coverage criteria. The rules apply to coverage beginning with plan year 2024.
The second rule (effective date: April 8, 2024) issued by the Biden Administration is intended to improve the use of electronic prior authorization processes, as well as the timeliness and transparency of decisions, and applies to Medicare Advantage and certain other insurers. Specifically, it shortens the standard time frame for insurers to respond to prior authorization requests from 14 to 7 calendar days starting in January 2026 and standardizes the electronic exchange of information by specifying the prior authorization information that must be included in application programming interfaces starting in January 2027. It also requires that beginning in 2026, insurers post all items and services subject to prior authorization and the share of prior authorization requests that were approved, denied, and approved after appeal. A bipartisan bill has also been introduced to codify pieces of this rule.
The third rule (effective date: June 3, 2024) also issued by the Biden Administration would have required Medicare Advantage plans to evaluate the effect of prior authorization policies on people with certain social risk factors (“health equity analysis”) starting with plan year 2025, but the Trump Administration announced in June 2025 that it would not enforce these requirements.
Additionally, lawmakers in Congress have introduced several bills aimed improving the prior authorization process, including codifying changes made through recent rulemaking, and requiring written clinical criteria for prior authorization requirements, which were both introduced on a bipartisan basis. Other legislation would penalize insurers when initially denied requests are overturned upon appeal too often, require plans to include prior authorization information in plan advertisements, and one proposal would prohibit the use of prior authorization altogether.
Methods
The analysis of Medicare Advantage uses organization determinations and reconsiderations – Part C data from the Centers for Medicare and Medicaid Services (CMS) Part C and D reporting requirements public use file for contract years 2019 – 2021 and the limited data set for contract years 2022 through 2024. Medicare Advantage insurers submit the required data at the contract level to CMS and CMS performs a data validation check.
Data for Medicare Advantage contracts is aggregated to the parent company level. Insurers with less than 1 million enrollees into “other insurers”.
This analysis reflects data on service determinations and does not include claims determinations (for payment for services already provided). We also do not include withdrawn or dismissed determination requests in this analysis.
The enrollment data are from the CMS Medicare Advantage enrollment file for March of each year at the contract-plan-county level. We then sum up to the contract level to merge with the determination and reconsideration data. Contract-plan-county combinations are not included if there are fewer than 11 enrollees. The traditional Medicare analysis uses data included “Prior Authorization and Pre-Claim Review Program Stats,” published by CMS on September 15, 2023, which reflects prior authorization reviews completed in fiscal years 2021 and 2022, “Prior Authorization and Pre-Claim Review Program Stats for Fiscal Year 2023,” published on January 17, 2025, and “Prior Authorization and Pre-Claim Review Program Stats for Fiscal Year 2024,” published on September 16, 2025. The total number of traditional Medicare beneficiaries is from the Medicare Monthly Enrollment Dashboard for 2021 through 2024. While CMS published data on the use of prior authorization in traditional Medicare for FY2023 and FY2024, the information for appeals are not comparable to FY2021 and FY2022 data and are therefore not included in this analysis.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.