ACA Preventive Services Are Back at the Supreme Court: Kennedy v. Braidwood
On June 27,2025, the U.S. Supreme Court issued the opinion for Kennedy v. Braidwood Management, finding that the ACA requirement that most private insurers and Medicaid expansion programs cover preventive services recommended by the United States Preventive Services Preventive Task Force (USPSTF) with no cost-sharing is constitutional. In its decision, the Court affirmed that USPSTF members are appointed constitutionally, and the Secretary of Health and Human Services can remove USPSTF members at-will and directly review and block Task Force recommendations before they take effect.
In this case, the Supreme Court narrowly considered whether the structure of USPSTF violates the Appointments Clause, but did not review the litigants’ other claims about the Advisory Committee on Immunization Practices (ACIP), and the Health Resources and Services Administration (HRSA). The federal district court will now resume briefing on the consideration of the plaintiffs’ claim that the Secretary of Health and Human Services’ ratification of HRSA and ACIP recommendations violates the Administrative Procedure Act. For more analysis of the Court’s decision please see Kennedy v. Braidwood: The Supreme Court Upheld ACA Preventive Services but That’s Not the End of the Story.
On April 21, 2025, the Supreme Court is hearing oral arguments in Kennedy v. Braidwood Management. In this case, Braidwood Management, Christian owned businesses and six individuals in Texas, have challenged the Affordable Care Act’s (ACA) requirement to cover preventive services. The Supreme Court is narrowly considering whether the structure of the US Preventive Services Task Force (USPSTF) — an independent entity convened by the federal government that makes recommendations for preventive services that nearly all private insurances must cover without cost-sharing — violates the U.S. Constitution’s Appointments Clause. That provision states that “officers of the United States” may only be appointed by the president, subject to the advice and consent of the Senate and the litigants are claiming that the USPSTF does not have the authority to set coverage requirements. The Supreme Court is not considering the litigants’ other claims including those that the recommendations violate the Religious Freedom Restoration Act (RFRA), or their Appointment’s Clause claims about the Advisory Committee on Immunization Practices (ACIP), or the Health Resources and Services Administration (HRSA).
Even though President Trump had supported ACA repeal in his first term, his administration is defending the lawsuit. On its face this may seem unexpected, but the outcome of the case could give the administration broader latitude to shape the recommendations issued by the entities that were originally established with the goal of providing independent analysis and review. This brief provides an overview of the most recent ACA case under review at the Supreme Court and discusses the implications of the potential rulings by the high court.
The ACA and Preventive Services
Section 2713 of the ACA requires most private health insurance plans and Medicaid expansion programs to cover a range of recommended preventive services without any patient cost-sharing. Preventive services include a range of services such as screening tests, immunizations, behavioral counseling, and medications that can prevent the development or worsening of diseases and health conditions. Preventive services that must be covered are those receiving an A or B grade by the U.S. Preventive Services Task Force (USPSTF), vaccines recommended by the Advisory Committee on Immunization Practices (ACIP), and the Health Resources and Services Administration (HRSA) recommendations issued by the Women’s Preventive Services Initiative and the Bright Futures for Children program. All of these entities review new recommendations and conduct periodic updates of existing recommendations.
What Is the Case?
In the original case, filed in 2022, the respondents claimed that the preventive services requirements for private health insurance are unconstitutional and also that the requirement to cover pre-exposure prophylaxis treatment (PrEP) (medication to prevent getting HIV from sex or injection drug use for those at risk) violates the Religious Freedom Restoration Act (RFRA). The respondents are six individuals and Christian-owned businesses. Braidwood Management, a for-profit closely held organization, owned by a trust, with Dr. Steven F. Hotze, as the sole trustee and beneficiary. Braidwood is self-insured and provides health insurance to its 70 employees. The other respondent is Kelley Orthodontics, who identify themselves as a “Christian professional association” owned by respondent, John Kelley. The respondents assert both economic harm for having to pay more money for a health plan that includes services they do not want or need, and religious harm for having to include services they object to.
In 2022, the District Court, agreeing with Braidwood’s arguments, ruled that the appointment of members to USPSTF violated the Appointments Clause and that the requirement to cover PrEP violates RFRA. However, the Court also found that the ACA’s delegation to ACIP and HRSA is not in violation of the Appointments Clause since the Secretary of HHS effectively has the authority to ratify or not the ACIP and HRSA recommendations. In 2023, the District Court issued a ruling striking down the ACA’s requirement for no cost coverage of preventive services recommended or updated by USPSTF on or after March 23, 2010. This ruling, however, was subsequently paused as the case made its way through the appeals process
In June 2024, the 5th Circuit Court of Appeals affirmed the district court’s ruling that the ACA’s requirement to cover without cost-sharing services recommended by United States Preventive Services Task Force (USPSTF) is unconstitutional. However, they ruled that a nationwide remedy was not proper and that only the plaintiffs are permitted to exclude USPSTF recommended services from their plans. The Appeals Court sent back to the district court the plaintiffs’ claim that the Secretary of Health and Human Services’ ratification of HRSA and ACIP recommendations violates the Administrative Procedure Act for further briefing and a judgment. The Supreme Court is considering only the arguments regarding whether the structure of USPSTF violates the Appointment’s Clause, not the other bodies that make preventive services recommendations, nor the religious harm included in the original case. However, a separate set of claims regarding HRSA and ACIP are still being considered by the district court and could be before the Supreme Court at a future date.
What Is the Supreme Court Considering?
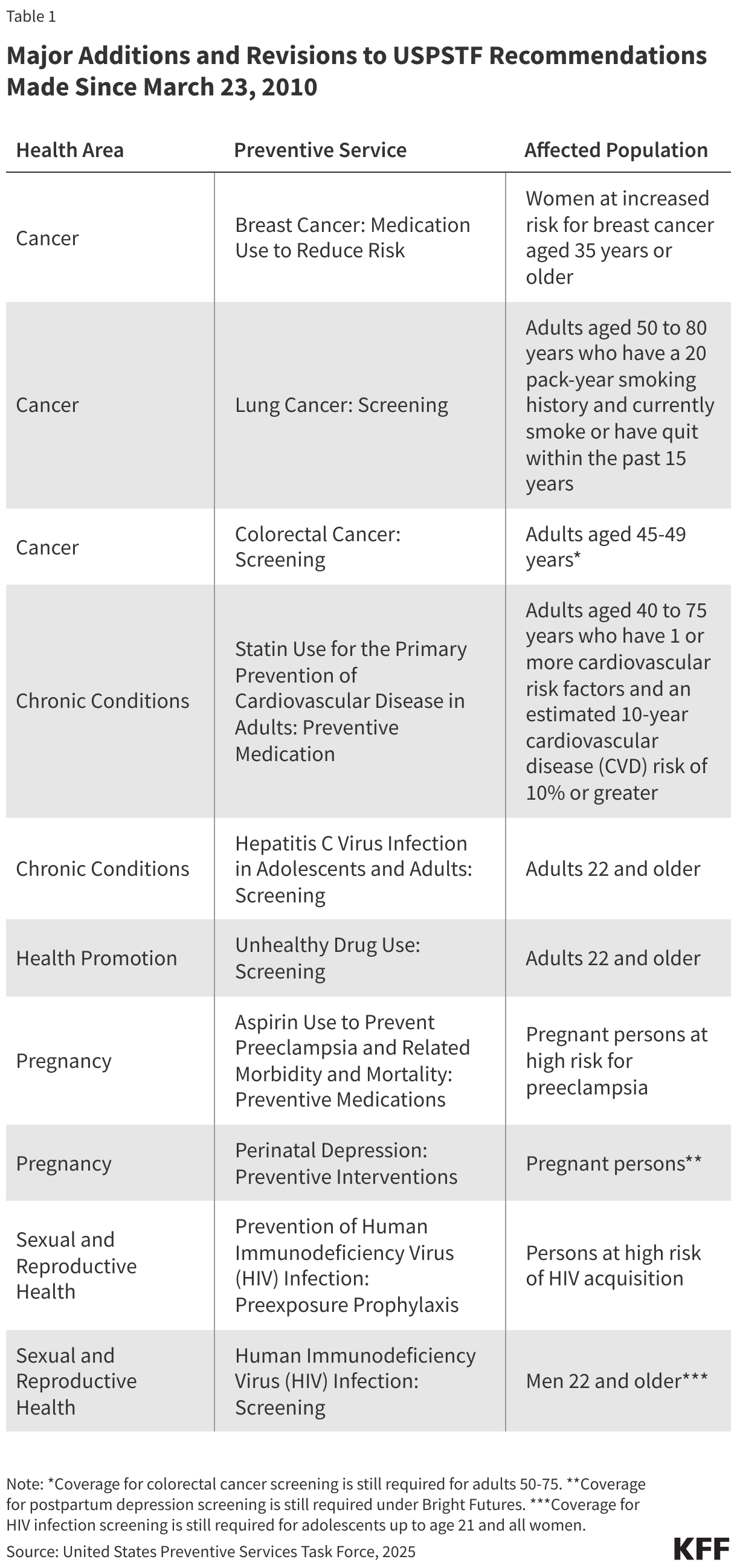
The current case before the Supreme Court is reviewing the 5th Circuit Court of Appeals decision holding that appointments of individuals to the USPSTF and the recommendations made by the USPSTF after the enactment of the Affordable Care Act in 2010 (see Table 1) violate the Appointments Clause of the U.S. Constitution since they were not appointed by the President and confirmed by the Senate.
Braidwood et al. contend that the requirement for health plans to cover preventive services recommended or amended by USPSTF since the enactment of the ACA in March 2010 violates the Appointments Clause of the Constitution. They argue this is unconstitutional since the ACA does not allow the Secretary of HHS to reject the recommendations made by the Task Force or require it to make specific recommendations, meaning that USPSTF members have the capacity to unilaterally determine the preventive care that private insurers must cover and act as officers of the United States. Additionally, they contend the Secretary lacks the authority to remove USPSTF members at will. They argue that for USPSTF’s structure and recommendations to be constitutional, members would have to be appointed by the president and Senate.
The federal government argues that the HHS Secretary has constitutionally appropriate oversight over USPSTF because they may remove members at will and determine when health insurance issuers must start providing coverage for new recommendations. HHS additionally argues that if the Court holds that capacity to remove members at will is not sufficient oversight, it can remedy this by construing federal law to allow the Secretary to review USPSTF recommendations directly, which would address any remaining questions of oversight. This degree of supervision by the Secretary of HHS, the agency argues, would mean that members of the Task Force are “inferior officers,” who may be appointed or removed by the Secretary and would not require appointment by the president and Senate.
Potential Impact on Coverage
If the Court rules in favor of Braidwood, private health insurers would no longer be required to cover, without cost sharing, preventive services recommended by USPSTF after 2010 when the ACA was enacted. Any new service that was recommended or updated by USPSTF after March 2010 (and is not also recommended by HRSA or ACIP) would no longer be required to be covered without out-of-pocket costs. For example, services and medications like statins to prevent heart disease, lung cancer screening, and PrEP to prevent HIV could be subject to copays, deductibles, or coinsurance, potentially deterring access to these services. This essentially means that the standards and recommendations that the federal government would be able to enforce would not reflect current or future standards and evidence, locking required preventive services in place as of the state of the science in 2010.
Although many of the friend of the court briefs presented to the Supreme Court for this case focus on the impact of coverage of USPSTF recommendations with no cost-sharing, a ruling in favor of the federal government does not guarantee that coverage will be required for these preventive services. As the federal government argues, HHS Secretary Robert F. Kennedy Jr. has the power to remove USPSTF members at will and to review the recommendations they issue. This means that the Trump administration could change the membership of the USPSTF in ways that may significantly alter the recommendations it issues. Additionally, in their briefs, the Trump Administration’s HHS contends the Secretary can direct that the implementation of recommendations issued by USPSTF can be delayed indefinitely and that the Secretary may have additional authority to supervise and veto Task Force recommendations. In their brief they state, “In addition to removing Task Force members at will, the Secretary may supervise and review their recommendations directly.”
The Supreme Court is expected to issue its ruling in June. Regardless of how the Court rules in this specific case, it will likely not be the final word on the ACA required coverage of preventive services recommended by USPSTF, ACIP and HRSA.