KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
After failed Senate votes late last year and no subsequent bipartisan agreement, the enhanced premium tax credits expired as of January 1. Some states, particularly those operating State-Based Marketplaces (SBMs), have been preparing for this possibility for months and are moving to blunt the impact on consumers by implementing their own state-funded subsidies and implementing other programs aimed at stabilizing the cost of unsubsidized premiums.
State-Specific Subsidies
SBMs have the flexibility under the Affordable Care Act to offer additional state-based subsidies on top of federal premium tax credits to further lower monthly premium payments for Marketplace enrollees. A few SBMs have enacted their own supplemental premium subsidies to maintain affordability and enrollment now that the enhanced premium tax credits have lapsed.
New Mexico has advanced two measures that would backfill the lost enhanced premium tax credits in their entirety for all consumers in 2026. BeWell, New Mexico’s Health Insurance Marketplace, will backfill all of the lost federal tax credits for enrollees with annual incomes up to 400% FPL. Additionally, for enrollees making above 400% of poverty, New Mexico financial assistance will cap premium payments for a benchmark plan at 8.5% of their household income, mirroring the structure of the enhanced premium tax credits.
Other states have moved to fully backfill the expired tax credits for a portion of enrollees. Maryland, for example, adopted a single-year state premium assistance program that replaces 100% of the lost federal subsidy for enrollees below 200% of the federal poverty level (FPL) ($31,300 for an individual signing up for coverage in 2026) and partial replacement of the lost enhanced tax credit for those with incomes above 200% up to 400% FPL. However, there is no additional state assistance to replace tax credits lost by people with annual incomes above 400% FPL, who are now completely ineligible for any tax credits with the reinstatement of the “subsidy cliff.”
California is allocating funds to fully replace the premium tax credits for enrollees making up to 150% FPL and partially replace the lost credits for those with incomes between 150% and 165% FPL in 2026. With California receiving about $2 billion annually in enhanced premium tax credits, only a small share of the federal tax credits will be backfilled by these state-specific subsidies. Like in Maryland, California also does not have any additional state assistance to replace enhanced premium tax credits for people with annual incomes above 400% who have lost eligibility for any federal premium assistance since January 1.
Some states, like Colorado and Washington, have also retooled or created state-specific subsidy programs to provide an additional flat dollar amount to enrollees. However, in many cases, these dollar amounts fall short of entirely backfilling lost federal tax credits. In Colorado, a maximum dollar amount of $80 per month for an individual enrollee (and an additional $29 for each subsequent family member) is provided to households making between 100% to 400% of poverty. This plan will backfill about 40% of the lost federal assistance. Washington is retooling their existing Cascade Care Savings program, setting new fixed dollar maximums for 2026 to provide some relief to consumers ($55 per member per month for those receiving federal tax credits and $250 per member per month for those not receiving subsidies).
Prior to the creation and expiration of the enhanced tax credits, some SBMs already had additional state assistance in place on top of federal premium tax credits. States such as New York, Connecticut, Vermont, Massachusetts, and New Jersey all have state-specific subsidies that are not directly related to the expiration of the enhanced premium tax credits and will remain in place whether or not they are extended. Additionally, New York and Oregon operate a basic health plan or similar program that provides coverage to certain low-income residents who would otherwise be eligible for Marketplace plans, offering lower premiums and cost sharing regardless of changes to federal tax credit policy.
Reinsurance Programs
Several states also operate Section 1332 reinsurance programs that reduce unsubsidized premiums by reimbursing insurers for a share of high-cost claims. These programs do not replace lost federal subsidies, but they help stabilize the unsubsidized premiums some consumers will face the full cost of in 2026. Specifically, these are individuals and families with annual incomes over 400% FPL who will be entirely locked out of eligibility for financial assistance with the reinstatement of the “subsidy cliff” and face some of the largest increases in premium payments.
Maryland’s reinsurance program, in place since 2019 and extended through 2028, has lowered premiums by as much as 35% relative to what they would have been, according to state findings, and is expected to continue softening premium growth when enhanced premium tax credits expire. Colorado, New Jersey, Georgia, and Oregon operate similar programs. Colorado and New Jersey say that these programs have reduced statewide unsubsidized premiums by roughly 20% and provide even greater relief in rural rating areas. In Georgia and Oregon, their reinsurance programs have reduced the cost of unsubsidized premiums by at least 10%.
Enrollment Assistance
On top of state-based subsidies and reinsurance programs, some states may also increase outreach to help consumers shop for lower-cost options. But navigator programs have faced repeated federal funding cuts, limiting the ability of states, particularly those without robust state-based outreach budgets, to rely on enrollment assistance as a tool for mitigating affordability challenges.
Limited Relief
A small subset of states (and just a portion of those that operate SBMs) have moved to blunt the impact of the enhanced premium tax credits expiration on enrollees. While expanded state subsidies and reinsurance programs may soften the impact of the enhanced premium tax credit expiration for some consumers, they are unlikely to substantially alter the projected coverage losses. Collectively, these efforts from a small handful of states represent only a small fraction of the roughly $35 billion it would take to extend the enhanced premium tax credits each year, underscoring that state-level actions can mitigate, but not replace, the role of federal policy in sustaining ACA Marketplace coverage.
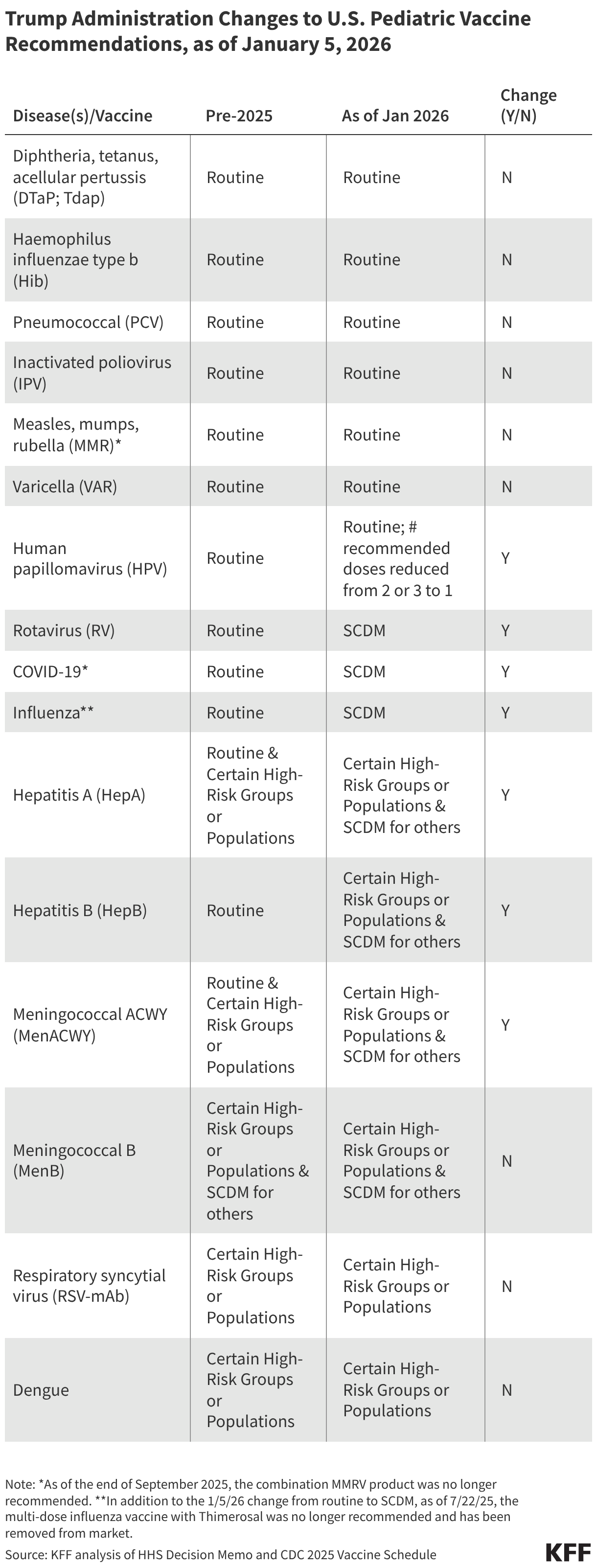
As widely expected, and following a recent Presidential memorandum, the Department of Health and Human Services (HHS) issued a memo on January 5, 2026 implementing major changes to the government’s recommended vaccination schedule for children, adding to other changes previously made in 2025. Collectively, these changes reduce the number of vaccines recommended for all children and, as such, have important implications for childhood immunizations and U.S. public health broadly, especially given the context of already declining childhood vaccination rates and ongoing outbreaks of diseases such as influenza and measles. While states, not the federal government, ultimately determine which vaccines are recommended for children and required for school entry, the federal government has significant influence over vaccine policy and access. This policy brief provides an overview and identifies several implications of these changes.
Starting in 2025, changes by HHS to routine vaccine recommendations for children have reduced the number of diseases targeted from 17 to 11 and the number of routine vaccines from 13 to 7 (see Table). Due to changes starting in October of last year, there are now six vaccines no longer recommended for routine use by all children in the United States: rotavirus, COVID-19, influenza, hepatitis A, hepatitis B, and meningococcal vaccines. Instead, some of these vaccines are now recommended for a narrower group of children, based on certain risk criteria or other specific factors, and all six have been moved from the routine category of vaccination to “shared clinical decision making” (SCDM), a process that is “individually based and informed by a decision process between the health care provider and the patient or parent/guardian.” Beyond these changes, while HPV vaccine remains routinely recommended, HHS has reduced the number of recommended doses from two or three (depending on age of initial vaccination) to one.
Insurance coverage for childhood vaccines is not expected to change, although there is one exception. Most insurers are required to cover the Advisory Committee on Immunization Practices (ACIP)/Centers for Disease Control and Prevention (CDC) recommended vaccines at no-cost (including those recommended through SCDM), either due to requirements of the Affordable Care Act or other federal statutes and as such, these changes should not affect coverage, as also stated by HHS officials. Thus, parents wishing to vaccinate their children against diseases no longer recommended for all children but available through SCDM may still do so without having to be concerned about out- of-pocket costs. One potential exception relates to the HPV vaccine: now that the federal government recommends just one dose of HPV (instead of the previously recommended two to three doses), insurers will not be required to cover an additional dose should parents seek one (the current commercial price for one dose is more than $300). Through the end of 2026, however, health insurers have pledged to continue to cover all vaccines that were recommended in the prior childhood vaccine schedule and several states have moved to mandate free coverage by state-regulated insurers, and could choose to include additional doses.
The new schedule positions the U.S. as an outlier among peer nations in routinely recommending so few vaccines for children. One of the main reasons cited for the new schedule was that the U.S. was an outlier compared to peer countries in recommending so many routine vaccinations for children. Denmark was cited, both at a recent federal advisory committee meeting and in the HHS decision memo, as a model for the U.S. to emulate. The changes made now closely align the U.S. with Denmark (with the only difference being the varicella vaccine which is recommended by the U.S. but not Denmark). No other country among the 20 peer nations that HHS compares the U.S. to in its decision memo recommends vaccines against as few diseases as Denmark, which makes that country, and now the U.S. also, an outlier in this group. For comparison, Australia, Austria, Germany, Greece, Ireland, Italy, Japan, New Zealand, Spain, and the United Kingdom all recommend vaccinating children against 14 or more diseases. More broadly, each country has its own process and unique set of circumstances when it comes to determining vaccine recommendations, and each has developed their childhood vaccination schedule after years of reviewing and weighing available evidence in light of many factors, such as differences in health delivery systems, insurance coverage, public health system capacity, and national priorities. To date no high-income country has made its vaccination decisions based only on what a “peer” country does.
The process used to make these changes marks a departure from the past and further changes are signaled ahead. Historically, any major changes to federal vaccine recommendations were developed through an established, deliberative process that included internal government review with experts from the Center for Disease Control and Prevention (CDC) and other agencies, as well as consideration and public debate via meetings of the Advisory Committee of Immunization Practices (ACIP), the external expert advisory group to CDC. Recent changes made under HHS Secretary Kennedy, however, have circumvented this process, and instead changes have been announced without much internal or external consultation, and without prior public notice. This occurred with Secretary Kennedy’s announcement on social media that HHS was narrowing its COVID-19 recommendations, and now with an announcement of a new childhood vaccine schedule that was not reviewed by CDC experts nor given a public hearing through ACIP. The White House and HHS have also stated they are examining other aspects of vaccine policy including examining whether the measles, mumps, rubella combination vaccine should be divided into separate shots, how vaccines are tested and safety is monitored, and whether liability protections for manufacturers should be reexamined, which could mean further changes to policy may be forthcoming without a standard review processes.
While HHS cites decreased vaccine uptake and declining trust as additional reasons for changing pediatric vaccine recommendations, it is unclear if these changes will address these issues and they could have the opposite effect. By narrowing the groups recommended to receive certain vaccines, the federal government’s changes could lead parents and providers to choose to vaccinate less often than they have previously. Taking a cue from the new federal vaccine schedule, some states may also loosen vaccine requirements for school attendance, which could also result in lower vaccination coverage. In addition, moving vaccines from a routine, universal recommendation to a shared clinical decision-making (SCDM) recommendation can add an additional step or introduce other barriers to vaccine access, further depressing vaccination rates. With six vaccines newly placed in the SCDM category, such barriers could lead to more missed opportunities for vaccinations. In addition, even though federal health officials state that the new schedule is designed to create more public trust in vaccines, it’s not clear how it may affect trust and it could very well do the opposite. Most parents in the U.S. do not believe there are too many recommended vaccines, though MAGA Republican and MAHA parents – a minority of parents overall – are more likely to agree that the government should recommend fewer vaccines. Many states and expert groups are already making vaccine recommendations that differ from those of the federal government, and the new schedule is likely to exacerbate the conflicting messages that parents and providers hear about vaccines. For now, parents and providers will have to navigate a landscape of conflicting messages and recommendations about vaccines, which sows confusion and ultimately makes it harder for people to know what to do.
There will be differential impacts of these changes across the country. Ultimately, it is state and local jurisdictions that hold primary responsibility for determining key childhood vaccine policies, including which vaccines are recommended for routine use and which are required for school attendance. In light of changing federal guidelines that in many cases have narrowed vaccine recommendations, manystates have taken steps to de-link state policies and recommendations from those coming from the federal government, particularly Democratic-led states. For example, KFF analysis finds that 24 states no longer use HHS/CDC as a source for vaccine recommendations (up from just 13 in September 2025) and instead turn to state level or external expert groups such as AAP for guidance; a smaller number mandate free insurance coverage by state-regulated insurers for their own set of recommended vaccines. The divergence between federal policy and the states is likely to grow after the latest changes to federal recommendations, which means vaccine coverage and access could increasingly vary according to where one lives. More limited access in some states could, in turn, lead to decreased vaccine coverage and increased incidence of vaccine preventable diseases.
Tracking how the new vaccine schedule impacts vaccination rates in the U.S. may be challenging due to other HHS policies. It remains to be seen how these new recommendations play out in terms of vaccination rates, but recent Trump administration policies may make tracking these changes more challenging. For example, CDC and other federal staffing and funding going to state and local public health efforts across the U.S. has been cut, jeopardizing data collection and analysis. Further, the Trump administration in December announced that, starting in 2026, states will no longer be required to report several measures related to immunization status to HHS as part of their Medicaid and CHIP reporting requirements. Given that nearly four in 10 children in the U.S. are covered by Medicaid, visibility on their vaccine status will be reduced going forward.
In a letter to state health officials last month, the Centers for Medicare & Medicaid Services (CMS) announced the removal of immunization measures from the Child Core Set and Adult Core Set. These “Core Sets” measure health care performance annually, with the goal of improving the health of Medicaid and Children’s Health Insurance Program (CHIP) enrollees. Dropping Medicaid vaccine reporting requirements may make it more challenging to monitor vaccination trends and the impact of recent vaccine policy changes. This policy watch describes the recent Trump administration changes to Medicaid vaccine reporting requirements and explores what impact this change may have on state Medicaid programs and enrollees.
The “Core Sets” are a set of quality measures designed to measure and improve health care quality and access. The Core Set of Children’s Health Care Quality Measures for Medicaid and CHIP, or the “Child Core Set”, includes quality measures that capture various aspects of children’s health such as behavior health care, preventive care, maternal health, acute and chronic conditions, oral health care, and experience of care as well as vaccination status. The Child Core Set was developed in 2009, voluntary annual state reporting began in 2010, and reporting became mandatory in 2024. There is also a separate set of quality measures for adult enrollees, the “Adult Core Set”. The Adult Core Set was developed in 2012, voluntary annual state reporting began in 2014, and the behavioral health measures became mandatory for states to report in 2024. To enforce compliance with mandatory measures, CMS has the authority to withhold federal Medicaid payments, though states can request a one-year exemption if they are unable to report for a specific population and measure. The Core Set data are made publicly available and are designed to measure health care access and quality for Medicaid/CHIP enrollees, allowing states to monitor health care quality, identify improvement opportunities, and address health disparities.
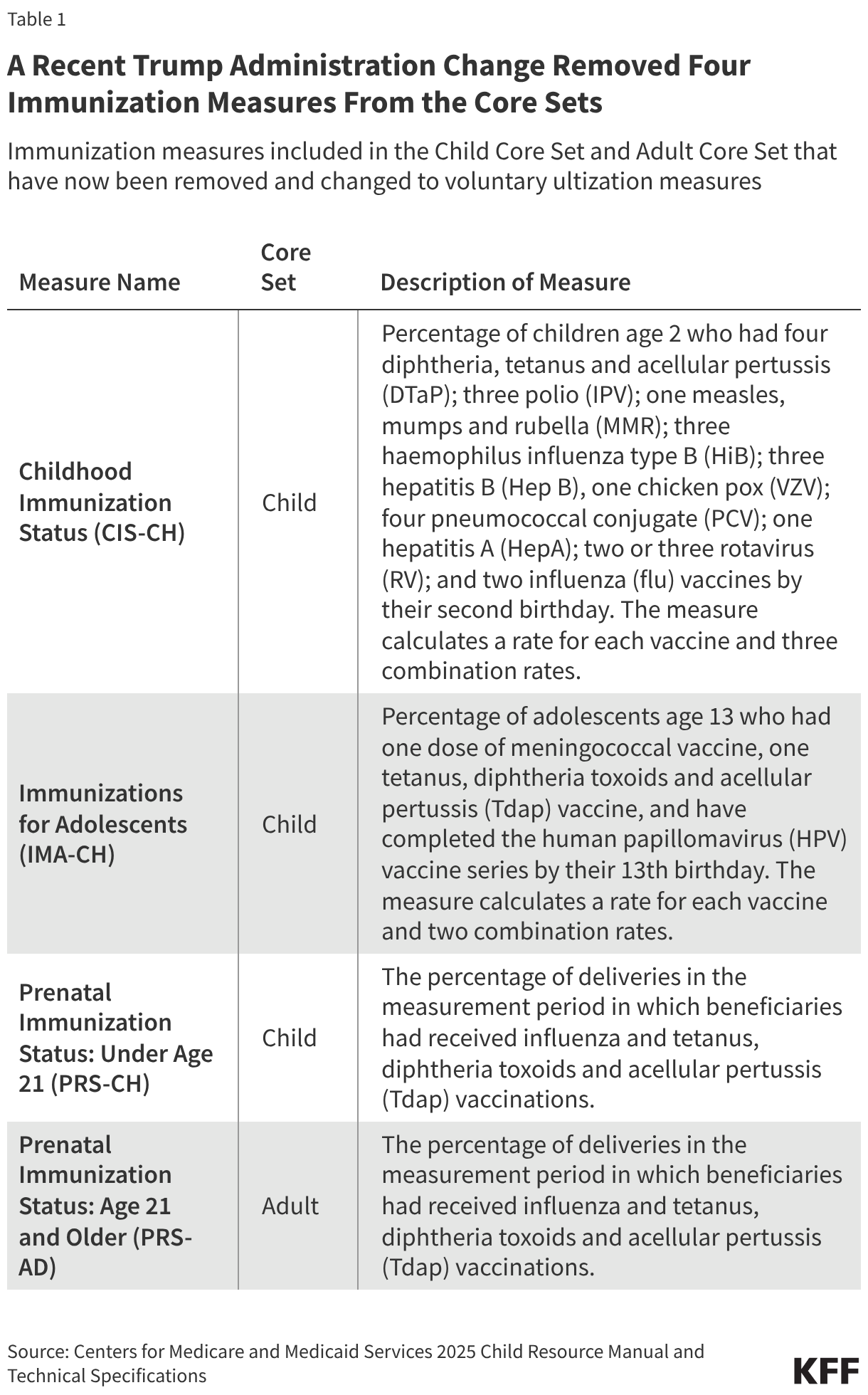
The Trump administration recently removed four immunization measures from the Core Sets, making them voluntary for states to report. CMS’s December 2025 letter to state health officials made all of the immunization-related measures in the Child Core Set and one of two immunization-related measures in the Adult Core Set “voluntary utilization measures” for 2026 and 2027 (see Table 1). The letter also states that federal Medicaid payments are not tied to performance on the immunization quality measures and encourages states not to use the immunization measures in any payment arrangements (for example, incentives for managed care plans). Two other measures for 2027 were retired (Medical Assistance with Smoking and Tobacco Use Cessation, MSC-AD, and the Asthma Medication Ratio, AMR-CH and AMR-AD), though CMS notes that they will explore adding other tobacco use and asthma measures in the future.
The recent Core Set changes did not follow the typical process for updates. To advance and improve the quality measures, CMS is required by federal law to update the Core Sets, ensuring the measures “reflect the testing, validation, and consensus process for the development of pediatric quality measures”. As finalized in federal regulation under the Biden Administration in 2023, the development of the Core Sets each year begins with a workgroup of Medicaid/CHIP stakeholders and quality measure experts who review the Core Sets and make recommendations for changes through the annual review and selection process. The workgroup’s recommendations are then published for public comment and submitted to CMS, who ultimately releases the final Core Sets based on the recommendations. CMS’s recent decision to remove the immunization measures did not follow this process, though the letter notes the Secretary has the “discretion to make changes to the Core Sets that he deems best to improve and strengthen the Core Sets” under federal law.
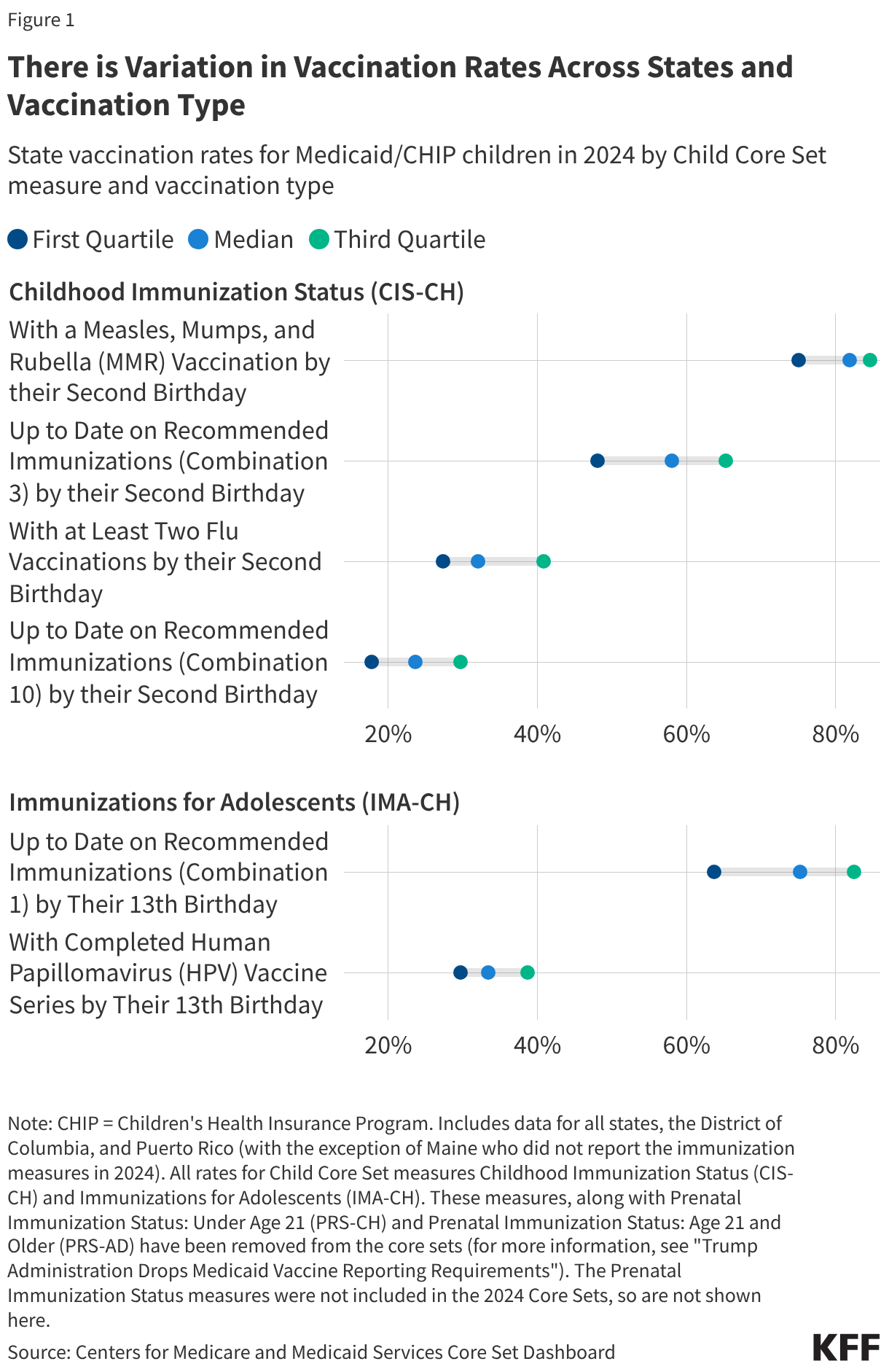
While seemingly a small, technical change, the removal of vaccine reporting in Medicaid and CHIP may make it more difficult to monitor and understand vaccination trends for a large share of children in the U.S. State-level data from the 2024 Child Core Set for the now removed immunization measures show variation in vaccination rates across states and vaccination type (Figure 1) and trends across the 2022-2024 Core Sets show declines in vaccination rates for some vaccines. These data can help state Medicaid programs understand vaccination trends, compare their state to others, inform state Medicaid policy, and improve rates to reach longstanding vaccination rate goals. Nearly four in 10 children in the U.S. are covered by Medicaid, making even small changes to the program relevant to broader children’s health trends.
It remains unclear how many states will continue to report the voluntary immunization measures and what will happen to these measures in future years. Prior to mandatory reporting, the number of states reporting the Child Core Set measures increased over time, with voluntary responses to CIS-CH and IMA-CH (show in Figure 1) reaching 46 to 48 responding states by 2023 depending on the vaccine. Given the infrastructure is already in place to report, states may continue to voluntarily report the immunization measures. However, CMS has indicated they will be considering options for new immunization measures to replace the now voluntary measures. They plan to engage stakeholders, including states, quality measure experts, providers as well as vaccine registry managers and electronic health record vendors, to develop measures that capture “whether parents and families were informed about vaccine choices, vaccine safety and side effects, and alternative vaccine schedules” and to explore whether data can account for “person and family preferences related to vaccines” and religious exemptions for vaccinations. Without the Child Core Set immunization measures, at this time it may still be possible to monitor Medicaid/CHIP children's vaccination trends through other data sources, such as the National Immunization Survey or individual state collected data, but these data are not easily accessible and may not be comparable across states.
Dropping vaccine reporting requirements could also make it more challenging to monitor recent declines in childhood vaccinations rates and the impact of vaccine policy changes. Children’s routine and seasonal vaccination rates have declined in recent years, due in part to rising vaccine hesitancy fueled by vaccine misinformation, increasingly partisan views on vaccine requirements, and a decline in trust of health authorities. In addition, the Administration recently announced significant changes to the children’s vaccination schedule, reducing the number of diseases targeted from 17 to 11 and the number of routine vaccines from 13 to 7. Changes to the vaccine schedule at the federal level (and confusion about the changes) coupled with other public health policy actions under the Trump administration could further drive down vaccination rates among children and increase incidence of vaccine preventable diseases. Limited vaccination status data means reduced visibility into vaccination trends and what impact recent policy changes may have.
In his latest JAMA Forum column, KFF’s Larry Levitt explores how unaffordable health care is in the U.S. in the context of the debate over extending enhanced Affordable Care Act premium tax credits and an upcoming election where affordability will likely be front and center.
Note: This brief was updated on May 21, 2026 to incorporate new data on abortion statistics.
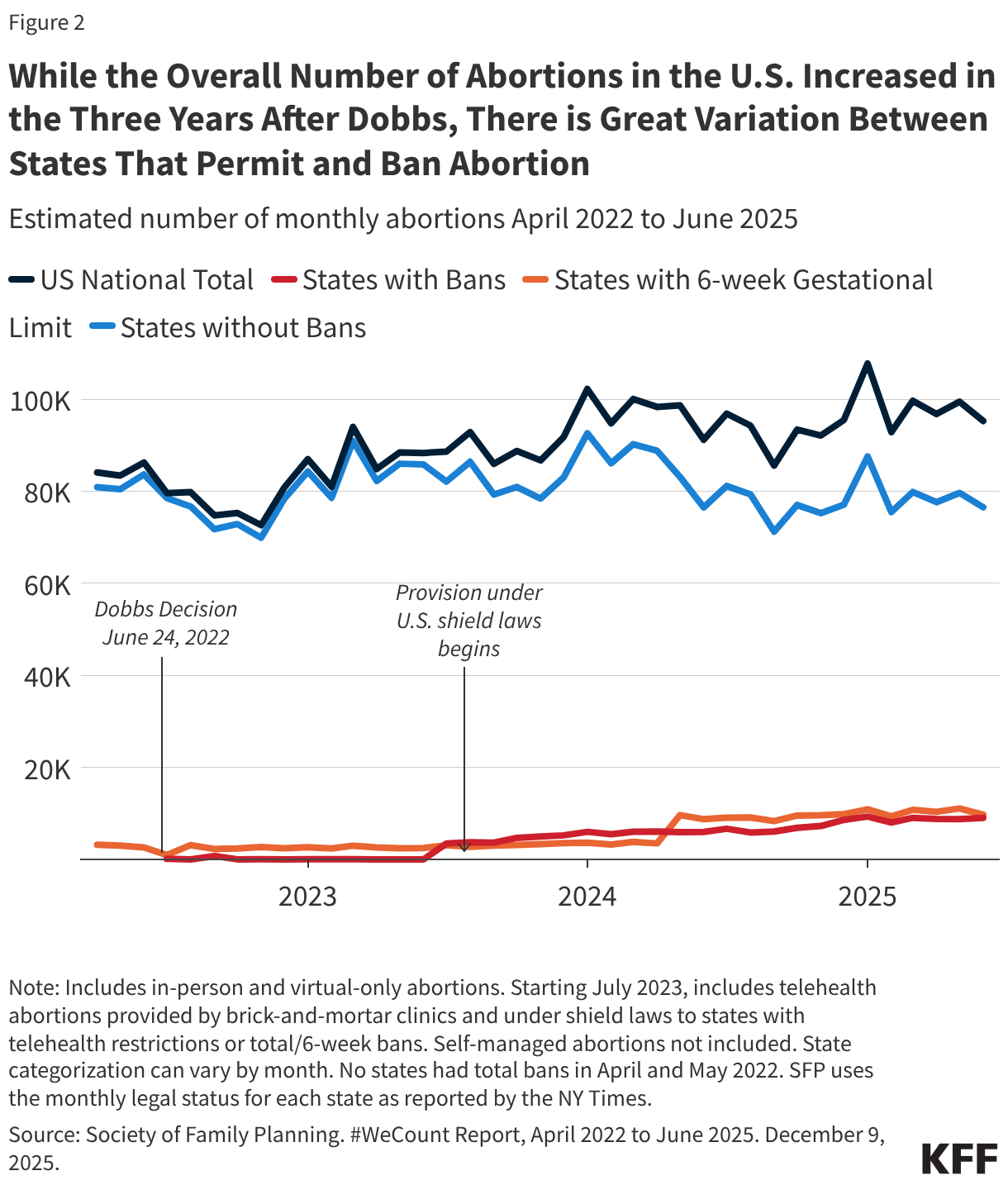
In the three years since the Supreme Court ruling that overturned Roe v. Wade, the total number of abortions nationally has slightly increased. The most recent data from the Society for Family Planning’s #WeCount project show that the average monthly abortion volume during the first half of 2025 was higher than the monthly average in 2024. From January to June 2025, there have been more than 590,000 abortions compared to 1.14 million abortions in all of 2024 and 1.06 million abortions in 2023. For most of the decade prior to the Dobbs ruling, there was a steady decline in abortion rates nationally, with a slight uptick in the years just before the ruling.
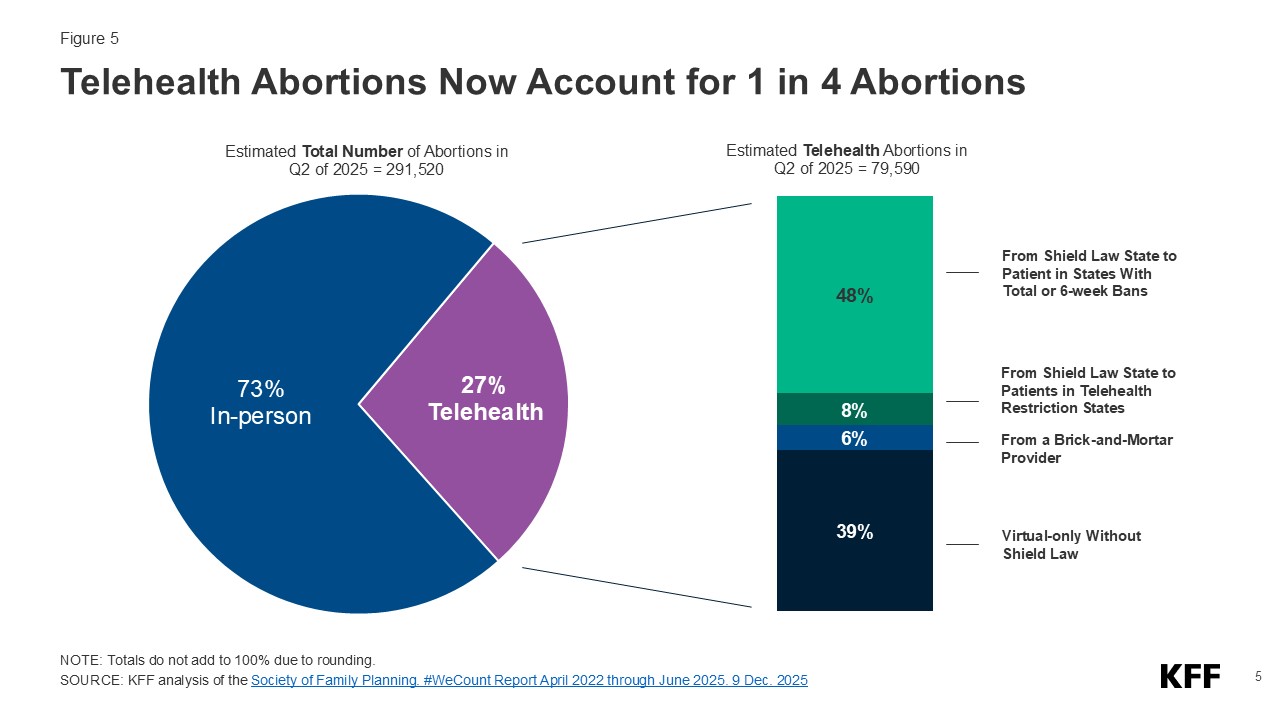
The upward trend in abortion volume is likely due to multiple reasons, including expanded telehealth capacity, the ability to mail medication abortion pills to patients, and the lower costs for telehealth abortions through virtual clinics compared to in-person care. Medication abortion via telehealth now accounts for 27% of all abortions.
In contrast to the abortion bans, several states have passed laws to protect abortion access for their residents and expand access to people seeking abortions from other states which have contributed in part to the increased the number of abortions in those states compared to pre-Dobbs time frame. Twelve (12) states require state-regulated private plans to cover abortion, many without cost-sharing, and 20 Medicaid programs use state-only funds to cover nearly all medically necessary abortions. Twenty-three (23) states passed shield laws intended to reduce the legal risks for clinicians who provide abortion care to patients who live in states where abortion is banned or restricted.
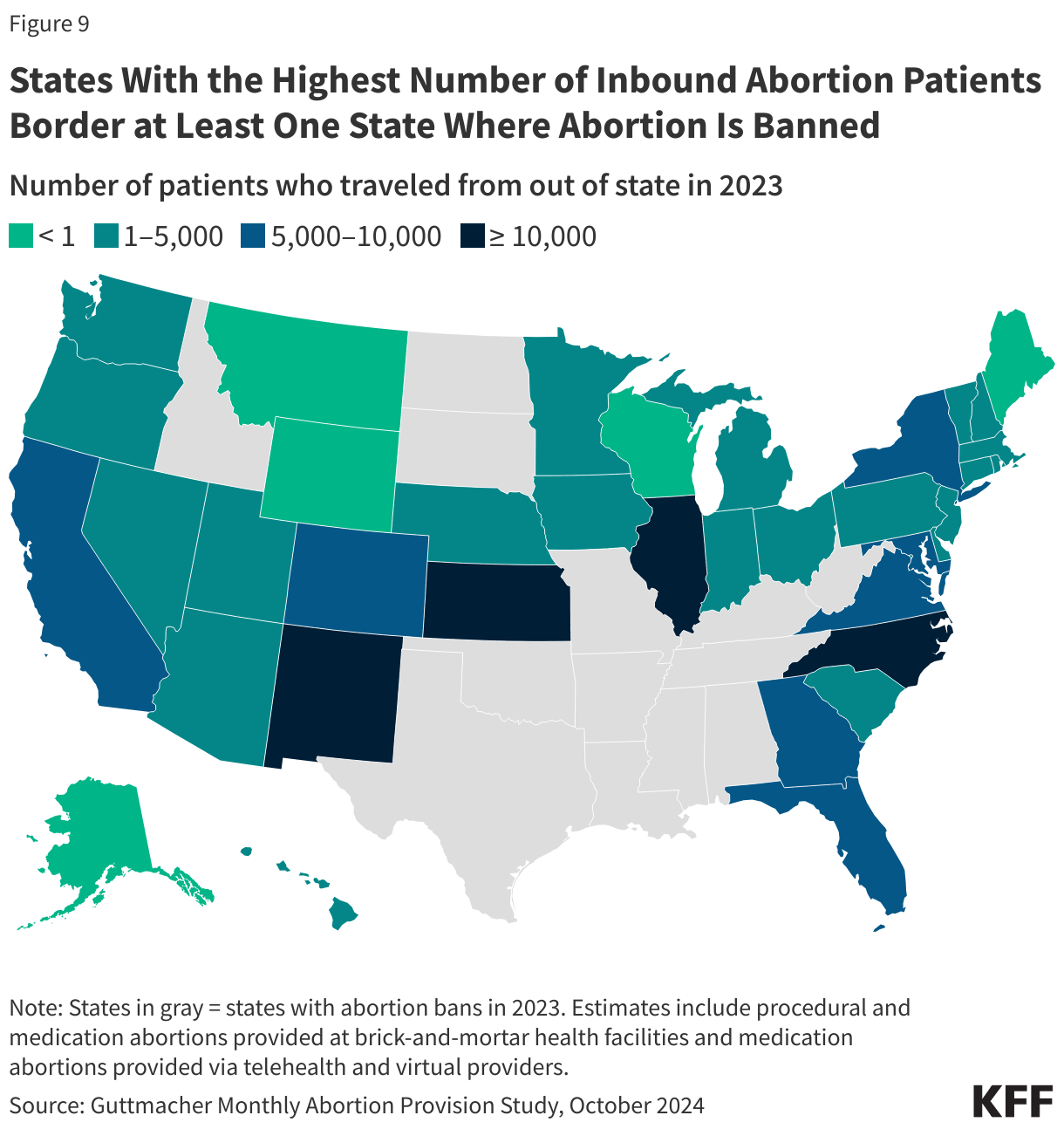
The upward trend in abortion volume can also be attributed to increased interstate travel. The travel rate for abortion care across state lines nearly doubled from 2020 to 2024, with Illinois, North Carolina, New Mexico, and Kansas experiencing the highest volume of out-of-state abortion patients last year.
Following the 2022 ruling in Dobbs v. Jackson Women’s Health Organization, it was generally expected that the abortion rate would drop due to the number of states that rapidly adopted abortion bans (13 states) and early gestational restrictions (6 states). There is no doubt these policies have made abortion access much more challenging or even impossible for those seeking abortion who live in restrictive states; yet, contrary to expectations, recent data show that the number of abortions in the U.S. overall has slightly increased in three years following the Supreme Court ruling. The combination of growth in telehealth availability for abortion care, lower telehealth costs, increased legal reproductive health care protections through state efforts, and higher rates of interstate travel, all likely contributed to the unexpected trajectory in abortion volume. However, the possibility of more state bans and restrictions combined with the ongoing legal challenges seeking to further restrict access may reverse this trend. Additionally, future actions that the Trump administration could take at the federal level could further limit abortion availability and access even in states that have enshrined the right to abortion, particularly if the administration restricts the distribution of medication abortion pills through the Comstock Act or targets the provision of telehealth abortions through regulatory revisions at the Food and Drug Administration.
This brief reviews the different sources of abortion data in the U.S., the factors that have affected abortion rates across the country before and after Dobbs, and what we may see as the Trump administration, Republican majorities in the House and Senate, and a conservative federal judiciary shape policy in the coming years.
How is abortion tracked at the state and federal level?
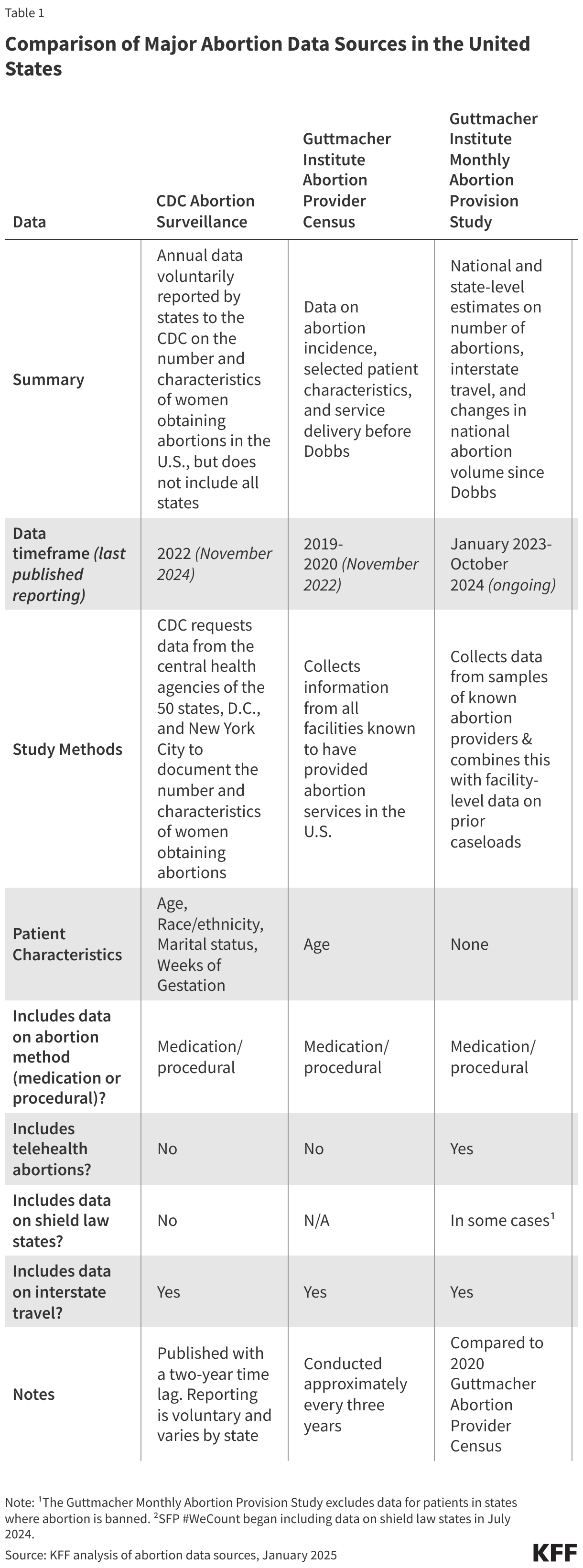
Three major organizations collect and report national and state-level data on abortion volume and rates: the federal Centers for Disease Control and Prevention (CDC), the Guttmacher Institute, and most recently, the Society of Family Planning through its (SFP) #WeCount project.
For decades, the federal CDC Abortion Surveillance System has requested data from the central health agencies of the 50 states, D.C., and New York City to document the number and characteristics of women obtaining abortions. Reporting to the CDC is voluntary and not all states participate in the surveillance system. Notably, California, Maryland, and New Hampshire have not reported data on abortions to the CDC system for years. Most states collect and report data on the demographic characteristics of patients, gestational weeks, and type of abortion procedure. CDC publishes data from the surveillance system annually, with the most recent data on abortions in 2022, reflecting a 2-year lag. Following the termination of federal staff from the agency’s the Reproductive Health Division, it was unclear whether the CDC would continue to update its Abortion Surveillance System which currently presents data from 2022 that was released in November 2024. It has been reported that the next Abortion Surveillance report is expected to be released during spring of 2026 with data from 2023.
Prior to the Dobbs ruling, the Guttmacher Institute, an independent research and advocacy organization, periodically conducted the Abortion Provider Census (APC), collecting data on abortion incidence, abortion facilities, and patient characteristics. Data from the APC are based primarily on questionnaires completed by known facilities that provide abortion in the country, information from state health departments, and Guttmacher estimates for a small portion of facilities. The most recent APC reports data from 2020. Following the Dobbs ruling, the Guttmacher Institute established an additional data collection initiative, the Monthly Abortion Provision Study, to track abortion volume within the formal U.S. health care system. This ongoing effort collects data on and provides national and state-level estimates on abortions while also tracking the changes in national abortion volume since 2020.
While the CDC and Guttmacher APC data differ in terms of collection methods, timeframe, and completeness, both have shown similar trends in abortion rates over the past decade. One notable difference is that Guttmacher’s survey has included continuous reporting from all states, which explains at least in part the higher abortion volume in their data.
Society of Family Planning’s (SFP) #WeCount is a newer national reporting initiative that measures changes in abortion access following the Dobbs ruling. The project provides semiannual reports on the monthly number of abortions by state and includes data on abortions provided through in-person health care settings and through telehealth. The #WeCount report started collecting data in April 2022 and has published two full years of abortion data since Dobbs.
How has the abortion rate changed over time?
For most of the decade prior to the Dobbs ruling, there was a steady decline in abortion rates nationally, but there was a slight increase in the years just before the ruling.
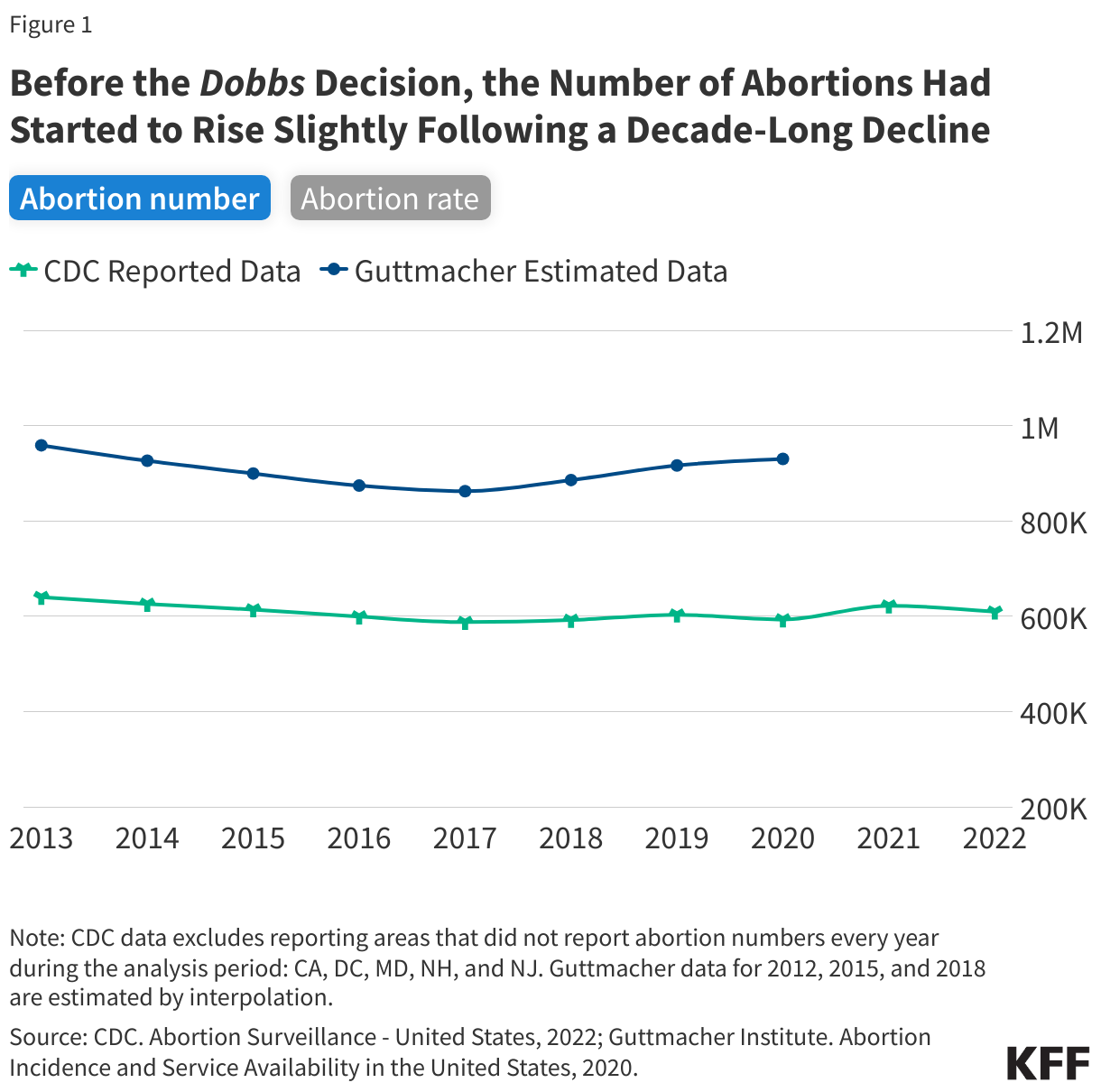
The most recent CDC data are from 2022, the same year as the Dobbs decision, and show that abortion rates declined from 2013 through 2017 and remained steady in the years leading up to the court decision (Figure 1). CDC reported 609,360 abortions in 2022 and a rate of 11.2 abortions per 1,000 women (excludes CA, DC, MD, NH, and NJ). In contrast, the Guttmacher Institute reported 930,160 abortions in 2020 and a rate of 14.4 abortions per 1,000 women. Guttmacher’s study showed a slight upward trend in abortion from 2017 to 2020 whereas CDC’s report showed a stable rate in abortions from 2017 to 2022 except for a slight uptick in 2019 and 2021.
Experts generally attribute the long-term decline in abortion rates to increased use of more effective methods of contraception. The slight increase in the years leading up to the Dobbs decision could be due to greater state-level coverage of Medicaid enrollees that made abortion access more affordable in some states as well as broader financial support from abortion funds to help individuals pay for the costs of abortion care.
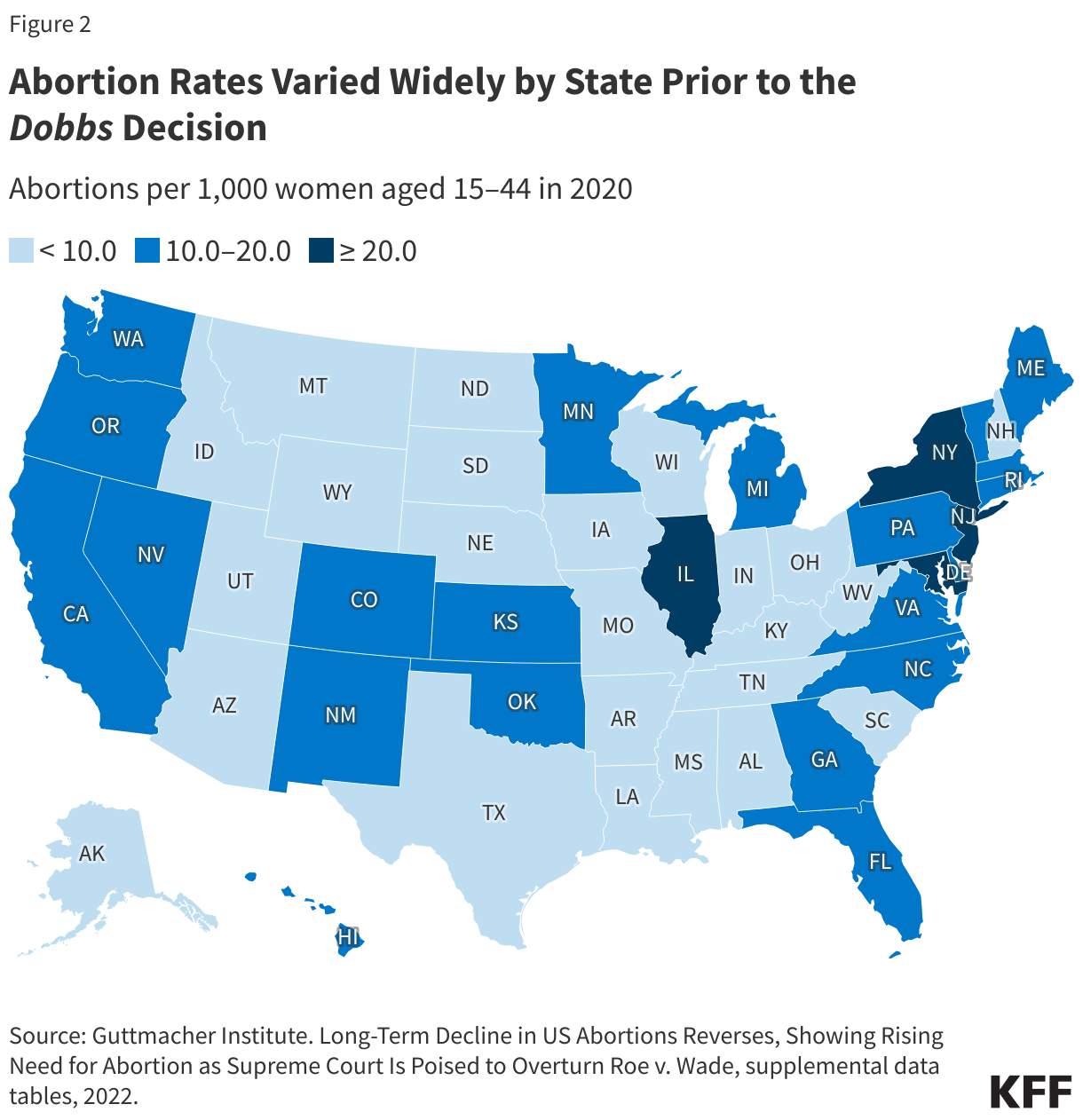
Even prior to the Dobbs ruling, abortion rates varied widely between states.
National averages can mask local and more granular differences. Some of the variation in abortion volume and rates has been due to the wide differences in state policies that have shaped the availability of abortion, with some states historically placing restrictions on abortion (such as targeted regulations of abortion providers, requirements for multiple visits, and mandatory waiting periods), that constrained abortion access and availability. In some states, there were only one or two abortion providers even before Dobbs.
What has happened to abortion volume since Dobbs?
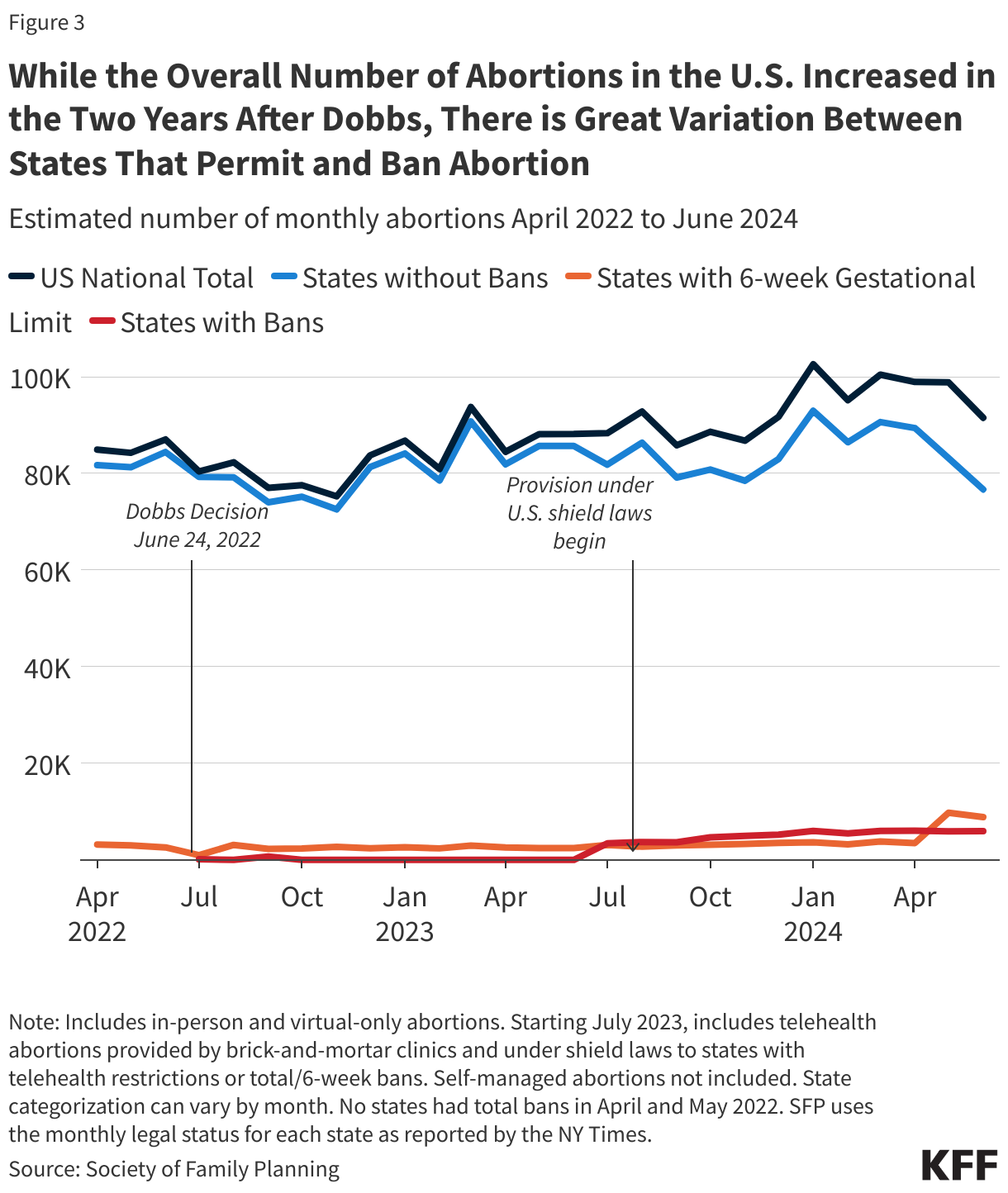
The SFP and Guttmacher Institute data both find that while the number of abortions in the U.S. dropped immediately following Dobbs, the total number of abortions nationally has increased two years following the ruling. However, the consistency observed at the national level obscures wide state-level variation and sharp declines in the number of abortions in states with bans and early gestational restrictions.
The latest SFP’s #WeCount data show that there were 591,770 abortions in the first half of 2025. In 2024, there were an estimated 1.14 million abortions, slightly up from 1.05 million in 2023. The monthly average number of abortions steadily increased from 88,180 abortions per month in 2023 to 95,250 abortions in 2024 to 98,630 in 2025 (January to June 2025)(Figure 3).
Why did the number of abortions increase after states instituted bans?
While it was not a total surprise that states without abortion bans had an increase in abortions following the Dobbs ruling, the reasons behind this increase are complex. The upward trend is likely due to a combination of increased interstate travel for abortion access by people coming from abortion ban states, the presence of state-level laws in states that protect providers who offer abortion services, lower costs associated with telemedicine medication abortions, and expanded virtual/telehealth capacity and the ability to mail medication abortions pills to patients among both bricks-and-mortar and telemedicine-only providers.
The Rise of Medication Abortion, Telehealth, and Virtual Clinics
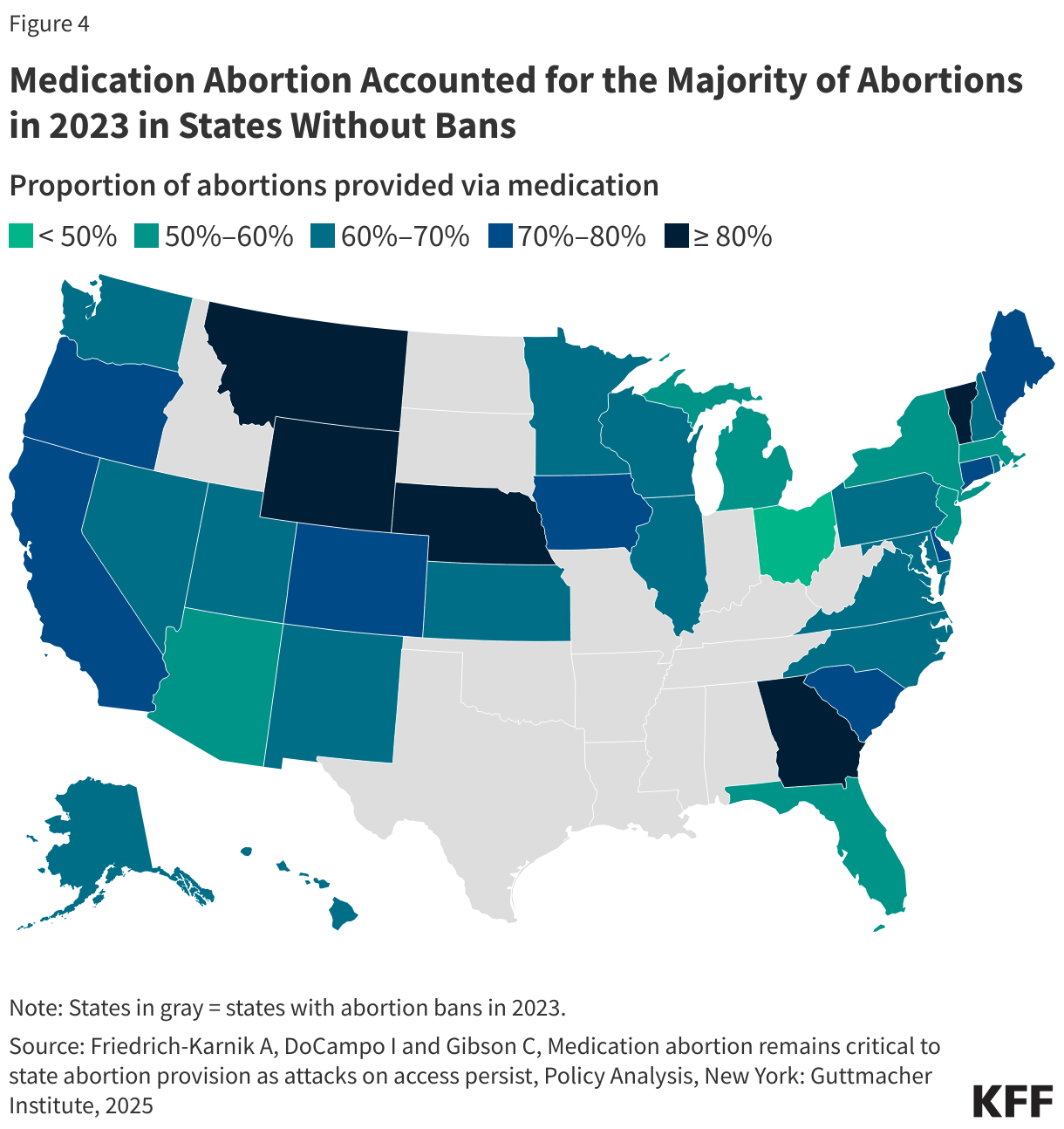
While procedural abortions are only performed in a clinical setting, medication abortion can be provided either in a clinical setting or remotely via telehealth. Medication accounts for nearly two thirds (63%) of abortions nationally. Approved by the U.S. Food and Drug Administration (FDA) in 2000, medication abortion has a solid safety and effectiveness record regardless of whether the pills are dispensed in person by a clinician (either medical doctor or advanced practice clinician) or via telehealth and mailed or dispensed through a retail pharmacy. When taken, medication abortion successfully terminates the pregnancy 91.9% to 99.7% of the time, with a 0.4% risk of major complications, and an associated mortality rate of less than 0.001 percent (0.0005%). Between 2% to 4% of medication abortions may need a procedural intervention with this regimen. The latest Guttmacher data show that in states without bans, medication accounted for the majority of abortions in 2023 (Figure 4). In five states (MT, WY, NE, GA, and VT), more than eight in ten abortions were medication abortions.
Access to medication abortion via telehealth had been historically limited by an FDA policy (Risk Evaluation Mitigation Strategy or REMS) that had permitted only physicians in a health care setting to dispense mifepristone in person. This resulted in a restriction on the ability to mail the pills or for retail pharmacies to dispense. In December 2021, the FDA revised this policy lifting the requirement that clinicians dispense the drug only in-person. This was done, in part, to alleviate the burden placed on the health care delivery system during the COVID-19 public health emergency. In January 2023, the FDA finalized a policy change that allows retail pharmacies to dispense medication abortion pills to patients with a prescription. These changes opened the door to greater use of telehealth for medication abortions.
The increase in telehealth abortions has also been driven in part by the rise in the number of virtual abortion clinics. The number of virtual clinics began to rise after the FDA revised its in-person dispensing requirement in 2021 and now accounts for a quarter (24%) of facilities that offer medication abortion services.
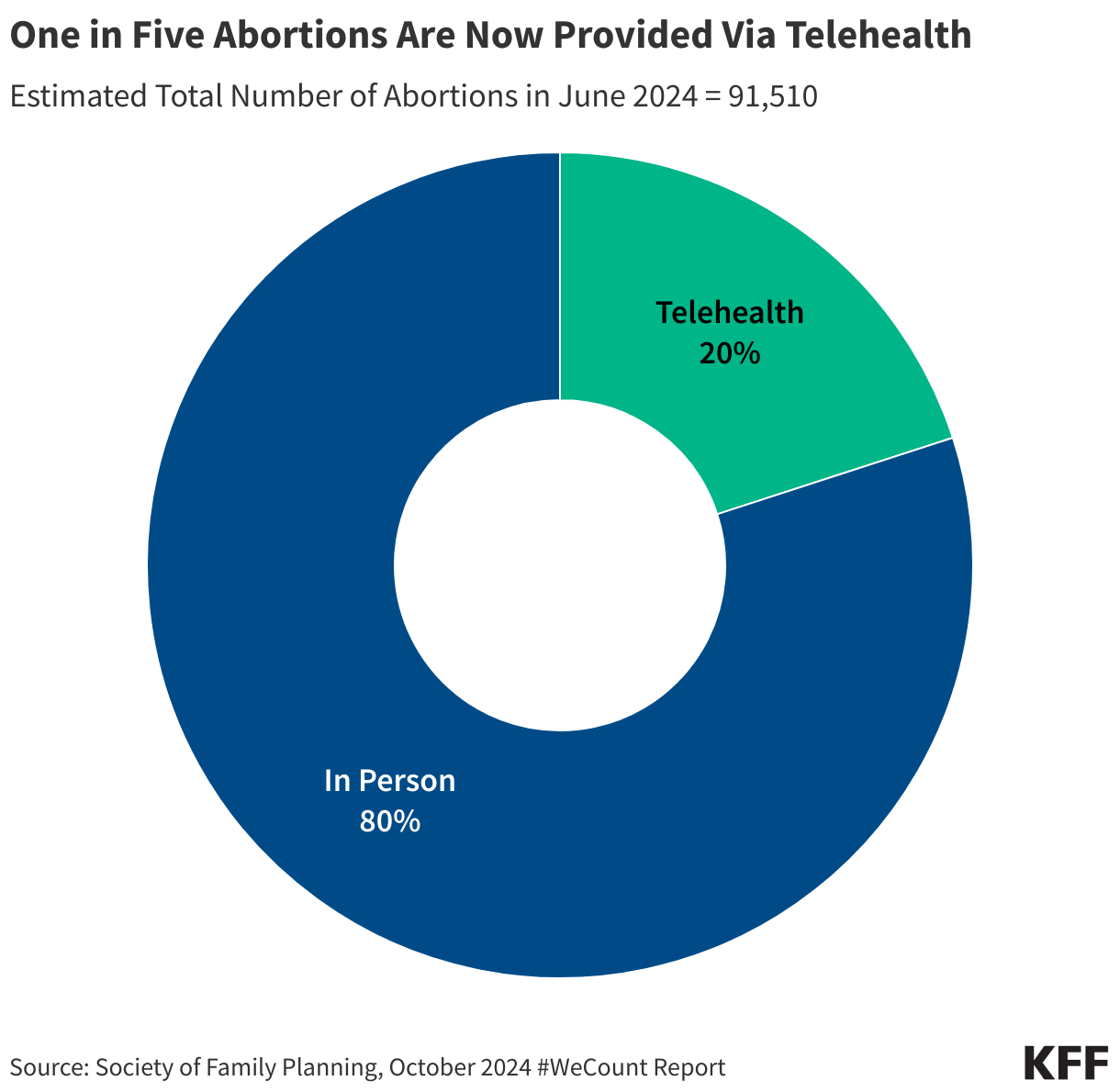
SFP’s #WeCount study breaks out monthly averages for telehealth abortions, and the most recent report shows that telehealth abortions accounted for 27% of all abortions in the second quarter of 2025 (Figure 5). The latest #WeCount reports distinguish between telehealth abortions provided by brick-and-mortar facilities from those provided under shield laws that give some legal protections to clinicians who provide abortion care via telehealth to people living in states with bans and restrictive policies. More than half of these telehealth abortions were performed under shield laws (56%), 6% of abortions were from online services offered by clinics that traditionally operate from physical locations (brick-and-mortar facilities), and four in ten (39%) were from virtual-only clinics. The provision of telehealth abortions varies widely across states, ranging from 8% of all abortions in some states and reaching 39% of all abortions in other states. Note: The counts for medication abortions, particularly those provided by mail, reflect the number of pills dispensed by providers, not necessarily complete abortions.
Costs for Telemedicine Abortions
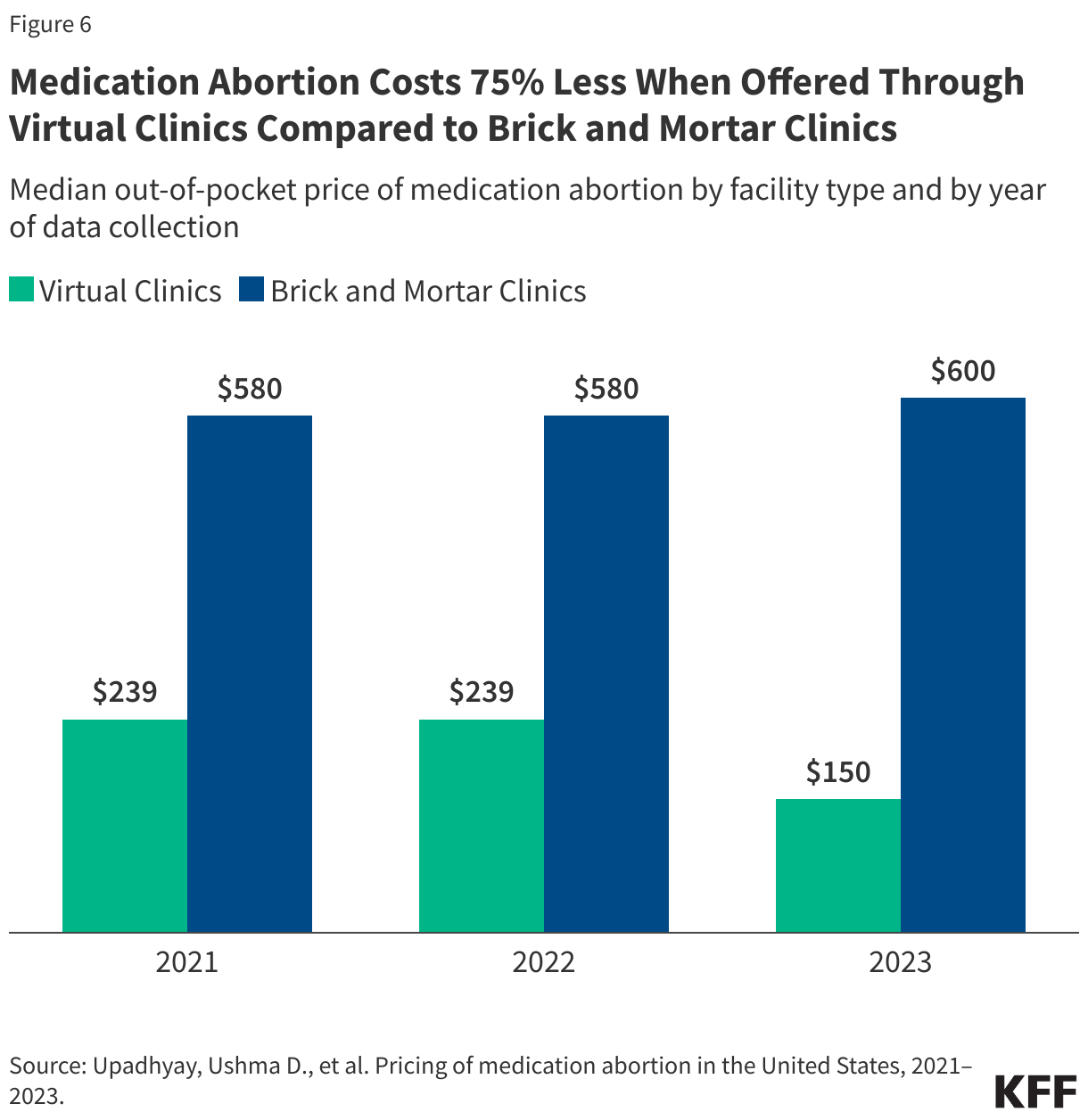
The median price of medication abortion offered through brick-and-mortar clinics increased from $580 in 2021 to $600 in 2023. In contrast, the median price of medication abortions via virtual clinics decreased from $239 in 2021 to $150 in 2023, which is 75% less than the cost of in-person care (Figure 6). Virtual clinics do not incur many of the costs of a physical clinic, such as building maintenance, meeting regulations for surgical centers, and security to handle protesters. The increased availability of telehealth and virtual clinics has lowered the costs of care and reduced financial barriers resulting from abortion services as well as travel and other related expenses.
Costs for some have also been offset by the availability of financial assistance and logistical support from national and local networks of abortion funds. Since Dobbs, these networks received a reported 39% more requests for abortion support and financially supported more than 100,000 individuals seeking abortion care. While donations to these networks increased immediately following Dobbs, the frequency of donations has slowed, and funds have begun to taper. Some organizations recently reported suspending operations altogether, signaling that abortion volume may consequently dwindle as demand outpaces donations.
State-Level Protections
Over the past several years, some of the states where abortion remains legal have passed laws to protect abortion access for their residents and expand access to people seeking abortions from other states. For example, residents in California are protected from civil liabilities for providing or receiving abortion services, and providers are protected from professional discipline. Policies that have been implemented include using state funds to cover abortions under Medicaid beyond federal limitations, raising Medicaid reimbursement rates for abortion services, requiring state-regulated private plans to cover abortion, and enacting shield laws to protect clinicians who provide abortions in their states either in person or via telemedicine.
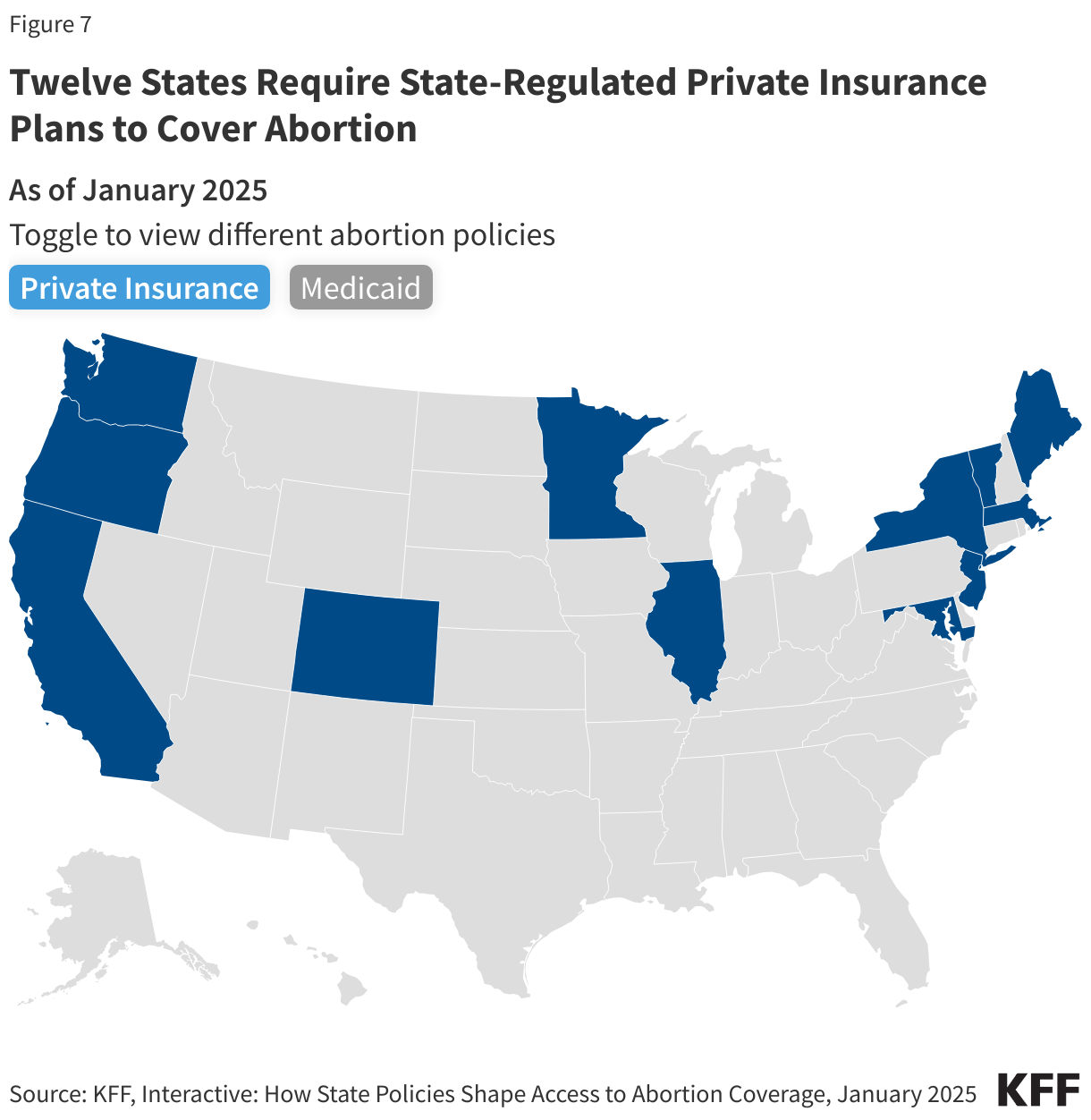
Today, 12 states require state-regulated private plans to cover abortion, some without any cost-sharing (Figure 7).
State actions to use their own revenues to pay for abortions have also expanded access to abortion services. States are not restricted by the federal Hyde Amendment (which bans the use of federal funds for abortion in Medicaid, Medicare and other public programs unless the pregnancy is a result of rape, incest, or if it endangers the woman’s life) and have the option to use state-only funds to cover abortions under other circumstances for women on Medicaid, which 20 states do currently.
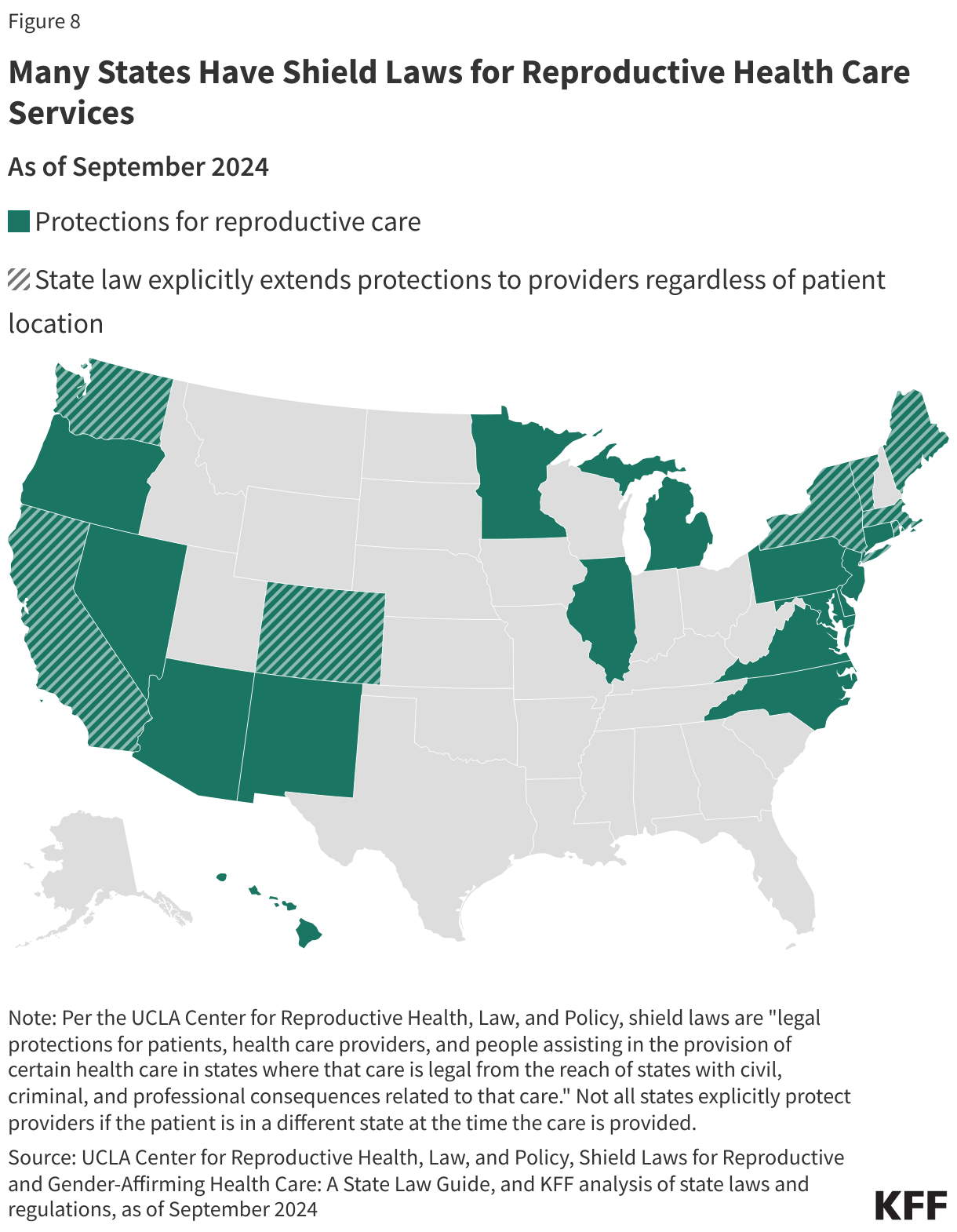
A growing number of states passed shield laws to reduce the legal risks for clinicians who provide abortion care to patients who live in states where abortion is banned or restricted. While the details of these laws vary state to state, some policies protect clinicians from professional discipline for offering health care that is criminalized in another state, and others protect clinicians who provide care to patients across state lines, such as by prescribing and mailing abortion pills via telehealth services to patients in their state of residence. Some states also passed broader shield laws to protect patients and people assisting with reproductive services from civil and criminal consequences. As of February 2025, 22 states and Washington D.C. have enacted shield laws, with 8 states extending explicit protections to clinicians regardless of patient location or state of residence (Figure 8).
Interstate Travel
The Guttmacher Institute Monthly Abortion Provision Study is the only data source so far to provide in-depth information on interstate travel pre- and post-Dobbs. Guttmacher estimates that prior to Dobbs, nearly one in ten people obtained an abortion by traveling across state lines in 2020. Even though abortion was legal, there were considerable restrictions in many states that made abortion access very limited, which led to the need for interstate travel for abortion care for some people. The latest data show that 155,000 patients traveled out of state for abortion care in 2024, a slight drop from 170,000 in 2023 but nearly double the number of travelers in 2020 (81,000). The states with the highest number of people traveling inbound for abortion care border at least one state where abortion is banned, including Illinois (36,920 patients), North Carolina (17,080 patients), Kansas (15,610 patients), and New Mexico (12,680 patients)(Figure 9).
The volume of interstate travel into Florida and North Carolina is especially notable as they were two of the last southern states in 2023 where abortion was legal beyond six weeks of gestation. However, the policies in these two states became more restrictive. North Carolina went from a 20-week ban to a 12-week ban in July 2023, and Florida’s 15-week ban changed to a 6-week ban in May 2024. The volume of interstate travel into Florida declined from 9,080 travelers in 2023 to 3,970 travelers in 2024 (data not shown). Conversely, the volume of interstate travel into North Carolina increased from 16,110 in 2023 to 17,080 in 2024 (data not shown). Virginia also had an increase in interstate travel for abortion, from 5,360 out-of-state travelers in 2023 to 9,410 travelers in 2024. This is largely due to Florida’s stricter gestational stage ban, which curtailed abortion access in the region and has resulted in patients in southern states having to travel elsewhere, such as to northern states, for abortion care.
While the data show that abortions slightly increased nearly three years after Dobbs, ongoing and impending legal challenges, state legislative efforts, and federal executive actions could further alter the reproductive care landscape and have impacts beyond abortion counts. A recent JAMA study, for instance, found that fertility rates have increased in states with complete or 6 week abortion bans, namely among populations with the greatest structural disadvantages and barriers to obtaining abortion care. A concurrent study showed infant mortality rates have also risen in these states, many of which are already experiencing some of the worst maternal, infant, and child health outcomes in the U.S. The findings from these studies underscore the widespread repercussions of policy efforts aimed at restricting abortion access.
Note: This brief was updated on January 7, 2026 to incorporate new data on abortion statistics.
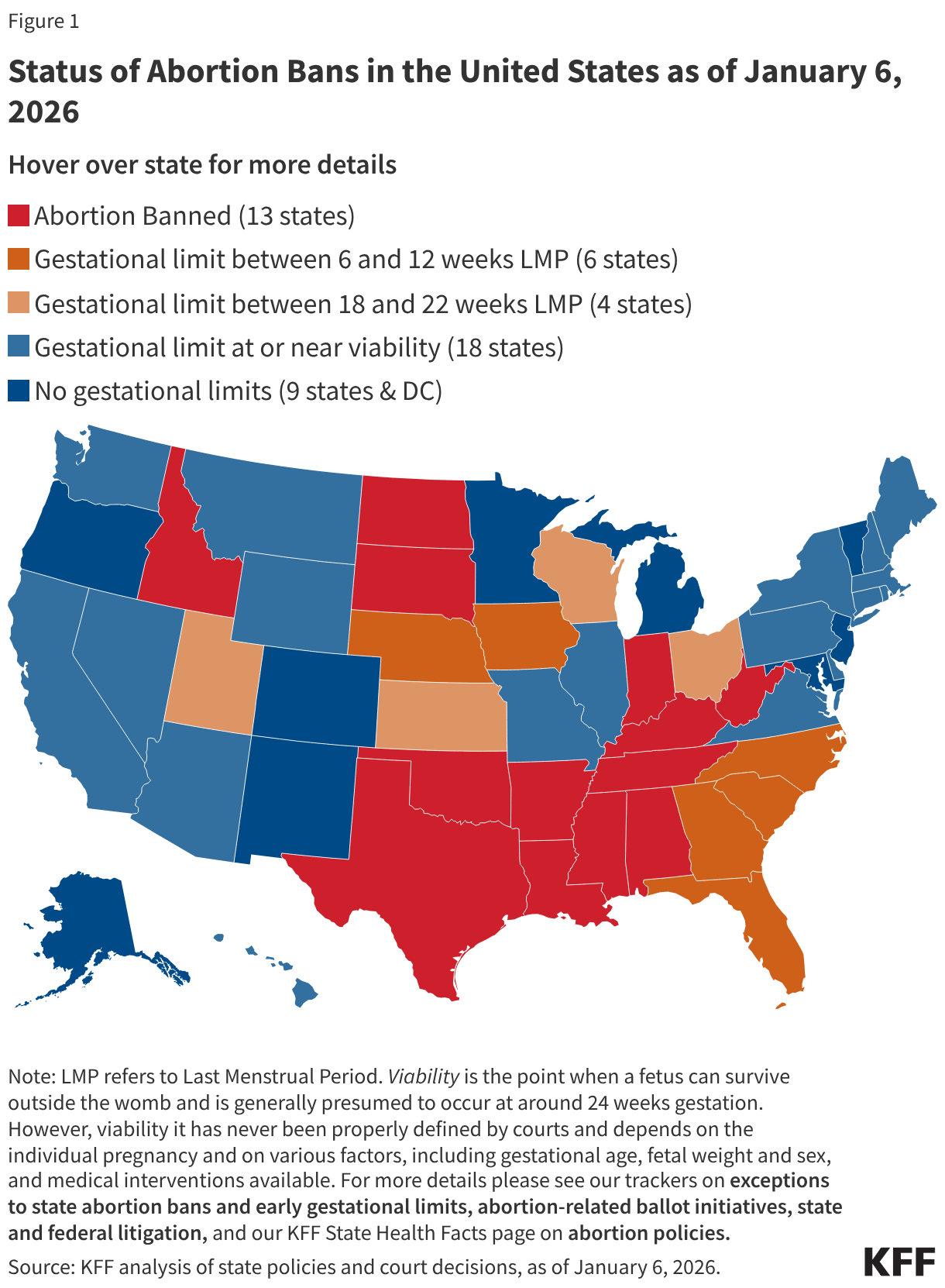
The Supreme Court’s 2022 ruling in Dobbs v. Jackson Women’s Health Organization overturned the constitutional right to abortion that had been in place for nearly 50 years under Roe v. Wade. Prior to the Dobbs ruling, abortions were permitted up to fetal viability in all states. That federal standard was eliminated under Dobbs, allowing states to ban or restrict abortion before viability. KFF is tracking and updating the status of abortion access and availability, with some states banning almost all abortions and some states protecting abortion access.
This issue brief answers some key questions about abortion in the United States and presents data collected before and since the Dobbs ruling.
Abortion is the medical termination of a pregnancy. It is a common medical service that many women obtain at some point in their life. There are different types of abortion methods, which the National Academy of Sciences, Engineering, and Medicine (NASEM) places in four categories:
Medication Abortion – Medication abortion, also known as medical abortion or abortion with pills, terminates a pregnancy by oral medications. There are two widely accepted protocols for medication abortion. In the U.S., the most common protocol involves the drugs mifepristone and misoprostol. Typically, an individual takes mifepristone first, followed by misoprostol 24-48 hours later. The U.S. Food and Drug Administration (FDA) has approved this abortion protocol up to the first 70 days (10 weeks) of pregnancy. Another medication abortion protocol uses misoprostol alone, which is also recommended for up to 70 days (10 weeks) of pregnancy, but it is not currently approved by the FDA and is more commonly used in other countries.
The Guttmacher Institute estimates that in 2023, medication was used for almost two thirds (63%) of all abortions. Many have confused emergency contraception (EC) pills with medication abortion pills, but EC does not terminate a pregnancy. EC is a contraceptive that prevents pregnancy by delaying or inhibiting ovulation and will not affect an established pregnancy.
Aspiration, a minimally invasive and commonly used gynecological procedure, is the most common form of procedural abortion. It can be used to conduct abortions up to 14-16 weeks of gestation. Aspiration is also commonly used in cases of early pregnancy loss (miscarriage).
Dilation and evacuation abortions (D&E) are usually performed after the 14th week of pregnancy. The cervix is dilated, and the pregnancy tissue is evacuated using forceps or suction.
Induction abortions are rare and conducted later in pregnancy. They involve the use of medications to induce labor and delivery of the fetus.
What does research show about the safety of abortions?
Decades of research have shown that abortion is a very safe medical service.
Despite its strong safety profile, abortion is the most highly regulated medical service in the country and is now banned in several states. Additionally, many states impose other limitations on abortion that are not medically indicated, including waiting periods and parental notification and consent requirements that typically delay receipt of services.
NASEM completed an exhaustive review on the safety and effectiveness of abortion care and concluded that complications from abortion are rare and occur far less frequently than during childbirth.
NASEM also concluded that safety is enhanced when the abortion is performed earlier in the pregnancy. State level restrictions such as waiting periods, ultrasound requirements, and gestational limits that impede access and delay abortion provision likely make abortions less safe.
When medication abortion pills are administered at or before 9 weeks gestation, the pregnancy is terminated successfully99.6% of the time, with a 0.4%risk of major complications, and an associated mortality rate of less than 0.001 percent.
Studies on procedural abortions, which include aspiration and D&E, have also found that they are very safe, with the rate of major complications less than 1% for aspiration abortions. Abortion medications and procedures are also often used for people experiencing miscarriages and stillbirths and can improve safety by preventing delays when a loss is inevitable.
Most OBGYN physicians say that the Dobbs decision has had a negative impact on maternal health and patient safety. In a national KFF survey of OBGYNs, more than six in ten say that racial and ethnic inequities in maternal health (70%), management of pregnancy-related medical emergencies (68%), and pregnancy-related mortality have all worsened (64%) since the Dobbs
(Back to top)
What is the status of abortion policy in the United States today?
Since the 2022 Dobbs ruling, abortion has been banned in 13 states, and another 6 states have implemented early gestational limits between 6 and 12 weeks. Most other states allow abortion to the point of fetal viability, which is generally considered around 24 weeks gestation.
All states that ban abortion have exceptions if an abortion is needed to prevent the death of the pregnant person. Additionally, some state bans make exceptions when the pregnancy is threatening the pregnant person’s health, when the pregnancy is the result of rape or incest, and when there is a lethal fetal anomaly. However, in practice, these exceptions have proven to be unworkable except in the most extreme circumstances. Furthermore, eight states that ban abortion do not make exceptions for cases of rape or incest and six do not have exceptions to protect the health of pregnant people.(Back to top)
The most recent data estimates that more than one million abortions (1,142,970) occurred in the U.S. in 2024 and there were more than half a million abortions (591,770) in the first six months of 2025.
Three different organizations currently track abortion volume at the state and the federal levels: the federal Centers for Disease Control and Prevention (CDC), the Guttmacher Institute, and the Society for Family Planning (SFP). The CDC has been collecting abortion data for decades, but several states do not provide data to the federal government (reporting to the CDC is voluntary) and there is a two-to-three-year time lag until the data become publicly available.
Since the Dobbs ruling, the Guttmacher Institute’s Monthly Abortion Provision Study and the SFP's #WeCount have been tracking state level changes in abortion volume based on data provided by abortion clinics and providers. Both studies provide national and state-level estimates on procedural and medication abortions but differ in some methodologic details. The Guttmacher study compares current abortion rates to 2020, while #WeCount compares rates to the months immediately before Dobbs in 2022. Neither source includes data on self-managed abortions, which are abortions that a pregnant person can do on their own by taking medication abortion pills without clinical supervision. For more details about data sources, see KFF’s issue brief on abortion trends.
For most of the decade prior to the Dobbs ruling, there was a steady decline in abortion rates nationally, but there was a slight increase in the years just before the ruling. Immediately following the Dobbs ruling, the number of abortions in the U.S. dropped as more states enforced bans and restrictions.
Paradoxically, the most recent data show that the abortion volume in the U.S. slightly increased overall in the three years following the Dobbs ruling.
The monthly average number of abortions steadily increased from 79,620 monthly abortions in 2022 (April to December 2022), to 88,180 abortions in 2023, to 95,250 abortions in 2024, and to 98,630 in 2025 (January to June 2025). This overall increase in the number of abortions nationally can be largely attributed to the growth of telehealth for medication abortion, increased availability of lower cost medication abortion pills through virtual clinics, and in particular shield law abortions, where clinicians in legal states are mailing pills to individuals residing in states with bans and restrictions. Additionally, in several states without bans, there has been increased interstate travel for abortion access, expanded capacity to see patients, increased measures to protect abortion rights and improve coverage of abortion care for residents and out-of-state patients, and the broader availability of low-cost abortion medication.
However, the small upswing nationally obscures the massive declines in abortion access to in-state providers in states with bans and restrictions as well as the hardships that many pregnant people experience in accessing abortion care. Additionally, there are month-to-month variations in all states, and changes in policy can cause larger shifts. For example, in May 2024 Florida implemented a ban on abortions after six weeks gestation (previously permitted up to 15 weeks), and subsequently there was a noticeable decline in abortions in the state and nationally.
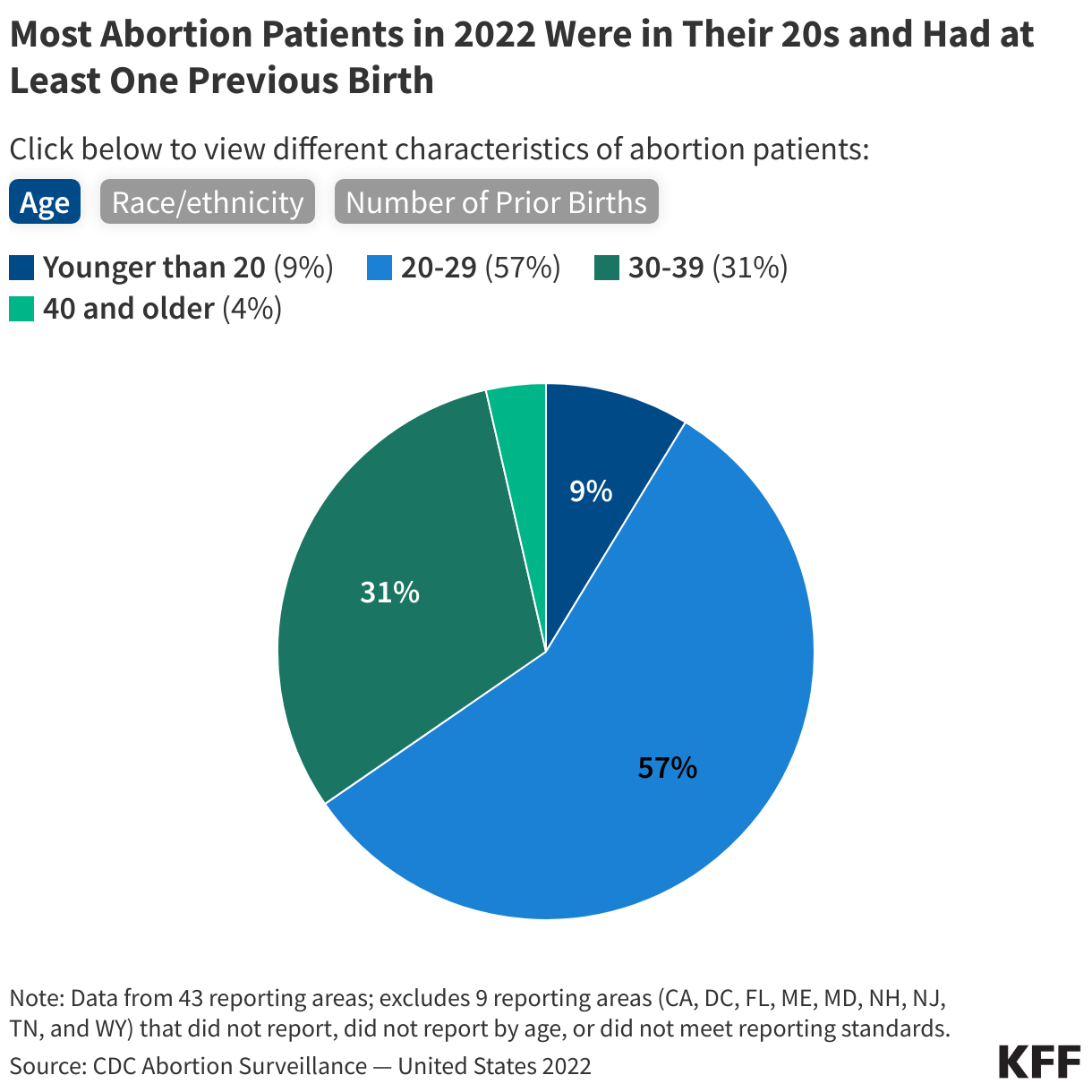
Most of the information about people who receive abortions comes from CDC data. In 2022, the most recent year CDC data are available, women across a range of age groups, socioeconomic status, and racial and ethnic backgrounds obtained abortions, but the majority were obtained by women who were in their twenties, low-income, and women of color.
Women in their twenties accounted for more than half (57%) of abortions. Nearly one-third (31%) were among women in their thirties and a small share were among women in their 40s (4%) and teens (9%).
Information on the race and ethnicity of people who obtain abortions is particularly limited, but based on available data, more than half of abortions were among women of color in 2022. Black women comprised 40% of abortion recipients, 32% were provided to White women, 21% to Hispanic women, and 7% were among women of other races/ethnicities. Additionally, White, Black, and American Indian and Alaska Native women are disproportionately represented among women ages 18-49 in states that have banned abortion compared to states that provide broader access to abortion. Many women who sought abortions have children. Approximately six in 10 (59%) abortion patients in 2022 had at least one previous birth.
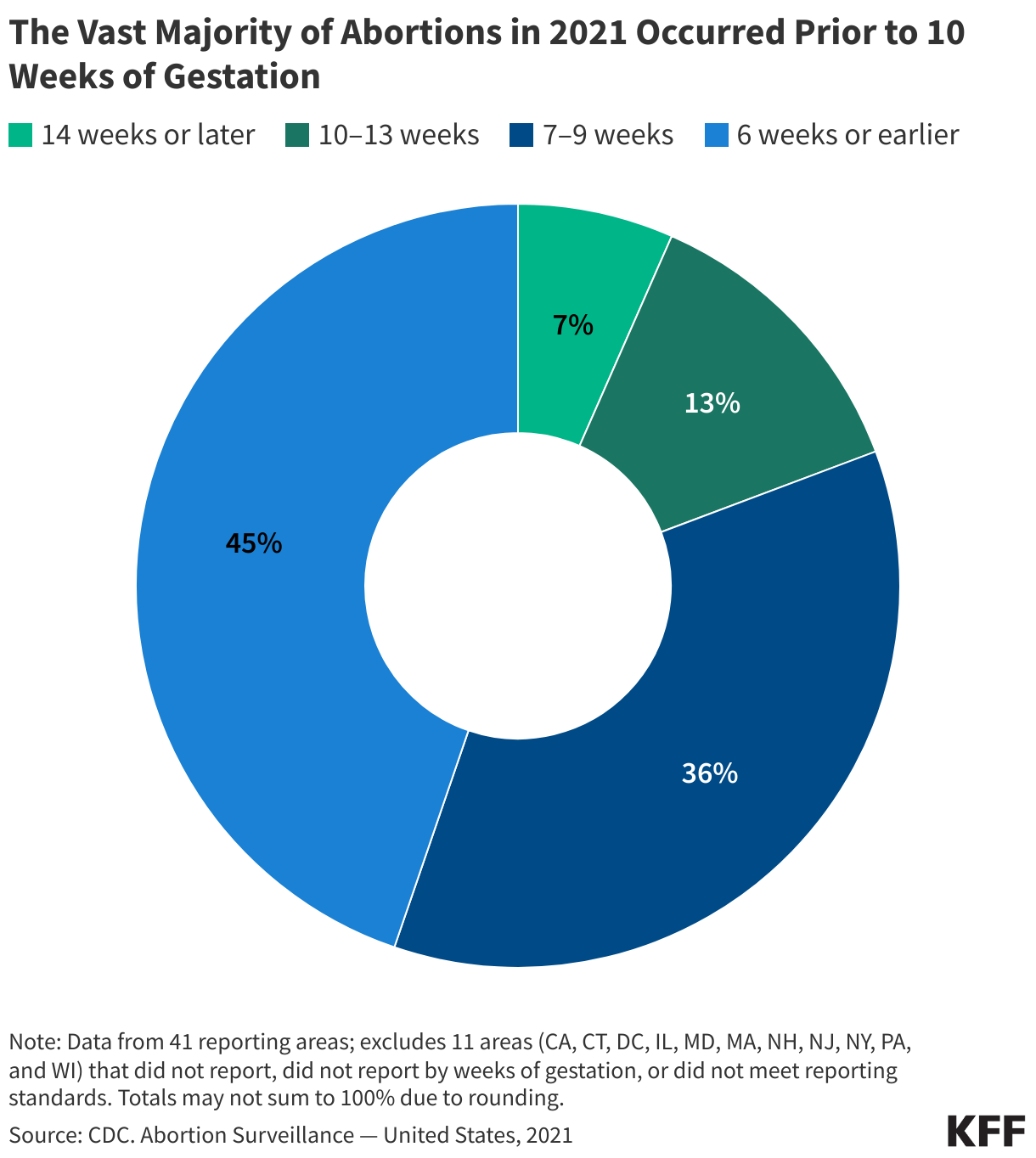
The vast majority (93%) of abortions occur during the first trimester of pregnancy according to data available from before the Dobbs decision.
Before the 2022 ruling in Dobbs, there was a federal constitutional right to abortion before the pregnancy is considered to be viable, that is, can survive outside of a pregnant person’s uterus. Viability is generally considered around 24 weeks of pregnancy. Most abortions, though, occur well before the point of fetal viability. When people have abortions later in pregnancy, it is often because the fetus is not viable and the pregnancy may endanger the pregnant person’s life.
Data from 2022 found that four in ten (40%) abortions occurred by six weeks of gestation, another four in ten (39%) occurred between seven and nine weeks, and 14% at 10-13 weeks. Just 7% of abortions occurred after the first trimester.
Abortions can be provided in a variety of settings. Recent data on site of abortion care are limited, but historically the majority of abortions have been provided at brick and mortar clinics that specialize in provision of reproductive health care. Some private office-based physicians also offer abortion services and in more recent years, there has been an emergence of virtual only clinics that offer medication abortions.
Brick-and-mortar clinics vary, but they can offer medication abortion, procedural abortions, and services for abortions later in pregnancy. Many clinics in states where abortion is restricted or banned stopped offering abortion services shortly after the Dobbs ruling and the overall number of brick-and-mortar independent clinics in the US has decreased over the years, with over 75 independent abortion clinics shutting down between 2022 and 2024. Contrary to expectations though, the number of abortions from these clinics increased overall since the Dobbs ruling. The distribution of facilities that offer abortion care varies widely by state and geographic region, and the increase is largely driven by the expansion of virtual abortion clinics. While virtual clinics can remove geographic barriers for those seeking abortion care, their services are limited to medication abortion which is only available to those seeking abortions early in pregnancy. Even prior to the ruling in Dobbs, access to abortion services was very uneven across the country. The proliferation of restrictions in many states, particularly in the South, greatly constrained the availability of services in some areas. In the wake of overturning Roe v. Wade, these geographic disparities have only widened.
Telehealth
Telehealth has grown as a delivery mechanism for abortion services. While procedural abortions must be provided in person in a clinical setting, medication abortion can be provided in a clinical setting or via telehealth without an in person visit. An estimated one in four abortions were provided via telehealth in the last quarter of 2024. Access to medication abortion via telehealth was limited for many years by an FDA policy that permitted only certified clinicians to dispense mifepristone within a health care setting. In December 2021, however, the FDA permanently revised this policy and no longer requires clinicians to dispense the drug in person. Additionally, in January 2023, the FDA finalized a policy change that allows retail pharmacies to dispense medication abortion pills to patients with a prescription. These policy changes opened the door to using telehealth for medication abortion.
Telehealth can be administered by providers from traditional brick-and-mortar clinics or by virtual-only clinics. Virtual clinics began to proliferate after the FDA revised its in-person dispensing requirement in 2021, rising from no virtual clinics in 2020 to 226 clinics in 2023 (representing 24% of facilities that offer medication abortion).
In a telehealth abortion, the patient typically completes an online questionnaire to assess (1) confirmation of pregnancy, (2) gestational age and (3) blood type. If determined eligible by a remote clinician, the patient is mailed the medications. This model does not require an ultrasound for pregnancy dating if the patient has regular periods and is sure of the date of their last menstrual period (in line with ACOG’s guidelines for pregnancy dating). If the patient has irregular periods or is unsure how long they have been pregnant, they may need to obtain an ultrasound to confirm the weeks of gestation and rule out an ectopic pregnancy and send in the images for review before receiving medications. The follow-up visit with a clinician can also happen via a telehealth visit.
Research has found that the provision of medication abortion via telehealth is as safe and effective as the provision of the pills at an in person visit. Yet, in some states that have not banned abortion, telehealth may not be available because of state-level restrictions enacted prior to the Dobbs ruling that require patients to take the pills at a physical clinic, require ultrasounds for all abortions, or directly ban telehealth for abortion care. Of the 36 states that have not banned abortion, 12 had at least one of these restrictions as of March 2024.
Medication abortion has emerged as a major legal and legislative front in the battle over abortion access across the nation. Multiple cases have been filed in federal and state courts regarding aspects of the FDA’s regulation of medication abortion as well as the mailing of medications.
Some states have passed shield laws, designed to reduce the legal risks for clinicians who provide abortion care to patients who live in states where abortion is banned or restricted. The shield laws bar the clinicians’ resident state from extraditing them if a restrictive state attempts to prosecute the clinician for performing an abortion that is otherwise legal in their home state. As of September 2024, 8 states have shield laws in place that explicitly protect providers regardless of patient location.
Data from SFP’s latest #WeCount report show that one in four (27%) abortions were provided via telehealth in early 2025. These telehealth abortions include those provided by brick-and-mortar clinics, virtual clinicians, and clinicians in states with shield laws who prescribe medication abortion to patients in states with bans or telehealth restrictions. Note: The counts for medication abortions, particularly those provided by mail, reflect the number of pills dispensed by providers, not necessarily complete abortions.
Self Managed Abortions
Self-managed abortions typically involve obtaining medication abortion pills from an online pharmacy that will send the pills by mail or by purchasing the pills from a pharmacy in another country, usually without the involvement of a physician or advanced practice clinician. While this can involve asynchronous contact with non-US-based clinicians, it does not typically involve a direct consultation with a clinician either in person or via telehealth.
It is difficult to track the volume of self-managed abortions since they are outside of the formal health care system, and it is unknown if all people who receive medication pills take them. One study estimated that at least 26,000 additional self-managed medication abortions took place in the six months following the Dobbs ruling. More than half of self-managed medication abortions pills were distributed through volunteers in community networks, while others were provided by telehealth organizations outside the formal U.S. health care system and online vendors.
Interstate Travel
The Guttmacher Institute Monthly Abortion Provision Study is the only data source so far to provide in-depth information on interstate travel pre- and post-Dobbs. Guttmacher estimates that prior to Dobbs, nearly one in ten people obtained an abortion by traveling across state lines in 2020. Even before Roe v Wade was overturned, abortion was highly restricted in many states. The latest data show that 155,000 patients traveled out of state for abortion care in 2024, a slight drop from 170,000 in 2023 but nearly double the number of travelers in 2020 (81,000). This has been offset by an increase in patients who are getting abortion pills via telehealth.
The states with the highest number of people traveling inbound for abortion care border at least one state where abortion is banned, including Illinois (36,920 patients), North Carolina (17,080 patients), Kansas (15,610 patients), and New Mexico (12,680 patients).
The costs of abortion services vary widely depending on the method, facility, and gestational age; the costs can be as low as $25 through virtual clinics but typically exceed $1,000 for abortions later in pregnancy.
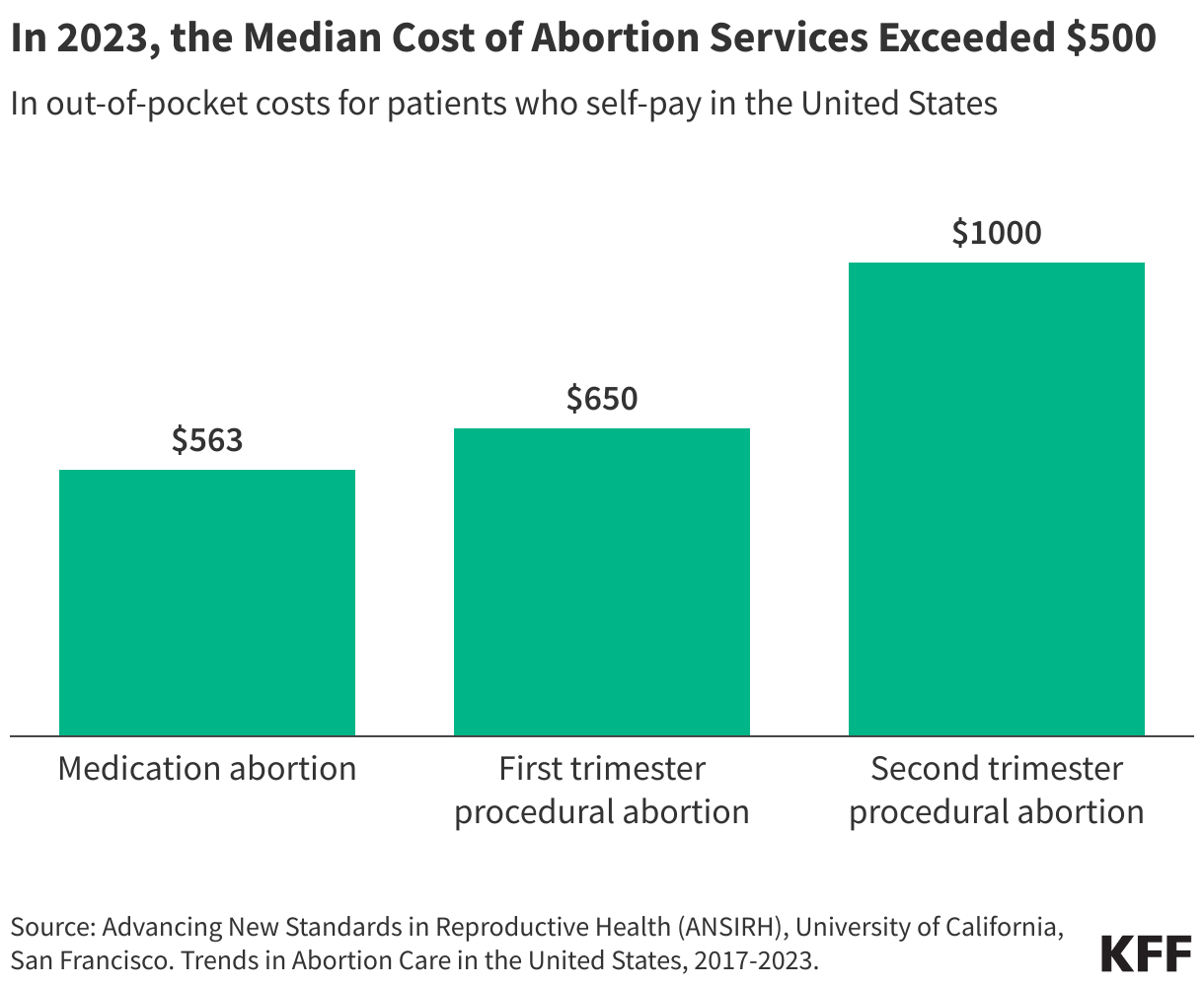
Obtaining an abortion can be costly. On average, the costs are higher for abortions in the second trimester than in the first trimester. The state bans and restrictions enacted since Dobbs can also result in additional nonmedical expenses for transportation, childcare, lodging, and lost wages. Many people pay for abortion services out of pocket, but some people can obtain assistance from local abortion funds, or coverage through their insurance plan or with state funds in some states.
Among all abortion-providing facilities in 2023, the median costs for people paying out of pocket in the first trimester were $563 for a medication abortion and $650 for a procedural abortion. For people with low incomes, who are more likely to seek abortion care, these costs are often unaffordable. The costs of abortion are higher in the second trimester compared to the first, with median self-pay reaching $1000. In the second trimester, more intensive procedures may be needed and local options are more limited in many communities that have fewer facilities.
Abortion funds are independent organizations that help pay for some of the costs of abortion services, typically medical care, travel, and accommodations if needed. Most abortion funds are regional and have connections to clinics in their area, but they do not reach all people seeking services. Since Dobbs, these networks received a reported 39% more requests for support, and while donations to these networks rose immediately following Dobbs, the frequency of donations slowed, and the resources available to funds have begun to taper.
The costs for abortion services through virtual clinics, such as AidAcess and Abuzz, as well as self-managed sites, are typically lower than in person services. In 2023, the median cost of medication abortion from virtual clinics was $150. Costs at online pharmacies listed on Plan C range from a low of $25 for abortion pills by mail without clinician consultation, to upwards of $150 for abortion by mail with a clinical consultation.
Does private insurance or Medicaid cover abortions?
Insurance coverage for abortion services is heavily restricted in certain private insurance plans and public programs like Medicaid and Medicare.
Among women of reproductive age, approximately one in three are covered by private insurance, one in five are covered by Medicaid, and one in ten are uninsured. States regulate fully-insured private plans in their state, whereas the federal government regulates self-funded plans. States can choose whether abortion coverage is included or excluded in private plans that are not self-funded. Increasingly, states that support abortion rights have enacted laws that mandate coverage in both Medicaid and state-regulated plans.
Prior to the Dobbs ruling, several states had enacted private plan restrictions and banned abortion coverage from ACA Marketplace plans. Currently, there are 10 states that have policies restricting abortion coverage in private plans and 25 that ban coverage in any Marketplace plans. Since the Dobbs ruling, some of these states have also banned the provision of abortion services altogether. Conversely, 12 states require private plans to cover abortion, nine of which require no cost-sharing for abortion.
For decades, the Hyde Amendment has banned the use of federal funds for abortion in Medicaid, Medicare and other public programs unless the pregnancy is a result of rape, incest, or if it endangers the pregnant persons’ life. States have the option to use state-only funds to cover abortions under other circumstances for those on Medicaid, which 20 states do currently.
Data from 2021, prior to Dobbs, estimated that a quarter (26%) of abortion patients used Medicaid to pay for abortion services, 11% used private insurance, and 60% paid out of pocket. People in states with more restrictive abortion policies were more likely to pay out of pocket compared to people living in less restrictive states.
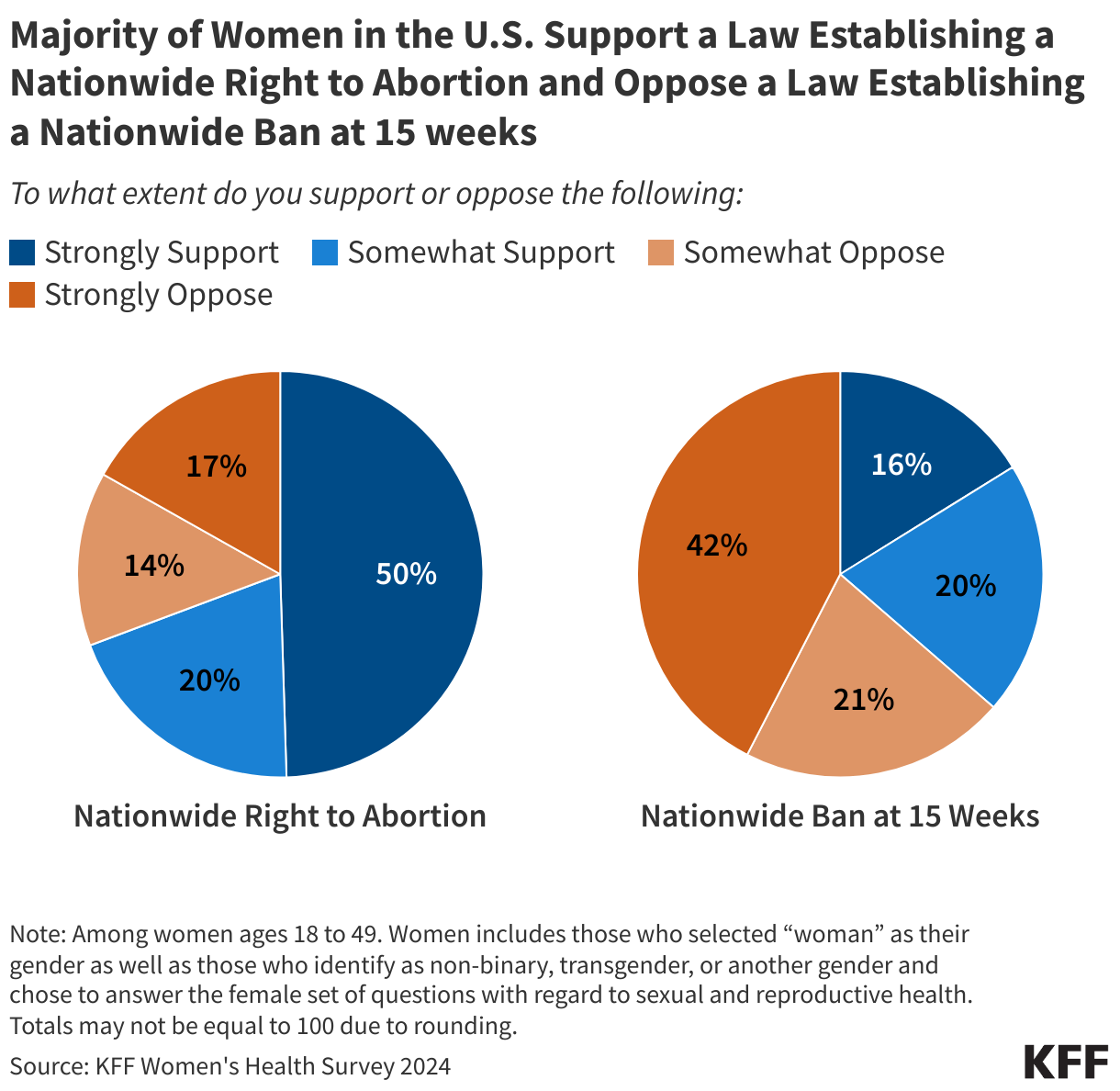
KFF’s national polls have consistently found that a majority of the public did not want to see Roev. Wade overturned and that most people feel that abortion is a personal medical decision. Similarly, findings from the 2024 KFF Women’s Health Survey show 70% of women of reproductive age—the age group that is most directly impacted by state abortion policies—support a nationwide right to abortion.
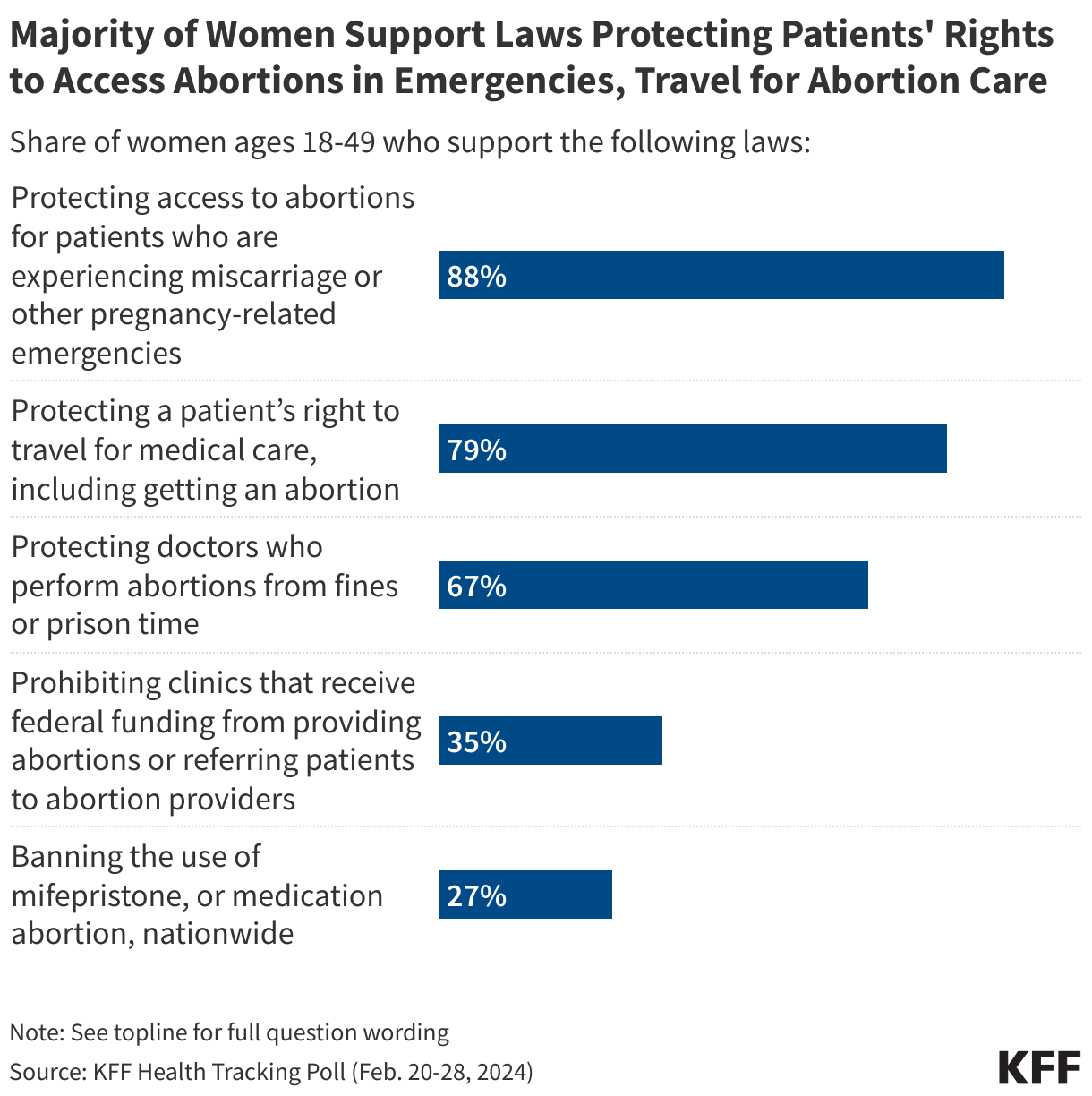
Furthermore, much of the public supports access to abortions for patients who are experiencing pregnancy-related emergencies (88%), a patient’s right to travel for abortion care (79%), and protecting doctors who perform abortions from legal penalties (67%).
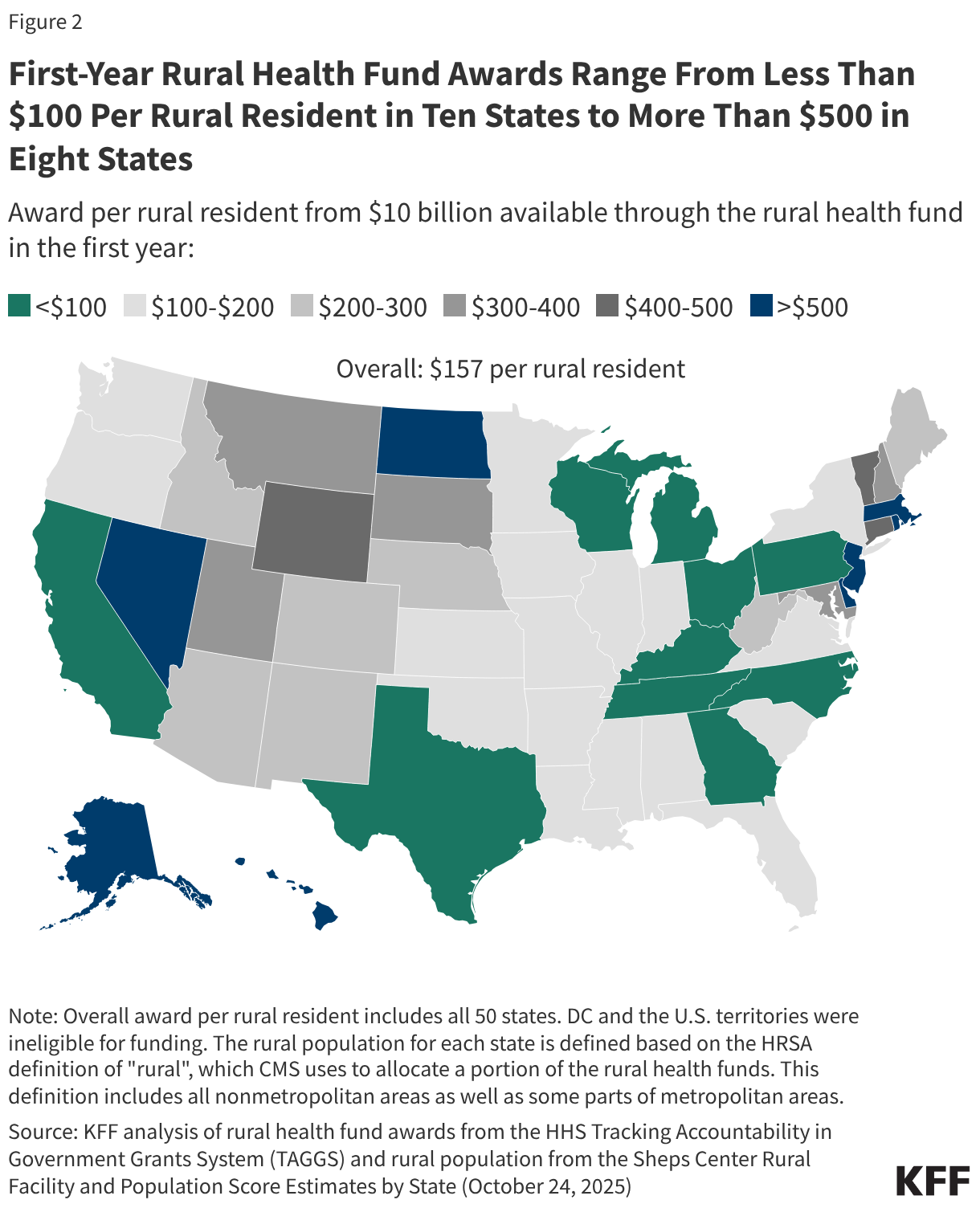
First-Year Rural Health Fund Awards Range From Less Than $100 Per Rural Resident in Ten States to More Than $500 in Eight
On December 29, 2025, the Centers for Medicare & Medicaid Services (CMS) announced first-year state awards from the $50 billion Rural Health Transformation Program (the “rural health fund”), which is being administered by a new Office of Rural Health Transformation. The rural health fund was created as part of the July 2025 budget reconciliation law, sometimes called the One Big Beautiful Bill, to help offset the impact on rural areas of the law—which includes an estimated $911 billion in federal Medicaid spending reductions over ten years, including an estimated $137 billion in rural areas. All 50 states applied for the rural health fund, and each state received an award. CMS will distribute $10 billion each year from fiscal years 2026 through 2030, beginning this year.
State awards for 2026, the first of five years, average $200 million, ranging from $147 million in New Jersey to $281 million in Texas (Figure 1). Differences in total awards across states in the first year (and most likely in future years) are modest relative to large differences in rural populations and rural health needs more generally. For example, Texas has about thirty times as many rural residents as New Jersey (4.3 million versus about 140,000) but is only receiving about twice as much funding in the first year ($281 million versus $147 million). Differences in total awards across states are relatively modest primarily because half of the rural health fund (50%) is being distributed equally across approved states, regardless of need, as required by law. Because all states have been approved for funding, each is slated to receive $100 million from this half of the fund in 2026 and in each year from 2027 through 2030.
Texas, Alaska and California are receiving the largest total awards in the first year. While Texas and California have the largest and fourth-largest rural populations in the country, respectively, Alaska has the fifth smallest rural population. Alaska likely received a relatively large award at least in part because a portion of the fund was distributed to the five largest states based on land area. New Jersey, Connecticut, and Rhode Island are receiving the smallest awards in the first year. These are all states with relatively small rural populations.
Figure 1
First-year awards per rural resident vary widely across states, ranging from less than $100 in ten states to more than $500 in eight states according to KFF analysis (see Figure 2). State awards are partially, but not closely, tied to rural population, meaning that first-year awards per rural resident are generally relatively small among states with the largest rural populations. For example, Texas has the largest rural population in the country—and the largest total award in the first year—but will receive the smallest payment per rural resident ($66 in 2026). In contrast, states like Rhode Island, New Jersey, and Alaska, with far fewer rural residents, will receive substantially higher amounts per rural resident ($6,305, $1,069, and $990 respectively, with Rhode Island being an extreme outlier). Only a quarter of the $50 billion fund is being distributed exclusively based on measures of state need, with just 5% of the fund that is based on rural population. Other measures of need, according to CMS, include the number of rural facilities, land area, the share of hospitals receiving Medicaid disproportionate share hospital (DSH) payments, and other factors.
While lawmakers created the fund in part to help offset the impact on rural hospitals of cuts under the reconciliation law, CMS has made clear that funding is intended to benefit rural communities more broadly by transforming health care systems. Examples of state initiatives based on the subset of stateapplications available to the public and abstracts posted on CMS’s website include initiatives related to Make America Healthy Again (MAHA) (such as improving access to healthy foods and preventing and managing chronic conditions), expanding telehealth services and remote patient monitoring, rural workforce development programs, and supporting regional collaboration among providers.
CMS stipulates that payments to hospitals and others for patient care cannot exceed 15% of total funds, though providers could benefit in other ways, such as through investments in existing buildings and infrastructure (restricted to 20% of total funds). It is unclear how much of the money will benefit rural hospitals either directly or indirectly and the extent to which this will offset hospitals’ losses under the reconciliation bill. Moreover, it is not yet clear how much information will be available to the public to track the flow of dollars from states to rural providers and other entities and to evaluate the effectiveness of state initiatives.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Many older adults and people with disabilities require assistance with self-care such as bathing, dressing, and eating. Help with such services is known as “long-term care” and may be provided in institutional settings such as nursing facilities or in people’s homes and the community, including assisted living facilities. Four-in-ten adults incorrectly believe that Medicare is the primary source of coverage for low-income people who need nursing or home care, but Medicaid is the primary payer—covering nearly two-thirds of all home care spending in the United States in 2023.
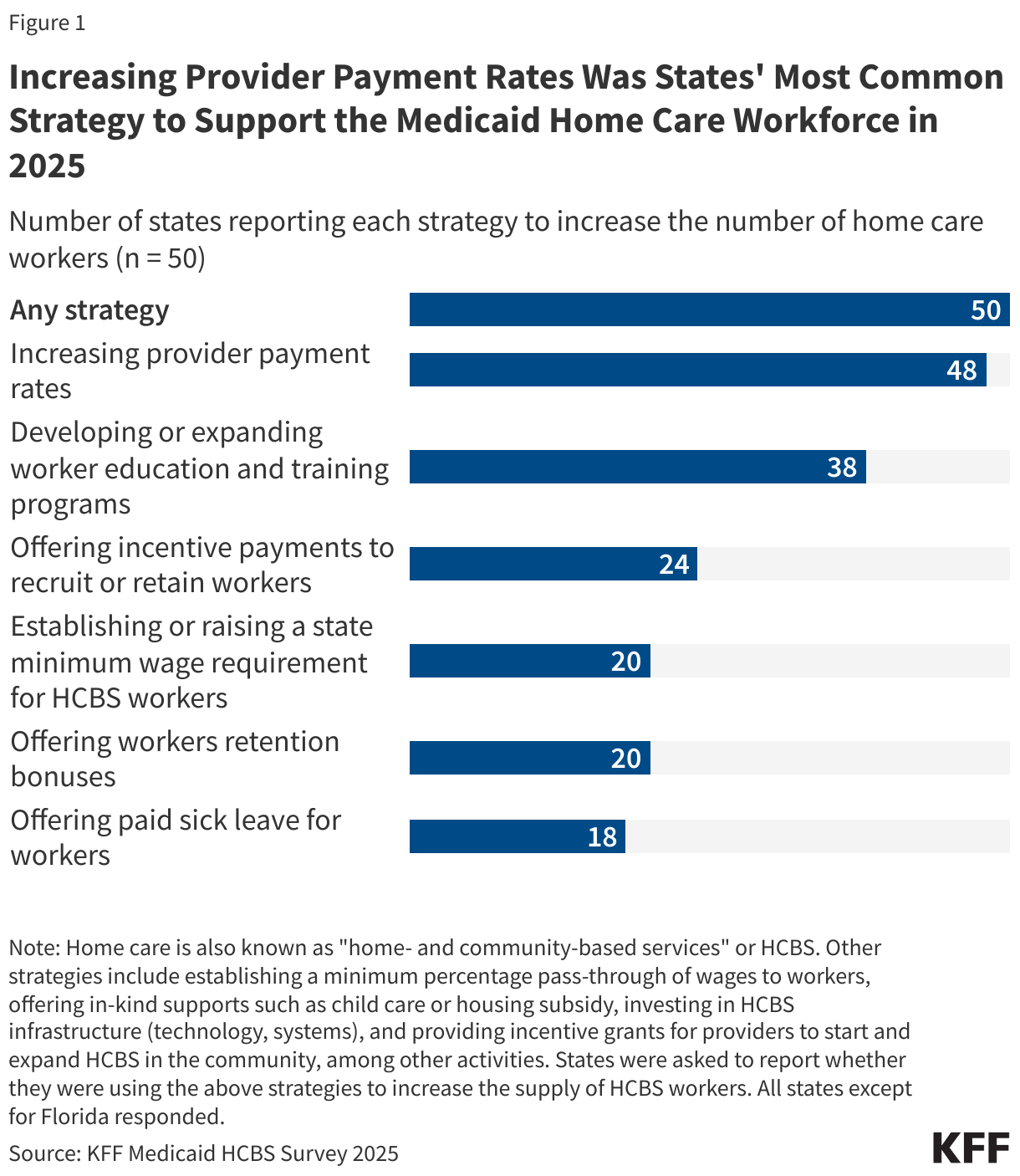
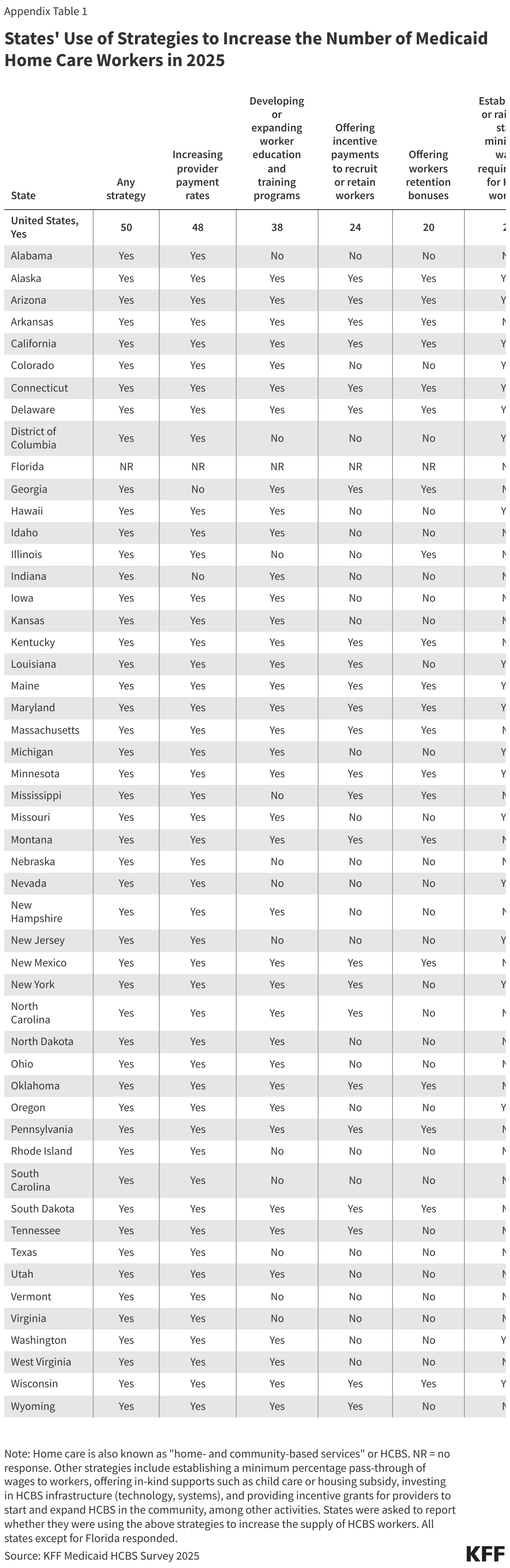
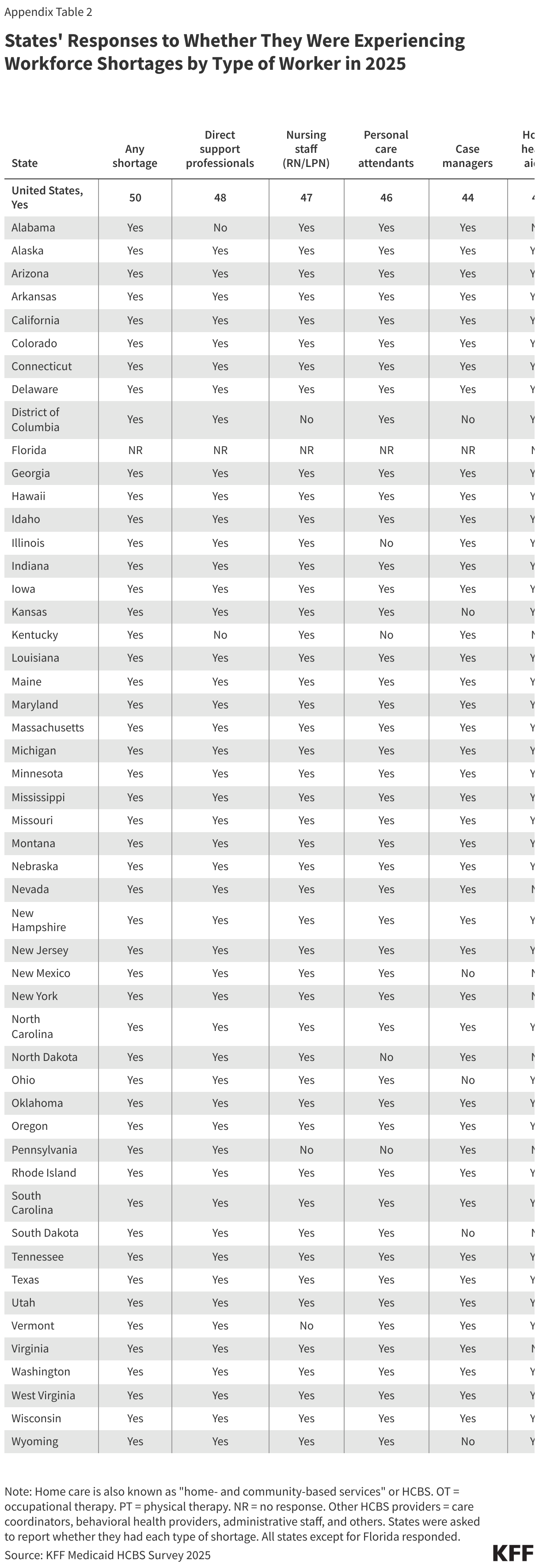
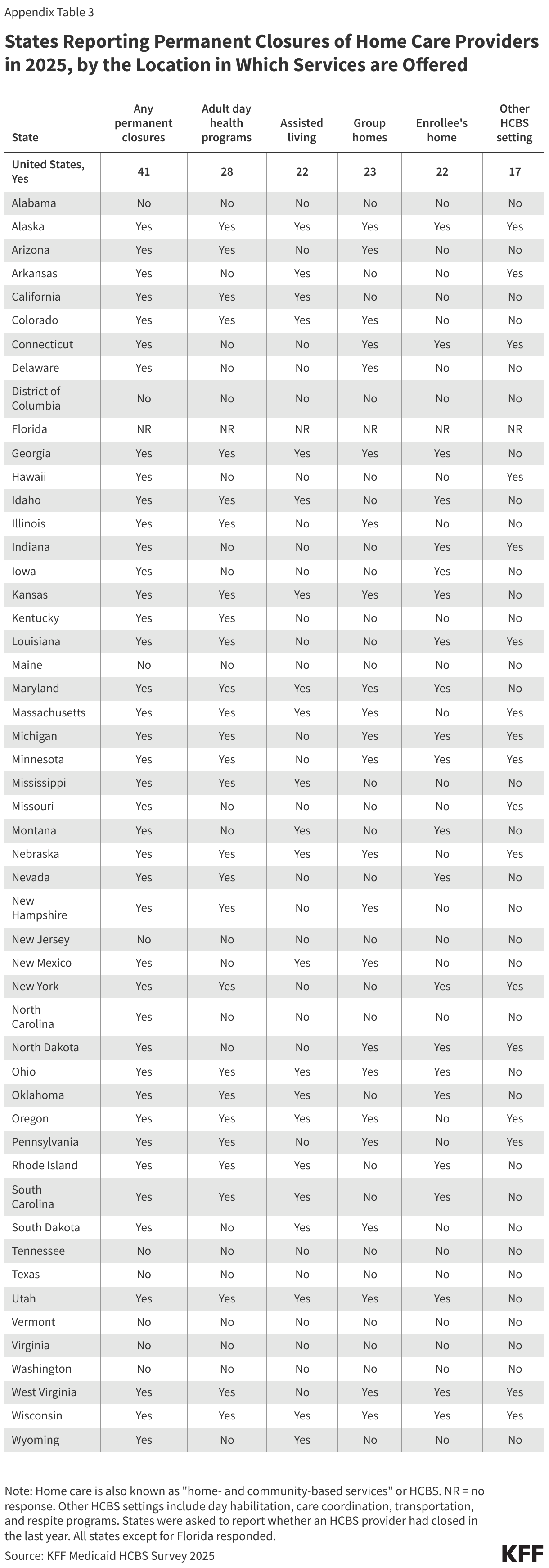
The 2025 reconciliation law is estimated to reduce federal Medicaid spending by $911 billion (roughly 14%) over a decade and may have broad implications for home care, including for the workforce, support for family caregivers, and states’ coverage of services. Over half of Medicaid spending finances care for people ages 65 and older and those with disabilities, the enrollees most likely to use home care and related services, and reductions of this magnitude will leave states with difficult choices to raise new revenues or reduce Medicaid spending. The reconciliation law also established a new type of 1915(c) home care waiver for people who do not need an institutional level of care. Take-up of the new waivers is expected to be low given the cuts to federal Medicaid spending and requirements for states to demonstrate that new waivers will not increase the average amount of time that people wait for existing waiver services. This issue brief provides an overview of what Medicaid home care (also known as “home- and community-based services” or HCBS) is, who is covered, and what services were available in 2025. Over 5 million people receive Medicaid covered home care services annually.
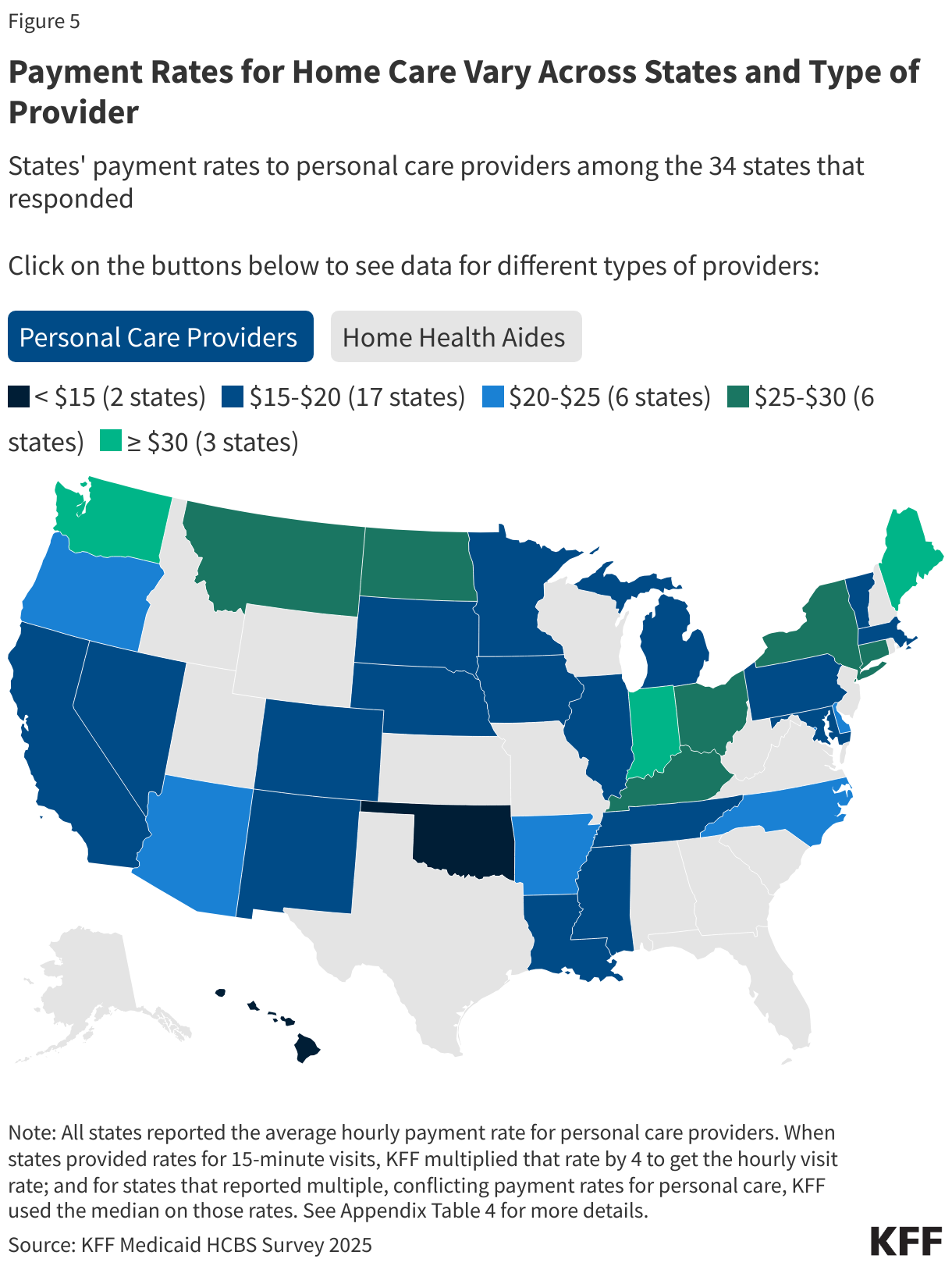
This brief is one of several describing data from the 23rdKFF survey of officials administering Medicaid home care programs in all 50 states and the District of Columbia (hereafter referred to as a state), which states completed between April and July 2025. Other issue briefs from the survey describe the number of people on waiting lists for home care, how states manage home care spending, how home care programs support family caregivers, and payment rates for home care providers. The survey was sent to each state official responsible for overseeing home care benefits (including home health, personal care, and waiver services for specific populations such as people with physical disabilities). All states except Florida responded to the 2025 survey, but response rates for certain questions were lower. Where possible, KFF supplemented survey data with previously reported or publicly available data to provide information for the states that did not respond. Survey findings are reported by state and waiver target population, although states often offer multiple waivers for a given target population. States generally completed the survey prior to enactment of the reconciliation law. Key takeaways include:
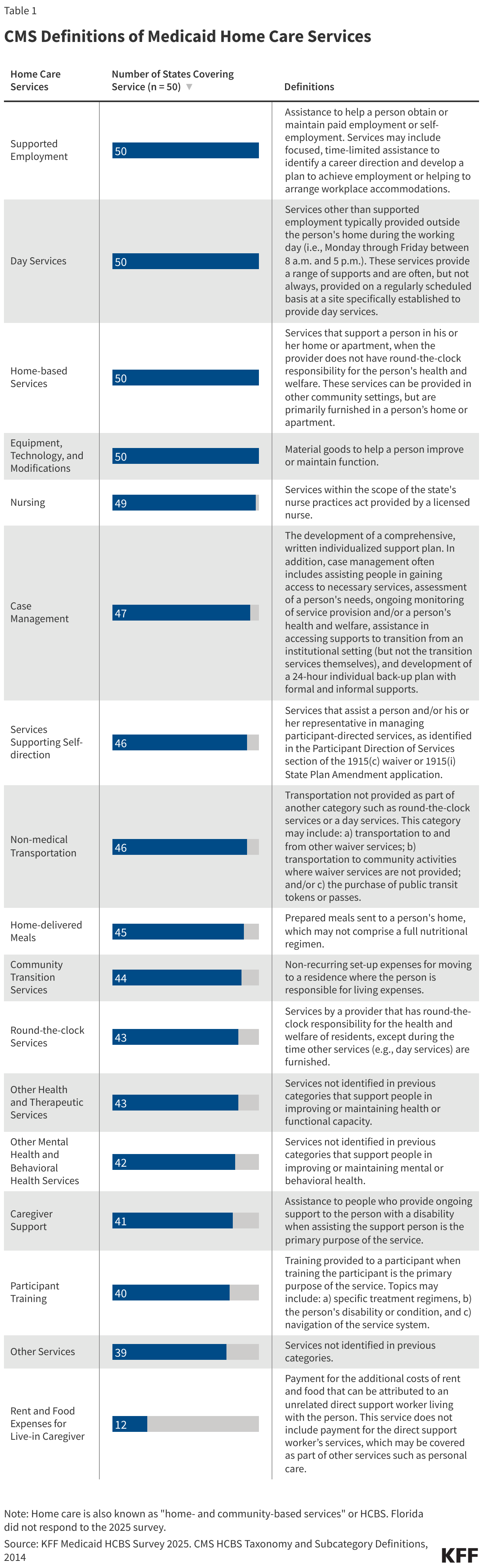
Nursing facility care is a required Medicaid benefit, but states can choose whether to provide most home care services. A key component of home care is personal care, which helps people who need assistance with self-care (such as bathing and dressing) and household activities (such as taking medications and preparing meals).
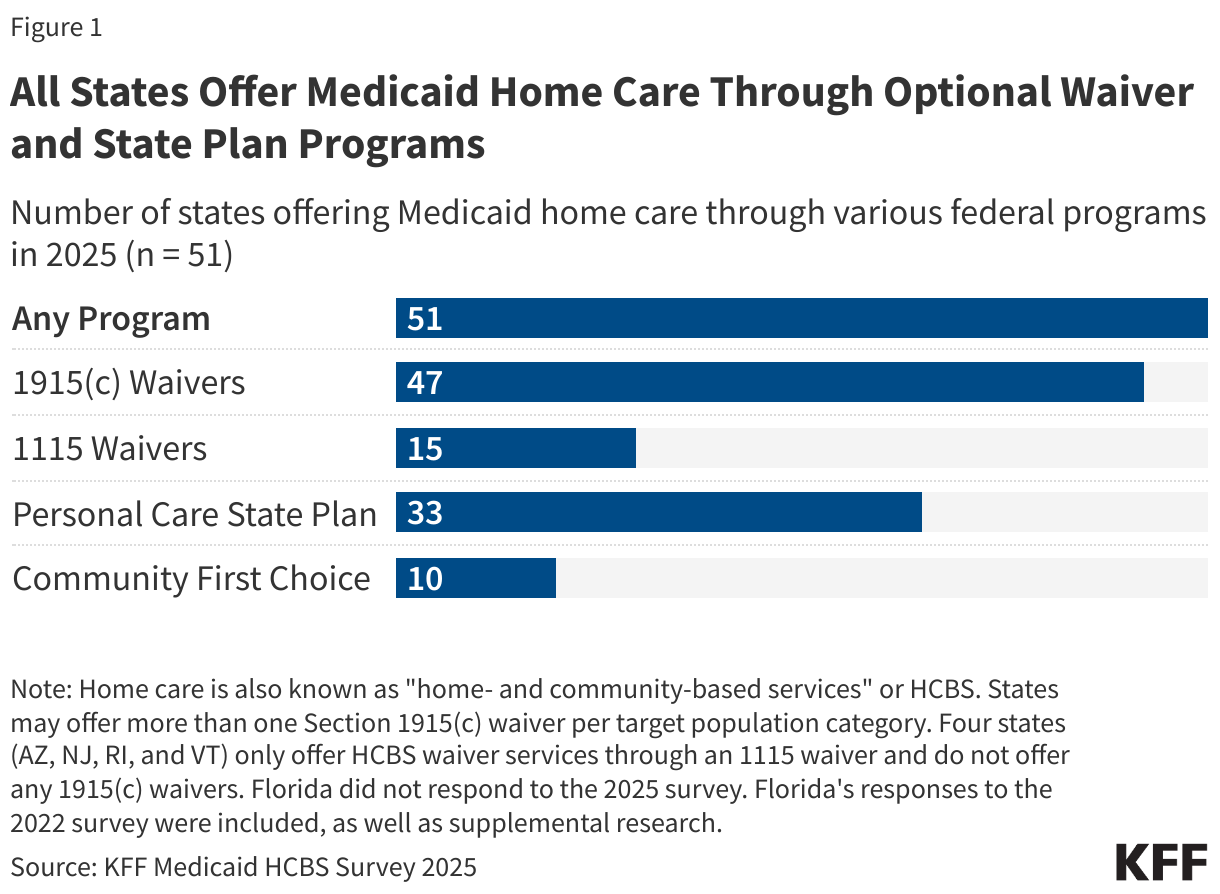
Medicaid home care can be offered through either the Medicaid state plan or as part of a specialized waiver. All states offer Medicaid home care through waivers, most commonly 1915(c) waivers (47 states).
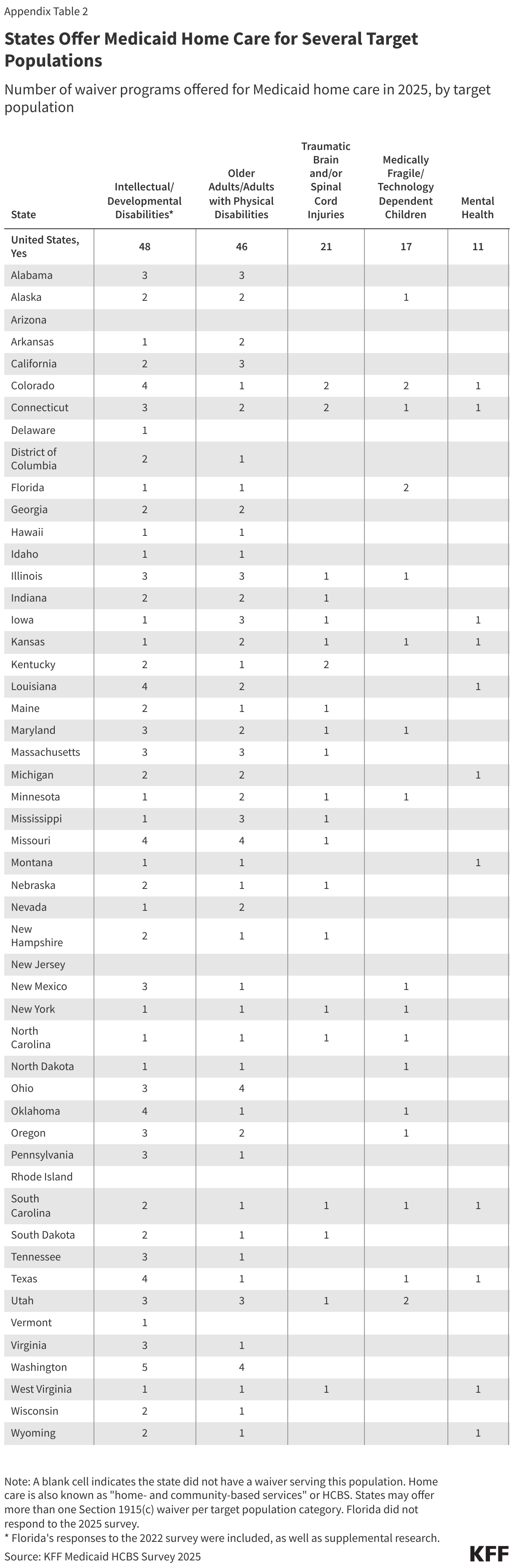
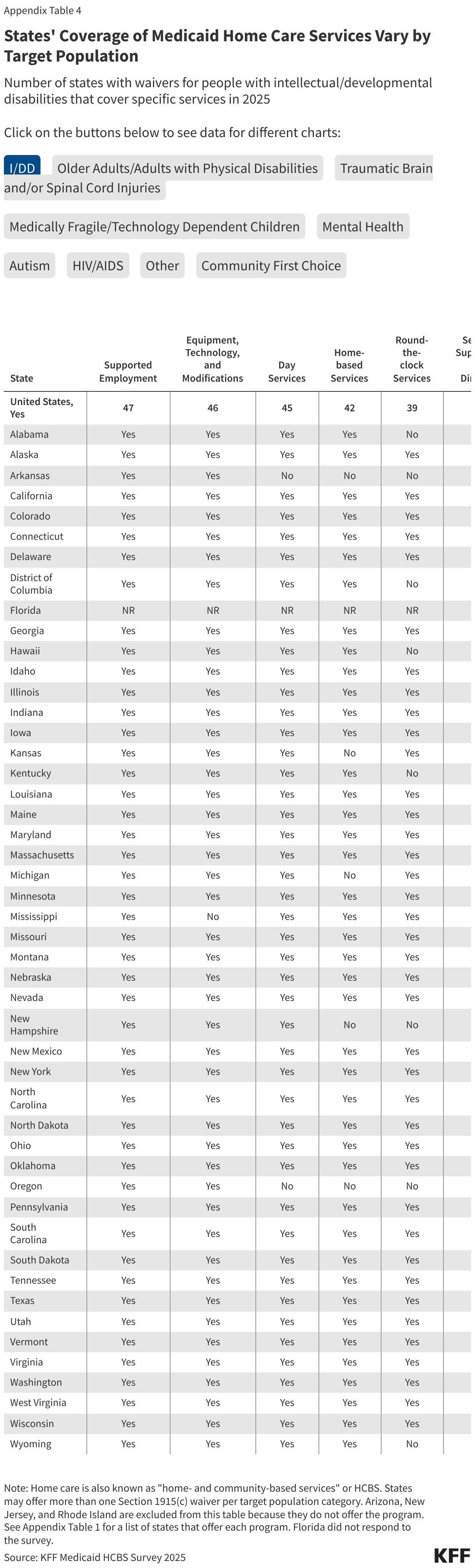
Most states provide Medicaid home care through waivers that offer benefits specifically targeted to people with intellectual or developmental disabilities (48) and people ages 65 and older or who have physical disabilities (46). For such waivers, most states offer multiple waivers for each population: Among states with intellectual or developmental disability waivers, only 16 offer one program, while 18 offer three or more; and among states with waivers serving people ages 65 and older or who have physical disabilities, 24 offer only one program and 10 offer three or more.
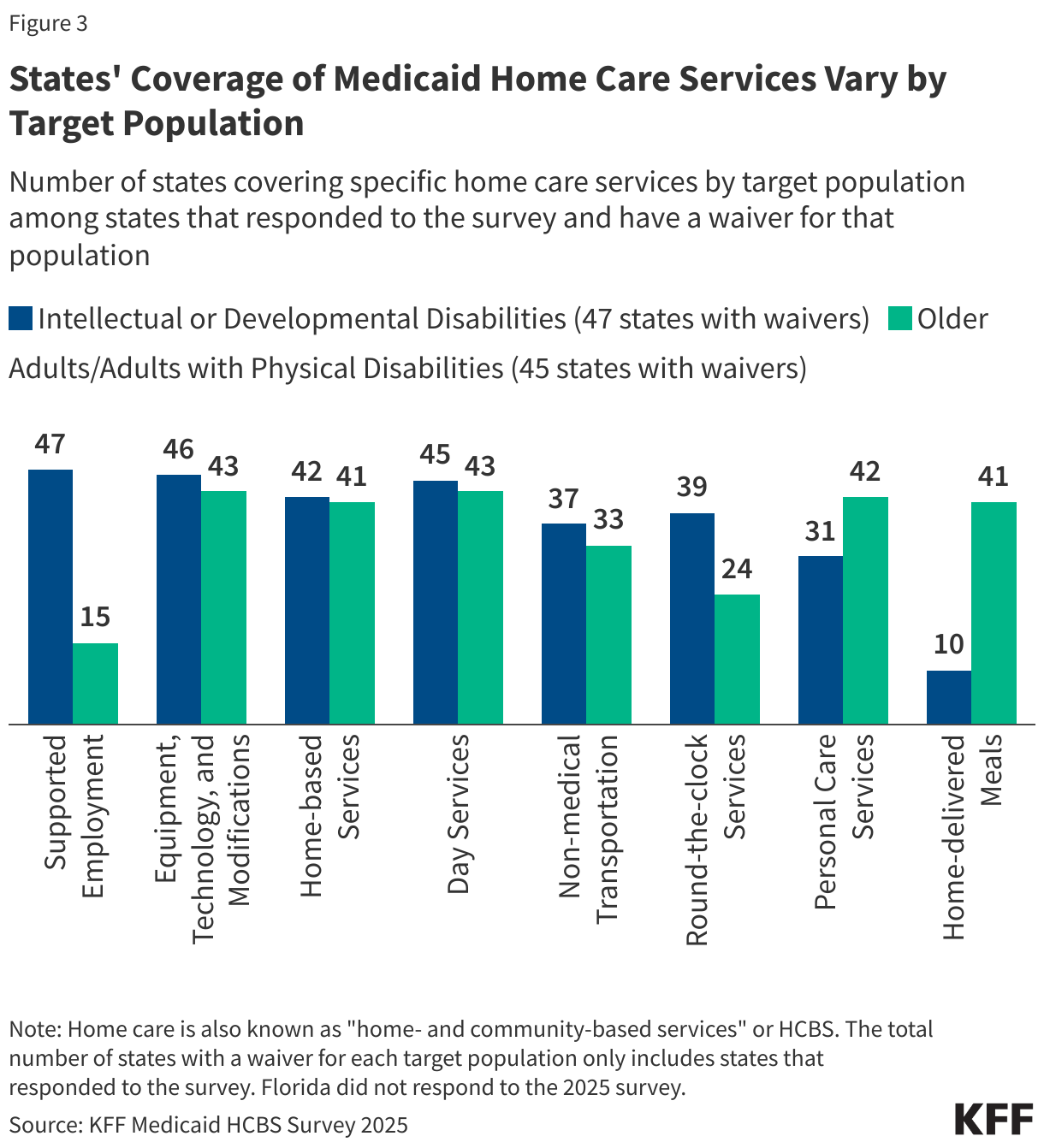
Waivers’ coverage of different home care services, such as day services, supported employment, and home-based services, vary by the target populations they serve.
What programs do states use to provide Medicaid home care?
Unlike institutional long-term care, nearly all home care is optional for states to provide under Medicaid. States are required to offer cover home health—which consists of part-time nursing services; home health aide services; and medical supplies, equipment, and appliances suitable for use in the home—but all other home care services are provided at the discretion of the states. States use various federal legal “authorities,” also known as programs, to offer home care, which are generally categorized as being part of the Medicaid state plan or part of a waiver. If services are provided through a state plan, they must be offered to all eligible individuals. In contrast, services provided under waivers, such as 1115s or 1915(c)s, may be restricted to specific groups based on geographic region, income, or type of disability. Waivers may include a wider range of service types than can be provided under state plans, but states may limit the number of people receiving waiver services. When the number of people seeking services exceeds the number of waiver slots available, states may use waiting lists to manage participation in the waiver.
All states have at least one home care program and many states have multiple programs. Home care is most frequently offered through 1915(c) waivers (47 states) and the personal care state plan benefit (33 states), and less frequently offered through 1115 waivers (15 states) or the Community First Choice option (10 states, Figure 1). KFF estimates that 5.1 million people used Medicaid home care in 2023 compared with only 1.4 million people who used institutional long-term care.
All states offer people assistance with self-care and household activities under the personal care benefit, but they use different programs to do so. The primary home care benefit is personal care, which provides people with assistance with the activities of daily living (such as eating and dressing) and the instrumental activities of daily living (such as preparing meals and managing medication). States most commonly cover personal care through waivers (48 states), followed by the state plan (33 states).
How are people eligible for Medicaid home care?
Most people who are eligible for Medicaid home care qualify on the basis of having a disability or being ages 65 and older. Medicaid eligibility pathways in which eligibility is based on old age or disability are known as “non-MAGI” pathways because they do not use the Modified Adjusted Gross Income (MAGI) financial methodology that applies to children, pregnant individuals, parents, and other non-elderly adults with low incomes. In addition to considering income and age or disability status, non-MAGI eligibility pathways usually require people to demonstrate that they have limited savings and other financial resources (e.g., assets). Because nearly all non-MAGI pathways are optional, eligibility levels vary substantially across states.
Most states allow people with somewhat higher incomes to qualify for Medicaid home care, but income is capped at 300% of the supplemental security income limit ($2,901 per month in 2025) and assets are usually limited to $2,000 per person. Medicaid enrollees who use long-term care must also meet requirements related to their functional needs which are generally measured in terms of the ability to perform activities of daily living such as eating and bathing. Over half of people who use Medicaid home care are also enrolled in Medicare; such people are also known as dual-eligible individuals
In 2025, states operated over 300 different programs for Medicaid home care, many of which targeted a specific population. Most programs (259) were operated through 1915(c) waivers with 15 operated through 1115 waivers. The most common waiver programs target people with intellectual or developmental disabilities (48 states) and people who are ages 65 and older or have physical disabilities (46 states). States are likely to offer multiple waiver programs for the most common target populations, but states with less common waivers, such as those serving people with traumatic brain or spinal cord injuries or mental health conditions, typically only offer one program per target population.
Each year, some states’ waiver programs change, but in general, the trend has been towards offering more waivers. In 2025, only one state, Oregon, had new waivers and no states eliminated waivers. In Oregon, there is a new 1115 waiver for people who are ages 65 and older or have physical disabilities that provides in-home support services and support for family caregivers and a new 1915(c) waiver that allows parents of minor children with disabilities to be paid for providing attendant care to their child.
What services does Medicaid home care cover?
Besides personal care, Medicaid home care covers an array of services to help people with the activities of daily living and the instrumental activities of daily living. KFF asked states about what services they provide through Medicaid home care programs using the Centers for Medicare and Medicaid Services’ list of services, which are categorized in a comprehensive taxonomy. The taxonomy was developed to provide common language for describing home- and community-based services across waivers and state plans. Those services vary widely, including adult day care, supported employment, round-the-clock care, services to support unpaid family or friends who are caregivers, home-delivered meals, and non-medical transportation (Table 1).
All responding states (50) cover supported employment, day services, home-based services, and equipment, technology, and modifications in any home care program (Appendix Table 3). States often also offer other additional services for specific populations that are uniquely tailored to the needs of waiver recipients. Examples of such services reported in the 2025 survey include:
Illness support, group counseling, and bereavement counseling in a waiver for children who are medically frail or technology dependent (Colorado);
Discovery and career planning, additional residential supports, and community navigators in a waiver for people with intellectual or developmental disabilities (Hawaii);
Dental services, permanent supportive housing, and prevocational/community career planning in a waiver for people with intellectual or developmental disabilities (Louisiana);
Other speech, hearing, language, occupational, and physical therapies in a waiver for people who are ages 65 and older or have physical disabilities (Texas).
Among the categories defined by the Centers for Medicare & Medicaid Services, the least-frequently covered service was rent and food expenses for a live-in caregiver. For the most common services, there is little change in the number of states offering each type of service in a given year. (The numbers reported for most services are higher in 2025 but in many cases, that reflects a higher state response rate in 2025 than in 2024.)
States use waivers that target specific populations to offer tailored benefits, and covered services differ among different types of waivers (Figure 3, Appendix Table 4). Some services, such as equipment, technology and modifications, home-based services, and day services, are covered by most states and in most waiver programs. However, other services are much more targeted to specific populations. Comparing services among the most commonly-offered waivers (those serving people with intellectual or developmental disabilities and people who are ages 65 and older or have physical disabilities), shows some services are widely covered by one type of waiver but not the other. For example, 47 states cover supported employment for people with intellectual or developmental disabilities, but only 15 cover the service for people who are ages 65 and older or have physical disabilities, a population less likely to be working. Alternatively, home-delivered meals are covered by 41 states under waivers serving people who are ages 65 and older or have physical disabilities, but only under 10 states’ waivers serving people with intellectual or developmental disabilities. By enabling states to cover, at times, different services per target population, waivers allow states to customize services to the needs of the specific populations they serve.
Within waivers, states may change the benefit offerings from year to year, highlighting the flexibility that home care waivers offer to states in managing program benefits and spending. Focusing on the most common waivers and benefits, some notable changes between 2024 and 2025 include the following. (Due to variation in the number of states responding to KFF’s survey and changes in the number of waivers offered between 2024 and 2025, comparing the number of states or waivers offering each type of service could be misleading. However, looking at changes in covered services within a specific waiver can illuminate the flexibility available to states.)
Oregon began offering coverage of equipment, technology, and modifications for waivers serving people who are ages 65 and older or have physical disabilities, and Idaho now covers case management services for waivers serving the same population.
D.C. and South Dakota started offering coverage of non-medical transportation for waivers serving people with intellectual or developmental disabilities, but Illinois and Kentucky no longer cover this service for those waivers.
Michigan, Nevada, and Washington began covering day services for waivers serving people with intellectual or developmental disabilities, and Idaho started offering this benefit for waivers serving people who are ages 65 and older or have physical disabilities.
How do states use managed care to provide home care?
All but 11 states use managed care to provide at least some home care (Figure 4). In managed care, states pay managed care plans a set fee—often called a capitation payment—for each person enrolled and the managed care plans are responsible for providing all services to enrollees. Use of managed care to provide home care has been growing over time, with states using managed care to make their Medicaid spending more predictable and to help coordinate the services enrollees use.
Managed care is more commonly used for home health benefits provided through the state plan or 1115 waivers than for 1915(c) waivers (Figure 5, Appendix Table 5). Among the 15 states with 1115 waivers, 10 use managed care plans to provide at least some home care; and over two-thirds of states use managed care plans to provide at least some home health through the state plan. Fewer than half of states use managed care plans to provide some personal care through the state plan. For 1915(c) waivers, over half of states (26) use managed care plans, 4 more states than in 2024, but managed care was much less common for waivers serving people with intellectual or developmental disabilities—of the 47 out of 51 responding states with such waivers, only 8 provided any of the benefits through managed care.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Appendix Tables
States Offering Medicaid Home Care Through Various Federal Programs
States Offer Medicaid Home Care for Several Target Populations
States Reporting Coverage of Each Medicaid Home Care Service Under Any Program
States' Coverage of Medicaid Home Care Services Vary by Target Population
All States Provide Optional Medicaid Home Care, Many Using Managed Care
KFF estimates that 5.1 million Medicaid enrollees use home care, which provides medical and supportive services to help people with the activities of daily living (such as eating and bathing) and the instrumental activities of daily living (such as preparing meals and managing medications). Medicare generally does not cover home care (also known as home- and community-based services or HCBS), and Medicaid paid for two-thirds of home care spending in the United States in 2023.
In Medicaid home care, many people “self-direct” their services, giving them greater autonomy over the types of services provided and who they are provided by; and in some cases, allowing payments to family caregivers. Payments for caregiving can help mitigate the financial struggles family caregivers experience when they are forced to reduce their hours of work or quit their jobs on account of their caregiving duties. KFF focus groups of caregivers found that family caregivers often reported struggling to make ends meet and having to reduce the hours they are working other jobs due to the demands of caregiving. Self-directed services can also help address shortages of paid home care workers, which can be one of the factors placing additional strain on family caregivers. Beyond paying for their caregiving, Medicaid supports family caregivers with services such as training, support groups, and respite care (which is paid care that allows family caregivers to take a break from their normal responsibilities).
The 2025 reconciliation law, passed on July 4, includes significant changes to the Medicaid program that are estimated to reduce federal Medicaid spending by $911 billion over the next decade. Given the substantial share of Medicaid spending that pays for home care, and the optional nature of most home care programs, cuts to home care programs could occur as states respond to the reductions in federal spending.
Such changes could affect Medicaid supports to family caregivers, all of which are optional for states to provide. A reduction in the availability of those supports could exacerbate challenges for people who need home care and are unable to find other sources of care due to workforce shortages, which may be amplified by the Trump Administration’s intensified immigration enforcement and restrictive policies, since nearly one-in-three home care workers are immigrants. For family caregivers, many may need to continue to provide care without payments and other Medicaid changes could affect access to health coverage. According to AARP’s 2025 Caregiving in the US report, there are over 8 million family caregivers for whom Medicaid is their source of health insurance (13% of 63 million total family caregivers).
Amidst this background, this issue brief describes the availability of self-directed services and supports for family caregivers in Medicaid home care in 2025, before most provisions in the reconciliation law take effect. The data come from the 23rdKFF survey of officials administering Medicaid home care programs in all 50 states and the District of Columbia (hereafter referred to as a state), which states completed between April and July 2025. The survey was sent to each state official responsible for overseeing home care benefits (including home health, personal care, and waiver services for specific populations such as people with physical disabilities). All states except Florida responded to the 2025 survey, but response rates for certain questions were lower. Survey findings are reported by state and waiver target population, although states often offer multiple waivers for a given target population. Key findings include:
All reporting states except Alaska allow Medicaid enrollees to self-direct their home care in at least some circumstances, and among those states, all allow enrollees to select, train, and dismiss their caregivers.
All responding states pay family caregivers under some circumstances and provide family caregivers with other types of support, including respite care (Figure 1, Appendix Table 1)
Family supports are most widely available for caregivers of people with intellectual or developmental disabilities (I/DD).
How Many States Allow Medicaid Enrollees to Self-Direct Their Home Care?
Nearly all states allow Medicaid enrollees to self-direct their home care in some circumstances (Figure 2, Appendix Table 2).Self-direction came out of the “consumer-directed” movement for personal care services that started with demonstration programs in 19 states funded through grants from the Robert Wood Johnson Foundation. Today, states may give people the option to self-direct home care through a wide variety of optional home care programs. States most frequently allow self-direction in waivers that serve people with intellectual or developmental disabilities, followed by people who are ages 65 and older or have physical disabilities. Among the 50 states responding to KFF’s survey, Alaska is the only state that reported not permitting self-direction under any of the home care programs.
Among states that authorize self-direction, all states allow enrollees to select, dismiss, and train workers (Figure 3). The ability to select, train, and dismiss workers is referred to as “employer authority” because it allows Medicaid enrollees (with the help of their designated representatives when appropriate) to decide who will be caring for them. All states with self-directed services programs provide employer authority to enrollees. Most states also allow enrollees to establish payment rates for their caregivers (41) and to determine how much Medicaid funding is spent among the various authorized services (39).
How Many States Pay Family Caregivers and Through Which Home Care Programs?
All responding states pay family caregivers through one or more Medicaid home care programs (Figure 1, Appendix Table 1). Family caregivers can generally be paid to provide personal care, which may be offered through several different types of Medicaid home care programs. Personal care may be provided through waivers such as the 1115 or 1915(c) programs, through the Medicaid state plan, or a combination of both. Waiver services tend to encompass a wider range of benefits than the state plan benefit, but waivers are usually restricted to specific groups of Medicaid enrollees based on geographic region, income, or type of disability; and are often only available to a limited number of people, resulting in waiting lists.
All responding states allow payments to family and friends through one or more waiver programs, but fewer states allow payments to legally responsible relatives. Forty-four states allow payments to legally responsible relatives through waiver programs. Payments to legally responsible relatives are less common than those to other family and friends because of additional legal requirements that pertain to payments to legally responsible relatives (Box 1). Payments to family caregivers are less common through the state plan—allowed by 24 states for other family and friends and by 6 states for legally responsible relatives. States pay family caregivers through the state plan less frequently because fewer states offer personal care through the state plan and because the legal requirements governing state plan services are more restrictive than those governing waiver services.
While all responding states allow payments to family caregivers, it is unknown what percentage of waiver participants are receiving paid care. KFF asked states, “What percentage of waiver recipients are receiving paid care from their legally responsible relatives/family members who are not legally responsible relatives?” Over two-thirds of states were unable to report the percentage of waiver recipients receiving paid care from either legally responsible relatives or other family members/friends. It is also unknown how often people with paid family caregivers also receive other paid care.
Box 1: What are the legal requirements for paying family caregivers?
Medicaid laws have more complicated requirements for states to pay legally responsible relatives than is the case for other types of family and friend caregivers. The specific legal requirements for paying family caregivers are complicated and differ across home care programs:
• For personal care offered through the state plan using section 1905 authority, there is a federal prohibition on paying for services provided by spouses and parents of minor children (which comprise most but not all legally responsible relatives). Other family and friends may be paid if they meet applicable provider qualifications, there are strict controls on the payments, and the provision of care is justified (which can be done when there is a lack of other qualified providers in the area).
• For home care offered through waiver programs, the requirements governing payments to family and friends are like those governing personal care through section 1905 authority. A key difference is that states may pay legally responsible relatives when the services being provided are “extraordinary care,” which is defined as care that exceeds the range of activities a legally responsible relative would ordinarily perform and is necessary to health, welfare, and avoiding institutionalization.
• For personal care offered through the state plan using one of the section 1915 authorities, states may pay legally responsible relatives using criteria like those of the waiver programs. However, some of those authorities designate a family member to be the recipient’s legal representative and may prohibit payments to legal representatives.
Payments for family caregivers are most common under waivers for people with intellectual or developmental disabilities (Figure 4, Appendix Table 3). Among the 47 states that responded to the survey and have waivers for people with intellectual or developmental disabilities, all 47 allow payments to family caregivers. There are fewer states with other types of waivers, and not all the other waivers allow payments to family caregivers. Among the 45 responding states with waivers for older adults and people with physical disabilities, 43 pay family caregivers, and among the 21 states with waivers for people with traumatic brain or spinal cord injuries, 19 do.
In most cases, family caregivers receive hourly wages like those of other employees, but 11 states have adopted programs known as structured family caregiving, in which family members are paid a per diem rate (Appendix Table 4). Structured family caregiving is a Medicaid benefit that supports unpaid caregivers of people who use Medicaid home care through waiver programs. In the structured program, Medicaid pays provider agencies a daily stipend for participants. The agency is responsible for directing a care coordinator or social worker and a nurse to oversee the family caregiver, answer health-related questions, and provide emotional support; conducting home visits about once per month; and passing a fixed percentage of the stipend (usually 50% - 65%) on to the family caregiver. Among the handful of payment rates reported in an overview of the program by the American Council on Aging, payments to family members are around $40 to $70 per day. States reported structured family caregiving programs in the following home care waivers:
Older adults and people with disabilities in 9 states (Connecticut, Georgia, Indiana, Louisiana, North Carolina, North Dakota, Ohio, Rhode Island, and South Dakota),
People with intellectual or developmental disabilities in 2 states (Indiana and New Hampshire),
Medically fragile children in North Carolina,
People with traumatic brain and/or spinal cord injuries in Indiana and
People with Alzheimer’s and related disorders in Missouri.
Although KFF’s survey only includes home care waivers, according to the American Council on Aging, two states offered structured family caregiving as a standalone program: Massachusetts offers it as a state plan benefit through a program for adults in foster care, and Nevada has a standalone waiver to provide the benefit for caregivers of people with Alzheimer’s and related dementias.
What Other Types of Support Does Medicaid Home Care Provide for Family Caregivers?
All responding states provide support for family caregivers—who may be paid or unpaid—and most offer more than one type of support (Figure 5, Appendix Table 5). All responding states reported covering respite care, which provides short-term relief for caregivers, allowing them to rest, travel, attend appointments, or spend time with other family and friends. Other commonly covered benefits include caregiver training (37 states), and counseling or support groups (26 states).
Respite care may be provided anywhere from a few hours to several weeks at a time. Medicare only covers respite care for people who are receiving hospice care, which is only available for people who are terminally ill and electing to receive comfort care instead of curative care for their illness. That makes Medicaid’s respite care the primary source of coverage for caregivers of people with Medicare and Medicaid. Respite care is offered most frequently under waivers for people with intellectual or developmental disabilities (44 states) and older adults and people with disabilities (44 states).
Daily respite care is offered by the most states (43), followed by institutional respite care (40 states, Figure 6, Appendix Table 6). Daily respite care is available under waivers for people with intellectual or developmental disabilities in 34 states and available in 32 states within waivers for people who are ages 65 and older or have physical disabilities. Twenty-two states provide institutional respite care within waivers for people who are ages 65 and older or have physical disabilities and within waivers for people with intellectual or developmental disabilities. Weekly respite care is the least frequently offered (24 states total), and over half of states (32) report offering other types such as hourly, monthly, or annual.
This work was supported in part by Arnold Ventures. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Appendix Tables
States' Policies to Allow Medicaid Home Care Payments to Spouses, Parents of Minor Children, and Other Legally Responsible Relatives for Caregiving
States' Policies to Allow Individuals to Self-Direct Medicaid Home Care by Waiver/Program
States' Policies to Allow Medicaid Home Care Payments to Spouses, Parents of Minor Children, and Other Legally Responsible Relatives as well as Family and Friends for Caregiving
States Offering the Structured Family Caregiver Program, Which Supports Unpaid Caregivers of Persons Who Are Using Medicaid Home Care, and Waivers the Program Is Offered Under
States’ Policies for Offering Different Types of Family Caregiving Supports
Types of Respite Care Offered by State and Home Care Program: Daily, Weekly, Institutional, and Other
Long-standing workforce challenges in Medicaid home care (also known as home- and community-based services or HCBS) impact care for the over 5 million people who use these services. Shortages and high turnover rates among the direct care workforce reflect demanding work and low wages, particularly among home care workers (who are direct care workers that provide HCBS). This issue brief describes states’ ongoing efforts to respond to shortages of home care workers and how they pay these workers, finding that increased payment rates are a key component of states’ efforts to address workforce shortages.
Such shortages could increase as states will face tough choices about how to absorb Medicaid cuts stemming from the 2025 reconciliation law, which is estimated to reduce federal Medicaid spending by $911 billion over the next decade. When faced with fiscal pressures in the past, states have responded with restrictions on home care, and as a result of the reconciliation law, states may again face significant pressures to cut Medicaid payment rates, offer fewer covered benefits, or restrict eligibility. The Medicaid cuts could also affect access to health coverage among home care workers because over one-in-three workers in home care settings are enrolled in Medicaid. Reduced access to health coverage among the workforce could exacerbate other challenges.
Workforce challenges may also worsen in future years because of changes in immigration policy. Nearly one-in-three home care workers are immigrants, and the Trump Administration’s intensified immigration enforcement and restrictive policies are deepening anxiety and fear among immigrants of all statuses. KFF survey data finds that 13% of immigrants have avoided going to work since January 2025 because of concerns about drawing attention to someone’s immigration status, a number which rises to 40% among people who are likely to be undocumented immigrants. Fewer immigrants overall and potentially lower rates of employment among immigrants could reduce the size of the home care workforce. With more limited immigration, there will be fewer workers overall to care for an aging population.
Amidst this evolving landscape, this issue brief describes Medicaid payment rates for home care and other workforce supports that are in place in 2025, before the majority of the 2025 reconciliation law provisions start taking effect. This issue brief is one of several reporting the data from the 23rdKFF survey of officials administering Medicaid home care programs in all 50 states and the District of Columbia (hereafter referred to as a state), which states completed between April and July 2025. The survey was sent to each state official responsible for overseeing home care benefits (including home health, personal care, and waiver services for specific populations such as people with physical disabilities). All states except Florida responded to the 2025 survey, but response rates for certain questions were lower. States generally completed the survey prior to enactment of the 2025 reconciliation law. Survey findings are reported by state and waiver target population, although states often offer multiple waivers for a given target population. Key takeaways include:
All responding states reported taking actions to address workforce shortages, with most states raising payment rates (Figure 1).
All states reported shortages of home care workers, most frequently among direct support professionals, nursing staff, personal care attendants, and case managers.
Most (41) states reported permanent closures of home care providers within the last year.
Among the 34 states that reported time-based payment rates for personal care providers, more than half pay less than $20 per hour.
How are States Addressing the Workforce Challenges in Home Care?
All responding states reported workforce shortages in 2025, with the most common shortages being among direct support professionals (48 states), followed by nursing staff (47 states) and personal care attendants (46 states) (Figure 2, Appendix Table 2). States were asked if they had shortages of each type of provider but were not provided with a definition of “shortage.” Most states also reported shortages in case managers (44 states), home health aides (41 states), certified nurse aides (39 states), community-based mental health providers (38 states), and occupational, physical, and speech therapy providers (30 states). In some cases, states may not have reported a shortage of a particular type of provider because that type of service is not offered through their home care program.
All states reported shortages for more than one type of provider, and 43 states reported shortages among five or more provider types. Such shortages may reflect low compensation coupled with demanding working conditions. In the spring of 2024, home care providers participating in KFF focus groups reported that their jobs had high physical demands and mental demands that were often “overwhelming.” The groups described their wages as low, particularly given the demands of their jobs; and how staffing shortages made their jobs harder because they may not know if they would be able to leave work at the end of their shift. In survey responses, states attributed shortages to low reimbursement rates, lack of qualified providers, and high turnover rates.
Within the last year, 41 states reported permanent closures of home care providers, which were most common among adult day health programs (28 states), followed by group homes (23 states), assisted living facilities, and the enrollee’s home (22 states each) (Figure 3, Appendix Table 3). States were asked if there were any permanent closures of providers that offer services for Medicaid enrollees based on the location in which the providers deliver care. For a setting such as an assisted living facility or group home, a closure could reflect either the closure of an assisted living facility or the closure of a home care agency that sent workers into facilities and group homes. States were not asked to provide a reason for the closures. Some states reported closures of supported employment providers (12 states), home health agencies (11 states), and community mental health providers (5 states). Most states reported closures among more than one type of provider: 35 states reported closures among two or more provider types, and 26 states reported closures among three or more provider types.
All responding states reported taking actions to address provider shortages, with 48 states increasing payment rates, 38 states developing or expanding worker education and training programs, and 24 states offering incentive payments to recruit or retain workers (Figure 1, Appendix Table 1). Less common initiatives included establishing or raising the state minimum wage (20 states), offering worker retention bonuses (20 states), and offering paid sick leave for workers (18 states). States also reported other types of initiatives to strengthen the workforce, including initiatives allowing people to receive paid care from family members. For example, Oregon created a new 1915(c) waiver that allows parents of minor children to be paid for providing attendant care to their child. States’ actions to address provider shortages in 2025 were similar to those in 2024.
All but 11 states use managed care to provide at least some home care, and in over half of the states with managed care, fee-for-service payment rates impact the payment rates that managed care plans pay home care providers. Out of the 39 states that use managed care to provide at least some home care, 20 states reported that the fee-for-service payment rates represent the minimum amount that plans must pay providers, 2 states, Michigan and Wisconsin, reported that the rate represents the maximum payment rate for managed care plans, 11 states reported that the fee-for-service rates do not affect payments by private plans, and 6 states responded that the answer was unknown or did not respond to the question.
How Much do States Pay for Medicaid Home Care?
KFF asked states to report their average hourly rate paid to two types of home care provider agencies (personal care agencies and home health agencies) and three types of specific home care providers (personal care providers, home health aides, and registered nurses), but many states were unable to report all rates (Appendix Table 4). The number of states that responded to the survey but did not provide hourly payment rates or reported that payment rates were unknown was 4 for personal care agencies and 32 for home health agencies. Many states also did not provide payment rates for specific provider types: For registered nurses and home health aides, more than half of states did not provide hourly payment rate information or reported that payment rates were unknown.
Starting July 2026, states are required to report detailed payment rates for personal care, home health, and other services, per the provisions of the Biden Administration final Access rule (see Box 1). In addition to reporting payment rates for certain home care services, starting in 2030, states must demonstrate that at least 80% of the payments went to compensation for providers, also described as “direct care workers.” Meeting that requirement will require states to know both agency and provider payment rates. Among the states that were able to report payment rates, only 15 could report payment rates for personal care agencies, home health agencies, personal care providers, and home health aides, all of which would be required under the rule. Those 15 states include states that reported a mix of hourly and non-hourly rates, which makes comparisons between provider and agency rates more complicated. These challenges highlight the difficulties states face as they implement the requirements in the new rule, which will take effect in July 2026 (Box 1).
Box 1: Biden Administration Final Access Rule’s Provisions on Home Care
On May 10, 2024, the Biden Administration released a final rule aimed at helping to ensure access to Medicaid services, which has several notable provisions aimed at increasing transparency and improving access to Medicaid home care, increasing home care payment rates, and addressing home care workforce challenges. Although the 2025 reconciliation law delayed other Medicaid rules until 2034, it did not address the final rule on access to Medicaid services.
The rule cites workforce shortages as a major contributor to home care access barriers among Medicaid enrollees. To address those access barriers, the rule requires states to implement the following requirements. Some of the rules take effect as early as 2026, which means guidance to states about how to implement the requirements could emerge soon.
• Starting July 2026, states must report state hourly payment rates for personal care, homemaker services, home health aide services, and habilitation and publish that information on the state website. If states rates vary across provider types, geographies, or other factors, the states must report each of those rates.
• For each type of payment rate, the disclosures must also include the number of Medicaid paid claims and the number of Medicaid enrollees who received the service within the calendar year.
• States must establish an interested parties advisory group (IPAG) comprised of direct care workers, Medicaid enrollees and their representatives, and other interested parties. The IPAG will meet at least every two years to advise and consult on the sufficiency of current and proposed payment rates for personal care, homemaker services, home health aide services, and habilitation.
• Starting July 2030, states must ensure that at least 80% of payments to Medicaid providers for designated home care go directly to compensation for direct care workers. Designated home care include personal care, homemaker services, home health aide services, and habilitation. States may adopt separate standards for small providers or exempt small providers that meet reasonable criteria.
Beyond payment rates, the Access rule includes other requirements aimed at increasing access to home care. Starting July 2027, states will be required to report the number of people on waiting lists for services and the average amount of time from when homemaker services, home health aide services, or personal care services are initially approved to when services begin and the percentage of authorized hours that are provided. The proposed rule also includes provisions that would strengthen requirements around person-centered planning and needs assessment, create new requirements around incident management, establish requirements for people to file grievances if they are receiving home care from the state Medicaid program, and require states to report on nationally-standardized quality measures.
The home care payment-related requirements are one component of a broader emphasis on addressing Medicaid payment rates. The Access rule also requires states to report all fee-for-service Medicaid payment rates on state websites, and to compare various service-specific rates to those of Medicare. A companion rule on Medicaid managed care requires states to submit an annual payment analysis comparing managed care plans’ payment rates to Medicare payment rates for selected services.
States reported many reasons why it was difficult to report payment rates, including the following.
Some states reported that services were bundled together in various ways and therefore, the payment rates were not distinguishable.
Among states with managed care, some states responded that they did not know the payment rates for agencies because the services were paid for by managed care plans and they did not have access to those payment rates.
Other states responded that they knew the payment rates for agencies but not what the agencies paid their home care workers. Multiple states reported that they do not “dictate” what agencies pay to providers or that individual providers negotiate their own payment rates with the agencies.
In addition to having difficulty reporting payment rates, many states reported different payment rates for personal care across different waivers, and the waiver payment rates often differ from the payment rates for personal care provided through the state plan. When states reported multiple payment rates for personal care, KFF used the median of those payment rates in the analysis.
The payment rates to home care providers show considerable variation and are somewhat higher than those reported by other organizations on account of differences in reporting and provider categorization (Figure 4). KFF’s survey estimates that median payment rates to providers are $19 per hour for personal care providers, $41 for home health aides, and $70 for registered nurses. It is difficult to compare those numbers to other sources of data for the following reasons.
Other organizations group classes of providers together differently. PHI reports that in 2024, the median rate for home care workers was $17 per hour and $18 per hour for residential care aides. The Bureau of Labor Statistics reports $17 per hour for home health and personal care aides in 2024.
Other organizations include payment rates for workers regardless of the source of payment whereas KFF rates only reflect the Medicaid rates. Medicaid often covers more intensive personal care services than other payers, which may contribute to the higher rates.
Payment rates to home health agencies are generally larger than those to personal care agencies, but there is considerable variation in both (Figure 4). Among states reporting hourly rates, the rates for home health agencies range from $25 to $159 whereas those for personal care agencies range from $14 to $44. Those states reported that the median hourly payment to home health agencies was $51 and $26 for personal care agencies. Between 2024 and 2025, the median payment rates for personal care agencies and most other provider types increased marginally.
Among states able to report any payment rate data, payments for personal care workers range from below $15 to over $30 per hour (Figure 5, Appendix Table 4). Rates for home health aides are somewhat higher than those of personal care workers, reflecting the additional training requirements for such workers. Among the states with payment rates for home health aides in the highest category, some states reported that the rates were per visit or per day (which is noted in Appendix Table 4). There were other states with particularly high payment rates that did not report providing rates per visit or per day, but the rates may still reflect a non-hourly payment basis.
Appendix Tables
States' Use of Strategies to Increase the Number of Medicaid Home Care Workers in 2025
States' Responses to Whether They Were Experiencing Workforce Shortages by Type of Worker in 2025
States Reporting Permanent Closures of Home Care Providers in 2025, by the Location in Which Services are Offered
States' Hourly Payment Rates for Home Care Agencies and Workers in 2025