What is Medicaid Estate Recovery?
Issue Brief
Established to provide another source of Medicaid funding and promote program integrity, the recovery of certain Medicaid costs after an enrollee dies (estate recovery) has been criticized for several reasons, including that it falls primarily on individuals with limited incomes, raises little revenue, and is applied very unevenly across the states. Family members may be unaware of the policy at the time of enrollment and only learn that the family home may be repossessed after the death of a loved one. Such criticisms have led to proposals (Box 1) that would modify or reduce the practice of estate recovery by Democrats, Republicans, and the Medicaid and CHIP Payment and Access Commission (MACPAC).
Estate recovery is a process that primarily affects older Medicaid enrollees who use long-term services and supports (LTSS). To be eligible for Medicaid coverage of LTSS, people must usually demonstrate having limited incomes (typically below $3,000 per month in 2024 for an individual) and financial resources (often below $2,000 for an individual), but some assets, including their home, are excluded from the calculation of financial resources. Many people only qualify after spending their assets on the out-of-pocket costs for LTSS, which may easily exceed $100,000 per year. The 1993 Omnibus Budget Reconciliation Act required state Medicaid programs to recover the costs of certain Medicaid benefits through a process called estate recovery. Specifically, states are required to recover the costs of LTSS and related hospital and prescription drug services for Medicaid enrollees ages 55 and older; and have the option to recover the costs for other services and populations. States may not take the family home if it is occupied by a spouse, child under the age of 21, child who is blind or has a disability, or a sibling with an equity interest in the home, but they may place a lien on real property for individuals who are alive but permanently institutionalized.
This issue brief sheds light on states’ policies towards estate recovery, drawing from KFF’s Survey of Medicaid Financial Eligibility & Enrollment Policies for Seniors & People with Disabilities which was conducted in March 2024 by KFF and Watts Health Policy Consulting. Overall, 49 states and the District of Columbia (hereafter referred to as a state) responded to the survey, though response rates to specific questions varied (Florida was the only state that did not respond).
Key takeaways include:
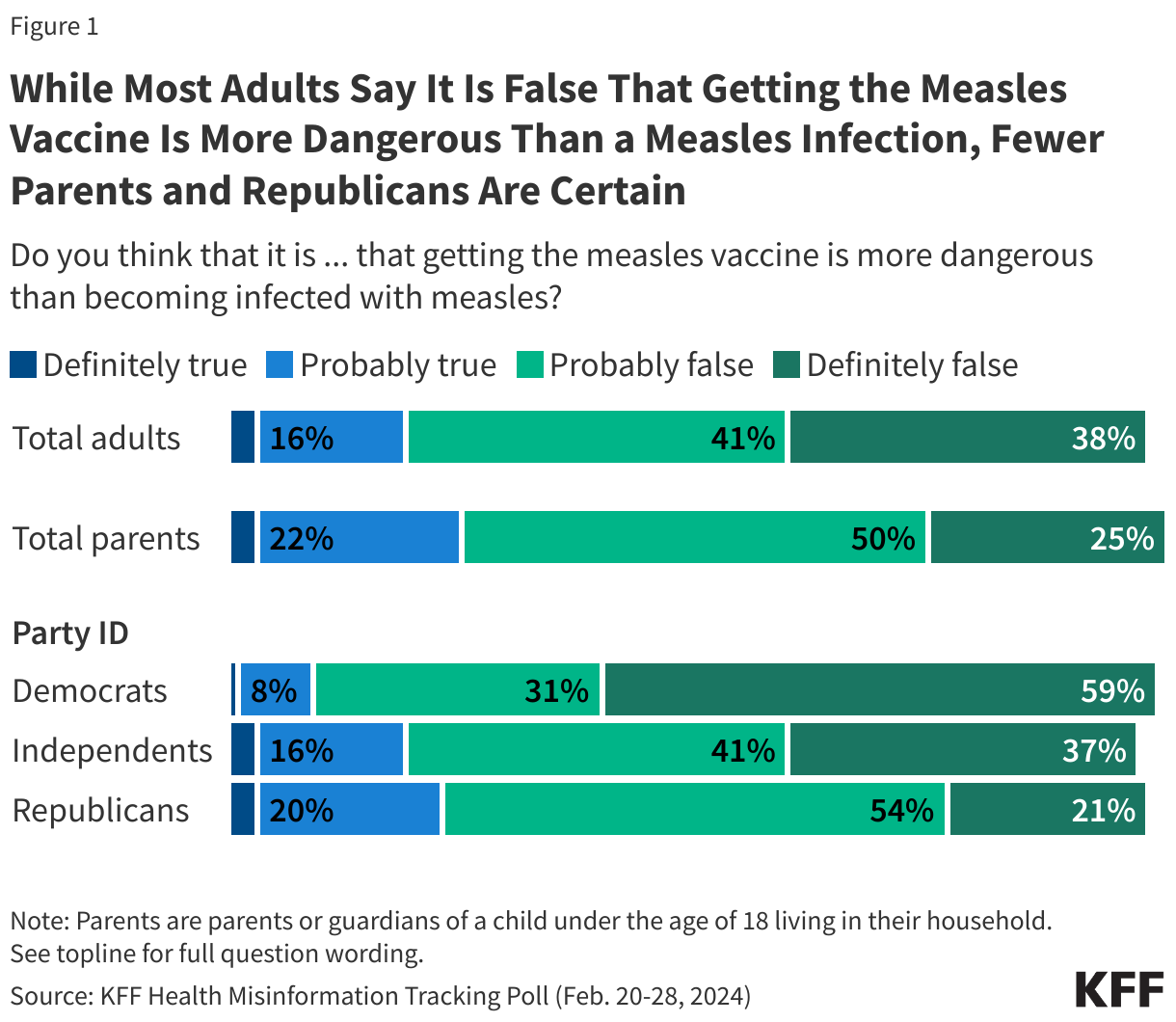
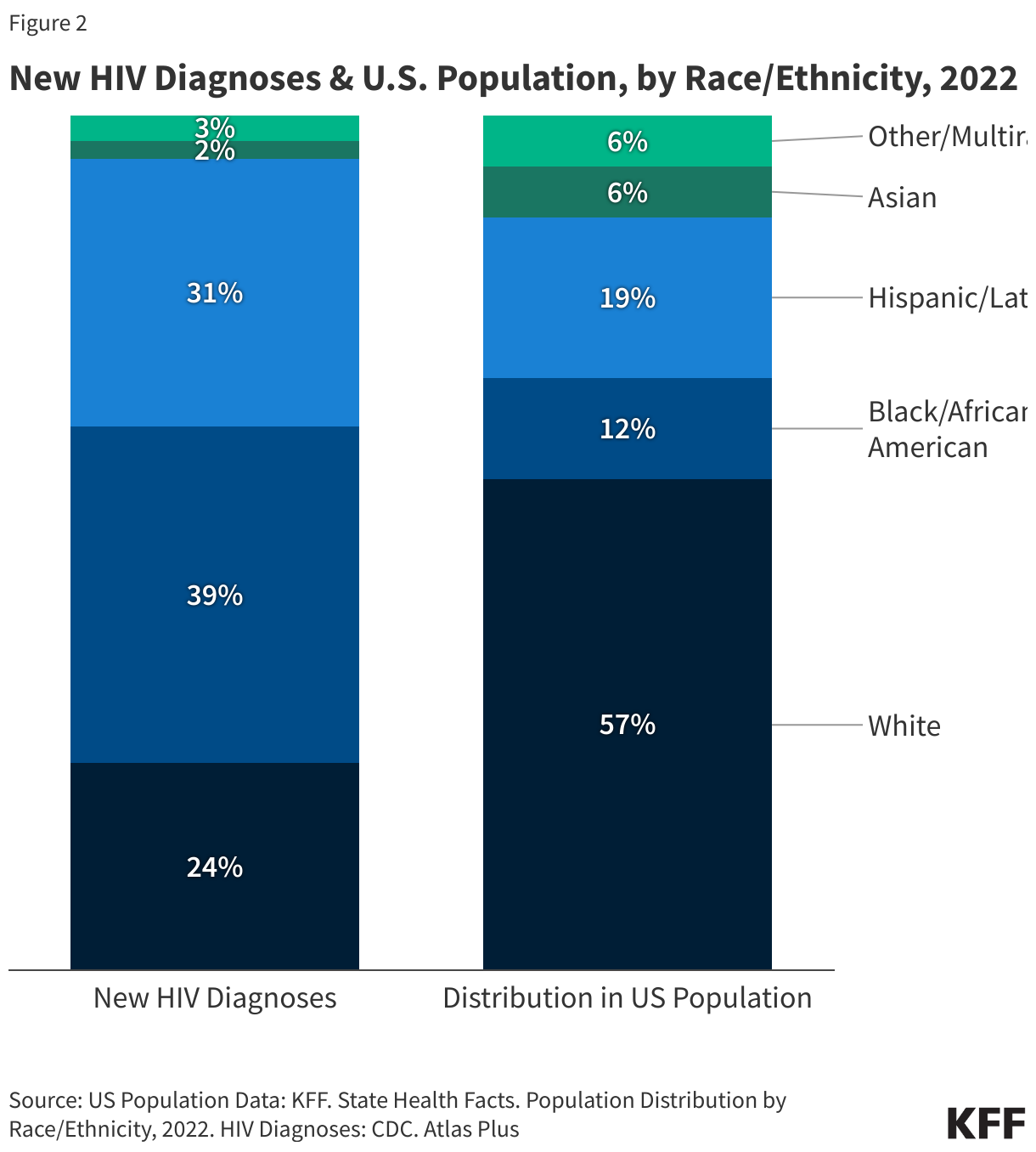
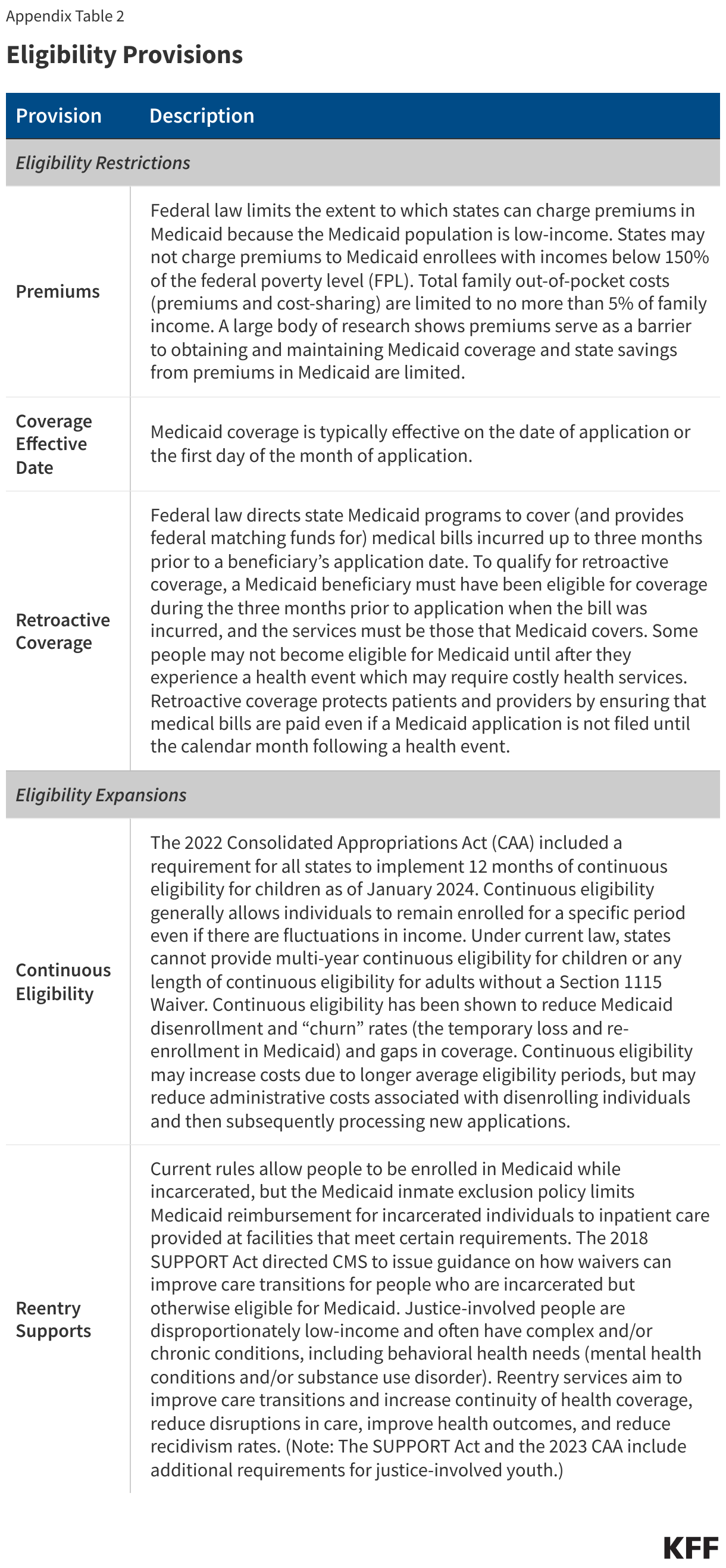
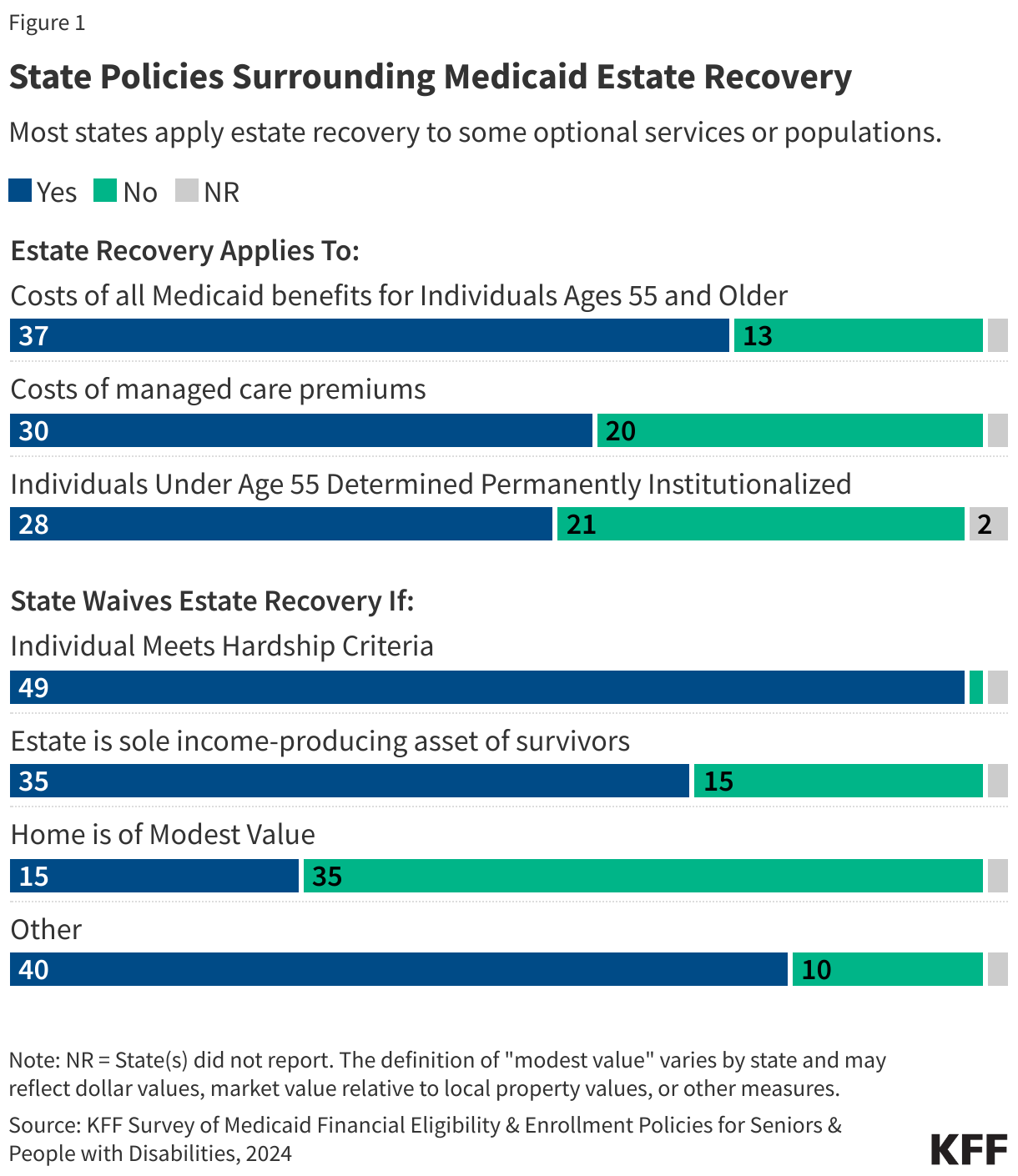
- Over half of states reported using estate recovery for the costs of populations and services for which federal law does not require estate recovery, with 28 states reporting estate recovery for some individuals under age 55 and 32 states reporting estate recovery for the costs of all Medicaid benefits for individuals ages 55 and older, and an additional 5 states reporting estate recovery for some optional benefits (Figure 1).
- Over half of states (30) reported using estate recovery to recoup the costs of premiums paid to managed care organizations on behalf of Medicaid enrollees.
- Federal law requires states to establish procedures for waiving estate recovery when recovery would cause hardships, but there are no specific procedures required. States reported waiving estate recovery under the following conditions: when the individual meets state-defined hardship requirements (49 states), if the estate is the sole income-producing asset of survivors (35 states), and when the home is of modest value (15 states). (The definition of “modest value” varies by state and may reflect dollar values, market value relative to local property values, or other measures.)
Why was estate recovery established and why is it a source of concern for policymakers?
Estate recovery was established as a tool to promote program integrity and ensure that people contribute to the costs of their health care. People must generally have very limited income and assets to qualify for Medicaid, but the value of the home is not counted towards the initial eligibility determination. Most eligibility pathways for people who use LTSS require people to have incomes under $3,000 each month and only $2,000 of savings for an individual or $3,000 for a couple. Despite stringent financial eligibility levels, some people with moderate incomes during their working years may become eligible for Medicaid during their retirement years if they need LTSS. Most Medicare beneficiaries live on fixed incomes, with half living on incomes below $36,000 per year and half having savings below $103,800 in 2023. The high costs of LTSS, easily exceeding $100,000 per year, may cause people to qualify for Medicaid after exhausting their savings even if they live in a home of some value. Proponents of estate recovery have indicated that it ensures Medicaid funding is used for the most needy, prevents people from relying on Medicaid instead of using their personal resources to pay for LTSS, and allows states to spend more on other Medicaid expenses. States are also required to establish a cost-effectiveness threshold, which determines whether the value of the estate is cost effective relative to the administrative costs of recovery; and is intended to preclude states from pursuing small estates.
Estate recovery is a source of concern to some policymakers because it disproportionately affects low-income families, creates high administrative costs relative to the revenue generated, and may deter eligible people from applying for Medicaid. A 2021 report to Congress by MACPAC summarizes those concerns, which include:
- Medicaid enrollees are generally low-income and estate recovery may perpetuate intergenerational poverty.
- Individuals with greater awareness of estate recovery and resources are often able to leverage legal mechanisms allowing them to bypass Medicaid estate recovery but preserve Medicaid eligibility. Individuals with fewer resources or only a family home often don’t have the income to hire an attorney to help implement such strategies.
- Estate recovery results in administrative costs to states that could exceed the value of the collections.
- Estate recovery raises relatively few revenues: $733 million in 2019, which offset 0.1% of the over $600 billion that Medicaid spent in 2019. Even in states with the highest relative recovery revenues, those revenues offset less than 1.0% of the states’ Medicaid spending.
- Estate recovery may deter some people from applying to Medicaid who are eligible even if they would not be subject to estate recovery. For example, Medicare beneficiaries who are only eligible for Medicaid coverage of Medicare premiums and cost sharing would not be subject to estate recovery, but limited understanding of the program may prevent them from applying.
States’ use of estate recovery varies considerably, with a small number of states accounting for most of the collections. Five states (Massachusetts, New York, Pennsylvania, Ohio, and Wisconsin) with the largest estate recoveries accounted for nearly 40% of all collections in FY 2019, the most recent year for which data are publicly available about all states’ collections. The same report showed survey data for 10 states, with those states reporting varying numbers of estates pursued, estates recovered, and the amounts recovered per state. Alaska pursued the fewest estates of the responding states (under 500 per year). At the other end of the spectrum were Iowa (pursuing over 15,000 estates each year) and New York (pursuing around 30,000 per year). The average amount recovered per estate ranged from around $5,000 or less in Missouri and Wisconsin to $30,000 per year or more in Alaska and Georgia.
Box 1: What are the current policy proposals to eliminate or reduce states’ use of estate recovery?
Democrats, Republicans, and the Medicaid and CHIP Payment and Access Commission (MACPAC) have all proposed changes to the estate recovery program. Such proposals include the following:
H.R. 7573 – Stop Unfair Medicaid Recoveries Act: H.R. 7573 would eliminate estate recovery programs entirely.
H.R. 8094 – To amend title XIX of the Social Security Act to modify certain asset recovery rules: H.R. 8094 would prohibit states from conducting estate recovery in cases where the family home is transferred to another person who is eligible for Medicaid or has income below 138% of the federal poverty level.
MACPAC – Medicaid Estate Recovery: Improving Policy and Promoting Equity: MACPAC recommended three legislative changes to Title XIX of the Social Security Act. Those changes include making estate recovery optional for states, allowing states that provide long-term services and supports (LTSS) through managed care plans to recover the costs of services used rather than the costs of the premiums the state paid, and directing the Department of Health and Human Services to establish minimum standards for hardship waivers. Minimum standards for hardship waivers would prevent states from pursuing recovery for assets that are the sole income-producing asset of survivors, homes of modest value, and estates valued under a certain threshold.
When does Medicaid estate recovery apply?
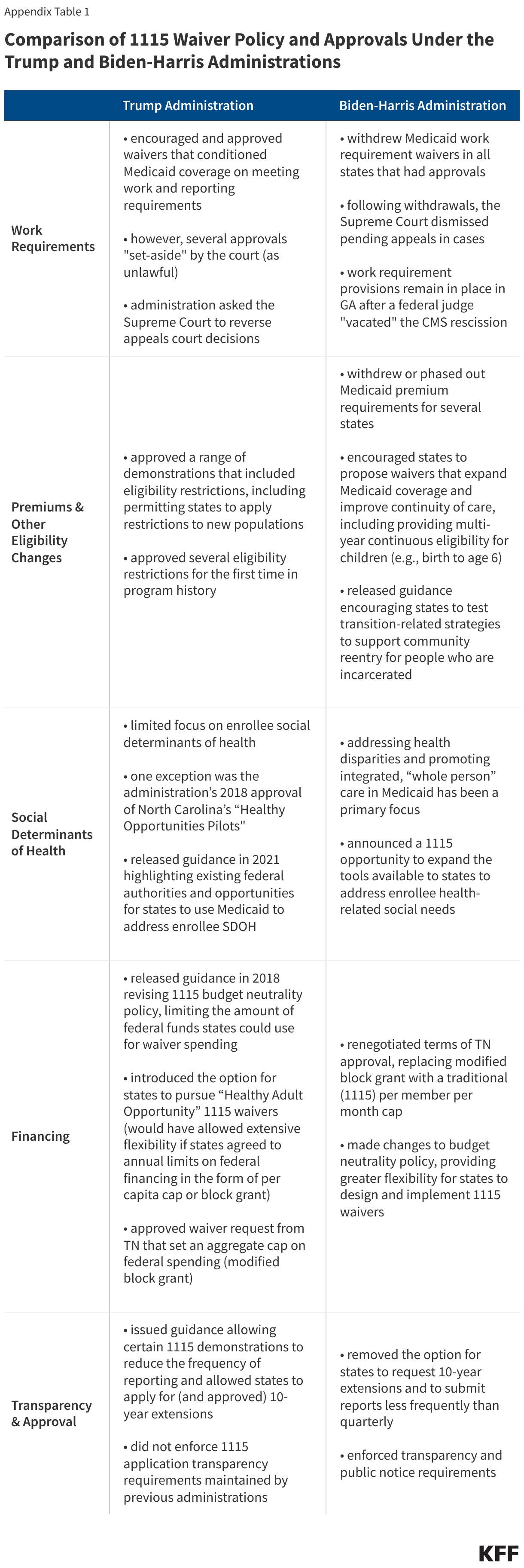
States must conduct estate recovery for some services and enrollees but may choose to apply estate recovery in additional circumstances, which contributes to the variation in how many estates are pursued and the amount states are recovering. Estate recovery is required for enrollees ages 55 and older who use LTSS, including enrollees eligible for Medicaid through the Affordable Care Act’s Medicaid expansion. For people ages 55 and older who use LTSS, states must recover the costs of nursing facility services, home- and community-based services (HCBS), and related hospital and prescription drug services (defined as those services provided during a nursing facility stay or while receiving HCBS). States may elect to recover the costs of all Medicaid-covered services. They may also elect to conduct estate recovery for individuals who are under the age of 55 if they have been determined to be permanently institutionalized.
Most states apply estate recovery beyond the federally-required circumstances: 37 states apply estate recovery to services for which it is optional and 28 determine permanent institutional status for individuals under age 55 (Appendix Table). For individuals under age 55, estate recovery most frequently applies to people in nursing facilities and in intermediate care facilities for individuals with intellectual disabilities. Among the states applying estate recovery for optional services, 5 states reported applying it to some optional services and 32 states reported applying it to all Medicaid-covered services, but several states noted that recovery could only occur if LTSS services were also rendered.
For people enrolled in managed care, estate recovery is based on the premium payments states make rather than on the services people use, which means some people are subject to estate recovery despite not using applicable services. When states provide benefits through managed care, states are required to seek recovery for the premiums paid if the enrollee would have been subject to estate recovery under a fee-for-service system. If the state recovers the costs of all Medicaid services, estate recovery must apply to the full Medicaid premium. If the state only recovers the costs of a subset of benefits, estate recovery must apply to the portion of the premium attributable to those benefits.
Over half of states apply estate recovery to the costs of managed care premiums. Among the 27 states with capitated managed care that includes LTSS, 11 states pursue estate recovery for the entire premium for people who use LTSS, and 10 states recover the entire premium for everyone enrolled in the plan. Fewer states (5) pursue only the premium attributable to LTSS used. Pennsylvania reported a unique approach, taking the smaller of the premium or the amount of claim spending on LTSS and related services each month. There is no recovery for months without LTSS spending. Among states with stand-alone LTSS managed care plans, 8 states recover the entire premium but only for people who use LTSS and 5 states recover the entire premium for everyone enrolled in the plan. Indiana’s managed LTSS program began in July 2024 and the state will pursue recovery for the entire capitation and any other amounts paid.
When do states waive estate recovery requirements?
Federal law requires states to waive estate recovery requirements when they impose “undue hardships,” but does not specify what constitutes a hardship, leading to significant variation in when states waive estate recovery. Guidance from the Centers for Medicare and Medicaid Services (CMS) provides three examples of potential hardships which include:
- Estate is sole income-producing asset of survivors such as a family farm;
- Home is of modest value, defined as roughly half the average home value in the county; or
- Other compelling circumstances.
The variable approach to hardship waivers has raised equity concerns because the ease with which they are granted varies across states. In some states, securing a hardship waiver may require an attorney, and the families with the fewest resources are least likely to be able to afford such services. In the 10 states included in MACPAC’s survey, the percentage of hardship applications granted in 2019 ranged from 29% in New York to 95% in Iowa.
In KFF’s survey, nearly all states (49) reported adopting at least one of the three potential hardship exemptions in CMS guidance, with the most common being to waiver the estate if it was the sole income-producing asset of survivors (Appendix Table). Specifically, 35 states reported using the income-producing asset criteria, although Arizona also required that the heir must own a business located on real property that is part of the estate and Georgia limits the hardship to farms with annual income of $25,000 or less. Washington does not waive recovery, only delays, when hardship exists. Criteria for delaying recovery include estates that are the sole income-producing property of survivors, when recovery would deprive the heir of shelter and they cannot afford alternative shelter, and when the survivor is a state-registered domestic partner.
Only 15 states reported waiving estate recovery for homes of modest value but the definition of “modest” was unclear in many cases. Only four states reported dollar thresholds to define “modest,” including: West Virginia $50,000 or less; Texas less than $10,000; Mississippi and North Dakota, less than $5,000. Seven states (California, Louisiana, Michigan, New Mexico, New York, South Carolina, and Virginia) defined modest value as one whose market value is 50% or less than the average or median price of homes in a county. Other states used more varied approaches including the following.
- Two states (Arkansas and Maine) waive estate recovery when it is not cost effective but did not provide another definition for homes of modest value.
- In some cases, states reported exempting portions of the home for all descendants. For example, Louisiana exempts either the first $15,000 or half of the median value of a home within the parish from the homestead and South Carolina exempts 50% or less of the average home price within a county from the home’s value. Such exemptions would also preclude estate recovery for homes under those exemption levels.
- Hawaii and Vermont did not describe general definitions of modest value, but both have exemptions that reflect the value of the home in circumstances when heirs cared for the descendent prior to their death.
Most states (40) described other circumstances that would trigger a hardship exemption. Many of those circumstances related to federal policies such as exempting homes that were occupied by surviving minors and when the estate is the sole income-producing asset of a family business. The most common other exemptions included those for heirs who had provided care in the home for enrollees prior to their death and exemptions that considered the income and resources of the heir. Idaho, Ohio, and Wisconsin waive estate recovery when it would result in the survivor becoming eligible for Medicaid or other public assistance.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Appendix



 Irving Washington
Irving Washington  Hagere Yilma
Hagere Yilma