KFF designs, conducts and analyzes original public opinion and survey research on Americans’ attitudes, knowledge, and experiences with the health care system to help amplify the public’s voice in major national debates.
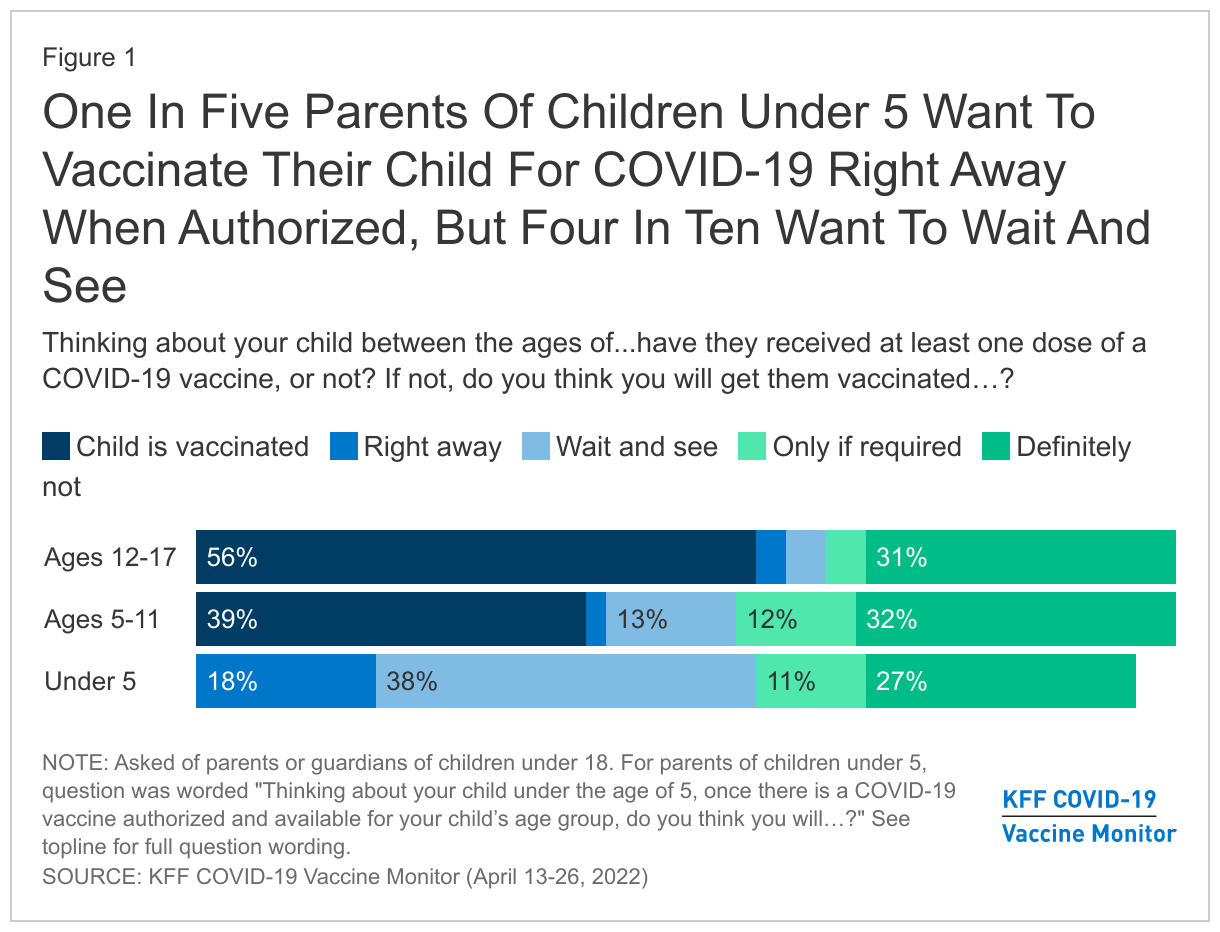
With news that Moderna has asked the FDA to authorize its COVID-19 vaccine for young children, the latest KFF COVID-19 Vaccine Monitor survey finds that about one in five parents of children under age 5 (18%) are eager to get their child vaccinated right away, while a larger share (38%) say they plan to wait a while to see how the vaccine is working for others. About four in ten parents of children under 5 are more reluctant to get their child vaccinated with 27% saying they will “definitely not” get their child vaccinated and 11% saying they will only do so if they are required. Just over half of parents of children in this age range say they do not have enough information about the vaccines’ safety and effectiveness for children under age 5.
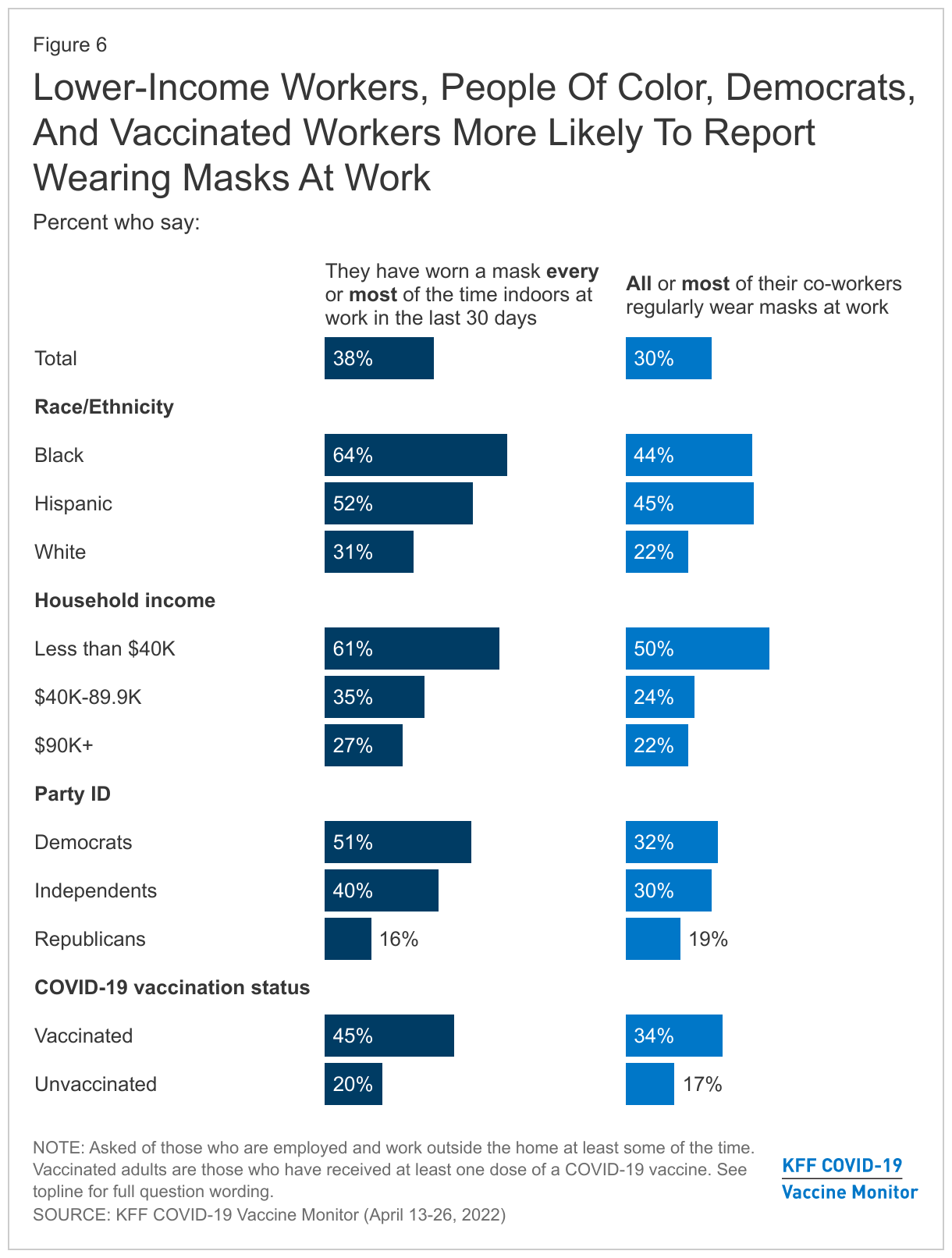
With mask mandates being lifted in many places, most workers say they and their coworkers are not regularly wearing masks when indoors at work. Just under four in ten (38%) of those who work outside their home say they wore a mask every time or most of the time when indoors at their place of work in the past 30 days, and 43% say they never wore a mask at work in the past 30 days. Black workers (64%), Hispanic workers (52%), and those with lower incomes (61%) are more likely than their counterparts to report wearing masks at work at least most of the time.
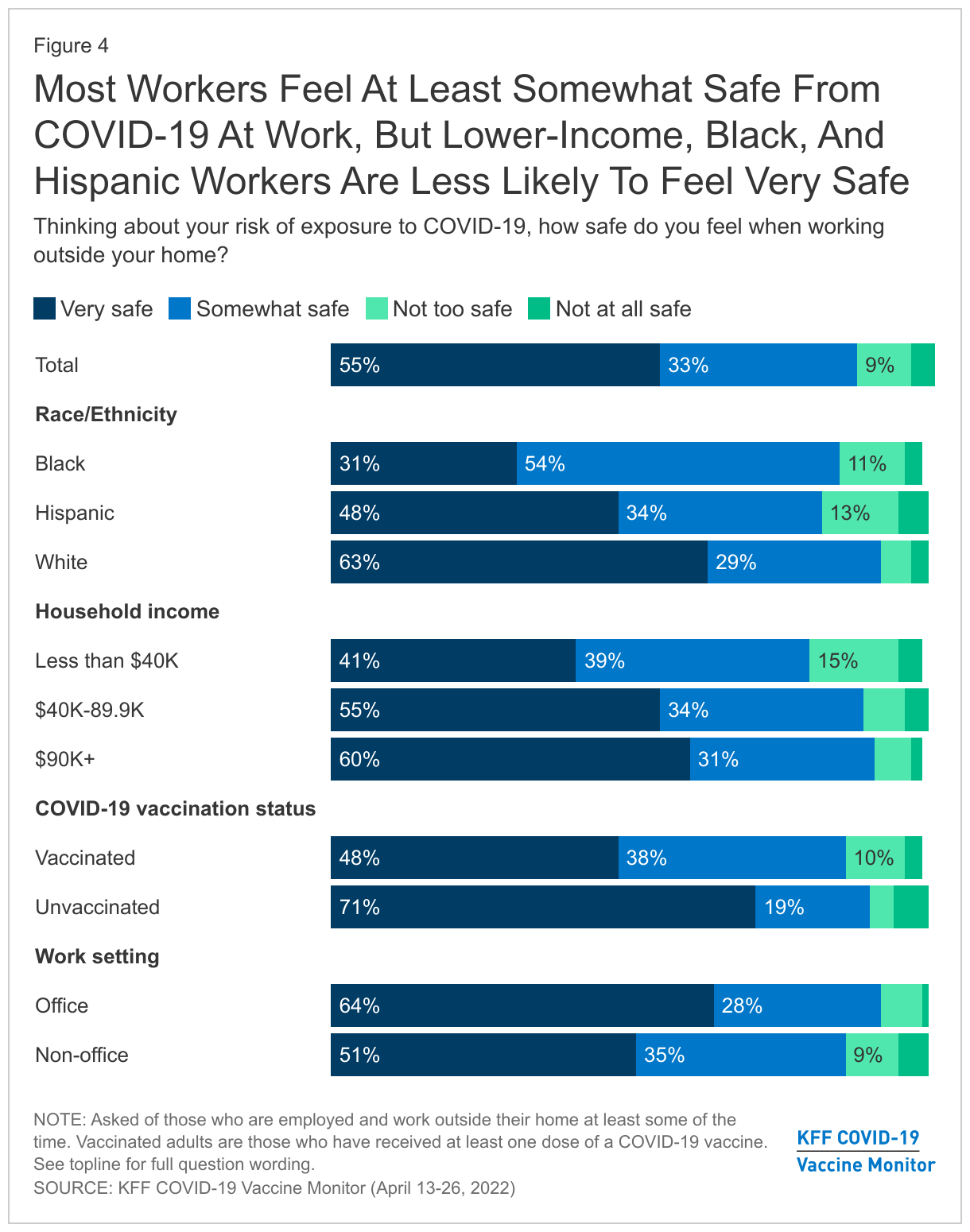
Most workers (88%) say they feel at least “somewhat safe” from COVID-19 in the workplace. However, Black and Hispanic workers and those with lower incomes are less likely than their counterparts to say they feel “very safe” from COVID-19 at work.
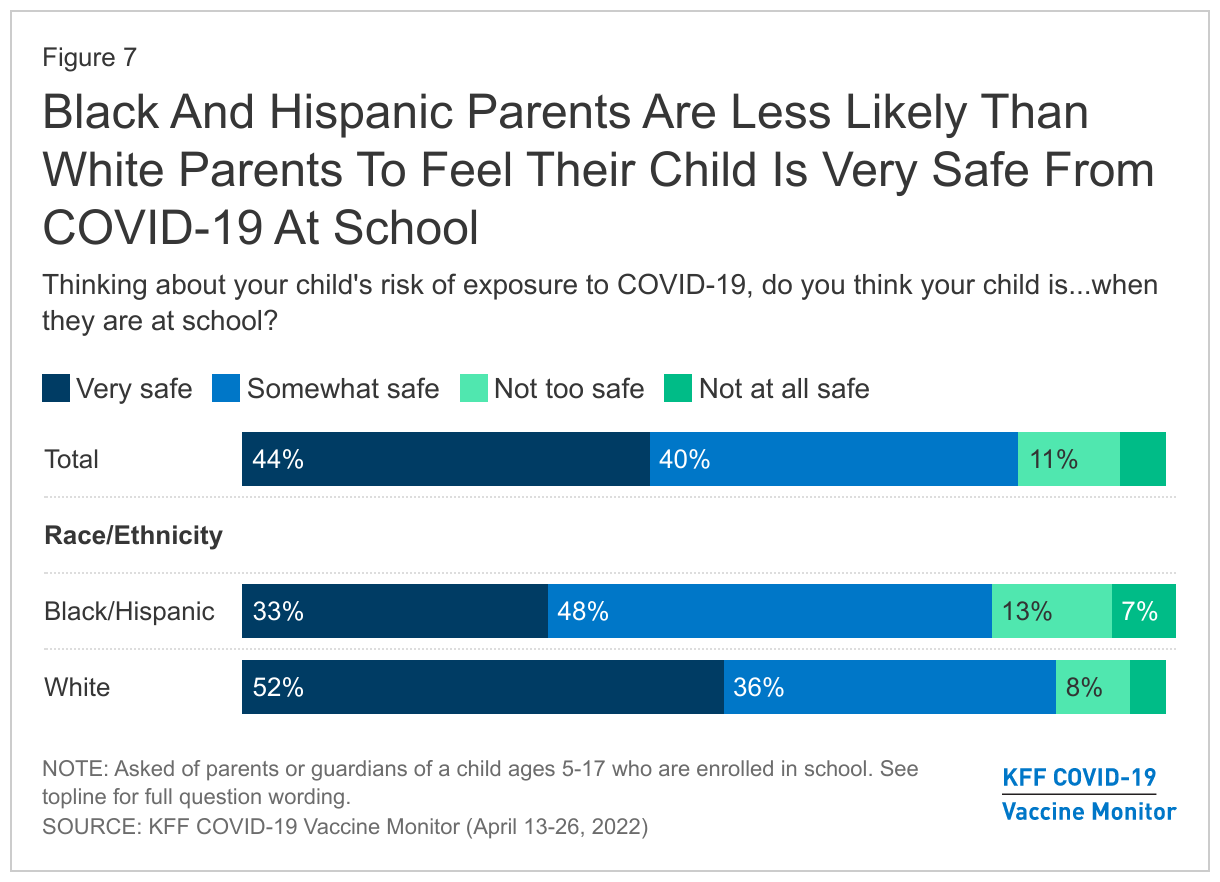
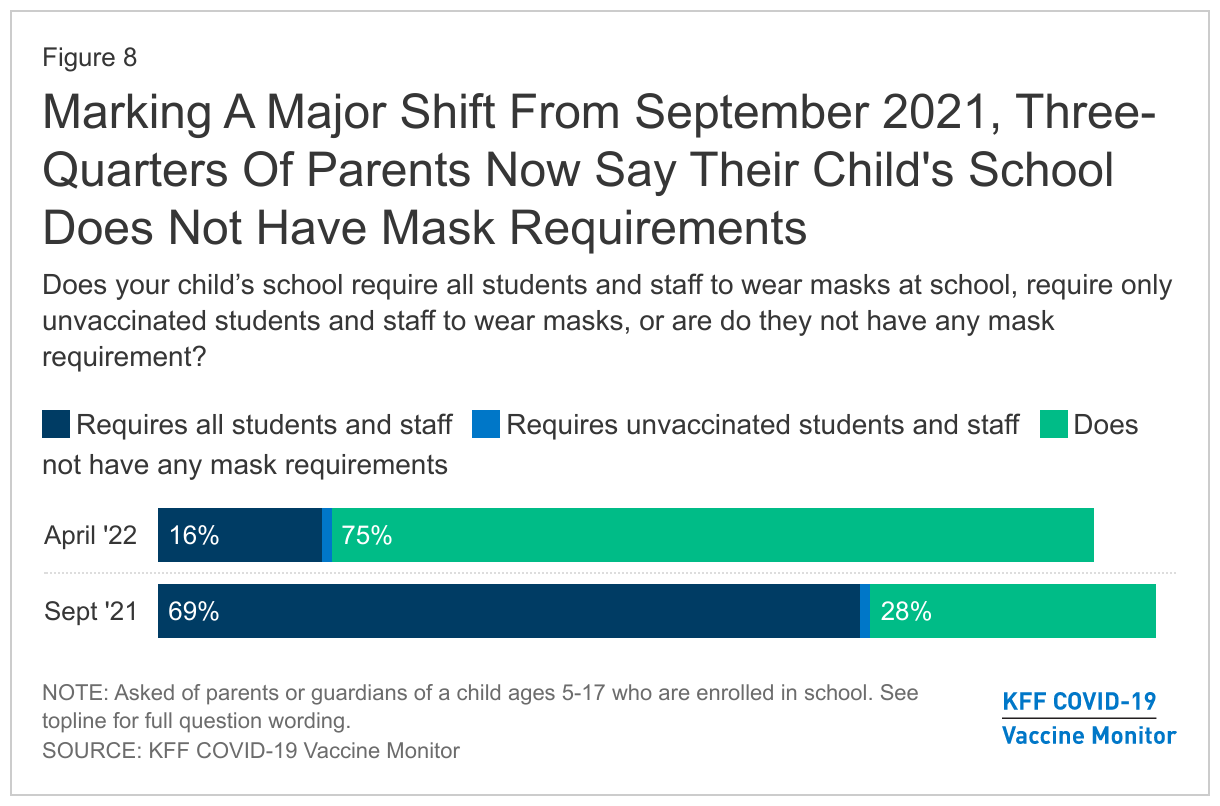
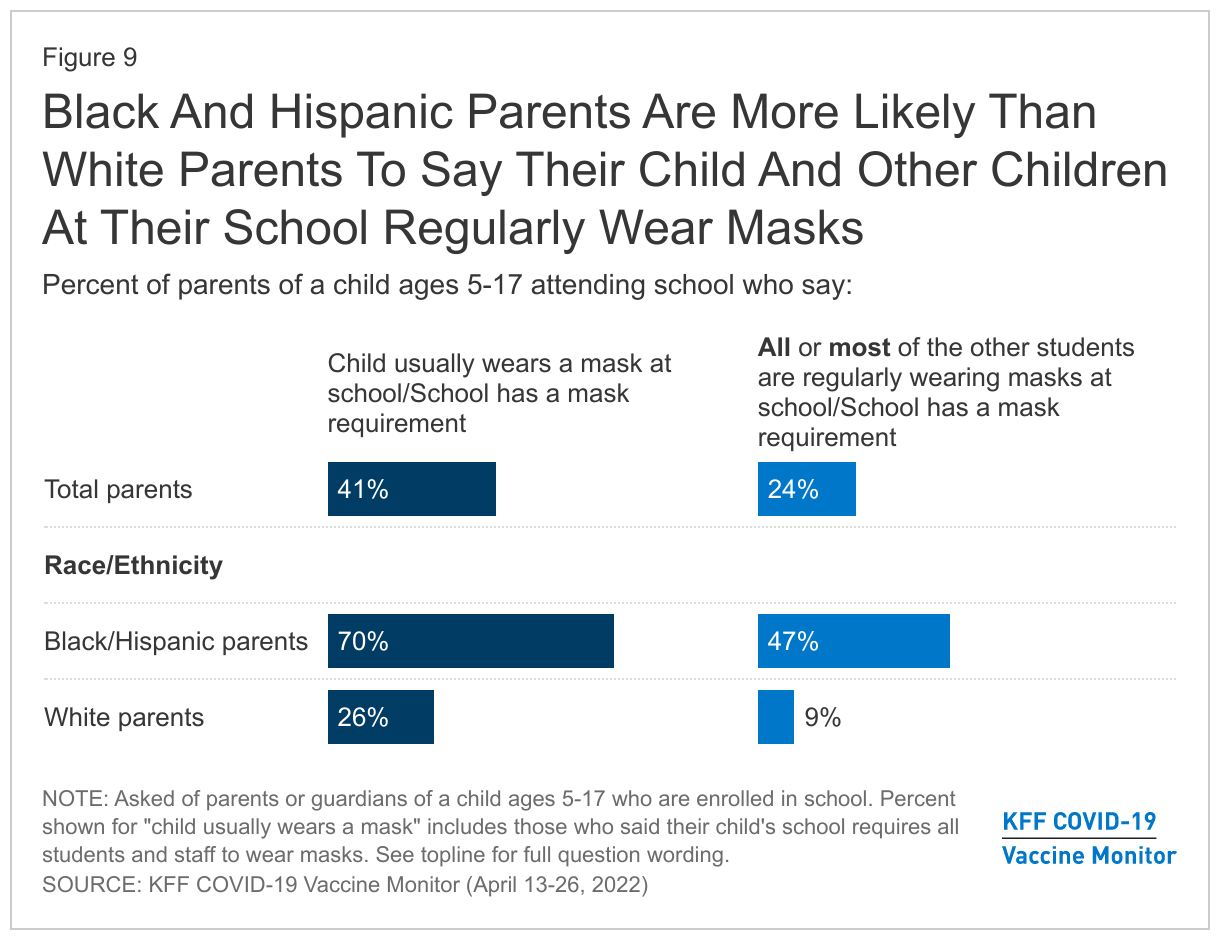
While most parents (84%) feel their child is at least “somewhat safe” from COVID-19 at school, parents who are Black or Hispanic are less likely to feel their child is “very safe” than White parents (33% vs. 52%). Fewer than two in ten parents overall now say their child’s school has a mask requirement in place, down from seven in ten last September. Notably, Black and Hispanic parents are almost three times as likely as White parents to say their child usually wears a mask at school.
Uptake of both COVID-19 vaccines and booster doses appears to have leveled off, with three-quarters of adults reporting that they’ve received at least one dose of a vaccine (relatively unchanged since September 2021) and close to half reporting at least one booster dose (the same share as in February). While previous Vaccine Monitor surveys indicated that Black and Hispanic adults were lagging behind White adults in booster uptake, the latest survey finds that similar shares of Black, Hispanic, and White adults now report receiving a booster.
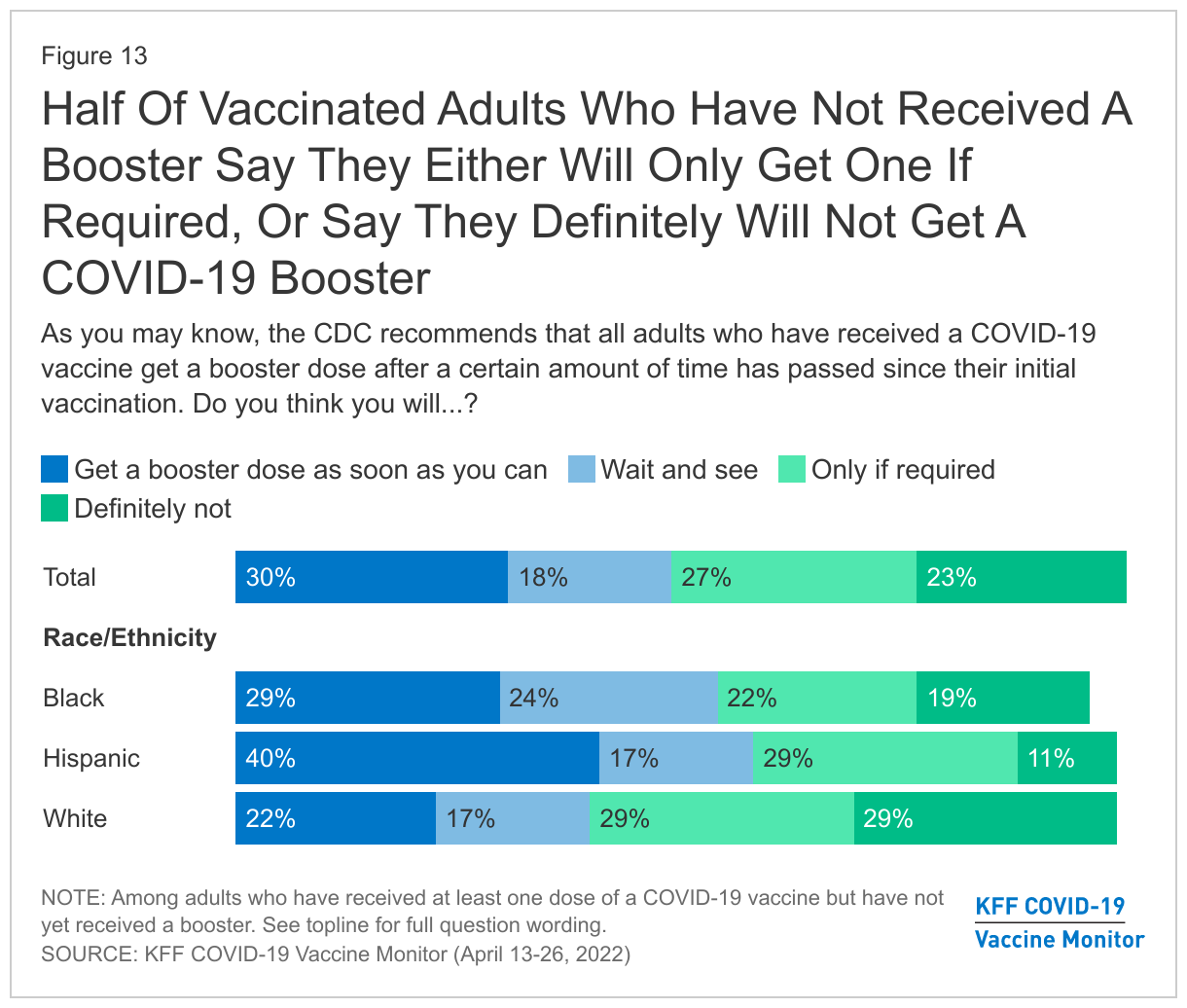
Prospects for further booster uptake are mixed, with half of those who are vaccinated but not boosted saying they will “definitely not” get a booster or get one only if required, and most of the eligible but unboosted population saying they feel they have sufficient protection from their initial vaccination or a prior infection.
With case rates beginning to rise again in the U.S., around a third of the public think there’s currently a new wave of COVID-19 hitting the country, while half say there is not a new wave, and the remainder are not sure. People’s perceptions about whether the country is experiencing a new wave of COVID-19 infections seem to reflect their view of what is happening among their own family and friends, with around six in ten reporting that among people they know, they’ve seen fewer COVID-19 cases in the past 30 days.
While most adults say their families and their employers are very prepared for future COVID-19 surges, fewer say the same about their local area or about the country overall. At the same time, when it comes to information about COVID-19 vaccines, people continue to trust personal sources like their own doctors and employers more than official sources like the CDC, FDA, or state governments. Trust in the CDC, FDA, Dr. Anthony Fauci, and President Biden as sources of reliable information on COVID-19 vaccines has declined since last summer, particularly among Republicans.
Parents’ Vaccination Intentions for Their Children
Though the FDA has still not authorized any COVID-19 vaccine for young children, Moderna recently announced that it has asked the FDA to authorize its vaccine for children under 6. Fielded prior to the Moderna announcement, the latest KFF COVID-19 Vaccine Monitor survey finds that one in five parents of children under 5 (18%) are eager to vaccinate their child and say they will do so right away once a COVID-19 vaccine is authorized for their age group. Almost four in ten parents of children under 5 say they want to “wait and see” before getting their young child vaccinated (38%). Another four in ten parents are more reluctant to get their young child vaccinated with 11% saying they will only do so if they are required and 27% saying they will “definitely not” get their child under 5 vaccinated for COVID-19.
Among parents of 5 to 11 year-olds, who have been eligible for vaccination since October, about four in ten (39%) say their child has gotten vaccinated while a large share say they will either only get their child vaccinated if they are required for school (12%) or say their child will definitely not get the COVID-19 vaccine (32%). Most parents of 12 to 17 year-olds say their teenager has been vaccinated (56%, fairly steady since January), while about three in ten (31%) say they will “definitely not” get their teen vaccinated and 4% say they will only do so if they are required.
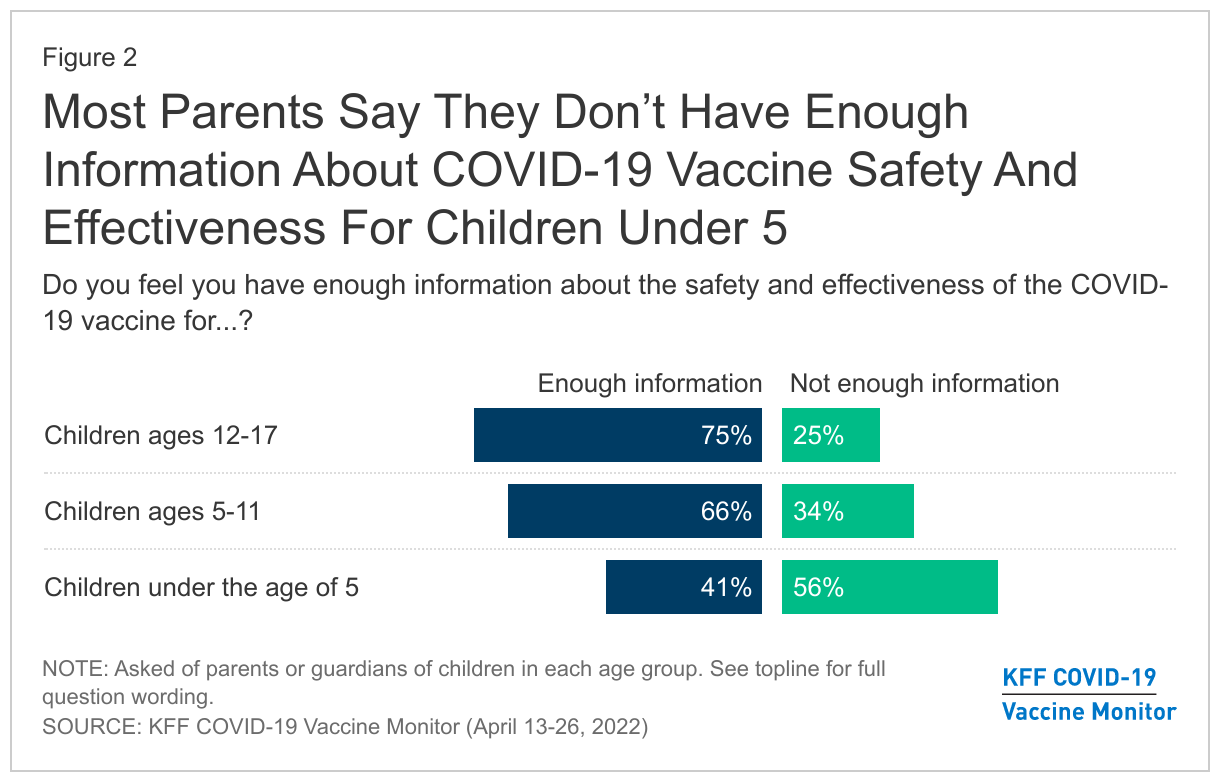
Lack of available information may be a factor in parents’ reluctance to get their youngest children vaccinated right away. A majority of parents of children under five say they don’t have enough information about the safety and effectiveness of COVID-19 vaccines for children in this age group (56%). By contrast, most parents of older children feel better informed, with three-fourths of parents of teens and two-thirds of parents of kids ages 5-11 saying they have enough information about vaccine safety and effectiveness for their age group.
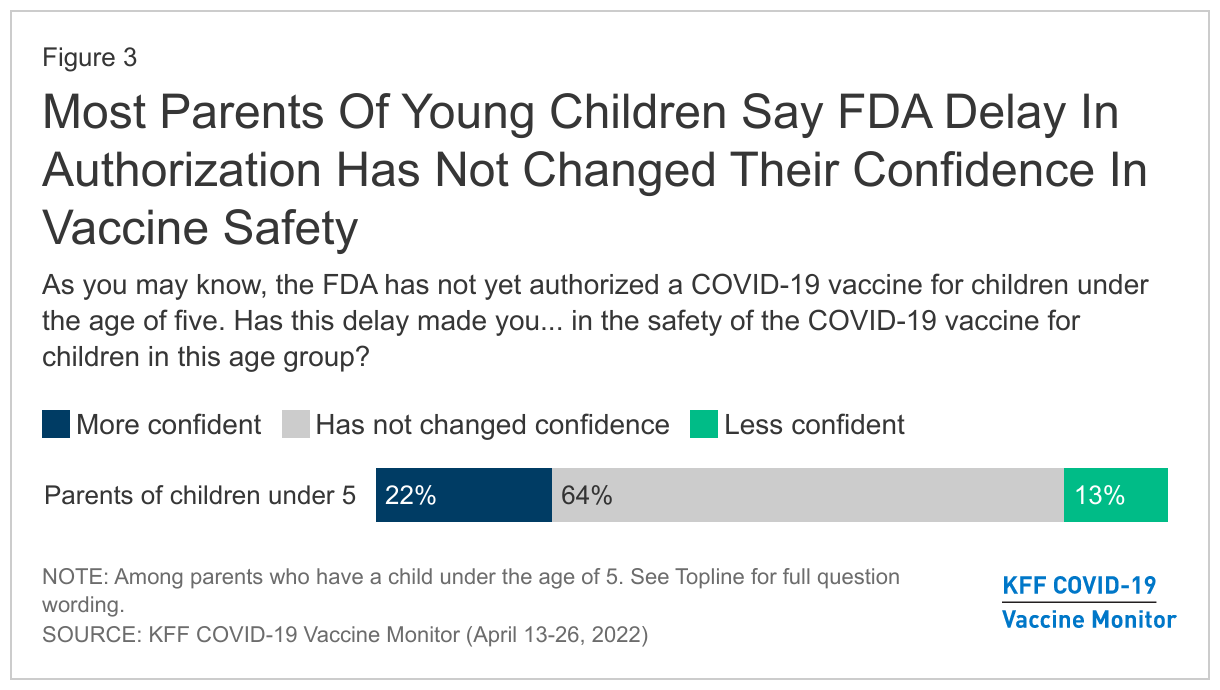
Moderna’s application for emergency use authorization for its COVID-19 vaccine in young children comes on the heels of a previous delay by the FDA, which announced in February that it was waiting for more data on the effectiveness of a third dose before evaluating the Pfizer-BioNTech vaccine for this age group. Most parents of young children (64%) say the FDA’s delay in granting emergency use authorization for a COVID-19 vaccine for children under five has not affected their confidence in the safety of the vaccines for this age group. About one-fifth (22%) parents say the delay has made them “more confident” in the vaccine’s safety for young children, while around one in eight (13%) say it has made them “less confident.”
COVID-19 And The Workplace
As many employees are returning to their offices or workplaces, and COVID-19 restrictions such as mask requirements are being lifted from restaurants, retail stores, and other venues, most workers say they feel at least somewhat safe from COVID-19 in their workplace. However, Black and Hispanic workers as well as those with lower incomes are less likely than their counterparts to report feeling “very safe” when they go to work.
Most workers with jobs outside the home say they feel at least somewhat safe from COVID-19 when they are at work, including over half who say they feel “very safe” (55%) and a third who feel “somewhat safe.” Around one in ten say they feel “not too safe” (9%) or “not safe at all” (4%).
White workers are twice as likely as Black workers to say they feel “very safe” from COVID-19 when working outside the home (63% vs. 31%), with smaller shares of Hispanic workers (48%) than White workers saying they feel “very safe.” Across income groups, a majority of those with household incomes of $40,000 or more say they feel “very safe” (57%) compared to about four in ten (41%) of those with incomes of under $40,000 who say the same. Unvaccinated workers also report feeling “very safe” at work outside their house (71%) at higher rates than vaccinated workers (48%), likely due to difference in perceptions of COVID-19 as a risk.
Vaccine Mandates In The Workplace
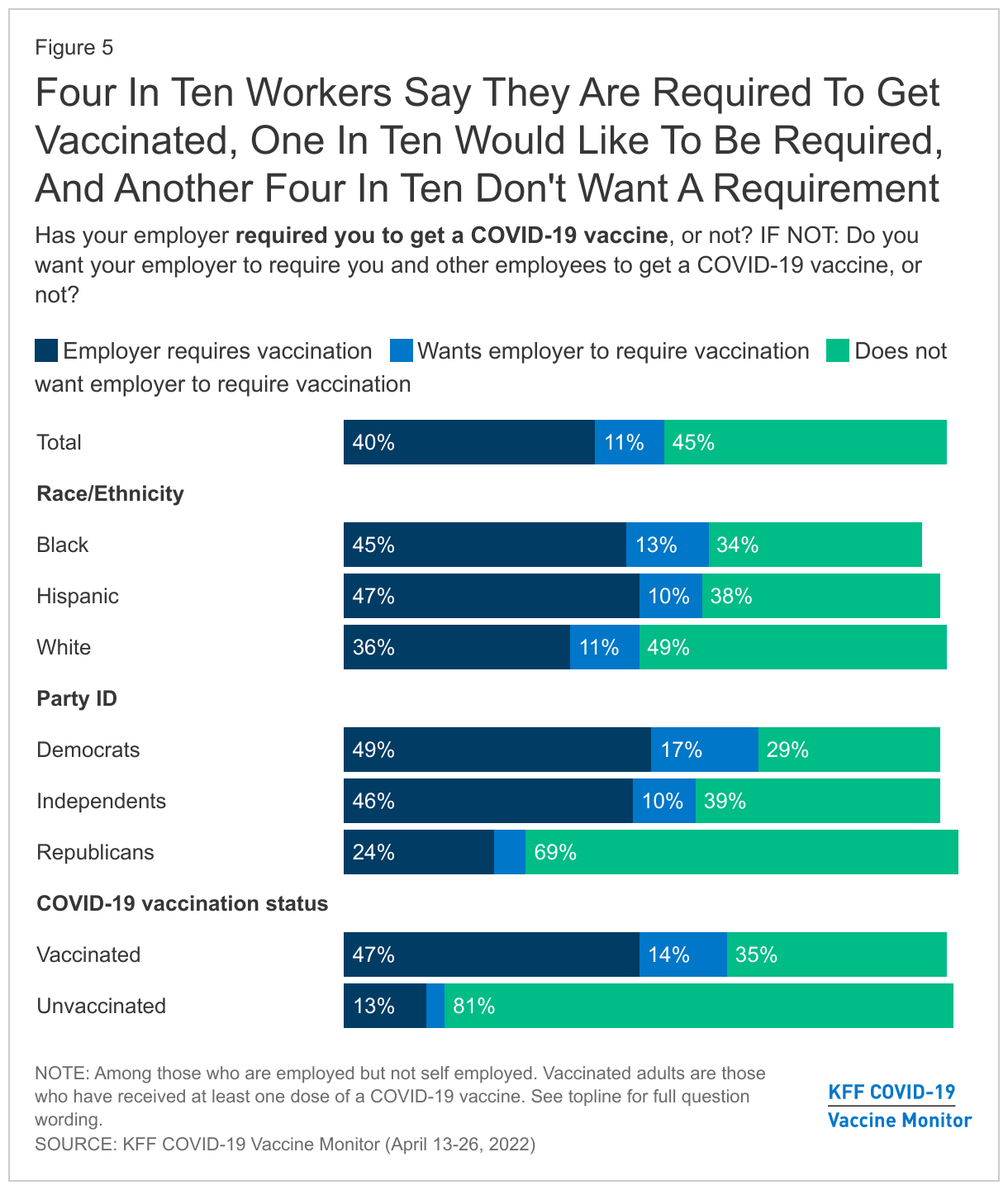
In January, following the Supreme Court’s ruling that blocked the policy, the Biden Administration withdrew its requirement for large employers to have workers get vaccinated for COVID-19 or be tested regularly. However, some workplaces have continued to mandate vaccines in the absence of federal policy. We find that four in ten workers say their employer is requiring on-site workers to be vaccinated for COVID-19, up from 29% in November 2021. This includes 9% of all workers who say their employer is requiring employees to have a COVID-19 booster in addition to their initial dose.
Among workers whose employer does not require on-site workers to be vaccinated for COVID-19, most (78%, or 45% of all workers) say they do not want their employer to have a vaccination requirement, while 20% of those without a requirement (11% of all workers) say they want their employer to require vaccination.
Majorities Black workers and Hispanic workers say they either have a vaccination requirement at work (45% of Black workers, 47% of Hispanic workers) or want their employer to add one (13% of Black workers, 10% of Hispanic workers), while around half of White employees (49%) don’t currently have a vaccine requirement and do not want a requirement. Among partisans, about two-thirds of Democrats and over half of independents either say their employer requires vaccines or they want their employer to require vaccines, while about seven in ten Republicans (69%) say they are not currently subject to such a requirement and do not want their employer to put one in place.
Mask Usage In The Workplace
With mask mandates being lifted in many places, most workers say they and their coworkers are not regularly wearing masks at work. About one-quarter (24%) of those who work at least partially outside their home say they have worn a mask “every time” when indoors at work in the past 30 days, with another 14% reporting they wore a mask most of the time. About one in five workers (19%) say they wore a mask “some of the time” when indoors at work in the past 30 days, while 43% say they have “never” worn a mask indoors at work in the past 30 days. Three in ten say “all” or “most” of their coworkers regularly wear masks at work while 16% say some of their coworkers regularly wear a mask. About half of employees say “very few” (27%) or “none” (26%) of their coworkers regularly wear a mask at work.
Black workers and Hispanic workers, as well as workers with lower incomes, are more likely than others to say they and their coworkers are regularly wearing masks at work. For example, workers with household incomes of $40,000 or less are more than twice as likely as those with incomes of $90,000 or more to say they mostly wear masks at work (61% vs. 27%) and to say that most of their coworkers do (50% vs. 22%). Further, nearly two-thirds of Black workers (64%) and half of Hispanic workers (52%) say they wear a mask at work at least most of the time compared to three in ten White employees (31%).
There are partisan differences as well, with workers who identify as Democrats more than three times as likely as those who identify as Republicans to report wearing a mask at work (51% vs. 16%). And despite being at a higher risk for catching and spreading the virus, a smaller share of unvaccinated than vaccinated adults report regularly wearing a mask in the workplace (20% vs. 45%) or say most of their coworkers wear one (17% vs. 34%).
COVID-19 And Schools
Though COVID-19 cases are again on the rise and some schools are reporting outbreaks among students and staff following spring break, most parents feel their children are at least “somewhat safe” from COVID-19 at school, and most feel their school is “doing about the right amount” to keep children safe.
Nearly half of parents with a child in school think their child is “very safe” (44%) from the risk of exposure to COVID-19 when they are at school and an additional 40% think their child is “somewhat safe”. However, parents who are Black or Hispanic are less likely than White parents to say they feel their child is “very safe” from COVID-19 when they are at school1 . Similarly, vaccinated parents are much less likely than unvaccinated parents to say they think their child is “very safe” (36% vs. 59%).
Additionally, seven in ten parents with a child enrolled in school say their child’s school is doing “about the right amount” to protect kids from COVID-19 at school. One in ten (11%) say their child’s school is doing “too much” while 18% feel their child’s school is “not doing enough” to protect kids from COVID-19 at school. There were no measured differences on how Black, Hispanic, and White parents assessed the job their child's school is doing.
The February KFF Vaccine Monitor, following the peak of an omicron wave of COVID-19 cases, found that parents were largely divided on whether schools should have mask requirements for students and staff. The current Monitor finds that there has been a large shift in mask requirements in schools since the beginning of the school year. Three-quarters of parents now say they their child’s school does not have a mask requirement, compared to September 2021 when seven in ten parents (69%) said their child’s school required all students and staff to wear masks.
About four in ten parents (41%) indicate their child regularly wears a mask at school – either because their school requires it or because it is something they do voluntarily. One in four (24%) say that all or most students in their child’s school are either subject to a mask requirement or wear masks regularly. Parents who are Black or Hispanic are more than twice as likely as White parents to say their child usually wears a mask (70% vs. 26%) and five times as likely to say that most other students at their child’s school wear masks (9% vs. 47%).
Trends In COVID-19 Vaccination Intentions And Uptake
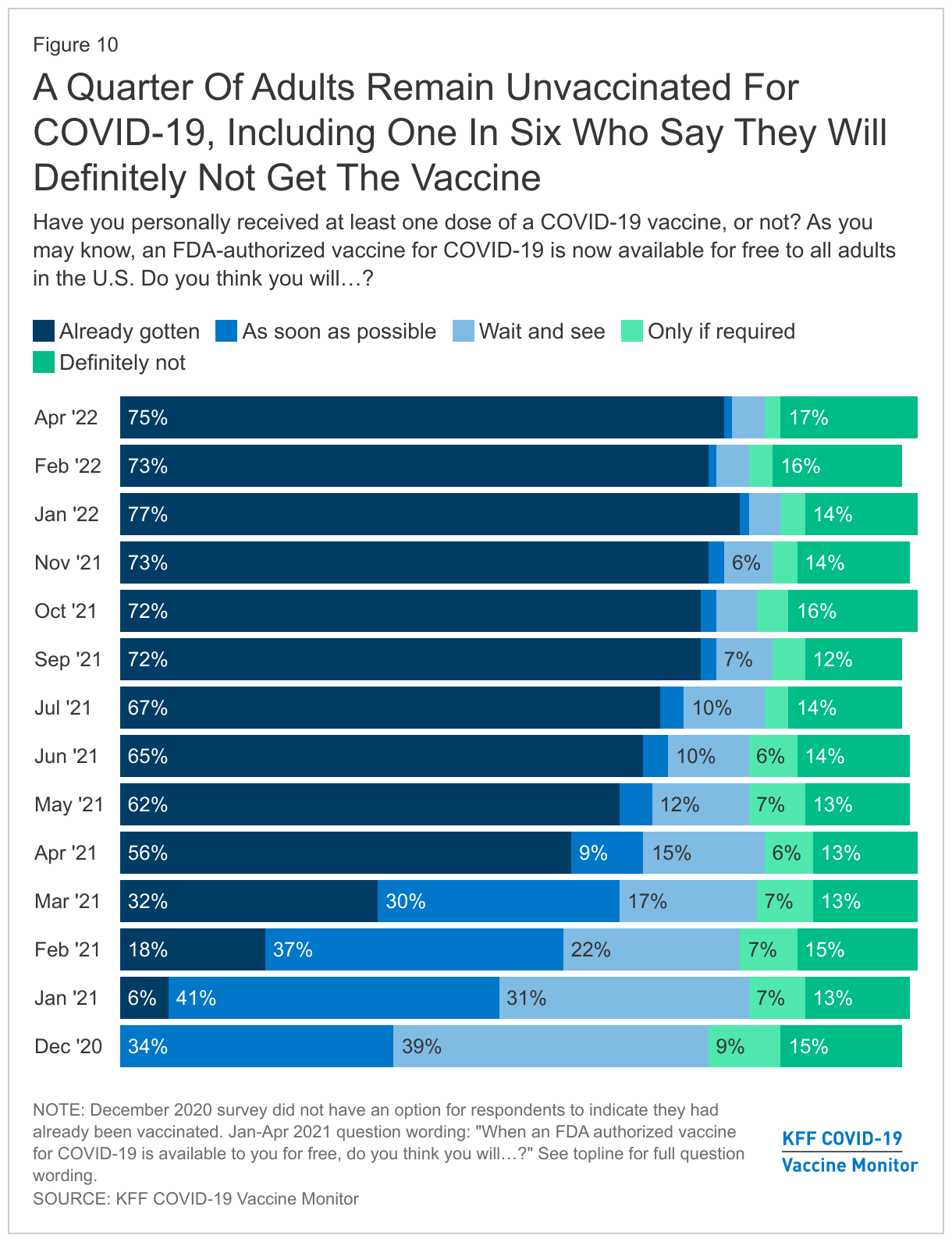
The latest KFF COVID-19 Vaccine Monitor survey finds that three in four adults (75%) say they have gotten at least one dose of a COVID-19 vaccine, a share that continues to hold relatively steady since September 2021. A quarter of adults remain unvaccinated, including about one in six (17%) who say they definitely will not get the vaccine, a share that has not changed substantially in nearly 18 months of polling.
When it comes to demographic uptake of the COVID-19 vaccine, Democrats (92%), adults 65 and older (88%), college graduates (86%), and those with a serious health condition (85%) continue to report the highest rates of being vaccinated. Republicans (55%), those under age 65 without health insurance (56%), and White Evangelical Christians (57%) are among those with the lowest vaccination rates.
Booster Doses Uptake And Intentions
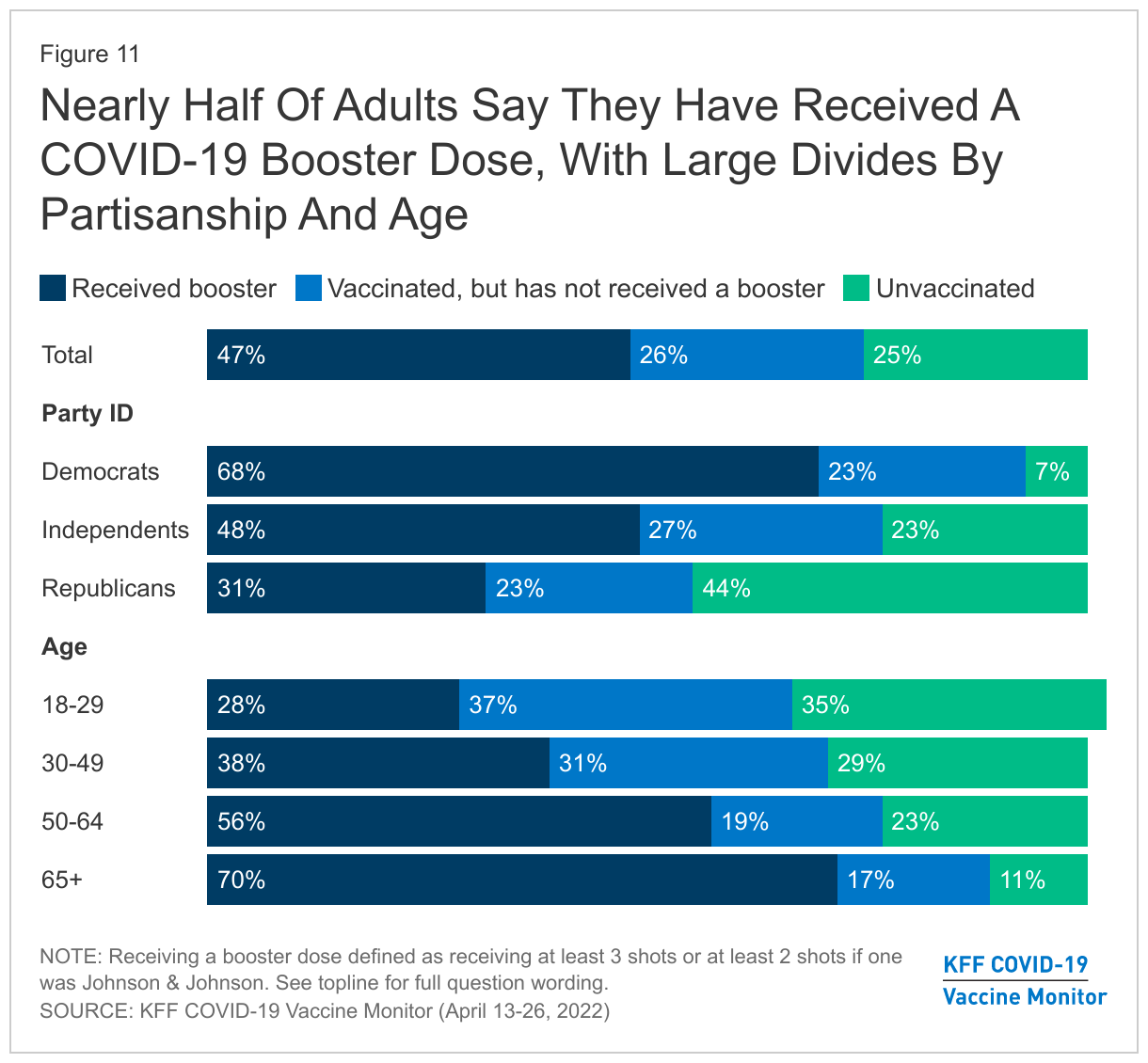
COVID-19 vaccine booster uptake has also slowed considerably2 . About half of all adults (47%) now report they have received a booster dose, the same share who said so in February. One in four adults (26%) report being vaccinated for COVID-19 but have not gotten a booster, while a quarter (25%) say they are unvaccinated. Booster uptake differs substantially by age, with the highest rate of being boosted among adults 65 and older, who are more at risk for COVID-19 complications (70%). There is also a large gap by partisanship, with Democrats more than twice as likely as Republicans to report being vaccinated and boosted (68% vs. 31%).
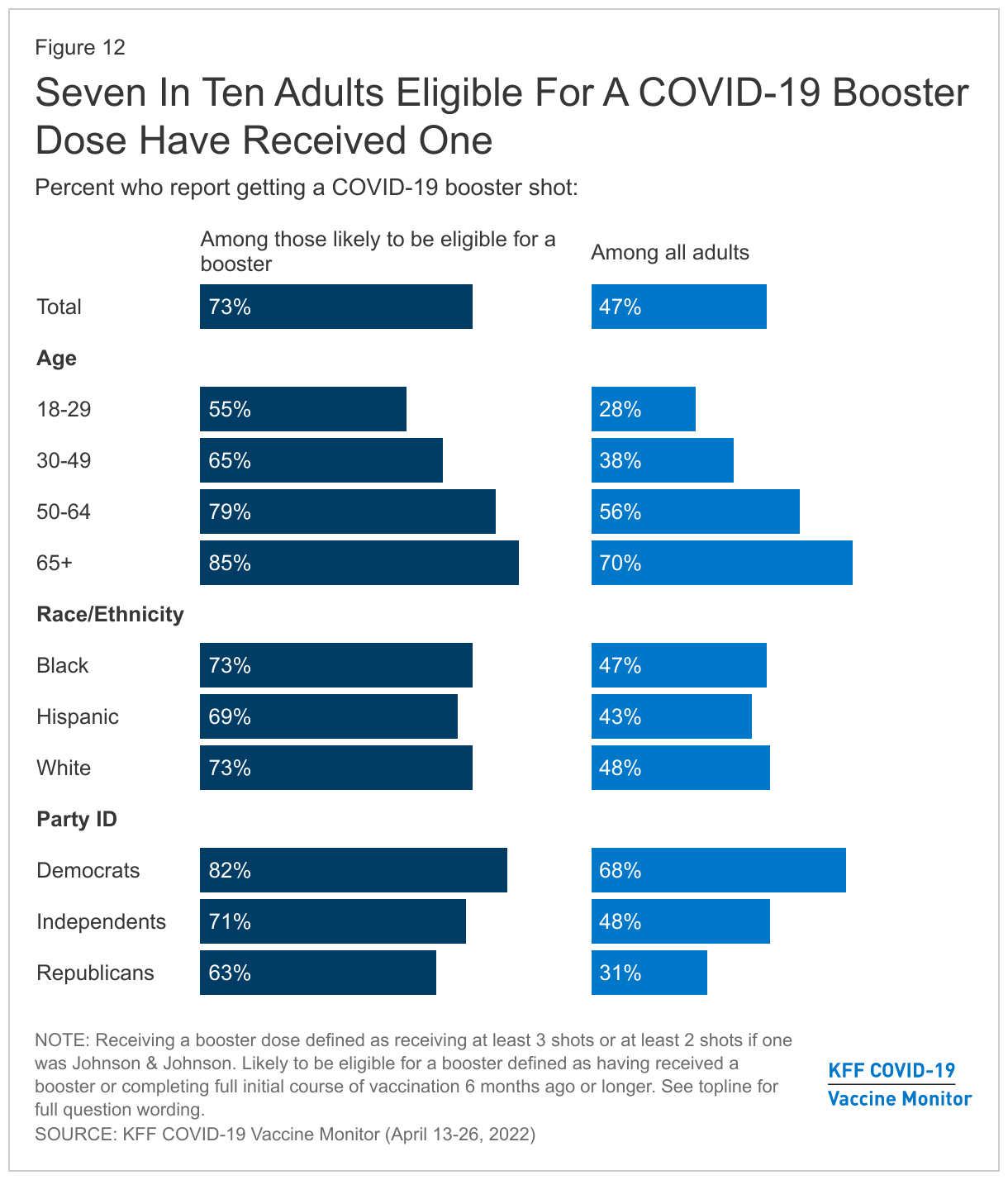
Previous Vaccine Monitor surveys identified a potential racial gap in COVID-19 booster uptake, with White adults appearing to outpace Black and Hispanic adults in the share who reported being boosted. The latest survey finds that similar shares of Black, Hispanic, and White adults now report receiving a booster, whether looked at as a share of the total population or among those likely to be eligible for a booster.
Notably, though younger adults continue to lag older adults and Republicans lag Democrats in the share who say they have gotten a booster dose of a COVID-19 vaccine, among those likely eligible for a booster, majorities across age groups, racial and ethnic groups, and party identification say they have received a booster dose.
Among vaccinated adults who have not yet received a booster dose, half say they will only get it “if required” (27%) or say they will “definitely not” get a booster (23%). Three in ten (30%) say they plan to get an additional dose “as soon as they can,” while 18% say they want to “wait to see” before getting a booster dose of the COVID-19 Vaccine. Four in ten vaccinated Hispanic adults who have not yet gotten a booster say they want to get one “as soon as they can”, compared to 22% of vaccinated but not yet boosted White adults who say the same. Around three in ten (29%) vaccinated but not yet boosted Black adults say they’ll get a booster dose as soon as they can. Notably, about three in ten vaccinated White adults who are not yet boosted say they will “definitely not” get a booster dose (29%) and a further 29% say they will only do so if they are required.
Reasons Why Some Vaccinated Adults Have Not Gotten A Booster
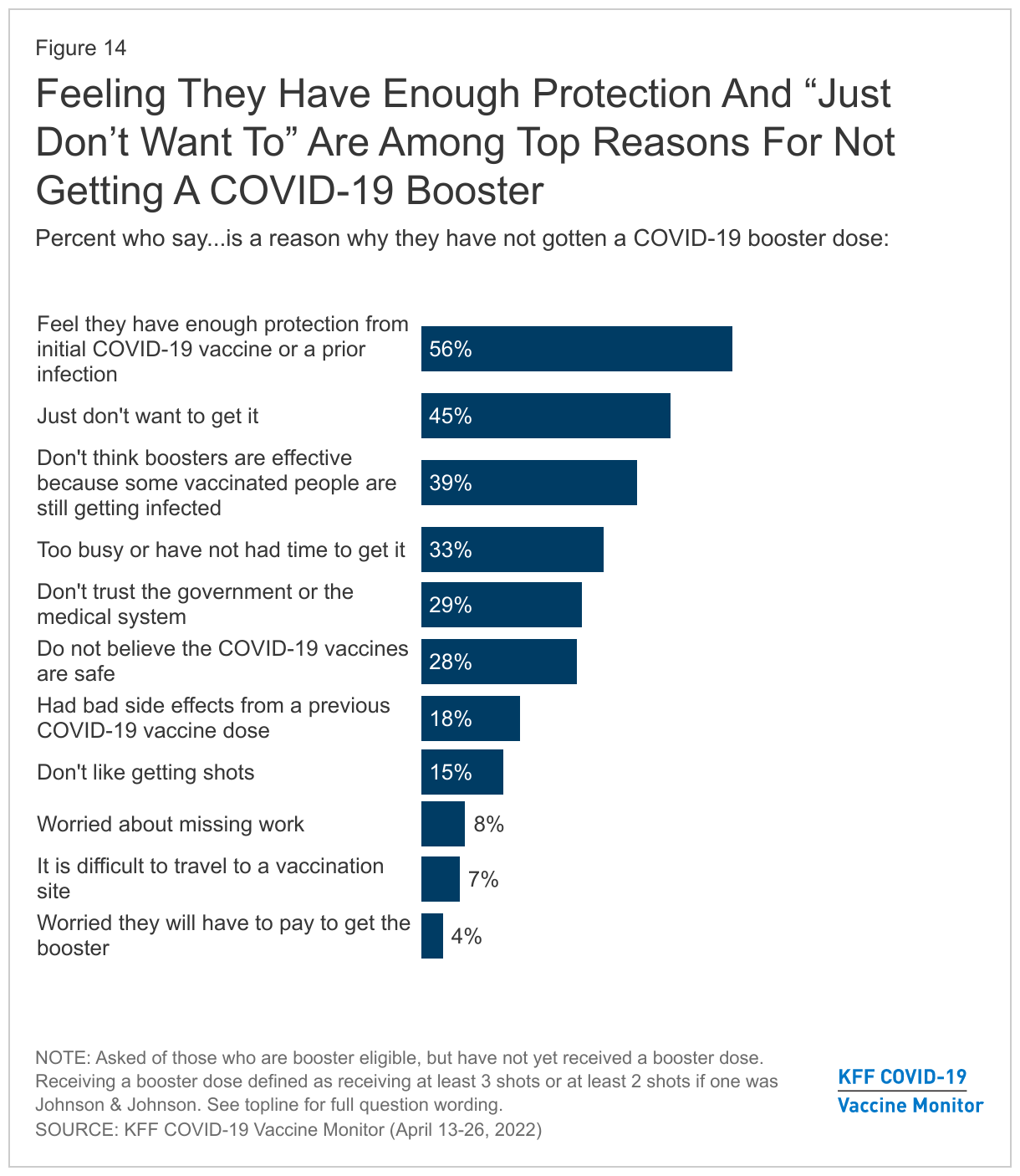
Adults who are eligible for a COVID-19 booster but have not yet received one cite a variety of reasons for not getting a booster. Chief among them is the view that they already have enough protection from either their initial vaccine doses or from a previous COVID-19 infection (56%). Other common reasons these booster-eligible adults say they have not yet gotten a booster include just not wanting to get it (45%), thinking boosters are ineffective because some vaccinated people are still getting infected (39%), and being too busy to go get the shot (33%). About three in ten cite not trusting the government or medical system (29%) or not believing the COVID-19 vaccines are safe (28%) as reasons for not getting a booster. Fewer cite other reasons like side effects from a previous dose (18%), they don’t like getting shots (15%), worries about missing work (8%), difficulties traveling to a vaccination site (7%), or worries about having to pay out of pocket (4%).
Perceptions Of Current Case Rates And Preparation For Future Waves
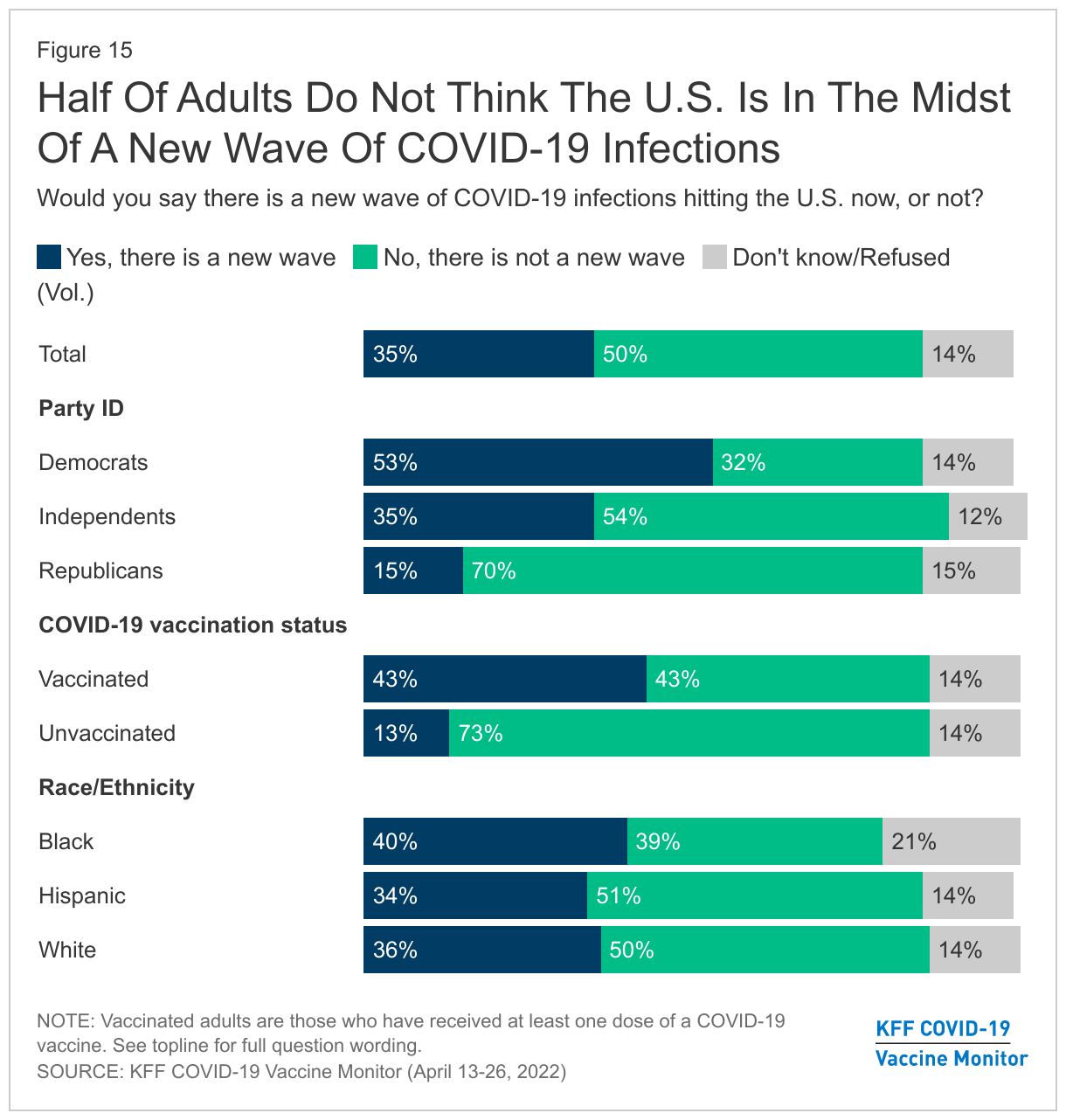
As COVID-19 cases are once again on the rise, a little more than a third (35%) of adults think there is a new wave of COVID-19 infections hitting the country. Half of adults say there is not a new wave of COVID-19 infections hitting the U.S. now and 14% are unsure if the country is in the midst of a new wave.
There are stark differences in partisan perceptions of the current state of COVID-19 infections as a slight majority of Democrats (53%) think that there is a new wave right now in the U.S., while seven in ten Republicans think there is not. Notably, almost three-quarters of unvaccinated adults (73%) do not think there is a new wave of COVID-19 infections in the U.S., consistent with prior surveys finding that unvaccinated adults tend to view the virus as less of a risk compared to those who are vaccinated.
People’s perceptions about whether the country is experiencing a new wave of COVID-19 infections seem to reflect their view of what is happening among their own family and friends. Around six in ten adults say that among the people they know, they have seen fewer COVID-19 cases in the past 30 days (62%) while two in ten say they have seen about the same number of cases (21%). Fewer than one in ten (6%) say they have seen more cases in the past 30 days among people they know. Additionally, around half of adults (51%) say that the people they know who have been infected with COVID-19 in the past 30 days are experiencing less severe symptoms than those infected in previous waves.
Preparedness For Future COVID-19 Waves
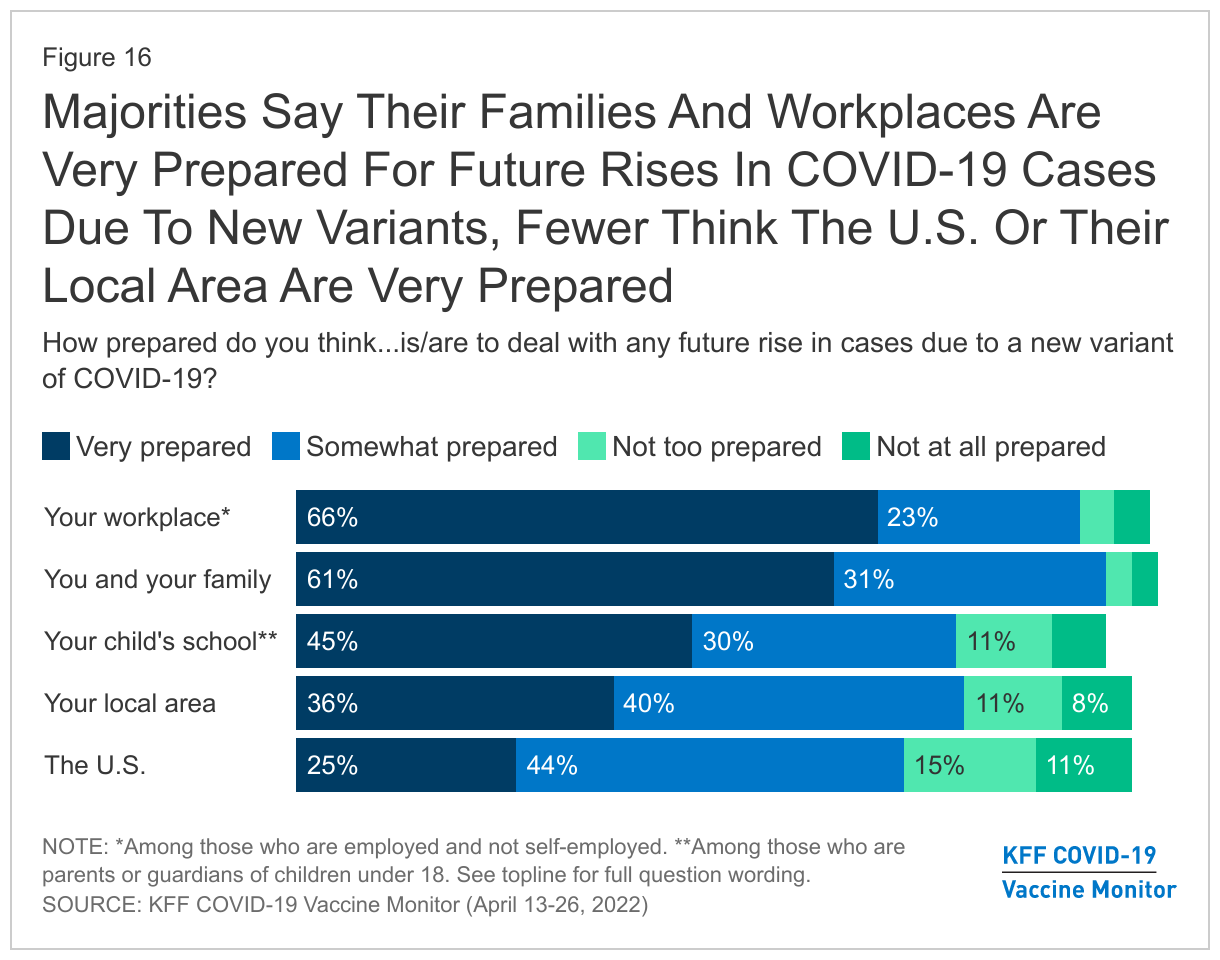
With a new omicron subvariant continuing to spread, six in ten adults (61%) say that they and their families are very prepared for any future rise of cases due to a new variant, and around two-thirds of employed adults say their workplace is very prepared (66%). Slightly less than half of parents (45%) say their child’s school is very prepared for a rise in COVID-19 cases due to new variants. However, around a third report that their local area more generally is very prepared for a rise in COVID-19 cases (36%).
In contrast to views of their personal level of preparation, fewer adults think the U.S. as a country is very prepared to deal with any future rise in cases due to a new variant of COVID-19. A quarter of adults say that the U.S. is very prepared to deal with any future rise in cases due to a new variant (25%), with 44% saying the country is somewhat prepared, and a quarter saying it is not too prepared (15%) or not prepared at all (11%).
Black and Hispanic adults and those with lower household incomes are less likely to say that they, their family, and their workplace are very prepared to deal with future COVID-19 cases. A larger share of White adults says they and their family are very prepared with any future rise in cases (65%) compared to Black (52%) and Hispanic adults (46%). In addition, larger shares of those with higher incomes say they and their family are very prepared (72% of those with a household income of $90,000 or more a year, compared to 55% of those with an income of less than $90,000). Similarly, White workers are more likely to say their workplace is very prepared (71%) than Black (48%) or Hispanic workers (56%).
Trust In COVID-19 Vaccine Information
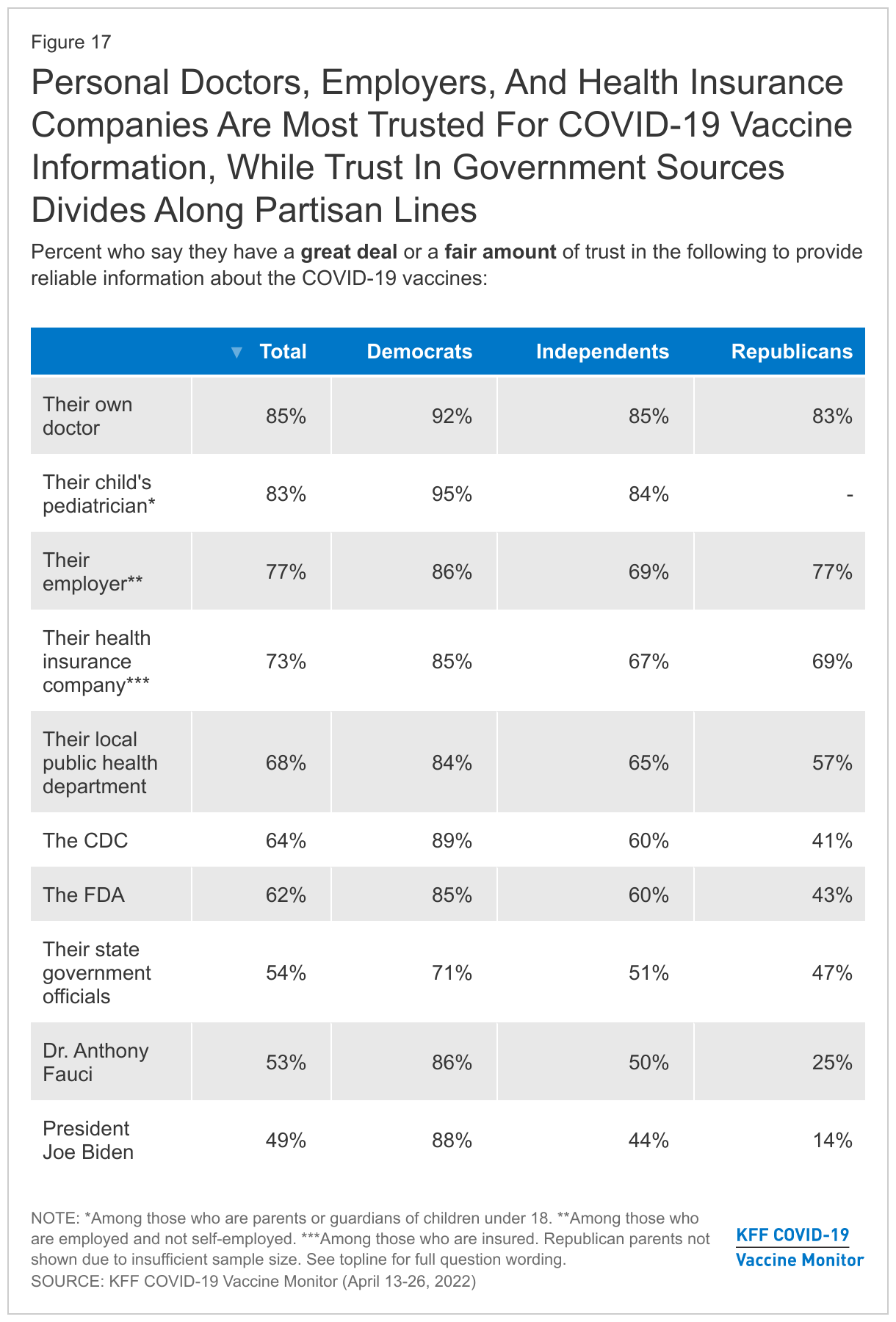
When asked who people trust to provide reliable information about the COVID-19 vaccines, people’s own doctors, including pediatricians top the list, with 85% of adults saying they trust their personal doctor “a great deal” or “a fair amount.” Similarly, 83% of parents say they trust their child’s pediatrician to provide them with reliable information about the COVID-19 vaccines. Majorities of workers trust their employer (77%), insured adults trust their health insurance company (73%), and majorities trust their local public health department (68%) for this information. About two-thirds trust COVID-19 vaccine information from the CDC (64%) or the FDA (62%) and about half of adults trust their state government officials (54%), Dr. Anthony Fauci (53%), and President Joe Biden (49%).
With the exception of their own employers, there are stark partisan differences in trust with Republicans being less likely than Democrats to trust each of the other sources of COVID-19 vaccine information asked about in the survey. Indeed, Republicans are particularly less likely than their Democratic counterparts to trust federal and institutional sources of information.
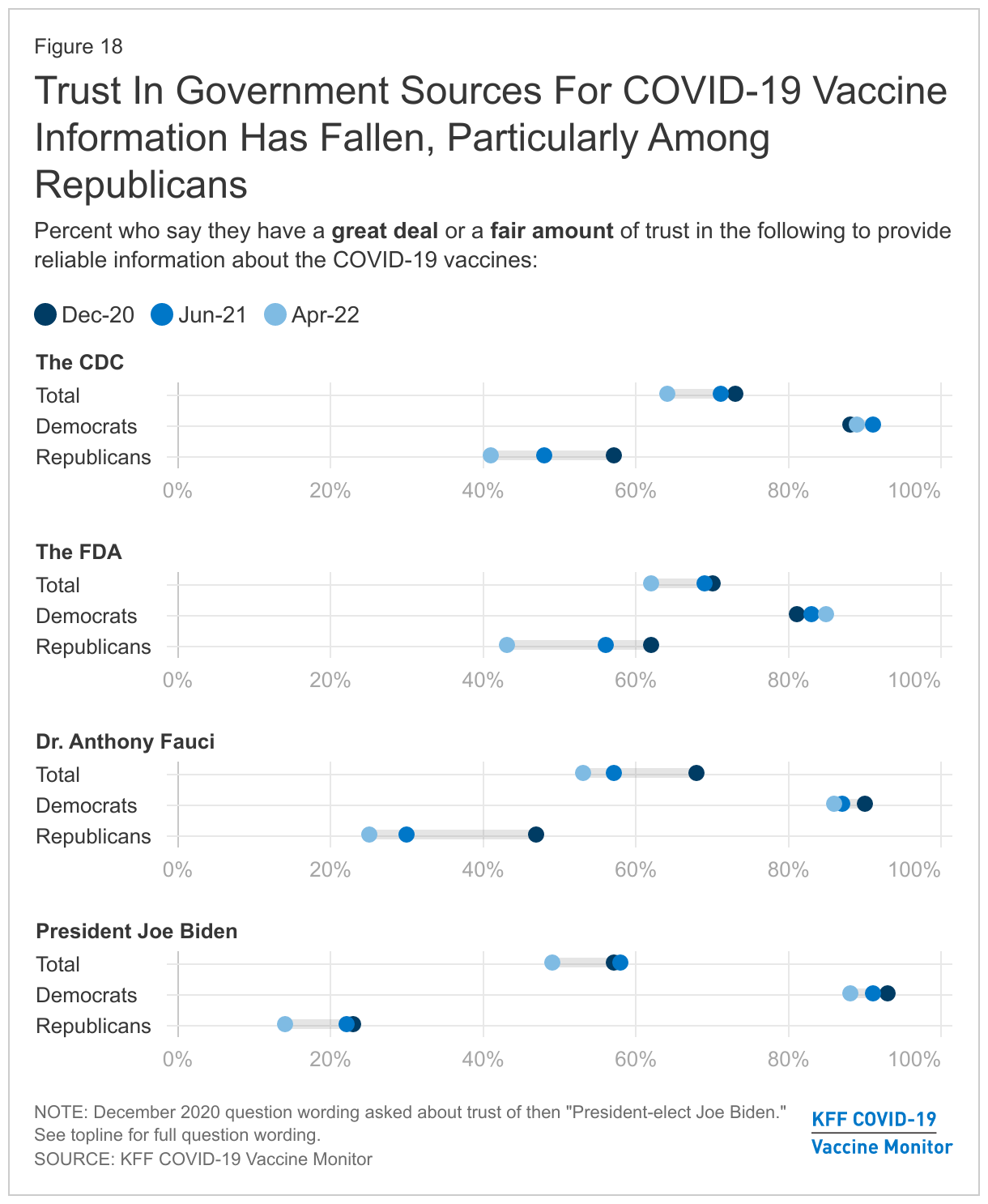
The share who says they trust President Biden, the FDA, the CDC, and Dr. Fauci to provide reliable information on COVID-19 vaccines has declined since December 2020. Despite some criticism of how the FDA and CDC have handled vaccine rollout and messaging, trust among Democrats has remained high. However, among Republicans, the share who say they trust the FDA fell from a majority (62%) to about four in ten (43%). Similarly, the share of Republicans who trust the CDC at least a fair amount fell from a majority in December (57%) to four in ten (41%). The share of Republicans who trust Dr. Fauci for such information fell by roughly half between December 2020 and now, from 47% to 25%. In addition, trust in President Biden, already low among Republicans in December when he was President-elect, sank even further.
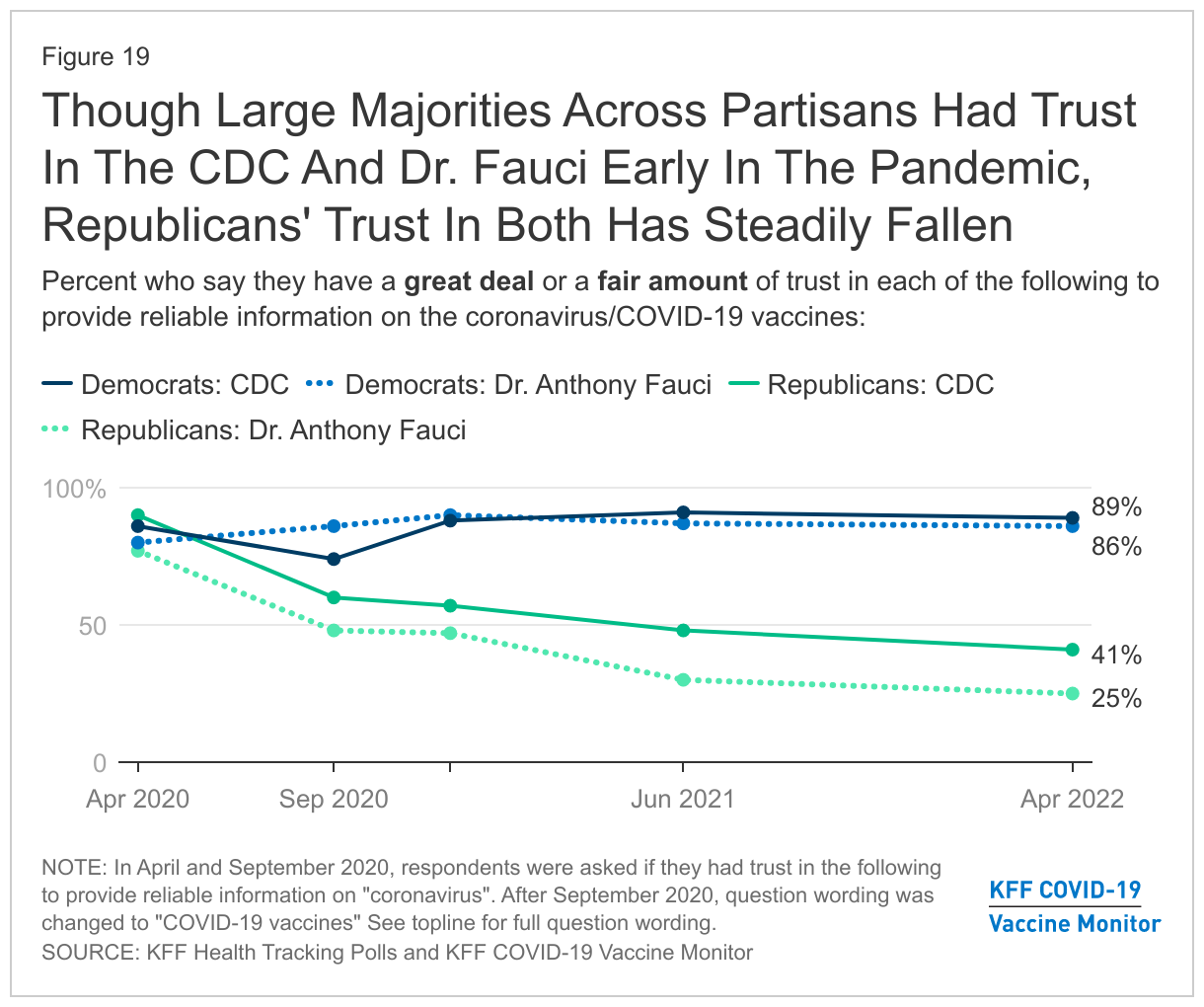
The recent downward movement in Republicans’ level of trust in the CDC and Dr. Fauci on coronavirus is a continuation of a trend that began earlier in the pandemic. In April 2020, under a different Administration, large shares of both Democrats and Republicans said they had at least a fair amount of trust in the CDC and in Dr. Anthony Fauci to provide reliable information about coronavirus in general. By September 2020, the shares of Republicans who said they trusted both fell by more than 25 percentage points each. This trend has continued as the question shifted to ask about sources of information on COVID-19 vaccines.
Methodology
This KFF COVID-19 Vaccine Monitor was designed and analyzed by public opinion researchers at the Kaiser Family Foundation (KFF). The survey was conducted April 13-26, 2022, among a nationally representative random digit dial telephone sample of 1,889 adults ages 18 and older (including interviews with 501 Hispanic adults and 500 non-Hispanic Black adults), living in the United States, including Alaska and Hawaii (note: persons without a telephone could not be included in the random selection process). Phone numbers used for this study were randomly generated from cell phone and landline sampling frames, with an overlapping frame design, and disproportionate stratification aimed at reaching Hispanic and non-Hispanic Black respondents as well as those living in areas with high rates of COVID-19 vaccine hesitancy. Stratification was based on incidence of the race/ethnicity subgroups and vaccine hesitancy within each frame. High hesitancy was defined as living in the top 25% of counties as far as the share of the population not intending to get vaccinated based on the U.S. Census Bureau’s Household Pulse Survey. The sample also included 115 respondents reached by calling back respondents that had previously completed an interview on the KFF Tracking poll at least nine months ago. Another 286 interviews were completed with respondents who had previously completed an interview on the SSRS Omnibus poll (and other RDD polls) and identified as Hispanic (n=122; including 51 in Spanish) or non-Hispanic Black (n=164). Computer-assisted telephone interviews conducted by landline (212) and cell phone (1,677; including 1,272 who had no landline telephone) were carried out in English and Spanish by SSRS of Glen Mills, PA. To efficiently obtain a sample of lower-income and non-White respondents, the sample also included an oversample of prepaid (pay-as-you-go) telephone numbers (25% of the cell phone sample consisted of prepaid numbers). Both the random digit dial landline and cell phone samples were provided by Marketing Systems Group (MSG). For the landline sample, respondents were selected by asking for the youngest adult male or female currently at home based on a random rotation. If no one of that gender was available, interviewers asked to speak with the youngest adult of the opposite gender. For the cell phone sample, interviews were conducted with the adult who answered the phone. KFF paid for all costs associated with the survey.
The combined landline and cell phone sample was weighted to balance the sample demographics to match estimates for the national population using data from the March 2021 U.S. Current Population Survey (CPS) on sex, age, education, race, Hispanic origin, region, and marital status, within race-groups, along with data from the 2010 Census on population density. The sample was also weighted to match current patterns of telephone use using data from the January-June 2021 National Health Interview Survey. The sample is also weighted to account for the possibility of partisan nonresponse based on three months of KFF national polls and this current survey. The weight takes into account the fact that respondents with both a landline and cell phone have a higher probability of selection in the combined sample and also adjusts for the household size for the landline sample, and design modifications, namely, the oversampling of potentially undocumented respondents and of prepaid cell phone numbers, as well as the likelihood of non-response for the recontacted sample. All statistical tests of significance account for the effect of weighting.
The margin of sampling error including the design effect for the full sample is plus or minus 3 percentage points. Numbers of respondents and margins of sampling error for key subgroups are shown in the table below. For results based on other subgroups, the margin of sampling error may be higher. Sample sizes and margins of sampling error for other subgroups are available by request. Sampling error is only one of many potential sources of error and there may be other unmeasured error in this or any other public opinion poll. Kaiser Family Foundation public opinion and survey research is a charter member of the Transparency Initiative of the American Association for Public Opinion Research.
This work was supported in part by grants from the Chan Zuckerberg Initiative DAF (an advised fund of Silicon Valley Community Foundation), the Ford Foundation, and the Molina Family Foundation. We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
Group
N (unweighted)
M.O.S.E.
Total
1,889
± 3 percentage points
COVID-19 vaccination status
Have gotten at least one dose of the COVID-19 vaccine
1,449
± 4 percentage points
Have not gotten the COVID-19 vaccine
429
± 7 percentage points
Race/Ethnicity
White, non-Hispanic
754
± 5 percentage points
Black, non-Hispanic
500
± 6 percentage points
Hispanic
501
± 5 percentage points
Parents
Total parents
477
± 7 percentage points
Parent with a child under age 5
181
± 11 percentage points
Parents with a child ages 5-11
227
± 10 percentage points
Parents with a child ages 12-17
230
± 9 percentage points
Party identification
Democrats
650
± 6 percentage points
Republicans
349
± 7 percentage points
Independents
577
± 6 percentage points
Notes for reading the topline:
Percentages may not always add up to 100 percent due to rounding.
Values less than 0.5 percent are indicated by an asterisk (*).
“Vol.” indicates a response was volunteered by the respondent, not offered as an explicit choice
Questions are presented in the order asked; question numbers may not be sequential.
All trends shown in this document come from KFF Health Tracking Polls or KFF COVID-19 Vaccine Monitors.
Endnotes
Black and Hispanic parents were combined for analysis as separate sample sizes were too small for individual analysis. ↩︎
Booster dose is in reference to the first booster dose after a full initial course of vaccination (3rd shot for those receiving the initial course of the Pfizer or Moderna vaccine, or 2nd shot for those receiving the Johnson & Johnson vaccine). This survey was fielded after the CDC announced eligibility for a second booster dose for some individuals but did not measure uptake of a second booster. ↩︎
In a new brief, KFF analysts explain and summarize the recent history of efforts to make work requirements a condition of eligibility for Medicaid in some states. Following years of administrative, political, and legal activity across two presidential administrations, recent Supreme Court action and skepticism about work requirements by the Biden administration signals a pause in efforts to reshape state Medicaid programs in this fashion.
The Trump Administration opened the door to such efforts by approving Section 1115 demonstration waivers that imposed mandatory work and reporting requirements as a condition of Medicaid eligibility. However, courts struck down many of these approvals. And the Supreme Court recently dismissed pending challenges in these cases, in part due to the Biden Administration’s earlier withdrawals of approved work requirement waivers in several states. Georgia has challenged the withdrawal of its work requirements in court, and an initial decision in the Georgia case is still pending.
Although few Medicaid work and reporting requirements were implemented due to litigation, state withdrawals, and/or pauses during the COVID-19 pandemic, KFF analysts find that available implementation data from Arkansas suggests that these requirements are confusing to enrollees and result in substantial Medicaid coverage losses, including among eligible individuals.
Future presidential administrations could revisit these waiver provisions. However, to survive legal challenges, the federal administrative record in any future approvals would likely have to support the conclusion that such waivers would further Medicaid program objectives, including promoting affordable health coverage for low-income people, our experts conclude.
The full analysis, and other data and analyses about Medicaid work requirements, are available on the Medicaid topic page of kff.org.
The Trump Administration aimed to reshape the Medicaid program by newly approving Section 1115 demonstration waivers that imposed work and reporting requirements as a condition of Medicaid eligibility. However, courts struck down many of these approvals and the Supreme Court recently dismissed pending challenges in these cases. The Court dismissed pending litigation in Arkansas and New Hampshire due to the expiration of Arkansas’ waiver as well as the Biden Administration’s earlier withdrawals of these approved work requirement waivers. The Biden Administration had concluded that these provisions reduce coverage and thus do not promote the objectives of the Medicaid program. States could have appealed these withdrawal decisions to the HHS Departmental Appeals Board, and Georgia has challenged the withdrawal of its work requirements in court. An initial decision in the Georgia case is currently pending.
Although few Medicaid work and reporting requirements were implemented due to litigation, state withdrawals, and/or pauses during the COVID-19 pandemic, available implementation data from Arkansas suggests that these requirements were confusing to enrollees and result in substantial coverage loss, including among eligible individuals. This recent history of Medicaid work requirements illustrates the tensions between states, changing presidential administrations, and the courts. This issue brief answers key questions about these provisions:
What is the history of Medicaid and work requirements?
What do we know about the impacts of Medicaid work requirements?
What is the current status and future of Medicaid work requirements?
Although the Biden Administration has concluded that it does not believe work requirements further Medicaid program objectives, a future presidential administration could revisit these waiver provisions. To survive an expected legal challenge, the administrative record in any future approvals would likely have to support the conclusion that such waivers would further Medicaid program objectives, including promoting affordable coverage for low income people.
What is the history of Medicaid and work requirements?
Prior to the Trump Administration, no states had received waiver approvals to condition Medicaid coverage on work and reporting requirements, and legislative attempts to incorporate work requirements into Medicaid statute failed.Policy arguments for and against Medicaid work requirements are grounded in views about whether Medicaid is akin to a public assistance program, like Temporary Assistance for Needy Families (TANF), or one that provides health insurance, in line with the Affordable Care Act (ACA) expansion of the program as one of several routes to increasing access to affordable health care for uninsured Americans. Adults who receive TANF cash assistance generally are required to participate in work, as one of the express purposes of TANF enumerated in statute is to “end the dependence of needy parents on government benefits by promoting job preparation, work, and marriage.” In contrast, Congress has not identified work as an objective for the Medicaid program. The ACA aimed to make Medicaid available to low-income adults through its Medicaid expansion, regardless of whether a person also met categorical eligibility requirements such as being pregnant, a parent, senior, or person with a disability. After implementation of the ACA’s Medicaid expansion, the Obama Administration signaled it would not approve state waiver requests to require work as a condition of Medicaid eligibility, concluding in its denial of Arizona’s request that work requirements “could undermine access to care and do not support the objectives of the [Medicaid] program.” In an effort to reframe Medicaid to a program akin to “public assistance”, unsuccessful Republican attempts to repeal and replace the ACA in 2017 proposed allowing states to require work as a condition of Medicaid eligibility.
In ways other than work requirements, Medicaid supports employment by providing affordable health coverage as well as voluntary employment referral and/or work support programs in some states.Research shows that being in poor health is associated with increased risk of job loss, while access to affordable health insurance has a positive effect on the ability to obtain and maintain employment. Medicaid coverage helps low-wage workers get care that enables them to remain healthy enough to work; acrossstates enrollees report that this coverage helps them to manage chronic conditions and supports their ability to work jobs that may be physically demanding. While most Medicaid adults who qualify through non-disability pathways are already working, some states have launched initiatives to support employment for Medicaid enrollees without making employment a condition of eligibility. A couple of states (including AR and IN) have offered voluntary employment referral programs relying on general enrollee notices rather than targeted outreach. Other states (including LA, ME, and MT) have incorporated intensive targeted outreach and case management services into their voluntary work support programs.
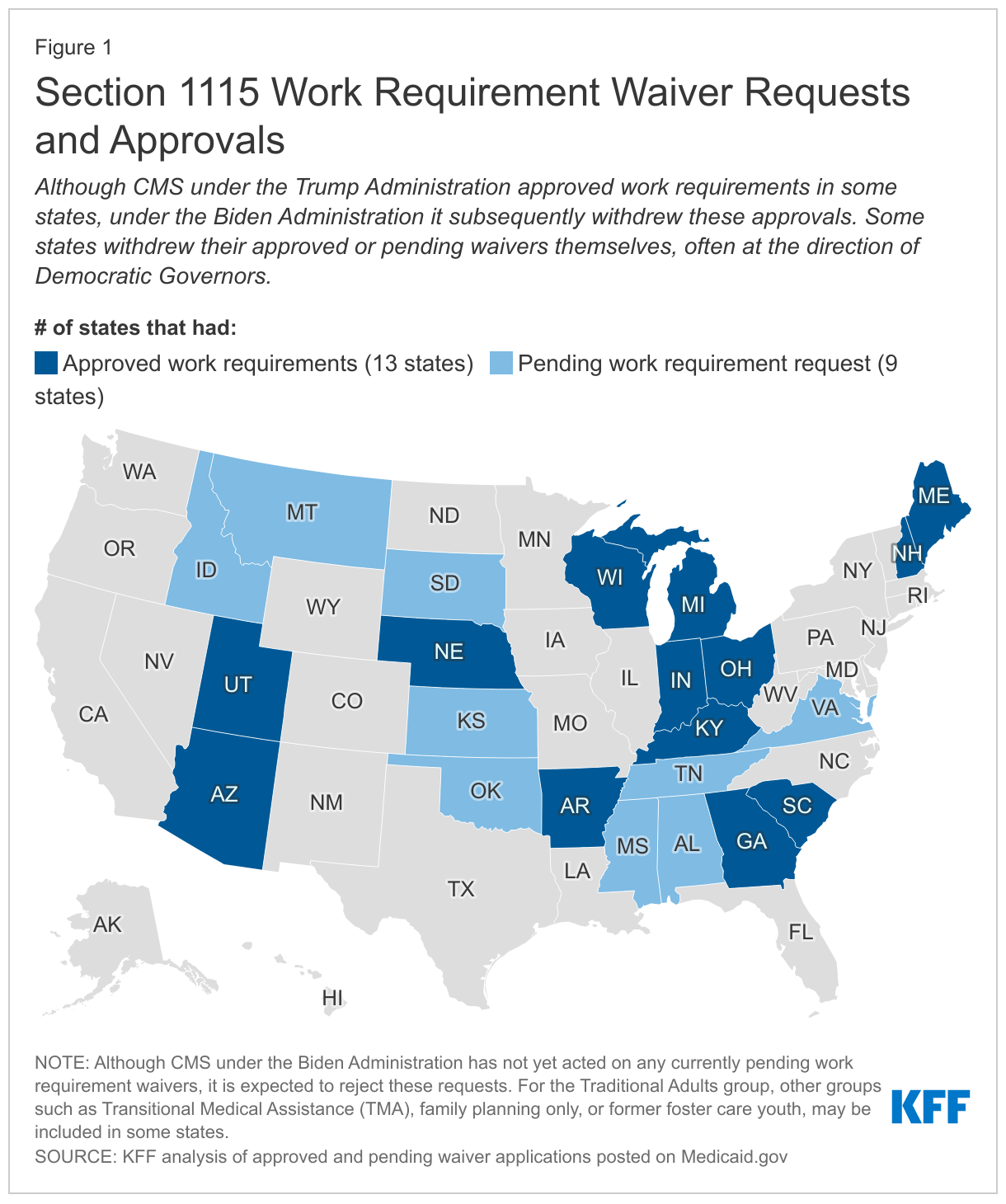
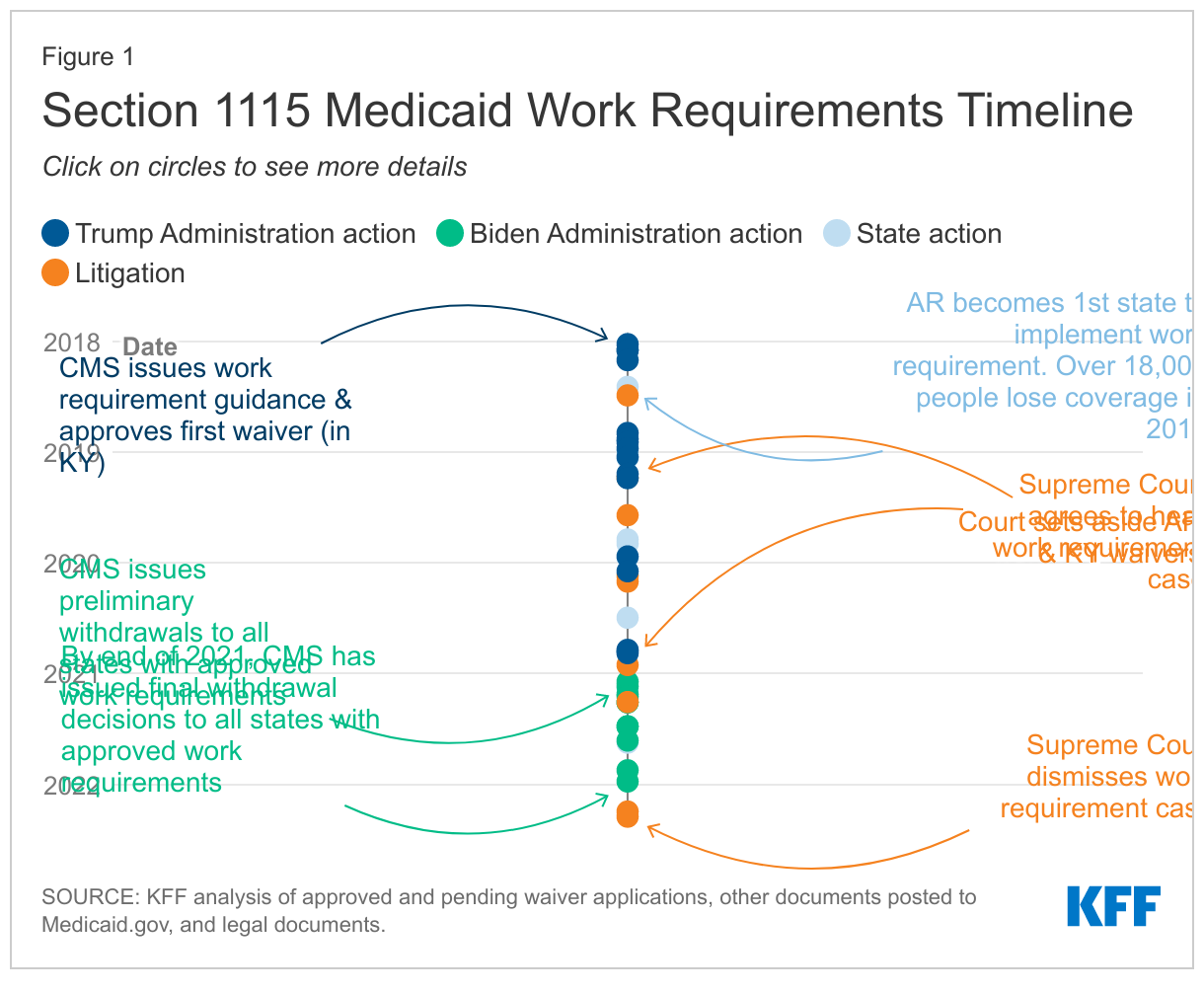
In a departure from previous administrations, the Trump Administration encouraged and approved Section 1115 waivers that conditioned Medicaid coverage on meeting work and reporting requirements in 13 states (Figure 1). Under Section 1115 of the Social Security Act, the Secretary of HHS can allow states to use federal Medicaid funds in ways that federal rules do not otherwise allow, as long as the initiative is an “experimental, pilot, or demonstration project” that “is likely to assist in promoting the objectives of [the program].” In January 2018, CMS issued guidance inviting states to request Section 1115 waivers that impose work and reporting requirements (referred to as “community engagement”) as a condition of Medicaid eligibility for non-elderly, non-pregnant adult beneficiaries who are eligible on a basis other than disability. The guidance asserted that such provisions would promote program objectives by helping states “in their efforts to improve Medicaid enrollee health and well-being through incentivizing work and community engagement.” In contrast to voluntary work support programs discussed above, the guidance was explicit that state initiatives to condition Medicaid eligibility on meeting work and reporting requirements could not use federal Medicaid funds for supportive services to help people overcome barriers to work, such as childcare or transportation. The next day, CMS approved the first Medicaid work requirement in Kentucky’s waiver. In total, CMS under the Trump Administration approved waivers with work requirements in 13 states. Across states, work requirement waivers were generally similar in conditioning Medicaid coverage for certain adults on reported employment or other qualifying activities, with some variation in technical details. For example, waivers varied by:
population, with most applying to expansion adults, a couple applying to both expansion and traditional adults, such as low-income parents, in expansion states, and some later approvals applying to low-income parents and some limited other populations in non-expansion states;
exemptions, such as for older age or medical frailty (although the work requirement guidance excluded people who are eligible for Medicaid based on a disability, many Medicaid adults with disabilities do not receive SSI benefits and are eligible due to low income rather than disability status, so they would be subject to work requirements unless the state makes an exemption and they are able to successfully navigate the exemption process);
qualifying activities in addition to employment (such as education, community service, and job search or training);
number of hours of qualifying activities required per week or month and how to report these (such as through an online account); and
consequences for noncompliance (typically disenrollment, though two states (GA and SC) required compliance to be established prior to enrollment and one state (NE) conditioned access to certain benefits, rather than eligibility, on compliance with work requirements).
Of the 13 states that had approved work requirements, only Arkansas implemented such requirements with consequences for noncompliance. Other states that began implementation did not disenroll those who did not comply and instead paused implementation due to litigation and/or the COVID-19 pandemic. For state-level detail on these approved waivers as well as additional requests that were not approved by the end of the Trump Administration, see Figure 1 and Appendix Table 1. For more information on the timing of work requirement approvals, as well as subsequent legal challenges and withdrawals (as discussed in the section below), see Appendix Figure 1.
What do we know about the impacts of Medicaid work requirements?
Research on the relationship between work and health, including experience with AFDC, TANF, and SNAP, suggest that the effects of work requirements on health and employment may be limited. In the 1990s, states used Section 1115 waivers in attempts to increase work among enrollees in the Aid to Families with Dependent Children (AFDC) program; however, an analysis suggested that a significant part of the AFDC targeted population faced obstacles to work including disability. Similarly, research finds that work requirements in TANF—the program that replaced AFDC—have had little impact on increasing employment over the long-term, as most TANF enrollees are either already working or face significant employment barriers that work requirements do not address. Studies also find that SNAP work requirements do not significantly increase employment but result in large reductions in SNAP participation. Finally, a review of research on the relationship between work and health found that although there is strong evidence of an association between unemployment and poorer health outcomes, there is limited evidence on the effect of employment on health.
As most Medicaid enrollees are already working or face barriers to work, work and reporting requirements may cause coverage loss among eligible enrollees without increasing employment. Prior to the pandemic, the majority (63%) of non-dual (i.e., not also enrolled in Medicare), non-SSI, nonelderly Medicaid adults were already working full or part-time. Among those not working, most were not working due to caregiving (12%), illness or disability (10%), or school attendance (7%). Many of these reasons would likely qualify as exemptions from work requirement policies in most states, leaving just 7% of Medicaid adults (who reported that they were retired, unable to find work, or were not working for another reason) to whom work requirement policies could be directed. A 2018 analysis suggests that if all states were to implement Medicaid work requirements, between 1.4 and 4.0 million Medicaid adults could lose coverage, with the majority of disenrollment occurring among individuals who comply with the requirements (i.e., are working enough hours to satisfy requirements) and remain eligible but lose coverage due to new administrative reporting burdens or red tape. Research suggests work requirements could have particular adverse effects on certain Medicaid populations, such as women, people with HIV, and adults with disabilities including those age 50 to 64. Finally, the one in four Medicaid enrollees living in homes with limited internet access may face particular challenges meeting work and reporting requirements, as many states disseminated information about these requirements online and/or required enrollees to report compliance online.
Available implementation data suggests that Medicaid work and reporting requirements were confusing to enrollees and result in substantial coverage loss, including among eligible individuals. As noted above, few states implemented approved Section 1115 waivers with work requirements due to litigation, state withdrawals, and/or the COVID-19 pandemic. However, Arkansas’ waiver was in effect from June 2018 through March 2019 (when it was set aside by a federal court), with evidence from this period suggesting that more than 18,000 people (about 25% of those subject to the requirement) lost coverage in 2018. While enrollees who lost coverage in 2018 could reapply for coverage in January 2019, the vast majority of those who lost coverage (89%) remained unenrolled in early 2019. Although Arkansas’s program included safeguards intended to protect coverage for people with disabilities and others who should not have been subject to the requirements from losing coverage (including “medically frail” and “good cause” exemptions and “reasonable accommodations” to assist with meeting the requirements), few people used these safeguard measures relative to the number who lost coverage. Among those who accessed “good cause” exemptions, the vast majority did so due to disability/other health issues or technical issues, primarily related to reporting. This difficulty with reporting underscores that Arkansas’ administrative processes presented barriers to eligible people retaining coverage including and beyond those with disabilities. Lack of computer literacy and internet access among enrollees created barriers to setting up online accounts as well as ongoing reporting. Research indicates that enrollees in Arkansas were unaware of or confused by the new work and reporting requirements, which did not provide an additional incentive to work beyond economic pressures.
What is the current status and future of Medicaid work requirements?
The Biden Administration began the process to withdraw Section 1115 work requirements in February 2021 and has since issued final withdrawals for all states that had approvals. CMS generally reserves the right to withdraw approved waiver authorities at any time it determines that these authorities are no longer in the public interest or promote Medicaid objectives. A January 2021 executive order from President Biden directed HHS to review waiver policies that may undermine Medicaid. CMS subsequently withdrew Medicaid work requirement waivers in all states that had approvals. These withdrawal letters cited evidence from Arkansas (described above) as well as additional data indicating that about 40% of those subject to work requirements (or 17,000 beneficiaries) in New Hampshire and 33% (or 80,000 beneficiaries) in Michigan were at risk of coverage loss, prior to implementation pauses. The letters also highlighted that job and income loss among the low-income population during the COVID-19 pandemic were likely to exacerbate the risks of coverage loss under work requirements. No states were implementing work requirements at the time of withdrawal, either due to the pandemic, litigation (see Appendix Table 2), or prior termination by the states themselves (see Figure 1).
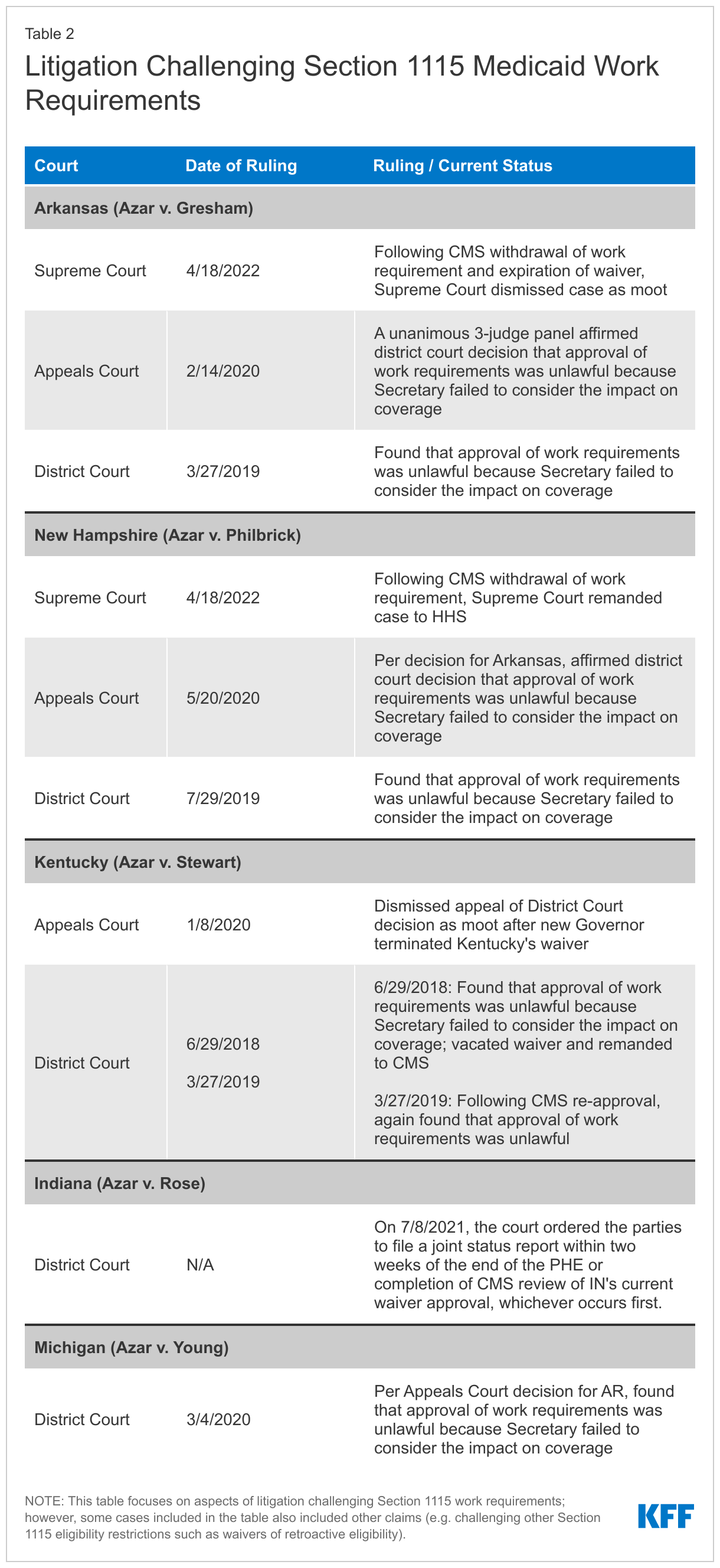
Following the Biden Administration’s withdrawals, in April 2022 the Supreme Court dismissed pending appeals in cases that had found work requirement approvals unlawful. Previously, in February 2020 a DC Circuit Court of Appeals panel affirmed in a unanimous opinion that the HHS Secretary’s approval of Medicaid work requirements in Arkansas was unlawful because the Secretary failed to consider the impact on coverage. The DC appeals court subsequently affirmed that the Secretary’s New Hampshire approval also was unlawful. Before leaving office, the Trump Administration asked the Supreme Court to reverse these appeals court decisions and the Court agreed to hear the cases in December 2020. However, following the Biden Administration’s withdrawals of the Arkansas and New Hampshire work requirements, in April 2021 the Supreme Court removed the cases from its oral argument calendar. In April 2022, the Biden Administration asked the Court to vacate the lower court decisions and dismiss the Arkansas case as moot (as that waiver had expired) and remand send the New Hampshire case back to HHS (as New Hampshire had not asked the Court to review the case involving its waiver). In April 2022, the Court granted this motion, effectively putting an end to the pending litigation. (For more information on work requirement litigation across states, see Appendix Table 2 and Figure 1.)
The Supreme Court’s dismissal does not preclude future presidential administrations from approving new Section 1115 work requirements. Each case challenging work requirements (see Appendix Table 2) has centered on the administrative record of the underlying waiver approvals under the Trump Administration, with courts finding that these approvals were unlawful because they were unsupported by the administrative records. Specifically, the courts found that the Secretary did not consider impacts on coverage contained in the administrative records. Although the Biden Administration has concluded that it does not believe work requirements further Medicaid program objectives, CMS under future presidential administrations could issue new guidance encouraging work requirement waivers and approve such waivers based on a different interpretation of program objectives—though these would likely face legal challenges. For example, although Arkansas removed its work requirement in its new waiver, the state noted that should federal law or regulations permit the use of a work requirement as a condition of eligibility in the future, it would seek to amend the demonstration accordingly. Separately, states had the opportunity to appeal the Biden Administration’s withdrawals of work requirement waivers to the HHS Departmental Appeals Board and Georgia has challenged the withdrawal of its work requirements (which would have been part of a limited coverage expansion) in court. Georgia’s challenge remains pending, with an initial decision expected later this summer.
Conclusion
As a health coverage program, Medicaid can support employment by providing health coverage and access to care and medications that enable people to work, and it can also provide voluntary employment referral and/or work support programs. In a departure from previous administrations, the Trump Administration encouraged and approved Section 1115 waivers that conditioned Medicaid coverage on meeting work and reporting requirements. Though few of these work requirements were implemented due to legal challenges, state withdrawals, and/or the COVID-19 pandemic, available data suggests that such requirements can result in substantial coverage loss, including among eligible individuals, as evidenced by the more than 18,000 individuals who lost coverage in seven months under Arkansas’ work and reporting requirement. Based in part on this data, the Biden Administration withdrew all approved work requirement waivers by the end of 2021; Georgia has since challenged the withdrawal of its work requirements in court. Following these withdrawals and the expiration of Arkansas’ waiver, the Supreme Court dismissed pending appeals in cases that had found work requirement approvals unlawful. Though the Court’s action does not preclude future presidential administrations from approving new Section 1115 work requirements, these would likely face legal challenges.
On May 2, news media reported a leaked draft of the Supreme Court majority decision for the Dobbs v. Jackson Women’s Health Organization, showing the Court plans to completely overturn Roe v. Wade. The draft opinion is not yet final and abortion remains legal nationwide for now. The final Court decision is expected late June.
Ahead of the final decision, you can find some KFF resources relevant to this Supreme Court case and abortion access:
This brief reviews the status of state actions to strengthen and guarantee abortion access to their residents, as well as to prepare for the likely increase in demand for abortion services in those states should the high court overturn the constitutional right to abortion established by Roe v. Wade.
This Policy Watch gives an overview of employers offering to cover travel expenses for workers who need to go out of state for an abortion in the context of increasing restrictions on abortion around the country. We discuss who is offering these benefits, the implications for workers, and some of the legal and political concerns for employers.
This issue brief provides background on the legal challenges to the Mississippi law in the context of the Supreme Court abortion precedents, addresses the intersections with the litigation that has arisen from S.B. 8, the Texas 6-week abortion ban, and explains the potential outcomes and how they could impact access to abortion around the country.
This brief outlines the intersection of federal policy regarding dispensing medication abortion with state laws regulating the provision of abortion services and mifepristone dispensing via telehealth and considers the implications of the recent FDA change in different states.
View a recent KFF briefing about issues that are central to women’s health and well-being, ranging from abortion to paid leave, that are being considered by the Supreme Court, Congress, and state policymakers.
This infographic highlights data and policies regarding the availability and effectiveness of medication abortion in the United States. Medication abortion accounts for more than half (54%) of all abortions before nine weeks gestation in the U.S.
This infographic updates a prior JAMA infographic that presents state policies related to abortion and their intersection with clinical practice. The graphic highlights state-level abortion specific policies, ranging from waiting period laws to medication abortion requirements.
Explore the latest national and state-specific data and policies on women’s health. Topics include health status, insurance and Medicaid coverage, use of preventive services, sexual health, maternal and infant health, and abortion policies. Many indicators provide state-level information for women of different racial and ethnic groups.
Uptake of pre-exposure prophylaxis (PrEP)—a preventive medication that reduces the risk of acquiring HIV through sex and injection drug use, has been slow, despite its high efficacy and recommended use for those at risk. Furthermore, disparities in access and use exist along racial, ethnic, and gender lines. The Centers for Disease Control and Prevention (CDC) estimates that in 2020 about 300,800 people were prescribed PrEP, representing only 25% of those with an indicated need for the medication.1 The use of telehealth to provide PrEP and associated services (“tele-PrEP”) is a trend that began before the COVID-19 pandemic but we find it has increased for some providers along with the growing use of telehealth generally. However, little is known about the tele-PrEP environment. This brief provides an overview of the tele-PrEP landscape, including how PrEP services (e.g., initial consults, lab work, prescribing, and ongoing monitoring) are provided and factors that facilitate its provision as well as barriers that remain. It is based on in-depth interviews conducted at the end of 2021 with representatives from the major national telehealth companies (those serving all or large portions of the U.S.) providing tele-PrEP and other select tele-PrEP programs. We also highlight two-state run programs – California and Iowa – and four community-based clinics that offer tele-PrEP programs. Collectively, the organizations included in this analysis are estimated to provide tele-PrEP services to over ten thousand clients. Key findings are as follows:
Tele-PrEP programs have different operational models and financing structures, each with implications for patient costs and company/program revenue. In some cases, services are offered for free to clients but more than half of private companies interviewed charge a fee. Some, but not all, work to enroll uninsured and underinsured patients in assistance programs or insurance coverage. Programs and companies generated revenue through fees charged to clients or organizations who contract with the private companies, by operating as both the pharmacy as well as the provider, and also through the 340B drug pricing program.
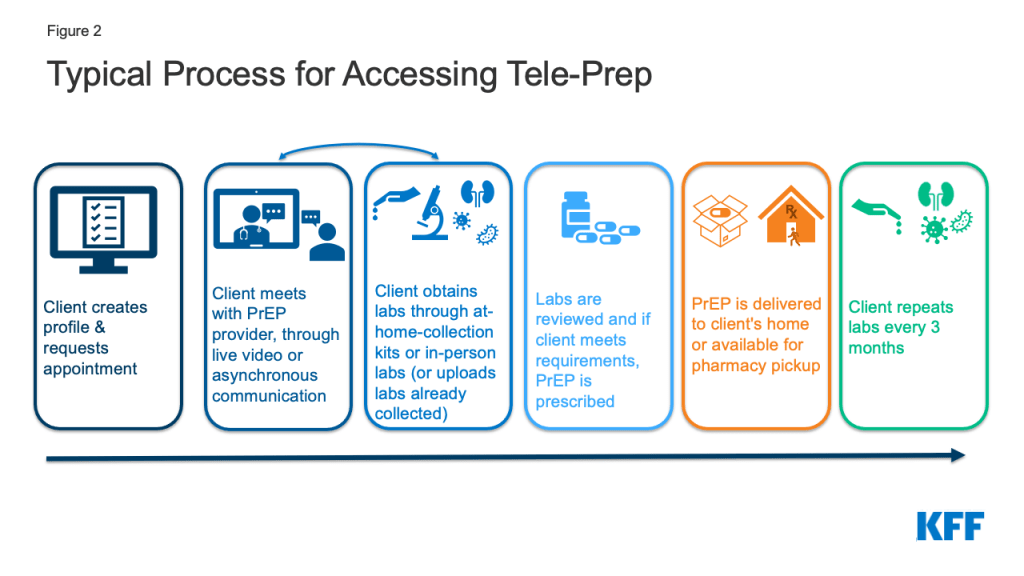
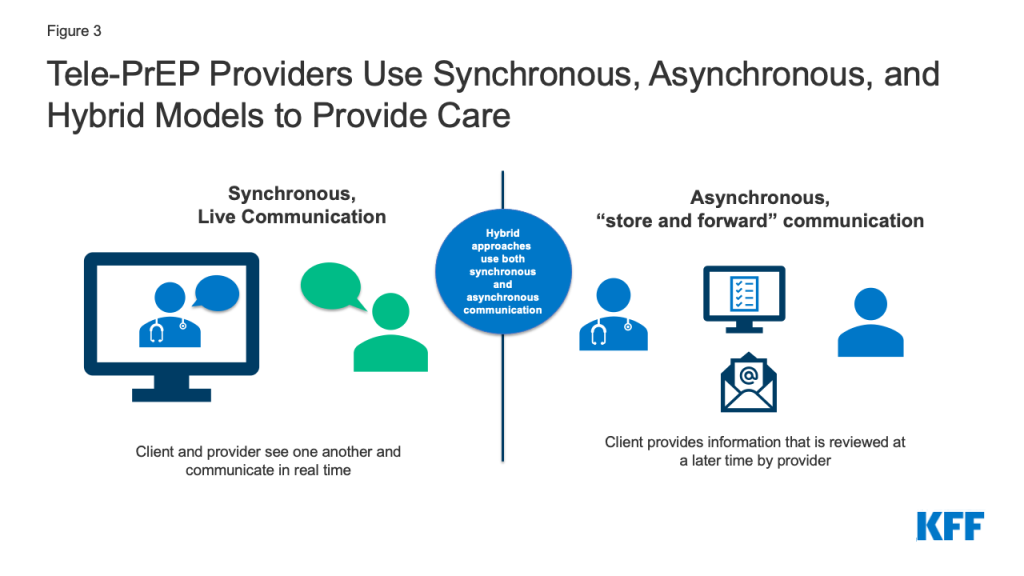
About half of respondents reported conducting visits primarily or exclusively via live video (i.e. using synchronous methods), one primarily uses asynchronous methods (e.g., via text, email, or delayed chat instead of phone or video), and about half use a hybrid approach.
Laboratory services, a central component to PrEP initiation and related on going care, and prescribing patterns also varied. For example, some respondents primarily used home lab collection kits while others referred patients to in-person labs. In some cases, this was based on client preference, and in others, in response to legal barriers. Likewise, some providers primarily offer generic PrEP while others tend to favor prescribing branded drugs, a choice that was typically tied to program design.
Some programs are primarily focused on PrEP provision, while others offer additional select services, and some provide PrEP as part of a comprehensive clinical program. All programs have a process for connecting people who are diagnosed with HIV to care and either can treat other sexually transmitted infections (STIs) or have linkages to STI care.
Respondents offered a range of reasons for providing tele-PrEP. While the private companies stood to earn a profit from their PrEP programs, the predominant reason given for offering this services across all respondents was to provide wider access to PrEP and some tied this objective to reaching the national goal of “ending the HIV epidemic.” For some, tele-PrEP was viewed as a way to address specific access barriers, including stigma associated with PrEP and structural challenges, such as getting time off work or transportation to appointments.
Clients served were mostly cisgender men who have sex with men, and in their 20s and 30s. Among interviewees who provided estimates, between 23% and 55% of patient populations were people of color. Insurance coverage distribution ranged significantly by tele-PrEP provider. Collectively, the national tele-PrEP companies included in the analysis served clients in all states, with most clients located in California, Texas, Florida, Georgia, and New York.
Factors that facilitated tele-PrEP provision included multi-state licensing, developing partnerships with community-based organizations, use of marketing, and assisting uninsured clients with insurance enrollments. Respondents’ opinions varied as to whether synchronous or asynchronous communication better facilitated provision of tele-PrEP. Barriers included the challenge of working with insurance companies and Medicaid, laws prohibiting some aspects of telehealth, and retention.
A spotlight on tele-PrEP provision in California reveals a changing landscape in the state. For example, the state policy environment is evolving to prohibit the use of step-therapy, which usually requires patients try a lower cost or generic drug before a more expensive or brand drug, and prior authorization for PrEP in many cases and to promote the use of home lab collection. The state tele-PrEP program is also undergoing structural changes. The focus on California is noteworthy given the largest share of PrEP users in the U.S. hail from the state.
Taken together and given the number of clients being served via this modality, we find that tele-PrEP offers an additional or alternative avenue for accessing PrEP services. However, little is known about how effectively tele-PrEP can be used to increase access and adherence overall or address disparities in PrEP use and how the client experience of tele-PrEP compares to in-person PrEP services. And despite it’s potential, access challenges to PrEP through tele-health remain: some populations are still being left out, particularly women and people of color, insurance barriers persist, certain policies can hamper uptake (e.g. multi-state licensing and credentialing requirements, coverage of home lab collection, etc.), and knowledge gaps about PrEP among both providers and individuals remain.
Issue Brief
Background
First approved by the FDA in 2012, pre-exposure prophylaxis (PrEP) is a preventive antiretroviral medication that reduces the risk of acquiring HIV through sex by approximately 99% and through injection drug use by at least 74%. Given its high efficacy, PrEP is seen as a cornerstone of efforts to “end HIV,” including in the federal National HIV/AIDS Strategy (NHAS) and the Ending the HIV Epidemic Initiative (EHE). PrEP is recommended for HIV negative people at high risk for acquiring HIV through sex or injection drug use and requires both a medication and routine associated provider visits and labs (see Table 1: PrEP Medications and Associated Services).
Table 1: PrEP Medications and Associated Services
Medications for PrEP and Availability at Time of Interviews
Brand Name
Generic Name (abbreviation)
Available at time of interviews
Formation
Truvada
Emtricitabine / Tenofovir (FTC/TDF)
Yes (brand and generic)
Pill
Descovy
Emtricitabine & Tenofovir Alafenamide (FTC/TAF)
Yes (brand only)
Pill
Apretude
Cabotegravir (CBG)
No
Injectable
Laboratory Screening and Visits for Oral PrEP* Initiating and Monitoring
Assessment and counseling
Assess for signs/symptoms of acute HIV (to ensure individual is HIV negative); assess and support adherence and HIV risk and risk-reduction behaviors; assess and manage adverse effects; conduct contraception/conception counseling as appropriate. Assessment includes reviewing recent higher risk behaviors and clinical presentation (see page 29 and Figure 2 in the guidelines referenced in this table).
Labs for Oral PrEP
HIV test (preferred: laboratory HIV 4th generation Antigen/Antibody; point of care oral fluid tests should not be used). At initiation and every three months; HIV RNA every 3 months.
Syphilis. At initiation and every 3 months for men who have sex with men and transgender women; semi-annually for others.
Gonorrhea. At initiation and every three months for men who have sex with men and transgender women; semi-annually for others.
Chlamydia. At initiation and every three months for men who have sex with men and transgender women; semi-annually for others.
Renal Function as measured by creatinine clearance (eCrCl). At initiation and every six months for patients aged ≥50 years or who have an eCrCl <90 ml/min at PrEP initiation, otherwise annually.
Hepatitis B. At initiation.
Hepatitis C. At initiation for men who have sex with men, transgender women, and people who inject drugs and every 12 months for those in these groups.
Cholesterol and triglycerides. For those using TAF/FTC only – at initiation and every 12 months.
Follow up visits
At least every 3 months
Source: U.S. Centers for Disease Control and Prevention: U.S. Public Health Service: Preexposure Prophylaxis for the Prevention of HIV Infection in the United States—2021 https://www.cdc.gov/hiv/pdf/risk/prep/cdc-hiv-prep-guidelines-2021.pdf*Visit and lab schedule is for oral PrEP only. Injectable PrEP was approved but not available at the time of the interviews. Details on labs and visits needed for injectable PrEP available at link above.
Several policy developments have occurred to help make PrEP more accessible. The CDC first recommended PrEP for certain high-risk groups in 2014. In 2019, the United States Preventive Services Task Force (USPSTF) issued its highest “A” grade recommendation for PrEP which, under the Affordable Care Act (ACA), means that most private health plans and Medicaid-expansion programs are required to cover PrEP without cost-sharing. In 2021, the government clarified that the USPSTF grade also covers PrEP services such as labs and provider visits (see Box on USPSTF). The federal government also launched the Ready, Set, PrEP program in 2019 to provide medication access to those without insurance. Despite these developments, PrEP uptake has been slow. Preliminary data shows that in 2020 just 25% (300,783) of the estimated 1.2 million people in the U.S. who have an indication for PrEP (i.e. those who have higher risk sexual or injection drug use experiences) were prescribed it2 and there are disparities in PrEP use along racial, ethnic, and gender lines. For instance, in 2019, Black or African American people accounted for an estimated 42% of new HIV infections but just 8% of PrEP prescriptions and for Latinos it was 29% and 14%, respectively.3 Likewise, in 2019 women accounted for an estimated 18% of new HIV infections but 9% of PrEP prescription.4
United States Preventive Services Task Force (USPSTF) PrEP Guidance
In 2019, the United States Preventive Services Task Force (USPSTF) issued its highest “A” grade recommendation for PrEP. As a result, most private health plans and Medicaid-expansion programs must cover the service without cost-sharing. However, questions surfaced about whether the recommendation included only the PrEP medication, or the services needed to support PrEP (e.g. provider visits, labs, etc.). Clarification came in July 2021 when federal guidance stated the “A” grade encompassed PrEP services such as HIV testing, STI testing, and PrEP specific office visits, among others. Awareness of and implementation of this policy change, however, is uneven. Some respondents were unaware of this policy development. Others were well versed in it, including those some who said that the change had been important for patient access and reduced costs and others who said that roll out has been uneven with some insurers still charging cost-sharing for these services.
A range of complex and interconnected issues affect PrEP access and utilization. While any provider with the prescribing authority can prescribe PrEP, many do not and some are not aware of it. Those seeking PrEP may not initiate conversations with providers due to stigma. Others might not have a regular provider or a provider competent in PrEP provision and PrEP awareness remains low among some groups with high indication. Actual and perceived costs may also be a barrier for some, particularly for those without health insurance. Additionally, the COVID-19 pandemic limited in-person health care access in certain cases, and made many people less comfortable accessing in-person health care.
The use of telehealth to provide PrEP and recommended services (or “tele-PrEP,”) without in person visits, began before the COVID-19 pandemic, but has increased because of the pandemic. Tele-PrEP may provide a new avenue for PrEP access, yet little is known about how these programs are organized and operationalized, and what the implications of relying on such an approach might be. Pastresearch has largely focused on client experiences.
This project sought to better understand the current role of tele-PrEP in the PrEP landscape, including identifying factors that facilitate tele-PrEP provision and access, as well as barriers that remain. We conducted in-depth semi-structured interviews with individuals in leadership roles at organizations providing or supporting the provision of tele-PrEP across the U.S.
We focused primarily on the national tele-PrEP providers given their intent to provide PrEP via telehealth at the outset (vs. clinics which may provide tele-PrEP as a part of their offerings) and spoke to representatives in leadership positions (i.e. CEOs or tele-PrEP program managers/leaders) from five of the six5 national companies we identified as providing comprehensive access to PrEP (e.g., they facilitate both the medical care and the prescription). These companies were identified through online searches, review of lists of tele-PrEP companies from organizations such as PleasePrEPMe, and based on conversations with stakeholders. To enrich the analysis and provide points of comparison, we also spoke to representatives from four brick-and-mortar clinics with tele-PrEP services selected for regional diversity (one from California, one from New York City, and two from Southern states), and state health officials from California and Iowa about their state-run tele-PrEP programs (representing two of the five states that offer tele-PrEP services). These states were selected because in 2019, California had the highest number of PrEP users, highest HIV prevalence and the second highest HIV incidence and diagnoses. In addition, the tele-PrEP companies included in this study regularly cited California as their largest market. Iowa was selected because the state has been identified as a leader in the tele-PrEP space, with a robust program and the program commonly provides assistance to other states. We also spoke with a representative from a lab company providing home collection services to most major tele-PrEP companies. About one-fifth of this lab’s business comes from tele-PrEP services. In all, we interviewed 12 individuals. Additional background calls were held with other stakeholders who conduct research on PrEP, work in the pharmaceutical industry, and work on PrEP policy and advocacy. Interviews were transcribed and coded by a primary and secondary coder to achieve intercoder reliability using both a priori and emergent codes. Codes were then charted (i.e., coded text was organized in a grid with themes across the top and respondents along the left side to allow for cross-theme/respondent analysis), and finally they were analyzed. Respondent and organization names of private companies and clinics have been withheld throughout the report as interviews were conducted on condition of anonymity.
Findings
Respondent details
The 12 Tele-PrEP providers fell into four categories:
National tele-health companies, some of which focused primarily on PrEP (5 companies)
Tele-PrEP programs located within clinics or hospital systems (4 programs)
State-run tele-PrEP programs: California and Iowa (2 programs)
A laboratory company that among other services, provides most major tele-PrEP companies with home collection kits and lab services (1 company)
Among the private companies, three began serving PrEP clients just prior to the pandemic’s onset or during the pandemic, after a pre-pandemic planning period. Two of these initiated their services at least a year before the start of the pandemic, with the oldest program serving PrEP patients since 2016. None of the private companies and neither state program cited the pandemic as the reason for offering tele-PrEP. However, some clinic-based programs said that they started their tele-PrEP offerings in response to the pandemic (see section on the COVID-19 Pandemic).
Financing/business model
There were generally four financing models supporting tele-PrEP programs, each of which has implications for patient costs and company/program revenue:
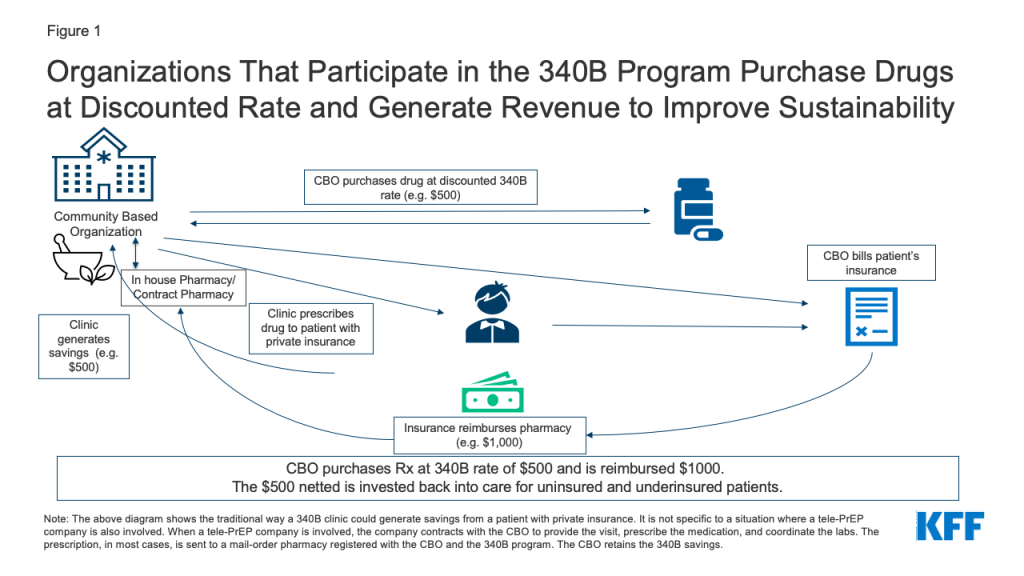
1. Clinic based tele-PrEP programs (4 respondents). Clinic based tele-PrEP programs are programs offered within another clinical setting, such as a hospital, a Federally Qualified Health Center (FQHC), or other type of brick-and-mortar clinic. The four clinic-based programs all accept insurance, including from private and public payers. One clinic-based provider requires patients to be seen at satellite clinics and uses telemedicine machines with video to connect with providers at a primary clinic location. The other respondents use more typical telehealth systems where the patient can be at a location of their choosing (e.g., in their home or car using a computer or smart phone). The satellite tele-PrEP provider charges a per visit fee for uninsured patients ($30) but no others do so. Two clinics have ways of covering costs for the uninsured, including by leveraging 340B savings (see Figure 1, description below, and box on the 340B program), utilizing pharmaceutical industry support for medication, and helping clients enroll in ACA health plans and Medicaid. Of these, one, a California based clinic, also relies on the state PrEP assistance program to cover labs, industry support for medications. One clinic located within a hospital system provides PrEP services to uninsured patients at a discounted rate and is exploring ways to connect with the hospital 340B program.
Figure 1: Organizations That Participate in the 340B Program Purchase Drugs at Discounted Rate and Generate Revenue to Improve Sustainability
2. Standalone Tele-PrEP Companies (3 respondents). Three private tele-PrEP companies have stand-alone operations (i.e., they have no formal business relationship with brick-and-mortar clinics). All three charge a fee to clients. In two cases, the fee covers the cost of the medical service and PrEP management and insurance is billed for labs and medication. Of these, one has a lower fee ($15 for three months) but also acts as the pharmacy so generates revenue from both the fee and the dispensing of medication. The other has a higher fee ($15 per month + $59 every three months for the visit) but no direct relationship with a pharmacy so is generating revenue from the fee only. Fees associated with labs and medication are additional for clients of these companies. Both accept private insurance and cash paying clients and one takes Medicaid clients but only in four states (California, Texas, New York, and Illinois). The third company in this group runs on a cash only model, so does not take Medicaid or private insurance, and charges clients a monthly fee ($70-$100 per month depending on the labs ordered). The fee covers the PrEP medication (which is a generic), provider visits, use of the platform, and labs. While these companies do not waive or subsidize costs of labs or fees for the uninsured, one respondent said they will sometimes refer uninsured patients to a tele-health company connected to a Community-Based Organization (CBO) to get free access (see below on the tele-PrEP/CBO hybrid model).
3. Tele-PrEP Company-Community Based Organization (CBO) Hybrids (2 respondents). Two of the private tele-PrEP companies have business models centered around CBO partnerships. With both companies, each tele-PrEP patient is connected to and becomes a patient of a local CBO that participates in the 340B drug pricing program. Qualifying organizations (such as community health centers or STI clinics) that participate in the 340B program are able to purchase drugs at a discounted rate through their own or contract pharmacies. Private insurance typically reimburses for these drugs at a higher rate than the 340B purchase cost. By design, the difference between the drug cost and the reimbursement (or savings) is kept by the program to enhance access to care for patients. (See more detail in box on the 340B Drug Pricing Program and Figure 1). A patient is not required to enter a brick-and-mortar facility in order for a prescription to qualify through the program. However, the patient is required to meet the federal definition of a 340B-eligible patient.6 The tele-PrEP partner company manages clinical visits, labs, pharmacy interactions, and provides the telehealth platform and thus, the CBO may have no direct interaction with the patient. In most cases, and in order for this model to work as designed, the patient fills their PrEP prescription through a registered mail order 340B contract pharmacy associated with the CBO. In exchange, the CBO generates and retains the 340B savings from the prescription. 340B savings are not kept by the tele-PrEP companies. However, patients can opt to fill their prescription elsewhere. While CBOs can direct their own patients to the telehealth affiliate company, more commonly, patients contact the tele-PrEP company directly and are associated with the CBO on the back end. Patients are required to sign an acknowledgment that they are patients of that CBO when they enroll with the tele-PrEP company. The companies do not bill for the labs or the visit. In exchange for the service provided, the CBO pays the tele-PrEP company a fee (either monthly or quarterly) for managing the patient’s PrEP and related services. Neither company charges the patient a fee (see Table 3).
One company covers advertising costs with the fee charged to the CBO and the other has the CBO cover the cost on top of their fee.
Both companies reported they were beginning to enroll eligible uninsured clients into ACA marketplace plans, which allows them to generate 340B savings for these clients. This became more important to them following January 2022 changes to Gilead’s PrEP assistance program (PAP) for uninsured clients (Gilead manufactures both branded oral PrEP medications). In the past, the PAP reimbursed prescribers closer to list price for medications, effectively allowing these organizations to generate savings as they would through 340B, if the client had private insurance. The new PAP policy states that the company will reimburse organizations for only the amount paid per bottle of medication, a dispensing fee, and an administrative fee. Organizations in states that did not expand their Medicaid programs were especially worried about this change as they had higher rates of uninsured clients relying on the PAP. Plan enrollment provides a new way for CBOs to generate 340B savings from PrEP prescriptions by helping these clients become insured. Clients also benefit from gaining insurance for other known or unseen future health needs.
One of the state officials remarked on the challenges in setting up a statewide program and that, especially for states without the capacity to create a program from scratch, there could be value in developing such CBO hybrid programs which would negate the need for staffing or infrastructure.
The 340B Drug Pricing Program and PrEP
The Federal 340B Drug Pricing Program enables safety net health providers to make health services and prescription drugs more affordable for uninsured and underserved people. Section 340B of the Public Health Services Act requires pharmaceutical manufacturers participating in the Medicaid program (virtually all manufacturers) to provide outpatient drugs at significantly reduced prices to 340B “covered entities” (e.g. safety net hospitals, Title X clinics, Federally Qualified Health Centers, among others).
The program promotes access to out-patient prescription drugs and care, including PrEP, in two ways. First, the cost of the drugs is reduced so it is less expensive to treat uninsured and underinsured patients. Second, 340B entities who have purchased drugs at discounted rates can typically get reimbursed at a higher rate for patients with insurance and generate income from the difference. For example, if a 340B entity purchases a drug for $500 and is reimbursed $1,000 by an insurance company (via the in-house or contract pharmacy), the provider generates $500 in savings which is then invested back into the program, funding care for those in need and to “to stretch scarce federal resources” further.
One notable element of the 340B program is its prohibition against so-called “duplicate discounts.” Covered entities are statutorily prohibited from obtaining both a 340B discount and a Medicaid drug rebate discount for the same medication and must have systems in place to prevent this.
4. State Programs (California and Iowa). Both state programs work to maximize access and minimize cost-barriers for PrEP patients in their states. The California state tele-PrEP service is part of the state’s PrEP Assistance Program which provides PrEP access for people who are uninsured, under-insured, or need to use the services for confidentiality reasons (e.g. so parents or partners are not made aware of PrEP use through insurance paperwork). This program covers costs for visits and labs and relies on manufacturer assistance for medications for those without insurance. California’s state program previously contracted with a national telehealth company to provide tele-PrEP but recently shifted to contracting with three CBOs in the state to provide tele-PrEP services remotely throughout the state (see process and fundamentals). It is unclear how or if patients were notified of the change or whether there were patients to notify as uptake of the private run program is reported to have been low. The focus of this program is on the uninsured, but the state does allow insured patients to use the tele-PrEP services as long as the CBO is in-network with the individual’s insurance. While the tele-PrEP component is virtual, the program requires clients to register in person at an enrollment site, of which there are hundreds across the state, a challenge noted by some stakeholders. (For more detail on the California program see the “Spotlight on Tele-PrEP in California” box).
The Iowa program does not bill for the tele-PrEP service and visit, which are subsidized with 340B savings. Insurance (including public and private coverage) is used to cover labs and medications. If uninsured clients engage with the program, they are screened for coverage eligibility and assisted with enrollment, if eligible. The small (less than 10%) share that remain uninsured are helped through industry assistance programs for medications and the state Title X7 network for labs. Those using Title X network labs may face a $5-$10 fee that can be waived if it poses a hardship.
Table 2: Fees Charged by Tele-PrEP Companies
CBO or Standalone Model
Fees
Other costs
Other detail
CBO
None
None
—
CBO
None
None
—
Standalone
Yes, $15 every three months
Labs and Medications covered by insurance
Company also acts as pharmacy (thus generating revenue in this role as well)
Standalone
Yes, $15 per month and $59 every three months for PrEP visit
Labs and Medications covered by insurance
—
Standalone
$70-$100 per month
None
Generic Rx provided at negotiated rate through contracted pharmacy
Process and Fundamentals
Tele-PrEP providers tended to follow a similar process. Most often, clients encounter their platforms, see a provider, obtain labs, receive a prescription after labs are reviewed, receive medication (either in person or by mail), and then three months later the process is repeated with another provider visit and certain labs. One exception is that clients of the California state tele-PrEP service have to enroll into the state program at in person PrEP Assistance Program enrollment sites. This in-person visit is administrative and not clinical in nature.
Figure 2: Typical Process for Accessing Tele-Prep
The telehealth systems used however, varied by provider:
About half of respondents (6), including the Iowa state program, reported that PrEP visits are primarily or exclusively conducted using synchronous video – meaning that the patient and the provider see one another and are communicating in real time.
Figure 3: Tele-PrEP Providers Use Synchronous, Asynchronous, and Hybrid Models to Provide Care
At the time of the interviews, one (1) provider primarily relied on asynchronous communication (e.g. via text, email, or delayed chat instead of phone or video), but said they speak with clients who need additional support on the phone, including when delivering sensitive information, such as an HIV diagnosis. This provider also noted that as of January 1, 2022, they would be active in states requiring video or phone for telehealth and were ready to fill those requirements in those locations. As such, the provider is now still primarily providing asynchronous care but offers synchronous services as required by state law.
Three (3) providers take a hybrid approach. These providers use synchronous video some of the time but also conduct communication asynchronously. Two of these providers typically use only limited synchronous video (e.g. once a year or for the first visit) and one allows the patient to decide whether they use video or asynchronous communications.
One (1) provider with a brick-and-mortar clinic sees patients at satellite clinics using telemedicine machines with video to connect with providers at a primary clinic location.
The California state program, previously contracted with a telehealth vendor using synchronous video to provide tele-PrEP services but recently brought services in-house and will rely on three community partners and a network of enrollment workers across the state to stand up the services. How services will be delivered will be determined by the systems the community partners already have in place.
Some respondents spoke of the value of at least occasional video visits, believing they could better engage with patients, but others believed patients generally preferred asynchronous communications.
Table 3: Tele-PrEP Process/Approach Used by Respondents
Provider
Model
Primarily Synchronous, Asynchronous, Hybrid
Notes
Provider 1
Private Company/CBO Hybrid
Hybrid
Video at least once per year, other times patient choice, general preference is asynchronous
Provider 2
Private Company/ CBO Hybrid
Hybrid
First visit is video, then more automated/asynchronous
Provider 3
Private Company
Asynchronous
Speaks with clients who need additional support on the phone
Provider 4
Private Company
Synchronous
Always synchronous video
Provider 5
Private Company
Hybrid
Patients can opt into a video visit. Most (about 60%) opt for asynchronous.
Provider 6
Clinic Based
Synchronous
Always synchronous video
Provider 7
Clinic Based
Synchronous
Always synchronous video
Provider 8
Clinic Based
Synchronous
Always synchronous video
Provider 9
Clinic Based/satellite program
Synchronous
Satellite program – patients at satellite clinics use telemedicine machines with video to connect with providers at a primary clinic location
Provider 11
State Program (California)
Unclear now (previously synchronous video)
State uses 3 community providers and follows their preferred method of communicating, previously used a telehealth provider that primarily uses synchronous approaches
Provider 10
State Program (Iowa)
Synchronous
Synchronous video is the program preference, occasionally reverts to phone if internet bandwidth fails
LabORATORY SERVICES
The process for obtaining labs necessary for PrEP initiation and monitoring also varied with some respondents favoring home lab kits and others referring patients to in-person community-based labs and some offering both options. Half of the tele-PrEP providers send patients to community sites, such as Quest or LabCorp, regional hospital hubs, or county clinic locations to get labs drawn. The remainder use both at home and in-person labs to some extent. While some providers stated their clients are roughly split as to whether they use in-person or at home testing, others, especially private companies, primarily use home testing (some for 90%-98% of clients) and use in-person testing only when specifically requested. Most respondents use home collection kits from a single company. However, the Iowa state program, currently using in-person testing, is working to develop their own test kit. Currently, the Iowa Program largely sends clients to brick-and-mortar locations but has a few clients who order home collection kits and pay for those themselves. The tele-PrEP program California previously contracted with used in person labs. Now lab options would be specific to the practices at the contracted CBO.
There was some variation in the types of labs conducted as part of standard PrEP initiation and maintenance. Among those who provided details, all report conducting at a minimum testing for HIV, hepatitis B, and creatinine clearance. Just one provider used only these labs at baseline. Others typically also test for chlamydia, gonorrhea, and syphilis and many included hepatitis C as well. One provider stated that while they encourage the full suite of tests, if a patient refuses the other STI tests, they will prescribe PrEP with just an HIV and creatinine test.
Providers discussed the challenges and opportunities with home versus on-site labs. Respondents mentioned difficulty getting insurance coverage for labs using at home collection in many cases, which was one reason some primarily worked with large in-person national labs, like Quest and LabCorp. Some discussed the new California law, SB-306, which requires insurance coverage of home tests but is facing implementation challenges (see box on SB-306). Some providers identified home collection as a good option for 3-site (pharyngeal, rectal, and urine) testing for chlamydia and gonorrhea, noting that certain commercial labs do not offer 3-site testing and New York state prohibits 3-site collection at in person labs. Some also report that patients are more comfortable taking their own swabs at home. However, others expressed concern with the less precise dried blood spot syphilis assay typically used in the home collection kits which can detect only whether someone has ever had syphilis, not whether someone has an active syphilis infection. Two respondents primarily using in-person lab settings also mail 3-site self-collect kits to patients and noted their ability to take advantage of the best of both testing opportunities by using this hybrid approach.
An additional challenge in New York is that the state generally prohibits self-collection unless the diagnostic has approval from the state lab’s “Clinical Laboratory Evaluation Program.” Given this, most tele-PrEP companies require New York patients to obtain in person labs.
The respondent from a lab servicing tele-PrEP companies mentioned CDC’s updated PrEP guidelines, noting the recommended labs for PrEP provision now include HIV RNA testing alongside a 4th generation HIV test which could pose challenges for home collection due to its expense and because HIV RNA is not currently available for home test kits. Another possible future challenge for home collection identified by respondents is whether the Food and Drug Administration (FDA) will seek to take a larger regulatory role in the home test space in the future, which could make getting tests approved more challenging and disrupt the industry.
California Law SB-306 Requires Coverage of At-Home STI Testing Kits
A new policy in California aims to address some of the reimbursement issues for at-home (i.e. self-collection) lab tests in the state. On January 1, 2022, California law SB-306 went into effect requiring health plans to provide coverage for home test kits for HIV and other STIs (including laboratory costs for processing the kits) that are deemed medically necessary or appropriate and ordered directly by a health care provider or furnished through a standing order for patient use. However, several implementation issues are surfacing. 1) Coverage through the state Medicaid program is contingent upon the addition of codes specific to home test kits in the Current Procedural Terminology (CPT) or healthcare Common Procedure Coding System (HCPCS) which do not yet exist. 2) There have also been implementation challenges ensuring that private health plans follow the law and cover both the kit and lab costs. 3) The labs used by tele-PrEP companies may not be in network for health plans which also poses challenges for reimbursement. Advocates and industry are currently working to try and establish appropriate billing codes for these remote diagnostics where needed and address implementation issues. The new law does not apply to some employer-sponsored health plans that are regulated by the federal government.
Pharmacies
Tele-PrEP provider pharmacy arrangements also varied. While some providers left pharmacy decisions entirely up to patients, others were incentivized to promote a particular type of pharmacy access. Those with 340B relationships, either because of a CBO-hybrid model or because as a clinic they were a 340B covered entity, benefit when patients uses their own pharmacy or a contract pharmacy. One 340B provider with a brick-and-mortar clinic, said that they have been losing out on savings as patients have been using tele-health and filling prescriptions at local pharmacies rather than at the clinic’s 340B pharmacy, and are considering ways to recapture the savings. The two national tele-PrEP companies using the hybrid model prefer patients to use a specialty mail-order pharmacy associated with their operation and registered with the CBO and as a 340B pharmacy so that the CBO is able to capture 340B savings. A third tele-PrEP company with an in-house pharmacy benefits from patients using their mail order service as it is part of their business model. The telehealth company with a cash pay business model exclusively uses a contracted pharmacy to deliver generic PrEP at a negotiated discounted rate. Several, but not all, providers with a preferred pharmacy network mentioned that while they had a preference, patients were free to choose alternative arrangements. Among providers who left pharmacy decisions up to patients, all said patients tended to prefer brick-and-mortar local pharmacies to mail order. For some patients, mail-order may be convenient and beneficial but for others home delivery can present challenges related to stigma/discretion or not having a safe place to leave packages.
Prescribing
All respondents reported starting their clients with a one-month prescription. After the first month, if a patient’s insurance would cover it, most providers offer 90-day prescriptions, a prescribing technique sometimes called “multi-month prescribing” which can be used to improve adherence. Two tele-PrEP companies using the CBO hybrid model note that they face insurance limitations with “multi-month-prescribing” and so write monthly prescriptions. In these cases, insurance companies require multi-month prescriptions to be filled through the insurer company’s contracted specialty pharmacy directly which would not enable these companies to leverage 340B savings for the CBO.
Half of providers said they aim for same day or rapid starts on PrEP where possible but noted some timing challenges while waiting for initial labs, particularly for a negative HIV test. The Iowa state program receives referrals from other parts of the state public health system said that patients often come in already having had an HIV test which makes rapid starts easier. Multiple companies mentioned that if patients come in with labs that they have done elsewhere (e.g. at LabCorp or Quest), it allows them to do a “rapid start” and they will issue the prescription same day. Despite these efforts, several providers stated that in reality, the time between first contact with the patient to PrEP in hand tends to typically be five days to a few weeks.
Medication
At the time of the interviews there were two branded drugs on the market for PrEP, Truvada and Descovy, both available in pill form. While there are multiple generic versions of Truvada available, there is no generic option for Descovy. Branded Descovy and Truvada are both manufactured by the same company, Gilead. The newest PrEP drug, Apretude, manufactured by ViiV, given as an injection every two months (after an initial two-dose series the first month) was not available at the time of the interviews. However, respondents were asked how they were planning for its arrival (see box on “Planning for Long-Acting Injectable PrEP”).
Table 4: Medications for PrEP Availability at Time of Interview
Brand Name
Generic Name (abbreviation)
Available at time of interviews
Formation
Truvada
Emtricitabine / Tenofovir (FTC/TDF)
Yes (brand and generic)
Pill
Descovy
Emtricitabine & Tenofovir Alafenamide (FTC/TAF)
Yes (brand only)
Pill
Apretude
Cabotegravir (CBG)
No
Injectable
About half of providers said they offer a combination of branded and generic drugs. These providers said prescribing decisions are primarily based on insurance, followed by patient need. Some also discussed the role advertising plays in prescribing, particularly as Truvada went generic and Descovy gained FDA approval for PrEP and was marketed heavily in certain markets. They noted patients would come in asking for Descovy by name and some spoke of educating patients on the clinical and monetary value of staying on Truvada or its generic equivalent after patients approached them with requests for Descovy, having seen advertising for it. Some had patients come in already on Descovy and some providers did similar education on generics/Truvada if they did not believe Descovy was clinically indicated.
One respondent mentioned the benefits of California SB 159 to their company as it allows their providers to prescribe more freely. SB 159 requires private health insurance (except for employer based self-insured plans) to cover medications without step therapy, which usually requires patients try a lower cost or generic drug before a more expensive or brand drug, or prior authorization unless there is a generic equivalent. Similarly, they noted Texas SB 680 which also prohibits payers from overriding provider decisions in certain scenarios.
Two private tele-PrEP providers using the CBO hybrid model report that the majority of their patients are on branded drugs and largely on Descovy. One of which reported that 95% of patients are on brand drugs and the other that 75%-80% of clients are on brand drugs. They note that brand drugs and the 340B revenue that can be generated from them for CBOs form the base of their business model. Two other telehealth companies primarily or exclusively provide generic PrEP. One runs their own pharmacy in house, which they generate revenue from, and the other uses a cash pay model and has negotiated a discounted rate through their contracted pharmacy for a generic. Both discussed educating patients on the role of generics.
The California state program requires uninsured clients requesting Descovy or Truvada to go through the manufacturer assistance program, noting most clients get branded drugs through the assistance program, rather than a generic through the state program. The Iowa program, which does leverage the 340B program, prescribes both brands and generics.
Those associated with 340B entities believed generics coming to the market had impacted revenue somewhat but not to a significant degree, noting that for many clients, they were able to continue to fill brand prescriptions to generate savings.
Planning for Long-Acting Injectable PrEP
Apretude, the new long-acting injectable medication for PrEP, was approved by the FDA towards the end of the interviews conducted for this project but not yet available for patients. Respondents were asked whether they were planning to incorporate the option into their business model and the about the conversations they were having with their patients regarding the drug. Most were unsure of how a provider administered injectable fit into the tele-health landscape but were actively trying to assess opportunities. Those with connections to CBOs and programs located within brick-and-mortar clinics appeared further along in the thought process, but many questions and potential barriers remain. Tele-PrEP providers with other models were considering whether they could coordinate with pharmacies to deliver the medication, though they recognized that those pharmacies would have to stock the drug.
Respondents predicted that the new PrEP option would likely require prior authorizations by most payers and believed that this might mean additional workload for their staff. However, some noted that they already had a team experienced in dealing with prior authorizations who were well positioned to handle it.
One provider from a brick-and-mortar clinic looked back on their experiences with injectable HIV treatment, noting key challenges with that roll out that they hoped would not be replicated in the injectable PrEP space, but feared might be. These challenges largely centered on insurers covering the medication as a medical benefit and not pharmacy benefit which meant the clinic had to have the drug onsite (and purchase it in advance) and then bill the insurer after it was administered. There were significant delays in reimbursement, especially at first as claims were getting rejected for the expensive medications. They also worried about equity, not wanting to be in a position of only making the injectable option available to people who have certain types of insurance.
Others though, were more pessimistic at the idea of incorporating a provider administered injectable into the tele-PrEP space saying that “it is hard to inject people through the screen.” Providers in this group said they were updating provider education as they recognized patients would potentially be asking about the option.
Marketing
Respondents reported varied approaches to marketing which can play an important role in the growth of these programs. Private companies tend to place the most emphasis on advertisingand commonly did so on dating apps aimed at men who have sex with men such as Grindr, Scruff, and Jack’d. Others, particularly those that have service lines beyond PrEP, advertise on sites like Tinder as well. These companies also use social media, including Facebook and Instagram, to advertise and generate content. Some also use Google ads. Two companies also report using influencers and hosting events/parties as forms of advertising, though one has said that this has slowed down given the pandemic. Beyond private companies, the Iowa program advertises using radio, Google ads, dating apps targeting men, and billboards in more rural areas and one clinic conducts social media advertising and develops YouTube videos. Another clinic receives referrals as a vetted PrEP provider promoted by their city health department which conducts advertising such as on the subway.
Other providers were not doing a lot of advertising and reported that most clients found out about their programs by word of mouth. Most in this group believe their programs might have higher uptake with more advertising. The California program for instance thought low uptake of their services may have been at least in part tied to limited advertising. One provider from a rural southern state expressed frustration with how difficult marketing has been for them due to a limited budget and barriers in trying to promote the tele-PrEP program through dating apps in a socially conservative state and clinical environment.
Support Services
Adherence support
Providers utilize different measures to encourage adherence and to ensure that patients get their labs and set up quarterly appointments. Some report those tools to encourage lab and visit maintenance are built into their platform, others send out a survey after three months to assess whether there are any important changes, and some rely on case managers, medical or physician assistant students, or pharmacists to promote lab and visit follow-ups and medication adherence and monitoring. The Iowa program explained they sometimes purchase adherence tools for those who need them such as key chain pill holders, travel pill cases, and timed bottle tops. Despite these efforts, challenges with adherence were common (see barriers section). However, some noted that adherence with PrEP is sometimes difficult to assess as it is not always clear if a patient has stopped PrEP but is still in need of it or stopped PrEP due to decreased risk, which would be clinically appropriate.
Linkage
Whether respondents can treat HIV or another STI detected through monitoring depends on the type of diagnosis and the infrastructure of the program. Most respondents report being able to treat STIs, such as chlamydia or gonorrhea, that require only a prescription pill. Of the two that did not, one is a CBO hybrid that refers individuals to its CBO partners, and the other is the Iowa state program which connects individuals to state disease intervention specialists. All report a process for connecting people who are diagnosed with HIV and other STIs to care. Some utilize existing CBO relationships and others describe a more manual process of connecting patients to HIV care. The degree of support offered in linkage for STI or HIV treatment appears to vary, while some respondents state only linking patients to local health departments or CBOs, others describe continuing to follow-up with the patient to ensure linkage and treatment was completed.
Some programs take care of patients diagnosed with HIV in-house, namely those connected to a hospital system or clinic, though three telehealth companies report they are seeking to expand service offerings into HIV care in the future. One telehealth company currently has a small HIV treatment and support cohort.
Other support services and linkages
Some respondents also reported providing other support and linkage services, including those related to mental health issues, substance use disorder treatment, and partner services. One telehealth company, the one with a small HIV care cohort, described a virtual support group for people with HIV which is open to those both within and outside of the cohort.
Financial and health insurance assistance
Most respondents enroll patients in pharmaceutical medication assistance or copay programs, as needed, including both the California and Iowa state programs. Most say they have used Gilead’s Advancing Access Program, designed for this purpose. A few have also used the federal Ready Set PrEP Program, which also provides free PrEP to uninsured people. The provider using the cash model does not use these programs and one small hospital-based program was unaware of them prior to the interview. In addition to PrEP specific assistance programs, several respondents report working to help enroll clients in insurance coverage for which they are eligible, including Medicaid but more often, ACA individual marketplace plans. ACA plan enrollment became more appealing after it was made clear the United States Preventive Services Task Force’s (USPSTF) “A” grade for PrEP means that most people with private insurance should have access to PrEP medication and services without cost-sharing (see box on USPSTF PrEP Guidance.)
Providers
Diverse types of clinicians staff tele-PrEP programs. In two cases, medical doctors lead all tele-PrEP work. In most cases, teams were led by either advanced practice nurses or pharmacists with one or a small number of supervising physicians. Two of the programs are fully led and staffed by advance practice nurses. In one case, the team was an even mix of advance practice nurses and doctors.
The tele-PrEP companies all provided services across multiple states and noted that having providers licensed in multiple states was important to their business model. Some saw their ability to facilitate multistate licensing for clinicians as a workplace incentive.
Providers are often supported by other staff such as navigators, counselors, and physician assistance to help with insurance enrollment, work on prior authorization or deal with other insurance issues. In most cases it is also this support staff work with patients on adherence, technical issues, and linkage to other care needs. Sometimes there is also coordination with other public health workers (see section on partnerships below).
Services
The services offered by tele-PrEP providers ranged from those focused exclusively on PrEP to those that provide PrEP within a broader array of services. (See Table 2.) Among those interviewed, two private companies and two hospital-based programs —limit their offerings to PrEP and related services. While the Iowa program is focused on PrEP, it provides linkages to other services. The California program has a list of allowable services that can be covered by the state program for uninsured clients. Two private companies offered PrEP alongside a few other select services. One company also offered contraception, STI testing and treatment (when not physician administered), post-exposure prophylaxis (PEP), acne services, anti-aging services, and migraine services. This company is the one with the small pilot HIV care and support cohort mentioned above. They are also exploring adding mental health, certain urgent care services (e.g. treatment for UTIs and yeast infections), and routine care in the future. The other company offering select services alongside PrEP, provides gender affirming hormone therapy (their specialty focus), erectile medication, and is looking to expand into virtual primary care, fertility, and behavioral health in the future. At the other end of the spectrum, PrEP is just one of a large range of comprehensive health services offered which was the case for one telehealth company and two clinic-based programs.
Among those providing more comprehensive services, the degree to which PrEP delivery was integrated into other care offerings varied. A respondent from one tele-PrEP company stated that while they have fairly comprehensive primary care offerings, their PrEP users tend to have low health needs and only use their PrEP services.
Some though, including the Iowa state program and one clinic, saw PrEP as integrated into their other services and/or as a way to get patients into primary care. Iowa saw potential in their stand-alone tele-PrEP program as being a “gateway” to other in-person health services.
Table 5: Service Offerings Among Tele-PrEP Providers
PrEP Only
PrEP and Select Services Only(e.g. PrEP and a handful of other select services)
Comprehensive Service Offerings(e.g. PrEP and a broad range of primary care services)
2 private companies
(both hybrid companies with CBO connections)
2 private companies(both standalone companies, not connected to CBOs)
1 private company(a standalone companies, not connected to CBOs)
2 clinical programs
—
2 clinical programs
2 state programs
—
—
Why Tele-PrEP?
Interviewees offered a range of reasons for providing tele-PrEP that generally aligned with why they believed patients sought out these services. For many, providing wider access to PrEP was specifically the aim of their program and some tied this objective to reaching the goal of “ending the HIV epidemic.” Private companies, state programs, and clinics alike expressed this view. While private companies sought to profit from PrEP delivery, particularly those companies that only provided PrEP or provided PrEP alongside only a handful of other services, representatives generally still expressed a mission driven focus rather than a financial one.
In some cases, broadening access to PrEP through telehealth was viewed as a way to address specific barriers such as stigma, time off, and transportation, among others. Others saw providing telehealth services as a way to stay relevant in a changing health care landscape, while reaching an underserved population, particularly when the existing approaches were not working for certain groups. One clinical program started offering telehealth services, including tele-PrEP, in response to the pandemic (see section on COVID-19).
Who is being served?
Most respondents aim to serve a broad range of PrEP clients, but a few focus on specific communities. One of the tele-PrEP companies specializes in serving the LGBTQ+ community and one of the hospital clinics focuses on serving young people. An additional provider has a relationship with a residential substance use treatment facility and provides tele-PrEP services to that population. Except where noted, client demographics of PrEP users at national companies did not differ much from those in clinical or state programs.
Region
Of the five national tele-PrEP companies, three served clients in all 50 states and DC (at least one of which also served Puerto Rico). One served clients in about half of states and one served clients in about two-thirds of states; both of these companies report they are continuing to add states to their network. Several companies stated that the largest share of their clients came from California. Texas, Florida, Georgia, and New York. Respondents noted that the states where most clients originate from track with population density and HIV prevalence. Other respondents focus their services on a single state due to the location of a clinic or state program and are unable to serve those outside the state through telehealth due to policy restrictions.
PrEP providers generally stated that while most of their clients were from urban areas, they have rural clients as well and see tele-PrEP playing an especially important role for these individuals who may face more stigma or have fewer local options for accessing PrEP in-person. However, some reflected that while telehealth is often discussed as a way to reach those in rural settings, the need for telehealth crosses the urban-rural divide.
Spotlight on Tele-PrEP in California
This box provides a spotlight on tele-PrEP provision in California, including specific issues identified by respondents. We focus on California given that the state has the largest number of PrEP users in the U.S. and was identified by tele-PrEP companies in this study as their largest or among their largest market(s). Additionally, California’s PrEP policy environment is evolving due to changes in state legislation and changes within the tele-PrEP Program.
***
The California tele-PrEP program was launched in the fall of 2019 and is part of the state’s PrEP Assistance Program (PrEP-AP), which provides PrEP, PrEP related services (e.g. labs) and certain other allowable services (e.g. STI treatment). While the tele-PrEP piece of the program is provided through remote access, clients must first enroll in-person at one of several hundred enrollment sites throughout the state before they can qualify, a requirement which may pose a barrier to some clients. In addition, clients must re-enroll annually, since they need to be re-screened for eligibility. The program is largely geared towards uninsured clients, though those who are privately insured can also use it as long as the provider seen is in-network with the client’s insurance company. For those with coverage, the program can cover copays. However, there is less need for assistance with PrEP specific services given new USPSTF guidance requiring PrEP related services be covered without cost-sharing (see also, box on USPSTF and PrEP). In addition, the state will consider some program clients as uninsured for confidentiality reasons (e.g. so as not to disclose PrEP use to a parent or spouse) to promote access for these groups.
When created, the tele-PrEP element of the PrEP-AP program was outsourced to a national tele-health company offering synchronous tele-PrEP services and using brick-and-mortar labs (as opposed to at-home lab kits). Uptake of that program is reported to have been limited. While it is unclear why uptake was so limited, one explanation offered was that there had been little advertising. When the state’s contract with the company expired at the end of 2021, it was not renewed for undisclosed reasons.
As of January 2022, state tele-PrEP services are delivered by three California based community-based organizations (CBOs) through an arrangement with the state. It is unclear how or if patients were notified of the change in vendors or if there were any clients enrolled at the end of 2021 to notify. While the three CBOs are physically situated in three locations, they can see patients from across the state virtually and are loosely assigned to geographic regions (i.e. Northern, Central, and Southern California, and the Los Angeles area). How tele-PrEP is now delivered (e.g. synchronously or asynchronously) is based on the system for telehealth delivery already in place at the partner CBO. Similarly, whether at-home labs are offered is driven by CBO protocol as are the panel of labs run. Prescriptions must be picked up at a pharmacy contracted with Magellan, the state’s pharmacy benefits manager, though some pharmacies offer home delivery through other vendors. In general, generics are provided and if a client requests or requires a brand name, Truvada or Descovy, they must go through the manufacturer assistance program. Most clients get branded drugs through the industry assistance program rather than a generic through the state program.
In addition to the above-described models for the state’s tele-PrEP providers, the state PrEP-AP program also permitted their in-person PrEP providers to see PrEP clients virtually because of the COVID-19 pandemic.
One respondent providing tele-PrEP to young people in the state discussed the value of having access to a range of California based safety net payers and programs to help ensure robust and discrete access including Medicaid expansion, the Family PACT program, ACA enrollments, and the state PrEP-AP program. They contrasted this experience with states without Medicaid expansion and more limited support systems.
Key issues identified in the interviews as impacting tele-PrEP provision in the state of California are as follows:
CA law SB-159 requires private health insurers (except for employer-based, self-insured plans) to cover medications without step therapy or prior authorization unless there is a generic equivalent. In the PrEP space this would mean providers are free to prescribe Descovy (which does not have a generic equivalent) without facing medication management barriers. One respondent from a tele-PrEP company noted this California law made prescribing Descovy easier in the state which happens to be their largest market.
CA law SB-306 requires health plans to provide coverage for home collection kits for HIV and other STIs testing deemed medically necessary or appropriate and ordered according to the law, making home collection more affordable. This is an important step towards access as in other parts of the country, respondents noted it is difficult to get reimbursement for home collection kits. However, reimbursement challenges remain for implementing the policy in Medicaid due to a lack of procedural codes. Implementation barriers also exist for private health plans as some may not be covering both the kit and the lab costs. There may also be coverage challenges if the labs used by tele-PrEP providers are not in-network with client insurance plans. Solutions to this barrier are being explored by advocates and industry.
Several private companies cited challenges with contracting with Medicaid as a reason they did not accept this form of coverage and one respondent specifically cited California as presenting particular challenges given its large number of Medicaid Managed Care Organizations. However, a separate respondent from a private company with similar concerns about the challenges in contracting with Medicaid stated that California is one of only handful of states where they do accept Medicaid clients and bill the program.
Numbers served
The number of PrEP clients being served varied significantly across respondents and not all provided a number or range. The national telehealth companies offering numbers each said they served thousands of clients. State and clinical programs tended to serve fewer clients, some with just 20 active clients. However, one clinical provider said that they served about one thousand clients exclusively through tele-PrEP, one thousand through their in-person option and an additional thousand patients though a hybrid of in-person PrEP and tele-PrEP. Collectively, the organizations included in this analysis are estimated to provide tele-PrEP services to over ten thousand clients.
Gender identity and Sexual Orientation
Respondents report primarily serving cisgender men, who typically made up about 90% or more of a patient population. Clients are largely LGBTQ+, though one respondent whose client population is 98% male said 19% do not identify as gay. Some said that the remaining share served were women and others said it was a mix of women and transgender clients. One respondent reported primarily serving transgender and nonbinary clients. The tele-PrEP provider with a satellite program had the largest share of women among their clients (25%) and believed that was possible because of the personal rapport they had built with these clients over time.
Race/ethnicity
Fewer than half of respondents were able to estimate the race/ethnicity makeup of their client population, though some said they plan to collect this data in the future. Among the four that provided specific estimates, between 23% and 55% of their patient populations were people of color. Most said this group primarily included Black and Hispanic people but one provider reported that 20-30% of their clients have Asian ethnicity. One national tele-PrEP company said that in California and Florida they primarily serve Latino people but in every other state White clients make up the largest racial/ethnic group of clients. Nationally, 61% of PrEP users were White in 2019 and there is higher unmet need for PrEP among people of color.
Age
Most providers report that their patients are typically in their 20s and 30s or gave an average or median age in the late 20s. A few said they also commonly served clients in their 40s. Most said that aside from these averages, they had clients in younger and older stages of life. One respondent’s clinical program serves only teens and young adults. Most respondents said that they were able to assist clients under 18 but had few or no clients in that age group. One respondent from a national company said they were not able to provide services to those under 18 due to policies at partner organizations.
Insurance
Insurance coverage distribution among clients ranged significantly by type of tele-PrEP provider and was tied closely to business models. Some private programs were cash pay or private insurance only, whereas others welcomed those who were uninsured or covered by Medicaid, typically clinics and some private companies. As noted earlier one private company only took Medicaid clients in handful of states (California, Texas, New York, and Illinois). Others treated those with Medicaid as uninsured rather than navigate those state programs. As noted, several programs report offering insurance enrollment assistance. The California program is generally for the uninsured population but a privately insured patient can use the services if one of the community partners is in their insurance network. The program will also treat some clients using the program for confidentiality reasons (e.g. so as not to disclose PrEP use to parents or a spouse) as uninsured. The Iowa program serves people with any type of insurance and most (about 70%) of clients have private coverage.
Facilitators
Respondents identified a variety of factors that support them in their ability to offer tele-PrEP or help patients stay engaged.
Staffing: Several respondents spoke of how their case management or support teams were essential to engaging clients, working through insurance barriers, enrolling clients in assistance programs, and insurance coverage and promoting retention. One respondent mentioned the importance of having a diverse group of clinicians that speak multiple languages. Another saw significant value in their program being staffed by pharmacists working at the top of their licensure.
Streamlining: Respondents discussed how the more they streamlined the process for patients, the easier it was for patients to engage. For example, when one organization launched their program, they would take full sexual history at enrollment, but moved away from the practice when they realized it deterred patients when asked to share that information upfront. Respondents also noted that it was important to see patients as soon as possible after they expressed interest and that the longer time between initial engagement and first appointment, the higher the probability of them not showing up to those appointments.
Partnerships: Several respondents spoke of formal and informal partnerships that made their programs more successful, including bringing in new PrEP patients and linking patients to services outside their programs. The Iowa program relies on linkages with their STI and HIV programs and their disease intervention specialists (DIS) who assess PrEP interest as standard procedure and provide referrals to the program. Two other programs (one clinic based and one private telehealth company) reported receiving referrals from the state. Others work with local Planned Parenthood or Title X providers to get labs for patients without insurance. One California provider also relies on wrap around support from the state family PACT program. Another provider running a hospital telehealth program gets support from an HIV specialty pharmacist in another program and receives patient referrals from a local substance use treatment center.
Other Facilitators Discussed Elsewhere in the Report
Asynchronous/Synchronous models (respondents differed in their beliefs as to which was more of a facilitator, with some preferring a hybrid approach)
Multi-state licensing for providers
Marketing
Insurance (ACA and Medicaid) Enrollment
Multi-month prescribing
USPSTF – “A” grade and subsequent guidance
Rapid Starts (for PrEP and for people diagnosed with HIV)
Using home labs for 3-site STI testing when not available at in-person settings
Barriers
Respondents also identified factors that made offering tele-PrEP or helping patients stay engaged more challenging.
Insurance: Issues related to working with insurance were the most frequently cited barriers. Respondents described reimbursement challenges for at-home self-collect labs with Medicaid and private insurance. Lack of billing codes for at-home self-collect tests has been especially challenging with respect to Medicaid and it appears not all private plans are reimbursing for both the test kit and the laboratory service. There are also challenges when the labs used for home collection are not in-network with insurance. Respondents also stated that some patients are still getting billed for labs and associated provider visits that should be covered without cost-sharing by their plans under USPSTF guidelines (see box on USPSTF guidelines). Finding ways to cover services for young privately insured patients who are still on their parents’ insurance but do not want to use their parents’ insurance for confidentiality reasons, was another barrier mentioned. Several respondents discussed that regulations around Medicaid were a barrier, including having to navigate state-by-state policies and low reimbursement rates. One respondent from a private company cited the large number of managed care organizations in the California Medicaid program as an example of how challenging contracting with Medicaid could be. Another private company takes Medicaid clients only in California, New York, Texas, and Illinois because contracting with Medicaid programs in all states would be too cumbersome. In fact, some companies considered Medicaid patients to be uninsured for the purposes of billing and reimbursement.
State Telehealth and Provider Credentialing Laws: Several respondents discussed limitations on provider credentialing that varied by state and one respondent mentioned there are some challenges with state regulations requiring oversight for physician assistants. Recruiting clinicians with multistate licenses also proved to be a barrier for some. One respondent mentioned that 12 states do not allow for asynchronous telehealth, which makes their asynchronous model of providing care through texting and e-mailing a challenge and will require them to adapt how they deliver tele-PrEP in those regions.
Tele-PrEP Uptake and Patient Awareness: A few of the smaller, clinically based providers had fairly low program uptake (i.e. fewer than 20 clients). These tended to be the providers that put less of an emphasis on advertising and without a significant presence in the HIV/LGBTQ+ community. The California state program also had low enrollment by the end of last year. One respondent stated that many patients are not aware that PrEP exists, especially women, or that they are unaware of where to get PrEP. This same respondent discussed difficulties in reaching the people through advertising.
Retention: Many respondents discussed challenges retaining patients, even after accounting for clinically appropriate attrition (e.g. a patient cycles off of PrEP because they are no longer at higher risk for HIV). One respondent explained that retention for women is more difficult than retention for men. A number of respondents had relatively high retention rates for one additional refill, but then found that patients dropped off afterwards. One respondent said patients typically stay for two or three months. Of the three respondents that shared longer term retention rates those ranged from 40%–“80% or 85%” which is comparable to rates reported for in-person PrEP. One respondent mentioned that while patients may appropriately go on a pause, some do not restart when they should or they may have exhausted their supply of meds and not have some on hand when they are ready to restart.
Other Barriers Discussed Elsewhere in the Report
NY state has limitations on self-collection testing and does not permit in-person three-site chlamydia and gonorrhea testing at in-person labs
Plans and pharmacies that have limitations around multi-month prescribing
Changes to the Gilead assistance program – uninsured patients no longer generating 340B savings
Knowledge limitations with assistance programs and USPSTF guidance, especially with smaller providers
Private insurance non-compliance with federal guidance on USPSTF prohibiting cost-sharing for PrEP related services.
CDC’s newest HIV screening recommendations include an HIV RNA testing which can be costly and is not currently available for home test kits
Challenges with home testing for syphilis – may detect past infections
Testing every three months for patients on PrEP can be seen as onerous
Reaching women
The COVID-19 Pandemic
The COVID-19 pandemic provided opportunities for some of the larger tele-PrEP companies to expand and accelerate their tele-PrEP offerings. As noted earlier, none of the private companies or state programs attributed the pandemic with the reason for launching their tele-PrEP programs, but one clinical program started theirs in response to the pandemic. Also, in addition to the tele-PrEP program, the California PrEP-AP program allowed their typically in-person providers to see PrEP clients virtually during and because of the COVID-19 pandemic. Multiple respondents described the proliferation and shift to telehealth as the silver lining of the pandemic.
Respondents also explained how the COVID-19 pandemic shifted patients’ perspectives and preferences for care. One company explained that when PrEP clinics were closed early in the pandemic and patients could not get in for their labs or refills, they turned to tele-PrEP. Then when clinics reopened, clients decided they preferred tele-PrEP over going into the clinic.
However, other smaller programs or hospital-based programs, especially the program that provides satellite tele-PrEP services, did not see an increase in clients due to the pandemic. Some of these programs had to shift to focusing on COVID and tele-PrEP became less of a priority.
Conclusion
In this analysis, we provide a first look at the growing area of PrEP provision through telehealth. We find there is significant variation in how tele-PrEP providers run their programs, differences that may have implications for both patient access as well as long-term sustainability. For example, some programs are exclusively PrEP focused, free to patients, and rely on income generated from 340B savings to form their business model. Others offer a range of services beyond PrEP and charge clients a fee or generate additional revenue from their own pharmacy. Despite these differences, and although some stand to profit from their businesses, tele-PrEP providers have the common goal of broadening PrEP access through a new modality and believe they are solving access barriers to PrEP, for at least some clients. Respondents discussed policy areas that stand to bolster or limit the success of these programs. Policy areas that hamper tele-PrEP success include challenges with insurance coverage (e.g. lack of coverage for home lab collection, limitations on multi-month prescribing, non-compliance with the USPSTF guidance, etc.), laws that make interstate practice/licensing cumbersome with respect to conducting telehealth sessions, and barriers to self-collect labs. Policies and practices identified that bolster tele-PrEP include leveraging staff skill sets to aid in patient engagement, streamlining programs, developing partnerships, advertising, supporting multistate licensing for staff, ACA enrollment, and private plans that are adhering to new USPSTF PrEP guidelines. While few respondents started their programs in response to COVID-19, tele-PrEP providers largely agreed that their ability to promote and scale their programs has been enhanced because of a national shift embracing telehealth in response to the global pandemic. These findings suggest that tele-PrEP may offer an additional or alternative avenue for accessing PrEP services, which may be especially notable as efforts to “end HIV” in the US hinge, in part, on increased PrEP uptake.
Table 6: Characteristics of Tele-PrEP Providers in the Study
Provider
Model
Primarily Synchronous, Asynchronous, Hybrid
Labs
Fees and Costs
Insurance
Pharmacy Preference
Rx Preferences
Provider 1
Private Company/CBO Hybrid
Hybrid
98% home collection and 2% use Quest or LabCorp.
None
70% privately insured.
Available to insured and uninsured people. Those with Medicaid and Medicare treated as uninsured.
Mail-order pharmacy associated with company and registered with CBO
95% branded (mostly Descovy) and 5% generic
Provider 2
Private Company/ CBO Hybrid
Hybrid
90% home collection and 10% use Quest of LabCorp
None
45% privately insured.
Available to insured and uninsured people. Those with Medicaid and Medicare treated as uninsured.
Mail-order pharmacy associated with company and registered with CBO
75%-80% branded (“lean Descovy”), 20%-25% generic
Provider 3
Private Company
Asynchronous
Home collection kit unless insurance mandates commercial lab.
Fee: $15 every three months.
Labs and Medications not covered by insurance.
Mostly private insurance, 7% cash pay. Medicaid patients accepted in Texas, New York, California and Illinois only.
Company pharmacy
90% generics and 10% brand (typically when insurance driven or clinically appropriate)
Provider 4
Private Company
Synchronous
Commercial labs, largely Quest and LabCorp.
Fee: $15 per month and $59 every three months for PrEP visit.
Labs and Medications not covered by insurance
Private insurance and cash pay only.
Mostly brick-and-mortar.
Unknown
Provider 5
Private Company
Hybrid
About half do home collection and half go to Quest.
Fee: $70-$100 per month inclusive of visit, lab, and Rx
None
Contracted pharmacy
All generics from preferred vendor.
Provider 6
Clinic Based
Synchronous
All labs done in the community.
None for the uninsured.Costs for the insured relate to insurance (unclear about USPSTF implementation)
Benefits from using 340B pharmacy but most patients use commercial pharmacies
Mostly on generics or Truvada.
Provider 7
Clinic Based
Synchronous
Most prefer commercial labs to home collection but will send 3-site collection kits to those who get other initial labs in person.
None for the uninsured. Insurance covers for others, team helps patient fight any cost-sharing (per USPSTF guidance.)
About half are privately insured, another about 20%- 30% are privately insured but can’t use it because it’s under their parents policies.
Most use brick-and-mortar pharmacies but “a lot are interested in mail-order.”
Mostly on generics or Truvada.
Provider 8
Clinic Based
Synchronous
Community based, including at regional hospital hubs, exploring home collection option.
Reduced pricing for the uninsured through hospital uninsured program (60%-65% off). Insurance used for the others.
Available to those with any insurance and the uninsured.
Wherever convenient for patient.
Truvada, Descovy, Generics – guided by insurance.
Provider 9
Clinic Based
Synchronous/Satellite
Mostly test in house at satellite locations. Some COVID home collection, but minimal.
$30 fee for uninsured patients.
Private and public insurance is accepted. The uninsured are seen for a fee.
In-house pharmacy.
Brand and generics prescribed.
Provider 10
Iowa State Program
Synchronous
Largely going to brick-and-mortar. A few pay cash for home collection. Developing own home test kit.
No program fees, possible lab fee of $5-$10 for the uninsured that can be waived.
70% private, 10% uninsured.
Preference their own pharmacy or partner pharmacy.
Brand and generics prescribed.
Provider 11
California State Program
Unclear now (previously synchronous video)
Follows community partner protocol.
Follows community partner protocol but most clients receive in person labs.
Generally, for uninsured population but a privately insured patient can use the services if one of the community partners is in a network. Patients using the service for confidentiality reasons are treated as uninsured.
Preferred state pharmacy network.
Uninsured clients requesting Descovy or Truvada must go through the manufacturer assistance program.
This work was supported in part by the California HIV/AIDS Policy Research Center (CHPRC) with APLA Health acting as fiscal intermediary.CHPRC/APLA Health also provided feedback on the final version of this report.
We value our funders. KFF maintains full editorial control over all of its policy analysis, polling, and journalism activities.
The 6th company did not respond to repeated requests for interviews. We identified a 7th company that was not included in the initial sampling frame. ↩︎
The Title X National Family Planning Program, administered by the U.S. Department of Health and Human Services (HHS), Office of Population Affairs (OPA), is the only federal program dedicated solely to supporting the delivery of family planning and related preventive health care. In return for federal support, the Title X program requires that its grantees meet very specific performance criteria. In addition to providing women, men, and teens with a broad range of contraceptive services and supplies and other preventive, screening, and treatment services, Title X grantee clinics must follow special federal confidentiality protections and are expected to adhere to national Quality Family Planning Guidelines (QFP). ↩︎
In 2020, only 25% of people who could benefit from pre-exposure prophylaxis (PrEP), a medication that reduces the risk of acquiring HIV, were prescribed it. Using telehealth to provide PrEP, “tele-PrEP,” is a new approach that shows potential for expanding access to PrEP use in the United States that predates the COVID-19 pandemic.
A new KFF analysis takes a deep dive into the tele-PrEP landscape, from the types of providers offering the service to the successes of the modality and the barriers that remain. Drawing from in-depth interviews with representatives from major telehealth companies who offer PrEP, as well as other types of providers, the KFF study finds a range of models are being utilized to provide the service, and considerable variation in tele-PrEP delivery approaches by provider. These differences have implications for clients, providers, and businesses.
While tele-PrEP offers an additional avenue for accessing services for some, questions remain about its potential to overcome barriers relating to insurance and the role it can play in increasing uptake and addressing persistent disparities in utilization.
The growth in Medicare spending is a federal budget issue and also a pocketbook issue for beneficiaries. The rise in Medicare spending has contributed to a rise in Medicare premiums and deductibles as a share of Social Security income over the past two decades. Between 2002 and 2022, Medicare Part B premiums alone increased from 6% to 10% of the average Social Security benefit. Adding in Part A and Part B deductibles for hospital and physician services, these costs combined have increased from 15% of the average Social Security benefit in 2002 to 19% in 2022.
The Medicare Trustees project that Medicare premiums and cost sharing will account for an increasing share of Social Security benefits in the future. While most beneficiaries have other sources of income in addition to Social Security that are not factored into these estimates, they also incur additional out-of-pocket costs for other health-related expenses, such as prescription drugs, cost sharing for physician visits, and costs for services not covered by Medicare, such as dental care and long-term services and supports.
There are persistent disparities in health and health care for people of color, which reflect structural and systemic inequities rooted in racism and discrimination. Inadequate, incomplete, and inconsistent race/ethnicity data is a longstanding challenge across many areas of health care. High-quality comprehensive data are key to enabling policymakers, community leaders, and other key stakeholders to identify and address these inequities and measure progress over time.
Medicaid and the Children’s Health Insurance Program (CHIP) provide health care coverage to low-income adults and children, and play a disproportionately large role in covering people of color, people experiencing poverty, individuals with limited English proficiency, and those who live at intersections of these characteristics. Medicaid/CHIP administrative data, also known as Transformed Medicaid Statistical Information System (T-MSIS) or TAF (T-MSIS Analytic File), hold the potential to inform disparities research through detailed demographic, service utilization, and spending data of Medicaid and CHIP beneficiaries —but there are current limitations. Key demographic variables, particularly race and ethnicity, vary in completeness and quality, raising questions about data usability and reliability. These quality issues may impede T-MSIS analytic file users’ abilities to understand racial and ethnic disparities and advance health equity among Medicaid and CHIP beneficiaries. In this issue brief, we use the Medicaid DQ Atlas and T-MSIS analytic files to examine the data quality of race/ethnicity and other demographic variables in calendar year (CY) 2019 T-MSIS data.
What is T-MSIS?
T-MSIS Analytic Files (TAF) provide beneficiary-level data including health care use, demographics, and enrollment data for Medicaid and CHIP enrollees in all 50 states, District of Columbia, Puerto Rico, Guam, and Virgin Islands. T-MSIS replaced the Medicaid Statistical Information System (MSIS) by 2016 and analytic files became available to researchers in Fall 2019. T-MSIS builds on data collected in MSIS to include: enhanced information about beneficiary eligibility; beneficiary demographics; provider data; fee-for-service and managed care service utilization; expenditure data for Medicaid and CHIP; and more. However, quality issues limit its full potential.
Variation of state data collection, naming, and categorization procedures, as well as state-specific data challenges contribute to T-MSIS quality issues. While federal requirements mandate some aspects of coverage and operation of Medicaid and CHIP programs, states have a great deal of flexibility in implementation and administration of their state’s program. This variation is reflected in state data systems, with each state collecting, categorizing, and storing data somewhat differently. For example, states vary in the number of categories they use to collect race/ethnicity data, as well as how these variables are named and combined to create aggregated race/ethnicity categories that conform to federal Office of Management and Budget (OMB) racial and ethnic data reporting standards. Furthermore, each state may individually have its own data quality problems, which, if left unnoticed or unresolved, may affect T-MSIS data quality unless they are caught by CMS’s efforts to improve data quality.
How do states collect race/ethnicity and how are these data presented in T-MSIS analytic files?
All Medicaid/CHIP agencies ask applicants to self-report their race and ethnicity, but it is not mandatory for applicants to do so. During Medicaid or CHIP eligibility determinations, race and ethnicity are not considered, and data not being used in Medicaid determinations must remain optional for applicants to report. States must indicate that submitting race/ethnicity data is optional, but this can lead to missing data, particularly if the instructions and rationale for providing race/ethnicity data are unclear, if the applicant has concerns or questions about how the data may be used, or if they do not feel they fit into one of the options provided.
The categories of race and ethnicity variables on Medicaid applications vary considerably across states. At a minimum, states are required to comply with 1997 OMB guidelines for race (5 categories) and ethnicity (2 categories) reporting standards, but can opt to collect more detailed data if it can be consolidated into the minimum reporting categories. An audit of state Medicaid enrollment applications conducted by State Health Access Data Assistance Center (SHADAC) revealed substantial variation in the number and type of race/ethnicity categories used by states, ranging from 5 to 37 race categories and 2 to 8 ethnicity categories. Since some states presented one set of categories in the online version of the application and a different set in the paper applications, the audit identified 62 unique race categories across the 50 states included in the analysis.
States also vary in the instructions and rationale provided to beneficiaries for reporting race/ethnicity data. Below, we highlight select examples of these instructions from SHADAC’s review of Medicaid applications:
You don’t have to answer this question. In most cases, your answer won’t be used to make a decision. But, if this person is American Indian or Alaska Native, telling us here may help this person get the most help possible.” – Florida’s Medicaid application instructions
“Providing your race and ethnicity can be helpful since it can speed up the application process. It may be used to automatically create your case.” – Delaware’s Medicaid application instructions
Given the substantial differences in how states collect data on race and ethnicity, CMS provides technical instructions to states about reporting race and ethnicity when submitting T-MSIS data. T-MSIS race and ethnicity data elements align with the 2011 HHS data standards. These categories may be more granular than some states’ Medicaid applications since states are only required to collect the less granular OMB standard values, though that is not always the case. Current OMB guidelines define ethnicity in two categories and race in five categories. The more detailed HHS standards reports race in 14 categories and ethnicity in five categories (Table 1).
The race and ethnicity data that states submit to T-MSIS are then converted into several key race and/or ethnicity variables available to researchers in the T-MSIS analytic files (TAF). Variables available to TAF users include: 1) a constructed seven-category combined race and Hispanic ethnicity variable (White, non-Hispanic; Black, non-Hispanic; Asian, non-Hispanic; American Indian and Alaska Native (AIAN), non-Hispanic; Hawaiian/Pacific Islander; Multiracial, non-Hispanic; Hispanic, all races); 2) a six-category Hispanic ethnicity variable; and 3) a disaggregated, constructed 20-category combined race and ethnicity variable, which includes seven ethnic categories for people of Asian descent, and four ethnic categories for Native Hawaiian and Pacific Islander people, in addition to the broader race and Hispanic ethnicity categories. The TAF does not include a variable that reports race solely.
How reliable are the T-MSIS race/ethnicity data?
To help TAF users evaluate the data quality of various measures, the Data Quality Atlas (DQ Atlas) was developed as a companion to T-MSIS data. The DQ Atlas, which is available for each year and release of data, provides data quality information about some, but not all, of the variables available in T-MSIS analytic files. One key data element the DQ Atlas provides is usability measures on race/ethnicity data. The DQ Atlas evaluates the completeness of race and ethnicity information in the T-MSIS analytic files and compares the T-MSIS estimates to the U.S. Census Bureau’s American Community Survey (ACS). Substantial missing data and/or data that do not line up with ACS estimates raise red flags about data quality. The DQ Atlas combines these two indicators of data quality to generate an overall rating system to alert researchers about the level of data concern. States are grouped into the following categories: low concern, medium concern, high concern, unusable, and unclassified. While many data elements in the DQ Atlas are evaluated using external benchmarks, some are only evaluated on the basis of missingness since not all measures have an external benchmark.
In the 2019 T-MSIS analytic file, over 70% of states (36 of 50 states plus D.C.) had race/ethnicity data categorized as medium concern, high concern, or unusable in the DQ Atlas(Figure 1). Only 15 states’ race/ethnicity data in T-MSIS analytic files were categorized as “low concern” in 2019. The DQ Atlas combines two measures to categorize states into concern categories: 1) missingness of the race/ethnicity variable and 2) alignment with ACS race/ethnicity estimates.
When examining missingness separately, the DQ Atlas finds that missing race/ethnicity data varies widely by state, ranging from 0% to 100% missing, with a national average of 22% missing. Over half of all states, including D.C., (63%) are missing more than 10% of race and ethnicity data (Figure 1).
When comparing separately to the ACS race/ethnicity benchmarks, the DQ Atlas finds that over half of states (55%) have one or more categories of race/ethnicity that are not aligned with race/ethnicity estimates from the American Community Survey (Figure 1). When T-MSIS race/ethnicity differs more than 10 percentage points from ACS race/ethnicity data, it is considered not aligned.
Similar analyses have been conducted by Medicaid and CHIP Payment and Access Commission (MACPAC), one of which identified race and ethnicity data as an area with “ongoing analytical challenges.”
CMS technical instructions note that there may be additional challenges when individuals select multiple races or ethnicity categories. Growing numbers of people are reporting they are “some other race” or “multiracial,” but some states only allow beneficiaries to report a single “multiracial” or “other” category instead of selecting multiple races. People who report more than one race are often grouped into a “multiracial” or “other’ category in reporting, limiting the ability to meaningfully interpret the data. States may also have technical challenges with reporting data to T-MSIS in cases when applicants select multiple races or ethnicities.
Are there other options for evaluating quality of T-MSIS race/ethnicity data?
Researchers can use the DQ Atlas’ categorizations to identify states with low data quality. In some cases, however, this may restrict sample sizes. For example, 15 states, representing approximately 37 million Medicaid beneficiaries, reported race/ethnicity data that were considered of low concern in CY 2019, according to the DQ Atlas (Figure 1). There are several other options to evaluate the quality of T-MSIS race/ethnicity and, in some cases, increase the analytic sample.
Increasing the threshold for missingness for states where T-MSIS data match ACS benchmarks. It may be possible to include states where missing data is slightly above 10% but all race/ethnicity estimates align with ACS reporting. There are eight states with an average of 12% of data missing whose race/ethnicity estimates are considered aligned with the ACS benchmarks (i.e., estimates within 10 percentage points). These states are currently categorized as “medium concern” because their missingness is just above the 10% threshold. However, including data from these states would add 8 additional states, and 17.4 million additional beneficiaries.
Adjusting alignment thresholds for ACS and T-MSIS race and ethnicity estimates. Although some states’ race and ethnicity data are closely aligned with ACS data, they are just above DQ Atlas’ threshold for allowable percentage point difference between estimates (i.e. estimates within 10 percentage points). State-level percent differences in estimate between ACS and T-MSIS vary from 0% to 61.8%, with an average misalignment of 5.6% overall. Slight increases to the allowable thresholds may result in increases to the usable sample. For example, increasing the allowable percentage point difference to 11.0 (from 10 percentage points) would result in four additional states where all race/ethnicity data match ACS benchmarks.
Broadening the definition of usable data. MACPAC, for example, cites that the DQ Atlas data quality categorizations of ‘low concern’ or ‘medium concern’ meet MACPAC’s minimum data standards for analysis. By adopting this approach to include states with low and medium concern data, the number of states that can be included in analyses using disaggregated race/ethnicity data increases to 29 and represents about 63.8 million Medicaid beneficiaries, when using 2019 Release 1 TAF data (users with access to more recent T-MSIS data may show a higher number of states categorized as low or medium concern). For researchers who adopt MACPAC’s approach, it may be helpful to consider the level of misalignment on a state-by-state basis. Specifically, DQ Atlas categorizes states with less than 10% of missing data and two or less misaligned race/ethnicity groups as medium concern. Aside from the definition of misalignment (that is, estimates that differ by at least 10 percentage points), the DQ Atlas does not account for the level of race/ethnicity group misalignment, which varies by up to 61 percentage points.
What information is available for other variables important for disparities and equity research?
T-MSIS analytic files include additional variables that are important for disparities and equity research, though less information is available about state data collection methods. In addition to race and ethnicity, T-MSIS includes beneficiary-level metrics on income, gender, age, primary language, English language proficiency, citizenship, receipt of Supplemental Security Income or Temporary Assistance for Needy Families, zip code, veteran status, and indicators of disability. While information on state data collection procedures for these other variables is more limited, a recent audit of state applications found most states collect primary language information on their applications, and some states also inquire separately about written language.
KFF analysis of CY 2019 T-MSIS analytic files finds wide variation in the magnitude of missing data across key indicators that are also important for equity research (Figure 2). Across all 50 states and D.C., zip code and SSI indicator have relatively low levels of missing data (3% and 10% missing, respectively), whereas other variables, such as English language proficiency and veteran status have very high levels of missing data (91% and 72% complete, respectively).
Looking Ahead
As a major source of health coverage for people of color, Medicaid can play a significant role in helping to address racial and ethnic health disparities. Prioritizing comprehensive and high-quality data on race and ethnicity is important to these efforts. Inadequate data can result in the failure to identify disparities or the implementation of policies that may exacerbate disparities and reinforce structural racism and inequities across the health care system. Most states are engaged in Medicaid initiatives to address racial and ethnic disparities, with some states focusing on racial and ethnic disparities in specific outcomes, like maternal/infant health and behavioral health. High quality and complete data, including measures of health equity, will be key for implementing and assessing the impacts of these efforts.
CMS has identified T-MSIS priority items to guide data quality improvement efforts, some of which include race/ethnicity and other variables. Other federal agencies, such as the Office of Inspector General, are taking notice and launching their own inquiries into data quality issues. States can also take action to improve data quality. An NORC analysis highlighted state efforts that resulted in better data quality and completeness, including expanding race, ethnicity, and language categories; making applications available in various languages and formats (online, phone, paper); using the Medicaid application instructions as an opportunity to explain how the state will use race, ethnicity, and language data to advance health equity to encourage completion of these sections; and linking race, ethnicity, and language data collection to equity-based performance measures. Some states, like California, require that managed care plans participate in filling gaps in race/ethnicity data by requiring health plans to obtain a minimum of 80 percent of enrollee race/ethnicity data. California’s enhanced reporting requirements are tied to financial incentives and penalties, which have resulted in improved race/ethnicity data.
Improvements to the quality of race/ethnicity data and other variables will take time. In the interim, researchers can explore other potential options to increase the usable sample of enrollees in the currently available T-MSIS analytic files. However, each analysis will require thoughtful discussions around data quality, limitations, and whether the data is sufficient for presentation at the state or national level.
A new KFF interactive provides essential facts and trends about spending on Medicare, the federal health insurance program that covers 65 million seniors and people with disabilities, or nearly 1 in 5 Americans.
In 2020, Medicare spending accounted for 12 percent of the federal budget and 20 percent of national health care spending. Given its size and importance, the program is often part of discussions about how to better manage total federal government spending, health care spending in the U.S., and the affordability of health care costs.
The new interactive, The Facts About Medicare Spending, provides the most current information available to help frame these discussions, based on the latest data from Medicare’s actuaries, the Congressional Budget Office, and other government sources. The interactive features information on Medicare enrollment growth, Medicare spending trends overall and per person, growth in Medicare spending relative to private insurance, spending on Medicare benefits and Medicare Advantage, Medicare Part A trust fund solvency challenges, and growth in out-of-pocket spending.
Among the highlights:
In 2020, Medicare benefit payments totaled $769 billion, up from just under $200 billion in 2000. Spending is projected to increase to nearly $1.5 trillion in 2031, due to growth in the Medicare population and increases in health care costs.
The number of Medicare beneficiaries is projected to grow from around 65 million people in 2020 to nearly 93 million people in 2060. The aging population is one factor contributing to higher Medicare spending, since spending per person is higher among older beneficiaries.
Medicare Advantage plans accounted for nearly half of all Medicare spending in 2021, up from just over a quarter in 2011, and the share is expected to keep growing. Payments to Medicare Advantage plans nearly tripled from $124 billion to $370 billion over that timeframe. That number is expected to rise to $801 billion by 2030.
Beneficiaries’ out-of-pocket spending has increased with the rise in Medicare spending. The amount that beneficiaries spend on certain Medicare premiums and deductibles has increased from 15 percent of the average Social Security benefit in 2002 to 19 percent in 2022.
The Medicare Trustees project that there will be enough money in the Part A trust fund to pay for hospital benefits in full until 2026, after which Medicare will be able to pay 91 percent of such costs, unless Congress takes action.
To see the interactive, as well as other data and analyses related to Medicare, visit kff.org
The public health and economic effects of the pandemic continue to affect the well-being of many people living in the United States. Over the course of the pandemic, millions have lost jobs or income and have faced difficulty paying for expenses including basic needs like food and housing. These social and economic challenges affect people’s health and well-being. Federal legislation has provided billions in funding to address the public health crisis of the pandemic and to provide economic support to many low-income people struggling to make ends meet. This brief provides an overview of how adults are faring across an array of measures of social determinants of health as of March 2 – March 14, 2022 based on data from the Census Bureau’s Household Pulse Survey, which was designed to quickly compile data about how people’s lives have been impacted by the coronavirus pandemic. For this analysis, we looked at a range of measures over the course of the pandemic. Unfortunately, the Household Pulse Survey does not provide pre-pandemic measures for comparison. While we have tracked data over time and there have been fluctuations at various points since March 2020, patterns of hardship remain largely consistent and changes in measures do not necessarily follow economic indicators or pandemic trends.
What are social determinants of health?
Social determinants of health are the conditions in which people are born, grow, live, work, and age.1 They include factors like socioeconomic status, education, neighborhood and physical environment, employment, and social support networks, as well as access to health care (Figure 1).
Figure 1: Social Determinants of Health
Though health care is essential to health, research shows that health outcomes are driven an array of factors outside the health care system may play an even larger role in shaping health. Extensive research concludes that addressing social determinants of health is important for improving health outcomes and reducing health disparities.2 Prior to the pandemic there were a variety of initiatives underway to address social determinants of health both in health and non-health sectors. The COVID-19 pandemic has not only disproportionately affected the health of people of color and other high-need groups, but also had disproportionate impacts on economic and social factors.
How are adults faring across a range of social determinants of health during the pandemic?
Across a wide range of metrics, large shares of people are experiencing hardship. Data for the most recent period, March 2 – March 14, 2022, show that (Figure 2):
More than one in eight adults (13.6%) reported that they or someone in their household had experienced a loss of employment income in the past four weeks;
More than six in ten (61.3%) of adults reported at least a little difficulty paying for usual household expenses in the past 7 days, and 31.8% used credit cards or loans to meet household spending needs;
7% of adults had no confidence in their ability to make next month’s housing payment (across renters and owners), and 10.3% reported food insufficiency in their household;
Nearly one in three (31.4%) adults reported symptoms of depression or anxiety.
Black and Hispanic adults fare worse than White adults across nearly all measures, with large differences in some measures. In early March 2022, three quarters of Black and Hispanic adults (74.4% and 75.2%, respectively) reported difficulty paying household expenditures compared to 55.5% of White adults; 9.6% of Black adults and 8.4% of Hispanic adults reported no confidence in their ability to make next month’s housing payment compared to 4.0% of White adults; and 20.4% of Black adults and 16.2% of Hispanic adults reported food insufficiency in the household compared to 7.1% of White adults. Furthermore, nearly a fifth of Black adults, and about one in four Hispanic adults reported living in a household that experienced a loss of employment income in the last four weeks (17.1% and 23.0%, respectively) compared to 10.2% of White adults.
Patterns of hardship over time indicate both the effects of the pandemic and related policies as well as longstanding disparities in social determinants of health. Data indicate that the share of people experiencing depression or anxiety, food insufficiency, loss of employment income, and having no confidence in paying for their housing peaked in December 2020 but have otherwise remained largely stable (data not shown). Notably however, the share of adults having at least a little difficulty paying usual household expenses in the past 7 days has risen significantly from 50.9% in early September to 61.3%. This could potentially be due to rising prices for many household goods. However, differences in rates of hardship among certain populations have been evident throughout the pandemic and to some extent reflect longstanding disparities that existed even before the pandemic.
While variation across age and gender was not as stark, younger adults (ages 18 to 44) fared worse on many measures compared to older adults. For example, higher shares of younger adults reported symptoms of anxiety and depression as well as having a little difficulty paying for usual household expenses. In addition, higher shares of women reported symptoms of depression or anxiety and difficulty paying usual household expenses in the past seven days compared to men.
Across most measures, adults with children in their household fared worse compared to overall adults. For example, 17.5% of adults with children in the household experienced loss of employment income in the household in the last four weeks compared to 13.6% of adults overall, and over two thirds (69.2%) of adults with children in the household reported difficulty paying for household expenses in the past week compared to the overall population of 61.3%. Adults in households with children were also more likely to report food insufficiency, symptoms of depression or anxiety, having no confidence in ability to make next month’s housing payment than the general population, and borrowing from friends or family to meet household spending.
What to watch going forward
Federal legislation provided billions of dollars to help address the ongoing health and economic effects of the pandemic, including direct economic support for individuals. This federal support may have contributed to some improvements in metrics since peaks early in the pandemic. However, some federal funding has expired, and the trajectory and duration of the pandemic is not clear with new variants and surges despite the availability of vaccines. Congress may consider broader legislative proposals that had been part of the Build Back Better Act which could expand health coverage and help to address health disparities across different demographic groups, but the status and outcome of that legislation is uncertain.
The authors thank former KFF Vice President Rachel Garfield and former KFF Senior Data Analyst Kendal Orgera for their role as authors of previous versions of this report.