KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Hospitals with More Private Insurance Revenue, Larger Operating Margins and Less Uncompensated Care Received More Federal Coronavirus Relief Funding Than Others
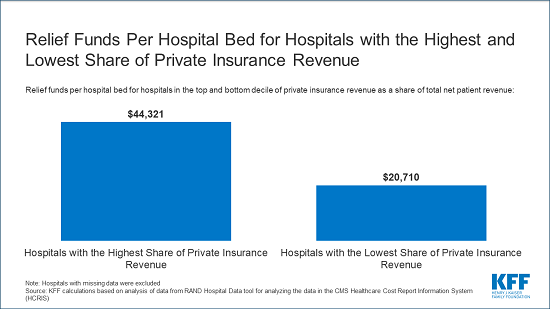
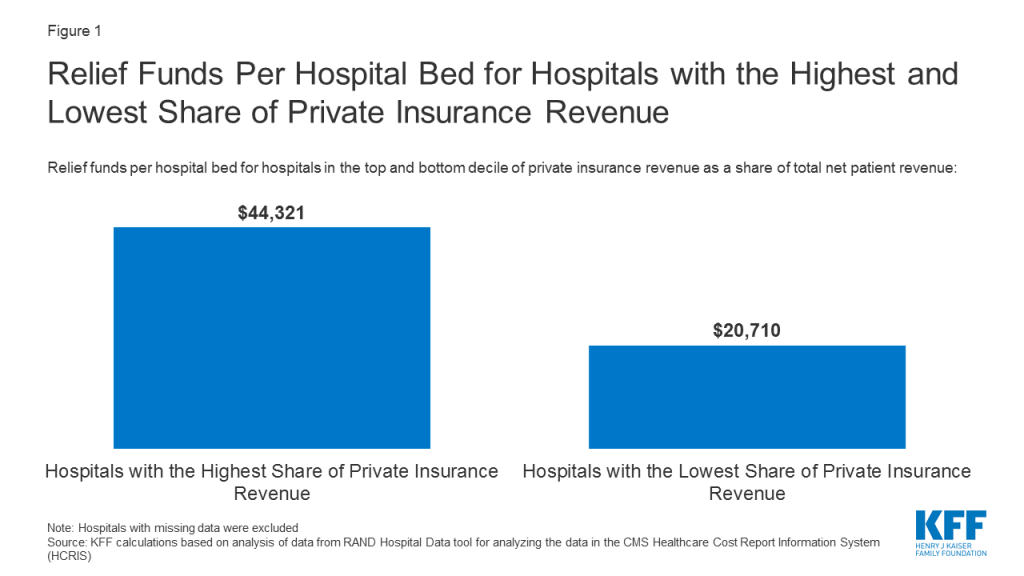
Hospitals that in normal times derive most of their revenue from patients with private insurance received more than twice as much federal coronavirus relief funding per bed than the hospitals that get the smallest share of private insurance money, finds a new KFF analysis of the first $50 billion in relief grants.
Institutions representing the top 10 percent of hospitals based on share of private insurance revenue received $44,321 in coronavirus relief per hospital bed, the analysis finds. That was more than double the $20,710 per hospital bed for the hospitals in the bottom 10 percent based on private insurance revenue.
The lopsided awards are the outgrowth of a distribution formula – determined by the Department of Health and Human Services in an attempt to get relief money out quickly – that favored hospitals with the highest share of revenue from patients with private insurance. These grants were provided using funding from the Coronavirus Aid, Relief, and Economic Security (CARES) Act and the Paycheck Protection Program and Health Care Enhancement Act, which both deferred to the HHS on how the money should be distributed.
Previous KFF analysis documented that private insurance typically reimburses at twice the rate of Medicare, with some hospitals commanding even higher reimbursement. This new study shows that the hospitals that are benefiting the most from that higher reimbursement are now getting the most taxpayer money in the form of coronavirus relief funds. Meanwhile hospitals that make most of their money treating people who are on Medicare and Medicaid, and therefore are typically paid at much lower rates, are getting relatively less help.
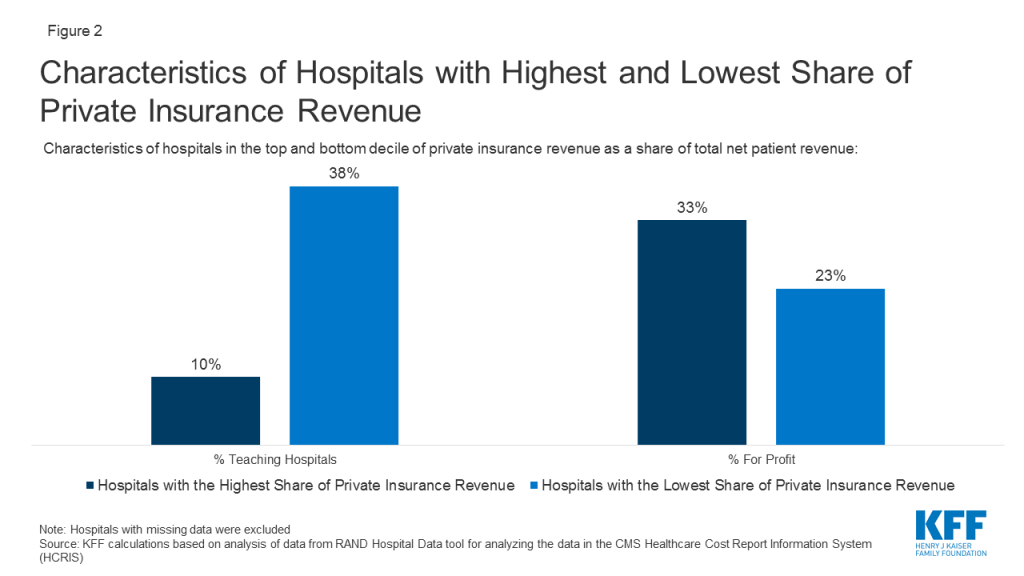
The analysis finds that the hospitals receiving more money are less likely to be teaching hospitals (10% vs 38%) and more likely to be for-profit (33% vs 23%). They had higher average operating margins (4.2% vs -9.0%) and provided less uncompensated care as a share of operating expenses (7.0% vs. 9.1%).
With additional relief money expected, our analysis of more than 4,500 hospitals focused on those with the highest and lowest shares of revenue from private payers to inform policy decisions regarding how to allocate any remaining grants to providers as well as any potential new funding from Congress. In its latest proposed coronavirus relief bill, the House has added details that would take steps to minimize the advantages for providers with more revenue from privately insured patients.
For the full analysis, as well as other data and analyses related to the COVID-19 pandemic, visit kff.org.
The Department of Health and Human Services (HHS) has now begun distributing $72.4 billion of the $175 billion allocated for grants to health care providers in the Coronavirus Aid, Relief, and Economic Security (CARES) Act and the Paycheck Protection Program and Health Care Enhancement Act. This relief fund is designed to provide an influx of money to hospitals and other health care entities to help them respond to the coronavirus pandemic. Congress stated the money can be used either for costs related to treating COVID patients or to reimburse for lost revenue due to the pandemic. The largest share of that $72.4 billion is the $50 billion that the Department of Health and Human Services allocated to providers who participate in Medicare based on their total net patient revenue from all sources.
This brief examines the implications of the decision to allocate funding based on total net patient revenue, which is total patient revenue minus contractual allowances and discounts. The brief focuses specifically on hospitals using data that hospitals report to the Centers for Medicare & Medicaid Services as part of the Healthcare Cost Report Information System (HCRIS). Hospital revenue is mainly a factor of volume and payment rates per service or patient diagnosis. Reimbursement rates vary widely by payer. Hospitals typically command rates from private insurers that average twice Medicare rates per patient, and some are paid substantially higher rates from private insurers in highly concentrated markets. We focused our analysis on hospitals with the highest and lowest shares of revenue from private payers to inform policy decisions regarding how to allocate any remaining grants to providers as well as any potential new funding from Congress.
Findings
The formula used to allocate the $50 billion in funding favored hospitals with the highest share of private insurance revenue as a percent of total net patient revenue. The hospitals in the top 10% based on share of private insurance revenue received $44,321 per hospital bed, more than double the $20,710 per hospital bed for those in the bottom 10% of private insurance revenue (Figure 1).
Figure 1: Relief Funds Per Hospital Bed for Hospitals with the Highest and Lowest Share of Private Insurance Revenue
When compared to the 457 hospitals with the lowest share of private insurance revenue, the 457 hospitals with the highest share of private insurance revenue are less likely to be teaching hospitals (10% vs 38%) and more likely to be for-profit (33% vs 23%) (Figure 2). The hospitals with the highest share of private insurance revenue also had higher operating margins (4.2% vs -9.0%) and provided less uncompensated care as a share of operating expenses (7.0% vs. 9.1%). Uncompensated care includes bad debt, charity care and unreimbursed Medicaid and children’s health insurance program expenses.
Figure 2: Characteristics of Hospitals with Highest and Lowest Share of Private Insurance Revenue
Discussion
Our analysis shows that the size of the relief fund grants varies dramatically per hospital bed based on a hospital’s payor mix. Hospitals with the lowest share of private insurance revenue received less than half as much funding for each hospital bed compared to the hospitals with the greatest share of revenue from private insurance. These hospitals’ large share of private reimbursement may be due either to having more patients with private insurance or charging relatively high rates to private insurers or a combination of those two factors. All things being equal, hospitals with more market power can command higher reimbursement rates from private insurers and therefore received a larger share of the grant funds under the formula HHS used. An alternative methodology for distributing the funds based on patient volume or that increased the size of the grant for providers that are more reliant on public payors such as Medicaid would have distributed the funding more evenly and less skewed by higher revenues from private insurers.
Our analysis focused on hospitals, but all entities that receive Medicare reimbursement were eligible for the $50 billion in relief funds. Those entities include hospice providers, skilled nursing facilities and individual physicians. Importantly, providers who did not have any Medicare reimbursement in 2019 were not eligible for grants from the $50 billion allocation. Some of these providers are pediatricians and obstetricians who do not serve Medicare patients. Others are providers who specialize in serving Medicaid patients and provide crucial services such as non-emergency medical transit, substance use disorder treatment, home-and community-based services, behavioral health services and dental care. HHS has stated that Medicaid-only providers will receive a separate allocation of funding, as will skilled nursing facilities and dentists.
Our analysis shows that hospitals with the highest share of private insurance revenue received a disproportionately high share of total funds. We would expect to see similar patterns for physicians and other entities that receive private insurance reimbursement. For example, community health centers that often see a relatively small share of patients with private insurance would have received less money than a private physician’s office that sees the same total patient volume but has more patients with private insurance. With HHS expected to release additional relief fund grants and Congress considering additional stimulus, this analysis demonstrates that the formula used to distribute funding has significant consequences for how funding is allocated among providers.
Methods and Data Limitations
We used the RAND Hospital Data tool to analyze data that hospitals report to the Centers for Medicare & Medicaid Services as part of the Healthcare Cost Report Information System (HCRIS). The HCRIS data was used because it provides the most complete set of data for all hospitals. The actual payments from the relief fund are based on data hospitals are submitting from their most recent tax filings or audited annual financial statements, which are not always publicly available. The individual hospitals in some hospital systems submit separate HCRIS data but may have applied for a relief fund grant as part of a larger hospital system. In those cases, our calculations of the hospital’s total revenues and the amount received from the relief fund would be based on that individual’s hospitals data and not the data for the larger system.
We used the total net patient revenue reported by each hospital to determine the amount of the $50 billion fund that will go to each hospital, using the formula provided by HHS and using a patient revenue denominator of $2.5 Trillion dollars. To analyze revenue from patients with private insurance, we used RAND’s calculation of private insurance revenues, which are not directly reported in the HCRIS data. Private insurance revenue is calculated by starting with total net patient revenues and then subtracting revenues from traditional (fee-for-service) Medicare, Medicare Advantage, Medicaid, SCHIP and state and local and privately funded indigent care programs, and amounts paid by insured patients who qualify for a hospital’s charity care program. Our definition of private insurance revenue therefore includes patient cost sharing from those with private insurance, including balance billing. The formula that HHS used would have included those amounts as part of total net patient revenue and thus they would have been factored into the amount that each provider received.
We used 2017 data because that was the most recent year when relatively complete data was available. Data were not adjusted for inflation, and some hospitals included in the dataset may no longer be operating or may have merged.
Our analysis includes 4,564 hospitals, 3,242 of which are short-term acute care hospitals paid on the inpatient prospective payment system and 1,322 are critical access hospitals. The data excluded other hospitals, such as children’s hospitals, cancer hospitals, psychiatric hospitals, long-term care hospitals, and Veterans Health Administration facilities. Our analysis used data as reported by hospitals, with some corrections from RAND for data that falls far outside the normal range of variation.
We also assumed that the $50 billion was allocated based on total net patient revenue. In fact, that money was allocated through two separate disbursements. The first $30 billion was distributed based on Medicare fee-for-service revenue and the remaining $20 billion was allocated with the intention of having the total $50 billion be distributed based on total net patient revenue. However, it has been reported that some providers have such a high share of Medicare fee-for-service payments that, in order for the $50 billion to be allocated based on total net patient revenue, those providers would have to give back some of the $30 billion based on Medicare fee-for-service. On May 6, HHS updated its Frequently Asked Questions document to clarify that it “does not intend to recoup funds as long as a provider’s lost revenue and increased expenses exceed the amount of Provider Relief funding a provider has received.” We did not account for that lack of recoupment in our analysis.
This work was supported in part by Arnold Ventures. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
The early years of the Affordable Care Act (ACA) exchanges and broader ACA-compliant individual market were marked by volatility. Markets in some parts of the country have remained fragile, with little competition, an insufficient number of healthy enrollees to balance those who are sick, and high premiums as a result. By 2017, however, the individual market generally had begun to stabilize, and by 2018 insurers in the ACA-compliant market were highly profitable, despite the elimination of cost-sharing subsidy payments and expansion of short-term plans. However, 2019 was the first year that the repeal of the individual mandate penalty went into effect, raising concerns that healthy enrollees would forgo coverage, leaving sicker and more expensive enrollees behind and requiring insurers to increase premiums. Nonetheless, Marketplace premiums fell slightly on average going into 2019, as it became clear that some insurers had raised 2018 rates more than was necessary (and premiums dropped again heading into 2020).
In this brief, we analyze data from 2011 through 2019 to examine how the individual insurance market performed under the ACA and, most recently, without the individual mandate in place. We use financial data reported by insurance companies to the National Association of Insurance Commissioners and compiled by Mark Farrah Associates to look at the average premiums, claims, medical loss ratios, gross margins, and enrollee utilization in the individual insurance market, as well as the amount of medical loss ratio rebates insurers expect to issue to 2019 enrollees. These figures include coverage purchased through the ACA’s exchange marketplaces and ACA-compliant plans purchased directly from insurers outside the marketplaces (which are part of the same risk pool), as well as individual plans originally purchased before the ACA went into effect.
We find that, on average, individual market insurers remained profitable through 2019. Further, despite the absence of the mandate penalty, data indicate that the individual market has not become significantly less healthy. These new data from 2019 offer further evidence that the individual market is stable even without a mandate penalty, though several factors – notably the coronavirus pandemic, economic downturn, and ongoing lawsuit seeking to strike down the ACA – cloud expectations somewhat for the future.
Medical Loss Ratios
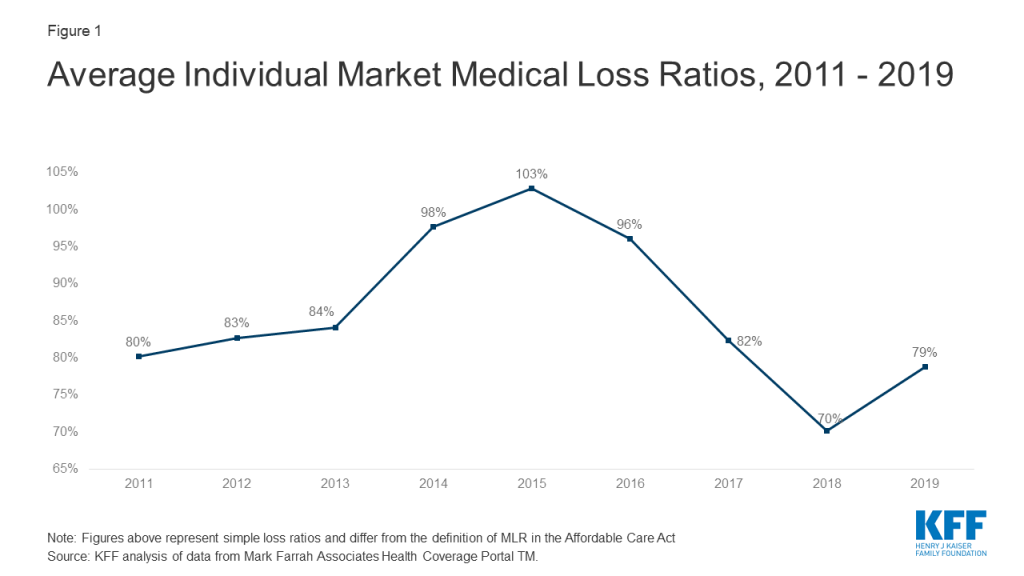
As we found in our previous analysis, insurer financial performance as measured by loss ratios (the share of health premiums paid out as claims) worsened in the earliest years of the ACA Marketplaces, but began to improve in recent years. This is to be expected, as the market had just undergone significant regulatory changes in 2014 and insurers had very little information to work with in setting their premiums.
The chart below shows simple loss ratios, which differ from the formula used in the ACA’s MLR provision.1 Loss ratios began to decline in 2016, suggesting improved financial performance. In 2017, following relatively large premium increases, individual market insurers saw significant improvement in loss ratios, a sign that individual market insurers on average were beginning to better match premium revenues to claims costs. Loss ratios continued to decline in 2018, averaging 70%, suggesting that insurers were able to build in the loss of cost-sharing subsidy payments when setting premiums and some insurers over-corrected. With such low ratios, insurers could not justify premium hikes for 2019, and loss ratios rebounded to average 79% in 2019.
Figure 1: Average Individual Market Medical Loss Ratios, 2011 – 2019
Margins
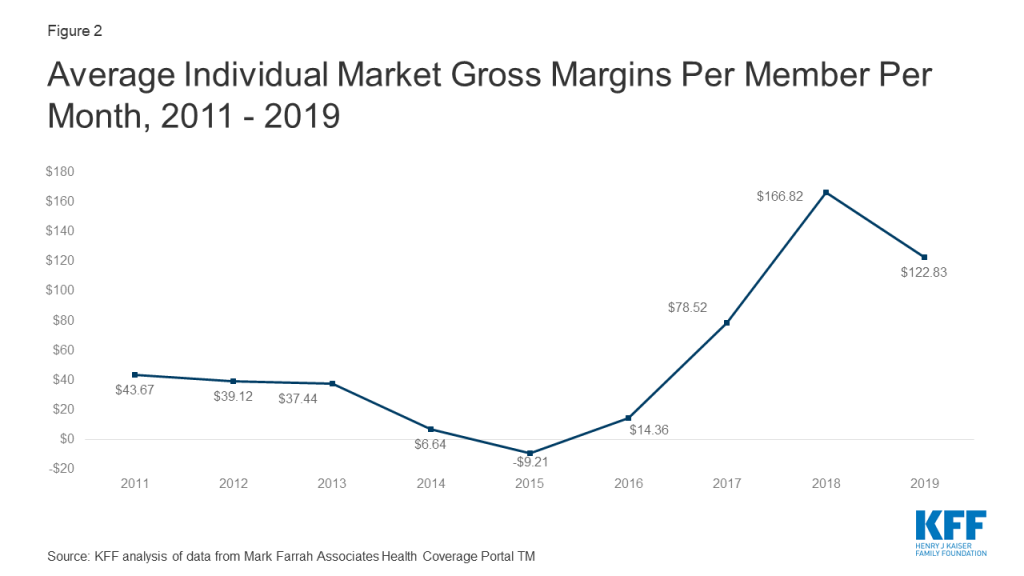
Another way to look at individual market financial performance is to examine average gross margins per member per month, or the average amount by which premium income exceeds claims costs per enrollee in a given month. Gross margins are an indicator of performance, but positive margins do not necessarily translate into profitability since they do not account for administrative expenses.
Figure 2: Average Individual Market Gross Margins Per Member Per Month, 2011 – 2019
Gross margins show a similar pattern to loss ratios. Insurer financial performance improved dramatically through 2018 (increasing to $167 per enrollee, from a recent annual low of -$9 in 2015). Margins fell an average of $44 per member per month from 2018 to 2019, but they remain higher than all other years before 2018. These data suggest that insurers in this market remain financially healthy, on average.
Underlying Trends
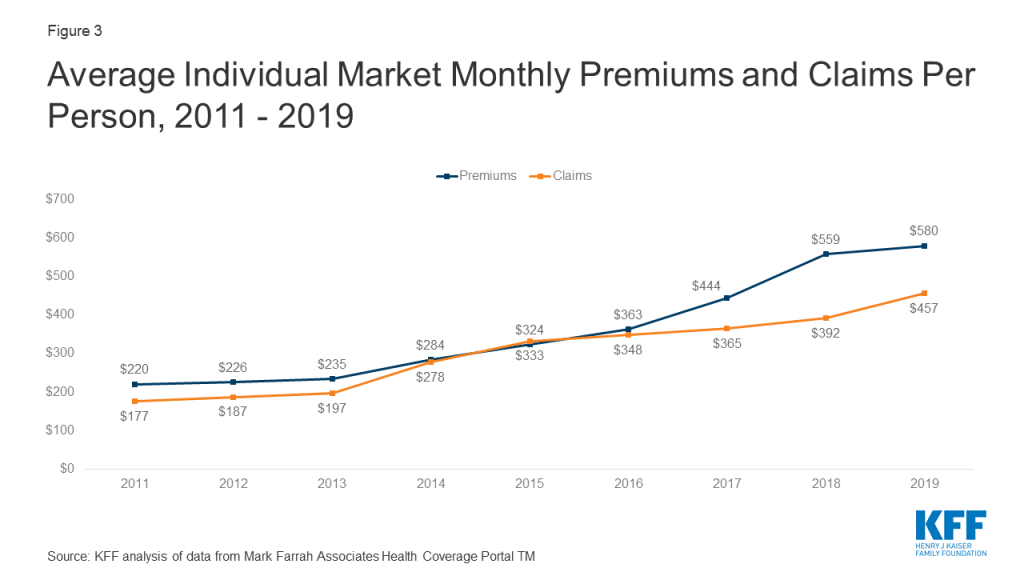
Premiums per enrollee rose slightly in 2019 following steep increases in 2018, while per person claims continued to grow modestly. On average, per member per month premiums grew 4% from 2018 to 2019, and per person claims grew 17%.2
Figure 3: Average Individual Market Monthly Premiums and Claims Per Person, 2011 – 2019
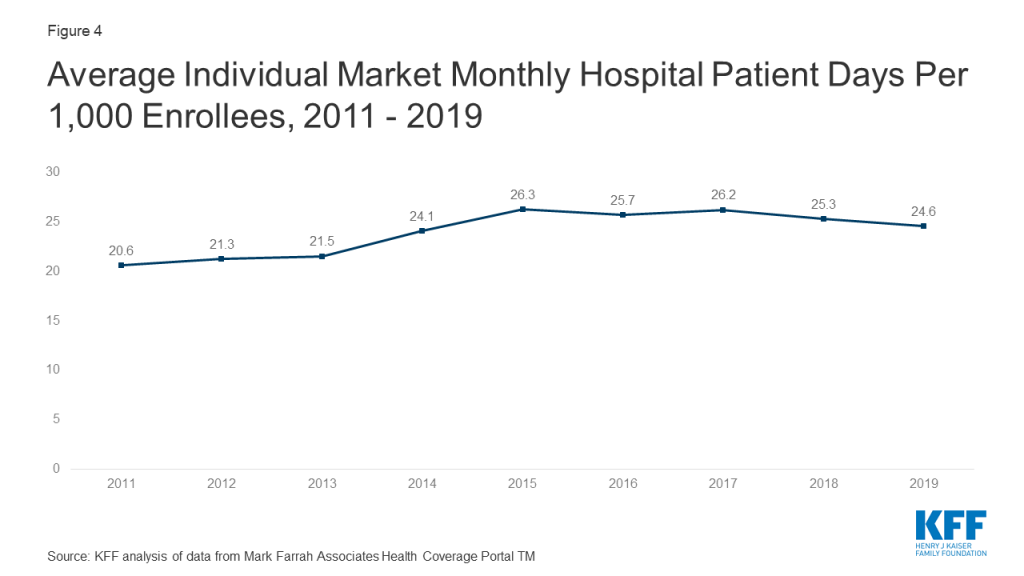
One concern about the elimination of the individual mandate penalty was whether healthy enrollees would drop out of the market in large numbers. However, the average number of days individual market enrollees spent in a hospital in 2019 was slightly lower than inpatient days in the previous four years.3
Figure 4: Average Individual Market Monthly Hospital Patient Days Per 1,000 Enrollees, 2011 – 2019
Taken together, these data on claims and utilization suggest that the individual market risk pool is relatively stable, though sicker on average than the pre-ACA market, which is to be expected since people with pre-existing conditions have guaranteed access to coverage under the ACA. Despite concerns that healthier enrollees may be dropping out of the market in recent years, somewhat lower average inpatient days indicate that the individual market did not get sicker, on average, during 2019.
Discussion
Annual results from 2019 suggest that despite the reduction of the individual mandate penalty to $0 the individual insurance market has remained stable. Insurer financial results from 2019 – the first year the repeal of the individual mandate penalty went into effect – reveal yet another favorable year for insurers in the ACA-compliant market. The repeal of the individual mandate penalty and expansion of short-term plans does not appear to have led to a significantly sicker group of enrollees, as hospitalization rates remain stable.
Our recent analysis also finds that individual market insurers expect to pay a record total of nearly $2 billion in rebates to consumers for falling below the ACA medical loss ratio threshold, which requires insurers to spend at least 80% of premium revenues on health care claims or quality improvement activities. This is more than double the amount insurers paid out in rebates last year. In total, across the individual, small group, and large group markets, insurers expect to issue about $2.7 billion in rebates this year based on their 2019 performance, nearly double last year’s previous record high of $1.4 billion.
While markets in some parts of the country have limited insurer participation and high premiums, the individual market on average remains profitable. In the last two years, some insurers have entered the market and others have expanded their footprints, as would be expected in a competitive marketplace. With a continuing legal battle threatening the exchange markets and the ACA as a whole, significant uncertainties remain. While insurers are now locked in to 2020 premiums for ACA-compliant plans, it remains to be seen how continued uncertainty around the coronavirus pandemic, the economic crisis, and the future of the ACA may affect premiums and plan participation in 2021 or beyond.
Methods
We analyzed insurer-reported financial data from Health Coverage Portal TM, a market database maintained by Mark Farrah Associates, which includes information from the National Association of Insurance Commissioners. The dataset analyzed in this report does not include NAIC plans licensed as life insurance or California HMOs regulated by California’s Department of Managed Health Care; in total, the plans in this dataset represent at least 80% of the individual market. All figures in this issue brief are for the individual health insurance market as a whole, which includes major medical insurance plans and mini-med plans sold both on and off exchange. We excluded some plans that filed negative enrollment, premiums, or claims and corrected for plans that did not file “member months” in the annual statement but did file current year membership.
To calculate the weighted average loss ratio across the individual market, we divided the market-wide sum of total incurred claims by the sum of all unadjusted health premiums earned. Medical loss ratios in this analysis are simple loss ratios and do not adjust for quality improvement expenses, taxes, or risk program payments. Gross margins were calculated by subtracting the sum of total incurred claims from the sum of unadjusted health premiums earned and dividing by the total number of member months (average monthly enrollment) in the individual insurance market. Using earned premiums adjusted for taxes and fees to calculate loss ratios and gross margins increases the MLR by 4 percentage points and decreases the gross margin per member by $31 in 2019. On average across all years, using earned premiums adjusted for taxes and fees increases the MLR by 3 percentage points and decreases the gross margin per member by $16.
Endnotes
The loss ratios shown in this issue brief differ from the definition of MLR in the ACA, which makes some adjustments for quality improvement and taxes, and do not account for reinsurance, risk corridors, or risk adjustment payments. Reinsurance payments, in particular, helped offset some losses insurers would have otherwise experienced. However, the ACA’s reinsurance program was temporary, ending in 2016, so loss ratio calculations excluding reinsurance payments are a good indicator of financial stability going forward. ↩︎
Average premiums per member per month increased in 2019, even while average unsubsidized premiums for the lowest-cost plans in each metal tier went down, because average premiums per member per month reflect changes in the age and geographic distribution of enrollees, changes in plans selected by enrollees, and changes in subsidy amounts. ↩︎
Hospital patient days for 2014 are not necessarily representative of the full year because open enrollment was longer that year and a number of exchange enrollees did not begin their coverage until mid-year 2014. ↩︎
The scale of the economic crisis caused by the coronavirus pandemic just came into clearer view with the release of the latest unemployment numbers, which shows an overall unemployment rate of 14.7% in April, up from 4.4% in March – reflecting an increase of nearly 16 million in the number of unemployed Americans in the last month alone. The unemployment rate is the number of people who are out of a job but actively looking for work as a share of the overall labor force. These unprecedented job losses are being experienced by people across a wide array of occupations and in all age groups.
While the unemployment rate is now highest among people in the youngest age cohort – those ages 16 to 24, where the rate of unemployment is 27.4% – the next highest rate of unemployment is among the oldest age cohort – those ages 65 and older, where the unemployment rate is 15.6%. (Estimates presented here for people ages 55-64 and 65 and older are not seasonally adjusted, because the Bureau of Labor Statistics does not calculate seasonal adjustments for these age cohorts; estimates for younger age cohorts are seasonally adjusted.)
The unemployment rate among people age 65 and older quadrupled between March and April 2020 from 3.7% to 15.6% (Figure 1). By comparison, the overall unemployment rate tripled from 4.4% to 14.7%. From March to April, 1.2 million adults age 65 and older lost jobs, as did another 2.4 million people ages 55 to 64. Altogether, people 55 and older account for just under one fourth of all Americans who lost their jobs in April, which is proportional to their share of the workforce. More than 1 in 5 of the nearly 23 million Americans who are now unemployed are older adults (55+).
Figure 1: The Unemployment Rate among People Age 65 and Older Quadrupled Between March and April 2020
This surge in unemployment reverses years of steadily declining unemployment rates among adults of all ages. And in fact, more adults have continued to work into their older years over time, with labor force participation rates increasing more rapidly for those aged 55 and over, and particularly for those ages 65 and over, than for younger age cohorts. But now, with millions of older adults suffering job losses due to the economic downturn caused by the COVID-19 pandemic, they may be forced to dip into retirement savings or claim Social Security benefits before their full retirement age, resulting in lower payments permanently and undermining their future economic security.
Another major challenge is that people who lose their jobs often lose health insurance. Losing coverage in the midst of a pandemic is especially troublesome, particularly for those who may become seriously ill if they are infected with the coronavirus – which is more likely among older adults. Older adults ages 55-64 may be able to purchase COBRA from a former employer, purchase coverage in the marketplace, or enroll in Medicaid, depending on their individual circumstances. People ages 65 and older who lose employer-sponsored health insurance along with their jobs can enroll in Medicare if they had deferred enrollment while they continued to work, but this is not an option for younger adults.
Overall, these grim unemployment statistics reinforce the fact that the coronavirus pandemic is not just a major public health challenge, but also a threat to economic and retirement security for millions of older adults as well.
As Unemployment Skyrockets, KFF Estimates More than 20 Million People Losing Job-Based Health Coverage Will Become Eligible for ACA Coverage through Medicaid or Marketplace Tax Credits
Nearly Six Million Are Not Eligible and Will Have to Pay the Full Cost of Coverage, and Many Could End Up Uninsured
Coverage Losses Will Affect At Least a Million Residents in Each of Eight States: California, Texas, Pennsylvania, New York, Georgia, Florida, Michigan and Ohio
With more than 31 million workers filing unemployment claims between March 1 and May 2 as the coronavirus crisis hit the nation’s economy, a new KFF analysis estimates 26.8 million people across the country would become uninsured due to loss of job-based health coverage if they don’t sign up for other coverage.
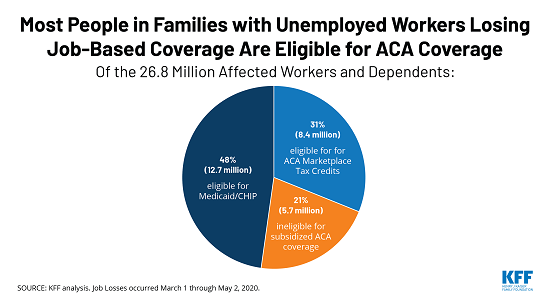
While most are eligible for coverage under the Affordable Care Act (ACA), not all will take it up. In addition, 5.7 million are not eligible for help under the ACA and would have to pay the full cost of their coverage, and many of them will likely remain uninsured.
The analysis estimates that, based on their incomes and other factors, most (79%) who lost employer coverage and became uninsured are likely eligible for subsidized coverage, either through Medicaid (12.7 million) or through the ACA’s marketplaces (8.4 million).
Overall, nearly 78 million people live in a family experiencing job loss since March 1. Some already have coverage from a source besides the previous employer, which they would retain, or could switch to coverage offered by their spouse’s employer or, for young adults, through parents.
At first, a small number (150,000) who live in states that have not expanded their Medicaid programs to cover low-income childless adults would fall into a “coverage gap,” ineligible for Medicaid but with incomes too low to qualify for tax credits to help with marketplace premiums. The analysis projects that this group would grow to 1.9 million by January 2021 when workers’ unemployment benefits expire, dropping their incomes below the threshold to qualify for tax credits.
“Unlike in past recessions, most of those who lose their job-based coverage will be eligible for health coverage because of the Affordable Care Act, though some may find coverage unaffordable even with subsidies,” Executive Vice President for Health Policy Larry Levitt said. “As unemployment benefits expire, however, about two million more people in states that did not expand their Medicaid programs under the ACA will move into the Medicaid coverage gap and have no affordable option.”
Eight states have at least a million affected residents and account for nearly half of all people losing employer coverage and becoming uninsured: California (3.4 million), Texas (1.6 million), Pennsylvania (1.5 million), New York (1.5 million), Georgia (1.4 million), Florida (1.4 million), Michigan (1.2 million) and Ohio (1 million). These are all large states with many workers in hard-hit industries that often provide health benefits.
The analysis reflects workers’ incomes while working and while employed, family status, and state of residence. It takes into account workers’ expected unemployment benefits, including the $600 per week additional federal supplement available through the end of July.
Other findings include:
The analysis estimates 6.1 million children are losing employer coverage, though the vast majority (5.5 million) are eligible for Medicaid or the Children’s Health Insurance Program in their states. These programs generally cover children at higher-income levels than adults.
As Congress continues to debate aid to states, the analysis estimates about 16.8 million people who lost employer coverage will be eligible for Medicaid by January 2021, placing a potential strain on state budgets and provider capacity.
The economic consequences of the coronavirus pandemic have led to historic levels of job loss in the United States. Social distancing policies required to address the crisis have led many businesses to cut hours, cease operations, or close altogether. Between March 1st and May 2nd, 2020, more than 31 million people had filed for unemployment insurance. Actual loss of jobs and income are likely even higher, as some people may be only marginally employed or may not have filed for benefits. Some of these unemployed workers may go back to work as social distancing curbs are relaxed, though further job loss is also possible if the economic downturn continues or deepens.
In addition to loss of income, job loss carries the risk of loss of health insurance for people who were receiving health coverage as a benefit through their employer. People who lose employer-sponsored insurance (ESI) often can elect to continue it for a period by paying the full premium (called COBRA continuation) or may become eligible for Medicaid or subsidized coverage through the Affordable Care Act (ACA) marketplaces. Over time, as unemployment benefits end, some may fall into the “coverage gap” that exists in states that have not expanded Medicaid under the ACA.
In this analysis, we examine the potential loss of ESI among people in families where someone lost employment between March 1st, 2020 and May 2nd, 2020 and estimate their eligibility for ACA coverage, including Medicaid and marketplace subsidies, as well as private coverage as a dependent (see detailed Methods at the end of this brief). To illustrate eligibility as their state and federal unemployment insurance (UI) benefits cease, we show eligibility for this population as of May 2020 and January 2021, when most will have exhausted their UI benefits.
What are coverage options for people losing ESI?
Eligibility for health coverage for people who lose ESI depends on many factors, including income while working and family income while unemployed, state of residence, and family status. Some people may be ineligible for coverage options, and others may be eligible but opt not to enroll. Some employers may temporarily continue coverage after job loss (for example, through the end of the month), but such extensions of coverage are typically limited to short periods.
Medicaid:Some people who lose their jobs and health coverage—especially those who live in states that expanded Medicaid under the ACA— may become newly eligible1 for Medicaid if their income falls below state eligibility limits (138% of poverty in states that expanded under the ACA). For Medicaid eligibility, income is calculated based on other income in the family plus any state unemployment benefit received (though the $600 per week federal supplemental payment available through the end of July is excluded). Income is determined on a current basis, so prior wages for workers recently unemployed are not relevant. In states that have not expanded Medicaid under the ACA, eligibility is generally limited to parents with very low incomes (typically below 50% of poverty and in some states quite a bit less); thus many adults may fall into the “coverage gap” that exists for those with incomes above Medicaid limits but below poverty (which is the minimum eligibility threshold for marketplace subsidies under the ACA). Undocumented immigrants are ineligible for Medicaid, and recent immigrants (those here for fewer than five years) are ineligible in most cases.
Marketplace: ACA marketplace coverage is available to legal residents who are not eligible for Medicaid and do not have an affordable offer of ESI; subsidies for marketplace coverage are available to people with family income between 100% and 400% of poverty. Some people who lose ESI may be newly-eligible for income-based subsidies, based on other family income plus any state and new federal unemployment benefit received (including the $600 per week federal supplement, unlike for Medicaid).2 While current income is used for Medicaid eligibility, annual income for the calendar year is used for marketplace subsidy eligibility. Advance subsidies are available based on estimated annual income, but the subsidies are reconciled based on actual income on the tax return filed the following year. People who lose ESI due to job loss qualify for a special enrollment period (SEP) for marketplace coverage.3 As with Medicaid, undocumented immigrants are ineligible for marketplace coverage or subsidies. However, recent immigrants, including those whose income makes them otherwise eligible for Medicaid, can receive marketplace subsidies.
ESI Dependent Coverage: People who lose jobs may be eligible for ESI as a dependent under a spouse or parent’s job-based coverage. Some people may have been covered as a dependent prior to job loss, and some may switch from their own coverage to coverage as a dependent.
COBRA: Many people who lose their job-based insurance can continue that coverage through COBRA, although it is typically quite expensive since unemployed workers generally have to pay the entire premium – employer premiums average $7,188 for a single person and $20,576 for a family of four – plus an additional 2%. People who are eligible for subsidized coverage through Medicaid or the marketplaces are likely to opt for that coverage over COBRA, though COBRA may be the only option available to some people who are income-ineligible for ACA coverage.
Short-term plans: Short-term plans, which can be offered for up to a year and can sometimes be renewed under revised rules from the Trump administration, are also a potential option for people losing their employer-sponsored insurance. These plans generally carry lower premiums than COBRA or ACA-compliant coverage, as they often provide more limited benefits and usually deny coverage to people with pre-existing conditions. Even when coverage is issued, insurers generally may challenge benefit claims that they believe resulted from pre-existing medical problems; given the long latency between initial infection and sickness with COVID-19, these plans are riskier than usual during the current pandemic. People cannot use ACA subsidies toward short-term plan premiums.
Our analysis examines eligibility for Medicaid, marketplace subsidies, and dependent ESI coverage. We do not estimate enrollment in COBRA, short-term plans, or temporary continuation of ESI. See Methods for more details.
How does coverage and eligibility change following job loss?
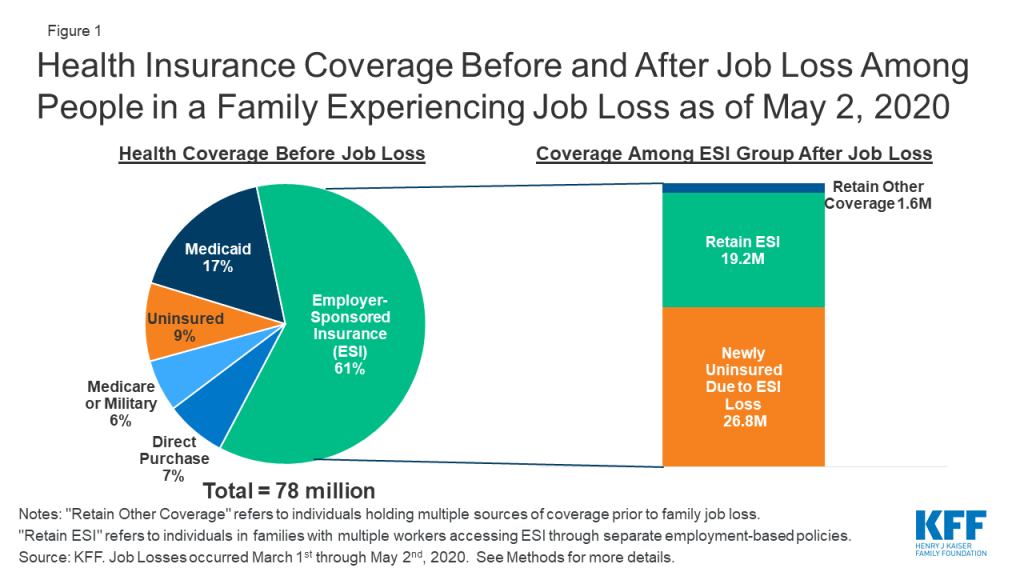
Between March 1st, 2020 and May 2nd, 2020, we estimate that nearly 78 million people lived in a family in which someone lost a job. Most people in these families (61%, or 47.5 million) were covered by ESI prior to job loss. Nearly one in five (17%) had Medicaid, and close to one in ten (9%) were uninsured. The remaining share either had direct purchase (marketplace) coverage (7%) or had other coverage such as Medicare or military coverage (6%) (Figure 1).
Figure 1: Health Insurance Coverage Before and After Job Loss Among People in a Family Experiencing Job Loss as of May 2, 2020
We estimate that, as of May 2nd, 2020, nearly 27 million people could potentially lose ESI and become uninsured following job loss (Figure 1). This total includes people who lost their own ESI and those who lost dependent coverage when a family member lost a job and ESI. Additionally, some people who otherwise would lose ESI are able to retain job-based coverage by switching to a plan offered to a family member: we estimate that 19 million people switch to coverage offered by the employer of a working spouse or parent. A very small number of people who lose ESI (1.6 million) also had another source of coverage at the same time (such as Medicare) and retain that other coverage. These coverage loss estimates are based on our assumptions about who likely filed for UI as of May 2nd, 2020 and the availability of other ESI options in their family (see Methods for more detail).
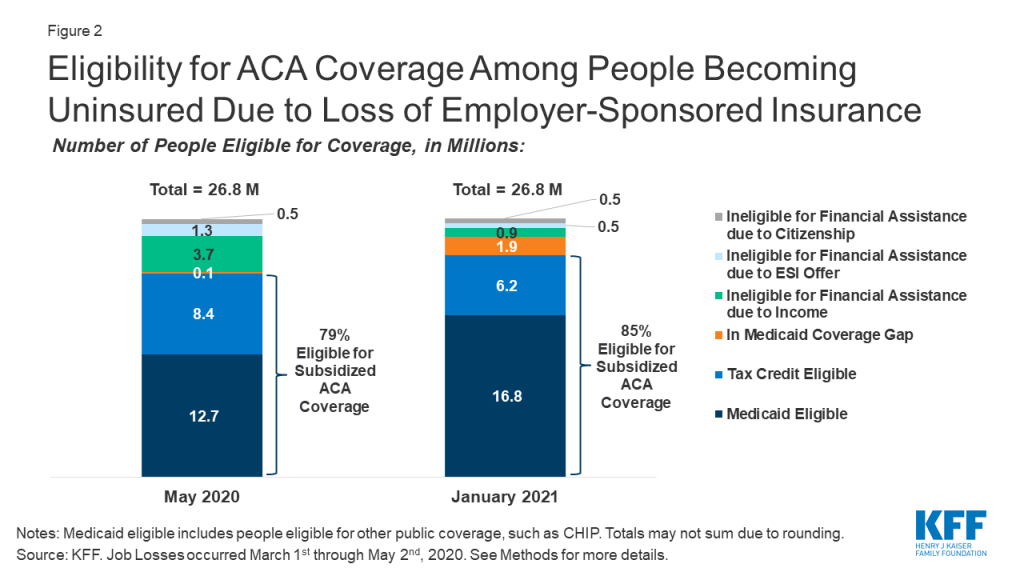
Among people who become uninsured after job loss, we estimate that nearly half (12.7 million) are eligible for Medicaid, and an additional 8.4 million are eligible for marketplace subsidies, as of May 2020 (Figure 2). In total, 79% of those losing ESI and becoming uninsured are eligible for publicly-subsidized coverage in May. Approximately 5.7 million people who lose ESI due to job loss are not eligible for subsidized coverage, including almost 150,000 people who fall into the coverage gap, 3.7 million people ineligible due to family income being above eligibility limits, 1.3 million people who we estimate have an affordable offer of ESI through another working family member, and about 530,000 people who do not meet citizenship or immigration requirements. We project that very few people fall into the coverage gap immediately after job loss (as of May 2020) because wages before job loss plus unemployment benefits (including the temporary $600 per week federal supplement added by Congress) push annual income for many unemployed workers in non-expansion states above the poverty level, making them eligibility for ACA marketplace subsidies for the rest of the calendar year.
Figure 2: Eligibility for ACA Coverage Among People Becoming Uninsured Due to Loss of Employer-Sponsored Insurance
By January 2021, when UI benefits cease for most people, we estimate that eligibility shifts to nearly 17 million being eligible for Medicaid and about 6 million being eligible for marketplace subsidies (Figure 2), assuming those who are recently unemployed have not found work. Many unemployed workers who are eligible for ACA marketplace subsidies during 2020 would instead be eligible for Medicaid or fall into the coverage gap during 2021. The number in the coverage gap grows to 1.9 million (an increase of more than 80% of its previous size), and the number ineligible for coverage due to income shrinks to 0.9 million.
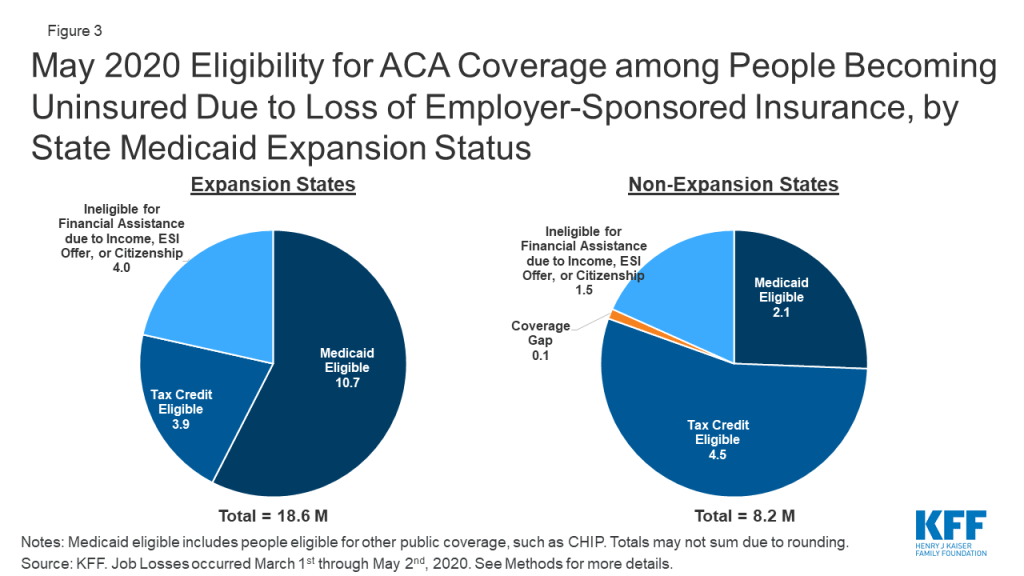
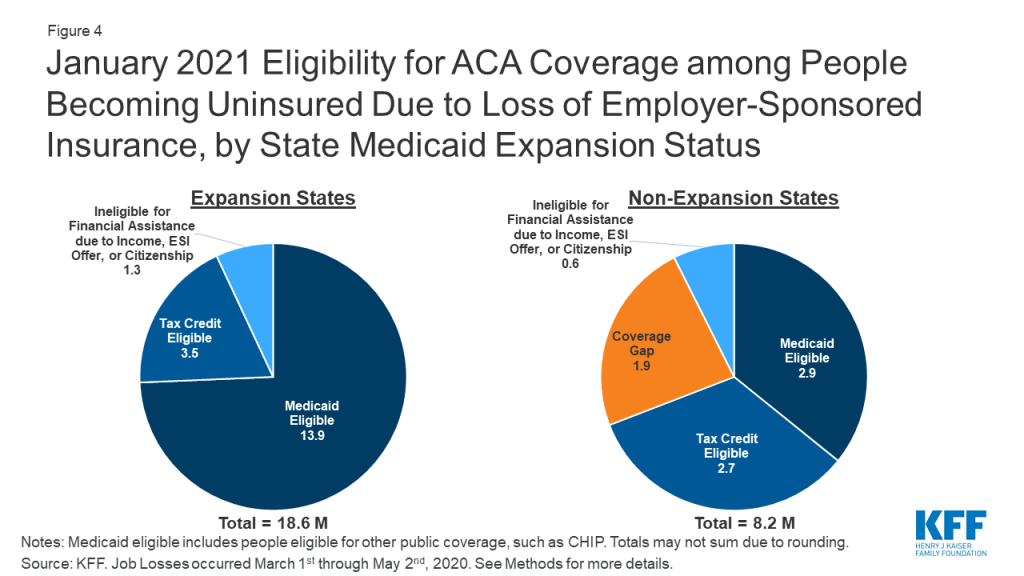
Estimates of coverage loss and eligibility vary by state, depending largely on underlying state employment by industry and Medicaid expansion status. Not surprisingly, states in which the largest number of people are estimated to lose ESI are large states with many people working in affected industries (Appendix Table 1). Eight states (California, Texas, Pennsylvania, New York, Georgia, Florida, Michigan, and Ohio) account for just under half (49%) of all people who lose ESI. Five of the top eight states have expanded Medicaid, and people eligible for Medicaid among the potentially newly uninsured as of May 2020 in these five states account for 40% of all people in that group nationally. Overall, patterns by state Medicaid expansion status show that people in expansion states are much more likely to be eligible for Medicaid, while those in non-expansion states are more likely to qualify for marketplace subsidies (Figure 3). However, the number of people qualifying for marketplace subsidies is similar across the two sets of states, as more people live in expansion states. Three states that have not expanded Medicaid, including Texas, Georgia, and Florida, account for 30% of people who become marketplace tax credit eligible nationally in May 2020. Assuming unemployment extends into 2021 when UI benefits would likely expire for most families, the proportion eligible for Medicaid would increase in expansion states while non-expansion states may see more nonelderly adults moving into the Medicaid coverage gap (Figure 4; Appendix Table 2).
Figure 3: May 2020 Eligibility for ACA Coverage among People Becoming Uninsured Due to Loss of Employer-Sponsored Insurance, by State Medicaid Expansion StatusFigure 4: January 2021 Eligibility for ACA Coverage among People Becoming Uninsured Due to Loss of Employer-Sponsored Insurance, by State Medicaid Expansion Status
Nearly 7 million people losing ESI and becoming uninsured are children, and the vast majority of them are eligible for coverage through Medicaid or CHIP. Within the 26.8 million people losing ESI and becoming uninsured in May 2020, 6.1 million are children. Because Medicaid/CHIP income eligibility limits for children are generally higher than they are for adults, the vast majority of these children are eligible for Medicaid/CHIP in May 2020 (5.5 million, or 89%) or January 2021 (5.8 million, or 95%).
Discussion
Given the health risks facing all Americans right now, access to health coverage after loss of employment provides important protection against catastrophic health costs and facilitates access to needed care. Unemployment Insurance filings continue to climb each week, and it is likely that people will continue to lose employment and accompanying ESI for some time, though some of them will return to work as social distancing curbs are loosened. The ACA expanded coverage options available to people, and we estimate that the vast majority of people who lose ESI due to job loss will be eligible for ACA assistance either through Medicaid or subsidized marketplace coverage. However, some people will fall outside the reach of the ACA, particularly in January 2021 when UI benefits cease for many and some adults fall into the Medicaid coverage gap due to state decisions not to expand coverage under the ACA.
Both ACA marketplace subsidies and Medicaid are counter-cyclical programs, expanding during economic downturns as people’s incomes fall. In return for additional federal funding to help states finance their share of Medicaid cost during the public health crisis, states must maintain eligibility standards and procedures that were in effect on January 1, 2020 and must provide continuous eligibility through the end of the public health emergency, among other requirements. These provisions may help eligible individuals enroll in and maintain Medicaid, particularly in light of state and federal actions prior to the crisis to increase eligibility verification requirements or transition people off Medicaid.
Our estimates only examine eligibility among people who lost ESI due to job loss and potentially became uninsured. Additional uninsured individuals—including some of the 9% of the 78 million individuals in families where someone lost employment—may also be eligible for Medicaid or subsidized coverage. It is possible that contact with state UI systems may lead them to seek and enroll in coverage, even if they were eligible for financial assistance before job loss but uninsured.
It is unclear whether people losing ESI and becoming uninsured will enroll in new coverage. We did not estimate take-up or enrollment in coverage options but rather only looked at eligibility for coverage. Even before the coronavirus crisis, there were millions of people eligible for Medicaid or marketplace subsidies who were uninsured. Eligible people may not know about coverage options and may not seek coverage; others may apply for coverage but face challenges in navigating the application and enrollment process. Still others may find marketplace coverage, in particular, unaffordable even with subsidies. As policymakers consider additional efforts to aid people, expanding outreach and enrollment assistance, which have been reduced dramatically by the Trump Administration, could help people maintain coverage as they lose jobs.
This is the first economic downturn during which the ACA will be in place as a safety net for people losing their jobs and health insurance. The Trump Administration is arguing in case before the Supreme Court that the ACA should be overturned; a decision is expected by next Spring. The ACA has gaps, and for many the coverage may be unaffordable. However, without it, many more people would likely end up uninsured as the U.S. heads into a recession.
Appendix
Appendix Table 1: May 2020 Eligibility for Coverage Among People Becoming Uninsured due to Job Loss
State
Total Uninsured Due to ESI Loss
Medicaid Eligible
Coverage Gap
Tax Credit Eligible
Ineligible for Financial Assistance due to Income, ESI Offer, or Citizenship
US Total
26,789,000
12,735,000
149,000
8,350,000
5,555,000
Alabama
425,000
107,000
14,000
246,000
57,000
Alaska
58,000
41,000
–
9,000
7,000
Arizona
452,000
314,000
–
73,000
66,000
Arkansas
169,000
95,000
–
47,000
28,000
California
3,427,000
2,068,000
–
701,000
659,000
Colorado
299,000
149,000
–
73,000
77,000
Connecticut
247,000
135,000
–
47,000
65,000
Delaware
76,000
46,000
–
15,000
14,000
DC
55,000
47,000
–
1,000
7,000
Florida
1,418,000
301,000
34,000
835,000
248,000
Georgia
1,444,000
376,000
24,000
775,000
268,000
Hawaii
200,000
104,000
–
63,000
33,000
Idaho
113,000
66,000
–
29,000
18,000
Illinois
846,000
469,000
–
199,000
178,000
Indiana
606,000
386,000
–
126,000
94,000
Iowa
251,000
127,000
–
76,000
49,000
Kansas
230,000
60,000
3,000
121,000
46,000
Kentucky
598,000
330,000
–
166,000
102,000
Louisiana
450,000
335,000
–
63,000
52,000
Maine
99,000
50,000
–
30,000
19,000
Maryland
369,000
220,000
–
72,000
78,000
Massachusetts
621,000
277,000
–
89,000
255,000
Michigan
1,211,000
774,000
–
219,000
218,000
Minnesota
535,000
264,000
–
79,000
192,000
Mississippi
218,000
54,000
6,000
130,000
28,000
Missouri
480,000
125,000
10,000
269,000
76,000
Montana
71,000
41,000
–
18,000
13,000
Nebraska
101,000
56,000
–
28,000
16,000
Nevada
434,000
254,000
–
85,000
95,000
New Hampshire
144,000
84,000
–
31,000
29,000
New Jersey
883,000
456,000
–
152,000
274,000
New Mexico
100,000
59,000
–
23,000
17,000
New York
1,471,000
880,000
–
291,000
300,000
North Carolina
723,000
167,000
13,000
408,000
134,000
North Dakota
53,000
23,000
–
16,000
14,000
Ohio
1,002,000
531,000
–
267,000
204,000
Oklahoma
310,000
75,000
5,000
177,000
53,000
Oregon
276,000
143,000
–
76,000
58,000
Pennsylvania
1,543,000
836,000
–
341,000
366,000
Rhode Island
134,000
75,000
–
21,000
38,000
South Carolina
403,000
111,000
5,000
225,000
62,000
South Dakota
32,000
8,000
–
17,000
7,000
Tennessee
417,000
136,000
4,000
210,000
67,000
Texas
1,608,000
328,000
30,000
881,000
370,000
Utah
162,000
92,000
–
45,000
24,000
Vermont
48,000
26,000
–
12,000
10,000
Virginia
533,000
306,000
–
125,000
102,000
Washington
835,000
426,000
–
150,000
259,000
West Virginia
130,000
82,000
–
29,000
18,000
Wisconsin
446,000
214,000
–
150,000
82,000
Wyoming
31,000
8,000
1,000
16,000
7,000
NOTES: Medicaid eligible includes people eligible for other public coverage. Totals may not sum due to rounding.SOURCE: KFF. See Methods for more details.
Appendix Table 2: January 2021 Eligibility for Coverage Among People Becoming Uninsured due to Job Loss
State
Total Uninsured Due to ESI Loss
Medicaid Eligible
Coverage Gap
Tax Credit Eligible
Ineligible for Financial Assistance due to Income, ESI Offer, or Citizenship
US Total
26,789,000
16,791,000
1,924,000
6,184,000
1,890,000
Alabama
425,000
151,000
115,000
138,000
21,000
Alaska
58,000
45,000
–
10,000
3,000
Arizona
452,000
332,000
–
91,000
30,000
Arkansas
169,000
118,000
–
41,000
10,000
California
3,427,000
2,541,000
–
597,000
289,000
Colorado
299,000
217,000
–
57,000
26,000
Connecticut
247,000
175,000
–
47,000
25,000
Delaware
76,000
54,000
–
17,000
5,000
DC
55,000
50,000
–
2,000
3,000
Florida
1,418,000
418,000
351,000
528,000
120,000
Georgia
1,444,000
545,000
398,000
408,000
94,000
Hawaii
200,000
145,000
–
39,000
16,000
Idaho
113,000
84,000
–
23,000
6,000
Illinois
846,000
619,000
–
161,000
66,000
Indiana
606,000
455,000
–
121,000
31,000
Iowa
251,000
182,000
–
57,000
12,000
Kansas
230,000
88,000
52,000
75,000
16,000
Kentucky
598,000
454,000
–
117,000
26,000
Louisiana
450,000
353,000
–
78,000
20,000
Maine
99,000
68,000
–
26,000
4,000
Maryland
369,000
268,000
–
68,000
33,000
Massachusetts
621,000
456,000
–
102,000
63,000
Michigan
1,211,000
933,000
–
218,000
61,000
Minnesota
535,000
394,000
–
107,000
34,000
Mississippi
218,000
77,000
58,000
75,000
8,000
Missouri
480,000
166,000
119,000
168,000
27,000
Montana
71,000
55,000
–
14,000
3,000
Nebraska
101,000
72,000
–
23,000
6,000
Nevada
434,000
331,000
–
64,000
39,000
New Hampshire
144,000
109,000
–
27,000
8,000
New Jersey
883,000
647,000
–
153,000
82,000
New Mexico
100,000
74,000
–
20,000
5,000
New York
1,471,000
1,112,000
–
258,000
101,000
North Carolina
723,000
233,000
178,000
261,000
52,000
North Dakota
53,000
37,000
–
13,000
3,000
Ohio
1,002,000
738,000
–
211,000
53,000
Oklahoma
310,000
114,000
74,000
103,000
19,000
Oregon
276,000
203,000
–
53,000
20,000
Pennsylvania
1,543,000
1,161,000
–
295,000
87,000
Rhode Island
134,000
98,000
–
26,000
10,000
South Carolina
403,000
139,000
99,000
141,000
24,000
South Dakota
32,000
11,000
7,000
12,000
2,000
Tennessee
417,000
149,000
86,000
157,000
25,000
Texas
1,608,000
540,000
382,000
530,000
157,000
Utah
162,000
123,000
–
29,000
10,000
Vermont
48,000
34,000
–
12,000
2,000
Virginia
533,000
382,000
–
110,000
42,000
Washington
835,000
637,000
–
140,000
58,000
West Virginia
130,000
98,000
–
27,000
5,000
Wisconsin
446,000
296,000
–
124,000
26,000
Wyoming
31,000
13,000
6,000
10,000
2,000
NOTES: Medicaid eligible includes people eligible for other public coverage. Totals may not sum due to rounding.SOURCE: KFF. See Methods for more details.
Methods
Methods and Definitions
This analysis uses our ACA eligibility model as applied to the 2018 American Community Survey as a baseline for all calculations. We rely on these calculations to assess the ACA eligibility of a cohort of workers prior to the pandemic (early 2020), during the pandemic (mid-2020), and in the following calendar year (early 2021). Assessing both insurance coverage changes and ACA eligibility at three time points might help policymakers understand both the immediate coverage needs of the population losing jobs due to the pandemic and the longer-term eligibility of the same population assuming they continue without wages into 2021.
In order to estimate the 2020 population within each state, we linearly extrapolated 2020 state population estimates based on 2018 and 2019 population estimates from the U.S. Census Bureau to determine a population increase factor between 2018 and 2020 within each state. We then applied this multiplier to the weight of each individual in the microdata to approximate state population sizes in mid-2020 rather than mid-2018. With the exception of this population multiplier, our baseline estimates (described in this brief as “May 2020”) align with other Kaiser Family Foundation products such as our ACA eligibility estimates of the uninsured population.
We summed initial unemployment insurance claims filed across the weeks ending March 7th, 2020 thru May 2nd, 2020 using the Department of Labor’s Employment & Training Administration state-specific statistics to arrive at a nationwide total job loss through early May of approximately 31 million workers. We also assumed unauthorized immigrants in the labor force lost employment proportionally without filing for unemployment. We did not make assumptions about other people losing jobs but not filing for unemployment insurance.
Within each state, we estimated who lost employment using sampling probabilities based on recent labor force changes by industry recorded by the March 2020 Current Population Survey. For example, leisure and hospitality workers appear more than five times as likely as agricultural workers to have lost a job in March 2020, and these relative probabilities guided sampling of who has become unemployed. We controlled to state unemployment totals (approximately 31 million nationally) for the citizen and legally-present immigrant population, and we separately controlled to state proportional unauthorized labor force unemployment estimate for the undocumented working population.
The American Community Survey does not distinguish between ESI policyholders and those covered as dependents. For all full-time workers losing jobs in our sample, we assumed a family-wide loss of ESI for all people who held ESI if there were no other workers present who both worked at least 30 hour weeks and earned at least $50,000 during the year. If a spouse with wage of at least $50,000 and weekly average hours over 30 were present within the family, we assumed the spouse held the policy (or another policy) and maintained ESI for the entire family. For part-time workers losing jobs, we assumed a family-wide loss of ESI only when no other workers were present within the family.
We calculated an industry-specific distribution of weekly state unemployment benefit payments from the 2019 Current Population Survey. We then applied a weekly state dollar amount onto most individuals who lost employment according to a random deviate sample using a gamma distribution. After adding unemployment benefit payments onto family income of those imputed to lose jobs, we then scaled each individual weekly payment to account for state-specific generosity using the Department of Labor’s 2018Q4 “Benefits Paid for Total Unemployment divided by Weeks Compensated for Total Unemployment” state-specific estimate divided by the nationwide average of $361.29. This nationwide weekly average amount matched our CPS-based calculated average. For any individuals imputed to receive a higher weekly state unemployment payment than the state maximum, we capped the imputed amount at the state maximum.
Medicaid eligibility is based on current monthly income. To calculate Medicaid eligibility immediately after job loss, we zeroed out wage and self-employment income for people who lost jobs and calculated monthly family income as a share of poverty based on other family income and the state weekly unemployment benefit. Following Medicaid eligibility policy, we did not include the Federal weekly supplemental unemployment payments of $600 in the Medicaid eligibility determination.
ACA marketplace subsidy eligibility is based on estimated annual income. To calculate ACA Marketplace subsidy eligibility immediately after job loss, we removed a share of annualized wages and self-employment income in proportion to the calendar week of job loss. For example, calendar year earned income for individuals imputed to lose jobs during the week of March 7th, 2020 were reduced by 75%. We also counted the receipt of Federal supplemental unemployment insurance payments of $600 for 17 weeks and multiplied the same imputed weekly state unemployment benefit by the maximum allowable weeks.
To re-calculate both Medicaid and ACA Marketplace subsidy eligibility for 2021, we assumed an exhaustion of both the state and Federal unemployment benefit amounts, no return to work among job losers, and counted only other income in the family.
Although our job loss imputation only edited the earned income and public assistance income of the individual worker, that worker’s income changes affect the Medicaid and marketplace tax credit eligibility of family members. Therefore, many statistics throughout this brief present the eligibility dynamics of Americans with any job loss in their family rather than solely the worker.
Medicaid/Other Public Eligible: Includes adults and children who were previously eligible for Medicaid and the Children’s Health Insurance Program (CHIP) but not enrolled as well as those newly eligible after job loss. Also includes some state-funded programs for immigrants otherwise ineligible for Medicaid.
Tax Credit Eligible: Includes individuals who are not eligible for other coverage, such as Medicaid or Employer-Sponsored Insurance (ESI), and who have incomes between 100% and 400% of the federal poverty level (FPL). This number also includes legally residing immigrants with incomes below the poverty level who do not qualify for Medicaid because they have lived in the U.S. for less than five years. Tax credit-eligible population in Minnesota and New York include uninsured adults who are eligible for coverage through the Basic Health Plan.
Ineligible for Financial Assistance due to Income, ESI Offer, or Citizenship: Includes individuals with incomes above 400% FPL and those with an offer of coverage from an employer (though we cannot determine whether the offer of ESI would be considered affordable under the ACA, which would make the individual ineligible for a premium tax credit). This number also includes undocumented immigrants who are barred from purchasing coverage through the Marketplace even without financial assistance.
In the Coverage Gap: Includes uninsured adults in states that have not expanded Medicaid and have incomes above the state’s Medicaid eligibility level (which, in many cases, is 0% FPL for adults without dependent children) but below the poverty, leading them to earn too much to qualify for Medicaid but not enough to qualify for tax credits. Adults in the coverage gap would be eligible for Medicaid if their state expanded under the ACA.
Endnotes
Medicaid already covers many workers, and Medicaid beneficiaries who lose their jobs and income will retain their Medicaid coverage, as there is no lower floor on income eligibility for Medicaid. ↩︎
Notably, eligibility for marketplace subsidies (but not Medicaid) includes the new federal supplemental unemployment insurance benefits recently enacted by Congress for people affected by COVID-19. This supplemental benefit could lead some unemployed low-wage workers who previously were in the “coverage gap” (income below poverty but above state Medicaid limits) to have income above poverty, making them newly eligible for Marketplace subsidies. ↩︎
People who were uninsured while working may be able to enroll in marketplace coverage if they live in a state with a state-run marketplace, most of which have re-opened enrollment to allow residents to obtain marketplace coverage if eligible. However, people who were uninsured while working and live in one of the 32 states that use the federal marketplace do not qualify for a “special enrollment period” to enroll in coverage through the federal marketplace. ↩︎
Millions of people are losing jobs due to the coronavirus pandemic and seeking financial assistance through Unemployment Insurance (UI) programs. While UI can provide an important source of temporary assistance for many people losing jobs, there have been reports of major challenges accessing UI benefits. Although many of these challenges stem from the inability of outdated systems to handle the large influx of applications, people may also face other challenges accessing benefits, such as lack of awareness of eligibility and difficulty completing the application and enrollment process, including providing required documentation. Over time, states have significantly streamlined Medicaid and the Children’s Health Insurance Program (CHIP) application and enrollment processes to overcome many similar challenges to connect eligible people to health insurance coverage. As such, previous experience enrolling individuals into Medicaid and CHIP can provide lessons learned that could help inform efforts to connect people to UI. This brief summarizes some key lessons learned and discusses how states could potentially apply these lessons to UI.
Unemployment Insurance
UI is a federal-state system that helps many people who have lost their jobs by temporarily replacing part of their wages while they seek work. States administer the program, within broad federal guidelines under oversight provided by the Department of Labor. To qualify for UI, a person must have lost a job through no fault of his or her own; be able to work, available to work, and actively seeking work; and have earned at least a certain amount of money during a base period prior to becoming unemployed. Within these broad requirements, states have substantial flexibility to establish eligibility criteria and benefit levels. The Coronavirus Aid, Relief, and Economic Security Act (CARES) expanded UI eligibility and benefits. It provides a $600 weekly federal supplement (available through July 31) to state unemployment benefits and extends the period for receiving unemployment benefits by up to 13 weeks. The Act also extends benefits to many types of workers (e.g., self-employed) who are not eligible for unemployment benefits under state laws.
Over half (55%) of working adults have lost a job or income due to the coronavirus pandemic, and a record 33 million people filed for UI between mid-March and April 25, 2020. However, reports describe UI application processing systems lacking capacity to process the recent surge in UI applications, leading to crashed websites and jammed phone lines, as well as delays in updates to UI systems to reflect the expanded eligibility and benefits provided under the CARES Act. Beyond systems-related problems, individuals may face other challenges accessing UI. For example, individuals may not know they are eligible for UI, particularly if they are not aware of the eligibility expansions under the CARES Act. Individuals also may have difficulty completing the UI application and providing necessary documentation, and there may be high demand for enrollment assistance since many people may be applying for UI for the first time and most will be applying from home due to social distancing policies. A recent survey finds that for every ten people who said they successfully filed for UI during the previous for weeks, three to four additional people tried to apply but could not get through the system to make a claim and two additional people did not try to apply because it was too difficult to do so.
Lessons from Medicaid and CHIP
States have taken an array of actions to help connect eligible people to Medicaid and CHIP coverage that may help inform efforts to connect people to UI. After the passage of CHIP, many states streamlined enrollment processes and conducted outreach and enrollment campaigns to promote enrollment of eligible children. The Affordable Care Act expanded coverage and built on previous state experience with CHIP by establishing streamlined and modernized enrollment processes across all states. Further, some states are taking additional steps to streamline Medicaid and CHIP enrollment in response to COVID-19.
Outreach and Enrollment Assistance
Previous Medicaid and CHIP experience showed that outreach and enrollment assistance were instrumental for making people aware of coverage options and helping them apply. Following implementation of the ACA, federal and state mass marketing campaigns helped raise awareness of coverage options. In addition, one-on-one assistance provided through trusted individuals was key to helping eligible individuals enroll. The federal government and states funded navigators and enrollment assistors to help individuals enroll. Many of these navigators and assisters were associated with community-based organizations. Utilizing trusted individuals within the community to provide outreach and enrollment assistance was particularly important for connecting with harder-to-reach populations and those who need more assistance, including individuals with limited English proficiency.
Outreach and enrollment assistance could be similarly helpful to connect eligible people to UI. This experience suggests that broad marketing campaigns could help raise awareness of expanded UI assistance. Further, it points to the importance of increasing the availability of assistance as demand for UI grows, especially phone-based or online assistance since most people will be applying from home. It also suggests that states may want to explore how they can work with community-based organizations to share information about eligibility for UI and provide enrollment assistance.
Streamlined Enrollment Processes
The ACA established streamlined eligibility and enrollment processes across all states. For example, it eliminated certain requirements, such as face-to-face interviews and asset tests for most groups. It also required states to provide multiple application options, including online, phone, mail, or in-person, and to use available data to verify information when possible. States have additional options to facilitate enrollment, including shortening and simplifying applications, relying on self-attestation of eligibility criteria when possible, and providing presumptive eligibility to individuals while the state completes processing of their application. Some states are taking additional steps to facilitate enrollment of eligible people in response to the COVID-19 outbreak, including further shortening applications, allowing for self-attestation of additional eligibility criteria, and expanding use of presumptive eligibility.
UI programs could draw on these state experiences by simplifying application and eligibility determination processes. UI programs typically require applicants to file claims with documents showing income eligibility (e.g., having a minimum amount of earnings for a number of weeks employed prior to filing) as well as non-monetary eligibility (including the reason for separating from work, availability for work, immigration documents, and/or forms for some jobs where the employers are exempt from paying into the UI program). Some states require a one-week waiting period to receive benefits, meaning that the second week claimed is the first week of payment. After being determined eligible for benefits, individuals will file continuing claims generally every 1-2 weeks, depending on the state, to document that the individual is still searching for work, among other requirements. Previous Medicaid and CHIP experience suggests that states could help facilitate access to UI by reducing these requirements. For example, a number of states have waived the one-week waiting period for benefits and waived or relaxed work search requirements. States could also explore options to shorten and simplify the application for benefits and expand use of self-attestation of eligibility criteria. States also could explore similar presumptive eligibility policies as Medicaid and CHIP to make an initial determination of eligibility and begin paying benefits based on limited information while they work through backlogs to complete verification and review of claims.
Coordination or Integration with Other Programs
All state systems coordinate enrollment in Medicaid, CHIP, and the Marketplace coverage, and many states coordinate Medicaid and CHIP enrollment with non-health programs. In half of states, individuals can use a single application to apply for Medicaid and other programs, such as food or cash assistance, and most of these states process eligibility determinations for these programs through a single system. In states that do not have an integrated application or system, eligibility workers can still refer people to apply for other programs. This integration and coordination helps facilitate access to across programs for eligible individuals.
UI programs could coordinate or integrate enrollment with other programs. Most state UI programs coordinate with other workforce programs, such as job training or placement agencies, but the extent to which UI is coordinated with other assistance programs is unclear. Broader coordination across programs and agencies could facilitate access to UI as well as other assistance programs. For example, states could take action to ensure revenue agencies can share 1099 tax filing information with UI programs to facilitate processing of applications for independent contractors and self-employed workers, who became newly eligible under the CARES Act. Coordination between UI and Medicaid, as well as the Affordable Care Act marketplaces, could be particularly helpful in facilitating access to coverage since many people losing job-based insurance will be eligible under those programs based on their UI benefits.
System Upgrades
Nearly all states have upgraded or replaced their Medicaid eligibility systems to implement the new processes established under the ACA. The ACA provided states enhanced federal funding to support eligibility system upgrades. It took many states years to upgrade or build new systems, and many are still refining and improving them. Medicaid and CHIP system upgrades have increasingly enabled states to use automated enrollment processes that rely on electronic data matches with other data sources, allowing eligible individuals to connect to coverage quickly and easily and reducing administrative burdens on states. Most states report that system upgrades and modernized processes have contributed to improvements in eligibility and enrollment operations compared to before the ACA.
System upgrades could help address the significant challenges many people are facing accessing UI benefits, especially since a number of states are still relying on outdated systems, but it will require significant time and investment to implement upgrades. In the interim, some states are gating access to systems, for example, by only allowing applicants to file on certain days based on the first letter of their last name. Waiving or reducing requirements to document work search activities may also reduce stress on systems. Some states have also redirected resources and staff to process applications. State UI programs have received federal grants to upgrade systems, but not a sustained federal match for costs.
Conclusion
UI offers an important source of temporary assistance to help people losing jobs as a result of the COVID-19 outbreak. The CARES Act expanded UI benefits to enhance this support. However, many people are facing significant challenges accessing UI benefits. Many of these challenges reflect limitations of outdated systems. However, people may face other challenges, including lack of awareness of eligibility for benefits and difficulty completing application and enrollment processes. Lessons learned from Medicaid and CHIP can help inform state efforts to address these challenges.
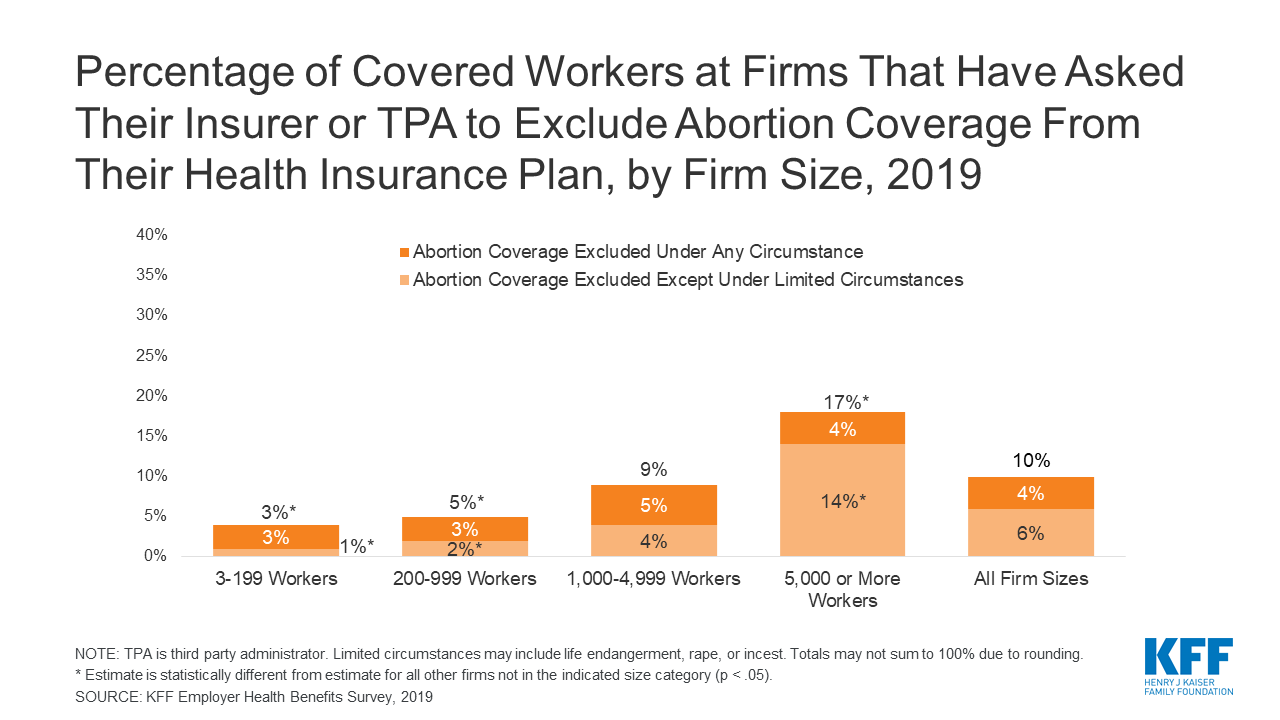
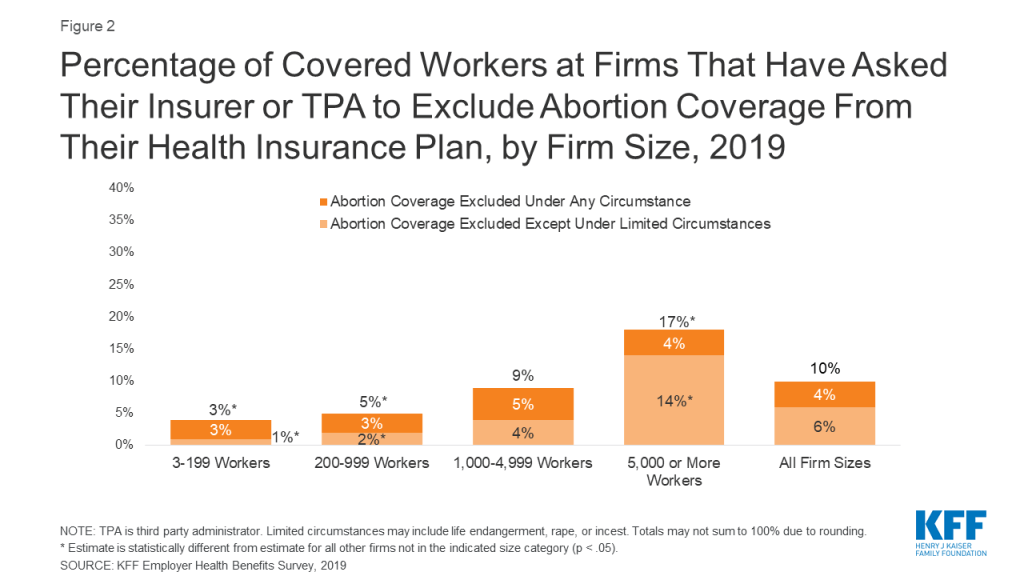
New analysis of KFF’s 2019 Employer Benefits Survey finds that 10% of workers covered by employer-sponsored health insurance are employed at a firm that has asked their insurer or third party administrator to exclude abortion coverage from their health plan. Employer-sponsored coverage is the primary source of health benefits in the U.S., covering 153 million Americans.
Four percent of covered workers are employed at firms that exclude coverage of abortion under any circumstance and 6% are employed at firms that exclude abortion coverage except under some limited circumstances. Covered workers at the largest firms are more likely to work at a firm that excludes abortion coverage than those at smaller firms. Lack of coverage means that people seeking abortion services must fully bear the cost of their abortion, which on average is around $500.
Overall, 3% of firms that offer health benefits reported that they exclude coverage of abortion in some or all circumstances. Employers who do not explicitly exclude abortion coverage may not necessarily include coverage, and some employers with abortion coverage may not cover it in all circumstances.
Congress is considering including COBRA subsidies in its next coronavirus relief package to help workers who lose their jobs keep their employer coverage. One of the sticking points of the debates has reportedly been whether or not the legislation will include a stipulation that federal funds cannot be used to pay for abortion coverage. Given that many employers do not know whether their plan covers abortion, this restriction could pose some logistical hurdles to implementation or restrictions on abortion coverage.
About 153 million Americans rely on employer-sponsored health insurance.1 The specific benefits and services covered by those plans are shaped by many factors including costs, employer policies and beliefs, as well as state and federal regulations. A recent increase in legislative efforts at the state level to limit coverage of abortion, including in private insurance plans, could leave more women without coverage for abortion. This gap in plan benefits could have considerable financial consequences for women seeking abortion services, particularly for those who are low-income.
In addition, there are discussions in Congress about including funds in the next Coronavirus relief package to subsidize COBRA premiums for workers who lost their jobs during the COVID-19 pandemic. One of the sticking points of the debates has been whether or not the legislation will include a stipulation that federal funds cannot be used to pay for abortion coverage in employer plans, which could have implications for coverage of abortion in employer plans and the logistics of a COBRA subsidy.
This issue brief presents data from the 2019 KFF Employer Health Benefits Survey on the share of covered workers who are employed by firms that have asked their insurer or third party administrator to exclude coverage for abortion from their health plan.
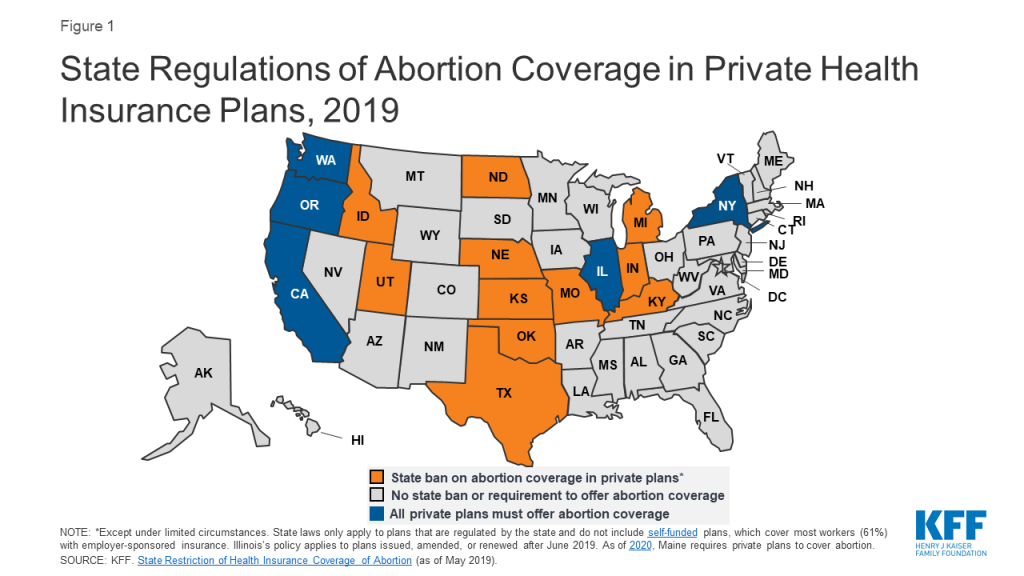
State Regulation of Abortion Coverage in Private Plans
Eleven states ban state-regulated private plans from including abortion coverage; most – but not all – have exceptions for pregnancies resulting from rape or incest or in cases in which it poses a threat to the life of the pregnant woman. Conversely, a handful of states have enacted policies that require coverage of abortion services in state-regulated private plans (Figure 1). However, neither the state-level abortion coverage inclusion or prohibition requirements apply to self-funded plans sponsored by private employers, which are exempt from most state insurance laws. Self-funding is common among larger employers. In total, about three out of five covered workers (59%) at private-sector firms are enrolled in a self-funded plan.2
Figure 1: State Regulations of Abortion Coverage in Private Health Insurance Plans, 2019
In all states (except those where abortion coverage is mandatory for fully-insured plans), employers may choose not to offer coverage for abortion, or only to cover it under limited circumstances such as in cases of rape or incest or life endangerment of the pregnant person (much like the federal law under the Hyde Amendment).
The lack of abortion coverage means that women must directly bear the full cost of the abortion. The cost of an abortion varies by the type of procedure, the location of the provider, and how far along in pregnancy it is performed. One study found that in 2011 and 2012, the average charge was $558 for a surgical abortion and $527 for a medication abortion at 10 weeks gestation. Abortions later in pregnancy can cost thousands of dollars. These costs can make abortion prohibitive for many people. According to a 2017 KFF poll, about one-third of individuals with employer-sponsored insurance (34%) would not be able to pay an unexpected medical bill of $500.
Employer Health Benefits Survey
KFF conducted the annual Employer Health Benefits Survey between January and July of 2019. It included 2,012 randomly-selected, non-federal public and private firms with three or more employes. The 2019 survey asked firms that offer health insurance: “Has your firm asked your insurer or TPA3 [third party administrator] to exclude abortion coverage from your health plan?” For more information on the survey methodology, see the Survey Design and Methods section.
At the firm level, 3% of firms that offer health benefits exclude coverage of abortion in at least some circumstances from their plan. While there are more than three million firms in the United States, most covered workers are employed by a relatively small number of firms.4 At the worker level, 10% of covered workers work at a firm that excludes coverage for abortion under some or all circumstances. This includes 4% of covered workers at firms that exclude coverage of abortion under any circumstance and 6% of covered workers at firms that exclude coverage of abortion except under some limited circumstances (which may include life endangerment, rape, or incest). It is important to note that although an employer may not have excluded abortion coverage, the plan may still not cover it. This is likely the case in states that ban abortion coverage in state-regulated plans.
Exclusion of abortion coverage varies by firm size (Figure 2). Covered workers at the largest firms (5,000 or more workers) are more likely (17%) than those at smaller firms to work at a firm that excludes coverage for abortion in at least some circumstances. Only 3% of small firms (3-199 workers) and 5% of moderately sized firms (200-999 workers) specifically requested any exclusion of abortion coverage from their plan.
Figure 2: Percentage of Covered Workers at Firms That Have Asked Their Insurer or TPA to Exclude Abortion Coverage From Their Health Insurance Plan, by Firm Size, 2019
Exclusion of abortion coverage also varies by other firm characteristics such as ownership structure, plan funding, and firm wage level (Figure 3). Covered workers at private-not-for-profit firms (18%) are more likely than those at private for-profit firms (6%) to work at a firm that excludes coverage for abortion under some or all circumstances. Private not-for-profit firms include many large health care and educational institutions that have religious affiliations, some of which are opposed to abortion and limit insurance coverage of it in their health plans. There were approximately 1.56 million non-profits registered with the IRS5 in 2015, but they do not collect uniform information on whether non-profits are religiously-affiliated. Thirteen percent of covered workers at public employers, such as state and local governments, restrict abortion coverage in at least some circumstances. In 2019, 20 states had bans on inclusion of abortion in their public employee insurance plans except in limited circumstances; two states had bans on abortion coverage under all circumstances. While not included in the survey, health plans for federal employees follow the Hyde Amendment rule that excludes coverage of abortion except in cases of rape, incest, or life endangerment.
Figure 3: Percentage of Covered Workers at Firms That Have Asked Their Insurer or TPA to Exclude Abortion Coverage From Their Health Insurance Plan, by Firm Characteristics, 2019
Covered workers at firms with a completely or partially self-funded plan (14%) are more likely than those at firms with a fully-insured plan (3%) to work at firm that excludes abortion coverage under at least some circumstances. Self-funded plans established by private employers (but not public employers) are exempt from most state insurance laws, including reserve requirements, mandated benefits, premium taxes, and many consumer protection regulations. Self-funding is common among larger firms because they can spread the risk of costly claims over a large number of workers and dependents. The survey did not ask the specific reason(s) the firm chose to self-fund their plan.
Discussion
Employer-sponsored health insurance is the primary source of health benefits in the U.S., covering 153 million Americans. Ten percent of covered workers are employed at a firm that has asked to exclude abortion from their health plan in least some circumstances. This percentage does not include the more than 20 million federal employees, veterans, military personnel, and dependents whose health plans contain the Hyde amendment rule excluding coverage for abortion except in limited circumstances. It also does not include private sector employees (and their dependents) whose employer did not ask for an exclusion but that reside in a state that bans abortion coverage in state-regulated plans.
Additionally, plans that do cover abortion may have restrictions on the situations in which they will pay for it, including limits on gestational age, number of abortions covered, or the method of abortion. This has been the case in individual plans that are available in some of the ACA Marketplaces in states that have not fully banned abortion coverage in private plans.
It is important to note that the survey did not ask if the firm’s plan includes abortion coverage. When this question was asked in prior years, a sizeable share of employers did not know whether their plan included coverage for abortion. In light of the extensive job loss resulting from the coronavirus pandemic, Congress is considering legislation to subsidize COBRA premiums to help unemployed and furloughed people afford to remain on their employer’s health insurance. Media reports have noted that there is bipartisan support for the subsidies, but disagreement over whether there should be a ban on subsidies that pay for abortion coverage in plans, citing the Hyde Amendment ban on federal funding of abortion. Uncertainty over whether or not an employer plan covers abortion could pose logistical challenges to the implementation of this legislation should it restrict or limit funds to health plans that include abortion coverage.
Employer-sponsored health insurance is the primary source of coverage for millions of workers in the U.S. Gaps in coverage of services effectively means that workers and their families may be required to bear the cost of that medical care. For the many workers and dependents who lack abortion coverage, these costs can translate into hundreds or thousands of dollars out-of-pocket for abortion services, placing a financial barrier to this service, particularly for low-wage workers.
This estimate excludes state and local government employees. While federal law (the Employee Retirement Income Security Act of 1974, or ERISA) generally exempts self-funded plans from state insurance regulations, states do have jurisdiction over the plans offered to state and local employees. ↩︎
A TPA is an administrator or insurer that provides administrative services such as claims management, commonly for self-funded plans. ↩︎
Some of the non-profits registered with the IRS have fewer than three employees. Only firms with at least three employees are included in the KFF Employer Health Benefits Survey. ↩︎
While use of telemedicine in the U.S. had been minimal prior to COVID-19, interest in and implementation of telemedicine has expanded rapidly during the crisis, as policymakers, insurers and health systems have looked for ways to deliver care to patients in their homes to limit transmission of the novel coronavirus. With growing demand for telemedicine, several changes have been made to telehealth policy, coverage and implementation, in order to make telemedicine more widely accessible during this state of emergency.
The federal government has focused on loosening restrictions on telehealth in the Medicare program, including allowing beneficiaries from any geographic location to access services from their homes. HHS has waived enforcement of HIPAA for telemedicine, while the DEA has loosened requirements on e-prescribing of controlled substances.
On a state level, many state governments have focused on expanding telehealth in their Medicaid programs, as well relaxing state-level restrictions around provider licensing, online prescribing and written consent. Many states are also mandating fully-insured private plans to cover and reimburse for telemedicine services equally to how they would for in-person care (service parity and payment parity).
Meanwhile, many commercial insurers have voluntarily addressed telemedicine in their response to COVID-19, focusing on reducing or eliminating cost sharing, broadening coverage of telemedicine and expanding in-network telemedicine providers.
Health systems have rapidly adapted to implement new telehealth programs or ramp up existing ones. This requires significant financial and workforce investment, which may be more difficult for smaller or less-resourced practices. Actions to rapidly expand telemedicine could come with tradeoffs, including concerns over privacy and quality of care.
A number of gaps remain in ensuring access to telemedicine during the COVID-19 pandemic. Service parity and payment parity for telehealth across all insurers would help increase access for patients and incentivize providers to offer these services, though it would also increase spending. Gaps in technology access and use among some groups of patients may also be a concern. It remains unclear if the U.S. will sustain this expanded use of telemedicine after the state of emergency ends, and to what extent low-income patients and patients with limited experience with or access to technology will be able to access these services.
Introduction
As clinicians seek new ways to serve patients and stem the rapid spread of the novel coronavirus in the United States, policymakers and insurers have looked to telemedicine or telehealth to provide care to patients in their homes. At a time when many people in the U.S. are under shelter in place orders, this approach to care allows patients to maintain social distancing, reduce their risk of exposure to the novel coronavirus and potentially avoid overburdening emergency departments and urgent care centers at this time. After many years of slow growth, telemedicine use has exploded across the nation in a few short weeks. The telemedicine landscape is complex, with many moving pieces as different players respond to COVID-19. The federal government has taken actions to broaden and facilitate the use of telemedicine, particularly though Medicare. States, health systems, and insurance carriers have also moved with unprecedented speed to shift many visits that were previously done in person to a telemedicine platform. This brief presents some of the many policy changes that have taken place in the field of telehealth by the federal government, state governments, commercial insurers and health systems in just the few short weeks since the COVID-19 outbreak hit the U.S. We highlight key considerations in achieving widespread implementation of telemedicine services during this pandemic and beyond, including easing of telemedicine regulations, broadening insurance coverage, strengthening telecommunications infrastructure, and patient facing issues like connectivity and quality of care.
What is telemedicine?
While varied definitions for telemedicine or telehealth exist, it is commonly defined as the remote provision of health care services using technology to exchange information for the diagnosis, treatment and prevention of disease. Telemedicine is usually defined narrowly by insurers to include technologies like live videoconference and remote patient monitoring, while telehealth is often defined more broadly, to include basic telecommunication tools, as simple as phone calls, text messages, emails, or more sophisticated online health portals that allow patients to communicate with their providers. However, telehealth and telemedicine are often used interchangeably.
Telemedicine can enable providers to deliver health services to patients at remote locations, by conducting “virtual visits” via videoconference or phone (Figure 1). During a telemedicine visit, a patient may see providers from their usual source of care, like Stanford Health, Kaiser Permanente, or Mount Sinai, or they may interact with providers employed by a stand-alone telemedicine platform like Amwell or Virtuwell. Telemedicine can also enable remote interactions and consultations between providers.
Figure 1: Telemedicine Can Facilitate a Broad Range of Interactions Using Different Devices and Modalities
How widespread was telemedicine use before COVID-19?
Before the onset of the COVID-19 pandemic, utilization of telemedicine in the U.S. was minimal. Telemedicine growth has been limited by lack of uniform coverage policies across insurers and states, and hurdles to establishing telemedicine in health systems (e.g. high startup costs, workflow reconfiguration, clinician buy-in, patient interest). The Peterson-KFF Health System Tracker analyzed a sample of health benefit claims from the IBM MarketScan Commercial Claims and Encounters Database; among enrollees in large employer health plans with an outpatient service, 2.4% had utilized at least one telehealth service in 2018 (up from 0.8% in 2016). Similarly, utilization of telemedicine by traditional Medicare and Medicaid and beneficiaries enrolled in managed care plans had been trending upward, but remained low.
How is telemedicine being used during the COVID-19 pandemic?
During the COVID-19 pandemic, there are multiple scenarios in which patients and providers are utilizing telemedicine to enable remote evaluations between a patient and a provider, while respecting social distancing. (Figure 2). Use of “virtual visits” via phone or videoconference can address non-urgent care or routine management of medical or psychiatric conditions, while online or app-based questionnaires can facilitate COVID-19 screening to determine the need for in-person care.
Figure 2: Telemedicine Is Being Used in Many Scenarios during the COVID-19 Pandemic
Many hospitals have instructed patients with suspected coronavirus symptoms or exposure to call their doctors or turn to telemedicine first, before showing up to the emergency room or urgent care visit. The Cleveland Clinic, University of Washington (UW), NYU Langone, Oregon Health Sciences University (OHSU), Intermountain Health Care, Medical University of South Carolina (MUSC), and Rush University Medical Center are all advising patients with suspected coronavirus to start by using a virtual visit or online screening, rather than presenting to an emergency room for testing. This is in line with the Centers for Disease Control and Prevention (CDC) encouragement that those who are mildly ill should call their doctors before seeking in-person care. For patients who are having more severe symptoms (e.g. difficulty breathing) or with complex comorbidities, evaluation from their home via telemedicine may not be appropriate, as in-person care intervention may be needed.
What measures have been taken so far to expand telehealth access in the U.S.?
In response to the novel coronavirus, demand for telemedicine is rapidly increasing. Telemedicine, what was once a niche model of health care delivery, is now breaking into the mainstream in response to the COVID-19 crisis. In China, telemedicine platform JD Health saw a tenfold increase in their services during the outbreak and is now providing nearly 2 million online visits per month. In the U.S., existing telemedicine platforms like Amwell and UPMC’s virtual urgent care have reported rapid increases in their utilization. A recent poll found 23% of adults have used telehealth services in light of the COVID-19 pandemic.
There are a myriad of telemedicine laws and regulations determine who can deliver which telemedicine services to whom, in what location, in what fashion, and how they will be reimbursed. The federal government regulates reimbursement and coverage of telemedicine for Medicare and self-insured plans, while Medicaid and fully-insured private plans are largely regulated on a state-by-state basis (Figure 3). This complexity in the regulatory framework for telemedicine creates challenges for patients in knowing what services are covered, and for providers in knowing what regulations to abide by.
Figure 3: Who Regulates Telemedicine in Health Plans?
As the COVID-19 pandemic evolves, so too are the emergency policies regarding telemedicine. The federal government, some states, and some health insurance carriers are trying to enable more telemedicine visits to be permitted and paid for. It is important to note that even when the federal government announces loosening of telemedicine restrictions that states have their own regulations and laws that shape coverage in state-regulated (fully insured) insurance plans and Medicaid. And even when regulations are temporarily lifted to facilitate telemedicine, health systems and patients will have their own challenges in implementing and accessing these services. While many of the telemedicine regulations have been temporarily relaxed, for telemedicine to be more broadly accessible to patients in the U.S. over the long term, several actions would need to happen (Figure 4). Next, we outline what changes have been made to telehealth policy and implementation by the federal government, state governments, commercial insurers and health systems in response to the COVID-19 emergency, as well as what gaps remain.
Figure 4: Actions to Expand Telemedicine Availability During the COVID-19 Pandemic
Federal Changes to Telehealth Policy
The federal government dictates several facets of telehealth policy, including nationwide patient privacy laws (e.g. HIPAA), federal prescribing laws for controlled substances, grant funding for telehealth initiatives and Medicare coverage of telehealth. In response to the COVID-19 emergency to make telemedicine more widely available, the federal government has taken action in all these domains.
HIPAA
Typically telemedicine platforms are required to comply with regulations under the Health Insurance Portability and Accountability Act (HIPAA), which health organizations and providers must follow to protect patient privacy and health information. However, on March 17, 2020 the U.S. Department of Health and Human Services (HHS) issued an announcement stating that, “Effective immediately… [HHS] will exercise enforcement discretion and will waive potential penalties for HIPAA violations against health care providers that serve patients in good faith through everyday communications technologies during the COVID-19 nationwide public health emergency.” This now allows widely accessible services like FaceTime or Skype to be used to telemedicine purposes, even if the service is not related to COVID-19. Potential concerns to this approach include the possibility that protected health information (PHI) that is discussed or sent over a non-HIPAA compliant platform may be accessed, shared or even sold by these platforms. The National Consortium of Telehealth Resource Centers (NCTRC) currently urges health centers to sign a Business Associate Agreement (BAA) with their chosen platform, to agree that the data exchanged are safeguarded. In addition to HIPAA, many states have their own laws and regulations to protect patient health information. Loosening enforcement of HIPAA will likely not impact state level regulations, meaning states would need to lift or loosen their own health information laws. Some states (e.g. CA, ME, MD, NM, ND, UT) have issued guidance to relax state-specific privacy standards for telehealth during the state of emergency.
Federal oversight of Controlled substances
Under the Controlled Substances Act, the Drug Enforcement Agency (DEA) normally requires an in-person evaluation before a provider can prescribe a controlled substance, limiting telemedicine’s use for e-prescribing of controlled substances without a prior in-person patient-provider relationship. However, during a state of national emergency, there are exceptions to this rule. For the duration of the COVID-19 public health emergency, DEA-registered providers can now use telemedicine to issue prescriptions for controlled substances to patients without an in-person evaluation, if they meet certain conditions. One of these conditions is that provider must still comply with state laws; many states have their own laws regulating telemedicine and controlled substances, which federal changes would not affect.
Medicare
Changes to Traditional Medicare: Based on new waiver authority included in the Coronavirus Preparedness and Response Supplemental Appropriations Act (and amended by the CARES Act), the HHS Secretary has waived certain restrictions on Medicare coverage of telehealth services for traditional fee-for-service (FFS) Medicare beneficiaries during the coronavirus public health emergency (first issued on January 31, 2020, and renewed on April 21, 2020). The waiver does the following: lifts the requirement that beneficiaries must live in rural areas in order to receive telehealth services, meaning beneficiaries in any geographic area could receive telehealth services; allows the patient’s home to qualify as an “originating site” from which they can access telehealth visits; allows telehealth visits to be delivered via smartphone with real-time audio/video interactive capabilities in lieu of other equipment; and removes the requirement that providers of telehealth services have treated the beneficiary in the last three years. A separate provision in the CARES Act allows federally qualified health centers (FQHCs) and rural health clinics (RHCs) to serve as “distant site” providers, and provide telehealth services to Medicare beneficiaries during the COVID-19 emergency period (Figure 5).
Figure 5: Key Changes to Coverage Restrictions for Medicare Fee-for-Service During the COVID-19 Emergency
CMS has also expanded access to the types of services that made be provided via audio-only telephones. In a March 2020 Interim Final Rule, CMS stated that it would allow providers to “evaluate beneficiaries who have audio phones only.” In a subsequent announcement, CMS broadened this to include behavioral health services and patient education services, but still not the full range of telehealth services that can be provided using two-way audio-video connection. This limits telehealth’s reach for Medicare beneficiaries without access to smartphones or other video communications. Other modifications to telehealth availability in response to the COVID-19 emergency include allowing both home health agencies and hospice providers to provide some services via telehealth, and allowing certain required face-to-face visits between providers and home dialysis and hospice patients to be conducted via telehealth. Additionally, CMS is temporarily waiving the Medicare requirement that providers be licensed in the state they are delivering telemedicine services when practicing across state lines, if a list of conditions are met. This change however, does not exempt providers from state licensure requirements (see section below on state licensing actions). Medicare is also temporarily expanding the types of providers who may provide telehealth services.
Importantly, these expanded telehealth services under Medicare are not limited to COVID-19 related services, rather they are available to patients regardless of diagnosis and can be used for regular office visits, mental health counseling, and preventive health screenings. Separate from the time-limited expanded availability of telehealth visits, traditional Medicare also covers brief, “virtual check-ins” via telephone or captured video image, and E-visits, for all beneficiaries. These visits are more limited in scope than a full telehealth visit.
Medicare covers all types of telehealth services under Part B, so beneficiaries in traditional Medicare who use these benefits are subject to the Part B deductible of $198 in 2020 and 20 percent coinsurance, although many beneficiaries have some source of supplemental coverage that helps pay their share of costs. However, the HHS Office of Inspector General is providing flexibility for providers to reduce or waive cost sharing for telehealth visits during the COVID-19 public health emergency.
Changes to Medicare Advantage: Medicare Advantage plans have been able to offer additional telehealth benefits not covered by traditional Medicare and have flexibility to waive certain requirements with regard to coverage and cost sharing in cases of disaster or emergency, such as the COVID-19 outbreak. In response to COVID-19, CMS has advised plans that they may waive or reduce cost sharing for telehealth services, as long as plans do this uniformly for all similarly situated enrollees. This guidance, however, is voluntary and plans will vary in their responses to this new flexibility.
Federal Funding for telehealth
The newly passed Coronavirus Aid, Relief, and Economic Security (CARES) Act includes additional funding to the Telehealth Network Grant Program (TNGP). This program currently awards a total of $8.7 million a year for telehealth technologies used in rural areas and medically underserved areas. The act strikes the current funds, and replaces it with $29 million for five years, starting in 2021. The bill also ends funding for the Telehealth Resource Center (TRC) Grant Program, which is currently funding TRCs at roughly $4.6 million a year for four years, since 2017.
State Changes to Telehealth Policy
A significant portion of telehealth policy is decided by state governments. Each state has its own laws regarding provider licensing, patient consent for telehealth and online prescribing laws. Importantly, states also are in charge of deciding which telehealth services will be covered by their Medicaid program, and most states also have laws governing reimbursement for telemedicine in full-insured private plans. Changes to state level regulations in response to COVID-19 are described next.
Licensing laws
Normally, clinicians must be licensed to practice in states where they offer telemedicine services, and states regulate which health professionals are credentialed to practice in their state. For example, if a clinician is located in California, but is providing services remotely to a patient in Oregon via telemedicine, the provider must be licensed in Oregon, the state where the patient is located. Nine states require special licenses specific to telemedicine. Others participate in “compacts” that allow providers in participating states an expedited process to practice in other compact states. However, to address COVID-19, out of state clinicians may be needed to conduct virtual visits with patients in states with the highest burden of cases. This requires they be licensed to practice across state lines. Almost all states are moving to temporarily waive out of state licensing requirements, so that providers with equivalent licenses in other states can practice via telehealth. The Federation of State Medical Boards is tracking these updates, and finds that currently 49 states have issued waivers regarding licensure requirements during the COVID-19 emergency.
STate Specific Online prescrIbing laws
Most states require a patient-provider relationship be established before e-prescribing of medications. Many telemedicine platforms use an online health questionnaire to establish that relationship, but in at least 15 states, this method is considered inadequate. Instead, a physical exam would be required before prescribing, either in-person, by live-video, or by a referring physician, depending on the state. For patients who are now turning to telemedicine visits rather than their usual source of in-person care, clinicians in some states may face legal barriers to online prescribing medications if they do not already have a pre-existing relationship with the patient. Many states are issuing emergency orders to remove in-person requirements before engaging in telehealth, for the duration of the public health emergency (e.g. AK, AZ, AR, DE, HI, IA, KS, KY, LA, MD, MS, MT, OH, OK, SD).
Consent Laws
Thirty-eight states and DC require providers to obtain and document informed consent from patients before engaging in a telehealth visit. In some states, this applies only to Medicaid beneficiaries, but in others this applies to all telehealth encounters regardless of payor. In most states, verbal consent is allowed, but in a minority of states, consent must be obtained in writing. In response to COVID-19, some state Medicaid programs that would normally require written consent have waived this requirement; for example, providers caring for Medicaid beneficiaries in Alabama, Delaware, Georgia, and Maine can now obtain verbal consent for telemedicine, rather than having the patient sign a written consent form.
Private Insurers and Employer Plans
As of Fall 2019, 41 states and D.C. had laws governing reimbursement for telemedicine services in fully-insured private plans, but private insurer laws enacted by states vary widely. In approximately half of states, if telemedicine services are shown to be medically necessary and meet the same standards of care as in-person services, state-regulated private plans must cover telemedicine services if they would normally cover the service in-person, called “service parity.” However, fewer states require “payment parity,” meaning telemedicine services to be reimbursed at the same rate as equivalent in-person services. CCHP finds only 6 states (CA, DE, GA, HI, MN, NM) that required payment parity prior to COVID-19, while a KFF analysis of telehealth laws suggests an additional 4 states followed payment parity as well (AR, CO, KY, NJ). In the remaining states, telemedicine is typically reimbursed at lower rates than equivalent in-person care. In response to COVID-19, more and more states are enacting service and payment parity requirements for fully-insured private plans. For example, at least 16 states are requiring payment parity for telehealth during the public health emergency.
In contrast to fully-insured health plans which must comply with both federal and state requirements, self-insured health plans are regulated by the federal government through the Department of Labor. These plans may cover telemedicine, but each plan can choose to cover these services or not. Prior analysis shows that the majority of large employer plans, including those that are self-insured, cover some telemedicine services.
Medicaid
Telehealth Policy Before the COVID-19 Emergency: The use of telehealth in the Medicaid program has grown as states have sought to address barriers to care including insufficient provider supply (especially specialists), transportation barriers, and rural access challenges. Historically, states have had broad flexibility to determine whether to cover telehealth/telemedicine, which services to cover, geographic regions telehealth may be used, and how to reimburse providers for these services. Prior to COVID-19, all states and DC provided some coverage of telehealth in Medicaid FFS but the definition and scope of coverage varied from state to state. The most commonly covered modality of telehealth was live video. Few states permitted “audio-only” telephone care to qualify as a telehealth service. Additionally, only 19 state FFS Medicaid programs allowed patient’s to access telemedicine from their homes (e.g. home was not an eligible “originating site”), limiting telemedicine’s reach for many low income people. Of note, state telehealth policies may differ between Medicaid FFS and managed care, an important distinction given most Medicaid beneficiaries are now in managed care plans. A study of Medicaid claims data showed beneficiaries enrolled in Medicaid managed care plans were more likely than those in FFS programs to use telemedicine.
Policy Changes in Response to COVID-19: In response to the COVID-19 outbreak, CMS issued guidance reiterating states can use existing flexibility to provide coverage for telehealth services: “States have broad flexibility to cover telehealth through Medicaid, including the methods of communication (such as telephonic, video technology commonly available on smart phones and other devices) to use.” They clarify, “No federal approval is needed for state Medicaid programs to reimburse providers for telehealth services in the same manner or at the same rate that states pay for face-to-face services.” The FAQ guidance also discusses how telehealth and telephonic services can be covered for FQHCs and rural health centers (RHCs) and under managed care contracts, if states choose to do so.
Almost all states are issuing emergency policies in response to the COVID-19 outbreak to make telehealth services more widely available in their Medicaid FFS programs and/or through Medicaid managed care plans. Importantly, most states are newly allowing both FFS and managed care Medicaid beneficiaries to access services from their home, and most are directing Medicaid plans to allow for reimbursement for some telephone evaluations. Many states are newly allowing FQHCs and RHCs to serve as distant site providers, and expanding which professions qualify as eligible to provide telehealth services through Medicaid.
States are also using 1915(c) Appendix K waivers to enable the provision of home and community-based services (HCBS) remotely by telehealth for people with disabilities and/or long-term care needs. Using Section 1135 waivers all 50 states and DC are relaxing licensing laws, many allowing out-of-state providers with equivalent licensing to practice in their state. Additionally, Medicaid programs in 46 states and DC have issued guidance to expand coverage or access to telehealth during this crisis, while 38 states and DC have granted payment parity for at least some telehealth services as of May 5, 2020. Despite most states moving to expand Medicaid coverage of telehealth services, these changes are not uniform across states, and barriers to implementing and accessing telehealth more broadly are likely to remain during this emergency. KFF is tracking other state Medicaid actions to address COVID-19, found here.
Voluntary Changes to Telehealth by Commercial Insurers
When not mandated by the state, private insurers are free to decide which telehealth services their plans will cover. Therefore, changes to telehealth benefits as a result of COVID-19 vary by insurer. Several major health insurance companies have voluntarily expanded telehealth coverage for fully-insured members (Appendix). Many insurers are reducing or eliminating cost sharing for telemedicine, for a limited period of time. For some plans this applies only to telehealth visits related to COVID-19, while for others this applies to any health indication. Some insurers are expanding their coverage of telehealth benefits, allowing more services, patient locations (e.g. home) and modalities (e.g. phone) to qualify for coverage. To make these services more readily accessible to patients, some insurers are working to increase their numbers of in-network telehealth providers within their existing networks of care, while others are contracting with specific telehealth vendors to provide these services. For example, First Choice Health will waive cost-sharing for telehealth if care is delivered via the 98point6 platform, and Oscar will do so if delivered by the Doctor on Call service. Florida Blue and Prominence Health Plan will waive copays for telehealth if using the Teladoc platform (Appendix). Therefore, patients may not be able to talk to their usual providers, if restricted to certain telehealth platforms by their insurance provider. Insurers responding to the novel coronavirus allow self-insured plans greater flexibility compared to fully insured plans in implementing these new changes, providing an opt-out or opt-in option.
Health System Changes to Telehealth
Prior to the start of the COVID-19 outbreak, more than 50 U.S. health systems already had telemedicine programs in place, including large health centers like Cleveland Clinic, Mount Sinai, Jefferson Health, Providence, and Kaiser Permanente. Meanwhile an estimated 15% of physicians had used telemedicine to facilitate interactions with their patients. However, many health systems did not have existing telemedicine infrastructure, and many providers are novices to providing care through telemedicine. As health systems and smaller practices implement or ramp up use of telemedicine in response to this crisis, there are many provider facing and patient facing considerations to address. Health systems will need to decide whether to invest in telemedicine infrastructure for long-term use, or if they are looking for shorter term, potentially cheaper, solutions solely to respond to this acute crisis.
Provider Facing Considerations
Investing in Telecommunications Infrastructure
For those wishing to initiate a telemedicine program before the COVID-19 emergency, significant financial and personnel investment was typically required. Costs included hiring programmers to create a telemedicine platform, ideally one that integrates into an existing electronic health record, protects patient privacy, and can charge for visits if needed. Alternatively, health systems could contract with existing telemedicine platforms to provide these services. In a 2019 study by Definitive Healthcare, many outpatient practices reported not investing in telehealth due to these financial barriers.
With new telehealth flexibility and relaxation of privacy laws in response to COVID-19, some of these financial hurdles may be lessened. For example, providers can now use phone calls, or affordable technologies like Facetime and Zoom, for many patient encounters, at least for the time being. If and when the regulatory environment around telehealth and HIPAA becomes more stringent, however, providers will need to decide whether to invest in more robust telemedicine platforms to continue to provide these services. This may be beyond what is feasible for many smaller practices, or less-resourced clinics.
During the COVID-19 crisis, ensuring reliable internet connection, and sound and video quality on both the patient and provider end remains important for any telehealth interaction. One concern is that resource limited health organizations may not have sufficient bandwidth to achieve this. During the current outbreak, many telemedicine platforms are experiencing high volumes of patients trying to access care online which has resulted in IT crashes and long wait times to obtain a virtual appointment in some systems. Investing in IT personnel may be necessary to troubleshoot problems with telehealth visits.
Workflow and Training
Implementing new telemedicine initiatives in response to COVID-19 oftentimes requires a redesign of longstanding clinical care models. With expanding use of telemedicine in clinical settings, health systems need to decide which providers they will divert to phone lines and/or video visits and how to manage their patient flow, while still ensuring enough staff to manage in-person care. This means some telemedicine platforms may need to hire more clinicians in order to keep up with demand. While larger health systems may have the financial resources to do this, smaller and more rural practices may be stretched thin as it is. Whether it be doctors, advance practice clinicians like nurse practitioners and physicians’ assistants, or registered nurses who facilitate telemedicine interactions, all will need to be trained on telemedicine technologies, requiring additional time and resources.
Malpractice and Liability Insurance
Clinicians must ensure their malpractice or liability insurance covers telemedicine, and if needed, that it covers services provided across state lines. Hawaii is the only state to require malpractice carriers to offer telemedicine coverage, and insurance premiums may be higher if covering telemedicine. During the COVID-19 outbreak, there are many clinicians who are first-time users of telemedicine, who must ensure they are covered before providing services.
Patient Facing Considerations
Access to Technology
Access to telemedicine may be particularly challenging for low-income patients and patients in rural areas, who may not have reliable access to internet through smartphones or computers. A KFF study showed that in 2017, sizable shares of non-elderly adults with Medicaid reported they had never used a computer (26%), did not use the internet (25%) and did not use email (40%). Additionally, a study by the Harvard School of Public Health showed that 21% of rural Americans reported access to high-speed internet is a problem for them or their family. Telemedicine solutions may also be less feasible for seniors. Because older patients are at higher risk for severe symptoms of coronavirus and in general require more frequent primary care, they may benefit greatly from telehealth to reduce in-person risk of exposure. However, many seniors may not feel comfortable or be able to use these technologies. According to Pew Research Center, 27% of U.S. adults aged 65+ reported they did not use the internet in 2019. Based on the results of a March 2020 KFF Health Tracking Poll, nearly seven in 10 adults 65 and older (68%) say they have a computer, smart phone or tablet with internet access at home (compared to virtually all adults ages 30-49 and 85% of adults ages 50-64). However, this may not translate to widespread use of telehealth among older adults, particularly when Medicare’s expansion of telehealth services for people in traditional Medicare is at the moment limited to the duration of the public health emergency. While studies show some interest in telehealth among older individuals, concerns include perceived poorer quality of care, privacy issues and difficulty using technology.
Quality of Care
While use of telehealth has opened the door for patients to maintain access to care during this public health crisis, ensuring quality of care of telehealth visits is still important. There are some inherent differences to evaluating patients remotely from their homes compared to in-person. For patients with possible coronavirus infection, taking a thorough history via telemedicine is relatively straightforward, including reviewing symptoms, travel history and exposure history. However, taking important vital signs like a temperature and oxygen saturation proves challenging, particularly if the patient does not have a thermometer or pulse oximeter at home. Without specialized equipment, providers also cannot listen to a patient’s lungs to assess for signs of pneumonia. Further, currently almost all coronavirus testing is happening in person, although the FDA recently approved the first at-home test. While a limited telemedicine assessment may be adequate to determine if a patient needs to present to an emergency room/urgent care or for testing, there are the limitations of telemedicine care for this purpose.
For patients utilizing telemedicine during the COVID-19 emergency for non-respiratory complaints, virtual evaluation may prove challenging as well. For example, if a pregnant person wishes to use telemedicine for a prenatal care visit to reduce their virus exposure, monitoring routine measurements like blood pressure, weight and fetal heart rate will prove challenging if not already set up to do so at home. If a patient needed to buy home monitoring equipment like a blood pressure cuff or a glucose monitor, it remains unclear if this would be paid for by the patient out of pocket, or by the health system.
What more could be done to expand and sustain access to telemedicine during the COVID-19 pandemic and beyond?
In response to the unprecedented pressure to expand services and control the transmission of the novel coronavirus, the federal government, many states governments and commercial insurers are expanding coverage of telemedicine and relaxing existing regulations. The federal government has focused on broadening telemedicine access for Medicare beneficiaries, and waiving enforcement of HIPAA to enable use of video platforms like Facetime and Skype. Many states have relaxed telemedicine written consent, licensing, and online prescribing laws, while expanding coverage in Medicaid and fully-insured private plans. Meanwhile, many health centers have rapidly redesigned their existing models of care to implement telemedicine.
While these unprecedented and swift measures have been taken to broaden telemedicine access during this pandemic, gaps in coverage and access to telemedicine remain. Coverage and reimbursement of telemedicine is still far from uniform between payors, and most changes to telehealth policy are temporary. If the U.S. wishes to invest in telemedicine over the longer term, more permanent measures may need to be taken. Avenues to consider to further expand telemedicine access include:
Ensuring service parity and payment parity for telemedicine care as compared to in-person care, to help expand covered services for patients, and incentivize clinicians to provide this model of care
Ensuring patients can access telemedicine services from their homes (home as “originating site”), to further enable social distancing practices
Allowing use of audio-only phone for telemedicine visits, to help ensure access for patients who do not have live-video technology
Investing in telecommunications infrastructure for less-resourced sites of care, and ensuring internet access to patients in rural areas. This may involve providing direct funding for health systems and smaller practices to implement telemedicine
There are potential trade-offs in loosening regulations on telemedicine, including privacy issues and quality of care. Depending on the insurer, some patients may be able to engage in telemedicine visits with their usual providers, while some may have to see providers from specific telemedicine vendors, outside of their usual source of care. This could create discrepancies in access and continuity of care. Additionally, expanding coverage of telemedicine may result in increasing health spending, if patients use telehealth in addition to in-person care, rather than as a substitute. With all these factors in mind, it will be up to policymakers, payors, and providers to determine if the changes made to telehealth policy in light of COVID-19 outweigh the potential concerns, if they should remain permanently, and if telemedicine helps enable accessible, quality health care.
Appendix
Commercial Insurers Make Changes to Telehealth Policies in Response to COVID-19(Updated 4/15/2020)
Temporary changes made by commercial insurers:
Reducing cost-sharing for covered telehealth services
Medical Mutual of Ohio: Allowing coverage of telephonic visits (without live video) during the current state of emergency
Increasing provider availability via telemedicine
Anthem: Increasing physician availability through its service, LiveHealth Online (LHO). Encouraging in-network doctors to join the platform
Florida Blue: Expanding network of primary care doctors and specialists who are able to treat patients virtually
Magellan Health: Permitting all credentialed and contracted behavioral health providers to conduct telehealth video sessions
Premera Blue Cross: Signed agreements with telemedicine platforms (98point6 and Doctor on Demand) to increase services for at least 90 days
Expanding eligible patient location
Viva Health: Members can access telehealth from any location, with any in-network physician, nurse practitioner or physician assistant
Reimbursement for telehealth
Aetna: Reimbursing for telemedicine at same rate as in-person visits (payment parity)
NOTES: This does not constitute a full list of private insurers who have changed their telehealth policies in response to COVID-19. Many new policies are time-limited, only apply to full insured members, and may change as the pandemic evolves.
SOURCE: AHIP. Health Insurance Providers Respond to Coronavirus (COVID-19). Updated April 15, 2020.