KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
About 153 million Americans rely on employer-sponsored health insurance.1 The specific benefits and services covered by those plans are shaped by many factors including costs, employer policies and beliefs, as well as state and federal regulations. A recent increase in legislative efforts at the state level to limit coverage of abortion, including in private insurance plans, could leave more women without coverage for abortion. This gap in plan benefits could have considerable financial consequences for women seeking abortion services, particularly for those who are low-income.
In addition, there are discussions in Congress about including funds in the next Coronavirus relief package to subsidize COBRA premiums for workers who lost their jobs during the COVID-19 pandemic. One of the sticking points of the debates has been whether or not the legislation will include a stipulation that federal funds cannot be used to pay for abortion coverage in employer plans, which could have implications for coverage of abortion in employer plans and the logistics of a COBRA subsidy.
This issue brief presents data from the 2019 KFF Employer Health Benefits Survey on the share of covered workers who are employed by firms that have asked their insurer or third party administrator to exclude coverage for abortion from their health plan.
State Regulation of Abortion Coverage in Private Plans
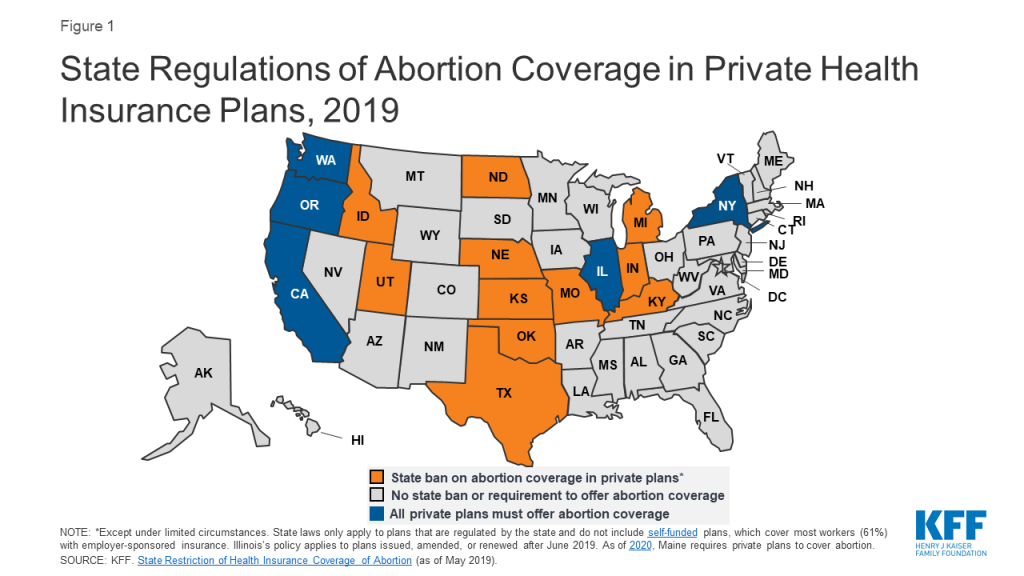
Eleven states ban state-regulated private plans from including abortion coverage; most – but not all – have exceptions for pregnancies resulting from rape or incest or in cases in which it poses a threat to the life of the pregnant woman. Conversely, a handful of states have enacted policies that require coverage of abortion services in state-regulated private plans (Figure 1). However, neither the state-level abortion coverage inclusion or prohibition requirements apply to self-funded plans sponsored by private employers, which are exempt from most state insurance laws. Self-funding is common among larger employers. In total, about three out of five covered workers (59%) at private-sector firms are enrolled in a self-funded plan.2
Figure 1: State Regulations of Abortion Coverage in Private Health Insurance Plans, 2019
In all states (except those where abortion coverage is mandatory for fully-insured plans), employers may choose not to offer coverage for abortion, or only to cover it under limited circumstances such as in cases of rape or incest or life endangerment of the pregnant person (much like the federal law under the Hyde Amendment).
The lack of abortion coverage means that women must directly bear the full cost of the abortion. The cost of an abortion varies by the type of procedure, the location of the provider, and how far along in pregnancy it is performed. One study found that in 2011 and 2012, the average charge was $558 for a surgical abortion and $527 for a medication abortion at 10 weeks gestation. Abortions later in pregnancy can cost thousands of dollars. These costs can make abortion prohibitive for many people. According to a 2017 KFF poll, about one-third of individuals with employer-sponsored insurance (34%) would not be able to pay an unexpected medical bill of $500.
Employer Health Benefits Survey
KFF conducted the annual Employer Health Benefits Survey between January and July of 2019. It included 2,012 randomly-selected, non-federal public and private firms with three or more employes. The 2019 survey asked firms that offer health insurance: “Has your firm asked your insurer or TPA3 [third party administrator] to exclude abortion coverage from your health plan?” For more information on the survey methodology, see the Survey Design and Methods section.
At the firm level, 3% of firms that offer health benefits exclude coverage of abortion in at least some circumstances from their plan. While there are more than three million firms in the United States, most covered workers are employed by a relatively small number of firms.4 At the worker level, 10% of covered workers work at a firm that excludes coverage for abortion under some or all circumstances. This includes 4% of covered workers at firms that exclude coverage of abortion under any circumstance and 6% of covered workers at firms that exclude coverage of abortion except under some limited circumstances (which may include life endangerment, rape, or incest). It is important to note that although an employer may not have excluded abortion coverage, the plan may still not cover it. This is likely the case in states that ban abortion coverage in state-regulated plans.
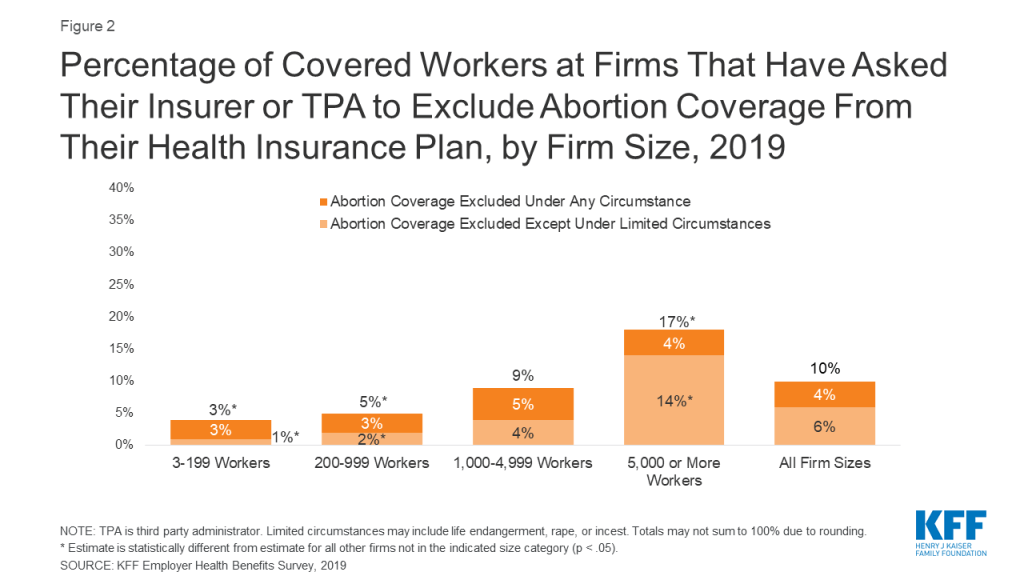
Exclusion of abortion coverage varies by firm size (Figure 2). Covered workers at the largest firms (5,000 or more workers) are more likely (17%) than those at smaller firms to work at a firm that excludes coverage for abortion in at least some circumstances. Only 3% of small firms (3-199 workers) and 5% of moderately sized firms (200-999 workers) specifically requested any exclusion of abortion coverage from their plan.
Figure 2: Percentage of Covered Workers at Firms That Have Asked Their Insurer or TPA to Exclude Abortion Coverage From Their Health Insurance Plan, by Firm Size, 2019
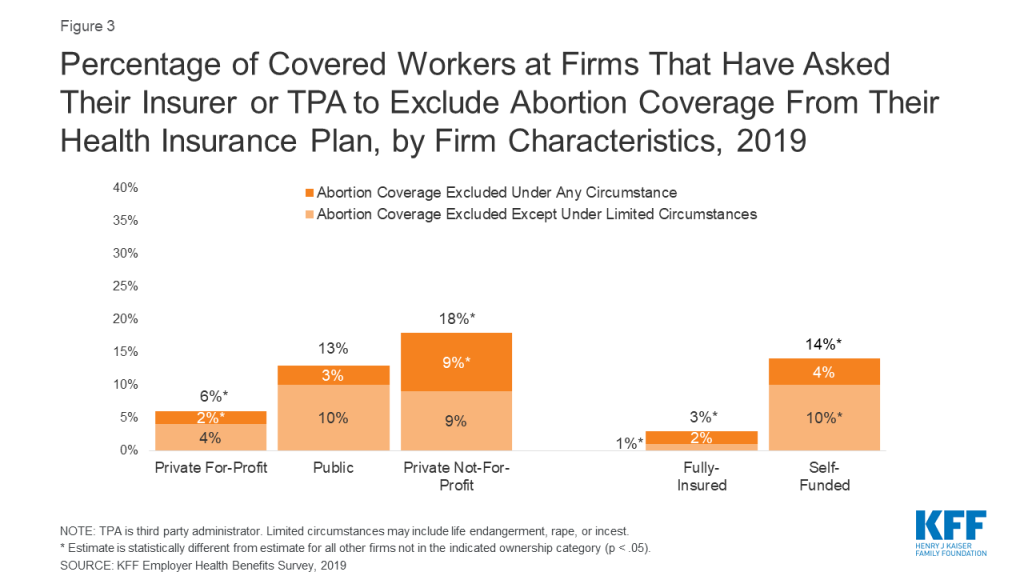
Exclusion of abortion coverage also varies by other firm characteristics such as ownership structure, plan funding, and firm wage level (Figure 3). Covered workers at private-not-for-profit firms (18%) are more likely than those at private for-profit firms (6%) to work at a firm that excludes coverage for abortion under some or all circumstances. Private not-for-profit firms include many large health care and educational institutions that have religious affiliations, some of which are opposed to abortion and limit insurance coverage of it in their health plans. There were approximately 1.56 million non-profits registered with the IRS5 in 2015, but they do not collect uniform information on whether non-profits are religiously-affiliated. Thirteen percent of covered workers at public employers, such as state and local governments, restrict abortion coverage in at least some circumstances. In 2019, 20 states had bans on inclusion of abortion in their public employee insurance plans except in limited circumstances; two states had bans on abortion coverage under all circumstances. While not included in the survey, health plans for federal employees follow the Hyde Amendment rule that excludes coverage of abortion except in cases of rape, incest, or life endangerment.
Figure 3: Percentage of Covered Workers at Firms That Have Asked Their Insurer or TPA to Exclude Abortion Coverage From Their Health Insurance Plan, by Firm Characteristics, 2019
Covered workers at firms with a completely or partially self-funded plan (14%) are more likely than those at firms with a fully-insured plan (3%) to work at firm that excludes abortion coverage under at least some circumstances. Self-funded plans established by private employers (but not public employers) are exempt from most state insurance laws, including reserve requirements, mandated benefits, premium taxes, and many consumer protection regulations. Self-funding is common among larger firms because they can spread the risk of costly claims over a large number of workers and dependents. The survey did not ask the specific reason(s) the firm chose to self-fund their plan.
Discussion
Employer-sponsored health insurance is the primary source of health benefits in the U.S., covering 153 million Americans. Ten percent of covered workers are employed at a firm that has asked to exclude abortion from their health plan in least some circumstances. This percentage does not include the more than 20 million federal employees, veterans, military personnel, and dependents whose health plans contain the Hyde amendment rule excluding coverage for abortion except in limited circumstances. It also does not include private sector employees (and their dependents) whose employer did not ask for an exclusion but that reside in a state that bans abortion coverage in state-regulated plans.
Additionally, plans that do cover abortion may have restrictions on the situations in which they will pay for it, including limits on gestational age, number of abortions covered, or the method of abortion. This has been the case in individual plans that are available in some of the ACA Marketplaces in states that have not fully banned abortion coverage in private plans.
It is important to note that the survey did not ask if the firm’s plan includes abortion coverage. When this question was asked in prior years, a sizeable share of employers did not know whether their plan included coverage for abortion. In light of the extensive job loss resulting from the coronavirus pandemic, Congress is considering legislation to subsidize COBRA premiums to help unemployed and furloughed people afford to remain on their employer’s health insurance. Media reports have noted that there is bipartisan support for the subsidies, but disagreement over whether there should be a ban on subsidies that pay for abortion coverage in plans, citing the Hyde Amendment ban on federal funding of abortion. Uncertainty over whether or not an employer plan covers abortion could pose logistical challenges to the implementation of this legislation should it restrict or limit funds to health plans that include abortion coverage.
Employer-sponsored health insurance is the primary source of coverage for millions of workers in the U.S. Gaps in coverage of services effectively means that workers and their families may be required to bear the cost of that medical care. For the many workers and dependents who lack abortion coverage, these costs can translate into hundreds or thousands of dollars out-of-pocket for abortion services, placing a financial barrier to this service, particularly for low-wage workers.
This estimate excludes state and local government employees. While federal law (the Employee Retirement Income Security Act of 1974, or ERISA) generally exempts self-funded plans from state insurance regulations, states do have jurisdiction over the plans offered to state and local employees. ↩︎
A TPA is an administrator or insurer that provides administrative services such as claims management, commonly for self-funded plans. ↩︎
Some of the non-profits registered with the IRS have fewer than three employees. Only firms with at least three employees are included in the KFF Employer Health Benefits Survey. ↩︎
While use of telemedicine in the U.S. had been minimal prior to COVID-19, interest in and implementation of telemedicine has expanded rapidly during the crisis, as policymakers, insurers and health systems have looked for ways to deliver care to patients in their homes to limit transmission of the novel coronavirus. With growing demand for telemedicine, several changes have been made to telehealth policy, coverage and implementation, in order to make telemedicine more widely accessible during this state of emergency.
The federal government has focused on loosening restrictions on telehealth in the Medicare program, including allowing beneficiaries from any geographic location to access services from their homes. HHS has waived enforcement of HIPAA for telemedicine, while the DEA has loosened requirements on e-prescribing of controlled substances.
On a state level, many state governments have focused on expanding telehealth in their Medicaid programs, as well relaxing state-level restrictions around provider licensing, online prescribing and written consent. Many states are also mandating fully-insured private plans to cover and reimburse for telemedicine services equally to how they would for in-person care (service parity and payment parity).
Meanwhile, many commercial insurers have voluntarily addressed telemedicine in their response to COVID-19, focusing on reducing or eliminating cost sharing, broadening coverage of telemedicine and expanding in-network telemedicine providers.
Health systems have rapidly adapted to implement new telehealth programs or ramp up existing ones. This requires significant financial and workforce investment, which may be more difficult for smaller or less-resourced practices. Actions to rapidly expand telemedicine could come with tradeoffs, including concerns over privacy and quality of care.
A number of gaps remain in ensuring access to telemedicine during the COVID-19 pandemic. Service parity and payment parity for telehealth across all insurers would help increase access for patients and incentivize providers to offer these services, though it would also increase spending. Gaps in technology access and use among some groups of patients may also be a concern. It remains unclear if the U.S. will sustain this expanded use of telemedicine after the state of emergency ends, and to what extent low-income patients and patients with limited experience with or access to technology will be able to access these services.
Introduction
As clinicians seek new ways to serve patients and stem the rapid spread of the novel coronavirus in the United States, policymakers and insurers have looked to telemedicine or telehealth to provide care to patients in their homes. At a time when many people in the U.S. are under shelter in place orders, this approach to care allows patients to maintain social distancing, reduce their risk of exposure to the novel coronavirus and potentially avoid overburdening emergency departments and urgent care centers at this time. After many years of slow growth, telemedicine use has exploded across the nation in a few short weeks. The telemedicine landscape is complex, with many moving pieces as different players respond to COVID-19. The federal government has taken actions to broaden and facilitate the use of telemedicine, particularly though Medicare. States, health systems, and insurance carriers have also moved with unprecedented speed to shift many visits that were previously done in person to a telemedicine platform. This brief presents some of the many policy changes that have taken place in the field of telehealth by the federal government, state governments, commercial insurers and health systems in just the few short weeks since the COVID-19 outbreak hit the U.S. We highlight key considerations in achieving widespread implementation of telemedicine services during this pandemic and beyond, including easing of telemedicine regulations, broadening insurance coverage, strengthening telecommunications infrastructure, and patient facing issues like connectivity and quality of care.
What is telemedicine?
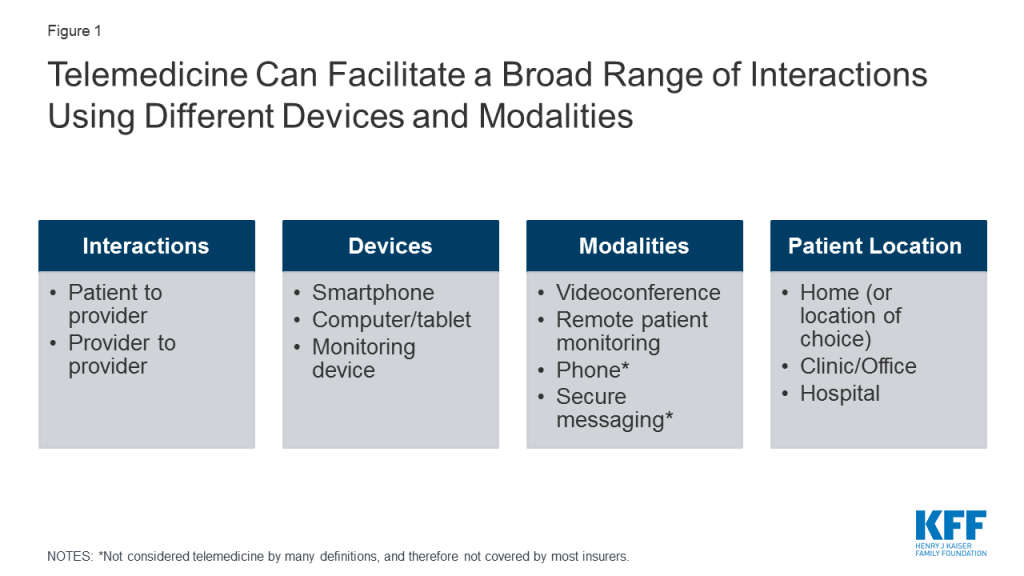
While varied definitions for telemedicine or telehealth exist, it is commonly defined as the remote provision of health care services using technology to exchange information for the diagnosis, treatment and prevention of disease. Telemedicine is usually defined narrowly by insurers to include technologies like live videoconference and remote patient monitoring, while telehealth is often defined more broadly, to include basic telecommunication tools, as simple as phone calls, text messages, emails, or more sophisticated online health portals that allow patients to communicate with their providers. However, telehealth and telemedicine are often used interchangeably.
Telemedicine can enable providers to deliver health services to patients at remote locations, by conducting “virtual visits” via videoconference or phone (Figure 1). During a telemedicine visit, a patient may see providers from their usual source of care, like Stanford Health, Kaiser Permanente, or Mount Sinai, or they may interact with providers employed by a stand-alone telemedicine platform like Amwell or Virtuwell. Telemedicine can also enable remote interactions and consultations between providers.
Figure 1: Telemedicine Can Facilitate a Broad Range of Interactions Using Different Devices and Modalities
How widespread was telemedicine use before COVID-19?
Before the onset of the COVID-19 pandemic, utilization of telemedicine in the U.S. was minimal. Telemedicine growth has been limited by lack of uniform coverage policies across insurers and states, and hurdles to establishing telemedicine in health systems (e.g. high startup costs, workflow reconfiguration, clinician buy-in, patient interest). The Peterson-KFF Health System Tracker analyzed a sample of health benefit claims from the IBM MarketScan Commercial Claims and Encounters Database; among enrollees in large employer health plans with an outpatient service, 2.4% had utilized at least one telehealth service in 2018 (up from 0.8% in 2016). Similarly, utilization of telemedicine by traditional Medicare and Medicaid and beneficiaries enrolled in managed care plans had been trending upward, but remained low.
How is telemedicine being used during the COVID-19 pandemic?
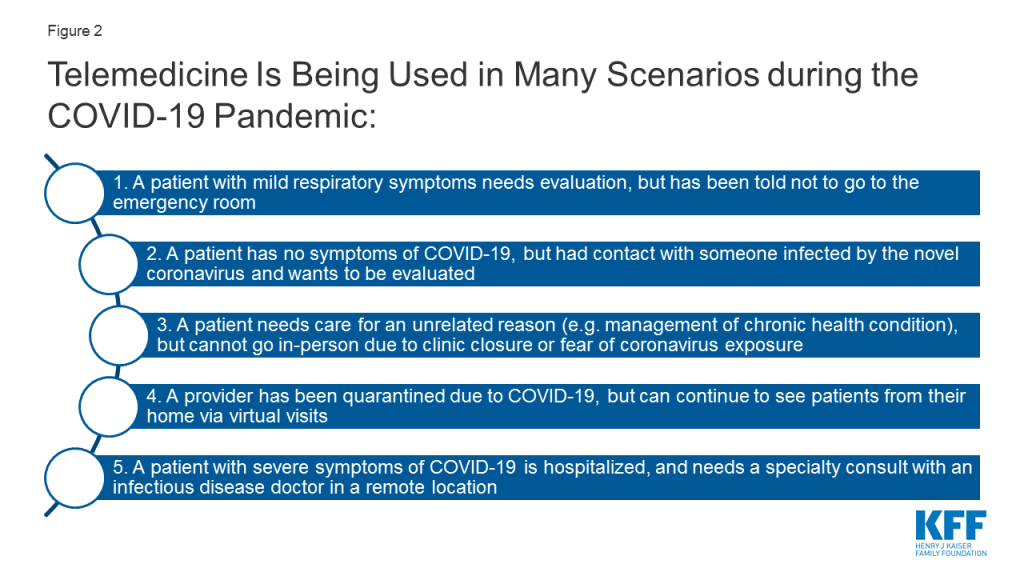
During the COVID-19 pandemic, there are multiple scenarios in which patients and providers are utilizing telemedicine to enable remote evaluations between a patient and a provider, while respecting social distancing. (Figure 2). Use of “virtual visits” via phone or videoconference can address non-urgent care or routine management of medical or psychiatric conditions, while online or app-based questionnaires can facilitate COVID-19 screening to determine the need for in-person care.
Figure 2: Telemedicine Is Being Used in Many Scenarios during the COVID-19 Pandemic
Many hospitals have instructed patients with suspected coronavirus symptoms or exposure to call their doctors or turn to telemedicine first, before showing up to the emergency room or urgent care visit. The Cleveland Clinic, University of Washington (UW), NYU Langone, Oregon Health Sciences University (OHSU), Intermountain Health Care, Medical University of South Carolina (MUSC), and Rush University Medical Center are all advising patients with suspected coronavirus to start by using a virtual visit or online screening, rather than presenting to an emergency room for testing. This is in line with the Centers for Disease Control and Prevention (CDC) encouragement that those who are mildly ill should call their doctors before seeking in-person care. For patients who are having more severe symptoms (e.g. difficulty breathing) or with complex comorbidities, evaluation from their home via telemedicine may not be appropriate, as in-person care intervention may be needed.
What measures have been taken so far to expand telehealth access in the U.S.?
In response to the novel coronavirus, demand for telemedicine is rapidly increasing. Telemedicine, what was once a niche model of health care delivery, is now breaking into the mainstream in response to the COVID-19 crisis. In China, telemedicine platform JD Health saw a tenfold increase in their services during the outbreak and is now providing nearly 2 million online visits per month. In the U.S., existing telemedicine platforms like Amwell and UPMC’s virtual urgent care have reported rapid increases in their utilization. A recent poll found 23% of adults have used telehealth services in light of the COVID-19 pandemic.
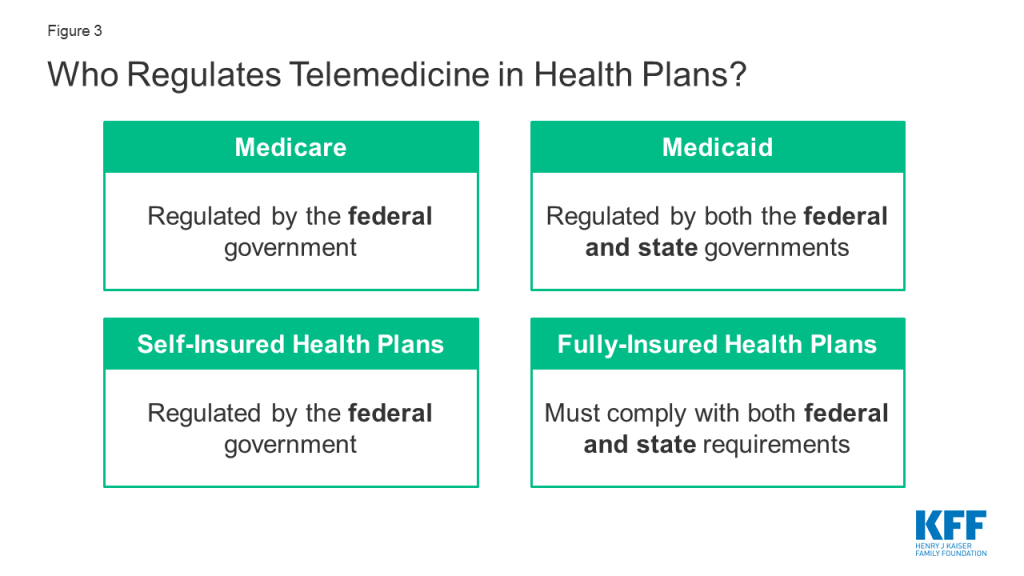
There are a myriad of telemedicine laws and regulations determine who can deliver which telemedicine services to whom, in what location, in what fashion, and how they will be reimbursed. The federal government regulates reimbursement and coverage of telemedicine for Medicare and self-insured plans, while Medicaid and fully-insured private plans are largely regulated on a state-by-state basis (Figure 3). This complexity in the regulatory framework for telemedicine creates challenges for patients in knowing what services are covered, and for providers in knowing what regulations to abide by.
Figure 3: Who Regulates Telemedicine in Health Plans?
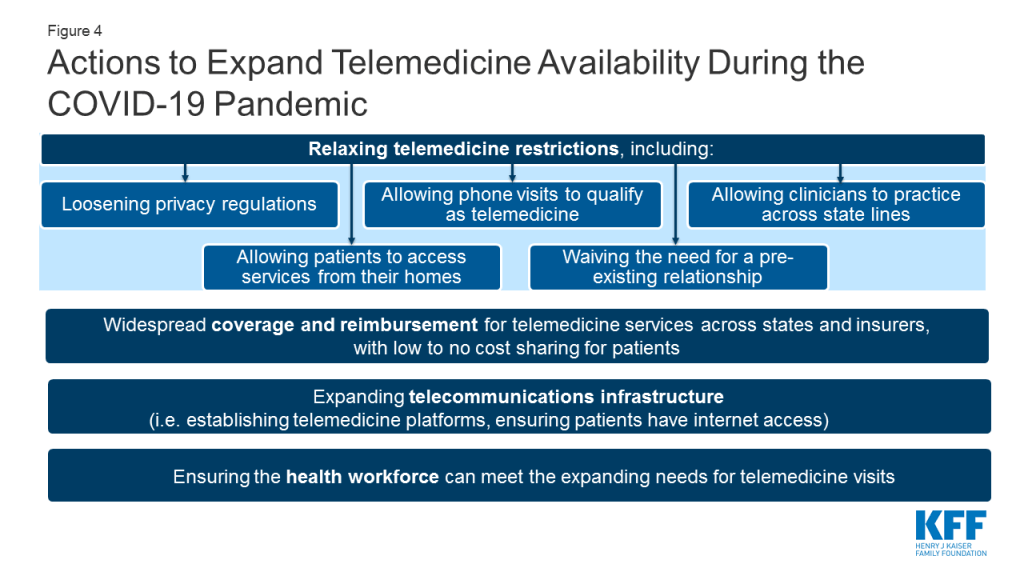
As the COVID-19 pandemic evolves, so too are the emergency policies regarding telemedicine. The federal government, some states, and some health insurance carriers are trying to enable more telemedicine visits to be permitted and paid for. It is important to note that even when the federal government announces loosening of telemedicine restrictions that states have their own regulations and laws that shape coverage in state-regulated (fully insured) insurance plans and Medicaid. And even when regulations are temporarily lifted to facilitate telemedicine, health systems and patients will have their own challenges in implementing and accessing these services. While many of the telemedicine regulations have been temporarily relaxed, for telemedicine to be more broadly accessible to patients in the U.S. over the long term, several actions would need to happen (Figure 4). Next, we outline what changes have been made to telehealth policy and implementation by the federal government, state governments, commercial insurers and health systems in response to the COVID-19 emergency, as well as what gaps remain.
Figure 4: Actions to Expand Telemedicine Availability During the COVID-19 Pandemic
Federal Changes to Telehealth Policy
The federal government dictates several facets of telehealth policy, including nationwide patient privacy laws (e.g. HIPAA), federal prescribing laws for controlled substances, grant funding for telehealth initiatives and Medicare coverage of telehealth. In response to the COVID-19 emergency to make telemedicine more widely available, the federal government has taken action in all these domains.
HIPAA
Typically telemedicine platforms are required to comply with regulations under the Health Insurance Portability and Accountability Act (HIPAA), which health organizations and providers must follow to protect patient privacy and health information. However, on March 17, 2020 the U.S. Department of Health and Human Services (HHS) issued an announcement stating that, “Effective immediately… [HHS] will exercise enforcement discretion and will waive potential penalties for HIPAA violations against health care providers that serve patients in good faith through everyday communications technologies during the COVID-19 nationwide public health emergency.” This now allows widely accessible services like FaceTime or Skype to be used to telemedicine purposes, even if the service is not related to COVID-19. Potential concerns to this approach include the possibility that protected health information (PHI) that is discussed or sent over a non-HIPAA compliant platform may be accessed, shared or even sold by these platforms. The National Consortium of Telehealth Resource Centers (NCTRC) currently urges health centers to sign a Business Associate Agreement (BAA) with their chosen platform, to agree that the data exchanged are safeguarded. In addition to HIPAA, many states have their own laws and regulations to protect patient health information. Loosening enforcement of HIPAA will likely not impact state level regulations, meaning states would need to lift or loosen their own health information laws. Some states (e.g. CA, ME, MD, NM, ND, UT) have issued guidance to relax state-specific privacy standards for telehealth during the state of emergency.
Federal oversight of Controlled substances
Under the Controlled Substances Act, the Drug Enforcement Agency (DEA) normally requires an in-person evaluation before a provider can prescribe a controlled substance, limiting telemedicine’s use for e-prescribing of controlled substances without a prior in-person patient-provider relationship. However, during a state of national emergency, there are exceptions to this rule. For the duration of the COVID-19 public health emergency, DEA-registered providers can now use telemedicine to issue prescriptions for controlled substances to patients without an in-person evaluation, if they meet certain conditions. One of these conditions is that provider must still comply with state laws; many states have their own laws regulating telemedicine and controlled substances, which federal changes would not affect.
Medicare
Changes to Traditional Medicare: Based on new waiver authority included in the Coronavirus Preparedness and Response Supplemental Appropriations Act (and amended by the CARES Act), the HHS Secretary has waived certain restrictions on Medicare coverage of telehealth services for traditional fee-for-service (FFS) Medicare beneficiaries during the coronavirus public health emergency (first issued on January 31, 2020, and renewed on April 21, 2020). The waiver does the following: lifts the requirement that beneficiaries must live in rural areas in order to receive telehealth services, meaning beneficiaries in any geographic area could receive telehealth services; allows the patient’s home to qualify as an “originating site” from which they can access telehealth visits; allows telehealth visits to be delivered via smartphone with real-time audio/video interactive capabilities in lieu of other equipment; and removes the requirement that providers of telehealth services have treated the beneficiary in the last three years. A separate provision in the CARES Act allows federally qualified health centers (FQHCs) and rural health clinics (RHCs) to serve as “distant site” providers, and provide telehealth services to Medicare beneficiaries during the COVID-19 emergency period (Figure 5).
Figure 5: Key Changes to Coverage Restrictions for Medicare Fee-for-Service During the COVID-19 Emergency
CMS has also expanded access to the types of services that made be provided via audio-only telephones. In a March 2020 Interim Final Rule, CMS stated that it would allow providers to “evaluate beneficiaries who have audio phones only.” In a subsequent announcement, CMS broadened this to include behavioral health services and patient education services, but still not the full range of telehealth services that can be provided using two-way audio-video connection. This limits telehealth’s reach for Medicare beneficiaries without access to smartphones or other video communications. Other modifications to telehealth availability in response to the COVID-19 emergency include allowing both home health agencies and hospice providers to provide some services via telehealth, and allowing certain required face-to-face visits between providers and home dialysis and hospice patients to be conducted via telehealth. Additionally, CMS is temporarily waiving the Medicare requirement that providers be licensed in the state they are delivering telemedicine services when practicing across state lines, if a list of conditions are met. This change however, does not exempt providers from state licensure requirements (see section below on state licensing actions). Medicare is also temporarily expanding the types of providers who may provide telehealth services.
Importantly, these expanded telehealth services under Medicare are not limited to COVID-19 related services, rather they are available to patients regardless of diagnosis and can be used for regular office visits, mental health counseling, and preventive health screenings. Separate from the time-limited expanded availability of telehealth visits, traditional Medicare also covers brief, “virtual check-ins” via telephone or captured video image, and E-visits, for all beneficiaries. These visits are more limited in scope than a full telehealth visit.
Medicare covers all types of telehealth services under Part B, so beneficiaries in traditional Medicare who use these benefits are subject to the Part B deductible of $198 in 2020 and 20 percent coinsurance, although many beneficiaries have some source of supplemental coverage that helps pay their share of costs. However, the HHS Office of Inspector General is providing flexibility for providers to reduce or waive cost sharing for telehealth visits during the COVID-19 public health emergency.
Changes to Medicare Advantage: Medicare Advantage plans have been able to offer additional telehealth benefits not covered by traditional Medicare and have flexibility to waive certain requirements with regard to coverage and cost sharing in cases of disaster or emergency, such as the COVID-19 outbreak. In response to COVID-19, CMS has advised plans that they may waive or reduce cost sharing for telehealth services, as long as plans do this uniformly for all similarly situated enrollees. This guidance, however, is voluntary and plans will vary in their responses to this new flexibility.
Federal Funding for telehealth
The newly passed Coronavirus Aid, Relief, and Economic Security (CARES) Act includes additional funding to the Telehealth Network Grant Program (TNGP). This program currently awards a total of $8.7 million a year for telehealth technologies used in rural areas and medically underserved areas. The act strikes the current funds, and replaces it with $29 million for five years, starting in 2021. The bill also ends funding for the Telehealth Resource Center (TRC) Grant Program, which is currently funding TRCs at roughly $4.6 million a year for four years, since 2017.
State Changes to Telehealth Policy
A significant portion of telehealth policy is decided by state governments. Each state has its own laws regarding provider licensing, patient consent for telehealth and online prescribing laws. Importantly, states also are in charge of deciding which telehealth services will be covered by their Medicaid program, and most states also have laws governing reimbursement for telemedicine in full-insured private plans. Changes to state level regulations in response to COVID-19 are described next.
Licensing laws
Normally, clinicians must be licensed to practice in states where they offer telemedicine services, and states regulate which health professionals are credentialed to practice in their state. For example, if a clinician is located in California, but is providing services remotely to a patient in Oregon via telemedicine, the provider must be licensed in Oregon, the state where the patient is located. Nine states require special licenses specific to telemedicine. Others participate in “compacts” that allow providers in participating states an expedited process to practice in other compact states. However, to address COVID-19, out of state clinicians may be needed to conduct virtual visits with patients in states with the highest burden of cases. This requires they be licensed to practice across state lines. Almost all states are moving to temporarily waive out of state licensing requirements, so that providers with equivalent licenses in other states can practice via telehealth. The Federation of State Medical Boards is tracking these updates, and finds that currently 49 states have issued waivers regarding licensure requirements during the COVID-19 emergency.
STate Specific Online prescrIbing laws
Most states require a patient-provider relationship be established before e-prescribing of medications. Many telemedicine platforms use an online health questionnaire to establish that relationship, but in at least 15 states, this method is considered inadequate. Instead, a physical exam would be required before prescribing, either in-person, by live-video, or by a referring physician, depending on the state. For patients who are now turning to telemedicine visits rather than their usual source of in-person care, clinicians in some states may face legal barriers to online prescribing medications if they do not already have a pre-existing relationship with the patient. Many states are issuing emergency orders to remove in-person requirements before engaging in telehealth, for the duration of the public health emergency (e.g. AK, AZ, AR, DE, HI, IA, KS, KY, LA, MD, MS, MT, OH, OK, SD).
Consent Laws
Thirty-eight states and DC require providers to obtain and document informed consent from patients before engaging in a telehealth visit. In some states, this applies only to Medicaid beneficiaries, but in others this applies to all telehealth encounters regardless of payor. In most states, verbal consent is allowed, but in a minority of states, consent must be obtained in writing. In response to COVID-19, some state Medicaid programs that would normally require written consent have waived this requirement; for example, providers caring for Medicaid beneficiaries in Alabama, Delaware, Georgia, and Maine can now obtain verbal consent for telemedicine, rather than having the patient sign a written consent form.
Private Insurers and Employer Plans
As of Fall 2019, 41 states and D.C. had laws governing reimbursement for telemedicine services in fully-insured private plans, but private insurer laws enacted by states vary widely. In approximately half of states, if telemedicine services are shown to be medically necessary and meet the same standards of care as in-person services, state-regulated private plans must cover telemedicine services if they would normally cover the service in-person, called “service parity.” However, fewer states require “payment parity,” meaning telemedicine services to be reimbursed at the same rate as equivalent in-person services. CCHP finds only 6 states (CA, DE, GA, HI, MN, NM) that required payment parity prior to COVID-19, while a KFF analysis of telehealth laws suggests an additional 4 states followed payment parity as well (AR, CO, KY, NJ). In the remaining states, telemedicine is typically reimbursed at lower rates than equivalent in-person care. In response to COVID-19, more and more states are enacting service and payment parity requirements for fully-insured private plans. For example, at least 16 states are requiring payment parity for telehealth during the public health emergency.
In contrast to fully-insured health plans which must comply with both federal and state requirements, self-insured health plans are regulated by the federal government through the Department of Labor. These plans may cover telemedicine, but each plan can choose to cover these services or not. Prior analysis shows that the majority of large employer plans, including those that are self-insured, cover some telemedicine services.
Medicaid
Telehealth Policy Before the COVID-19 Emergency: The use of telehealth in the Medicaid program has grown as states have sought to address barriers to care including insufficient provider supply (especially specialists), transportation barriers, and rural access challenges. Historically, states have had broad flexibility to determine whether to cover telehealth/telemedicine, which services to cover, geographic regions telehealth may be used, and how to reimburse providers for these services. Prior to COVID-19, all states and DC provided some coverage of telehealth in Medicaid FFS but the definition and scope of coverage varied from state to state. The most commonly covered modality of telehealth was live video. Few states permitted “audio-only” telephone care to qualify as a telehealth service. Additionally, only 19 state FFS Medicaid programs allowed patient’s to access telemedicine from their homes (e.g. home was not an eligible “originating site”), limiting telemedicine’s reach for many low income people. Of note, state telehealth policies may differ between Medicaid FFS and managed care, an important distinction given most Medicaid beneficiaries are now in managed care plans. A study of Medicaid claims data showed beneficiaries enrolled in Medicaid managed care plans were more likely than those in FFS programs to use telemedicine.
Policy Changes in Response to COVID-19: In response to the COVID-19 outbreak, CMS issued guidance reiterating states can use existing flexibility to provide coverage for telehealth services: “States have broad flexibility to cover telehealth through Medicaid, including the methods of communication (such as telephonic, video technology commonly available on smart phones and other devices) to use.” They clarify, “No federal approval is needed for state Medicaid programs to reimburse providers for telehealth services in the same manner or at the same rate that states pay for face-to-face services.” The FAQ guidance also discusses how telehealth and telephonic services can be covered for FQHCs and rural health centers (RHCs) and under managed care contracts, if states choose to do so.
Almost all states are issuing emergency policies in response to the COVID-19 outbreak to make telehealth services more widely available in their Medicaid FFS programs and/or through Medicaid managed care plans. Importantly, most states are newly allowing both FFS and managed care Medicaid beneficiaries to access services from their home, and most are directing Medicaid plans to allow for reimbursement for some telephone evaluations. Many states are newly allowing FQHCs and RHCs to serve as distant site providers, and expanding which professions qualify as eligible to provide telehealth services through Medicaid.
States are also using 1915(c) Appendix K waivers to enable the provision of home and community-based services (HCBS) remotely by telehealth for people with disabilities and/or long-term care needs. Using Section 1135 waivers all 50 states and DC are relaxing licensing laws, many allowing out-of-state providers with equivalent licensing to practice in their state. Additionally, Medicaid programs in 46 states and DC have issued guidance to expand coverage or access to telehealth during this crisis, while 38 states and DC have granted payment parity for at least some telehealth services as of May 5, 2020. Despite most states moving to expand Medicaid coverage of telehealth services, these changes are not uniform across states, and barriers to implementing and accessing telehealth more broadly are likely to remain during this emergency. KFF is tracking other state Medicaid actions to address COVID-19, found here.
Voluntary Changes to Telehealth by Commercial Insurers
When not mandated by the state, private insurers are free to decide which telehealth services their plans will cover. Therefore, changes to telehealth benefits as a result of COVID-19 vary by insurer. Several major health insurance companies have voluntarily expanded telehealth coverage for fully-insured members (Appendix). Many insurers are reducing or eliminating cost sharing for telemedicine, for a limited period of time. For some plans this applies only to telehealth visits related to COVID-19, while for others this applies to any health indication. Some insurers are expanding their coverage of telehealth benefits, allowing more services, patient locations (e.g. home) and modalities (e.g. phone) to qualify for coverage. To make these services more readily accessible to patients, some insurers are working to increase their numbers of in-network telehealth providers within their existing networks of care, while others are contracting with specific telehealth vendors to provide these services. For example, First Choice Health will waive cost-sharing for telehealth if care is delivered via the 98point6 platform, and Oscar will do so if delivered by the Doctor on Call service. Florida Blue and Prominence Health Plan will waive copays for telehealth if using the Teladoc platform (Appendix). Therefore, patients may not be able to talk to their usual providers, if restricted to certain telehealth platforms by their insurance provider. Insurers responding to the novel coronavirus allow self-insured plans greater flexibility compared to fully insured plans in implementing these new changes, providing an opt-out or opt-in option.
Health System Changes to Telehealth
Prior to the start of the COVID-19 outbreak, more than 50 U.S. health systems already had telemedicine programs in place, including large health centers like Cleveland Clinic, Mount Sinai, Jefferson Health, Providence, and Kaiser Permanente. Meanwhile an estimated 15% of physicians had used telemedicine to facilitate interactions with their patients. However, many health systems did not have existing telemedicine infrastructure, and many providers are novices to providing care through telemedicine. As health systems and smaller practices implement or ramp up use of telemedicine in response to this crisis, there are many provider facing and patient facing considerations to address. Health systems will need to decide whether to invest in telemedicine infrastructure for long-term use, or if they are looking for shorter term, potentially cheaper, solutions solely to respond to this acute crisis.
Provider Facing Considerations
Investing in Telecommunications Infrastructure
For those wishing to initiate a telemedicine program before the COVID-19 emergency, significant financial and personnel investment was typically required. Costs included hiring programmers to create a telemedicine platform, ideally one that integrates into an existing electronic health record, protects patient privacy, and can charge for visits if needed. Alternatively, health systems could contract with existing telemedicine platforms to provide these services. In a 2019 study by Definitive Healthcare, many outpatient practices reported not investing in telehealth due to these financial barriers.
With new telehealth flexibility and relaxation of privacy laws in response to COVID-19, some of these financial hurdles may be lessened. For example, providers can now use phone calls, or affordable technologies like Facetime and Zoom, for many patient encounters, at least for the time being. If and when the regulatory environment around telehealth and HIPAA becomes more stringent, however, providers will need to decide whether to invest in more robust telemedicine platforms to continue to provide these services. This may be beyond what is feasible for many smaller practices, or less-resourced clinics.
During the COVID-19 crisis, ensuring reliable internet connection, and sound and video quality on both the patient and provider end remains important for any telehealth interaction. One concern is that resource limited health organizations may not have sufficient bandwidth to achieve this. During the current outbreak, many telemedicine platforms are experiencing high volumes of patients trying to access care online which has resulted in IT crashes and long wait times to obtain a virtual appointment in some systems. Investing in IT personnel may be necessary to troubleshoot problems with telehealth visits.
Workflow and Training
Implementing new telemedicine initiatives in response to COVID-19 oftentimes requires a redesign of longstanding clinical care models. With expanding use of telemedicine in clinical settings, health systems need to decide which providers they will divert to phone lines and/or video visits and how to manage their patient flow, while still ensuring enough staff to manage in-person care. This means some telemedicine platforms may need to hire more clinicians in order to keep up with demand. While larger health systems may have the financial resources to do this, smaller and more rural practices may be stretched thin as it is. Whether it be doctors, advance practice clinicians like nurse practitioners and physicians’ assistants, or registered nurses who facilitate telemedicine interactions, all will need to be trained on telemedicine technologies, requiring additional time and resources.
Malpractice and Liability Insurance
Clinicians must ensure their malpractice or liability insurance covers telemedicine, and if needed, that it covers services provided across state lines. Hawaii is the only state to require malpractice carriers to offer telemedicine coverage, and insurance premiums may be higher if covering telemedicine. During the COVID-19 outbreak, there are many clinicians who are first-time users of telemedicine, who must ensure they are covered before providing services.
Patient Facing Considerations
Access to Technology
Access to telemedicine may be particularly challenging for low-income patients and patients in rural areas, who may not have reliable access to internet through smartphones or computers. A KFF study showed that in 2017, sizable shares of non-elderly adults with Medicaid reported they had never used a computer (26%), did not use the internet (25%) and did not use email (40%). Additionally, a study by the Harvard School of Public Health showed that 21% of rural Americans reported access to high-speed internet is a problem for them or their family. Telemedicine solutions may also be less feasible for seniors. Because older patients are at higher risk for severe symptoms of coronavirus and in general require more frequent primary care, they may benefit greatly from telehealth to reduce in-person risk of exposure. However, many seniors may not feel comfortable or be able to use these technologies. According to Pew Research Center, 27% of U.S. adults aged 65+ reported they did not use the internet in 2019. Based on the results of a March 2020 KFF Health Tracking Poll, nearly seven in 10 adults 65 and older (68%) say they have a computer, smart phone or tablet with internet access at home (compared to virtually all adults ages 30-49 and 85% of adults ages 50-64). However, this may not translate to widespread use of telehealth among older adults, particularly when Medicare’s expansion of telehealth services for people in traditional Medicare is at the moment limited to the duration of the public health emergency. While studies show some interest in telehealth among older individuals, concerns include perceived poorer quality of care, privacy issues and difficulty using technology.
Quality of Care
While use of telehealth has opened the door for patients to maintain access to care during this public health crisis, ensuring quality of care of telehealth visits is still important. There are some inherent differences to evaluating patients remotely from their homes compared to in-person. For patients with possible coronavirus infection, taking a thorough history via telemedicine is relatively straightforward, including reviewing symptoms, travel history and exposure history. However, taking important vital signs like a temperature and oxygen saturation proves challenging, particularly if the patient does not have a thermometer or pulse oximeter at home. Without specialized equipment, providers also cannot listen to a patient’s lungs to assess for signs of pneumonia. Further, currently almost all coronavirus testing is happening in person, although the FDA recently approved the first at-home test. While a limited telemedicine assessment may be adequate to determine if a patient needs to present to an emergency room/urgent care or for testing, there are the limitations of telemedicine care for this purpose.
For patients utilizing telemedicine during the COVID-19 emergency for non-respiratory complaints, virtual evaluation may prove challenging as well. For example, if a pregnant person wishes to use telemedicine for a prenatal care visit to reduce their virus exposure, monitoring routine measurements like blood pressure, weight and fetal heart rate will prove challenging if not already set up to do so at home. If a patient needed to buy home monitoring equipment like a blood pressure cuff or a glucose monitor, it remains unclear if this would be paid for by the patient out of pocket, or by the health system.
What more could be done to expand and sustain access to telemedicine during the COVID-19 pandemic and beyond?
In response to the unprecedented pressure to expand services and control the transmission of the novel coronavirus, the federal government, many states governments and commercial insurers are expanding coverage of telemedicine and relaxing existing regulations. The federal government has focused on broadening telemedicine access for Medicare beneficiaries, and waiving enforcement of HIPAA to enable use of video platforms like Facetime and Skype. Many states have relaxed telemedicine written consent, licensing, and online prescribing laws, while expanding coverage in Medicaid and fully-insured private plans. Meanwhile, many health centers have rapidly redesigned their existing models of care to implement telemedicine.
While these unprecedented and swift measures have been taken to broaden telemedicine access during this pandemic, gaps in coverage and access to telemedicine remain. Coverage and reimbursement of telemedicine is still far from uniform between payors, and most changes to telehealth policy are temporary. If the U.S. wishes to invest in telemedicine over the longer term, more permanent measures may need to be taken. Avenues to consider to further expand telemedicine access include:
Ensuring service parity and payment parity for telemedicine care as compared to in-person care, to help expand covered services for patients, and incentivize clinicians to provide this model of care
Ensuring patients can access telemedicine services from their homes (home as “originating site”), to further enable social distancing practices
Allowing use of audio-only phone for telemedicine visits, to help ensure access for patients who do not have live-video technology
Investing in telecommunications infrastructure for less-resourced sites of care, and ensuring internet access to patients in rural areas. This may involve providing direct funding for health systems and smaller practices to implement telemedicine
There are potential trade-offs in loosening regulations on telemedicine, including privacy issues and quality of care. Depending on the insurer, some patients may be able to engage in telemedicine visits with their usual providers, while some may have to see providers from specific telemedicine vendors, outside of their usual source of care. This could create discrepancies in access and continuity of care. Additionally, expanding coverage of telemedicine may result in increasing health spending, if patients use telehealth in addition to in-person care, rather than as a substitute. With all these factors in mind, it will be up to policymakers, payors, and providers to determine if the changes made to telehealth policy in light of COVID-19 outweigh the potential concerns, if they should remain permanently, and if telemedicine helps enable accessible, quality health care.
Appendix
Commercial Insurers Make Changes to Telehealth Policies in Response to COVID-19(Updated 4/15/2020)
Temporary changes made by commercial insurers:
Reducing cost-sharing for covered telehealth services
Medical Mutual of Ohio: Allowing coverage of telephonic visits (without live video) during the current state of emergency
Increasing provider availability via telemedicine
Anthem: Increasing physician availability through its service, LiveHealth Online (LHO). Encouraging in-network doctors to join the platform
Florida Blue: Expanding network of primary care doctors and specialists who are able to treat patients virtually
Magellan Health: Permitting all credentialed and contracted behavioral health providers to conduct telehealth video sessions
Premera Blue Cross: Signed agreements with telemedicine platforms (98point6 and Doctor on Demand) to increase services for at least 90 days
Expanding eligible patient location
Viva Health: Members can access telehealth from any location, with any in-network physician, nurse practitioner or physician assistant
Reimbursement for telehealth
Aetna: Reimbursing for telemedicine at same rate as in-person visits (payment parity)
NOTES: This does not constitute a full list of private insurers who have changed their telehealth policies in response to COVID-19. Many new policies are time-limited, only apply to full insured members, and may change as the pandemic evolves.
SOURCE: AHIP. Health Insurance Providers Respond to Coronavirus (COVID-19). Updated April 15, 2020.
Every Friday, we’re recapping the latest on coronavirus from our tracking, policy analysis, polling, and journalism. Total cases in the U.S. are still climbing, and surpassed 1.2 million this week. Approximately 76,000 have died in the U.S. from COVID-19. Meanwhile, since last Thursday, actions to ease social distancing requirements went into effect in 28 states and 14 states extended social distancing measures. One of the most notable updates to our data trackers was that 33 total states are now reporting 25,000 across 6,000 LTC facilities. Two weeks ago, only 6 states reported this data.
Here are more of the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: This week, total cases worldwide passed 3.85 million – with approximately 591,000 new confirmed cases added between April 30 and May 7. There were approximately 36,000 new confirmed deaths worldwide between April 30 and May 7.
U.S. Cases and Deaths: There have been over 1.26 million total confirmed cases in the U.S. There were approximately 188,000 new confirmed cases and 13,000 confirmed deaths in the United States between April 30 and May 7.
U.S. Tests: There have been approximately 8.1 million total COVID-19 tests with results in the United States — with over 2 million added since April 30. 15.4% of those tests were positive.
Adults at Higher Risk of Serious Illness if Infected with Coronavirus: 38% of all U.S. adults are at risk of serious illness if infected with coronavirus (92,560,223 total) due to their age (65 and over) or pre-existing medical condition. Of those at higher risk, 45% are at increased risk of serious illness if infected with coronavirus due to their existing medical condition such as such as heart disease, diabetes, lung disease, uncontrolled asthma or obesity. Among nonelderly adults, low-income, American Indian/Alaska Native & Black adults have a higher risk of serious illness if infected with coronavirus. For both race and household income, the higher risk of serious illness if infected with coronavirus is chiefly due to a higher prevalence of underlying health conditions and longstanding disparities in health care and other socioeconomic factors.
Social Distancing: 28 states have eased social distancing measures: Alabama, Alaska, Colorado, Florida, Georgia, Hawaii, Idaho, Indiana, Iowa, Kansas, Kentucky, Maine, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, North Dakota, Ohio, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, Vermont, and West Virginia. 14 states have extended social distancing measures: Arkansas, Illinois, Maryland, Michigan, New Hampshire, New Jersey, New Mexico, New York, Oklahoma, Oregon, Rhode Island, Tennessee, Vermont, and Washington
Stay At Home Order: original stay at home order in place in 29 states, stay at home order eased or lifted in 16 states, no action in 6 states
Mandatory Quarantine for Travelers: original traveler quarantine mandate in place in 20 states, traveler quarantine mandate eased or lifted in 3 states, no action in 28 states
Non-Essential Business Closures: original non-essential business closures still in place in 22 states, some or all non-essential business permitted to reopen (some with reduced capacity) in 23 states, no action in 6 states
Large Gatherings Ban: original gathering ban/limit in place in 40 states, gathering/ban limit eased or lifted in 9 states, no action in 2 states
State-Mandated School Closures: Closed in 7 states, closed for school year in 36 states, recommended closure in 1 state, recommended closure for school year in 6 states, rescinded in 1 state
Restaurant Limits: Original restaurant closures still in place in 35 states, restaurants re-opened to dine-in service in 15 states, no action in 1 state
Primary Election Postponement: Postponement in 14 states, cancelled in 1 state, no postponement in 36 states
Emergency Declaration: There are emergency declarations in all states and D.C.
Waive Cost Sharing for COVID-19 Treatment: 3 states require; state-insurer agreement in 3 states; no action in 45 states
Free Cost Vaccine When Available: 9 states require; state-insurer agreement in 1 state; no action in 41 states
States Requires Waiver of Prior Authorization Requirements: For COVID-19 testing only in 5 states; for COVID-19 testing and treatment in 6 states; no action in 40 states
Early Prescription Refills: State requires in 18 states; no action in 33 states
Premium Payment Grace Period: Grace period extended for all policies in 11 states; grace period extended for COVID-19 diagnosis/impacts only in 5 states; no action in 35 states
Marketplace Special Enrollment Period: Marketplace special enrollment period in 12 states; no special enrollment period in 39 states
Paid Sick Leave: 13 states enacted, 2 proposed, no action in 36 states
Approved Section 1115 Waivers to Address COVID-19: 1 state has an approved waiver
Approved Section 1135 Waivers: 51 states have approved waivers
Approved 1915 (c) Appendix K Waivers: 38 states have approved waivers
Approved State Plan Amendments (SPAs): 29 states have temporary changes approved under Medicaid or CHIP disaster relief SPAs, 1 state has an approved traditional SPA
Other State-Reported Medicaid Administrative Actions: 51 states report taking other administrative actions in their Medicaid programs to address COVID-19
At-Home SARS-CoV-2 Diagnostic Tests Could be a Breakthrough, But What Are the Limitations? (Blog)
What We Can Learn from HIV in Communicating about COVID-19 (Blog)
Lifting Social Distancing Measures in America: State Actions & Metrics (Blog)
When Will The Unemployed Go Back To Work? Many Laid Off Workers Expect To Get Jobs Back In The Short-Term But Experts Caution About Long-Term Unemployment (Blog)
The first SARS-CoV-2 diagnostic test with a home collection option by LabCorp received emergency use authorization (EUA) from the Food and Drug Administration (FDA) on April 21, 2020. LabCorp is initially prioritizing healthcare workers and first responders and then expects to make the tests available more broadly. On May 8, 2020 the FDA granted a second EUA to Rutgers’ RUCDR Infinite Biologics for an at-home test using a saliva-based specimen. At-home tests may be a promising avenue to get more people tested in a timely manner and also reduce the risk of exposure in health care settings. An at-home SARS-CoV-2 test would not be the first at-home test for an infectious disease. For several years now, Americans have been able to purchase at-home sexually transmitted infection (STI) tests from online sellers, and experiences with these tests can offer some lessons on the challenges that we might anticipate with the widespread adoption of at-home SARS-CoV-2 testing.
Before the Food and Drug Administration (FDA) authorized any at-home tests for SARS-CoV-2, several companies began development of at-home diagnostic tests. A few of the companies that were already offering at-home tests for STIs and other conditions (e.g. Nurx and Everylywell), jumped on the opportunity to develop and distribute at-home diagnostic tests soon after the FDA issued a policy to accelerate approval of diagnostic tests for COVID-19 in the early days of the outbreak. However, on March 20, 2020 the FDA clarified that test self-collection and at-home tests were not authorized under the initial policy, so these companies subsequently discontinued the distribution of at-home tests, with some redirecting their tests to hospitals and healthcare providers or providing them though clinics (Table 1).
Among the issues that have arisen are state level restrictions on at-home tests, accurate reporting of results to public health authorities, the ability of individuals to safely and correctly collect their own samples, as well as affordability and coverage. Lessons learned from at-home STI testing products highlight other logistical hurdles that could make the mass distribution of an at-home SARS-CoV-2 test challenging.
State policies blocking at-home testing: Existing state direct-to-consumer testing laws currently limit at-home testing in New York, New Jersey, and Rhode Island (which has been a barrier to the availability of STI at-home STI testing in those states). Many of these laws only allow tests to be ordered by licensed physicians and not consumers. LabCorp states that their new FDA-authorized at-home SARS-CoV-2 diagnostic test is not available in Maryland, New Jersey, New York, or Rhode Island, states with large numbers of COVID-19 cases and deaths.
Public health surveillance: The Coronavirus Aid, Relief, and Economic Security (CARES) Act requires every laboratory that performs or analyzes a test that is intended to detect SARS-CoV-2 or to diagnose a possible case of COVID-19 to report the test results to HHS. COVID-19 was also added to the Centers for Disease Control and Prevention’s (CDC) list of national notifiable diseases on April 5, 2020, which often prompts states or local jurisdictions to mandate reporting through law or regulation. Syphilis, chlamydia, gonorrhea, and chancroid are also national notifiable diseases. Most STI home-testing companies have individuals send in their samples, the lab reports the results of the test back to the individual, and the companies report the results to public health agencies that report to the CDC. OraSure Technologies, a company that is currently working on an at-home rapid diagnostic test for SARS-CoV-2 with federal support, has been offering a rapid at-home HIV test that provides the results to individuals without the need to send back a specimen to the lab. It has been up to the individual to contact a provider to confirm the HIV test results and that provider then reports the confirmatory results to the CDC. To keep track of how many people have been tested for SARS-CoV-2 and the prevalence of the virus in the community, at-home testing companies that run the results will need to be required by law to report the test results to public health agencies. However, if a test is developed and approved that provides results at home, unless there is a system of consumers to easily report the test results to public health agencies, we won’t get a full picture of test results and the number of community infections.
Home specimen collection: Many at-home STI tests are FDA-approved laboratory tests and are often sent to labs accredited by the College of American Pathologists (CAP) and certified under the Clinical Laboratory Improvement Amendments (CLIA). The Centers for Medicare & Medicaid Services (CMS) regulates all laboratory testing (except research) performed on humans in the U.S. through the CLIA. While there is concern that self-collected specimens may be more prone to variability and error in the collection (leading to inaccurate results), a systematic review and meta-analysis of self-collected vs. clinician-collected vaginal swabs and urine samples for chlamydia and gonorrhea found self-collected samples to be similarly accurate and a good option for those that otherwise might not be tested. Nasal swabs, particularly of the nasopharynx, the hard to reach cavity between the nose and the throat, may be more challenging to self-collect than those collected by a health care provider. Some companies are proposing saliva tests, which may make self-collection easier. Some companies proposing saliva tests, like the newly approved test from Rutgers’ RUCDR Infinite Biologics, may make self-collection easier.
Cost and Coverage: Historically, few at-home STI tests few accept private insurance or Medicaid. However, the Families First Coronavirus Response Act (P.L. 116-127), and the CARES Act require private insurance, Medicare, Medicare Advantage plans, Medicaid, and the Children’s Health Insurance Program to cover (without cost-sharing or other cost-containment measures) a SARS-CoV-2 test if the test has received an EUA from the FDA or if it is FDA-approved. LabCorp’s test received an EUA from the FDA on April 21, 2020. However, in addition to the costs of STI test kits ($24-$522), some companies charge a consultation fee that ranges from $10-$99 that is not covered by insurance. A few companies like Nurx accept private insurance in 28 states and DC and Medicaid in California, Illinois, and Texas, but consumers with insurance must still pay $75 for the kit contents and the processing. The FDA-approved LabCorp SARS-CoV-2 test costs $119 and as of April 30, 2020, they say they can file your insurance or utilize federal funds to cover the upfront cost of this test. Home-testing companies, however, historically have not accepted insurance for their other diagnostic tests, so a mechanism to charge insurers would need to be developed and implemented to make these tests more widely accessible once they are approved, particularly to low-income individuals.
Using platforms with these ready at-home tests is an attractive avenue to ramp up testing and reduce exposure of health care workers and individuals in the community. Because asymptomatic people may need diagnostic testing multiple times after potential exposure, an at-home test would be a convenient way to do broad scale testing. However, in addition to the many concerns about the accuracy of the tests, there are still challenges in assuring that individuals can easily and accurately collect their own specimens, and receive the financial protections that federal law now provides. Finally, there are not yet systems in place to assure that if rapid result at-home tests are approved, the results can be reported to public health agencies to be included in surveillance statistics and allow for contact tracing for people who test positive.
Designed for health care professionals to test patients at home—at launch will only be available for health care professionals
Not available in NJ, RI, and MD
Tests not available to the public and only available for healthcare facilitiesCompany also working with FDA to have an Emergency Use Application approved for individual at-home testing kit
Among Non-Elderly Adults, Low-Income, American Indian/Alaska Native and Black Adults Have Higher Risk of Developing Serious Illness if Infected With Coronavirus
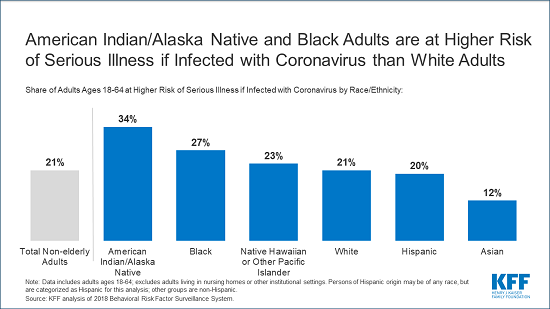
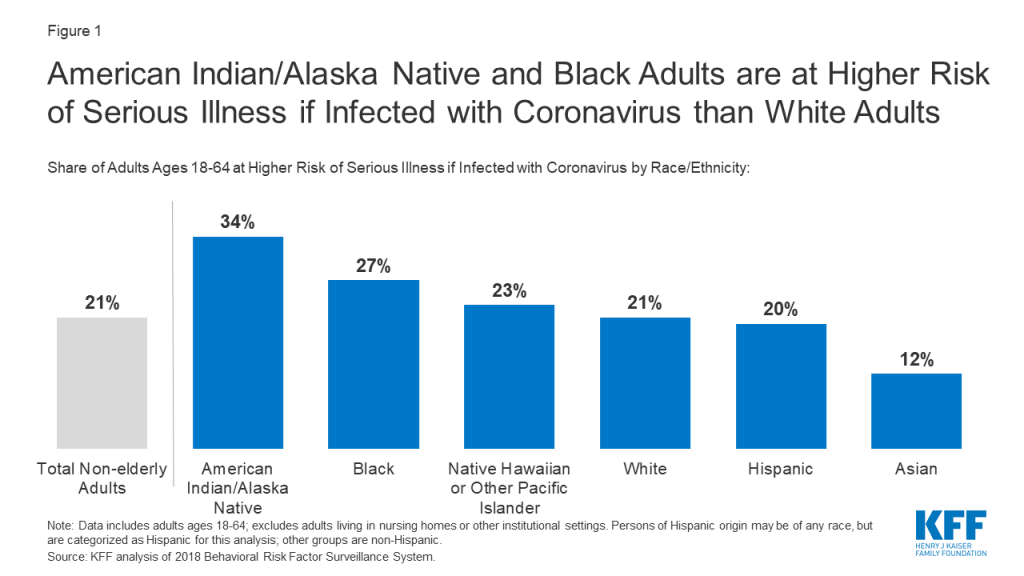
Among non-elderly adults, American Indian/Alaska Native and Black adults are more likely than Whites to be at higher risk of serious illness if infected with the new coronavirus — chiefly due to a higher prevalence of underlying health conditions and longstanding disparities in health care and other socio-economic factors, according to a new KFF analysis. People in lower-income households are also at higher risk.
The analysis finds that the share of non-elderly adults at higher risk of serious illness is 34 percent among American Indian/Alaska Natives and 27 percent among Blacks, compared to 21 percent of Whites. Asian adults are the least likely to be at higher risk of serious illness if infected (12%).
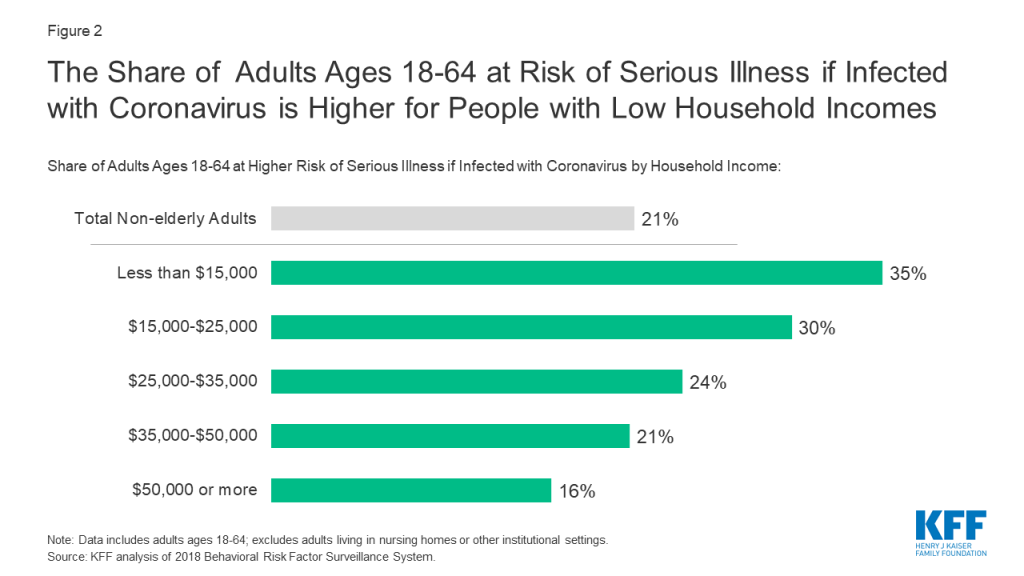
The analysis also finds that more than one in three (35%) non-elderly adults with household incomes below $15,000 are at higher risk of serious illness if infected with coronavirus, more than double the rate found among adults with household incomes greater than $50,000 (16%). Here again the higher risk arises due to a higher prevalence of underlying health conditions among non-elderly people with low incomes.
The new analysis builds upon previous work by KFF examining how many people in the U.S. are at higher risk of developing serious illness from coronavirus. The findings comport with emerging data on COVID-19 cases and deaths that suggest that serious illness from the disease is disproportionately affecting people in communities of color, due to the underlying health conditions and economic challenges faced by such groups.
Also available is a new short animation that examines the populations at higher risk for serious illness if they are infected with the coronavirus that causes COVID-19.
For the full analysis, and other KFF data and analyses related to COVID-19, visit kff.org.
The number of confirmed cases of coronavirus in the U.S. has steadily climbed and is now the highest in the world. The Centers for Disease Control and Prevention (CDC) and state and local governments continue to release data about the characteristics of people who have developed serious illness when infected with coronavirus, as well as the number of hospitalizations and deaths due to COVID-19. These emerging national and state-level data suggest that serious illness resulting from coronavirus disproportionately affects people in communities of color, due to the underlying health and economic challenges that they face. Similarly, adults with low incomes are more likely to have higher rates of chronic conditions compared to adults with high incomes, which could increase their risk of serious illness if infected with coronavirus.
To provide greater insight into the characteristics of people at greater risk of illness if infected with the novel coronavirus, we build on a prior analysis of higher risk adults in the U.S. to break down these numbers by race/ethnicity and household income in 2018. Our definition of higher risk includes: non-elderly adults between the ages of 18 and 64 with heart disease, chronic obstructive pulmonary disease (COPD), uncontrolled asthma, diabetes, or a body mass index (BMI) greater than 40, following the risk factors identified by the CDC. See Methods for more information.
Key Findings
Our prior analysis found about one in five adults (21%) ages 18-64 have a higher risk of developing serious illness if they become infected with coronavirus, due to an underlying health condition. This analysis finds:
More than one in three (34%) American Indian/Alaska Native non-elderly adults are at higher risk of serious illness if infected with the coronavirus; this share is greater than all other racial and ethnic groups (Figure 1).
Figure 1: American Indian/Alaska Native and Black Adults are at Higher Risk of Serious Illness if Infected with Coronavirus than White Adults
More than one in four (27%) Black non-elderly adults are at higher risk of serious illness if infected with coronavirus, compared to about one in five (21%) White adults.
Asian non-elderly adults have the smallest share (12%) of adults at higher risk of serious illness among the racial and ethnic groups included in this analysis.
More than one in three (35%) non-elderly adults with household incomes below $15,000 are at higher risk of serious illness if infected with coronavirus, compared to about one in seven (16%) adults with household incomes greater than $50,000 (Figure 2).
Figure 2: The Share of Adults Ages 18-64 at Risk of Serious Illness if Infected with Coronavirus is Higher for People with Low Household Incomes
Discussion
Most people who are infected with the novel coronavirus are not expected to become seriously ill, however, about one in five non-elderly adults (21%) have an underlying medical condition which puts them at higher risk of serious illness if they get infected. Among people ages 18-64, American Indian/Alaska Native and Black adults are more likely than White adults to be at a higher risk of serious illness due to underlying health conditions and longstanding disparities in health care and other socio-economic factors. Even though the shares of Hispanic and Native Hawaiian or Pacific Islander nonelderly adults at higher risk for serious illness if infected are similar to that of White adults, these groups face disparities in other health, social, and economic factors that may contribute to barriers to health care associated with coronavirus. Although our analysis finds Asian adults are the least likely to be at higher risk for serious illness, this finding may mask subgroups of Asian adults who may be at higher risk.
Federal and state governments are strengthening their efforts to collect and report data by demographics on coronavirus testing, hospitalizations, and deaths. Even so, efforts to analyze these data are limited by the large number of missing responses, and limited surveillance in certain communities. Comprehensive nationwide data, broken down by race and ethnicity and income, are needed to understand how COVID-19 is affecting communities in the U.S. and how best to target coronavirus testing and other resources accordingly.
Methods
This brief analyzes data from the nationally-representative, cross-sectional 2018 Behavioral Risk Factor Surveillance System (BRFSS) of adults ages 18 to 64 living in the community. BRFSS is an ongoing, state-based, random-digit-dialed telephone survey of non-institutionalized civilian adults. The 2018 survey has over 430,000 respondents. Information about the BRFSS is available at http://www.cdc.gov/brfss/index.html. For this analysis, we calculated the share of people at risk of serious illness if they get infected with coronavirus, using BRFSS, by race/ethnicity and self-reported annual household income. The estimates of the percentage of adults at higher risk by race/ethnicity and household income use the BRFSS survey weights to account for the complex sampling design. Data exclude missing values for race/ethnicity and income; data also exclude approximately 15 percent of non-elderly adults who did not know or refused to report their household income. Data exclude adults living in Guam or Puerto Rico. Data represent adults who report ever being told by a doctor that they have one of the listed conditions. Because the CDC guidelines suggest that those with moderate or severe asthma are at greater risk than those with mild asthma, we adjusted the overall total to account for the share with uncontrolled asthma, adjusting the overall total by 62 percent, based on CDC prevalence.
How many adults in the United States are at a higher risk of serious illness if they are infected with coronavirus and who are they? Watch this two minute video to get informed about these highest-risk populations.
As we, and others, navigate how to communicate about COVID-19 and the urgent public health issues it brings, there is much that can be learned in looking at HIV messaging and how it has evolved.
Don’t overlook the basics. In a rapidly changing environment where scientific advances are coming fast, it is important not to lose sight of the basics. Even after more than three decades into the HIV epidemic, we still see a need to cover fundamentals, like how HIV is – and is not – transmitted and that testing is the only way to know if you (or someone else) has it. As the COVID-19 conversation shifts to testing, treatment, and vaccines, there will still be a need for reinforcing messaging about frequent handwashing, not touching your face, and physical distancing.
Focus on normalizing, not moralizing. Blame and shame are terrible public health motivators. In fact, they can have the opposite effect. We have seen the stigma around HIV keep people from taking the very actions needed to stem the epidemic, like getting tested or using protection. Despite best efforts, COVID-19 infections will happen. Some individuals – for reasons beyond their control and not for lack of effort – will be at greater risk. Effective messages empower.
It can be hard to assess personal risk. There is a tendency to look for what makes us different from those who are affected. In HIV, one of the greatest barriers to reaching even those at higher risk is a sense that “it can’t – or won’t – happen to me.” The reality, of course, is that if you are exposed and not protected, there is a chance you will get infected. That’s true for any virus. First person, relatable stories can be effective in breaking down this misconception.
Asymptomatic people are a key audience. As with HIV, not everyone with COVID-19 displays symptoms right away, or at all. Messaging needs to highlight risk, and need for prevention, even when symptoms are not visible.
Responsibility lies with everyone. Collective action and social solidarity are critical to confronting COVID-19. The burden cannot fall only on those who are positive – or symptomatic. Sheltering in place relies on those who may be at lower risk staying home to protect the broader community and frontline workers. Just as an effective HIV response includes messaging both for those who are negative about what they can do to stay that way, as well as for those who are living with HIV, so too must COVID-19 communications.
Acknowledge disproportionate impact without furthering stigma. While every community has experienced some type of fallout from COVID-19, emerging data indicates that Black and Latinx people are disproportionately impacted. These are some of the same populations most affected by HIV. While it is important to shine a light on communities carrying the heaviest burden, it must come with an understanding of why it is happening (lack of health care access, structural racism, social networks, etc.), which are many of the same issues that drive other health disparities, including HIV.
Watch out for unintentional stigma. Most Americans carry some type of risk and many will test positive for COVID-19. They need to be encouraged – and supported – in sharing this information, without fear of judgement about how it happened, even as we continue to educate about prevention. Preserving confidentiality, when possible, is important.
Don’t message in a vacuum. Life circumstances bring different challenges. Sheltering in place will come with economic uncertainty for many. Those struggling with mental health issues may feel increased stress/isolation/anxiety. The most effective messaging reflects and responds to the real-life issues people face. In communicating about HIV, we often are addressing challenges that go beyond the doctor’s office.
Look ahead to messaging about living with COVID-19. COVID-19 is going to be part of our lives for a long time and we need to talk about not just how to survive it, but how to live with it. There has been a huge shift from the early days of the HIV epidemic when it was a death sentence to now, where it is a treatable, manageable condition. While we maintain urgency, it is also important to convey hope.
Connect to resources. To be successful, messaging needs to connect back to concrete actions, including local resources where people can get help. Geo-based, mobile-friendly locators that direct people to testing, treatment, and access to care in their areas will be critical. These tools will need to be developed for COVID-19, as they have been for HIV, and promoted widely.
While much remains unknown about what our future with COVID-19 looks like, and even as we still are learning about the disease itself, what we have learned from messaging about HIV can offer a useful roadmap.
Since the early 1990s, KFF has produced some of the largest, most successful HIV public information campaigns on HIV, many with leading media, both here and abroad. In 2009, we launched Greater Than AIDS, a social impact response that works in partnership with health departments and other community allies to reach those most affected with life-saving information. In 2019, Greater Than AIDS media messages generated more than 360 million impressions and 15.4 million video views.