KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
With much attention on the public’s view on Medicare drug price negotiations, the latest KFF Tracking Poll finds large majorities support allowing the federal government to negotiate and this support holds steady even after the public is provided the arguments being presented by parties on both sides of the legislative debate (83% total, 95% of Democrats, 82% of independents, and 71% of Republicans).
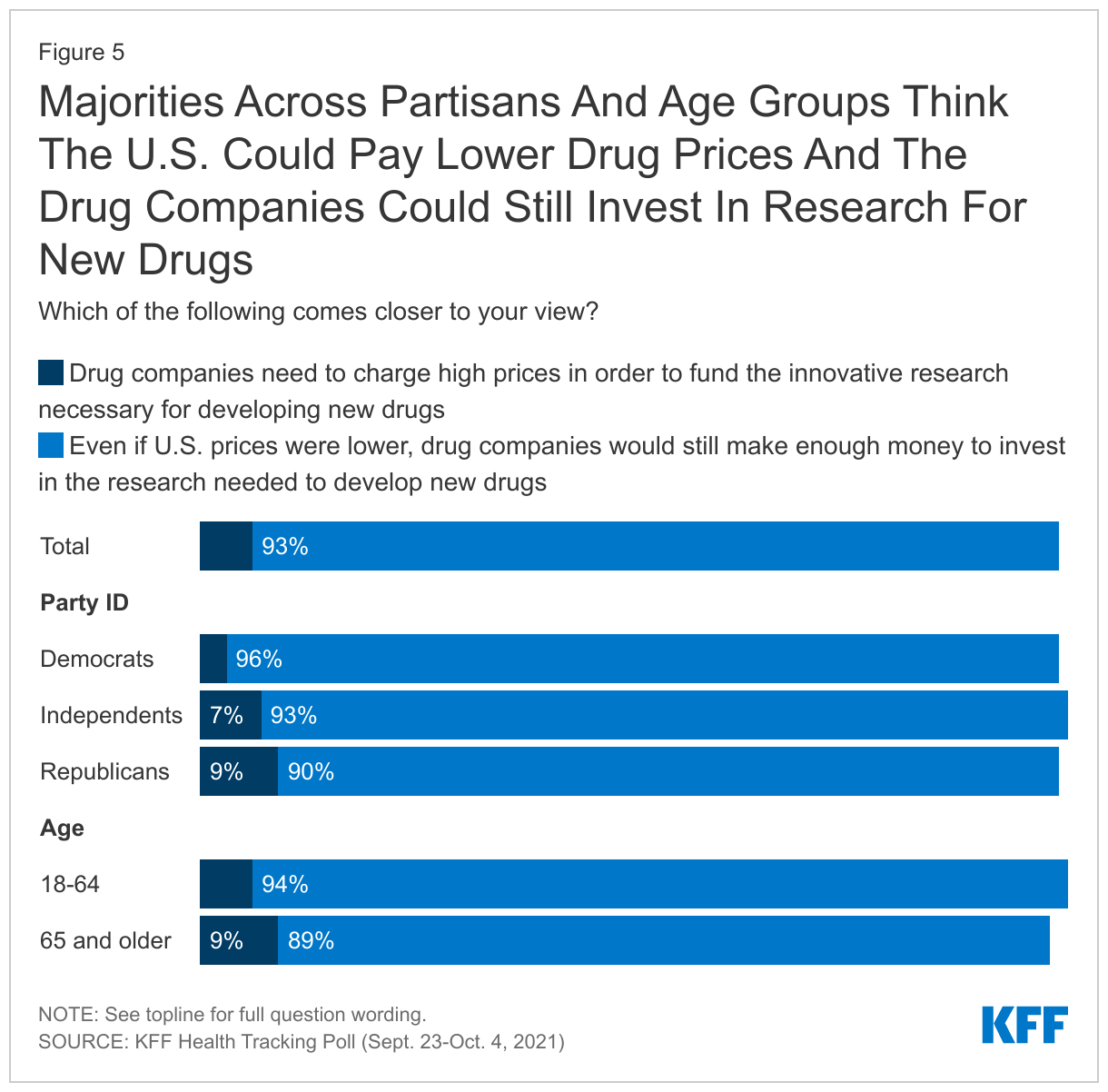
Most adults – across partisans – don’t believe high drug prices are needed for drug companies to invest in new research instead agreeing that “even if U.S. prices were lower, drug companies would still make enough money to invest in the research needed to develop new drugs.” The results suggest that while hearing individual arguments may shift some views, the public still largely favors allowing Medicare drug negotiations when presented with the entirety of the public debate.
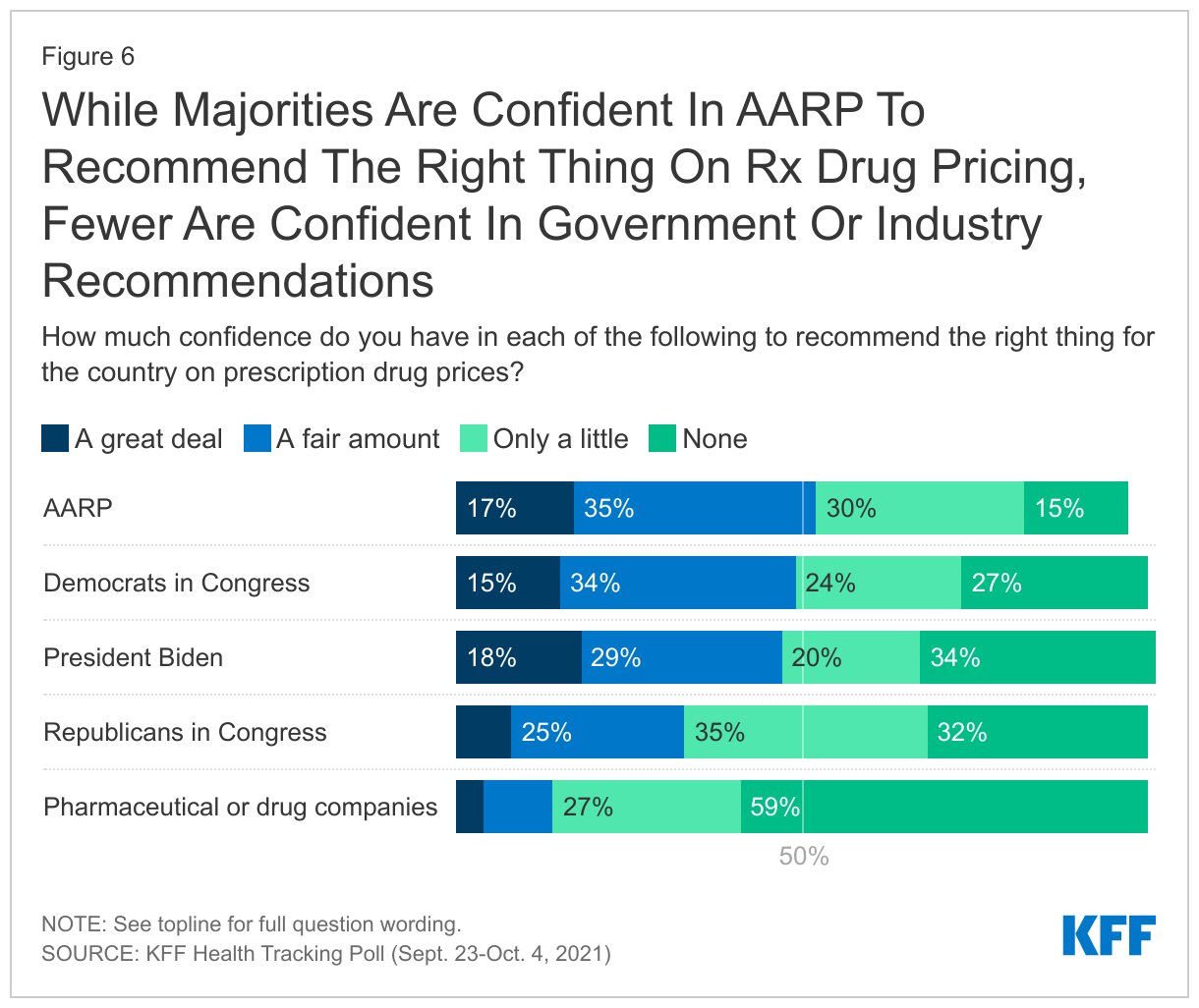
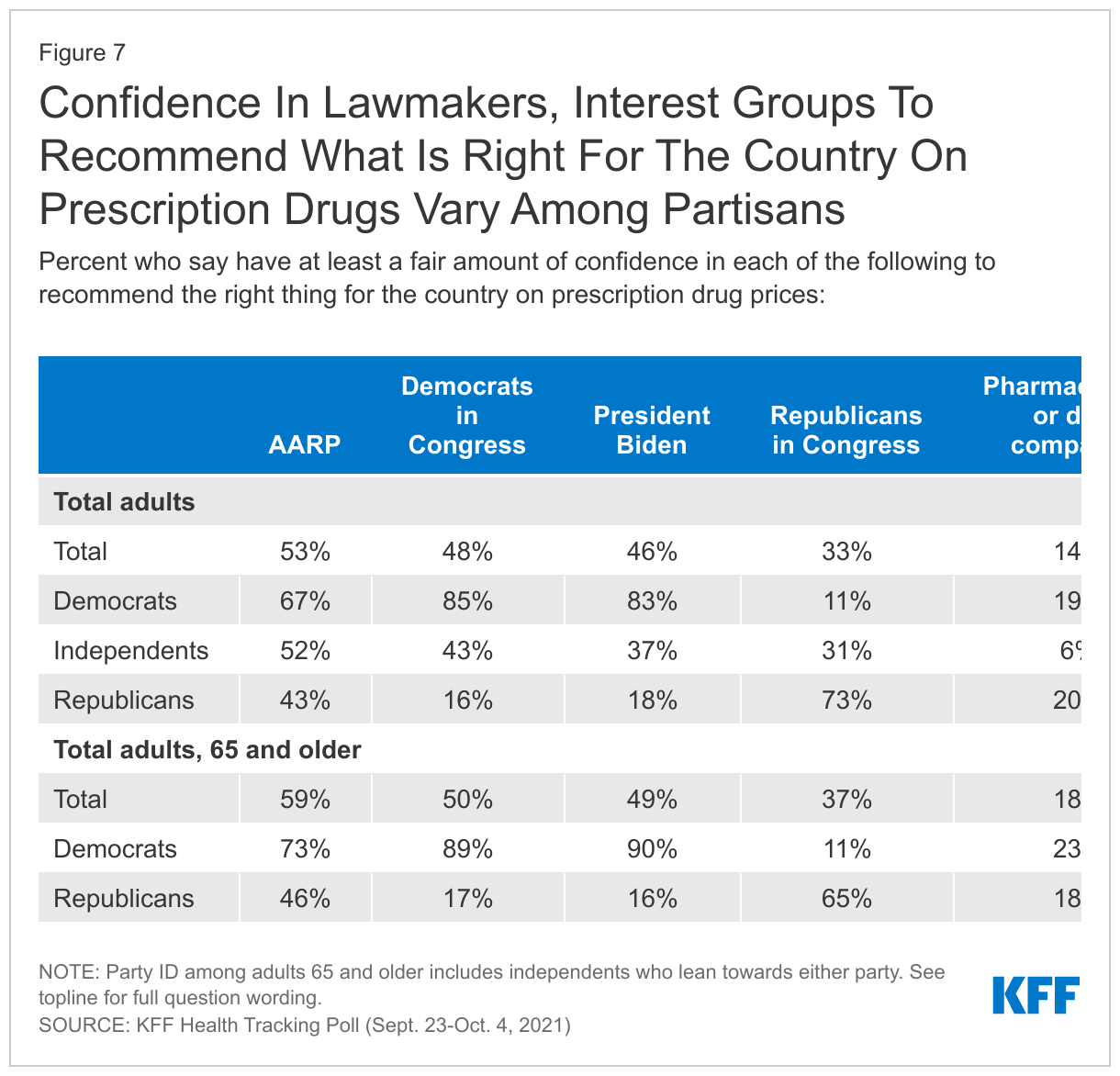
As the debate over how to address prescription drugs continues, less than half of the public say they have confidence in President Biden or either party in Congress to recommend the right thing for the country on prescription drug prices, but Democratic lawmakers fare better than Republican ones. Among interest groups, AARP garners a slight majority of adults saying they are confident in the organization’s ability to recommend the right thing for the country on prescription drug pricing while fewer (14%) have the same level of confidence in pharmaceutical companies.
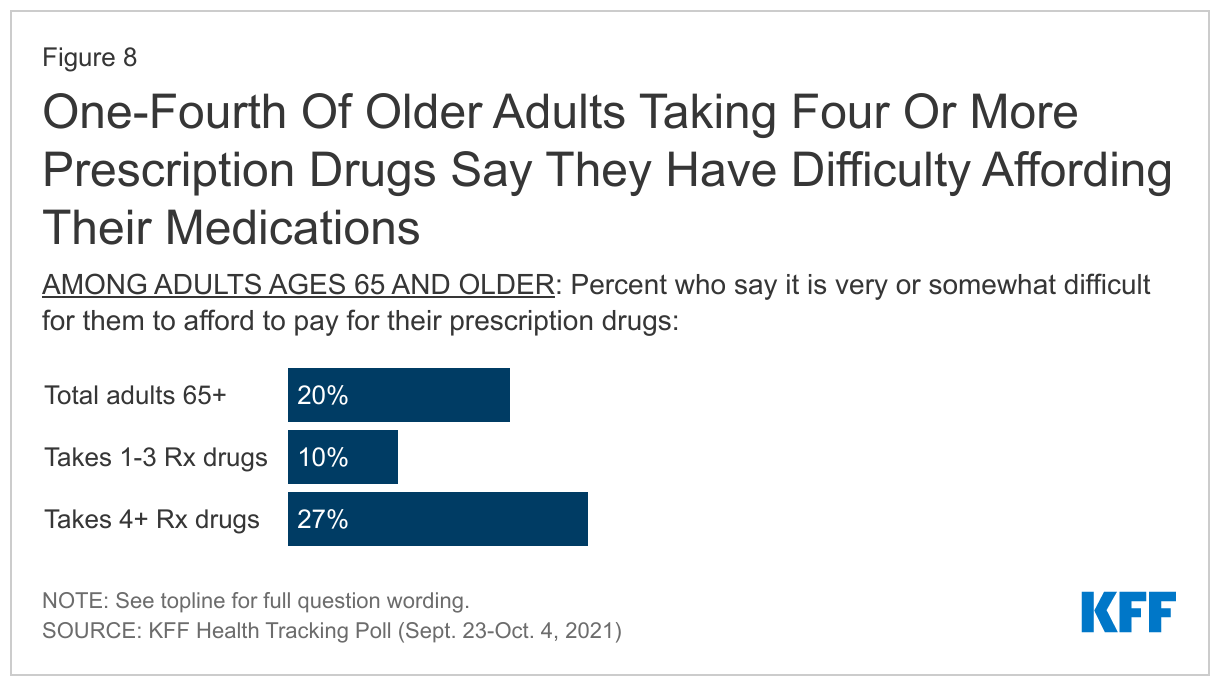
While 85% of adults ages 65 and older report having some type of insurance that helps pay for prescription drugs, one in five older adults still report difficulty affording their prescription drugs, including 17% of older adults with some type of prescription drug coverage. The share who report difficulty affording prescription drugs increases to more than one in four among adults 65 and older who take four or more prescription drugs.
Public Favors Medicare Drug Negotiations
About eight in ten U.S. adults (83%) and adults 65 and older (78%) say they think the cost of prescription drugs is “unreasonable.” Lowering prescription drug prices in the U.S. has been a health care policy priority for decades and earlier this year, it topped the list of health care issues the public wanted Congress to tackle. One proposal aimed at lowering the cost of prescription drugs is to allow the federal government to negotiate the price of prescription drugs for people on Medicare and private insurance.
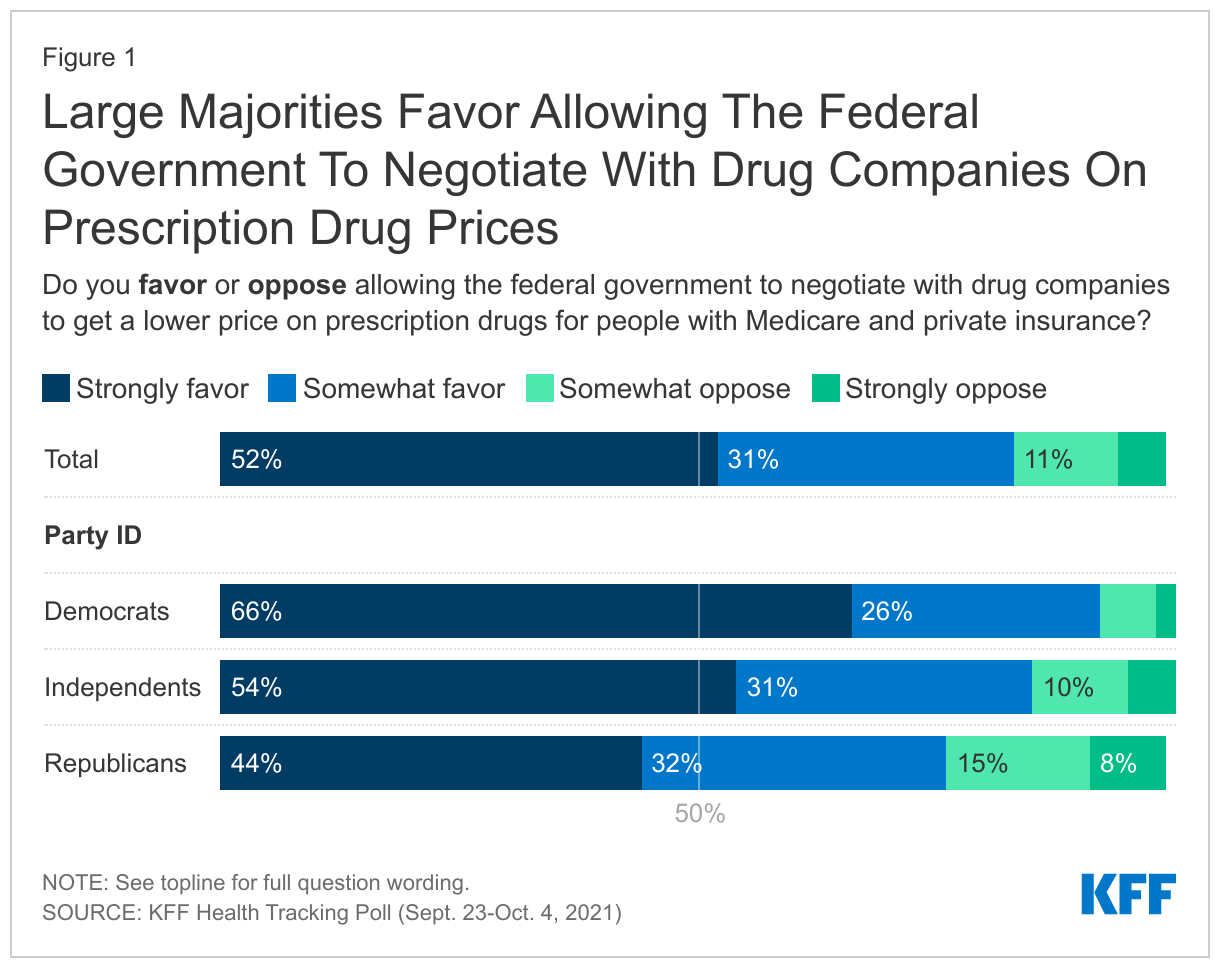
The Democrats’ budget reconciliation package includes a proposal to allow the federal government to negotiate prescription drug prices on behalf of Medicare beneficiaries and people enrolled in private plans. The proposal, which has been part of previous legislative proposals and previously estimated by The Congressional Budget Office (CBO) to result in about $450 billion in savings to Medicare1 , has met strong opposition from the pharmaceutical industry, as well as some lawmakers. Yet, the proposal is largely popular among the public across partisans as well as among seniors, the group most directly impacted by such legislation. Eight in ten adults (83%) say they either “strongly favor” or “somewhat favor” allowing the federal government to negotiate with drug companies as do 84% of older adults (65 and older), including the vast majority (93%) of those ages 65 and older who identify as either a Democrat or lean Democratic, and three-fourths (76%) of older adults who are Republican or lean Republican.
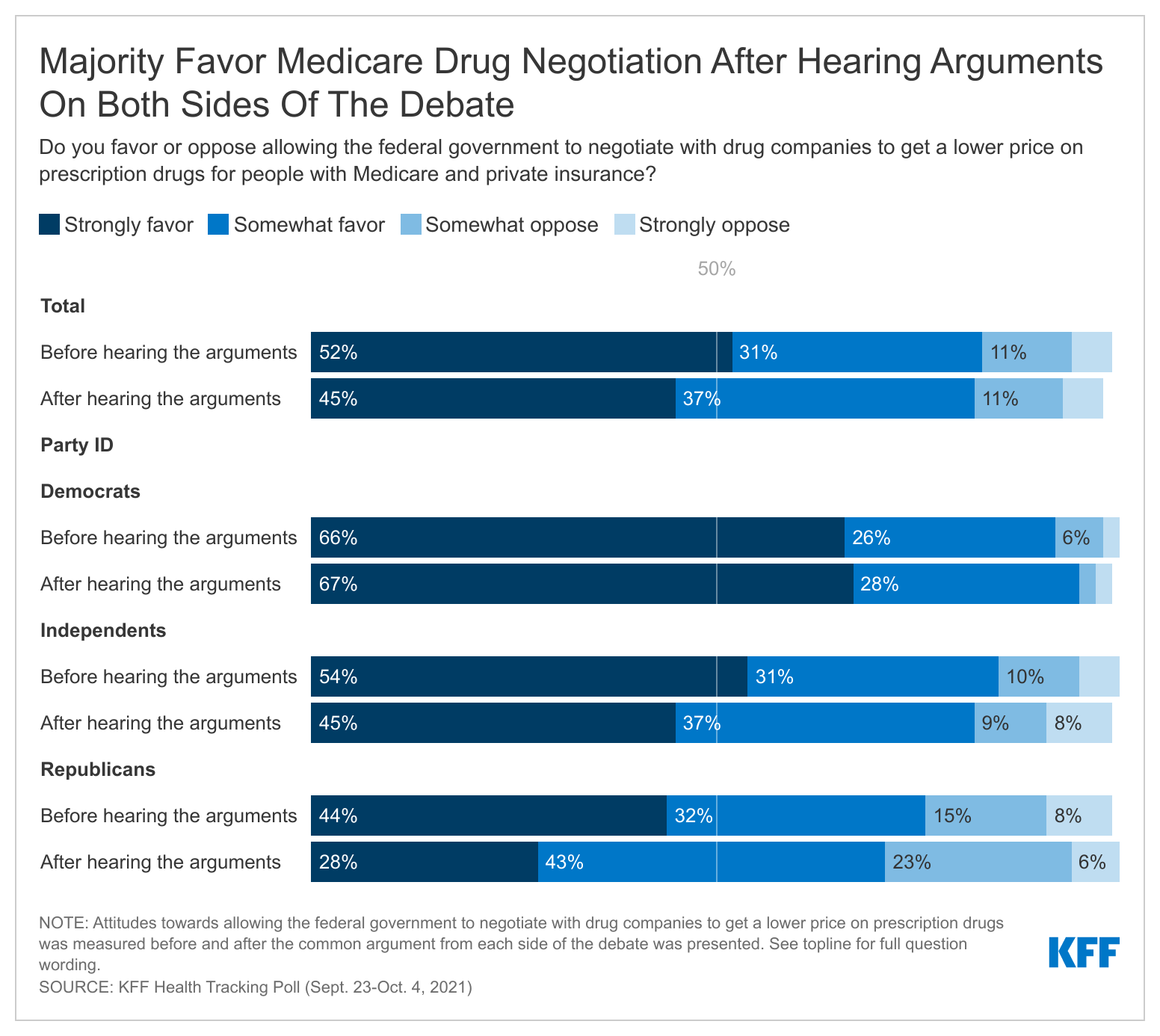
Previous KFF polls have found that some attitudes are malleable on this issue as the public hears arguments from either side of the debate around Medicare drug price negotiations. The latest poll finds that when the public are presented with the main arguments being made by advocates on both sides of the debate, the shift in opinion is modest and support for negotiation remains high. After gauging initial support allowing the federal government to negotiate prices with drug companies, the poll presented respondents with arguments both for and against the proposal.
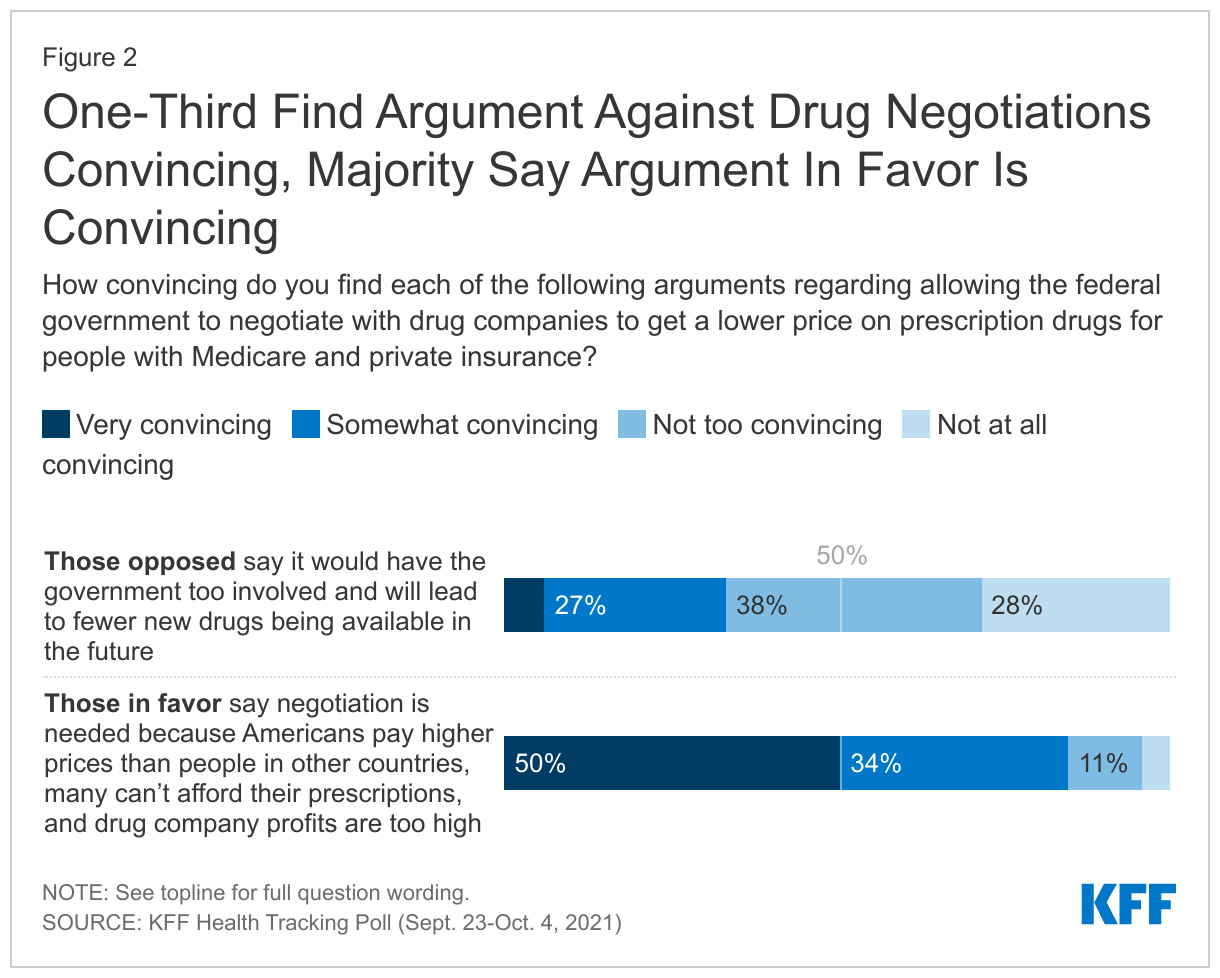
Argument against: People opposed to allowing the federal government to negotiate prices with drug companies say this would have the government too involved and will lead to fewer new drugs being available in the future.
Argument in favor: People in favor of allowing the federal government to negotiate prices with drug companies say this is needed because Americans pay higher prices than people in other countries, many can’t afford their prescriptions, and drug company profits are too high.
One-third of the public say the argument from those opposed to drug price negotiations is convincing compared to a large majority (84%) who say they found the argument from those in favor convincing.
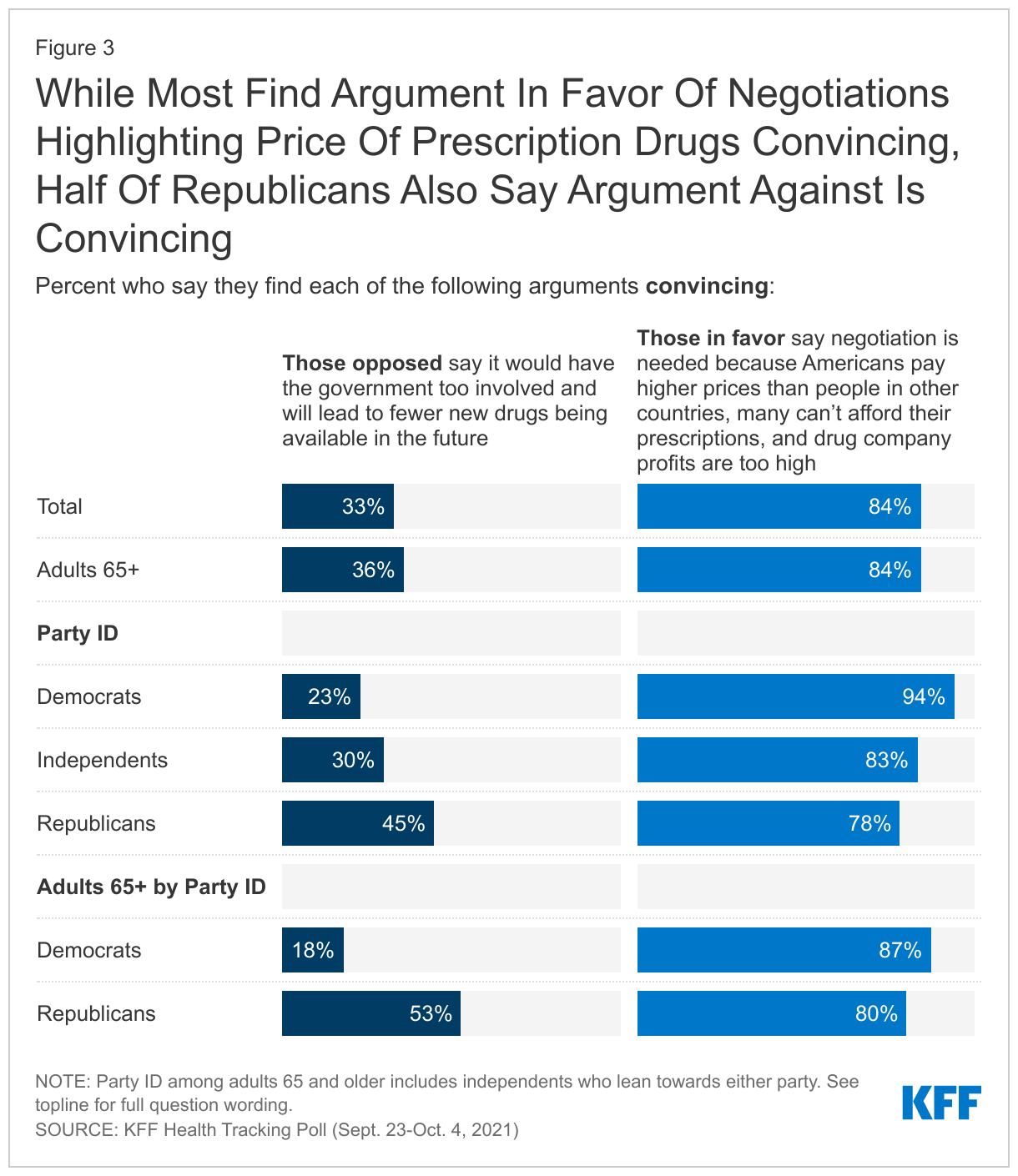
Majorities of all adults as well as those 65 and older, across partisans, say they found the argument in favor of drug negotiations convincing while a smaller share said the same about the argument against the drug negotiations. Nearly half (45%) of all Republicans said the argument from those opposed, which highlights the increased role of the government and the drug companies’ stance that this will lead to fewer drugs coming to market, is also convincing. More than half (53%) of adults 65 and older who are Republican or Republican-leaning say they found the argument against drug negotiations convincing, compared to 18% of Democrat or Democratic-leaning older adults.
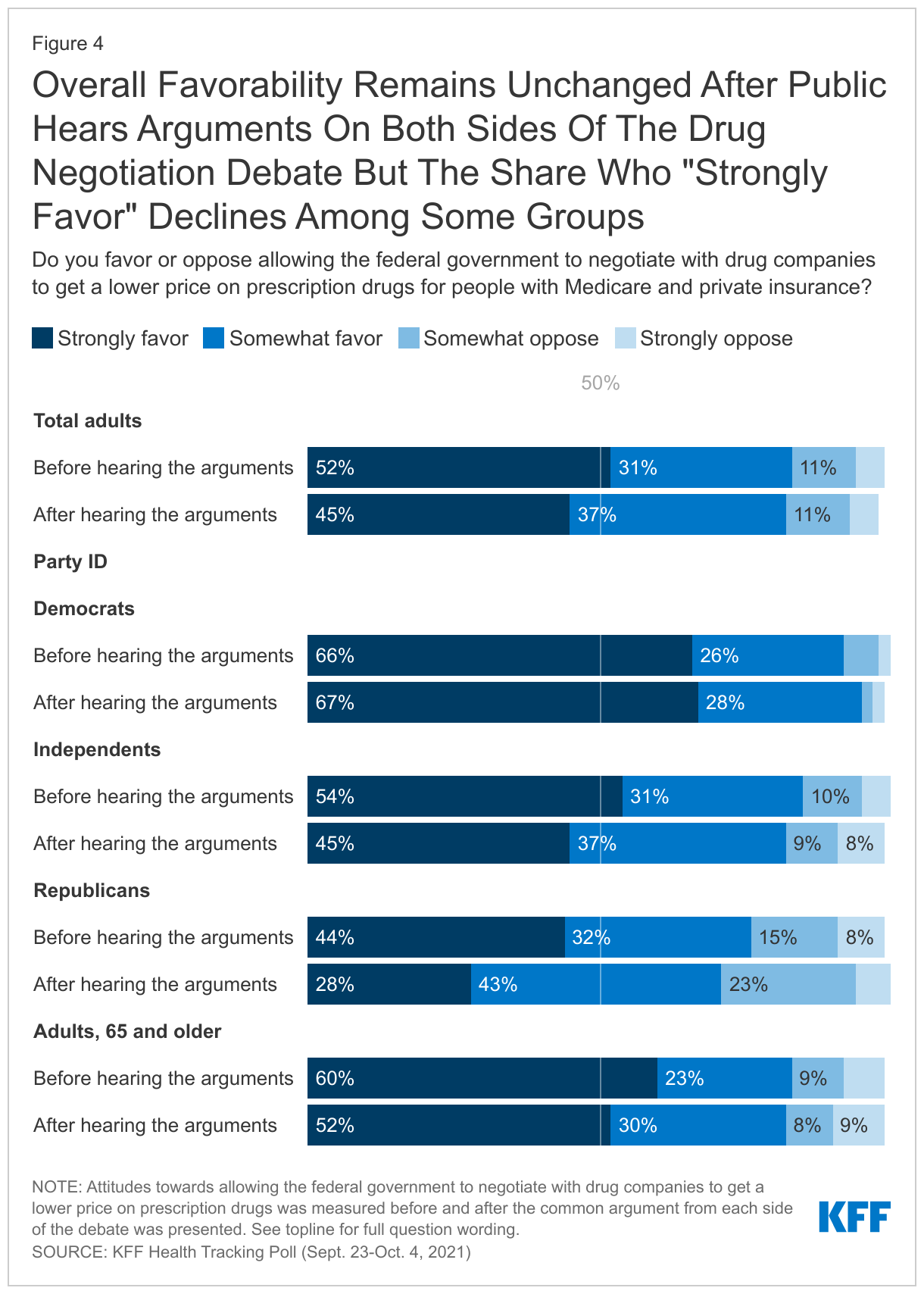
After hearing the arguments for and against the proposal to allow the federal government to negotiate prices with drug companies, attitudes remained relatively unchanged with a majority continuing to favor this proposal. While overall favorability stays the about same, there are some small shifts among groups especially in the share who “strongly favor” this proposal. For example, overall Republican support for drug negotiations decreases five percentage points but there is a large shift among those who say they “strongly favor” after hearing both arguments (44% to 28%). But even so, a majority of Republicans (71%) continue to support the proposal after hearing the arguments.
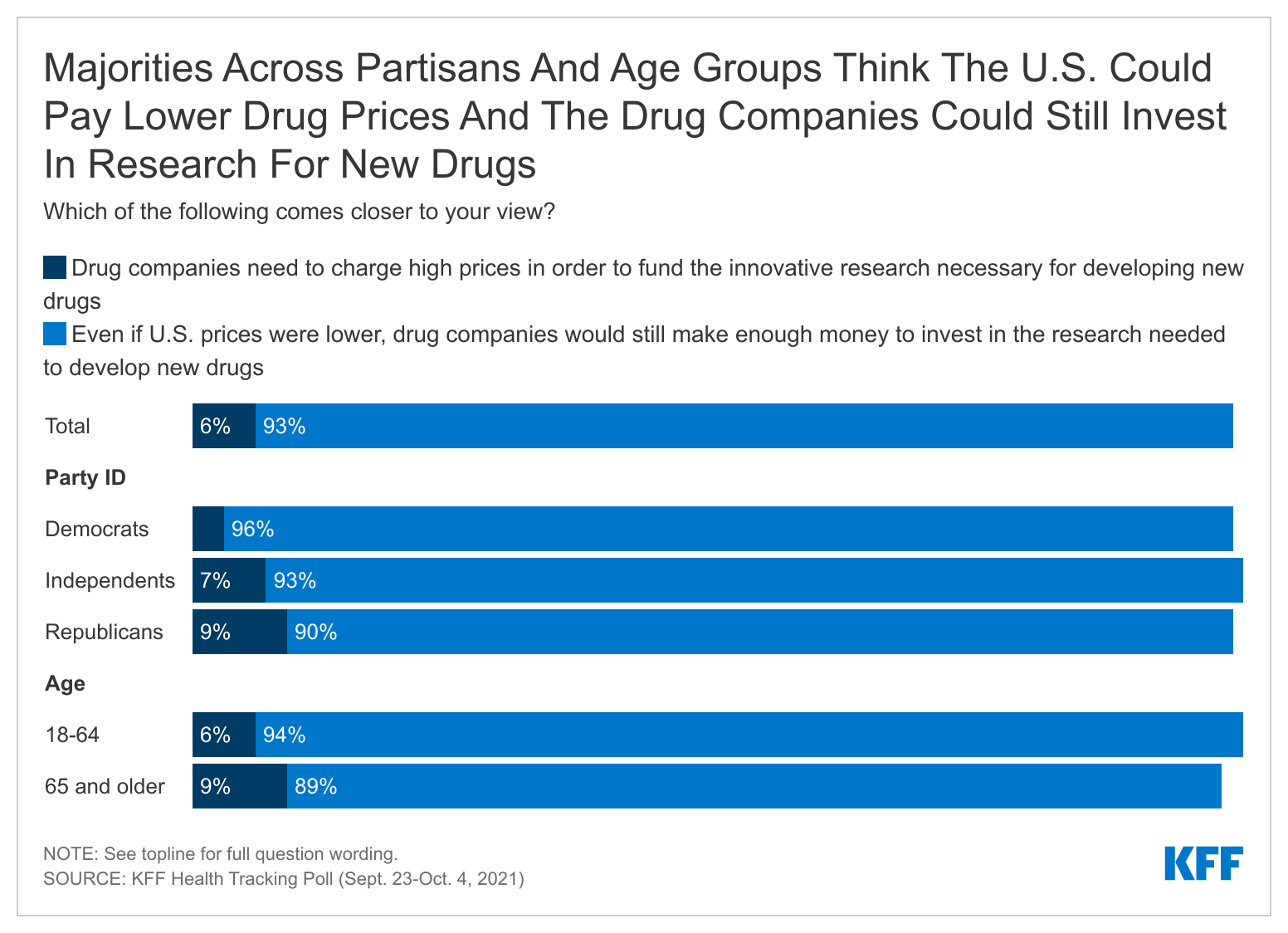
The pharmaceutical industry has argued that allowing the federal government to negotiate prescription drug prices will lead to less research and development of new prescription drugs. KFF polling finds few people (6%) saying they think “drug companies need to charge high prices in order to fund the innovative research necessary for developing new drugs” while a large majority (93%) say “that even if U.S. prices were lower, drug companies would still make enough money to invest in the research needed to develop new drugs” comes closer to their view. This view is consistent across partisanship and age groups.
Few Have Public’s Confidence To Recommend The Right Thing On Prescription Drug Pricing
Neither President Biden nor members of either party in Congress has gained the full confidence of the public to do what’s right for the country on prescription drug pricing. Slightly less than half of the public say they have “a great deal” or “a fair amount” of confidence in President Biden (46%) or Democrats in Congress (48%) to recommend the right thing for the country on prescription drug prices. One-third of the public (33%) say they have at least a fair amount of confidence in Republicans in Congress and few are confident that pharmaceutical companies will recommend the right thing (14%).
A slight majority of adults are confident in AARP’s ability to recommend the right thing for the country on prescription drug pricing. AARP is a non-partisan interest group focusing on the issues that impact adults over the age of 50 that has strongly advocated for Medicare drug negotiations.
AARP also has the confidence of older adults with about six in ten adults 65 and older saying they have at least “a fair amount” of confidence in AARP to recommend what is right for the country on prescription drugs.
One In Five Seniors Struggle Affording Prescription Drugs
The latest KFF Health Tracking Poll finds that 85% of adults ages 65 and older report having some type of insurance that helps pay for prescription drugs. Even still, one in five older adults report difficulty affording their prescription drugs, including 17% of older adults with some type of prescription drug coverage. The share who report difficulty affording prescription drugs increases to more than one in four among adults 65 and older who take four or more prescription drugs.
Methodology
The KFF Health Tracking Poll was conducted in English and Spanish with a nationally representative sample of 1,146 U.S. adults aged 18 or older, including an oversample of 474 adults ages 65 and older. The survey was conducted online and via phone from September 23-October 4, 2021, combining sample from two online probability-based panels and telephone samples recruited from random digit dialing (RDD). Sampling, data collection, weighting and tabulation were managed by SSRS of Glen Mills, PA in close collaboration with Kaiser Family Foundation researchers. The KFF team developed the questionnaire, analyzed the data and contributed financing for the survey.
Panel surveys were conducted through two online panels: (1) The SSRS Opinion Panel, a representative probability-based panel of U.S. adults ages 18 and older, recruited using the SSRS Omnibus poll (a weekly dual-frame RDD telephone survey) and through address-based sampling (ABS) (n=939). (2) The IPSOS KnowledgePanel, a probability-based online panel of U.S. adults ages 18 and older recruited through ABS targeting panelist (n=85). In order to reach adults 65 and older, a group less likely to be reached through an online panel, as well as those who do not have access to the internet, 122 interviews were completed by telephone, (including 79 among those who had previously indicated they do not use the internet).
The combined online, cell phone, and landline sample was weighted to match the sample demographics to estimates for the national population. A multi-stage weighting process was used to adjust for the fact that not all survey respondents were selected with the same probabilities and to account for systematic non-response. In the first weighting stage, adjustments were made regarding the probabilities of selection to the two web panels, and for probability of selection and non-response to the telephone callback samples. Each of these surveys were probability samples of the U.S. adult population that were weighted to the Census Bureau’s March 2020 Current Population Survey (CPS), by gender, age, race/ethnicity, education, and Census region. The data were also weighted to match internet usage metrics based on the U.S. Census’s 2019 American Community Survey, civic engagement metrics based on the September 2019 CPS Volunteering and Civic Life Supplement, and to match party identification within age groups from previous KFF RDD samples.
All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 4 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Most of the Public Lacks Confidence that President Biden, Congressional Democrats or Republicans Will Do the Right Thing on Drug Prices
Allowing the federal government to negotiate with drug companies to lower drug prices for Medicare beneficiaries and people enrolled in private plans – a key cost-saving proposal in the Democrats’ massive reconciliation bill – is favored by large majorities across political partisans, even after they hear arguments from both sides, a new KFF Health Tracking Poll finds.
Initially 83% of the public say they favor allowing the federal government to negotiate with drug companies to lower drug prices on behalf of people enrolled in Medicare beneficiaries and private plans. This includes 91% of Democrats, 85% of independents, and 76% of Republicans, as well as majorities of seniors (84%), who would be most affected by such a provision.
To gauge the potential impact of a national debate over the proposal, the survey asked the public to assess a summary of key arguments being made for and against the plan. Those arguments do little to move the share of the public that favors or opposes the proposal, though affected the intensity of support among Republicans. While Republican support held steady (76% to 71%), the share who “strongly favor” it dipped (44% to 28%).
When asked specifically about each argument, most (84%) of the public, including three-quarters (78%) of Republicans, say the argument in favor – “this is needed because Americans pay higher prices than people in other countries, many can’t afford their prescriptions, and drug company profits are too high” – is convincing.
On the other side, a third (33%) say the argument against – “this would have the government too involved and will lead to fewer new drugs being available in the future” – is convincing. This includes nearly half (45%) of Republicans.
The public also rejects the argument that high prices are necessary for supporting research into new drugs.
When asked which comes closer to their view, 93%, including 90% of Republicans, say “that even if U.S. prices were lower, drug companies would still make enough money to invest in the research needed to develop new drugs”, while just 6% say that “drug companies need to charge high prices in order to fund the innovative research necessary for developing new drugs.”
The poll also reveals that the public does not have a lot of confidence in Washington to address the issue. Less than half the public say they have confidence in President Biden (46%) and Democrats in Congress (48%) to recommend the right thing on prescription drug prices, while a third say they have confidence in Republicans in Congress (33%).
Among key interest groups, more say they are confident in the recommendations of AARP (53%), which has strongly advocated for drug-price negotiations, than say so about drug companies (14%).
Additional findings from the KFF Health Tracking Poll will be released later this week.
Designed and analyzed by public opinion researchers at KFF, the KFF Health Tracking Poll was conducted from September 23-October 4 among a nationally representative sample of 1,146 adults including an oversample of adults, 65 and older (474). Interviews were conducted in English and Spanish online (1,024) and by telephone (122). The margin of sampling error is plus or minus 4 percentage points for the full sample. For results based on subgroups, the margin of sampling error may be higher.
In Focus Groups, Direct Care Workers and Unpaid Caregivers Describe Low-Wage, Physically-Challenging Work That is Often Mentally Overwhelming and Marked By Uncertainty
In recent focus group interviews, 32 paid direct care workers and unpaid caregivers who assist seniors and people with disabilities with self-care and household activities describe daily work defined by low pay, physical demands and mental stress that has been made worse by the pandemic.
KFF conducted the four focus groups in July and August 2021 with 24 direct care workers and eight unpaid caregivers to help provide context for the ongoing debate in Congress about increasing federal funding for Medicaid home and community-based services (HCBS). Medicaid is the nation’s primary payer for such services. Among other uses, new funding could help raise wages for direct care workers, provide training opportunities and offer supports to family caregivers such as respite care and peer supports.
Key takeaways from the focus groups include:
These jobs are mentally demanding as well as physically taxing. Paid caregivers reported that the mental demands of their jobs had intensified during COVID-19. Among other things, they cited the fear of infecting their clients or bringing the virus home to infect their families. Unpaid family caregivers described the mental demands associated with caregiving as often “overwhelming.”
Uncertainty is a constant. A number of paid caregivers described regularly experiencing uncertainty about whether they would be able to leave work at the end of their shift due to staffing shortages and scheduling challenges that were exacerbated by the pandemic. (It is unclear how vaccination mandates might contribute to workforce shortages, as participants in the paid direct care worker groups were divided about whether to receive the COVID-19 vaccine.)
Caregivers feel there is a mismatch between their work and their wages. Paid direct care workers universally agreed that their wages are low and do not reflect the demands of their jobs. They described their financial situation as “getting by” and “living paycheck to paycheck.” Some participants in the unpaid caregiver group said the demands of caregiving made it impossible to have paid work.
The racially and geographically diverse group of focus group participants worked in a range of job types, both full- and part-time, and cared for people with a variety of disabilities and long-term care needs. The report presents key highlights from the focus groups including caregiver characteristics; physical and mental caregiving demands; the impact of workforce shortages; wages, finances, and opportunities for advancement; and what caregivers would like policymakers to know about their work. While these focus groups are not necessarily generalizable to all caregivers, they can provide insight into their experiences to help inform current policy debates.
The American Rescue Plan Act (ARPA), passed earlier this year, provides states with a one-year, 10 percentage point increase in federal Medicaid matching funds (FMAP) for HCBS. Congress is currently debating efforts to increase federal matching funds, without a time limit, for state spending on Medicaid HCBS as part of an overall budget reconciliation package, although the final funding amount remains in flux as policymakers weigh competing priorities.
The COVID-19 pandemic has intensified longstanding issues surrounding the unmet need for home and community-based services (HCBS) among seniors and people with disabilities and shortages in the direct care workforce that provides these services. The Biden Administration recently announced that it will require vaccination for staff in Medicaid and Medicare certified home health agencies, along with nursing homes and other health care settings. However, a notable share of direct care workers are vaccine hesitant, so new requirements may exacerbate existing staff shortages. Efforts to develop policies to expand HCBS and strengthen the direct care workforce have centered on Medicaid as the primary payer for these services. The American Rescue Plan Act (ARPA), passed earlier this year, provides states with a one year 10 percentage point increase in federal Medicaid matching funds (FMAP) for HCBS. Congress is currently debating efforts to build on the ARPA investments as part of an overall budget reconciliation package, and the final funding amount remains in flux as policymakers weigh competing priorities.
To help inform the ongoing debate, KFF conducted four focus groups in July and August 2021 with direct care workers and unpaid caregivers who provide HCBS, assisting seniors and people with disabilities with daily self-care and household activities. These focus groups are not necessarily generalizable to all caregivers, but can provide insight into their experiences to help inform current policy debates. Key findings include the following:
In addition to physical demands, paid caregivers reported that their jobs had mental demands, which intensified during the pandemic. A number of unpaid family caregivers explained that the mental demands associated with caregiving were often “overwhelming.”
A number of paid caregivers described regularly experiencing uncertainty about whether they would be able to leave work at the end of their shift due to staffing shortages and scheduling challenges, which were exacerbated by the pandemic. It is unclear how vaccination mandates might contribute to workforce shortages, as participants in the paid direct care worker groups were divided about whether to receive the COVID-19 vaccine. While the majority of those weighing in on this issue were vaccinated, a vocal minority were unvaccinated. Among the unvaccinated, some expressed hesitancy, while at least one said their opposition was strong enough to lead them to leave their job if faced with an employer mandate.
It is perhaps not surprising, but participants in the paid direct care worker groups universally agreed that their wages are low and do not reflect the demands of their jobs. They described their financial situation as “getting by” and “living paycheck to paycheck.” Those who live in a household with two wage earners universally noted that their spouse was the “primary breadwinner” and observed that their earnings alone were not enough to support a family. Some participants in the unpaid caregiver group said that their caregiving demands made it impossible for them to have paid work.
Efforts to develop policies to expand HCBS and strengthen the direct care workforce have centered on Medicaid as the primary payer for these services. The American Rescue Plan Act, passed earlier this year, provides states with a one year 10 percentage point increase in federal Medicaid matching funds (FMAP) for HCBS. President Biden then proposed a landmark $400 billion federal investment in Medicaid HCBS as part of his American Jobs Plan. Funding in the current House bill has been reduced to $190 billion, the majority of which would be available as a permanent seven percentage point FMAP increase for HCBS for states that choose to participate and meet program requirements. This legislation is part of the overall budget reconciliation package, and the final funding amount remains in flux as policymakers weigh competing priorities.
To help inform the ongoing debate, KFF conducted four focus groups in July and August 2021 with direct care workers and unpaid caregivers who provide HCBS, assisting seniors and people with disabilities with daily self-care and household activities. The groups included a total of 24 paid direct care workers and eight unpaid caregivers. Participants worked in a range of job types and cared for people with a variety of disabilities and long-term care needs. We sought diversity in how long people had worked as caregivers, those working full vs. part-time, and racial/ethnic background. We also sought to recruit people primarily serving Medicaid enrollees. All groups were held by online video conference, allowing for participation from states across the country.1 KFF worked with PerryUndem Research/Communication to conduct the focus groups.
This issue brief presents findings from the focus groups including caregiver characteristics; physical and mental caregiving demands; the impact of workforce shortages; wages, finances, and opportunities for advancement; and what caregivers would like policymakers to know about their work.
Who are caregivers?
The paid direct care workers in our focus groups generally reflect the national data in terms of gender, race/ethnicity, and full vs. part-time work status. Box 1 describes national data about caregiver demographics. Most of our focus group participants are women and included people who identified as white, Black, Hispanic, and Asian. They work in a variety of job types, including home health aides, personal care attendants, direct service professionals (DSPs), and certified nursing assistants, and most work full-time. Workers’ years of experience ranges from less than one to over 25 years, with most having worked between one and five years in the field. Most are employed by provider agencies, though a few worked for state agencies, and some were hired directly by clients who self-direct their Medicaid services.
The direct care worker focus group participants care for people with a range of disabilities and in a variety of community-based settings. Their clients include seniors, including some with dementia; nonelderly adults with physical disabilities such as Parkinson’s disease, cerebral palsy, multiple sclerosis, and spina bifida; children and adults with intellectual or developmental disabilities (I/DD) such as Down’s syndrome and autism; children who are medically fragile; and people with mental illness. They work in individual client homes, group homes, day programs, and schools. The number of clients per week ranged from one to more than five. The vast majority of participants reported that their clients receive services covered by Medicaid.
Many focus group participants who are paid caregivers started as unpaid family caregivers. Several participants described being drawn to caregiving jobs for their paid employment because they had first experienced taking care of family members (including young children or siblings as well as relatives with disabilities) and/or had seen relatives who worked in paid caregiving jobs and were able to “make a difference” in their clients’ lives. A male direct care worker in Texas observed, “[y]ou have to have a service-oriented, nurturing, caring spirit and be genuinely interested in helping out [the] person. . . that you’re assisting.” A frequently cited attribute for success on the job was “patience.” Others underscored the importance of “social skills,” both in terms of establishing rapport and “creati[ing] a bond with [your] client” and in communicating with family members.
“I love being able to help people. . . So I think just seeing the positive effects of what I’m doing, even it’s something small, how big of a difference it makes for somebody. I love that. It’s such a good thing for me.” – 24-year-old female paid caregiver in Pennsylvania
“[S]ome of these patients, they value your company. Like they’re lonely so that’s what gives me the most gratification. . .” – 34-year-old female paid caregiver in New York
Nearly all participants in the unpaid caregiver group were women and described themselves as the primary caregiver for someone receiving Medicaid, typically a family member. This group was about evenly divided between people who identified as white or Black. They care for seniors with physical disabilities and/or dementia, and nonelderly people with autism, serious mental illness, and physical disabilities. Some had paid employment, either full or part-time, in addition to their caregiving responsibilities. They describe Medicaid as helpful in covering doctor visits, prescriptions, medical tests, supplies, transportation, and home health aide services. Transportation to medical appointments and daily supplies such as gloves, wipes, and adult diapers were cited as items that participants would find expensive to cover out-of-pocket without Medicaid. A couple of participants noted that Medicaid home health aide services allowed them to do paid work as well.
Participants in the unpaid family caregiver group experienced a variety of circumstances that led to them assuming their caregiving roles. Some were parents of a child born with I/DD and had been caregiving since their child’s birth and into adulthood. A woman in Florida described the sudden onset of her adult daughter’s caregiving needs: her daughter had been living on her own and working when she began experiencing symptoms that led to discovery of a brain tumor. She now lives with her mother and requires constant care. Several participants who are caring for aging parents observed that they expected to be caregiving eventually but had not anticipated their parents to need care as soon as they did. Most participants in the unpaid caregiver were not formally trained as caregivers and reported varied experiences with accessing the information and resources they needed to support them in their caregiving roles. Some had one-time training when they began caregiving, while others had no training. Participants generally agreed that information was not easy to find and required time and persistence to pursue. Several cited their family member’s doctor as the most helpful source of information about available resources.
“I just feel like there’s not anyone out there that, you know, helps us and guides us in the right direction for what we need or what we want.” – 56-year-old female unpaid caregiver in Ohio
“I was able to learn a lot just by talking to someone at the Senior Resource Center, which has helped tremendously.” – 60-year-old female unpaid caregiver in Minnesota
Box 1: National Characteristics of Paid and Unpaid Caregivers
National data show that the paid long-term care workforce is disproportionately low-wage, female, and Black. Aides and personal care workers are much more likely to be low-wage earners, compared to other types of long-term care workers, such as health care providers and social and behavioral health workers. Across care settings, 70% of aides and personal care workers earn less than $30,000 (the 40th percentile of overall long-term care worker earnings). Aides and personal care workers also are more likely to live in poverty than other types of long-term care workers (15% versus 6%). Just under 60% of home health workers and 62% of aides and personal care workers are employed full-time. The vast majority (88%) of aides and personal care workers are female, and nearly half are Black or Hispanic (32% and 16%, respectively). Another analysis shows that, while most (60%) health care workers with direct patient contact working in long-term care settings have private health insurance, 21% have Medicaid or other public coverage, and 14% are uninsured.2
The majority of unpaid family caregivers are white and female. A 2020 AARP survey found that over 20 percent of Americans (about 53 million people) had cared for a relative or friend in the past year, up from about 43.5 million people in 2015. Six in 10 family caregivers are white (61%), 17% percent are Hispanic, 14% are Black, 5% are Asian/Pacific Islander, and 3% identify another race/ethnicity including multiracial. Just over 60 percent of family caregivers are female, and over half are age 50 or older. Over half are caring for a parent, and the average duration of caregiving is 4.5 years. One in 5 family caregivers reports high financial strain as a result of caregiving, and 45% have experienced at least one negative financial impact due to caregiving, such as taking on more debt. Just over 60 percent of family caregivers have paid employment, with most of this group reporting that caregiving has impacted their work.
The pandemic has affected both paid and unpaid caregivers. A 2020 survey found that over half of DSPs reported that their work life was “worse or much worse” since the pandemic. Another 2020 survey found that unpaid family caregivers scored significantly worse on well-being measures (such as anxiety and depression) compared to non-caregivers. Family caregivers also were more likely to report increased worries about food and financial security since the pandemic began, compared to non-caregivers. Additionally, family caregivers reported that the pandemic made it more difficult to perform caregiving.
What are the physical and mental demands of caregiving?
Participants in the paid direct care worker groups described daily caregiving work involving a variety of physical demands. Typical tasks include helping clients with eating, bathing, and toileting; preparing meals, doing laundry and other household chores; and managing medications. They described the physical demands of their jobs, including lifting and transferring patients in and out of bed and wheelchairs. Other common job characteristics included long hours and unpredictable schedules.
“The physicals demands. . . include the transporting of the. . . patients. . . who were bedridden [to the bathroom]… we didn’t have the bed lift to really lift them up, we would have to do it ourselves and. . . it would be a lot.” – 21-year-old male paid caregiver in New York
“The most strenuous job was when [client] would have her behavior, she would lay down on the ground and she was 250 pounds and just lay there.” – 51-year-old female paid caregiver in Florida
Participants in the paid direct care worker groups also described their jobs’ mental demands, which intensified during the pandemic. Several said that they “love” their work but also acknowledged that everyone is not well suited for the demands of caregiving jobs. They described the demands of caring for clients with challenging behaviors. They cited increased stress especially in the pandemic’s early days. Participants described the uncertainty of working during the pandemic and fear of infecting their clients or bringing the virus home to infect their families.
“It’s hard to get a break, and eventually you just kind of get worn out over the course of the day.” – 78-year-old male paid caregiver in California
“Mentally, you just feel like. . . you can never just sit down and. . . regroup. . . You always feel like there’s something to do, especially with COVID adding more things onto your daily schedule. . . it’s very hectic.” – 21-year-old male paid caregiver in New York
“When the pandemic hit everything shut down…[Clients] could not understand why, and you had to sit there and try to explain to them…they would get frustrated at me, curse me, and spit at me.” – 51-year-old female paid caregiver in Florida
“I would say that my anxiety is honestly probably an all-time high…How do you social distance as a home health care aide?…It makes life challenging, it makes, you know my job challenging, riding the subway is a challenge. There were a lot of times where I was not taking mass transit and that was an additional cost to me.” – 42-year-old male paid caregiver in New York
Similarly, participants in the unpaid caregiver group recounted a range of daily caregiving duties with a variety of physical demands. They assist with preparing meals, bathing, dressing, running errands, laundry, managing medication, and monitoring to ensure safety and prevent falls. Nearly all participants live with the person for whom they care. Many noted that they “don’t really get breaks” from their caregiving duties. Participants described relying on other family members to fill in when they needed someone to cover their caregiving responsibilities, rather than formal respite care.
Participants in the unpaid family caregiver group also explained the mental demands associated with caregiving, which they often described as “overwhelming.” They described the all-encompassing nature of their caregiving role, which existed prior to the pandemic. Participants described caregiving during the pandemic as “scary,” “extremely busy,” “very stressful,” and “a nightmare.” Several had experienced COVID-19 infections themselves or in their households. A 60 year old woman in Minnesota lost her stepmother to COVID-19, which led to her having to assume caregiving responsibilities for her father.
“It’s always a challenge. It is tiring emotionally, physically.” – 51-year-old male unpaid caregiver in California
“I just find it very stressful, very challenging sometimes. . .to find a moment for ourselves because it can be so overwhelming.” – 42-year-old female unpaid caregiver in Illinois
“I never thought I’d feel this tired.” – 44-year-old female unpaid caregiver in Illinois
“I would say it’s been kind of a nightmare for us. My son is autistic…he has some tumors on his brain and he gets very violent and so through the whole pandemic, he was not able to do all of the things that he used to… it was very hard for him to be stuck in the house and not get to go places.” – 56-year-old female unpaid caregiver in Ohio
How are caregivers affected by workforce shortages?
Several participants in the paid direct care worker groups described regularly experiencing uncertainty about whether they would be able to leave work at the end of their shift due to staffing shortages and shifts not being filled if a worker called out. These issues existed prior to the COVID-19 pandemic. A few participants mentioned the toll that working overnight shifts took on their schedules, especially when balancing another job and/or school. Some participants had regular weekly hours, while others said that their schedules changed from week to week, and they did not know their schedule for the upcoming week until a couple of days before the week started.
“It’s mostly common that we have a shortage of staff in most states…I definitely agree like I would start a certain time and wouldn’t know if I [would] leave… Having a shortage doesn’t help either, so if your relief doesn’t come and there is a shortage, you’re just working.” – 21-year-old male paid caregiver in New York
“Some Tuesday mornings when I think I’m going home at six, the owner would call and say, two of them had to go to the doctor, so I would never come home until Wednesday night.” – 51-year-old female paid caregiver in Florida
On the other hand, participants who provide self-directed services said that they and their clients enjoyed the flexibility to decide how to allocate their allotted hours during the week. Self-direction is a service delivery model that typically allows beneficiaries to select and dismiss their direct care workers, determine worker schedules, set worker payment rates, and/or allocate their service budgets.
“I can be with [my client] for 30 hours a week. We can divide that up any way we want to… how it fits our schedules best. . . it’s very flexible.” – 60-year-old male paid caregiver in Texas
The COVID-19 pandemic created additional scheduling challenges and intensified pre-existing staffing shortages for paid direct care workers. Participants agreed that COVID-19 led some of their colleagues to leave their caregiving jobs for fear of getting sick themselves or bringing the disease home to a family member and observed that staffing shortages intensified during the pandemic. Those working in group homes found that they had to increase staffing during the day when outside day programs shut down due to stay-at-home orders, and clients were suddenly at home during the day. Participants also underscored that “social distancing is impossible” when helping clients with personal care needs.
“You never knew who was going to call out. So you always stayed prepared. You always had an extra overnight bag ready just in case.” – 51-year-old female paid caregiver in Florida
“A lot of the [day] programs were closed. So instead of us having an eight-hour break where [group home residents] went to program, now we had to fill the first shift…Not only in the home that I supervise, there was other homes where there was call offs, so I found myself going to assist other people.” – 42-year-old female paid caregiver in Missouri
Unpaid caregivers also were affected by the pandemic’s disruption of in-home and day program services on which some unpaid caregivers relied so that they could work outside the home. A 56 year old woman in Ohio had to leave her paid employment to care for her adult son with autism after the pandemic began and his day program closed. A 42 year old woman in Florida said that her adult daughter’s home health aide stopped coming during the early days of the pandemic, but services later resumed. A couple of participants noted that they no longer had the same home health aide coming consistently since the pandemic, which created additional disruption and required additional time to orient new aides. Others described discontinuing in-home services during the pandemic due to fear of infection.
“I had to quit working, because he was no longer in school anymore… we were transitioning into the adult program, and then could only go back one day, and then it shut down… I wasn’t able to go back to work.” – 56-year-old female unpaid caregiver in Ohio
It is unclear how vaccination mandates might contribute to workforce shortages, as participants in the paid direct care worker groups were divided about whether to receive the COVID-19 vaccine. While the majority of those weighing in on this issue were vaccinated, a vocal minority were unvaccinated. Among the unvaccinated, some expressed hesitation, while at least one said that their opposition was strong enough to lead them to leave their job if faced with an employer mandate. A number of participants described contracting COVID-19 themselves or working where there were outbreaks among staff or clients, but these experiences did not necessarily mean that they wanted to be vaccinated. A female paid caregiver in California had just learned that her employer was adopting a vaccine mandate and was preparing to leave her job rather than comply. A female paid caregiver in Maryland who had had COVID-19 said that she did not want to be vaccinated due to “anxiety” and seeing family members who were vaccinated experiencing breakthrough infections. A female paid caregiver in Missouri said that she did not want the COVID-19 vaccine after becoming ill when she received a flu vaccine. Participants noted that clients increasingly were requesting workers who are vaccinated to fill open shifts. Unlike the division among participants in the paid caregiver groups, those in the unpaid family caregiver group generally were supportive of vaccination.
“I don’t know if I was going to be having a job next month because they wanted everybody to be, all their workers to be vaccinated.” – 41-year-old female paid caregiver in California
“I’m not getting vaccinated. . . I just don’t trust it.” – 45-year-old female paid caregiver in Maryland
“I am not vaccinated. But I’ve noticed that when they do call me to offer shifts, sometimes the agency may say this particular consumer will prefer someone who has been vaccinated. So, you know, the consumer does have the right to specify it. For my own personal reasons, I’m just a little hesitant right now.” – 24-year-old female paid caregiver in Pennsylvania
Participants in the paid direct care worker groups who were vaccinated cited the benefits they saw for themselves as well as their clients. A male paid caregiver in Texas who has diabetes reported getting vaccinated as soon as he was eligible, while a female paid caregiver in New Jersey said that she felt comfortable getting the vaccine after doing her own research and preferred that route to getting vaccinated through her employer. One paid caregiver in Texas working with immune compromised children was frustrated that some families were not getting vaccines despite additional risks to their children
“I got the vaccination because my job required it, but I was going to get it anyway as soon as I was in line. I was in line as a senior. But I got it earlier because I was in line first as a caregiver.” – 66-year-old female paid caregiver in Pennsylvania
“I got [the COVID-19 vaccine] at the nearby hospital… I did it on my own terms because I don’t want to put my own family at risk, especially my grandmother, and my other clients… [Clients] feel more comfortable with someone that’s vaccinated in their home.” – 22-year-old female paid caregiver in New Jersey
“I’m diabetic so when I got the chance to get vaccinated at the beginning of this year, I didn’t doubt it.” – 54-year-old male paid caregiver in Texas
How do caregivers feel about their wages, overall finances, and opportunities for advancement?
Perhaps not surprisingly, participants in the paid direct care worker groups universally agreed that their wages were low and did not reflect the demands of their jobs. They described their financial situation as “getting by” and “living paycheck to paycheck.” Those who live in a household with two wage earners universally noted that their spouse was the “primary breadwinner” and observed that their earnings alone were not enough to support a family. Some noted that they had been able to earn additional money by picking up extra hours during the pandemic when colleagues called out, though they also noted the additional stress of working more long shifts. On the other hand, one woman described the financial challenges her family faced during the pandemic when her husband was out of work and their income was limited to her caregiving wages. Full-time employees generally reported access to employer-sponsored health insurance, and some employers offered retirement savings plans. Some but not all had paid vacation days, and most did not have paid sick leave.
Participants in the paid direct care worker groups generally did not receive raises and expressed the desire to have good job performance recognized with wage increases. Those who had asked for raises generally reported that their employers said that this was not feasible due to low Medicaid reimbursement rates. A 24 year old female paid caregiver in Pennsylvania who had been working at her employer for four years said that small hourly increases were available based on an annual evaluation: “based on your performance, they’ll give you like maybe an extra 30 cents an hour, an extra 20 cents.” She reported that her employer had been in business for 17 years, and during that time the starting hourly rate had increased only from $9 to $10.
“You’re not going to get rich, you know, and it’s not about that, it’s more of. . . I know that I’m going to be helping people at the end of the day. . .” – 41-year-old female paid caregiver in California
“We’re over worked and underpaid. And it’s not really an easy job. . . This job is not for the weak. You have to love what you do.” – 51-year-old female paid caregiver in Florida
“[O]bviously we need money. . . to support ourselves, that’s how we get by, we pay bills, we eat. . . put food on the table and put clothes on our back. But you [have] got to do this. . . because you love to do it, and that’s the only way that you’ll be able to get through those 12, 24 hour shifts sometimes.” – 21-year-old male paid caregiver in New York
“[T]o grow a family, yes, it is necessary to have two incomes, because as a home health [aide]. . . even though. . . we live here in Texas, it’s not very expensive, [but] it’s not enough to raise a family.” – 54-year-old male paid caregiver in Texas
Participants in the paid direct care worker groups are interested in opportunities for training that lead to wage increases and the ability to advance in their careers. Some participants said that their employers offered online or in-person training on topics such as safe lifting practices, allergy management, and tracheotomy and gastrointestinal tube care and that they were paid for their training time. However, these trainings did not appear to be tied to wage increases or career advancement, and most participants did not feel that their jobs offered a career ladder to higher wages based on increased skills or job responsibilities.
“With my company there is no real career advancement… there is no training program to move you into let’s say a managerial role… [I]t’s not like. . . somebody ever sits me down for my annual review and says. . . okay, where do you see yourself in two or three years. . . I’ve never had a conversation like that. . . I don’t think those conversations are typical.” – 42-year-old male paid caregiver in New York
Some participants in the unpaid caregiver group have paid employment in addition to their caregiving, while others said that their caregiving demands made it impossible for them to work. Those that are working often described their outside jobs (often from home) as a break from caregiving, though they also noted difficulty in balancing their paid employment with their caregiving responsibilities. A 42 year old woman in Florida who cares for her adult daughter noted that she lost a job due to her inability to focus, which led to mistakes, because she was preoccupied with her daughter’s needs. Others agreed with her description of “always being in caretaker mode.” She has now found another job but noted that she is unable to go to work or take her younger daughter to school if the home health aide for her adult daughter does not show up on time. A 44-year-old woman in Illinois who cares for her adult brother with serious mental illness and a brain tumor said that her caregiving responsibilities only allowed her to work part-time.
“I had another job, but I was let go because I couldn’t focus. I was making so many mistakes… [T]his job I have now is working from home, but that makes it ten times harder for me to focus because [my daughter is] right in the next room.” – 42-year-old female unpaid caregiver in Florida.
What is Congress considering to support caregivers and what do caregivers want policy makers to understand?
The Congressional debate about the overall budget reconciliation package and the amount of new federal funding for Medicaid HCBS is continuing. President Biden proposed $400 billion in new federal funds for Medicaid HCBS, while the current House bill includes $190 billion. Box 2 describes key provisions of the new funding as they relate to paid and unpaid caregivers.
Box 2: Key Provisions in the Current House Bill Related to Caregivers
Most of the new Medicaid HCBS funds in the House budget reconciliation bill are dedicated to a new “HCBS Improvement Program,” which would provide states with a permanent seven percentage point increase in federal Medicaid matching funds for HCBS. To qualify for the enhanced funds, states would have to engage in certain activities to expand Medicaid HCBS and strengthen the direct care workforce.
A number of the activities tied to the proposed enhanced federal HCBS funds focus specifically on paid and unpaid caregivers. For example, states would have to provide supports to family caregivers, such as respite care, caregiver assessments, peer supports, or paid family caregiving. States also would have to update, and increase as appropriate, HCBS payment rates to support the recruitment and retention of direct care workers, and review these rates every three years. Payment rate increases would have to be at least proportionately passed through to direct care workers. States would have to update qualification standards and develop training opportunities for HCBS providers and provide resources for family caregivers. States also would have to monitor and report on factors such as direct care worker wages, benefits, turnover, and vacancy rates.
Under the new program, states also could receive an increase in the federal matching rate for administrative costs, from 50% to 80%, through September 2031, for activities such as modifying provider rate setting processes, adopting or improving training programs for direct care workers and family caregivers, and adopting or enhancing registries to connect HCBS enrollees and direct care workers. Additionally, states could receive another two percentage point increase in federal Medicaid HCBS matching funds for two years if states adopt certain activities to support self-direction. These activities include developing a worker registry to help enrollees find workers; recruiting and training independent providers; supporting enrollees who self-direct services by processing worker timesheets and payments; and supporting family caregivers as paid providers.
Participants in the paid direct care worker groups cited improving wages as the top issue for policymakers to address. There was a general feeling of being “overworked and underpaid,” which existed prior to the pandemic. Participants emphasized the importance of any reimbursement rate increases being passed through to direct care worker wages. Participants also supported increased training, especially if tied to career advancement and higher wages, and access to the equipment and supplies they need to perform their jobs safely.
“I think [higher wages] would attract more people to the job. . . having more money. . . within your pocket would allow more people. . . to be able to sustain themselves and not be discouraged from. . . not being paid enough” – 21-year-old male paid caregiver in New York
“if [policymakers] do give an increase to whatever the reimbursement rate to the agencies is, maybe they could specify something in their contract just to say, you know, caregivers should be making at least this amount.” – 24-year-old female paid caregiver in Pennsylvania
Participants in the unpaid caregiver group asked for recognition of the value of the services that they provide for their family members. They all said that they wanted to keep their family members at home and were willing to provide the caregiving necessary to avoid having them institutionalized. At the same time, they did not think that people who have not had the experience of family caregiving fully understand the challenges it presents. One suggested providing tax credits to family caregivers to recognize that in-home care is less expensive than nursing home care. Other suggestions included additional opportunities for community integration and a centralized website with current information about caregiver supports. They also emphasized that policies should be flexible enough to recognize that each person has unique needs to be met and administrative burdens to access services should be minimized.
“Nobody knows how much you’re sacrificing for yourself to take care of somebody else… I would never want to put my parents or my son in a nursing home… And I just think that a lot of people just don’t understand what it is that we go through.” – 56-year-old female unpaid caregiver in Ohio
“There’s people in different degrees of caregiving, lower-level, higher levels, and so those need to be taken into consideration. Those that really have severely disabled [family members], whether it’s emotionally or physically, they need to have the support…it’s a 24/7-hour job. They need to be supported through whatever means necessary.” – 51-year-old male unpaid caregiver in California
“Keeping somebody out of a nursing home really reduces the cost; I’d like them to recognize that us as caregivers are really saving tons of money, we’re providing good quality service, keeping our loved ones with us.” – 60-year-old female unpaid caregiver in Minnesota
Looking Ahead
The COVID-19 pandemic has intensified long-standing issues related to the unmet need for HCBS, such as growth in the aging population and direct care workforce shortages. Many states used Medicaid emergency authorities to support HCBS providers during the pandemic by increasing reimbursement rates and/or offering retainer payments. CMS guidance encourages states to identify any temporary policy changes adopted under emergency authorities that increased access to HCBS and to consider making those changes permanent. However, states’ ability to do so could be limited by budgetary constraints. While the American Rescue Plan Act provides a temporary increase in federal matching funds for Medicaid HCBS, the expiration of this increase after one year could limit states’ ability to adopt longer-term HCBS program expansions.
Congressional debate about the overall budget reconciliation package and the amount of new federal funding for Medicaid HCBS is continuing. President Biden proposed $400 billion in new federal funds for Medicaid HCBS, while the current House bill includes $190 billion.
The major HCBS program in the bill would increase federal matching funds, without a time-limit, for state spending on Medicaid HCBS. To qualify for the new funds, states would have to take certain actions, a number of which are relevant to addressing issues raised by caregivers in our focus groups. For example, states would have to review, and update as necessary, HCBS provider reimbursement rates every three years, and any rate increases would have to be passed through to direct care workers. These actions could help to address issues with low wages cited by focus group participants. To receive the new funds, states also would have to develop training opportunities for paid HCBS providers as well as for unpaid family caregivers, which could help to address needs in these areas expressed by focus group participants. Another set of activities under the new program centers on states providing supports to family caregivers, such as respite care, caregiver assessments, peer supports, or payment as providers. Participants in the unpaid caregiver group cited these areas as gaps in which additional resources and supports are needed. How much the reconciliation package does to address the concerns raised by caregivers will depend in large part on the level of funding committed. There is pressure to reduce the overall price tag in the package, and planned HCBS expansions could be reduced further as they compete with other priorities.
Participants in the paid direct care worker groups live in Alabama, California, Florida, Illinois, Missouri, New Jersey, New York, Pennsylvania, South Carolina, Texas, and Washington. Participants in the unpaid family caregiver group live in California, Florida, Illinois, Minnesota, New York, Ohio, and Oregon. ↩︎
With millions of U.S. school children returning to in-person learning for the 2021-2022 school year, schools are grappling with how best to keep students, and the larger school community, safe as the COVID-19 pandemic continues and most elementary students are still not eligible for vaccination. While school policy is primarily made at the state and local levels, the Centers for Disease Control and Prevention (CDC) has issued guidance recommending a layered approach for COVID-19 prevention and mitigation in K-12 schools that promotes, among other things, vaccination as the best way to prevent severe illness, hospitalization and death, universal masking for students, teachers, staff, and visitors to schools, and regular screening testing of students and staff, particularly those who are unvaccinated, so that measures can be taken to prevent further transmission.
To better understand the extent to which states have adopted policies consistent with CDC guidance, we examined state policies for all 50 states and DC focused on COVID-19 prevention strategies in K-12 public schools for the 2021-2022 school year. We looked at policies in the following areas: vaccine mandates for school employees and students; mask requirements; and requirements for COVID-19 screening testing of students and staff. We also sought to identify where states left such decisions up to local school districts. We used data from the National Center for Education Statistics on projected public school enrollment in 2021 to obtain the number of elementary and secondary public school students by state.
As of October 5, 2021, we find that most states have left COVID-19 prevention decisions up to local school districts, and in some cases, have prohibited local districts from implementing them. As a result, there is wide variation in the use of such strategies across the country and within states, including by school district or even by individual schools. In addition, large shares of K-12 public school students live in states that do not mandate COVID-19 prevention strategies in schools, though, in many cases allow local districts to implement such measures and do provide funding and other assistance. Specific findings in each area are as follows:
COVID-19 Vaccine Mandates: Most states (40) do not require school employees to get vaccinated. Of the 11 that do, they are primarily in the Northeast and West. Overall, seven in ten (70%) K-12 public school students live in states without such requirements while the remainder (30%) are in the 11 states that have vaccine requirements.So far, California is the only state to mandate that all eligible students be vaccinated, though that requirement is not scheduled to take effect until July 1, 2022 for students in grades 7-12. The mandate for younger children will take effect six months following full FDA approval of the vaccine for the age group. This is likely to be an area that will change, as all states mandate vaccines for school children in many instances including for measles, mumps, and rubella (MMR), diphtheria, tetanus, and pertussis (DTaP/Tdap), and chickenpox.
Mask Requirements: Currently, 18 states require masks in school—11 states have broader statewide face mask requirements that also apply to schools, while mask mandates in 7 of these states are specific to schools (and certain other settings). Twenty-five states do not have a statewide requirement for masks in schools but allow for local school districts to institute such requirements. An additional 8 states prohibit schools from requiring masks, though these bans are being challenged in court in nearly all of the states.States in the Northeast are most likely to require masks, and none prohibit them, while states in the Midwest are the least likely to require them. Two thirds of states that prohibit masks are in the South. The majority of K-12 public school students either live in states that do not require masks (43%) or prohibit such requirements (25%). About one-third (32%) live in states that do require them (although because of decisions by local school districts in many states to require masks, a larger share of students attend schools that require them). None of the 8 states that prohibit masks have vaccine mandates in schools.
COVID-19 Screening Testing: Almost all states (45) have left COVID-19 testing decisions up to local school districts. Both DC and New York are exceptions, with each requiring screening for all schools. DC conducts opt-out surveillance testing of a random sample of at least 10% of asymptomatic students each week, while New York requires weekly testing of all teachers and staff, with an opt out for those who are fully vaccinated. Four states require testing in certain situations: Nevada requires students who are not fully vaccinated to be regularly tested if they travel to other schools for athletic events; Michigan requires all unvaccinated individuals ages 13-19 participating in school and non-school sponsored sports to be tested weekly; Utah has a Test to Stay policy to support in-person education that requires testing of all students during COVID-19 outbreaks; and Washington requires student athletes who are not fully vaccinated but involved in high-contact sports to be regularly tested.Several states, including Maine and Massachusetts, have established voluntary pooled testing programs in which local districts can participate, and other states are using federal COVID-19 funding to support schools that would like to implement COVID-19 testing programs.
>
Implications
States have staked out different approaches to mandating COVID-19 prevention measures in K-12 public schools, although most have left decisions up to local school districts, where most school policies are made, or even to individual schools. While some states have adopted CDC-recommended COVID-19 strategies, most are not requiring schools to implement proven and effective COVID-19 interventions that can help to keep children and school communities safe. As a result, there is wide variation in the use of such strategies across the country and within states, including by school district or even individual schools. In addition, large shares of K-12 public school students live in states that do not mandate such strategies, including 70% of students who live in states that do not require school staff to get vaccinated and more than two-thirds who live in states that either do not require masks or prohibit them. Most states also leave decisions regarding the use of regular COVID-19 testing, a proven public health intervention to identify those who might be infectious and reduce onward transmission, up to local districts or individual schools, although in several cases, states make resources available to support them including in instituting school-wide, regular screening programs.
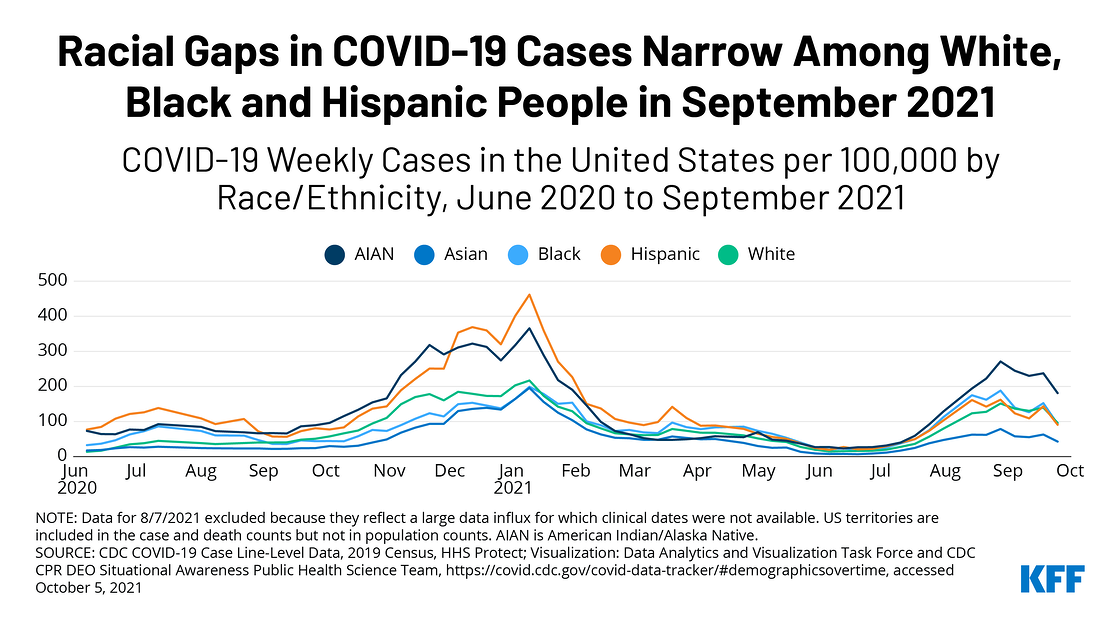
As the COVID-19 pandemic’s focus shifts from urban to rural areas, and more people resume public activities, a new KFF analysis of case and death data from the Centers for Disease Control and Prevention reveals narrower disparities affecting Black and Hispanic people compared to White people now than earlier in the pandemic.
The analysis examines trends in cases and deaths since early in the pandemic where race and ethnicity is known. While cumulative data show that Black, Hispanic and American Indian and Alaska Native people have been disproportional impacted overall, recent data show much closer rates of new cases and deaths among White, Black and Hispanic people. In contrast, American Indian and Alaska Native people are experiencing higher rates of new cases than other groups.
Some factors likely contributing to these shifts:
COVID-19 vaccinations have increased protections and reduced illness and death across all racial and ethnic groups. Vaccination rates among Black and Hispanic adults also are approaching parity with the rate among White adults. That’s a significant shift from earlier this year, when vaccination rates lagged among Black and Hispanic adults in part due to access barriers. The latest KFF COVID-19 Vaccine Monitor report now shows the uninsured, Republicans, rural residents and White Evangelical Christians as the least vaccinated groups.
The pandemic initially hit hardest in urban areas, which often include a racially diverse population, but is increasingly hitting more rural areas, which have higher concentrations of White and American Indian and Alaskan Native people.
Earlier in the pandemic, when most states implemented social distancing measures and limited public activities, risk of exposure and infection was highest for essential workers, who continued to work outside their home and are disproportionately people of color.
The analysis notes that while disparities have narrowed, many of the underlying structural inequities in health and health care and social and economic factors that placed people of color at increased risk early in the pandemic remain. They may remain at risk as the pandemic continues to evolve or if future health threats emerge.
As the Congressional debate over budget reconciliation legislation intensifies, stakeholders are keeping a close eye on a proposal to allow the federal government to negotiate drug prices in Medicare, which is currently prohibited under federal law. The so-called “non-interference clause” prohibits the federal government from “interfering” in negotiations between drug companies and the private plans that deliver Part D coverage, and also prohibits the government from requiring a particular formulary or price structure for drugs. The proposal under consideration amends the non-interference clause by adding an exception that would allow the government to negotiate prices with drug companies for a relatively small number of high-cost drugs, with an excise tax levied on drug companies that do not agree to participate in the negotiation process or comply with the negotiated price. This proposal would yield savings upwards of $450 billion, based on an earlier estimate from the Congressional Budget Office.
The pharmaceutical industry’s latest ad campaign claims that drug price negotiation would “restrict access to medicines in Medicare” by removing “a provision that protects access to medicines” and that patients “would be stuck with whatever medicines the government says you can have.” Another drug industry ad says that allowing the government to negotiate drug prices means “politicians…[will] decide which medicines you can and can’t get.”
This is not accurate. In fact, the proposed drug price negotiation program does not authorize the federal government to decide which medications people on Medicare can and cannot get and does not establish or require a particular prescription drug formulary. Insurers that offer Medicare prescription drug plans would continue to make decisions about which drugs to cover, or not, subject to protections provided under current law and regulations. The legislation under consideration leaves in place the non-interference clause and its specific restrictions with the exception of the proposed drug price negotiation program. Under this program, the negotiation process would not apply to most prescription drugs, instead focusing on a relatively small number with the highest spending and lacking generic or biosimilar competitors.
While there is nothing in the proposed legislation that would allow the federal government to dictate which drugs Medicare beneficiaries can access, it is possible that downward pressure on prices from negotiation could lead drug companies to bring fewer drugs to market. The Congressional Budget Office has estimated that reductions in future profits of 15% to 25% for high revenue drugs, which CBO expects would be similar to the effect of the current drug price negotiation proposal, would lead to 2 fewer drugs in the first decade (a reduction of 0.5%), 23 fewer drugs over the next decade (a reduction of 5%), and 34 fewer drugs in the third decade (a reduction of 8%). But the effect of lower prices on the number and type of new drugs that do and don’t come to market in the future is impossible to know with certainty. CBO does not forecast whether the drugs that don’t come to market would be innovative lifesaving treatments or “me too” drugs that offer little value in terms of improved health. CBO also notes that lower prices could potentially improve affordability and access to drugs for patients, leading to improved health.
Allowing the federal government to negotiate drug prices, which is supported by a large majority of the public, would lower cost sharing and premiums for Medicare beneficiaries and produce significant savings for the federal government that could be used to cover the costs of other spending priorities, such as adding new Medicare dental, hearing, and vison benefits, filling the Medicaid “coverage gap”, and making permanent subsidy enhancements for people in Marketplace plans. With much at stake in the outcome of the debate over this proposal, it’s no surprise that the rhetoric is getting heated. But while the pharmaceutical industry may want to frame the debate over drug price negotiation by focusing on the federal government limiting access to medications, this framing doesn’t accurately reflect what’s in the current legislative proposal. There are trade-offs involved in the proposal to negotiate drug prices, but that is not one of them.
Since the rollout of the COVID-19 vaccines began, one issue that has been of focus is racial equity in COVID-19 vaccination rates. Ensuring equity in COVID-19 vaccinations is important given that COVID-19 has disproportionately affected people of color and may widen underlying disparities in health. Data are key for identifying disparities in COVID-19 vaccination rates and directing resources and efforts to address them. However, there are gaps in the federally reported COVID-19 vaccination data by race/ethnicity from the Centers for Disease Control and Prevention (CDC). To help fill these gaps in federal data, KFF and others have conducted ongoing analysis of state-reported vaccination data by race and ethnicity and regular COVID-19 Vaccine Monitor surveys with adults. These data have provided further insight into COVID-19 vaccination patterns by race/ethnicity, but also are subject to limitations. This brief provides an overview of these data sources, discusses their limitations, and explains why their findings may vary.
Vaccination Rates Across Data Sources
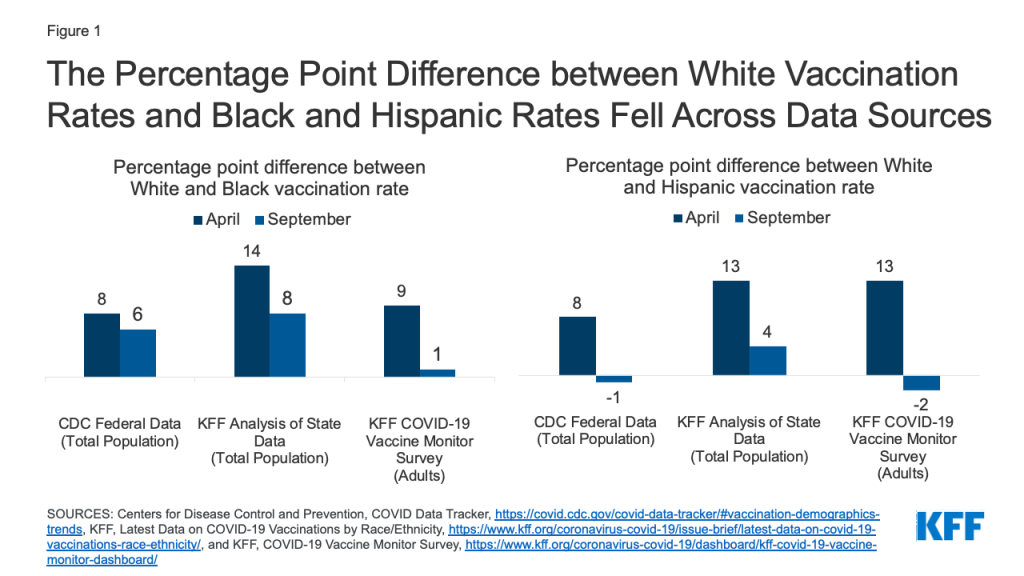
The federal and state administrative data and Vaccine Monitor surveys all show that Black and Hispanic people have been less likely to receive a COVID-19 vaccine compared to their White counterparts since the vaccination rollout began but that these disparities have narrowed over time. However, they vary in findings of the magnitude of this narrowing (Figure 1 and Table 1):
The federal data from the CDC show that between late April and late September 2021, the percentage point gap between White and Black rates for the whole population fell by 2 percentage points (from 8 to 6 percentage points) while the gap between White and Hispanic rates fell by 9 percentage points (from 8 to -1 percentage points).
The state-reported data find that the gap between White and Black rates for the total population fell by 6 percentage points over this period (from 14 to 8 percentage points), while the difference between White and Hispanic rates fell by 9 percentage points (from 13 to 4 percentage points).
Vaccine Monitor survey data show the same trend with the difference between rates for White and Black adults falling by 8 percentage points (from 9 to 1 percentage points) and the gap between White and Hispanic adults narrowing by 15 percentage points (from 13 to -2 percentage points).
Figure 1: The Percentage Point Difference between White Vaccination Rates and Black and Hispanic Rates Fell Across Data Sources
Table 1: Percent of People who Have Received at Least One COVID-19 Vaccine Dose by Race/Ethnicity
As of September 2021, the federal data from CDC show similar vaccination rates between Hispanic and White people, with lower rates persisting for Black people, and the highest rate for American Indian and Alaska Native and Asian people. Analysis of state data finds that Black and Hispanic people are less likely than White people to be vaccinated, but with a narrower gap for Hispanic people. The Vaccine Monitor survey data show that the gaps in rates for Black and Hispanic adults compared to White adults have closed, with no statistically significant differences in vaccination rates across these groups. A Pew Research Center survey conducted in August had similar findings.
This variation in findings reflects differences in what the data sources are measuring. Vaccination rates from the Vaccine Monitor surveys are based on adults, while the rates based on federal and state administrative data are for the total population (including children under 12 who are currently not eligible for vaccination). The inclusion of children in vaccination rates may lead to larger disparities due to racial differences in vaccination rates among adolescents eligible for the vaccines (ages 12-17) and because of the greater racial diversity of children relative to adults. Moreover, both the survey and administrative data are subject to different sources of measurement error, as discussed further below.
Federal COVID-19 Vaccination Data by Race/Ethnicity
The CDC reports the distribution of COVID-19 vaccinations and the percent of the total population who have received a COVID-19 vaccine by race/ethnicity at the national level. However, as of September 27, 2021, information on race/ethnicity was missing for over 40% of people who received at least one dose. Moreover, the data do not represent all states and jurisdictions, since not all states and territories are reporting demographic data on vaccine recipients to CDC. Given these data gaps, CDC indicates that the data are not generalizable to the entire population of individuals with COVID-19 vaccination. CDC does not report state-level data on COVID-19 vaccinations by race/ethnicity. Moreover, although CDC reports vaccinations by race/ethnicity and age separately, it does not publicly report data that allows for analysis of vaccinations by race/ethnicity and age. As such, the data cannot be used to examine whether there are larger racial disparities in vaccination rates among certain age groups, such as adolescents or younger adults.
State COVID-19 Vaccination Data by Race/Ethnicity
In the absence of CDC reporting state-level COVID-19 vaccination data by race/ethnicity, KFF has conducted ongoing analysis of data reported directly by states. As of September 20, 2021, 45 states, including Washington, D.C., were publicly reporting data on people who had received at least one COVID-19 vaccine by race/ethnicity and KFF was able to calculate total vaccination rates by race/ethnicity across 43 of these states. (Two states were excluded from the total due to differences in how they report their data). In general, these data are more complete than the data reported by CDC, with lower shares of vaccinations with unknown or missing race/ethnicity in most states. However, they also have gaps, limitations, and inconsistencies. As with the federal data, they do not include data from all states and jurisdictions and some states have relatively high shares of vaccinations with unknown race/ethnicity. For example, in Alabama, 37% of vaccinations had unknown race as of September 20, 2021. Further, states vary in their racial/ethnic classifications used to report the data, including how they classify people who identify as more than one race. Some state reported data does not include vaccinations administered through federal programs, including the Indian Health Service or the Long-Term Care Partnership Program.
COVID-19 Vaccine Monitor and Other Survey Data
Since December 2020, KFF has been conducting ongoing, nationally representative surveys of U.S. adults through the COVID-19 Vaccine Monitor. While these surveys have a broader purpose of measuring vaccine confidence, information needs, trusted messengers and messages, we have also used them to track the share of adults who report being vaccinated for COVID-19 over time. These surveys rely on probability-based sampling methods and researchers take extra steps to ensure the inclusion of populations that are often missed in surveys (including interviewing in English and Spanish and oversampling pre-paid cell phones that are commonly used by lower-income adults). Each survey also includes extra interviews with Black and Hispanic adults – using weighting to adjust survey respondents to match the distribution of adults in the U.S. — to be able to have greater statistical confidence when reporting on those groups (see the full methodology for more details).
Like all surveys, the Vaccine Monitor surveys are subject to a margin of sampling error around each estimate. For the September survey, the margin of sampling error was plus or minus 3 percentage points for the full sample, 4 percentage points for White adults, and plus or minus 7 percentage points for both Black and Hispanic adults. In addition, surveys may have other sources of error, including nonresponse error (certain types of people choosing not to participate in the survey or declining to answer the question about whether they have been vaccinated), measurement error (respondents not understanding the question that was asked), and social desirability bias (respondents giving answers they think the interviewer wants to hear). Despite these potential sources of error, the Vaccine Monitor surveys have tracked quite closely with CDC estimates of the share of adults overall vaccinated over time, and a recent Pew Research Center analysis of 98 different public polls conducted by 19 different polling organizations between December 2020 and June 2021 (including the Vaccine Monitor surveys) found that polling estimates of the adult vaccination rate have been within about 2.8 percentage points, on average, of the rate calculated by the CDC.
Conclusion
Data are pivotal for identifying and addressing disparities in health and health care. Over the course of the COVID-19 pandemic, gaps in data available by race/ethnicity have limited efforts to understand and address disparities. The availability and quality of data have improved over the course of the pandemic, but data gaps and limitations remain. To help fill gaps in federally reported data on COVID-19 vaccinations by race/ethnicity, KFF and others have conducted ongoing analysis of state-reported data on COVID-19 vaccinations and regular COVID-19 Vaccine Monitor surveys of adults, which have provided increased understanding of COVID-19 vaccination patterns by race/ethnicity. This, in turn, has helped to direct resources and efforts to address racial disparities in vaccination rates. While the federal, state, and survey data all show narrowing racial disparities in COVID-19 vaccination rates over time, they vary in the magnitude of this narrowing, with some surveys showing that gaps have closed, while the administrative data pointing to some remaining differences. This variation in findings reflects both differences and limitations across the datasets. Going forward, continued efforts to increase the availability of comprehensive, high-quality data will be key for identifying and addressing disparities for COVID-19 and in health and health care more broadly. Moreover, it will be important to continue to prioritize equity as vaccination efforts continue, people become eligible for booster shots, and eligibility expands to children, particularly given significant racial diversity of children.
Medicaid is a key source of coverage for low-income pregnant people in the United States, covering more than four in ten births nationally, but many people who qualify for Medicaid because they are pregnant lose that coverage 60 days postpartum, especially if they live in a state that has not expanded Medicaid. In recent years there has been a growing interest among state and federal policymakers in extending Medicaid postpartum coverage beyond the 60-day mark to help address racial disparities and improve maternal and infant health. Earlier this year, federal legislation was enacted that gives states a temporary option to extend postpartum coverage beyond 60 days, and Congress is currently considering additional legislation to require such extended coverage.
Federal law requires that all states cover pregnant individuals with incomes at least up to 138% of the federal poverty level (FPL), although many states have set higher income eligibility levels, and they must extend coverage for 60-days postpartum. Some people lose that coverage after the postpartum period because they have no eligibility pathway even though they have incomes below the federal poverty level. Following the 60-day postpartum period, in states that have adopted the Affordable Care Act (ACA)’s Medicaid expansion, individuals with incomes below 138% FPL have a continued pathway to Medicaid coverage and those with higher incomes may qualify for subsidized coverage through the ACA marketplace plans; however, individuals in non-expansion states may become uninsured because Medicaid eligibility levels for parents are much lower than for pregnant people. For example, in Alabama, which has not sought a postpartum coverage extension, the Medicaid eligibility level for parents is 18% FPL, which is approximately $4,000/year for a family of three.
The federal American Rescue Plan Act (ARPA) enacted in March 2021 gives states the option to extend postpartum coverage to pregnant individuals to a full year. The coverage option is available for five years starting on April 1, 2022 and states must provide a full scope of benefits without limitations on coverage during the extension. Prior to ARPA’s enactment, states had to seek permission from the Centers for Medicare and Medicaid Services (CMS) by applying for a Section 1115 waiver to extend the postpartum period beyond 60 days, although none of these applications were approved until April 2021. Even though the new option under ARPA will not be effective until April 2022, postpartum coverage has been continuous since the start of the coronavirus pandemic because Medicaid disenrollment has been suspended during the public health emergency.
Largely in response to the new federal option, at least 25 states have taken steps to extend Medicaid postpartum coverage. To date, most of these are expansion states, but actions in non-expansion states will ensure continued coverage following the current postpartum period. Prior to the enactment of ARPA, California and Texas had limited state-funded postpartum coverage in place and a few states had submitted waivers to CMS to extend postpartum coverage through Medicaid, although, in some cases, targeted to narrow groups, such as those with a diagnosed substance use disorder, or for less than 12 months. States often seek approval of a demonstration waiver to do something they cannot do under current law. A few states are still seeking waivers to implement prior to April 2022 or to extend postpartum coverage in ways more limited than the new ARPA option.
Recent state actions to extend postpartum coverage for 12 months include:
Thirteen states (California, Colorado, Connecticut, DC, Maine, Maryland, Minnesota, New Jersey, Ohio, South Carolina, Tennessee, Washington, and West Virginia) enacted legislation, a first step to implementing a coverage extension;
New York and North Carolina are debating proposed legislation;
Two states (Indiana and Pennsylvania) announced plans to adopt the new option using existing authority; and
Illinois received approval to extend postpartum coverage for 12 months through a waiver (waivers are pending in three states—Florida, Massachusetts, and Virginia).
Although recent federal action has prompted many states to consider extending postpartum coverage, some states still won’t have a pathway for coverage beyond the current 60-day postpartum period, and Congress is currently considering proposals to require such coverage. Uneven adoption of the ARPA option means postpartum individuals in many states remain at risk of losing Medicaid coverage just two months after giving birth. Postpartum people with household incomes below the poverty level in non-expansion states often do not have another coverage option and become uninsured when they lose Medicaid coverage. Currently, Congress is considering a provision in the Build Back Better Act that would require all states to extend Medicaid postpartum coverage from 60 days to 12 months, ensuring continuity of Medicaid coverage for postpartum individuals in all states to more broadly reduce disparities and improve maternal and infant health outcomes. However, there is a push to lower the overall amount of spending in the package, and the extension of postpartum coverage could be forced to compete against other priorities.
A new KFF analysis examines key characteristics of children with special health care needs, the affordability and adequacy of their health coverage, and the implications for such children of potential new federal Medicaid money to assist families in caring for them.
Medicaid is a significant source of coverage for medical, behavioral health, and long-term services and supports for children with special health care needs, including home and community-based services (HCBS) that they need to live at home with their families. During the pandemic, children have experienced health care disruptions, mental health challenges, and economic hardships, and these issues may have been intensified for those with special health care needs.
The American Rescue Plan Act provides a temporary increase in federal Medicaid matching funds for state spending on HCBS. As part of the budget reconciliation legislation, the House currently is considering $190 billion in additional Medicaid HCBS funding that states could use to support the HCBS provider workforce, offer new or expanded HCBS benefits, and/or serve more HCBS enrollees, though the final funding amount has not yet been set.
The analysis provides context for those ongoing policy discussions. Key findings include:
• Medicaid/CHIP covers almost half of the 13.9 million children in the U.S. with special health care needs, though the share varies by state.
• Children with special health care needs covered by both Medicaid/CHIP and private insurance have the greatest health care needs, and children who are covered only by Medicaid/CHIP are more likely to have greater health needs compared to those with private insurance only.
• While families of Medicaid/CHIP-only children with special health care needs are more likely to face financial difficulty, they find their health care more affordable than those with private insurance only. This is due to Medicaid’s cost-sharing protections.
• Even though children with special health care needs covered by Medicaid/CHIP-only have greater health care needs, they are more likely than those with private insurance alone to report that their benefits are always adequate to meet their needs.
For the full analysis, as well as other data and analyses about health care priorities in the budget reconciliation discussion on Capitol Hill, visit kff.org.