KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
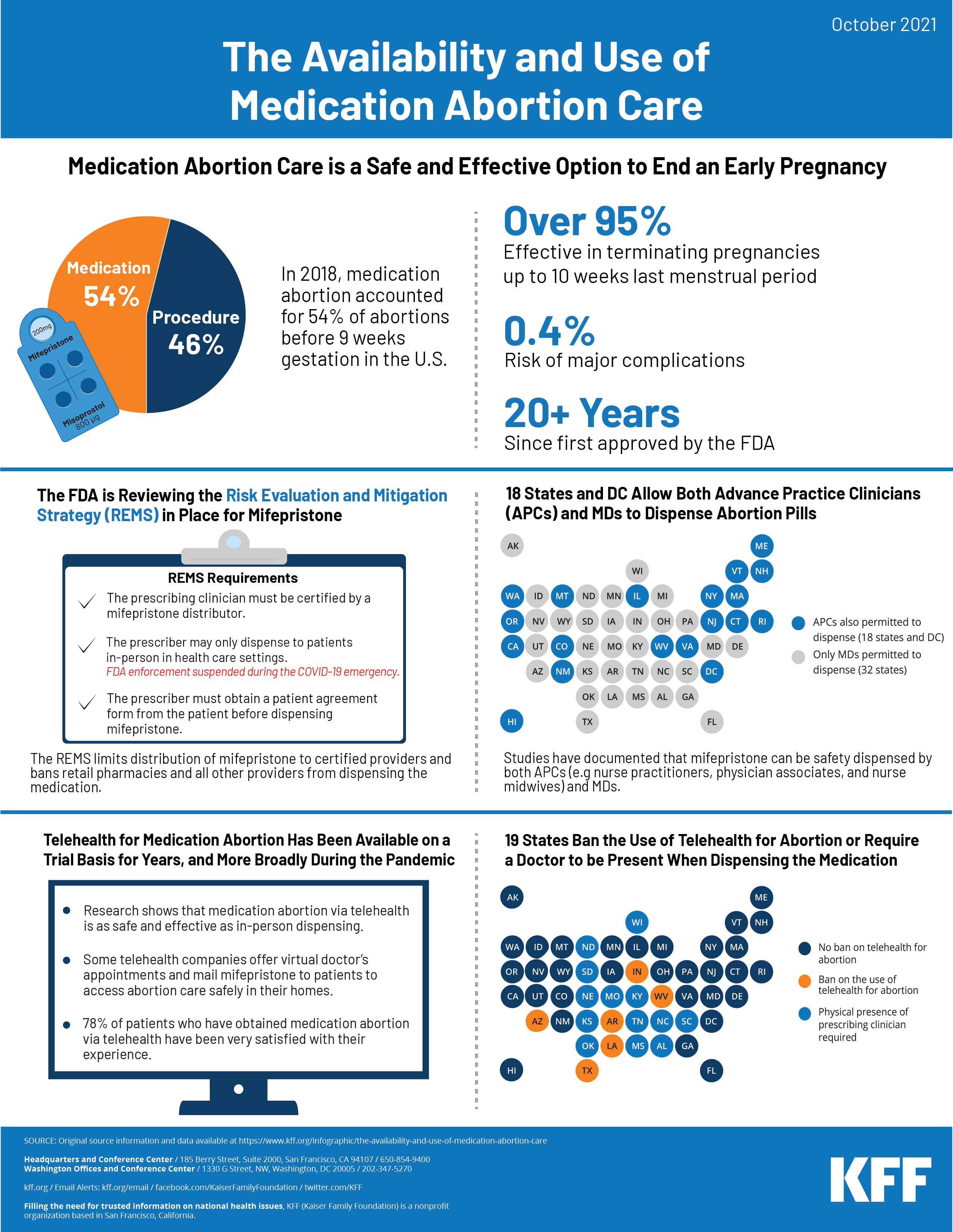
Medication abortion, also known as medical abortion or abortion with pills, is an FDA approved pregnancy termination protocol that involves taking two different drugs, mifepristone and misoprostol, for use up to the first 70 days (10 weeks) of pregnancy. Studies show that medication abortion care is safe and effective. This infographic highlights data and policies regarding the availability and effectiveness of medication abortion in the United States. Medication abortion accounts for more than half (54%) of all abortions before nine weeks gestation in the United States.
On April 12, 2021 , the FDA’s Center for Drug Evaluation and Research notified the American College of Obstetricians and Gynecologists (ACOG) that they are suspending enforcement of the Risk Evaluation and Mitigation Strategy (REMS) requirement for mifepristone that requires prescribers to dispense to patients in-person during the COVID-19 emergency. This temporarily allows providers in the 32 states and DC that do not have laws that otherwise ban this practice to dispense mifepristone using the telehealth protocol for medication abortion. The FDA has also undertaken a full review of the REMS for mifepristone and the results of that review are expected later in 2021..
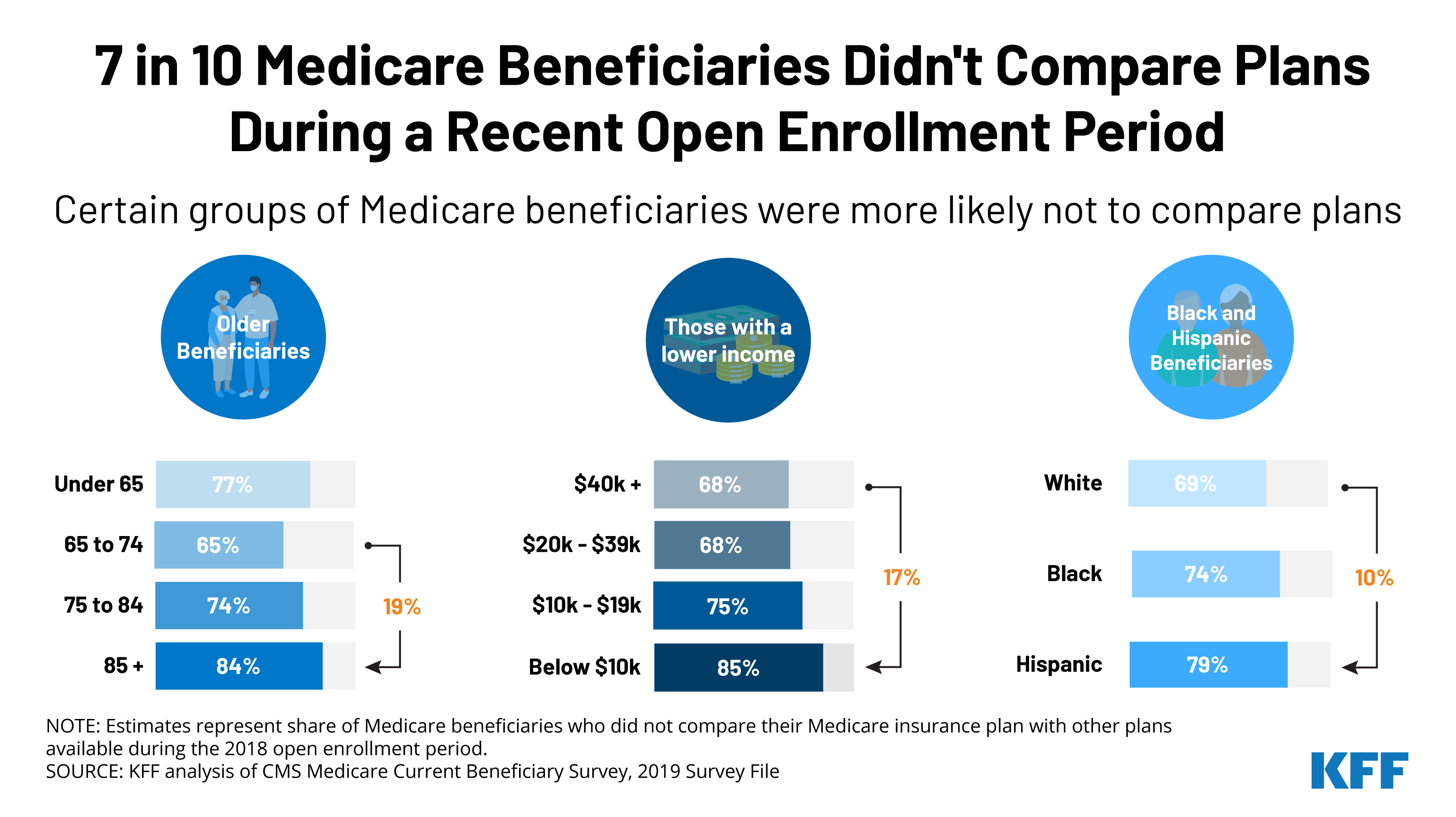
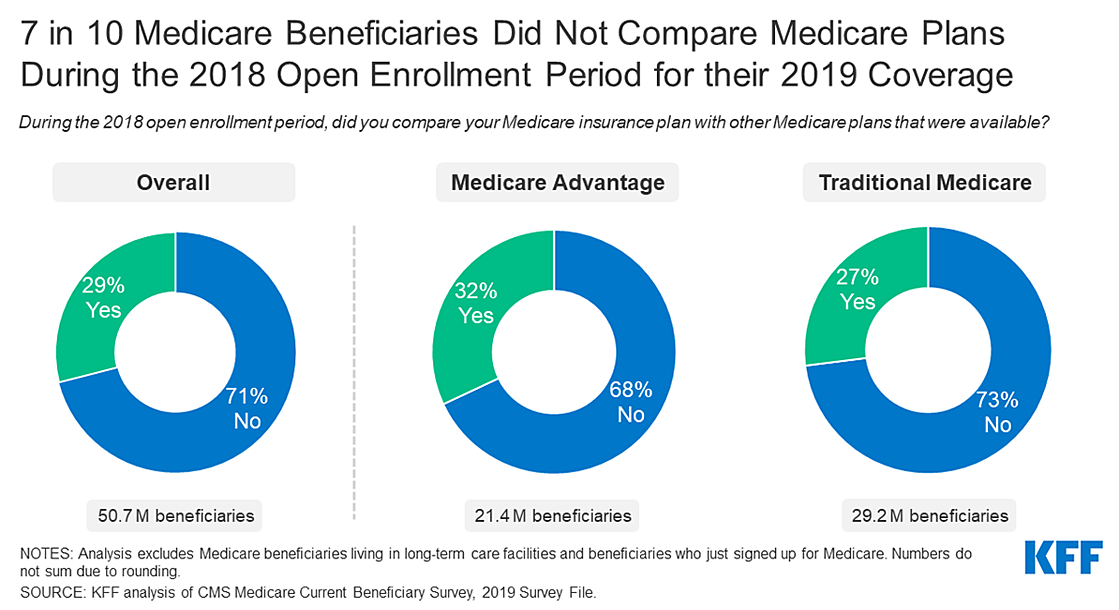
The Medicare open enrollment period is now underway, and beneficiaries are encouraged to review their coverage options to see if they can get better coverage or lower costs by switching plans. However, about 7 in 10 (71%) beneficiaries say they did not compare plans during a recent open enrollment period, and some groups were even less likely to do so.
Our recent analysis found that among beneficiaries who could be most affected by plan changes from year to year, like beneficiaries in relatively poor health, age 75 and older or under age 65 with long-term disabilities, a larger percentage reported that they did not compare plans during the 2018 open enrollment period. Additionally, a larger percentage of people on Medicare who are Black and Hispanic, with low income, with fewer years of education, or enrolled in Medicaid did not compare plans during a recent open enrollment period. While this could indicate that many enrollees are satisfied with their existing coverage, past KFF analysis has found that many Medicare beneficiaries reported that the process of choosing their Medicare plan was frustrating and difficult, and most do not switch plans.
Senate Appropriations Committee Releases FY 2022 State and Foreign Operations (SFOPs) and Labor Health and Human Services (Labor HHS) Appropriations Bills
The Senate Appropriations Committee released its FY 2022 State, Foreign Operations, and Related Programs (SFOPs) (links to bill and report) and Labor, Health and Human Services, Education, and Related Agencies (Labor HHS) (links to bill and report) appropriations bills and accompanying reports on October 18, 2021. The SFOPs bill includes funding for U.S. global health programs at the State Department and the U.S. Agency for International Development (USAID), while the Labor HHS bill includes funding for global health programs at the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health (NIH).[i] Key highlights are as follows (see table for additional detail):
State, Foreign Operations, and Related Programs (SFOPs):
Funding provided to the State Department and USAID under the SFOPs bill and through the Global Health Programs (GHP) account, which represents the bulk of global health assistance, totals $10.4 billion in the bill, $1.2 billion above the FY21 enacted level, $303 million above the President’s FY22 request, but $288 million below the FY22 House level. Funding for all global health programs at State and USAID either increased or remained flat compared to the FY21 enacted level (the largest increase is for global health security). Several program areas in the Senate bill are below House levels, including bilateral HIV/AIDS, tuberculosis, malaria, and family planning and reproductive health. Details on specific programs are as follows (unless otherwise specified, totals represent funding through the Global Health Programs account):
Funding for global health security totals $1 billion in the bill, which is $810 million (426%) above the FY21 enacted level ($190 million), $87 million (10%) above the FY22 Request ($913 million[ii]), and matches the FY22 House level.
Bilateral HIV funding through the President’s Emergency Plan for AIDS Relief (PEPFAR) is $4.7 billion in the Senate FY22 bill, matching the FY21 enacted and FY22 Request levels, but $150 million (3%) below the FY22 House bill ($4.85 billion).
The bill includes $1.56 billion as the U.S. contribution to the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund), matching the FY21 enacted, FY22 Request, and FY22 House level.
Funding for tuberculosis (TB) totals $400 million, $81 million (25%) above the FY21 enacted and FY22 Request level ($319 million), and $69 million (15%) below the FY22 House ($469 million).
Funding for malaria through the President’s Malaria Initiative (PMI) totals $800 million, $30 million (4%) above the FY21 enacted and FY22 request level ($770 million), and $20 million (2%) below the FY22 House level ($820 million).
The bill includes $941 million for maternal and child health (MCH) programs, an increase of $85.5 million (10%) above the FY21 enacted level ($855.5 million), $61.5 million (7%) above the FY22 Request ($879.5 million), and $61 million (7%) above the FY22 House level ($880 million). Specific areas under MCH include:
Gavi, the Vaccine Alliance funding totals $290 million, matching the FY21 enacted, FY22 Request, and FY22 House level.
Polio funding through the GHP account totals $101 million, $36 million (55%) above the FY21 enacted, FY22 Request, and FY22 House level ($65 million).
$139 million for the U.S. contribution to the United Nations Children’s Fund (UNICEF) provided through the International Organizations and Programs (IO&P) account, matching the FY21 enacted, FY22 Request, and FY22 House level.
Funding for nutrition totals $160 million, $10 million (7%) above the FY21 enacted and FY22 Request level ($150 million), and matching the FY22 House level.
Bilateral family planning and reproductive health (FP/RH) funding totals $650 million, $75 million (13%) above the FY21 enacted level ($575 million), $66 million (11%) above the FY22 Request ($584 million), but $110 million (15%) below the FY22 House level ($760 million).
Funding for the United Nations Population Fund (UNFPA) totals $55 million, $22.5 million (69%) above the FY21 enacted level ($32.5 million), $1 million (2%) below the FY22 Request ($56 million), and $15 million (21%) below the FY22 House level ($70 million).
Funding for the vulnerable children program totals $30.5 million, $5.5 million (22%) above the FY21 enacted and FY22 Request level ($25 million) and $0.5 million (2%) above the FY22 House level ($30 million).
Funding for neglected tropical diseases (NTDs) totals $112.5 million, $10 million (10%) above the FY21 enacted and FY22 Request level ($102.5 million), and matching the FY22 House level.
The SFOPs bill also includes the following policy provisions and transfer authorities:
A permanent repeal of the Mexico City Policy, representing the first time it has been included in the underlying bill in the Senate.
A provision directing USAID and the U.S. Global AIDS Coordinator that, for operating units implementing more than one global health program area, at least 10% of each GHP program line is spent on “cross-cutting health systems strengthening activities.”
States that up to $100 million be made available under the GHP account for the Emergency Reserve Fund, which is a mechanism that is used to quickly respond to emerging infectious disease outbreaks.
Provides the authority to transfer an amount “not to exceed an aggregate total of $200,000,000 of the funds appropriated by this Act” for international infectious disease outbreaks.
States that up to $250 million of funding from the GHP account “may be made available for a contribution to an international financing mechanism for pandemic preparedness.”
Labor, Health and Human Services, Education, and Related Agencies (Labor HHS):
Total global health funding at CDC and NIH through the Labor HHS bill is not yet known, as funding for some programs at NIH is determined at the agency level rather than specified by Congress in annual appropriations bills. [iii] Of the known amounts[iv], the Senate bill totals $694 million, which is $17 million above the FY21 enacted level, but $100 million below the FY22 Request and $246 million below the FY22 House level. Funding for all global health programs at CDC and NIH in the Senate bill either increased or remained flat compared to the FY21 enacted level. Several program areas in the Senate bill are below House levels, including parasitic diseases and global public health protection at CDC. Details on specific programs are as follows:
Funding provided to CDC for global health through the Labor HHS bill totals $598 million, an increase of $5 million (1%) above the FY21 enacted level ($593 million), $250 million (42%) above the FY22 Request ($698 million), but $245 million (29%) below the House FY22 level ($843 million). All of the increase at CDC compared to FY21 is for polio. Global health funding at CDC includes:
$128.4 million for global HIV/AIDS, matching the FY21 enacted, FY22 Request, and FY22 House level.
$9.2 million for global tuberculosis (TB), matching the FY21 enacted, FY22 Request, and FY22 House level.
$231 million for global immunization, $5 million (2%) above the FY21 enacted, FY22 Request, and FY22 House level ($226 million). Within this total are the following:
Funding for polio totals $181 million, $5 million (3%) above the FY21 enacted, FY22 Request, and FY22 House level ($176 million).
Funding for CDC’s other global vaccines/measles program totals $50 million, matching the FY21 enacted, FY22 Request, and FY22 House level.
$26 million for parasitic diseasesand malaria, matching the FY21 enacted level and $5 million (16%) below the FY22 Request and FY22 House level ($31 million).
$203 million for the global public health protection program, matching the FY21 enacted level, $100 million (33%) below the FY22 Request ($303 million), and $245 million (55%) below the FY22 House ($448 million).
Funding for the Fogarty International Center (FIC) at NIH totals $96.3 million, $12.2 million (15%) above the FY21 enacted level ($84 million) and essentially matching the FY22 Request and FY22 House level.
Resources:
FY2022 State, Foreign Operations, and Related Programs Appropriations Bill – Bill
FY2022 State, Foreign Operations, and Related Programs Appropriations Bill – Report
FY2022 Labor, Health and Human Services, Education, and Related Agencies Appropriations Bill – Bill
FY2022 Labor, Health and Human Services, Education, and Related Agencies Appropriations Bill – Report
The table (.xlsx) below compares global health funding in the FY 2022 Senate SFOPs and Labor HHS appropriations bills to the FY 2021 enacted funding amounts as outlined in the “Consolidated Appropriations Act, 2021” (P.L. 116-260; KFF summary here), the President’s FY 2022 request (KFF summary here), and the House FY 2022 SFOPs and LHHS bills (KFF summaries here and here).
See the KFF budget tracker for details on historical annual appropriations for global health programs.
Table: KFF Analysis of FY22 Senate Appropriations for Global Health
Department / Agency / Area
FY21Enactedi(millions)
FY22Request(millions)
FY22Houseii(millions)
FY22Senateii(millions)
Difference(millions)
FY22 Senate– FY21 Enacted
FY22 Senate– FY22 Request
FY22 Senate– FY22 House
State, Foreign Operations, and Related Programs (SFOPs) – Global Health
HIV/AIDS
$4,700.0
$4,700.0
$4,850.0
$4,700.0
$0 (0%)
$0 (0%)
$-150 (-3.1%)
State Department
$4,370.0
$4,370.0
$4,520.0
$4,370.0
$0(0%)
$0(0%)
$-150(-3.3%)
USAID
$330.0
$330.0
$330.0
$330.0
$0(0%)
$0(0%)
$0(0%)
of which Microbicides
$45.0
$45.0
$45.0
$45.0
$0(0%)
$0(0%)
$0(0%)
Global Fund
$1,560.0
$1,560.0
$1,560.0
$1,560.0
$0 (0%)
$0 (0%)
$0 (0%)
Tuberculosisiii
–
$321.0
–
–
–
–
–
Global Health Programs (GHP) account
$319.0
$319.0
$469.0
$400.0
$81(25.4%)
$81(25.4%)
$-69(-14.7%)
Economic Support Fund (ESF) account
Not specified
$2.0
Not specified
Not specified
–
–
–
Malaria
$770.0
$770.0
$820.0
$800.0
$30 (3.9%)
$30 (3.9%)
$-20 (-2.4%)
Maternal & Child Health (MCH)iv
–
$1,039.5
–
–
–
–
–
GHP account
$855.5
$879.5
$880.0
$941.0
$85.5(10%)
$61.5(7%)
$61(6.9%)
of which Gaviv
$290.0
$290.0
$290.0
$290.0
$0(0%)
$0(0%)
$0(0%)
of which Polio
$65.0
$65.0
$65.0
$101.0
$36(55.4%)
$36(55.4%)
$36(55.4%)
UNICEFvi
$139.0
$139.0
$139.0
$139.0
$0(0%)
$0(0%)
$0(0%)
ESF account
Not specified
$21.0
Not specified
Not specified
–
–
–
of which Polio
Not specified
$0.0
Not specified
Not specified
–
–
–
Nutritionvii
–
$154.8
–
–
–
$-154.8 (-100%)
–
GHP account
$150.0
$150.0
$160.0
$160.0
$10(6.7%)
$10(6.7%)
$0(0%)
ESF account
Not specified
$4.0
Not specified
Not specified
–
–
–
AEECA account
–
$0.8
–
–
–
–
–
Family Planning & Reproductive Health (FP/RH)viii
$607.5
$639.7
$830.0
$705.0
$97.5 (16%)
$65.3 (10.2%)
$-125 (-15.1%)
Bilateral FP/RHviii
$575.0
$583.7
$760.0
$650.0
$75(13%)
$66.3(11.4%)
$-110(-14.5%)
GHP accountviii
$524.0
$550.0
$760.0
$650.0
$126(24%)
$100(18.2%)
$-110(-14.5%)
ESF accountviii
$51.1
$33.7
Not specified
Not specified
–
–
–
UNFPAix
$32.5
$56.0
$70.0
$55.0
$22.5(69.2%)
$-1(-1.8%)
$-15(-21.4%)
Vulnerable Children
$25.0
$25.0
$30.0
$30.5
$5.5 (22%)
$5.5 (22%)
$0.5 (1.7%)
Neglected Tropical Diseases (NTDs)
$102.5
$102.5
$112.5
$112.5
$10 (9.8%)
$10 (9.8%)
$0 (0%)
Global Health Security
$190.0
$913.3
$1,000.0
$1,000.0
$810(426%)
$86.7 (9.5%)
$0 (0%)
GHP account
$190.0
$905.0
$1,000.0
$1,000.0
$810(426.3%)
$95(10.5%)
$0(0%)
USAID GHP accountx
$190.0
$655.0
$1,000.0
$1,000.0
$810(426.3%)
$345(52.7%)
$0(0%)
State GHP accountxi
–
$250.0
–
–
–
–
–
ESF account
Not specified
$8.3
Not specified
Not specified
–
–
–
Emergency Reserve Fund
xii
$90.0
xii
xii
–
$-90 (-100%)
–
SFOPs Total (GHP account only)
$9,196.0
$10,051.0
$10,641.5
$10,354.0
$1,158 (13%)
$303 (3%)
$-287.5 (-2.7%)
Labor Health & Human Services (Labor HHS)
Centers for Disease Control & Prevention (CDC) – Total Global Health
$592.8
$697.8
$842.8
$597.8
$5 (0.9%)
$250 (42.2%)
$-245 (-29.1%)
Global HIV/AIDS
$128.4
$128.4
$128.4
$128.4
$0(0%)
$0(0%)
$0(0%)
Global Tuberculosis
$9.2
$9.2
$9.2
$9.2
$0(0.2%)
$0(0%)
$0(0%)
Global Immunization
$226.0
$226.0
$226.0
$231.0
$5(2.2%)
$5(2.2%)
$5(2.2%)
Polio
$176.0
$176.0
$176.0
$181.0
$5(2.8%)
$5(2.8%)
$5(2.8%)
Other Global Vaccines/Measles
$50.0
$50.0
$50.0
$50.0
$0(0%)
$0(0%)
$0(0%)
Parasitic Diseases
$26.0
$31.0
$31.0
$26.0
$0(0%)
$-5(-16.1%)
$-5(-16.1%)
Global Public Health Protection
$203.2
$303.2
$448.2
$203.2
$0(0%)
$-100(-33%)
$-245(-54.7%)
Global Disease Detection and Emergency Response
$193.4
$293.4
Not specified
Not specified
–
–
–
of which Global Health Security (GHS)
Not specified
Not specified
Not specified
Not specified
–
–
–
Global Public Health Capacity Development
$9.8
$9.8
Not specified
Not specified
–
–
–
National Institutes of Health (NIH) – Total Global Health
$918.8
Not specified
Not specified
Not specified
–
–
–
HIV/AIDS
$616.7
$617.1
Not specified
Not specified
–
–
–
Malaria
$218.0
Not specified
Not specified
Not specified
–
–
–
Fogarty International Center (FIC)
$84.0
$96.3
$96.8
$96.3
$12.2(14.5%)
$-0.1(-0.1%)
$-0.6(-0.6%)
Labor HHS Total
$1,511.6
Not yet known
Not yet known
Not yet known
–
–
–
Notes:
i – The FY21 final bill includes a provision giving the Secretary of State the ability to transfer up to $200,000,000 from the ‘Global Health Programs’, ‘Development Assistance’, ‘International Disaster Assistance’, ‘Complex Crises Fund’, ‘Economic Support Fund’, ‘Democracy Fund’, ‘Assistance for Europe, Eurasia and Central Asia’, ‘Migration and Refugee Assistance’, and ‘Millennium Challenge Corporation’ accounts “to respond to a Public Health Emergency of International Concern.”
ii – The FY22 House and Senate SFOPs bills provide the authority to transfer an amount “not to exceed an aggregate total of $200,000,000 of the funds appropriated by this Act” for international infectious disease outbreaks. The FY22 House SFOPs bill states that an unspecified amount of funding from the GHP account “may be made available for a contribution to an international financing mechanism for pandemic preparedness.” The FY22 Senate SFOPs bill states that up to $250 million of funding from the GHP account “may be made available for a contribution to an international financing mechanism for pandemic preparedness.”
iii – Some tuberculosis funding is provided under the ESF account, which is not earmarked by Congress in the annual appropriations bills and determined at the agency level (e.g. in FY19, TB funding under the ESF account totaled $3.6 million).
iv – Some MCH funding is provided under the ESF account, which is not earmarked by Congress in the annual appropriations bills and determined at the agency level (e.g. in FY19, MCH funding under the ESF account totaled $14.42 million).
v – The FY21 final bill text provides additional funding to Gavi to support coronavirus response efforts, stating, “For an additional amount for ‘Global Health Programs’, $4,000,000,000, to remain available until September 30, 2022, to prevent, prepare for, and respond to coronavirus, including for vaccine procurement and delivery: Provided, That such funds shall be administered by the Administrator of the United States Agency for International Development and shall be made available as a contribution to the GAVI, Alliance.”
vi – UNICEF funding in the FY21final, FY22 House, and FY22 Senate bills include an earmark of $5 million for programs addressing female genital mutilation.
vii – Some nutrition funding is provided under the ESF account, which is not earmarked by Congress in the annual appropriations bills and determined at the agency level. (e.g. in FY17, nutrition funding under the ESF account totaled $21 million).
viii – The FY21 final bill states that “not less than $575,000,000 should be made available for family planning/reproductive health.” The FY22 request funding amounts are based on a bilateral total of $583.7 million as specified in the FY22 OMB Budget Appendices for the Department of State and Other International Programs. The FY22 House SFOPs bill text states that “not less than $760,000,000 shall be made available for family planning/reproductive health.” According to the FY22 House SFOPs bill report, $760 million is provided through the GHP account; however, it is possible that the administration could provide additional funding for FPRH activities through the ESF account. The FY22 Senate SFOPs bill text states that “not less than $650,000,000 shall be made available for family planning/reproductive health.” According to the bill report, $650 million is provided through the GHP account; however, it is possible that the administration could provide additional funding for FPRH activities through the ESF account.
ix – The FY21 final bill and FY22 House and Senate SFOPs bill texts state that if this funding is not provided to UNFPA it “shall be transferred to the ‘Global Health Programs’ account and shall be made available for family planning, maternal, and reproductive health activities.”
x – According to the Department of State, Foreign Operations, and Related Programs FY22 Congressional Budget Justification, $300 million of this funding is “for contributions to support multilateral initiatives leading the global COVID response through the Act-Accelerator platform.”
xi – According to the Department of State, Foreign Operations, and Related Programs FY22 Congressional Budget Justification, this funding is “to support a new health security financing mechanism, which would be developed alongside U.S. partners and allies, to ensure global readiness to respond to the next outbreak.”
xii – The FY21 final bill states that “up to $50,000,000 of the funds made available under the heading ‘Global Health Programs’ may be made available for the Emergency Reserve Fund.” The FY22 House SFOPs bill text states that “up to $90,000,000 of the funds made available under the heading ‘Global Health Programs’ may be made available for the Emergency Reserve Fund.” The FY22 Senate SFOPs bill text states that “up to $100,000,000 of the funds made available under the heading ‘Global Health Programs’ may be made available for the Emergency Reserve Fund.”
[i] Total funding for global health is not currently available as some funding provided through USAID and DoD is not yet available.
[ii] The FY22 Request provided $913 million for global health security, of which $905 million was through the GHP account and $8.3 million through the ESF account.
[iii] Funding for global HIV/AIDS and malaria research programs provided through the NIH is not yet known.
[iv] Known amounts include total global health funding at CDC and funding for the Fogarty International Center at NIH.
The Online News Association has named KFF’s Kaiser Health News and The Associated Press winners of its 2021 University of Florida Award in Investigative Data Journalism for their joint project “Underfunded and Under Threat.” The award is one of the highest honors in data journalism.
The joint KHN-AP investigation revealed that public health departments around the country had become understaffed and poorly equipped to confront the worst pandemic in a century. Their analysis found that at least 38,000 state and local public health jobs disappeared since 2008, and spending for local public health departments dropped by 18% per capita since 2010.
The joint KHN-AP investigation revealed that public health departments around the country had become understaffed and poorly equipped to confront the worst pandemic in a century. Their analysis found that at least 38,000 state and local public health jobs disappeared since 2008, and spending for local public health departments dropped by 18% per capita since 2010.
Journalists from both news organizations drew upon more than a dozen data sources to assess hundreds of state and local health departments. Reporters interviewed more than 150 people, surveyed all 50 statehouses, filed dozens of records requests and sorted through legislation across the country.
Even during the height of the coronavirus crisis, many states spent little of their federal covid-19 relief funding on public health departments, and state legislatures continued to undermine the public health system with budget cuts.
KHN and AP also followed the story throughout the pandemic, showing how the politicization of public health measures prompted physical threats against public health workers, with the backlash triggering the largest exodus of public health leaders in American history and a massive legislative rollback of public health powers.
AP and KHN also routinely shared data and offered guidance to news organizations to help them localize the findings of the investigation for their communities. The award — one of many KHN has received over the years — honors work that effectively uses data to tell a story, presents that data well to users and has relevance and journalistic impact.
About KFF and KHN
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
About AP
The Associated Press is an independent global news organization dedicated to factual reporting. Founded in 1846, AP today remains the most trusted source of fast, accurate, unbiased news in all formats and the essential provider of the technology and services vital to the news business. More than half the world’s population sees AP journalism every day.
Hulu’s new miniseries “Dopesick” was built on journalism, and its creators hope it will spark a renewed public discussion about the nation’s opioid crisis, show executives said during a recent panel discussion hosted by KFF’s Kaiser Health News and Hulu.
The event brought together the lead creative powers behind the show along with a journalist from KHN and a policy expert from KFF to unpack the making of “Dopesick” and what the show has to say about the origins of the opioid crisis. KFF’s journalists and policy experts have been tracking the devastating epidemic with on-the-ground stories as well as data-driven analyses for a number of years. The panelists brought their different lenses — creative, journalistic and policy — to focus on the devastating impact of opioids on ordinary Americans and the often ineffective efforts to combat this continuing public health emergency.
The panel discussion, moderated by Chaseedaw Giles, KHN’s digital strategy and audience engagement editor, featured executive producer, writer and showrunner Danny Strong; journalist Beth Macy, who authored the book on which the show is based; KHN correspondent Aneri Pattani, who has reported extensively on opioid policy, substance use and mental health; and KFF senior policy analyst Nirmita Panchal, whose analytical work focuses on mental health and substance use.
“What was unique about my collaboration with Beth is that the journalism side of the process never ended,” Strong said. “We would do interviews together, people would leak documents to us. … It was this unusual process in which we were writing a scripted drama and then simultaneously doing active investigative journalism.”
Macy, who was in the show’s writers’ room full time, said writers would incorporate into scripts revelations from newly released court filings in ongoing cases against Purdue Pharma, the company behind the drug OxyContin, which features prominently in the eight-episode miniseries.
“New documents were coming out all the time,” Macy said. “We would take turns — you go through this, I’ll go through this. And then we would all report back to Danny and decide what the best highlights were.”
In a 40-minute discussion, the panelists explored a wide range of topics about the show and the real-life opioid crisis it depicts, weaving in stories from people Pattani has interviewed for KHN radio and print pieces and findings from Panchal’s analyses. Topics included:
• How the show employed the tools of fiction, such as composite characters, to tell a larger truth
• The important role played by medication-assisted treatment, which combines medications with counseling and behavioral therapy in the treatment of opioid addiction
• The current state of the opioid crisis, marked by a record-high 93,000 deaths from drug overdoses in 2020; the expansion of the problem beyond largely rural, white communities; and the rise of highly addictive synthetic opioids like fentanyl
• The role of politics in the funding for, and availability of, different types of treatment
The economic fallout and social isolation of the COVID-19 pandemic have exacerbated the opioid epidemic, Panchal said. She noted that about 1 in 3 people now say they are experiencing anxiety and depression, compared to about 1 in 10 before the pandemic.
“The job loss, financial hardship, poor mental health — these are things that can often go hand in hand with substance use,” Panchal said.
Pattani noted that there are divisions among political leaders at all levels about how best to tackle the opioid crisis, with some pushing for more medication-assisted treatment, others favoring traditional rehab centers and some emphasizing a criminal justice approach to the problem.
Everyone is representing a district that has constituents affected by this,” she said. “I haven’t talked to a politician who says we don’t need to address the opioid epidemic, but I think they all disagree on how.”
“Dopesick” premiered on Hulu Oct. 13, with new installments of the miniseries available on Hulu every Wednesday. The panel discussion, recorded in KFF’s Washington, D.C., offices without a live audience due to COVID-19, can be viewed anytime on kff.org.
About KFF and KHN
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
About Hulu and “Dopesick”
From Executive Producer Danny Strong and starring and executive-produced by Michael Keaton, “Dopesick” examines how one company triggered the worst drug epidemic in American history. The series takes viewers to the epicenter of America’s struggle with opioid addiction, from the boardrooms of Big Pharma to a distressed Virginia mining community, to the hallways of the Drug Enforcement Administration. Defying all odds, heroes will emerge in an intense and thrilling ride to take down the craven corporate forces behind this national crisis and their allies. The limited series is inspired by The New York Times bestseller by Beth Macy.
The eight-episode series stars Michael Keaton, Peter Sarsgaard, Michael Stuhlbarg, Will Poulter and John Hoogenakker, with Kaitlyn Dever and Rosario Dawson. Guest stars include Phillipa Soo and Jake McDorman.
“Dopesick” is written by Emmy winner Danny Strong (“Empire,” “Recount,” “Game Change”) and directed by Oscar winner Barry Levinson (“Paterno,” “Rain Man”). Executive producers for “Dopesick” include Strong, John Goldwyn (“Dexter”), Keaton, Levinson, Warren Littlefield (“The Handmaid’s Tale,” “Fargo,” “The Old Man”), Beth Macy (“Dopesick”) and Karen Rosenfelt (“Twilight”).
This brief reviews final 2022 premium rate filings for Marketplace-participating individual market insurers in all 50 states and the District of Columbia. Although the ACA individual market represents a small share of the privately insured population, the rate filings for this market are detailed and publicly accessible, making them a useful source of information on how health insurers are thinking about their likely costs for the next year.
Most of the 311 rate filings reviewed,We find that most insurers expect spending and utilization to return to pre-pandemic levels in 2022 and do not expect COVID-19 to affect costs in the individual market. A majority of rate changes for 2022 are moderate, with most insurers posting premium increases or decreases of a few percentage points.
The brief is available on the Peterson-KFF Health System Tracker, an online information hub dedicated to monitoring and assessing the performance of the U.S. health system.
The October KFF Health Tracking Poll finds one in five adults in the U.S. report receiving ongoing support for daily activities such as bathing, dressing, or remembering medications, and a similar share say they are providing those type of services for a close friend or family member. About one in five adults (18%) also say they or a family member need either new or additional support from paid nurses or aides beyond what they are currently getting. The most common reason why people haven’t gotten the support they need is cost. More than three-fourths of those who say they need more help (14% of all adults) say “not being able to afford the cost of the care” is a reason why they or their family member has not received the additional support from paid nurses or aides.
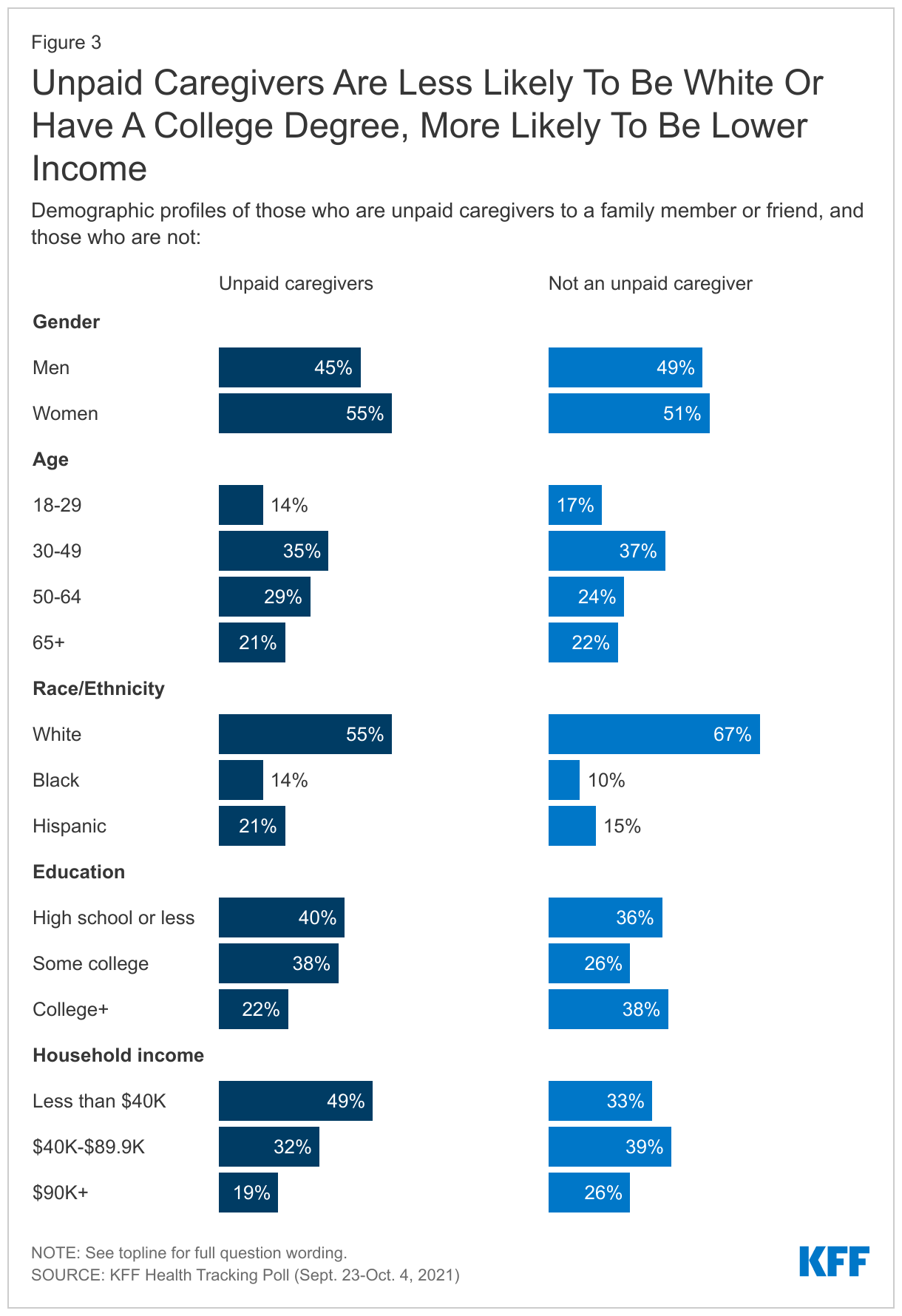
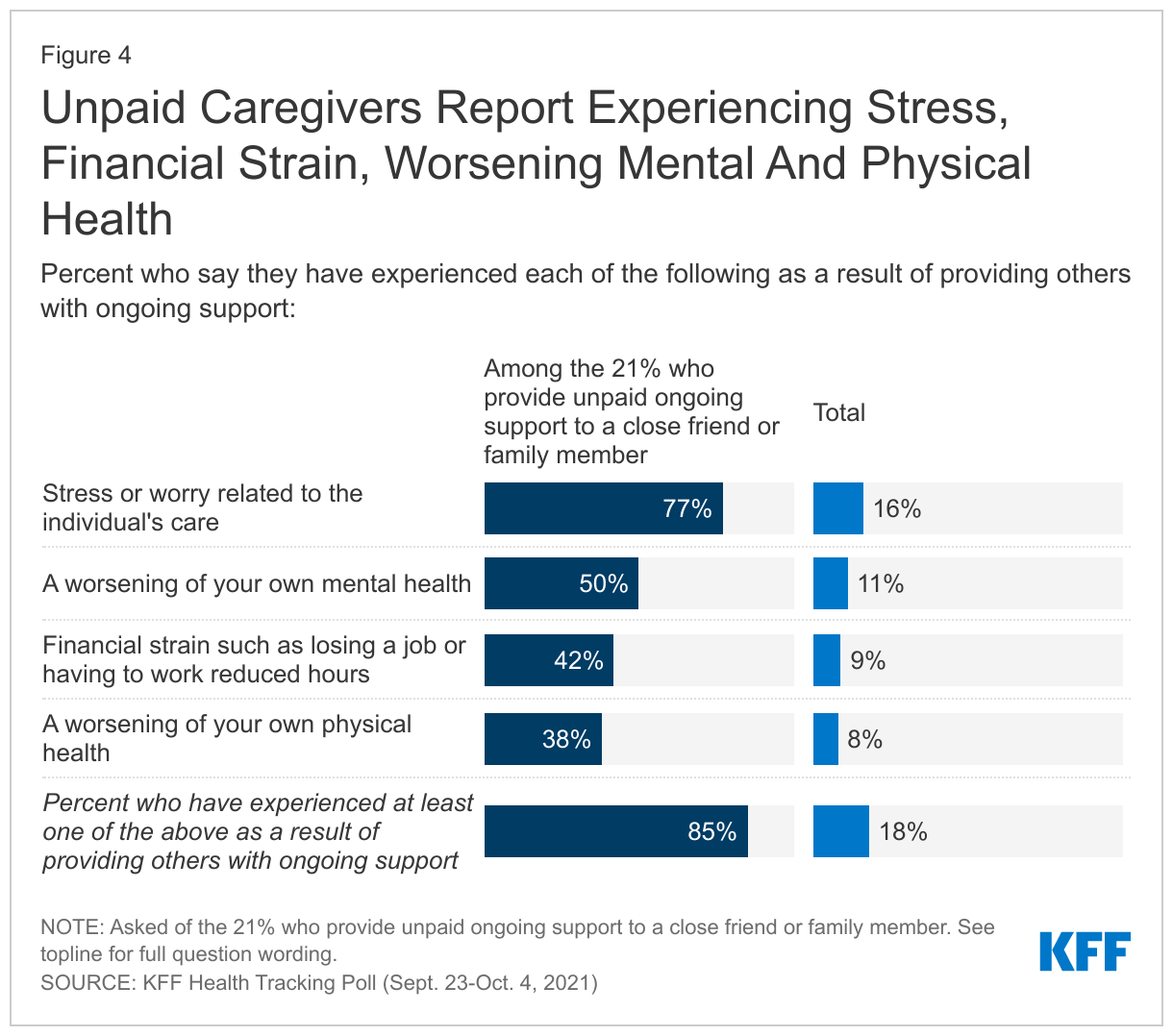
Many unpaid caregivers say providing support to friends or family members has caused them to worry or stress (77%), experience worsening of their own mental health (50%), financial strain due to inability to work (42%), or worsening of their own physical health (38%). Unpaid caregivers are more likely to be racial and ethnic minorities, those with lower education, and report lower levels of household income.
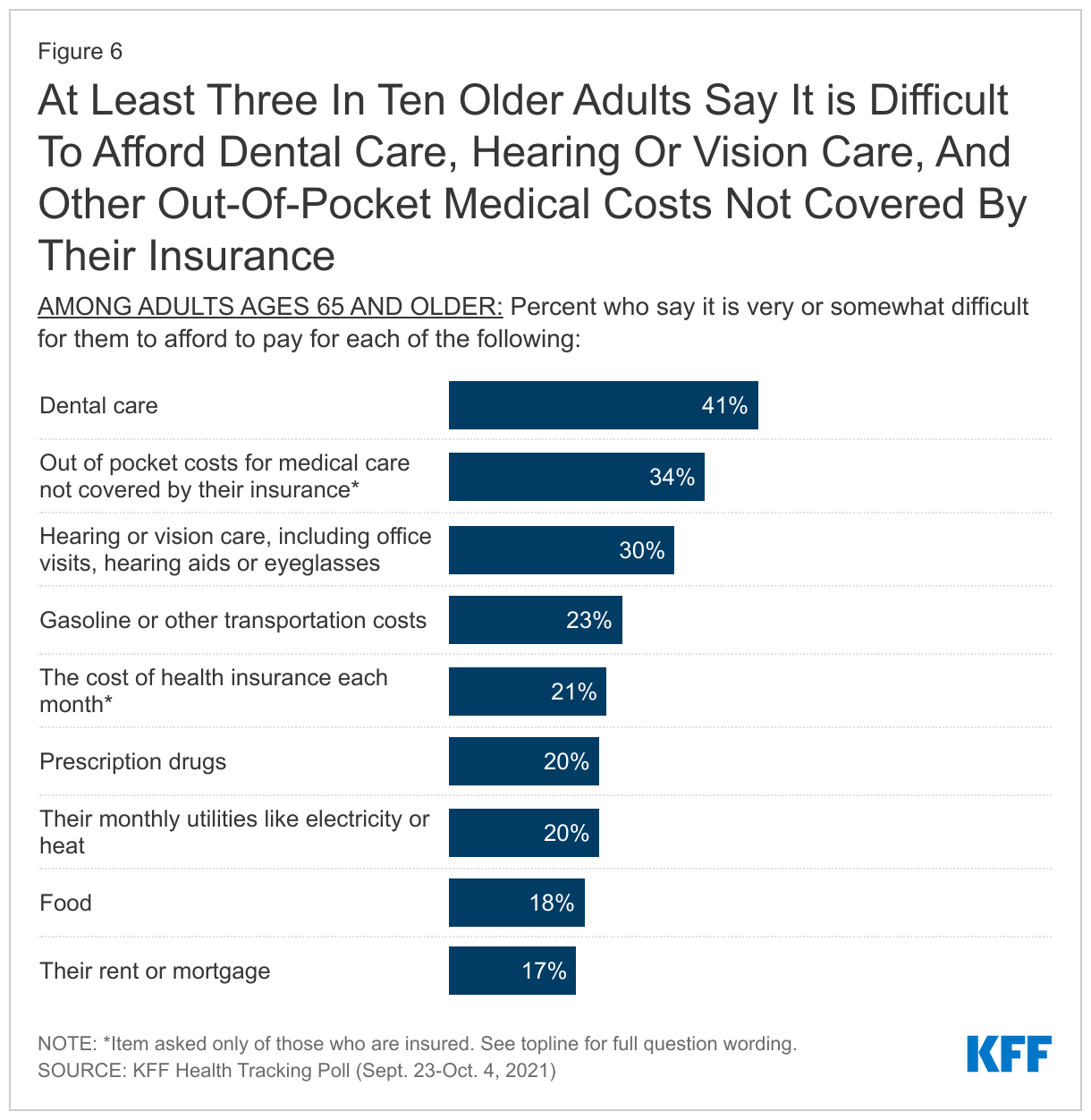
Significant shares of older adults in the U.S. report difficulty paying for various aspects of health care, especially services not generally covered by Medicare. Four in ten older adults (41%) report difficulty paying for dental care while three in ten report difficulty affording hearing or vision care (30%). Dental, vision, and hearing coverage are three benefits not generally covered by Medicare but are part of Democratic lawmakers’ proposals as part of the reconciliation spending package.
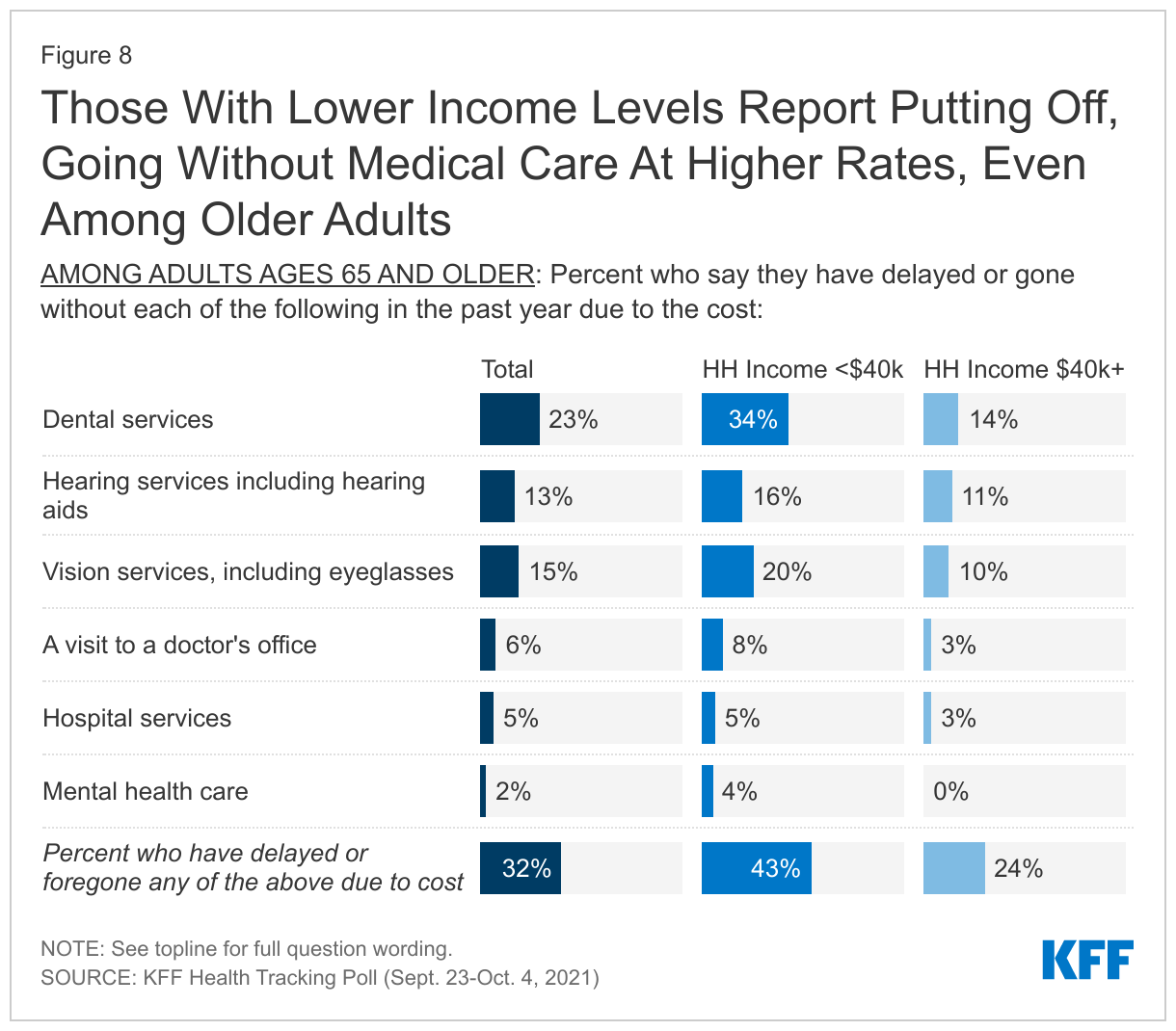
Many older adults who are eligible for Medicare also report putting off or foregoing medical care due to costs. While Medicare helps older adults pay for routine doctor visits and hospital stays, substantial shares of lower income older adults report putting off or foregoing services not covered by Medicare. Overall, more than four in ten older adults in households earning less than $40,000 annually report delaying or going without some form of medical care over the past year due to costs (compared to 24% of older adults with household incomes over $40,000), including dental care (34%), vision care (20%), and hearing services including hearing aids (16%).
With substantial shares of the public reporting financial strains associated with help with everyday activities for themselves or family members, and seniors reporting difficulty paying for some health care expenses, the latest KFF poll finds broad support for many of the proposals in the reconciliation package being currently discussed in Congress.
Home And Community Based Services
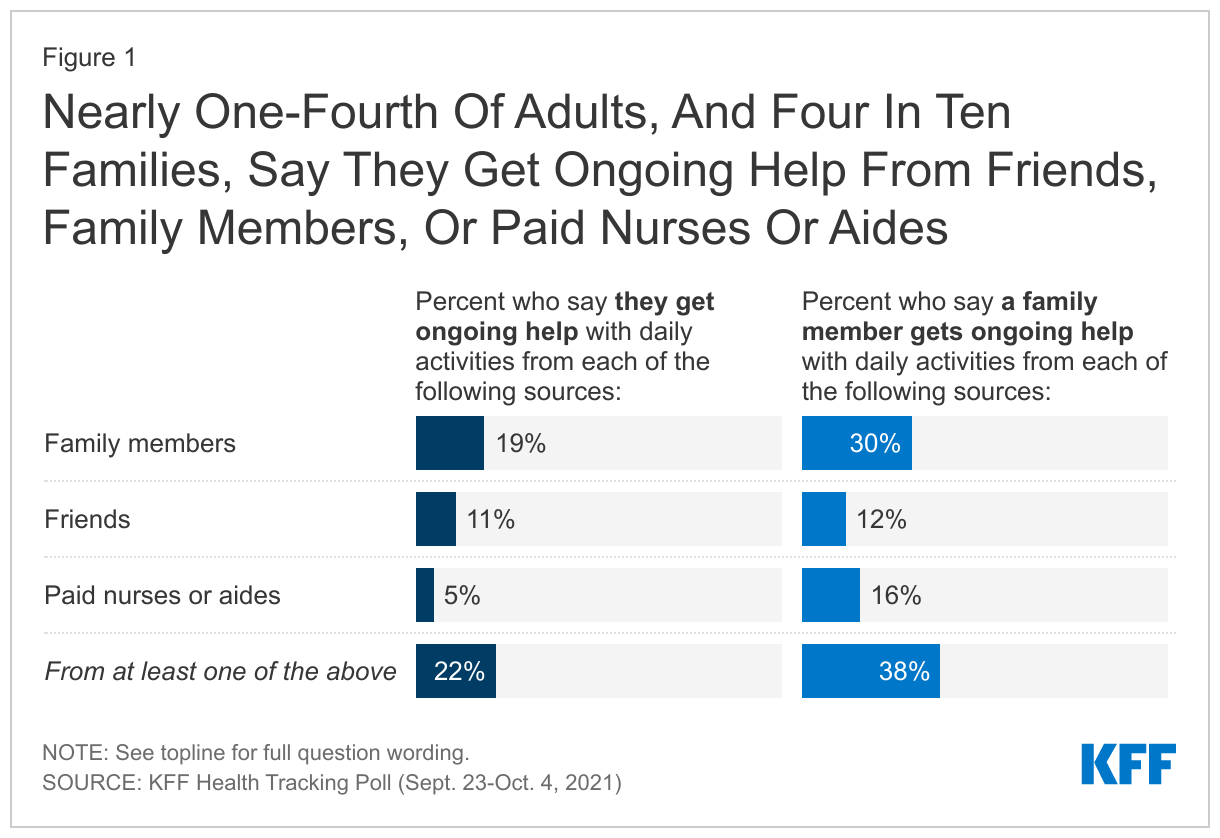
One in five adults, including 27% of adults 65 and older, say they are currently receiving ongoing support with everyday activities from either a family member (19%), a friend (11%), or paid nurses or aides (5%). Additionally, nearly four in ten (38%) adults say a family member gets ongoing help from at least one of these sources including another family member (30%), paid nurses or aides (16%) or friends (12%).
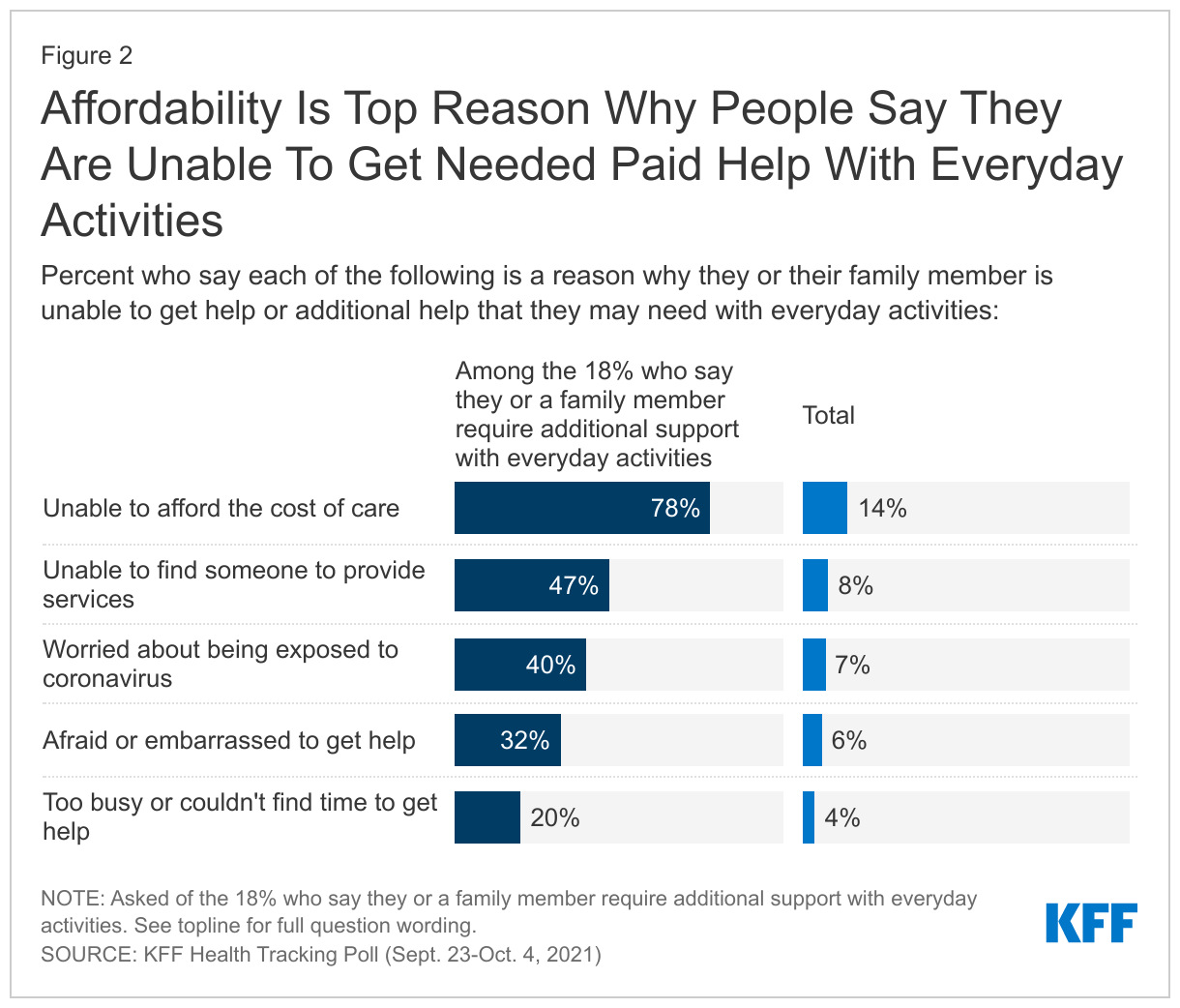
About one in five adults (18%) say they or a family member need either new or additional support from paid nurses or aides beyond what they are currently getting. The most common reason why people haven’t gotten the support they need is cost. More than three-fourths of those who say they need more help (14% of all adults) say “not being able to afford the cost of the care” is a reason why they or their family member has not received the additional support from paid nurses or aides. Other reasons include not being able to find someone to provide the services (47%, or 8% of all adults)1 , being worried about being exposed to coronavirus (40%, 7% of all adults), being afraid or embarrassed to get help (32%, 6%), or being too busy or unable to find the time to get help (20%, 4%).
With many reporting difficulty paying for cost of home and community based care, the poll also gauged support for Democratic proposals to increase funding to Medicaid to pay workers and expand home and community-based services (HCBS). Medicaid is the primary payer for long-term services and supports (LTSS), including home and community-based services (HCBS), that help seniors and people with disabilities with daily self-care and independent living needs. Majorities across partisans (79% total, 95% of Democrats, 76% of independents, 67% of Republicans) support increased funding to Medicaid to pay workers and expand home and community-based services (HCBS).
The toll On Unpaid Caregivers
With Congress discussing possible new tax credits to help with home and community based care, one in five adults (21%) say they are currently providing unpaid support with everyday activities to either a friend or family member, excluding the type of care young children need. Majorities across partisans also favor new tax credit to help people pay for such care (82% total, 94% of Democrats, 80% of independents, 73% of Republicans).
The KFF October Tracking Poll finds unpaid caregivers are more likely to be Black or Hispanic (14% and 21%) compared to those who are not unpaid caregivers (10% and 15%). About eight in ten unpaid caregivers to family and friends do not have a college degree, and about half have household incomes under $40,000.
Consistent with recent focus groups conducted by KFF, the poll finds most unpaid caregivers (85%, 18% of all adults) report experiencing at least one of several negative outcomes due to their caregiving responsibilities. Over three-fourths of unpaid caregivers (16% of all adults) say they have experienced stress or worry related to the care of the individual they are caring for, with an additional half (11% of all adults) say they have experienced a worsening of their own mental health as a result of providing this ongoing support. About four in ten (9% of total) say they have experienced financial strain, such as losing a job or having to work reduced hours. A similar share (38% and 8% of total) also say they have experienced a worsening of their own physical health.
Expanding Medicare Benefits
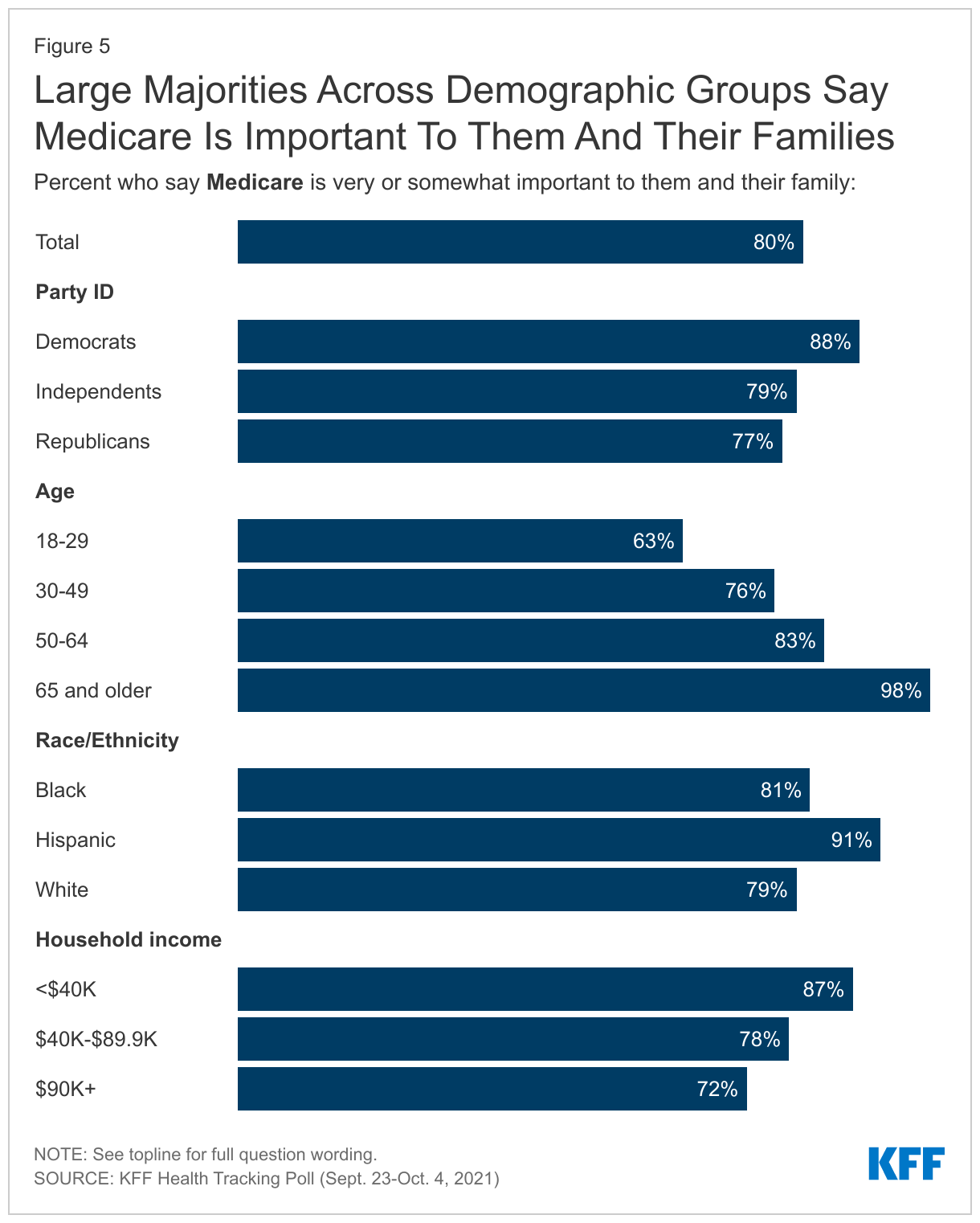
With Congress debating changes to the current Medicare program, eight in ten adults—and nearly all older adults—say Medicare is important to them and their family members. This includes at least seven in ten adults across partisanship, income groups, and racial and ethnic identity.
Significant shares of older adults in the U.S. report difficulty paying for various aspects of health care, especially services not generally covered by Medicare.2 Four in ten older adults (41%) report difficulty paying for dental care while three in ten report difficulty affording hearing or vision care (30%). Two in ten report difficulty affording their prescription drugs. Additionally, one-third report difficulty affording their out-of-pocket health care costs and one in five report the same about their monthly health insurance costs – shares comparable to those who report difficulty affording other household expenses such as rent or mortgage, gasoline, monthly utilities, or food and groceries.
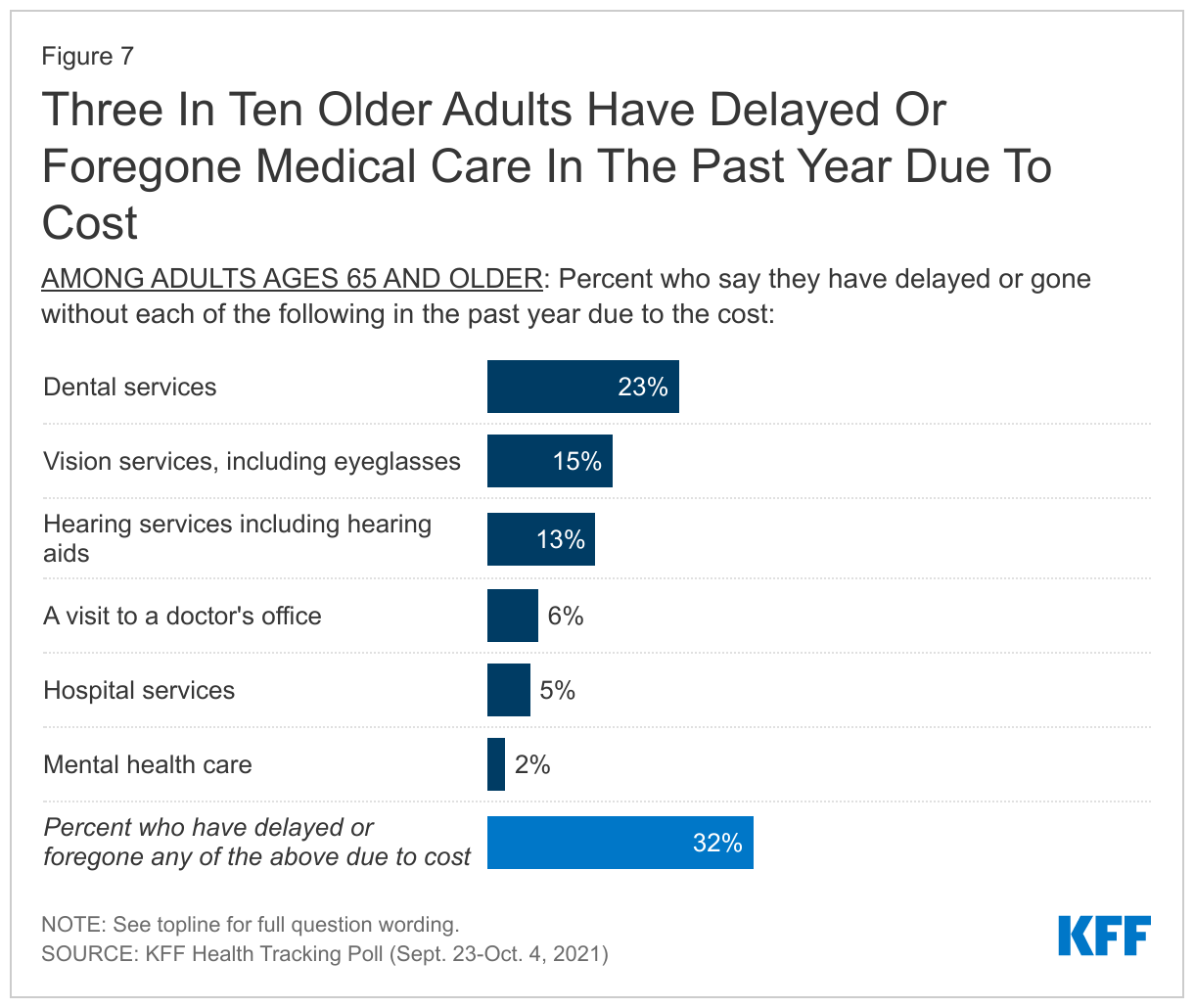
Dental services are the most common type of medical care that people have delayed or gone without with about with about one in four (23%) of adults ages 65 and older saying they have put off dental care in the past year due to cost. This is followed by vision services or eyeglasses (15%) and hearing aids (13%). Dental, vision, and hearing coverage are three benefits not generally covered by Medicare.
Few older adults report delaying or going without a doctor’s office visit (6%), hospital services (5%) or mental health care (2%) due to cost. Overall, three in ten adults 65 and older report delaying or going without certain medical care during the past year due to cost (32%).
Even among older adults who are eligible for Medicare, those with lower incomes report delaying or going without care at higher rates. More than four in ten older adults in households earning less than $40,000 annually report delaying or going without some form of medical care over the past year due to costs (compared to 24% of older adults with household incomes over $40,000). While Medicare helps older adults pay for routine doctor visits and hospital stays, substantial shares of lower income older adults report putting off or foregoing dental care (34%), vision care (20%), and hearing services including hearing aids (16%) that are not generally covered by Medicare.3
A large majority of the public (90%) favor expanding Medicare coverage to include dental, vision, and hearing coverage, including 97% of Democrats, 90% of independents, and 85% of Republicans. This proposal is also largely favored by adults 65 and older, including 96% of those in that age group who identify as Democrats or Democratic-leaning and 82% of their Republican counterparts. Proposals aimed at curbing the price individuals have to pay for their prescription drugs are favored by majorities of the public with at least eight in ten overall and at least three-fourths across partisans saying they favor each of the proposals asked about. Eighty-eight percent of adults favor limiting how much drug companies can increase the price for prescription drugs each year to not outpace the rate of inflation (including 93% of Democrats, 86% of independents, 89% of Republicans) and a similar share (85%) favor placing an annual limit on out-of-pocket prescription drug costs for people on Medicare (favored by 88% of Democrats, 85% of independents, 84% of Republicans). The proposed changes to Medicare drug negotiations as part of the reconciliation package poll findings were released earlier this week.
The Affordable Care Act
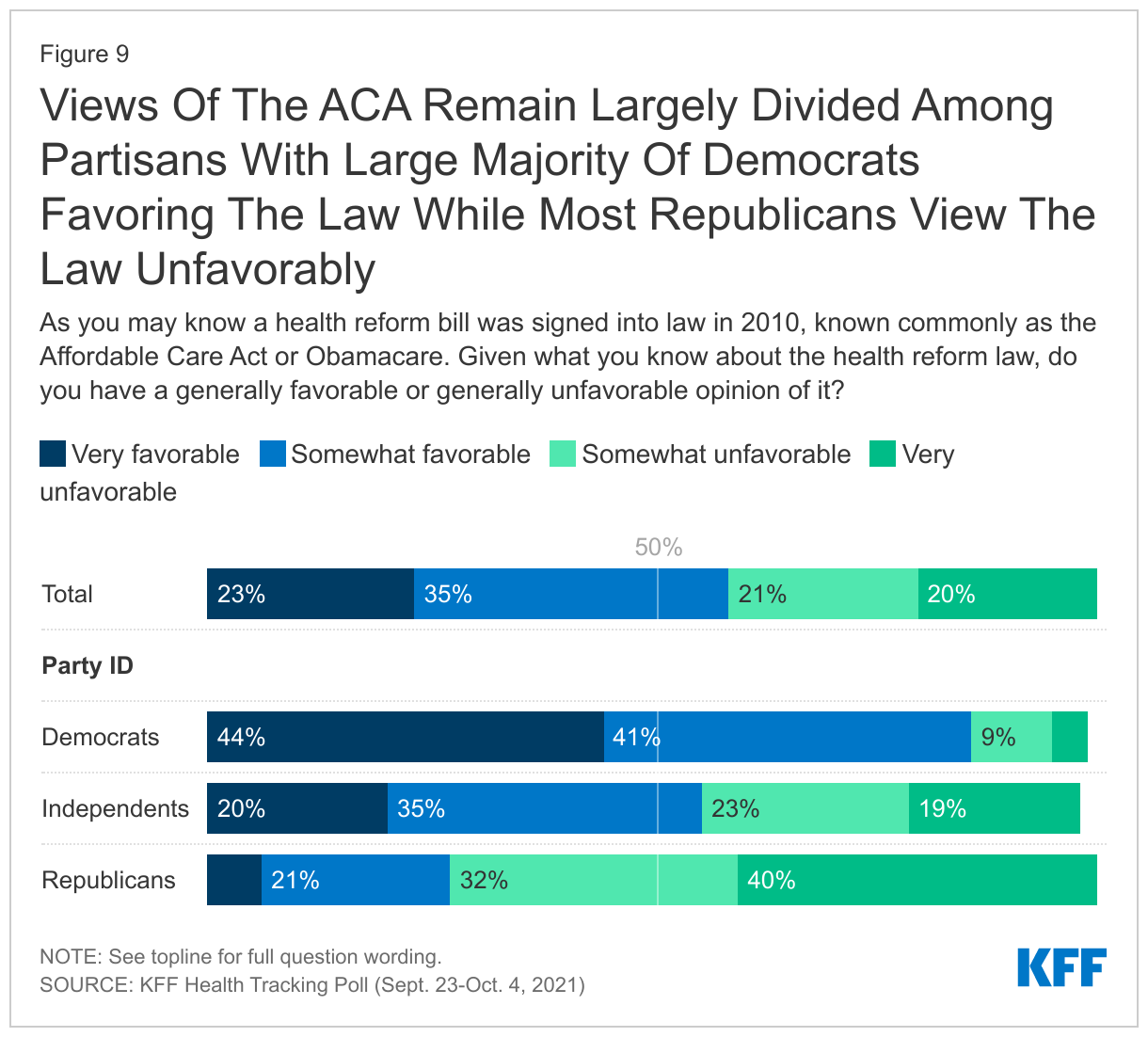
Views of the 2010 Affordable Care Act are still largely driven by party identification with nearly nine in ten Democrats saying they view the law favorably, while three-fourths of Republicans say they hold an unfavorable view. Independents are slightly more favorable than unfavorable with more than half saying they hold a positive opinion of the ACA. KFF has been polling on the ACA since its passage and since 2017 views have been more favorable than unfavorable but still sharply divided on party lines.
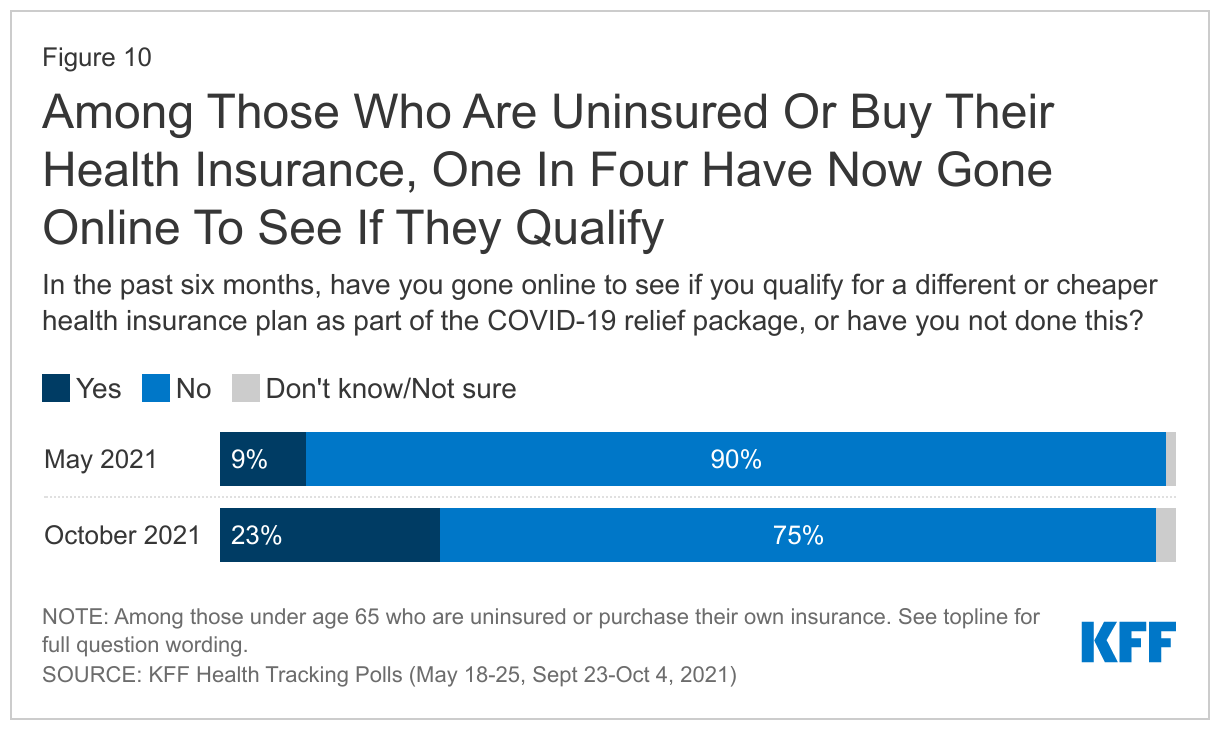
The COVID relief bill passed in early March 2021 providing additional financial help for people who buy their own health insurance coverage. Previous KFF polling found that a small minority of those likely eligible for additional financial help or coverage reporting going online to see if they qualify for a different or cheaper health insurance plan.
Among those under 65 years old, nine percent of those who are either uninsured or buy their own coverage reported going online in the in the two months before mid-May 2021 to see if they qualify for a different or cheaper health insurance plan or Medicaid as part of the COVID relief package. Four months later, the latest KFF polling finds that about one in four (23%) of those likely eligible for this assistance have gone online to see if they qualify, though majorities (75%) still have not.
In addition, changes to health insurance coverage provided under the Affordable Care Act continue to be seen through a partisan lens, with overwhelming majorities of Democrats and smaller majorities of Republicans expressing support. Overall, eight in ten adults favor making permanent the financial help to low- and moderate- income Americans who buy their own health insurance coverage (94% of Democrats, 79% of independents, 63% of Republicans). Three in four favor the federal government stepping in to provide insurance options for lower income people living in states that haven’t expanded their Medicaid programs (94% of Democrats, 76% of independents) but this is supported by a small majority (54%) of Republicans.
While the poll finds broad support for many of the Democratic proposed changes to the country’s health care system including the ACA, Medicaid, and Medicare, the poll did not ask about the potential costs and savings associated with each provision, or the size and scope of Democrats’ broader legislative plan, which includes many provisions unrelated to health care.
Methodology
The KFF Health Tracking Poll was conducted in English and Spanish with a nationally representative sample of 1,146 U.S. adults aged 18 or older, including an oversample of 474 adults ages 65 and older. The survey was conducted online and via phone from September 23-October 4, 2021, combining sample from two online probability-based panels and telephone samples recruited from random digit dialing (RDD). Sampling, data collection, weighting and tabulation were managed by SSRS of Glen Mills, PA in close collaboration with Kaiser Family Foundation researchers. The KFF team developed the questionnaire, analyzed the data and contributed financing for the survey.
Panel surveys were conducted through two online panels: (1) The SSRS Opinion Panel, a representative probability-based panel of U.S. adults ages 18 and older, recruited using the SSRS Omnibus poll (a weekly dual-frame RDD telephone survey) and through address-based sampling (ABS) (n=939). (2) The IPSOS KnowledgePanel, a probability-based online panel of U.S. adults ages 18 and older recruited through ABS targeting panelist (n=85). In order to reach adults 65 and older, a group less likely to be reached through an online panel, as well as those who do not have access to the internet, 122 interviews were completed by telephone, (including 79 among those who had previously indicated they do not use the internet).
The combined online, cell phone, and landline sample was weighted to match the sample demographics to estimates for the national population. A multi-stage weighting process was used to adjust for the fact that not all survey respondents were selected with the same probabilities and to account for systematic non-response. In the first weighting stage, adjustments were made regarding the probabilities of selection to the two web panels, and for probability of selection and non-response to the telephone callback samples. Each of these surveys were probability samples of the U.S. adult population that were weighted to the Census Bureau’s March 2020 Current Population Survey (CPS), by gender, age, race/ethnicity, education, and Census region. The data were also weighted to match internet usage metrics based on the U.S. Census’s 2019 American Community Survey, civic engagement metrics based on the September 2019 CPS Volunteering and Civic Life Supplement, and to match party identification within age groups from previous KFF RDD samples.
All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 4 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Note that sampling error is only one of many potential sources of error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
Group
N (unweighted)
M.O.S.E.
Total
1,146
± 4 percentage points
Age
18-64
672
± 5 percentage points
65+
474
± 7 percentage points
Party Identification
Democrats
476
± 6 percentage points
Republicans
231
± 8 percentage points
Independents
322
± 7 percentage points
Endnotes
A shortage of direct care workers predated and has been intensified by the COVID-19 pandemic, characterized by low wages and limited opportunities for career advancement. The direct care workforce is disproportionately female and Black. Debate in Congress to increase funding for Medicaid HCBS is aimed at strengthening the direct care workforce. ↩︎
In this column for the JAMA Health Forum, Larry Levitt explores why the Medicaid “coverage gap” still exists in 12 states that have not expanded their Medicaid programs under the Affordable Care Act, why it matters, and why eliminating it could prove challenging.
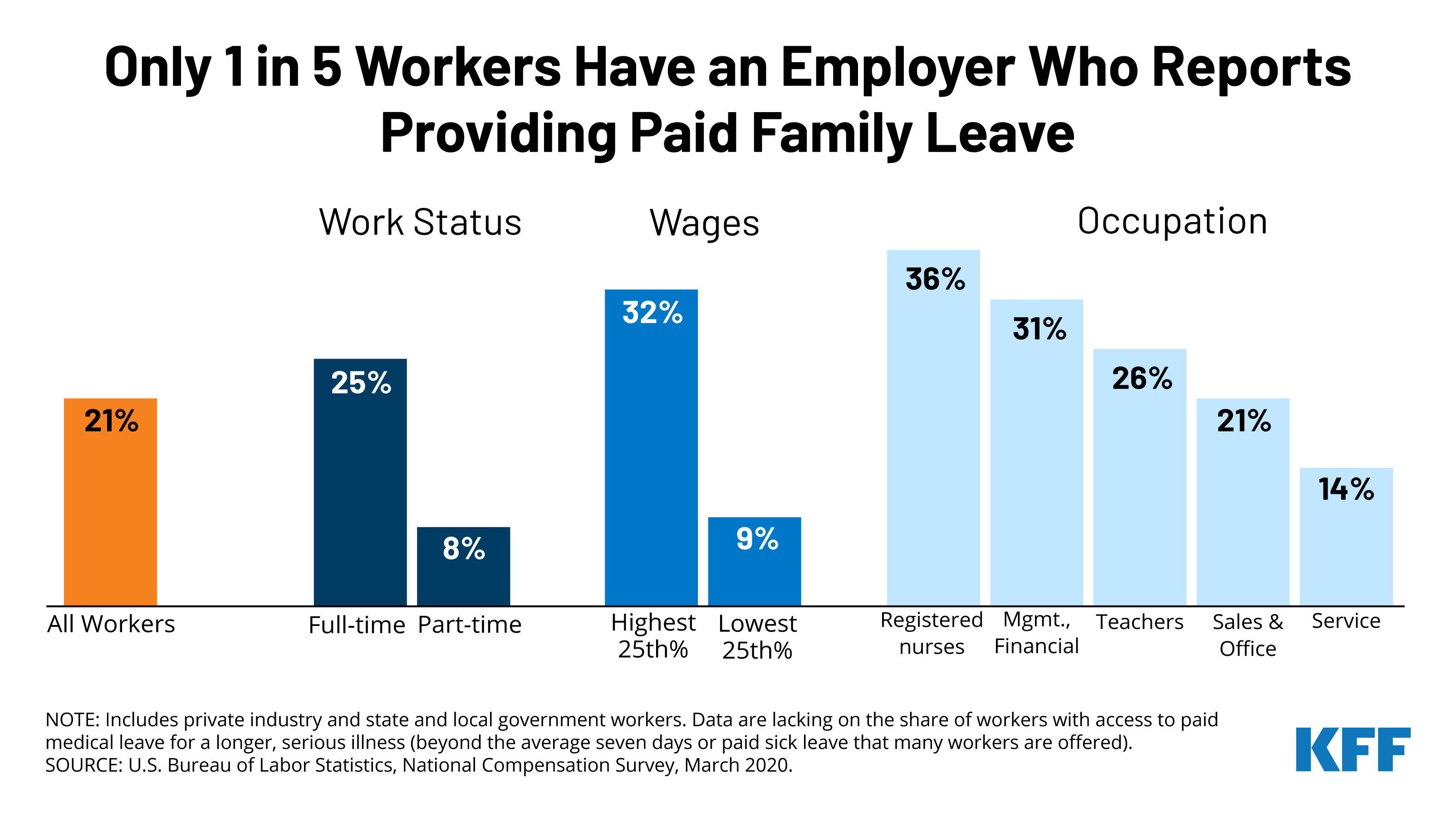
Most people will need to take time off work to care for themselves or their families at some point, but only one in five (21%) workers have access to paid family leave through their employer. That share is even lower for low-wage and part-time workers, and in certain occupations.
Congress is considering creating a universal paid family and medical leave program as part of the Build Back Better Act, which Democrats are looking to pass through the budget reconciliation process relying on Democratic votes. The proposal guarantees 12 weeks of paid family and medical leave annually to all workers in the United States for several qualifying reasons, including welcoming a new child, recovering from a serious illness, and caring for a seriously ill family member. It’s unclear how the program would be financed or whether more changes will be made as pressure to reduce the cost of the social spending package could limit the bill’s scope.
With the Medicare open enrollment period set to begin October 15, a new KFF analysis finds that 7 in 10 beneficiaries (71%) say that they didn’t compare their coverage options during a recent open enrollment season. Twenty-nine percent said they did compare Medicare plans.
But not shopping around can have a big impact on enrollees’ coverage and costs. The Centers for Medicare & Medicaid Services (CMS) recommends that beneficiaries review and compare Medicare plans each year.
The new analysis examines the share of Medicare beneficiaries who compared plans during the 2018 open enrollment period for coverage in 2019, the share who compared drug coverage in Medicare Advantage and stand-alone drug plans, and variation by demographic characteristics, based on an analysis of the 2019 Medicare Current Beneficiary Survey (the most recent year available).
Other key findings include:
• The share of beneficiaries who said they did not compare their options was higher among beneficiaries who are Black (74%) and Hispanic (79%), ages 85 and older (84%), with low incomes (85%), and those enrolled in both Medicare and Medicaid (87%).
• When it comes to Part D drug coverage, 81 percent of Medicare Advantage drug plan enrollees and 72 percent of Medicare stand-alone drug plan enrollees said they did not compare drug coverage offered by their current plan to other plans.
• Nearly half (47%) of all beneficiaries with Medicare said they had never visited the official Medicare website for information, 53 percent reported they had never called the 1-800-MEDICARE helpline and 31 percent said they did not read the Medicare & You handbook.
Medicare beneficiaries with traditional Medicare can compare and switch Medicare Part D stand-alone prescription drug plans or join a Medicare Advantage plan, the privately run alternative to traditional Medicare. At the same time, enrollees in Medicare Advantage can compare and switch Medicare Advantage plans or elect coverage under traditional Medicare with or without a stand-alone drug plan.
Coverage and costs vary widely among both Medicare Advantage plans and Part D prescription drug plans. Plans can change from one year to the next, as can beneficiaries’ health care needs, which could lead to unexpected and avoidable costs, and disruptions in care for beneficiaries who stay put and do not at least review their options annually.