Introduction
KFF estimates that nearly 6 million people receive Medicaid long-term services and supports (LTSS) for assistance with activities of daily living (such as eating, bathing, and dressing) and instrumental activities of daily living (such as preparing meals, managing medication, and housekeeping). LTSS are provided to people who need such services because of aging, chronic illness, or disability and may be provided in institutional settings such as nursing facilities (1.6 million people) or in people’s homes and the community (4.2 million people). This analysis examines the characteristics of Medicaid enrollees who use LTSS, how enrollees who use LTSS differ from those who do not use LTSS, and how enrollees who use different types of LTSS differ from each other. For details on methods, please see KFF’s previous data note, which described the number of people who use LTSS and how much Medicaid spends on those people.
Key takeaways include:
- Age, Sex, and Race: Over half (56%) of Medicaid enrollees who use LTSS broadly are under 65, but the age distribution varies by type of service. Most enrollees who use Medicaid home- and community-based services (HCBS) are under age 65, while most enrollees who use institutional LTSS are ages 65 and older. Among enrollees who use LTSS, males are generally younger than females. Over twice as many males are under the age of 18 compared with females (16% vs. 8%). Just over half (51%) of all Medicaid enrollees who use LTSS are White, 19% are Black, and 14% are Hispanic.
- Eligibility Group: Over two-thirds (70%) of enrollees who use LTSS and are under 65 qualify for Medicaid because of a disability. The Affordable Care Act (ACA) Medicaid expansion has expanded access to LTSS: 1 in 5 enrollees under 65 who use institutional LTSS and 1 in every 10 enrollees under 65 who use Medicaid HCBS are eligible for Medicaid through the ACA expansion.
- Medicare Coverage: 62% of Medicaid enrollees that use LTSS are also enrolled in Medicare, and the share is higher among those who use institutional LTSS (79%) compared with those who use HCBS (56%).
- Health Conditions: Enrollees who use LTSS are much more likely to be diagnosed with ongoing health conditions than enrollees who do not use LTSS, with the highest rates of diagnoses among older enrollees who use institutional LTSS.
What are the demographic characteristics of Medicaid enrollees who use LTSS?
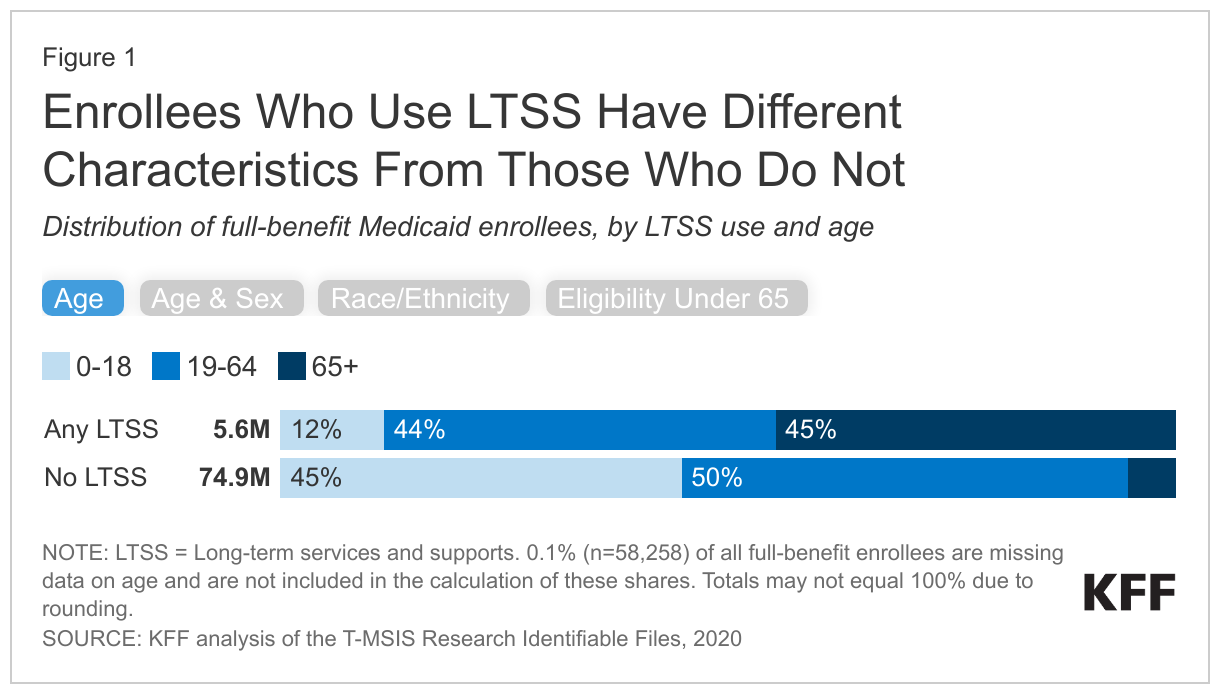
Over half (56%) of Medicaid enrollees who use LTSS are under 65, but those who use LTSS are still older than those who do not use LTSS (Figure 1). LTSS are commonly associated with people ages 65 and older, but many younger enrollees use LTSS because of chronic illness or disability. The remaining 45% of enrollees who use LTSS are 65 and older. In comparison, only 5% of Medicaid enrollees who do not use LTSS are ages 65 and older.
Male Medicaid enrollees who use LTSS are more likely to be under 65 and twice as likely to be under 18 as female enrollees who use LTSS (Figure 1). The younger age distribution of males may be related to higher rates of diagnoses of intellectual and developmental disabilities among young boys than among young girls. Male enrollees who use LTSS may also be younger than female enrollees who use LTSS since women generally live longer than men.
Medicaid enrollees who use LTSS are more likely to be White and less likely to be Hispanic compared to those who don’t use LTSS (Figure 1). These data are from the 31 states that reported “low/medium concern” data quality levels with their race and ethnicity data in 2020. People who are White comprise just over half (51%) of all Medicaid enrollees who use LTSS, but only 39% of enrollees who don’t use LTSS. People who are Hispanic comprise just 14% of all Medicaid enrollees who use LTSS, but 25% of enrollees who don’t use LTSS. This pattern may, in part, reflect differences in age distribution across racial and ethnic groups, with over half (53%) of Hispanic enrollees under age 19 compared with 37% of White enrollees (data not shown). The share of enrollees who are Black is similar among those who use LTSS and those who do not (19% and 20% respectively).
Just over two-thirds (70%) of people who use Medicaid LTSS and are under age 65 qualify for Medicaid because of a disability (Figure 1). Among Medicaid enrollees under age 65 who do not use LTSS, only 12% are eligible for Medicaid because of a disability. The remaining 30% of enrollees who use LTSS are eligible through the child eligibility group, the Affordable Care Act (ACA) expansion group, or through another adult eligibility group.
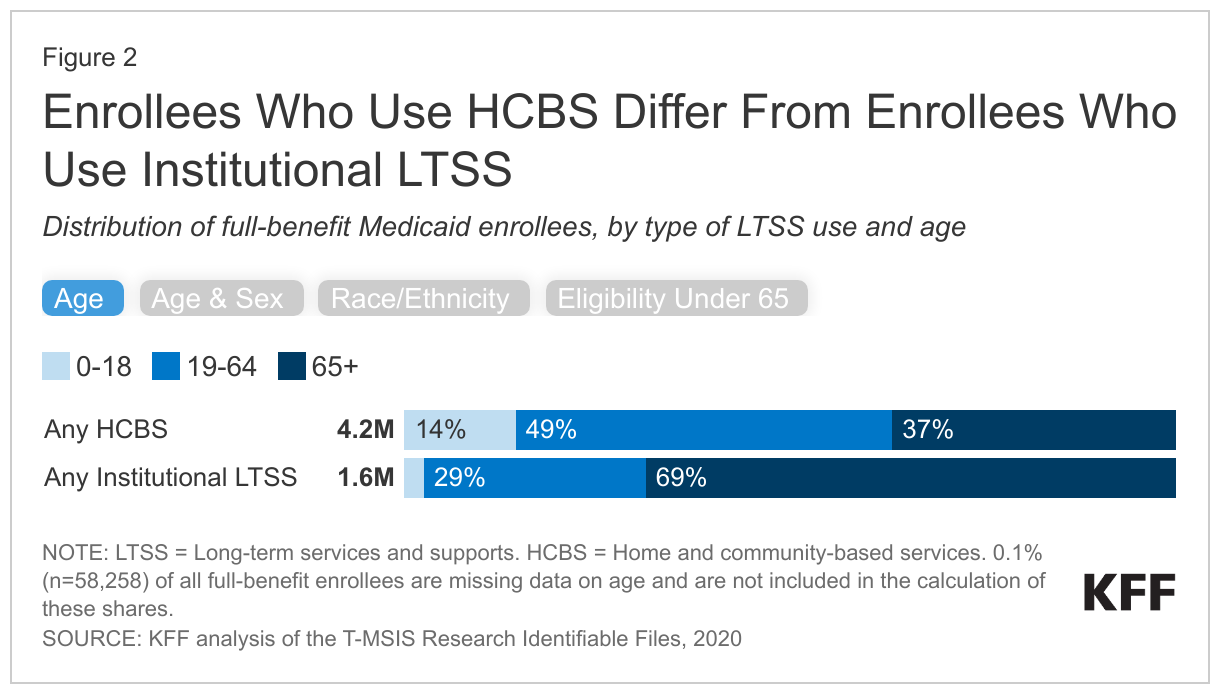
Enrollees who use Medicaid HCBS are more likely to be younger, Black or Hispanic, and receive Medicaid because of a disability when compared to enrollees who use institutional LTSS (Figure 2). There are notable differences in the characteristics of people who use HCBS and institutional LTSS. Among people who use HCBS, 14% are under age 19, and 49% are ages 19-64, whereas over two-thirds of people who use institutional LTSS are ages 65 and older. Among both groups, females who use LTSS have an older age distribution than males who use the same type of LTSS. Enrollees who use HCBS are more likely to be Black or Hispanic (36%) than enrollees who use institutional LTSS (24%). People who are White comprise 47% of people who use HCBS but 64% of people who use institutional LTSS. These differences likely reflect to the younger age distribution of Hispanic enrollees who use any LTSS: 19% of Hispanic enrollees who use LTSS are ages 0-18 compared with 10% of White enrollees (data not shown). Among both enrollees who use institutional LTSS or HCBS, most people under the age of 65 are eligible for Medicaid because of a disability, but the percentage of people eligible for Medicaid through an ACA expansion is 10% among people who use HCBS and 20% among people who use institutional LTSS.
What share of Medicaid enrollees who use LTSS are also enrolled in Medicare?
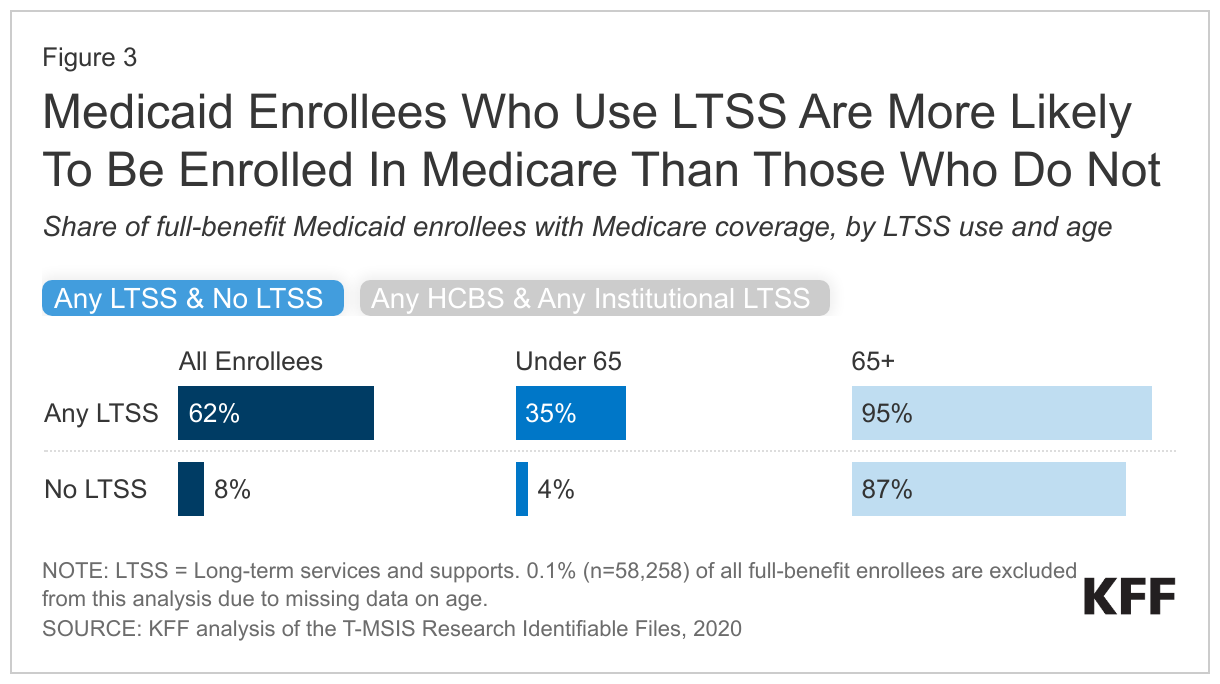
Most (62%) Medicaid enrollees who use LTSS are also enrolled in Medicare (“dual-eligible individuals”) (Figure 3). Only 8% of Medicaid enrollees who don’t use LTSS have Medicare. The high rate of Medicare coverage among Medicaid enrollees who use LTSS reflects the older age distribution of enrollees who use LTSS and high rates of eligibility for Medicaid based on a disability. To be eligible for Medicare, people must generally be ages 65 and older, or have a disability that qualifies them for the federal disability insurance program (people in that program are only eligible for Medicare after a 2-year waiting period). Nearly all enrollees over age 65 are enrolled in Medicare regardless of whether they use LTSS. Enrollees under 65 who use LTSS have higher rates of Medicare coverage when compared to those who do not use LTSS (35% compared with 4%).
The percentage of enrollees with Medicare is higher among those who use institutional LTSS (79%) compared with those who use HCBS (56%) (Figure 3). 34% of enrollees who are under 65 and use HCBS also have Medicare coverage, compared to 40% of enrollees who are under 65 and use institutional LTSS. Nearly all enrollees over 65 who use either HCBS or institutional LTSS have Medicare coverage.
What share of Medicaid enrollees who use LTSS have a diagnosis of at least one ongoing health condition?
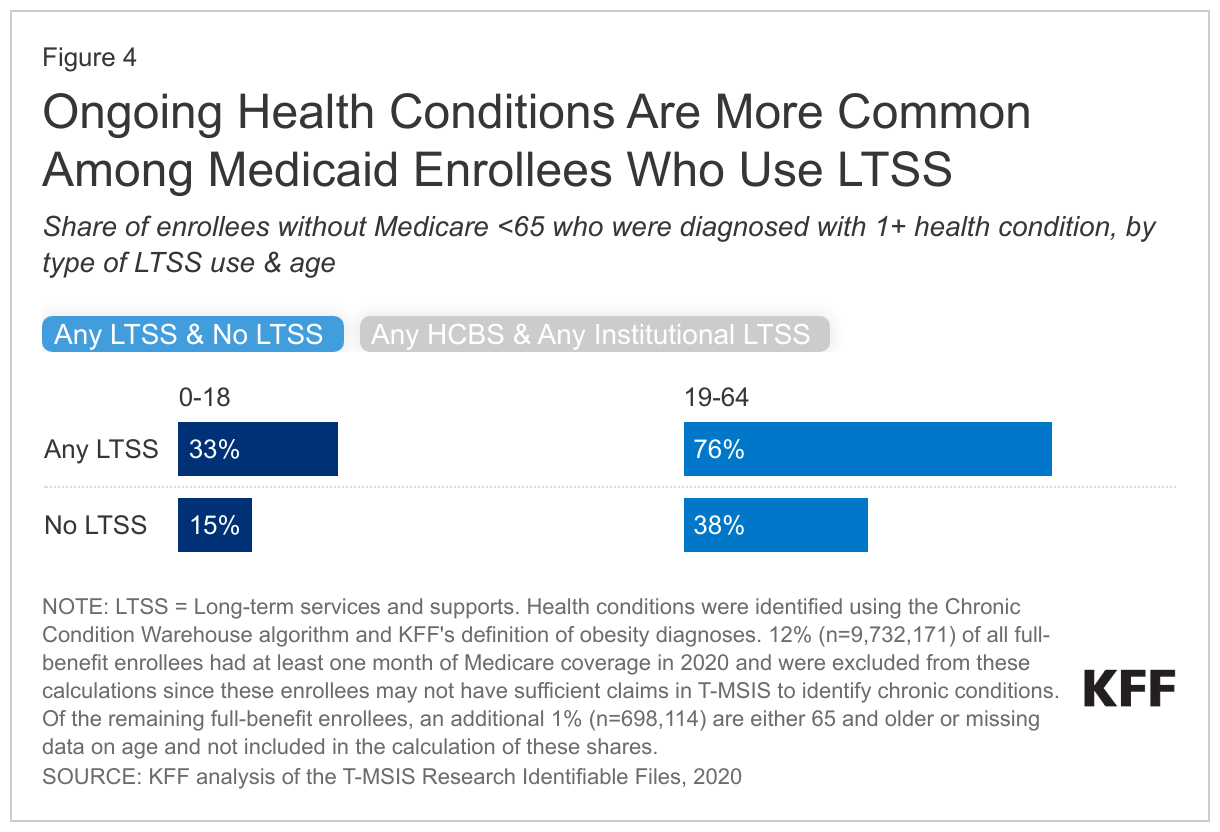
Rates of ongoing health conditions are higher among Medicaid enrollees under 65 without Medicare who use LTSS compared with those who don’t use LTSS (Figure 4). Rates of chronic conditions are only available for Medicaid enrollees who do not have Medicare because for dual-eligible individuals, Medicare is the primary payer of acute care services and health conditions may not show up in the Medicaid data (Box 1). All enrollees 65 and older are also excluded because fewer than five percent of people 65 and older do not have Medicare. Health conditions include a list of 30 chronic conditions maintained by the Centers for Medicare & Medicaid Services and an indicator for whether enrollees had an obesity diagnosis in the Medicaid claims data (defined as ICD-10 diagnosis codes within E66.0, E66.1, E66.2, E66.8, E66.9, Z68.3, Z69.4, and Z68.54.)
Among enrollees under 65 without Medicare, 33% of enrollees ages 0-18 who use LTSS have a diagnosis of at least one ongoing health condition compared with 15% of those who don’t use LTSS. Similarly, 76% of those 19-64 who use LTSS have a diagnosis of at least one ongoing health condition compared to 38% who do not use LTSS. Enrollees who do not have a diagnosis for an ongoing health condition may receive LTSS for any number of other reasons, including frailty. Frailty is a complex health state that describes the decline in health and increased physical vulnerability that comes with aging, chronic and progressive illness, or in the aftermath of a major accident or stroke. People with frailty may not have a diagnosis for any ongoing health conditions, but frailty is a significant reason that people need help with daily personal care activities such as bathing or dressing.
Rates of health conditions are only slightly higher among those who use institutional LTSS compared with those who use HCBS (Figure 4). For enrollees who use HCBS, 33% of those ages 0–18 have a chronic condition compared with 74% of those ages 19-64. These rates are only slightly lower than enrollees who use institutional LTSS. For enrollees who use institutional LTSS, 37% of enrollees ages 0–18 have a chronic condition compared with 89% of enrollees ages 19-64.
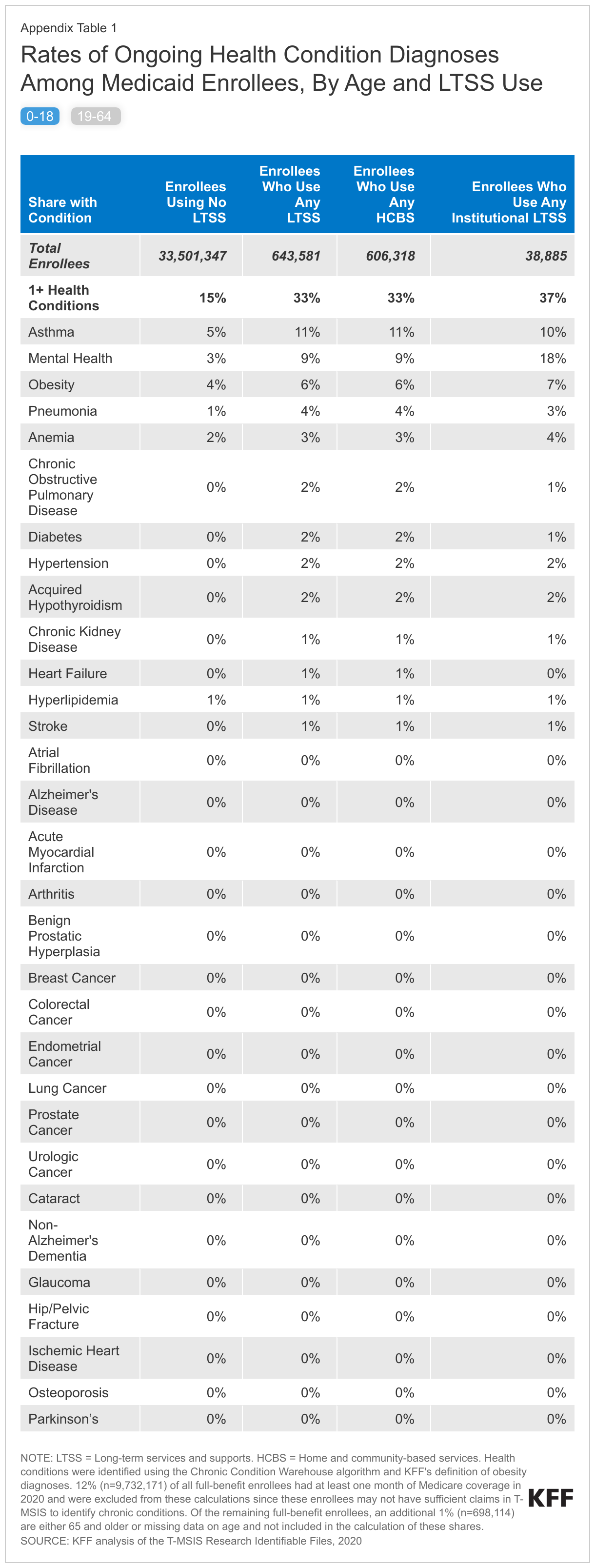
Among Medicaid enrollees under age 65, certain health conditions, in particular, are higher among those who use LTSS than among those who don’t (Appendix Table 1). Among enrollees ages 0-18, 9% of enrollees without Medicare who use LTSS have a mental health diagnosis compared with only 3% of those who don’t use LTSS. Similarly, among enrollees 19-64, 33% of enrollees who use LTSS have a mental health condition compared with only 12% of those who don’t use LTSS; and 18% of enrollees who use LTSS have an obesity diagnosis compared with 8% of enrollees who don’t. Other health conditions, such as pneumonia (10% vs 2%) and diabetes (27% vs 7%), are similarly more common among enrollees ages 19-64 using LTSS when compared to those who don’t.
For Medicaid enrollees under age 65 who use LTSS, the most common chronic conditions are similar for people who use HCBS and institutional care, although the rates of those conditions are somewhat higher among people who use institutional care (Appendix Table 1). Among enrollees under age 19, the three most common conditions include: mental health conditions (affecting 9% of children who use HCBS and 18% of children who use institutional LTSS), asthma (affecting 11% of children who use HCBS and 10% of children who use institutional LTSS), and obesity (affecting 6% of children who use HCBS and 7% of people who use institutional LTSS). Among enrollees ages 19-64, the most common conditions include hypertension (affecting 36% of adults who use HCBS and 57% of adults who use institutional LTSS), mental health conditions (affecting 31% of adults who use HCBS and 45% of adults who use institutional LTSS), and diabetes (affecting 26% of adults who use HCBS and 35% of adults who use institutional LTSS).
Box 1: Identifying Health Conditions Among Medicaid Enrollees
KFF identifies people’s health conditions through diagnosis codes on Medicaid claims and encounter data. Claims are records of bills submitted by providers in order to be reimbursed by the state Medicaid program. Encounter data are records of the services received by people who are enrolled in Medicaid health plans. Unlike claims, they do not include payment information because the health plans pay providers instead of the state Medicaid program.
Some Medicaid enrollees—known as dual-eligible individuals—also have Medicare and for those people, Medicare is the primary payer for most health care services. Medicaid pays for Medicare premiums and in most cases, cost sharing. For dual-eligible individuals who are eligible for full Medicaid, Medicaid also covers supplemental benefits such as LTSS and non-emergency medical transportation. In many cases, there will be no Medicaid claims or encounter data when services are covered by Medicare. Without claims, there are no diagnosis codes for dual-eligible individuals. As a result, it is impossible to accurately identify rates of health conditions in Medicaid data for dual-eligible individuals. Approximately 9.7 million full-benefit duals are excluded from the calculations in Figure 4.
What key issues may impact those who use Medicaid LTSS?
Are there sufficient workers to meet the higher staffing levels sought in proposed rules? Long-standing staffing shortages in long-term care facilities predate the COVID-19 pandemic, but the pandemic exacerbated them and the number of workers employed at skilled nursing care and elderly care facilities was still below pre-pandemic levels in October 2023. The federal government recently released a proposed rule that would create new requirements for nurse staffing levels in nursing facilities. KFF analysis finds that fewer than 1 in 5 could currently meet the required number of hours for registered nurses and nurse aides, but facilities will have several years to come into compliance and the proposed rule includes hardship exemptions. For HCBS, the Biden Administration recently released a proposed rule aimed at ensuring access to Medicaid services, which has several notable provisions aimed at addressing HCBS workforce challenges. States would be required to report payment rates for certain HCBS, to demonstrate that payment rates are “adequate” to provide the level of services in enrollees’ personalized care plans, and to ensure at least 80% of payments are passed through to worker compensation for certain types of HCBS.
Will there be additional barriers to accessing Medicaid HCBS as public health emergency authorities end and enhanced federal funding runs out? Recognizing the importance of keeping people out of congregate settings and that HCBS workforce challenges were exacerbated during the COVID-19 public health emergency, the federal government provided states with new authorities and funding to maintain access to HCBS during the public health emergency (PHE). States used the additional funding and flexibility to increase payment rates, pay family caregivers, and expand access to HCBS. Although many states are working to make the PHE changes permanent, KFF findings indicate that some states will revert to their pre-PHE policies, potentially reducing access to HCBS or payments to providers. Funding made available by the American Rescue Plan Act to “enhance, expand, and strengthen” HCBS is also set to expire in March 2025, although states may exhaust the additional funding before that time.
As the population continues to age and more people need Medicaid LTSS, how might policy makers aim to expand access to care? As the 25th anniversary of the Olmstead court decision—which requires people with disabilities to be served in the most integrated setting that is appropriate—nears, there may be increased attention on the extent to which integration has occurred and where further integration is still needed. Along those lines, a recent proposed rule clarifies the obligation for states to provide services in the most integrated setting appropriate—codifying the Olmstead decision and clarifying that failing to provide services in the most integrated setting appropriate is a form of discrimination. Data describing the differences between people who are using institutional LTSS and HCBS helps illuminate which populations are most likely to receive integrated care and which are still served in primarily segregated settings. Beyond the people who are currently using Medicaid LTSS, there are close to 0.7 million people on waiting lists or interest lists for Medicaid HCBS. While these data are an imperfect measure of unmet need, they do suggest there has been consistent unmet need for these services and have been described as contributing to the risk of unnecessary institutional for people with disabilities. Recent research also finds that there are disparities in HCBS spending, access, and outcomes among communities of color, including higher rates of unmet LTSS needs.
Appendix Table