10 FAQs: Medicare’s Role in End-of-Life Care
About eight of 10 of the 2.6 million people who died in the US in 2014 were people on Medicare, making Medicare the largest insurer of health care provided during the last year of life.1 In fact, roughly one-quarter of traditional Medicare spending for health care is for services provided to Medicare beneficiaries in their last year of life—a proportion that has remained steady for decades.2 The high overall cost for health care received in the last year of life is not surprising given that many who die have multiple serious and complex conditions.
Aside from cost, several other factors contribute to difficult clinical and policy discussions about whether patients are getting the care they want or need as they approach the end of their lives. Research has found, for example, that most adults (90 percent) say they would prefer to receive end-of-life care in their home if they were terminally ill, yet data show that only about one-third of Medicare beneficiaries (age 65 and older) died at home.3
In 2016, Medicare began covering advance care planning—discussions that physicians and other health professionals have with their patients regarding end-of-life care and patient preferences—as a separate and billable service. The following 10 FAQs provide information on Medicare’s role in end-of-life care and advance care planning. In addition to defining relevant terms, and explaining Medicare’s current and future coverage for end-of-life care, these FAQs also describe recent relevant rules released by the Administration and additional proposals from Congress regarding advance care planning and care for people with serious and terminal illness.
Q1: What is “end-of-life care” and does Medicare cover it?
A: End-of-life care encompasses all health care provided to someone in the days or years before death, whether the cause of death is sudden or a result of a terminal illness that runs a much longer course. For people ages 65 and over, the most common causes of death include cancer, cardiovascular disease, and chronic respiratory diseases.4 Medicare covers a comprehensive set of health care services that beneficiaries are eligible to receive up until their death. These services include care in hospitals and several other settings, home health care, physician services, diagnostic tests, and prescription drug coverage through a separate Medicare benefit. Many of these Medicare-covered services may be used for either curative or palliative (symptom relief) purposes, or both. Medicare beneficiaries with a terminal illness are eligible for the Medicare hospice benefit that includes additional services—not otherwise covered under traditional Medicare—such as bereavement services. The Medicare hospice benefit is discussed in more detail in Question 5.
Q2: What is “advance care planning” and does Medicare cover it?
A: Advance care planning involves multiple steps designed to help individuals a) learn about the health care options that are available for end-of-life care; b) determine which types of care best fit their personal wishes; and c) share their wishes with family, friends, and their physicians. In some cases, patients who have already considered their options may need only one advance care planning conversation with their physician. However, experts state that frequently, beneficiaries may require a series of conversations with their physician or other health professionals to clearly understand and define their end-of-life wishes.5
Starting January 1, 2016, Medicare began covering advance care planning as a separate service provided by physicians and other health professionals (such as nurse practitioners who bill Medicare using the physician fee schedule). Medicare now covers advance care planning provided in medical offices and facility settings, including hospitals. As with most other physician services, beneficiaries are subject to cost sharing for advance care planning provided by their physician or health professional. If Medicare beneficiaries desire advance care planning during their annual wellness visit, physicians and other health professionals may provide it during the visit and bill Medicare separately for it. However, beneficiaries will have not have any cost sharing liability for advance care planning provided in conjunction with their annual wellness visits.
Q3: Are policymakers, such as CMS or Congress, considering changes in Medicare’s coverage of advance care planning?
A: Yes. The agency that runs Medicare, the Centers for Medicare and Medicaid services (CMS), finalized regulations in fall 2015 that allow Medicare to pay physicians and other qualified health care professionals for providing advance care planning to beneficiaries.6 Specifically, in a proposed regulation released July 8, 2015, CMS introduced two new billing codes—previously recommended by the American Medical Association—for advance care planning provided to Medicare beneficiaries. On October 30, 2015, CMS finalized these proposed provisions, allowing physicians and other health professionals to bill Medicare for advance care planning, as a separate service, starting January 1, 2016. Previous Medicare coverage rules only allowed reimbursement for advance care planning under very limited circumstances.7
In Congress, prior to this new CMS regulation on advance care planning, two bipartisan bills pertaining to advance directives and end-of-life care were introduced—one in the Senate and one in the House. In the Senate, Sen. Mark Warner and Sen. Johnny Isakson introduced the Care Planning Act of 2015 (S.1549), with other cosponsors.8 This legislation included coverage under Medicare for advanced illness planning and care coordination services, including structured discussions about treatment options and patient preferences, to Medicare beneficiaries who have a serious progressive or life-threatening illness. In the House, Rep. Earl Blumenauer and 59 cosponsors introduced the Personalize Your Care Act of 2013 (H.R.1173).9 This legislation included Medicare and Medicaid coverage for advance care planning consultations between patients and doctors or other health care professionals.
Q4: What are “advance directives”? Are health care facilities, such as hospitals or skilled nursing facilities, required to keep records of Medicare patients’ advance directives?
A: Advance directives are written instructions that are intended to reflect a patient’s wishes for health care to guide medical decision-making in the event that a patient is unable to speak for her/himself. Advance directives typically result from advance care planning and often take the form of a living will, which defines the medical treatment that patients prefer if they are incapacitated, or designation of a certain person as a medical power of attorney.10 Advance directives fall under state regulation, and the required forms for formal advance directives vary from state to state.11
Studies have found that about 4 in 10 Americans ages 65 and older do not have advanced directives or have not written down their own wishes for end-of-life medical treatment.12 Additionally, demographic differences appear to play a role in the likelihood of having advanced directives.13 Specifically, African Americans and Hispanics have advance directives at lower rates compared to whites, as do people with lower incomes and lower levels of completed education.14 Researchers have identified several factors that contribute to these differences, including cultural and religious differences, communication challenges between patients and medical staff, distrust of medical care systems, and awareness of advance directive options.15
The Patient Self-Determination Act, which took effect in 1991, included a list of Medicare requirements for health care facilities regarding advance directives. Under this law, facilities such as hospitals and skilled nursing facilities must ask each patient upon admission if he or she has an advance directive and record its existence in the patient’s file.16 Facilities cannot require any patient to create an advance directive before providing treatment or care, and likewise, Medicare patients are not required to have an advance directive before they receive care.17 Recent surveys show that among long-term care patients, those receiving care in a facility (such as a nursing home or hospice facility) are more likely to have advance directives in place.18
Q5: Does Medicare cover hospice care? How many Medicare beneficiaries use hospice?
A: Yes. For terminally ill Medicare beneficiaries who do not want to pursue curative treatment, Medicare offers a comprehensive hospice benefit covering an array of services, including nursing care, counseling, palliative medications, and up to five days of respite care to assist family caregivers. Hospice care is most often provided in patients’ homes.19 Medicare patients who elect the hospice benefit have little to no cost-sharing liabilities for most hospice services.20 In order to qualify for hospice coverage under Medicare, a physician must confirm that the patient is expected to die within six months if the illness runs a normal course. If the Medicare patient lives longer than six months, hospice coverage may continue if the physician and the hospice team re-certify the eligibility criteria.
Of all Medicare beneficiaries who died in 2014, 46 percent used hospice—a rate that has more than doubled since 2000 (21 percent).21 The rate of hospice use increases with age, with the highest rate existing among decedents ages 85 and over. Hospice use is also higher among women than men and among white beneficiaries than beneficiaries of other races/ethnicities. Hospice care accounts for about 10 percent of traditional Medicare spending in beneficiaries’ last year of life.22 Medicare Advantage plans do not cover hospice care; therefore, when a Medicare Advantage enrollee receives hospice care, his or her hospice coverage falls under traditional Medicare (Parts A and B).23
While many researchers, policymakers, and patient advocates cite the numerous benefits of hospice care in providing appropriate end-of-life care to Medicare patients, questions have been raised about the growth in for-profit hospice agencies, citing differences in the average care needs of the patients they serve compared with those served by non-profit agencies.24
Q6: What is “palliative care” and does Medicare cover it?
A: Palliative care can be integral to end-of-life care in that it generally focuses on managing symptoms and providing comfort to patients and their families. While palliative care is common among people receiving end-of-life care, it is not necessarily restricted to people with terminal illnesses. The Center to Advance Palliative Care emphasizes that palliative care is commonly used among people living with serious, complex, and chronic illnesses, including cancer, heart disease, general pain, or depression.25 Close to half (45 percent) of all Medicare beneficiaries have four or more chronic conditions for which palliative care services may be clinically indicated to alleviate symptoms—either in combination with or instead of curative treatment.26 The Medicare hospice benefit (described in Question 7) also covers palliative care for beneficiaries with terminal illness.
Q7: How much does Medicare spend on end-of-life care, and for which services?
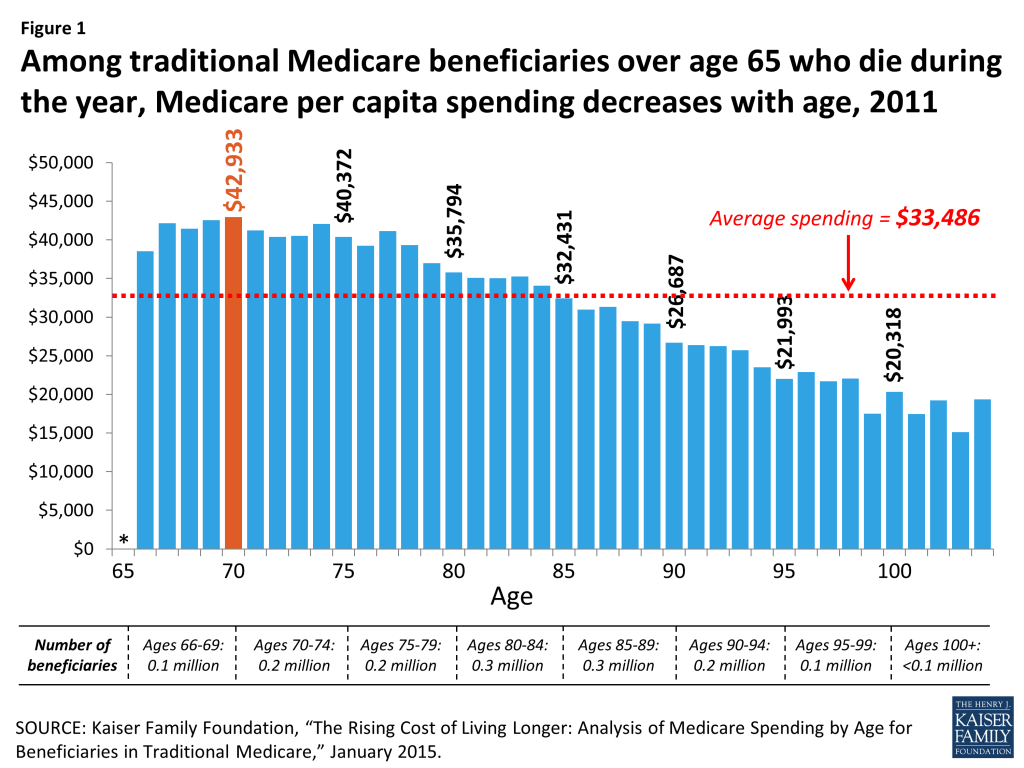
A: Among seniors in traditional Medicare who died in 2014, Medicare spending averaged $34,529 per beneficiary – almost four times higher than the average cost per capita for seniors who did not die during the year.27 Other research shows over the past several decades, roughly one-quarter of traditional Medicare spending for health care is for services provided to beneficiaries ages 65 and older in their last year of life.28
Medicare spending during the year of death decreases with age after age 73 (Figure 1), suggesting that patients, families, and providers may be opting for less intensive and less costly end-of-life interventions for beneficiaries as they grow older. Specifically, per capita Medicare spending among decedents in 2014 peaked at age 73 ($43,353) and decreased by almost half ($23,181) by age 95.29 Approximately half of total Medicare spending for people who died in a given year goes toward hospital inpatient expenses, while hospice and skilled nursing services each accounted for about 10 percent of Medicare spending.30
Q8: Did the Affordable Care Act (ACA) affect Medicare coverage for end-of-life care or advance care planning?
A: No. The final ACA legislation did not include provisions that would allow physicians or other health professionals to seek separate Medicare payment for consultations on advance care planning. A House-passed predecessor bill (H.R.3200) included provisions that would have established Medicare reimbursement for advance care planning, as well as programs to increase public awareness of advance care planning, but these provisions were dropped from the final ACA legislation.31 Confusion regarding the ACA persisted even after it passed, as seen in a Kaiser Family Foundation survey which found that in 2013, more than one-third (35 percent) of people ages 65 and over incorrectly believed that a panel was created by the ACA to make end-of-life decisions for Medicare beneficiaries.32
Q9: Has the Institute of Medicine (IOM) made any recommendations regarding advance care planning and end-of-life care?
A: In fall 2014, the IOM released a comprehensive report, Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life, which included five recommendations aimed to increase the quality of end-of-life care and improve the ability for patients to choose their own treatment plan.33 In brief, the IOM recommendations call for:
- Coverage of comprehensive care for patients with advanced serious illnesses who are nearing the end of life by both government and private health insurers;
- The development of quality metrics and standards for clinician-patient communication and advanced care planning, with insurance reimbursement tied to performance on these standards;
- Strengthening clinical training and licensing/credentialing requirements in palliative care;
- Federal and regulatory action to establish financial incentives for integrating medical and social services for people nearing the end of life, including electronic health records that incorporate advanced care planning;
- Widespread efforts to provide information to the public on the benefits of advance care planning and the ability to for individuals to choose their own course of treatment.
Q10: How does the public feel about advance care planning and Medicare’s role in end-of-life preferences?
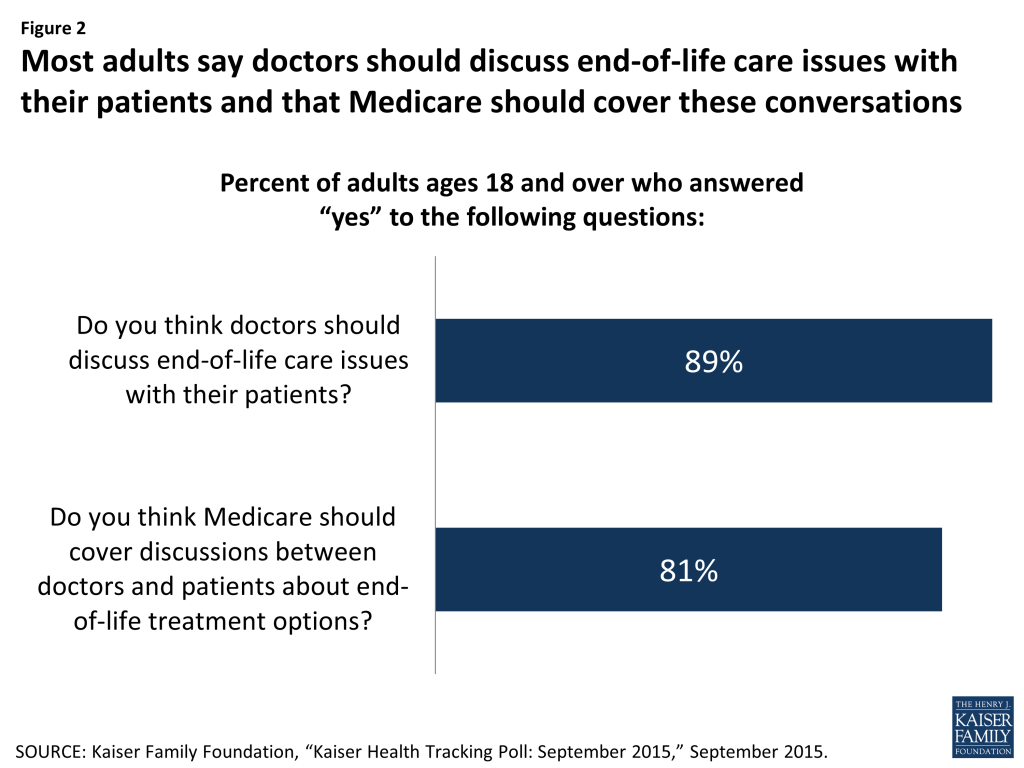
A: By and large, the public supports having doctors discuss end-of-life care issues with their patients, and having Medicare and private insurance cover these discussions (Figure 2). A recent Kaiser Family Foundation survey found that about 9 in 10 adults (89 percent) say doctors should discuss end-of-life care issues with their patients, yet only 17 percent of adults say they have had such a discussion with their doctor or health care provider. Among adults ages 65 and older, the share is somewhat higher (27 percent). Among all adults who said they had not had a discussion with their doctor or other health care provider about end-of-life care wishes, half said that they would want one. The majority of adults (81 percent) say Medicare should cover discussions between doctors and patients about end-of-life treatment options—comparable to the share (83 percent) favoring private insurance coverage for similar conversations.34 (This survey was conducted prior to the release of final regulations allowing Medicare coverage of advance care planning.)
- Juliette Cubanski, Tricia Neuman, Shannon Griffin, and Anthony Damico, “Medicare Spending at the End of Life: A Snapshot of Beneficiaries Who Died in 2014 and the Cost of Their Care,” Kaiser Family Foundation, July 14, 2016, https://modern.kff.org/medicare/issue-brief/medicare-spending-at-the-end-of-life/. ↩︎
- Gerald F. Riley and James D. Lubitz, “Long-Term Trends in Medicare Payments in the Last Year of Life,” Health Serv Res 2010;45 (2): 565-76; Christopher Hogan et al., “Medicare Beneficiaries’ Costs of Care In The Last Year of Life,” Health Aff (Millwood) 2001;20(4):188-95. ↩︎
- Approaching Death: Improving Care at the End of Life, Institute of Medicine, 1997; Joan M. Teno et al., “Change in End-of-Life Care for Medicare Beneficiaries,” JAMA 2013;309(5):470-77. ↩︎
- “Deaths: Final Data for 2010” 2013, Table 10. ↩︎
- Pam Belluck, “Coverage for End-of-Life Talks Gaining Ground,” NY Times, August 30, 2014, http://www.nytimes.com/2014/08/31/health/end-of-life-talks-may-finally-overcome-politics.html. ↩︎
- Centers for Medicare and Medicaid Services, 42 CFR Parts 405, 410, 411, 414, 425, 495, July 8, 2015, https://s3.amazonaws.com/public-inspection.federalregister.gov/2015-16875.pdf. Centers for Medicare and Medicaid Services, 42 CFR Parts 405, 410, 411, 414, 425, and 495 October 30, 2015. https://s3.amazonaws.com/public-inspection.federalregister.gov/2015-28005.pdf. ↩︎
- Prior to January 2016, neither physicians nor beneficiaries could seek reimbursement from Medicare for advance care planning if those discussions are the sole purpose of the visit. Instead, to be covered under Medicare, these discussions must have occurred either when they were part of appointments made for other reasons (such as illness or injury) or during the one-time “Welcome to Medicare” visit that may occur within a beneficiary’s first 12 months of Medicare enrollment. In 2010, CMS included advance care planning as a voluntary part of the ACA-established annual wellness visit in Medicare, but retracted this provision before it could take effect in January of 2011. CMS explained that it retracted this provision because the agency did not have ample “opportunity to consider prior to the issuance of the final rule the wide range of views on this subject held by a broad range of stakeholders.” ↩︎
- Care Planning Act of 2015, S.1549, 114th Cong., available at https://www.congress.gov/114/bills/s1549/BILLS-114s1549is.pdf. ↩︎
- Personalize Your Care Act of 2013, H.R.1173, 113th Cong., available at https://www.congress.gov/113/bills/hr1173/BILLS-113hr1173ih.pdf. ↩︎
- U.S. House, Omnibus Budget Reconciliation Act of 1990, Conference Report (to Accompany H.R. 5835), 101 H. Rpt. 101-964, printed Oct. 27, 1990, Sec. 4206; Adrienne L. Jones, Abigail J. Moss, and Lauren D. Harris-Kojetin, “Use of Advance Directives in Long-term Care Populations,” Centers for Disease Control and Prevention: Division of Health Care Statistics, January 2011, http://www.cdc.gov/nchs/data/databriefs/db54.pdf. ↩︎
- National Institute on Aging, “Advance Care Planning: Tips from the National Institute on Aging,” reprinted March 2014, http://www.nia.nih.gov/sites/default/files/advance_care_planning_tipsheet_0.pdf. ↩︎
- Pew Research Center, “Views on End-of-Life Medical Treatments,” November 2013, http://www.pewforum.org/2013/11/21/views-on-end-of-life-medical-treatments/. ↩︎
- Anne Wilkinson, Neil Wenger, and Lisa R. Shugarman, “Literature Review on Advance Directives” HHS Office of the Assistant Secretary for Planning and Evaluation, June 2007, available at http://aspe.hhs.gov/daltcp/reports/2007/advdirlr.pdf; Deborah Carr, “Racial Differences in End-of-Life Planning: Why Don’t Blacks and Latinos Prepare for the Inevitable?” OMEGA 2011;63(1):1-20; GB Zaide et al., “Ethnicity, race, and advance directives in an inpatient palliative care consultation service,” Palliat Support Care 2013;11(1):5-11; Lauren H. Nicholas et al., “Regional Variation in the Association Between Advance Directives and End-of-Life Medicare Expenditures,” JAMA 2011;306(13):1447-53; Kimberly S. Johnson, Maragatha Kuchibhatla, and James A. Tulsky, “What explains racial differences in the use of advance directives and attitudes toward hospice care?” J Am Geriatr Soc 2008;56(10):1953-58. ↩︎
- Nicholas et al. 2011. ↩︎
- Johnson, Kuchibhatla, and Tulsky 2008; Wilkinson, Wenger, and Shugarman 2007. ↩︎
- American Bar Association: Division for Public Education, “Law for Older Americans,” accessed May 29, 2015, http://www.americanbar.org/groups/public_education/resources/law_issues_for_consumers/patient_self_determination_act.html. ↩︎
- Health care providers can, however, refuse a treatment, but must notify the patient and/or their agent upon admission of any objections to the advance directive. For more information, see GAO report “Patient Self-Determination Act: Providers Offer Information on Advance Directive but Effectiveness Uncertain,” p. 45, August 1995, available at http://www.gpo.gov/fdsys/pkg/GAOREPORTS-HEHS-95-135/pdf/GAOREPORTS-HEHS-95-135.pdf. ↩︎
- Jones, Moss, and Harris-Kojetin 2011. ↩︎
- Medicare Payment Advisory Commission, Report to the Congress: Medicare Payment Policy, Chapter 12: “Hospice Services,” March 2015. ↩︎
- There is no deductible for hospice care in traditional Medicare. In general, cost-sharing is limited to copayments of up to $5 per prescription for outpatient prescription drugs (typically for pain and symptom management) and 5 percent coinsurance for inpatient respite care, if used. ↩︎
- Kaiser Family Foundation analysis of a five percent sample of 2014 Medicare claims from the CMS Chronic Conditions Data Warehouse. ↩︎
- Riley and Lubitz 2010. ↩︎
- MedPAC 2015. ↩︎
- Melissa W. Wachterman, Edward R. Marcantonio, Roger B. Davis, and Ellen P. McCarthy, “Association of hospice agency profit status with patient diagnosis, location of care, and length of stay.” JAMA 2011;305(5):472-9; R. C. Lindrooth and B. A. Weisbrod, “Do religious nonprofit and for-profit organizations respond differently to financial incentives? The hospice industry.” J Health Econ 2007;26(2):342-57. ↩︎
- Center to Advance Palliative Care, “About Palliative Care,” accessed May 29, 2015, https://www.capc.org/about/palliative-care/. ↩︎
- Kaiser Family Foundation, A Primer on Medicare: Key Facts About the Medicare Program and the People it Covers, March 2015, https://modern.kff.org/medicare/report/a-primer-on-medicare-key-facts-about-the-medicare-program-and-the-people-it-covers/. ↩︎
- Cubanski et al., 2016. ↩︎
- Riley and Lubitz 2010; Hogan et al. 2001. ↩︎
- Cubanski et al., 2016. ↩︎
- Ibid. ↩︎
- H.R. 3200, “America’s Affordable Health Choices Act of 2009,” 111th Cong. (2009), available at https://www.congress.gov/bill/111th-congress/house-bill/3200/text#toc-H896364C11C714348B7CF0E5B4357ADD0. ↩︎
- Kaiser Family Foundation, “Kaiser Health Tracking Poll: March 2013,” March 2013, https://modern.kff.org/health-reform/poll-finding/march-2013-tracking-poll/. ↩︎
- Institute of Medicine, Dying in America: Improving Quality and Honoring Individual Preferences Near the End of Life, September 17, 2014, pp. S-8 – S-16; For more information, see David G. Stevenson, Presentation at National Action Conference, March 20, 2015, Washington, D.C., available at http://www.iom.edu/Activities/Aging/TransformingEndOfLife/2015-MAR-20/Videos/Panel%20on%20Financing%20for%20Health%20and%20Social%20Services/21-Stevenson-Video.aspx. ↩︎
- Bianca DiJulio, Jamie Firth, and Mollyann Brodie, “Kaiser Health Tracking Poll: September 2015,” September 2015, available at https://modern.kff.org/health-costs/poll-finding/kaiser-health-tracking-poll-september-2015/. ↩︎