VOLUME 20
Fluoride Bans and Food Safety Doubts
Summary
This Monitor covers how fears about fluoride as a neurotoxin are impacting public health and how trust in food safety is eroding following the USDA’s disbandment of two food safety panels. It also discusses approaches to addressing false information and the accuracy of AI chatbots, like ChatGPT, in answering health questions compared to traditional search engines.
Recent Developments
CDC and EPA Will Re-Evaluate Water Fluoridation Recommendations as Communities Push to Ban Fluoride
Source: KFF Health News
On April 7, Health and Human Services (HHS) Secretary Robert Kennedy Jr., a fluoridation skeptic, announced that he is assembling a task force of health experts to study fluoride and will ask the Centers for Disease Control (CDC) to change its water fluoridation recommendation. At the same time, the Environmental Protection Agency (EPA), which regulates fluoride levels in public water systems, said it will review new evidence on the health effects of water fluoridation. Fluoride, a naturally occurring mineral, was first added to public water in Grand Rapids in 1945 to prevent tooth decay and has since spread to around 70% of the U.S. population. The CDC, American Dental Association, and the American Academy of Pediatrics support adding fluoride to drinking water to prevent cavities, and multiple studies have shown that water fluoridation reduces tooth decay by about 25% in children and adults.
Opponents of water fluoridation have linked the practice to illnesses without scientific backing for decades, including bone cancer and AIDS. Public debate over fluoride was reignited last September when a federal judge in California ordered the Environmental Protection Agency (EPA) to regulate fluoride in drinking water over concerns of cognitive effects on children. More recently, a January review published in JAMA Pediatrics found that as fluoride exposure increased, children’s IQ tended to decrease. The authors note that most of the studies they reviewed were from countries where the fluoridation level far exceeded the United States’ recommended level of 0.7 milligrams per liter, and, according to the review, no studies of fluoride exposure and children’s IQ have been performed in the United States.
Fears that fluoride is a neurotoxin are contributing to efforts to ban it. In March, Utah became the first state to ban fluoride in public drinking water under a new law that will take effect on May 7, and dozens of other cities and local governments are considering similar actions. However, dentists and researchers warn that ending community fluoridation, especially in rural communities where dental care access is more limited, could risk exacerbating this lack of access. More than 150 towns and counties have voted to end fluoridation since 2010, and 14 states this year have considered or are considering ending fluoride mandates or banning fluoridation. According to a KFF Health News analysis, at least 230 counties face dentist shortages and mostly or completely unfluoridated drinking water.
Polling Insights:
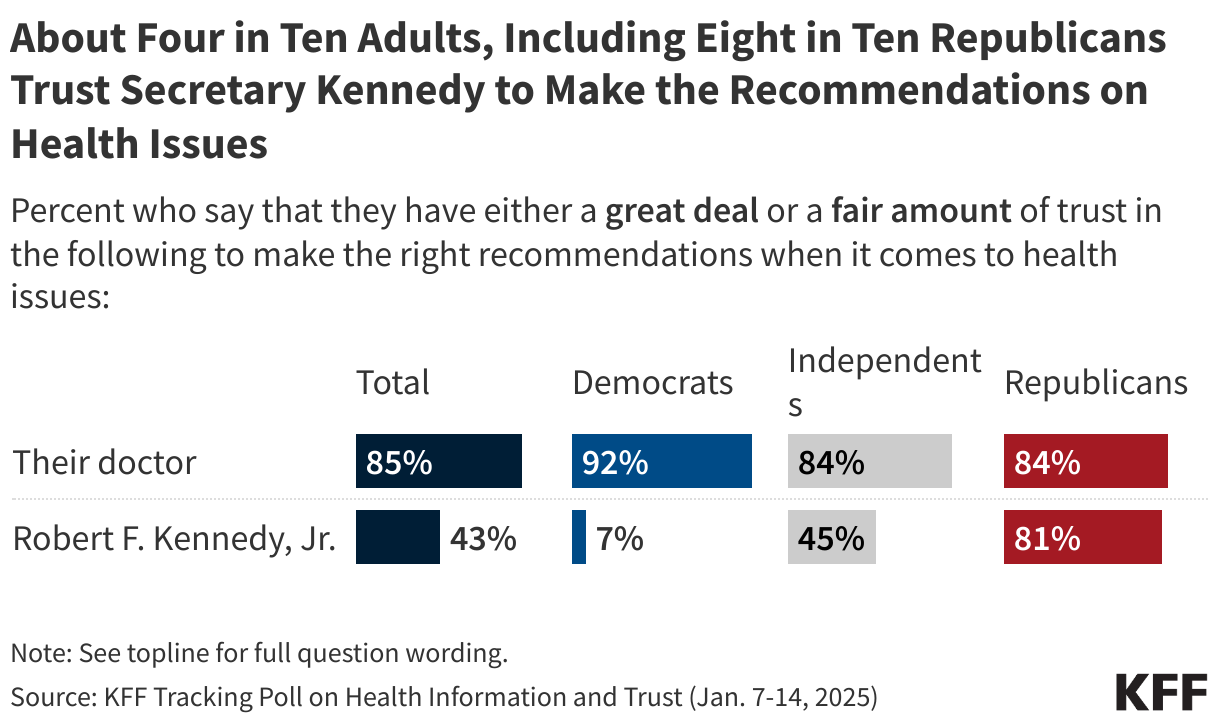
A January KFF tracking poll found that about four in ten adults say they have a great deal or a fair amount of trust in Secretary Robert F. Kennedy Jr. (43%). However, there are large partisan differences in trust. Few Democrats express trust in health recommendations from Secretary Kennedy (7%), whereas among Republicans, about eight in ten say they trust Secretary Kennedy (81%). Notably, Republicans are as likely to say they trust Secretary Kennedy as they are to trust their own doctors (84%) to make the right recommendations on health issues.
Shifts in Public Confidence in Food Safety after USDA Disbands Two Safety Panels

The USDA’s decision to disband two advisory panels on food safety in March prompted a sharp uptick in online discussion, reflecting both genuine concern and emerging misinformation. Between March 5 and March 11, there were approximately 9,000 news articles, social media posts, and comments mentioning the committees. Most of these posts expressed concern that the elimination of these committees would lead to more foodborne illnesses. However, some posts and comments, primarily on Instagram, responded to these fears by misleadingly claiming that a plant-based diet prevents foodborne illness entirely. While animal products are more likely to be contaminated with bacteria and viruses that can cause foodborne illness, plant products can also be contaminated. A CDC study looking at the origins of foodborne illness outbreaks in the U.S. found that produce contributed to 46 percent of cases. This nuance is often lost in posts promoting plant-based diets as completely risk-free.
The response to the USDA’s decision reflects a broader decline in trust in the government’s ability to ensure food safety. In recent years, public concern about food additives and ingredients such as seed oils and artificial coloring has grown, sometimes fueled by false or overstated claims that misrepresent their risks.
Training to Identify False Health Information Builds Resilience, but Follow-Up Reminders Are Needed for Long-Term Impact

The rapid spread of false or misleading claims on social media makes it difficult for fact-checkers to keep up as new versions of persistent narratives quickly resurface during high-profile health policy and news events. Many health communicators work with limited time and resources, and reactive debunking alone may not keep up with the scale and speed of misinformation. Instead, building resilience to false or misleading information by training people on how to recognize and reject false information before they encounter it may offer a more sustainable approach. However, resilience requires reinforcement, as people forget what they’ve learned, and repeated exposure to falsehoods makes them seem more believable over time – a phenomenon known as the “illusory truth effect.” A study published in Nature Communications finds that using “booster” messages – follow-up reminders that repeat key lessons – can strengthen people’s ability to recognize false or misleading information after their initial training. The researchers used either an article, a video, or a game to train people to recognize and reject false information. They found that the article and video had the longest-lasting effects, but resilience lasted longer when participants received a refresher. These findings suggest that, without reinforcement, communicators and educators risk losing the impact of their initial intervention. Even with limited resources, adding brief follow-up messages can help sustain the impact of health literacy interventions over time in a complicated information environment.
Efforts to fact-check health information are further complicated by a lack of agreement about what counts as false health information. For example, KFF’s 2023 Health Misinformation Pilot Poll asked adults to cite COVID-19 misinformation they had encountered and found that many examples directly contradicted each other – what one person considered misinformation, another considered accurate. Instead of combatting misinformation directly, it may be more effective to focus on common goals that can bring people together and improve the way trusted messengers communicate. One study in the HKS Misinformation Review suggests that rather than simply labeling claims as “misinformation,” health communicators and educators should consider why people disagree in the first place. The authors explain that false information often spreads because of deeper differences in values, identities, or ways of understanding the world, not just gaps in knowledge. Health communicators and educators can address these deeper differences by creating respectful conversations that explore the emotional, cultural, and social context that underlie people’s beliefs. This might involve focusing on shared concerns, like protecting loved ones or keeping communities healthy, rather than simply pointing out what’s true or false. While this approach may be more complex and slower than fact-checking alone, the study from HKS Misinformation Review suggests that it is likely to build more trust and lead to longer-term changes in how people engage with health information.
AI & Emerging Technology
Accuracy of Search Engines and Large Language Models in Providing Health Information
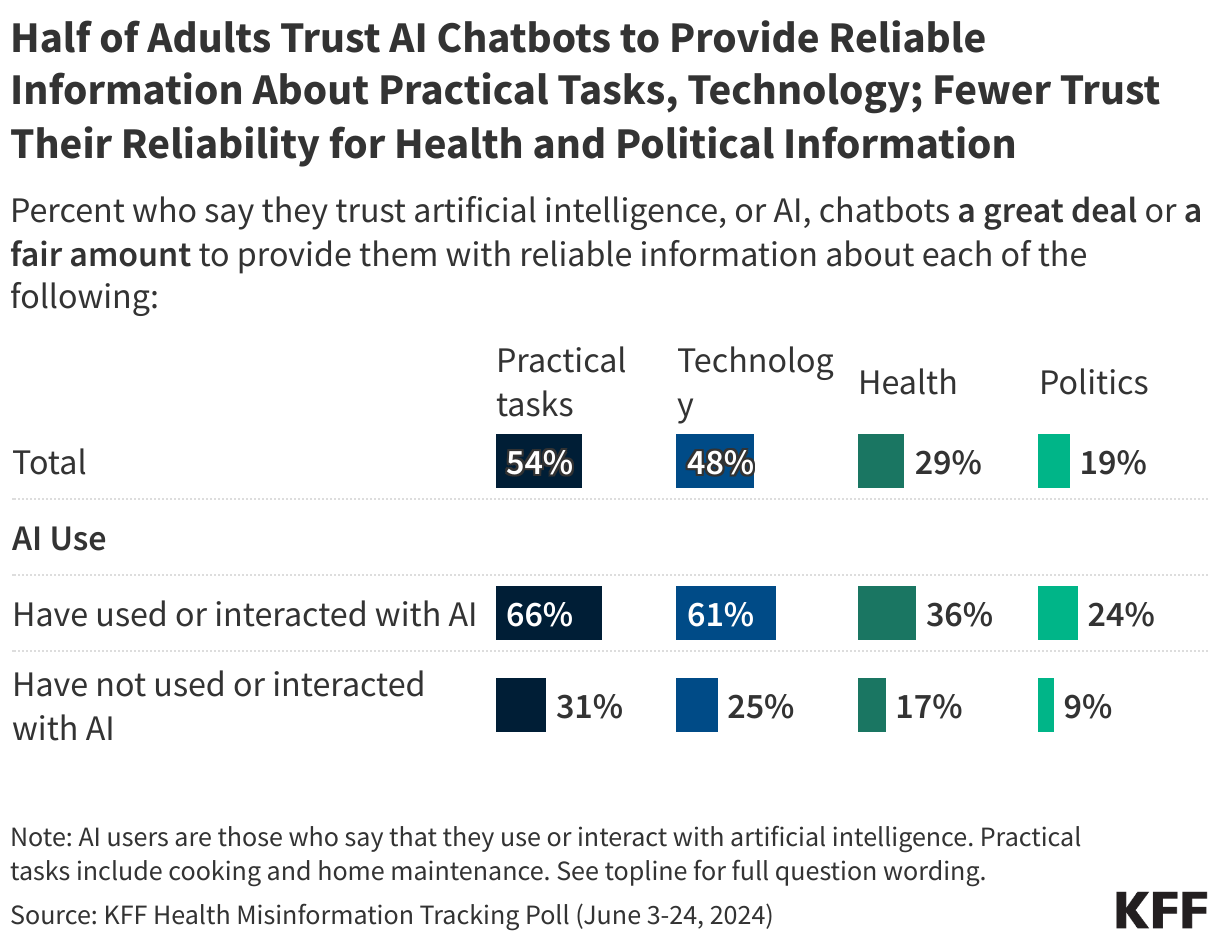
A 2024 KFF poll found that while most adults reported regularly using search engines for health information and advice on a weekly basis, few (13%) said they regularly used AI chatbots for this purpose. Additionally, 70% of adults say they trust AI chatbots “not too much” or “not at all” to provide them with reliable health information. A recent study published in Nature Digital Medicine, however, suggests that LLMs may provide more accurate results than traditional search engines. Search engines, like Google or Bing, work by indexing large amounts of web content and ranking results based on keywords and popularity, often directing users to existing websites. LLMs, on the other hand, are trained on large datasets and generate original responses based on patterns in the data, rather than retrieving exact matches from the web. Unlike search engines, which display a list of sources, LLMs typically present a single answer, which can feel more direct but may also hide the reasoning or sources behind it. The study found that search engines share correct answers 50-70% of the time, with 10-15% of top-ranked results containing harmful advice. In contrast, LLMs generally outperformed the search engines, although they still provided incorrect answers, particularly with poorly framed prompts.
As AI continues to shape the health information landscape, traditional search engines are integrating more AI capabilities. For example, Google’s AI Overviews provide AI-generated summaries at the top of search queries, although their accuracy can vary. These summaries are powered by LLM-like technology, blending the retrieval functions of a search engine with the generative abilities of a chatbot. More recently, Google introduced the “What People Suggest” feature, which uses AI to collect and present comments from patients with similar health conditions to help users understand how others have described their experiences. However, relying on the experiences of others may impact the quality of the information provided, as it introduces subjective perspectives that may not always align with medical evidence or expert advice.
About The Health Information and Trust Initiative: the Health Information and Trust Initiative is a KFF program aimed at tracking health misinformation in the U.S., analyzing its impact on the American people, and mobilizing media to address the problem. Our goal is to be of service to everyone working on health misinformation, strengthen efforts to counter misinformation, and build trust.

The Monitor is a report from KFF’s Health Information and Trust initiative that focuses on recent developments in health information. It’s free and published twice a month.
Sign up to receive KFF Monitor
email updates
Support for the Health Information and Trust initiative is provided by the Robert Wood Johnson Foundation (RWJF). The views expressed do not necessarily reflect the views of RWJF and KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities. The Public Good Projects (PGP) provides media monitoring data KFF uses in producing the Monitor.