Key Takeaways
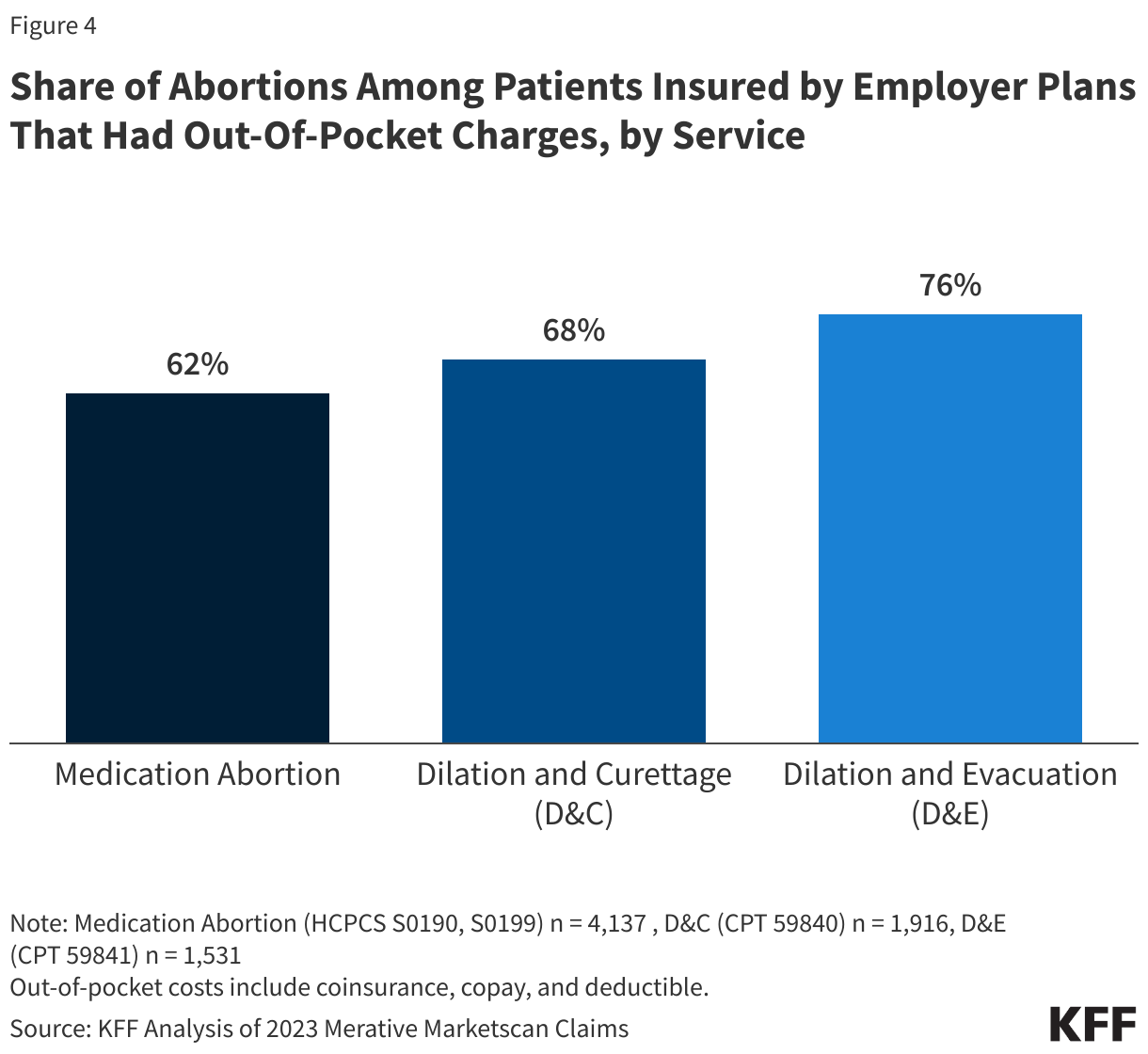
- Most females who used their private insurance to pay for their abortion had out-of-pocket costs for their services, including 62% of those who accessed medication abortion, 68% of those who obtained a D&C procedure, and 76% of those who received a D&E procedure.
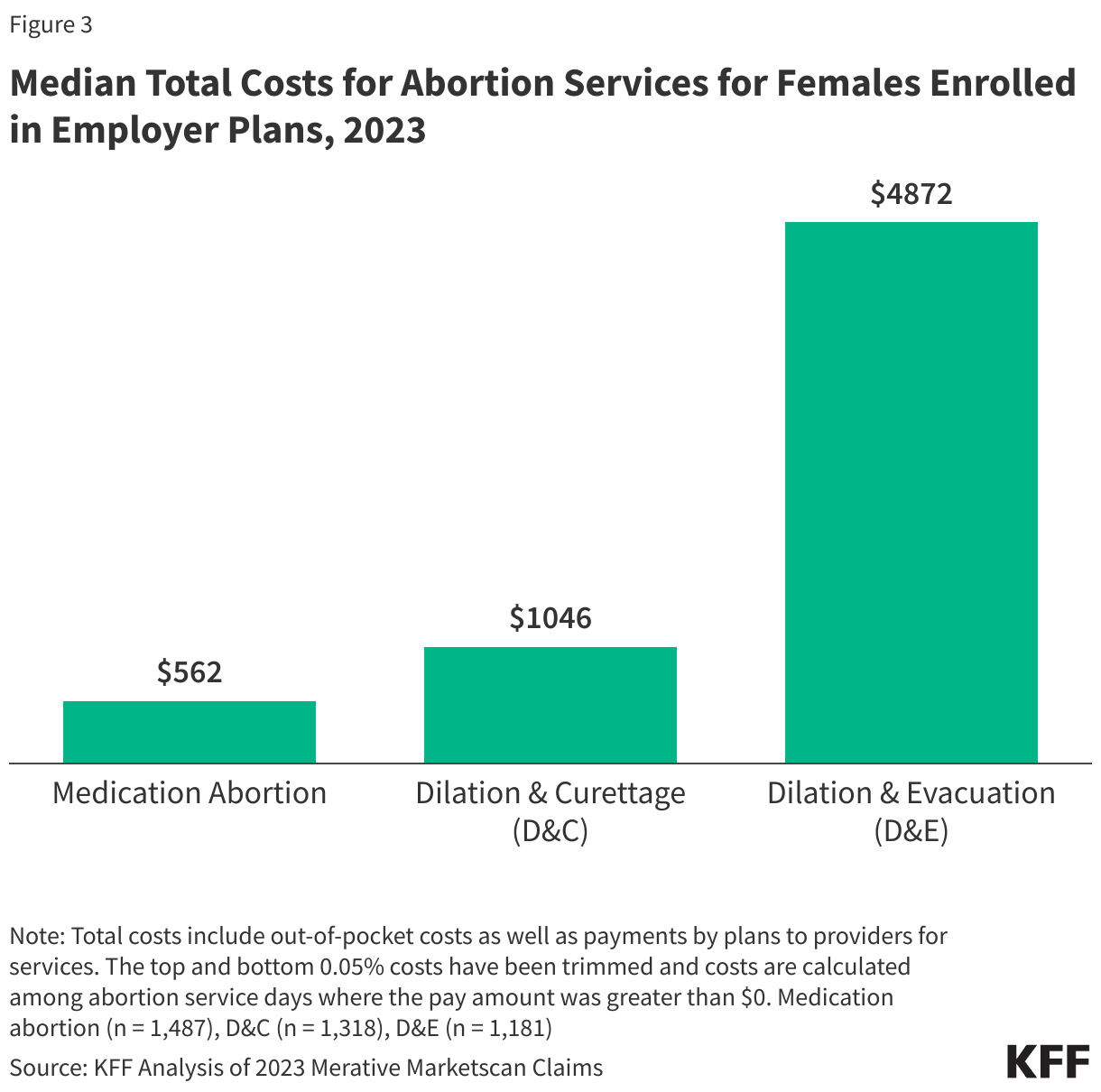
- Median private insurance reimbursement rates for abortion and ancillary services ranged from $562 for medication abortion to $1,046 for D&C, and $4,872 for D&E procedures.
- For those with coverage through employer sponsored insurance plans, median out-of-pocket costs were less than $100 for medication abortion and D&C procedures but rose to over $200 for D&E procedures, typically done later in pregnancy. However, a quarter of females with private insurance paid more than $100 for medication abortion and D&C procedures, and close to $1,000 for D&E procedures.
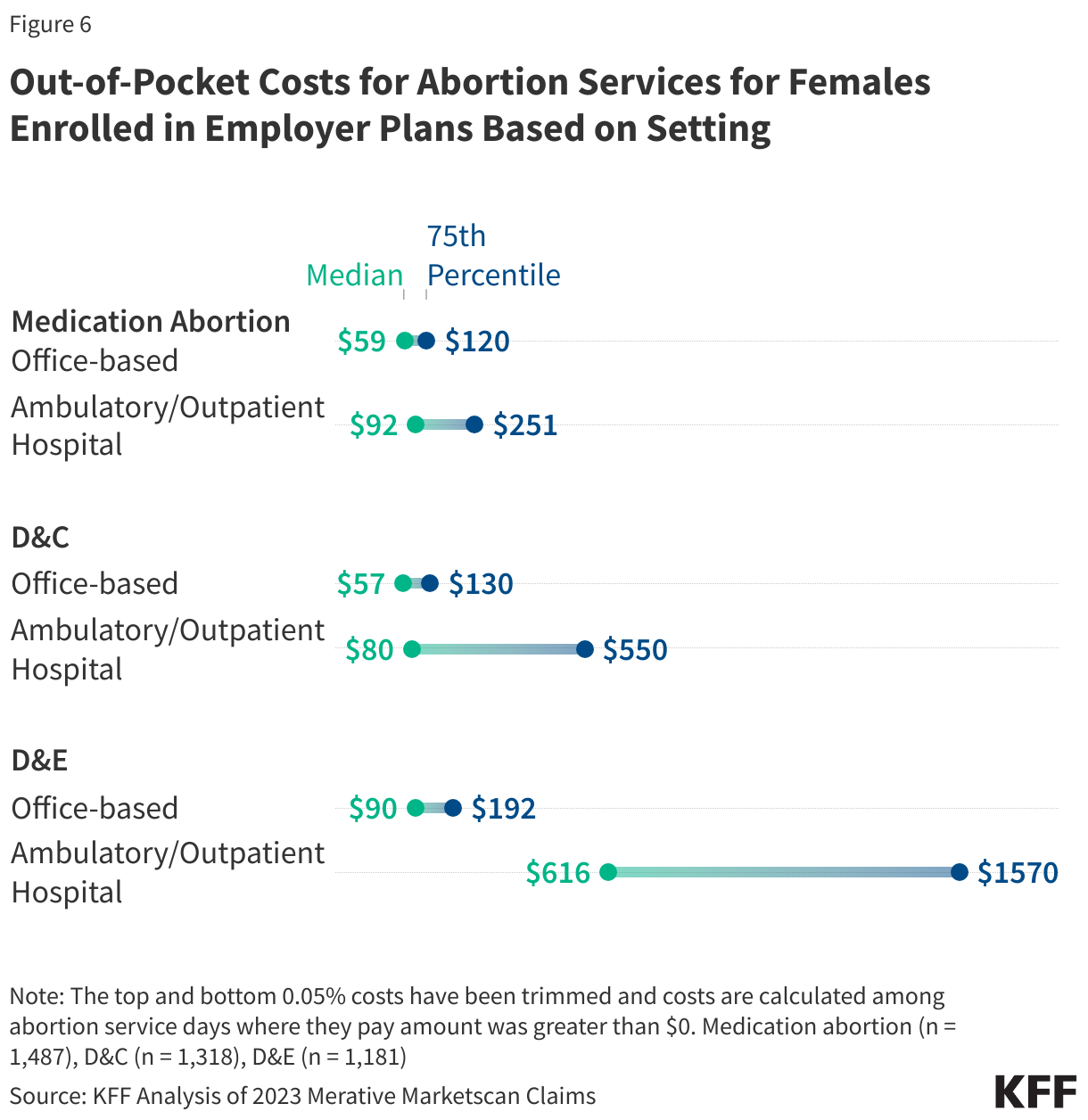
- Out-of-pocket costs were substantially higher for D&C and D&E procedures provided in ambulatory/outpatient hospital settings than office-based settings.
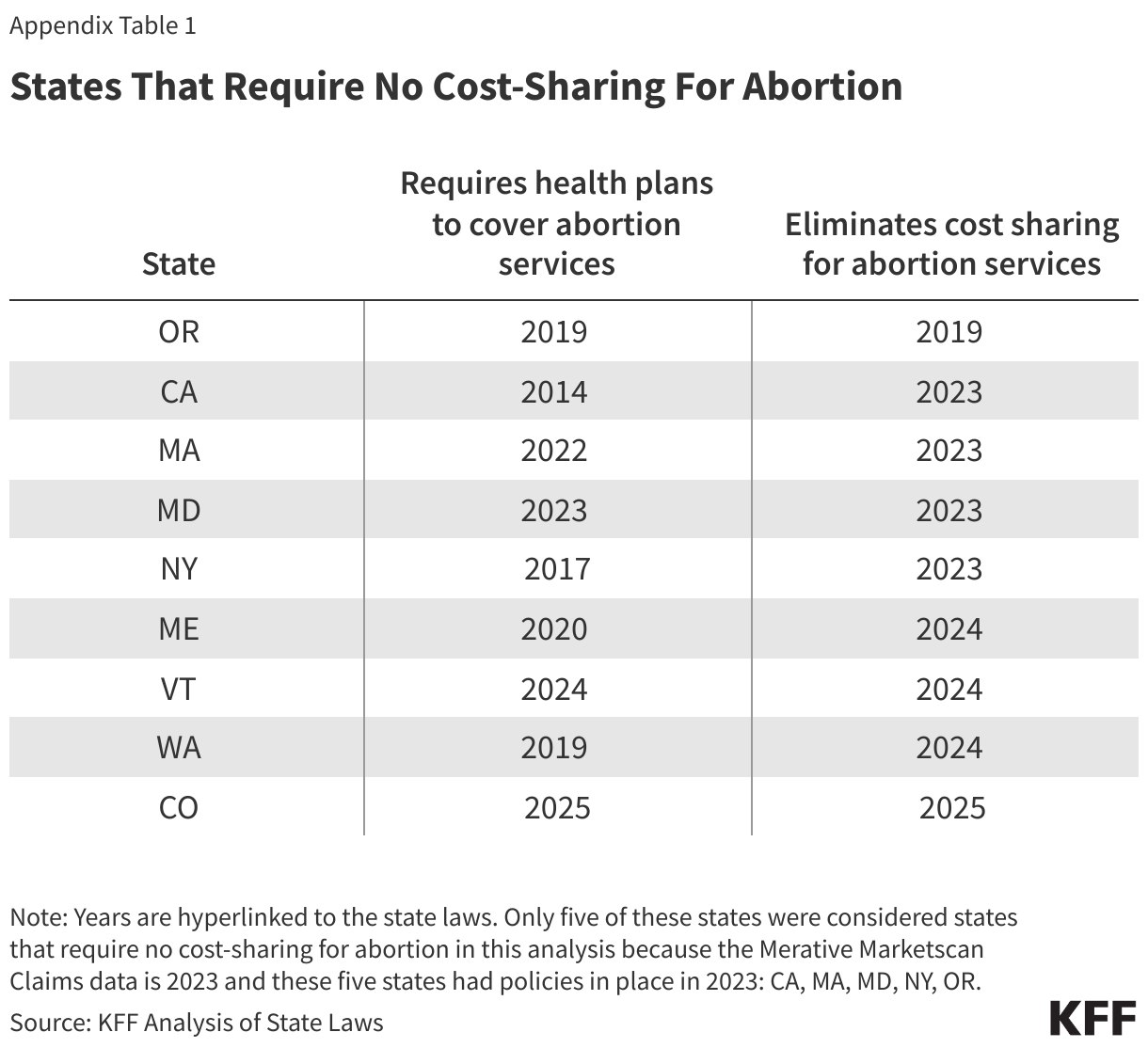
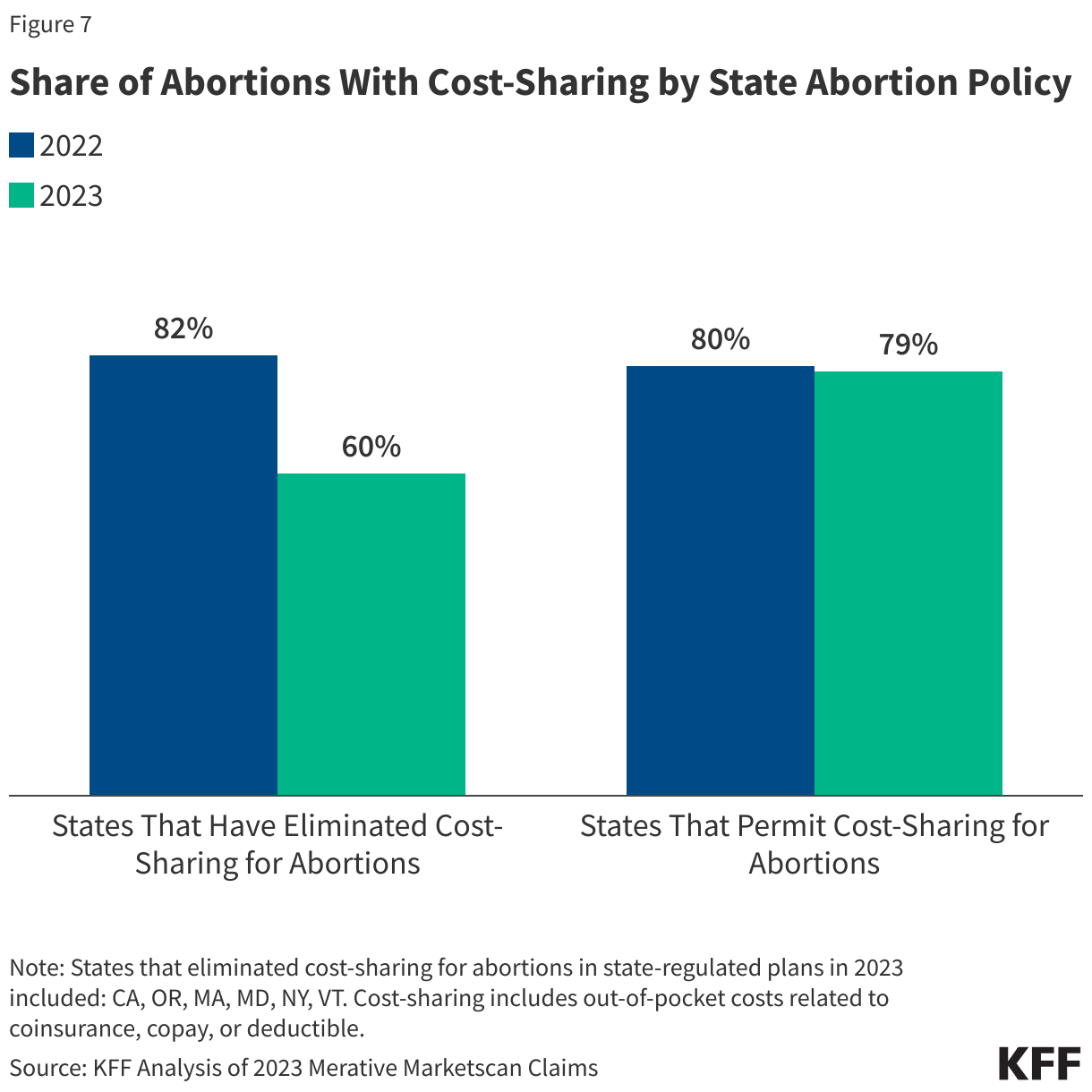
- In the five states that had policies eliminating cost-sharing for abortion services in place in 2023, the share of women with cost-sharing for an abortion decreased substantially from 82% in 2022 to 60% in 2023, while it was unchanged in states that permit cost-sharing for abortion (80% in 2022 and 79% in 2023).
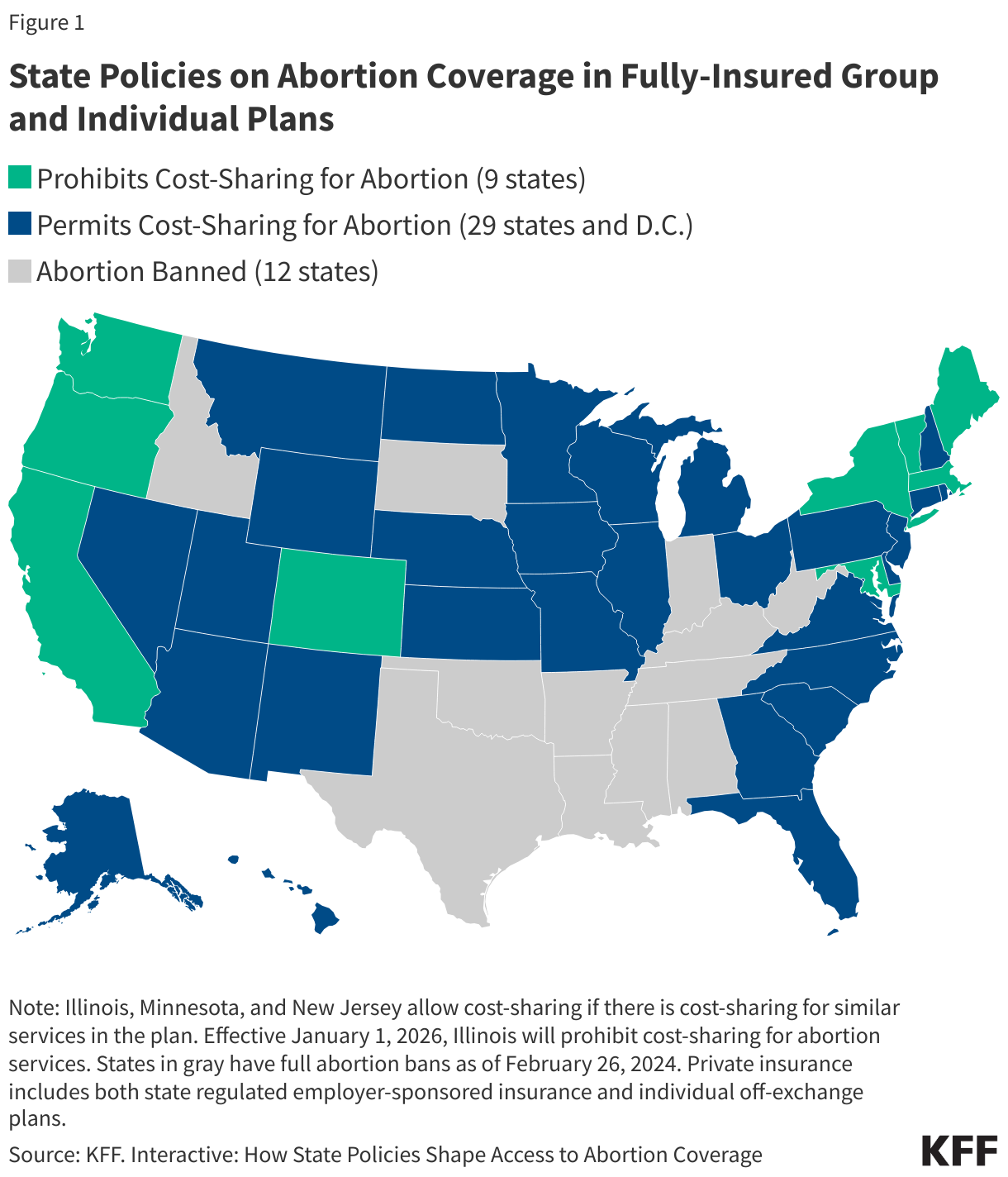
In recent years, insurance coverage of abortion has been the focus of state lawmakers in their efforts to either restrict or expand access to abortion services. Since the passage of the ACA in 2010, many of the states that now have moved to ban or restrict abortion have banned state regulated plans sold through their state exchanges from covering abortion. However, since 2022 when Roe v Wade as overturned, many states that support abortion rights enacted laws requiring coverage, typically free of cost-sharing, to support access to services (Figure 1).
Even before these state actions, many women did not use their insurance to pay for abortions, even when it was covered, because of the highly confidential and stigmatized nature of abortion care. As a result, most people with private insurance end up paying the full costs of abortion that can range from $563 for medication abortion to upwards of $895 for second-trimester abortion. The result has been that those full costs have been borne by women even when they are insured, and insurance has not had to pay for a service that is often covered.
In their efforts to shore up and protect access to abortion and reproductive rights after the Dobbs decision, a handful of states have enacted policies, requiring first dollar coverage for abortion services for people enrolled in state regulated plans. The intent of these policies is to reduce financial barriers to abortion by making the services more affordable. To get a better understanding of how much private plans are reimbursing health care providers for abortion and related services (see Medicaid reimbursement analysis) and document the out-of-pocket spending that people incur when they use their insurance, we conducted an analysis of the 2023 Merative Marketscan claims database, a large national sample of healthcare claims for people enrolled in employer sponsored insurance plans in both the state-regulated and self-insured markets.
Costs for Ancillary Abortion Services
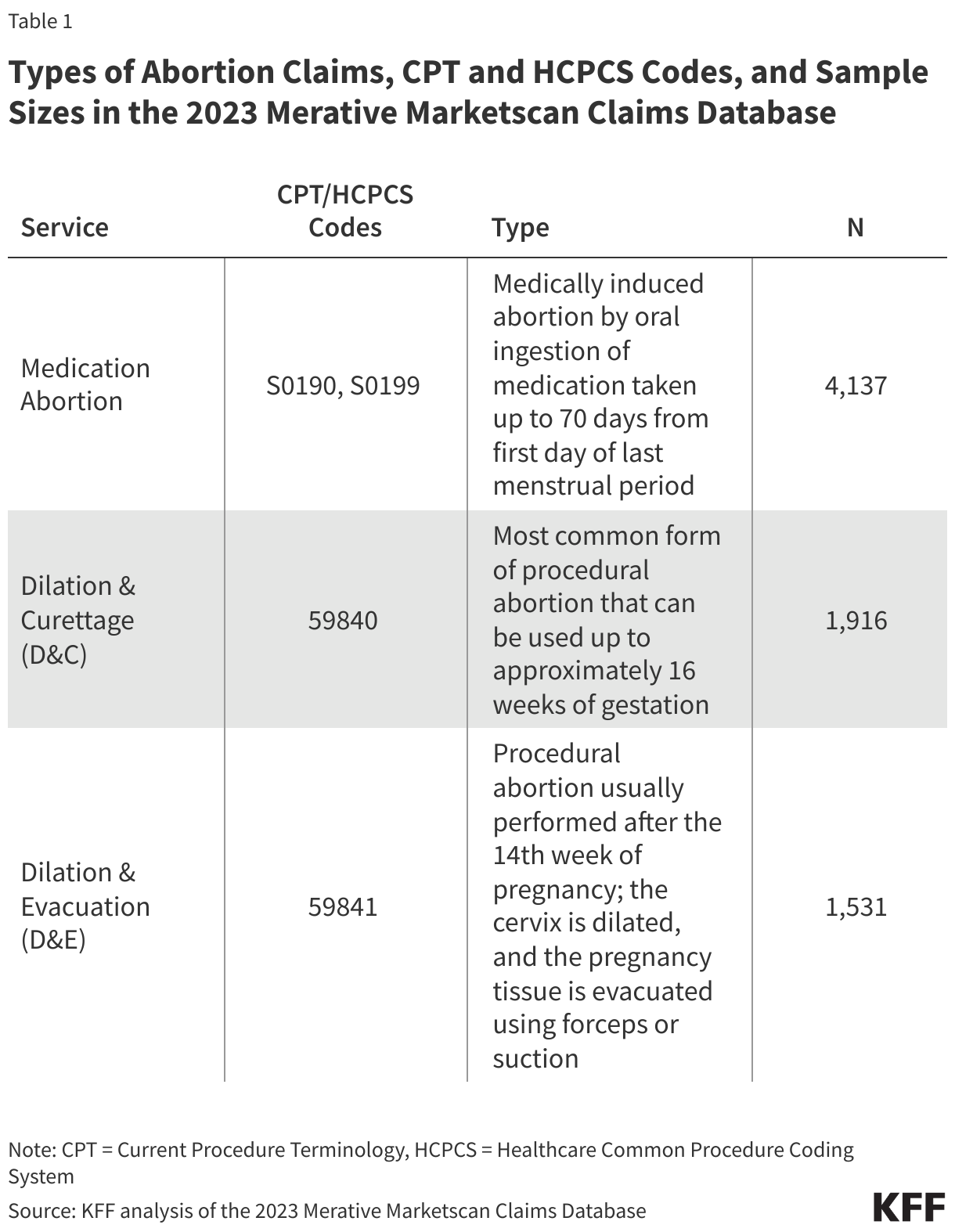
For medication abortion, there are typically two different approaches to billing for services provided: (1) billing the medications plus any ancillary services; or (2) billing the medications plus the global medication abortion code (S0199), a bundled code that includes all associated services and supplies. For abortion procedures (such as D&Cs and D&Es), most providers bill for the procedure plus any associated services and supplies (Table 1). However, some states have implemented a bundled reimbursement that includes the procedure and associated services and supplies.
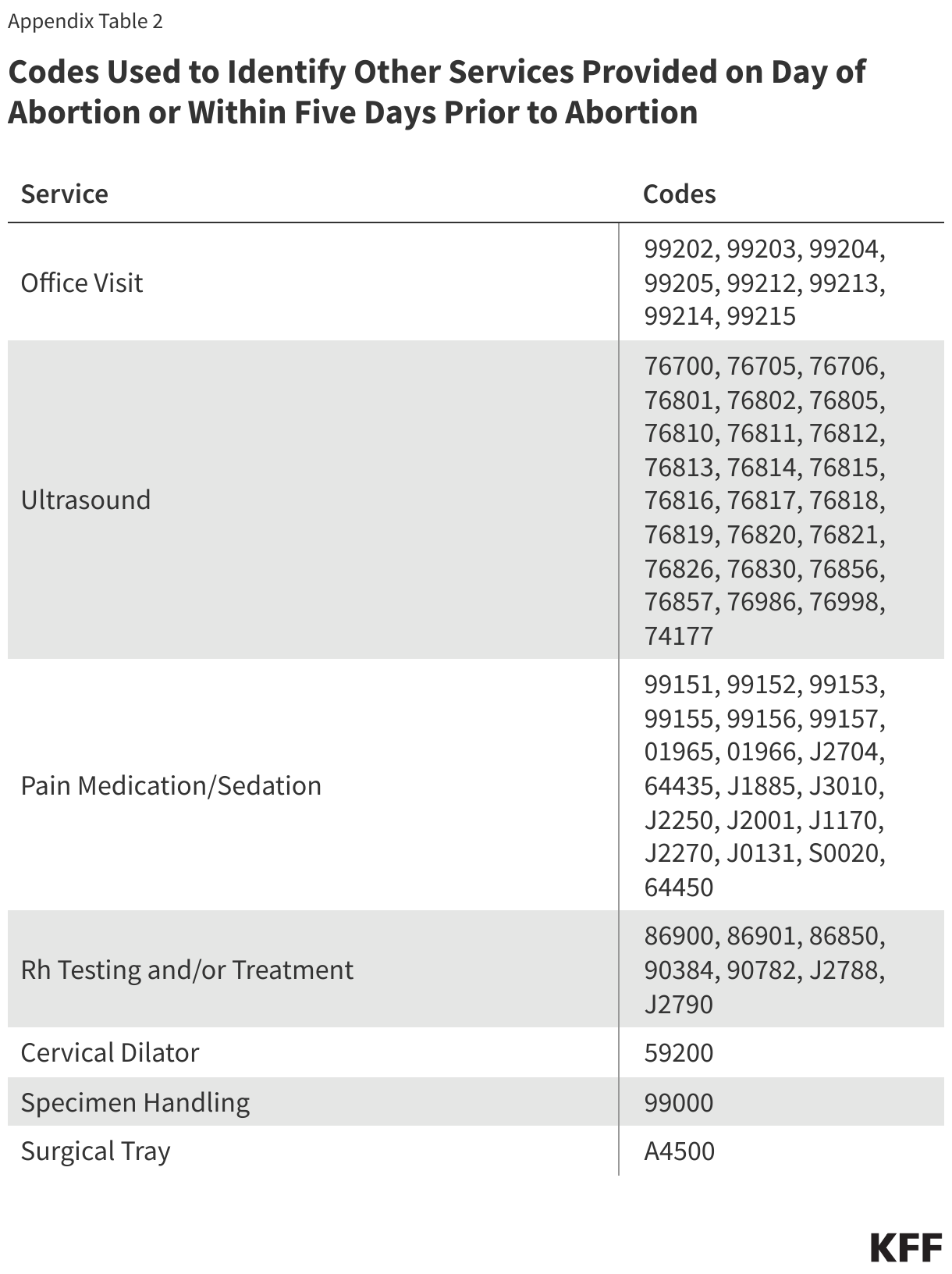
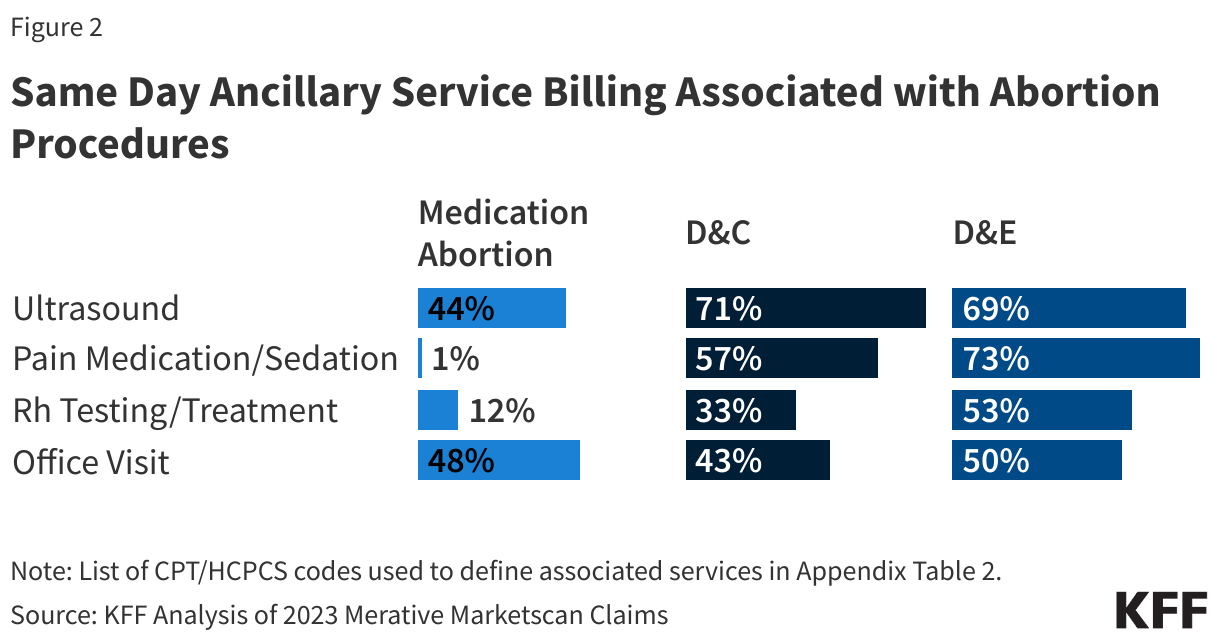
For non-bundled scenarios, other services commonly billed as part of the abortion service include ultrasounds, pain medication/sedation, Rh testing and/or treatment, the office visit, cervical dilator, specimen handling, and the surgical tray (Figure 2).
Ultrasound: Ultrasounds were commonly billed with a D&C procedure (71%) and D&E procedure (69%); 44% of medication abortions also include a separate ultrasound claim. This is likely an undercount of ultrasound provision because ultrasounds could be bundled into the abortion codes, especially for the global medication abortion code. Ultrasound is not a medical requirement for first-trimester abortion care but is required by some state laws. Medication abortion without ultrasonography has been shown to be as effective and safe as medication abortion with ultrasonography.
Pain Medication and/or Sedation: A claim for pain medication and/or sedation was billed with many D&E procedures (73%) and over half of D&C procedures (57%). Other medications may be provided that are bundled as part of the procedure and not separately billed.
Rh testing and/or treatment: One third of D&C procedures (33%) and over half of D&E procedures (53%) included a claim for Rh testing and/or treatment (53%). Only 12% of medication abortions included a claim for Rh testing and/or treatment. have shown that induced first-trimester abortion is not a risk factor for Rh sensitization, indicating that Rh testing and treatment are unnecessary before 12 weeks’ gestation.
Office Visit: Comprehensive office visits are often considered part of the abortion procedure and may not be separately reimbursable. However, half of D&E procedures (50%), four in ten (43%) D&C procedures, and nearly half 48%) of medication abortions included a separate office visit claim within 5 days of the abortion.
Surgical Tray, Specimen Handling, and Cervical Dilator: Other services that providers bill for with an abortion include the surgical tray used during the surgical procedure, specimen handling, and a cervical dilator. These may appear less commonly in claims because they may be bundled with the procedure code for the abortion. Cervical dilators are sometimes inserted a day or two before a procedure.
Total Costs of Abortion Care
The median total costs of abortion services and all ancillary services billed for on the day of the abortion including the insurance payment plus any out-of-pocket expenses paid by the consumer including coinsurance, deductible, and copay were $562 for medication abortion, $1,046 for D&C, and $4,872 for D&E procedures, which usually occur later in pregnancy (Figure 3). Higher costs may also be associated with abortions taking place in emergency situations. We found 3% of abortions included an evaluation management code for an emergency room visit or an ambulance ride on the day of the abortion or within the five days prior to the abortion.
Most incurred out-of-pocket costs for their abortion services including 62% of those obtaining a medication abortion, 68% of those obtaining a D&C procedure, and 76% of those obtaining a D&E procedure (Figure 4). This can include copays, coinsurance, or deductible amounts. Among those with some out-of-pocket costs, 62% had a copay, 29% paid something towards their deductible, and 40% had some coinsurance payment.
Among those with out-of-pocket costs, half with a medication abortion or D&C procedure paid less than $70. However, a quarter paid more than $121 for a medication abortion and more than $194 for a D&C. Median out-of-pocket amounts on the day of a D&E procedure were $235, but those in the upper quartile paid close to $1,000 out-of-pocket (Figure 5).

The site of abortion services can have a substantial impact on the amount of out-of-pocket costs incurred by the patient. While out-of-pocket costs for medication abortion are similar in office-based and ambulatory/outpatient hospital settings, procedural abortions in ambulatory/outpatient hospital settings result in higher out-of-pocket costs for patients compared to those in office-based settings. The differences are largest for D&E procedures where the median out-of-pocket costs for a D&E procedure in an office-based setting is $90 compared to $616 in an ambulatory/outpatient hospital setting. Those in the upper quartile paid around $200 and more out-of-pocket for an office-based D&E procedure, while those in an ambulatory/outpatient hospital setting paid more than $1500 out-of-pocket (Figure 6). Higher out-of-pocket costs in ambulatory/outpatient hospital settings compared to office-based setting is not unique to abortion services.
Of the nine states that have passed policies eliminating cost-sharing for abortion in state-regulated plans, five were in effect in 2023, which is the most recent year of the Merative Marketscan Claims data: OR, CA, MA, MD, and NY. On average, in these five states, the share of women with cost-sharing for an abortion decreased substantially from 82% in 2022 to 60% in 2023 (Figure 7). In states that permit cost-sharing for abortions in their state-regulated plans, there was essentially no change in the share of women with cost-sharing for abortions from 2022 (80%) to 2023 (79%).
The reduction in the share of women with cost-sharing for abortion seems to be largely driven by a large reduction in California, which is also the state with the largest number of abortions in the Merative Marketscan Claims. However, Maryland, New York, and Oregon also saw reductions in the share of women with cost-sharing for abortion from 2022 to 2023. The Merative Marketscan Claims data include both state-regulated and self-funded plans that are generally not subject to state requirements for insured plans and it is not possible to determine which plans in the claims data are state-regulated or self-funded. Therefore, the reduction in cost-sharing in states that have eliminated cost-sharing for abortions could represent women enrolled in state-regulated plans or it could demonstrate a spillover effect into self-funded plans following state requirements or both.
On the Horizon
Policies that eliminate cost-sharing for abortion services could encourage individuals to use their insurance to pay for their abortion service rather than pay directly for the services. For many this will be a substantial reduction in out-of-pocket costs, potentially making abortion services more accessible and affordable for those with coverage. Women with low incomes are disproportionately affected as they are less likely to be able to afford the out-of-pocket costs for an abortion without relying on assistance or forgoing the service.
While eliminating out-of-pocket costs for abortion care could increase plan premiums, the University of California found these increases if implemented in the state would be less than 0.01% of premium costs, a minor increase. Plans pay significantly more for pregnancy care and labor and delivery than abortion services. Abortion care also tends to be more isolated episodes without requiring substantial ongoing care and therefore has lower impact on premiums.
It should be noted that even if out-of-pocket costs for abortion services are eliminated, the many costs outside of the actual service, such as travel, lodging, unpaid time off, can still place a financial burden on individuals seeking abortion services, particularly for those living in states where abortion is banned or restricted and must travel for their care.
Methods
The 2023 Merative Marketscan claims database was used to examine the amounts paid by insurance for abortion and related services, the share of females ages 18 to 49 who had out-of-pocket charges for their abortion, and the amount of out-of-pocket costs paid for the abortion and associated services on the day of the abortion and within five days prior to the abortion. Out-of-pocket costs were calculated by summing the coinsurance, copay, and deductible costs among those with any out-of-pocket costs (i.e. greater than $0). Claims representing 7,685 unique abortions: 4,137 medication abortion claims, 1,916 dilation and curettage (D&C) claims, and 1,531 dilation and evacuation (D&E) claims were identified (Table 1). All spending on the day of the abortion, as well as other associated services provided within the 5 days prior to the abortion, including ultrasounds, office visits, pain medication/sedation, Rh testing and/or treatment, cervical dilator, specimen handling, and the surgical tray were also included in the analysis since many state laws mandating coverage, include the abortion itself as well as abortion-related medical services.