Medicaid: What to Watch in 2026
At the start of 2026, many issues are at play that could affect Medicaid coverage, financing, and access to care. Medicaid, which is administered by states within broad federal rules, provides comprehensive health and long-term care coverage to one in five low-income Americans. A more tenuous fiscal climate in 2026 coupled with implementation of the 2025 reconciliation law will put pressure on state Medicaid programs. While major legislative changes to Medicaid at the federal level are unlikely in 2026, key areas to watch include federal policy actions such as new regulations or guidance related to work requirements, implementation guidance for other components of the 2025 reconciliation law, and states’ policy actions in response to federal policy changes and state budget pressures.
Medicaid issues are likely to intersect with broader health care coverage and affordability debates, including the expiration of the enhanced premium tax credits for Affordable Care Act (ACA) coverage and efforts by the administration to control drug prices and hold insurance companies accountable, leading up to the mid-term elections in November 2026. At the federal level, these elections could affect the make-up of Congress and at the state level, they could affect control of state legislatures and governors’ offices. There will be 39 gubernatorial elections (18 incumbent governors running for reelection and 21 incumbent governors who are either term-limited or not seeking reelection).
Medicaid Coverage
In 2026, states will begin implementing Medicaid policy changes that are estimated to increase the number of people without health insurance by 7.5 million in 2034. Over half (5.3 million) of people newly uninsured from Medicaid changes would come from new work requirements for Medicaid enrollees in the ACA Medicaid expansion group or enrollees in partial expansion waiver programs (Georgia and Wisconsin) starting January 1, 2027. Beyond work requirements, the 2025 reconciliation law made other Medicaid eligibility changes, including pausing implementation of some provisions in two Biden-era eligibility and enrollment rules (that aimed to streamline complex processes), restricting Medicaid eligibility for certain lawfully-present immigrants, and requiring states to conduct more frequent eligibility redeterminations for ACA expansion adults.
States will need to make major policy decisions and systems upgrades, likely in advance of formal federal guidance, to be ready to implement work requirements in January 2027. Operationalizing new Medicaid work requirements will require changes to state eligibility systems and processes, enhanced data sharing infrastructure, and targeted enrollee outreach and education, all of which will demand staff resources and funding that will limit attention to other Medicaid priorities. The short timeline for making these changes means states will need to move forward with key decisions before formal guidance from the Centers for Medicare and Medicaid Services (CMS) may be available, increasing the risk that they will have to make adjustments to align with federal policy, which could increase costs. Despite these challenges, some states have indicated a desire to implement work requirements before the January 2027 deadline. To date, Nebraska is the first to announce it will begin enforcing federal work requirements early, starting May 1, 2026.
Federal immigration policies and state policy choices could have implications for Medicaid coverage in 2026. In addition to federal legislative changes, broader immigration policies, such as changes to the public charge rules, new agreements for CMS to share Medicaid data with Department of Homeland Security (DHS) and Immigration and Customs Enforcement (ICE), and continued public immigration enforcement activity could result in fewer legal immigrants obtaining or maintaining Medicaid coverage. In the face of increasing fiscal pressure, several states have announced they are rolling back state-funded coverage for immigrants who are not eligible for federally-funded Medicaid, which will further limit coverage options for immigrants. States may also adopt other eligibility restrictions in an effort to reduce state costs.
Medicaid Financing
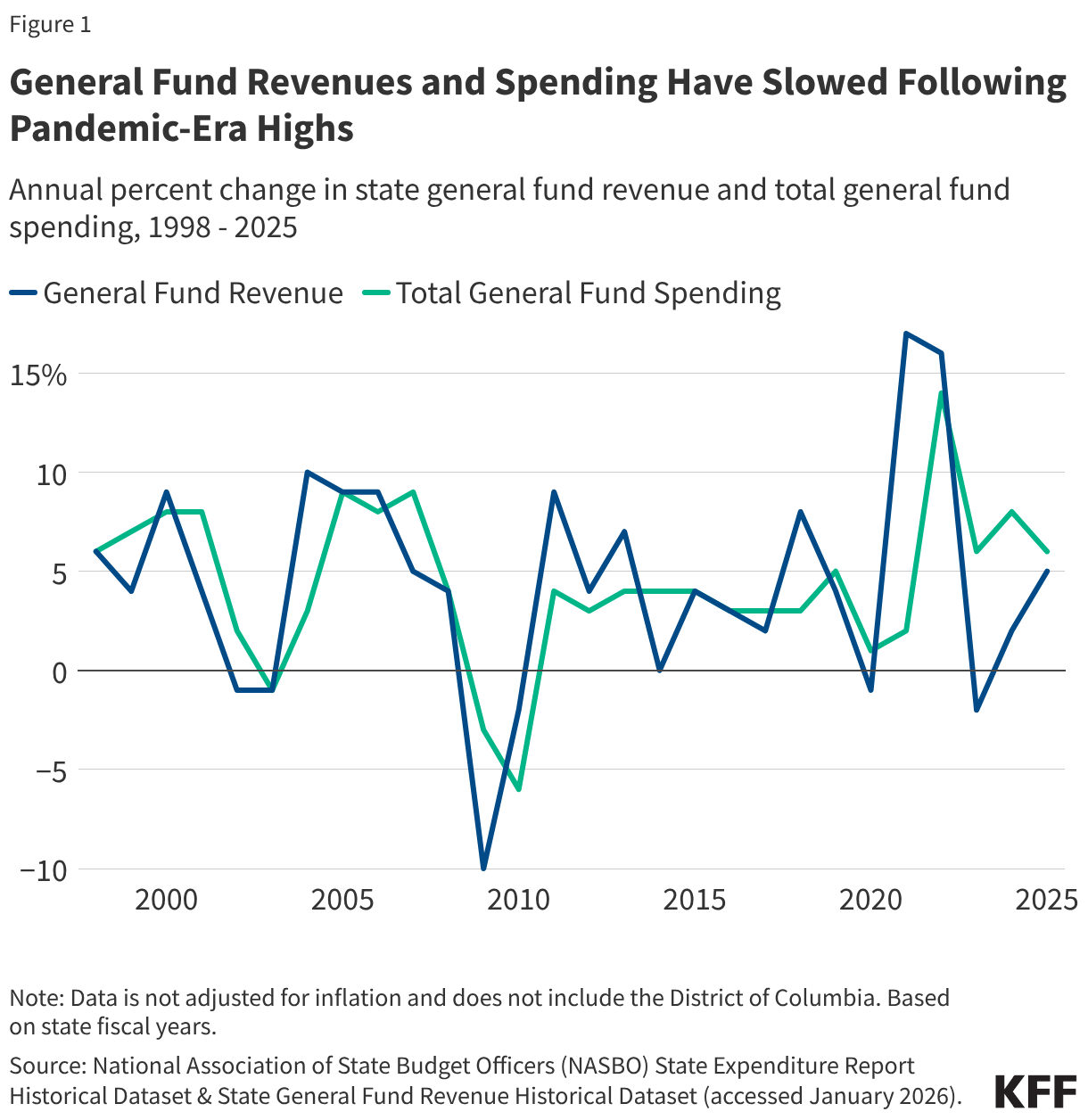
Cuts to federal Medicaid spending will exacerbate the fiscal challenges states are experiencing because of slowing revenue growth and increasing spending demands. The 2025 reconciliation law made historic cuts to federal Medicaid financing, which are estimated to reduce federal Medicaid spending by $911 billion over 10 years. Although the most significant changes to federal Medicaid financing don’t take effect until October 2027 or later, some states will experience more immediate effects resulting from changes to federal requirements governing provider taxes. One of the most immediate effects is that states are prohibited from establishing any new provider taxes or increasing existing taxes. Historically, states have used provider taxes as a means of sustaining Medicaid funding in times of slowing revenue growth or increasing spending demands, but that tool is no longer available because of the new prohibition.
Some states may also face reductions to states’ budgeted revenues for 2026 because of more immediate changes to federal provider tax rules. This would occur in two types of cases:
- States that had adopted new provider taxes for state fiscal year (FY) 2026 may not be able to implement those taxes if they had not done so by July 4, 2025, and
- States that have implemented provider taxes with a special waiver from CMS known as a “uniformity waiver,” may need to revise their taxes as early as April 1, 2026 because of new limits on the use of such waivers (estimated to affect at least seven states including California, Illinois, Massachusetts, Michigan, Ohio, New York, and West Virginia).
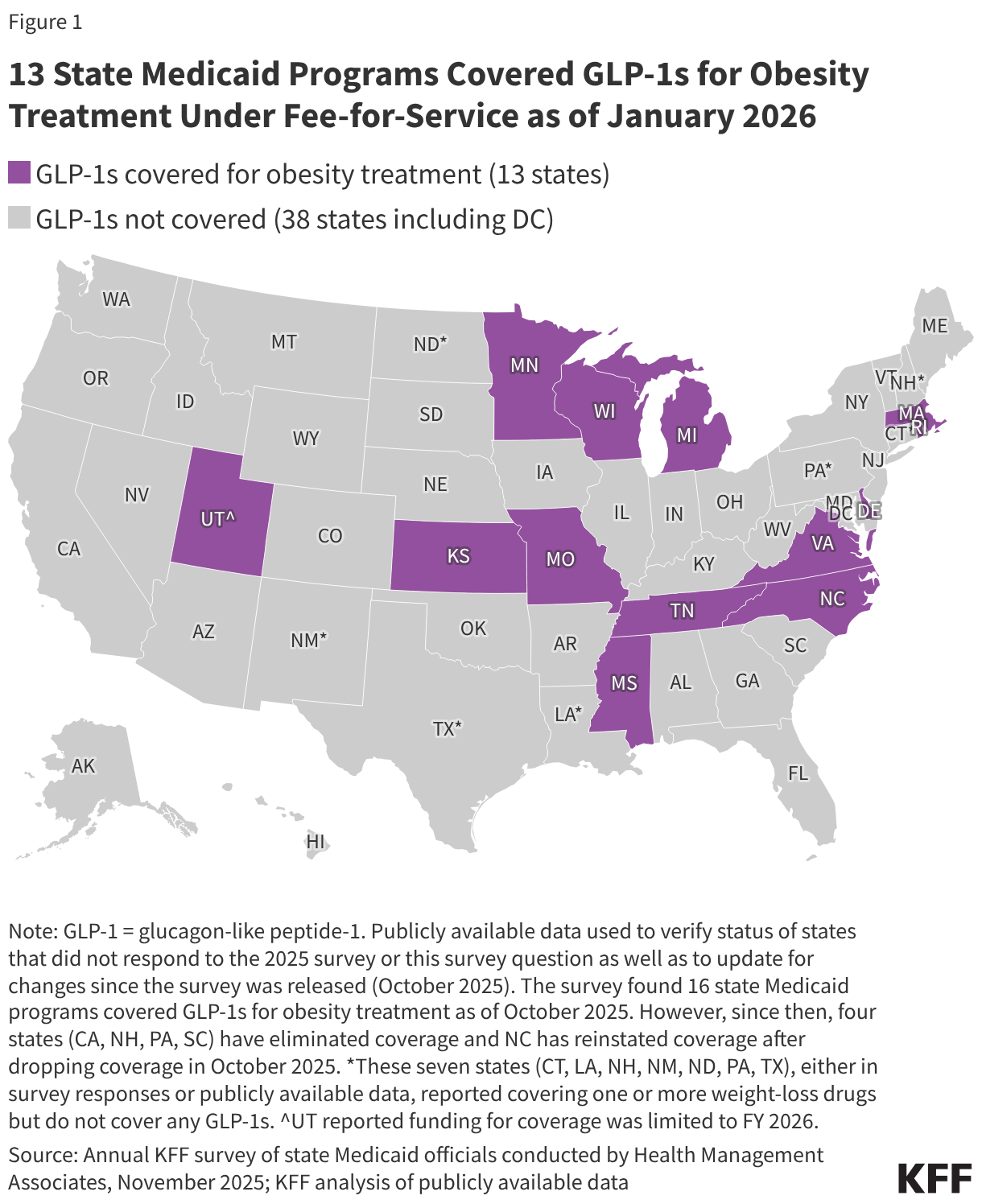
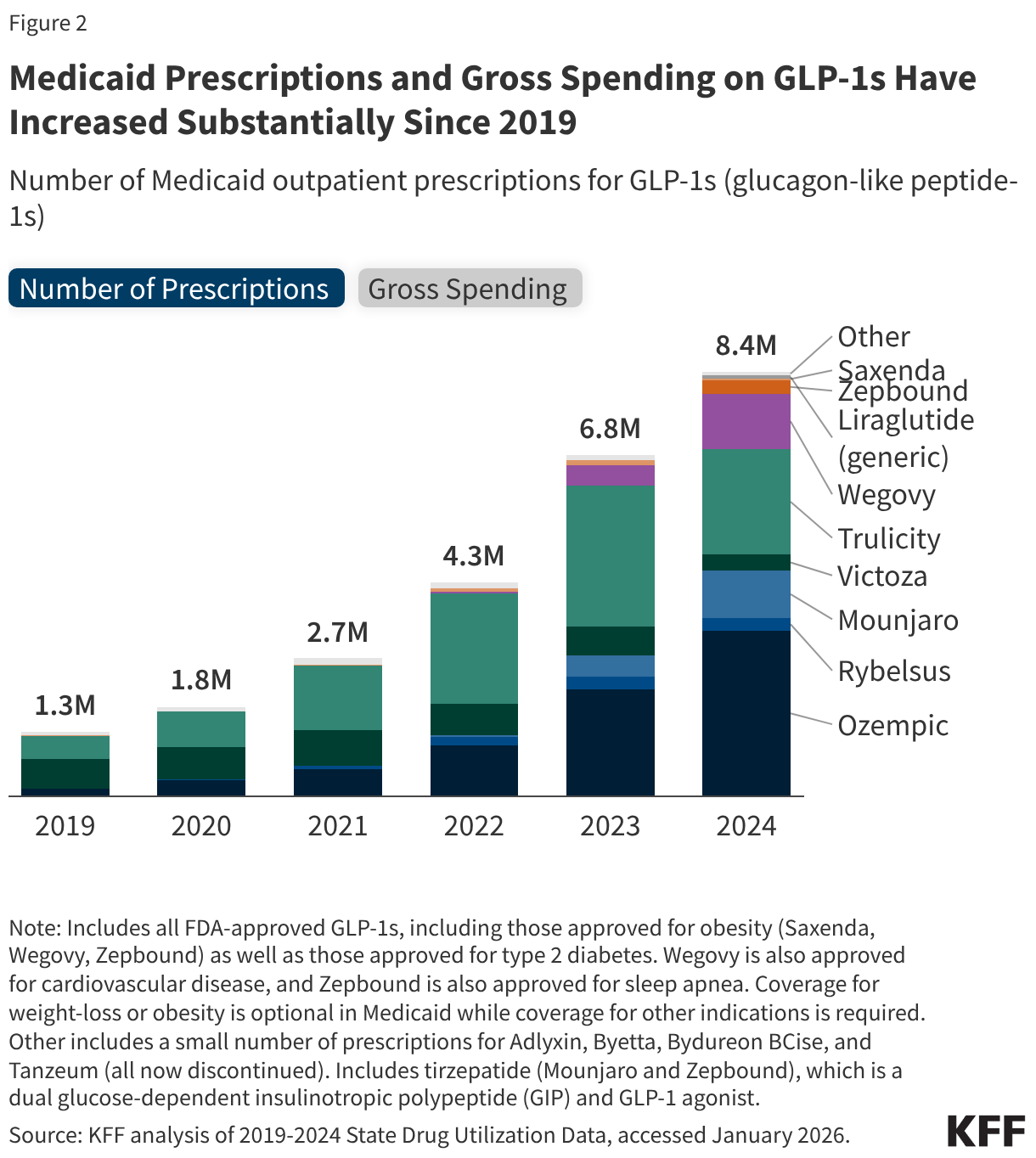
To address slowing revenue growth and increasing spending demands, states may seek to restrict Medicaid provider reimbursement rates, benefits, or eligibility to reduce state Medicaid spending. For example, four states eliminated GLP-1 coverage for obesity treatment in late 2025 likely reflecting recent state budget challenges and fiscal uncertainty. While state Medicaid programs must cover nearly all drugs, a long-standing statutory exception allows states to choose whether to cover weight-loss drugs under Medicaid, resulting in limited state coverage of GLP-1s for obesity treatment. Recent governors’ budgets have included restrictions for other Medicaid benefits including dental and home care. States’ fiscal challenges in 2026 stem from factors other than the 2025 reconciliation law, but the law may exacerbate such challenges. Beyond limiting revenues in states affected by the provider tax provisions, states will need to spend more to implement the law’s requirements, most notably the new work requirements that start January 1, 2027. While the 2025 reconciliation law included some resources to implement policy changes, states may need to make additional investments in systems or workforce to comply with multiple and complex policy changes. Because states pay less than 50% of total Medicaid costs, reductions in state funding will have even larger effects on total Medicaid spending. For example, on average, states accounted for 35% of total Medicaid spending in federal fiscal year 2024. At that rate, a decrease of $100 million in state Medicaid spending would decrease total Medicaid spending by $286 million.
Recent Trump administration prescription drug initiatives could result in savings for state Medicaid programs, though questions remain about the implementation and impact of the deals. In fall 2025, the Trump administration announced reaching agreements with some drug manufacturers, including Pfizer and AstraZeneca, to provide most-favored nation (MFN) prescription drug pricing in Medicaid. MFN prices will be available to state Medicaid programs through the GENEROUS (GENErating cost Reductions fOr U.S. Medicaid) Model, a voluntary drug payment model through which CMS will negotiate supplemental drug rebates based on prices paid in other countries. The Trump administration also recently announced the BALANCE (Better Approaches to Lifestyle and Nutrition for Comprehensive hEalth) Model, another voluntary model that intends to expand access to obesity drugs in Medicaid and Medicare by negotiating lower GLP-1 prices with manufacturers. While lower prices for state Medicaid programs through the recently announced models could result in reduced Medicaid prescription drug spending and potentially expanded coverage of obesity drugs, how the new lower costs under the models compare to the net prices state Medicaid programs currently pay and how states or manufacturers will respond remain unclear. Due to the design of the Medicaid Drug Rebate Program (MDRP), Medicaid programs already typically pay lower prices, net of rebates, than other payers. Further, the recent announcements will not impact costs for Medicaid enrollees as they already pay little or no copays for prescription drugs.
Medicaid Access to Care
State decisions to restrict provider reimbursement rates or benefits in response to federal Medicaid spending cuts could limit access to care for some Medicaid enrollees in 2026. Changes to Medicaid financing will make it difficult for states to increase payment rates to providers and may create pressure for states to restrict payment rates. Reduced or stagnant payment rates to providers coupled with rising costs and increases in the number of people who are uninsured (from Medicaid and Marketplace coverage changes) could pressure providers to reduce staff, services or potentially close. Some providers already struggling financially, such as rural hospitals or hospitals serving a high share of Medicaid enrollees, could face more challenges. An influx of funding from the Rural Health Transformation Program may help to mitigate some challenges in the near term, but those funds are temporary and not expected offset the full magnitude of Medicaid funding cuts over the next ten years. Restricting Medicaid coverage of “optional” services (like behavioral health or home care) could result in less access to care for people with complex health conditions. This may be particularly likely for home care services, where existing tools for managing spending such as caps on total spending or enrollment make it easier for states to limit spending in the future.
The administration may shape Medicaid access through actions to curtail or approve new Section 1115 Medicaid demonstration waivers. Such waivers allow states an avenue to test new approaches in Medicaid if the Department of Health and Human Services (HHS) Secretary determines the waiver is likely to “promote the objectives of the Medicaid program.” Waiver priorities may shift from one presidential administration to another. For example, the Trump administration has rescinded Biden-era 1115 waiver guidance on covering health-related social needs (HRSN) services, indicated plans to phase out certain waiver financing tools (related to use of “Designated State Health Programs” (DSHP), notified states that it does not anticipate approving or extending waivers with continuous eligibility provisions for children and adults or workforce initiatives. While the Trump administration has indicated the phase out or rescission of certain Biden-era waiver policies, the administration has not provided details about its priorities for the use of 1115 waivers. The 2025 reconciliation law included a new provision that requires the Chief Actuary at CMS to certify that 1115 waivers are not expected to result in an increase in federal expenditures compared to federal expenditures without the waiver. While “budget-neutrality” for waivers has been required under long-standing policy and practice, typically the calculations are determined on a per enrollee basis over the course of the waiver and are negotiated between states and the administration.
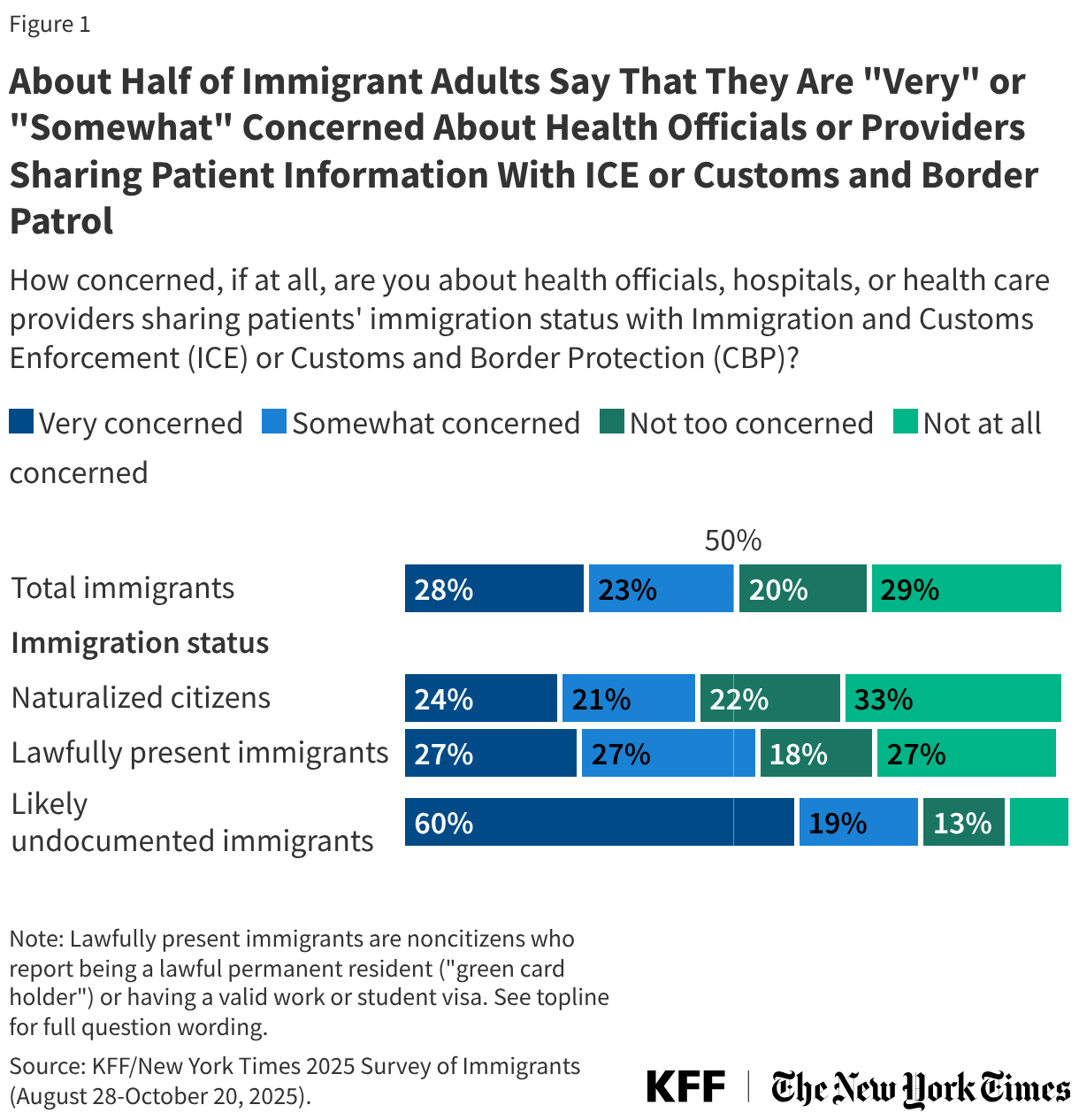
Workforce challenges tied to reimbursement rate policies and changes in immigration policy could also exacerbate access challenges. KFF survey data finds that 13% of immigrants have avoided going to work since January 2025 because of concerns about drawing attention to someone’s immigration status, a number which rises to 40% among people who are likely to be undocumented immigrants. Such concerns are most significant for the long-term care workforce because Medicaid is the dominant payer for care and more than one in four long-term care workers are immigrants. Beyond long-term care, immigrants constitute a large share of workers in other health care fields, including over one in four physicians in US hospitals.
What to Watch
The issues identified in this policy watch could have major implications for Medicaid coverage, financing, and access to care. Key questions for each of these areas will be important to monitor as debates evolve leading up to the mid-term elections, which will have significant implications for Medicaid and health policy in general in the years ahead.
Medicaid coverage changes:
- How will federal guidance shape implementation of work requirements and other eligibility changes in the reconciliation law?
- How will states implement Medicaid work requirements? How many states will implement work requirements ahead of the January 2027 deadline? Will any states be granted good faith waivers to delay implementation?
- Will states adopt additional eligibility restrictions in budgets for FY 2027?
- How will aggregate and state enrollment trends evolve during 2026?
Medicaid financing changes:
- How will federal Medicaid financing changes affect state budgets and provider rates in 2026?
- How will state financing challenges affect the development of their FY 2027 budgets?
- Will states be able to offset reduced federal funding with state funding or will states adopt policies to restrict Medicaid? What policies will states adopt to reduce state Medicaid spending?
- Will states be able to sustain recent increases in provider rates or expansions in services, particularly for long-term care and behavioral health?
Medicaid access changes:
- How will broader changes in Medicaid coverage affect access to care?
- How will changes in Medicaid 1115 waiver policy affect access to care?
- Will changes in financing result in hospital or other provider closures and what will that mean for access to care? Will funding for providers from the rural health transformation fund offset restrictions from other federal and state policies?
- How will broader immigration policies affect the long-term care workforce and access to services that are predominantly funded by Medicaid?