State Plans for CHIP as Federal CHIP Funds Run Out
Federal funding for the Children’s Health Insurance Program (CHIP) expired on September 30, 2017. CHIP covers 8.9 million children in working families who earn too much to qualify for Medicaid but cannot afford or access private coverage. (See here for state Medicaid and CHIP eligibility limits for children.) This fact sheet provides an overview of state plans for CHIP as they grow closer to exhausting federal funds amid continued delay of Congressional action to extend funding. It is based on data collected from state Medicaid and CHIP officials by the Kaiser Family Foundation (KFF) and Health Management Associates (HMA) during November 2017, which updates data earlier reported in Summer 2017. The findings show that about three-quarters of states anticipate exhausting funding by the end of March 2018 and that several states have begun or will begin notifying families about coverage reductions before the end of 2017. As such, further delay in Congressional action is likely to result in confusion among families that could lead to coverage losses and administrative costs even if funding is extended in the next few weeks. See Appendix Table 1 for state data.
When Will States Run out of Funding?
Remaining funds available to states, including redistribution funds, are limited and anticipated to run out soon. Federal stopgap funds available to states include remaining federal funds from each state’s federal fiscal year (FY) 2017 CHIP allotment and redistribution funding from prior years provided by the Centers for Medicare and Medicaid Services (CMS) from a limited amount of unspent funds across all states. However, once states exhaust those funds, no additional funds will be available unless Congress enacts legislation. As of December 6, 2017, nine states have exhausted their FY 2017 allotments and have received redistribution funds from CMS to continue coverage. CMS is expected to release the final redistribution payments in the near-term, but these amounts will be insufficient to cover states’ FY 2018 CHIP shortfalls.1
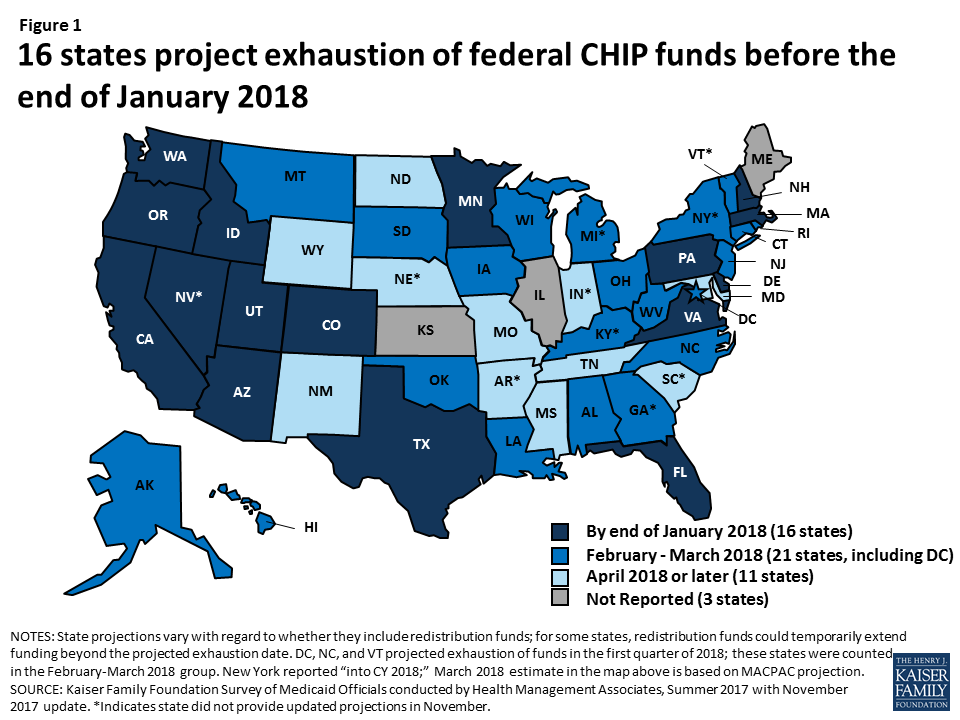
A third of states anticipate exhausting funding by the end of January 2018 (Figure 1). Among the 48 states2 that provided an estimate of when they will exhaust federal funds, including the 38 states that provided an update in November 2017, 16 states projected they will exhaust federal funds by the end of January 2018, and an additional 21 states projected they will exhaust federal funds by the end of March 2018. State projections are fluid and change as enrollment and costs fluctuate and states receive redistribution funds.
The majority of states will face a budget shortfall without an extension of federal funds because nearly all states assumed continued federal CHIP funding in their state fiscal year (SFY) 2018 state budgets. Because state budgets for SFY2018 have already been adopted, special legislative sessions and/or Governor action will likely be needed to address these shortfalls.
What are State Options to Respond to the Loss of Federal Funds?
State options to respond to the loss of federal CHIP funds vary based on how they have implemented their CHIP program. States have implemented their CHIP programs by creating a separate CHIP program, through a CHIP-funded Medicaid expansion, or using a combination of both approaches. Regardless of how states implement their program, they receive the enhanced (relative to Medicaid) matching rate for CHIP coverage, which was further increased by 23 percentage points under the Affordable Care Act (ACA). As of FY2016, about four in ten children covered through CHIP were in separate CHIP programs, and six in ten were in CHIP-funded Medicaid expansions.3
- States are not required to maintain separate CHIP coverage. States with separate CHIP programs can transition enrollees to Medicaid at the lower federal Medicaid match rate or discontinue coverage. Some states have state laws that require them to close the program and/or discontinue coverage if federal funds decrease. For example, Arizona must freeze enrollment if the federal match rate decreases, West Virginia must close the program if federal funding levels fall below the levels allotted in 1997, and Colorado cannot access provider taxes it uses to support coverage for some CHIP children without federal match.
- States are required to maintain CHIP-funded Medicaid expansion coverage under the ACA maintenance of effort (MOE) requirement. They will face increased costs since they will receive the lower federal Medicaid match rate for this coverage.
What are Current State Plans for Addressing the Loss of Federal Funds?
Many states with separate CHIP programs are planning to reduce coverage in response to the loss of federal funding, and several plan to begin notifying families before the end of the year. Overall, 14 of the 24 states that reported November 2017 data and have a separate CHIP program indicated plans to reduce or limit separate CHIP coverage for children or pregnant women, while most of the remaining 10 states reported they had not yet determined specific plans for reducing coverage.
- A total of 14 states reported plans to terminate or phase out coverage for children, including 5 states that plan to end coverage by the end of January 2018 (Figure 2).4 In addition, three states plan to take action in February (AL, OK, and WV), one state plans to take action in March (SD). The additional five states (MS, NC, ND, PA, and WY) plan to take action later or did not indicate a date for planned action. States will begin notifying families of the upcoming changes one month or more in advance of the planned action date. As of December 6, 2017, at least three states had begun informing families about potential changes. Colorado sent a warning to families about potential coverage losses5 and Utah6 and Oklahoma7 had posted notices on their websites warning of potential coverage reductions.

- Seven states reported plans to close new enrollment for children or establish a cap on the total number of children that can be enrolled in their separate CHIP program. Connecticut reported it will close enrollment or establish an enrollment cap on December 20th, 2017, and Alabama, North Carolina, and Virginia reported plans to close enrollment or establish an enrollment cap in January. Mississippi, Pennsylvania, and Utah also reported plans to take this action but did not specify planned dates of action.
- In addition, several states reported plans to reduce CHIP coverage for pregnant women. Colorado and Virginia both plan to terminate or phase out coverage for enrolled pregnant women on January 31, 2018. Virginia also plans to close new enrollment for pregnant women or establish an enrollment cap on January 1, 2018. Oklahoma has also indicated plans to terminate coverage for pregnant women covered through its unborn child option as of February 28, 2018.8
Several states indicated plans to transition children from separate CHIP programs to Medicaid. For example, Oregon, which anticipates exhausting its federal CHIP funds in December 2017, plans to transition children to Medicaid on January 1, 2018. In addition, Idaho and Louisiana indicated plans to transition children in February. States will face increased state costs for children transitioned from CHIP to Medicaid because they will receive the lower federal Medicaid match rate for this coverage.
States with CHIP-funded Medicaid expansion coverage must determine how they will fund the increased cost of covering these children at the lower federal Medicaid match rate. States can address these shortfalls by reducing costs in Medicaid, making reductions in other areas of the budget, or increasing revenues (Box 1). States will face challenges replacing federal dollars since many were already facing shortfalls heading into SFY 2018.9
Box 1: Examples State Plans to Cover Increased Costs for CHIP-funded Medicaid Expansion Coverage
Alaska reported that it will request supplemental funding from the state general fund to address its estimated $7 million shortfall for SFY 2018.
Utah reported that it will end its separate CHIP coverage and that it requested approximately $11.3 million in additional funding from the state legislature to cover increased costs of its CHIP-funded Medicaid expansion coverage.
Hawaii reported that it would make reductions in other areas of the budget (outside of Medicaid/CHIP) and request an emergency appropriation for SFY 2018 to address its estimated $9.3 million shortfall.
How Will Coverage Reductions and Changes Affect Families and States?
Reductions in CHIP coverage will result in coverage losses for children and negative effects on children’s health and family finances. If states close enrollment and/or discontinue coverage for children in separate CHIP programs, some children could shift to their parents’ employer-sponsored plans or Marketplace plans, but others would become uninsured. Previously, some states closed enrollment in CHIP for limited periods in response to state budget pressures, and studies show that this led to coverage losses, left eligible individuals without access to coverage, and had negative effects on health and family finances (Appendix 2).
Implementing program changes to CHIP will also require administrative time and costs for states. States reported having to take an array of actions to implement program changes (Box 2). States need to build in time to conduct these actions as they plan to make program changes. In addition, states face administrative costs associated with these actions. For example, Connecticut estimates that implementing program changes will cost $250,000, Oklahoma estimates costs of $1.1 million, Pennsylvania estimates costs of $3.4 million, and South Dakota estimates costs of $200,000.10 Colorado previously estimated that eligibility system changes alone would cost $300,000.11 CMS indicated that states must factor such costs associated with the close out of the program into calculations of use of remaining federal funds.12
Box 2: Administrative Actions to Implement Program Changes
- Notifying families
- Translating notices
- Submitting state plan amendments to CMS
- Conducting tribal consultation
- Making changes to eligibility systems and other systems
- Training eligibility staff
- Redetermining eligibility for other programs
- Notifying providers, managed care organizations (MCOs), and other stakeholders
- Updating contracts with MCOs, vendors, and other third parties.
What Actions Remain for Congress to Extend Funding?
Multiple steps still remain for Congress to extend federal CHIP funding. As of early December 2017, the House had passed a bill to extend CHIP funding. In early October 2017, the Senate Finance Committee reported a bill out of committee to extend funding. However, the full Senate has not yet taken up action to extend funding. Final legislation still requires passage by the full Senate, resolution of any differences between the House and Senate bills, and signature by the President.
Further delay in Congressional action is likely to result in confusion among families that could lead to coverage losses and administrative costs even if Congress later extends funding. As states begin to notify families of changes in CHIP coverage, there is the potential for confusion among families that could lead to coverage losses, even if Congress later extends funding. Moreover, states are already beginning to take action to implement program changes, resulting in administrative time and costs. States will face additional administrative burdens and costs associated with reversing these changes and restarting coverage, if funding is extended.
| Appendix Table 1: State CHIP Budget Assumptions and Projected Dates of Exhaustion of Federal Funds | |||||
| State | Has separate CHIP coverage? | SFY 2018 budget assumes continued federal funding? | SFY 2018 budget assumes ACA enhanced match continues? | State estimate of when it will exhaust federal funding1 | State reported update to funding exhaustion date in November 2017? |
| Alabama | Yes | Yes | Yes | February 2018 | Yes |
| Alaska | Yes | No | March 2018 | Yes | |
| Arizona | Yes | Yes | Yes | December 2017 | Yes |
| Arkansas | Yes | Yes | Yes | June 2018 | |
| California | 2 | Yes | No | January 2018 | Yes |
| Colorado | Yes | Yes | Yes | January 2018 | Yes |
| Connecticut | Yes | Yes | Yes | February 2018 | Yes |
| Delaware | Yes | Yes | Yes | January 2018 | Yes |
| DC | Yes | NR | 1st Q 2018 | Yes | |
| Florida | Yes | Yes | Yes | January 2018 | Yes |
| Georgia | Yes | Yes | NR | January to March 20183 | |
| Hawaii | Yes | Yes | February 2018 | Yes | |
| Idaho | Yes | Yes | Yes | January 2018 | Yes |
| Illinois | Yes | Yes | No | NR | |
| Indiana | Yes | Yes | NR | Summer 2018 | |
| Iowa | Yes | Yes | Yes | March 2018 | Yes |
| Kansas | Yes | NR | NR | NR | |
| Kentucky | Yes | Yes | Yes | February 2018 | |
| Louisiana | Yes | Yes | Yes | February 2018 | Yes |
| Maine | Yes | Yes | NR | NR | |
| Maryland | Yes | Yes | April 2018 | Yes | |
| Massachusetts | Yes | Yes | Yes | January 2018 | Yes |
| Michigan | Yes | Yes | February/March 2018 | ||
| Minnesota | Yes | NR | November 2017 | Yes | |
| Mississippi | Yes | Yes | Yes | April 2018 | Yes |
| Missouri | Yes | Yes | No | Spring/Summer 2018 | Yes |
| Montana | Yes | Yes | Yes | February 2018 | Yes |
| Nebraska | Yes | No | 2nd Q 2018 | ||
| Nevada | Yes | Yes | NR | October/November 2017 | |
| New Hampshire | No | N/A | December 2017 | Yes | |
| New Jersey | Yes | Yes | Yes | March 2018 | Yes |
| New Mexico | Yes | NR | July 2018 | Yes | |
| New York | Yes | Yes | Yes | March 20184 | |
| North Carolina | Yes | Yes | Yes | 1st Q 2018 | Yes |
| North Dakota | Yes | Yes | Yes | May 2018 | Yes |
| Ohio | Yes | NR | February 2018 | Yes | |
| Oklahoma | Yes5 | No | N/A | March 2018 | Yes |
| Oregon | Yes | Yes | Yes | December 2017 | Yes |
| Pennsylvania | Yes | Yes | Yes | January 2018 | Yes |
| Rhode Island | Yes | Yes | March 2018 | Yes | |
| South Carolina | Yes | Yes | SFY 2019 | ||
| South Dakota | Yes | Yes | Yes | March 2018 | Yes |
| Tennessee | Yes | Yes | Yes | Late spring | Yes |
| Texas | Yes | Yes | Yes | January 2018 | Yes |
| Utah | Yes | Yes | Yes | January 2018 | Yes |
| Vermont | Yes | No | 1st Q 2018 | ||
| Virginia | Yes | Yes | Yes | January 2018 | Yes |
| Washington | Yes | Yes | Yes | September 2017 | Yes |
| West Virginia | Yes | Yes | Yes | February 2018 | Yes |
| Wisconsin | Yes | Yes | Yes | March 2018 | Yes |
| Wyoming | Yes | Yes | Yes | April 2018 | Yes |
| NOTES: NR: Not reported. N/A: Not applicable; state budget does not assume continuation of CHIP funding. 1State projections vary with regard to whether they include redistribution funds; for some states, redistribution funds could temporarily extend funding beyond the projected exhaustion date. 2 Some counties in California provide separate CHIP coverage. 3Georgia reported Feb/March 2018 if they suspend eligibility, Jan 2018 if eligibility not suspended. 4New York reported “into CY 2018” in Summer 2017 and did not provide an updated estimate; March 2018 estimate is based on MACPAC projection. 5 Oklahoma has a separate CHIP program that provides premium assistance to some children and coverage for pregnant women through the unborn child option.SOURCES: Kaiser Family Foundation Survey of Medicaid Officials in 50 States and DC conducted by Health Management Associates, Summer 2017 with November 2017 updates. List of states with separate CHIP coverage is from a national survey conducted by the Kaiser Family Foundation with Georgetown University Center for Children and Families, January 2017, http://www.kff.org/medicaid/report/medicaid-and-chip-eligibility-enrollment-renewal-and-cost-sharing-policies-as-of-january-2017-findings-from-a-50-state-survey/. | |||||
Appendix 2: Effects of Previous State Enrollment Caps and Freezes
After Arizona froze CHIP enrollment in December 2009, enrollment fell by more than 60% from about 46,900 to 17,600 as of July 2011 (Figure 2).13 Just over four in ten disenrolled children moved to Medicaid due to declines in family income, but many others likely became uninsured.14 The children’s uninsured rate in Arizona grew following the enrollment freeze.15 Over the same period, the waiting list for CHIP grew to over 100,000 children and was continuing to grow at a rate of about 10,000 children per month.16

In North Carolina, enrollment fell by nearly 30% from about 72,000 to 51,300 when it froze enrollment between January and October 2001. The number of children determined eligible for CHIP but placed on a waiting list grew to over 34,000.17 Most (60%) children added to the waiting list were previously enrolled in Medicaid and were unable to transition to CHIP.
Enrollment freezes negatively affected children’s health and family finances. In North Carolina, parents with children affected by the enrollment freeze said their children experienced periods of being uninsured and that almost all needed care during the time that they lacked coverage.18 Parents often had to delay care while their children were uninsured and reported difficulties obtaining prescription medications for their children.19 Parents also reported that obtaining care while their children were uninsured resulted in significant financial hardships, requiring them to cut back on necessities, borrow money from family or friends, and accrue debt for missed payments on bills.20
- Brian Neale, “Programmatic and Financial Information Regarding CHIP in a Federal Funding Shortfall” (Center for Medicare and CHIP Services, November 2017), https://www.medicaid.gov/federal-policy-guidance/downloads/cib110917.pdf. ↩︎
- The District of Columbia is counted as a state for the purposes of this report. ↩︎
- Medicaid and CHIP Payment and Access Commission, Child Enrollment in CHIP and Medicaid by State, (December 2016), https://www.macpac.gov/publication/child-enrollment-in-chip-and-medicaid-by-state/. ↩︎
- Utah Department of Health, “Children’s Health Insurance Program,” accessed on December 6, 2017, http://health.utah.gov/chip/ ↩︎
- Colorado Department of Health Care Policy and Financing, “Families to Begin Receiving Letters on Future of CHP+” November 27, 2017, https://www.colorado.gov/hcpf/news/families-begin-receiving-letters-future-chp ↩︎
- Utah Department of Health, “Children’s Health Insurance Program,” accessed on December 6, 2017, http://health.utah.gov/chip/ ↩︎
- Oklahoma HealthCare Authority, “Children’s Health Insurance Program (CHIP) Updates,” last updated November 29, 2017, http://www.okhca.org/about.aspx?id=21203 ↩︎
- Ibid. ↩︎
- Larisa Antonisse, Elizabeth Hinton, Robin Rudowitz, Kathleen Gifford, and Nicole McMahon, Governors’ Proposed Budgets for SFY 2018: Focus on Medicaid and Other Health Priorities (Washington, DC: Kaiser Family Foundation, April 2017), http://modern.kff.org/report-section/governors-proposed-budgets-for-fy-2018-focus-on-medicaid-and-other-health-priorities-issue-brief/ ↩︎
- Cost estimate for Oklahoma is combined federal and state costs. Other states did not specify whether the estimates they provided are for state costs alone or federal and state costs combined. ↩︎
- Colorado’s projected cost for eligibility system changes is from the state’s response to the Summer 2017 Medicaid budget survey. ↩︎
- Centers for Medicare and Medicaid Services, “Contingency Planning for a Title XXI Shortfall,” Children’s Coverage TAG, July 25, 2017. ↩︎
- Kaiser Commission on Medicaid and the Uninsured, The Arizona KidsCare CHIP Enrollment Freeze: How Has it Impacted Enrollment and Familes? (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, September 2011), http://modern.kff.org/medicaid/issue-brief/the-arizona-kidscare-chip-enrollment-freeze-how/ ↩︎
- Ibid. ↩︎
- Elisabeth Wright Burak, Children’s Health Coverage in Arizona: A Cautionary Tale for the Future of the Children’s Health Insurance Program (CHIP) (Washington, DC: Georgetown Center for Children and Families, January 2015), http://ccf.georgetown.edu/wp-content/uploads/2015/01/Childrens-Coverage-in-Arizona-A-Cautionary-Tale-for-the-Future-of-Childrens-Health-Insurance-Program.pdf ↩︎
- Kaiser Commission on Medicaid and the Uninsured, The Arizona KidsCare CHIP Enrollment Freeze: How Has it Impacted Enrollment and Familes? (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, September 2011), http://modern.kff.org/medicaid/issue-brief/the-arizona-kidscare-chip-enrollment-freeze-how/ ↩︎
- Ian Hill, Brigette Courtot, and Jennifer Sullivan, “Coping With SCHIP Enrollment Caps: Lessons From Seven States’ Experiences” Health Affairs 26 no.1 (January/February 2007): 258-268, http://content.healthaffairs.org/content/26/1/258.full.pdf ↩︎
- Pam Silberman, Joan Walsh, Rebecca Slifkin, and Stephanie Poley, The North Carolina Health Choice Enrollment Freeze of 2001 (Washington, DC: Kaiser Commission on Medicaid and the Uninsured, January 2003), https://modern.kff.org/wp-content/uploads/2002/12/4081-north-carolina-health-choice.pdf ↩︎
- Ibid. ↩︎
- Ibid. ↩︎