Addressing Abortion Access through State Ballot Initiatives
This brief is not updated as efforts to get abortion-related measures on the ballot progress. For an up-to-date list of states that may have abortion-related state constitutional amendment measures on the ballot, please see our ballot tracker.
Updated on February 9, 2024
Key Takeaways
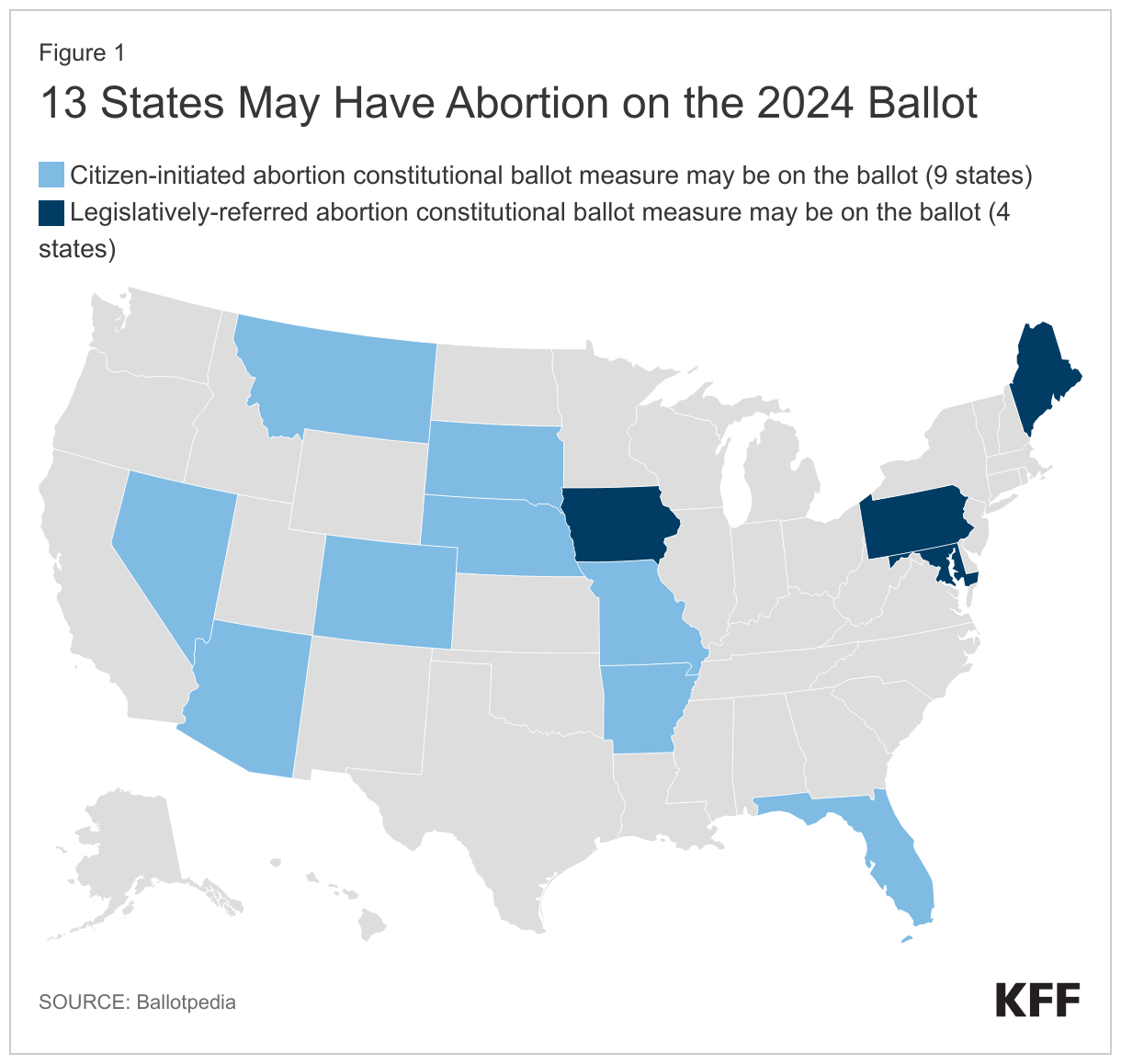
- There are efforts underway to put constitutional amendments regarding abortion on the 2024 ballot in as many as 13 states: Arizona, Arkansas, Colorado, Florida, Iowa, Maine, Maryland, Missouri, Montana, Nebraska, Nevada, Pennsylvania, and South Dakota.
- Since Dobbs, 6 states – California, Kansas, Kentucky, Michigan, Vermont, and Ohio – have voted on abortion related constitutional amendments, and the side favoring access to abortion prevailed in every state.
- Citizen-initiated constitutional amendments are a powerful tool that is being utilized to allow voters to garner signatures to place abortion on the ballot without directly involving the legislature or the governor.
- This approach, however, cannot be used in 15 of the states that currently have abortion bans or early gestational limits on the books because they do not have a pathway for citizens to place potential constitutional amendments on the ballot. In those states, the legislature controls the process.
Since the Supreme Court’s Dobbs decision overturning Roe v. Wade, voters in 6 states have weighed in on constitutional amendments regarding abortion. Every time these constitutional amendments have been on the ballot, voters have elected to approve measures that would explicitly protect abortion and deny those that sought to limit abortion. Since then, potential ballot initiatives have captured nationwide attention, and in 2024, 13 states may have abortion measures on their ballot. These measures seek to either explicitly affirm that the state constitution protects the right to abortion or that nothing in the constitution confers such a right. Advocates on both sides are hoping that having abortion on the ballot will motivate voter turnout in this election cycle. This issue brief explains why initiatives have become so popular with advocates on both sides of the issue, reviews the current initiatives that are in progress and may appear in on state ballots the next general election, and outlines the processes states have available to them to use to place initiatives on the ballot.
Interest in Reproductive Rights Ballot Measures Post-Dobbs
State constitutional amendments have drawn much interest since SCOTUS’ decision in Dobbs because they provide more stable protections than laws or state Supreme Courts’ decisions recognizing a right to abortion. Laws are relatively easy to amend or repeal if there is a change in the make-up of the state legislature. For swing states, where neither party has a strong hold on the majority of the legislature, it is difficult to ensure that abortion protections or restrictions will not be repealed if there is a change in party control. Additionally, state Supreme Court rulings recognizing a right to abortion – or stating that there is no such right – in the state constitution may be overruled when there are subsequent changes in the make-up of the court. For example, the South Carolina Supreme Court ruled in January 2023 that the state’s 6-week ban was unconstitutional, but after the legislature appointed a new justice to replace a retiring justice, the Court reversed its ruling in August 2023 and found the restriction is constitutional. Constitutional amendments, on the other hand, would have to be repealed with a ballot measure receiving a majority of the popular vote.
Furthermore, in states where their supreme court has interpreted and recognized a right to abortion based on the state constitution, a constitutional amendment declaring there is no right to abortion would supersede the Court’s decision and allow abortion restrictions and bans to survive judicial review. For example, the goal of the 2022 Kansas ballot measure was to negate the state Supreme Court’s ruling that the Kansas constitution protects the right to abortion. If the ballot measure had passed and the Kansas constitution had been amended to state that nothing in it creates a right to abortion, the state legislature would have been able to ban or severely restrict abortion in Kansas. Conversely, in states where their supreme court has ruled the state constitution does not protect the right to abortion, amending the state constitution to include an explicit right to abortion would supersede supreme court precedent and require the court to block an abortion ban.
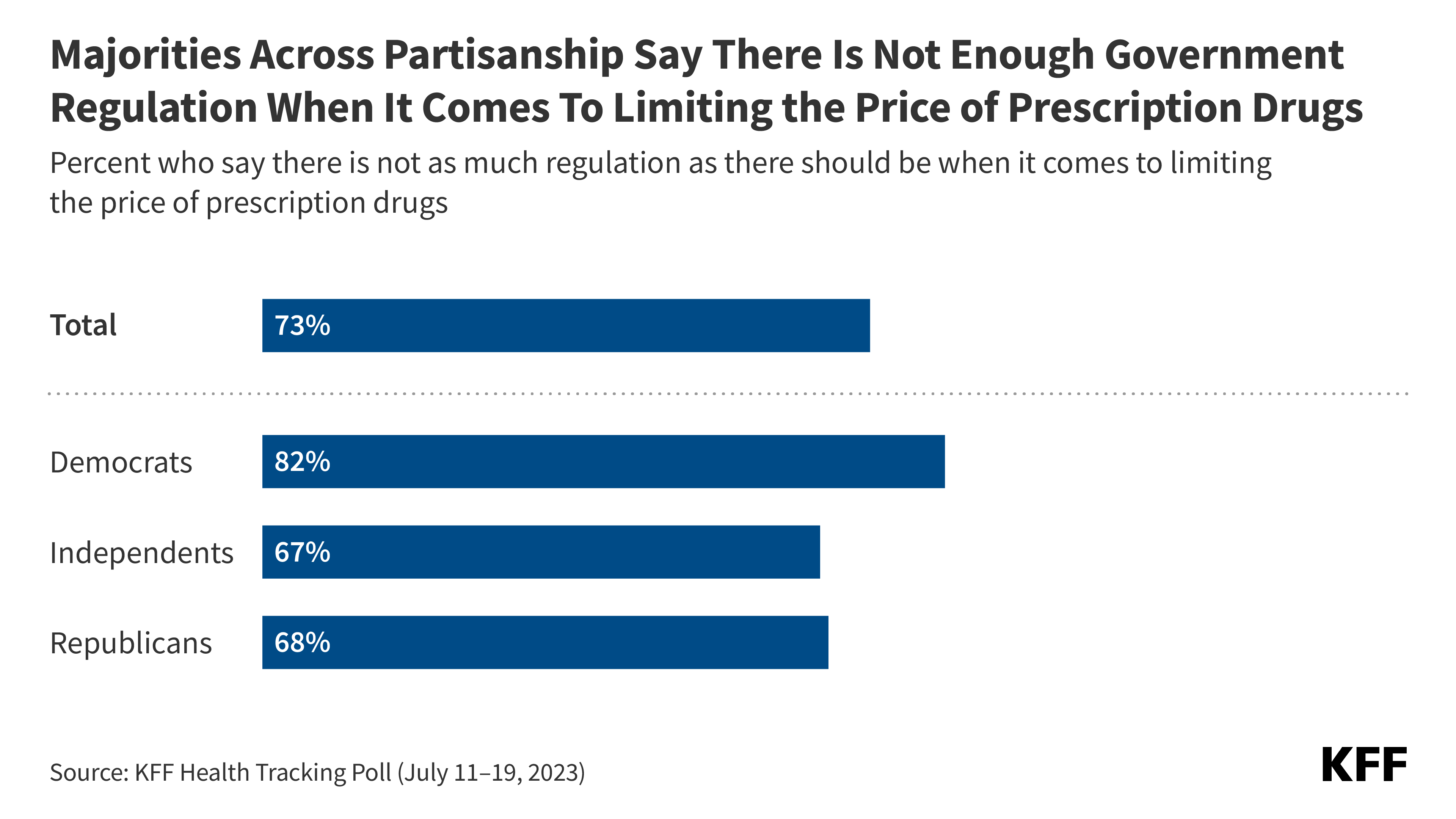
Importantly, aside from providing stronger, more stable protections and changing the judicial review of abortion laws, ballot measures seeking to amend state constitutions place issues directly in front of voters. In states where the legislature has sought to limit abortion in ways that are more restrictive than the public favors, a citizen-initiated ballot measure is a way to enact constitutional protections for abortion without directly involving the legislature or Governor. And once the constitution is amended, state policy makers cannot repeal these protections or fully ban or restrict abortion. Citizen-initiated ballot measures provide a direct pathway for the electorate to decide whether or not abortion should be legal in their state, regardless of how their elected representatives have decided to approach abortion policy. According to a recent KFF poll, nationally, the majority of voters say abortion should be legal in all or most cases.
Constitutional Ballot Measures in 2022 and 2023
Due to the advantages presented by ballot measures amending state constitutions, legislatures and citizen groups in several states have moved to add measures enshrining a right to abortion in their constitutions or declaring that there is no such right in the constitution. In 2022, there were four legislatively referred measures on the ballot regarding abortion or reproductive rights more broadly. In 2022, Michigan voters passed the first citizen-initiated constitutional measure protecting the right to abortion and in 2023, Ohio voters also passed a similar citizen-initiated constitutional measure protecting the right to abortion.

Constitutional Ballot Measures That May Be on the 2024 Ballot
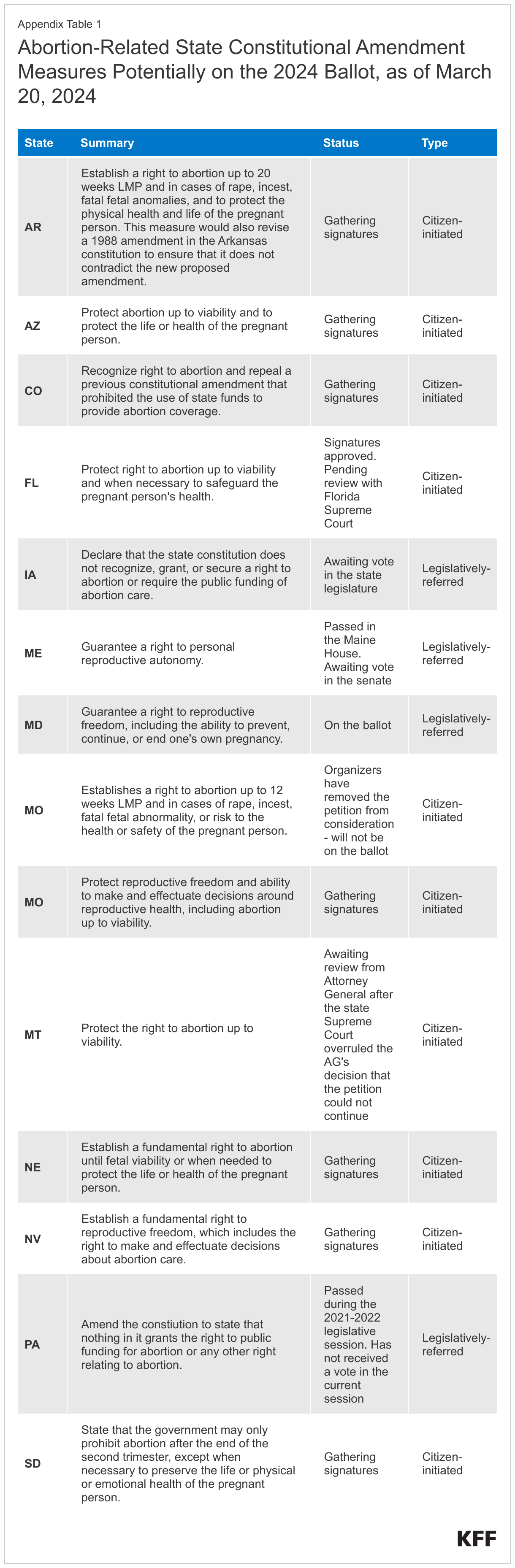
Abortion rights groups are seeking to qualify ballot initiatives to uphold abortion rights in three states (Colorado, Montana, and Nevada) where there is no early gestational limit and in six states that ban abortion or have early gestational limits (Arizona, Arkansas, Florida, Missouri, Nebraska, South Dakota) in 2024. There is ongoing litigation challenging the abortion bans in most of these states, but without a constitutional amendment establishing a right to abortion, it is not certain that the respective supreme courts in these states will find the bans unconstitutional, or in the case of Florida, that the Court will uphold its prior decisions recognizing a right to abortion. However, if the initiatives establishing a right to abortion succeed in these states, abortion-rights advocates would have the certainty that these bans will be blocked in court.
Four state legislatures have constructed potential initiatives for constitutional amendments pertaining to abortion. The legislatures in Iowa and Pennsylvania have introduced measures that would amend the state constitution to declare that it does not protect the right to abortion. In Maine and Maryland, state representatives drafted initiatives protecting the right to reproductive freedom or autonomy (which includes the right to abortion). The Maryland initiative passed in the legislature and so far, is the only measure that is certain to appear on the 2024 ballot. The remaining legislatively-referred initiatives must pass in both chambers of the state legislatures, and the citizen-initiated measures are either gathering signatures, or awaiting initial approval or signature certification. See Appendix A for state-by-state details.
Pathways to Getting an Initiative on the Ballot
Legislatively-Referred Initiatives
For legislatively-referred initiatives seeking to amend a state constitution by the electorate, state legislators draft language for the initiative and introduce it to the legislature, in a process that is similar to how they introduce language for bills. Both chambers of the state’s legislature must vote to approve the language before it is placed on the ballot. In every state except for Delaware, initiatives seeking to amend a state’s constitution must be placed on the ballot and cannot be enacted without voter approval.
The process of approving a ballot initiative in the state legislature differs from state to state. While most states require the initiative to pass only once in the legislature, some states require it to pass over two successive legislative sessions. States also have differing requirements for what percentage of the legislature must vote in favor of the initiative for it to move forward, ranging from a simple majority to a two-thirds majority. Once the measure is on the ballot, there are also differing requirements for what share of the votes it must receive to become law.
Citizen-Initiated Measures
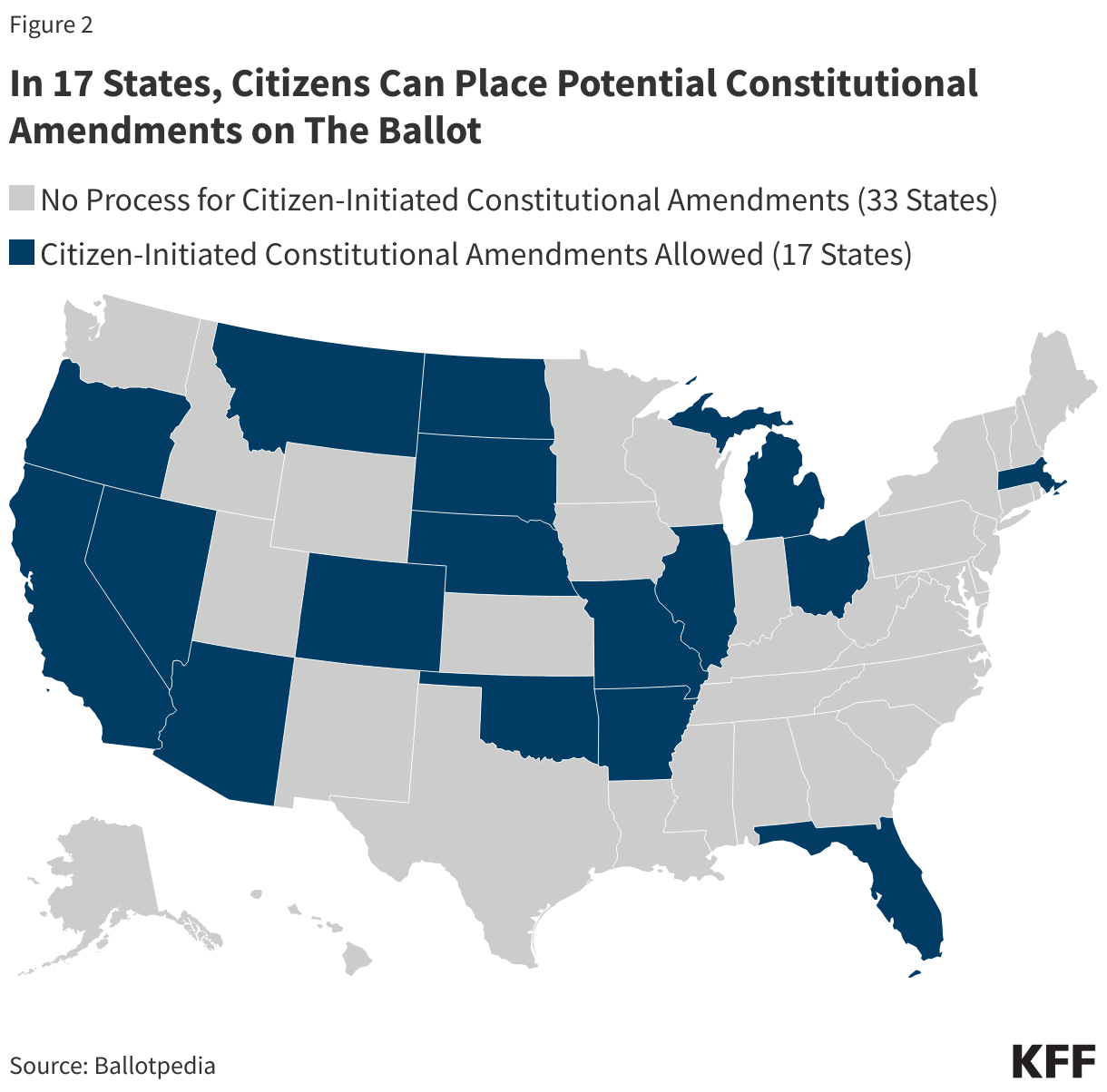
Citizens are allowed to propose a constitutional amendment for the ballot in 17 states. The rules for doing so differ slightly from state to state, but generally, citizen groups must submit a draft of the proposed amendment and ballot title to a government official – usually the Secretary of State – for approval. Once the petition has been approved, groups must gather signatures in support of their measure, often with distribution requirements across the states’ congressional districts, and submit their support signatures for validation. If enough signatures from a sample are deemed valid, the measure is cleared to be on the ballot, where it must receive anywhere from a simple majority to 60% of the vote in favor to be approved.
There are different stages of review for ballots in each state. Some states require that ballot measures address only one subject, and the reviewing body or official might reject a petition if they decide it violates this requirement. Petitions may also be rejected if they contain vague or confusing language. However, beyond these considerations, state officials are generally not allowed to reject a petition based on its substance. In the past few years, this has meant that state attorneys general, secretaries of state, or electoral boards that oppose abortion have nevertheless had to approve petitions for ballot measures that would enshrine the right to abortion in the state’s constitution. This has also resulted in state legislatures taking steps to attempt to make it more difficult for measures to pass or even get on the ballot in the first place. For instance, in Ohio, Missouri, Florida, Oklahoma, and Utah, these attempts have included proposed measures to increase the percentage of the vote needed for the ballot initiative to pass. Lawmakers in Missouri and North Dakota have additionally attempted to increase the number of signatures needed to get a measure approved. The North Dakota 2024 constitutional ballot measure additionally seeks to require that constitutional ballot initiatives pass in two separate elections (the primary and general elections) before they can successfully amend the constitution.
Citizen-Initiated Ballot Measures Are Not an Option in All States
Not every state has a pathway for a citizen-initiated constitutional amendment. In twelve states that currently ban abortion or have early gestational limits in effect, there is no process for a citizen-initiated ballot measure. Three additional states (Wyoming, Iowa, and Utah) that have abortion bans currently blocked by courts, also have no process for a citizen-initiated ballot measure. In these fifteen states, unless the state legislatures repeal their bans, the only avenue reproductive rights supporters have to potentially change the legal status of abortion, short of electing pro-choice legislators and policy makers, is to challenge these bans in court. If the State Supreme Court upholds the bans, they will remain in place. This is the current situation in Idaho, Indiana, and South Carolina. Their respective supreme courts ruled their state constitutions do not protect the right to abortion and that the states’ abortion bans are constitutional. Since these rulings, abortion-rights advocates have not had any avenues to change the legal status of abortion in these states. Litigation challenging abortion bans in seven other states (Georgia, Iowa, Kentucky, Louisiana, North Carolina, Utah, Wyoming) with bans and no process for a citizen-initiated ballot measure is making its way through the courts. There are no legal challenges to the bans in Alabama, Mississippi, or West Virginia.
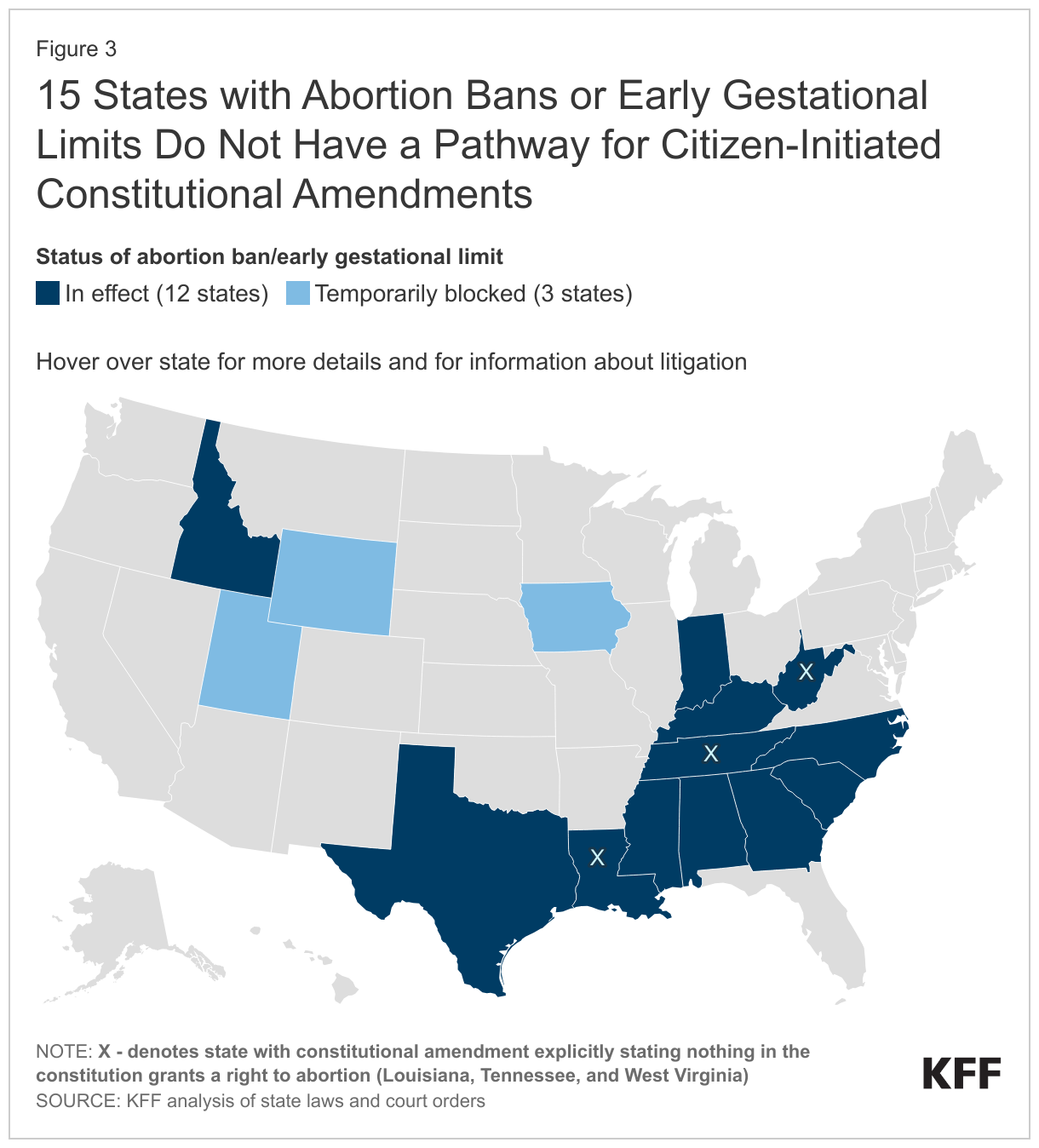
Moreover, three states with abortion bans in place and no process for a citizen-initiated ballot measure (Louisiana, Tennessee, and West Virginia), have state constitutional amendments that explicitly state their constitutions do not protect the right to abortion. These amendments preclude these states’ Supreme Courts from ruling that an abortion ban is unconstitutional because it violates a right to abortion. In other words, the only way for the legal status of abortion to change in these states is for their legislatures to repeal their bans or pass a new constitutional amendment protecting the right to abortion. In two of these states (Louisiana and Tennessee) and in Idaho, Indiana, and Texas, there is ongoing litigation focused only on whether the exceptions to the bans are constitutional, but not challenging the underlying bans
Citizen-Initiated Ballot Measures for State Statutes
In 21 states, citizens can initiate laws and place proposed laws on the ballot. The process for placing on the ballot an initiative that would enact a law is very similar to that for placing constitutional amendment initiatives, except that they typically require either fewer signatures for approval or fewer affirmative votes to pass. Some states with processes for statute ballot initiatives restrict the legislature’s ability to repeal or amend laws initiated by citizens. Other states simply treat these laws as they would any other law written by state representatives, and as such, can be repealed or amended as easily as any other law. This process allows citizens to propose laws that the current state legislators would not support. Currently, there are two proposed citizen-initiated statutes, brought by anti-abortion advocates, that may appear on the 2024 ballot, one in Colorado and the other in Nebraska. Both proposed statutes would ban abortion in each respective state, and both have been cleared for signature gathering. If they obtain the required number of signatures, these measures may appear on the ballot in 2024. In both states, abortion rights supporters are also seeking to place constitutional amendments protecting the right to abortion on the ballot. The placement of a statute seeking to ban abortion, and a constitutional amendment to protect the right to abortion on the same ballot is anticipated to cause confusion. In the unlikely event that both measures pass, the constitutional amendment would block the implementation of the abortion ban.
Looking Ahead
When the Supreme Court’s decision in Dobbs gave states the ability to ban or limit abortion, the legal landscape at the state level was activated as never before. In many states, legislators moved quickly to pass new statutes banning, or severely limiting access to abortion, and reproductive rights supporters turned to courts to challenge many of these new and already-existing laws. As the legality of and restrictions of abortion has been debated in state legislatures and courthouses, ballot measures amending state constitutions have emerged as a potential tool for proponents on both sides of the issue. State constitutional amendments explicitly stating whether the state’s constitution protects the right to abortion offer more stable protections for individuals’ right to abortion or the state’s right to ban abortion. These initiatives are being closely watched and it remains to be seen whether they will have an impact on voter turnout, as well as the outcome of candidate races.
Additionally, as the post-Dobbs legal landscape has shifted and begun to settle, many states have abortion laws on the books that do not reflect popular sentiment around abortion. Citizen-initiated constitutional ballot measures allow citizens to put abortion rights directly before the voters, although this is not an option in every state. Still, in many of the states where this is an option, advocacy groups on both sides of the issue are seeking to use this powerful tool to address the legality of abortion in their state.
Appendix