KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
Here’s our recap of the past week in the coronavirus pandemic from our tracking, policy analysis, polling, and journalism.
With U.S. coronavirus case and death cumulative totals continuing to lead the world, KFF President and CEO Drew Altman wrote a featured essay for The BMJ discussing two fundamental policy decisions made by the Trump Administration that set the U.S. on the controversial and highly criticized course it has taken on COVID-19. He writes, “The US coronavirus failure was not inevitable and does not have to be permanent. But it is historically aberrant for our federal government to follow and not lead in a national crisis, and equally unusual for our country to divide rather than unify in a time of crisis.” Additionally, KFF released an overview of President Trump’s record on health care, which features a section on his COVID-19 response.
An analysis by Epic Health Research Network and KFF of 50 million patients’ records finds disparities for people of color across the spectrum of the COVID-19 pandemic, including higher rates of infection, hospitalization and death. Further, people of color are sicker when they test positive and the disparities in hospitalization and death remain when accounting for underlying health conditions and differences in sociodemographic factors.
As public health officials and policymakers prepare for an eventual COVID-19 vaccine, a Policy Watch post examines flu vaccination rates, highlighting the lower rates among adults of color. Insights into the potential barriers and issues that should be addressed as part of a vaccination strategy are discussed.
Here are the latest coronavirus stats from KFF’s tracking resources:
Global Cases and Deaths: Total cases worldwide surpassed 30 million this week – with an increase of approximately 1.9 million new confirmed cases in the past seven days. There were approximately 35,400 new confirmed deaths worldwide, bringing the total to nearly 945,000 confirmed deaths.
U.S. Cases and Deaths: Total confirmed cases in the U.S. neared 6.7 million this week. There was an approximate increase of 278,000 confirmed cases between September 11 and September 17. Approximately 6,000 confirmed deaths in the past week brought the total in the United States to approximately 197,600.
On June 19, 2020, the Trump Administration issued final regulations implementing Section 1557 of the Affordable Care Act. Section 1557 prohibits discrimination based on race, color, national origin, sex, age, and disability in health programs and activities receiving federal financial assistance. Notably, it is the first federal civil rights law to prohibit discrimination in health care based on sex. The final rule, issued in the midst of the ongoing COVID-19 pandemic, significantly narrows the scope of a rule issued in 2016 by the Obama Administration by:
Eliminating the general prohibition on discrimination based on gender identity and sex-stereotyping and specific health insurance coverage protections for transgender individuals;
Adopting blanket abortion and religious freedom exemptions for health care providers;
Eliminating the provision preventing health insurers from varying benefits in ways that discriminate against certain groups, such as people with HIV or LGBTQ people;
Reducing protections that provide access to interpretation and translation services for individuals with limited English proficiency;
Eliminating provisions affirming the right of private individuals to challenge alleged violations of Section 1557 in court and obtain money damages (leaving the right to sue for courts to decide) and requirements for non-discrimination notices and grievance procedures;
Narrowing the regulations’ reach by only covering specific activities that receive federal funding, but not other operations, of health insurers and no longer applying the regulations to all HHS-administered programs; and
Eliminating prohibitions against discrimination based on gender identity and sexual orientation in ten other federal health care regulations outside Section 1557.
Just after the Administration published the final rule, the Supreme Court ruled that sex discrimination includes sexual orientation and gender identity in the employment context. Based on that decision, two federal courts issued nationwide preliminary injunctions blocking parts of the final rule: NY and DC courts blocked provisions excluding sex stereotyping from the definition of sex discrimination, and the DC court also blocked the religious freedom exemption. The NY court is now considering whether to block other provisions of the rule, and other lawsuits are pending.
Introduction
On June 19, 2020, the Department of Health and Human Services (HHS) finalized revised regulations implementing Section 1557 of the Affordable Care Act (ACA),1 which prohibits discrimination in health care based on race, color, national origin, sex, age, and disability in health programs and activities receiving federal financial assistance.2 The final rule (which mirrors a proposed rule issued by HHS in June of last year3 ) is a significant departure from the Obama Administration regulations issued in 2016. Specifically, the final rule eliminates nondiscrimination protections based on gender identity, as well as specific health insurance coverage protections for transgender individuals, adopts blanket abortion and religious freedom exemptions for health care providers, reduces protections for those with limited English proficiency, and limits the activities and entities covered, among other provisions. It also eliminates prohibitions on discrimination based on gender identity and sexual orientation in ten other federal regulations outside Section 1557.
The changes were scheduled to take effect on August 18, 2020, but a Supreme Court ruling in Bostock v Clayton County, Georgia,4 issued just days after the final regulation was released, found that discrimination based on sex encompasses sexual orientation and gender identity in the context of employment. Based on that decision, two federal courts have issued nationwide preliminary injunctions blocking the Administration from implementing parts of the final rule. A NY court blocked the implementation of provisions excluding sex stereotyping from the definition of sex discrimination.5 After the plaintiffs requested clarification about the scope of the preliminary injunction order, the court directed the plaintiffs to submit a list of provisions of the 2020 rule, beyond the definition of sex discrimination, that should be stayed in light of the Supreme Court’s Bostock decision for the court’s consideration.6 The DC court blocked the implementation of provisions excluding sex stereotyping from the definition of sex discrimination as well as provisions incorporating a blanket religious freedom exemption from claims of sex discrimination.7Several other legal challenges to the rule are also pending.8
This issue brief summarizes HHS’s final rule and provides a side-by-side comparison to the Obama Administration 2016 rule (Table 1). It also examines HHS’s changes to other regulations, separate from Section 1557 (Table 2). Finally, it assesses the current status of the final rule in light of the recent Supreme Court ruling and subsequent legal challenges (Table 3). Figure 1 presents a timeline of key dates in Section 1557 implementation, including the development and revision of regulations and subsequent legal challenges. A more expansive timeline is contained in Table 4.
Background and HHS’s Rationale for Changes
Section 1557 incorporates protections from existing civil rights laws. These include Title VI of the Civil Rights Act of 1964 (race, color, and national origin), Title IX of the Education Amendments of 1972 (sex), the Age Discrimination Act of 1975, and Section 504 of the Rehabilitation Act of 1973 (disability). Notably, Section 1557 is the first federal civil rights law to prohibit discrimination on the basis of sex in health care. Section 1557’s protections took effect when the ACA was enacted on March 23, 2010. Implementing regulations issued by HHS under the Obama Administration became effective on July 18, 2016.9
Figure 1: Key Dates in Section 1557 Implementation
The provisions of the 2016 rule that included gender identity and termination of pregnancy in the definition of sex discrimination were vacated by a federal trial court in Franciscan Alliance v. Azar. This case was brought in August 2016 by a group of religiously affiliated health care providers and states, led by Texas.10 In December 2016, a Texas federal district court issued a nationwide preliminary injunction preventing HHS from enforcing the challenged provisions while the case was pending. In October 2019, the court issued a final decision finding violations of the Administrative Procedures Act and the Religious Freedom Restoration Act and vacating the 2016 regulation’s inclusion of gender identity and termination of pregnancy in the definition of sex discrimination as exceeding the authority delegated to HHS by Congress. Specifically, the court found that HHS should have limited its regulatory definition of sex discrimination to a binary definition encompassing biological differences between males and females. The court also found that HHS should have incorporated Title IX’s blanket abortion and religious exemptions into its Section 1557 regulations. In January 2020, the religiously affiliated health care providers appealed to the 5th Circuit Court of Appeals, seeking to have the entire Obama Administration rule vacated. The case is now being briefed and will proceed at the same time as the various lawsuits challenging the Trump Administration’s final regulations (described below).
In contrast to the Franciscan Alliance case, other federal courts have granted relief to private individuals alleging Section 1557 discrimination claims based on gender identity. These courts relied on the text of Section 1557 as enacted in statute, not the contested regulation. For example, a federal district court permanently enjoined the Wisconsin Medicaid program’s categorical exclusion of gender affirming services from coverage, relying on the statute as enacted by Congress.11 Another federal district court case was brought on behalf of a transgender boy, who committed suicide after experiencing “extreme distress” from hospital staff repeatedly referring to him as a girl while he was admitted for psychiatric inpatient care.12 That court allowed a claim for emotional distress damages to proceed, finding that Section 1557’s statutory language prohibiting sex-based discrimination includes discrimination based on gender identity.13
In issuing its June 2020 final rule, HHS under the Trump Administration stated that its changes were needed to “address legal concerns,” relieve costs and regulatory burden, and reduce confusion, because it now views the regulations as inconsistent with or duplicative of other civil rights provisions.14 In support of its changes, HHS cited the Franciscan Alliance decision, though HHS’s changes to the regulations go beyond the issues raised in that case. In addition to gender identity and termination of pregnancy, HHS’s revised Section 1557 regulations substantially change, or in some cases entirely eliminate, existing provisions related to health insurance benefit design; language access; notices, grievance procedures, and enforcement; and which entities are covered (Table 1). Beyond the Section 1557 regulations, HHS removes prohibitions on discrimination based on gender identity and sexual orientation in ten other Medicaid, private insurance, and education program regulations (Table 2). It also adds abortion and religious exemptions to existing regulations that prohibit sex discrimination in education programs under Title IX.
Key Changes in the Trump Administration’s Final Rule
Sex Discrimination
Gender Identity
In the final rule, HHS eliminates entirely Section 1557’s regulatory definition of sex discrimination, as defined by the 2016 rule to include gender identity and sex stereotyping. The preamble notes that, while HHS “declines to replace it with a new regulatory definition. …the final rule reverts to, and relies upon, the plain meaning of the term [sex] in the statute” which in “its original and ordinary public meaning refers to the biological binary of male and female that human beings share with other mammals.”15 HHS also eliminates the definition of gender identity, which previously included gender expression and transgender status. In addition, it removes specific provisions that required covered entities to treat individuals consistent with their gender identity. Neither the 2020 final rule nor the 2016 rule recognizes discrimination on the basis of sexual orientation alone as a prohibited form of sex-based discrimination.16
Removing gender identity and sex stereotyping from the definition of prohibited sex-based discrimination could allow health care providers to refuse to serve individuals who are transgender or who do not conform to traditional sex stereotypes. For example, a health care provider could refuse to treat a patient for a cold or a broken arm based on the patient’s gender identity or refuse to accept a transgender individual in favor of a person who is not transgender when accepting new patients.17 The resulting inability to access needed health care services could exacerbate health disparities experienced by LGBTQ people, such as higher rates of depression and suicide attempts, higher risk of HIV/AIDS, higher use of tobacco and drugs, and higher risk of breast cancer.18 As noted above, two federal district courts in NY and DC have issued nationwide preliminary injunctions blocking the Administration from implementing the provisions of the final rule excluding sex stereotyping from the definition of sex discrimination, and the NY court is now considering whether additional provisions of the final rule should be stayed in light of Bostock. Because the Franciscan Alliance court previously vacated the 2016 rule’s inclusion of gender identity from the definition of sex discrimination, other federal district courts could not subsequently restore the prior regulatory provision. However, given the Supreme Court’s recent Bostock decision (discussed below), further litigation is likely to address the inclusion of gender identity as part of prohibited sex discrimination under Section 1557.
The final rule no longer explicitly prohibits covered entities from denying or limiting services that are ordinarily or exclusively available to one sex or gender when those services are sought by an individual of a different sex or gender. In contrast, the 2016 regulation prohibited differential coverage of services based on the fact that an individual’s sex assigned at birth, gender identity, or gender in a medical or health plan record differs from the one to which such services are ordinarily or exclusively available. For instance, under the previous regulation, health plans could not deny medically necessary treatment for ovarian cancer in a transgender man based on his gender identity.19 Commenters responding to the Administration’s draft rule issued in 2019 worried that the rule ”would allow or encourage providers to deny basic healthcare to individuals who identify as transgender.”20 While HHS noted that ”all people should be treated with dignity and respect, regardless of their characteristics including their gender identity, and they should be given every protection afforded by the Constitution and the laws passed by Congress,”21 the rule does not extend such protections to transgender people.
The final rule also eliminates the provision that prohibits a health plan from categorically or automatically excluding or limiting coverage for health services related to gender transition. Under the final rule, it appears an issuer could deny coverage for a hysterectomy that a provider determines is medically necessary to treat a patient’s gender dysphoria, even though hysterectomies are covered in other circumstances.22 Despite evidence to the contrary, as cited in the preamble to the Obama Administration’s 2016 rule,23 HHS now argues that there is a lack of consensus on care for transgender people and explicitly states, “a medical provider may rightly judge a hysterectomy due to the presence of malignant tumors to be different in kind from the removal of properly functioning and healthy reproductive tissue for psychological reasons, even if the instruments used are identical.”24 This is in contrast to the 2016 regulation which stated that such categorical exclusions are outdated and do not reflect current standards of care.25
Changes to Regulations Beyond Section 1557: Gender Identity and Sexual Orientation
Beyond the Section 1557 regulations, HHS also eliminates explicit nondiscrimination protections related to gender identity and sexual orientation in ten other existing regulations. HHS characterizes these changes as “limited conforming amendments.”26 These regulations include those that govern Medicaid managed care entities, state Medicaid programs, PACE organizations, group and individual health insurance issuers, Marketplaces, qualified health plan issuers, agents and brokers that assist with Marketplace applications and enrollment, and education programs that receive federal financial assistance. In the past, these regulations, some of which had been in place for several years, provided explicit protections against discrimination based on sexual orientation and gender identity. Without these protections, Medicaid managed care entities could discriminate against LGBTQ beneficiaries in policies authorizing covered services, and PACE organizations could refuse to serve someone based on their sexual orientation, for example.27
Abortion and religious exemptions
The final Section 1557 rule allows health care providers and other covered entities to invoke blanket abortion and religious objection exemptions from the regulations’ general prohibition on sex discrimination.28 The regulation incorporates provisions from Title IX that exempt covered entities from complying with the general prohibition against sex discrimination if doing so (1) involves providing or paying for abortion29 or (2) would be inconsistent with the organization’s religious tenants.30 The regulation also exempts entities from having to comply with the Section 1557 regulations if doing so would violate a specific list of existing, as well as any future, federal abortion and religious exemption laws.31 Additionally, as noted above, HHS eliminates the 2016 regulatory definition of sex-based discrimination, which had included discrimination on the basis of pregnancy, false pregnancy, termination of pregnancy, or recovery therefrom, and childbirth or related medical conditions.32 Commenters noted that the regulation might open the door to discrimination based on abortion history.33 “Commenters also identified a variety of other women’s healthcare services related to pregnancy that may be implicated, including prenatal and postpartum services, tubal ligations, and birth control (both as a contraceptive and when used to treat other medical conditions). . . [and] infertility treatments including in vitro fertilization ….”34 In its response, HHS ”decline[d] to speculate on particular hypotheticals related to the termination of pregnancy and will proceed on the specific facts and circumstances of each case that may arise.”35
This change means that people seeking abortion or other health care services that violate a provider’s religious beliefs may be denied, delayed, or discouraged from seeking necessary care, placing them at risk of serious or life-threatening results in emergencies and other circumstances where the individual’s choice of health care provider is limited.36 The Obama Administration regulation provided that covered entities did not have to comply with Section 1557’s prohibition of discrimination on the basis of sex if doing so would have violated existing federal abortion and religious exemption laws, but it did not include a blanket religious exemption.37 When the Obama Administration issued Section 1557 regulations in 2016, HHS rejected incorporating Title IX’s blanket religious exemption because Title IX is limited to educational institutions, which it concluded are significantly different from the health care context.38 While students and parents typically have a choice about whether to select a religiously affiliated educational institution, individuals’ choice of health care provider may be limited, especially in rural areas, locations where hospitals are run by religious institutions, or emergencies.39 In 2016, HHS explained that it instead would rely on the Religious Freedom Restoration Act to make individual case-by-base determinations about “whether a particular application of Section 1557 substantially burdened a covered entity’s exercise of religion, and if so, whether there were less restrictive alternatives available.”40 This meant that, under the Obama Administration regulation, there may have been some instances in which a provider’s religious beliefs would have exempted it from providing services, but other instances, based on the facts of a particular case, in which an individual was entitled to receive services despite a provider’s religious objection. As noted above, the DC federal district court issued a nationwide preliminary injunction blocking the implementation of the Trump Administration provisions incorporating a blanket religious freedom exemption from claims of sex discrimination.
Non-Discrimination in Health Coverage
In addition to the specific gender identity provisions discussed above, HHS also eliminates the entire regulation prohibiting discrimination in health insurance issuance, coverage, cost-sharing, marketing, and benefit design. Under the 2016 regulations, covered entities were prohibited from taking the following actions on the basis of race, color, national origin, sex, age, or disability:
Denying, canceling, limiting, or refusing to issue or renew a health insurance policy;
Denying or limiting coverage of a health insurance claim;
Imposing additional cost sharing or other limitations or restrictions on coverage; or
Using discriminatory marketing practices or insurance benefit designs.
Without these provisions, health plans could, for example, cover inpatient treatment for eating disorders for men but not women or cover bariatric surgery for adults except those with certain developmental disabilities.41 Other benefit designs that might be discriminatory include placing all or most prescription drugs used to treat a specific condition on a health plan’s highest cost formulary tier, applying age limits to services that have been found to be clinically effective at all ages, or requiring prior authorization or step therapy for all or most medications in drug classes such as protease inhibitors for HIV or immune suppressants regardless of medical evidence.42 Other ACA provisions regarding guaranteed issue continue to apply.
Language Access
In the final rule, HHS reduces the standards governing access to language assistance services, including oral interpretation and written translation, for individuals with limited English proficiency (LEP). Specifically, HHS replaces the requirement in the 2016 regulation for covered entities to take reasonable steps to provide meaningful access to “each individual with LEP eligible to be served or likely to be encountered”43 with a requirement to provide meaningful access to ”limited English proficient individuals” generally. Language access protections are required to prevent discrimination based on national origin. HHS notes that commenters expressed concerns that this change would weaken nondiscrimination requirements and result in some LEP individuals being unable to access health care; many commenters further indicated that lack of understanding in a medical setting could cause harm and possibly death to patients with LEP.44 In response, HHS indicated that the 2016 standard was a stringent requirement that could be interpreted to require an entity to provide language assistance services to every LEP individual with which it comes in contact. It says that by adopting this revised language, it is applying the same standard to both health and human service programs within the department and that it conforms to existing LEP guidance.45
HHS also replaces the test to determine when covered entities must provide language access services with one that removes the emphasis on the importance of the communication to the specific individual. Under the 2016 regulation, the test to determine whether an entity is in compliance with requirements to provide meaningful access to LEP individuals gave “substantial weight” to the nature and importance of the health program or activity and the communication at issue to the specific individual. Under the final rule, HHS applies a different test that balances a variety of factors to determine when language assistance services are required, including the overall number of LEP individuals eligible to be served or likely to be encountered, the frequency with which any LEP individuals come into contact with the covered program or activity, and the costs involved. HHS also eliminates the provision that allows HHS to consider whether the covered entity has an effective written language access plan when assessing compliance with requirements to provide meaningful access. In addition, HHS eliminates remote video interpreting standards and instead includes standards only for remote audio interpreting services. Some commenters expressed concerns that the revised test to assess compliance with providing meaningful access to LEP individuals places too much of an emphasis on costs and is too broad, lacks clarity, and does not ensure that translation and other language services are available under important medical circumstances, In response, HHS notes that the revised test is consistent with existing LEP guidance and intended to strike a balance between ensuring access by LEP individuals while not imposing undue burdens on small businesses, small local governments, or small nonprofits.46
HHS eliminates requirements that non-discrimination notices (discussed further below) must include the availability of language assistance services and taglines in the top 15 languages spoken by LEP individuals in the state. Some commenters stated that the removal of the notice and tagline provisions will result in LEP individuals having less knowledge of available language assistance and will be more likely to rely on informal sources of assistance through family members.47 HHS responded that the rule maintains the requirement that covered entities provide a notice of discrimination and taglines whenever necessary to ensure meaningful access, and that it is only removing the requirement that all significant communications contain taglines. It also says that this requirement caused significant unanticipated expenses and indicates it has determined that the financial burden on covered entities was not justified by the protections or benefits it provided to LEP individuals.48
Notice and Enforcement
The final rule eliminates all of the previous Section 1557 nondiscrimination notice and grievance procedure requirements. Covered entities with at least 15 employees no longer must adopt a grievance procedure or designate at least one employee to coordinate its Section 1557 responsibilities. Covered entities also no longer must provide notice of their nondiscrimination policies in significant communications (such as handbooks and outreach publications), physical locations where the entity interacts with the public, and on their website homepage. HHS notes that the regulations implementing Title VI, Title IX, the Age Act and Section 504 “already contain notice provisions” and concluded that creating a single notice standard in the Section 1557 regulation “has led to an unjustifiable burden and understandable confusion.”49
HHS projects that all of its proposed Section 1557 changes will result in approximately $2.9 billion in undiscounted cost savings over the first five years after implementation, primarily from eliminating the notice and tagline requirements.50 HHS says that its original cost projections for the notice and tagline requirements did not account for approximately $585 million in additional average annual costs over the next five years.51
Although HHS eliminated provisions that recognize the right of private individuals and entities to file lawsuits in federal court to challenge alleged violations of Section 1557, HHS states that it no longer intends to take a position about whether the statute in fact provides such a right. Instead, HHS says that “[t]o the extent that Section 1557 permits private rights of action, plaintiffs can assert claims under Section 1557 itself rather than under the Department’s Section 1557 regulation.”52 This leaves the right to sue under Section 1557 for courts to decide. For example, in the cases cited above, individuals filed lawsuits in federal court alleging that the Wisconsin Medicaid program’s categorical exclusion of gender affirming services from coverage and California hospital staff’s repeated mis-gendering of a transgender boy who was admitted for inpatient psychiatric care and subsequently committed suicide were unlawful discrimination, relying on the statute as enacted by Congress. HHS also eliminated the regulation that provides that money damages are available to compensate those injured by violations of Section 1557. Instead, HHS will rely on the enforcement provisions of the underlying civil rights statutes, Title VI, Title IX, the Age Act, or Section 504, when determining when money damages are available for a violation of Section 1557.53
Scope of Applicability
Covered Entities Receiving Federal Financial Assistance
The final rule narrows the scope of the regulations to cover only the specific programs and activities that receive federal funding, and not all operations, of health insurers that are not principally engaged in the business of providing health care. The prior rule applied Section 1557’s non-discrimination protections broadly to health programs and activities, defining them to include all operations of an entity receiving federal financial assistance that is principally engaged in the provision or administration of health-related services or health-related insurance coverage. For example, all health plans offered by an issuer that participated in a Marketplace were subject to Section 1557.54 Under the final rule, if this issuer is not principally engaged in the business of providing health care (as opposed to health insurance), only its Marketplace plans are covered and any plans it offers outside the Marketplace are not subject to Section 1557. The change also means that the regulations do not apply to short term limited duration insurance, employer-sponsored group health plans, self-insured church plans, the Federal Employees Health Benefits Program, or non-Federal governmental plans, so long as coverage is offered by an entity that is not principally engaged in the business of providing healthcare and does not receive Federal financial assistance.55 In support of this change, HHS states that the “‘business of providing . . . health care’ differs substantially from the business of providing health insurance coverage (or other health coverage) for such health care.”56 The end result is to reduce the number and type of entities required to comply with Section 1557’s non-discrimination protections. The final rule continues to apply to health care providers, such as physicians’ practices, hospitals, nursing homes, and organ procurement centers that receive federal funds such as Medicare (excluding Part B57 ) or Medicaid payments; health-related education and research programs; state Medicaid, CHIP, and public health agencies; and state-based Marketplaces.58
HHS programs and activities
HHS also applies the regulations only to health programs and activities that it administers under ACA Title I (Marketplaces), instead of all HHS-administered programs and activities. Health programs and activities conducted by HHS outside ACA Title I include other CMS programs and activities, the Health Services Research Administration (such as clinics operated by the National Health Service Corps), the Centers for Disease Control, the Indian Health Services (including IHS tribal hospitals), and the Substance Abuse and Mental Health Services Administration.59 Under the prior regulation, these programs were subject to the Section 1557 regulations.
discrimination based on association
The final rule eliminates the prohibition against discrimination based on an individual’s association or relationship with someone else based on that other person’s race, color, national origin, sex, age, or disability. These grounds for discrimination were recognized by the former Section 1557 regulations. Examples of discrimination based on association that were recognized by the prior regulations include a doctor refusing to see a white patient because the patient has a biracial child or a health plan issuer excluding a provider from its network because the provider’s patients are primarily LEP individuals.60 A hearing parent who is required by a hospital to interpret for her deaf child would no longer be able to pursue a discrimination claim based on association under the Section 1557 regulations.61
Disability Discrimination
Although HHS requested public comment on whether some of Section 1557’s disability discrimination provisions should be changed, it did not adopt many changes in this area. Specifically, HHS did not exempt entities with less than 15 employees from the requirement to provide auxiliary aids and services to ensure effective communication with people with disabilities nor did HHS create an undue hardship exemption from the provision requiring covered entities to make reasonable modifications in policies, practices, and procedures to avoid disability-based discrimination. Instead, HHS notes that the entities would not be required to comply with either of these provisions if they can demonstrate that doing so would result in a fundamental alternation of their services, programs, or activities or an undue financial or administrative burden, consistent with the ADA regulations.62 HHS also did not create additional exemptions for covered entities subject to the architectural standards applicable to public buildings, especially with regard to multi-story building elevator and TTY requirements, noting that the ”great majority” of entities already are subject to these standards.63 HHS did finalize a change to the definition of auxiliary aids and services by eliminating ”acquisition or modification of equipment and devices; and other similar services and actions” from the list of examples.64
The Supreme Court’s Bostock Decision and Legal Challenges to the Final Rule
Just after the Administration published its final rule in June 2020, the Supreme Court decided Bostock v. Clayton County, Georgia, a sex-based employment discrimination case with implications for Section 1557. In Bostock, the Court found that Title VII of the Civil Rights Act of 1964 protects employees against discrimination because of their sexual orientation or gender identity. In the preamble to the Section 1557 final rule, the Trump Administration acknowledged the Bostock decision, which was still pending at that time. Specifically, the Administration said that it “continues to expect that a holding by the U.S. Supreme Court on the meaning of ‘on the basis of sex’ under Title VII will likely have ramifications for the definition of ‘on the basis of sex’ under Title IX [as] Title VII case law has often informed Title IX case law.”65 However, HHS also noted that the “binary biological character of sex (which is ultimately grounded in genetics) takes on special importance in the health care context” and asserted that “[t]hose implications might not be fully addressed by future Title VII rulings even if courts were to deem the categories of sexual orientation or gender identity to be encompassed by the prohibition on sex discrimination in Title VII.”66 Rather than revisiting its revised Section 1557 rule in light of Bostock after the Court issued its decision, the Administration argued that Bostock’s “holding was limited to Title VII” and the case‘s “applicability to contexts outside of employment discrimination is a question for future courts to decide.”
Relying in part on Bostock, two federal district courts have issued nationwide preliminary injunctions preventing the Administration from implementing parts of the Section 1557 final rule. On August 17, 2020, the day before the final rule was to take effect, the Eastern District of New York blocked the Administration from implementing provisions excluding sex stereotyping from definition of sex discrimination in Walker v. Azar, a case brought by two transgender women of color. On September 2, 2020, the DC federal district court blocked the Administration from implementing provisions excluding sex stereotyping from the definition of sex discrimination as well as from incorporating a blanket religious exemption from sex discrimination claims in Whitman-Walker Clinic v. HHS, a case brought by health care and social service providers who serve LGBTQ people and LEP people. While the plaintiffs in both the NY and DC cases also sought to have gender identity restored to the Section 1557 rule’s definition of sex discrimination, both courts concluded that they lacked authority to do so because the Franciscan Alliance court previously vacated the inclusion of gender identity from the 2016 regulations.67 The preliminary injunctions issued by the NY and DC courts block implementation of the 2020 regulations, reverting back to the 2016 regulations, which as a result of Franciscan Alliance no longer include gender identity in the definition of sex discrimination. After the NY plaintiffs requested clarification about the scope of the preliminary injunction order, the court directed the plaintiffs to submit a list of provisions of the 2020 rule, beyond the definition of sex discrimination, that should be stayed in light of Bostock for the court’s consideration.
Given the Bostock decision, it is likely that further litigation will address whether gender identity should be restored to Section 1557’s definition of sex discrimination. As the DC court noted when issuing its preliminary injunction, the Supreme Court in Bostock “expressly assumed that ‘sex’ [in Title VII] ‘refer[red] only to biological distinctions between male and female.”68 Notably, the Supreme Court went on to conclude that “it is impossible to discriminate against a person for being homosexual or transgender without discriminating against that individual based on sex.”69 The DC acknowledged that other federal courts, both pre- and post-Bostock have concluded that sex discrimination under Title IX includes gender identity, and “Bostock, at the very least, has significant implications for the meaning of Title IX’s prohibition on sex discrimination.”70 Consequently, for purposes of deciding whether the Trump Administration’s changes to Section 1557’s regulatory definition of sex discrimination violated the Administrative Procedures Act, the DC court concluded that “it was arbitrary and capricious for HHS to eliminate the 2016 Rule’s explication of that prohibition without even acknowledging — let alone considering — the Supreme Court’s reasoning or holding” in Bostock.71
The remaining provisions of the Trump Administration’s final rule remain in effect. The DC court denied the Whitman-Walker plaintiffs’ request to apply the preliminary injunction to other parts of the final rule, including (1) the elimination of the prohibition on categorical coverage exclusions for gender-affirming care, (2) the elimination of notice and tagline requirements, (3) the restriction of the rule’s scope to apply only to HHS-administered programs and activities under ACA Title I, and not all HHS programs and activities, (4) the exclusion of certain activities of health insurance issuers not principally engaged in the business of providing health care from the final rule, and (5) provisions regarding the appropriate legal standard to be applied to Section 1557 claims.
Other cases challenging the Trump Administration’s Section 1557 final rule are pending. A transgender man and health and social service providers serving LGBTQ and LEP people filed a case in Massachusetts federal district court (Boston Alliance of Gay, Lesbian, Bisexual & Transgender Youth v. HHS), and a group of 23 states led by New York filed a case in the Southern District of New York (NY v. HHS). The plaintiffs in NY v. HHS have filed a motion for partial summary judgement, seeking to have the entire 2020 rule vacated. In another case brought by the state of Washington (WA v. HHS), the Western District of Washington denied a preliminary injunction, finding that the state did not have standing to bring a lawsuit challenging the final rule because it had not established that it was injured. Subsequently, the state voluntarily dismissed the case without prejudice. Table 3 summarizes the current litigation challenging the final rule.
Looking Ahead
The final rule, issued in the midst of the ongoing COVID-19 pandemic, substantially narrows, and in many cases entirely eliminates, the prior regulations’ existing nondiscrimination protections in meaningful ways. Section 1557 sought to standardize the protections and processes that prohibit discrimination in health care for all protected populations. Section 1557 also recognizes intersectional discrimination that affects people who belong to multiple protected classes; for example, discrimination against an African-American woman could be discrimination on the basis of both race and sex.72 While HHS maintains that it “is committed to ensuring the civil rights of all individuals who access or seek to access health programs or activities of covered entities,”73 the final rule substantially scales back non-discrimination protections.
The Supreme Court’s Bostock decision has significant implications for the final rule’s elimination of protections based on gender identity and sexual orientation, with two federal district courts blocking the Administration from implementing parts of the rule. Nationwide preliminary injunctions issued by federal district courts in NY and DC prevent the Administration from implementing provisions removing sex stereotyping from the rule’s definition of sex discrimination, and the NY court is now considering whether to expand its preliminary injunction to block additional provisions of the rule in light of Bostock. The DC court’s preliminary injunction also prevents the Administration from implementing the provision adopting a blanket religious exemption from sex discrimination claims. In another case, the state of NY is asking another NY federal district court to grant its motion for partial summary judgment, vacating the entire 2020 rule. The final outcome of these cases, other pending challenges to the Trump Administration’s final rule, and the pending Franciscan Alliance case challenging the 2016 rule will continue to shape the Section 1557 regulations.
Moreover, the final rule, while reshaping the regulatory protections, does not change the underlying statutory protections of Section 1557 as enacted by Congress. As noted above, some federal courts have recognized claims of discrimination and awarded relief under Section 1557 based on the statute itself and may continue to do so, regardless of regulatory changes. While the HHS Office for Civil Rights’ enforcement of Section 1557 is substantially narrowed under the rule, in terms of the scope of covered entities and the type of claims constituting prohibited discrimination, federal courts could continue to apply Section 1557’s statutory protections more broadly and provide relief to individuals experiencing discrimination in the health care context. Finally, regardless of the outcome of these challenges, the final rule does not prohibit states from outlawing health care discrimination on the basis of gender identity, sexual orientation, or other grounds beyond those recognized under federal law,74 as several states already have done.75
This work was supported in part by the Elton John AIDS Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Defines sex discrimination to include discrimination on the basis of gender identity, sex stereotyping, pregnancy, false pregnancy, termination of pregnancy, or recovery therefrom, childbirth or related medical conditions.
Provides that compliance with § 1557’s prohibition of discrimination based on sex is not required if doing so would violate existing abortion and religious exemption laws. Does not include Title IX’s blanket abortion and religious exemptions applied to educational institutions.
Adds Title IX’s blanket abortion and religious exemptions and provide that any § 1557 regulatory requirement will not be imposed if it would violate, depart from, or contradict definitions, exemptions, affirmative rights, or protections provided by existing and future abortion and religious exemption laws.78
Discrimination in Health Coverage
Nondiscrimination in health-related insurance and other health-related coverage79
Prohibits covered entities from taking the following actions on the basis of race, color, national origin, sex, age, or disability:
Denying, canceling, limiting, or refusing to issue or renew a health insurance policy
Denying or limiting coverage of a health insurance claim
Imposing additional cost sharing or other limitations or restrictions on coverage
Using discriminatory marketing practices or insurance benefit designs
Permits insurers to apply medical necessity rules when determining covered benefits.
Removes entire provision.
Coverage protections for transgender individuals80
Requires that covered entities treat individuals consistent with their gender identity, except that entities are prohibited from denying or limiting health services that are ordinarily or exclusively available to individuals of one sex or gender based on the fact that the individual’s sex assigned at birth, gender identity, or gender in a medical or health insurance plan record differs from the one to which such health services are ordinarily or exclusively available.
Prohibits an insurance plan from categorically or automatically excluding or limiting coverage for all health services related to gender transition or otherwise denying or limiting coverage or denying a claim for specific health services related to gender transition if such a policy results in discrimination against the individual seeking services.
Removes entire provision.
Language Access
Meaningful access for individuals with limited English proficiency (LEP)82
Requires covered entities to take reasonable steps to provide meaningful access to each individual with LEP eligible to be served or likely to be encountered.
When assessing an entity’s compliance, OCR will take into account and give substantial weight to the nature and importance of the health program or activity and the communication at issue to the individual with LEP. OCR also will consider other relevant factors, including whether the entity has an effective written language access plan.
Requires covered entities to offer a qualified interpreter when oral interpretation is a reasonable step to provide meaningful access and to use a qualified translator when translating written content.
Requires covered entities to take reasonable steps to ensure meaningful access by LEP individuals (remove reference to each individual).
When evaluating an entity’s compliance, OCR may assess how the entity balances the number or proportion of LEP individuals eligible to be served or likely to be encountered; the frequency with which LEP individuals come in contact with the entity’s health program or activity; the nature and importance of the entity’s health program or activity; and the resources available to the entity and costs.
The entity’s individualized assessment of the above factors will determine whether language assistance services are required to provide meaningful access.
Remote interpreting services
Includes standards for video remote interpreting services.
Removes video remote interpreting standards and require only audio remote interpreting.
Requires covered entities to provide non-discrimination notices (described below) in English and include taglines in the top 15 languages spoken by individuals with LEP in the state. Notices must indicate the availability of language assistance services.
Effective communication – auxiliary aids and services85
Requires covered entities to provide appropriate auxiliary aids and services to people with impaired sensory, manual, or speaking skills, where necessary to afford an equal opportunity to benefit from the health program or activity.
Omits “acquisition or modification of equipment and devices; and other similar services and actions” from the list of examples. Does not exempt entities with less than 15 employees but notes that ADA fundamental alternative and undue burden defenses continue to apply.
Building construction and architectural standards86
Adopts the 2010 ADA Standards for Accessible Design for new construction or alternation of facilities of covered entities that receive federal funding and state-based Marketplaces.
No change. Does not adopt additional exemptions regarding multi-story building elevators and TTY standards.
Requires covered entities to make reasonable modifications in policies, practices, and procedures to avoid disability-based discrimination, unless doing so would fundamentally alter the nature of the health program or activity.
No change. Does not adopt undue hardship exemption but notes that ADA fundamental alternation and undue burden defenses continue to apply.
Notice and Enforcement
Designation of responsible employee and adoption of grievance procedures88
Requires covered entities that employ at least 15 people to adopt a grievance procedure and designate at least one employee to coordinate § 1557 responsibilities.
Required covered entities to provide notice of their nondiscrimination policies in significant communications (such as handbooks and outreach publications), physical locations where the entity interacts with the public, and on their website homepage.
The notice had to include the bases of discrimination prohibited under § 1557, the availability of free auxiliary aids and services and language assistance services, how to access those services, contact information for the employee responsible for § 1557 compliance, the entity’s grievance procedures, and OCR complaint procedures.
Included sample notice, tagline, and grievance procedure.
Small-sized publications could have included a shorter non-discrimination statement and taglines in the top 2 non-English languages spoken.
Provided that compensatory damages are available for violations of § 1557 in appropriate administrative and judicial actions brought under the regulations.
Removes entire provision. Instead, relies on enforcement provisions of Title VI, Title IX, Age Act, and Section 504.
Provided that private individuals and entities can sue in federal court to challenge alleged violations of § 1557 by entities receiving federal financial assistance and state-based Marketplaces
Removes entire provision. HHS no longer takes a position on whether Section 1557 itself provides a private right of action.
Applies § 1557 regulations to health programs and activities that receive federal financial assistance from HHS, all health programs and activities administered by HHS, and state-based Marketplaces.
Defines health programs and activities to include all operations of an entity that is principally engaged in the provision or administration of health-related services or health-related insurance coverage.
Applies § 1557 regulations to entities principally engaged in the business of providing health care that receive federal financial assistance, health programs and activities administered by HHS under Title I of the ACA (but not other HHS-administered health programs and activities), and state-based Marketplaces.
Applies § 1557 regulations to health insurance programs administered by entities that are not principally engaged in the business of providing health care only to the extent that those programs receive federal financial assistance. Would not apply to all operations of entities that are not principally engaged in the business of providing health care (as opposed to health insurance).
Prohibits discrimination against an individual known or believed to have a relationship or association with someone else based on that person’s race, color, national origin, age, disability, or sex.
Removes entire provision.
Table 2: Key Changes to Other HHS Anti-Discrimination Regulations
Prohibits Medicaid managed care entities from discriminating against individuals eligible to enroll or using any policy or practice that has the effect of discriminating on the basis of sexual orientation or gender identity.
Removes sexual orientation and gender identity as prohibited bases of discrimination.
Requires state Medicaid programs to ensure that each Medicaid managed care entity participates in state efforts to promote service delivery in a culturally competent manner to all enrollees, regardless of gender, sexual orientation or gender identity.
Replaces gender, sexual orientation or gender identity with sex.
Access and cultural conditions for state Medicaid program services97
Requires state Medicaid programs to have methods to promote access and service delivery in a culturally competent manner to all beneficiaries, regardless of gender, sexual orientation or gender identity.
Replaces gender, sexual orientation or gender identity with sex.
Program of All-Inclusive Care for the Elderly (PACE)98
Prohibits PACE organizations from discriminating against any participant in the delivery of PACE services based on sexual orientation.
Provides that each PACE participant has the right to not be discriminated against in the delivery of required PACE services based on sexual orientation.
Removes sexual orientation as prohibited basis of discrimination.
Group and Individual Health Insurance
Group and individual health insurance markets – guaranteed availability of coverage99
Prohibits health insurance issuers from employing marketing practices or benefit designs that discriminate based on gender identity and sexual orientation.
Removes sexual orientation and gender identity as prohibited bases of discrimination.
Prohibits states and Marketplaces from discriminating based on gender identity and sexual orientation when establishing Marketplace standards and functions, eligibility determinations, enrollment periods, SHOP functions, QHP certification, and health plan quality improvement.
Removes sexual orientation and gender identity as prohibited bases of discrimination.
Federally-facilitated Marketplace standards of conduct101
Prohibits agents and brokers that assist with or facilitate enrollment of individuals or applying for premium tax credits and cost sharing reductions in qualified health plans (QHPs) through a federally-facilitated Marketplace from discriminating based on gender identity and sexual orientation.
Removes sexual orientation and gender identity as prohibited bases of discrimination.
Prohibits QHP issuers from discriminating based on gender identity and sexual orientation.
Removes sexual orientation and gender identity as prohibited bases of discrimination.
Direct enrollment in a Federally-facilitated Marketplace103
Prohibits QHP issuers from marketing or conduct that discriminates based on gender identity and sexual orientation.
Removes sexual orientation and gender identity as prohibited bases of discrimination.
Sex Discrimination
Education programs or activities receiving federal financial assistance104
Not addressed in regulation. Contained in statute.
Adds provision prohibiting covered entities from being required to perform or pay for an abortion.105
Education programs or activities receiving federal financial assistance106
Prohibits recipients of federal financial assistance from discriminating against any person in the application of any rules of appearance on the basis of sex when providing any aid, benefit or service to a student.
Removes provision prohibiting discrimination based on the application of rules of appearance.
Table 3: Lawsuits Challenging the Trump Administration’s Section 1557 Final Rule, as of 9/14/20
Health care and social service providers who serve LGBTQ people and LEP people
9/2/20 court issued nationwide preliminary injunction preventing Administration from implementing (1) provisions excluding sex stereotyping from definition of sex discrimination and (2) provisions incorporating blanket religious freedom exemption from claims of sex discrimination.
The court denied plaintiffs’ motion for a preliminary injunction to block the final rule’s (1) elimination of the provision prohibiting categorical coverage exclusions for gender-affirming care, (2) elimination of notice and tagline requirements, (3) restriction of the rule’s scope to apply only to HHS-administered programs and activities under ACA Title I, and not all HHS programs and activities, (4) exclusion from the rule of certain activities of health insurance issuers not principally engaged in the business of providing health care, and (5) provisions amending the appropriate legal standard to be applied to Section 1557 claims.
After the plaintiffs requested clarification about the scope of the preliminary injunction order, the court issued a 9/8/20 order directing plaintiffs to submit a list of provisions of the 2020 rule, beyond the definition of sex discrimination, that should be stayed in light of the Supreme Court’s Bostock decision by 9/15/20, and HHS to respond by 9/22/20.
Table 4: Section 1557 and Sex Discrimination Timeline
Date
Event
Impact
March 23, 2010
ACA signed
Provides new coverage options and protections for people in the United States, including Sec. 1557 nondiscrimination protections which incorporate sex nondiscrimination protections from Title IX of the Civil Rights Act.
May 18, 2016
Final 2016 Obama Administration regulations implementing Section 1557 issued.
The 2016 implementing regulations specifically included “gender identity” and “sex-stereotyping” in its definition of “sex”, extending the ACA’s sex non-discrimination protections to transgender and gender nonconforming people.
August 23, 2016
Franciscan Alliance v. Azar filed in federal district court in Texas (Judge Reed O’Connor) challenging parts of the final regulation.
Plaintiffs, including multiple states and religious health care entities, challenge the Obama Administration’s final rule defining discrimination “on the basis of sex” to include discrimination based on “gender identity” and “termination of pregnancy.”
December 31, 2016
Texas federal district court issues preliminary injunction blocking enforcement of parts of the 1557 regulation.
Texas federal district court issued a nationwide injunction enjoining HHS from enforcing the parts of the 2016 nondiscrimination regulation pertaining to discrimination on the basis of gender identity or termination of pregnancy. (The statute, Sec. 1557, stands and injured parties can still file suit in court)
July 10, 2017
Texas federal district court grants request to remand rule back to HHS for reconsideration and stays litigation.
Following President Trump’s election and at the request of DOJ, Texas federal district court remands the rule back to HHS for reconsideration and to comply with the court’s earlier ruling. The suit is stayed while rule is remanded to the agency and preliminary injunction remains in place.
December 17, 2018
Texas federal district court allows Franciscan Alliance litigation to resume per plaintiff’s requests.
Court orders litigation to move forward, despite that Trump Administration has not yet issued proposed regulations
May 24, 2019
Trump Administration releases proposed rules relating to Section 1557 implementation.
Proposed rules would revise the Obama Administration’s regulations implementing Section 1557 including the definition of sex and in particular the inclusion of gender identity, sex-stereotyping, and termination of pregnancy. The rule proposes to remove explicit protections based on sexual orientation and gender identity in regulations outside of Section 1557. In addition, rule proposes to allow providers and other covered entities to invoke blanket abortion and religious objection exemptions from the regulations’ general prohibition on sex discrimination.
October 15, 2019
Texas federal district court vacates the parts of the 2016 rule prohibiting discrimination based on gender identity and termination of pregnancy, citing violations of the Administrative Procedure Act (APA) and the Religious Freedom Restoration Act (RFRA).
The order sets aside these sex-based protections in the 2016 rule. Injured parties are still able to address claims of discrimination based on gender identity and termination of pregnancy through litigation, relying on the statue itself.
January 21, 2020
Plaintiffs appeal the Texas federal district court decision to 5th Circuit.
Despite succeeding in having gender identity and termination of pregnancy provisions of the 2016 rule vacated, plaintiffs appealed the lower court’s decision, seeking to have the entire Obama Administration rule vacated.
June 2, 2020
5th Circuit grants appellants a stay in the Franciscan Alliance case.
Appellants requested and were granted a stay in proceedings until 21 days after the Supreme Court issues its decision in Bostock v. Clayton County, GA which could impact their case.
June 12, 2020
Trump Administration releases final rules relating to Section 1557 implementation.
Final Section 1557 implementing rules are essentially unchanged from the proposed rules as described above.
June 15, 2020
The Supreme Court issues a decision in Bostock v. Clayton County, GA finding that sex nondiscrimination protections under Title VII of the Civil Rights Act extend to gender identity and sexual orientation in the employment context.
Because Section 1557 incorporates sex discrimination protections under Title IX of the Civil Rights Act, and courts traditionally look to Title VII when interpreting Title IX, the Bostock decision raises questions about the validity and survivability of the Trump Administration’s Section 1557 rules.
June 22, 2020 – July, 20, 2020
5 lawsuits filed challenging the Trump Administration final rule:
Whitman-Walker Clinic v. HHS, No. 1:20-cv-1630 (E.D.NY)
Boston Alliance of Gay, Lesbian, Bisexual & Transgender Youth v. HHS, No. 1:20-cv-11297 (D. Mass.)
Walker v. Azar, No. 1:20-cv-2834 (D.D.C.)
NY v. HHS, No. 1:20-cv-5583 (S.D.NY)
Washington v. HHS, No. 2:20-cv-01105-JLR (W.D.Wa.)
The suits challenge the final rule on a number of grounds, including that it is contrary to the Bostock ruling.
August 17, 2020
In Walker v. Azar, citing the Bostock decision, the federal court for the Eastern District of New York, issues a preliminary injunction setting aside the changes the Trump Administration final rule made to the 2016 Obama Administration rule on the definition of “sex” and in particular protections based on “gender identity” and “sex stereotyping.”
The ruling reinstates the 2016 rule’s definition of sex but cannot undo the vacatur of the “gender identity” provisions in the Franciscan Alliance case. Therefore the ruling largely revives the 2016 rule’s sex nondiscrimination protections as they apply to “sex-stereotyping” which the court suggests, in the order, can offer gender identity protections as transgender people are “inherently gender non-conforming.”
August 11, 2020
Fifth Circuit resumes proceedings in the Franciscan Alliance appeal following the ruling in Bostock.
Given that the appellants were waiting for a Bostock decision to resume litigation, watching how litigation in this case plays out will provide critical insight into how lower courts apply the Supreme Court’s Title VII ruling to Title IX.
September 3, 2020
In Whitman-Walker Clinic v. HHS, the D.C. District Court issued a preliminary injunction
As was the case in Walker, the injunction enjoins HHS from repealing the 2016 rule’s definition of sex discrimination insofar as it includes sex stereotyping. It also enjoins HHS from enforcing its incorporation of the religious exemption contained in Title IX, including as they relate to termination of pregnancy or treatment of a transgender or gender nonconforming person.
September 8, 2020
After the plaintiffs requested clarification about the scope of the preliminary injunction order, the Walker v. Azar court directed the plaintiffs to submit a list of provisions of the 2020 rule, beyond the definition of sex discrimination, that should be stayed in light of the Supreme Court’s Bostock decision for the court’s consideration. Plaintiffs’ list is due on September 15th, and HHS’s response is due on September 22nd.
The NY court’s preliminary injunction could be expanded to encompass additional provisions of the final 2020 rule.
After HHS, under the Trump Administration, agreed with the plaintiffs that the challenged 2016 regulation was unlawful, the court allowed River City Gender Alliance and the American Civil Liberties Union of Texas to intervene in the case, concluding that HHS would not adequately represent the interests of transgender people, people who have terminated pregnancies, and people who seek reproductive healthcare. ↩︎
“Insofar as the application of any requirement under this part would violate, depart from, or contradict definitions, exemptions, affirmative rights, or protections provided by any of the statutes cited in paragraph (a) of this section [including Title IX]. . . such application shall not be required or imposed.” 45 C.F.R. § 92.6 (b). ↩︎
The Title IX abortion exemption provides that “[n]othing in this title shall be construed to require or prohibit any person, or public or private entity, to provide or pay for any benefit or service, including the use of facilities related to an abortion. . . .” 20 U.S.C. § 1688. ↩︎
The Title IX religious exemption provides that the prohibition of discrimination on the basis of sex “shall not apply to an educational institution which is controlled by a religious organization if the application of this subsection would not be consistent with the religious tenants of such organization.” 20 U.S.C. § 1681 (a)(3). ↩︎
HHS specifically references the Coats-Snowe Amendment, the Church Amendments, the Religious Freedom Restoration Act, ACA § 1553, ACA § 1303, the Weldon Amendment, and any related, successor, or similar federal laws or regulations. 45 C.F.R. § 92.6 (b). ↩︎
Cf. prior 45 C.F.R. § 92.2 (b)(2) (providing that “[i]nsofar as the application of any requirement under this part would violate applicable Federal statutory protections for religious freedom and conscience, such application shall not be required”). ↩︎
85 Fed. Reg. at 37166 (“This final rule. . . does not deny States the ability to provide protections that exceed those required by Federal civil rights laws.“). ↩︎
Former 45 C.F.R. u00a7 92.2 (b); New 45 C.F.R. u00a7 92.6. ↩︎
HHS specifically references the Coats-Snowe Amendment, the Church Amendments, the Religious Freedom Restoration Act, ACA u00a7 1553, ACA u00a7 1303, the Weldon Amendment, and any related, successor, or similar federal laws or regulations. u00a7 92.6 (b). ↩︎
HHS assumes that tagline requirements for Marketplaces, 45 C.F.R. u00a7 155.205 (c)(2)(iii)(A), and Qualified Health Plan Issuers, HHS Notice of Benefits and Payment Parameters for 2016; Final Rule, 80 Fed. Reg. 10750, 10788 (Feb. 27, 2015), also would be u201cfully repealed because they depend on, or refer to, the Final [1557] Rule for authority for the tagline requirementu201d but that other CMS tagline requirements for group health plans and health insurance issuers, navigators, non-navigator assistance personnel, Medicaid, Medicaid managed care, CHIP, CHIP managed care, hospitals qualifying for tax-exempt status, and Medicare Advantage (Part C) and Prescription Drug (Part D) plans would remain in effect. 84 Fed. Reg. at 27881. ↩︎
Former 45 C.F.R. u00a7 92.202 (b). New u00a7 92.102. ↩︎
Former 45 C.F.R. u00a7 92.203 (a). New u00a7 92.103. ↩︎
Former 45 C.F.R. u00a7 92.205. New u00a7 92.105. ↩︎
Former 45 C.F.R. u00a7 92.7. New 45 C.F.R u00a7 92.5. ↩︎
HHS assumes that tagline requirements for Marketplaces, 45 C.F.R. u00a7 155.205 (c)(2)(iii)(A), and Qualified Health Plan Issuers, HHS Notice of Benefits and Payment Parameters for 2016; Final Rule, 80 Fed. Reg. 10750, 10788 (Feb. 27, 2015), also will be u201cfully repealed because they depend on, or refer to, the 2016 [1557] Rule for authority for the taglines requirement.u201d Although these regulations have not yet been amended, HHS clarifies that covered entities do not need to independently comply with them. Instead, compliance with those other regulations is deemed if entities comply with the revised Section 1557 regulation. However, other CMS tagline requirements for group health plans and health insurance issuers, navigators, non-navigator assistance personnel, Medicaid, Medicaid managed care, CHIP, CHIP managed care, hospitals qualifying for tax-exempt status, and Medicare Advantage (Part C) and Prescription Drug (Part D) plans remain in effect. 85 Fed. Reg. at 37230-37231. ↩︎
HHS specifically references the First Amendment, Title IXu2019s religious exemptions, the Religious Freedom Restoration Act, the Coats-Snowe Amendment, ACA u00a7 1303, and appropriations riders related to abortion such as the Hyde Amendment, the Helms Amendment, and the Weldon Amendment. 45 C.F.R. u00a7 86.18 (c). ↩︎
The usually highly anticipated release of the Census Bureau’s annual health insurance estimates, which occurred this past Tuesday for 2019 data, felt a bit different this year. While researchers and policymakers are accustomed to dealing with somewhat outdated data from federal surveys, the unprecedented social and economic changes that have occurred since the data were collected amplified the time lag and made the estimates seem even older than in past years. Current data on insurance coverage in the US is needed to design an adequate response to the pandemic and economic crisis, but the 2019 estimates still provide a useful baseline for interpreting what’s happening during the pandemic.
Prior to the pandemic, the uninsured rate had been increasing incrementally for several years despite an improving economy. After historic declines in the number of uninsured people and the uninsured rate following the adoption and implementation of the 2010 Affordable Care Act (ACA), resulting in nearly 20 million more people covered through 2016, the number and rate of nonelderly uninsured people began to increase in 2017. The uninsured count grew from 26.7 million (10.0%) in 2016 to 27.6 million (10.2%) in 2017, 28.2 million (10.4%) in 2018, and, as was announced this week, 29.2 million (10.8%) in 2019 (Figure 1).
Figure 1: Number of Uninsured and Uninsured Rate among the Nonelderly Population, 2010-2019
The 2.3 million person growth in the number of uninsured occurred despite improvements in several household economic measures, including median household income, earnings, and poverty and despite small gains in employer-based coverage over this period, which were offset by declines in Medicaid and direct purchase coverage. This pattern likely reflects a combination of factors, including rollback of outreach and enrollment efforts for ACA coverage, changes to Medicaid renewal processes, public charge policies, and elimination of the individual mandate penalty for health coverage. Notably, recent declines in coverage have occurred among both adults and children.
Because most people in the US still get their health coverage as a fringe benefit of a job, the recent economic downturn may disrupt coverage for millions of people. The economic fallout of the coronavirus pandemic has led to historic levels of job loss, with over 50 million people filing for unemployment insurance benefits since March 21st. Prior to the pandemic, nearly six in ten nonelderly people in the US received their health coverage through their job or a family member’s job. Early KFF estimates of the implications of job loss found that nearly 27 million people were at risk of losing employer-sponsored health coverage due to job loss. Other modeled estimates similarly predict millions losing employer health coverage, though the scale varies somewhat. Many of these people may have retained their coverage, at least in the short term, under furlough agreements or employers continuing benefits after layoffs. Indeed, recent KFF analysis of enrollment in the fully-insured group market found that enrollment in that market declined by just 1.3% from March to June 2020. Employer-based insurance losses could mount if unemployment remains high.
The availability of health coverage through the Affordable Care Act during this economic downturn means people losing their coverage have other options, but policy actions to scale back the ACA may mean people are unaware of or have difficulty accessing that coverage. Expanded coverage through Medicaid in the 37 states that have implemented the Medicaid expansion along with the availability of subsidized and unsubsidized coverage through the Marketplaces will enable many people losing their job-based insurance to retain health coverage. Following enrollment declines in 2018 and 2019, recent data indicate Medicaid enrollment increased by 2.3 million or 3.2% from February 2020 to May 2020. Additionally, as of May 2020, enrollment data reveal nearly 500,000 people had gained Marketplace coverage through a special enrollment period (SEP), in most cases due to the loss of job-based coverage. The number of people gaining Marketplace coverage through a SEP in April 2020 was up 139% compared to April 2019 and up 43% in May 2020 compared to May 2019. While millions of people are gaining coverage through Medicaid and the Marketplaces, reductions in outreach and enrollment assistance have reduced the availability of on-the-ground assistance for consumers who have lost coverage meaning many others may not be enrolling because they are not aware this coverage is available or don’t know how to enroll.
The pandemic has disrupted not only people’s health coverage but also the ability of federal surveys to measure coverage. Understanding real-time changes in insurance coverage is a key input into policy actions to address the implications of the pandemic on people’s health and well-being. However, to date, limited data is available on this topic. Large national surveys—those typically used as the basis for such information—are lagged, with the most recent data reflecting the first quarter of 2020, just prior to the pandemic. Many real-time surveys have faced challenges of high rates of survey nonresponse (not responding to the survey at all) particularly among populations most likely affected by the economic downturn, or unusually high rates of item nonresponse (skipping particular survey questions). In the Census Bureau’s Household Pulse Survey, designed to provide quick turnaround data on issues related to the pandemic, most weeks had a larger number of responses of “don’t know” or “did not report” to the question about health coverage than the number of uninsured. These measurement challenges may reflect people’s confusion about their current coverage amidst layoffs and job uncertainty or operational challenges in administering surveys that ask about health coverage (e.g., inability to conduct in person surveys).
While current survey data is limited and administrative and claims data are showing only moderate shifts in coverage, it is likely that large shifts in health coverage in the US are underway or imminent given loss of employment in recent months. It is possible that many of the people in families experiencing job loss were already uninsured, but given that prior to the pandemic the uninsured population in a family with a full-time worker totaled 20.2 million, there are still people among the 50 million who filed for unemployment benefits that may lose their employer coverage if they do not regain their jobs. In the midst of a health and economic crisis, the gap in real-time data to assess changes in health coverage poses a challenge.
Democratic Nominee Biden Holds Slight Lead Over President Trump in Arizona, while the Candidates are Virtually Tied in Florida and North Carolina, KFF/Cook Polls Find
Sun Belt Swing Voters Prefer Biden’s Leadership Style, But Half View Trump as a Strong Leader In Arizona, Democrat Kelly Leads Sen. McSally; in N.C, Gov. Cooper Leads Republican Forest, while Sen. Tillis and Democrat Cunningham are Running Neck and Neck
Democratic presidential nominee Joe Biden holds a slight lead over President Trump in Arizona (45% to 40%), while the two candidates are within the margin of sampling error in Florida (Biden 43%, Trump 42%) and North Carolina (Biden 45%, Trump 43%), finds new KFF/Cook Political Report polls of voters in three critical Sun Belt states carried by President Trump in his 2016 victory.
With the presidential election less than two months away, the new polls highlight one common factor about the race in each state: It’s largely about President Trump.
The vast majority (86%) of Trump voters across the three states say their vote is mainly for President Trump, while most Biden voters (53%) say their vote is mainly against President Trump.
Trump voters are also more likely than Biden voters to say they are “very enthusiastic” about voting in November across the three states (74% vs. 58%). The gap is narrowest in Florida, where 74% of Trump voters and 60% of Biden voters say they are very enthusiastic.
The closeness of the race is reflected in President Trump’s job approval ratings in each state: Arizona (46% favorable, 50% unfavorable), Florida (48% favorable, 51% unfavorable) and North Carolina (48% favorable, 50% unfavorable).
When asked about Joe Biden generally, voters in all three states are also roughly split between those who approve (50% in AZ and NC, 51% in FL) and disapprove (AZ 49%, NC 50%, FL 48%).
The new partnership survey of more than 3,400 voters across the three states, including at least 1,000 in each state, provides a glimpse into the concerns motivating voters in these key battlegrounds. Additional findings probing voters’ views about the economy, coronavirus, health care and other topics in the three Sun Belt states will be released soon.
The project explores the views of the critical group of nearly 1 in 4 voters in each state who are not certain who they will vote for. These “swing” voters include those who say they probably will vote for one of the candidates but are not completely certain as well as those who are truly undecided. This group is large enough in each state, especially since the races are so close, to determine the outcome, and the poll explores the factors that may influence both whether they vote and who they decide to vote for.
Across the three states, swing voters are more likely to identify as moderate (61%) and independents (43%) than voters who have already made up their mind. They are also somewhat younger on average than decided voters, and more likely to be Hispanic (22%, compared to 13% of decided voters).
Swing voters are more likely to say they prefer Joe Biden’s leadership style (50%) to President Trump’s style (39%) across the three states. At the same time, half (46%) describe President Trump as a strong leader, while four in 10 (39%) say the same about Joe Biden.
Large majorities of swing voters in each state also view President Trump as “unpredictable” with most of them viewing that quality as a bad thing. On the flip side, large majorities of swing voters in each state view Joe Biden as “part of the Washington establishment,” with most of them viewing that quality as a bad thing.
Swing voters are also somewhat more likely to say they approve of Joe Biden (56%) than of President Trump (45%), with the largest gap in Florida (Biden 60% approve, Trump 45% approve).
Democrats Lead in Arizona Senate and N.C. Gubernatorial Race; N.C. Senate Race in Virtual Tie
In Arizona, Democratic challenger Mark Kelly leads Republican Sen. Martha McSally in the Arizona Senate race (44%-36%).
In North Carolina, Democratic Gov. Roy Cooper leads Republican challenger Dan Forest (48%-38%), while Democratic challenger Cal Cunningham is within the margin of error in his race against Republican Sen. Thom Tillis (41%-37%).
The Economy and Coronavirus Top Voters’ Issues Across the States, But Partisans Differ
To the extent specific issues will matter in the presidential race, voters rank the economy as the top issue across the three states (32% say it is their most important issue), followed by criminal justice and policing (17%) and the coronavirus outbreak (16%).
Partisans prioritize the issues differently, with half (52%) of Republicans naming the economy as their most important issue, with criminal justice and policing a distant second (22%). Democrats rank coronavirus, a public health issue, as their most important issue (28%), followed by race relations (23%) and health care generally (18%). Independent ranks the economy first (31%), followed by coronavirus (17%) and criminal justice and policing (15%).
Among swing voters, the economy is the top issue in each of the three states, followed by criminal justice and policing, and health care. The coronavirus outbreak is further down their list of concerns.
On most issues, including the coronavirus, race relations, and health care, voters in the three states trust Joe Biden more than President Trump. On the economy, which is voters’ top issue, more trust President Trump (54%) than Joe Biden (44%). Voters trust the two candidates equally on criminal justice and policing, and immigration.
Methodology
Designed and analyzed by public opinion researchers at KFF in collaboration with Cook Political Report, the poll was conducted between Aug. 29 and Sept. 13, among a representative random sample of 3,479 registered voters in three Sun Belt states (1,298 in Arizona, 1,009 in Florida, and 1,172 in North Carolina). The poll relies on an innovative probability-based methodology designed to address shortcomings with telephone-only surveys based on either voter-registration rolls or random-digit dialing. Voters were contacted via mailing address using registration-based sampling and encouraged to participate in the survey either online or by telephone and follow-up contacts were made using outbound telephone calls. The margin of sampling error is plus or minus 4 percentage points in Florida and 3 percentage points in Arizona and North Carolina. For results based on subgroups, the margin of sampling error may be higher.
Throughout the 2020 election, the Kaiser Family Foundation and Cook Political Report have collaborated on a series of projects examining the attitudes and experiences of voters in several key battleground states leading up the 2020 presidential election. In November 2019, we released the Blue Wall Voices Project, a survey of 3,222 voters in the four states constituting the “Democratic Blue Wall” – the area in the Upper Midwest that was previously considered a Democratic stronghold. The Sun Belt Voices Project is our newest collaboration and includes 3,479 interviews with voters in Arizona, Florida, and North Carolina – three states in which shifting population characteristics may give Democrats an advantage in the more traditionally Republican region of the U.S. Using an innovative probability-based approach of contacting registered voters and allowing poll respondents to participate online or over the telephone, KFF and The Cook Political Report interviewed 1,298 voters in Arizona, 1,009 voters in Florida, and 1,172 voters in North Carolina from August 29 to September 13, 2020. For more details, please see the methodology section of this report.
Sun Belt Voices Project
A Collaboration Between KFF and The Cook Political Report
Key Findings
Most voters have made up their minds about how they will vote for president, with results suggesting very close elections in each of the three Sun Belt states included in this project. With most voters in Arizona, Florida, and North Carolina reporting they have already made up their minds about which presidential candidate they plan to vote for in November, the poll, fielded August 29-September 13, finds former Vice President Joe Biden with a slight lead in Arizona (Trump: 40%, Biden: 45%), and the results in Florida and North Carolina within the margin of sampling error; Florida (Trump: 42%, Biden: 43%), North Carolina (Trump: 43%, Biden: 45%).
About one in five voters are “swing voters” but that doesn’t mean all of these votes are up for grabs. In all three states, nearly one-fourth of voters are swing voters. This includes about one in ten voters who say they are truly “undecided” and a similar share of voters who say they are “probably” going to vote for one candidate, but haven’t definitively made up their minds. Few of those who say they are “probably” going to vote for one candidate say there is a “chance” they would vote for the other candidate, suggesting that some of these “swing” voters just may not vote on election day.
Swing voters are younger, have more moderate views, and a larger share are Hispanic voters, and also give Biden higher approval ratings than Trump. The crucial group of voters who have not yet decided who they plan to vote for in the 2020 election are younger, and larger shares identify as political moderates and independents. In addition, a larger share of swing voters than decided voters are Hispanic voters. They are also more likely to approve of former Vice President Biden than President Trump.
Half of swing voters prefer Biden’s leadership style but less than half see either candidate as a “strong leader.” Half of swing voters say, regardless of who they plan to vote for, they prefer Biden’s leadership style over President Trump’s (39% say they prefer Trump’s leadership style). Yet, less than half of swing voters say strong leader describes either President Trump (46%) or Joe Biden (39%). In addition, nearly two-thirds (64%) of swing voters say President Trump is unpredictable and this is a bad thing including a majority of swing voters in Arizona, Florida, and North Carolina.
President Trump is a motivating force for both Trump voters and Biden voters. Large majorities of voters who say they are going to vote for President Trump (either “definitely” or “probably”) say their vote is mainly a vote for Trump rather than a vote against Biden (86% v. 14%). On the other hand, more than half of Biden voters (53%) say their vote is mainly a vote against President Trump rather than a vote for Biden.
Trump voters report higher levels of enthusiasm than Biden voters. President Trump’s voters have the enthusiasm advantage in each of the three Sun Belt states included in this poll with about three-fourths of Trump voters in Arizona (73%), Florida (74%), and North Carolina (75%) saying they are “very enthusiastic” to vote for him. Comparatively, about six in ten Biden voters in each of these states say the same (Arizona: 53%, Florida: 60%, N.C.: 57%).
The 2020 election is about different issues, depending on voters’ party identification. Similar to national poll results, the economy is the top presidential election issue for Republican Sun Belt voters, while Democratic voters are prioritizing the coronavirus outbreak and race relations. On most issues, a larger share of voters trust Joe Biden to do a better job than President Trump. However, on the economy – voters’ top issue overall – more voters trust Trump than Biden (54% compared to 44%).
Top Issues for Sun Belt Voters
One-third of voters (32%) in Arizona, Florida, and North Carolina, three key states in the West and South’s Sun Belt region, say the economy is going to be the most important issue in their 2020 vote choice. This is followed by, criminal justice and policing (17%), the coronavirus outbreak (16%) health care (12%), and race relations (12%). Few voters (5%) say immigration is their top issue. This is also consistent with a recent shift in national polling in which the economy and the coronavirus outbreak, a public health issue, has displaced health care more generally as the top issue for voters.
Figure 1: The Economy Is Top Issue For Sun Belt Voters In Arizona, Florida, And North Carolina
The economy is the top issue among voters in Arizona (32%), Florida (34%), and North Carolina (31%), followed by criminal justice and policing and the coronavirus outbreak, with both of these two issues ranking similarly among Arizona, Florida, and North Carolina voters.
Figure 2: Voters In Sun Belt Region Prioritize The Economy In Their 2020 Vote For President
Partisan voters have very different priorities for the 2020 election when it comes to the top issues driving their votes. Overall, half of Republican voters in these 3 states (52%) say the economy is the most important issue in their 2020 vote choice, more than twice as many as say any other issue. One in five (22%) choose criminal justice and policing, an issue touted often by President Trump, as the most important issue. Democrats, on the other hand, are prioritizing the coronavirus outbreak in their 2020 vote choice with nearly three in ten saying it is the most important issue (28%), followed by race relations (23%) health care (18%), and the economy (14%). Three in ten independents (31%) say the economy is the most important issue followed by the coronavirus outbreak (17%).
Figure 3: Partisan Voters Have Different Views On Top Issues For 2020 Presidential Election
This partisan divide on the key issues in the 2020 election is consistent across each of the three states examined in this poll with large shares of Republican voters in Arizona, Florida, and N.C. saying the economy is the most important issue while Democratic voters in Arizona and Florida chose the coronavirus outbreak as their top issue. N.C. Democratic voters were divided between the coronavirus outbreak and race relations as their top issues. Few Republican voters in any of the three states chose either the coronavirus outbreak or race relations as their top issue. About three in ten independent voters chose the economy as their top issue.
Table 1: Partisans Across Key Sun Belt States Are Divided On Most Important Issue For 2020
Percent of voters who say each issue will be the most important in deciding their vote for president:
The economy
The coronavirus outbreak
Criminal justice and policing
Race relations
Democratic voters
AZ
15%
30%
7%
18%
FL
14
31
13
22
NC
15
22
15
27
Independent voters
AZ
31
20
16
8
FL
32
17
16
8
NC
30
16
13
14
Republican voters
AZ
47
7
26
<1%
FL
54
4
20
3
NC
50
4
24
3
With the economy topping the issues for voters heading into the 2020 election, the Sun Belt Voices Project finds that this is the one issue on which President Trump has a trust advantage over Joe Biden. Slightly more than half (54%) of voters in the Sun Belt states say they trust Donald Trump to do a better job dealing with the economy compared to 44% who say they trust Joe Biden. Joe Biden, on the other hand, has the advantage on other key issues such as health care, race relations, and the coronavirus outbreak. Voters were split between the two candidates on who they trust to do a better job handling immigration and criminal justice and policing.
Figure 4: Sun Belt Voters Trust Biden To Handle Race Relations, Health Care, And Coronavirus; Trust Trump To Handle The Economy
Once again, this is consistent across all three states with only one variation; President Trump has the advantage when it comes to the economy while Biden holds an advantage on health care, race relations, and the coronavirus outbreak. On immigration and criminal justice and policing, voters are more divided on which candidate they think will do a better job.
Table 2: Who Do Voters Trust To Handle Key Issues?
Percent of voters who say they trust… will do a better job dealing with each of the following issues:
Arizona
Florida
North Carolina
Race relations
Trump
40%
41%
42%
Biden
57
56
55
Biden +17
Biden +15
Biden +13
The coronavirus outbreak
Trump
43
45
43
Biden
54
52
54
Biden +11
Biden +7
Biden +11
Health care
Trump
44
45
45
Biden
53
52
53
Biden +9
Biden +7
Biden +8
Criminal justice and policing
Trump
47
49
48
Biden
50
48
50
Biden +3
Trump +1
Biden +2
Immigration
Trump
47
48
49
Biden
51
49
49
Biden +4
Biden +1
—
The economy
Trump
52
55
53
Biden
45
43
45
Trump +7
Trump +12
Trump +8
The Current State Of Races In Key Sun Belt States
President Trump and former Vice President Biden have slightly fewer than four in ten voters in each of the three states saying they are “definitely” going to vote for them. Thirty-eight percent of Arizona voters as well as 37% of Florida voters and 39% of N.C voters say they are “definitely going to vote for Joe Biden.” This is similar to the share of voters who say they are “definitely going to vote for President Trump” in Arizona (35%), Florida (37%), and North Carolina (37%). One in ten voters say they are “probably going to vote for President Trump” (AZ: 5%; FL: 5%; N.C: 6%), or “probably going to vote for Joe Biden” (AZ: 7%; FL: 6%; N.C: 6%); while another one in ten say they are undecided (AZ: 11%; FL: 11%; N.C: 9%),
Figure 5: Most Sun Belt Voters Say They Have Already Made Up Their Mind About Which Candidate They Are Voting For In 2020
Putting together “definitely” and “probably” groups, these results indicate that, with less than two months before the 2020 November election, the presidential race in each of these three Sun Belt states is very close with Biden having a slight edge in Arizona (Trump: 40%, Biden: 45%), and within the margin of sampling error in Florida (Trump: 42%, Biden: 43%) and North Carolina (Trump: 43%, Biden: 45%).
Overwhelmingly, President Trump and Vice President Joe Biden are garnering support from their key “bases,” the groups that tend to support one party’s candidate over another and are predicted to vote in favor of the candidate. President Trump has majority support among conservative voters, rural voters, as well as white voters with lower levels of education. In addition, nine in ten (89%) voters who voted for him in 2016 say they plan to vote for him in 2020 while 5% of these voters say they are going to vote for Biden and 5% are still undecided.
Figure 6: Majorities Of Rural, Conservative, And Lower Educated Voters In Sun Belt States Say They Are Voting For President Trump
Biden, on the other hand, garners majority support from black voters, liberal voters, voters who voted for Secretary Clinton in 2016. More than half of moderate voters (56%) also say they are going to vote for Biden in November.
Figure 7: Large Majorities of Black Voters, Liberal And Moderate Voters Say They Are Voting For Joe Biden
Who Are the Decided Voters and Swing voters?
Three-fourths of voters in Arizona, Florida, and North Carolina say they have already made up their minds about which candidate they plan to vote for in the 2020 presidential election and the results indicate a very close election in these states. A majority of Democratic voters and Republican voters in each state say they aren’t going to cast a vote for the other party’s candidate. About eight in ten Democratic and Democratic-leaning independent voters in Arizona (81%), Florida (83%) and North Carolina (80%) say they are definitely going to vote for Joe Biden.
Figure 8: About Eight In Ten Democratic Voters Say They Are Definitely Going To Vote For Biden
Similar shares of Republican and Republican-leaning voters say they are “definitely going to vote for President Trump” including three-fourths of Arizona (73%), and eight in ten voters in Florida (79%), and N.C. (81%). There is a small but noticeable share of Republican and Republican-leaning voters who say they are “definitely” going to vote for Joe Biden, including 6% in Arizona.
Figure 9: Most Republican Voters Say They Are Voting For President Trump
Nearly one-fourth of voters in each of the three states are “swing voters,” a crucial group of voters who have not yet made up their minds about which candidate they plan to vote for. There are not significant differences on the share of voters who are “swing voters” across these Sun Belt states, with similar shares of voters in Arizona (23%), Florida (22%), and North Carolina (21%) saying they are either “probably” going to vote for a candidate or are “undecided.” This is also consistent with our national KFF Health Tracking Poll data which also finds about one-fourth of voters are “swing voters.”
It is important to note that not all “swing voters” could potentially change their vote to support the other party’s candidate. One-third of those who say they are probably going to vote for President Trump say there is “a chance” they will vote for Joe Biden (2% of all voters) and one-fifth of those who say they are probably going to vote for Joe Biden say there is “a chance” they are going to vote for President Trump (1% of all voters); most “probably” voters, on the other side of the ballot, say there is “no chance” they will vote for the other party’s candidate (67% of voters probably voting for President Trump or 4% overall, 80% of voters probably voting for Joe Biden or 5% overall). This is similar across Arizona, Florida, and North Carolina with few voters saying they are “probably” going to vote for one candidate but there is “a chance” they would vote for the other candidate.
Figure 10: About One In Five Sun Belt Voters Haven’t Made Up Their Minds About Who They Are Voting For
On most demographics, swing voters look very similar to their counterparts (voters who say they have already decided who they are going to vote for in the 2020 election), but they differ on three key variables: age, party identification, and ideology. Swing voters generally are more likely to say they are moderate in terms of their ideology (61%) and a larger share identify as political independents (43%) than their decided counterparts (10%). In addition, swing voters are slightly younger as a whole with about six in ten under the age of 50. In addition, nearly one in four swing voters are Hispanic voters (22%) compared to 13% of decided voters.
Figure 11: Demographic Differences Among Swing Voters And Decided Voters
While a similar share of swing voters say they are Democrats or Democratic-leaning independents (27%) as say they are Republicans or Republican-leaning independents (30%), their top issue for their vote choice is more like the priorities of Republicans than Democrats. Large shares of swing voters in each of the three states (AZ: 38%, FL: 37%, N.C.: 32%) say the economy is going to be the most important issue in deciding their vote for president while significantly fewer say the same about any other issue – including the coronavirus outbreak (AZ: 9%, FL: 13%, N.C.: 13%).
Figure 12: The Economy Is Top Issue For Swing Voters In Arizona, Florida, And N.C.
Job Approval
Throughout President Trump’s presidency, his overall net approval as remained largely stable except for a short dip over the summer – perhaps in response to his handling of the coronavirus outbreak. More recently, his overall job approval has been around 45% in national polling. President Trump has similar job approval among voters in these Sun Belt states – with one notable exception. Arizona voters are more disapproving than approving of the job Trump is doing as president, resulting in a negative net approval of – 8 percentage points.
Figure 13: President Trump Has Higher Negative Net Approval Among Arizona Voters
Among the small share of voters who haven’t made up their minds about which candidate to vote for, these swing voters are divided on their views of both President Trump and former Vice President Biden with a slightly larger share saying they approve of Biden. Overall, about half of swing voters approve, which is about as many as disapprove, of both the job Donald Trump is doing as president (Approve: 45%; Disapprove: 54%) and of Joe Biden generally (Approve: 56%; Disapprove: 42%), with slight variations within states. To see the full percentages for job approval for both President Trump and Biden in each of the three states, see the Appendix Table 1.
Figure 14: Swing Voters Give Trump Negative Ratings While Biden Receives Slightly More Positive Ratings
The connection between voters’ overall approval of both candidates and their ultimate choice in which candidate to vote for has been illustrated by others, especially in light of President Trump’s relatively stable overall job approval numbers throughout his presidency. Despite the twists and turns of the campaign and the various national issues that have captured voters’ attention, voters’ approval of the candidates continues to be one of the strongest predictors of vote choice. Our analysis of these Sun Belt states finds there is a small share of voters (5%) who say they “approve” of both former Vice President Biden and the job Donald Trump is doing as president (5% of voters in Arizona, 6% of voters in Florida, and 3% of voters in North Carolina). Overall, these voters tend to be less partisan, are more likely to identify as independents and moderates, and more than half are swing voters with 53% saying they are currently undecided about which candidate they plan to vote for while 9% say they are probably going to vote for President Trump and 7% say they are going vote for Biden.
Other Key races to Watch
In addition to the presidential election, there are other important Senate races in Arizona and North Carolina, a gubernatorial race in North Carolina, as well as congressional races throughout each of the three states. To see the views of voters across demographics within each state, check out our state interactives.
As of the second week of September, a larger share of voters in Arizona say they are voting for Mark Kelly, NASA astronaut than incumbent Sen. Martha McSally (44% compared to 36%).
Figure 15: The State Of The Race: Arizona
In North Carolina, Democratic Governor Roy Cooper (48%) has a lead over Republican Lt Governor Dan Forrest (38%), while the Senate election between Republican incumbent Thom Tillis and Cal Cunningham is within the margin of error.
Figure 16: The State Of The Race: North Carolina
Trump Voters Report Higher Enthusiasm In Key Sun Belt States, Motivation To Turnout Is Equal Across Partisans
Three-fourths of voters (74%) who say they are voting for President Trump report being “very enthusiastic” about their vote with an additional one-fifth (19%) saying they are “somewhat enthusiastic.” Voters who say they are voting for Joe Biden report lower levels of enthusiasm with six in ten (58%) saying they are “very enthusiastic” with an additional 27% saying they are “somewhat enthusiastic.” One in seven Biden voters (15%) say they are either “not very enthusiastic” or “not at all enthusiastic” about voting for him compared to 6% of Trump voters who report the same.
Figure 17: Three-Fourths Of Trump Voters Are “Very Enthusiastic” Compared To Six In Ten Biden Voters
Six in ten (61%) Biden voters say that his choice of Sen. Kamala Harris as his running mate makes them “more enthusiastic” about voting for him while one-third (34%) say “it does not make a difference.” Only 5% of Biden voters say the choice of Harris as the Vice President nominee makes them “less enthusiastic” about voting for the Democratic ticket.
President Trump’s voters have the enthusiasm advantage in each of the three Sun Belt states included in this poll with about three-fourths of Trump voters in Arizona (73%), Florida (74%), and North Carolina (75%) saying they are “very enthusiastic” to vote for him. Comparatively, about half of Biden voters in Arizona (53%) and about six in ten Biden voters in Florida (60%) and N.C. (57%) say they are “very enthusiastic” about their vote.
Figure 18: Larger Shares Of Trump Voters In Key Sun Belt States Report Being Very Enthusiastic To Vote In 2020
Last year’s Blue Wall Voices Project found that a larger share of Democratic voters saying they were “more motivated” to vote in the 2020 election compared to the 2016 election. The latest polling in these Sun Belt states finds that majorities of both Democratic and Republican voters say they are “more motivated” to vote in this year’s election.
Table 3: Neither Party Has Advantage On Motivation
Percent who say they are more motivated to vote in the 2020 election than in the 2016 election:
Arizona
Florida
North Carolina
Total
58%
59%
66%
Democratic voters
64
63
71
Independent voters
50
55
63
Republican voters
65
67
71
Trump Is A Motivating Force For Voters
While Biden voters may not be as enthusiastic about their vote choice as Trump voters, this doesn’t mean that they aren’t motivated to vote. Instead, their motivation may be less for their vote choice, and more against President Trump.
Half of Biden voters (53%) in the Sun Belt states polled say their vote is mainly a vote “against Donald Trump” compared to 14% of Trump voters who say their vote is mainly one “against Joe Biden.” Nearly nine in ten (86%) Trump voters say their vote is mainly one “for Donald Trump.”
Figure 19: Large Share Of Biden Voters Say Their Vote Is Mainly A Vote Against President Trump
Biden voters who say their vote is mainly a vote “against Donald Trump” are younger and less partisan than their counterparts (those who say their vote is “for Joe Biden”).
Voters Still See Trump As The Unconventional Candidate
President Trump has long touted his unconventional leadership style and in 2016, he ran as the candidate who was going to deliver a shock to business as usual in Washington, D.C. Perhaps unsurprisingly, vast majorities of Democrats say they prefer Biden’s leadership style (96%) over President Trump’s (3%), while most Republicans say they prefer President Trump’s leadership style (92%). Independents in these three Sun Belt states slightly prefer Biden’s leadership style as do a majority of swing voters. Half of swing voters say regardless of who they intend to vote for, they prefer Joe Biden’s leadership style over President Trump’s. Four in ten (39%) swing voters say they prefer Trump’s leadership style while one in ten (11%) are unsure which style they prefer.
Figure 20: Half Of Swing Voters In Sun Belt States Say They Prefer Biden’s Leadership Style
When given a list of characteristics that could describe President Trump, two-thirds of voters say unpredictable (68%) is a term that describes him while most voters say that being too old to be president (81%) and part of the Washington establishment (71%) are not terms to describe him. Most voters also say that cares about people like me is also not a description of President Trump (56%); however, 85% of Republican voters say this does describe him. Partisans are also divided on whether a strong leader is a good describer of President Trump with 92% of Republican voters saying it “does describe him” while 90% of Democratic voters and 53% of independent voters say it “does not describe him.”
Figure 21: Two-Thirds Of Voters Describe Trump As Unpredictable
Two-thirds of voters say unpredictable is a characteristic that describes President Trump but whether that is a “good thing” or a “bad thing” depends on partisanship. Four in ten Republican voters (41%) say President Trump is unpredictable but 27% of them say being unpredictable is a “good thing” while the vast majority of Democrats (86%) as well as most independent voters (58%) say that Donald Trump is unpredictable and this is a “bad thing.”
Figure 22: Partisans Divided On Whether Being “Unpredictable” Is A Good Or Bad Thing
Majorities of voters say that being part of the Washington establishment describes Joe Biden (72%) but once again, whether that is a “good thing” or a “bad thing” depends on partisanship. Two-thirds of Democratic voters say being part of the establishment describes Joe Biden but most (53% of all Democratic voters) say Biden being part of the Washington establishment is a “good thing,” while most Republicans (66%) and half of independent voters (41%) say Biden is part of the establishment and this is a “bad thing.”
Figure 23: Partisans Divided On Whether Biden Being “Part Of The Washington Establishment” Is A Good Or Bad Thing
Seven in ten voters say being part of the Washington establishment describe Biden, about half of voters say cares about people like me (53%), very liberal (53%), and moderate (52%) describes Biden. Slightly more than half of voters say being too old to be president and strong leader do not describe Biden (53% and 55%, respectively).
Figure 24: Seven In Ten Voters Describe Joe Biden As Being Part Of Washington Establishment
Views of what characteristics describe and do not describe Biden and Trump fall largely along party lines with majorities of Democratic voters saying strong leader describes Biden and most Republican voters say the same about President Trump.
Swing voters, on the other hand, may have their voting decisions impacted by such messages. Most swing voters say that moderate is a term that describes Biden well, with most of them and nearly half of voters overall saying this is a “good thing” (AZ: 44%, FL: 49%, N.C.: 46%). In addition, six in ten swing voters in Florida and N.C. say cares about people like me is something that describes Biden well.
Table 4: Swing Voters’ Views Of Biden
Percent of swing voters who say each of the following describes Joe Biden…
Arizona swing voters
Florida swing voters
N.C. swing voters
Too old to be president
51%
42%
39%
Part of the Washington establishment
69
70
62
Is this a good thing?
25
35
25
Is this a bad thing?
41
32
35
Very liberal
52
42
45
Is this a good thing?
17
15
16
Is this a bad thing?
34
26
29
Moderate
59
62
54
Is this a good thing?
44
49
46
Is this a bad thing?
13
11
7
Cares about people like me
46
61
57
Strong leader
38
38
42
A majority of swing voters in Arizona (59%), Florida (66%), and North Carolina (61%) say President Trump is unpredictable and this is a bad thing. Less than half of this share say President Trump cares about people like me and no more than half say that being a strong leader describes him well.
Table 5: Swing Voters’ Views Of Trump
Percent of swing voters who say each of the following describes Donald Trump…
Arizona swing voters
Florida swing voters
N.C. swing voters
Too old to be president
19%
16%
17%
Part of the Washington establishment
25
28
26
Is this a good thing?
9
13
12
Is this a bad thing?
15
15
12
Unpredictable
74
82
81
Is this a good thing?
14
14
18
Is this a bad thing?
59
66
61
Cares about people like me
25
30
34
Strong leader
45
46
46
The Aca And Health Care
These additional findings were released September 23.
With the recent news of the passing of Supreme Court Justice Ruth Bader Ginsburg, the latest from the Sun Belt Voices Project – a collaboration between KFF and The Cook Political Report – takes a look at how increased attention to California v. Texas, the Supreme Court case challenging the constitutionality of the Affordable Care Act, could motivate voters in the 2020 election. The poll, conducted prior to the death of Justice Ginsburg, found that the top issues for Arizona, Florida and N.C. voters two months out from the 2020 election were the economy, the coronavirus outbreak, race relations and criminal justice and policing. Health care as an election issue ranked lower for these voters. Yet with less than two months before the Supreme Court hearing of the highly politicized ACA case, health care policy may once again dominate election coverage.
Key Findings
Joe Biden has a slight advantage over President Trump among Arizona, Florida, and North Carolina voters on two key health care issues in the 2020 presidential campaign: the future of the Affordable Care Act and maintaining protections for people with pre-existing conditions. Yet, these are largely driven by partisanship with majorities of Democratic voters saying Biden has the better approach while most Republican voters say the same about President Trump.
Swing voters, on the other hand, give Biden the overwhelming advantage on all key health care issues including the ACA (Biden: 65%, Trump: 28%) and pre-existing condition protections (Biden: 64%, Trump: 28%). These are voters who say they are either entirely undecided or not firm in their vote choice and for some, there is a chance they may vote for the other candidate
Health care has long been an important voting issue among suburban voters, including in the 2018 midterm elections. The latest polling in Arizona, Florida, and North Carolina finds suburban voters are closely divided on which presidential candidate they trust to handle health care. Suburban women give Biden a slight edge on his handling of heath care, while other groups of suburban voters say they trust Trump. When it comes to specific key health care policy areas, suburban voters prefer Biden on the ACA (Biden +10 percentage points) and maintaining pre-existing conditions protections (Biden +8 percentage points), but are divided on their trust of the candidates to lower the costs of health care and prescription drugs.
The Future Of The Affordable Care Act
One of the top issues deciding the 2018 election was health care, most notably – the continued protections for people with pre-existing medical conditions. An analysis of campaign advertisements by the Wesleyan Media Project found nearly half (46%) of airings in federal races mentioned health care as did three in ten gubernatorial ads. In addition, one-third of health care ads were about coverage for people with pre-existing conditions. This is consistent with KFF polling which found voters in two bellwether states, Florida and Nevada, were more likely to say they would vote for candidates who wanted to maintain the ACA’s protections for people with pre-existing conditions.
With the Supreme Court deciding not to hear California v. Texas, the case challenging the future of the ACA, until after the 2020 election, many experts expected this issue to be a smaller issue during the campaigns. Yet with the recent passing of Supreme Court Justice Ginsburg, this case is now front-and-center in the 2020 election as a new justice could determine the future of the 2010 Affordable Care Act.
The latest polling from three key sun belt states (Arizona, Florida, and North Carolina) finds former Vice President Biden has a considerable advantage among voters on which presidential candidate they think has the better approach to determining the future of the Affordable Care Act as well as maintaining protections for people with pre-existing health conditions. More than half of voters in Arizona, Florida, and North Carolina say Joe Biden has the better approach on the ACA (AZ: 55%, FL: 55%, N.C.: 55%) compared to four in ten voters from each state who say Donald Trump.
Figure 1: More Than Half Of Arizona, Florida, And North Carolina Voters Say Biden Has The Better Approach To Determining The ACA’s Future
This is similar to the share who say Biden has the better approach to maintaining protections for people with pre-existing conditions (AZ: 55%, FL: 54%, N.C.: 53%) compared to President Trump (AZ: 40%, FL: 41%, N.C.: 43%).
Figure 2: More Than Half Of Arizona, Florida, And North Carolina Voters Say Biden Has Better Approach To Maintaining Pre-Existing Protections
Views on which candidate has the better approach to handle all health care issues – including the future of the ACA and pre-existing conditions – are largely driven by party identification. As seen in Table 1, vast majorities of Democratic voters in Arizona, Florida, and North Carolina say Biden has the better approach on health care issues while at least eight in ten Republicans voters in each of the three states say Trump has the better approach. Independents in Arizona and Florida mostly give the advantage on health care issue to Biden, while independent voters in North Carolina are more divided on some health care issues.
Table 1: Partisans Say Their Party’s Candidate Has Better Approach to Handle Key Health Care Issues
Do you think Donald Trump or Joe Biden has the better approach to…?
Arizona
Florida
North Carolina
Dem
Ind
Rep
Dem
Ind
Rep
Dem
Ind
Rep
…lowering the cost of health care for individuals
Donald Trump
3%
36%
87%
2%
41%
86%
4%
45%
91%
Joe Biden
95
58
8
96
56
11
95
50
6
…determining the future of the Affordable Care Act, sometimes called Obamacare
Donald Trump
3
36
82
3
34
80
2
39
87
Joe Biden
96
60
14
95
59
15
98
57
9
…lowering prescription drug costs
Donald Trump
5
39
87
3
45
87
5
48
93
Joe Biden
92
53
8
94
51
9
93
49
6
…protecting people from surprise medical bills from out-of-network care
Donald Trump
4
33
82
3
35
84
3
40
87
Joe Biden
92
57
11
94
58
10
95
53
8
…making sure everyone has access to health care and insurance
Donald Trump
3
30
81
2
38
85
3
39
88
Joe Biden
96
63
14
96
61
12
96
57
9
…maintaining protections for people with pre-existing health conditions
Donald Trump
3
32
82
3
34
84
3
39
88
Joe Biden
95
61
14
95
61
11
96
57
8
Swing Voters Give Biden Advantage On health Care Issues
Swing voters, the crucial group of voters who are either entirely undecided or probably going to vote for a candidate but haven’t decided yet, overwhelmingly give Biden the advantage on all key health care issues including the ACA and maintaining pre-existing conditions. More than twice as many swing voters say Biden (65%) has the better approach on the ACA than President Trump (28%) as well as on maintaining pre-existing condition protections (64% v. 28%). In fact, on all key health care issues asked about in the survey, Biden has the advantage among swing voters. This is despite the fact swing voters don’t have a candidate preference with 24% saying they are probably going to vote for President Trump, 29% saying they are probably going to vote for Joe Biden, and 47% truly undecided.
Figure 3: Sun Belt Swing Voters Overwhelmingly Trust Biden To Handle Key Health Care Issues
The advantage Biden has on key health care issues is consistent among swing voters in Arizona, Florida, and North Carolina.
Table 2: Swing Voters In Key Sun Belt States Trust Biden On Health Care Issues
Do you think Donald Trump or Joe Biden has the better approach to…?
Arizona Swing Voters
Florida Swing Voters
North Carolina Swing Voters
…lowering the cost of health care for individuals
Donald Trump
35
31
41
Joe Biden
53
63
50
…determining the future of the Affordable Care Act, sometimes called Obamacare
Donald Trump
32
24
33
Joe Biden
60
69
61
…lowering prescription drug costs
Donald Trump
38
39
42
Joe Biden
49
54
51
…protecting people from surprise medical bills from out-of-network care
Donald Trump
30
27
32
Joe Biden
55
63
56
…making sure everyone has access to health care and insurance
Donald Trump
25
27
32
Joe Biden
63
67
60
…maintaining protections for people with pre-existing health conditions
Donald Trump
28
26
33
Joe Biden
60
68
59
Suburban Voters and Health Care
In the 2016 presidential election, President Trump won overwhelming support from rural voters while Secretary Clinton garnered majority support from urban voters; suburban voters were more divided between the two candidates. The Sun Belt Voices Project interviewed over 500 suburban voters in each of the three states polled (571 in Arizona, 683 in Florida, and 527 in North Carolina) and finds President Trump holding a slight lead among North Carolina suburban voters (50% v. 41%) while suburban voters in Arizona and Florida are more divided (AZ: 45% v. 41%, FL: 43% v. 43%).
Figure 4: Suburban Voters Are Divided In Arizona And Florida, Trump Has Advantage In North Carolina Suburbs
But the suburbs are increasingly demographically diverse and candidate preference varies across key demographic groups. President Trump garners support from at least half of suburban men (51%), white suburban voters (54%), and suburban voters with lower levels of education (50% of those with a high school diploma or less). Former Vice President Biden, on the other hand, garners support from at least half of Black (73%) and Hispanic voters (50%) living in the suburbs, and those with higher levels of education (52% of those with at least a college degree).
Not All Suburbs Are The Same
Just as suburban areas are becoming increasingly demographically diverse, many suburban areas within states look and vote very differently. Looking at suburban voters in Arizona, Florida, and North Carolina, we examine some key suburban areas:
Arizona – Former Vice President Joe Biden has a strong lead in Pima County (the area around Tucson) over President Trump, but voters in Maricopa County are more divided in their 2020 vote choice with similar shares of voters in this county saying they plan to vote for President Trump (42%) and Joe Biden (42%). Within Maricopa County, Phoenix voters overwhelmingly support Biden. The economy is by far the top issue for Maricopa County voters (34%) while Pima County voters are divided between the economy (28%) and the coronavirus outbreak (24%).
Florida – Florida suburbs are also divided along geographic regions of the state with Miami suburbs voting very differently than northern parts of the state including the panhandle. Recent elections have looked closely at areas along the expanded I-4 corridor, an area many experts say is crucial to President Trump’s re-election. Voters in this area of Florida choose the economy as their top 2020 issue (28%) but are currently divided in which presidential candidate they plan to vote for with 40% saying President Trump and 45% saying Joe Biden. Biden has a commanding lead in the Miami suburbs while President Trump holds the advantage in the northern part of the state.
North Carolina – There is an increasing trend within N.C. with voters living on the edges of urban city centers voting more like traditionally suburban voters. Using categories developed by Old North State Politics we find that “urban county suburban” voters are one group that are prioritizing criminal justice and policing (22%) as a top 2020 voting issue along with the economy (27%). In addition, voters in these areas within North Carolina are more divided in their vote choice with 42% saying they plan to vote for President Trump and 48% saying they plan to vote for Joe Biden.
Suburban Voters Are divided On Which Candidate They Trust On Health Care, But Most Say Biden Has Better APproach to ACA ANd Pre-Existing COndition Protections
Suburban voters are divided on which candidate they trust to do a better job handling health care with half of suburban voters saying they trust each candidate. A larger share of suburban women voters say they trust Joe Biden on health care, while President Trump garners more support among all suburban white voters. To see which candidate suburban voters trust to handle all key issues, see Appendix Table 2.
Figure 5: Suburban Voters Are Split On Who They Trust To Deal With Health Care
While suburban voters overall are divided on which candidate they trust to do a better job dealing with health care, when it comes to the future of the Affordable Care Act and maintaining pre-existing conditions protections, a slightly majority of suburban voters give Biden the advantage.
Among suburban voters, Former Vice President Biden has a 10 point advantage over President Trump on determining the future of the ACA (53% v. 43%), a landmark legislation of the Obama/Biden presidency. In addition, Biden also has a slight advantage on maintaining pre-existing condition protections (52% v. 44%). On all other key issues, the difference between the two candidates is within the margin of sampling error.
Figure 6: Suburban Voters Think Biden Has Better Approach On ACA And Pre-Existing Conditions, Divided On Other Key Health Care Issues
There is some variation across states with North Carolina suburban voters more closely divided in which candidate has the better approach to handle some health care issue including the future of the ACA and maintaining protections for people with pre-existing conditions, and President Trump having a clear advantage on lowering overall health care costs and prescription drug costs.
Table 3: Suburban Voters On Which Candidate Has The Better Approach To Deal With Key Health Care Issues
Do you think Donald Trump or Joe Biden has the better approach to…?
Arizona Suburban Voters
Florida Suburban Voters
North Carolina Suburban Voters
…determining the future of the Affordable Care Act, sometimes called Obamacare
Donald Trump
46%
40%
49%
Joe Biden
51
55
48
…maintaining protections for people with pre-existing health conditions
Donald Trump
46
42
49
Joe Biden
50
54
47
…lowering the cost of health care for individuals
Donald Trump
49
45
55
Joe Biden
47
52
42
…lowering prescription drug costs
Donald Trump
51
45
55
Joe Biden
45
51
43
…protecting people from surprise medical bills from out-of-network care
Donald Trump
47
42
50
Joe Biden
47
52
44
…making sure everyone has access to health care and insurance
Donald Trump
45
44
51
Joe Biden
51
53
46
How Votes Will Be Cast In 2020
These additional findings were released September 25.
As part of the latest collaboration between KFF and The Cook Political Report, this analysis examines how the coronavirus outbreak is changing voting in the 2020 election. With former Vice President Biden holding a slight lead over President Trump in Arizona (Biden 45%, Trump 40%), and the race is within the margin of sampling error in Florida and North Carolina, how many Americans will vote in the 2020 election, especially with strong differences among partisans, may have significant implications on the narrative of the 2020 election results.
Key Findings
With the coronavirus pandemic changing how many Americans plan to cast their vote, the latest release from the Sun Belt Voices Project finds that only one in five Arizona voters, and one-third of N.C. voters (33%) and Florida voters (32%) say they still plan on voting in person on Election Day.
This poll suggests that many of the last ballots to be counted in North Carolina, where mail-in ballots will be accepted up to three days after Election Day as long as they are postmarked by November 3rd. Most of those who plan to vote by mail in Arizona, Florida, and North Carolina say they will be voting for Joe Biden (AZ: 56%, FL: 64%, N.C.: 71%). Voters who plan to vote in-person on Election Day, on the other hand, say they plan on casting a ballot for President Trump (AZ: 66%, FL: 60%, N.C.: 66%).
Among those who say they are planning to head to the physical polls in November, about one in five are worried that voting in person may expose them to coronavirus (10% of voters overall). A smaller share of Republican voters express concerns about voting in person (9%) compared to independent (20%) and Democratic voters (38%).
In addition to concerns about exposure to coronavirus, majorities of Arizona, Florida, and N.C. voters in each of the states say they are worried about various factors that could interfere with having a fair and accurate 2020 election including voter suppression (AZ: 62%, FL: 62%, N.C.: 65%) and voter fraud (AZ: 56%, FL: 59%, N.C.: 58%). Yet, partisan voters hold very different views, with most Democratic voters worried about voter suppression and most Republican voters in Arizona, Florida, and N.C. worried about voter fraud.
Voting During A Pandemic
With the expectation that millions of Americans will cast their votes using mail-in ballots for the first time in the 2020 election, there has been criticism from the Trump Administration about the validity of voting-by-mail while Democrats have raised concerns about potential voter suppression.
Arizona, Florida, and North Carolina are three states in which voters can ask to vote-by-mail due to the coronavirus outbreak. Arizona has a longer history of voting-by-mail with the state legislature allowing any Arizona voter to vote-by-mail for any reason as early as 1991. In 2016, 75% of Arizona voters voted by mail. Florida has had vote-by-mail in place since 2002 but, prior to the coronavirus outbreak, only about 29% of Florida voters chose to cast a mail-in ballot. Mail-in voting has been a contentious issue in North Carolina, but in June the state legislature passed a bill designed to making voting by mail easier during the coronavirus pandemic. In 2016, 4% of North Carolina voters voted by mail.
Democrats and Biden Supporters plan to vote by mail while Republicans and Trump supporters plan to vote in person
Due to concerns over the spread of COVID-19, voting by mail is expected to account for a large portion of ballots in November with larger shares of voters nationwide saying they plan to vote by mail.
More than half of Arizona voters (57%) say they plan to vote by mail, as do one-third of Florida voters (33%) and one in five North Carolina voters (20%). One-third of N.C. voters (33%) and Florida voters (32%) say they plan to vote in person on Election Day, as do one in five (19%) Arizona voters.
While Arizona and Florida have had “no excuse” absentee or mail-in voting options prior to this year’s election, mail-in voting is new to many North Carolina voters. Arizona is the only one of these three states that has had large shares of absentee or vote-by mail records, which is made easier by the state’s legislation to allow residents able to be put on a permanent vote-by-mail list, as opposed to most states’ requirements that each ballot is applied for, and in N.C.’s case, a witness is required for application. Among the highest in the country, 75% of Arizona’s ballots were collected early, through absentee or by mail in the 2016 general election.
Figure 1: Most Arizona Voters Plan To Vote By Mail, Majorities Of N.C. And Half Of Florida Voters Will Vote In Person Early Or On Election Day
Larger shares of voters choosing to vote by mail or absentee ballot poses challenges for both state election boards as well as news organizations covering the election night results. While ballots must be received by the end of Election Day, November 3rd, in both Arizona and Florida, North Carolina ballots must be postmarked by November 3rd and received by November 6th.
This poll suggests that many of the last ballots to be counted in North Carolina may be disproportionately for former Vice President Joe Biden. Most in-person Election Day voters say they plan on casting a ballot for President Trump (AZ 66%; FL 60%; N.C. 66%), while majorities of the voters who say they plan on voting by mail say they will be voting for Joe Biden (AZ 56%; FL 64%; N.C. 71%). Due to the high prevalence of mail voting that already exists in Arizona, three in ten voters (31%) who plan on voting by mail in Arizona say they are voting for President Trump.
Table 1: Voters In Key Sun Belt States Plan To Cast Their In Person Votes For President Trump, Mail In Ballots For Joe Biden
Percent who say they are…
“Probably” or “Definitely” voting for Joe Biden
“Probably” or “Definitely” voting for President Trump
Among Arizona voters who say they plan to vote…
…in person on Election Day
20%
66%
…in person through early voting
46
46
…by mail or absentee ballot
56
31
Among Florida voters who say they plan to vote…
…in person on Election Day
27
60
…in person through early voting
43
50
…by mail or absentee ballot
64
25
Among North Carolina voters who say they plan to vote…
…in person on Election Day
24
66
…in person through early voting
53
41
…by mail or absentee ballot
71
17
Swing voters – those who say they are either probably voting for President Trump or Joe Biden or are undecided – are less settled on their preferred method of voting which may indicate their reluctance to vote at all. One-fifth of swing voters in Arizona say they are unsure of how they plan to vote (18%), as are one-fourth of swing voters in Florida and N.C. (26% and 25%, respectively). This is compared to 11% of decided voters in Arizona and N.C., and 14% in Florida who say they are unsure.
Voting in Person
Among those who are choosing to still head to the physical polls in November, about one in five are worried that voting in person may expose them to the coronavirus (10% of voters overall). Partisans differ in their worry. While majorities of voters across partisans who say they plan to vote in person are not too or not at all worried about exposure to coronavirus while doing so, nearly four in ten Democrats say they are very or somewhat worried (38%) and one in ten Republicans say the same (9%). Of course, the decision to vote in person may have taken into account any potential worry.
Figure 2: Larger Shares Of Democrats Planning To Vote In Person Are Worried About Exposure To COVID-19
A Fair And Accurate Election
About nine in ten voters (92%) in these three states are worried about at least one threat to holding a fair and accurate presidential election in 2020, and more than half of voters say they are worried about each of the possible threats provided in the survey. More than half of voters in Arizona, Florida, and North Carolina are worried that voter suppression (63%), the coronavirus outbreak (61%), voter fraud (58%), technical problems at polling places (57%), or interference by a foreign country (54%) will interfere with the 2020 election.
Figure 3: Nine in Ten Sun Belt Voters Are Worried About At Least One Potential Interference With A Fair And Accurate Election
Majorities of voters in each of the states say they are at least “somewhat worried” that each of these will interfere with the election, and nine in ten are worried about at least one of the potential interferences.
Table 2. Voters In Arizona, Florida, and North Carolina Share Worries Around The 2020 Election
Percent who say they are very or somewhat worried that each of the following will interfere with a fair and accurate presidential election in 2020:
Arizona Voters
Florida Voters
North Carolina Voters
Voter suppression
62%
62%
65%
The coronavirus pandemic
59
60
64
Voter fraud
56
59
58
Technical problems at polls or voting places
58
58
54
Interference by a foreign country
57
53
56
Worried about any of these (NET):
92
92
93
The sources of potential worry around the 2020 election vary across partisans. Larger shares of Democrats than Republicans say that they are at least somewhat worried that voter suppression (84% v. 44%), foreign interference (77% v. 33%), the coronavirus pandemic (74% v. 51%) and technical problems at polling locations (66% v. 52%) will interfere with a fair and accurate presidential election.
On the other hand, voter fraud caused by people who are ineligible to vote casting ballots in the election is a larger worry for Republicans (80%) than Democratic voters (40%) or independent voters (54%).
Figure 5: Majorities Of Sun Belt Voters Say They Are Confident The 2020 Presidential Election Will Be Held In A Fair And Accurate Way
Despite this, majorities of voters – across partisanship – are still confident that the 2020 presidential election will be held in a fair and accurate way (59% of Arizona voters, and 57% of Florida voters and N.C. voters) with one in five voters saying they are “very confident” (AZ: 18%, FL: 19%, N.C.: 17%). This is consistent across party identification with about six in ten Democrats (59%), Republicans (62%), and independent voters (56%) saying they are at least somewhat confident that the 2020 election will be fair and accurate.
Black And Hispanic Voters
These additional findings were released October 7, 2020.
The latest release from KFF and The Cook Political Report’s Sun Belt Voices Project looks at what is motivating the vote choices of both Black and Hispanic voters in Arizona, Florida, and North Carolina – three key battleground states. While larger shares of Black and Hispanic voters report being impacted by the coronavirus, either by knowing someone who has gotten sick or by losing their income or job, it is no more of a voting issue for voters of color than it is for White voters. And while majorities of Black voters across the three states say they are voting for Vice President Biden, Hispanic voters in Florida and Arizona have different voting plans with Biden garnering majority support in Arizona and President Trump leading among Florida Hispanic voters.
The Coronavirus Outbreak
Black and Hispanic people in the U.S. have been disproportionately impacted by the coronavirus outbreak both in terms of the share of populations who have been hospitalized or died due to COVID-19 or reported that they lost their job or income because of a coronavirus-related layoff. Black and Hispanic voters in Arizona, Florida, and North Carolina are no exception with three-fourths of Black voters (77%) and eight in ten Hispanic voters (81%) in these states saying they know someone who has either tested positive for coronavirus or thought they had it, compared to two-thirds of white voters.
Figure 1: At Least Three-Fourths Of Black Voters And Hispanic Voters Say They Know Someone Who Has Had Coronavirus
In addition, nearly four in ten Black (36%) and Hispanic voters (41%) say they have lost a job or income due to the coronavirus compared to three in ten White voters (28%). Black voters are also more likely than White or Hispanic voters to say that both the health impacts and economic impacts of the coronavirus have been “worse for people of color.” Majorities of White voters say the impacts of coronavirus on White people and people of color have been about the same.
Figure 2: Half Of Black Voters In Sun Belt States Say Health And Economic Impacts Of Coronavirus Have Been Worse On People Of Color
With larger shares of Black and Hispanic voters being directly affected by the coronavirus outbreak, it is not surprising that about two-thirds of Black voters (66%) and Hispanic voters (68%) report that worry or stress related to the coronavirus has had a negative impact on their mental health – including three in ten who say it has had a “major impact.” This is compared to 56% of white voters who say the same, including 17% who say it has had a “major impact.”
Figure 3: Three In Ten Black And Hispanic Sun Belt Voters Say Worry Or Stress From Coronavirus Has Had Major Impact On Mental Health
What Is Driving Black Voters and Hispanic voters?
Yet, Black and Hispanic voters in these Sun Belt states are no more likely to say coronavirus is an important issue to their 2020 vote choice than White voters. About one in six Black voters (14%), White voters (16%), and Hispanic voters (15%) say the coronavirus outbreak is the most important issue to their 2020 presidential vote. Other issues, most notably, the economy rank higher. The economy is among the top issues for voters across racial groups but a larger share of Black voters also say race relations (29%) is the top issue driving their 2020 vote choice compared to one in ten White and Hispanic voters (9%). This is in light of recent protests in response to police shootings of unarmed Black Americans and President Trump’s focus on “law and order.”
Table 1: Top Issues In 2020 Presidential Election Among Sun Belt Voters
Percent who say each of the following is the most important issue to their vote:
Total Voters
Black Voters
Hispanic Voters
White Voters
The economy
32%
24%
32%
34%
Criminal justice and policing
17
19
14
18
The coronavirus outbreak
16
14
15
16
Race relations
12
29
9
9
Health care
12
10
17
11
Immigration
5
2
9
5
None of these issues are important
5
2
4
6
Which Candidate Do Black Voters and Hispanic Voters Support?
The majority of Black voters in the Sun Belt states (75%) say they plan on voting for Joe Biden in the November presidential election and few (5%) say they plan on voting for President Trump. This is consistent with Black adults’ views of President Trump throughout his presidency, in which he has never garnered higher than 25% favorability among Black adults in the past 3 and a half years.
Hispanic Voters In Two Key Battlegrounds
Florida and Arizona are two battleground states with Hispanic voters increasingly making up larger shares of the electorate with one in four 2018 voters in Arizona identifying as Hispanic as were two in ten Florida voters.
Now, six in ten Hispanic voters in Arizona say they are either “probably” or “definitely” going to vote for Joe Biden (61%) with 18% say they are going to vote for President Trump, another 16% are undecided. In Florida, Hispanics are more divided but lean in favor of former Vice President Biden. About half of Hispanic voters in Florida (46%) say they plan on voting for Joe Biden while 37% say they plan on voting for President Trump, which is within the margin of sampling error for this small subgroup of voters.
Figure 4: Biden Has Clear Advantage Among Hispanic Voters In Arizona, Florida Hispanic Voters Are More Divided In Their 2020 Vote Choice
There are many reasons why Hispanic voters in Arizona and Florida have different 2020 presidential vote preferences as there are significant demographic differences between the two voting groups including their education levels, their nativity, and their party affiliation.
Figure 5: Demographic Differences Among Arizona And Florida Hispanic Voters
Florida Hispanic voters weren’t always divided in their support for the Democratic and Republican nominees for President. In 2016, the vast majority of Hispanic voters supported Hillary Clinton. Even in the Sun Belt Voices project, only one-fourth of Florida Hispanic voters say they voted for President Trump in the 2016 election (68% say they voted for Hillary Clinton). The poll finds one in ten Florida Hispanic voters (10%) say they voted for Clinton in 2016 and are now voting for President Trump in 2020 while 3% of Hispanic voters saying they vote for Trump in 2016 and are now voting for Biden.
How Voters Plan To Cast Ballots
A previous KFF and The Cook Political Report release analyzed how voters planned to cast ballots in each of the three Sun Belt states. When we look at how people plan to vote among different racial and ethnic groups we find about one-fourth of Black voters saying they plan to vote by mail or absentee (27%) compared to one-third of White voters, and four in ten (39%) Hispanic voters. Black voters, especially in Southern states, have historically been more likely to show up to vote in-person but with the coronavirus pandemic upending usual voting behaviors, it is important to better understand how people plan to vote. The latest data from North Carolina’s State Board of Elections, compiled by Michael McDonald of the University of Florida, finds that while similar shares of White and Black voters have begun returning ballots in North Carolina, the rate at which the ballots are being rejected for error is larger among Black voters.
Table 2: How Black Voters, Hispanic Voters, And White Voters Plan To Cast Their Ballots
Percent who say in the upcoming election, they plan to vote…
Total Voters
Black Voters
Hispanic Voters
White Voters
Planning to vote in-person (NET)
51%
50%
42%
53%
…in-person on Election Day
30
23
30
32
…in-person through early voting
20
27
12
21
Planning to vote by mail or absentee ballot
33
27
39
33
Not sure yet
16
22
20
14
Arizona Crosstabs
Florida Crosstabs
North Carolina Crosstabs
Methodology
The Sun Belt Voices Project was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF) in collaboration with the Cook Political Report. The survey was conducted August 29th – September 13th, 2020, among a representative random sample of 3,479 registered voters in three Sun Belt states (1,298 in Arizona, 1,009 in Florida, and 1,172 in North Carolina). All registered voters included in the sample were sent an invitation letter including a link to complete the survey online, a toll-free number that respondents could call to complete the survey with a telephone interviewer, and $2 pre-incentive. Respondents who were living in Census block-groups identified as low-education and respondents identified as likely Hispanic were offered $10 post-incentive if they completed the survey. All respondents were then sent a reminder postcard, which included a QR code. Respondents who were flagged in the voter file as both a) speaking Spanish and b) speaking either primarily or only their native language, received bilingual mailings, including text in both English and Spanish.
The sample was designed to reach respondents less likely to complete surveys online, by oversampling areas with a relatively low percentage of college graduates. Sample that could be matched to telephone numbers and that had not yet completed the survey online or by inbound computer-assisted telephone interview (CATI) were called by CATI interviewers to attempt to convert this sample to completed interviews. A total of 3,116 respondents completed the questionnaire online, 89 by calling in to complete, and 274 were completed as outbound CATI interviews. Data collection was carried out in English and Spanish by SSRS of Glen Mills, PA. The registered voter sample was provided by L2. KFF paid for all costs associated with the survey.
A series of data quality checks were run on the final data, which resulted in 37 completes being removed from the data. Weighting involved multiple stages: First, each state sample was weighted to account for sampling methodology including the oversampling of low-educational attainment areas and to the proportions of the voter file reachable or unreachable by outbound phone-call. Second, each state’s sample was weighted to match the voter file distribution on gender, age, race/ethnicity, metropolitan status, state region, as well as the 2018 CPS Voter Supplement estimates for educational attainment, including race by education. To address additional non-response among partisans not accounted for by demographics, the weight was adjusted to match registered party identification and both 2018 voter turnout and 2016 voter turnout from voter file. The final weight combined each state’s weight and balanced the combined total sample to state distributions. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 2 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Group
N (unweighted)
M.O.S.E.
Total
3,479
±2 percentage points
Arizona
1,298
±3 percentage points
Florida
1,009
±4 percentage points
North Carolina
1,172
±3 percentage points
Appendix
Appendix Table 1
Percent who say they approve or disapprove of:
Total Voters
Swing Voters
Total Sun Belt Voters
Arizona
Florida
North Carolina
Total Sun Belt Swing Voters
Arizona Swing Voters
Florida Swing Voters
N.C. Swing Voters
Donald Trump
Approve (NET)
48%
46%
48%
48%
45%
46%
45%
47%
Strongly approve
32
31
31
33
7
9
7
7
Somewhat approve
16
15
17
15
38
36
38
40
Disapprove (NET)
52
54
51
52
54
54
54
53
Somewhat disapprove
8
7
8
7
23
21
24
24
Strongly disapprove
44
46
43
45
30
32
30
29
Net approval (percentage points)
-4
-8
-3
-4
-9
-8
-9
-6
Joe Biden
Approve (NET)
50%
50%
51%
50%
56%
52%
60%
52%
Strongly approve
25
22
25
26
7
5
7
7
Somewhat approve
26
28
26
24
50
47
53
44
Disapprove (NET)
49
49
48
50
42
46
39
46
Somewhat disapprove
13
13
13
12
27
30
26
27
Strongly disapprove
36
36
35
37
15
16
12
19
Net approval (percentage points)
+1
+1
+3
0
+14
+6
+21
+6
*Swing voters include those who said they will probably vote for Donald Trump, probably vote for Joe Biden, are undecided, or don’t know who they will vote for in the upcoming election.
Appendix Table 2
Percent who say they trust … to better handle each of the following issues:
Suburban Voters In Arizona, Florida, and North Carolina
On December 27, 2019, the Trump Administration published final regulations that change how ACA Marketplace plans that include coverage for abortion must bill and consumers must pay premiums for that coverage.
The regulations, currently blocked by court orders, will require issuers to send two separate monthly bills: one bill for the non-Hyde abortion coverage (at least $1 per member per month) and one bill for the premium for the coverage of all other services. Consumers will be asked to pay their monthly premium in two separate transactions.
HHS estimates that these regulations will disrupt coverage for many consumers and increase costs for issuers. They also place new administrative and reporting requirements on issuers and add new oversight responsibilities for state insurance regulators.
Currently, one third of ACA enrollees reside in one of 17 states and DC that still offer ACA Marketplace plans that include coverage for abortions. In 6 of those states, abortion coverage is mandated and this regulation is in direct conflict with state law.
Seven states and DC, Planned Parenthood and four individuals represented by the ACLU are challenging the regulations in federal court. Three federal district courts have ruled in favor of the plaintiffs, blocking the implementation of the regulations. The Trump Administration has appealed two of these decisions to the 9th Circuit Court of Appeals, and the 4th Circuit Court of Appeals.
Ultimately, this regulation could further reduce the number of plans that make the abortion coverage available through the ACA Marketplace in states that have not already enacted abortion coverage restrictions.
Introduction
On December 27, 2019, the Trump Administration issued final regulations to address “Exchange Program Integrity.” A major element of the rules affects insurers, consumers, and state insurance regulators in the states that either allow or require abortion coverage. The Affordable Care Act (ACA) allows states to ban plans from offering abortion as a benefit on their Qualified Health Plans (QHPs) and requires plans that cover abortion to segregate policyholder payments for abortion coverage from all other premium charges. The Administration issued the proposed rules in November 2018 and received over 75,000 comments from a range of stakeholders, including insurers, state-based exchanges, state insurance regulators, and consumer advocacy organizations. Many commented that HHS had underestimated the burdens and costs to issuers and consumers. The final regulations maintain most of the elements of the proposed rules with some minor changes. In addition, following the comments, HHS increased its estimates for the costs that these regulations will have for consumers, issuers, and exchanges. This provision was originally slated to become effective June 27, 2020; however, in response to the COVID-19 pandemic, the Center for Medicare and Medicaid Services (CMS) pushed the effective date back by 60 days to August 26, 2020. However, three federal district courts have issued orders blocking the implementation of the regulations.
The Trump administration says the new regulations will be confusing for consumers and burdensome to issuers, but believes it is more consistent with “congressional intent” and is a “better implementation” of the ACA’s statutory requirement for separate payments. These rules could disrupt coverage for many consumers, add to coverage costs, place administrative and reporting requirements on issuers, and add new oversight responsibilities for state insurance regulators. Also, this regulation will likely result in plan decisions (when permitted by state law) to eliminate abortion coverage from their policies in order to avoid additional administrative requirements, placing the costs of abortion care directly on women enrollees and potentially limiting their access to these services. The rule is consistent with ongoing Trump Administration efforts to limit the number of abortions in the U.S. This brief provides an overview of current ACA-related abortion coverage policies, analyzes the potential impact of the new regulations and provides an overview of the legal challenges to the final rule.
How have ACA Marketplace plan policyholders been paying for abortion coverage?
The ACA requires all QHPs to provide coverage for 10 Essential Health Benefits (EHB), but prohibits abortion services from being included as an EHB. States may ban plans offered through the ACA Marketplace from covering any abortions–even if the pregnancy is a result of rape or incest or a threat to the woman’s life as permitted under the Hyde Amendment. Since the ACA was implemented, 26 states have banned abortion coverage on their ACA Marketplace (Figure 1).
Figure 1: In 17 States and DC, at Least One ACA Exchange Plan Offers Benefits that Include Abortion Coverage
As of February 2020, however, six states require abortion coverage in all state regulated plans including all the plans on their ACA Marketplace.1 Eleven states and DC neither ban nor require abortion coverage but offer at least one plan on their ACA Marketplace that includes abortion coverage.
The ACA and the relevant regulatory section requires plans that offer coverage for abortion beyond Hyde limitations to segregate the federal funds used to subsidize premium costs for the EHBs from the premiums costs that pay for that coverage. Plans have been required to collect a separate payment for abortion coverage and notify consumers regarding the inclusion or exclusion of abortion in the Summary of Benefits and Coverage at enrollment. Any plan that includes coverage of abortions beyond Hyde limitations must estimate the actuarial value of such coverage by taking into account the cost of the abortion benefit, but it must be valued at least $1 per enrollee per month. This estimate cannot take into account any savings that might be achieved as a result of the abortions (such as the savings of not paying claims for prenatal care, delivery or postnatal care).
In 2015, the Obama Administration provided guidance on how this statute should be implemented, allowing options that simplified the billing and payment process for plans that include abortion coverage yet kept funds segregated. They allowed insurers to send “the enrollee a single monthly invoice or bill that separately itemizes the premium amount for non-excepted abortion service” or “sending the enrollee a notice at or soon after the time of enrollment that the monthly invoice or bill will include a separate charge for such services and specify the charge.”
In October 2017, the Trump Administration issued a bulletin reinforcing the 2015 notice. They also indicated that the Center for Medicare and Medicaid Services (CMS) would fully enforce the requirements related to abortion coverage in the Federally Facilitated Exchange (FFE) and, if states failed to require compliance in plans offered by the State-Based Exchanges (SBE), CMS would step in. In August 2018, 101 members of Congress signed a letter to Secretary Alex Azar stating their dissatisfaction with the Obama Administration policy, and urging the Trump Administration to issue new regulations that they believe were needed to reflect the intent of the law.
What do the new regulations change?
On December 27, 2019, the Trump Administration published final regulations addressing exchange program integrity that make made significant changes to how issuers must bill and consumers should pay for non-Hyde abortion coverage in Marketplace plans that include abortion coverage. HHS takes the position that the Obama-era regulation fail to consider that “Congress intended that QHP issuers collect two distinct (that is, ‘‘separate’’) payments, one for the coverage of non-Hyde abortion services, and one for coverage of all other services covered under the policy, rather than simply itemizing these two components in a single bill, or notifying the enrollee that the monthly invoice or bill will include a separate charge for these services.”
Under the final rule:
Issuers must send two separate monthly bills, either by mail or electronically to each policyholder: one bill would be for the non-Hyde abortion coverage (at least $1 per member per month) and one bill would be the premium for everything else excluding the non-Hyde abortion coverage. Issuers may send two separate bills in a single envelope, but must send two separate emails if billing electronically.
Consumers will be instructed by the issuer to pay in two separate transactions. If the consumer is paying by mail, the consumer may send two checks in one envelopes or but in the cases where the policyholder pays through electronic funds transfer, the consumers must make two electronic payments.
How could the new regulations affect enrollees and insurers?
HHS projects that the new regulation will cause enrollment to decrease slightly and ACA premiums to increase by up to 1 percent in plan year 2021 and each year thereafter. They also project federal outlays for premium tax credits to increase by about $106 million in 2021 and $96 million in 2022 and
HHS also estimates the separate billing and payment policy will result in significant costs. They project that costs to insurers, state-based exchanges, the federal exchange, and consumers will be about $546.1 million in 2020, $232.1 million in 2021, $230.7 million in 2022, and $229.3 million annually in 2023 and onwards.
Consumers enrolled in 24 States and DC (that do not bar abortion coverage) will be affected, but the impact will be greatest for enrollees residing in the six states that mandate abortion coverage and in the additional 11 states and DC that offer plans with coverage.HHS revised its initial estimate of 1.3 enrollees and now estimates that 3.4 million enrollees to Marketplace plans will be impacted by the regulation (Table 1). HHS estimates that in 2020 consumer costs will total $35.5 million, but this estimate does not factor in the costs to consumers of a separate payment, the potential loss of coverage nor the costs to re-enroll. For all policyholders, HHS estimates that the annual enrollee burden will be approximately 2 million hours with an associated annual cost of approximately $25.1 million.
Table 1: State Abortion Coverage Policies and Enrollment
State Abortion Coverage Rules for QHPs
Number of States
Number of Enrollees
Mandatory in all plans
6
2.3 million
No ban, at least one plan offers abortion coverage
Some consumers will be confused by receiving separate invoices for the same insurance policy and the need to make two separate payments each month. HHS states that sending policyholders two separate bills will cause confusion because they might not understand why they are getting two different bills and why they need to make these payments separately. However, HHS has said that “. . .although policy holders may experience burden related to reading and understanding the separate bills, there are non-quantifiable benefits to policy holders in QHPs covering non-Hyde abortion who hold conscience objections to such coverage or policy holders who seek a better understanding of what their health care dollars are purchasing. HHS continues to believe that, although these changes will increase enrollee burden, this burden is reasonable and justified because it will achieve better alignment of the regulatory requirements for QHP issuer billing of premiums with the separate payment collection requirement in section 1303 of the PPACA.”2
While the final rule allows insurers to send the two bills in one envelope, saving insurers the cost of two mailings, some consumers may not notice two bills sent in the same envelope for the same plan. HHS took the position in the proposed rule that sending two separate bills will reduce consumer confusion because consumers may “inadvertently miss or discard a second paper bill in a single envelope.” In addition, HHS acknowledges that some banks might flag payments as potentially fraudulent because two payments are made in the same day or because one payment is for $1. This could result in the termination for the consumer, and additional costs for issuers.
Men and women who are beyond their reproductive years may be most likely to be confused about the separate bill for abortion coverage. They may think the abortion coverage is a rider and not part of their plan, and decide not to pay the $1 without recognizing that they are making incomplete payments on their full insurance. Abortion coverage is not a rider. In fact, the CMS prohibits plans from selling any coverage riders on the Marketplace and a recent review of insurance plans finds there are no abortion riders available to individuals outside the Marketplace.
Some consumers may fail to pay their premium in full and have their coverage terminated for delinquent payment. The rule states that if a subscriber fails to pay in separate transactions but pays the total amount in one payment, then the issuer is not permitted to cancel the coverage. It does not speak, however, to what issuers should do if the payment is not made in full—that is, if the policyholder pays for the EHB share of the premium but does not make the abortion payment.
What happens when individuals fail to pay some or all of their premiums?
If the premiums are not paid in full, insurers may terminate coverage. The grace period and the timing of the loss of coverage depend on whether the individual qualifies for the federal Alternative Premium Tax Credit (APTC) and state law,
Policyholders who are also eligible for APTC qualify for a three months grace period before their coverage is terminated for incomplete or non-payment. For these policyholders, the issuer must pay for all claims for covered services provided to the policyholder in the first month of the grace period, but may suspend payments for claims for services rendered during the second and third months of the grace period
People not receiving APTC have a much shorter grace period. Currently, the general practice is 31 days but it may vary in each state. Issuers may terminate coverage if a consumer either fails to pay the outstanding premium or an amount that satisfies any applicable premium threshold, before the end of the grace period.
In response to the COVID-19 national emergency, CMS issued guidance stating CMS will exercise enforcement discretion to permit issuers of Qualified Health Plans (QHPs) to extend payment deadline for premiums during the national emergency.
SOURCE: CMS, Health Plan Coverage Effectuation: Payments, Grace Periods, and Terminations, 2019.
When an issuer may begin the termination process for delinquent payments varies. Insurers could terminate coverage if QHP premium payments are not made in full following a grace period. Some insurers may have opted to set a premium threshold, which is a dollar amount or a percentage of the premium that the policyholder may owe before the process to terminate the policy for nonpayment is initiated. The amount the policyholder owes for non-payment is cumulative and over time, even a premium threshold will not be protective for policyholders who may be confused about or unaware they have not paid their premiums in full.
While, HHS has stated that they will not take enforcement action against issuers who do not initiate a grace period and termination for nonpayment in full because of this new policy, they also will not permit issuers to waive the separate premium payment for abortions because policyholders must pay the cost. States have different laws about grace periods, and terminations, and not all states will be able to provide any leeway to issuers to not terminate policyholders who fail to pay the full premium.
HHS will permit issuers to change benefits mid plan year or allow consumers to opt out of abortion coverage, but this will conflict with many states’ laws.
In the preamble to the rule, HHS states in order to mitigate the current lack of transparency for non-Hyde abortion coverage in plans, they will not take enforcement action against issuers of ACA Marketplace plans that “modify the benefits of a plan at the time of enrollment or during a plan year to effectively allow enrollees to opt out of coverage of non-Hyde abortion services by not paying the separate bill for such services.” Because modifying benefit midyear or altering benefits for just some enrollees may be violate state insurance law, HHS is encouraging states and their exchanges to also not take enforcement action against issuers.
It is not clear how issuers could modify plan benefits midyear or change the benefits only for some policyholders, or how issuers would be able to distinguish between consumers opting out and those failing to pay the full premium. Also, this new federal flexibility is in direct conflict with state laws that require abortion coverage to be included in all ACA Marketplace plans, and is contrary to many state insurance regulations on altering benefit packages mid-year.
Some issuers might eliminate abortion coverage from their plans altogether because of the additional cost and administrative requirements. As a result, women enrollees will bear the cost of abortion services, even in states that permit Marketplace plans to offer abortion coverage. To implement this process, issuers will need to establish a protocol for sending two separate bills. HHS has calculated that this would affect 94 issuers with 1,467 plans (representing 32 percent of individual market on-Exchange plans in 21 states and estimated costs per issuer ($4.1 million)) totaling an estimated $385 million for all plans. These estimates do not include the cost of printing the extra bills as well as additional staffing that will be needed to answer enrollee questions and address delinquent payments. Insurers could experience declining enrollment when enrollees default on coverage payments, even when they have the resources to cover the costs.
The preamble to the final regulations specify that plans may take into account the administrative expense of including coverage of non-Hyde abortions in calculating the premiums associated with that abortion coverage. However, this is in direct conflict with the statutory language that states these funds are to be “used exclusively to pay for [abortion] services” not an issuer’s administrative cost of providing that service.3
States that operate their own ACA Marketplaces will face additional costs and new administrative responsibilities.
There are 12 states that face additional impacts because they operate their own state-based ACA Marketplace. HHS estimates the total one-time cost for all 12 State Exchanges affected by these requirements will be approximately $9 million in 2020. Total ongoing costs for all 12 State Exchanges is estimated to be approximately $2.4 million in 2020, $4.8 million in 2021, $3.6 million in 2022 and $2.4 million 2023 onwards. HHS estimates that on average, each of these states will incur in 2020 one-time costs of $750,000 and ongoing annual costs of approximately $200,000 for the six months of implementation in 2020, and $400,000 in 2021. HHS estimates cost will decrease in the following year.
In addition, HHS estimates an additional administrative responsibility for a State Exchange that performs premium billing and payment processing. For all three state exchanges (MA, RI, VT) that perform premium billing and payment processing, HHS estimate the total one-time cost will be 94,500 hours totally approximately $12.3 million for these three exchange to implement the final rule. While many comments for the proposed rule outlined additional expenses for state regulators and exchanges to counter consumer confusion by creating consumer notices, responding to increased demand at call centers, and re-enrolling consumers who are dropped from their insurance, HHS does not include any additional costs for these groups to implement the new regulation.
What is the current availability of abortion coverage in 2020 ACA Marketplaces?
Even before the new regulations were issued, abortion coverage was only available to a minority of ACA plan policyholders. As a result of state decisions to ban abortion coverage and issuers’ choices to exclude abortion coverage where there is no state ban, only one third of enrollees live in a state where abortion coverage is offered in the ACA Marketplace (Figure 2). At the time of the ACA debate about abortion coverage, some experts predicted that imposing these kinds of requirements on plans that cover abortion services would have a chilling effect on abortion coverage. This prediction has been borne out. Seven states have no formal legal ban on abortion coverage, yet no plans are available that offer coverage. The exact reasons why the plans do not offer abortion coverage is not clear.
Figure 2: An Estimated One Third of Enrollees Covered by ACA Marketplace Plans Live in a State Where Abortion Coverage Is Offered
This regulation adds to the challenge of including abortion coverage and it is likely that the newly required payment process will make additional insurers consider dropping abortion coverage to simplify their billing practices and avoid the need for additional paperwork, staffing, reporting, and oversight. Abortion coverage is particularly at risk in DC and the 11 states currently offering plans that cover abortion, but that do not have a mandate. In Colorado and New Jersey, only one issuer on the ACA Marketplace offer abortion coverage and does not offer plans in every county.
What have been the legal challenges to the final rule?
Three federal district courts have ruled in favor of the plaintiffs challenging the regulations, and the Administration is blocked from implementing the regulations. Seven states and DC have filed legal challenges to this final rule alleging irreparable injuries to the states’ sovereign and proprietary interests (Figure 3). California, New York, District of Columbia, Maine, Maryland, Oregon and Vermont filed a lawsuit together in the federal district court in the northern district of California. Washington filed a separate lawsuit in the district court in the eastern district of Washington. The states claim the implementation of the final regulation should be blocked because the regulation:
Figure 3: Legal Challenges to Regulations on Payments for Abortion Coverage in ACA Marketplace Plans
Imposes onerous and unnecessary regulatory barriers aimed at restricting women’s constitutionally protected right to access abortion care;
Seeks to frustrate state sovereignty by coercing states to change their policies relating to the protection of abortion care;
Violates Section 1554 of the ACA, which prohibits the promulgation of any regulation that creates unreasonable barriers to the ability of individuals to obtain appropriate medical care; and
Exceeds HHS’s statutory authority under Section 1303 of the ACA, the section of the law that describes the requirements for segregating premium payments for abortion services.
Planned Parenthood of Maryland and four individual consumers represented by the ACLU also filed a lawsuit in the district court of Maryland. They also allege the Administration violated the Administrative Procedures Act by not adequately quantifying the costs and benefits of the rule, conflicting with Sections 1303 (the and 1554 of the ACA, and providing no opportunity for public comment on the “opt-out” provision included in the final rule but not in the proposed rule.
Rulings in Favor of the Plaintiffs Block the Implementation of the Regulations
On April 9, 2020, the U.S. District Court in the Eastern District of Washington ruled that the regulations clearly conflict with Washington’s Single Invoice State, and “cannot be squared with the ACA’s multiple non-preemption provisions.” The court ruled the regulation invalid and without force in the State of Washington. The Trump Administration has appealed this decision to the 9th Circuit Court of Appeals.
On July 10, 2020, the U.S. District Court for the District of Maryland found the regulations arbitrary and capricious, vacated the regulations and enjoined the enforcement. The Trump Administration has appealed this decision to the 4th Circuit Court of Appeals.
On July 20, 2020, the U.S. District Court in the Northern District of California ruled in favor of the State of California and the five other states, finding that the regulations are arbitrary and capricious.
Looking Forward
This rule is consistent with the Trump Administration’s stated priority to limit abortion access and other regulatory actions that could lead to the erosion of ACA related improvements for women’s health coverage. HHS itself finds that these regulations will likely cause consumer confusion, lead to coverage terminations. Prior experience in other states confirms that insurers could move to drop abortion coverage, further eroding the availability of coverage for a health service that many women rely on. Depending on the outcome of the presidential election, the legal challenges may become moot or may ultimately be decided by the Supreme Court.
Appendix
Appendix Table 1: State Policy on Abortion Coverage in Marketplace Plans
State
State QHP Abortion Coverage Policy in 2020
Availability of Abortion Coverage on Marketplace in 2020
Effectuated Enrollment in Marketplace, 2019
United States
6 states required;18 states & DC Not Banned;26 Banned
Although Oregon law mandates abortion coverage, Providence Health Plan is exempt from the requirement, as they excluded coverage in all individual, small employer, and large employer group plans in 2017. Similarly, Providence Health Plan is exempt in Washington, where state law includes a religious conscience clause. ↩︎
Analysis of Epic Electronic Health Record Data Shows People of Color Fare Worse than White Patients at Every Stage of the COVID-19 Pandemic, Including Higher Rates of Infection, Hospitalization and Death
Disparities in Hospitalization and Death Persist Even after Accounting for Differences in Sociodemographic Factors and Underlying Health Conditions, And People of Color are Sicker When They Test Positive
People of color were more likely to test positive for COVID-19 and to require a higher level of care at the time of diagnosis compared to White patients, according to a new analysis from Epic Health Research Network and KFF. They also were more likely to be hospitalized and die from the novel coronavirus than White patients were.
The racial disparities in illness and death are not fully explained by differences in underlying sociodemographic characteristics and health conditions, finds the study, which analyzed Epic electronic health record data for roughly 50 million patients from 53 health systems representing 399 hospitals across 21 states.
The findings suggest that people of color may face increased barriers to testing that contribute to delays in obtaining testing until they are in more serious condition compared to White patients. They also demonstrate that people of color are bearing a disproportionate burden of negative health outcomes related to the COVID-19 pandemic at every stage – risk of exposure, access to testing, severity of illness, and likelihood of death.
The analysis, a joint project of EHRN and KFF, builds upon the findings of other studies and contributes to the research by providing insight into the experiences of a large patient population across a range of states and health systems, examining variation in the level of care patients required at the time they tested positive for COVID-19 by race and ethnicity, and assessing the extent to which underlying sociodemographic characteristics and health conditions explain racial disparities in hospitalization and death.
Key findings include:
Although testing rates differed little by race and ethnicity, among those tested, Hispanic patients were over two-and-a-half times more likely to have a positive result (311 per 1,000) and Black and Asian patients were nearly twice as likely to test positive (219 and 220 per 1,000, respectively) for COVID-19 compared to White patients (113 per 1,000). Further, larger shares of Black, Hispanic, and Asian patients were in an inpatient setting when they tested positive for COVID-19 compared to White patients. They also were more likely to require oxygen or ventilation at the time of diagnosis.
COVID-19 infection rates among Hispanic and Black patients were over three and two times higher, respectively, compared to the rate for White patients (143 and 107 vs. 46 per 10,000).
Hospitalization rates for Hispanic and Black patients with COVID-19 were more than four times and over three times higher, respectively, compared to the rate for White patients (30.4 and 24.6 vs. 7.4 per 10,000). Death rates for both groups were over twice as high as the rate for White patients (5.6 and 5.6 compared to 2.3 per 10,000). Asian patients also faced significant disparities in these measures.
Among patients who tested positive for COVID-19, Black, Hispanic, and Asian patients remained at higher risk for hospitalization and death compared to White patients with similar sociodemographic characteristics and underlying health conditions, suggesting that other barriers, including racism and discrimination, are affecting outcomes through avenues not captured by these measures.
“Understanding the factors underlying COVID-19 infections and severe complications can help us devote resources appropriately to the most vulnerable communities,” said Christopher Alban, MD, Epic Vice President of Clinical Informatics. “This study adds nuance to our understanding of inequities in our COVID-19 response by showing racial and ethnic disparities that persist when comparing populations with similar health and socioeconomic status.”
“This analysis points to delays in testing for people of color, who are sicker and more likely to be infected when they do get tested,” said KFF President and CEO Drew Altman. “The findings highlight the continued importance of addressing racial disparities in responding to COVID-19 as in health care more broadly.”
About Epic Health Research Network
EHRN is a journal for the 21st century, designed for rapid sharing of knowledge with healthcare professionals, researchers, government, and learners to help solve medical problems. For more information, visit ehrn.org.
About KFF
Filling the need for trusted information on national health issues, KFF (Kaiser Family Foundation) is a nonprofit organization based in San Francisco, California. KFF is not affiliated with Kaiser Permanente.
This analysis builds on a continually growing body of research on racial disparities in COVID-19 by examining testing, infection, hospitalization, and death by race and ethnicity among patients in the Epic health record system. It contributes to the research in this area by providing insight into the experiences of a large patient population across a range of states and health systems, examining variation in the level of care patients required at the time they tested positive for COVID-19 by race and ethnicity, and assessing the extent to which underlying sociodemographic characteristics and health conditions explain racial disparities in hospitalization and death. Overall, it shows that, despite being at increased risk of exposure to the virus, people of color did not have markedly higher testing rates compared to White patients and were more likely to be positive when tested and to require a higher level of care at the time they tested positive. Moreover, it builds on previous research showing people of color have higher rates of hospitalization and death due to COVID-19 by finding that these disparities persist after controlling for sociodemographic characteristics and underlying health conditions. Key findings include:
Differences in testing rates by race and ethnicity were small, but people of color were more likely, compared to White patients, to be positive when tested and to require a higher level of care at the time they tested positive for COVID-19. Although there were not large differences in testing by race and ethnicity, among those tested, Hispanic patients were over two and a half times more likely to have a positive result (311 per 1,000) and Black and Asian patients were nearly twice as likely to test positive (219 and 220 per 1,000, respectively) compared to White patients (113 per 1,000). Further, larger shares of Black, Hispanic, and Asian patients were in an inpatient setting when they tested positive for COVID-19 compared to White patients, and they also were more likely to require oxygen or ventilation at the time of diagnosis.
Black, Hispanic, and Asian patients had significantly higher rates of infection, hospitalization, and death compared to their White counterparts. The infection rate for Hispanic patients was over three times higher than the rate in White patients (143 vs. 46 per 10,000), and the rate among Black patients was over two times as high (107 per 10,000). The hospitalization rate for Hispanic patients was more than four times as high as the rate in White patients (30.4 vs. 7.4 per 10,000), and the rate in Black patients was over three times as high (24.6 per 10,000). Death rates for both groups were over twice as high as the rate for White patients (5.6 and 5.6 compared to 2.3 per 10,000). Asian patients also faced significant disparities in these measures.
Racial disparities in hospitalization and death persisted among positive patients even after controlling for certain sociodemographic factors and underlying differences in health, with Asian patients exhibiting the highest relative risk. Among patients who tested positive for COVID-19, Black, Hispanic, and Asian patients remained at higher risk for hospitalization and death compared to White patients with similar sociodemographic characteristics and underlying health conditions. Asian patients were at the highest risk relative to White patients, followed by Hispanic and Black patients.
As previously documented, the higher infection rate among people of color likely reflects their increased risk of exposure to coronavirus due to their work, living, and transportation situations. They are more likely to be working in low-income jobs that cannot be done from home, to be living in larger households in densely populated areas, and to utilize public or shared modes of transportation. Despite being at increased risk of exposure to the virus, people of color did not have markedly higher testing rates compared to White patients and were more likely to be positive when tested and to require a higher level of care at the time they tested positive for COVID-19. These findings suggest that people of color may face increased barriers to testing that contribute to delays in them obtaining testing until they are in more serious condition.
The higher hospitalization and death rates among patients of color, in part, reflect higher infection rates and higher rates of underlying health conditions as well as social and economic inequities and barriers to care. However, the persistence of disparities after controlling for COVID-19 infection, certain sociodemographic factors, and underlying health conditions show that differences in these underlying factors do not fully explain the disparities in hospitalization and death. This finding suggests that other factors, including racism and discrimination, are negatively affecting their health outcomes through additional avenues.
Together, the findings point to the importance of considering health equity in COVID-19 response and relief efforts and health care more broadly, and, in particular, improving access to testing before individuals develop severe illness in order to slow the spread of infections. They also illustrate the importance of considering a wide array of factors both within and beyond the health care system and addressing structural and systemic racism and discrimination as root causes as part of efforts to address health disparities. These efforts will be key for narrowing the disparate effects of COVID-19, ensuring equitable distribution of treatments and a vaccine as they are developed, and preventing widening disparities in health care more broadly looking forward.
Issue Brief
Introduction
A continually growing body of research consistently shows people of color are bearing a disproportionate burden of COVID-19 cases, deaths, and hospitalizations and that they may face barriers to testing. For example, KFF analysis of state reported data shows that Black individuals account for more cases and deaths relative to their share of the population in most states reporting data. Other analysis of state-reported data finds higher mortality rates among Black and American Indian and Alaska Native (AIAN) people, disparities for Asian and Native Hawaiian and Pacific Islander (NHOPI) individuals in certain areas, and a recent rise in mortality rates for NHOPI and Hispanic people. Data also show that Black, Hispanic, and AIAN people are at increased risk of hospitalization due to COVID-19. Information on testing by race and ethnicity has been limited but suggests people of color may face increased barriers to testing.
This analysis builds on this body of research by examining COVID-19 testing, infection, hospitalization, and death as of July 2020 by race and ethnicity among active patients in the Epic health record system, which includes 53 health systems representing 399 hospitals across 21 states (see Methods for more details). It contributes to the research in this area by providing insight into the experiences of a large patient population across a range of states and health systems, examining variation in the acuity of patients by race and ethnicity at the time they test positive for COVID-19, and assessing whether racial disparities in hospitalization and death persist after controlling for sociodemographic characteristics and underlying health conditions.
Overview of the Epic Patient Population
The analysis is based on Epic Health Research Network (EHRN) and KFF analysis of data for roughly 50 million patients in the Epic health record system who have interacted with the health system in the past two years and have known race and ethnicity. Findings are presented for Black, Hispanic, Asian, and White patients. Due to data limitations, we do not present findings for smaller population groups, including AIAN and NHOPI patients, or people who report multiple races. As availability of data for smaller population groups increases over time, it may allow for future analyses focused on the experiences of these populations.
The Epic active patient population includes somewhat higher shares of Black and White patients and lower shares of Hispanic and Asian patients compared to the total U.S. population. For example, among the Epic active patient population, 15% of patients are Black, 10% are Hispanic, 3% are Asian and 69% are White. Among the total U.S. population, 13% of individuals are Black, 19% are Hispanic, 6% are Asian, and 60% are White. Just over half of the active patient population is female (54%), similar to the share of the overall U.S. population (51%). The active patient population includes a smaller share of children under age 19 compared to the total population (13% vs. 24%) and a larger share of adults age 65 or older (24% vs. 16%).
Key Findings
We examined overall rates of testing, infection, hospitalization and death associated with COVID-19 among the total active population by race and ethnicity. In addition, we assessed the share of positive cases among individuals tested and the level of care individuals required at the time they tested positive by race/ethnicity.
Testing, Positivity Rates, and Level of Care at Time Tested
There were small differences in rates of testing by race and ethnicity. Black and Hispanic patients were slightly more likely to be tested compared to White patients (489 and 461 vs. 408 per 10,000) while the testing rate among Asian patients was lower compared to White patients (345 vs. 408 per 10,000) (Figure 1).
Figure 1: COVID-19 Testing Rate among Active Epic Patients by Race/Ethnicity, as of July 2020
Among those tested, Black, Hispanic, and Asian patients were more likely than White patients to test positive for the virus. Hispanic patients had the highest positivity rate, which was over two and half times higher than the rate for White patients (311 vs. 113 per 1,000) (Figure 2). Black and Asian patients were nearly twice as likely to test positive (219 and 220 per 1,000, respectively) compared to White patients (113 per 1,000).
Figure 2: Positive COVID-19 Test Rate Among Active Epic Patients by Race/Ethnicity, as of July 2020
Black, Hispanic, and Asian patients also required a higher level of care at the time they tested positive for COVID-19 compared to White patients. Larger shares of Black, Hispanic, and Asian patients were in an inpatient setting when they tested positive for COVID-19 compared to White patients (Figure 3). They also were more likely to require oxygen or ventilation at the time of they tested positive.
Figure 3: Level of Care at Time Patient Tested Positive for COVID-19 among Active Epic Patients by Race/Ethnicity, as of July 2020
Infection, Hospitalization, and Death Rates
Overall, Black, Hispanic, and Asian patients had significantly higher rates of infection compared to White patients. Infection rates among Black and Hispanic patients were over two and three times higher, respectively, compared to the rate for White patients (107 and 143 vs. 46 per 10,000) (Figure 4). The infection rate among Asian patients was also significantly higher than the rate for White patients (76 vs. 46 per 10,000).
Figure 4: COVID-19 Cases among Active Epic Patients by Race/Ethnicity, as of July 2020
Black, Hispanic, and Asian patients also had significantly higher rates of hospitalization and death due to COVID-19 compared to White patients. The hospitalization rates for Black and Hispanic patients were over three and four times higher, respectively, compared to the rate for White patients (24.6 and 30.4 vs. 7.4 per 10,000), and their death rates were over twice as high as the rate for White patients (5.6 and 5.6 vs. 2.3 per 10,000) (Figure 5). Asian patients also faced significant disparities in these measures.
Figure 5: COVID-19 Hospitalization and Death Rates among Active Epic Patients by Race/Ethnicity, as of July 2020
Risk of Hospitalization and Death by Race/Ethnicity
Building on our examination of hospitalization and death rates, we conducted statistical analysis to assess whether racial disparities in hospitalization and death persist after controlling for certain sociodemographic characteristics and underlying conditions that are known to increase risk of illness and death. This analysis provides insight into the extent to which racial disparities in hospitalization and death are explained by differences in these underlying factors.
In this analysis, we controlled for age, sex, and health conditions that a previous EHRN analysis had identified as being significantly associated with higher risk of hospitalization and death (including, hypertension, diabetes, heart failure, chronic obstructive pulmonary disease (COPD), cerebrovascular disease or stroke, and obesity). We also controlled for social vulnerability based on where each person lives, using the CDC’s Social Vulnerability Index. The CDC’s Social Vulnerability Index identifies the level of social vulnerability associated with a census area based on 15 social factors, including poverty, income, employment, education, age, household composition, housing, transportation, and racial/ethnic distribution. It was developed to help public health officials and emergency response planners identify and map the communities that will most likely need support before, during, and after a hazardous event.
Among patients who tested positive for COVID-19, people of color remained at increased risk for hospitalization and death after controlling for sociodemographic factors and underlying health conditions. Asian patients were at the highest risk relative to White patients, followed by Hispanic and Black patients. Specifically, Asian patients were 57% more likely to be hospitalized and 49% more likely to die than White patients with the same age, sex, social vulnerability, and comorbidities (Figure 6). Similarly, Hispanic patients were 53% and 30% more likely to be hospitalized and die compared to White patients with similar characteristics and underlying health conditions, and Black patients were 33% and 19% more likely to be hospitalized and die after controlling for these factors. These findings show that differences in these underlying sociodemographic factors and health conditions do not fully explain the higher rates of hospitalization and death experienced by people of color. They suggest that other factors, including racism and discrimination, are negatively affecting COVID-19 health outcomes through additional avenues that are not captured by these measures, as discussed further below.
Figure 6: Risk of Hospitalization and Death among Epic Patients who Tested Positive for COVID-19
Implications
Consistent with other research, these findings show that, among patients across a range of health systems and states, people of color were at significantly increased risk for infection from coronavirus compared to their White counterparts. As previously documented, people of color face increased risk of exposure to coronavirus due to their living, working, and transportation situations. They are more likely to be working in low-income jobs that cannot be done from home, to be living in larger households in densely populated areas, and to utilize public or shared modes of transportation.
Despite being at increased risk of exposure to the virus, people of color did not have markedly higher testing rates compared to White patients and were more likely to be positive when tested and to require a higher level of care at the time they tested positive for COVID-19. These findings suggest that people of color may face increased barriers to testing that contribute to delays in them obtaining testing until they are in more serious condition compared to White patients. Other research suggests that people of color may face longer wait and travel times to access testing and have more limited access to testing within their neighborhood. Moreover, people of color are more likely to be uninsured and to face other barriers to health care, which may contribute to delays in obtaining testing or treatment. The findings from this analysis may understate barriers to testing as they represent active patients who are already connected to a health care system. Individuals who are not connected to a health system or provider may face further barriers to testing and care.
The findings build on previous studies that show people of color are at significantly increased risk for hospitalization and death due to COVID-19 and that these disparities persist after controlling for sociodemographic characteristics and underlying health conditions. These findings, in part, reflect their higher infection rates and higher rates of underlying health conditions that increase their risk of experiencing serious illness if they are infected with the virus. They also may reflect increased barriers to care, which can result in them delaying care and ultimately experiencing more serious conditions. However, this analysis further shows that racial disparities persist among patients who tested positive for COVID-19 after controlling for age, sex, social vulnerability, and comorbidities. Given that a wide body of research has demonstrated that racial health disparities are not driven by biologic differences, this finding suggests that there are other ways racism and discrimination may be negatively affecting COVID-19 health outcomes that are not captured by these measures. For example, research shows that people of color receive poorer quality of care. It also shows that the health care system’s historic mistreatment and abuse of communities of color and ongoing bias and discrimination among providers contribute to negative patient experiences and mistrust of the health care system. Research further suggests that chronic exposure to racism and discrimination create physiological or hormonal responses that negatively affect health (i.e., weathering).
In sum, consistent with a growing body of research, these findings show that people of color are bearing a disproportionate burden of negative health outcomes related to the COVID-19 pandemic at every stage – rates of infection, access to testing, and severity of illness and death. Other analysis also shows that the pandemic is taking a larger economic toll on people of color. While these disparities, in part, reflect social and economic inequities and underlying differences in health, the findings also show that they are not fully explained by these differences. Together, the findings point to the importance of considering health equity in COVID-19 response and relief efforts and health care more broadly, and, in particular, improving access to testing before individuals develop severe illness in order to slow the spread of infections. They also illustrate the importance of efforts to address disparities considering a wide array of factors both within and beyond the health care system and addressing structural and systemic racism and discrimination as root causes. These efforts will be key for narrowing the disparate effects of COVID-19, ensuring equitable distribution of treatments and a vaccine as they are developed, and preventing widening disparities in health care more broadly looking forward.
Methods
The analysis is based on EHRN and KFF analysis of data from the Epic health record system, which includes data for patients from 53 health systems representing 399 hospitals across 21 states. Overall, the system includes data for roughly 55 million active patients. Active patients include those who have interacted with the health system in the past two years, as indicated by either a face-to-face visit or an order placed in their chart. The analysis was restricted to the 89% of active patients who had known race/ethnicity, resulting in a total of roughly 50 million active patients included in the analysis.
The analysis presents findings for Black, Hispanic, Asian, and White patients. Due to data limitations, we do not present findings for smaller population groups, including AIAN and NHOPI patients, or people who report multiple races. As availability of data for smaller population groups increase over time, it may allow for future analysis focused on the experiences of these populations.
We examined testing, infection, hospitalization, and death rates related to COVID-19 among active patients. In addition, we identified the level of care required at the time a patient tested positive for COVID-19 by race and ethnicity.
Further, we performed statistical analysis using data from 332,956 people who tested positive for COVID-19 to examine increased risk of hospitalization and death for Black, Hispanic, and Asian patients relative to White patients after controlling certain sociodemographic characteristics and health conditions known to increase risk of illness and death.
Specifically, we controlled for age, sex, and health conditions that a previous EHRN analysis had identified as being significantly associated with higher risk of hospitalization and death. These conditions included hypertension, diabetes, heart failure, chronic obstructive pulmonary disease (COPD), cerebrovascular disease or stroke, and obesity. The prior EHRN analysis also suggested a significant risk for patients who were immunocompromised. However, that condition was not included in the model due to continued refinements in the definition of an immunocompromised state. In addition, we controlled for social vulnerability based on where each person lives, using the CDC’s Social Vulnerability Index. The CDC’s Social Vulnerability Index identifies the level of social vulnerability associated with a census area based on 15 social factors, including poverty, income, employment, education, age, household composition, housing, transportation, and racial/ethnic distribution. It was developed to help public health officials and emergency response planners identify and map the communities that will most likely need support before, during, and after a hazardous event. Statistical controls were performed using Cox Proportional Hazards models using 95% confidence intervals.
Lily Rubin-Miller, MPH, Christopher Alban, MD, MBA and Sean Sullivan, MS, MPH are with the Epic Health Research Network. Samantha Artiga, MHSA is with KFF.
A new KFF brief provides a comprehensive overview of the coverage and use of fertility services in the United States, highlighting cost and insurance coverage gaps as key barriers faced by low-income people, Black and Hispanic people, LGBTQ individuals, infertile couples and single individuals seeking these services.
The coronavirus pandemic has worsened the availability of medical services and the financial situations of many Americans. Utilization of fertility services has declined, and medical professional societies issued guidelines earlier this year to stop new fertility treatment cycles, non-urgent diagnostic procedures and the criteria to resume such care. However, even before the pandemic several populations experienced disparities in access to such services.
Most patients pay out of pocket for fertility services which typically range in costs based on treatment and duration from the low thousands to tens of thousands of dollars. There is limited coverage of such services by private insurance plans and Medicaid. Fifteen states have laws requiring certain private insurers to cover some infertility treatments and these laws vary widely in the populations eligible and services covered. Only one state, New York, requires its Medicaid program to cover fertility treatment and eight states cover some diagnostic services. Additionally, surveys indicate that about 1 in 5 employers cover some form of infertility treatments.
Many people require fertility assistance. This includes men and women with infertility, many LGBTQ individuals, and single individuals who desire to raise children. An estimated 10% of women report that they or their partners have ever received medical help to become pregnant.
Despite a need for fertility services, fertility care in the U.S. is inaccessible to many due to the cost. More often than not, fertility services are not covered by public or private insurers. Fifteen states require some private insurers to cover some fertility treatment, but significant gaps in coverage remain. Only one state Medicaid program covers any fertility treatment, and no Medicaid program covers artificial insemination or in-vitro fertilization.
Most patients pay out of pocket for fertility treatment, which can amount to well over $10,000 depending on the services received. This means that in the absence of insurance coverage, fertility care is out of reach for many people.
Fewer Black and Hispanic women report ever having used medical services to become pregnant than White women. This is a result of many factors, including lower incomes on average among Black and Hispanic women as well as barriers and misconceptions that may dissuade women from seeking assistance with fertility.
LGBTQ individuals also face heightened barriers to accessing fertility care, as they often do not meet definitions of “infertility” that would qualify them for covered services. Transgender individuals undergoing gender-affirming care may also not meet criteria for “iatrogenic infertility” that would qualify them for covered fertility preservation.
Introduction
Many people require fertility assistance to have children. This could either be due to a diagnosis of infertility, or because they are in a same-sex relationship or single and desire children. While there are several forms of fertility assistance, many services are out of reach for most people because of cost. Fertility treatments are expensive and often are not covered by insurance. While some private insurance plans cover diagnostic services, there is very little coverage for treatment services such as IUI and IVF, which are more expensive. Most people who use fertility services must pay out of pocket, with costs often reaching thousands of dollars. Very few states require private insurance plans to cover infertility services and only one state requires coverage under Medicaid, the health coverage program for low-income people. This widens the gap for low-income people, even when they have health coverage. This brief examines how access to fertility services, both diagnostic and treatment, varies across the U.S., based on state regulations, insurance type, income level and patient demographics.
Diagnosis and Treatment Services
Infertility is most commonly defined1 as the inability to achieve pregnancy after 1 year of regular, unprotected heterosexual intercourse, and affects an estimated 10-15% of heterosexual couples. Both female and male factors contribute to infertility, including problems with ovulation (when the ovary releases an egg), structural problems with the uterus or fallopian tubes, problems with sperm quality or motility, and hormonal factors (Figure 1). About 25% of the time, infertility is caused by more than one factor, and in about 10% of cases infertility is unexplained. Infertility estimates, however do not account for LGBTQ or single individuals who may also need fertility assistance for family building. Therefore, there are varied reasons that may prompt individuals to seek fertility care.
Figure 1: There Are Multiple Reasons Someone May seek Fertility Assistance
A broad array of diagnostic and treatment services may be necessary to assist in fertility (Table 1). Diagnostics typically include lab tests, a semen analysis and imaging studies or procedures of the reproductive organs. If a probable cause of infertility is identified, treatment is often directed at addressing the source of the problem. For example, if someone has abnormal thyroid hormone levels, thyroid medications may help the patient achieve pregnancy. If a patient has large fibroids distorting the uterine cavity, surgical removal of these benign tumors may allow for future pregnancy. Other times, other interventions are needed to help the patient achieve pregnancy. For example, if a semen analysis reveals poor sperm motility or the fallopian tubes are blocked, the sperm will not be able to fertilize the egg, and intrauterine insemination (IUI) or in-vitro fertilization (IVF) may be necessary. These procedures also facilitate family building for LGBTQ and single individuals, with use of donor egg or sperm, with or without a gestational carrier (surrogacy).
NOTES: This is not an exhaustive list of infertility services.SOURCE: ACOG. Evaluating Infertility. 2017; ACOG. Treating Infertility. 2019; American Society for Reproductive Medicine. Infertility: An Overview. Patient Information Series. 2017
Utilization of Fertility Services
Our analysis of the 2015-2017 National Survey of Family Growth (NSFG) finds that 10% of women2 ages 18-49 say they or their partner have ever talked to a doctor about ways to help them become pregnant (data not shown).3 Among women ages 18-49, the most commonly reported service is fertility advice (Figure 2).
Figure 2: Women and Their Partners Seek Various Fertility Services to Help Become Pregnant
The CDC finds that use of IVF has steadily increased since its first successful birth in 1981. According to the most recent data, an estimated 1.8% of U.S. infants are conceived annually using assisted reproductive technology (ART) (e.g., IVF and related procedures).4 The proportions are highest in the Northeast (MA 4.7%, CN 3.9%, NJ 3.9%), and lower in the South and Southwest (NM 0.4%, AR 0.6%, MS 0.6%).
Utilization of fertility services has dropped drastically during the COVID-19 public health emergency. On March 17, 2020 the American Society for Reproductive Medicine (ASRM) issued guidelines to stop all new fertility treatment cycles and non-urgent diagnostic procedures. Since then, ASRM has provided updated guidance on what conditions should be met and measures should be taken before safely resuming fertility care. During this time, a study by Strata Decision Technology of 228 hospitals across 40 states found patient encounters for infertility services were down 83% from March 22 to April 4, 2020 compared to this time the year prior.
Cost of Services
Many patients lack access to fertility services, largely due to its high cost and limited coverage by private insurance and Medicaid. As a result, many people who use fertility services must pay out of pocket, even if they are otherwise insured. Out of pocket costs vary widely depending on the patient, state of residence, provider and insurance plan. Generally, diagnostic lab tests, semen analysis and ultrasounds are less expensive than diagnostic procedures (e.g., HSG) or surgery (e.g., hysteroscopy, laparoscopy). Meanwhile treatment using fertility medications is less expensive than IUI and IVF, but even the less costly treatments can still result in thousands of dollars of out of pocket costs. Many people must try multiple treatments before they or their partner can achieve a pregnancy (typically medication first, followed by surgery or fertility procedures if medications are unsuccessful). A study of nearly 400 women undergoing fertility care in Northern California demonstrates this overall trend, with the lowest out of pocket spending on treatment with medication only and the highest costs for IVF services (Figure 3). Prior research showed the cost of just one standard cycle of IVF was approximately $12,500 in 2009, but is likely higher today due to rising health care costs overall. Furthermore, many patients require several rounds of treatment before achieving a pregnancy, with costs accruing each cycle making these interventions financially inaccessible for many. In addition to costs for the actual treatment, patients can be saddled with out of pocket expenses for office visits, diagnostic tests/procedures, genetic testing, donor sperm/egg use and storage fees and wages lost from time off work.
Figure 3: Fertility Treatments Typically Cost Patients Thousands of Dollars
Insurance Coverage
Insurance coverage of fertility services varies by the state in which the person lives and, for people with employer-sponsored insurance, the size of their employer. Many fertility treatments are not considered “medically necessary” by insurance companies, so they are not typically covered by private insurance plans or Medicaid programs. When coverage is available, certain types of fertility services (e.g., testing) are more likely to be covered than others (e.g., IVF). A handful of states require coverage of fertility services for some fully-insured private plans, which are regulated by the state. These requirements, however, do not apply to health plans that are administered and funded directly by employers (self-funded plans) which cover six in ten (61%) workers with employer-sponsored health insurance. States also have purview over the benefits covered by their Medicaid programs. The federal government has authority over benefit requirements in federal health coverage programs, including Medicare, the Indian Health Service (IHS) and military health coverage.
Private Insurance
Fifteen states have laws in effect requiring certain health plans to cover at least some infertility treatments (a “mandate to cover”) (Figure 4). Additionally, Colorado recently enacted a requirement for individual and group health benefit plans to cover infertility diagnosis, treatment and fertility preservation for iatrogenic infertility, effective January 2022. Among states that do not have a mandate to cover, nine states5 and DC have a benchmark plan that includes coverage for at least some infertility services (diagnosis and/or treatment) for most individual and small group plans sold in that state.6 Two states (CA and TX7 ) require group health plans to offer at least one policy with infertility coverage (a “mandate to offer”), but employers are not required to choose these plans.
Figure 4: Most States Do Not Require Private Insurers to Provide Infertility Benefits
However, in states with “mandate to cover” laws, these only apply to certain insurers, for certain treatment services and for certain patients, and in some states have monetary caps on costs they must cover (Appendix 1). For example, in OH and WV, the requirement to cover infertility services only applies to health maintenance organizations (HMOs). In other states, almost all insurers and HMOs are included in the mandate. Many states provide exemptions for small employers (<50 employees) or religious employers. In addition, state laws do not apply to self-funded (or self-insured) employer plans, which are regulated by federal law. Sixty-one percent of covered workers are enrolled in a self-funded plan.
Even in states with coverage laws, not all patients are eligible for infertility treatment. In HI, someone with unexplained infertility only qualifies for IVF after five years of infertility. In others, patients are eligible after 1 year. Some states place age limits on female patients who can access these services (e.g., ineligible if 46 or older in NJ or if under age 25 or older than 42 in RI). Others place restrictions based on marital status; for example, until May 2020, IVF benefits were only available to married women in MD. Recently enacted legislation now expands coverage to unmarried women. Additionally, it is not always made clear if LGBTQ individuals meet eligibility criteria for these benefits, without a diagnosis of infertility. Furthermore, many costs associated with surrogacy are often not covered by insurance.
States also vary in which treatment services they require plans to cover. Some states mandate insurers to cover cryopreservation for persons with iatrogenic infertility, while others do not. Four states with insurer mandates do not cover IVF. Eleven states do, but with a dollar limit on coverage (e.g., $15,000 lifetime max in AR and $100,000 in MD and RI) or a limit on the number of cycles they will cover (e.g., one cycle of IVF in HI and three cycles in NY).
Do state mandates for IVF coverage affect use of services?
IVF utilization appears to be higher in states with mandated IVF coverage. CDC data from 2016 showed that in three of the four states deemed by the CDC to have “comprehensive coverage”8 for IVF (IL, MA, NH), use of assisted reproductive technology was 1.5 times higher than the national rate. Similarly, a national study found that IVF availability and utilization9 were significantly higher in states with mandated IVF coverage. A study in MA found IVF utilization increased after implementation of their IVF mandate, but overutilization by patients with a low chance of pregnancy success was not found. State level mandates can also help reduce inequities in access. For example, a recent bill proposed in the CA legislature would reverse existing limitations on fertility coverage and make the benefit available to single women and women in same sex relationships.
What does it cost to cover fertility benefits?
While the costs of fertility treatments can be very expensive for those who lack coverage, the cost of covering fertility benefits varies depending on the services covered and utilization with implications for state budgets, employers, and policy holders. For example, in 2019, New York passed a bill to require IVF and fertility preservation services for comprehensive private health insurance policies. The New York State Department of Financial Services estimated that premiums would increase 0.5% to 1.1% due to mandating IVF coverage, and 0.02% for mandating fertility preservation for iatrogenic infertility (caused by medical treatments).
An analysis of a bill proposed in CA to require private plans and Medi-Cal managed care plans to cover IVF services estimated that per member per month premiums would increase by approximately $5 in the private market and less than a $1.00 for Medi-Cal plans. Overall though, out of pocket spending for individuals seeking services would decrease substantially.
Data from MA, CT and RI suggest that mandating coverage does not appear to raise premiums significantly. All three states have been mandating infertility benefits for over 30 years, and estimate the cost of infertility coverage to be less than 1% of total premium costs. In 2017, California was considering a more limited bill that would require fertility preservation for iatrogenic infertility in certain individual and group health plans. As the bill was introduced, it was estimated to result in a net annual increase of $2,197,000 in premium costs or 0.0015% for enrollees in plans subject to the mandate.
While these costs could be modest in comparison to the costs of paying out-of-pocket for these services, there are other costs to coverage mandates. The ACA requires states to offset some of the costs for any state mandated benefits beyond essential health benefits (EHBs) in the individual and small group market. This requirement was estimated to cost NY $59 to $69 million per year if covering one cycle or $98 to $116 million per year if covering unlimited cycles of IVF.
What share of employers offer fertility benefits?
Large employers are more likely than smaller employers to include fertility benefits in their employer-sponsored health plans. According to Mercer’s 2017 National Survey of Employer-Sponsored Health Plans, 56% of employers with 500 or more employees cover some type of fertility service, but most do not cover treatment services such as IVF, IUI, or egg freezing. Coverage is higher for diagnostic evaluations and fertility drugs. Coverage is more common among the largest employers and those that offer higher wages (Figure 5).
Figure 5: Large Employers More Often Cover Fertility Benefits Than Smaller Employers
Public Coverage
Medicaid
NSFG data show that significantly fewer women with Medicaid have ever used medical services to help become pregnant compared to women with private insurance. As of January 2020, our analysis of Medicaid policies and benefits reveal only one state, New York, specifically requires their Medicaid program to cover fertility treatment (limited to 3 cycles of fertility drugs) (Figure 6). However, some states may require Medicaid to cover treatments for conditions that impact fertility, while not directly stated in their policies. For example, states may cover thyroid medications, or cover surgery for fibroids, endometriosis or other gynecologic abnormalities if causing pelvic pain, abnormal bleeding or another medical problem, other than infertility. No state Medicaid program currently covers artificial insemination (IUI), IVF, or cryopreservation (Appendix 2).
Some states specifically cover infertility diagnostic services; GA, HI, MA, MI, MN, NH, NM and NY all offer at least one Medicaid plan with this benefit, but the range of diagnostics covered varies. For example, New York Medicaid specifically covers office visits, HSGs, pelvic ultrasounds and blood tests for infertility. Meanwhile, the infertility assessment covered by Georgia Medicaid includes lab testing, but not imaging or procedural diagnostics. Other states specifically do not cover infertility diagnostics, or more generally do not cover “infertility services,” which likely includes diagnostics. Others do not mention infertility diagnostics in their Medicaid policies, meaning the beneficiary would need to check with their Medicaid program to see if these services are covered (Appendix 2).
The Medicaid program’s lack of coverage of fertility assistance has a disproportionate impact on women of color. Among reproductive age women, the program covers three in ten (30%) who are Black and one quarter who are Hispanic (26%), compared to 15% who are White. Because eligibility for Medicaid is based on being low-income, people enrolled in the program likely could not afford to pay for services out of pocket.
The relative lack of Medicaid coverage for fertility services stands in stark contrast to Medicaid coverage for maternity care and family planning services. Nearly half of births in the U.S. are financed by Medicaid, and the program finances the majority of publicly-funded family planning services. Therefore, while there is broad coverage of many services for low-income people during pregnancy and to help prevent pregnancy, there is almost no access to help low-income people achieve pregnancy.
Figure 6: One State Medicaid Program Covers Infertility Treatment and Eight Cover Some Diagnostics
Medicare
While most beneficiaries of Medicare are over the age of 65+, Medicare also provides health insurance to approximately 2.5 million reproductive age adults with permanent disabilities. According to the Medicare Benefit policy manual, “reasonable and necessary services associated with treatment for infertility are covered under Medicare.” However, specific covered services are not listed, and the definition of “reasonable and necessary” are not defined.
Military
TRICARE: TRICARE, the insurance program for military families, will cover some infertility services, if deemed “medically necessary” and if pregnancy is achieved through “natural conception,” meaning fertilization occurs through heterosexual intercourse. Diagnostic services are covered, including lab testing, genetic testing, and semen analysis. Treatment to correct physical causes of infertility are also covered. However, IUI, IVF, donor eggs/sperm and cryopreservation are not typically covered, unless the service member had a serious injury while on active duty resulting in infertility.
Veterans Affairs (VA): Infertility services are covered by the VA medical benefits package, if infertility resulted from a service-connected condition. This includes infertility counseling, blood tests, genetic counseling, semen analysis, ultrasound imaging, surgery, medications and IVF (as of 2017). However, the couple seeking services must be legally married, and the egg and sperm must come from said couple (effectively excluding same sex couples). Donor eggs/sperm, surrogacy or obstetrical care for non-Veteran spouses are not covered.
Infertility Services In Publicly Funded Clinics
The CDC’s and Office of Population Affairs’ (OPA) Quality Family Planning recommendations address provision of basic infertility services. Family planning providers are recommended to provide at minimum patient education about fertility and lifestyle modifications, a thorough medical history and physical exam, semen analysis, and if indicated, referrals for lab testing of hormone levels, additional diagnostic tests (endometrial biopsy, ultrasound, HSG, laparoscopy) and prescription of medications to promote fertility. However, studies of publicly funded family planning clinics suggest that availability of infertility services is uneven. In a 2013-2014 study of 1615 publicly funded clinics, a high share reported offering preconception care (94% for women and 69% for men), but fewer offered any basic infertility services (66% for women and 45% for men). Provision of any infertility treatment was uncommon (16% of clinics), likely requiring referrals to specialists who may not accept Medicaid or uninsured patients.10 The majority of patients who rely on publicly funded clinics are low-income and would not likely be able to afford infertility services and treatments once diagnosed.
Per the Indian Health Services (IHS) provider manual, basic infertility diagnostics should be made available to women and men at IHS facilities, including a history, physical exam, basal temperature charting (to predict ovulation), semen analysis and progesterone testing. In facilities with OBGYNs, HSG, endometrial biopsy and diagnostic laparoscopy should also be available. However, it is unclear how accessible these services are in practice, and provision of infertility treatment is not mentioned.
Key Populations
Racial and ethnic minorities
The ability to have and care for the family that you wish for is a fundamental tenet of reproductive justice. For those who need it, this includes access to fertility services. The share of racial and ethnic minorities who utilize medical services to help become pregnant is less than that of non-Hispanic White women, despite research that has found higher rates of infertility among women who are Black and American Indian / Alaska Native (AI/AN). Our analysis of 2015-2017 NSFG data shows that while 13% of non-Hispanic White women reported ever going to a medical provider for help getting pregnant, just 6% of Hispanic women and 7% of non-Hispanic Black women did so (Figure 7). A higher share of Black and Hispanic women are either covered by Medicaid or uninsured than White women and more women with private insurance sought fertility help than those with Medicaid or the uninsured. A variety of factors, including differences in coverage rates, availability of services, income, and service‐seeking behaviors, affect access to infertility care. Furthermore, other societal factors also play a role. Misconceptions and stereotypes about fertility have often portrayed Black women as not requiring fertility assistance. Combined with the history of discriminatory reproductive care and harm inflicted upon many women of color over decades, some may delay seeking infertility care or may not seek it at all.
Figure 7: Women Seeking Help to Become Pregnant Tend to Be Age 35+, White, Higher Income, and Privately Insured
Other research has found that use of fertility testing and treatment also varies by race. An analysis of NSFG data found that among women who reported using medical services to help become pregnant, similar shares of Black (69%), Hispanic (70%) and White (75%) women received fertility advice. However, less than half (47%) of Black and Hispanic women who used medical services to become pregnant reported receiving infertility testing, compared to 62% of White women, and even fewer women of color received treatment services. According to an analysis of surveillance data of IVF services, use is highest among Asian and White women and lowest among American Indian / Alaska Native (AI/AN) women. Racial inequities may exist for fertility preservation as well; a study of female patients in NY with cancer found disproportionately fewer Black and Hispanic patents utilized egg cryopreservation compared to White patients. On average, more Black, Hispanic, and AI/AN people live below the federal poverty level than people who are White or of Asian/Pacific Islander descent. The high cost and limited coverage of infertility services make this care inaccessible to many people of color who may desire fertility preservation, but are unable to afford it.
Iatrogenic Infertility
Iatrogenic, or medically induced, infertility refers to when a person becomes infertile due to a medical procedure done to treat another problem, most often chemotherapy or radiation for cancer. In these situations, persons of reproductive age may desire future fertility, and may opt to freeze their eggs or sperm (cryopreservation) for later use. The American Society for Reproductive Medicine (ASRM) encourages clinicians to inform patients about fertility preservation options prior to undergoing treatment likely to cause iatrogenic infertility.
However, the cost of egg or sperm retrieval and subsequent cryopreservation can be prohibitive, particularly if in the absence of insurance coverage. Only a handful of states (CT, DE, IL, MD, NH, NJ, NY, and RI) specifically require private insurers to cover fertility preservation in cases of iatrogenic infertility. No states currently require fertility preservation in their Medicaid plans.
LGBTQ populations
LGBTQ people may face heightened barriers to fertility care, and discrimination based on their gender identity or sexual orientation. Section 1557 of the Affordable Care Act (ACA) prohibits discrimination in the health care sector based on sex, but the Trump Administration has eliminated these protections through regulatory changes. Without the explicit protections that have been dropped in the current rules, LGBTQ patients may be denied health care, including fertility care, under religious freedom laws and proposed changes to the ACA. However, these changes are being challenged in the courts because they conflict with a recent Supreme Court decision stating that federal civil rights law prohibits discrimination based on sexual orientation and gender identity.
In a committee opinion, ASRM concluded it is the ethical duty of fertility programs to treat gay and lesbian couples and transgender persons, equally to heterosexual married couples. They write that assisted reproductive therapy should not be restricted based on sexual orientation or gender identity, and that fertility preservation should be offered to transgender people before gender transitions. This allows transgender individuals the ability to have biological children in the future if desired. Despite this recommendation, in aforementioned states with mandated fertility preservation coverage for iatrogenic infertility, it remains unclear if this benefit extends to transgender individuals, whose gender affirming care can result in infertility. Additionally, many state laws regarding mandates for infertility treatment contain stipulations that may exclude LGBTQ patients. For example, in Arkansas, Hawaii and Texas and at the VA, IVF services must use the couple’s own eggs and sperm (rather than a donor), effectively excluding same sex couples. In other states, same-sex couples do not meet the definition of infertility, and thus may not qualify for these services. Data are lacking to fully capture the share of LGBTQ individuals who may utilize fertility assistance services. Research studies on family building are often not designed to include LGBTQ respondents’ fertility needs.
Single Parents
Single persons are often excluded from access to infertility treatment. For example, the same IVF laws cited above that require the couple’s own sperm and egg, effectively exclude single individuals too, as they cannot use donors. Some grants and other financing options also stipulate funds must go towards a married couple, excluding single and unmarried individuals. This is in opposition to the ASRM committee opinion, which states that fertility programs should offer their services to single parents and unmarried couples, without discrimination based on marital status.
Looking Forward
On a federal level, efforts to pass legislation to require insurers to cover fertility services are largely stalled. The proposed Access to Infertility Treatment and Care Act (HR 2803 and S 1461), which would require all health plans offered on group and individual markets (including Medicaid, EHBP, TRICARE, VA) to provide infertility treatment, is still in committee (and never made it out of committee when proposed during the 115th congress). There has been some more movement on the state level. Some states require private insurers to cover infertility services, the most recent of which was NH in 2020. Currently, NY continues to be the first and only state Medicaid program to cover any fertility treatment.
For those who desire to have children, obtaining fertility care can be a stressful process. Stigma around infertility, intensive and sometimes long or painful treatment regimens, and uncertainty about success can take a toll. On top of that, in the absence of insurance coverage, infertility care is cost prohibitive for most, particularly for low-income people and for more expensive services, like IVF or fertility preservation. Significant disparities exist within access to infertility services across, dictated by state of residence, insurance plan, income level, race/ethnicity, sexual orientation and gender identity. Achieving greater equity in access to fertility care will likely depend on addressing the needs faced by low-income persons, people of color and LGBTQ persons in fertility policy and coverage.
Appendices: Appendix 1: Private Insurance
Appendix 1: States That Require Private Insurance Coverage of Infertility Services
Infertility coverage required:(As of May 2020)
State (Statute year)
By which insurers?
For which indications?
For which treatments?
AR
(1987, 2011)
Included: all individual and group insurers*
Excluded: HMOs; self-insurers
Eligible: Infertility due to male factor, endometriosis, blocked fallopian tube (or unexplained for 2 years)
Ineligible: if egg/sperm not from spouse
Covered: IVF (lifetime max $15,000)
Not covered: Fertility preservation for iatrogenic infertility
CA
(1990)
Mandate to offer, not cover: group insurers must let employers know coverage for diagnostic tests and some treatment is available (excludes IVF and fertility preservation), but employers do not need to provide coverage to employees
CO
(Effective 2022)
Passed House Bill 20-1148 in April 2020 to mandate coverage for infertility diagnosis and treatment, and fertility preservation for iatrogenic infertility. Applies to all individual and group health benefit plans renewed or issued after January 1, 2022, but religious employer may request exemption.
CT
(1989, 2005)
Included: Health insurance organizations
Excluded: Persons on plan for <12 months; religious employers; self-insurers
Eligible: Infertility for 1 year or iatrogenic infertility
Not Covered: Lifetime max of 4 cycles of ovulation induction, 3 cycles of IUI
DE
(2018)
Included: Individual and group insurers, HMOs **
Excluded: <50 employees; religious employers; self-insurers
Eligible: Infertility or iatrogenic infertility
Covered: consultation, diagnostics, medications, IUI, IVF and other treatments; fertility preservation for iatrogenic infertility
Not Covered: Egg retrieval after age 45, >6 egg retrievals, surrogacy compensation, reversal of voluntary sterilization
HI
(1989, 2003)
Included: Individual and group insurers
Excluded: self-insurers
Eligible: 5 years of unexplained infertility, OR infertility due to male factors, endometriosis, blocked/ removed fallopian tubes
Ineligible: if egg/sperm not from spouse
Covered: 1 cycle of IVF, all outpatient expenses arising from IVF
IL
(1991, 1996)
Included: Group insurers and HMOs*; individual insurers for iatrogenic infertility
Excluded: <25 employees; religious employers; self-insurers
Eligible: 1 year of infertility or iatrogenic infertility
Covered: Diagnostics, IUI, IVF, and other treatments; fertility preservation for iatrogenic infertility
Not Covered: More than 6 egg retrievals
MD
(2000)
Included: Individual and group insurers*
Excluded: <50 employees; religious employers; self-insurers
Eligible: Infertility due to male factor, endometriosis, blocked/removed fallopian tubes (or if unexplained for 2 years)
Covered: 3 cycles of IVF per life birth (lifetime max $100,000); fertility preservation for iatrogenic infertility
Not Covered: Storage of sperm/eggs
MA
(1987, 2010)
Included: All insurers and HMOs*
Excluded: self-insurers
Eligible: Infertility for 1 year if age <35, 6 months if 35+
Covered: IUI, IVF, cryopreservation and others (no lifetime limit on cost or cycles)
Not Covered: Surrogacy, reversal of sterilization
MT
(1987)
Included: HMOs
Excluded: all other insurers
Eligible: No definition of infertility
Covered: must cover “infertility services,” does not define which
NH
(2020)
Included: Group insurers***
Excluded: Small business health options program; extended transition to ACA- programs; self-insurers
Eligible: Ability to become/cause pregnancy is impaired
Covered: Diagnostics, treatment including medications, egg/sperm procurement; fertility preservation for iatrogenic infertility
Not Covered: reversal of voluntary sterilization; some aspects of care if surrogate involved
NJ
(2001)
Included: Group insurers; HMOs; State Health Benefits Program; School Employees Health Benefits Program*
Excluded: <50 employees; religious employers; self-insurers
Eligible: Infertility for 1 year if age <35, 6 months if 35+; single female unable to conceive with 12 IUIs if <35, 6 IUIs if >35; persons involuntarily sterilized
Ineligible: >46 years old
Covered: diagnostics, medications, surgery, IUI, IVF, and other treatments (max 4 egg retrievals per lifetime)
Not Covered: reversal of voluntary sterilization; cryopreservation
NY
(1990, 2002, 2020)
Included: Large group insurance market for IVF (>100 employees); all commercial markets for cryopreservation
Excluded: Individual and small group markets for IVF; self-insurers
Eligible: Infertility for 1 year if age <35, 6 months if 35+
Ineligible:
Covered: diagnostic procedures, medications, 3 cycles of IVF; fertility preservation if iatrogenic infertility
Not Covered: surrogacy, reversal of elective sterilization
OH
(1991)
Included: HMOs
Excluded: all other insurers
Eligible: No definition of infertility
Covered: diagnostic and exploratory procedures to correct cause for infertility (endometriosis, blocked fallopian tube, testicular failure)
Not Covered: IVF and other treatments
RI
(1989, 2007)
Included: Insurers and HMOs*
Excluded: Self-insurers
Eligible: Infertility for 1 year; iatrogenic infertility
Ineligible: women aged <25 of >42 (unless for fertility preservation)
Covered: diagnostics and treatment, including IVF; fertility preservation for iatrogenic infertility (up to 20% copay allowed)
Not Covered: >$100,000 on treatment
TX
(1987, 2003)
Mandate to offer, not cover: Group insurers must offer IVF as a benefit, employers can choose whether or not to include it. If choose to include, must be egg/sperm from spouse.
UT
(2014)
Included: Insurers*
Excluded: Self-insurers
Eligible: no definition of infertility; persons wishing to adopt
Covered: $4000 adoption indemnity, can also be used for infertility treatment
WV
(1995)
Included: HMOs
Excluded: all other insurers
Eligible: no definition of infertility
Covered: must cover “infertility services,” does not define which
NOTES: *Insurers must cover if they also provide pregnancy-related benefits. ** Must cover infertility services to same extent as other pregnancy-related services. ***Must cover if also provide medical/hospital expenses.AL, AK, AZ, CO, DC, FL, GA, ID, IN, IA, KS, KY, LA, ME, MI, MN, MS, MO, NE, NV, NM, NC, ND, OK, OR, PA, SC, SD, TN, VT, VA, WA, WI, and WY do not require private insurers to cover infertility treatments.SOURCES: NCSL. State Laws Related to Insurance Coverage for Infertility Treatment. 6/12/2019; American Society for Reproductive Medicine (ASRM). State Infertility Insurance Laws; Resolve. Infertility Coverage by State; Colorado House Bill 20-1158
Appendices: Appendix 2: Medicaid
Appendix 2: State Medicaid Coverage of Infertility Services
Covered and Non-Covered Services by State(As of January 2020)
Not Covered: Infertility studies/procedures for diagnosing/treating infertility (Family Planning Manual)
CO
Covered: Basic fertility and reproductive health counseling is provided (Family Planning Services Benefits)
Not Covered: Sterilization reversal. Infertility treatment, counseling and testing. Tests normally associated with infertility management (e.g., HSG and semen analysis) covered only to confirm success of a sterilization
CT
Covered: Lab tests to detect the presence of conditions affecting reproductive health (Member Handbook)
Covered: infertility diagnosis/treatment when infertility is a symptom of a suspected medical problem (e.g., thyroid disease). No coverage if the sole purpose is achieving pregnancy (Physician services)
Covered: infertility office visits, diagnosis (HSG, pelvic ultrasounds, lab tests), fertility drugs (bromocriptine, clomiphene citrate, letrozole, tamoxifen). Limited to 3 cycles of treatment per lifetime (Infertility Benefit)
Not Covered: Infertility treatments beyond those described above.
NC
Not Covered: Infertility services and related procedures. Services to manage/treat complications of women’s health problems, including heavy bleeding or infertility (Family Planning Services)
ND
Not Covered: Diagnostic, medical, surgical or pharmaceutical services related to infertility. Removal of long acting reversible contraceptive devices to regain fertility (Provider manual)
Not Covered: Will not pay for medical procedures if goal is fertility (semen analysis, fallopian tube repair, laparoscopy). Covered if reproductive system disease requires treatment to maintain overall health, and is medically necessary (Provider Manual). No fertility drugs (Pharmacy manual)
NOTES: * Benefits vary between Medicaid managed care plans. Information collected on individual Medicaid managed care plans when information on fertility benefits not found in member benefits or provider manuals pertaining to all Medicaid plans.ⱡ OR covers basic infertility counseling as part of The Oregon Reproductive Health Program for low income women, but not a Medicaid benefitSOURCES: Information compiled from member handbooks and provider manuals as linked above, available online as of January 2020 (see links above).
Endnotes
The evaluation of fertility can start after six months if the woman is over the age of 35. ↩︎
Data and research often assume cisgender identities and may not systematically account for people who are transgender and non-binary. The language used in this brief attempts to be as inclusive as possible while acknowledging that the data we are citing uses gender labels that we cannot change without misrepresenting the data. ↩︎
The CDC reports the percentage of women (ages 15-49) who have ever received “infertility services” (12.7%) which also includes medical help to prevent miscarriage. We report on the percentage of adult women (ages 18-49) who have ever received medical help to become pregnant, excluding medical help once women are already pregnant. ↩︎
The CDC does not track the number of births as a result of other fertility assistance, like fertility medications or IUI. However, in the 2012 CDC National Public Health Action Plan for the Detection, Prevention and Management of Infertility, they recommended the development of surveillance systems which would monitor the utilization and health outcomes of non-IVF treatment for infertility. ↩︎
IL has a mandate to cover that applies only to group plans; however, the state’s benchmark plan includes coverage for infertility treatment, so individual plans in IL also cover these services. ↩︎
The TX benchmark plan includes coverage for diagnosis of infertility, so individual plans in TX also cover this service. ↩︎
“Comprehensive coverage” for ART defined by CDC as covering at least four oocyte (egg) retrievals. ↩︎
Availability was judged by the number of physicians performing IVF per 1,000 reproductive age women, and utilization was calculated by number of IVF cycles per 100,000 reproductive age women. ↩︎
Definitions of preconception care, basic infertility services and infertility treatment were left up to the interpretation of the respondent. ↩︎

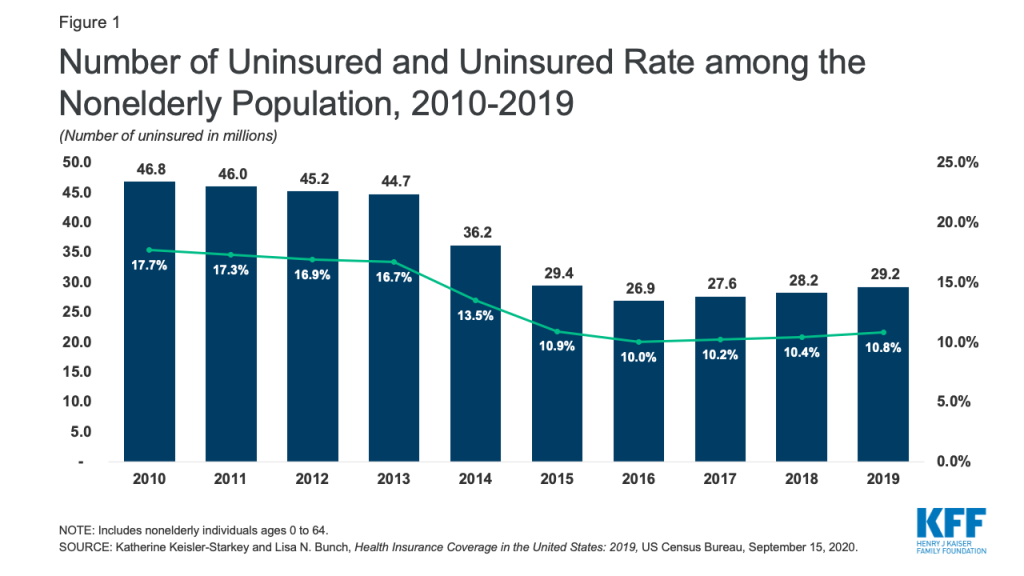
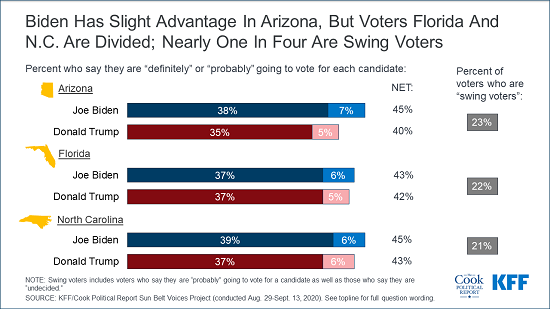
_poll%20chart%202_kff.cook.png?width=1100&upscale=true&name=Alert%20Charts_FINAL%20(5)_poll%20chart%202_kff.cook.png)
_poll_3_chart.png?width=1100&upscale=true&name=Alert%20Charts_FINAL%20(5)_poll_3_chart.png)
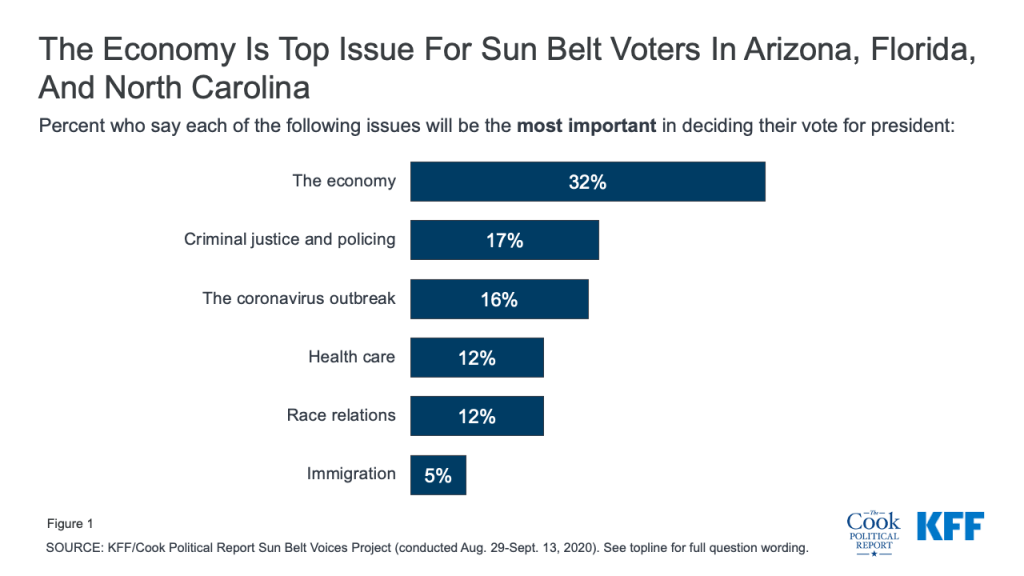
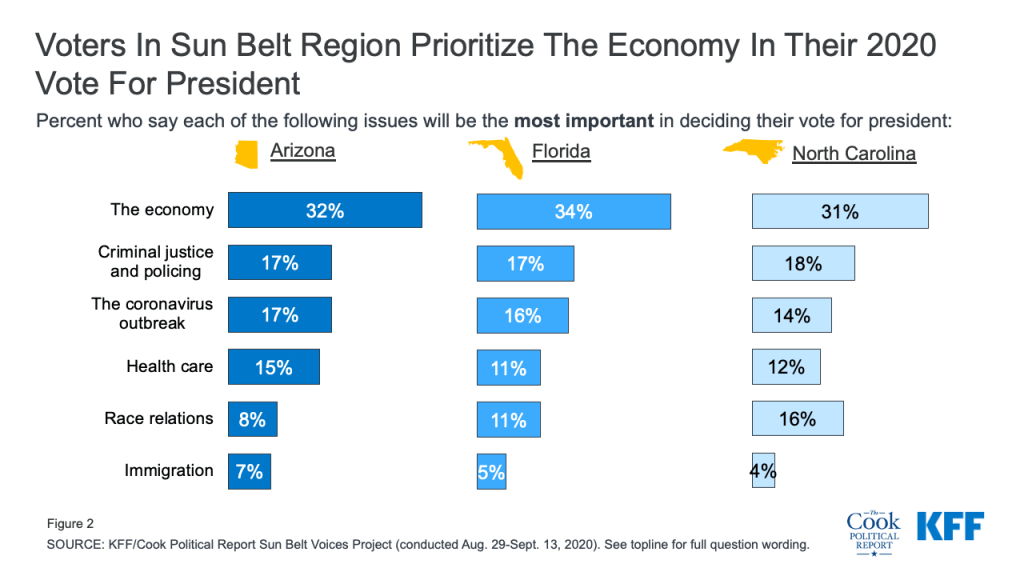
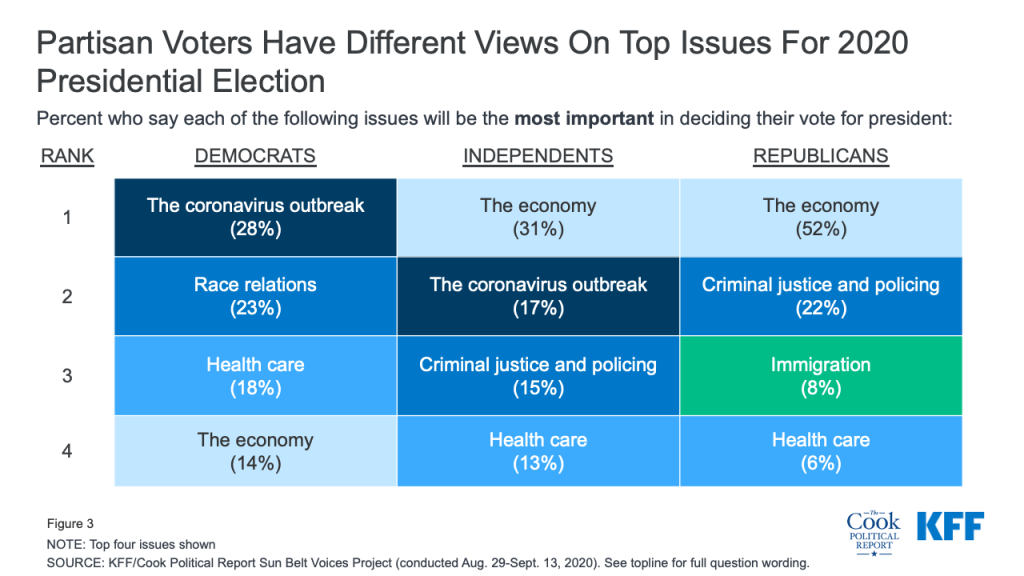
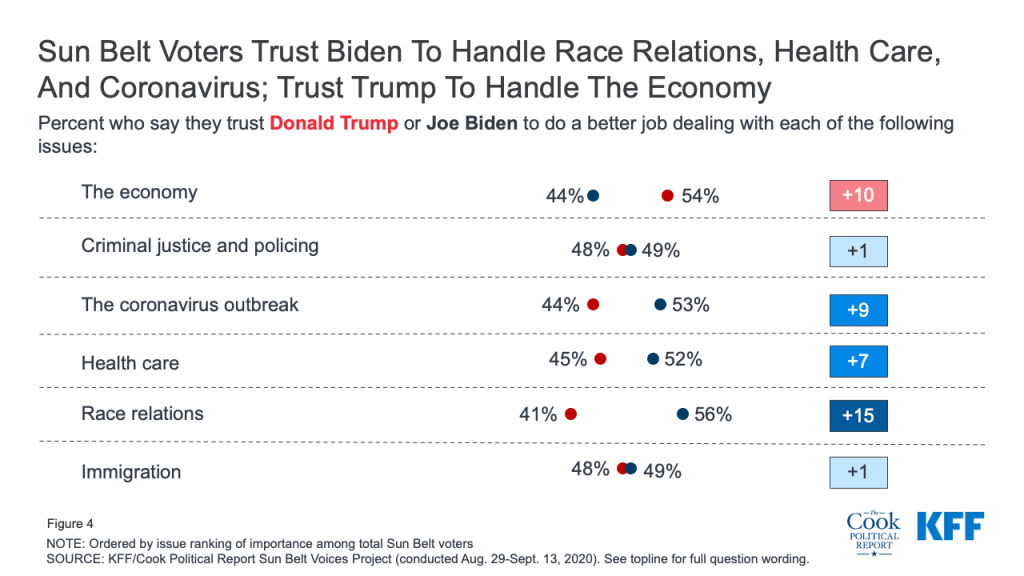
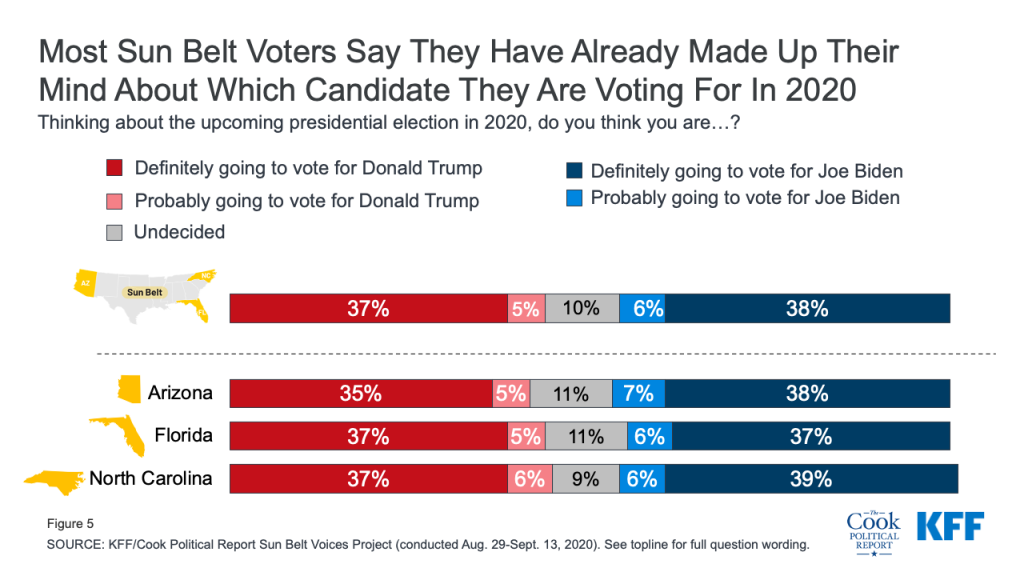
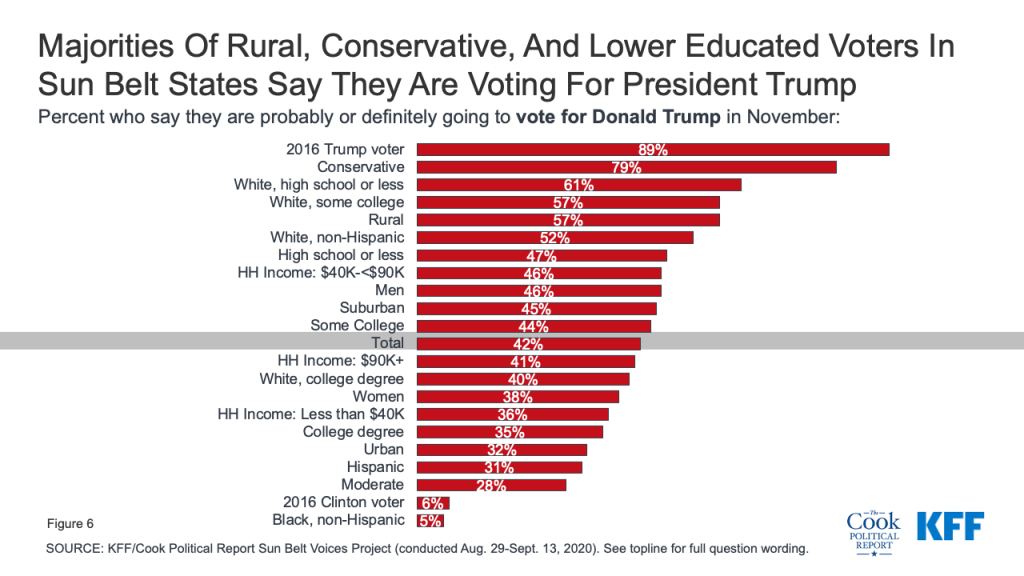
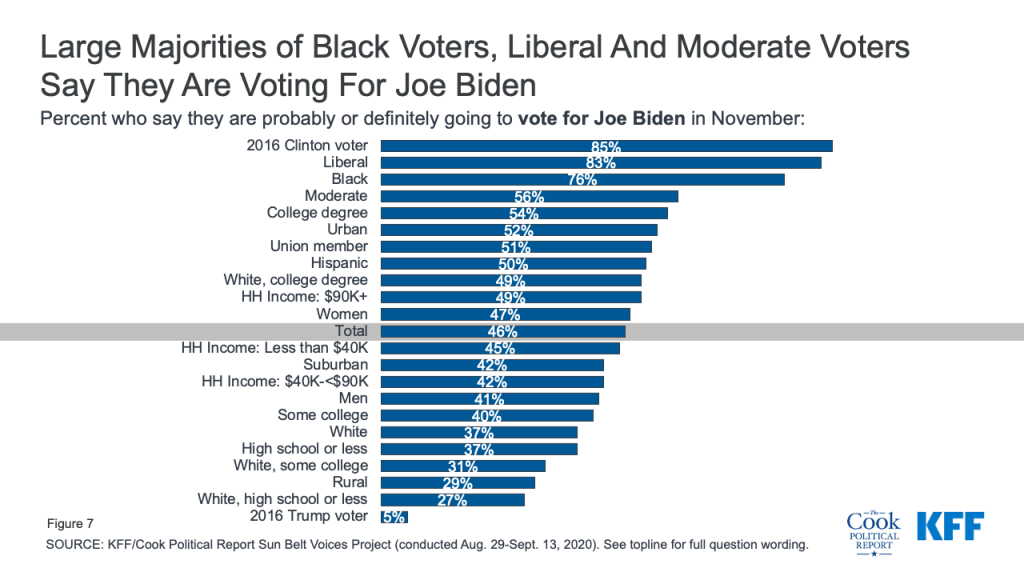
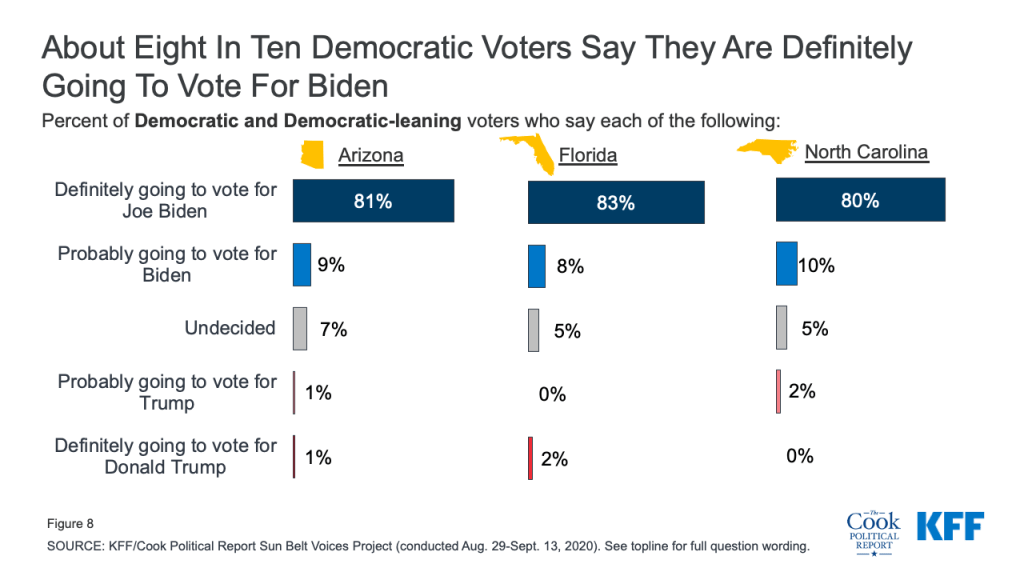
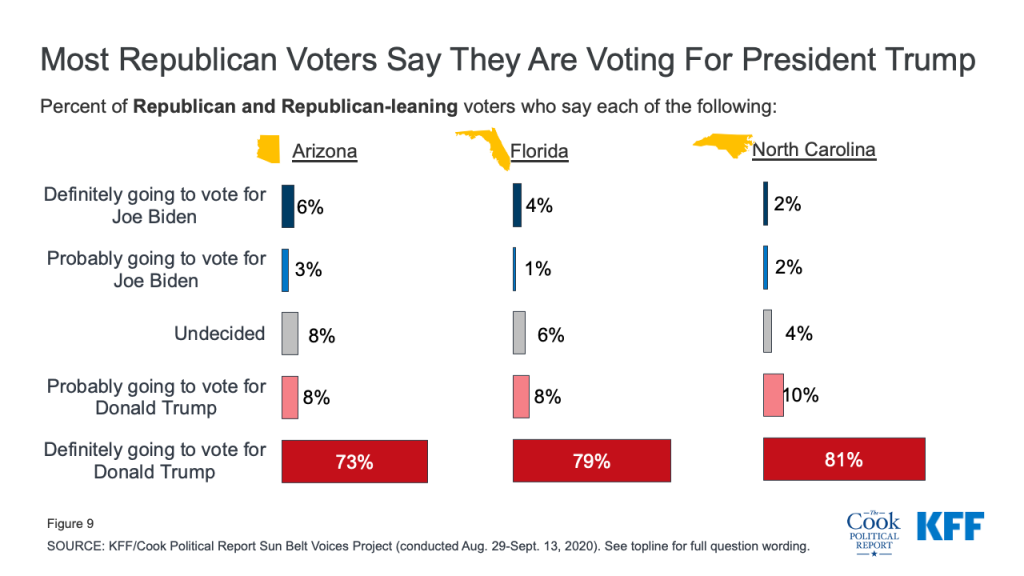
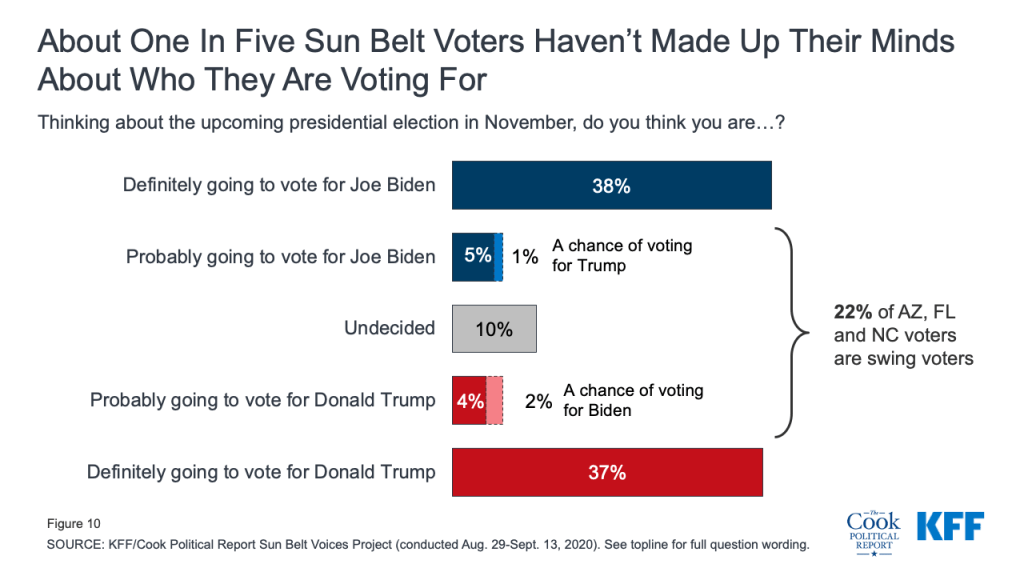
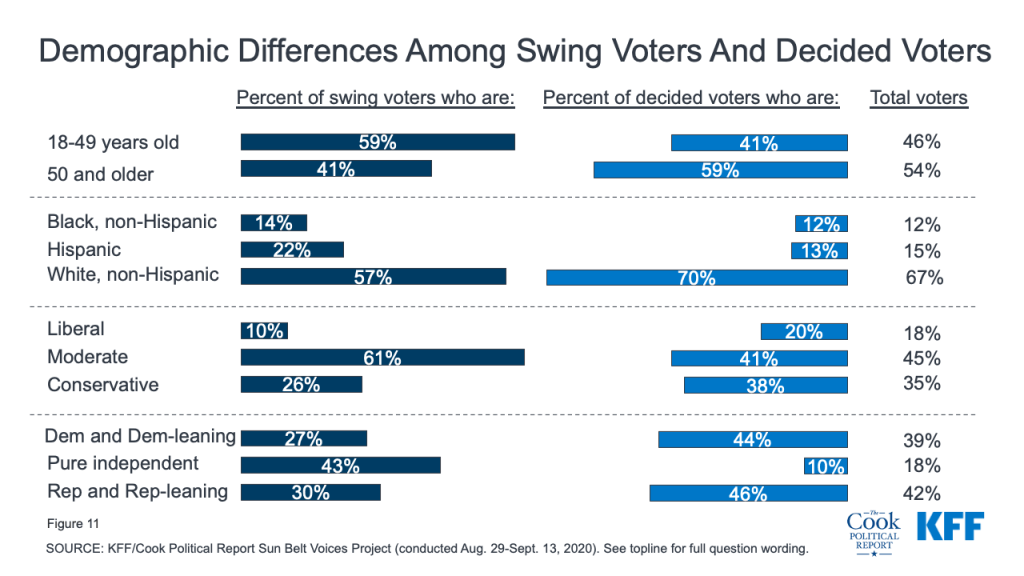
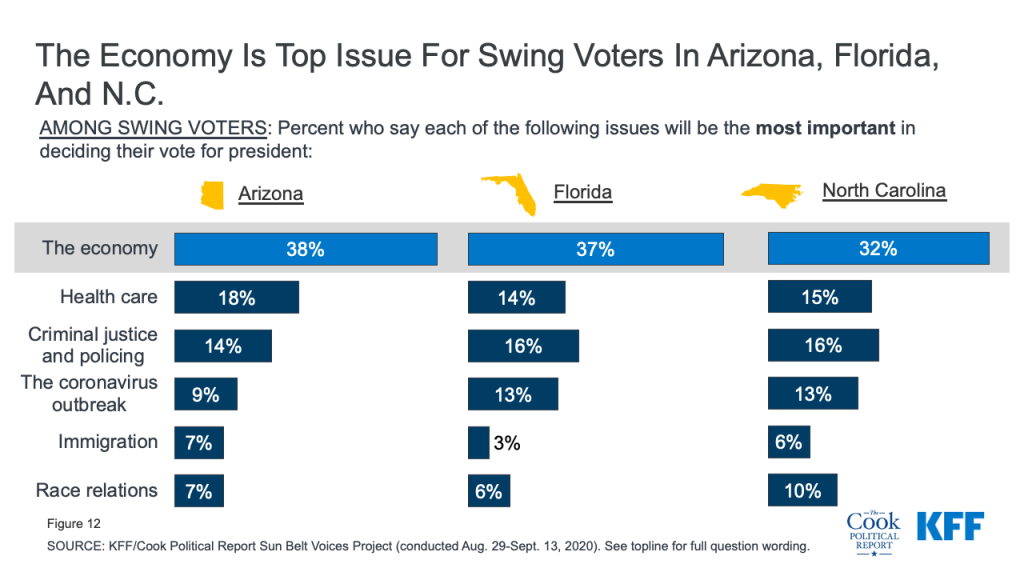
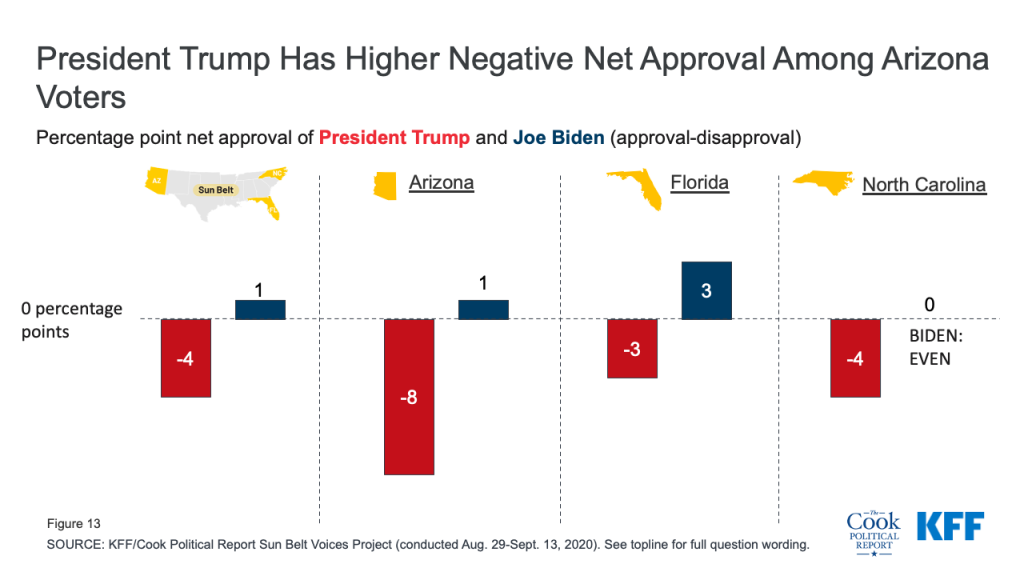
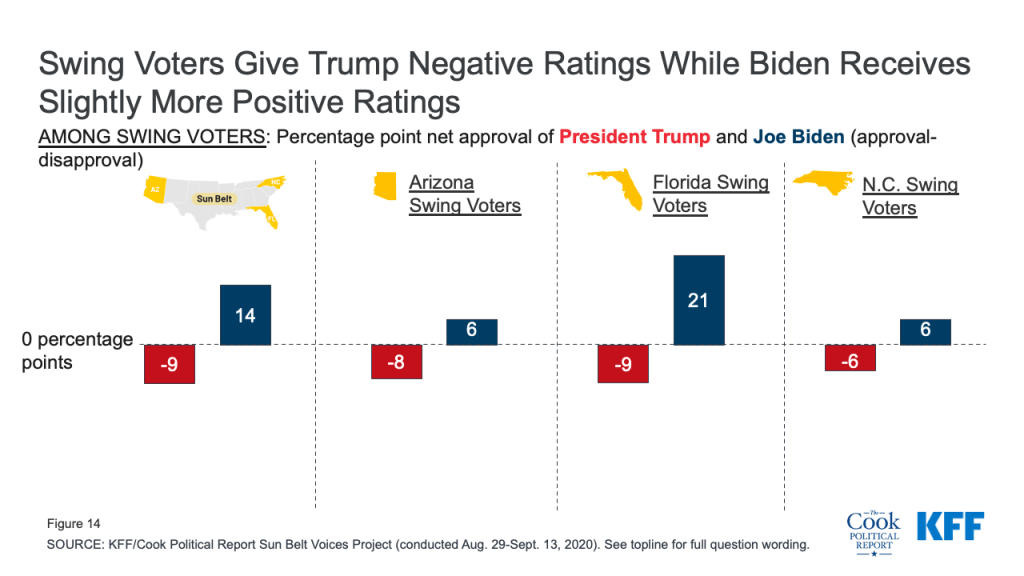
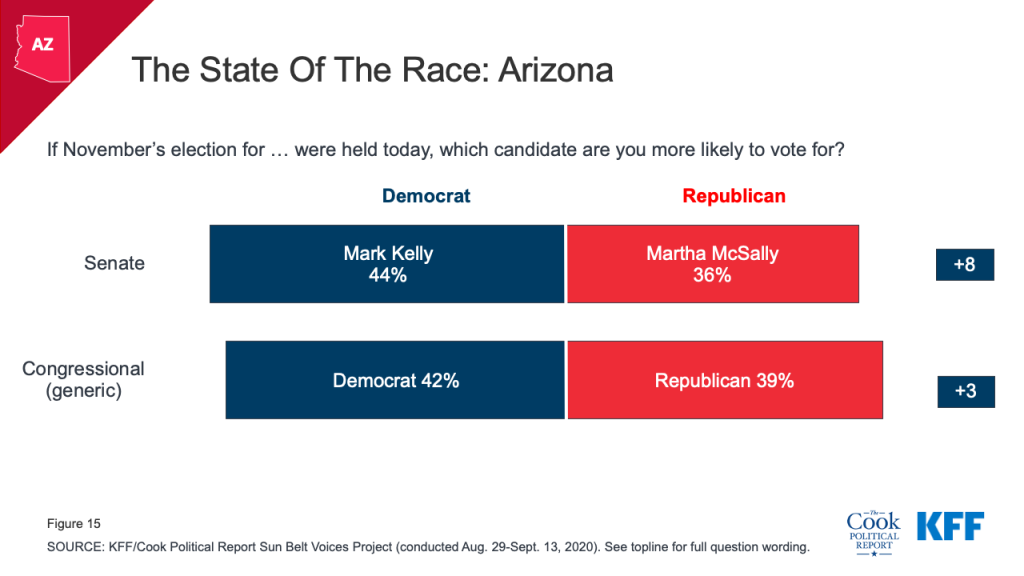
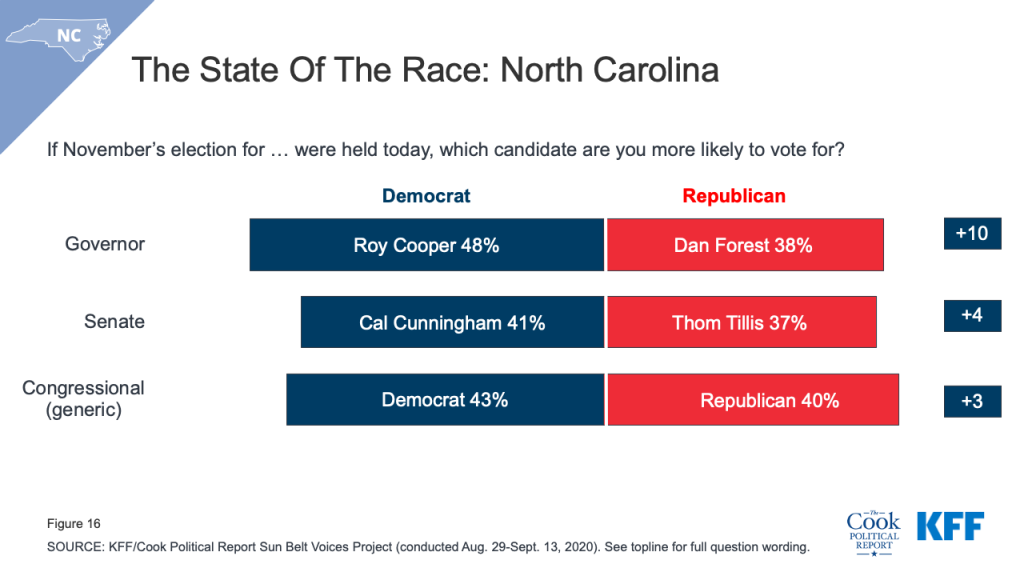
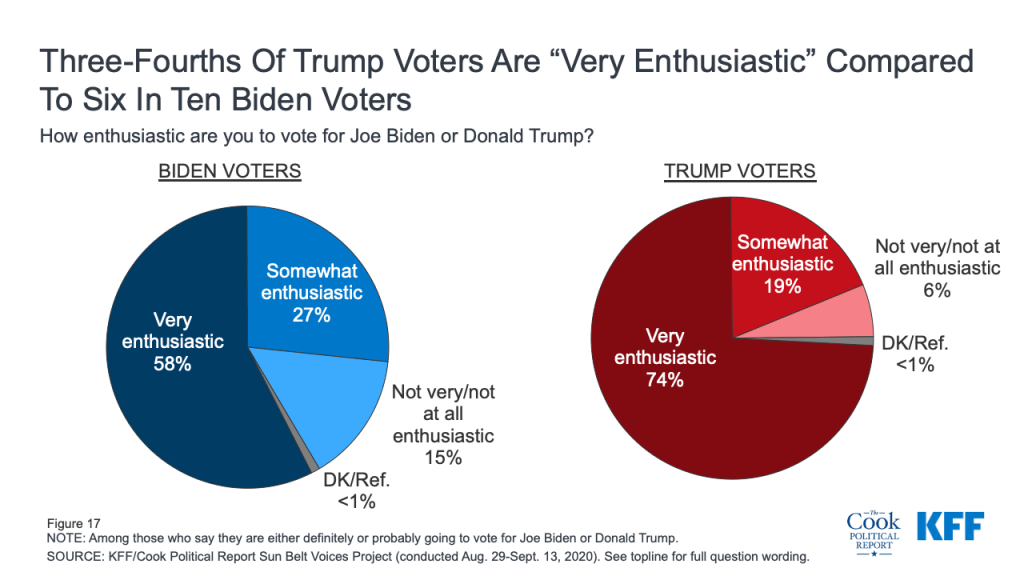
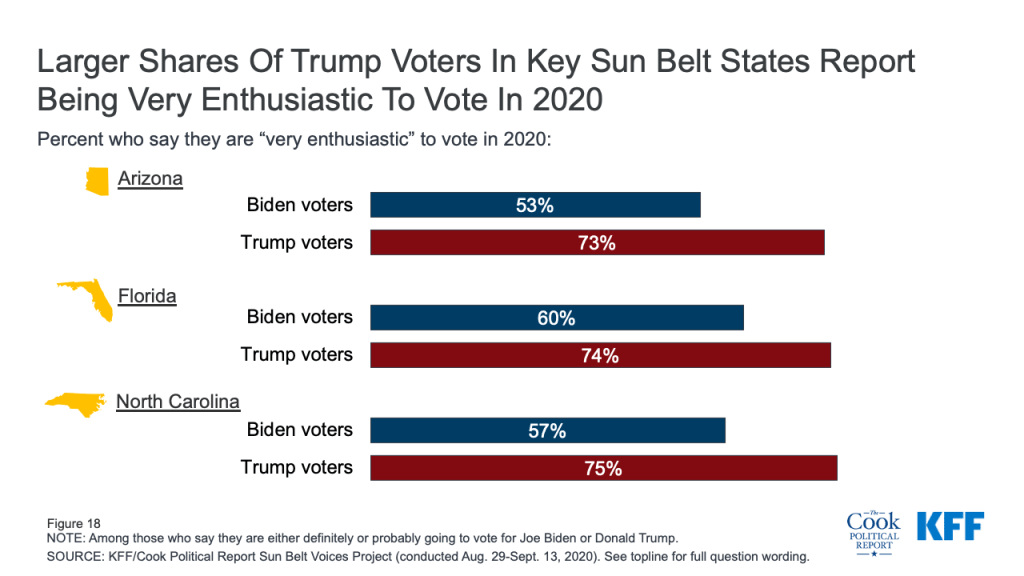
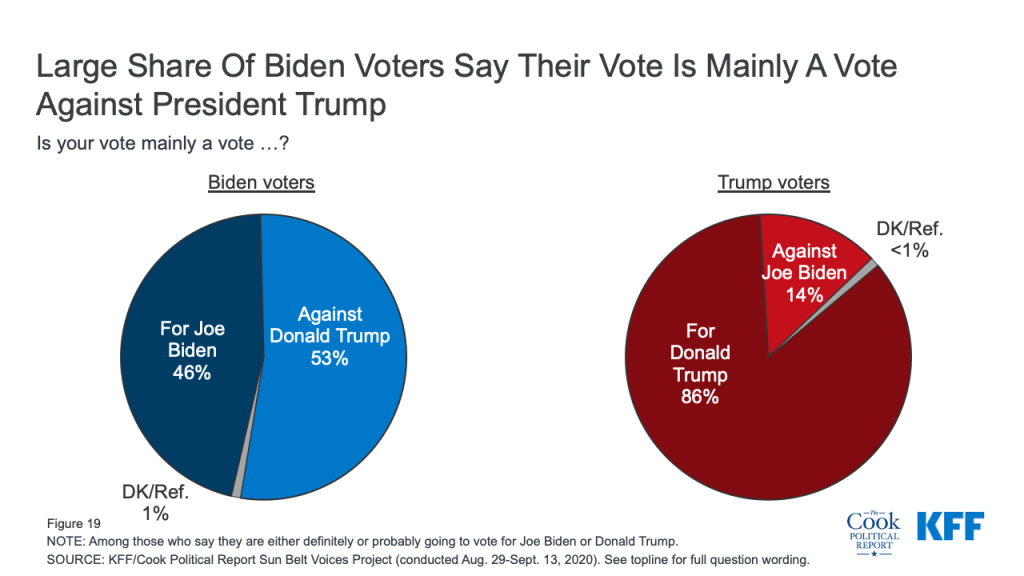
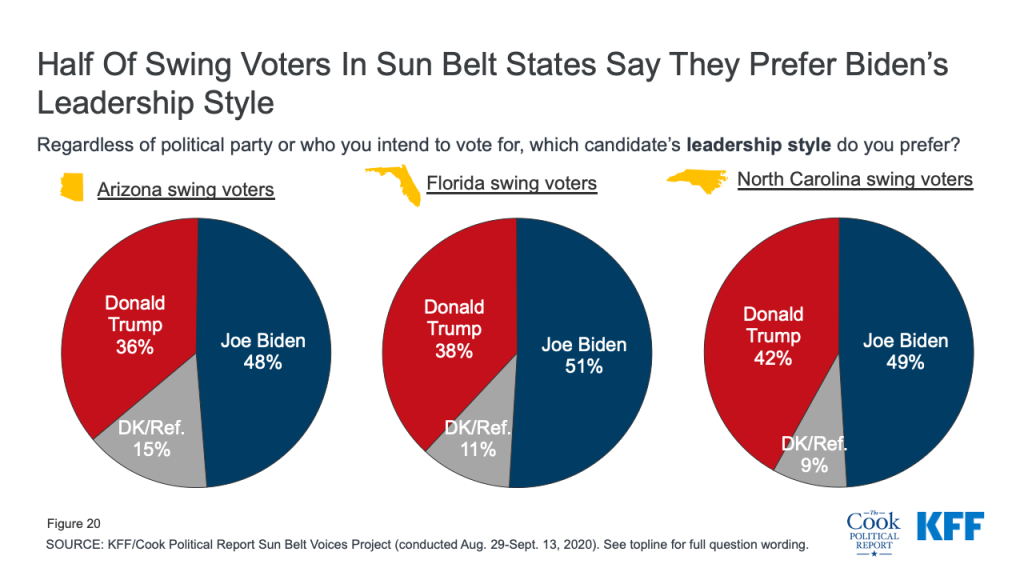
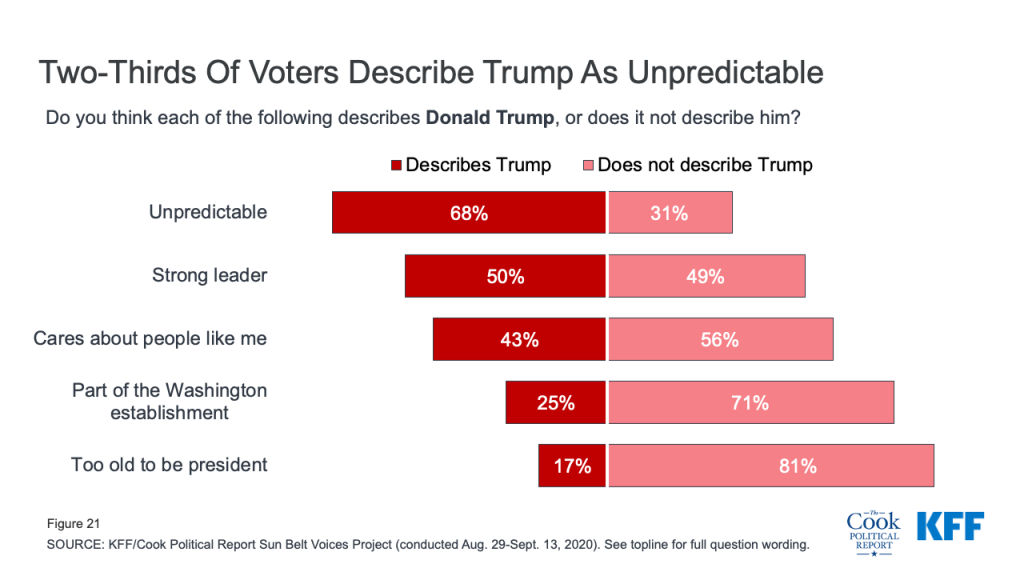
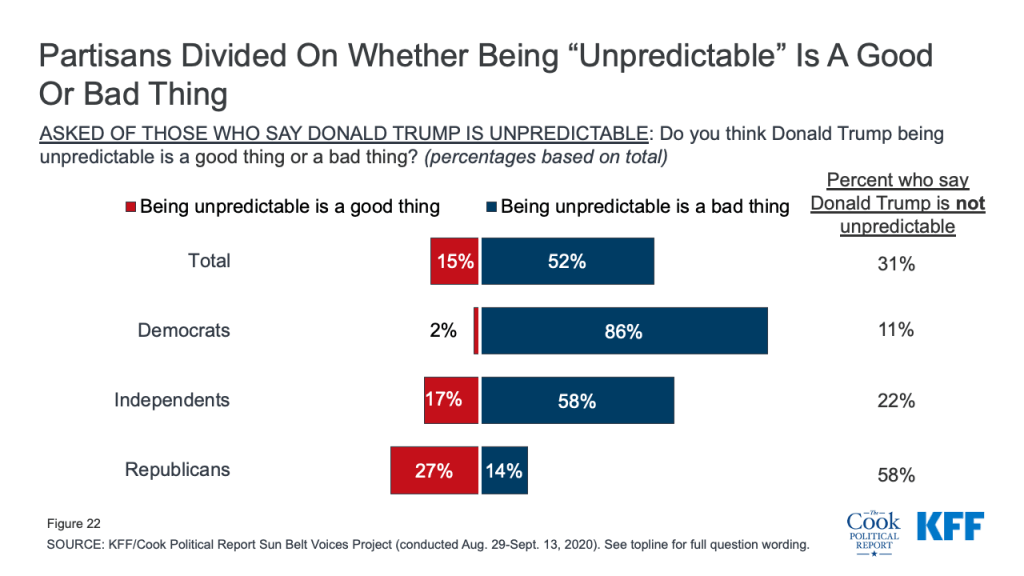
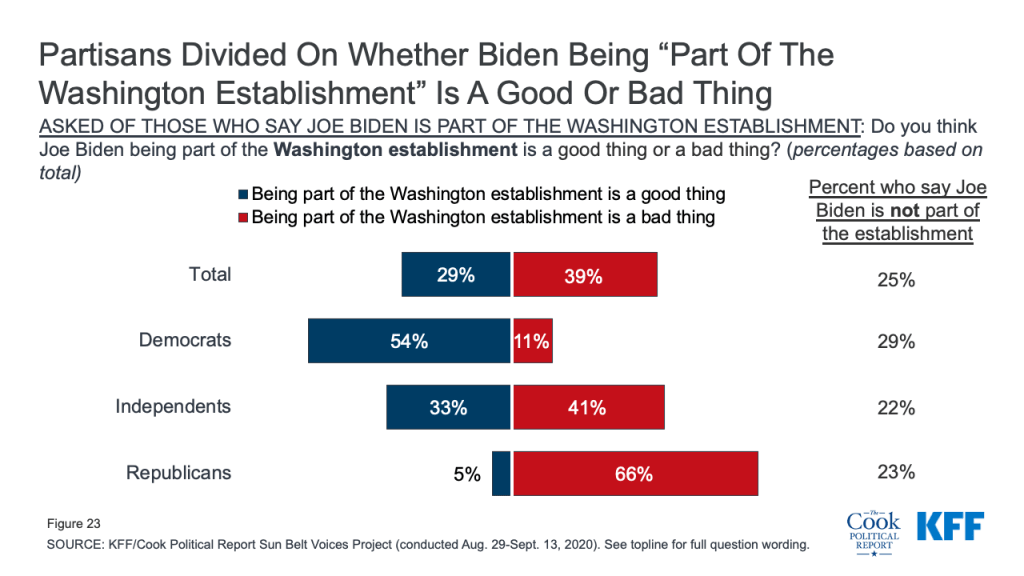
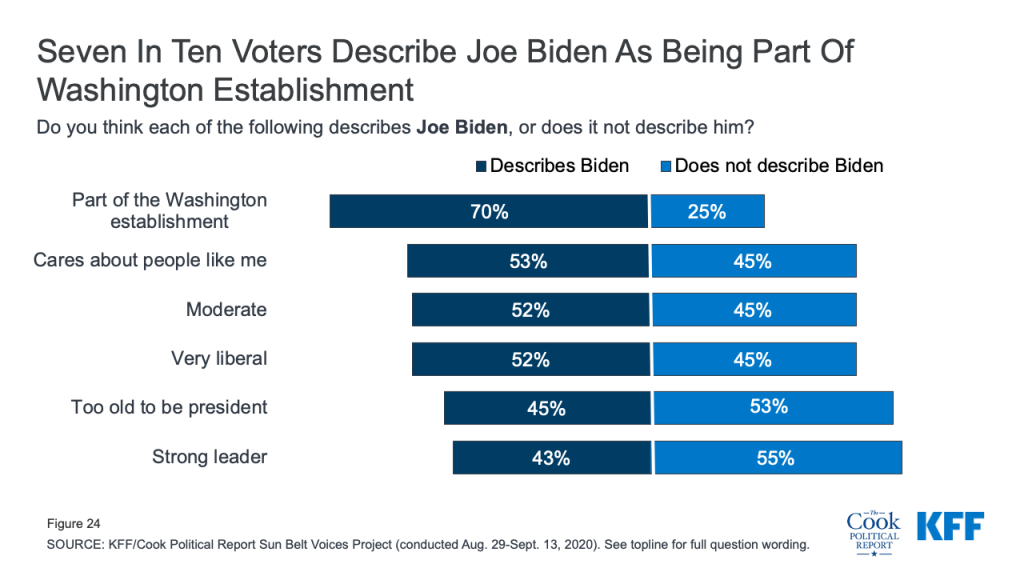
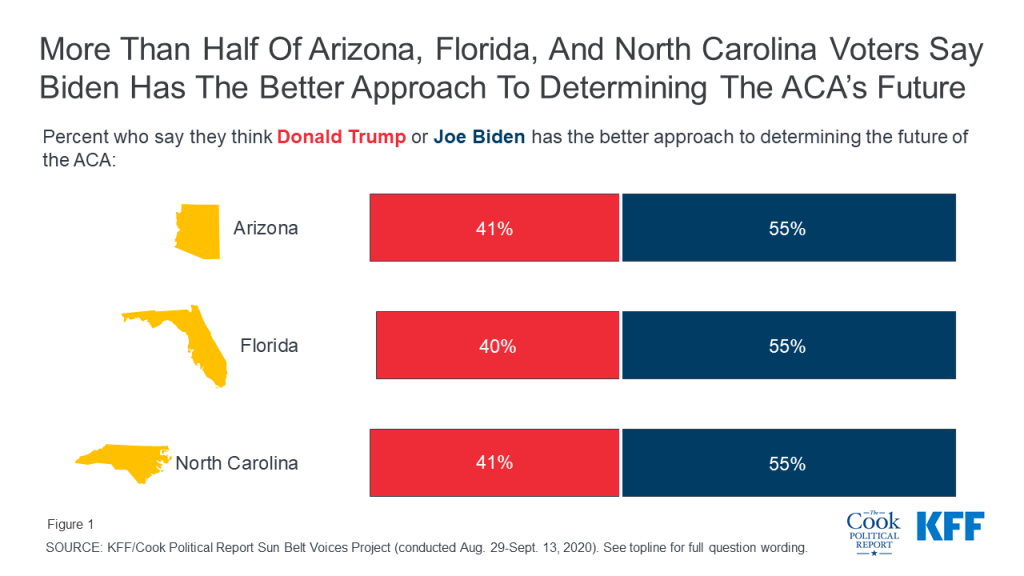
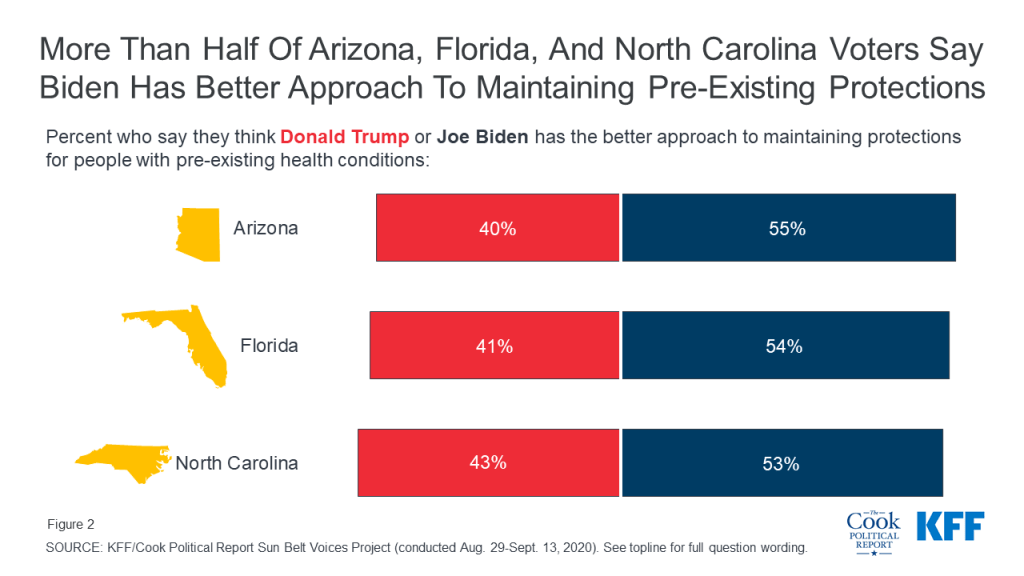
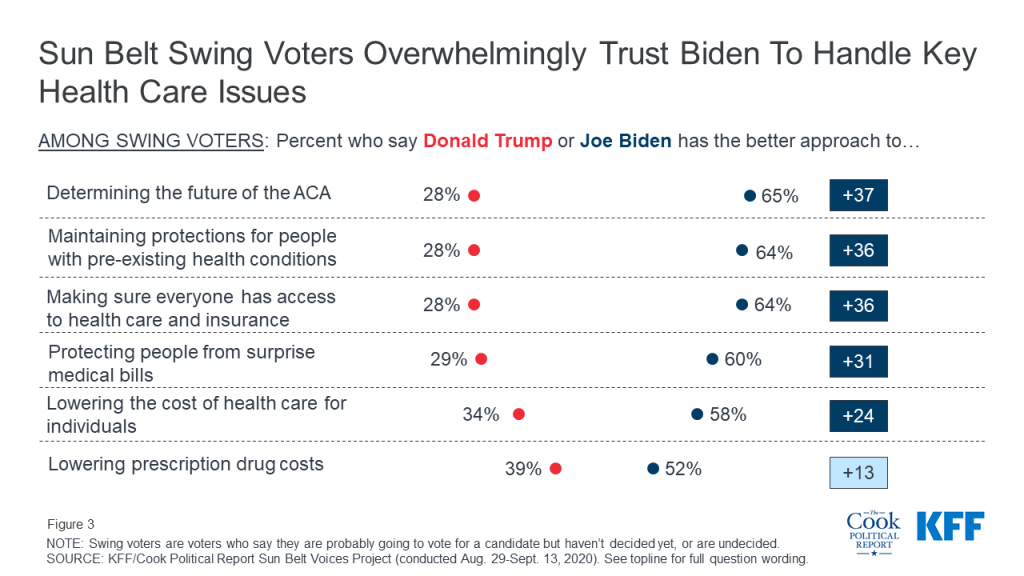
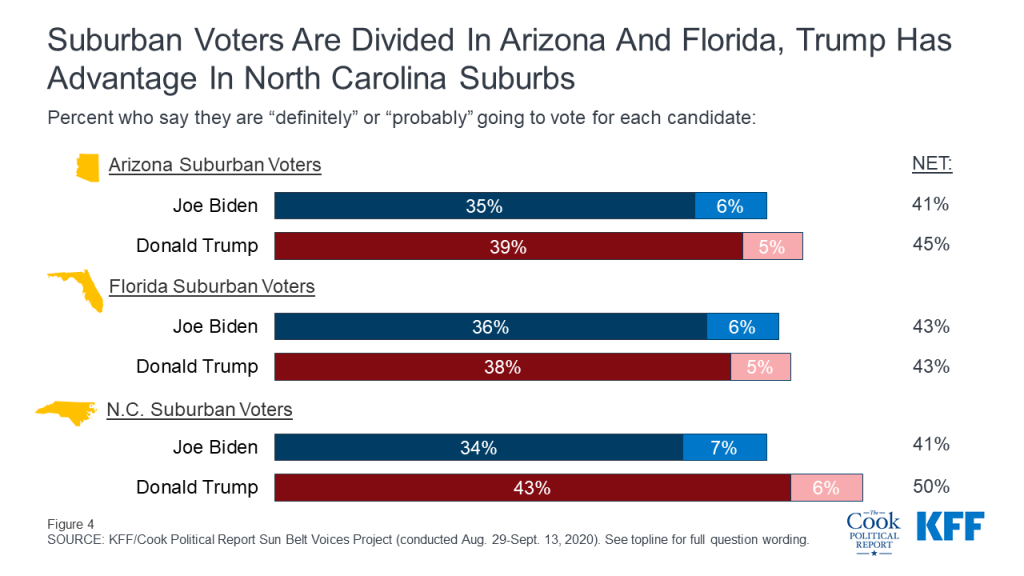
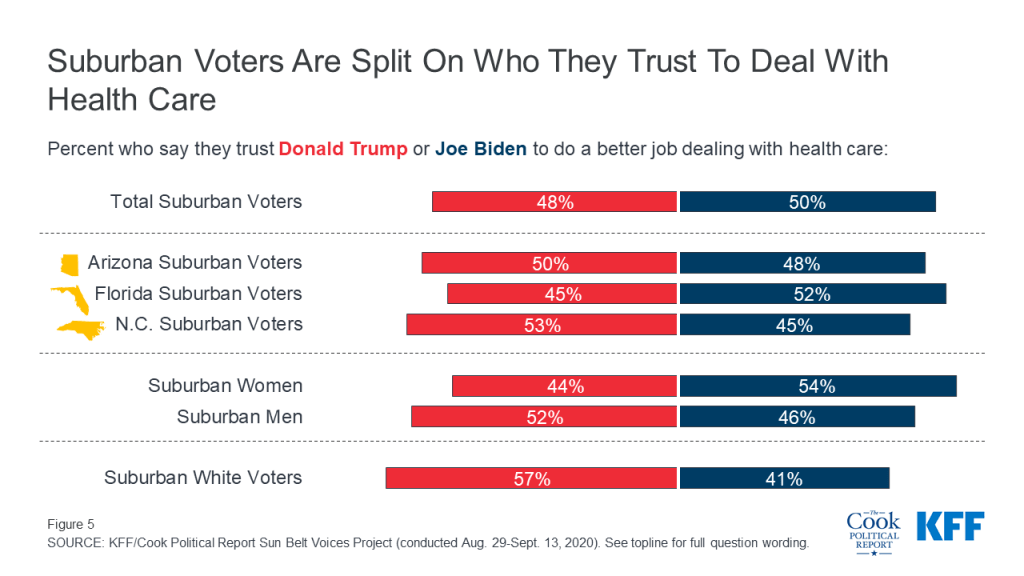
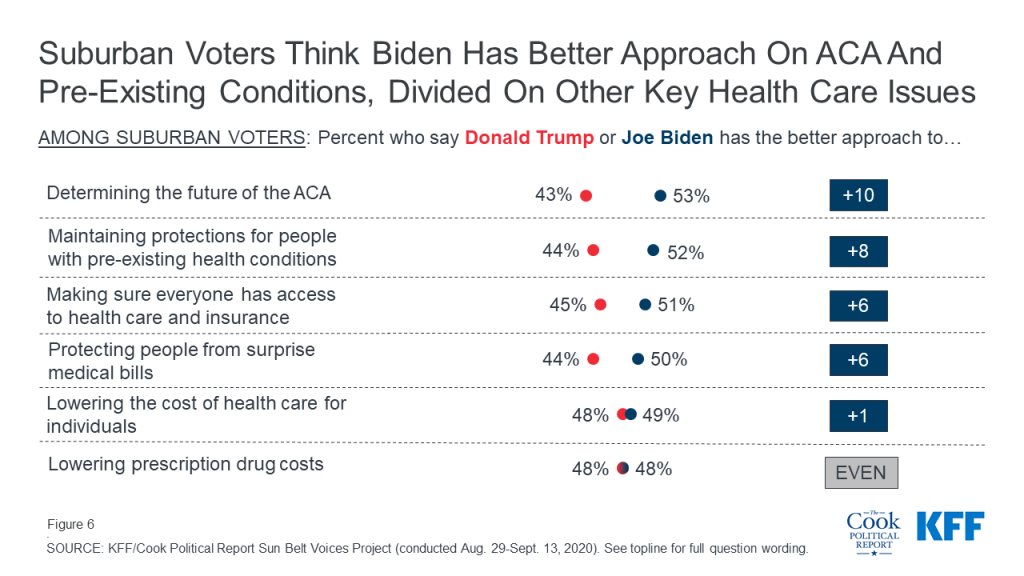
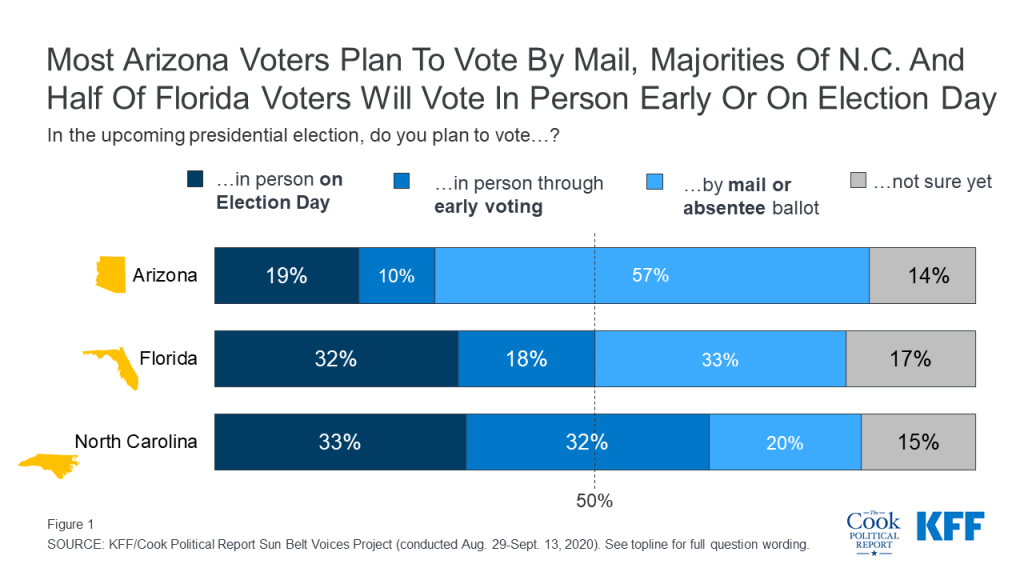
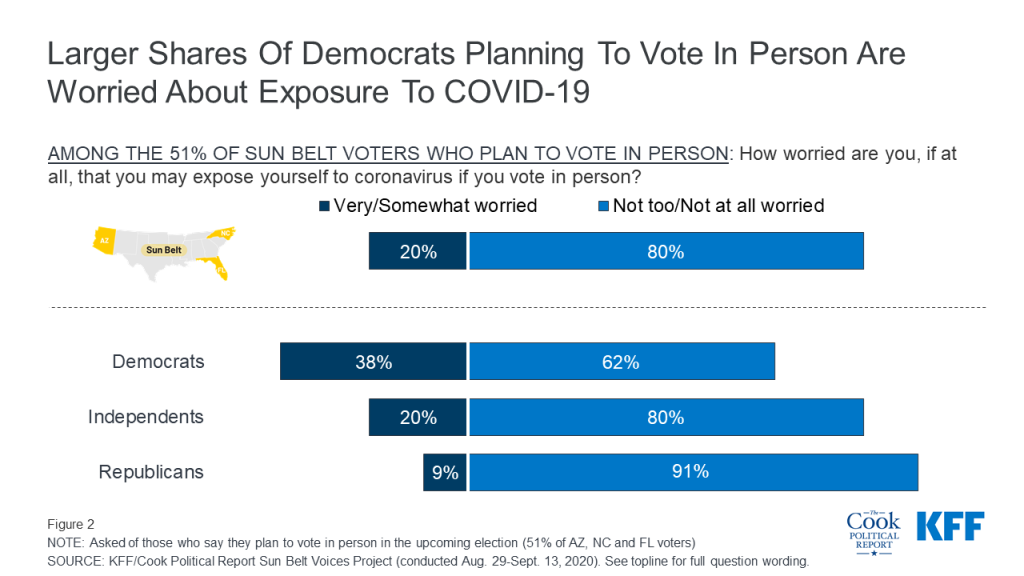
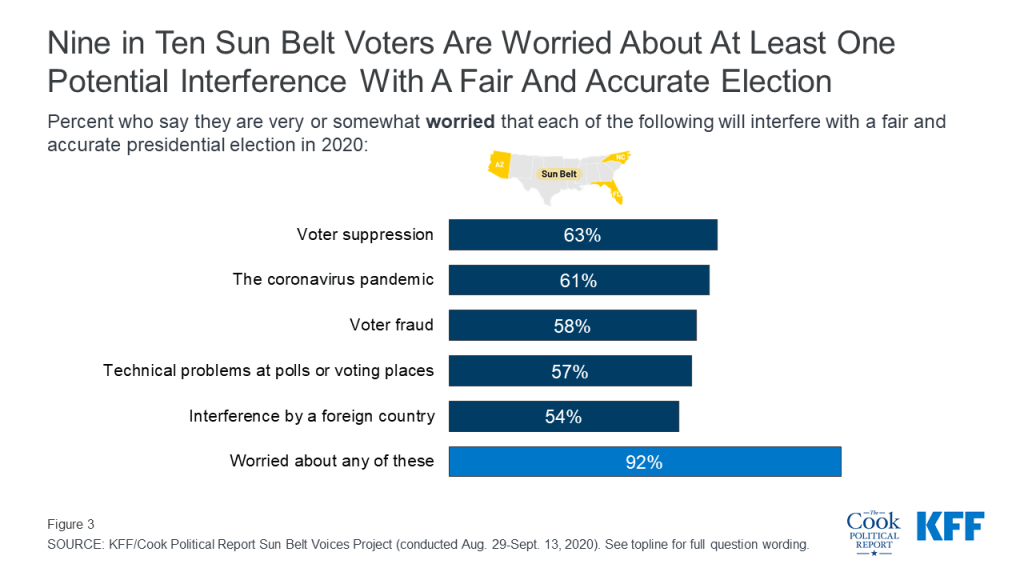
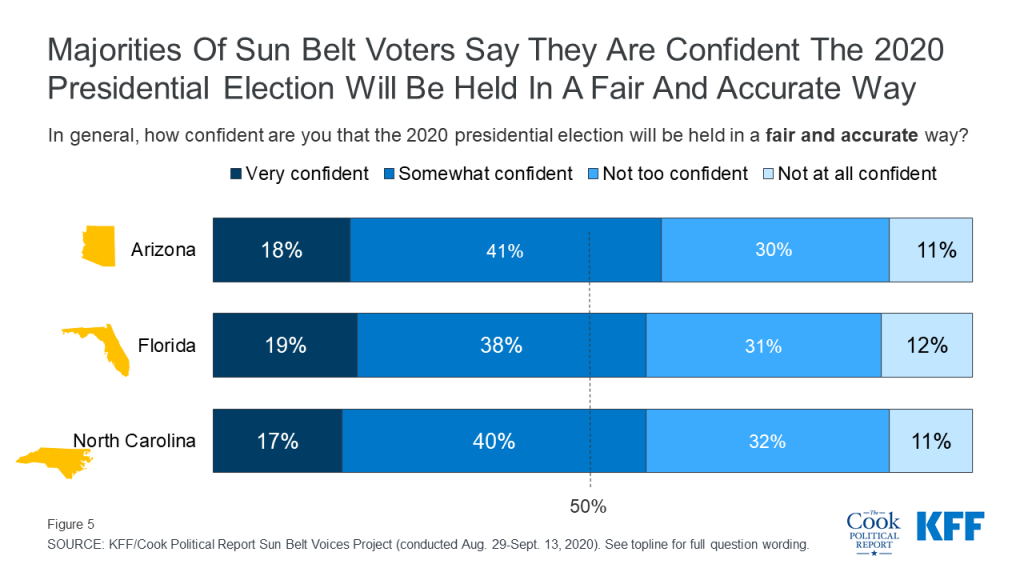
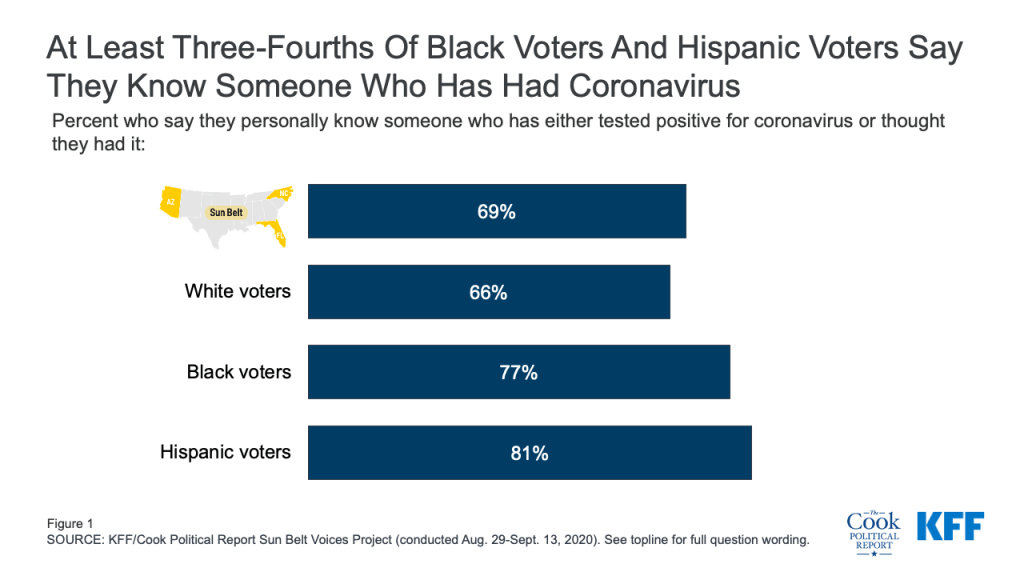
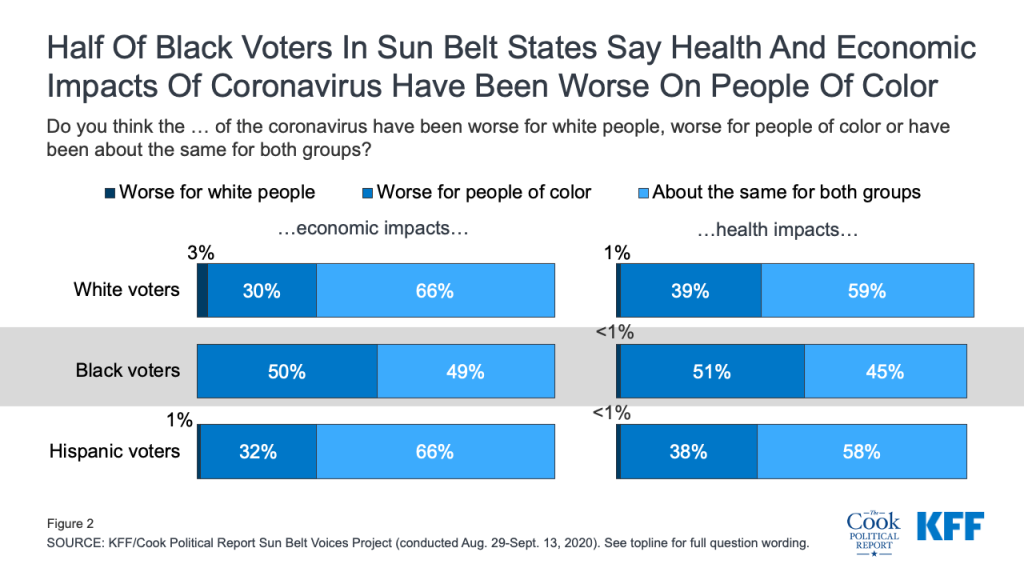
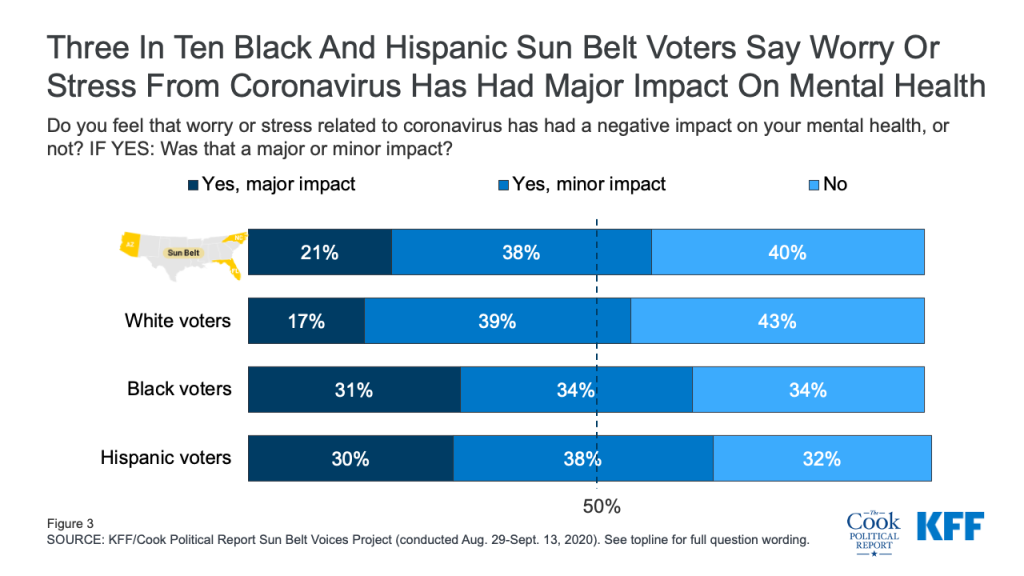
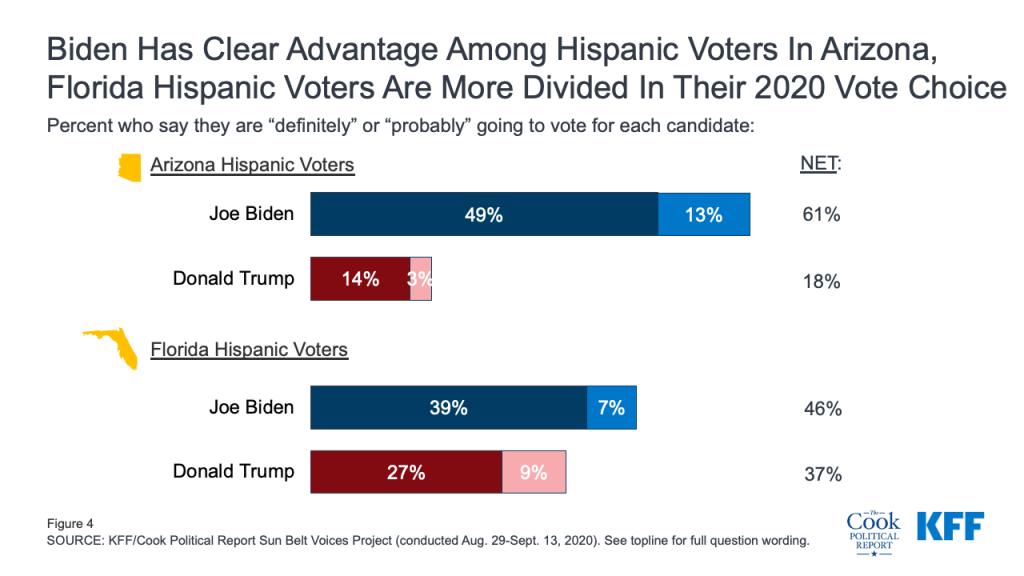
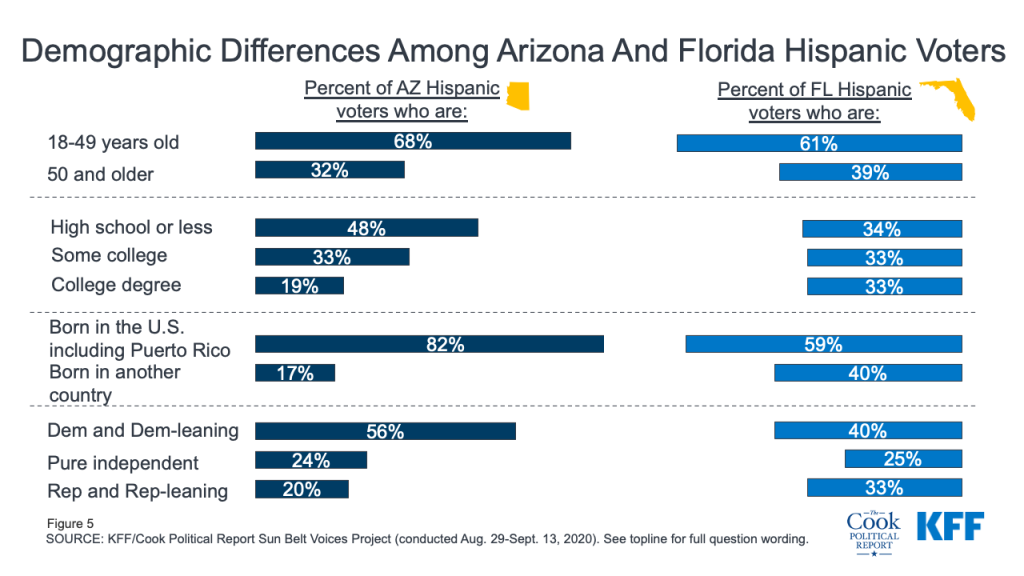
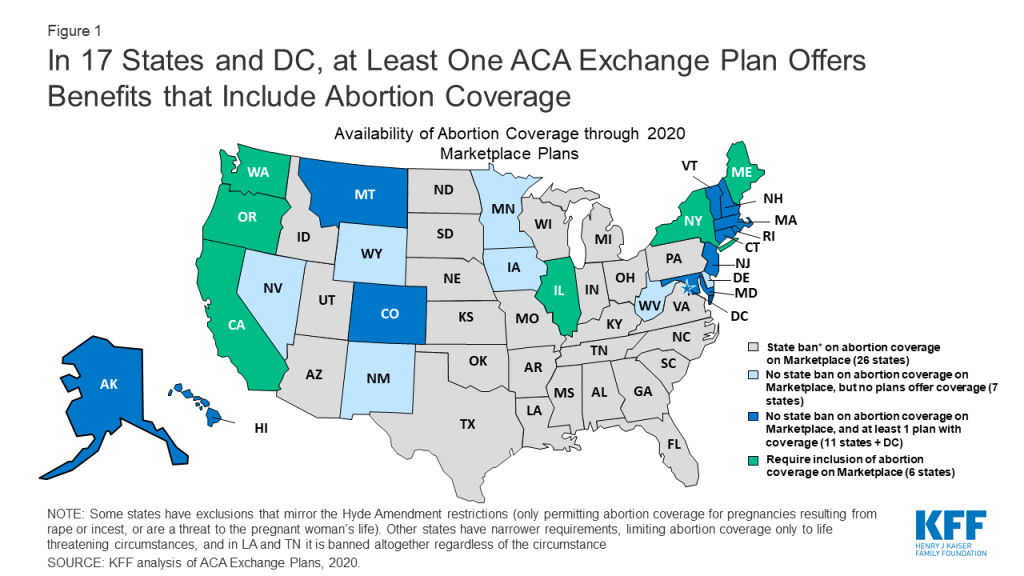
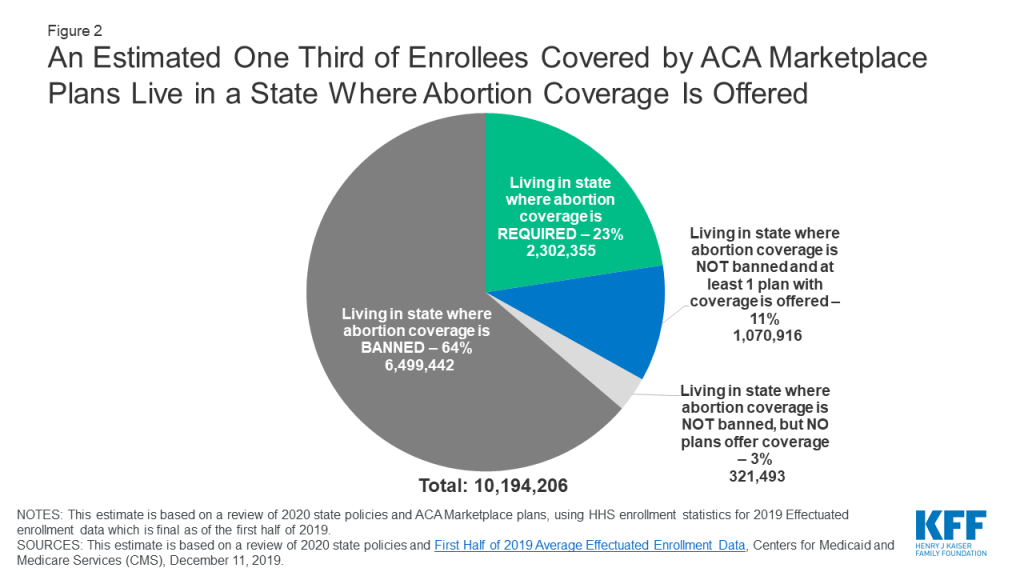
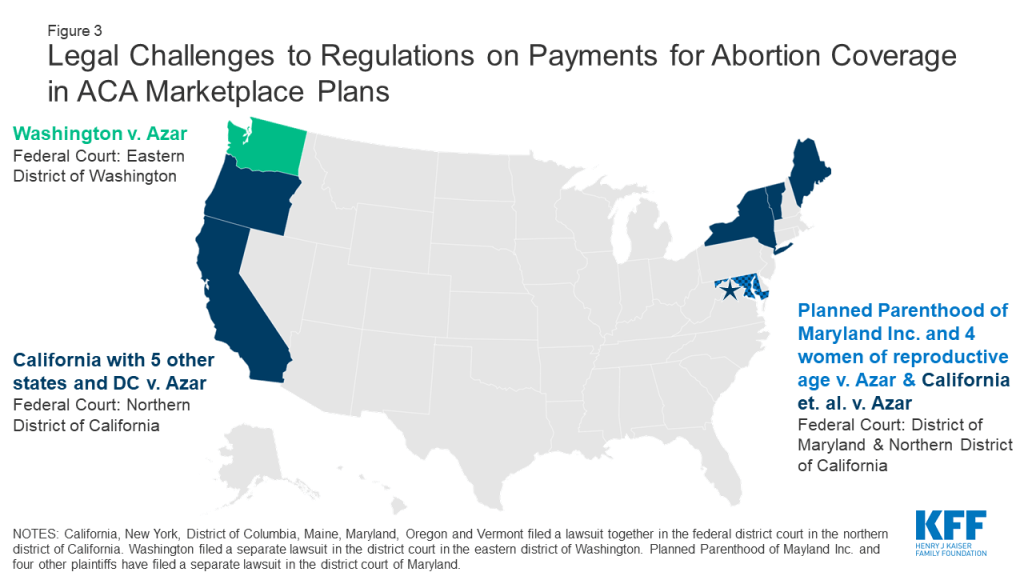
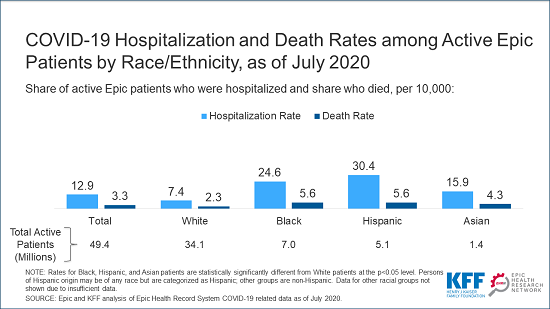
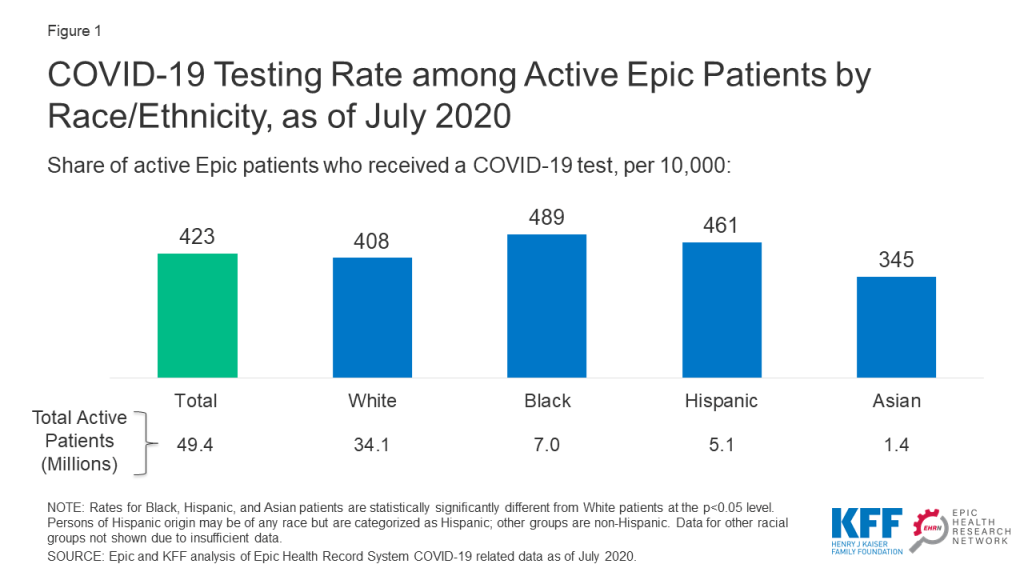
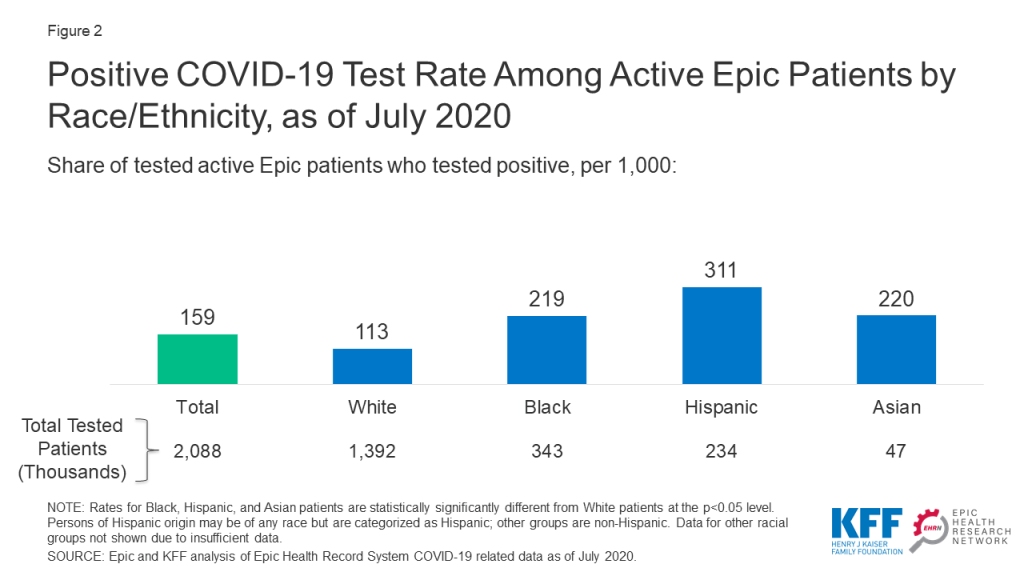
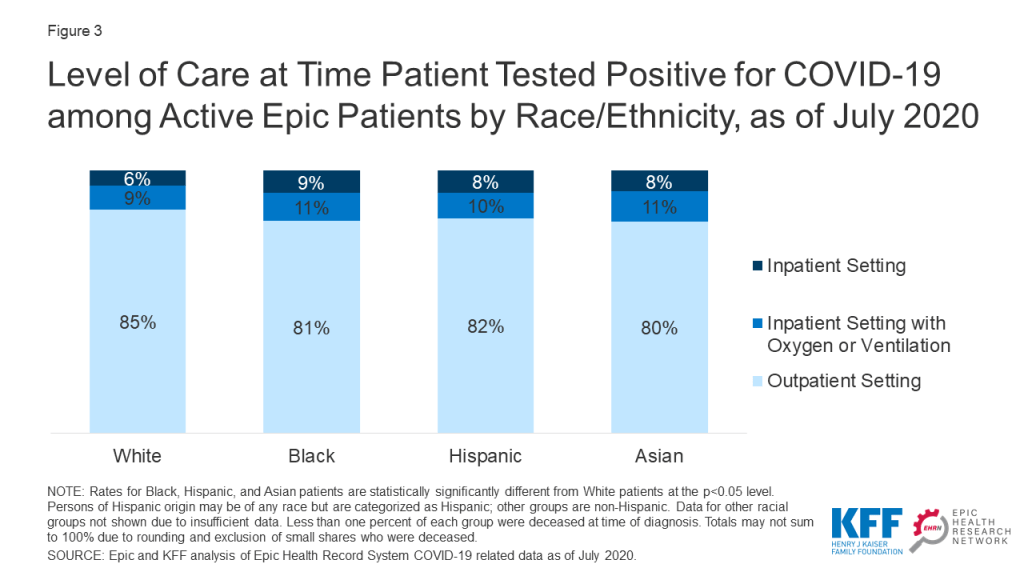
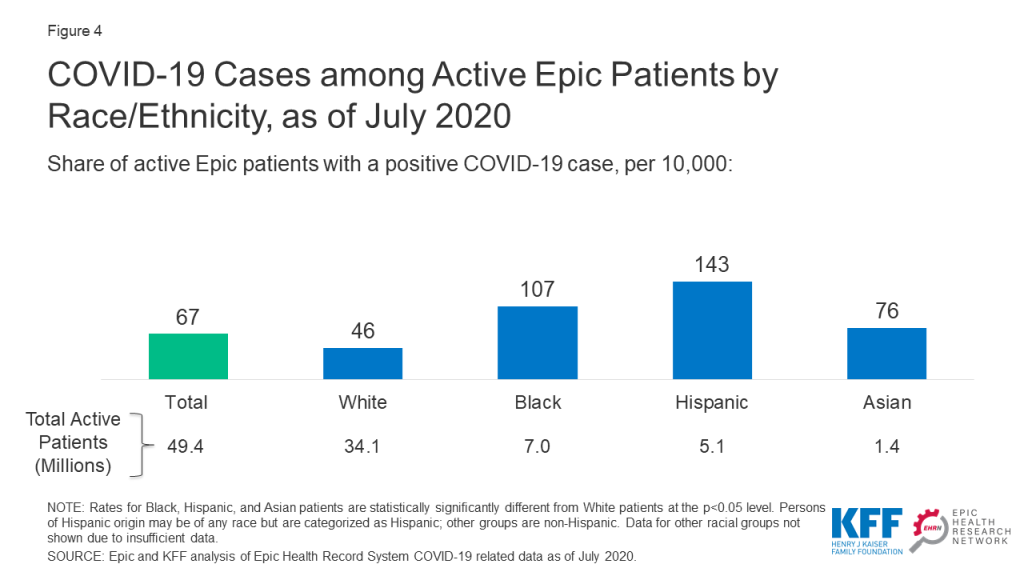
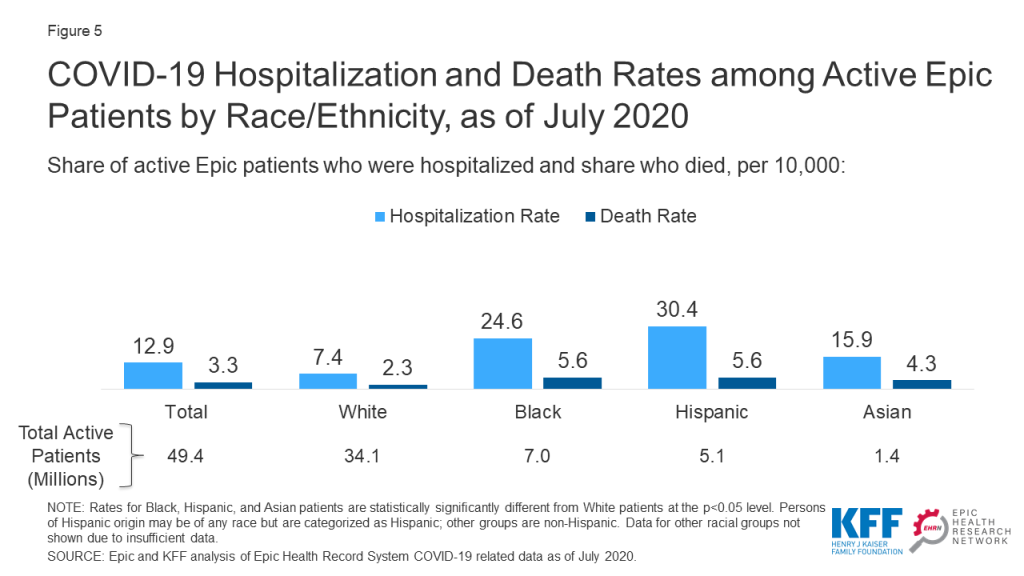
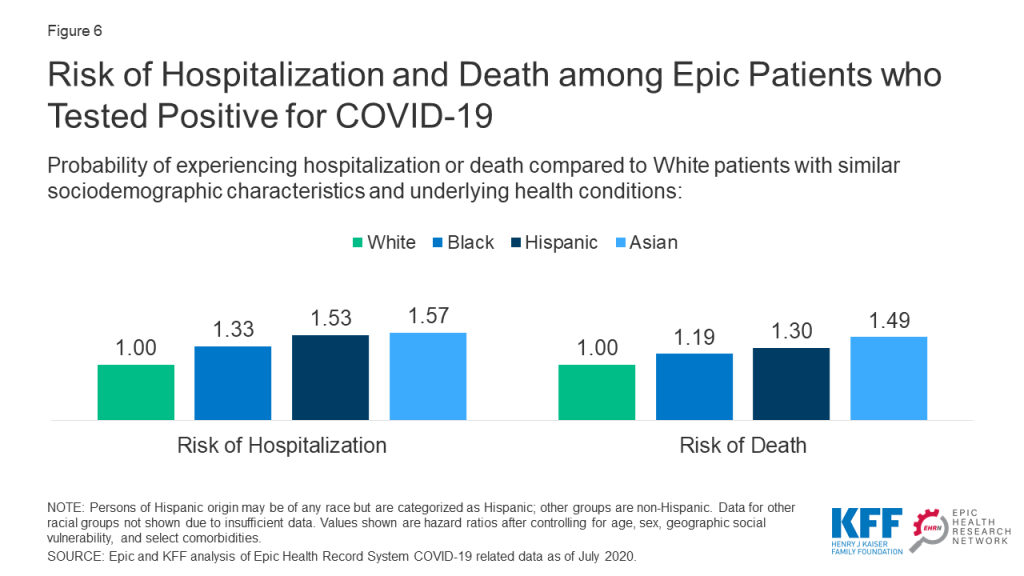
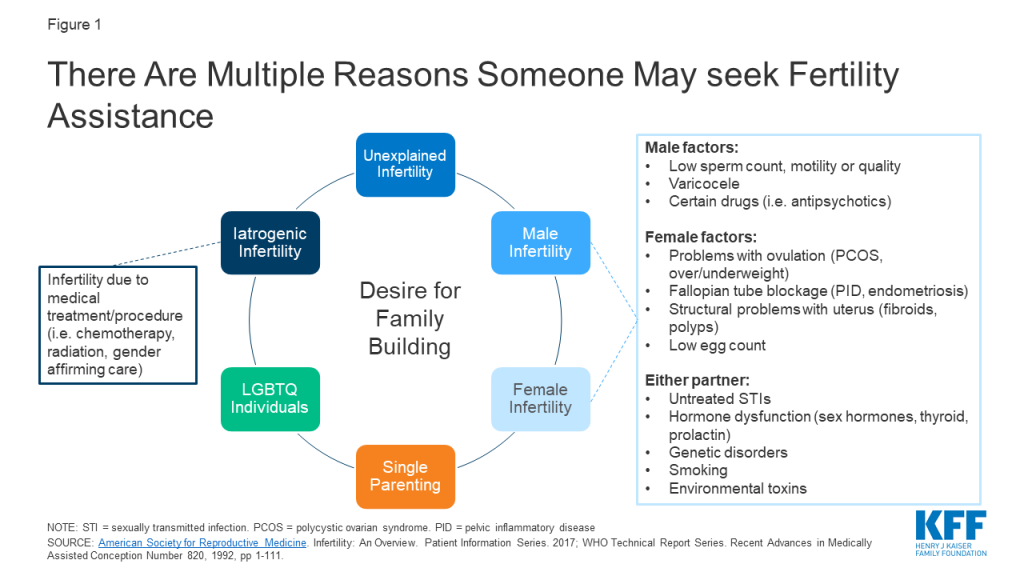
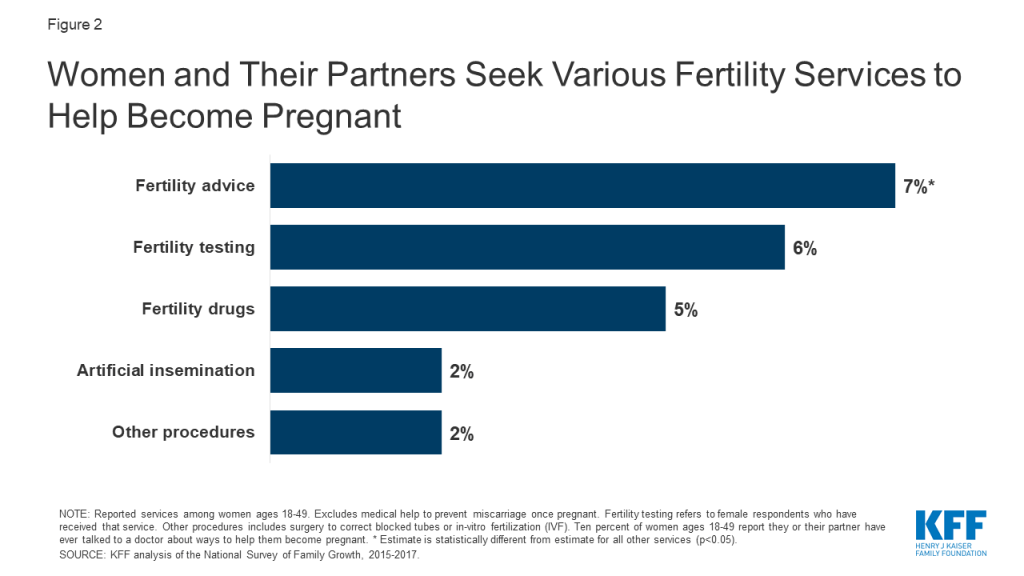
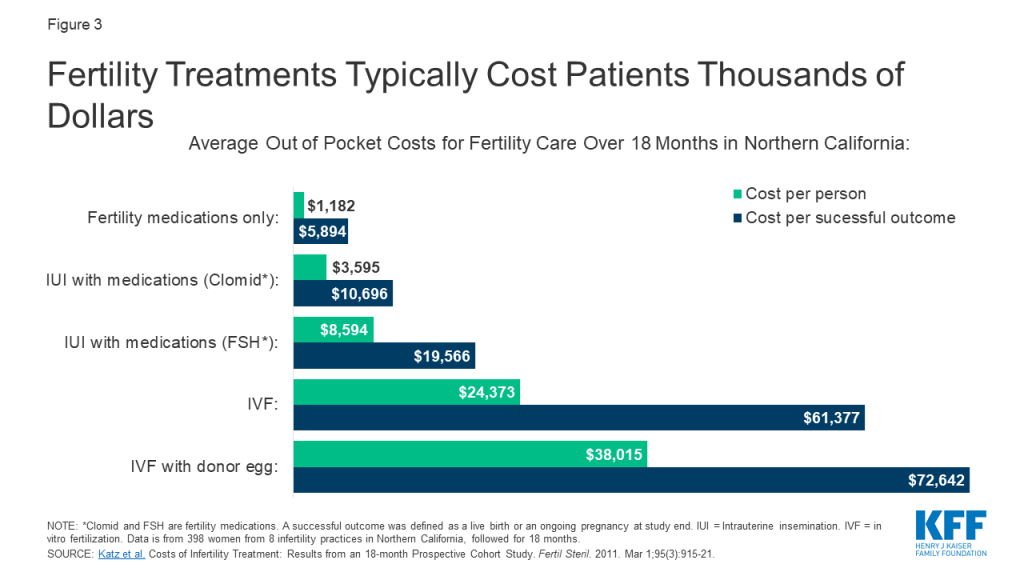
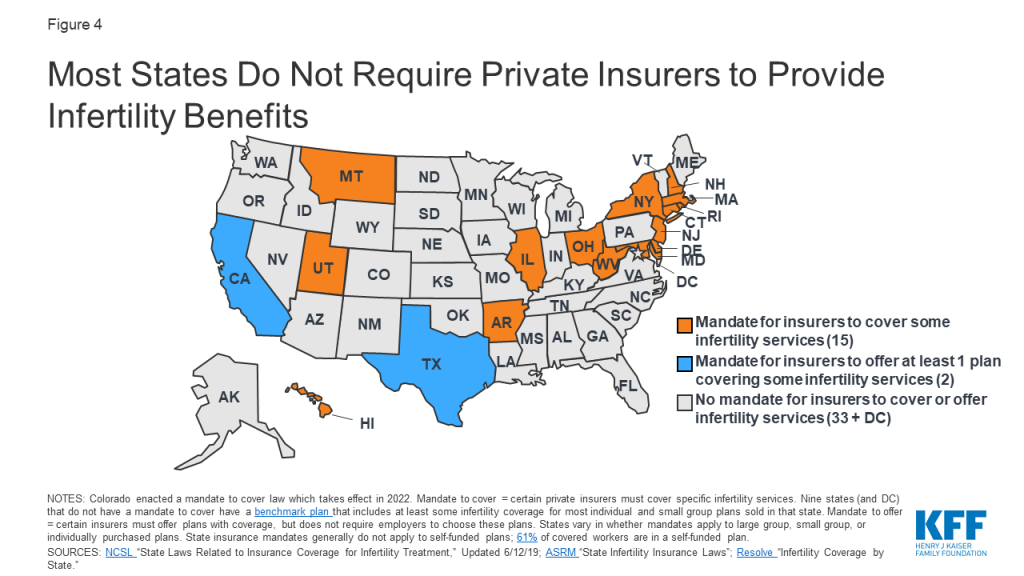
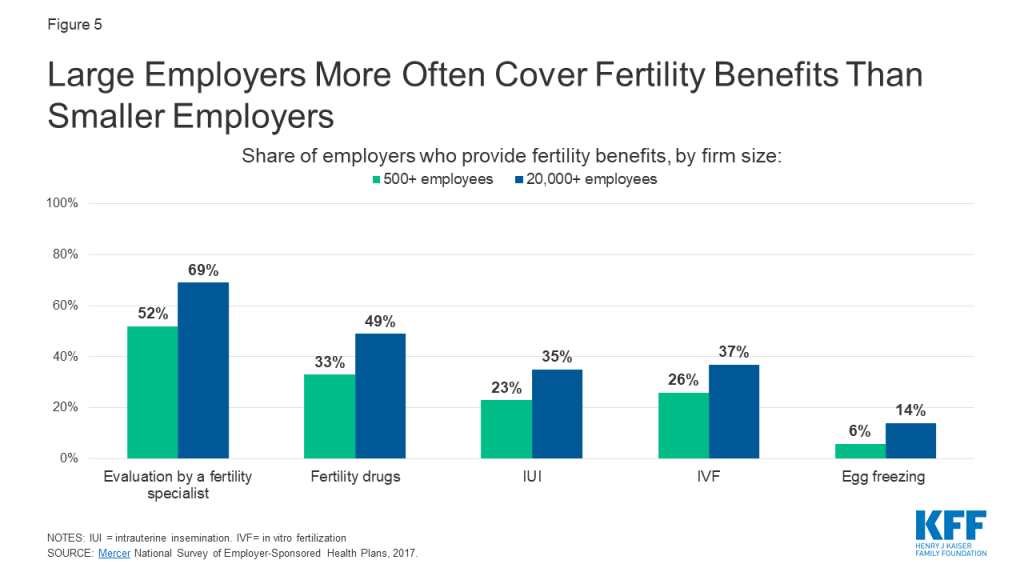
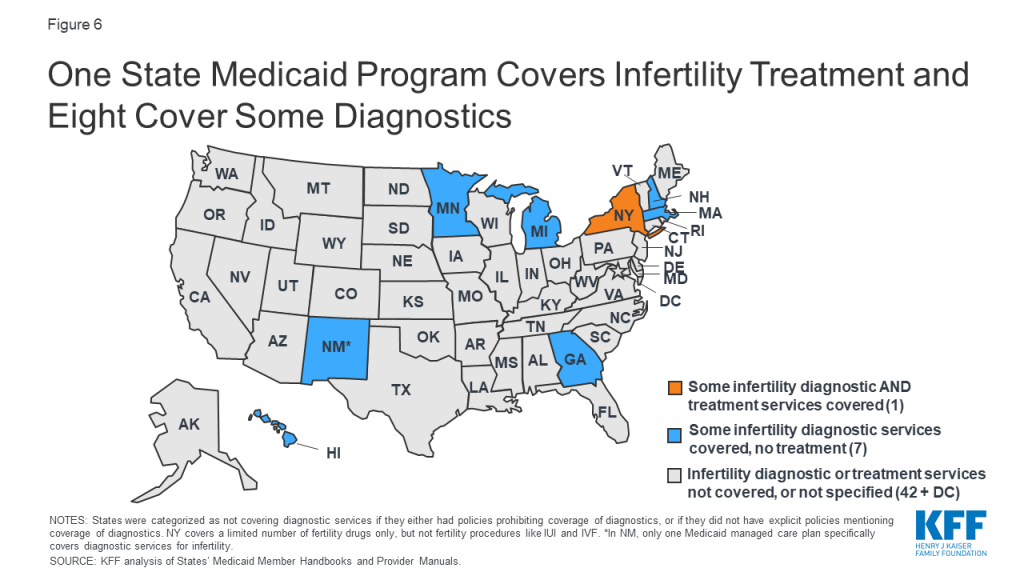

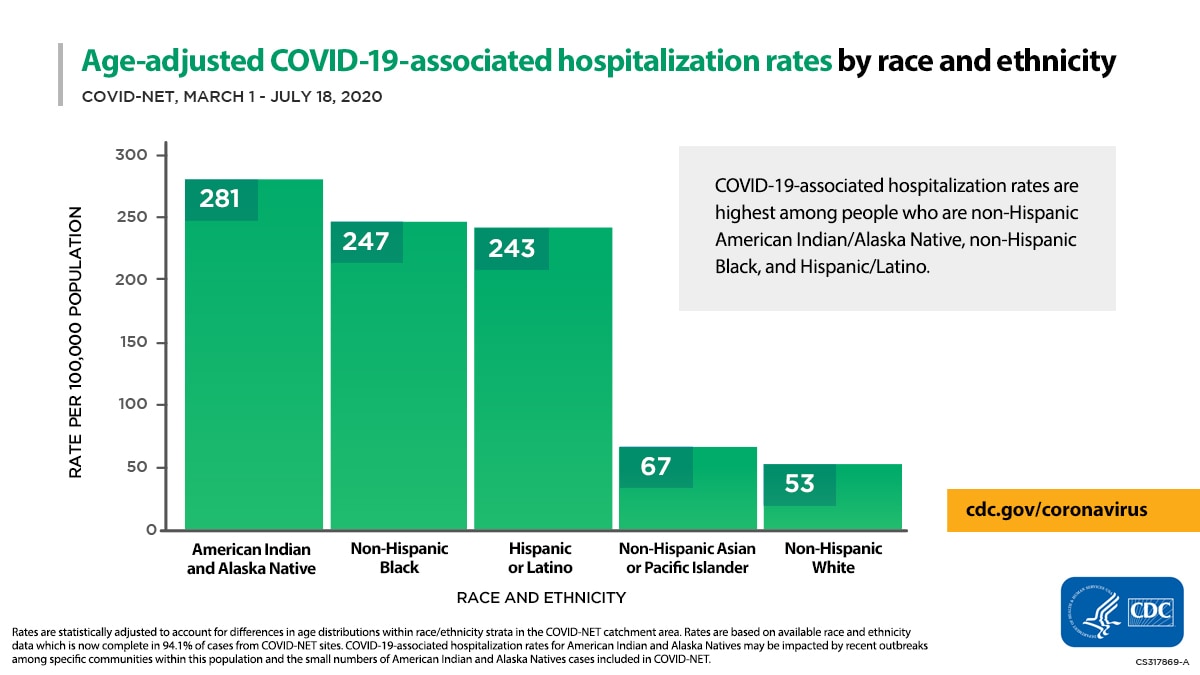{kind=link}